Chapter 5 - Patterns of Illegal Drug Use - Sage Publications
37
134 CHAPTER 5 Patterns of Illegal Drug Use W hat is known about the use and abuse of illegal drugs, drug treat- ment, and consequences associated with drug use is derived primarily from several large-scale surveys and selected compila- tions of justice and health statistics. Although information on drug use in the United States, Canada, and many European coun- tries is plentiful, data on substance use in other regions of the world, particularly Third World countries, are much scarcer. Available data have enabled researchers to demonstrate that drug use varies signifi- cantly in the population and that it is more common in some populations than in others (i.e., drug use is correlated with certain populations and statuses). Among the correlates of illegal drug use is age, as the use of drugs is much more common in late adolescence and early adulthood than at any other point in the lifecourse. Gender is another important pre- dictor of illegal drug use; males are more likely than females to use illegal drugs. Drug use also varies by race/ethnicity, but in con- trast to what is commonly believed, whites are among the most likely to use illegal drugs. In part, racial and ethnic differences in substance use are a function of differ- ences in social class. Social class is a mea- sure that captures differences in economic prosperity and educational attainment and is another important correlate of drug use. Finally, residence characteristics, such as whether one lives in an urban area as opposed to a small town or rural area, are important for understanding drug use, with levels of illegal drug use generally highest in large cities. The correlates of illegal drug use are the primary focus of this chapter and are dis- cussed in depth below. However, in order to understand research on the correlates of drug use, it is necessary to have a basic understanding of the methods and sources of data used to generate this information. The two most widely used and perhaps the best sources of information on substance use and abuse are the Monitoring the Future Study and the National Survey on Drug Use and Health. Both are large, ongo- ing surveys based in the United States, which have collected data on substance use and abuse for decades. The former is pre- dominately focused on substance use by adolescents, although it also provides infor- mation on adults, while the latter is a house- hold survey focusing mainly on adults, although data on youth aged 12–17 are also included. Surveys of drug use have been conducted in foreign countries, and data sources such as the European School Survey Project on Alcohol and Drugs and the British Crime 05-Mosher.qxd 11/28/2006 5:13 PM Page 134
Transcript of Chapter 5 - Patterns of Illegal Drug Use - Sage Publications

134
C H A P T E R 5Patterns of Illegal Drug Use
W hat is known about the use andabuse of illegal drugs, drug treat-
ment, and consequences associated withdrug use is derived primarily from severallarge-scale surveys and selected compila-tions of justice and health statistics. Althoughinformation on drug use in the UnitedStates, Canada, and many European coun-tries is plentiful, data on substance use inother regions of the world, particularlyThird World countries, are much scarcer.Available data have enabled researchers to demonstrate that drug use varies signifi-cantly in the population and that it is morecommon in some populations than in others(i.e., drug use is correlated with certainpopulations and statuses).
Among the correlates of illegal druguse is age, as the use of drugs is muchmore common in late adolescence and earlyadulthood than at any other point in thelifecourse. Gender is another important pre-dictor of illegal drug use; males are morelikely than females to use illegal drugs. Druguse also varies by race/ethnicity, but in con-trast to what is commonly believed, whitesare among the most likely to use illegaldrugs. In part, racial and ethnic differencesin substance use are a function of differ-ences in social class. Social class is a mea-sure that captures differences in economicprosperity and educational attainment and
is another important correlate of druguse. Finally, residence characteristics, suchas whether one lives in an urban area asopposed to a small town or rural area, areimportant for understanding drug use, withlevels of illegal drug use generally highestin large cities.
The correlates of illegal drug use are theprimary focus of this chapter and are dis-cussed in depth below. However, in orderto understand research on the correlates of drug use, it is necessary to have a basicunderstanding of the methods and sourcesof data used to generate this information.The two most widely used and perhaps thebest sources of information on substanceuse and abuse are the Monitoring theFuture Study and the National Survey onDrug Use and Health. Both are large, ongo-ing surveys based in the United States,which have collected data on substance useand abuse for decades. The former is pre-dominately focused on substance use byadolescents, although it also provides infor-mation on adults, while the latter is a house-hold survey focusing mainly on adults,although data on youth aged 12–17 are alsoincluded.
Surveys of drug use have been conductedin foreign countries, and data sources suchas the European School Survey Project onAlcohol and Drugs and the British Crime
05-Mosher.qxd 11/28/2006 5:13 PM Page 134

Survey provide us with information onpatterns and correlates of substance useoutside the United States. Other key sourcesof information on substance use and abusetarget populations that are of specific inter-est, such as people requiring drug treatmentor those accused of criminal offenses. Onevery useful data source in this area is theArrestee Drug Abuse Monitoring (ADAM)study. There are also sources of informationon drug use that compile data from varioushealth, social service, and justice agencies.One of these is the Drug Abuse WarningNetwork (DAWN), which collects data ondrug-related incidents from emergencyroom physicians and coroners.
Finally, ethnographic studies of druguse that rely on direct observation and/or interviews of drug users and people indrug-related fields provide invaluable dataon drug use and abuse. These data areparticularly useful for examining drug useby populations that may be excluded fromthe data sources mentioned above. Thereare many individual studies of drug use thatemploy ethnographic data, and we draw onthese throughout the book. However, oneongoing source of ethnographic data thatdeserves attention is Pulse Check. PulseCheck collects interview and ethnographicdata on drug use from epidemiologists, fieldresearchers, law enforcement officials, anddrug treatment professionals to provideinformation on drug use from people whodeal with these issues first hand.
Criminal justice data also provide impor-tant information on drug use, drug sales, andthe consequences of these behaviors. Data onarrests and incarcerations for drug offensesare available from organizations such as theBureau of Justice Statistics, but these data aremore focused on the response to drug usethan drug use per se. Therefore, we limit ourdiscussion of these data sources.
We now turn our attention to a discus-sion of the primary sources of data on drug
use, followed by a discussion of the keycorrelates of illegal drug use.
SELF-REPORT SURVEYS
The application of the self-report surveymethod to the study of deviant behaviorbegan in the 1940s and 1950s, and theseearly surveys included measures of sub-stance use (Porterfield, 1946; Short & Nye,1957; Straus & Bacon, 1953). Surveyresearch allowed the study of deviance bygoing “straight to the source” or by askingpeople about their illegal and deviantbehavior. This was an important break-through in the study of crime and devianceand was especially significant for the studyof victimless, though often illegal, behaviorssuch as drug use.
One of the major advantages of the self-report method is that it enables inferencesto be drawn about a general populationbased on a relatively small sample of sub-jects, provided that every person in thepopulation has an equal chance of beingselected for the sample. With a properlydrawn sample, we can examine numerousissues related to drug use with a relativelyhigh degree of accuracy, including whetherthe use of a particular substance is increas-ing or decreasing, demographic differencesin use and abuse patterns, how availableand expensive the drug is on the street,whether treatment resources are availableand adequate for those wanting help, atti-tudes about drugs and drug policy in thegeneral population, and what the conse-quences of use and abuse are.
The flexibility of surveys also allowsthem to be used to examine substanceuse and abuse by those who may be mostlikely to have experience with drugs ordrug-related problems, such as people insubstance treatment centers or prison. Self-report surveys also provide a great deal of
Patterns of Illegal Drug Use 135
05-Mosher.qxd 11/28/2006 5:13 PM Page 135

flexibility in terms of the issues coveredand questions asked. For example, majornational surveys have added questions onthe use and availability of drugs such asmethamphetamine and ecstasy when itbecame clear that these drugs were anissue of growing concern to the public, and questions on the cost of particular drugs have also been added to surveys in the past as one measure of examining thesuccess of interdiction efforts. In sum, thebroad flexibility of surveys, and the factthat they allow us to study large popula-tions relatively cheaply and accurately,makes them an extremely useful tool forsocial research in general and research onsubstance use in particular.
Despite the numerous benefits of theself-report method, there are a number ofissues and limitations to survey researchthat must be considered when interpretingfindings. One major concern with surveyresearch on substance use is that some ofthe people who are most likely to use andabuse illegal drugs are also among the mostdifficult to contact. This problem is com-monly referred to as coverage error, and itcan hamper the ability of a survey to yieldfindings that are generalizable to the entirepopulation (Dillman, 2000). For example,the most widely used sources of informationon substance use by adolescents are basedon middle and high school student popula-tions. Although student-based drug surveysprovide valuable data, because they arebased on student populations they excludehigh school dropouts and are less likely tocapture students with high rates of absen-teeism. This is important because the U.S.Department of Education estimates that10% to 15% of students permanently dropout of school, and dropouts are more likelythan enrolled students to use illegal drugs and alcohol (Johnston, O’Malley, &Bachman, 2003a). Dropouts are also morelikely to use more serious drugs, such as
cocaine and heroin, and to use substancesin more harmful ways (e.g., “daily” use)than are students who remain in school(SAMHSA, 2003e).
Because of these factors, surveys ofstudent populations are likely to underre-port the overall level of substance use andabuse by young people (SAMHSA, 2002e).Further complicating the interpretationof student-based data on drug use is thefact that dropout and absenteeism ratesmay also vary according to other socio-demographic characteristics. For example,Hispanics have been found to have signifi-cantly higher dropout rates at every ageand social class, and because this affectstheir survey participation, it also affects thereported levels of substance use and abusefor this group (Johnston et al., 2003a; U.S.Department of Health and Human Services[DHHS], 2003).
Like surveys on students, general popula-tion surveys are also likely to underestimatelevels of drug use and dependency as aresult of coverage error. For example,household surveys will disproportionatelymiss people who use drugs, especially thosewho use “hard” drugs or are addicted todrugs, because these individuals are morelikely to be homeless or to be living invarious institutions, meaning they will bemissed in samples of households (Ramsay& Partridge, 1999).
Another issue of concern in surveyresearch on drug use is underreporting byrespondents. Underreporting involves the ten-dency of survey respondents to lie, minimize,or fail to answer questions that are perceivedto be “threatening” to the respondent(Aquilino & LoSciuto, 1990). Related tounderreporting is the issue of social desirabil-ity, which is the tendency of respondents toreply to sensitive questions in ways that theybelieve to be more socially appropriate. Forexample, research has found people to be lesslikely to report sensitive and illegal behavior,
DRUGS AND DRUG POLICY136
05-Mosher.qxd 11/28/2006 5:13 PM Page 136

particularly as respondent anonymitydecreases (e.g., answering the question in per-son rather than in an anonymous written sur-vey) or as the respondent feels less in controlof the interview process (Fendrich & Vaughn,1994). These issues are further complicatedby the fact that the underreporting of druguse is likely to vary not only by the surveymode but by a number of sociodemographicvariables and the type of substance as well.For example, underreporting may be higherwhen questions are asked about “harder”drugs such as heroin, cocaine, and metham-phetamine, ostensibly because the additionalstigma (and legal consequences) associatedwith these drugs increases the pressure torespond in socially desirable ways (Fendrich& Vaughn, 1994). Similarly, research hasindicated that members of racial/ethnicminority groups, members of the lower class,and those with lower levels of education maybe more likely to underreport substance useeven when controlling for other relevant vari-ables (Mensch & Kandel, 1988).
Although survey data on drug use there-fore should be regarded with caution, mostresearchers believe these data are reason-ably valid indicators of substance use andabuse and that response validity can be heldto a reasonably high level, provided thesurvey is properly conducted. An exampleof the relatively high validity potential indrug surveys is provided by the drugs com-ponent of the British Crime Survey (BCS),which has previously inserted a fictitiousdrug called “Semeron” into its measures ofdrug use as a validity check. In 1998, 9,988people responded to the BCS, and of these,4% claimed to have ever heard of Semeron,but only four respondents claimed to haveused it in their lifetime and only one respon-dent claimed to have used it in the previousmonth (Home Office, 2001). In sum, thereare limitations to the use of survey data forthe study of drug use and abuse, but thesedata can be extremely valuable, provided
that they are used cautiously and with theirlimitations in mind.
Monitoring the Future
The Monitoring the Future (MTF) studyis perhaps the most commonly used sourceof information on legal and illegal drug useby American adolescents and young adults(Johnston et al., 2003b). With approximately100 questions on substance use, MTF sur-veys address respondents’ use of a variety ofillegal drugs, alcohol, tobacco, psychoactivepharmaceuticals (nonmedical use), andinhalants during the last 30 days (both“daily” use and ever used in last 30 days),the last year, and in their lifetime. In addi-tion to this, MTF includes questions regard-ing the age at first use for various drugs; thefrequency and quantity of use; perceivedavailability of dugs; peer norms regardingdrug use; beliefs about the health and socialrisks associated with drug use; and expectedfuture use of drugs, among other things(Johnston et al., 2003b).
First implemented in 1975, MTF beganas a cross-sectional survey of high schoolseniors alone, but quickly developed into alongitudinal project that has also expandedto include additional age groups. Beginningin 1991, MTF extended their study toinclude 8th and 10th graders, and nowabout 18,000 8th graders from 150 schoolsand 17,000 10th graders from 140 schoolsare surveyed annually (Johnston et al.,2003b). In all, each year the high schoolsample involves approximately 45,000students from about 400 public and privatesecondary schools in the United States.Surveys of 8th and 10th graders areconducted anonymously, but 12th-graderespondents are asked to confidentiallyprovide their names, enabling follow-upsurveys of a random sample of graduatingseniors for a number of years after theirgraduation (Johnston et al., 2003b).
Patterns of Illegal Drug Use 137
05-Mosher.qxd 11/28/2006 5:13 PM Page 137

Longitudinal information collected bythe MTF project began with the graduat-ing class of 1976. Today, from the original15,000 to 17,000 senior respondents thatparticipate in the survey each year, a repre-sentative sample of 2,400 persons is drawnand these individuals are then followed andsurveyed by mail. The longitudinal datacollected by the MTF allow researchers toexamine the association of adolescent sub-stance use with a number of outcomes inlater life, including college enrollment andcompletion, marriage, parenthood, employ-ment, and the use and abuse of substancesin adulthood. The examination of adultsubstance use and abuse by MTF is alsofacilitated by oversampling proceduresdesigned to include adequate numbers
of frequent marijuana users (i.e., “dailyusers”) and serious drug users in the sample(Johnston et al., 2003c).
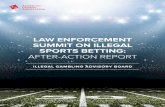
Although the MTF study suffers from thelimitations of school-based surveys discussedabove, it is an excellent source of informa-tion on the prevalence and incidence of sub-stance use by American adolescents. MTFdata are especially adept at monitoring changein substance use over time. As illustrated inFigure 5.1, findings from the MTF surveydemonstrate that the use of illicit drugs byAmerican adolescents decreased significantlyfrom the late 1970s (i.e., several years priorto the beginning of the “war on drugs”) tothe early 1990s. These data indicate that54% of seniors reported some illicit drug usein 1979, but in the years to follow drug use
DRUGS AND DRUG POLICY138
0
10
20
30
40
50
60
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
Year
%
Marijuana Cocaine Crack Heroin
Amphetamines Crystal Meth Hallucinogens Ecstasy (MDMA)
Figure 5.1 Annual Reported Illegal Drug Use by 12th Graders, 1975–2002SOURCE: Data obtained from Johnston, O’Malley, & Bachman (2003b, tables D-2, D-6, D-10, D-16, D-18,D-20, D-24, D-35, D-40).
05-Mosher.qxd 11/28/2006 5:13 PM Page 138

declined steadily, so that by 1992 only 27%reported illicit drug use (half the figure for1979). After 1992, illicit drug use began toincrease, and by 2002, 41% of seniorsreported some illicit drug use in the past year(Johnston et al., 2003b).
Figure 5.1 also illustrates several“spikes” in drug use patterns over time. Forexample, in the 1970s, marijuana useincreased substantially prior to peaking inthe late 1970s and then declining. Similartrends are evident for amphetamine use inthe early 1980s, cocaine and crack cocaineuse in the mid- and late 1980s, and ecstasyand crystal methamphetamine use in thelate 1990s and early 2000s.
Other Surveys onAdolescent Drug Use
Another useful source of informationon adolescent substance use is the YouthRisk Behavior Survey (YRBS). Similar inmany ways to the MTF study, the YRBSis a school-based study that is representa-tive of American students enrolled in the9th through 12th grades. The YBRS is imple-mented biennially by the Centers for DiseaseControl and Prevention, which developed the survey in order to monitor serious healthrisks posed to American adolescents andyoung adults (U.S. Department of Health andHuman Services, Centers for Disease Controland Prevention [DHHS-CDC], 2003a).Substance use is one of six categories of high-risk behavior targeted by the survey and isaddressed by 14 questions on illegal drug useand 16 questions on alcohol and tobacco usein the 2003 survey. Because the YRBS has aparticular focus on issues of risk and health,it examines some things that the MTF studydoes not (DHHS-CDC, 2003b). For example,questions included on substance use and riskin the YRBS address respondents’ frequencyof driving while intoxicated or riding in a carwith an intoxicated driver and whether
substance use was present at their last sexualintercourse. Measures such as these haveenabled researchers to link forms of drug usewith a variety of negative health outcomesincluding accidental death; suicide; unwantedpregnancy; and the transmission of disease,including HIV (Manski, Pepper, & Petrie,2001).
An important source of data on sub-stance use and abuse by adolescents inEuropean countries is the European SchoolSurvey Project on Alcohol and Drugs(ESPAD; Hibell et al., 1999). Examiningroughly 95,000 10th-grade students in 30participating countries, the ESPAD was pat-terned after the MTF survey and is designedto enable comparisons between Europeancountries and the United States. Recentfindings identified by the ESPAD indicatethat European youth are more likely to be current users of tobacco and alcohol, butless likely to be current users of illegaldrugs, compared to youth in the UnitedStates. For example, approximately 17% of10th graders in 30 European nations werefound to have used cannabis in their life-time, as compared to 41% in the UnitedStates (Hibell et al., 1999).
Comparisons of ESPAD data with datafrom the United States indicate that youth in the United States have higher rates of usefor every illicit drug as compared to any ofthe 30 European countries participating inthe ESPAD study. However, adolescents inthe United Kingdom, the Netherlands, theCzech Republic, Estonia, and Poland reportedrates of use for amphetamines, LSD, otherhallucinogens, cocaine, ecstasy, and crackthat were reasonably close to those reportedin the United States (Hibell et al., 1999).
The National Survey onDrug Use and Health
Another key source of information onsubstance use in the United States is the
Patterns of Illegal Drug Use 139
05-Mosher.qxd 11/28/2006 5:13 PM Page 139

National Survey on Drug Use and Health(NSDUH). Formerly called the NationalHousehold Survey of Drug Abuse (NHSDA),the NSDUH is clearly the most representa-tive source of data on drug use in the UnitedStates because it samples from the generalUnited States civilian population aged 12and above. Only 2% of this population isnot represented by the NSDUH, and this ismainly persons who are in the military, cor-rectional facilities, or residential treatmentprograms or persons who are homeless butnot in shelters (Manski et al., 2001).
Drawing an annual sample of roughly70,000 people, the NSDUH includes mea-sures examining the lifetime, past year, andpast month use of tobacco, alcohol, mari-juana, cocaine, crack cocaine, hallucinogens(with separate measures included for PCPand LSD), heroin, inhalants, and thenonmedical use of prescription drugs (withseparate measures included for stimulants,sedatives, tranquilizers, and analgesics)(SAMHSA, 2001). Summary measures arealso provided that examine the use of any
illicit drug and the use of any illicit drugexcluding marijuana (SAMHSA, 2001).Respondents are asked about the age atwhich they were first exposed to and useda particular drug; when they last used aparticular drug; and their perceptions ofthe availability of drugs, the risks associ-ated with drug use, and the behavioral andhealth consequences associated with use.Finally, the NSDUH also collects sociode-mographic data on respondents, includingage, gender, race, educational level, jobstatus, income, and housing situation(SAMHSA, 2002b).
VALIDITY OF SURVEYFINDINGS ON DRUG USE
One way to assess the validity of survey find-ings on drug use is to compare results acrosssurveys when measures allow. As can be seenin Table 5.1, findings on adolescent sub-stance use reported by the NSDUH are verysimilar to those reported by the Monitoring
DRUGS AND DRUG POLICY140
Table 5.1 Comparison of NSDUH and MTF Drug Use Prevalence Rates
NSDUH (Persons aged 18–25) MTF (Persons aged 19–24)
Drug and Usage Percentages 2001 Percentages 2002 Percentages 2001 Percentages 2002
MarijuanaLifetime 53.0 53.8 56.3 56.1Past month — 17.3 19.6 19.8
CocaineLifetime 14.9 15.4 12.4 12.9Past month — 2.0 2.5 2.5
EcstasyLifetime 13.5 15.1 15.0 16.0Past month — 1.1 2.2 1.6
LSDLifetime 16.6 15.9 15.2 13.9Past month — 0.1 1.0 0.4
SOURCE: SAMHSA (2003e).
NOTE: — indicates data not available.
05-Mosher.qxd 11/28/2006 5:13 PM Page 140

the Future study across a number of mea-sures of drug use.
In general, data generated by theNSDUH are excellent for examining theprevalence of drug use in the general popu-lation. As noted, however, one limitationof these data is that they likely underreportthe use of more serious drugs, such asheroin and cocaine, as well as the extent ofdrug problems and dependency. This is dueto the fact that the individuals most likelyto use heroin and cocaine and experiencedrug problems, such as the homeless, arenot covered in household surveys. Despiteits shortcomings, the NSDUH is a well-designed study and the data are widelyused to examine drug use and abuse inAmerica.
OTHER SURVEYSON ADULT DRUG USE
A key source of international data on adultsubstance use is the self-reported drug usecomponent of the British Crime Survey(BCS). The BCS is a large-scale householdsurvey that provides information on experi-ences with crime, victimization, and drug usein England and Wales. First implemented in1982, the BCS now interviews approxi-mately 10,000 respondents between the agesof 16 and 59 annually. The drug-use compo-nent of the BCS includes measures of the life-time, previous year, and previous month use
of cannabis, cocaine, crack cocaine,amphetamines, ecstasy, LSD, “magic mush-rooms,” heroin, methadone (not prescribedby a doctor), tranquilizers, amyl nitrite,steroids, inhalants, and two “catch-all” ques-tions for drug use (Home Office, 2001). TheBCS is the primary source of information ondrug use in the United Kingdom, and thesedata have yielded some very interesting find-ings. For example, data indicate that one-third of respondents acknowledged havingever used an illicit drug, but only 11% hadused in the past year and only 6% had usedin the past month (Home Office, 2001).Other findings, which reflect patterns seen inthe United States, indicate that unemploy-ment is strongly associated with drug use byyoung people, with 40% of unemployedyoung people reporting use in the past yearas compared to 25% for those with jobs(Home Office, 2001).
Another key source of international dataon drug use, of which the BCS is a regularcontributor, is the European MonitoringCenter for Drugs and Drug Addiction(EMCDDA). The EMCDDA developedwhen many countries in the European Unionagreed that it made little sense to focus solelyon drug use and policy in their own countryto the neglect of those around them.According to the EMCDDA (1997), “themultifaceted and changing nature of illicitdrug use, and its intercontinental andEuropean character, imply that it tran-scends political, economic, and geographical
Patterns of Illegal Drug Use 141
Underreporting is always a concern in survey research on drug use, but alternative methodsof measuring drug use may be even more problematic. One example of this is a recent studythat estimated cocaine use in Italy by measuring the presence of benzoylecgonine, a urinarybyproduct of cocaine that has no other source, in a local river. Using water samples collectedfrom the Po River and waste treatment facilities in the cities located along the river,researchers concluded that the levels of benzoylecgonine in the water indicated that approx-imately 27 in 1,000 young people in the region were daily cocaine users, a rate which farexceeded the estimates derived from official surveys (Zucatto et al., 2005).
05-Mosher.qxd 11/28/2006 5:13 PM Page 141

boundaries” (p. 3). In recognition of this, theEMCDDA examines drug use and problemsacross several countries by collecting exist-ing national survey data and comparingcross-nationally where possible (EMCDDA,2002b). As it was initiated only recently,the EMCDDA is still developing, and onlycertain countries have provided data that are sufficiently uniform to allow for cross-national comparisons. As of 2002, the coun-tries providing data suitable for comparisonare England and Wales, Spain, Germany,and Greece. However, several other coun-tries, including Denmark, Finland, Ireland,Italy, and Portugal, are expected to submitcomparable data soon, and other countriesare expected to participate in the more dis-tant future (EMCDDA, 2002b).
Among the cross-national analysesreleased by the EMCDDA is a comparisonof cannabis use by birth cohorts in Germany,Greece, and Spain from 1938–1982 (Kraus& Augustin, 2002). Results of this studyindicated that the percentage of people whoreport ever using cannabis has increasedsubstantially over time, but that the patternof increase has varied by country. Forexample, sharp increases in use were seen inSpain in the 1970s, and similar increaseswere seen in the 1990s in Germany. Theaverage age for first use of cannabis also var-ied: 18 in Germany and Spain but 20 inGreece. Across all three countries, age wasfound to be a key protective factor becauseafter the age of 25 very few people willinitiate the use of cannabis (Kraus &Augustin, 2002).
Another interesting study that employedEMCDDA data examined cannabis use inthe general populations of England andWales, Germany, Spain, and Greece. Korfand Benschop (2002) found cannabis usepatterns to have increased substantially ineach of these countries in the last fourdecades, with the most pronounced changeoccurring in the new federal states of
Germany, where cannabis use rapidlyincreased with the fall of the Berlin Wall.
DATA ON SUBSTANCE USEBY ADULT OFFENDERS—ADAM AND I-ADAM
The data sources described above aredesigned to examine substance use in the gen-eral population, and as a consequence, theymiss certain “high risk” populations. This isimportant because data on high-risk popula-tions (e.g., criminal offenders) are essentialfor a complete understanding of drug use and its consequences. A particularly valuablesource of information for examining theseissues is the Arrestee Drug Abuse Monitoring(ADAM) program, which collects self-reported information on drug use by recentarrestees. ADAM grew out of the Drug UseForecasting (DUF) program, which wasdeveloped by the National Institute of Justice(NIJ) in 1987 to provide information aboutillegal drug use among persons who had beenarrested (Manski et al., 2001). AlthoughDUF was “virtually the only source of con-tinuous information on drug use within anoffender population,” serious problems withits sampling procedures resulted in therestructuring of the DUF program into theADAM program in 1997 (p. 84).
Unfortunately, the collection of newdata by the ADAM program was discontin-ued by the NIJ in January 2004, but in2002, 35 sites provided data to the pro-gram, reporting on over 30,000 adult male,10,000 adult female, and 3,000 juvenilearrestees (ADAM, 2003b). As with the DUFprogram that preceded it, the ADAM pro-gram uses trained interviewers to administera structured questionnaire to arresteeswithin 48 hours of the individual arrivingin a booking facility, and also collects aurine specimen from the arrestee, enablingverification of the self-reported drug use.
DRUGS AND DRUG POLICY142
05-Mosher.qxd 11/28/2006 5:13 PM Page 142

Interview participation rates are quite highin the ADAM program, with more than80% of approached arrestees agreeing to beinterviewed (ADAM, 2003a). Numeroustopics are addressed by ADAM surveys,with arrestees asked which drugs they usedand how often they used them, their age atfirst use of each substance, what their hous-ing situation was in the previous year, howthey supported themselves, whether theyhad health insurance, and how and wherethey purchased their drugs. There are alsomeasures addressing the respondents’ men-tal health and any heavy use of alcohol anddrugs, which might be useful in developingtreatment programs. Basic demographic dataon the subjects are also collected.
A distinguishing component of theADAM data is that following the interviewstage, subjects are asked to voluntarily pro-vide a urine sample, which can then be usedto verify self-reported substance use and esti-mate levels of over- or underreporting. TheADAM urinalysis can detect 10 differentdrugs, but focuses on the so-called NIDA-5,or the five most commonly used illegal drugsas identified by the National Institute ofDrug Abuse: marijuana, cocaine, metham-phetamine, opiates, and phencyclidine (PCP)(ADAM, 2003a). ADAM protocol requiresthat arrestees be interviewed and testedwithin 48 hours of their booking because allof the NIDA-5 drugs that ADAM tests for,with the exception of marijuana, remaindetectable in the urine for no more than threedays following ingestion (marijuana remainsdetectable for up to 30 days). The validity ofADAM data is bolstered by the fact that the vast majority of arrestees who agree to be interviewed also agree to provide a urinesample. For example, a recent ADAM reportindicated that 34 of 35 sites reported urinal-ysis completion rates above 80%, with ratesranging from a respectable 74.7% in Albany,NY to as high as 97.9% in Oklahoma City,OK (ADAM, 2003a).
In addition to their ability to assess thevalidity of self-reported drug use throughurinalysis, ADAM data provide valuableinformation on the extent of substance useby known offenders. A key finding identi-fied through the use of ADAM data is thata majority of male arrestees used at leastone of the NIDA-5 drugs shortly before theirarrest, with figures ranging from 52.2% ofarrestees in Anchorage, Alaska to 79.9% inNew York (ADAM, 2003a). These datahave also been used to examine change indrug use patterns over time and to demon-strate differences in the use of particularsubstances by region. One example of thisis that a significant portion of arresteestested positive for methamphetamineuse in certain cities—including 35.9% inHonolulu, Hawaii and 29.3% in Sacramento,California—but in Eastern cities, almostno arrestees tested positive for the drug.Indeed, of the 13 ADAM sites located eastof the Mississippi River, the city with thehighest percentage of arrestees testingpositive for methamphetamine use wasCharlotte, NC, with 1.4%, and in Albany,Chicago, Detroit, Fort Lauderdale, Miami,and Philadelphia there were no arresteeswho tested positive for methamphetaminein 2002 (ADAM, 2003a).
In recognition of the increasingly globalnature of the drug trade, the NationalInstitute of Justice launched the InternationalArrestee Drug Abuse Monitoring (I-ADAM)program in 1998 (ADAM, 2002). Efforts atunderstanding substance use across nationalborders are often confounded by the factthat laws, penalties, and recording proce-dures vary greatly depending upon thecountry in question. I-ADAM attemptedto address this problem by implementinga common survey, similar to the ADAMsurvey used in the United States, in anumber of different countries. Australia,Chile, England, Malaysia, Scotland, SouthAfrica, the Netherlands, Taiwan, and the
Patterns of Illegal Drug Use 143
05-Mosher.qxd 11/28/2006 5:13 PM Page 143

United States all participated in the I-ADAMprogram at some point, and these data haveenabled international comparisons of sub-stance use among arrestees (ADAM, 2002).
DRUG ABUSE WARNINGNETWORK STATISTICS
Another valuable source of official infor-mation on substance use and abuse is theDrug Abuse Warning Network (DAWN).DAWN provides data on drug-related emer-gency department (ED) visits and deathsthat are related to substance use by collect-ing data from hospitals and coroners/medi-cal examiners. So, unlike the data sourcesdescribed above, DAWN data are aimed atinvestigating negative health outcomes asso-ciated with drug use.
The DAWN program recently revisedits data collection procedures and, as a result,DAWN data collected in 2003 and after arenot comparable with data obtained priorto 2003 (SAMHSA, 2005b). Currently,DAWN collects emergency department dataon all persons who have received treatmentin the emergency department of a hospitalsampled by DAWN for a problem that thehospital medical staff determined was relatedto drug use. Information is also provided onthe specific condition that prompted thedrug-related visit, such as whether the indi-vidual came to the emergency departmentas the result of a drug overdose, suicideattempt, or an adverse reaction to pharma-ceuticals (SAMHSA, 2003d).
Drug-related incidents are reported byDAWN if they involve one or more of thefollowing drug categories:
• Illicit drugs• Prescription and over-the-counter
medications• Dietary supplements• Non-pharmaceutical inhalants
• Alcohol in combination with any of thedrugs mentioned above
• Alcohol alone for patients aged 21 andolder
Emergency department data reported byDAWN are also grouped into drug episodesand drug mentions, due to the fact that alco-hol and up to six other drugs can be includedon the report corresponding to a single emer-gency room visit. A drug episode is definedas “an [emergency department] visit thatwas induced by or related to the use of anillegal drug(s) or the non-medical use of alegal drug,” while a drug mention “refers toa substance that was recorded (‘mentioned’)during a drug-related episode” (SAMHSA,2003e, p. 25). As a result of these recordingprocedures, findings reported by DAWNinclude many more mentions than episodes,and this tends to artificially inflate the levelof drug-related health problems reported.
In addition to data on drug-relatedemergency room visits, data on deaths thatare either directly or indirectly related tosubstance use are collected by DAWN fromparticipating medical examiners and coro-ners across the country (SAMHSA, 2005b).Using the same drug categories employedfor the collection of ED data (mentionedabove), drug-related deaths are tabulated byDAWN under the following categories:
• Suicide• Homicide by drugs• Adverse reaction to medication• Overmedication• Accidental ingestion• All other accidental• Could not be determined
Recent findings reported by DAWNindicate that legal drugs were involved infar more emergency department visits thanillegal drugs. As can be seen in Figure 5.2,in 2002, psychotherapeutic drugs (e.g.,
DRUGS AND DRUG POLICY144
05-Mosher.qxd 11/28/2006 5:13 PM Page 144

antidepressants), alcohol in combinationwith some other substance, and painkillersrepresented three of the four leading causesof drug-related emergency department visits,being mentioned in over 621,000 cases.
A crucial factor to consider when usingDAWN data is that they examine only onekey consequence of drug use and abuse:health-related problems that result in anemergency department visit and/or death.Thus, DAWN data measure “events”(emergency department incidents anddeaths), which can tell us about drug-related problems such as overdose (particu-larly among high-risk populations) but notabout drug use in the general population.Only a small fraction of drug users everwind up in an emergency department for adrug-related problem, so these data are inno way representative of drug use in the
general population. Further, a single indi-vidual may wind up in an emergencydepartment several times in a year for adrug-related problem, a situation that isprobably most likely among certain (again,nonrepresentative) populations such as drugaddicts. As each of these emergency depart-ment visits would be recorded without anymention that the visits involved the sameperson, they can only be used to estimatethe incidence of drug-related emergencydepartment episodes, not the prevalence ofsuch events.
An additional issue to consider is thatDAWN data focus on acute drug-relatedproblems (e.g., overdose) and not thechronic types of drug-related medical prob-lems (e.g., cancer, cirrhosis) that are morelikely to be generated by legal drugs such asalcohol and tobacco (Faupel et al., 2004).
Patterns of Illegal Drug Use 145
0
10,0
00
20,0
00
30,0
00
40,0
00
50,0
00
60,0
00
70,0
00
80,0
00
90,0
00
100,
000
110,
000
120,
000
130,
000
140,
000
150,
000
160,
000
170,
000
180,
000
190,
000
200,
000
210,
000
220,
000
Number of Emergency Department Visits
Psychotherapeutics*
Alcohol-in-combination
Cocaine
Painkillers
Marijuana
Heroin
Amphetamines
Methamphetamine
PCP
Ecstasy
GHB
Figure 5.2 Emergency Department Visits by Drug Mention, United StatesSOURCE: SAMHSA (2003b).
NOTE: Psychotherapeutics include the antidepressants, antipsychotics, anxiolytics, sedatives and hypnotics, andCNS stimulants.
05-Mosher.qxd 11/28/2006 5:13 PM Page 145

Finally, there are several factors likely toinfluence whether a person who is experi-encing a drug-related health problemseeks medical help at an emergency depart-ment, including whether the individual hasinsurance coverage, what his or her educa-tional level is, and his or her proximity toa hospital. Thus, it is important for thosewho use DAWN data to interpret these datacautiously and with an awareness of theselimitations.
PULSE CHECK
Quite distinct from the data sources discussedabove is Pulse Check, published by the Officeof National Drug Control Policy (ONDCP)since 1992. Pulse Check is unusual in that itcollects ethnographic information and inter-view data from a variety of sources workingin diverse areas of the drug-use field and com-piles and synthesizes this information into asingle semi-annual report. For example, in2002, Pulse Check was based on one-hourinterviews with 78 epidemiologists, ethnogra-phers (researchers who spend extensive timein “the field” studying drug use first hand),law enforcement officials, and drug treat-ment providers located throughout theUnited States (ONDCP, 2002d). WhilePulse Check results cannot be taken as repre-sentative of the United States, in part becausesites were not randomly selected, the roughly20 cities that currently participate are quitediverse in terms of region, size, and demo-graphic composition.
The diversity of cities studied by PulseCheck increases confidence in the findingsand enables researchers to examine trendsand differences in drug use and abuse byregion and city. This is interesting, given thefact that certain drugs appear to be concen-trated in particular regions. For example,in 2002, Pulse Check found metham-phetamine to be considered “the most
serious drug problem” in Western andMidwestern cities such as Honolulu, HI,Billings, MT, and Sioux Falls, SD, but thedrug is hardly mentioned in interviews withPulse Check representatives in Southern andNortheastern cities.
Consistent with the ethnographicapproach, Pulse Check data are moredescriptive in nature, asking experts aboutdrug use, emerging drug problems, the avail-ability of different drugs, changes in need/demand for treatment, and drug-relatedcrime, among other topics. Respondents arealso asked about their experiences with drug-related issues in terms of the age, gender, andrace/ethnicity of drug users and sellers.
One interesting finding from a recentPulse Check report is that purchasing illegaldrugs appears to be much easier in somecities than in others. This issue was exam-ined by interviewing undercover police anddrug users about how easy they believed itwas to buy illegal drugs. Often, police anddrug users agreed on how difficult it was tobuy drugs, but sometimes they differed sig-nificantly. For example, ranking the diffi-culty of obtaining a substance from 0–10,with 10 representing “extremely difficult,”undercover police in Boston ranked accessi-bility to methamphetamine as 4, while usersranked it as extremely inaccessible, with a10. Conversely, in Detroit, police rankedaccessibility to cocaine as 8, while usersthought it to be much more accessible,ranking it with a 3. These differences are interesting and may be useful to policy makers in evaluating drug controlstrategies.
Findings from Pulse Check are useful interms of their simplicity, timeliness, andability to incorporate the perspectives ofdifferent professionals in the drug field. Asthe name indicates, these data are designedto keep a finger on the “pulse” of the drugproblem, and they tap information thatwould otherwise be unavailable. It is clear
DRUGS AND DRUG POLICY146
05-Mosher.qxd 11/28/2006 5:13 PM Page 146

that these data provide a unique perspectiveand are rich in detail, but they are less adeptat providing representative information on the prevalence and incidence of drug usein large populations. Accordingly, they arebest used in conjunction with broad sourcesof data such as NHDUH.
The data sources discussed above enableus to examine both legal and illegal sub-stance use. It is important to note that thereare significant differences between thesedata sources that must be considered inorder to properly interpret findings fromstudies using these sources. For example,some sources of data focus on adults, whileothers target high school students, and somedata sources don’t examine drug use in thegeneral population at all, but focus on drug-related incidents such as arrests or healthproblems resulting from drug use. Each ofthese data sources is valuable and providesa unique contribution to our knowledge ofsubstance use, but data must be interpretedcarefully because the specific focus andmethodology behind each data source has agreat deal to do with the findings reported.This caution should be kept in mind as weuse these data to examine the patterns andcorrelates of illegal drug use.
CORRELATES OFILLEGAL DRUG USE
The data sources discussed above enableresearch on several sociodemographic factorsthat are associated with illegal drug use.Important correlates of drug use includeage, gender, race/ethnicity, social class, andresidence characteristics such as urbanity.In our discussion of the correlates of druguse we will predominately rely on informa-tion provided by general population drugsurveys (MTF, NSDUH), although weinclude findings from ADAM, DAWN, andother sources where appropriate. Research
findings on the correlates of drug useillustrate that there is significant variationin the use of both legal and illegal drugs, withsome populations being much more likelyto use drugs and to experience negativeconsequences associated with use.
Age
The relationship between age and illegaldrug use varies somewhat depending uponthe data source and type of substance, butdrug use is typically highest in late adoles-cence and early adulthood. Illegal drug useremains relatively common through themid-twenties, but patterns of use tend todecrease rapidly as people age into middleand late adulthood (see Figure 5.3).
As can be seen in Tables 5.2 and 5.3,adolescence represents a time during whichillicit drug use increases rapidly, but it isduring early adulthood that illegal druguse is at its highest. In our discussion of thetheoretical explanations for substance use,we examined some of the reasons for this.However, one key reason for these rela-tively high use patterns during adolescenceand early adulthood is the independence ofusers during this time period. During thisperiod of the lifecourse, people are rela-tively free from the constraints and res-ponsibilities that inhibit drug use. Foradolescents, this is a period during whichthere is typically less and less time spentwith family, which generally acts as a pro-tective factor against substance use, andan increasing amount of time spent withpeers, which is generally a risk factor forsubstance use (Hoffman, 1994). This gen-eral lack of attachments and responsibili-ties, which serve to occupy time, mayalso be important for substance use due tothe boredom that may potentially result.Recent research from Columbia University’sNational Center on Addiction and SubstanceAbuse indicates that boredom plays a key
Patterns of Illegal Drug Use 147
05-Mosher.qxd 11/28/2006 5:13 PM Page 147

role in substance use among adolescents,with those who reported being “frequentlybored” 50% more likely to get drunk anduse illegal drugs (National Center onAddiction and Substance Abuse, 2004).
Similarly, for young adults, many ofwhom are enrolled in college, this agetypically represents a time of independencefrom parental authority and a relative lackof serious commitments such as a family orcareer. A relative abundance of free time,living on one’s own, meeting new peoplethrough education or work, and generallyexperiencing life as an adult for the firsttime tends to encourage experimentationwith a variety of things, including the use of illegal drugs (Schulenberg, O’Malley,Bachman, Johnston, & Laetz, 2004). Theexperimental use of substances amongyoung people is very common, and perhapsexperimentation, at this point in the life-course, should not be viewed as necessarilyor inevitably bad or harmful. Althoughresearch has concluded that the abuse
of psychoactive substances, both legal andillegal, may pose serious risks to healthand well-being, limited experimental usemay also serve some positive functions.For example, research has concluded thatexperimental substance use during lateadolescence may be constructive in thedevelopmental process, particularly in rela-tion to peer bonding, independence, andidentity experimentation (Schulenberget al., 2004).
Regardless, the use of legal and illegaldrugs is most prevalent during early adult-hood, but use declines as people age intotheir middle and late twenties and con-straints on time and behavior becomeincreasingly prevalent. In the mid- and latetwenties, people often graduate from col-lege, move on to more serious career-trackjobs, get married, have children, and spendless time socializing with friends. All ofthese factors have a preventative effect onsubstance use (Hirschi, 1969; Kandel,1980) and are important in understanding
DRUGS AND DRUG POLICY148
0
5
10
15
20
25
30
35
40
45
%
12 13 14 15 16 17 18 19 20 21 22 23 24 25
26–3
0
31–3
4
35–3
9
40–4
4
45–4
9
50–5
4
55–5
9
60–6
4
65+
Age
Figure 5.3 Illicit Drug Use in the Past Year by AgeSOURCE: SAMSHA (2003e).
05-Mosher.qxd 11/28/2006 5:13 PM Page 148

the relatively low and declining patterns ofillegal drug use through middle adulthoodand the later lifecourse.
An interesting paradox regarding ageand drug use is that while adolescents andyoung adults are much more likely to useillegal drugs, they are far less likely thanolder users to experience serious health-related problems with drug use. Forexample, data collected by the Drug AbuseWarning Network (DAWN) on the morethan 670,000 drug-related visits to hospitalemergency departments in 2002 indicatethat only 30% of drug-related emergencydepartment intakes were for persons aged25 and younger, with almost 50% of allemergency department visits involvingpersons who were aged 35 and older(SAMHSA, 2003c). Deaths due to drug useare even more likely to occur among older
populations, which, again, make up a muchsmaller portion of all drug users. Of themore than 1,600 drug-related emergencydepartment fatalities reported to DAWN in2002, over 70% involved persons aged 35and over and approximately 35% involvedpersons who were at least 45 years of age(SAMHSA, 2003c).
Another interesting finding on age andsubstance use is that there is a resurgence ofsubstance use and abuse among the elderly.Substance use problems among the elderlyare somewhat distinct, in that they almostuniversally involve the abuse of alcoholand/or prescription drugs, with illegal druguse being very rare. Substance use and addic-tion among the elderly has been regarded asan “invisible epidemic” by some (Levin &Kruger, 2000) and is apt to be increasinglyproblematic in the future because the number
Patterns of Illegal Drug Use 149
Table 5.2 Percentages Reporting Past Year Illegal Drug Use, by Age
8th Grade 10th Grade 12th Grade College 19–28 Years
Drug 2001 2002 2001 2002 2001 2002 2001 2002 2001 2002
Marijuana/hashish 15.4 14.6 32.7 30.3 37.0 36.2 35.6 34.7 29.2 29.3
Hallucinogens 3.4 2.6 6.2 4.7 9.1 6.6 7.5 6.3 5.4 4.7
LSD 2.2 1.5 4.1 2.6 6.6 3.5 4.0 2.1 3.4 1.8
PCP — — — — 1.8 1.1 — — 0.6 0.3
MDMA (ecstasy) 3.5 2.9 6.2 4.9 9.2 7.4 9.2 6.8 7.5 6.2
Rohypnol 0.7 0.3 1.0 0.7 0.9 1.6 — — — —
GHB 1.1 0.8 1.0 1.4 1.6 1.5 — 0.6 — 0.8
Ketamine 1.3 1.3 2.1 2.2 2.5 2.6 — 1.3 — 1.2
Cocaine 2.5 2.3 3.6 4.0 4.8 5.0 4.7 4.8 5.8 5.9
Crack 1.7 1.6 1.8 2.3 2.1 2.3 0.9 0.4 1.3 1.0
Amphetamines 6.7 5.5 11.7 10.7 10.9 11.1 7.2 7.0 5.8 5.9
Methamphetamine 2.8 2.2 3.7 3.9 3.9 3.6 2.4 1.2 2.8 2.5
Crystal meth (“ice”) — — — — 2.5 3.0 0.6 0.8 1.1 1.4
Heroin 1.0 0.9 0.9 1.1 0.9 1.0 0.4 0.1 0.5 0.2
Other narcotics — — — — 6.7 7.0 5.7 5.9 5.0 5.1
SOURCE: Adapted from Johnston et al. (2003c, Table 2–2, pp. 39–44).
NOTE: — indicates data not available.
05-Mosher.qxd 11/28/2006 5:13 PM Page 149

of substance abusers over the age of 50 isexpected to double between 1999 and 2020(Korper & Council, 2002).
Increased substance use and abuse inold age is consistent with many of theexplanations for substance use discussedabove. Similar to the young, senior citizenstypically have a great deal of free timebecause retirement has often relieved themof employment commitments. For most,their children have grown up and left thehouse, and if the individual then suffers anillness or the loss of a spouse, this mayfurther isolate him or her and result inincreased time spent alone and detachmentfrom society in general. Significant lifechanges in late adulthood, particularlythose that are traumatic, may encouragesubstance use and abuse in a variety of
ways. For example, research has indicatedthat following retirement or the loss of aspouse, individuals may abuse substancesbecause of the despair they feel over theunwanted life change, due to their inabilityto manage unstructured free time, or somecombination of these factors (Benshoff,Harrawood, & Koch, 2003).
As noted, substance use by geriatricpopulations is expected to increase substan-tially in the future as members of the “babyboomer” generation move into their senioryears. In the 20 years following WWII,more than 77 million babies were born inthe United States and consequently, recordnumbers of people will turn 65 in the nextdecade. This has important implications interms of substance use and treatment as thiscohort came of age in the 1960s when
DRUGS AND DRUG POLICY150
Table 5.3 Percentages Reporting Past 30-Day Illegal Drug Use, by Age
8th Grade 10th Grade 12th Grade College 19–28 Years
Drug 2001 2002 2001 2002 2001 2002 2001 2002 2001 2002
Marijuana/hashish 9.2 8.3 19.8 17.8 22.4 21.5 20.2 19.7 16.7 16.9
Hallucinogens 1.6 1.2 2.1 1.6 3.3 2.3 1.8 1.2 1.2 0.9
LSD 1.0 0.7 1.5 0.7 2.3 0.7 1.0 0.2 0.7 0.3
PCP — — — — 0.5 0.4 — — 0.0 0.1
MDMA (ecstasy) 1.8 1.4 2.6 1.8 2.8 2.4 1.5 0.7 1.8 1.3
Rohypnol 0.4 0.2 0.2 0.4 0.3 — — — — —
GHB — — — — — — — — — —
Ketamine — — — — — — — — — —
Cocaine 1.2 1.1 1.3 1.6 2.1 2.3 1.9 1.6 2.2 2.2
Crack 0.8 0.8 0.7 1.0 1.1 1.2 0.1 0.3 0.4 0.3
Amphetamines 3.2 2.8 5.6 5.2 5.6 5.5 3.3 3.0 2.4 2.5
Methamphetamine 1.3 1.1 1.5 1.8 1.5 1.7 0.5 0.2 1.0 1.0
Crystal meth (“ice”) — — — — 1.1 1.2 0.1 0.0 0.4 0.5
Heroin 0.6 0.5 0.3 0.5 0.4 0.5 0.1 0.0 0.3 *
Other narcotics — — — — 3.0 3.1 1.7 1.6 1.7 1.7
SOURCE: Adapted from Johnston et al. (2003c, Table 2-2, pp. 39–44).
NOTE: — indicates data not available.
* Less than .05% but greater than 0%.
05-Mosher.qxd 11/28/2006 5:13 PM Page 150

illegal drug use was more common and atti-tudes towards drug use were more lenient.Research has found that baby boomers havemaintained a comparatively liberal attitudetoward drug use as they have aged (particu-larly when compared to cohorts who cameof age in the 1950s), and this more liberalattitude is likely to result in higher levels ofsubstance use by this group in their senioryears (Patterson, Lacro, & Jeste, 1999).
Gender/Sex
In general, males are more likely to useand abuse illegal drugs than are females,although the magnitude of the gender gapvaries over time, by substance, and also bythe point in the lifecycle (Kandel, 1980). Ascan be seen in Figures 5.4 and 5.5, patternsof illegal drug use by gender are very similarover time, indicating that many of the samefactors influence drug use by adolescent
males and females. Boys are more likely toreport first drug use at younger ages, but bylate adolescence, illegal drug use is relativelysimilar for males and females for most sub-stances (DHHS-CDC, 2003b; Johnston et al.,2003c). As illustrated in Table 5.4, dataindicate that across several different illegaldrugs, use in the past year is virtually identi-cal for adolescent boys and girls (SAMHSA,2003b). However, the similar use patternsevidenced in adolescence quickly change as people age into adulthood. For example,looking at the findings on cocaine usereported in Table 5.4, there are virtually nogender differences during adolescence, but inyoung adulthood men become considerablymore likely to use cocaine, and for adultsaged 26 and over, men are nearly three timesas likely to use the drug.
The fact that the gender gap in illegal druguse becomes increasingly pronounced withage may be, in part, because the social stigma
Patterns of Illegal Drug Use 151
0
10
20
30
40
50
6019
75
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
Year
%
Male Female
Figure 5.4 Annual Reported Marijuana Use, 12th Graders, by Gender, 1975–2002
SOURCE: Johnston et al. (2003b).
05-Mosher.qxd 11/28/2006 5:13 PM Page 151

DRUGS AND DRUG POLICY152
0
5
10
15
20
25
30
35
4019
75
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
Year
%
Male Female
Figure 5.5 Annual Reported Use of Illicit Drugs Other Than Marijuana, 12th Graders, byGender, 1975–2002
SOURCE: Johnston et al. (2003b).
Table 5.4 Percentages Reporting Past Year Drug Use by Age Category and Gender, 2002
Drug and Sex Age 12–17 Age 18–25 Age 26 and Older
Marijuana
Male 16.3 33.8 9.6Female 15.2 25.7 4.7
Any illicit drug
other than marijuana
Male 13.3 22.4 7.0Female 13.7 18.0 5.1
Cocaine
Male 2.1 8.4 2.8Female 2.0 5.1 1.0
Hallucinogens
Male 4.0 9.9 0.9Female 3.7 7.0 0.4
SOURCE: SAMHSA (2003e).
05-Mosher.qxd 11/28/2006 5:13 PM Page 152

and perceived consequences associated withsubstance use become more salient forwomen than men as age increases. Indeed,womengenerallyviewsubstanceuseand abusemore negatively, seeing it as more risky, andreport being less tolerant of it as compared tomen (Kauffman, Silver, & Poulin, 1997). Thisis not surprising given the distinctly differentways in which males and females are typicallysocialized. Specifically, men are expectedto be more self-reliant, risk-taking, andassertive, while women have traditionallybeen expected to be more nurturing and def-erential. Societal institutions such as thefamily, education, the economy, and religion,as well as everyday interpersonal interaction,reinforce these social norms and influencegender differences in virtually all forms ofsocial behavior, including substance use(Ensminger & Everett, 2001).
The use of psychoactive substances forpleasure or recreational purposes seemsespecially contrary to the “traditional femalerole,” particularly as it relates to mother-hood. Because of this, substance use is lesslikely to be tolerated for women than formen (Ensminger & Everett, 2001; Lemle &Mishkind, 1989). Conversely, substance useand even abuse by males is more likely to beexcused as “boys being boys,” and researchhas found men to be more likely to reportusing drugs for recreational purposes(Ensminger & Everett, 2001). Thus, the factthat drug-using behavior is much more simi-lar for males and females in adolescence thanlater in the lifecourse is perhaps due to thefact that, for females, the perceived andactual consequences of drug use are relativelyminor during adolescence as compared toadulthood.
However, it is important to note that evenduring adolescence, boys are much morelikely than girls to use drugs in the ways mostlikely to generate problems. This includes theheavy or daily use of alcohol and illegaldrugs, the use of certain “hard” drugs, or
the use or sale of alcohol and illegal drugson school property (DHHS-CDC, 2003b;Robbins, 1989). These measures may reflectthe general tendency of women to be moreconservative about substance use even duringadolescence, when gender differences aresmallest. As age increases, the socialconsequences of drug use increase for bothmen and women, but consequences becomemore severe for women, and thus the gendergap in illegal drug use becomes morepronounced.
Patterns of drug use by gender can bemisleading if substance use is only consid-ered in terms of illegal drugs. For example,research has found women to be more likelyto use and abuse legal, medically prescribedpsychoactive drugs, ostensibly for ther-apeutic purposes such as the relief of mentaldistress (Ensminger & Everett, 2001;Merline, O’Malley, Schulenberg, Bachman,& Johnston, 2004). These gendered motiva-tions for drug use may be important becauseperhaps the only difference between takingValium to “relieve mental distress” and hav-ing some drinks with the guys after work “toblow off steam” is that the behaviors arethought to be more, or less, socially appro-priate for one gender or the other. Perhapswomen, particularly later in the lifecourse,are more likely to abuse pharmaceuticals ascompared to other drugs because placingtheir substance use/abuse in a medical con-text gives it a degree of legitimacy, and thusenables them to conform more closely tosocietal expectations of femininity.Accordingly, gender differences in substanceuse may be more likely to involve the typeand pattern of substance use rather than the general tendency to use consciousness-altering substances per se.
Race/Ethnicity
Similar to the variation in illegal drug useacross age and gender, there are substantial
Patterns of Illegal Drug Use 153
05-Mosher.qxd 11/28/2006 5:13 PM Page 153

differences in the use of illegal substancesamong racial/ethnic groups. Our focus inthis section is on the five major ethnicgroups in the United States: whites, blacks,Hispanics, Native Americans, and Asianand Pacific Islanders. However, we under-stand that significant heterogeneity existswithin each of these groups and that this diversity has important implications.Accordingly, where available data allow,we discuss within-group differences in druguse as well.
A common misperception is that blacksand Hispanics are more likely to use illegaldrugs than are whites, but extensiveresearch has demonstrated that this is notthe case. Indeed, the most striking findingidentified regarding racial/ethnic differencesin drug use is the consistently low patternsof use reported by African Americansthrough adolescence and young adulthood(see Figure 5.6). Excepting Asians, amongadolescents and young adults, AfricanAmericans are the group least likely toreport nearly all forms of drug use(Bachman, Wallace, O’Malley, Johnston,
Kurth, & Neighbors, 1991; Johnston et al.,2003b, 2003c; Wallace & Bachman, 1991).
Conversely, when examining racial/ethnic differences in drug use among adults, whites, blacks, and Hispanics tendto demonstrate very similar patterns of use,with Asians again reporting the lowest pat-terns of use and American Indians typicallyreporting the highest levels of use (see Table5.5). Thus, patterns of substance use tend to vary substantially by racial/ethnic groupand by age within each racial/ethnic group.We provide specific theoretical explanationsfor these different patterns of substance useand abuse by racial/ethnic group below.
As noted earlier, there are some method-ological concerns relating to the surveymethod that may influence reported drug useby race/ethnic group. One of these concernsis specific to school surveys (such as theMTF, YRBS) and the differential dropoutrates that are evidenced by racial/ethnicgroups. Some have suggested that the higherlevels of drug use reported by white adoles-cents may be accounted for by the fact that disadvantaged minority students who
DRUGS AND DRUG POLICY154
0
10
20
30
40
50
60
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
%
White Hispanic Black
Figure 5.6 Annual Reported Use of Any Illicit Drug by Race, 12th Graders, 1977–2002SOURCE: Johnston et al. (2003b).
05-Mosher.qxd 11/28/2006 5:13 PM Page 154

become heavily involved with both legal andillegal drugs may be more likely than compa-rable white students to drop out of school ordisplay high rates of truancy. Hispanics dohave considerably higher dropout rates thanblacks or whites (Johnston et al., 2003b),and this is likely to influence reported useby Hispanics in later grades (especially 12thgrade). Consequently, actual drug use byHispanic adolescents is likely higher thanrevealed in school-based surveys (Johnston etal., 2003b). However, the fact that blacksdemonstrate a lower prevalence of substanceuse beginning with 8th-grade students is
significant, as truancy and dropouts are quitemodest at this point and are thus unlikely to substantially affect survey response(Johnston et al., 2003b).
Another issue of concern is that bothadolescent and adult minorities may bemore likely to underreport sensitive behav-iors such as substance use (Fendrich &Vaughn, 1994), perhaps because they per-ceive the survey process to be more threat-ening than do whites (Aquilino & LoSciuto,1990). For example, Mensch and Kandel(1988) compared responses to drug usequestions over two response periods and
Patterns of Illegal Drug Use 155
Table 5.5 Past Year Reported Use of Illicit Drugs by Race and Age Category, 2002
Any Illicit Any Illicit Drug Other
Age and Race Drug Than Marijuana Marijuana Cocaine Hallucinogens
Adolescents aged 12–17Total 22.2 13.5 15.8 2.1 3.8Whites 24.0 14.9 17.6 2.5 4.7Blacks 18.5 8.8 12.0 0.2 1.0Hispanics 20.8 13.3 14.1 2.4 3.3Asians 10.6 6.7 5.1 0.2 1.2Native Americans 35.5 20.6 29.4 * *
Adults aged 18–25Total 35.5 20.2 29.4 6.7 8.4Whites 39.6 24.3 33.8 8.5 10.9Blacks 30.9 10.2 27.0 1.3 3.6Hispanics 27.0 15.8 20.0 5.7 3.9Asians 18.6 10.0 15.8 2.2 5.6Native Americans 49.4 26.2 39.0 5.4 10.1
Adults aged 26 and olderTotal 10.4 6.0 7.0 1.8 0.7Whites 10.2 5.8 7.2 1.6 0.7Blacks 13.5 6.7 10.1 3.7 0.4Hispanics 10.5 7.4 5.0 1.7 0.4Asians 4.8 4.3 1.3 0.2 0.7Native Americans 10.5 5.7 6.2 1.8 1.7
SOURCE: Adapted from SAMHSA (2003g, tables 1.32B, 1.35B, 1.37B, 1.40B, 1.42B, 1.45B, 1.47B, 1.50B, 1.52B,1.55B).
* Low precision, no estimate reported.
05-Mosher.qxd 11/28/2006 5:13 PM Page 155

found that blacks, Hispanics, and thosewith less than a high school education weremore likely to deny previously reportedsubstance abuse. However, Mensch andKandel (1988) also noted that underreport-ing occurred at only the lowest levels of use,and others have found few differences inunderreporting by race/ethnicity and social class (Bachman et al., 1991; Tittle,Villemez, & Smith, 1978). Regardless, thereis reason to treat findings of racial/ethnicdifferences in substance use with a healthydegree of skepticism.
Despite the relatively similar patternsof substance use demonstrated acrossracial/ethnic groups, the consequences ofsubstance use and abuse are felt mostacutely by disadvantaged minorities.Indeed, as noted by Wallace (1999b), “thecost that substance use exacts fromAmericans is not distributed equally acrossthe population; rather, its impact is experi-enced disproportionately by black andHispanic adults, families, and children”(p. 1122). The extremely high costs associ-ated with minority substance use, coupledwith relatively modest use patterns, haveprompted researchers to suggest that thereare “two worlds” of minority substanceuse—a relatively large population practicingtemperance or abstinence and a smallerpopulation that uses drugs and alcoholmuch more heavily (Wallace, 1999b). Aswill be discussed in depth below, althoughmotivations for substance use and abusevary to some degree across the groups,issues of social and economic disadvantageappear to be very important for understand-ing why these “two worlds” of minority sub-stance use exist.
African Americans
Despite the rhetoric and media attentionto the contrary, African Americans reportcomparatively low patterns of illegal drug
use. Conservative patterns of use are partic-ularly evident among adolescent subjects,with black adults reporting substance usepatterns that are more similar to those ofwhites. Research examining these distinctpatterns over the lifecourse has focused onthe unique set of environmental and socialcircumstances affecting many black youth.This includes studies on racial segregationand urban poverty, which have demon-strated that, regardless of social class,blacks are much more likely to live in areascharacterized by a variety of social prob-lems, including a greater visibility andaccess to both licit and illicit drugs (E. Anderson, 1990, 1999; Massey &Denton, 1993; Wilson, 1987). For example,Lillie-Blanton et al. (1993) examined racialdifferences in crack cocaine use and foundthat once environmental conditions, includ-ing drug availability, were controlled for,the use of crack did not differ significantlyby race/ethnicity.
Other research on African Americansubstance use has examined the hyper-availability of both legal and illegal drugs inpredominately black communities. Forexample, Wallace (1999a) points to existingresearch that has found black youth, ascompared to white youth, to be more likely(1) to perceive that marijuana, cocaine,and heroin are fairly easy or very easy toobtain in their community, (2) to have seensomeone selling drugs in their communityoccasionally or often, and (3) to reportseeing someone drunk or high in theircommunity occasionally or often. Paradox-ically, the hyperavailability of drug use inminority communities may have both a neg-ative and positive effect on levels of AfricanAmerican substance use. Research hasfound that partly because of this hypera-vailability, some black youth may actuallybe deterred from substance use (Wallace,1999b). Although exposure and availabilitywill increase access and the probability of
DRUGS AND DRUG POLICY156
05-Mosher.qxd 11/28/2006 5:13 PM Page 156

substance use for some, this hyperavailabilityalso means that black youth are apt to wit-ness or experience the numerous social illsthat accompany substance abuse (Wallace,1999b). Ironically, these problems mayactually serve an indirect protective func-tion for some black youth because thethreat posed by illegal drugs is likely to bemore immediate and less likely to be viewedas an abstraction, as it may be for manywhite youth.
Perhaps due in part to the more deleteri-ous environmental conditions facing manyblack youth, the relationship betweenblack parents and adolescents has beenfound to be particularly strong (Giordano,Cernkovich, & DeMaris, 1993). In regardsto substance use, research on adolescentshas found blacks to be more concernedabout parental disapproval while whitesreport being more concerned about peerdisapproval (Warheit, Vega, Khoury, Gil, &Elfenbein, 1996). Possibly due in partto this fact, young blacks are typically lesspeer-oriented than are whites. Research hasdemonstrated that black adolescents scorelower in terms of peer intimacy, indicatelower levels of need for peer approval, expe-rience less peer pressure, and consider itless important to associate with a group of friends (Giordano et al., 1993; Wallace,1999b). As existing research has foundparental and peer relationships to be amongthe most important factors for understand-ing substance use (Wallace & Bachman,1991), with parental bonds more likely tobe a protective factor and peer bonds (ascompared to parental) to be a risk factor,these differences may have importantimplications for understanding racial/ethnicdifferences in substance use.
As noted above, although substance use by African American adolescents is rel-atively modest, illegal drug use by AfricanAmerican adults is comparatively high.Depending upon the substance and data
source, rates of illegal drug use amongAfrican American adults rival and evenexceed those of whites. As Wallace (1999a)summarizes these different patterns of useby race and age,
Among adolescents, black youth are nomore likely, and in many instances havebeen found to be less likely, than whiteyouth to be past, present, or heavy users of licit or illicit drugs. As black and whiteyoung people make the transition intoyoung adulthood, however, there is evi-dence that drug use declines significantlyamong white young adults while it contin-ues to increase among black young adults.(pp. 21–22)
Research examining these contrastingpatterns of substance use has found socio-economic status to be especially salient. Forexample, Barr et al. (1993) examined theeffects of race and class on substance use andfound poverty and educational level to becentral to explaining differences in substanceuse among African Americans. When analy-ses examined illicit drug use by white andblack males making over $25,000 per year (arelatively modest figure), the drug use pat-terns were very much the same, with blacksslightly less likely to use illicit drugs thanwhites. However, differences in drug useincreased as income declined, to the pointthat for those making less than $7,000 peryear, blacks used illicit drugs at five times therate for comparably impoverished whites.
Similar findings were identified by Barrand colleagues (1993) when social class dif-ferences in drug use were compared usingeducation as the measure of social class.Again, among college-educated black andwhite males, there were few differences,with blacks slightly less likely to use illicitdrugs than whites. However, as educationalattainment declined, racial differences indrug use increased, to the point that blackmales with less than a high school degree
Patterns of Illegal Drug Use 157
05-Mosher.qxd 11/28/2006 5:13 PM Page 157

used drugs at more than three times the rateof comparable whites.
Findings such as these suggest thatpoverty, joblessness, and a lack of educa-tional opportunity may be more likely toresult in illicit drug use and abuse by blacksthan comparably disadvantaged whites.Perhaps this is because blacks experiencingthese conditions are very likely to be amongthe “truly disadvantaged,” and this is notthe case for whites. Research on the trulydisadvantaged by Wilson (1987, 1996)and others has noted that while thenumber of middle class blacks has increasedin recent years, due in part to an increasingcommitment to civil rights and programssuch as affirmative action, inner-city minor-ity communities have grown more isolatedand impoverished because they have lost themost successful members of their communi-ties to the suburbs (Massey & Denton,1993; Wilson, 1987). The cumulative dis-advantage present in these communitiesclearly distinguishes minority poverty fromwhite poverty. As Wilson (1987) has notedregarding the difference between poorwhites and poor blacks, poor whites live “inareas which are ecologically and economi-cally very different from poor blacks . . .with respect to jobs, marriage opportuni-ties, and exposure to conventional rolemodels” (pp. 59–60). Accordingly, drug useand abuse may be one of the many negativeconsequences these social conditions havefor impoverished minorities.
Other research examining the compara-tively high rate of substance use by AfricanAmericans in early adulthood as comparedto adolescence has suggested that thischange may in part “reflect their responseto the harshness of the racialized socialsystem from which their parents had pre-viously shielded them” (Wallace, 1999a,p. 30). That is, racism, poverty, and limitedopportunities for employment, education,and advancement may increasingly act as
stressors and sources of emotional strain onminorities once they have left the relativelysheltered environment provided by theirparents. Additionally, because class andrace are inexorably linked in Americansociety, minorities are not only more likelyto encounter these numerous sources ofstrain, but are also less likely to have accessto social institutions and coping resourcesthat help people manage these problems(Peterson et al., 2000). For example, protec-tive factors such as employment (especiallyprofessional), educational participation andsuccess, and family stability are less preva-lent in impoverished minority communities(Anderson, 1990; Wilson, 1987). Residencein a disadvantaged community also providesminorities with less access to conventionalcoping resources. This includes medicalcare; mental health resources; substanceabuse treatment centers; and outlets forconventional leisure such as shopping malls,recreation centers, and libraries (Petersonet al., 2000; Wallace, 1999b; Wallace &Bachman, 1991; Williams & Collins, 1995).Accordingly, substance use may be oneoutlet for people who “self-medicate” tocope with the stress and problems theseimpoverished conditions generate in theirlives.
Hispanics
As compared to African Americans,Hispanics tend to report patterns of illegaldrug use that are similar to those reportedby whites. Currently, the Hispanic popula-tion in the United States is rapidly growing,and Hispanics now constitute the secondlargest racial/ethnic group in America (U.S.Census Bureau, 2002). Many sources ofinformation on substance use, as well as theU.S. Census, use the term “Hispanic” torefer to a diverse group of Americans whohave either immigrated to the United Statesthemselves or whose ancestors immigrated
DRUGS AND DRUG POLICY158
05-Mosher.qxd 11/28/2006 5:13 PM Page 158

from Mexico (approximately 60% of allHispanics), Puerto Rico, Cuba, or Centraland South America. Although this is a veryheterogeneous group, “the Spanish lan-guage and certain cultural customs and tra-ditions that are based on Catholicism andold Spanish culture bind many Hispanicswith a sense of common culture” (Castro,Proescholdbell, Abeita, & Rodriguez,1999). However, because of the diversitypresent in this group, many of those whoare identified as Hispanic prefer to be calledSpanish Americans or Latinos, as the term“Hispanic” refers to the colonizing nationof Spain. As Castro et al. (1999) point outwith regard to this, Americans would likelyresent being referred to as “English people”simply because they speak English andreside in areas that were once colonized by Great Britain. The diversity in theseHispanic subgroups is also reflected in theirrelatively distinct patterns of substance use.Accordingly, we first examine the use ofillegal drugs by Hispanics as a group andthen examine and contrast patterns ofillegal drug use by Mexican Americans,Puerto Rican Americans, Cuban Americans,and Hispanic Americans identifying withvarious countries in Central and SouthAmerica.
Patterns of illegal substance use evi-denced by Hispanics are quite similar tothe patterns of whites, and are similar torates of use by African Americans in adult-hood. As noted earlier, data on adolescentsobtained from school surveys such as MTFand YRBS tend to underestimate the level ofsubstance use by Hispanics, particularly forolder adolescents, because of high Hispanicdropout rates. For example, among familiesin the bottom 20% of yearly income,dropout figures were 13.9% for whites,21.9% for blacks, and 42.4% for Hispanics(DHHS, 2003). Even within the upper class,dropout rates were much higher forHispanics, with figures of 2.0% for whites,
2.5% for blacks, and 11.0% for Hispanics(DHHS, 2003). Although dropout rates arelikely to influence findings on adolescentsubstance use by Hispanics, available dataindicate that whites remain more likelyto use illegal drugs than Hispanics (seeFigure 5.6 and Table 5.5).
Exposure and access to drugs are impor-tant factors for understanding Hispanicsubstance use, particularly among adoles-cents. As with African Americans, Hispanicsare more likely than whites to reside inareaswhere illegaldruguse is frequently wit-nessed and where drugs are more easilyobtained (Wallace, 1999b). Data also indi-cate that Hispanic adolescents are signifi-cantly more likely than whites to be offered,sold, or given illegal drugs on school prop-erty (DHHS-CDC, 2003b). In part, thesefactors may account for the finding thatHispanics are more likely to report drug useat young ages (Johnston et al., 2003b).Despite the greater exposure of Hispanicadolescents to drugs, research has con-cluded that drug use by this group is pre-dicted largely by the same risk factors thatinfluence drug use among other adolescents:things such as family disruption, low schoolcommitment or achievement, and delin-quent peers (Moore, 2001).
Hispanic patterns of drug use are likelyto vary with a number of cultural, environ-mental, and economic factors. Indeed, someHispanic populations have been much moreadversely affected by illegal drug use thanothers have, and a drug that has been par-ticularly harmful to certain Hispanic com-munities is heroin. For example, the highestdrug mortality rates in the nation are notfound in Los Angeles or New York, but inthe heavily Hispanic Rio Arriba County innorthern New Mexico. This extremelypoor county is located along the drug smug-gling route from Mexico to Denver andis characterized by exceptionally high ratesof black tar heroin use. This is the primary
Patterns of Illegal Drug Use 159
05-Mosher.qxd 11/28/2006 5:13 PM Page 159

reason that the drug-related mortality ratein Arriba County is 35 per 100,000 whenthe US average is 2.5 per 100,000 (“HelpingAddicts,” 2001).
Partially in response to the situation inArriba County and similarly affected areas,New Mexico Governor Gary Johnson hascalled for and instituted more progressivedrug policies on substance use, focusing ontreatment and harm reduction rather thanpunishment. This has included giving familiesof heroin addicts overdose kits that includethe drug Narcan, which is used to keepvictims of heroin overdose alive. In Española,a city in Arriba County, Police Chief WayneSalazar has even argued that his officersshould carry Narcan while on duty: “It wouldbe no different than if we responded to thescene of a bad accident where we had to per-form CPR or first aid. We’re trying to save alife” (“Helping Addicts,” 2001).
Reflecting the considerable diversity inHispanic populations, there is significantvariation in the use of illegal substancesamong Hispanic subgroups. Perhaps the bestongoing source of data on these trends is the NSDUH, which provides information onsubstance use by Mexican Americans, PuertoRican Americans, Cuban Americans, andHispanic Americans identifying with variouscountries in Central and South America.Although the 2002 NSDUH did not reportfindings on Cuban respondents out of con-cerns with data precision, there were sig-nificant differences in the use of marijuanaamong the other subgroups. As Tables 5.6and 5.7 illustrate, Puerto Ricans were morelikely to report the use of marijuana than anyother Hispanic subgroup, and this trend wasparticularly evident for adult respondents.
Similar findings were identified byZayas, Rojas, and Malgady (1998), who
DRUGS AND DRUG POLICY160
Table 5.6 Percentages Reported for Marijuana Use by Hispanic Subgroup: Persons 12 to 17Years Old
Hispanic Subgroup Lifetime Past Year Past Month
Mexican 19.2 13.1 6.3
Puerto Rican 22.1 17.0 8.4
Central or South American 17.5 14.0 6.6
Cuban * * *
SOURCE: SAMHSA (2003g).
* Low precision; no estimate reported.
Table 5.7 Percentages Reported for Marijuana Use by Hispanic Subgroup: Persons 18 Yearsand Older
Hispanic Subgroup Lifetime Past Year Past Month
Mexican 32.1 7.6 3.6
Puerto Rican 45.1 13.8 6.2
Central or South American 22.7 6.9 3.8
Cuban 20.7 7.3 4.0
SOURCE: SAMHSA (2003g).
05-Mosher.qxd 11/28/2006 5:13 PM Page 160

examined various Hispanic populations(Colombian, Puerto Rican, Dominican) andfound Puerto Ricans to be more likely touse illegal drugs than other Hispanic men.However, these findings are not universaland are likely to vary with a number ofother factors. For example, a study byWarheit et al. (1996) examined 5,370 ado-lescents in Dade County, Florida, of whichover 3,400 were Hispanic, and foundColombians to be more likely than Cubans,Nicaraguans, and Puerto Ricans to use ille-gal drugs. The authors concluded the differ-ences in substance use evidenced by thesegroups were mostly due to differences inlevels of acculturation.
Acculturation involves the adoption ofnew cultural information and social skillsby an immigrant group, which often replacetraditional cultural beliefs, practices, andinteraction patterns to some degree (Vega,Alderete, Kolody, & Aguilar-Gaxiola,1998; Vega & Gil, 1998). Acculturation istypically measured with indicators such aslanguage use and preference, ethnic identifi-cation, and nativity of both the respondentand the respondent’s parents (Randolf,Stroup-Benham, Black, & Markides, 1998).Acculturation is particularly relevant forHispanic groups with a relatively high per-centage of recent immigrants, and it hasbeen found to be important for understand-ing substance use by Hispanics as comparedto the general population.
Although low acculturation can be stress-ful due to the social isolation brought on byfactors such as communication difficulties, itcan also serve a protective function (Vega,Gil, & Wagner, 1998). This is the case withthe use and abuse of drugs and alcohol, asmany Hispanic groups are traditionallymore conservative in terms of substance usethan American society more generally. Forexample, surveys on drug use in LatinAmerican countries have consistently identi-fied very low patterns of illegal drug use,
even in countries that are key producersand exporters of illegal drugs (Vega,Alderete, et al., 1998; Vega, Gil, et al.,1998). This includes research on Mexico,the country in which most HispanicAmericans originated, which has lower ratesof use for alcohol and other drugs than doesthe United States (Caetano & Medina-Mora,1989; Vega, Gil, et al., 1998).
Much of the effect of acculturation hasfocused on alcohol use and abuse (discussedin detail in Chapter 6), but numerous studieshave also identified an association betweenacculturation and illegal drug use (Amaro,Whitaker, Coffman, & Heeren, 1990; Vega,Alderete, et al., 1998; Vega, Gil, et al., 1998;Warheit et al., 1996). This includes researchthat has found crack cocaine smoking to behigher among more acculturated Hispanics(e.g., those who choose to speak Englishrather than Spanish) (Wagner-Etchegaray,Schultz, Chilcoat, & Anthony, 1994). Otherresearch on the effect of acculturation ondrug use has concluded that Hispanics areoften frustrated with their social acceptanceand unmet expectations of success andachievement, especially Hispanic men bornin the United States (Vega, Gil, et al., 1998).Additional research has found that accultur-ated Hispanics, particularly Hispanic females,are exposed to values that tend to encourageor be more tolerant of drug use and abusethan are their traditional values (Vega,Alderete, et al., 1998; Vega, Gil, et al.,1998).As Vega, Gil, et al. (1998) note, “there issomething about American society thatengenders experimentation and addiction ata much higher rate than experienced in othernations” (p. 125).
American Indians
Similar to Hispanics, American Indiansare a tremendously diverse population.Although many people believe AmericanIndians to be a relatively homogeneous
Patterns of Illegal Drug Use 161
05-Mosher.qxd 11/28/2006 5:13 PM Page 161

group, the more than two million AboriginalNorth Americans living in the continentalUnited States, Alaska, and Canada are dis-persed into over 500 tribes with over 200distinct languages (Caetano, Clark, & Tam,1998). Existing research has found AmericanIndians to demonstrate among the highestpatterns of substance use and abuse, partic-ularly among adolescents and young adults,as compared to all other racial/ethnic groups(Beauvais, 1998; Beauvais, Oetting, &Edwards, 1985; Mail & Johnson, 1993;May, 1982; Oetting, Edwards, Goldstein, &Garcia-Mason, 1980; Plunkett & Mitchell,2000; Young, 1988). For example, as canbe seen in Table 5.5 above, household surveydata examining adolescents and young adultshave found American Indians to report muchhigher levels of lifetime, yearly, and recentuse for marijuana and illicit drugs. AmericanIndians are also the only racial/ethnic groupto evidence few, if any, gender differences inthe use of certain substances. Research onAmerican Indian females has found them tobe as or even more likely than AmericanIndian males to use a number of legal andillegal drugs (Bachman et al., 1991; Beauvais,Oetting, Wolf, & Edwards, 1989; Wallace &Bachman, 1991).
High patterns of substance use amongAmerican Indians can be attributed largely tothe fact that, as a group, American Indiansexperience extreme levels of social and eco-nomic disadvantage (Akins, Mosher, Rotolo,& Griffin, 2003; Wallace & Bachman, 1991).Data from the Indian Health Service (2001)indicate that American Indians fare muchworse than the general population across keyeconomic, social, and health indicators andthis disadvantage results, at least in part, fromthe nature and quality of reservation landsallotted Indians by the federal government.Although only one-third of all AmericanIndians currently live on reservations, theconditions of disadvantage characterizingmany American Indians are due, at least in
part, to this legacy (Beauvais, 1998).Reservation lands are often socially and geo-graphically isolated, and although unemploy-ment and poverty rates for Indians areextremely high in general, this is particularlythe case on reservations (Beauvais, 1998).The high levels of unemployment experiencedby Indians is important for understandingtheir patterns of substance use and abusebecause research has linked substance abusewith unemployment in the general population(Kandel & Yamaguchi, 1987; Kandel &Davies, 1990; Wilson, 1996).
Another consequence of life on reserva-tions is limited access to health care. Forexample, a recent report by SurgeonGeneral Dr. David Satcher indicated thatAmerican Indians and indigenous Alaskansliving in isolated, rural communities have“severely” limited mental health treatmentoptions (“Report: Minorities Lack,” 2001).This may be particularly important forAmerican Indian substance use, as a lackof access to mental health resources mayencourage substance use and abuse as aform of coping and it may inhibit recoveryshould addiction result. Perhaps partly dueto these factors, American Indians who liveon reservations have higher rates of alcoholand drug use than those who live off reser-vations (Beauvais et al., 1985).
The extreme socioeconomic disadvantageexperienced by American Indians has beenfound to be crucial for understanding theirpatterns of substance use and abuse. Forexample, research by Wallace and Bachman(1991) concluded that the effect of socioeco-nomic status was central in accounting forhigher levels of substance use by AmericanIndian adolescents: “Once background dif-ferences are adjusted, the white versusAmerican Indian differences in drug useare virtually eliminated” (p. 343). Researchexamining American Indian adults hasreached similar conclusions, finding thatthe higher rates of substance use among
DRUGS AND DRUG POLICY162
05-Mosher.qxd 11/28/2006 5:13 PM Page 162

American Indians were “at least partiallyexplained by the disadvantaged situationof American Indians, particularly withrespect to socio-demographic and individualrisk/protective factors” (Akins et al., 2003,pp. 64–65). Accordingly, when interpretingfindings on substance use and abuse byAmerican Indians, it is important to take intoaccount the unique economic and socialcircumstances characterizing this group.
Asians and Pacific Islanders
Similar to Hispanics and AmericanIndians, those who are classified as Asianand Pacific Islanders (API) are extremelydiverse. In the 2000 U.S. Census, the term“Asian” was used to refer to people identify-ing origins with any of the original peoples ofthe Far East, Southeast Asia, or the IndianSubcontinent, including Cambodia, China,India, Japan, Korea, Malaysia, Pakistan, thePhilippine Islands, Thailand, and Vietnam(Barnes & Bennett, 2002). At the time ofthe 2000 Census, the API population in theUnited States was 11.9 million people or4.2% of the total population, with Chinesecomprising roughly 23% of all API; Filipinos20%; Asian Indians 16%; and Japanese,Korean, and Vietnamese comprising roughly10% each (U.S. Census Bureau, 2002).
API typically report the lowest usepatterns for virtually all forms of legaland illegal drugs. For example, researchexamining illegal drug use by high schoolseniors from 1976–2000 found Asian youthto report the lowest levels of marijuana useacross this entire time period (Wallace et al.,2003). These trends of low use by Asianadolescents have been found across othersubstances as well, and for both males andfemales (Bachman et al., 1991; Wallace &Bachman, 1991). Similar patterns have beenidentified in household surveys of adults(see Table 5.5 above), with Asian adultsreporting the lowest levels of illegal drug
use, whether measured as past month, pastyear, or lifetime use (SAMHSA, 2003e).
Although there is some concern regardingthe representativeness of the Asian popula-tion captured by drug surveys (Castro et al.,1999), with more affluent and acculturatedAsian populations (e.g., Japanese) potentiallyoverrepresented, other data support theconclusion that Asians are the group leastlikely to use illegal drugs. For example, datafrom the Drug Abuse Warning Network onemergency department visits involvingdrugs and alcohol found that in the year2000, there were over 632,000 reports forwhites, 235,000 for blacks, and 120,000for Hispanics, but Asians were involved in only 6,227 substance-related emergencydepartment visits (DHHS, 2003). AlthoughAsians constitute just over 4% of the U.S.population, this figure still represents verylow levels of substance use problems giventheir national population figures.
In part, the relatively modest substanceuse evidenced by API may reflect their rela-tively high social standing in the UnitedStates. As a group, Asians report income andeducational levels that are very similar towhites and dissimilar to other minoritygroups. For example, U.S. Census data indi-cate that the per capita income for Asianswas $22,352 in the year 2000, as comparedto $25,278 for whites, $15,197 for blacks,and $12,306 for Hispanics. The relativelyhigh income levels reported by Asians reflecttheir high educational attainment andrelative overrepresentation in high-payingprofessional/managerial occupations. Asiansreported the highest level of educationalattainment in the United States in 2000,with 44.1% having obtained a bachelor’sdegree or more and 17.4% having obtainedan advanced degree, figures that are nearlydouble the rates reported by whites, thesecond highest category at 26.1% and 9.5%,respectively (Bauman & Graf, 2003). Somehave speculated that the commitment to
Patterns of Illegal Drug Use 163
05-Mosher.qxd 11/28/2006 5:13 PM Page 163

education among Asian families may alsoresult in lower levels of adolescent and youngadult substance use because Asian youth,devoting more time to their studies, spendless time in peer-oriented activities that facil-itate substance use (Wallace & Bachman,1991). As noted earlier, this tendency tospend less time with peers during adolescenceis also demonstrated by African Americans,who similarly report low levels of adolescentsubstance use.
Despite the low levels of substance usereported by Asians as a group, it is impor-tant to note that there is significant varia-tion in substance use among API subgroups.These distinct patterns of drug use areindicative of the marked differences inincome, education, and culture evidencedby the distinct peoples classified as Asian orPacific Islanders. As Yu and Whitted havenoted on the complexities of measuring dif-ferences in Asian subgroups, “lumpingdiverse ethnic groups which do not evenshare a common history, linguistic roots, orreligious belief” causes important differ-ences in health patterns to be glossed over(cited in Castro et al., 1999). So while manyhave labeled Asians a “model minority” interms of their success and integration inAmerican society, this label is overly sim-plistic because it refers to only some Asiangroups while ignoring the many disadvan-taged Asian populations in America(Niedzwiecki & Duong, 2004; Yin, 2000).
The limited data available on Asiansubgroup differences in illegal substance usemakes broad conclusions difficult, but someAsian groups do appear to use substancesat higher rates than others. For example, itappears that Pacific Islanders may be the mostlikely of the API group to use illegal drugs(SAMHSA, 2003a). Japanese, Asian Indians,and Filipinos are also more likely than otherAPI to report illegal substance use, althoughat levels that are still modest in comparison tothe general population (SAMHSA, 2003b).
Variation in income, education, andespecially acculturation may be importantfor understanding substance use differencesacross Asian subgroups. Specifically, in addi-tion to their comparatively high substanceuse, Japanese, Filipinos, and Asian Indiansare also among the most affluent and sociallyintegrated of Asian subgroups, particularlyin comparison to Southeast Asian groups.While 12.4% of the U.S. population lived inpoverty in 2000, poverty rates for Japanese,Filipino, and Indian Americans were 9.2%,7.0%, and 10.4%, respectively. Conversely,these figures were 19.1% for Laotians,29.3% for Cambodians, and 37.6% forHmongs (Niedzwiecki & Duong, 2004).Similar findings are identified with educa-tion, as over 60% of Asian Indians and 40%of Japanese and Filipinos had obtained abachelor’s degree or higher in 2000, whileonly 7% of Hmongs, 8% of Laotians, 9% ofCambodians, and 20% of Vietnamese hadreached this educational level (Niedzwiecki& Duong, 2004).
To account for the pronounced differ-ences in income and educational attainmentamong Asian subgroups, it is important tounderstand the historical context of Asianimmigration to the United States. SomeAsian populations have constituted a signifi-cant portion of the U.S. population for overa century (as is the case with the Chinese,Japanese, and Filipinos). As a consequence,these groups are considerably more assi-milated and acculturated to mainstreamAmerican life and the relatively high preva-lence of substance use that accompanies this. Conversely, groups originating fromSoutheast Asia primarily immigrated to theUnited States following the Vietnam Warand corresponding unrest in Southeast Asiagenerally (Makimoto, 1998). Unlike otherAsian groups, most notably the Japanese, themore recent immigrants were largely illiteratein both their native language and in English,and were extremely poor as well. These
DRUGS AND DRUG POLICY164
05-Mosher.qxd 11/28/2006 5:13 PM Page 164

factors have slowed the assimilation ofSoutheast Asian immigrants into mainstreamAmerica, and this has impacted their patternsof substance use (Makimoto, 1998).
Census data on “linguistic isolation”support this, finding that although 4.1%of the general U.S. population may havedifficulty communicating in English, thisfigure is roughly 24% for Asians in general,32% for Cambodians and Laotians, 35%for Hmong, and 45% for Vietnamese(Niedzwiecki & Duong, 2004). Conversely,linguistic isolation is relatively low forJapanese, Chinese, and Asian Indians, inpart due to their high average educationalattainment (Makimoto, 1998).
The linguistic and social isolation of cer-tain Asian groups has implications for ourunderstanding of their substance use. First,this isolation is likely to mean that thesegroups will be more apt to use substances ina manner consistent with their native cul-ture (which, although quite high for alco-hol, is less so for illegal drugs) (Makimoto,1998). As noted in our discussion ofHispanic differences above, foreign culturalgroups are typically more conservative interms of substance use than Americansociety in general (Castro et al., 1999). Asthe Asian groups with some of the highestuse patterns are also some of the most afflu-ent and educated, perhaps it is their level ofacculturation that accounts for these usepatterns. Indeed, among immigrant groups,higher levels of income and education typi-cally accompany acculturation (Castro et al.,1999), and it may be that the influence ofacculturation on substance use outweighsthe protective effect of high income andeducation experienced by some minorities.
Social Class
As noted in our discussion of racial/ethnicdifferences in illegal drug use, social classis an important factor in understanding
substance use and abuse. As with race/ethnicity, the relationship between socialclass and substance use is often misunder-stood. For example, common measures ofsocial class, such as income and educationallevel, do not reveal, as many assume, thatmembers of the lower class are more likelyto use illegal drugs. As can be seen in Figure5.7, data from the Monitoring the FutureStudy, which uses parents’ educationalattainment to measure socioeconomic sta-tus, indicate that social class does not pre-dict illegal drug use in a general sense.Although adolescents with parents report-ing the lowest levels of education were morelikely than any other group to report the useof heroin and cocaine, middle class adoles-cents were most likely to report the use ofany illicit drug, marijuana, amphetamines,and narcotics other than heroin.
Similar findings on drug use and socialclass have been identified for adults. Again,using educational attainment as the measureof social class, data from the NSDUH indi-cate that those with a relatively high educa-tional level report the highest use of illegaldrugs, followed by those with little education.For example, adults reporting “some college”as their highest level of educational attain-ment also reported the highest past year mar-ijuana use (at 12.7%), followed by those withless than a high school education (10.4%)and high school graduates (10.2%), with col-lege graduates being least likely to report usein the past year (8.2%) (SAMHSA, 2003b).
Similarly, poverty, in and of itself, is notstrongly related to drug use in the generalU.S. population (Johnston et al., 2003b).This finding has been identified in overseasstudies as well. For example, the BritishCrime Survey (BCS), which includes numer-ous measures of substance use, has founddrug use by young people from the “poorestand richest of households” to vary onlyslightly, with yearly use rates being 33% and26%, respectively (Home Office, 2001).
Patterns of Illegal Drug Use 165
05-Mosher.qxd 11/28/2006 5:13 PM Page 165

Despite the fact that poverty and loweducational attainment do not appear to berelated to higher levels of drug use in thegeneral population, there are importantqualifications to this finding. One of theseis that extreme poverty (e.g., income at200% below the federal poverty level ormore) may be associated with substanceuse and abuse, possibly due to the lim-ited availability of coping and treatmentresources in very poor communities(Wallace, 1999a). Additionally, the effectof social class on drug use does not appearto be consistent across racial/ethnic groups.Because samples of the general U.S. popu-lation (like the population itself) are dis-proportionately white, research findingsbased on such data tend to reflect relation-ships that are specific to whites. This isimportant because research has found that
although social class is largely irrelevant forunderstanding white patterns of substanceuse and abuse (i.e., among whites, rates ofuse are relatively high across all socialclasses), this is not the case for otherracial/ethnic groups. For example, as notedearlier, Barr et al. (1993) demonstrated theimportance of income and educational levelfor illegal drug use by African Americans,but found these variables to be largelyirrelevant for understanding drug use by whites. In part, these findings may be because poverty, especially extremepoverty, typically involves exposure tonumerous sources of disadvantage, and thiscumulative or extreme poverty is mostcommonly seen in predominately minoritycommunities (E. Anderson, 1990; Massey& Denton, 1993; Wilson, 1987). This isimportant because research on drug use
DRUGS AND DRUG POLICY166
0
5
10
15
20
25
30
35
40
45
%
Any ill
icit d
rug
Mar
ijuan
a
Cocain
e
Met
ham
phet
amine
Halluc
inoge
ns
Amph
etam
ines
Ecsta
sy
Other
nar
cotic
s
Heroin
Low Med. Low Medium Med. High High
Figure 5.7 Past Year Drug Use of 12th Graders by Parents’ EducationSOURCE: Johnston et al. (2003b).
05-Mosher.qxd 11/28/2006 5:13 PM Page 166

often studies poverty by examining onlyone critical feature of poverty in isolation(e.g., income or educational level) ratherthan examining it in its cumulativecontext (Barr et al., 1993). However, whenpoverty is considered along with themany other social disadvantages thattypically accompany it, such as unemploy-ment or underemployment, welfare depen-dency, low educational attainment orsuccess, family disruption, and isolationand alienation from the broader society, ithas been found to be an important predic-tor of illegal drug use (Boardman, Finch,Ellison, Williams, & Jackson, 2001).
Rural/Urban Location
The size of place in which one resides hasbeen found to be associated with illegalsubstance use. Although there are manyexceptions to this based on age and type ofsubstance, larger places typically have higher
rates of illegal drug use, especially whencomparing large metropolitan areas to verysmall towns or rural areas (see Table 5.8).One reason for this general trend is thataccess to particular drugs may be limited forthose living in rural areas. In part, this isbecause small towns may not have sufficientnumbers of people interested in certain drugs(e.g., those less commonly used) for drug salesto occur there. This may make it more diffi-cult for rural residents to obtain illegal drugs,thereby affecting their use of these substances.
As will be discussed in more detail in thenext chapter, the use of psychoactive sub-stances in rural areas is more similar to usein urban areas than would appear to be thecase if only illegal drug use is considered.This is because drug use in small towns andrural areas disproportionately involves theuse of legal substances such as alcohol orthe illicit use of substances such as prescrip-tion drugs or inhalants. National surveyshave found the illicit use of prescription
Patterns of Illegal Drug Use 167
Table 5.8 Percentages Reported of Lifetime Prevalence of Use of Various Illegal Drugs by Sizeof Place, Individuals Aged 19–30
Drug Farm/Country Small Town Medium City Large City Very Large City
Marijuana 46.2 56.4 57.4 59.4 60.8Hallucinogens 14.1 17.3 19.2 22.1 25.7LSD 12.2 13.4 15.5 16.8 19.2PCP 2.8 1.4 3.6 1.6 4.1MDMA (ecstasy) 8.8 9.8 13.4 17.4 19.1Cocaine 10.4 12.9 12.3 15.2 17.7Crack cocaine 5.1 4.8 3.7 4.0 4.9Heroin 1.2 1.5 1.7 1.9 2.1Other narcotics 8.8 11.1 12.3 12.6 14.4Amphetamines 14.4 14.5 15.0 14.0 16.3Crystal
methamphetamine 2.9 4.0 3.3 4.6 5.6Steroids 2.0 2.2 1.5 1.5 2.2
SOURCE: Adapted from Johnston et al. (2003c, table 4-2).
NOTE: A small town is defined as having less than 50,000 inhabitants; a medium city as 50,000–100,000; a largecity as 100,000–500,000; and a very large city as having more than 500,000 residents. Within each level of populationdensity, suburban and urban respondents are combined.
05-Mosher.qxd 11/28/2006 5:13 PM Page 167

drugs and inhalants to be very similaramong rural areas, small towns, and largermetropolitan areas, despite the morecommon use of other drugs in larger areas(Johnston et al., 2003c). Similar findingswere identified by Cronk and Sarvela(1997), who found cocaine and marijuanato be more commonly used in urban thanrural areas, but that the use and especiallyabuse of legal drugs (e.g., binge drinking) inrural areas exceeded that in urban areas.
Another reason illegal drug use is lesscommon in rural areas is the more promi-nent role of social institutions such asreligion and family. Being raised in aconventional family and participation inreligious activities have both been foundto act as protective factors for illegal drug use (Hawkins, Jenson, Catalano, &Lishner, 1988; Jang & Johnson, 2001;Thomas, Farrell, & Barnes, 1996). Theseprotective factors more commonly charac-terize those living in rural areas, andresearch has found them to be importantfor understanding lower levels of substanceuse by rural residents (Albrecht, Amery, &Miller, 1996; Bachman et al., 1991).
Although the use of certain drugs, forexample ecstasy, may be much more likelyto occur in large cities as compared tosmall towns and rural areas, this trend isnot universal. Indeed, some “hard drugs”have been found to be comparatively com-mon in rural areas and small towns—as wasthe case with heroin in rural Arriba County,New Mexico (covered earlier in our dis-cussion of Hispanic drug use). Similarly,data provided by the MTF study (Table 5.8above) indicate that young adult ratesof use for crack cocaine, crystal metham-phetamine, and steroids in smaller areasmay rival or even surpass those found inlarge cities (Johnston et al., 2003c).
Research specifically investigating theuse and production of methamphetaminein rural Nebraska used ADAM data to
conclude that arrestees in some ruralNebraska counties were more likely to testpositive for methamphetamine use thanthose arrested in the neighboring metropoli-tan area of Omaha (Herz, 2000). In part, thismay be due to the relatively inexpensive costof the drug and the relative poverty of theserural areas, as well as the fact that metham-phetamine is often produced in isolated rurallocations (U.S. Department of Justice, 2003).
The physical and social isolation of ruralcommunities may also influence both legaland illegal substance use, and especiallyabuse patterns. Although spatial isolationmay make access to certain illegal drugsmore difficult, analogous to the isolation ofminorities in disadvantaged urban communi-ties, substance abuse treatment resources arelikely to be more limited for rural residentsshould they need them. For example,research by Warner and Leukfeld (2001)indicates that rural residents often find them-selves forced to travel large distances in orderto obtain health-related services. Ruralpeople may also be more likely to be charac-terized by cultural traits that make seekingtreatment for substance abuse more difficultor less likely, most notably conservatism and a strong belief in self-reliance (Warner &Leukfeld, 2001). Thus, although the isola-tion and more conservative nature of mostsmall/rural areas may serve a protective func-tion against some forms of illegal drug use,this effect appears to be decreasing over time,and differences in illegal drug use patternsmay simply indicate that rural residents aremore likely to use and abuse legally availablesubstances (Cronk & Sarvela, 1997).
CONCLUSION
This chapter has discussed several correlatesof illegal drug use as well as provided anoverview of the primary sources of informa-tion available on substance use and abuse.
DRUGS AND DRUG POLICY168
05-Mosher.qxd 11/28/2006 5:13 PM Page 168

The two most widely used and perhaps thebest sources of information on substance useand abuse are the Monitoring the FutureStudy and the National Survey on Drug Useand Health, which have collected data onsubstance use and abuse in the United Statesfor decades. Similar data sources provide uswith information on substance use in nationsabroad. Other key sources of information onsubstance use and abuse target populationsthat may be of specific interest, such as thoseaccused of criminal offenses (ADAM) orthose seeking help at hospital emergencydepartments for drug-related problems(DAWN). Finally, ethnographic and inter-view data, such as those collected by PulseCheck, provide a “front line” look at personsand issues sometimes missed by other sourcesof data. All of these data sources areextremely valuable for an understanding ofsubstance use and abuse, but every one alsohas methodological limitations that must beconsidered when interpreting findings ondrug use.
These data sources have enabledresearchers to document and examine whydrug use is more common among somepopulations than others. One correlate ofillegal drug use is age; the use of drugs ismuch more common in late adolescenceand early adulthood than at any other pointin the lifecourse. Research has found that theamount of free time and relative lackof constraints (e.g., career, spouse, kids) dur-ing this period of life may be important forunderstanding these patterns of high use.Gender is another predictor of illegal druguse, with males being more likely thanfemales to use illegal drugs. However, genderdifferences in drug use vary significantly withage. During adolescence, differences are min-imal, although males may be more likely touse drugs in harmful ways. At the stage of lateadulthood, gender differences in illegal druguse also increase, although this may, at leastpartially, reflect a tendency of women to use
more socially accepted drugs, such as psy-choactive pharmaceuticals. It is possible thatthis is because with age, the social condemna-tion of illegal drug use becomes greater forfemales as compared to males, possibly due toan association with motherhood.
Drug use also varies significantly byrace/ethnicity, and in contrast to what isportrayed by the media and believed bymany in the general population, whites areamong the most likely to use illegal drugs.Among adolescents and young adults, exten-sive research has found Asians to demon-strate the lowest patterns of substance use,followed by blacks, then Hispanics andwhites, with Native Americans demonstrat-ing the highest patterns of use. However, ageis also important in understanding racial/eth-nic differences in illegal drug use: Amongadults, use patterns by Native Americans,blacks, whites, and Hispanics are somewhatsimilar, with Asians again reporting the low-est patterns of use. Several factors are impor-tant for understanding these patterns, includingpoverty, education, employment, access tosocietal resources and opportunities, alien-ation, stress, and acculturation. Social class isalso an important factor for understandingdrug use and problems associated with use,although the importance of social class variesacross race/ethnicity and age.
Finally, whether one lives in an urban asopposed to a more rural area or small townis an important predictor of illegal drug use.However, rates of drug use and abuse inurban, semi-urban, and rural areas may bequite similar if one considers all psychoac-tive substances rather than just illegal drugs.
REVIEW QUESTIONS
1. What are the two most useful surveyson drug use in the United States? Whatare the strengths and limitations of thesesurveys?
Patterns of Illegal Drug Use 169
05-Mosher.qxd 11/28/2006 5:13 PM Page 169

2. Aside from surveys, what other sources ofdata on drug use in the United States areavailable? What are the advantages anddisadvantages of these sources, comparedto surveys?
3. At what point in the lifecourse does illegaldrug use peak, and why is this the case?
4. What is known about gender differencesin the use of illegal drugs? How does thegender gap in illegal drug use differ overthe lifecourse?
5. Which racial/ethnic groups are most likelyto use illegal drugs during adolescence?Do these patterns change when consider-ing adult populations?
6. What is hyperavailability, and how doesit help explain racial/ethnic differences indrug use?
7. What factors account for the modestlevels of illegal drug use by black adoles-cents as compared to white adolescents?
8. What is the relationship between socialclassandsubstanceuse?Are there instancesin which poverty is strongly related todrug use and abuse? What are the impli-cations of this for understanding racialdifferences in illegal drug use?
9. What is acculturation and what effectdoes it have on levels of illegal drug useamong Hispanics?
10. What factors are associated with the com-paratively high levels of illegal drug usereported by American Indians?
11. What factors account for differencesin patterns of drug use across Asiansubgroups?
12. What is the relationship between rural/urban location and drug use?
INTERNET EXERCISES
1. Access data on patterns of adolescentdrug use provided by the current Monitoringthe Future study at http://www.monitoringthefuture.org/pubs/monographs/overview2005.pdf.
Scroll down to Table 2 (p. 48) andcompare patterns of past year use from1991 to 2004. What percentage of 12thgraders used marijuana during the pastyear? What percentage used cocaine? Whatpercentage of 12th graders reported use ofmethamphetamine in 1999? What percent-age reported use last year? Do these trendssurprise you?
2. Recall that Pulse Check providesdata on drug use and abuse by interviewing“front line” sources on drug use, such aslaw enforcement officials, drug treatmentproviders, and ethnographic researchers.Access the Pulse Check reports for Bostonand Los Angeles at http://www.whitehousedrugpolicy.gov/publications/drugfact/pulsechk/january04/index.html. (You’ll need toclick on the “city snapshot” link for each cityto get the report.)
What do these reports indicate aboutproblems with cocaine and metham-phetamine in each city? What does this tellyou about the use of particular drugs byregion?
DRUGS AND DRUG POLICY170
05-Mosher.qxd 11/28/2006 5:13 PM Page 170














![FROM SCALE TO REVENUE€¦ · QuickBooks Yes Sage 50 – US Edition (formerly Sage Peachtree) Yes Sage 100 ]Contractor (formerly Sage Master Builder) Yes Sage 100 ERP (formerly Sage](https://static.fdocuments.in/doc/165x107/5f70586f8b6ad8086367e0a5/from-scale-to-revenue-quickbooks-yes-sage-50-a-us-edition-formerly-sage-peachtree.jpg)