Chapter 33 - The Brain and Spinal Cord · changes (particularly in the spinal cord with...
37
835 SHIAO Y. WOO The Brain and Spinal Cord 33 TOLERANCE OF THE CENTRAL NERVOUS SYSTEM TO IRRADIATION Postirradiation Cerebral Necrosis Postirradiation Myelopathy Other Late Effects CENTRAL NERVOUS SYSTEM NEOPLASMS TUMORS COMMON IN CHILDREN Medulloblastoma Astrocytoma Brainstem Gliomas Ependymomas Pineal Region and Germ Cell Tumors Craniopharyngioma Primitive Neuroectodermal Tumors Tumors in Children Younger than 3 Years TUMORS COMMON IN ADULTS Malignant Gliomas: Anaplastic Astrocytoma and Glioblastoma Multiforme Oligodendroglioma Meningioma Primary Malignant Lymphoma of the Central Nervous System Carcinoma Metastatic to the Brain SPINAL CORD TUMORS TOLERANCE OF THE CENTRAL NERVOUS SYSTEM TO IRRADIATION The central nervous system (CNS) is a relatively sensitive, often dose-limiting tissue in curative radiation therapy for CNS and adjacent neoplasms. 1 Radiation injury has been documented on the basis of clinical signs, imaging findings, and histopathologic correlations. 2-6 CNS effects are more pronounced in children and seem to be inversely related to age, with the youngest children having the greatest CNS sensitivity. Of further concern is that numerous chemother- apy agents are associated with unique or enhanced sequelae when given in conjunction with radiation therapy. 7 Studies of laboratory models of cerebral and spinal cord changes have helped to clarify the pathophysiology of radiation-induced neural damage and to associate the extent of damage with time, dose, delivery, and volume. 8-10 For example, Caveness 11 reported a detailed investiga- tion of the clinical, histologic, and physiologic findings in primates after irradiation comparable with that used clini- cally. In that study, a single fraction of 20 Gy was uniformly fatal by week 26; this dose produced increased intracranial pressure and ventriculomegaly with scattered necrotic foci most dramatically affecting the brainstem. A single frac- tion of 15 Gy produced discrete microfoci of white matter necrosis by 26 weeks, with coalescing areas of white matter necrosis evident by 56 weeks. Pathologic findings were less pronounced in animals killed 78 weeks after irradiation, suggesting that some recovery had taken place. No clini- cal or histologic abnormalities were observed after whole- brain irradiation with a single fraction of 10 Gy or with 40 Gy delivered in 20 fractions over 4 weeks. In experiments more relevant to clinical radiation ther- apy, delivering 60 Gy to the whole brain in fractions of 2 Gy over a period of 6 weeks caused papilledema and anorexia in pubertal monkeys, but no overt clinical findings were apparent in adult primates. Histologically, the adult brains showed discrete microfoci of white matter necrosis with calcifications by 26 weeks; healing of the degenerative foci along with increased microcalcifications was seen by 52 weeks. The radiation-induced changes were quantita- tively greater in younger animals. After 80 Gy delivered in 40 fractions, confluent areas of necrosis appeared in the cerebral hemispheres of younger animals by 32 weeks, pro- gressive necrosis was observed at 52 weeks, and coalescent necrotic regions and atrophy were seen by 78 weeks. Caveness’ findings at lower dose levels are similar to the mineralizing microangiopathy seen in children with acute leukemia treated with cranial irradiation (20 to 24 Gy) and methotrexate. 12 Small, coalescent foci of necrosis related to microvascular changes may account for the clinically silent lacunar lesions evident in magnetic resonance imag- ing (MRI) studies of long-term survivors of childhood brain tumors. 13 Postirradiation CNS effects are typically classified tem- porally as acute, subacute, and late reactions. Fractionated radiation rarely produces clinically apparent acute changes, even when the total dose approaches 70 to 80 Gy. 14 Anec- dotal reports of transient exaggeration of neurologic signs have been related theoretically to perilesional or intralesion- al edema that develops at the beginning of irradiation. 15-17 Young and colleagues 18 found abrupt neurologic deteriora- tion in 50% of patients who were given large (7.5- to 10- Gy) fractions for the treatment of symptomatic cerebral metastases; the investigators attributed this effect to the radiation therapy. Although no similar phenomena were reported in studies by the Radiation Therapy Oncology Group (RTOG) in which 6-Gy fractions were adminis- tered, this finding might have been related to the more consistent use of corticosteroids by the RTOG. 16 Subacute CNS effects are rather common. Jones 19 observed transient, self-limited paresthesias with neck flexion (Lhermitte’s sign) that lasted for 1 to 2 months after spinal cord irradiation. These paresthesias, which occur in 15% to 25% of patients after mantle irradiation for Hodgkin disease, are thought to result from transient
Transcript of Chapter 33 - The Brain and Spinal Cord · changes (particularly in the spinal cord with...

shiao Y. Woo
The Brain and Spinal Cord 33
TOLERANCE OF THE CENTRAL NERVOUS SYSTEM TO IRRADIATIONPostirradiation Cerebral NecrosisPostirradiation MyelopathyOther Late Effects
CENTRAL NERVOUS SYSTEM NEOPLASMS
TUMORS COMMON IN CHILDRENMedulloblastomaAstrocytomaBrainstem GliomasEpendymomasPineal Region and Germ Cell Tumors
CraniopharyngiomaPrimitive Neuroectodermal TumorsTumors in Children Younger than 3 Years
TUMORS COMMON IN ADULTSMalignant Gliomas: Anaplastic
Astrocytoma and Glioblastoma Multiforme
OligodendrogliomaMeningiomaPrimary Malignant Lymphoma of the
Central Nervous SystemCarcinoma Metastatic to the Brain
SPINAL CORD TUMORS
toleranCe of the Central nervous system to IrradIatIon
The central nervous system (CNS) is a relatively sensitive, often dose-limiting tissue in curative radiation therapy for CNS and adjacent neoplasms.1 Radiation injury has been documented on the basis of clinical signs, imaging findings, and histopathologic correlations.2-6 CNS effects are more pronounced in children and seem to be inversely related to age, with the youngest children having the greatest CNS sensitivity. Of further concern is that numerous chemother-apy agents are associated with unique or enhanced sequelae when given in conjunction with radiation therapy.7
Studies of laboratory models of cerebral and spinal cord changes have helped to clarify the pathophysiology of radiation-induced neural damage and to associate the extent of damage with time, dose, delivery, and volume.8-10 For example, Caveness11 reported a detailed investiga-tion of the clinical, histologic, and physiologic findings in primates after irradiation comparable with that used clini-cally. In that study, a single fraction of 20 Gy was uniformly fatal by week 26; this dose produced increased intracranial pressure and ventriculomegaly with scattered necrotic foci most dramatically affecting the brainstem. A single frac-tion of 15 Gy produced discrete microfoci of white matter necrosis by 26 weeks, with coalescing areas of white matter necrosis evident by 56 weeks. Pathologic findings were less pronounced in animals killed 78 weeks after irradiation, suggesting that some recovery had taken place. No clini-cal or histologic abnormalities were observed after whole-brain irradiation with a single fraction of 10 Gy or with 40 Gy delivered in 20 fractions over 4 weeks.
In experiments more relevant to clinical radiation ther-apy, delivering 60 Gy to the whole brain in fractions of 2 Gy over a period of 6 weeks caused papilledema and anorexia in pubertal monkeys, but no overt clinical findings were apparent in adult primates. Histologically, the adult brains showed discrete microfoci of white matter necrosis
835
with calcifications by 26 weeks; healing of the degenerative foci along with increased microcalcifications was seen by 52 weeks. The radiation-induced changes were quantita-tively greater in younger animals. After 80 Gy delivered in 40 fractions, confluent areas of necrosis appeared in the cerebral hemispheres of younger animals by 32 weeks, pro-gressive necrosis was observed at 52 weeks, and coalescent necrotic regions and atrophy were seen by 78 weeks.
Caveness’ findings at lower dose levels are similar to the mineralizing microangiopathy seen in children with acute leukemia treated with cranial irradiation (20 to 24 Gy) and methotrexate.12 Small, coalescent foci of necrosis related to microvascular changes may account for the clinically silent lacunar lesions evident in magnetic resonance imag-ing (MRI) studies of long-term survivors of childhood brain tumors.13
Postirradiation CNS effects are typically classified tem-porally as acute, subacute, and late reactions. Fractionated radiation rarely produces clinically apparent acute changes, even when the total dose approaches 70 to 80 Gy.14 Anec-dotal reports of transient exaggeration of neurologic signs have been related theoretically to perilesional or intralesion-al edema that develops at the beginning of irradiation.15-17 Young and colleagues18 found abrupt neurologic deteriora-tion in 50% of patients who were given large (7.5- to 10-Gy) fractions for the treatment of symptomatic cerebral metastases; the investigators attributed this effect to the radiation therapy. Although no similar phenomena were reported in studies by the Radiation Therapy Oncology Group (RTOG) in which 6-Gy fractions were adminis-tered, this finding might have been related to the more consistent use of corticosteroids by the RTOG.16
Subacute CNS effects are rather common. Jones19 observed transient, self-limited paresthesias with neck flexion (Lhermitte’s sign) that lasted for 1 to 2 months after spinal cord irradiation. These paresthesias, which occur in 15% to 25% of patients after mantle irradiation for Hodgkin disease, are thought to result from transient

PART 10 Central Nervous System836
demyelination. Comparable transitory neurologic changes, called the somnolent syndrome, occur after cranial irradia-tion such as that given for acute leukemia; mild encepha-lopathy or focal neurologic changes can appear after the treatment of intracranial tumors.20,21 The cranial syndrome is thought to stem from a transient demyelinating event and is the result of the effects of radiation on the replicat-ing oligodendrocytes.8 MRI can detect specific dose-related changes in gray and white matter within several weeks of conventionally fractionated irradiation.22 The potential for self-limited neurologic deterioration, most often occurring during the second month after irradiation, is important to bear in mind because clinical and radiologic changes can sometimes mimic tumor progression.23,24
Late reactions of the normal brain are the dose-limiting toxicities for radiation treatment. Clinical manifestations of focal neurologic deficits, encephalopathy, or neuropsy-chological dysfunction accompany various morphologic findings, such as atrophy, calcifications, diffuse white mat-ter degeneration, and focal necrosis. Permanent or progres-sive myelopathy can result from spinal cord irradiation. Late changes in hypothalamic-pituitary function manifest as specific radiation-induced endocrine deficits.
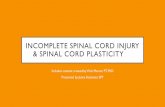
Postirradiation Cerebral NecrosisPostirradiation cerebral necrosis, the most direct effect of CNS irradiation, is thought to result from direct effects of radiation on the replicating glial cell compartments and the capillary endothelial cells.8,9 The theoretical relation-ship between primary glial cells (i.e., type II astrocytes and oligodendrocytes) and vascular endothelial components is shown in Figure 33-1.8,25-29 Clinical signs of postir-radiation cerebral necrosis are seen 6 to 36 months after
Vascularendothelium Astrocyte I Astrocyte II Oligodendrocyte
Blood-brain barrier (BBB)
Myelinated nerve fiber
Inter-nodal
Paranodal
Earlydemyelination
Transient edema(high dose)
1–2months?
?
3–6 monthsProgressiveBBB
breakdown
Capillariesvenules
White matternecrosis
Late delayed effects
Progressivedemyelination
Glialatrophy
Telangiectasiainfarcts
FIGURE 33-1. The direct effects of radiation on glial cells (as-trocyte II and oligodendrocyte) and the indirect effects resulting from vascular changes are shown in a scheme developed by van der Kogel. (From van der Kogel AJ. Central nervous system radiation injury in small animal models. In Gutin PH, Leibel SA, Sheline GE [eds]: Radiation Injury to the Nervous System. New York: Raven Press, 1991, pp 91-112.)
therapy.15,16,30 Cerebral changes often mimic residual or recurrent tumor, with mass effect, enhancement, or cyst formation evident on computed tomography (CT) scans; these changes occur at or near the site of the primary tumor (i.e., the high-dose volume for intracranial neoplasms).31
Cerebral necrosis unrelated to intraparenchymal neo-plasms has been described in reviews by Kramer and colleagues32 and Sheline and coworkers.16 Necrosis has been observed after therapy for extracranial tumors (pre-dominantly those of the skin and paranasal sinuses) and for noninvasive pituitary tumors or craniopharyngiomas. Postirradiation necrosis is a dose-related phenomenon with a relative threshold radiation dose of 50 to 55 Gy if treatment is given in a conventional fractionation schedule (1.8- to 2-Gy fractions given once daily).16,30,33,34 Marks and colleagues30 reported the occurrence of necrosis in 5% of 139 patients with intracranial tumors treated with con-ventional fractionation to doses higher than 45 Gy; 6 of the 7 patients who had necrosis were given total doses in excess of 63 Gy.
The dose-time relationship is critical in determining CNS tolerance, with fraction size the dominant factor among patients receiving doses of 60 to 63 Gy. Necrosis in patients who receive less than 60 Gy usually has been associated with fractions of greater than 2.5 Gy.16 Aristiza-bal and colleagues33 documented necrosis after treatment for pituitary tumors in 3% of 106 patients given less than 2.2 Gy per day (total dose of about 50 Gy) compared with 15% of 13 patients given doses of greater than 2.2 Gy daily. The influence of fraction size was made apparent in the isoeffect analyses of brain necrosis reported by Sheline and colleagues.16
Sheline and coworkers16 contend that the brain can tol-erate a total radiation dose of 50 to 54 Gy given in fractions of 2 Gy once daily. At that dose, cerebral necrosis is esti-mated to occur in 0.04% to 0.4% of patients. The likelihood of necrosis is higher among patients with primary brain tu-mors, although the incidence is still estimated to be less than 5% among patients receiving a dose of 55 Gy at 1.8 to 2 Gy per fraction.34 Tolerance is affected by age; experimental and clinical data indicate that children younger than 2 years can tolerate approximately 10% to 20% less radiation to the brain than those older than 2 years.11,35,36
Postirradiation MyelopathyPostirradiation myelopathy is the spinal cord equivalent of cerebral necrosis. The myelopathy manifests as sensory and motor signs referable to a single cord level, signs that are often clinically indicative of hemisection of the cord (Brown-Séquard syndrome).37,38 Symptoms occur as early as 6 months after treatment (median, 20 months).39 The pathophysiology of spinal cord myelopathy is similar to that of cerebral necrosis, and there is continued debate concerning the relative importance of vascular endothelial changes (particularly in the spinal cord with end-arterial blood supply to portions of the thoracic cord) and direct effects of the radiation on glial elements.28,29,40
The time-dose relationship and tolerance of the spinal cord to irradiation have been analyzed in the context of extraspinal tumors. The thoracic spinal cord seems to be the most sensitive portion; few instances of lumbar myelopa-thy have been reported. Phillips and Buschke41 suggested that the thoracic spine could tolerate a dose as high as

33 The Brain and Spinal Cord 837
50 Gy given in fractions of 2 Gy once daily. Abbatucci and colleagues42 observed cervical cord myelopathy after doses of 55 Gy or more. The incidence of myelopathy rises rapidly with increasing doses, approaching 50% at 65 Gy.29 Many clinical trials of large-fraction irradiation for lung cancer have confirmed that the frequency of reactions increases as the fraction size exceeds 2.5 Gy.43-46 Fraction size also seems to correlate inversely with the latent interval before the development of myelopathy42; however, no experimen-tal evidence exists to suggest improved tolerance to frac-tions less than 2 Gy.47 The Continuous Hyperfractionated, Accelerated Radiation Therapy (CHART) regimen for lung cancer was originally based on a presumed cord tolerance of a low dose per fraction, but that regimen initially was associated with an unacceptable risk of myelopathy.48,49 Tolerance decreases as the volume or length of cord irradi-ated increases.41,42
Other Late EffectsA unique late effect of cranial irradiation combined with chemotherapy, called leukoencephalopathy, has been observed in children with acute lymphoblastic leukemia, adults with small cell carcinoma of the lung, and patients with primary CNS tumors.12,50,51 Leukoencephalopathy is a profoundly demyelinating, necrotizing reaction that usu-ally occurs 4 to 12 months after combined treatment with methotrexate and radiation.52 Dementia and dysarthria may progress to seizures, ataxia, focal long-tract signs, or death. Although most of these symptoms regress after systemic, intrathecal, or intraventricular methotrexate therapy is discontinued, patients are left with permanent neurologic deficits. The occurrence of leukoencephalopathy in patients treated with systemic and intrathecal methotrex-ate without radiation and a dose-effect relationship that is more apparent for methotrexate than for radiation suggest that the clinical leukoencephalopathy is more significantly related to the methotrexate than to the radiation.7 How-ever, white matter changes interpreted as leukoencepha-lopathy (and so coded in the NCI Common Terminology Criteria for Adverse Events) must be distinguished from the clinical syndrome previously described.
Decline in intellectual function has been related to cra-nial irradiation of adults and particularly of children.53-57 Neurocognitive changes in children correlate significantly with cranial irradiation, young age at diagnosis and ther-apy, and functional level at the time the irradiation was begun.53-55,58,59 The occurrence of dose-related neuroco-gnitive alterations suggests a role for continued, if cautious, reduction in the full cranial radiation dose for patients with medulloblastoma, for example, who exhibit favorable pre-senting signs.60 Changes in white matter volume obtained by MRI segmentation constitute an objective variable that is closely tied to intellectual function and that may permit more detailed studies of the effects of radiation therapy and chemotherapy in the current generation of clinical trials.61 Intellectual impairment in adults has occurred primarily after intensive chemotherapy and radiation for the preven-tion of metastasis from small cell carcinoma of the lung and for treatment of primary CNS lymphomas.62
Peripheral nervous system tissue is relatively resistant to irradiation. Acute and subacute symptoms or signs occur infrequently; transient cranial nerve neuropathies are observed only with high-dose, single-fraction, high–linear
energy transfer (LET) radiation for pituitary or parasellar tumors.63 The optic chiasm is often considered a dose-lim-iting structure when irradiation for suprasellar or adjacent temporal lobe lesions is being planned, and special attention is given to limiting the risk of dose-related visual complica-tions.64 Optic nerve or chiasm injury has been documented in almost 20% of patients treated with fraction sizes of 2.5 Gy or greater (to total doses of 45 to 50 Gy), compared with 0 of 27 patients and 0 of 500 patients treated with fraction sizes of 1.7 to 2 Gy to the same level.16,65 Late injury to the brachial plexus observed after the treatment of breast cancer similarly seems to occur largely after high-dose fractions.66
Central nervous system neoplasms
Primary tumors of the CNS represent 2% of all cases of cancer in the United States. Approximately 20,500 new cases are diagnosed annually.67 The incidence of these tumors exceeds that of Hodgkin disease in adults, and they account for 20% of all cases of childhood cancer.
The natural history of tumors of the brain and spinal cord is relatively unusual because aggressive malignant lesions rarely disseminate beyond the neuraxis. Categoriz-ing CNS tumors as benign or malignant is often difficult because histologically low-grade or benign neoplasms are sometimes associated with a poorer prognosis than certain histologically malignant tumors. It is instead the potential for local invasiveness or metastasis along the cerebrospinal fluid (CSF) pathways that determines the “malignancy” of CNS tumors. The challenge for neurosurgeons and radia-tion oncologists is to remove or devitalize neoplastic tis-sue in the functionally vital, anatomically confined nervous system.
tumors Common In ChIldren
Brain tumors in children account for one in five cases of childhood cancer. The incidence of primary CNS tumors, particularly the astrocytic lesions, increased in children during the first half of the 1990s; since then, the incidence has leveled off, perhaps because of the added diagnostic sensitivity of MRI.68 Pediatric brain tumors arise most often in the posterior fossa. Posterior fossa tumors often produce symptoms and signs of increased intracranial pressure because the growing tumor obstructs the flow of CSF through the fourth ventricle. Ataxia often accom-panies pressure-related headaches and morning vomiting. Brainstem gliomas cause cranial nerve palsies, ataxia, and long-tract signs, including lateralizing weakness and sen-sory deficits.
Supratentorial tumors occur in the cerebral hemispheres and the central or deep-seated areas of the thalamus, hypothalamus, suprasellar area, and pineal–third ventricular region. Symptoms are local and include lateralizing neuro-logic deficits and seizures, which are associated with hemi-spheric and thalamic tumors; visual and endocrine changes; and specific oculomotor findings, which are associated with tumors of the pineal region.
Primary tumors of the spinal cord account for only 5% of tumors in children. Metastasis to the CNS is uncommon

PART 10 Central Nervous System838
in childhood cancer. Contiguous extradural compression within the spinal canal or at the base of the skull (e.g., in neuroblastoma, rhabdomyosarcoma, primary bone tumors) is more common than hematogenous metastasis to the brain.
Common primary intracranial tumors diagnosed in chil-dren are listed in Table 33-1.25,26 The histologic classification of pediatric brain tumors has been relatively standardized by the World Health Organization (WHO).69 The most com-mon tumors are the astrocytic lesions (i.e., astrocytomas, malignant gliomas, and brainstem gliomas). Medulloblasto-ma, which accounts for 20% of all childhood CNS tumors, is part of the broader category of supratentorial primitive neu-roectodermal tumors (PNETs) and other embryonal CNS tumors (i.e., cerebral neuroblastoma, ependymoblastoma, and pineoblastomas).69-71
Biologic findings increasingly define the nature of CNS tumors in children, providing some associations with tumor aggressiveness and outcome. Medulloblastoma, for exam-ple, is often associated with gene deletions in chromosomal region p17; expression of the EGFR gene (formerly desig-nated ERBB1), which encodes the epidermal growth fac-tor receptor, and NTRK3 (formerly called TRKC), which encodes the neurotrophic tyrosine kinase receptor type 3, are negatively and positively correlated with outcome, respectively.72,73 Several other molecular markers, such as cyclin-dependent kinase 6, MYC, apurinic or apyrimidinic endonuclease activity, and members of the WNT pathway, also have prognostic significance.74-77 Several investigators have proposed combining information on gene expression patterns and clinical stage for stratifying risk groups in medulloblastoma.78,79
TABLE 33-1. Relative Incidence of Brain Tumors in Children
Tumor Type Incidence (%)
Infratentorial 55
Medulloblastoma 25
Astrocytoma (cerebellum) 15
Brainstem glioma 10
Ependymoma (fourth ventricular region) 6
Supratentorial 45
Astrocytoma 23
Malignant glioma (anaplastic astrocytoma, glioblastoma multiforme)
6
Embryonal (primitive neuroectodermal) tumors
4
Ependymoma 3
Craniopharyngioma 6
Pineal region tumors 4
Oligodendroglioma 2
Modified from Duffner PK, Cohen ME, Myers MH, et al. Survival of children with brain tumors: SEER program, 1973-1980. Neurology 1986;36:597-601; Childhood Brain Tumor Consortium. A study of childhood brain tumors based on surgical biopsies from 10 North American institutions: sample description. J Neurooncol 1988;6:9-23.
MedulloblastomaMedulloblastoma represents 20% of childhood brain tumors. Common throughout the pediatric age range, the median age at diagnosis is 6 years, and 25% of tumors occur in children younger than 3 years. Approximately 10% to 20% of medulloblastomas occur in adults, predominantly in the third to fifth decades. The classic presenting triad of posterior fossa tumors such as medulloblastomas consists of headaches and vomiting, which are signs of increased intracranial pressure and ataxia.
Medulloblastoma is by definition a posterior fossa tumor, most often arising in the cerebellar vermis, within the cere-bellar hemispheres (typically in adolescents and frequently as the desmoplastic variant) or along the cerebellopontine peduncle. The tumor grows to fill the fifth ventricle and often attaches to the brainstem. Medulloblastoma is the characteristic “seeding” CNS tumor and is associated with subarachnoid dissemination through the CSF; metastasis may be apparent from cytologic findings or from images of radiographic deposits within the intracranial subarach-noid space (i.e., along the convexities or within the basal cisterns, sometimes limited to the region of the pituitary stalk) or within the spinal subarachnoid space. Subarach-noid disease is apparent at diagnosis in 20% to 25% of affected children.13,80 Extraneural disease, usually involv-ing the bone or bone marrow, is an uncommon finding at diagnosis or disease recurrence.81
The embryonal CNS tumors represent a group of his-tologically related neoplasms that occur predominantly in children (Box 33-1).69 The WHO classification defines the embryonal tumors as round, blue, small cell tumors that tend to seed the neuraxis and respond to radiation and chemotherapy, although the prognosis varies widely. Less common tumors in this category include the supratentorial PNETs; the rare, primitive medulloepithelioma; and atypical or rhabdoid tumor (see “Tumors in Children Younger than 3 Years”). Pineoblastoma is classified separately (see “Pineal Region and Germ Cell Tumors”). The term posterior fossa PNET is synonymous with medulloblastoma.69
BOX 33-1. Embryonal Central Nervous System Tumors*
MedulloblastomaCentral neuroblastomaEpendymoblastomaPrimitive neuroectodermal tumor (PNET)†
Additional Tumors with a Distinct Histology and Different Genetic Pathway of EvolutionMedulloepitheliomaAtypical teratoid or rhabdoid tumor
Pineal Parenchymal Tumor Classified Clinically as an Embryonal TumorPineoblastoma
*In the definition proposed by Kleihues and Cavenee,69 embryonal central nervous system tumors are “histologically identifiable entities [that] all develop on the background of an undifferentiated round-cell tumor but show a variety of divergent patterns of differentiation.”†PNET refers to supratentorial tumors; tumors that occur in the posterior fossa are known as medulloblastomas.

33 The Brain and Spinal Cord 839
Medulloblastoma is thought to originate from the prim-itive external granular layer of the developing cerebellum. The tumor is characterized by undifferentiated small, round, blue cells, often including neuroblastic rosettes and with various degrees of neuronal and glial differentiation. The desmoplastic tumors are classically identified by their prominent nodularity and dense areas of reticular fibers.69 Other histopathologic subsets include medulloblastoma with extensive nodularity or advanced neuronal differentiation and large cell or anaplastic medulloblastoma.73
Surgery and StagingSurgery is the initial therapy, with the goal of maximal resection for the sake of therapy and reestablishing CSF flow. Intraoperative ventriculostomy has replaced the routine initial placement of a ventriculoperitoneal shunt; with current surgical approaches, less than 25% of children require postoperative conversion of the temporary ventric-ulostomy to a permanent ventriculoperitoneal shunt. Gross total resection is limited only by substantial invasion of the tumor into the brainstem or infiltration into the peduncle. Gross total or near-total resection (i.e., more than 90% of the tumor removed, with less than 1.5 cm2 of residual disease) is achieved in almost 90% of children older than 3 years in the United States.82 The operative mortality rate should be less than 1% or 2% for children treated with cur-rent approaches, and the postoperative morbidity is typical-ly acceptable, with a small proportion of children left with permanent new cranial nerve deficits or marked ataxia.82,83 The posterior fossa syndrome, marked by severe truncal ataxia, difficulties with speech and swallowing stemming from bulbar effects, and sometimes mutism, seems to be associated with extensive dissection along the lower brain-stem; symptoms usually abate considerably over several months after the surgery, although late residual deficits of various degrees of severity have been seen.84
Postoperative neuraxis staging is standard in defining risk groups and subsequent therapy for medulloblastoma and the other embryonal tumors. Immediate postopera-tive cranial MRI or CT (preferably done within 1 to 3 days of surgery) defines the postoperative residual effect, which is a more reliable prognostic factor than the opera-tive coding of the extent of resection.82 Neuraxis staging begins with a contrast-enhanced spinal MRI (preferably more than 10 days after surgery to eliminate the confu-sion of findings with postoperative debris) and subsequent lumbar CSF cytologic studies; routine bone scanning and bone marrow assessments are standard only in investiga-tional settings.13,80 Staging is based on the extent of re-sidual tumor (average risk is defined as the presence of ≤1.5 cm2 of residual tumor) and the presence or absence of subarachnoid or extraneural metastasis (defined accord-ing to a modification of the Chang system85) (Box 33-2). Most important from the standpoint of planning therapy is determining whether isolated CSF cytologic evidence of metastatic disease (M1 disease), imaging evidence of intra-cranial disease outside the posterior fossa (M2 disease), or imaging evidence of spinal metastasis (M3 disease) is pres-ent; extranodal disease is classified as M4.85 Standard or average-risk disease is defined as that which has been totally removed or has residual tumor volume of less than 1.5 cm2 with M0 disease; almost 60% to 65% of children enrolled in U.S. studies at the turn of the century were so classified.
The presence of only local residual disease is uncommon in children with high-risk disease; more often, these children have neuraxis dissemination.
Radiation TherapyPostoperative management consists of radiation therapy and chemotherapy.86 Infants and young children (i.e., those younger than 3 years) are treated in accordance with developing investigational approaches (see “Tumors in Children Younger than 3 Years”). The standard sequence of therapy for children 3 years old or older is to begin radia-tion therapy within 28 to 31 days of surgery, followed by chemotherapy.87 Although studies of preirradiation che-motherapy have added significantly to our knowledge of chemosensitivity, randomized trials have shown no benefit from administering chemotherapy before the radiation, and in some instances, results have suggested that this sequence is ultimately detrimental to disease control.88-91
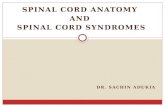
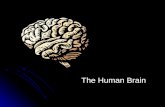
Radiation therapy for medulloblastoma is technically demanding and biologically unforgiving. It requires the systematic inclusion of the entire subarachnoid space (i.e., craniospinal irradiation [CSI]) followed by a boost to the posterior fossa. One standard technique involving immo-bilization of patients in the prone position is illustrated in Figure 33-2. Lateral craniocervical fields encompass the intracranial and upper cervical spine regions, with particu-lar attention to including the subfrontal and infratemporal regions (at the cribriform plate in the midline subfrontal area and along the infratemporal regions) (Fig. 33-3).
The conventional dose to the neuraxis in patients given surgery and radiation is 36 Gy (delivered in 1.8-Gy
BOX 33-2. Chang Staging System for Medulloblastoma
Primary Tumor (T)*T1 Tumor less than 3 cm in diameterT2 Tumor at least 3 cm in diameterT3a Tumor larger than 3 cm in diameter with
extension into the aqueduct of Sylvius and/ or into foramen of Luschka
T3b Tumor larger than 3 cm in diameter with unequivocal extension into the brainstem
T4 Tumor larger than 3 cm in diameter with extension up past the aqueduct of Sylvius and/or down past the foramen magnum (i.e., beyond the posterior fossa)
Distant Metastasis (M)M0 No evidence of gross subarachnoid or
hematogenous metastasisM1 Microscopic tumor cells found in cerebrospinal
fluidM2 Gross nodule seedings demonstrating in the
cerebellar, cerebral subarachnoid space, or in the third or lateral ventricles
M3 Gross nodular seeding in spinal subarachnoid space
M4 Metastasis outside the cerebrospinal axis
*The T stage is no longer thought to be prognostically related to outcome.Modified from Chang CH, Housepian EM, Herbert C Jr. An operative staging system and a megavoltage radiotherapeutic technic for cerebellar medulloblastoma. Radiology 1969;93:1351-1359.

PART 10 Central Nervous System840
Posteriorspine
A BFIGURE 33-2. A, Classic craniospinal irradiation configurations, with a divergent posterior spinal field matching opposed lateral craniocervical fields. The collimator rotation enabling the craniocervical fields to be matched to the divergence of the posterior spi-nal field is typically modified at least every 5 fractions. Field markings for medulloblastoma are determined by the cribriform plate at the orbital level (see Fig. 32-3). B, The parallel inferior border from the craniocervical fields is achieved by couch rotation, calculated to achieve a three-dimensional match in the depicted plane.
fractions once daily). The progression-free survival rate for patients with localized disease after maximal resection and CSI (36 Gy) is approximately 65% at 5 to 10 years (Table 33-2).36,92-96 A randomized study of patients with average-risk medulloblastoma conducted by the Pediatric Oncol-ogy Group (POG) and Children’s Cancer Group (CCG) in the late 1980s established the superiority of a total dose of
FIGURE 33-3. A conventional fluoroscopic image used for simulating the lateral craniocervical fields used in craniospi-nal irradiation for medulloblastoma (see Fig. 33-2). The long arrow indicates the margins along the cribriform plate. The radiopaque dot and the small arrows indicate the anterior mar-gins of the lateral orbital rims. Divergence rather than a collima-tor angle is needed when only the subarachnoid space is to be targeted.
36 Gy compared with 23.4 Gy for CSI and the benchmark outcome of more than 90% tumor removal with less than 1.5 cm2 of residual disease.92 Later findings suggest that the combination of reduced-dose CSI (23.4 Gy) and che-motherapy produces disease control rates comparable with or superior to those for conventional-dose CSI alone.97 Large-scale prospective studies are documenting the effi-cacy of what is now considered the standard treatment for localized medulloblastoma, which is radiation (CSI dose of 23.4 Gy) followed by cisplatin-containing chemotherapy.
Reports of outcome from nonrandomized, single-arm trials, further supported by neuropsychological findings from the POG-CCG study previously mentioned, suggest that cognitive function in children with average-risk disease after therapy is superior among those given CSI to 23.4 Gy instead of 36 Gy, especially in children 3 to 8.5 years old.60 The current Children’s Oncology Group (COG) trial is testing, in children between 3 and 7 years old with average-risk disease, whether the CSI dose can be further reduced from 23.4 Gy to 18 Gy. Children with metastatic disease at presentation (i.e., M1 to M3 disease) require a dose of 36 to 39 Gy to the neuraxis. The use of proton therapy for CSI has a theoretical advantage over photon therapy because of the lack of exit dose from proton therapy. Miralbell and colleagues estimated that the risk of second neoplasms could be reduced with proton therapy relative to photon therapy.98
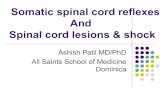
Irradiation includes a boost to the posterior fossa region, classically defined as the entire infratentorial volume. The use of opposed lateral posterior fossa fields has been stan-dard, but radiation oncologists are increasingly using a three-dimensional conformal radiation therapy approach99 to spare the auditory apparatus and, when possible, the pituitary-hypothalamic region (Fig. 33-4). Proton therapy for pediatric medulloblastoma is also being considered as a way of maximizing target dose coverage and sparing normal tissues (Fig. 33-5). The cumulative dose deliv-ered to the posterior fossa is typically 54 to 55.8 Gy. A few institutional summaries of patterns of treatment fail-ure for patients with medulloblastoma and descriptions of preliminary experience with target volumes confined

33 The Brain and Spinal Cord 841
TABLE 33-2. Survival Rates after Craniospinal Irradiation for Medulloblastoma
Study and Reference Period Number of Patients Survival Rate at 5 Years (%) Survival Rate at 10 Years (%)
Bloom et al, 196936 1950-1964 71 40 30
Berry et al, 198193 1958-1978 122 56 43
Hughes et al, 198694 1977-1985 53 64 42
Bloom et al, 199095 1970-1981 53 53 45
Jenkin et al, 199096 1977-1987 72 71 63
Thomas et al, 200092 1978-1991 42 (CSI = 36 Gy) 67* 67*
46 (CSI = 23 Gy) 52* 52*
*Event-free survival rates at 5 and 8 years.CSI, craniospinal irradiation.
A
FIGURE 33-4. A, Treatment plans for a three-dimensional conformal technique demonstrating the ideal dose distribution for a six-field, non-coplanar approach targeting the entire posterior fossa. Anatomically, this approach includes the tentorium as it extends superiorly in the posterior clinoid and then inferiorly to define the anterior and superior margins of the posterior fossa. The inferior and posterior margins are defined by the calvarium and the lower margin of foramen magnum. (Continued)
to the operative or tumor bed highlight investigational approaches that are being studied prospectively in a COG study.100,101
Chemotherapeutic AgentsSeveral categories of chemotherapeutic agents have shown efficacy in medulloblastoma: alkylating agents (e.g., cyclophosphamide, lomustine), platinating agents (e.g., cis-platin, carboplatin), topoisomerase II inhibitors (e.g., eto-poside), and the vinca alkaloids (e.g., vincristine). The most common adjuvant treatment for standard- or average-risk disease was described by Packer and colleagues87 and con-sists of concurrent vincristine during irradiation and post-irradiation cycles of lomustine, cisplatin, and vincristine. The addition of concurrent carboplatin or etoposide and high-dose, peripheral stem cell–supporting chemotherapy regimens has been studied in two separate protocols for the treatment of high-risk disease.102 The first report of
a multi-institutional phase II trial of this approach showed 5-year event-free survival rates of 83% for children with average-risk disease and 70% for children with high-risk disease.103
Although posterior fossa recurrence previously was regarded as the dominant pattern of failure, later stud-ies have indicated that more patients exhibit neuraxis or combined local and disseminated failure. Approaches to the management of disease recurrence are not standardized but often include chemotherapy, further surgery for local-ized disease, and the judicious use of additional irradiation. Secondary or salvage therapies are rarely successful.
AstrocytomaAstrocytomas are the most common glial tumors in chil-dren, developing in the cerebellum, brainstem, cerebral hemispheres, diencephalon (i.e., thalamus, hypothalamus, and third ventricular region, including the optic chiasm),

PART 10 Central Nervous System842
B
FIGURE 33-4.—cont’d B, Three-dimensional conformal dose distribution demonstrates coverage of the primary tumor site, which in this case is the operative bed after surgical resection of a medulloblastoma. A multifield, non-coplanar, 6-MeV photon approach uses a gross tumor volume that outlines the operative bed, expanded by 2 cm (as modified by anatomic boundaries) to identify the clinical target volume. A 5-mm planning target volume geometrically surrounds the clinical target volume.
or spinal cord.104-106 In adults, low-grade tumors occur primarily in the cerebral hemispheres and thalamus; how-ever, malignant astrocytomas far exceed the number of his-tologically benign lesions beyond the age of 20 years.
The WHO grades astrocytomas as grade I (juve-nile pilocytic astrocytoma [JPA]) or grade II (fibrillary astrocytoma or astrocytoma not otherwise specified); high-grade lesions are deemed grade III (anaplastic [malignant] astrocytoma) or grade IV (glioblastoma multiforme).69 Grossly, the tumors are solid with discrete or infiltrat-ing margins or cystic. Pilocytic astrocytomas are biologi-cally nonaggressive lesions that are often cystic, occurring predominantly in the cerebellum and diencephalon in children (Fig. 33-6).
The natural history of astrocytomas depends on the age of the patient and the site of origin and histologic classifi-cation of the tumor. Pilocytic tumors rarely progress to a more malignant histology; however, fibrillary astrocytomas progress to a more malignant histology in 30% to 50% of cases.107-109 The proliferative index, assessed by staining for Ki-67 with the murine monoclonal antibody MIB1, has been reported to influence prognosis.110
Cerebellar AstrocytomasCerebellar astrocytomas involve the vermis or hemispheres in 75% of patients; in 25% of children, tumors manifest as transitional neoplasms that involve the cerebellum and the cerebellar peduncles or adjacent brainstem.111-114 Cerebel-lar astrocytomas are classically cystic lesions; the textbook appearance consisting of a large cyst associated with a mural nodule occurs in about one fourth of cases. Grossly, most tumors are mixed cystic and solid lesions or apparently solid tumors with small cystic components. Histologically, 75% of astrocytomas in this location are JPAs.111,112,114,115 Debate continues about whether high-grade gliomas occur
in the cerebellum in children; if they do, they are quite uncommon.116
Therapy for cerebellar astrocytomas is largely surgical. Reports from institutions indicate that gross total resection is done in 65% to 90% of cases, although this rate has risen to approximately 85% to 90% in recent series.100,112,114,115 Resection is more often incomplete in patients with tumors involving the cerebellar peduncles or the brainstem.112-115 The operative mortality rate should be less than 4%, unlike the rate for patients with medulloblastomas and ependy-momas that may invade the adjacent brainstem. Morbidity after radical resection of cerebellar astrocytomas usually is limited.
Recurrence of tumor after radioimaging confirmation of complete surgical removal is uncommon; in the most recent series, the recurrence rate is less than 10%.112,114,117,118 Prognosis most closely parallels the extent of resection; multivariate analyses have also identified solid (rather than cystic) lesions, transitional lesions (versus those confined to the cerebellum), and lesions showing a fibrillary or dif-fuse histology (versus JPA) as potentially significant prog-nostic factors.112,114,115,119 A direct correlation between the volume of residual tumor and outcome has also been reported.112
Indications for radiation therapy are limited in patients with cerebellar astrocytomas. Although radiation therapy has been suggested to be effective for incompletely resected solid lesions, enthusiasm is generally limited for postopera-tive irradiation for any cerebellar astrocytomas.117,120 A small subset of tumors, often those that primarily involve the cerebellar peduncle, will recur after initial surgery; our approach to the treatment of such tumors is to use irradia-tion only after tumor progression after a second attempt at resection. MRI (T2-weighted or fluid attenuation inver-sion recovery [FLAIR] sequences) and MRI/CT fusion are

33 The Brain and Spinal Cord 843
A D
B E
C F
FIGURE 33-5. Medulloblastoma treatment plans. Posterior fossa axial slices are shown for three-dimensional conformal radiation therapy (3D CRT) (A), intensity-modulated radiation therapy (IMRT) (B), and protons (C). Isodose lines are designated for 3D CRT and IMRT: blue, 30.6 Gy; red, 15 Gy; yellow, 10 Gy; purple, 5 Gy. Isodose lines are designated for protons: red, 30.6 Gy; green, 15 Gy. For craniospinal irradiation, axial slices are shown for 3D CRT electrons (D), 3D CRT photons (E), and protons (F). Isodose lines are designated for 3D CRT and IMRT: blue, 23.4 Gy; red, 20 Gy; yellow, 10 Gy; purple, 5 Gy. Isodose lines are designated for protons: aqua/green, 23.4 Gy; light blue, 20 Gy; darker blue, 10 Gy; indigo, 5 Gy. (Continued)
useful for target delineation, and a margin of 0.5 to 1 cm seems adequate. The total dose is 50 to 54 Gy in conven-tional fractionation.
Supratentorial AstrocytomasSupratentorial astrocytomas include diencephalic or central lesions and lesions of the cerebral hemispheres. In children, total resection can be achieved for up to 90% of astrocytomas in the cerebral hemisphere.104,108,121,122 Diffuse cerebral lesions, including those labeled gliomatosis cerebri, can arise in several cerebral lobes with an often low-grade histologic appearance (i.e., fibrillary, WHO grade II) but clinically malignant potential. Similarly, thalamic tumors represent a mix of circumscribed JPAs and diffuse, some-times bithalamic fibrillary tumors; up to 40% of thalamic
gliomas are histologically malignant (i.e., WHO grade III to IV, anaplastic astrocytoma or glioblastoma).122-124 Biopsy alone has been the standard surgery for most tha-lamic astrocytomas because knowledge of the tumor his-tology is important in guiding therapy.95,125,126 However, Bernstein and colleagues127 reported that major resections were performed in up to 33% of patients with circum-scribed thalamic tumors, and the incidence of major opera-tive morbidity was only 7%. Further experience confirmed that limited or aggressive resection might each have a role in the treatment of low-grade thalamic gliomas.128
The role of radiation therapy in childhood astrocytomas is evolving. It is thought to depend on tumor histology and site, age of the patient, and presence or absence of clinical signs. Several reviews129 have shown that radiation therapy

PART 10 Central Nervous System844
G H
I
FIGURE 33-5.—cont’d Sagittal slices are shown for 3D CRT electrons (G), 3D CRT photons (H), and protons (I). Isodose lines are designated for 3D CRT and IMRT: green, 54 Gy; orange, 35 Gy; blue, 20 Gy; red, 15 Gy; yellow, 10 Gy; purple, 5 Gy. Isodose lines are designated for protons: orange, 54 Gy; green, 35 Gy; light blue, 20 Gy; aqua/green, 15 Gy; violet, 10 Gy; dark purple, 5 Gy. (From Lee CT, Bilton SD, Famiglietti RM, et al. Treatment planning with protons for pediatric retinoblastoma, medulloblastoma, and pelvic sarcoma: how do protons compare with other conformal techniques? Int J Radiat Oncol Biol Phys 2005;63:362-372.)
is effective in terms of tumor response, prolonged progres-sion-free interval, and long-term disease control. A joint CCG-POG prospective trial of postoperative irradiation for incompletely resected astrocytomas was abandoned in the early 1990s because the proportion of children in whom gross total or near-total resection could be achieved had increased substantially and because the wisdom of performing irradiation before symptomatic or radioimag-ing-documented progression of disease precluded uniform acceptance of irradiation as a randomized option. Prelimi-nary experience in that trial suggested that observation might be appropriate after substantial resection because disease seems to progress in only a minority of such cases 3 to 5 years after surgery126 (J. Wisoff, personal communica-tion, 2001). For some patients with central low-grade glio-mas (e.g., tectal plate or midbrain; less often, hypothalamic or thalamic), cautious observation can identify indolent, stable tumors that may not require immediate intervention if the child is neurologically stable.106,130 However, this approach implies a commitment to intervene with sur-gery or radiation, or both, when clinical or radiographic evidence of tumor progression appears.
The systematic use of postoperative irradiation has also been questioned in adults.125,131-133 Adults more often have sizable peripheral cerebral hemispheric tumors. Out-come at 5 and 10 years seems to be improved for patients given radiation therapy for incompletely (as opposed to
completely) resected tumors.131-134 A trial by the Euro-pean Organisation for Research and Treatment of Cancer to evaluate postoperative observation versus irradiation for WHO grade I and II hemispheric lesions in adults showed no convincing advantage for early irradiation or for low-dose (45 Gy) versus high-dose (60 Gy) therapy.135
The effect of radiation therapy is well documented for central supratentorial lesions. Neurologic improve-ment has been observed in 80% of patients after irradia-tion for diencephalic tumors. Objective reduction in the size of supratentorial astrocytomas has been confirmed in approximately one half of the patients studied by prospec-tive CT assessment. Long-term survival of patients with biopsy-proven diencephalic lesions usually has required irradiation to therapeutic dose levels.125 Limited-volume, fractionated irradiation has been reported to control most such lesions, with toxicity apparently being more limited in the pediatric age group.136
Optic Pathway GliomaTumors of the optic nerves and chiasm are low-grade astrocytomas that occur predominantly in young children, often younger than 3 to 5 years. In 25% to 30% of cases, the tumors are associated with neurofibromatosis.137 Tumors of the optic nerve often behave as hamartomatous lesions, although up to 50% may extend proximally toward the chiasm. Chiasmatic gliomas manifest with visual and often

33 The Brain and Spinal Cord 845
with endocrine signs; it is often difficult to distinguish chi-asmatic from hypothalamic tumors. In collected reports of 500 cases, 25% of patients with chiasmatic involvement died of tumor-related events.138,139 In an often-quoted series of 36 children, Hoyt and Baghdassarian140 indicated that chiasmatic tumors were indolent and nonthreatening. However, follow-up at a median of 20 years documented a 25% tumor-related mortality rate in a population weighted toward the apparently more benign tumor associated with neurofibromatosis.141,142
The efficacy of radiation therapy for tumors of the optic chiasm with or without hypothalamic involvement has been documented in numerous series.138,143,144 Visual acuity or visual fields are improved in approximately 25%
A
h.t.
B
h.t.
FIGURE 33-6. Midline sagittal T1-weighted MRI scans depict a hypothalamic–optic chiasmatic juvenile pilocytic astrocytoma that filled much of the sella and suprasellar region at diagnosis (A) and at 2 years after completion of radiation therapy (54 Gy delivered in 30 fractions in a multifield, three-dimensional con-formal approach) (B). The involution is typical of juvenile pilo-cytic astrocytomas at this site, including the fairly long interval to reduction. h.t., hypothalamic tumor.
of patients receiving radiation therapy, and neuroimaging shows a reduction in the size of the lesion in these patients.145,146 Survival rates after irradiation for chiasmatic gliomas reportedly range between 75% and 100% in large series of patients followed for 5 to 10 years.138,143-145
Controversy regarding management appropriately sur-rounds the often-benign clinical course of the disease in relation to the potential for treatment-related morbid-ity with surgery or irradiation. Exophytic JPAs arising in the chiasmatic or hypothalamic region are amenable to incomplete surgical resection147; the potential advantage of partial resection lies in delaying more definitive irradiation. Particularly among younger children, a balance between disease progression and the potential risk of adverse endo-crine and intellectual effects from irradiation has favored a conservative approach.138,143 Packer and colleagues148-150 described their experience with chemotherapy, particularly the carboplatin and vincristine regimen. In most young children, previously progressive or symptomatic disease was stabilized with chemotherapy; objective responses were documented in up to 50% of cases, and the median time to disease progression was in excess of 3 years. Initial management with relatively toxicity-free chemotherapy approaches is logical for children with progressive symp-tomatic chiasmatic or hypothalamic tumors, certainly for those younger than 3 to 5 years and possibly for all children before puberty. The frequency and durability of disease control are not clear for children for whom irradiation is begun when their disease progresses during or after chemo-therapy. Outside the investigational setting, the treatment of choice remains primary irradiation for children between 5 and 10 years old because long-term disease control can be achieved in up to 90% of these cases.138,143-145
Radiation Therapy TechniqueRadiation therapy for low-grade astrocytomas uses local target volumes to encompass the typically discrete primary tumor quite narrowly.136,151,152 Uncommonly, low-grade tumors diffusely infiltrate one or more cerebral lobes, requir-ing more wide-field or total cranial irradiation (Fig. 33-7). Low-grade, often pilocytic, astrocytomas are associated with multifocal disease or subarachnoid involvement at diagnosis (or, less commonly, at recurrence) in 15% to 20% of patients with childhood astrocytomas.153-155 Multifocal or metastatic disease is rarely confined to the spinal sub-arachnoid region; multiple disease sites are almost always apparent on cranial MRI studies, obviating any requirement for spinal imaging or staging in patients with this tumor. Specific histologic subtypes of tumors (i.e., pleomorphic xanthoastrocytoma and meningocerebral astrocytoma) can directly infiltrate the contiguous meninges, but this seems to be associated with an indolent, benign course after sur-gery alone.156-158
Establishing the target volume requires detailed MRI. A 1-cm margin beyond the abnormalities shown on T1- or T2-weighted images seems adequate on the basis of early follow-up data from patients for whom three-dimensionally planned and delivered radiation techniques were used.136,151,152,159 A phase II trial by the COG is using MRI/CT fusion for target delineation, a 0.5-cm margin for clinical target volume, and a 0.3- to 0.5-cm margin for planning target volume. The planning target volume is treated by us-ing a conformal technique to 54 Gy in 30 fractions.

PART 10 Central Nervous System846
A dose-response relationship for astrocytoma has not been well defined. In most series, a radiation dose of approximately 50 Gy delivered in 1.8-Gy, once-daily frac-tions has proved adequate.129,138 However, in statistical analyses of rather sizable series of patients, Albright125 and Laws108 and their associates observed an apparent bene-fit conferred by doses above 40 Gy. Justifying dose levels above 54 to 55 Gy in children is difficult in view of the increase in risk at radiation levels approaching cerebral tol-erance. For adults with supratentorial astrocytomas, Shaw and colleagues,134 having shown a dose-response relation-ship indicating improved survival after at least 53 Gy, rec-ommend levels of 55 to 60 Gy. However, two randomized studies of adults with low-grade gliomas testing 50.4 Gy versus 64.8 Gy or 45 Gy versus 59.6 Gy showed no signifi-cant difference in outcome between the lower doses and the higher doses.135,160
PrognosisLaws and colleagues108 reviewed the Mayo Clinic expe-rience with 461 patients of all ages with supratentorial astrocytomas treated between 1915 and 1975. The most important correlates of 10- and 15-year survival were age (86% long-term survival for children and adolescents younger than 20 years versus 33% for those 20 years old or older) and the degree of tumor involvement, reflect-ed by the neurologic deficit and the extent of resection (37% survival rate for patients after biopsy or limited re-moval compared with 55% for those after subtotal or total resection). In Shaw’s review134 of the same Mayo experi-ence with adult patients with supratentorial astrocytomas,
FIGURE 33-7. MRI scan demonstrates the diffuse, multilobar involvement of a biopsy-proven fibrillary astrocytoma. Although predominantly in the left temporal lobe, the lesion also extends throughout the left parietal, right parietal, and mesencephalic regions. Objective improvement in response to irradiation is often transitory. This type of diffuse cerebral tumor, sometimes called gliomatosis cerebri, is a supratentorial lesion analogous to the more typical diffusely infiltrating pontine glioma.
a role for radiation therapy was clearly indicated for most patients with astrocytomas, with 5- and 10-year survival rates of 68% and 39%, respectively, after at least 53 Gy. Patients treated with less than 53 Gy or no irradiation had a 5-year survival rate of 47% (both groups) and 10-year survival rates of 27% and 11%, respectively.
The long-term potential for radiation therapy to con-trol disease specifically in children with hemispheric astro-cytomas has been documented in reviews by Bloom95 and Jenkin96 and their colleagues, who independently reported that the survival rate reached a plateau between 5 and 15 years after postoperative irradiation. The benefit of add-ing irradiation after incomplete resection for children with supratentorial hemispheric tumors was made apparent in the Pittsburgh series reported by Pollack and colleagues.161
Site-specific survival rates suggest that patients with hypothalamic and chiasmatic astrocytomas enjoy longer survival times than do patients with most other types of supratentorial astrocytomas. Bloom and colleagues95 cited 5-year survival rates of 60% to 70% for patients with tha-lamic or hypothalamic tumors after primary irradiation. Albright and colleagues125 reported a mean survival dura-tion of 5.1 years after radiation therapy for patients with diencephalic gliomas compared with a mean survival time of less than 1 year for patients who did not undergo irradia-tion. The virtual lack of tumor progression beyond 5 years after radiation therapy further suggests a role for radiation therapy as a curative modality in the primary management of hypothalamic or chiasmatic tumors.145,162
Brainstem GliomasTumors of the brainstem most often involve the pons (70%), followed by the medulla (15% to 20%) and the midbrain (10% to 15%).163,164 Brainstem gliomas are char-acterized as diffusely infiltrating or focal, depending on the pattern of involvement; focal tumors are well demarcated, confined to one anatomic segment of the brainstem, and occupy less than one half of the brainstem.165 Most focal tumors are JPAs histologically; they occur more often in the midbrain or medulla but can arise in the pons.163,166-
168 Pontine gliomas are largely diffuse (Fig. 33-8).164,165 Dorsally exophytic lesions are relatively benign tumors that usually arise at the pontomedullary junction or from the medulla; histologically, they are JPAs.166-169 In the past, brainstem tumors have been treated conservatively, with histologic confirmation limited to focal or cystic lesions for which knowledge of the histology or drainage might facili-tate treatment.163,164 Findings from biopsied cases indicate that malignant glioma exists in 40% of patients at diagno-sis164; the remaining tumors are largely fibrillary astrocy-tomas.163,170 At autopsy, however, malignant gliomas are found in more than 80% of cases.164,170
Radiation therapy is primarily used for diffusely infil-trating brainstem gliomas. Substantial neurologic improve-ment occurs in 60% to 70% of patients with diffusely infiltrating pontine gliomas, although long-term survival is limited to 10% to 20% of patients with these gliomas.164 Dorsally exophytic tumors are usually identified during surgery for a tumor that otherwise fills much of the fourth ventricle. The lesions in more than one half of the patients remain indolent after incomplete resection; the 40% or more of tumors that do progress are most often controlled with radiation (Fig. 33-9).167,168

33 The Brain and Spinal Cord 847
A B
FIGURE 33-8. A, Sagittal MRI scan depicts a diffusely infiltrating brainstem glioma involving much of the pons and extending to-ward the midbrain and the medulla. B, A typical two-dimensional treatment approach is shown. Use of three-dimensional conformal techniques also may be advantageous.
Radiation Therapy TechniqueBrainstem gliomas tend to infiltrate longitudinally, usu-ally extending beyond the pons to involve the midbrain or medulla and extending peripherally into the cerebel-lum or medial temporal lobes (see Fig. 33-8). Irradiation is limited to the brainstem and immediately adjacent neural tracts. The infiltrative nature of these tumors can be better appreciated on T2-weighted MRI studies. Clinical target volumes are defined with 2-cm margins along the tracts of infiltration (i.e., into the midbrain or medulla, through the peduncles, and into the adjacent cerebellum).171 Given the poor overall outcome for patients with pontine lesions, many centers continue to use two-dimensional, opposed lateral fields in this setting, providing a margin around the known tumor extent.
The standard dose for brainstem gliomas is 54 to 56 Gy, given in a conventional fractionation scheme. In a series of trials, hyperfractionated doses given to total doses of 66, 70 to 72, and 76 to 78 Gy indicated no real benefit from the higher doses.172-174 Most long-term survivors have been adults or children with focal brainstem lesions often located outside the pons (i.e., in the midbrain or medulla).172
The decade-long experience with hyperfractionated therapy for these tumors has encouraged neurosurgeons, radiation oncologists, and pediatric oncologists to enroll patients in multi-institutional protocols. In a randomized trial conducted by the POG, conventional fractionation to 54 Gy was documented to be as effective as 70 Gy given in twice-daily 1.2-Gy fractions.175 This trial also documented the apparent negative effect of irradiation in combination with concurrent cisplatin in this setting.175,176
PrognosisThe 5-year overall survival rates are 10% to 20% for children with brainstem gliomas and 20% to 30% for adults.172-174 Median survival after irradiation is only 8 months for patients with classic intrinsic tumors in the pons. Hoffman and colleagues166,167 initially identified as highly favorable a subset of children in whom exophytic tumors extended into the fourth ventricles. However, it is
now understood that these tumors are usually JPAs168; sur-vival after surgery, with or without radiation, approaches 90% in this selected group.166-168 Intrinsic pontine tumors, constituting most of the classically identified brainstem gliomas, are usually associated with multiple cranial nerve palsies, diffusely hypodense lesions on CT or MRI stud-ies, and a high-grade histologic appearance indicative of an infiltrating, aggressive neoplasm. Long-term survival rates
FIGURE 33-9. Sagittal MRI scan shows a dorsally exophytic brainstem glioma. This discrete, briskly enhancing tumor fills much of the fourth ventricle, attaching along the posterior aspect of the brainstem at the pontomedullary junction. Invasion may not be apparent on imaging, and at surgery, lesions often are found to blend imperceptibly with the underlying brainstem.

PART 10 Central Nervous System848
for the latter group have consistently been less than 15%. Less common intrinsic tumors that are focal and confined to a segment of the pons or midbrain are associated with slightly better long-term survival rates.165
Chemotherapy regimens have little effect on brainstem gliomas. Adjuvant therapy did not affect outcome in the only published randomized trial.177
EpendymomasIntracranial ependymomas occur predominantly in young children, but they are also seen in older children and adults. Ependymomas also occur as primary spinal cord neo-plasms, but this presentation is more common in adults. Posterior fossa ependymomas typically manifest with the same symptom triad as other posterior fossa tumors in chil-dren—headache, vomiting, and ataxia. Associated symp-toms include torticollis and lower cranial nerve dysfunction. The median age of children with these tumors is 4 years; however, almost 30% of infant brain tumors (i.e., those in children younger than 3 years) are ependymomas.178,179 Infratentorial lesions in younger children may occur more often in girls than in boys. Supratentorial lesions more often manifest with seizures or focal neurologic abnormalities and are most common in adolescents and adults.
Tumors of the posterior fossa occur predominantly in children; these tumors show a predilection for the fourth ventricle in young children and often involve or origi-nate within the region of the foramen of Luschka (Fig. 33-10).179,180 Direct extension through the foramen mag-num into the upper cervical spinal canal is a characteristic pattern of growth. Ependymomas disseminate into the sub-arachnoid space in approximately 12% of children.95,181-184 However, this manifestation is more often seen at diagno-sis or as a primary site of recurrence in very young chil-dren and may be associated with an anaplastic histology; in older children, this pattern is more common after local recurrence than earlier in the disease.183,184 Supratentorial tumors often arise in regions adjacent to the ventricular system, and growth occurs largely through intraparenchy-mal extension.185
Ependymomas arise from the ependymal cells lining the ventricular system and the central spinal canal. The tumor characteristically includes ependymal rosettes and perivascular pseudorosettes. Ependymomas are differen-tiated or low-grade lesions; variants include cellular, clear cell, tanycytic, and papillary types.69 In one series, 15% to 30% of ependymomas were classified as anaplastic tumors (i.e., WHO grade III), marked by increased cellularity and mitotic rate. The tumors usually are well demarcated but can show parenchymal invasion.69,115 Although ependy-momas were regarded by leading neuropathologists in the 1980s as being of little clinical significance, an association has since been recognized between an anaplastic histology and a less favorable outcome.186-192 Ependymoblastomas are rare embryonal tumors and are discussed with the other supratentorial PNETs.
Surgery is the initial intervention for most intracranial ependymomas. Even extensive tumors of the fourth ventri-cle can often be grossly resected; total resection of tumors extending into or arising in the cerebellopontine angle has been achieved.180,190 The advantage of near-total or total resection is apparent, with considerable improvement in disease control in children in whom complete resection was achieved.189-191 The price of this control is a significant incidence of new postoperative neurologic deficits, includ-ing the posterior fossa syndrome and major new bulbar signs (e.g., palsies of cranial nerves IX and X resulting in difficulty with speech and airway protection), sometimes requiring postoperative tracheostomy or the placement of a feeding tube.88 Institutional experience shows that gross total resection can be accomplished in 50% to 60% of patients with infratentorial ependymoma; however, a total resection rate as high as 90% has been reported.190
Postoperative irradiation is essentially routine for patients with ependymomas, almost regardless of age, because ad-juvant radiation has been shown to increase disease control rates in several major series.190,192 However, a single expe-rience suggests that disease could be controlled in a certain subgroup of children with supratentorial ependymomas who are treated with total resection alone; in this ongoing
A B
FIGURE 33-10. A typical ependymoma involving the fourth ventricle. A, Axial CT scan reveals a lesion that fills much of the fourth ventricle and extends through the right foramen of Luschka. B, Sagittal MRI scan shows the tumor extending caudally along the medulla and below the foramen magnum into the upper cervical spinal canal.

33 The Brain and Spinal Cord 849
COG prospective trial, only a small proportion of patients with such ependymomas is being treated with observation only.193 For all lesions of the fourth ventricle or cerebel-lopontine angle, high rates of tumor control have been achieved only for patients treated with local postoperative radiation and radical resection.189-191,194 Long-term disease control was accomplished in approximately 70% of such children, compared with 20% to 30% of those treated with incomplete resection and similar radiation.
Ependymomas respond to a variety of chemotherapeu-tic agents, including cyclophosphamide and vincristine, cisplatin and carboplatin, and etoposide. A randomized trial of adjuvant lomustine, vincristine, and prednisone conducted by the CCG showed no benefit from this chemotherapy.195 The initial experience in infants with ependymomas indicated an inverse relationship between the duration of chemotherapy (equivalent to the time of initiating radiation therapy) and disease control, encour-aging current institutional and cooperative group trials to limit the use of chemotherapy for this tumor; only for the youngest children (<18 months old) has a brief (3 to 4 month) course of chemotherapy been used before radiation (or second resection and radiation if measurable disease is apparent at the completion of chemotherapy).194 For infants, interest in chemotherapy dose escalation contin-ues because of positive preliminary results from the second POG study of infant brain tumors, results that suggested that dose-intensified chemotherapy produced better dis-ease control rates than did standard chemotherapy.196 In older children, the usefulness of limited-duration chemo-responsiveness in facilitating second operative resections before radiation is being examined in a COG trial.
Most clinical experience with ependymomas is based on treatment volumes for infratentorial lesions that include the entire posterior fossa and often the upper cer-vical spinal canal to one to two vertebral levels below the caudal tumor extent. Because recurrent disease is almost always localized to the initial tumor bed and often the site of attachment and because minimal residual disease is left adjacent to the brainstem or peduncle, current prospec-tive investigations are targeting only the local tumor bed (with margins as tight as 1 cm) using three-dimensional conformal or intensity-modulated radiation therapy (Fig. 33-11).159 However, findings during an as yet insufficient follow-up period indicate that the limited treatment vol-umes should be used with caution outside a controlled set-ting. For supratentorial lesions, a 1- to 2-cm margin around the initial tumor extent is indicated, with potential modi-fications when the normal brain is reconfigured by tumor resection. Treatment volumes for differentiated and ana-plastic ependymomas usually are not different.197,198 Pre-vious interest in CSI for anaplastic infratentorial lesions has not continued into contemporary protocols or treatment standards, except in cases in which neuraxis involvement is documented at diagnosis.
Classically, radiation doses of 45 to 54 Gy have been used.182,189,192 However, doses of 54 to 55.8 Gy have been reported to achieve superior results and are indicated even after gross total resection.199,200 Despite apparently encour-aging results from a small POG trial of hyperfractionated radiation (70 Gy given twice daily in 1.2-Gy fractions) for patients with posterior fossa ependymomas, no substanti-ated role has been established for altered fractionation. The
potential value of dose escalation is being explored in trials testing cumulative doses approaching 60 Gy.159
Pineal Region and Germ Cell TumorsA unique group of tumors occur in the pineal region: germ cell tumors, pineal parenchymal tumors, and glial and ependymal tumors (Table 33-3).69,116,201 Intracranial germ cell tumors occur predominantly in the pineal region, although they can also arise in the anterior third ventricu-lar (suprasellar) region and, less commonly, in thalamic or deep cerebral hemispheric areas.
This unique group of tumors manifests with clinically and histologically linked syndromes. Pineal region germinomas occur predominantly in adolescent boys and are associated with multifocal or metastatic disease in the anterior third ventricular region in 10% to 40% of cases.202-206 Suprasellar (anterior third ventricular) germ cell tumors occur more broadly throughout the pediatric age group and about equally in girls and boys; these tumors are often germinomas but also include other germ cell types. Pineal parenchymal tumors in children are overwhelmingly malignant pineoblastomas, with a considerable proportion occurring in infants and children younger than 2 to 3 years as highly aggressive, widely metastasizing, small, round, blue cell tumors. Pineocytomas are decidedly less common in children occurring more often in adults.69,207-209
Regardless of histology, pineal region tumors typically manifest with Parinaud’s syndrome, consisting of near-light dissociation (i.e., pupillary responses are diminished to
FIGURE 33-11. The treatment plan shows the isodose volumes for a three-dimensional conformal approach, using multiple non-coplanar 6-MeV photon fields to encompass the tumor within the lower aspect of the posterior fossa and the upper-most spinal canal. The target volume in contemporary protocols more often addresses the tumor bed or surgical bed than the full posterior fossa.

PART 10 Central Nervous System850
light but are maintained with attempted accommodation), lack of upward gaze, and incomplete ability to accommo-date. Obstructive hydrocephalus often occurs when the tumors are near the sylvian aqueduct. Suprasellar lesions can also manifest as hydrocephalus when the growing tumor obstructs the foramen of Monro; diabetes insipidus and visual field deficits are often apparent.
Although sometimes debated in the past, it is important to histologically establish the diagnosis of pineal region tumors. Suprasellar lesions have usually been biopsied be-cause of their relative accessibility and the broad differential diagnosis that includes astrocytomas of the hypothalamic or chiasmatic region and craniopharyngioma. Germ cell tumors can occasionally be definitively diagnosed on the basis of chemical markers. Any significant elevation of the alpha-fetoprotein level in the serum or CSF is diagnostic of a malignant germ cell histiotype (typically embryonal car-cinoma, yolk sac tumor, or teratocarcinoma), and marked elevation of β-human chorionic gonadotrophin level (β-HCG; typically more than 100 to 1000 mIU/mL) is diag-nostic of a choriocarcinoma or malignant mixed germ cell tumor (with choriocarcinomatous elements).210,211 Mod-erate elevation of the β-HCG level (50 to 100 mIU/mL) is compatible with a germinoma, but cytologic or histologic evidence is required to confirm the diagnosis.212 After a diagnosis is established, neuraxis staging (e.g., spinal MRI, lumbar CSF cytology) is mandatory for any of the germ cell tumors and pineoblastoma.
TABLE 33-3. Histologic Classification and Relative Incidence of Pineal Region Tumors
Histologic Type* Relative Frequency†
Tumors of Germ Cell Origin
Germinoma 60% to 80%
Teratoma (differentiated, immature, malignant)
65%
Endodermal sinus tumor 18%
Embryonal carcinoma 7%
Choriocarcinoma 5%
Tumors of Pineal Parenchymal Origin
14%
Pineoblastoma
Pineocytoma
Tumors of Glial Origin 15%
Astrocytoma
Malignant glioma
Ganglioglioma (ganglioneuroma)
Ependymoma
*Modified from Burger PC, Scheithauer BW, Vogel FS (eds). Surgical Pathology of the Nervous System and its Coverings, 3rd ed. New York: Churchill Livingstone, 1991.†Modified from Burger PC, Scheithauer BW, Vogel FS (eds). Surgical Pathology of the Nervous System and its Coverings, 3rd ed. New York: Churchill Livingstone, 1991; Kleihues P, Cavenee WK (eds). Tumours of the Nervous System. Lyon, France: IARC Press, 2000.
An open craniotomy is usually required to biopsy su-prasellar tumors.213 Biopsy has been possible during third ventriculoscopy, often at the time of ventriculoperitoneal shunt insertion or third ventriculostomy. Pineal region tumors can be approached stereotactically, but their chal-lenging location adjacent to the major draining intracra-nial veins has led many neurosurgeons to prefer an open approach. Tumor resection is feasible in the pineal region, although done in only a few instances because of the high rate of potential complications. Although insertion of a ventriculoperitoneal shunt is often necessary, the notable incidence of shunt metastasis (with tumor arising through-out the peritoneal cavity),212,213 although low in absolute terms, is relatively more common for this group of tumors than for any other intracranial lesions. Performance of a third ventriculostomy, rather than placement of a ventricu-loperitoneal shunt, is encouraged for accomplishing inter-nal decompression.
Radiation Therapy TechniqueRadiation therapy is highly curative in patients with germinomas in the pineal region, anterior third ventricle, or multiple midline locations.205,211,214-220 Considerable debate, however, surrounds the appropriate radiation vol-ume for these tumors.206 Given the recognized incidence of intraventricular and subarachnoid dissemination, cra-niospinal (or less often, full cranial) irradiation has been recommended for pineal region and suprasellar germino-mas.205,214,221 The outcome in many series indicates that disease is controlled in up to 95% of patients treated with full neuraxis radiation as a component of their therapy (Table 33-4).203,206,215,218-225 Local irradiation, variably defined as encompassing the primary tumor site with a margin or the entire third ventricular region, has been associated with long-term disease-free survival rates of more than 80% (see Table 33-4).203,206,215,218-225 The inci-dence of neuraxis dissemination varies from less than 10% to 35%.206,214,219,221,226 No consensus has been reached regarding the appropriate radiation volume because cure rates are relatively high for local and full-neuraxis irradia-tion, and the toxic effects associated with the relatively low doses necessary for this disease are exquisitely age related.218,220
Evidence is increasing that 45 Gy delivered to the pri-mary tumor site is adequate to ensure virtually uniform control of pineal region and suprasellar germinomas. Wider-field components (craniospinal or, as done at some institutions, full cranial irradiation) can be limited to doses of 25 Gy.216,218,219 CSI doses as low as 18 to 19.8 Gy in children with no detectable leptomeningeal metastasis from germinomas at diagnosis have been reported to be effective in preventing leptomeningeal recurrence.227
Considerable interest has been expressed in chemo-therapy for intracranial germinomas. Although a high rate of response has been documented, durable control of dis-ease has been achieved in only about one half of the pa-tients treated with chemotherapy only, including some of the more rigorous treatment regimens that carry a 5% to 10% rate of toxicity-related death.222,224,225,228 CSI is often a successful salvage treatment for germinomas that recur after such therapy.218
Early studies conducted by Allen and colleagues223,229 established that disease control was excellent after combined

33 The Brain and Spinal Cord 851
TABLE 33-4. Therapy and Outcome in Intracranial Germinomas
Therapy
Radiation Therapy
Chemotherapy 5-Year NED Rate (%) Study and ReferenceCSI Local (Gy)
RT only + 50-55 85 Shibamoto et al, 1988221
+ 45-55 86 Rich et al, 1985203
+ 45-59 97 Hardenbergh et al, 1997219*
+ 45-50 91 Bamberg et al, 1999222
CrI, VtI 50-54 91 Wolden et al, 1995206
0 40-50 87 Calaminus et al, 1994220
0 44 90 Haddock et al, 1997215
+ 50 100 Merchant et al, 2000218
Chemotherapy and reduced RT
0 30 Cyclophosphamide 91 Allen et al, 1987223
0 40 VP-16/CBCDA; VP-16/ ifosfamide
96† Bouffet et al, 1999224
0 30 (CBCDA or CDDP); vinblastine; bleomycin
92 Calaminus et al, 1994220
Chemotherapy only 0 0 CDDP, VP-16, bleomycin 42 Balmaceda et al, 1996225
*Includes cases from Rich et al, 1985203 (CSI or CrI, dose of 15 to 44 Gy).†Event-free survival at 3 years.CBCDA, carboplatin; CDDP, cisplatin; CrI, full cranial irradiation; CSI, craniospinal irradiation (dose levels 24 to 30+ Gy for localized tumors); NED, no evidence of disease; RT, radiation therapy; VP-16, etoposide; VtI, full ventricular volume irradiation (typically to doses of 20 to 36 Gy), +, used; 0, not used.
chemotherapy (with cyclophosphamide or carboplatin) followed by limited-volume, reduced-dose radiation. Strat-egies incorporating moderately aggressive chemotherapy and local radiation (to 30 to 36 Gy for patients showing a good partial or complete response, as shown on imag-ing studies and by normalization of any elevated markers) or limited-dose CSI (for those with disease dissemination) result in disease control rates exceeding 90%, with limited toxic effects.220,222,224,228 Whether such an approach of-fers any advantage over radiation therapy alone is unclear; prospective trials of this approach are being conducted in Europe and by the COG. It is difficult to improve on the disease control rates produced by primary irradiation, al-though prepubertal patients and those who require CSI before completion of skeletal growth may benefit from a combined-modality approach.
In patients with malignant germ cell tumors (i.e., em-bryonal or yolk sac carcinoma, choriocarcinoma), treat-ment with radiation therapy alone has rarely controlled disease in more than 25% to 40% of cases.213,220 Combined radiation and chemotherapy seems to be beneficial in such cases, but the chemotherapy must be relatively aggressive, and the radiation dose to the craniospinal axis is usually 24 to 36 Gy, followed by a boost dose to the tumor bed of 9 to 25 Gy, depending on the response to prior chemo-therapy.230,231
PrognosisA fairly favorable outcome has been observed for patients with pineoblastomas treated with radiation therapy (in-cluding CSI) and chemotherapy (including alkylating
agents or nitrosoureas in conjunction with vincristine).232 Disease has been controlled in up to 60% of patients, compared with the 0% to 10% survival rates for infants treated with prolonged chemotherapy with or without radiation.178
CraniopharyngiomaCraniopharyngiomas are histologically benign tumors de-rived from squamous cell rests in the region of the pituitary stalk. More than one half of these tumors occur in patients younger than 18 years, and craniopharyngiomas represent 3% to 9% of the intracranial tumors of children. The tumor arises as an extra-axial lesion, typically a densely calcified, solid tumor in the suprasellar region with large cystic com-ponents (Fig. 33-12). These histologically classic adaman-tine tumors occur in children and adults.233 Less common are the noncalcified, squamous papillary type, which usu-ally occur in adults.69,115
Total surgical resection is usually curative in patients with craniopharyngiomas.233-240 The decision about whether to use surgery or radiation therapy depends on the site of origin and growth of the tumor, which often damages the hypothalamus or optic chiasm and sometimes damages the adjacent major vessels. Although encapsulated, the lesion usually adheres to these vital structures, even though it does not infiltrate to the level of the tuber cinereum.234-236 Modern microsurgical techniques allow total resection in up to 75% of cases, with operative mortality rates of 1% to 3%.236,241-243 The incidence of long-term functional deficits may be higher among patients who undergo radical resec-tion than among those treated with radiation.237,244-247

PART 10 Central Nervous System852
Kramer and colleagues248,249 established the effectiveness of high-dose radiation after limited cyst aspiration, initially reporting 5-year survival for 9 of 10 patients and with later follow-up showing 13- to 15-year survival for 6 of 6 chil-dren.250 Subsequent series showed similarly impressive long-term survival data.239,251-254 Bloom and colleagues95 updat-ed Kramer’s initial findings, reporting a 10-year survival rate of 85% for the children and a 10-year relapse-free survival rate of 80%.95 Disease control is even better in young adults (92% at 20 years for patients 16 to 39 years old at the time of diagnosis).254 These latter figures are equal to the best results observed in primary surgical series when corrected to account for cases with incomplete resection.235,243
Radiation Therapy TechniqueRadiation therapy for craniopharyngioma is designed to narrowly encompass the solid and cystic components of a well-delineated, central neoplasm. Much of the published information involves treatment using coronal arcs of 180 to 220 degrees; three-dimensional conformal or fraction-ated stereotactic radiation therapy is being used to improve dose conformity.239,251-254
Craniopharyngiomas show a radiation dose-response relationship. Bloom and colleagues95,181 reported a supe-rior outcome in response to 50 to 55 Gy compared with the response to less than 50 Gy. Doses of 50 to 54 Gy at 1.8 Gy per fraction are recommended for children. It is not clear that higher doses are necessary or desirable for adults. Doses in excess of 60 Gy are associated with significantly greater toxicity, especially in the visual system, with little improvement in survival.95,181,255
Single-fraction radiosurgery has been used more broadly in Europe than in the United States.255,256 Radiosurgery may be appropriate for children with small foci of residual disease, particularly disease that is limited to intrasellar de-posits or foci of disease remote from the hypothalamus and chiasm.255,257
FIGURE 33-12. Midline sagittal non-enhanced MRI scan dem-onstrates a craniopharyngioma involving the upper aspect of the sella, with a solid component extending into the suprasellar region along the pituitary-hypothalamic stalk. The cystic com-ponent is visible superiorly.
PrognosisExcellent long-term survival rates have been attained for patients who undergo total resection or planned limited surgery and radiation. The proportion of patients in recent series who underwent successful resection approximates 75%.233-241,243,258 However, even the most vociferous ad-vocates of surgery acknowledge the existence of residual calcifications or apparently viable, radiographically obvious tumor in up to 50% of postoperative CT studies of patients who have undergone gross total resection.234-236 The rate of disease recurrence after complete resection ranges from 10% to 30%.233-235,241-243,259 Despite the benign nature of craniopharyngioma, tumor progresses in 70% to 90% of pa-tients after incomplete resection and without radiation at a median of 2 to 3 years.254,259,260
Primary radiation after cyst decompression or par-tial resection has been associated with progression-free survival rates of 80% to 95% at 5 to 20 years.95,181,238,
251-255,258,259,261 Survival rates of 90% to 100% are common among children and adults.
The relative toxicity of primary surgery and radiation for craniopharyngioma are becoming increasingly appar-ent. Diabetes insipidus occurs in 75% to 100% of patients after complete surgical resection.233,241,246,247 Endocrine dysfunction involving other pituitary-hypothalamic hor-mones has occurred in 40% to 80% of patients after sur-gery.246,247 Hypothalamic obesity is apparent in more than 50% of long-term survivors; it is less common among those who undergo limited surgery and radiation.246,247 Undesir-able personality changes are associated with resections that damage the hypothalamus.
An increased endocrine deficit has been identified in patients whose primary treatment was surgery compared with those who underwent limited resection and radia-tion.246 Up to 25% of children show significant decreases in vision after resection241,243; reports of visual compli-cations from radiation therapy have been anecdotal.255 Overall performance, intellectual function, and memory seem to be equal or better in the population treated by conservative surgery and radiation than in those treated surgically.237,245,253,255
Primitive Neuroectodermal TumorsIn 1973, Hart and Earle262 described the cerebral PNET as a malignant embryonal tumor that affects children and young adults. The tumor accounts for approximately 3% of supratentorial neoplasms. PNETs are large, often cystic hemispheric tumors characterized histologically by a highly cellular, undifferentiated infiltrate that includes vascular endothelial hyperplasia and necrosis.69,262,263 In classic descriptions, focal areas of glial or neuronal differentiation constitute less than 5% to 10% of the tumor. The clini-cally similar cerebral neuroblastoma is distinguished from the Hart/Earle PNET by its degree of neuronal differen-tiation.264-266 The specific cerebral PNET encountered in a patient, however, must be distinguished from the broad concept of PNETs advanced by Rorke and colleagues, as discussed earlier in this chapter.69,70,162,267
Cerebral PNETs infiltrate widely despite their cir-cumscribed gross appearance. The tumor can also arise multifocally. About one third of cases involve ventricu-lar or spinal subarachnoid dissemination.261 The more

33 The Brain and Spinal Cord 853
differentiated cerebral neuroblastoma has been associated with CSF metastasis in an equal proportion of patients at autopsy, although isolated involvement of the subarach-noid space is uncommon.261,264,266,268
Studies conducted by the CCG have documented the efficacy of combining chemotherapy (the tested regi-men included lomustine, prednisone, and vincristine) with CSI for children with cerebral PNETs who are more than 3 or 4 years old.232,263,267,269-271 Long-term survival approached 60% in this group. For infants and young chil-dren, therapeutic approaches are comparable with those used for other embryonal CNS lesions in this age group (see “Tumors in Children Younger than 3 Years”). Despite anecdotal reports of disease control after cranial irradia-tion, CSI is considered standard therapy for supratentorial PNETs, including cerebral neuroblastoma and pineoblasto-ma.232,268 The doses and techniques used for supratentorial PNETs are similar to those described for medulloblastoma, with typically a 2-cm margin planned around the tumor bed to define the clinical target volume.
Tumors in Children Younger than 3 YearsBetween 15% and 20% of pediatric brain tumors occur in infants and children younger than 3 years. The most common tumors in this age group are astrocytomas (pri-marily optic chiasmatic or hypothalamic tumors; cere-bellar astrocytomas are uncommon), embryonal tumors (medulloblastoma, PNET, and pineoblastoma), ependy-moma, and malignant gliomas.272-274 Tumors occurring almost uniquely in this age group include atypical tera-toid or rhabdoid tumors and choroid plexus neoplasms (papillomas and carcinomas).275-279 Desmoplastic in-fantile astrocytoma and ganglioglioma are uncommon, and when they do occur, they are typically large tumors that are biologically benign.280 The operative mortality is relatively high in this age group because of tumor pre-sentations (often sizable, midline or multilobed supra-tentorial lesions) and the relative lack of elasticity of the still-myelinating brain.
The infant brain is particularly vulnerable to the effects of radiation therapy, particularly with regard to neurocog-nitive development.281 Survival rates for patients in this age group with ependymoma or medulloblastoma are sig-nificantly lower than those for other age groups because the tumor in these very young patients is often advanced at presentation and because tumoricidal radiation doses can-not be used.95,177,181,271,282-284
The use of prolonged chemotherapy after surgery to delay or obviate the use of radiation therapy for very young children has been studied for almost 20 years (Fig. 33-13).178,285-291 Trials of treatment for medulloblastoma in infants conducted by the POG, CCG, and International Society of Paediatric Oncology (SIOP) have documented that chemotherapy is effective in only a minority of patients; durable disease control has been achieved in 20% to 30% of patients with chemotherapy alone and in only 35% of those treated with response-defined consolidative radiation.178,288-292 Salvage radiation has achieved a surpris-ing degree of secondary control after progression during chemotherapy, but the dose required to overcome chemo-therapy resistance produces late changes in intelligence quotient that make this an ethically unacceptable alterna-tive.291,293 A trial from Germany in which postoperative
intravenous and intraventricular chemotherapy without radiation therapy was used for infants with medulloblas-toma showed 5-year progression-free survival rates of 82%, 50%, and 33% for infants who had complete resection, residual tumor, and macroscopic metastases, respective-ly.294 Because these results seem to be better than those in any previous report, they will need confirmation. For infants with ependymoma, earlier intervention with radiation after prolonged chemotherapy may help control disease; however, this strategy too seems to work in only a minority of cases.194 Chemotherapy alone has been an unsuccessful postoperative intervention.295 Reports of sur-vival of patients with pineoblastoma and atypical teratoid or rhabdoid tumors treated with this approach have been anecdotal.178,194,232,296
The current generation of infant brain tumor trials foc-uses on the judicious use of irradiation. Based on preliminary data for children with recurrent medulloblastoma, the frontline approach in the Pediatric Brain Tumor Consortium and COG trials is to introduce early, limited-volume, three-dimensional conformal radiation therapy to the posterior fossa and primary tumor site alone for patients with M0 medulloblastoma and to the local tumor bed only for those
Years postdiagnosis
Time from diagnosis in years
A0 2 4 6 8
0
120
0
10.90.80.70.60.50.40.30.20.1
90
60
304 8
10 1
Pro
babi
lity
B
Inte
llige
nce
quot
ient
Progression-free survival
(51 ± 10%)
(21 ± 8%)
Survival
FIGURE 33-13. A, Survival and progression-free survival for 29 infants and children younger than 4 years with medulloblasto-ma. During the study period (1984-1995), prolonged chemother-apy was used in the hope of delaying or obviating the substantial neurotoxicity associated with irradiation in young children. The stable progression-free survival rate after 18 months (21%) reflects the use of irradiation as adjuvant therapy (for those with resected or stable disease during 12 to 24 months of chemo-therapy); the 51% overall survival rate at 5 years reflects a high salvage rate obtained from the use of craniospinal irradiation for persistent or progressive disease. B, Among the 19 patients who survived for more than 24 months, the high survival rate came at the cost of a steady decline in full-scale intelligence quotient scores, from a pretreatment level approximating 90 to a level just above 60 at 7 years. (From Walter AW, Mulhern RK, Gajjar A, et al. Survival and neurodevelopmental outcome of young children with medulloblastoma at St. Jude Children’s Research Hospital. J Clin Oncol 1999;17:3720-3728.)

PART 10 Central Nervous System854
with supratentorial PNETs.292 For patients with atypical teratoid or rhabdoid tumors, targeted radiation volumes are used after just 2 months of chemotherapy for children 12 months of age and older.296 For those with ependymo-mas, the trend is toward immediate postoperative radia-tion, at least for patients with tumors that can be grossly resected.159
tumors Common In adultsMalignant Gliomas: Anaplastic Astrocytoma and Glioblastoma MultiformeThe dominant primary intracranial tumors that occur in adults in terms of frequency and mortality are the malignant gliomas. These tumors occur in the cerebral hemispheres as sizable, rapidly growing lesions with a characteristic ringlike, enhancing appearance on CT or MRI, with central necrosis, infiltrating margins, and sur-rounding low-density changes (Fig. 33-14). Malignant gliomas occur in all age groups but predominate in the fifth and sixth decades, and they account for 35% to 45% of all adult brain tumors.
Histologically, malignant gliomas are heterogeneous neoplasms composed of fibrillary astrocytes; gemistocytes; large, bizarre glial cells; and small anaplastic cells.69,115 In Kernohan and Sayre’s classic categorization297 of astrocytic neoplasms, which defined these tumors as grade III and grade IV astrocytomas, malignant gliomas were thought to represent progressively dedifferentiated astrocytic tumors marked by a certain degree of pleomorphism, hyperchro-maticism, and mitosis. In contemporary neuropathology, malignant gliomas are classified as anaplastic astrocytoma or the more malignant glioblastoma multiforme, with the latter identified by the presence of tumor necrosis.298 Anaplastic astrocytomas account for 10% to 15% of malig-nant gliomas; more than 85% are glioblastomas.299
Malignant gliomas typically infiltrate the adjacent nor-mal brain. Detailed comparisons of imaging and histologic findings have established the anatomy of malignant glio-mas. Histologically, the central low-density region seen on neuroimaging studies is a necrotic and hypocellular area. The surrounding ring of enhancing tissue is composed of densely cellular tumor. The hypodense area beyond the en-hancing tissue seen on CT scans is hypocellular and edema-tous but infiltrated by small anaplastic T cells.300 In 50% of cases, scattered tumor cells immediately surrounding the hypodense volume are evident histologically.301 The often sizable area of increased signal on T2-weighted MRI similarly contains infiltrates of viable T cells.302 Tumor cells characteristically extend along neural tracts and across the corpus callosum.301 Distant subarachnoid or subependy-mal extension occurs in 5% to 9% of patients with malig-nant gliomas.303,304
Surgery for malignant gliomas is usually limited to subtotal resection. Macroscopically, complete removal is achieved in only 10% to 20% of cases.305-308 The extent of residual tumor visualized on postresection CT scans seems to correlate with outcome, with increased time to progres-sion and survival being associated with smaller residual tu-mor volumes among adults and children.297,309
Radiation therapy has been the most effective treat-ment for these aggressive lesions, but it usually can only delay disease progression or recurrence. Early clinical trials conducted by the Brain Tumor Study Group con-firmed the clinical efficacy of radiation. Median survival increased from 14 weeks after surgery to 36 weeks for patients given postoperative radiation.306 The survival rate at 1 year was 24% for patients also treated with radiation therapy, compared with only 3% for patients who had surgery only.306 One fourth to one half of patients who receive radiation therapy show clinical improvement. Up to 60% of patients are able to return to work and achieve full function.310-312
A B
FIGURE 33-14. MRI scans show a glioblastoma multiforme arising in the left thalamic region and extending just beyond midline. A, Gadolinium-enhanced T1-weighted MR image shows a ring-enhancing periphery with a dark, necrotic center. B, T2-weighted MR image shows surrounding edematous changes.

33 The Brain and Spinal Cord 855
Despite documented improvement in time to progres-sion and survival, the response to radiation illustrated by imaging studies is complex and rarely indicative of rapid or significant disease reduction. Essentially all glioblastomas and 65% to 80% of anaplastic astrocytomas recur within 2 to 5 years and result in rapid death, causing malignant gliomas to live up to their reputation of being one of the most aggressive and lethal tumors.310 Although the anat-omy of malignant gliomas suggests that disease extension or metastasis is the source of recurrence, recurrent disease almost always arises from within the central or enhancing portion of the tumor.313-317 The central tumor is relatively radioresistant, perhaps because of an inherent lack of ra-diosensitivity or a hypoxic, relatively radioinsensitive ne-crotic core.316,317 This pattern of intralesional recurrence has stimulated several lines of clinical investigation to over-come hypoxic cell resistance; considerable interest has also been expressed in exploiting the time-dose relationship to identify an altered fractionation regimen of value in treating this tumor.299,312 Several trials have tested modifications in radiation delivery, including physical modalities other than photons and local boost techniques incorporating intersti-tial brachytherapy or stereotactic radiosurgery.318-329
Early trials of radiosensitizers focused on the nitro-imidazoles misonidazole and etanidazole.330 Later stud-ies have investigated carbogen and nicotinamide. Despite some improvement realized from use of these agents with suboptimal radiation, clinically meaningful benefit was not achieved.331,332 Long-standing interest in the halogenated pyrimidines bromodeoxyuridine and iododeoxyuridine has resulted in several trials of their use with conventional and altered fractionation, but only a marginal benefit has been suggested by the results.333-336
The use of radiation with high-LET particles has been examined in clinical trials as a possible way of overcoming the apparent oxygen-related radioresistance of these tu-mors. However, the use of fast–neutron beam radiation has produced no significant improvement over conventional photon radiation.318,322,337 The rationale for using proton radiation stems more from the ability to restrict the vol-ume of tissue irradiated than from its being less affected by oxygenation; trials of doses as high as 90 Gy suggest a potential benefit in terms of central tumor control, but no early demonstration of improvement in outcome has been seen.338
Stereotactic interstitial implantation of radioactive sources has been done at several European centers since the 1950s. Over the past 2 decades, prospective studies of temporary stereotactic brain implants using high-activity iodine 125 (125I) have evaluated the toxicity and efficacy of volume-limited, high-dose radiation delivery.319-321 Among selected patients with limited-volume recurrent malignant gliomas, geometrically planned implantations of radiation sources delivering an average of 60 Gy to the enhancing lesion over 6 days resulted in survival durations of approxi-mately 1 year for those with glioblastomas and 1.5 years for those with anaplastic astrocytomas.319-321,326,339 Results of the Brain Tumor Cooperative Group’s prospective ran-domized trial suggested that interstitial boost radiation could be beneficial in appropriately selected cases.340
Patients with malignant gliomas who are potentially suitable for local types of therapy (e.g., brachytherapy, ra-diosurgery) are those with a relatively favorable prognosis,
constituting 20% to 40% of cases. The criteria for implanta-tion include Karnofsky performance status scores above 70, unifocal supratentorial lesions less than 6 cm in the great-est diameter, and no involvement of the midline, corpus callosum, or subependyma.319,321 A retrospective review of unselected patients treated with standard external beam ra-diation therapy to the brain (EBRT) revealed that outcome was significantly better among implant-eligible patients with glioblastoma (median survival of 14 months) than among those who were ineligible (median survival of less than 6 months),341 indicating that any perceived improve-ment in outcome in patients attributed to the brachyther-apy may be artificial. However, median survival duration and 2- and 3-year survival rates for patients with glioblas-toma treated with 125I brachytherapy seem to be superior in single-institution experiences and in comparison with the previously described findings.319,321,341 Comparable data for anaplastic astrocytomas are less convincing.321,341
Symptomatic local necrosis occurs in 40% to 50% of patients with interstitial implants, and this often requires surgical intervention.320,321,326,327,332 Ultimate survival has been reported to be superior in patients who require a second operation, which presumably reflects the combination-treatment effect.320
Stereotactic radiosurgery has been used to achieve a high-dose boost. Eligibility criteria are selective, typically includ-ing single lesions less than 4 to 5 cm in diameter without subependymal extension and more than 5 mm away from the optic chiasm or brainstem. In the initial U.S. series, which included a high proportion of patients who had un-dergone limited surgical resection, the median survival time was at least equal to that among patients with implants: 26 months for those with glioblastoma and more than 36 months for those with anaplastic astrocytoma.342,343 In a multi-institutional trial of 189 patients, the median sur-vival time was 86 weeks for those with glioblastoma who met all criteria for gamma knife intervention, compared with 40 weeks for those with more extensive tumors or a less favorable performance status score.323,328,341 The inci-dence of symptomatic necrosis may be less than that for patients with interstitial implants.271
Several trials in the United States, Europe, and Japan have assessed modifications in the radiation time-dose relationship.299,312,338,344-347 Despite an early suggestion that hyperfractionated delivery to higher doses might be ben-eficial, subsequent studies conducted by the RTOG have shown no substantial benefit from such therapy. A large randomized dose-escalating trial conducted by the RTOG tested hyperfractionated doses of 64.8 to 81.6 Gy, given in 1.2-Gy fractions twice daily with an interfractional interval of 4 to 8 hours. The results indicated that the ideal dose response occurred at 72 Gy, although the superiority of this schedule over 60 Gy delivered in conventionally frac-tionated radiation therapy was inapparent.344 Patients who received doses of 75 to 81.6 Gy fared less well.344 Without documentation of any reduction in neurotoxicity from hy-perfractionated delivery, few objective data indicate that the therapeutic ratio and effect of hyperfractionation are greater than those for conventional fractionation.344,348,349
Alternative time-dose regimens have included accelerat-ed hyperfractionation (1.5- or 1.6-Gy fractions given twice daily), accelerated fractionation (1.9- or 2.0-Gy fractions given three times daily), and hypofractionation (fractions

PART 10 Central Nervous System856
of 2.5 to 6 Gy).332,334-347 Although the hypofractionation regimens may expedite palliation in patients with advanced or unfavorable conditions, these regimens have provided no overall benefit.
Chemotherapy has been investigated extensively for the treatment of glioblastomas. As sole adjuvants to surgery, nitrosoureas have been ineffective.306 When combined with radiation, nitrosoureas or combinations of agents (e.g., carmustine-hydroxyurea plus procarbazine-teniposide, carmustine-hydroxyurea, vincristine-procarbazine) have been associated with only marginally improved survival times for patients enrolled in prospective studies.306,311,350 Despite one report of encouraging early results with pen-ciclovir,351 a randomized trial conducted by the Medical Research Council in the United Kingdom of more than 670 patients showed no survival benefit for patients given penciclovir in addition to standard radiation therapy.352 Two randomized trials testing concurrent temozolomide plus radiation therapy with radiation therapy alone demonstrated a significant survival benefit for the combination.353-354 In a trial by the European Organisation for Research and Treatment of Cancer, the survival benefit from temo-zolomide was more apparent when the MGMT gene was epigenetically silenced.355 The current RTOG trial uses MGMT status in the tumor as one of the criteria for stratifi-cation. Many biological agents are available for the treatment of malignant gliomas, including compounds with specific biological targets (e.g., epidermal growth factor, platelet- derived growth factor) and antiangiogenesis agents.356 One ongoing trial is using a vaccine against a truncated form of the epidermal growth factor receptor (EGFRvIII) for patients whose glioblastomas have undergone gross total resection and demonstrate overexpression of EGFRvIII. Studies of lo-cal chemotherapy, specifically carmustine-impregnated wa-fers (Gliadel), have yielded inconclusive results in patients with malignant gliomas, producing an apparent response but being of uncertain value as an adjuvant therapy.357
Radiation Therapy TechniqueRadiation therapy remains the most effective single agent in prolonging survival in patients with malignant gliomas. It should consist of standard EBRT with wide local coverage of the neoplasm.310,314 Anatomic studies of tumor extent, imaging analyses of patterns of recurrence, and clinical tri-als have shown that the appropriate initial target volume should extend 2 to 3 cm beyond the low-density periphery shown on CT scans or 2 cm beyond the abnormal signal shown on T2-weighted MRI studies.301,302,314,315,350 Mar-gins of less than 2 cm are theoretically inadequate because of the histologic nature of the tumor301 and the way in which the initial sites of disease progress.315
The use of limited high-dose treatment volumes deliv-ered by three-dimensional conformal or proton radiation may be associated with a relative increase in the peripheral failure rate.338,358 Central or intralesional disease progres-sion is less common in patients with interstitial implants. Studies of patterns of failure in series of patients treated with brachytherapy have shown that disease recurs primar-ily in the tumor margin, often within 2 cm of the high-dose implant; the incidence of distant intracranial recurrence is also relatively high.316,317
Dose-response data were established early in clinical trials involving patients with malignant gliomas. Walker
and colleagues306 showed that median survival time im-proved from 28 weeks for patients given 50 Gy in 25 to 28 fractions to 42 weeks for patients given 60 Gy in the first Brain Tumor Study Group studies (Fig. 33-15).306 Three-dimensional conformal and proton-based regimens have made it possible to escalate doses to 70 to 90 Gy; however, although central tumor control may be improved, no increase in survival has been found.338,358 As summa-rized earlier, none of the altered fractionation regimens has been shown to improve outcome over that achieved with conventionally fractionated radiation to 60 to 65 Gy (in 1.8- to 2-Gy fractions given once daily).345 No data exist to suggest that these recommendations for radiation therapy for adults be adjusted for children; however, the require-ment for high-dose radiation to reasonably large volumes limits the use of this modality in young children with ma-lignant gliomas.
PrognosisReports of survival beyond 2 years for adults with glio-blastoma remain anecdotal.359 However, approximately 15% to 25% of patients with anaplastic astrocytoma sur-vive 5 years, with gradually decreasing survival beyond that time documented in most series. Levin and col-leagues351 reported that adjuvant penciclovir chemother-apy is associated with a 35% survival rate at 3 to 5 years for patients with anaplastic lesions; however, these and similar results seen in other small series were not sub-stantiated in a Medical Research Council trial.314,352,360 Other factors influencing prognosis include age (survival is progressively better among younger patients, with the best among 18 to 39 year olds, the next best among 40 to 59 year olds, and the worst among those 60 years old or older) and initial performance status.305,325 Among chil-dren with malignant gliomas, the overall progression-free survival rates at 3 to 5 years range from 15% to 20%; for the small subset with completely resected lesions, corresponding survival rates of up to 75% have been reported.309,361,362
Rads
Sur
viva
l in
wee
ks
70
30
40
50
60
20
104500 5000 5500 6000
75th percentile0.174
0.110
0.004Median
25th percentile
FIGURE 33-15. Dose-response analysis for survival of adults with malignant gliomas. (Data from Walker MD, Green SB, Byar DP, et al. Randomized comparisons of radiotherapy and nitro-soureas for the treatment of malignant glioma after surgery. N Engl J Med 1980;303:1323-1329.)

33 The Brain and Spinal Cord 857
OligodendrogliomaOligodendroglioma is a relatively uncommon tumor that occurs in all age groups. The tumor arises most often in the frontal lobes and occasionally involves the infratento-rial or spinal regions. The most common symptom is sei-zures. The relatively nonaggressive nature of this tumor is indicated by the median survival time, which is more than 5 years from the onset of symptoms and diagnosis.363 The co-deletion of the short arm of chromosome 1 (1p) and the long arm of chromosome 19 (19q) has been associ-ated with less aggressive behavior of the tumor and better response to therapy.364,365
Primary surgical resection is the initial therapy for low-grade oligodendrogliomas.366,367 The role of postoperative radiation has been poorly defined. In a small, retrospective study, Sheline and colleagues368 found an improvement in 5-year survival rates for patients who underwent irradia-tion compared with those who did not (85% versus 55%), but the survival rate at 10 years was not statistically im-proved. Chin and colleagues369 reported a progression-free survival rate of 100% at 5 years for 24 patients complet-ing postoperative radiation. Lindegaard and colleagues370 observed a benefit from radiation only among those who had undergone incomplete surgical resection. In a study of a similar group of patients treated during roughly the same period, Reedy and colleagues371 found no survival advan-tage from radiation therapy.
In the absence of a prospective trial assessing the effi-cacy of radiation therapy, it seems justified and prudent to use postoperative radiation for subtotally resected lesions. Local fields to doses of 50 to 54 Gy approximate the treat-ment recommended for other low-grade tumors.106,372
Although 5-year survival rates in excess of 65% to 90% have been observed in major clinical series, the ultimate survival rate beyond 15 or 20 years was only 30% in two large reviews from an earlier era that exam-ined the pathologic behavior of tumors from more than 500 patients.363,373 Late tumor progression and death take place more than 5 to 10 years after diagnosis. Histologic grading is of increasing importance because a role for penciclovir chemotherapy in the treatment of anaplas-tic oligodendrogliomas has been established.374 Long-term survival is higher for patients younger than 40 or 50 years.373
MeningiomaMeningiomas are common CNS tumors, most often occur-ring as intracranial tumors along the convexities or in para-sagittal regions. The usually benign meningioma constitutes 15% of adult CNS tumors, with a female-to-male ratio of 2.5 to 1. The natural history of this tumor was elegantly de-scribed in Cushing and Eisenhardt’s 1938 monograph,375 in which they identified the broad dural attachment (or local infiltration), growth along or into the venous sinuses, and osseous invasion or overlying reactive bone formation that typify these lesions. Angioblastic meningiomas have a less favorable outcome than the other so-called benign tumors.376 Less than 10% of meningiomas are malignant, and these lesions seem to be associated with an unfavorable outcome.376-378
Surgery is the primary treatment for most peripherally located intracranial meningiomas. Local tumor recurrence
after complete resection occurs in 10% to 20% of cases, re-lated in part to the extent of dural and sinus excision.376-379
Symptomatic tumor recurrence or progression takes place in approximately 50% of patients with subtotally excised lesions, most often in patients with meningiomas of the sphenoid ridge and parasellar areas, which represent almost 30% of all meningiomas (Fig. 33-16).376,379-381 The efficacy of radiation therapy for incompletely resected meningio-mas has been well documented. Wara and colleagues382 reported local tumor recurrence in 74% of patients after incomplete resection and in 29% of patients given post-operative radiation. Progression-free survival rates beyond 5 years average 70% to 90% for patients undergoing incom-plete resection and radiation; disease control rates in excess of 70% to 80% at 8 to 10 years are associated with survival rates exceeding 90%.383-385 Similar outcomes have been observed among patients who receive radiosurgery alone or as an adjunct to incomplete surgery.386-389 Neurologic improvement has occurred in 44% of patients after radia-tion for unresected primary lesions.376 Serial CT studies have confirmed the regression of neoplasms in response to radiation therapy (see Fig. 33-16).381 In sites such as the optic nerve sheath, operative intervention may be associ-ated with a significant functional deficit. Primary irradia-tion can improve tumor-related defects in visual acuity and visual fields in these patients.390
Radiation Therapy TechniqueBecause meningiomas are locally infiltrating tumors that produce local tissue changes by means of direct tumor ex-tension or have subclinical, limited multicentricity,391 local irradiation should include a reasonable margin despite the circumscribed appearance of these tumors on CT scans. Large tumors of the sphenoid ridge may extend beyond the cranial vault into the orbit or the facial or cervical re-gions. Optimal radiologic assessment of tumor extent and the use of wide inferior treatment margins are important in these cases.381 Three-dimensional conformal techniques, intensity-modulated radiation therapy, and proton therapy are suitable for the treatment of meningiomas.
Carella and colleagues383 were unable to identify a dose-response relationship for meningiomas between 50 and 75 Gy. However, excellent local tumor control has been achieved at doses approaching CNS tolerance, and the rec-ommended treatment is a total dose of 50 to 55 Gy given in 25 to 30 fractions.376,381,384 The use of radiosurgery as the primary treatment for selected lesions has produced equally positive results; at many centers, radiosurgery is the treatment of first choice for limited-volume lesions that are difficult to approach surgically or are residual or recurrent after initial resection.386,388,389,392,393
PrognosisThe benign nature of meningiomas is confirmed by the limited number of recurrences seen in patients after to-tal surgical resection. After incomplete resection, however, the median time to clinically apparent tumor progression is 4 years after surgery. The median intervals to tumor pro-gression in patients given radiation therapy exceed 5 to 10 years.381,383,384
Initial postoperative irradiation for incompletely resected or biopsied meningiomas has achieved excellent local tumor control, as described in the previous paragraphs.

PART 10 Central Nervous System858
FIGURE 33-16. CT scans of an orbital sphenoidal meningioma demonstrate residual disease after surgery (top row) and 2 years after irradiation (bottom row). (From Petty AM, Kun LE, Meyer GA. Radiation therapy for incompletely resected meningiomas. J Neurosurg 1985;62:502-507.)
Indications for initial or delayed radiation therapy remain controversial, although increasing information suggests that incompletely resected lesions along the cavernous sinus and those with malignant histologic features may warrant im-mediate postoperative irradiation.377,385,389,392 No appar-ent decrease in tumor control has been observed in most series of patients who undergo repeat surgery and radia-tion therapy for disease that recurs after initial incomplete resection.376,380,384 A more rapid rate of tumor regrowth after subtotal excision has been indicated in children, rais-ing some concern about the advisability of delaying radio-therapeutic intervention in this age group.394,395
Identifying the histologic subtype of meningioma69,378 is important because the local recurrence rate is higher for malignant (anaplastic) meningiomas and because postoper-ative radiation therapy can effectively control these tumors. For example, Dziuk and colleagues377 and others378,380 have reported 15% to 80% differences in 5-year progression-free survival rates related to radiation. A long-term disease control rate of only 25% at 5 years has been observed for patients who receive single-fraction radiosurgery, in most cases for recurrent malignant meningiomas.393
Primary Malignant Lymphoma of the Central Nervous SystemPrimary malignant lymphoma of the CNS was previously a rare neoplasm, occurring spontaneously in conjunction with immunosuppression. However, the frequency with which it occurs has increased greatly in conjunction with
the acquired immunodeficiency syndrome (AIDS) epi-demic.396-398 The tumor occurs primarily in the supraten-torial region, most often as an isodense, diffusely enhancing lesion involving the basal ganglia or thalamus, the periven-tricular white matter, or the corpus callosum.399 Up to 15% to 40% of tumors are multifocal intracranial lesions.400,401 The CSF contains tumor cells in 10% to 20% of cases; in-volvement of the ocular vitreous at diagnosis or metachro-nously occurs in 10% to 25% of cases.400,402
The lesion is usually classified as an immunoblastic or lymphoblastic diffuse, large cell, malignant lymphoma, most often of a B-cell immunophenotype. Systematic evaluation is necessary to distinguish primary lymphoma of the brain from secondary CNS manifestations of malig-nant lymphoma, although intraparenchymal deposits oc-cur more often with primary tumors than with secondary tumors.
Surgery is limited, often to biopsy alone, but radiation therapy produces a high rate of objective response. Neu-rologic improvement can be achieved in up to 70% of pa-tients, but median survival has been only 7 to 8 months.403 Long-term survival after radiation alone has been lim-ited.398,400,401,404,405 Chemotherapy has shown increas-ing efficacy in patients with CNS malignant lymphoma, with rates of objective response often exceeding 50% to 70% in those treated with regimens including high-dose methotrexate or, less often, with conventional systemic chemotherapy regimens (e.g., cyclophosphamide, doxoru-bicin, vincristine, and prednisone).406-410 The combination

33 The Brain and Spinal Cord 859
of preirradiation chemotherapy and cranial irradiation re-sulted in median survival times as long as 60 months and 4-year progression-free and overall survival rates of ap-proximately 50% in a moderate-size series from Memorial Sloan-Kettering Cancer Center.408,411 One drawback to the use of combined methotrexate-radiation regimens has been their considerable neurotoxicity, which sometimes produces frank dementia, particularly in patients older than 60 years.407,408,412
Radiation Therapy TechniqueGiven the size and often the multiplicity of most prima-ry CNS lymphomas, the minimal target volume is often full cranial irradiation.401-404 Isolated subarachnoid spinal recurrence after cranial radiation occurs in 4% to 25% of patients.106,404 The inability to control the primary tumor within the cranium in a high proportion of patients and the need to coordinate radiation with chemotherapy have led clinicians away from considering CSI. This raises a valid argument for avoiding spinal irradiation in deference to the potential benefits conferred by chemotherapy.
A radiation dose-response relationship has been suggested in the treatment of primary malignant lym-phoma of the CNS. Murray and colleagues401 reviewed 198 cases reported in the literature and found a statisti-cally significant improvement in the 5-year survival rate for patients given doses of more than 50 Gy (42% versus 13%) (Fig. 33-17).401 However, an analysis at Memorial Sloan-Kettering Cancer Center did not find additional benefit from doses higher than 45 Gy. Recurrence of tumor at the primary site even in patients treated with doses of 50 to 55 Gy led to a major RTOG trial, the results of which failed to demonstrate a significant added benefit from high-dose cranial irradiation.403 In small series of patients, however, the addition of radiation therapy seems to have prolonged disease control and improved survival relative to the out-come for patients given chemotherapy only.398,408,411
PrognosisOverall survival in patients with primary malignant lym-phoma seems to have increased among those treated with combined, sequential chemoradiotherapy; median survival times have increased several-fold to approximately 4 to 5 years. However, most patients do die of the disease, some-times as long as 5 years after diagnosis.408,411
Carcinoma Metastatic to the BrainIntracranial metastasis, primarily in the cerebrum, occurs in 10% to 15% of patients with cancer.413 Of the types of can-cer that metastasize preferentially to the brain, cancer of the lung and breast predominate, and gastrointestinal and renal carcinomas are less common. Brain metastasis often occurs at multiple sites. In a classic autopsy series, solitary metasta-ses were found in approximately 40% of cases, two to three lesions in 25% of cases, and four or more foci in 35%.414
Treatment of brain metastases is palliative; long-term survival can be achieved for up to 20% of patients with fa-vorable presenting characteristics, such as age younger than 60 to 65 years, favorable performance status (typically, a Karnofsky performance status score of at least 70), control of the primary tumor, and absent or controlled extracra-nial metastasis.415-417 Corticosteroids alone can transiently reduce symptoms in 60% of patients.347 However, cranial
irradiation achieves more prolonged palliation, with objec-tive improvement in neurologic function in 50% to 70% of patients treated in this manner.319
Earlier time-dose studies showed the relative equiva-lence of the following treatment regimens: 30 to 36 Gy given in 10 to 12 fractions; 20 Gy given in 5 fractions; and 40 Gy given in 15 fractions.417a The current standard ther-apy is 30 Gy given in 10 fractions; however, randomized trials to assess the benefit of surgery or radiosurgery in se-lected settings favor 37.5 Gy given in 15 fractions.418,419
For patients with a solitary metastasis, the addition of surgical resection or radiosurgery has significantly improved survival time (from a median of 15 weeks to a median of 40 weeks in a randomized trial reported by Patchell and col-leagues420) and the rate of local control at metastatic sites (from less than 50% for patients treated with cranial irradi-ation alone to 80% for patients undergoing resection). This increase in survival also has been associated with improved functional outcome.420 In several series, the outcome from radiosurgery has been similar to that from operative removal; in all of these series, the patients with favorable factors (e.g., age, performance status, absence of disease at other sites) are the ones who benefit the most from the addition of local therapy.388,418,419,421,422 Surgery and radiosurgery seem to achieve equivalent results in most reports.419,421 Detailed analyses have shown that the addition of full cranial irradia-tion improves survival and local tumor control and may be associated with long-term survival of a small but meaning-ful number of patients undergoing aggressive local thera-py.423 One randomized trial comparing radiosurgery alone
Survival (months)
Frac
tion
surv
ival
1.00
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0.1
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60
<50 Gy
P<.05
³50 Gy
FIGURE 33-17. Dose-response analysis for survival of patients with primary cerebral malignant lymphoma after irradiation. (From Murray K, Kun L, Cox J. Primary malignant lymphoma of the central nervous system. J Neurosurg 1986;65:600-607.)

PART 10 Central Nervous System860
with the combination of radiosurgery and whole-brain irra-diation showed significantly fewer intracranial recurrences with the combination therapy, although survival times were similar in both groups.424 Results for patients with malig-nant melanoma that has metastasized to the brain have generally paralleled those seen for patients with other car-cinomas; however, local therapy may be particularly advan-tageous for patients with few metastatic sites and favorable performance status.421,425
The treatment selected for patients with brain metastasis depends on the absence or presence of the clinical features consistently associated with improved outcome (i.e., age younger than 60 to 65 years, Karnofsky performance status score of 70 or higher, and the lack of apparent or symptom-atic disease at the primary site or other extracranial loca-tions). However, there does seem to be a definite advantage to surgery or radiosurgery for patients with only one meta-static focus; a similar advantage seems to exist for those with only two or three metastatic foci.388,418,419,421,422,426 In all of these patients and in those with more advanced cranial or ex-traneural disease, the addition of full cranial irradiation is an important and worthwhile palliative intervention.415,418,423
spInal Cord tumors
Primary tumors of the spinal cord represent 10% to 15% of CNS neoplasms. Extramedullary tumors, including schwannomas and meningiomas, account for almost one half of the lesions in the spinal canal. Primary intramedul-lary neoplasms are most often gliomas or vascular tumors.
Intramedullary gliomas include ependymomas (60%) and astrocytomas (30%). Ependymomas occur more often in the lumbar region, affecting the conus and cauda equina. Spinal ependymomas usually are low-grade neoplasms; those occurring in the cauda equina usually are well- differentiated myxopapillary tumors.427 The ependymo-mas tend to develop as discrete lesions, facilitating subtotal or gross total resection.
Gross total resection led to systemic disease control in recent series with a 5-year follow-up. Aggressive surgery, however, is associated with postoperative neurologic dete-rioration in 15% of patients.428 Response to radiation is well documented, with 75% of patients showing improvement in neurologic status and progression-free survival rates of 70% to 100% at 10 years.429-431 A local tumor control rate of 80% with no identifiable long-term neurologic toxicity despite doses in excess of 45 Gy indicates that radiation has a role in the treatment of patients whose spinal tumors are incompletely resected.431 Patients with tumors of the cauda equina region and conus have particularly high sur-vival rates after radiation or surgical resection.432,433
Spinal astrocytomas are evenly distributed along the length of the spinal cord. These lesions often contain cystic components and most often are low-grade fibril-lary tumors. Astrocytomas are more infiltrating than ep-endymomas, limiting surgery to cyst decompression and partial resection.432 Epstein and colleagues,434-437 how-ever, described operative techniques that can be used to completely resect many low-grade astrocytomas in chil-dren and adults. Aggressive operative intervention is not advantageous for high-grade spinal astrocytomas.429,438,439 Long-term control in patients with spinal astrocytomas treated with radiation is less predictable than that in
patients with ependymomas despite frequent neurologic improvement.429,431 The disease-free survival rate at 5 to 10 years ranges from 25% to 60% among patients with spi-nal astrocytomas.429,438,439 However, the histologic grade affects outcome, in that patients with low-grade astrocyto-mas enjoy a short-term (5-year) survival rate of as high as 89%, compared with 0% among patients with higher-grade tumors (e.g., glioblastoma).438
Spinal cord tolerance is an important consideration when reviewing results of patients with intramedullary tumors treated with radiation.440 Doses of approximately 50 Gy are recommended for most spinal cord tumors; however, higher doses and the suggestion of a dose-response effect at or above 50 Gy have been reported for localized spinal cord lesions.441,442
Extradural metastasis is the most common oncologic di-agnosis for patients with spinal cord disease. An estimated 5% of patients who die of cancer have clinical signs of epi-dural metastases.443 Extradural involvement usually results from the contiguous extension of a vertebral metastasis, most often in patients with primary cancer of the breast, lung, or prostate. Less common are vertebral metastases from malignant lymphomas and myeloma or carcinomas of the kidney and gastrointestinal tract.
Early evaluation with spinal MRI has been advocated for patients with pain and radiographic evidence of vertebral metastasis without objective neurologic signs.443,444 The treatment of epidural metastases is controversial, largely with respect to the use of surgery before radiation. Con-ventional procedures have included decompressive lami-nectomy, at least for patients with rapidly evolving signs or complete block shown by myelography; patients for whom the diagnosis is uncertain or the diagnosis of malignancy is not established require surgical intervention.339
Retrospective and prospective studies comparing lami-nectomy and postoperative radiation with radiation alone confirm an apparent advantage to surgical intervention only for patients with nonambulatory symptoms; however, there has been little difference in outcome for most pa-tients.443,445-447 Experience with vertebral body resection in selected cases indicates improved neurologic outcome after a more aggressive operative approach.448-450 Primary irradiation is often the treatment of choice for certain his-tologic types of tumors known to respond relatively rapidly and for patients with residual functional deficits.
Irradiation for spinal cord compression is considered a radiotherapeutic emergency. Prompt initiation of dexa-methasone and high-dose (2- to 4-Gy) fractions are indi-cated. After two or three treatments, the dose per fraction and total dose depend on the type of malignancy and clini-cal status of the patient.
Carcinomatous meningitis or diffuse leptomeningeal infiltration is a relatively uncommon late manifestation of systemic cancer. Primary tumors are usually carcinomas of the breast or lung; small cell lung cancer in particular is often associated with intracranial metastasis. Symptoms and signs referable to the spine predominate in 25% of pa-tients; signs related to spinal root infiltration are often ap-parent.451 Treatment consists of cranial irradiation or CSI (depending on the histologic findings and coordinated use of chemotherapy), with or without intrathecal or systemic chemotherapy. Responses to treatment are common, but long-term survival results are largely anecdotal.

33 The Brain and Spinal Cord 861
REFERENCES
1. Schultheiss TE , Kun L E , Ang K K, et al. Radiation response of the central nervous system. Int J Radiat Oncol Biol Phys 1995;31:1093-1112.
2. Fajardo LF, Berthrong M, Anderson RE. Central nervous system and spinal cord. In Radiation Pathology. New York: Oxford Uni-versity Press, 2001, pp 351-361.
3. Burger PC, Mahaley MS Jr, Dudka L, et al. The morphologic effects of radiation administered therapeutically for intracra-nial gliomas: a postmortem study of 25 cases. Cancer 1979;44: 1256-1272.
4. Constine LS, Konski A, Ekholm S, et al. Adverse effects of brain irradiation correlated with MR and CT imaging. Int J Radiat Oncol Biol Phys 1988;15:319-330.
5. Valk PE, Dillon WP. Radiation injury of the brain. AJNR Am J Neuroradiol 1991;12:45-62.
6. Gutin PH. Treatment of radiation necrosis of the brain. In Gutin PH, Leibel SA, Sheline GE (eds): Radiation Injury to the Nerv-ous System. New York: Raven Press, 1991, pp 271-282.
7. DeAngelis LM, Shapiro WR. Drug/radiation interactions and central nervous system injury. In Gutin PH, Leibel SA, Sheline GE (eds): Radiation Injury to the Nervous System. New York: Raven Press, 1991, pp 361-382.
8. Van der Kogel AJ. Central nervous system radiation injury in small animal models. In Gutin PH, Leibel SA, Sheline GE (eds): Radiation Injury to the Nervous System. New York: Raven Press, 1991, pp 91-112.
9. Fike JR, Gobbe GT. Central nervous system radiation injury in large animal models. In Gutin PH, Leibel SA, Sheline GE (eds): Radiation Injury to the Nervous System. New York: Raven Press, 1991, pp 113-136.
10. Ostertag CB. Experimental central nervous system injury from implanted isotopes. In Gutin PH, Leibel SA, Sheline GE (eds): Radiation Injury to the Nervous System. New York: Raven Press, 1991, pp 183-190.
11. Caveness WF. Experimental observations: delayed necrosis in normal monkey brain. In Gilbert HA, Kagen AR (eds): Radia-tion Damage to the Nervous System. New York: Raven Press, 1980, pp 1-38.
12. Price RA, Jamieson PA. The central nervous system in childhood leukemia. Subacute leukoencephalopathy. Cancer 1975;35 (Pt 2):306-318.
13. Fouladi M, Langston J, Mulhern R, et al. Silent lacunar lesions de-tected by magnetic resonance imaging of children with brain tu-mors: a late sequela of therapy. J Clin Oncol 2000;18:824-831.
14. Salazar OM, Rubin P, Feldstein ML, et al. High dose radiation therapy in the treatment of malignant gliomas: final report. Int J Radiat Oncol Biol Phys 1979;5:1733-1740.
15. Kramer S, Lee KF. Complications of radiation therapy: the cen-tral nervous system. Semin Roentgenol 1974;9:72-83.
16. Sheline GE, Wara WM, Smith V. Therapeutic irradiation and brain injury. Int J Radiat Oncol Biol Phys 1980;6:1215-1228.
17. Sheline GE. Irradiation injury of the human brain: a review of clinical experience. In Gilbert HA, Kagen AR (eds): Radiation Damage to the Nervous System. New York: Raven Press, 1980, pp 39-58.
18. Young DF, Posner JB, Chu F, et al. Rapid-course radiation ther-apy of cerebral metastases: results and complications. Cancer 1974;34:1069-1076.
19. Jones A. Transient radiation myelopathy (with reference to Lhermitte’s sign of electrical paresthesia). Br J Radiol 1964;37: 727-744.
20. Freeman JE, Johnston PGB, Voke JM. Somnolence after prophy-lactic cranial irradiation in children with acute lymphoblastic leukaemia. Br Med J 1973;4:523-525.
21. Boldrey E, Sheline G. Delayed transitory clinical manifestations after radiation treatment of intracranial tumors. Acta Radiol Ther Phys Biol 1966;5:5-10.
22. Steen RG, Koury M, Granja CI, et al. Effect of ionizing radia-tion on the human brain: white matter and gray matter T1 in pediatric brain tumor patients treated with conformal radiation therapy. Int J Radiat Oncol Biol Phys 2001;49:79-91.
23. Hoffman WF, Levin VA, Wilson CB. Evaluation of malignant glioma patients during the postirradiation period. J Neurosurg 1979;30:624-628.
24. Longee DC, Fiedman HS, Djang NW, et al. Transient late mag-netic resonance imaging changes suggesting progression of brain stem glioma: implications for entry criteria for phase II trials. Neurosurgery 1988;23:248-253.
25. Duffner PK, Cohen ME, Myers MH, et al. Survival of children with brain tumors: SEER program, 1973-1980. Neurology 1986;36:597-601.
26. Childhood Brain Tumor Consortium. A study of childhood brain tumors based on surgical biopsies from 10 North American institutions: sample description. J Neurooncol 1988;6:9-23.
27. Groothuis DR, Wright DC, Ostertag CB. The effect of 125I interstitial radiotherapy on blood-brain barrier function in normal canine brain. J Neurosurg 1987;67:895-902.
28. Schultheiss TE, Stephens LC. The pathogenesis of radiation myelopathy: widening the circle. Int J Radiat Oncol Biol Phys 1992;23:1089-1091.
29. Schultheiss TE, Stephens LC. Invited review: permanent radia-tion myelopathy. Br J Radiol 1992;65:737-753.
30. Marks JE, Baglan RJ, Prassad SC, et al. Cerebral radionecrosis: incidence and risk in relation to dose, time, fractionation and volume. Int J Radiat Oncol Biol Phys 1981;7:242-252.
31. Mikhael MA. Dosimetric considerations in the diagnosis of radiation necrosis of the brain. In Gilbert HA, Kagen AR (eds): Radiation Damage to the Nervous System. New York: Raven Press, 1980, pp 59-92.
32. Kramer S, Southard ME, Mansfield CM. Radiation effect and tolerance of the central nervous system. Front Radiat Ther On-col 1972;6:332-345.
33. Aristizabal S, Caldwell WL, Avila J. The relationship of time-dose fractionation factors to complications in the treatment of pituitary tumors by irradiation. Int J Radiat Oncol Biol Phys 1977;2:667-673.
34. Leibel SA, Sheline GE. Tolerance of the brain and spinal cord to conventional irradiation. In Gutin PH, Leibel SA, Sheline GE (eds): Radiation Injury to the Nervous System. New York: Raven Press, 1991, pp 239-256.
35. Clemente CD, Yamazaki JN, Bennett LR, et al. Brain radiation in newborn rats and differential effects of increased age. Neurology 1960;10:669-675.
36. Bloom HJG, Wallace ENK, Henk JM. The treatment and prog-nosis of medulloblastoma in children. AJR Am J Roentgenol 1969;105:43-62.
37. Boden G. Radiation myelitis of the brain stem. J Fac Radiol (Great Britain) 1950;2:79-94.
38. Pallis CA, Louis S, Morgan RL. Radiation myelopathy. Brain 1961;84:460-479.
39. Schultheiss TE, Higgins EM, el-Mahdi AM. The latent period in clinical radiation myelopathy. Int J Radiat Oncol Biol Phys 1984;10:1109-1115.
40. Myers R, Rogers MA, Hornsey S. A reappraisal of the role of glial and vascular elements in the development of white mat-ter necrosis in irradiated rat spinal cord. Br J Cancer 1986;7: 221-223.
41. Phillips TL, Buschke F. Radiation tolerance of the thoracic spinal cord. Am J Roentgenol Rad Ther Nucl Med 1969;105:659-664.
42. Abbatucci JS, Delozier T, Quint R, et al. Radiation myelopathy of the cervical spinal cord: time, dose and volume factors. Int J Radiat Oncol Biol Phys 1978;4:239-248.
43. Hatievoll R, Host H, Kaalhus O. Myelopathy following radio-therapy of bronchial carcinoma with large single fractions: a ret-rospective study. Int J Radiat Oncol Biol Phys 1983;9:41-44.
44. Wara WM, Phillips TL, Sheline GE, et al. Radiation tolerance of the spinal cord. Cancer 1975;35:1558-1562.
45. Cohen L, Creditor M. An isoeffect table for radiation tolerance of the human spinal cord. Int J Radiat Oncol Biol Phys 1981;7: 961-966.
46. Van der Kogel AJ. Radiation tolerance of the rat spinal cord: time-dose relationships. Radiology 1977;122:505-509.

PART 10 Central Nervous System862
47. Ang KK, van der Kogel AJ, van der Schueren E. Lack of evidence for increased tolerance of rat spinal cord with decreasing fraction doses below 2 Gy. Int J Radiat Oncol Biol Phys 1985;11:105-110.
48. Dische S, Saunders MI. Continuous, hyperfractionated, acceler-ated radiotherapy (CHART): an interim report upon late mor-bidity. Radiother Oncol 1989;16:67-74.
49. Dische S. Accelerated treatment and radiation myelitis. Radi-other Oncol 1991;20:1-2.
50. Norrell H, Wilson CB, Slagel DE, et al. Leukoencephalopathy following the administration of methotrexate into the cerebro-spinal fluid in the treatment of primary brain tumors. Cancer 1974;33:923-932.
51. Lee JS, Umsawasdi T, Lee Y-Y, et al. Neurotoxicity in long-term survivors of small cell lung cancer. Int J Radiat Oncol Biol Phys 1986;12:313-321.
52. Bleyer WA. Neurologic sequelae of methotrexate and ioniz-ing radiation: a new classification. Cancer Treatment Reports 1981;65:89-98.
53. Mulhern RK, Ochs J, Kun LE. Changes in intellect associated with cranial radiation therapy. In Gutin PH, Leibel SA, Sheline GE (eds): Radiation Injury to the Nervous System. New York: Raven Press, 1991, pp 325-340.
54. Mulhern RK, Kovnar E, Langston J, et al. Long-term survivors of leukemia treated in infancy: factors associated with neuropsy-chologic status. J Clin Oncol 1992;10:1095-1102.
55. Jannoun L, Bloom HJG. Long-term psychological effects in chil-dren treated for intracranial tumors. Int J Radiat Oncol Biol Phys 1990;18:747-753.
56. Hochberg FH, Slotnick B. Neuropsychologic impairment in astrocytoma survivors. Neurology 1980;30:172-177.
57. Maire J, Coudin B, Guerin J, et al. Neuropsychologic impairment in adults with brain tumors. Am J Clin Oncol 1987;10: 156-162.
58. Kun LE, Mulhern RK, Crisco JJ. Quality of life in children treated for brain tumors: intellectual, emotional, and academic function. J Neurosurg 1983;58:1-6.
59. Radcliffe J, Packer RJ, Atkins TE, et al. Three- and four-year cog-nitive outcome in children with noncortical brain tumors treated with whole-brain radiotherapy. Ann Neurol 1992;32:551-554.
60. Mulhern RK, Kepner JL, Thomas PRM, et al. Neuropsycho-logical functioning of survivors of childhood medulloblastoma randomized to receive conventional (3,600 cGy/20) or reduced (2,340/13) dose craniospinal irradiation: a Pediatric Oncology Group study. J Clin Oncol 1998;16:1723-1728.
61. Mulhern RK, Reddick WE, Palmer SL, et al. Neurocognitive defi-cits in medulloblastoma survivors and white matter loss. Ann Neurol 1999;46:834-841.
62. Craig JB, Jackson DV, Moody D, et al. Prospective evaluation of changes in computed cranial tomography in patients with small cell lung carcinoma treated with chemotherapy and prophylac-tic cranial irradiation. J Clin Oncol 1984;2:1151-1156.
63. Urie MM, Fullerton B, Tatsuzaki H, et al. A dose response analysis of injury to cranial nerves and/or nuclei following proton beam radiation therapy. Int J Radiat Oncol Biol Phys 1992;23:27-29.
64. Parsons JT, Bova FJ, Fitzgerald CR, et al. Radiation optic neu-ropathy after megavoltage external-beam irradiation: analysis of time-dose factors. Int J Radiat Oncol Biol Phys 1994;30: 755-763.
65. Harris JR, Levene MB. Visual complications following irradia-tion for pituitary adenomas and craniopharyngiomas. Radiology 1976;120:167-171.
66. Svensson H, Westling P, Larsson LG. Radiation-induced lesions of the bronchial plexus correlated to the dose-time-fraction schedule. Acta Radiol 1975;14:228-238.
67. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2007. CA Cancer J Clin 2007;57:43-66.
68. Linabery AM, Ross JA. Trends in cancer incidence among chil-dren in the U.S. (1992-2004). Cancer 2008;112:416-432.
69. Kleihues P, Cavenee WK (eds). Tumours of the Nervous System. Lyon, France: IARC Press, 2000.
70. Rorke L. The cerebellar medulloblastoma and its relationship to primitive neuroectodermal tumors. J Neuropathol Exp Neurol 1983;42:1-15.
71. Hart MN, Earle KM. Primitive neuroectodermal tumors of the brain in children. Cancer 1973;32:890-898.
72. Grotzer MA, Janss AJ, Fung JA, et al. TrkC expression predicts good clinical outcome in primitive neuroectodermal brain tumors. J Clin Oncol 2000;18:1027-1035.
73. McLendon RE, Friedman HS, Fuchs HE, et al. Diagnostic mark-ers in paediatric medulloblastoma: a Pediatric Oncology Group study. Histopathology 1999;34:154-162.
74. Mendrzyk F, Radlwimmer B, Joos S, et al. Genomic and protein expression profiling identifies CDK6 as novel independent prognostic marker in medulloblastoma. J Clin Oncol 2005;34: 8853-8862.
75. Aldosari N, Bigner SH, Burger PC, et al. MYCC and MYCN oncogene amplification in medulloblastoma. A fluorescence in situ hybridization study on paraffin sections from the Children’s Oncology Group. Arch Pathol Lab Med 2002;126:540-544.
76. Bobola MS, Finn LS, Ellenbogen RG, et al. Apurinic/apyrimidinic endonuclease activity is associated with response to radiation and chemotherapy in medulloblastoma and primitive neuroec-todermal tumors. Clin Cancer Res 2005;11:7405-7414.
77. Clifford SC, Lusher ME, Lindsey JC, et al. Wnt/Wingless path-way activation and chromosome 6 loss characterize a distinct molecular sub-group of medulloblastomas associated with a favorable prognosis. Cell Cycle 2006;5:2666-2670.
78. Lamont JM, McManamy CS, Pearson AD, et al. Combined his-topathological and molecular cytogenetic stratification of medul-loblastoma patients. Clin Cancer Res 2004;10:5482-5493.
79. Gajjar A, Hernan R, Kocak M, et al. Clinical, histopathologic and molecular markers of prognosis: toward a new disease risk strati-fication system for medulloblastoma. J Clin Oncol 2004;22: 971-974.
80. Gajjar A, Fouladi M, Walter AW, et al. Comparison of lumbar and shunt cerebrospinal fluid specimens for cytologic detection of leptomeningeal disease in pediatric patients with brain tumors. J Clin Oncol 1999;17:1825-1828.
81. Kleinman GM, Hockberg FH, Richardson EP Jr. Systemic metastases from medulloblastoma: report of two cases and review of the literature. Cancer 1981;48:2296-2309.
82. Albright AL, Wisoff JH, Zeltzer PM, et al. Effects of medullob-lastoma resections on outcome in children: a report from the Children’s Cancer Group. Neurosurgery 1996;38:265-271.
83. Cochrane DD, Gustavsson B, Poskitt KP, et al. The surgical and natural morbidity of aggressive resection for posterior fossa tumors in childhood. Pediatr Neurosurg 1994;20:19-29.
84. Aguiar PH, Plese JP, Ciquini O, et al. Transient mutism follow-ing a posterior fossa approach to cerebellar tumors in children: a critical review of the literature. Childs Nerv Syst 1995;11: 306-310.
85. Chang CH, Housepian EM, Herbert C Jr. An operative staging system and a megavoltage radiotherapeutic technic for cerebel-lar medulloblastoma. Radiology 1969;93:1351-1359.
86. Kun LE, Constine LS. Medulloblastoma: caution regarding new treatment approaches. Int J Radiat Oncol Biol Phys 1991;20: 897-899.
87. Packer RJ, Sutton LN, Elterman R, et al. Outcome for children with medulloblastoma treated with radiation and cisplatin, CCNU, and vincristine chemotherapy. J Neurosurg 1994;81: 690-698.
88. Heideman RL, Kovnar EH, Kellie SJ, et al. Preirradiation chemo-therapy with carboplatin and etoposide in newly diagnosed embryonal pediatric CNS tumors. J Clin Oncol 1995;13: 2247-2254.
89. Kovnar EH, Kellie SJ, Horowitz ME, et al. Pre-irradiation cispla-tin and etoposide in the treatment of high-risk medulloblastoma and other malignant embryonal tumors of the central nervous system: a phase II study. J Clin Oncol 1990;8:330-336.
90. Bailey CC, Gnekow A, Wellek S, et al. Prospective randomized trial of chemotherapy given before radiotherapy in childhood medulloblastoma. International Society of Paediatric Oncol-ogy (SIOP) and the (German) Society of Paediatric Oncology (GPO): SIOP II. Med Pediatr Oncol 1995;25:166-178.

33 The Brain and Spinal Cord 863
91. Hartsell WF, Gajjar A, Heideman RL, et al. Patterns of failure in children with medulloblastoma: effects of pre-irradiation chem-otherapy. Int J Radiat Oncol Biol Phys 1997;39:15-24.
92. Thomas PR, Deutsch M, Kepner JL, et al. Low-stage medul-loblastoma: final analysis of trial comparing standard-dose with reduced-dose neuraxis irradiation. J Clin Oncol 2000;18: 3004-3011.
93. Berry MP, Jenkin RDT, Keen CW, et al. Radiation treatment for medulloblastoma: a 21-year review. J Neurosurg 1981;55: 43-51.
94. Hughes EN, Winston K, Cassady JR, et al. Medulloblastoma: results of surgery and radical radiation therapy at the JCRT 1968-1984. Int J Radiat Oncol Biol Phys 1986;12:179.
95. Bloom HJG, Glees J, Bell J. The treatment and long-term prog-nosis of children with intracranial tumors: a study of 610 cases, 1950-1981. Int J Radiat Oncol Biol Phys 1990;18:723-745.
96. Jenkin D, Goddard K, Armstrong D, et al. Posterior fossa medul-loblastoma in childhood: treatment results and a proposal for a new staging system. Int J Radiat Oncol Biol Phys 1990;19: 265-274.
97. Packer RJ, Goldwein J, Nicholson HS, et al. Treatment of chil-dren with medulloblastomas with reduced-dose craniospinal ra-diation therapy and adjuvant chemotherapy: a Children’s Can-cer Group study. J Clin Oncol 1999;17:2127-2136.
98. Miralbell R, Lomax A, Cella L, et al. Potential reduction of the incidence of radiation-induced second cancers by using proton beams in the treatment of pediatric tumors. Int J Radiat Oncol Biol Phys 2002;54:824-829.
99. Fukunaga-Johnson N, Sandler HM, Marsh R, et al. The use of 3D conformal radiotherapy (3D CRT) to spare the cochlea in patients with medulloblastoma. Int J Radiat Oncol Biol Phys 1998;41:77-82.
100. Merchant TE, Happersett L, Finlay J, et al. Preliminary results of conformal radiation therapy for medulloblastoma. Neurooncol-ogy 1999;1:177-187.
101. Fukunaga-Johnson N, Lee JH, Sandler HM, et al. Patterns of fail-ure following treatment for medulloblastoma: is it necessary to treat the entire posterior fossa? Int J Radiat Oncol Biol Phys 1998;42:143-146.
102. Strother D, Ashley D, Kellie SJ, et al. Feasibility of four consecu-tive high-dose chemotherapy cycles with stem-cell rescue for patients with newly diagnosed medulloblastoma or supratentorial primitive neuroectodermal tumor after craniospinal radio-therapy: results of a collaborative study. J Clin Oncol 2001;19: 2696-2704.
103. Gajjar A, Chintagumpala M, Ashley D, et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medul-loblastoma (St Jude Medulloblastoma-96): long-term results from a prospective, multicentre trial. Lancet Oncol 2006;7: 813-820.
104. Gajjar A, Sanford RA, Heideman R, et al. Low-grade astrocy-toma: a decade of experience at St. Jude Children’s Research Hospital. J Clin Oncol 1997;15:2792-2799.
105. Leibel SA, Sheline GE, Wara WM, et al. The role of radiation therapy in the treatment of astrocytomas. Cancer 1975;35: 1551-1557.
106. Morantz RA. Radiation therapy in the treatment of cerebral astrocytoma. Neurosurgery 1987;20:975-982.
107. Wallner KE, Gonzales MF, Edwards MSB, et al. Treatment results of juvenile pilocytic astrocytoma. J Neurosurg 1988;69: 171-176.
108. Laws ER, Taylor WF, Clifton MB, et al. Neurosurgical manage-ment of low-grade astrocytoma of the cerebral hemispheres. J Neurosurg 1984;61:665-673.
109. Krieger MD, Gonzalez-Gomez I, Levy ML, et al. Recurrence patterns and anaplastic change in a long-term study of pilocytic astrocytomas. Pediatr Neurosurg 1997;27:1-11.
110. Roessler K, Bertalanffy A, Jezan H, et al. Proliferative activity as measured by MIB-1 labeling index and long-term outcome of cerebellar juvenile pilocytic astrocytomas. J Neurooncol 2002;58:141-146.
111. Ilgren EB, Stiller CA. Cerebellar astrocytomas. Clinical char-acteristics and prognostic indices. J Neurooncol 1987;4: 293-308.
112. Smoots DW, Geyer JR, Lieberman DM, et al. Predicting disease progression in childhood cerebellar astrocytoma. Childs Nerv Syst 1998;14:636-648.
113. Tomita T, Chou P, Reyes-Mugica M. IV ventricle astrocytomas in childhood: clinicopathological features in 21 cases. Childs Nerv Syst 1998;14:537-546.
114. Pencalet P, Maixner W, Sainte-Rose C, et al. Benign cerebellar astrocytomas in children. J Neurosurg 1999;90:265-273.
115. Sgouros S, Fineron PW, Hockley AD. Cerebellar astrocytoma of childhood: long-term follow-up. Childs Nerv Syst 1995;11: 89-96.
116. Burger PC, Scheithauer BW, Vogel FS (eds). Surgical Pathology of the Nervous System and its Coverings, 3rd ed. New York: Churchill Livingstone, 1991.
117. Garcia DM, Marks JE, Latifi HR, et al. Childhood cerebellar astrocytomas: is there a role for postoperative irradiation? Int J Radiat Oncol Biol Phys 1990;18:815-818.
118. Schneider JH, Raffel C, McComb JG. Benign cerebellar astrocy-tomas of childhood. Neurosurgery 1992;30:58-63.
119. Ilgren EB, Stiller CA. Cerebellar astrocytomas: therapeutic man-agement. Acta Neurochir 1986;81:11-26.
120. Larson DA, Wara WM, Edwards MSB. Management of child-hood cerebellar astrocytoma. Int J Radiat Oncol Biol Phys 1980;18:971-973.
121. Hirsch J-F, Rose CS, Pierre-Kahn A, et al. Benign astrocytic and oligodendrocytic tumors of the cerebral hemispheres in chil-dren. J Neurosurg 1989;70:568-572.
122. Hoffman HJ, Soloniuk DS, Humphreys RP, et al. Management and outcome of low-grade astrocytomas of the midline in chil-dren: a retrospective review. Neurosurgery 1993;33:964-971.
123. Reardon D, Gajjar A, Walter AW, et al. Bithalamic involvement predicts poor outcome among children with thalamic glial tumors. Pediatr Neurosurg 1998;29:29-35.
124. Krouwer HGJ, Prados MD. Infiltrative astrocytomas of the tha-lamus. J Neurosurg 1995;82:548-557.
125. Albright AL, Price RA, Guthkelch AN. Diencephalic gliomas of children: a clinicopathologic study. Cancer 1985;55:2789-2793.
126. Cairncross JG, Laperriere NJ. Low-grade glioma: to treat or not to treat? Arch Neurol 1989;46:1238-1239.
127. Bernstein M, Hoffman HJ, Halliday WC, et al. Thalamic tumors in children: long-term follow-up and treatment guidelines. J Neurosurg 1984;61:649-656.
128. Kelly PJ. Stereotactic biopsy and resection of thalamic astrocyto-mas. Neurosurgery 1989;25:185-194.
129. Leibel SA, Sheline GE. Review article: radiation therapy for neo-plasms of the brain. J Neurosurg 1987;66:1-22.
130. Boydston WR, Sanford RA, Muhlbauer MS, et al. Gliomas of the tectum and periaqueductal region of the mesencephalon. Pediatr Neurosurg 1991;17:234-238.
131. Medbery CA, Straus KL, Steinberg SM, et al. Low-grade astro-cytomas: treatment results and prognostic variables. Int J Radiat Oncol Biol Phys 1988;15:837-841.
132. Whitton AC, Bloom HJG. Low-grade glioma of the cerebral hemispheres in adults: a retrospective analysis of 88 cases. Int J Radiat Oncol Biol Phys 1990;18:783-786.
133. Leighton C, Fisher B, Bauman G, et al. Supratentorial low-grade glioma in adults: an analysis of prognostic factors and timing of radiation. J Clin Oncol 1997;15:1294-1301.
134. Shaw EG, Daumas-Duport C, Scheithauer BW, et al. Radiation therapy in the management of low-grade supratentorial astrocy-tomas. J Neurosurg 1989;70:853-861.
135. Karim AB, Maat B, Hatlevoll R, et al. A randomized trial of dose-response in radiation therapy of low-grade cerebral glioma: EORTC study 22844. Int J Radiat Oncol Biol Phys 1996;36: 549-556.
136. Dunbar SF, Tarbell NJ, Kooy HM, et al. Stereotactic radiotherapy for pediatric and adult brain tumors: preliminary report. Int J Radiat Oncol Biol Phys 1994;30:531-539.

PART 10 Central Nervous System864
137. Listernick R, Louis DN, Packer RJ, et al. Optic pathway glio-mas in children with neurofibromatosis 1: consensus statement from the NF1 Optic Pathway Gliomas Task Force. Ann Neurol 1997;41:143-149.
138. Horwich A, Bloom HJG. Optic gliomas: radiation therapy and prognosis. Int J Radiat Oncol Biol Phys 1985;11:1067-1079.
139. Alvord EC, Lofton S. Gliomas of the optic nerve or chiasm: out-come by patient’s age, tumor site, and treatment. J Neurosurg 1988;68:85-98.
140. Hoyt WF, Baghdassarian SA. Optic glioma of childhood: natural history and rationale for conservative management. Br J Oph-thalmol 1969;53:793-798.
141. Imes RK, Hoyt WF. Childhood chiasmal gliomas: update on the fate of patients in the 1969 San Francisco study. Br J Ophthal-mol 1986;70:179-182.
142. Wong JYC, Wara W, Sheline GE. Optic gliomas: a reanalysis of the University of California, San Francisco, experience. Cancer 1987;60:1847-1855.
143. Jenkin D, Angyalfi S, Becker L, et al. Optic glioma in children: surveillance, resection, or irradiation? Int Radiat Oncol Biol Phys 1993;25:215-225.
144. Bataini JP, Delanian S, Ponvert D. Chiasmal gliomas: results of irradiation management in 57 patients and review of literature. Int J Radiat Oncol Biol Phys 1991;21:615-623.
145. Tao ML, Barnes PD, Billett AL, et al. Childhood optic chiasm gliomas: radiographic response following radiotherapy and long-term clinical outcome. Int J Radiat Oncol Biol Phys 1997;39: 579-587.
146. Fletcher WA, Imes RK, Hoyt WF. Chiasmal gliomas: appearance and long-term changes demonstrated by computerized tomog-raphy. J Neurosurg 1986;65:154-159.
147. Wisoff JH, Abbott R, Epstein F. Surgical management of exo-phytic chiasmatic-hypothalamic tumors of childhood. J Neuro-surg 1990;73:661-667.
148. Packer RJ, Lange B, Ater J, et al. Carboplatin and vincristine for recurrent and newly diagnosed low-grade gliomas of childhood. J Clin Oncol 1993;11:850-856.
149. Packer RJ, Ater J, Allen J, et al. Carboplatin and vincristine chemotherapy for children with newly diagnosed progressive low-grade gliomas. J Neurosurg 1997;86:747-754.
150. Mahoney DH, Cohen ME, Friedman HS, et al. Carboplatin is ef-fective therapy for young children with progressive optic path-way tumors: a Pediatric Oncology Group phase II study. Neu-rooncology 2000;2:213-220.
151. Somaza SC, Kondziolka D, Lunsford LD, et al. Early outcomes after stereotactic radiosurgery for growing pilocytic astrocyto-mas in children. Pediatr Neurosurg 1996;25:109-115.
152. Grabb PA, Lunsford LD, Albright AL, et al. Stereotactic radiosurgery for glial neoplasms of childhood. Neurosurgery 1996;38:696-702.
153. Pollack IF, Hurtt M, Pang D, et al. Dissemination of low grade astrocytomas in children. Cancer 1994;73:2869-2878.
154. Prados M, Mamelak AN. Metastasizing low grade gliomas in chil-dren. Redefining an old disease. Cancer 1994;73:2671-2673.
155. Gajjar A, Bhargava R, Jenkins JJ, et al. Low-grade astrocy-toma with neuraxis dissemination at diagnosis. J Neurosurg 1995;83:67-71.
156. Kepes JJ, Rubinstein LJ, Eng LF. Pleomorphic xanthoastrocy-toma: a distinctive meningocerebral glioma of young subjects with relatively favorable prognosis: a study of 12 cases. Cancer 1979;44:1839-1852.
157. Taratuto AL, Monges J, Lylyk P, et al. Superficial cerebral astro-cytoma attached to dura. Cancer 1984;54:2505-2512.
158. Fouladi M, Jenkins J, Burger P, et al. Pleomorphic xanthoastro-cytoma (PXA): favorable outcome following complete surgical resection. Neuro Oncol 2001;3:184-192.
159. Merchant TE, Zhu Y, Thompson SJ, et al. Preliminary results from a phase II trial of conformal radiation therapy for pediatric patients with localized low-grade astrocytomas and ependymoma. Int J Radiat Oncol Biol Phys 2002;52: 325-332.
160. Shaw E, Arusell R, Scheithauer B, et al. Prospective randomized trial of low- versus high-dose radiation therapy in adults with supratentorial low-grade glioma: initial report of a North Cen-tral Cancer Treatment Group/Radiation Therapy Oncology Group/Eastern Cooperative Oncology Group Study. J Clin On-col 2002;20:2367-2376.
161. Pollack IF, Claassen D, Al-Shboul Q, et al. Low grade gliomas of the cerebral hemispheres in children: an analysis of 71 cases. J Neurosurg 1995;82:536-547.
162. McLaurin RL, Breneman J, Aron B. Hypothalamic gliomas: re-view of 18 cases. Concepts Pediatr Neurosurg 1987;7:19.
163. Albright AL, Price RA, Guthkelch AN. Brainstem gliomas of children: a clinicopathologic study. Cancer 1983;52:2313-2319.
164. Albright AL, Guthkelch AN, Packer RJ, et al. Prognostic factors in pediatric brainstem gliomas. J Neurosurg 1986;65:751-755.
165. Barkovich AJ, Krischer J, Kun LE, et al. Brain stem gliomas: a classification system based on magnetic resonance imaging. Pedi-atr Neurosurg 1990;16:73-83.
166. Hoffman HJ, Becker I, Craven MA. A clinically and pathologi-cally distinct group of benign brainstem gliomas. Neurosurgery 1980;7:243-248.
167. Stroink AR, Hoffman HJ, Hendrick EB, et al. Diagnosis and management of pediatric brainstem gliomas. J Neurosurg 1986;65:745-750.
168. Khatib ZA, Heideman RL, Kovnar EH, et al. Predominance of pilocytic histology in dorsally exophytic brain stem tumors. Pediatr Neurosurg 1994;20:2-10.
169. Fisher PG, Breiter SN, Carson BS, et al. A clinicopathologic reappraisal of brain stem tumor classification. Identification of pilocytic astrocytoma and fibrillary astrocytoma as distinct enti-ties. Cancer 2000;89:1569-1576.
170. Mantravadi RVP, Phatak R, Bellur S, et al. Brainstem gliomas: an autopsy study of 25 cases. Cancer 1982;49:1294-1296.
171. Schulz-Ertner D, Debus J, Lohr F, et al. Fractionated stereotactic conformal radiation therapy of brain stem gliomas: outcome and prognostic factors. Radiother Oncol 2000;57:215-223.
172. Shrieve DC, Wara WM, Edwards MSB, et al. Hyperfractionated radiation therapy for gliomas of the brainstem in children and in adults. Int J Radiat Oncol Biol Phys 1992;24:599-610.
173. Freeman CR, Krischer JP, Sanford RA, et al. Final results of a study of escalating doses of hyperfractionated radiotherapy in brain stem tumors in children: a Pediatric Oncology Group study. Int J Radiat Oncol Biol Phys 1993;27:197-206.
174. Freeman CR, Bourgouin PM, Sanford RA, et al. Long term sur-vivors of childhood brain stem gliomas treated with hyperfrac-tionated radiotherapy, clinical characteristics and treatment re-lated toxicities. Cancer 1996;77:555-562.
175. Mandell LR, Kadota R, Freeman C, et al. There is no role for hyperfractionated radiotherapy in the management of children with newly diagnosed diffuse intrinsic brainstem tumors: results of a Pediatric Oncology Group phase III trial comparing conven-tional vs. hyperfractionated radiotherapy. Int J Radiat Oncol Biol Phys 1999;43:959-964.
176. Freeman CR, Kepner J, Kun LE, et al. A detrimental effect of a combined chemotherapy-radiotherapy approach in children with diffuse intrinsic brain stem gliomas? Int J Radiat Oncol Biol Phys 2000;47:561-564.
177. Tait DM, Thornton-Jones H, Bloom HJG, et al. Adjuvant chem-otherapy for medulloblastoma: the first multicenter control trial of the International Society of Paediatric Oncology (SIOP I). Eur J Cancer Clin Oncol 1990;26:464-469.
178. Duffner PK, Horowitz ME, Krischer JP, et al. Postoperative chemotherapy and delayed radiation in children less than three years of age with malignant brain tumors. N Engl J Med 1993;328:1725-1731.
179. Ilgren EB, Stiller CA, Hughes JT, et al. Ependymomas: a clinical and pathologic study, part 1: biologic features. Clin Neuropathol 1984;3:113-121.
180. Sanford RA, Kun LE, Heideman RL, et al. Cerebellar pontine angle ependymoma in infants. Pediatr Neurosurg 1997;27: 84-91.

33 The Brain and Spinal Cord 865
181. Bloom HJG. Intracranial tumors: response and resistance to therapeutic endeavors. 1970-1980. Int J Radiat Oncol Biol Phys 1982;8:1083-1113.
182. Vanuystel LJ, Bessell EM, Ashley SE, et al. Intracranial ependy-moma: long-term results of a policy of surgery and radiotherapy. Int J Radiat Oncol Biol Phys 1982;23:313-319.
183. Goldwein JW, Glauser TA, Packet RJ, et al. Recurrent intracra-nial ependymomas in children: survival, patterns of failure, and prognostic factors. Cancer 1990;66:557-563.
184. Rezai AR, Woo HH, Lee M, et al. Disseminated ependymo-mas of the central nervous system. J Neurosurg 1996;85: 618-624.
185. Centeno RS, Lee AA, Winter J, et al. Supratentorial ependymo-mas. Neuroimaging and clinicopathological correlation. J Neu-rosurg 1986;64:209-215.
186. Rawlings CE III, Giangaspero F, Burger PC, et al. Ependymomas: a clinicopathologic study. Surg Neurol 1988;29:271-281.
187. Rorke LB. Relationship of morphology of ependymoma in chil-dren to prognosis. Prog Exp Tumor Res 1987;30:170-174.
188. Ross GW, Rubinstein LJ. Lack of histopathological correlation of malignant ependymomas with postoperative survival. J Neu-rosurg 1989;70:31-36.
189. Rousseau P, Habrand JL, Sarrazin D, et al. Treatment of intracra-nial ependymomas of children: review of a 15-year experience. Int J Radiat Oncol Biol Phys 1994;28:381-386.
190. Pollack IF, Gerszten PC, Martinez AJ, et al. Intracranial ependy-momas of childhood: long-term outcome and prognostic factors. Neurosurgery 1995;37:655-667.
191. Healey EA, Braners PD, Kupsky WJ, et al. The prognostic signifi-cance of postoperative residual tumor in ependymoma. Neuro-surgery 1991;28:666-672.
192. Nazar GB, Hoffman HJ, Becker LE, et al. Infratentorial ependy-momas in childhood: prognostic factors and treatment. J Neuro-surg 1990;72:408-417.
193. Hukin J, Epstein F, Lefton D, et al. Treatment of intracranial ependymoma by surgery alone. Pediatr Neurosurg 1998;29: 40-45.
194. Duffner PK, Krischer JP, Sanford RA, et al. Prognostic factors in infants and very young children with intracranial ependymomas. Pediatr Neurosurg 1998;28:215-222.
195. Lefkowitz I, Evans A, Sposto R, et al. Adjuvant chemotherapy of childhood posterior fossa (PF) ependymoma: craniospinal ir-radiation with or without CCNU, vincristine (VCR) and pred-nisone (P) [abstract]. Proc Am Soc Clin Oncol 1989;8:87a.
196. Strother D, Kepner J, Aronin P, et al. Dose-intensive (DI) chem-otherapy (CT) prolongs event-free survival (EFS) for very young children with ependymoma (EP). Results of Pediatric Oncology Group (POG) Study 9233 [abstract]. Proc Am Soc Clin Oncol 2000;19. 585a, 2302.
197. Goldwein JW, Corn BW, Finlay JL, et al. Is craniospinal irradia-tion required to cure children with malignant (anaplastic) in-tracranial ependymomas? Cancer 1991;67:2766-2771.
198. Merchant TE, Haida T, Wang M-H., et al. Anaplastic ependymo-ma: treatment of pediatric patients with or without craniospinal radiation therapy. J Neurosurg 1997;86:943-949.
199. Kovnar EH, Curran W, Tomita T, et al. Hyperfractionated irradiation for childhood ependymoma: improved local control in subtotally resected tumors [abstract]. Paper presented at the Eighth International Symposium on Pediatric Neuro-Oncology, May 6-9, 1998, Rome, Italy.
200. Aggarwal R, Yeung D, Muhlbauer M, et al. Efficacy and feasibil-ity of stereotactic radiosurgery in the primary management of unfavorable pediatric ependymoma. Radiother Oncol 1997;43: 269-273.
201. Herrick MK. Pathology of pineal tumors. In Neuwelt EA (ed): Diagnosis and Treatment of Pineal Region Tumors. Baltimore: Williams & Wilkins, 1984, pp 31-60.
202. Glenn OA, Barkovich AJ. Intracranial germ cell tumors: a com-prehensive review of proposed embryonic deprivation. Pediatr Neurosurg 1996;24:242-251.
203. Rich TA, Cassady JR, Strand RD, et al. Radiation therapy for pineal and suprasellar germ cell tumors. Cancer 1985;55: 932-940.
204. Ho DM, Lieu H-C. Primary intracranial germ cell tumor. Patho-logic study of 51 patients. Cancer 1992;70:1577-1584.
205. Dernaley DP, A’Hern RP, Whittaker S, et al. Pineal and CNS germ cell tumors: Royal Marsden Hospital experience 1962-1987. Int J Radiat Oncol Biol Phys 1990;18:773-781.
206. Wolden SL, Wara WM, Larson DA, et al. Radiation therapy for primary intracranial germ-cell tumors. Int J Radiat Oncol Biol Phys 1995;32:943-949.
207. Borit A, Blackwood W, Mair WGP. The separation of pineocy-toma from pineoblastoma. Cancer 1980;45:1408-1418.
208. DiSclafani A, Hudgins RJ, Edwards MSB, et al. Pineocytomas. Cancer 1989;63:302-304.
209. Schild SE, Scheithauer BW, Schomberg PJ, et al. Pineal paren-chymal tumors. Clinical, pathologic, and therapeutic aspects. Cancer 1993;72:870-880.
210. Schild SE, Haddock MG, Scheithauer BW, et al. Nongermino-matous germ cell tumors of the brain. Int J Radiat Oncol Biol Phys 1996;36:557-563.
211. Shibamoto Y, Takahashi M, Sasai K. Prognosis of intracranial ger-minoma with syncytiotrophoblastic giant cells treated by radia-tion therapy. Int J Radiat Oncol Biol Phys 1997;37:505-510.
212. Jennings MT, Gelman R, Hochberg F. Intracranial germ-cell tumors: natural history and pathogenesis. J Neurosurg 1985;63: 155-167.
213. Jenkin D, Berry M, Chan H, et al. Pineal region germinomas in childhood: treatment considerations. Int J Radiat Oncol Biol Phys 1990;18:541-545.
214. Sung D, Harisiadis L, Chang CG. Midline pineal tumors and suprasellar germinomas: highly curable by irradiation. Radiology 1978;128:745-751.
215. Haddock MG, Schild SE, Scheithauer BE, et al. Radiation ther-apy for histologically confirmed primary central nervous system germinoma. Int J Radiat Oncol Biol Phys 1997;38:915-923.
216. Shibamoto Y, Takahashi M, Abe M. Reduction of the radiation dose for intracranial germinoma: a prospective study. Br J Can-cer 1994;70:984-989.
217. Shirato H, Nishio M, Sawamura Y, et al. Analysis of long-term treatment of intracranial germinoma. Int J Radiat Oncol Biol Phys 1997;37:511-515.
218. Merchant TE, Sherwood SH, Mulhern RK, et al. CNS germi-noma: disease control and long-term functional outcome for 12 children treated with craniospinal irradiation. Int J Radiat Oncol Biol Phys 2000;46:1171-1176.
219. Hardenbergh PH, Golden J, Billet A, et al. Intracranial germi-noma: the case for lower dose radiation therapy. Int J Radiat Oncol Biol Phys 1997;39:419-426.
220. Calaminus G, Bamberg M, Baranzelli MC, et al. Intracranial germ cell tumors: a comprehensive update of the European data. Neuropediatrics 1994;25:26-32.
221. Shibamoto Y, Abe M, Yamashita J, et al. Treatment results of intracranial germinoma as a function of the irradiation volume. Int J Radiat Oncol Biol Phys 1988;15:285-290.
222. Bamberg M, Kortmann R-D, Calaminus G, et al. Radiation therapy for intracranial germinoma: results of the German Co-operative Prospective Trials MAKEI 83/86/89. J Clin Oncol 1999;17:2585-2592.
223. Allen JC, Kim JH, Packer RJ. Neoadjuvant chemotherapy for newly diagnosed germ cell tumors of the central nervous system. J Neurosurg 1987;67:65-70.
224. Bouffet E, Baranzelli MC, Patte C, et al. Combined treatment modality for intracranial germinomas: results of a multicentre SFOP experience. Br J Cancer 1999;79:1199-1204.
225. Balmaceda C, Heller G, Rosenblum M, et al. Chemotherapy without irradiation. A novel approach for newly diagnosed CNS germ cell tumors: results of an international cooperative trial. J Clin Oncol 1996;14:2908-2915.
226. Linstadt D, Wara WM, Edwards MSB, et al. Radiotherapy of pri-mary intracranial germinomas: the case against routine craniospi-nal irradiation. Int J Radiat Oncol Biol Phys 1988;15:291-297.
227. Maity A, Shu HK, Janss A, et al. Craniospinal radiation in the treatment of biopsy-proven intracranial germinomas: twenty-five years’ experience in a single center. Int J Radiat Oncol Biol Phys 2004;58:1165-1170.

PART 10 Central Nervous System866
228. Buckner JC, Peethambaram PP, Smithson WA, et al. Phase II trial of primary chemotherapy followed by reduced-dose radia-tion for CNS germ cell tumors. J Clin Oncol 1999;17:933-940.
229. Allen JC, DaRosso RC, Donahue B, et al. A phase II trial of preir-radiation carboplatin in newly diagnosed germinoma of the cen-tral nervous system. Cancer 1994;74:940-944.
230. Robertson PL, DaRosso RC, Allen JC. Improved prognosis of intracranial non-germinoma germ cell tumors with multimodal-ity therapy. J Neurooncol 1997;32:71-80.
231. Aoyama H, Shirato H, Yoshida H, et al. Retrospective multi- institutional study of radiotherapy for intracranial non-germino-matous germ cell tumors. Radiother Oncol 1998;49:55-59.
232. Jakacki RI, Zeltzer PM, Boyett JM, et al. Survival and prognostic factors following radiation and/or chemotherapy for primitive neuroectodermal tumors of the pineal region in infants and chil-dren: a report of the Children’s Cancer Group. J Clin Oncol 1995;13:1377-1383.
233. Adamson TE, Wiestler OD, Kleihues P, et al. Correlation of clin-ical and pathological features in surgically treated craniopharyn-giomas. J Neurosurg 1990;73:12-17.
234. Hoffman HJ, De Silva M, Humphreys RP, et al. Aggressive surgi-cal management of craniopharyngiomas in children. J Neurosurg 1992;76:47-52.
235. Hoffman HJ. Surgical management of craniopharyngioma. Pedi-atr Neurosurg 1994;21:44-49.
236. Yarsargil MG, Curcic M, Kis S, et al. Total removal of craniophar-yngiomas: approaches and long-term results in 144 patients. J Neurosurg 1990;73:3-11.
237. Sanford RA. Craniopharyngioma: results of survey of the American Society of Pediatric Neurosurgery. Pediatr Neurosurg 1994;21:39-43.
238. Scott RM, Hetelekidis S, Barnes PD, et al. Surgery, radiation, and combination therapy in the treatment of childhood craniophar-yngioma—a 20-year experience. Pediatr Neurosurg 1994;21: 75-81.
239. Wen B-C., Hussey DH, Staples J, et al. A comparison of the roles of surgery and radiation therapy in the management of crani-opharyngiomas. Int J Radiat Oncol Biol Phys 1989;16:17-24.
240. Sweet WH. History of surgery for craniopharyngiomas. Pediatr Neurosurg 1994;21:28-38.
241. Tomita T, McLone DG. Radical resections of childhood crani-opharyngiomas. Pediatr Neurosurg 1993;19:6-14.
242. Yasargil MC, Curcic M, Kis S, et al. Total removal of craniophar-yngiomas: approaches and long-term results in 144 patients. J Neurosurg 1990;73:3-11.
243. Tomita T, McLone DG. Radical resections of childhood crani-opharyngiomas. Pediatr Neurosurg 1993;19:6-14.
244. Fischer EG, Welch K, Shillito J Jr, et al. Craniopharyngiomas in children: long-term effects of conservative surgical procedures combined with radiation therapy. J Neurosurg 1990;73: 534-540.
245. Fischer EG, Welch K, Shilito J Jr, et al. Craniopharyngiomas in children. Long-term effects of conservative surgical proce-dures combined with radiation therapy. J Neurosurg 1990;73: 534-540.
246. Sklar CA. Craniopharyngioma: endocrine sequelae of treatment. Pediatr Neurosurg 1994;21:120-123.
247. Curtis J, Daneman D, Hoffman HJ, et al. The endocrine outcome after surgical removal of craniopharyngiomas. Pediatr Neurosurg 1994;21:24-27.
248. Kramer S, Southard M, Mansfield CM. Radiotherapy in the management of craniopharyngiomas. AJR Am J Roentgenol 1968;103:44-52.
249. Kramer S, McKissock W, Concannon JP. Craniopharyngiomas: treatment by combined surgery and radiation therapy. J Neuro-surg 1961;18:217-226.
250. Kramer S, Southard M, Mansfield CM. Radiotherapy in the management of craniopharyngiomas: further experience and late results. Am J Roentgenol Radium Ther Nucl Med 1968;103: 44-52.
251. Regine WF, Kramer S. Pediatric craniopharyngiomas: long-term results of combined treatment with surgery and radiation. Int J Radiat Oncol Biol Phys 1992;24:611-617.
252. Brada M, Thomas DGT. Craniopharyngioma revisited. Int J Radiat Oncol Biol Phys 1993;27:471-475.
253. Hetelididis S, Barnes PD, Tao ML, et al. Twenty year experience in childhood craniopharyngioma. Int J Radiat Oncol Biol Phys 1993;27:189-195.
254. Rajan B, Ashley S, Gorman C, et al. Craniopharyngioma—long term results following limited surgery and radiotherapy. Radi-other Oncol 1993;26:1-10.
255. Flickinger JC, Lunsford LD, Singer J, et al. Megavoltage external beam irradiation of craniopharyngiomas: analysis of tumor control and morbidity. Int J Radiat Oncol Biol Phys 1990;19: 117-122.
256. Lunsford LD, Pollack BE, Kondziolka DS, et al. Stereotactic op-tions in the management of craniopharyngioma. Pediatr Neuro-surg 1994;21:90-97.
257. Backlund EO, Axelsson B, Bergstrand CG, et al. Treatment of craniopharyngiomas—the stereotactic approach in a ten to twenty-three years’ perspective. Surgical, radiological and oph-thalmological aspects. Acta Neurochir 1989;99(Pt 1):11-19.
258. Baskin DS, Wilson CB. Surgical management of craniopharyngi-omas: a review of 74 cases. J Neurosurg 1986;65:22-27.
259. Merchant TE, Kiehna EN, Sanford RA, et al. Craniopharyngi-oma: the St. Jude Children’s Research Hospital experience. Int J Radiat Oncol Biol Phys 2002;53:533-542.
260. Hoogenhout J, Otten BJ, Kazem I, et al. Surgery and radiation therapy in the management of craniopharyngiomas. Int J Radiat Oncol Biol Phys 1984;10:2293-2297.
261. Sung DI, Chang CH, Harisiadis L, et al. Treatment results in craniopharyngiomas. Cancer 1981;47:847-852.
262. Hart MN, Earle KM. Primitive neuroectodermal tumors of the brain in children. Cancer 1973;32:890-897.
263. Kosnik EJ, Boesel CP, Bau J, et al. Primitive neuroectodermal tumors of the central nervous system in children. J Neurosurg 1978;48:741-746.
264. Bennett JP, Rubinstein LJ. The biological behavior of primary cerebral neuroblastoma: a reappraisal of the clinical course in a series of 70 cases. Ann Neurol 1984;16:21-27.
265. Cruz-Sanchez FF, Rossi ML, Hughes JT, et al. Differentiation in embryonal neuroepithelial tumors of the central nervous sys-tem. Cancer 1991;67:965-976.
266. Berger MS, Edwards MSB, Wara WM, et al. Primary cerebral neuroblastoma: long-term follow-up review and therapeutic guidelines. J Neurosurg 1983;59:418-423.
267. Gaffney CC, Sloane JP, Bradley NJ, et al. Primitive neuroec-todermal tumors of the cerebrum: pathology and treatment. J Neurooncol 1985;3:23-33.
268. Berger MS, Edwards MSB, LaMasters D, et al. Pediatric brain-stem tumors: radiographic, pathological, and clinical correla-tions. Neurosurgery 1983;12:298-302.
269. Horten BC, Rubinstein LJ. Primary cerebral neuroblastoma: a clinicopathological study of 35 cases. Brain 1976;99:735-756.
270. Ashwal S, Hinshaw DB Jr, Bedros A. CNS primitive neuroec-todermal tumors of childhood. Med Pediatr Oncol 1984;12: 180-188.
271. Zeltzer PM, Boyett JM, Finlaye JL, et al. Metastasis stage, ad-juvant treatment, and residual tumor are prognostic factors for medulloblastoma in children: conclusions from the Children’s Cancer Group 921 randomized phase III study. J Clin Oncol 1999;17:832-845.
272. Stiller CA, Bunch KJ. Brain and spinal tumors in children aged under two years: incidence and survival in Britain, 1971-1985. Br J Cancer 1992;66:S50-S53.
273. Cohen BH, Packer RJ, Siegel KR, et al. Brain tumors in children under 2 years: treatment, survival and long-term prognosis. Pedi-atr Neurosurg 1993;19:171-179.
274. Brown K, Mapstone TB, Oakes WJ. A modern analysis of intrac-ranial tumors of infancy. Pediatr Neurosurg 1997;26:25-32.
275. Gilles FH, Sobel EL, Tavare CJ, et al. Age-related changes in diagnoses, histological features, and survival in children with brain tumors: 1930-1979. Neurosurgery 1995;37:1056-1068.

33 The Brain and Spinal Cord 867
276. Rorke LB, Packer RJ, Biegel JA, et al. Central nervous system atypical teratoid/rhabdoid tumors of infancy and childhood: definition of an entity. J Neurosurg 1996;85:56-65.
277. Burger PC, Yu I-T, Tihan T, et al. Atypical teratoid/rhabdoid tu-mor of the central nervous system: a highly malignant tumor of infancy and childhood frequently mistaken for medullob-lastoma. A Pediatric Oncology Group study. Am J Surg Pathol 1998;22:1083-1092.
278. Pancelet P, Sainte-Rose C, Lellough-Tubiana A, et al. Papillomas and carcinomas of the choroid plexus in children. J Neurosurg 1998;88:521-528.
279. Weiss E, Behring B, Behnke J, et al. Treatment of primary malig-nant rhabdoid tumor of the brain: report of three cases and re-view of the literature. Int J Radiat Oncol Biol Phys 1998;41: 1013-1019.
280. Taratuto AL, Monges J, Lylyk P, et al. Superficial cerebral astro-cytoma attached to dura: report of six cases in infants. Cancer 1984;54:2505-2512.
281. Mulhern RK, Hancock J, Fairclough D, et al. Neuropsychologi-cal status of children treated for brain tumors: a critical review and integrative analysis. Med Pediatr Oncol 1992;20:181-191.
282. Evans AE, Jenkin RDT, Sposto R, et al. The treatment of medul-loblastoma. Results of a prospective randomized trial of radiation therapy with and without CCNU, vincristine, and prednisone. J Neurosurg 1990;72:572-582.
283. Deutsch M. Radiotherapy for primary brain tumors in very young children. Cancer 1982;50:2785-2789.
284. Jenkin D, Greenberg M, Hoffman H, et al. Brain tumors in chil-dren: long-term survival after radiation therapy. Int J Radiat Oncol Biol Phys 1995;31:445-451.
285. Allen JC, Helson L, Jereb B. Preradiation chemotherapy for just this minute diagnosed childhood brain tumors: a modified phase II trial. Cancer 1983;52:2001-2006.
286. Baram TZ, van Eys J, Dowell RE, et al. Survival and neurologic outcome in infants with medulloblastoma treated with sur-gery and MOPP chemotherapy: a preliminary report. Cancer 1987;60:173-177.
287. Horowitz ME, Mulhern RK, Kun LE, et al. Brain tumors in the very young child: postoperative chemotherapy in combined- modality treatment. Cancer 1988;61:428-434.
288. Duffner PK, Horowitz ME, Krischer JP, et al. The treatment of malignant brain tumors in infants and very young children: an update of the Pediatric Oncology Group experience. Neuroon-cology 1999;1:152-161.
289. Geyer JR, Zeltzer PM, Boyett JM, et al. Survival of infants with primitive neuroectodermal tumors or malignant ependymomas of the CNS treated with eight drugs in 1 day: a report from the Children’s Cancer Group. J Clin Oncol 1994;12:1607-1615.
290. Kuhl J, Beck J, Bode U, et al. Delayed radiation therapy (RT) after postoperative chemotherapy (PCH) in children less than 3 years of age with medulloblastoma. Results of the trial HIT-SKK’87, and preliminary results of the pilot trial HIT-SKK’92 [abstract]. Med Pediatr Oncol 1995;25:250.
291. Walter AW, Mulhern RK, Gajjar A, et al. Survival and neu-rodevelopmental outcome of young children with medullob-lastoma at St. Jude Children’s Research Hospital. J Clin Oncol 1999;17:3720-3728.
292. Dupuis-Girod S, Hartmann O, Benhamou E, et al. Will high dose chemotherapy followed by autologous bone marrow trans-plantation supplant craniospinal irradiation in young children treated for medulloblastoma? J Neurooncol 1996;27:87-98.
293. Gajjar A, Mulhern RK, Heideman RL, et al. Medulloblastoma in very young children: outcome of definitive craniospinal irra-diation following incomplete response to chemotherapy. J Clin Oncol 1994;12:1212-1216.
294. Rutkowski S, Bode U, Deinlein F, et al. Treatment of early child-hood medulloblastoma by postoperative chemotherapy alone. N Engl J Med 2005;352:978-986.
295. Grill J, Le Deley M-C., Gambarelli D, et al. Postoperative chem-otherapy without irradiation for ependymoma in children under 5 years of age: a multicenter trial of the French Society of Pedi-atric Oncology. J Clin Oncol 2001;19:1288-1296.
296. Hilden JM, Watterson J, Longee DC, et al. Central nervous system atypical teratoid tumor/rhabdoid tumor: response to intensive therapy and review of the literature. J Neurooncol 1998;40:265-275.
297. Kernohan JW, Sayre GP. Tumors of the Central Nervous Sys-tem. Washington, DC: American Registry of Pathology, Armed Forces Institute of Pathology, 1952.
298. Nelson JS, Taukada Y, Schoenfeld D, et al. Necrosis as a prog-nostic criterion in malignant supratentorial, astrocytic gliomas. Cancer 1983;52:550-554.
299. Werner-Wasik M, Scott CB, Nelson DF, et al. Final report of a phase I/II trial of hyperfractionated and accelerated hyper-fractionated radiation therapy with carmustine for adults with supratentorial malignant gliomas. Radiation Therapy Oncology Group study 83-02. Cancer 1996;77:1535-1543.
300. Burger PC, Heinz ER, Shibata T, et al. Topographic anatomy and CT correlations in the untreated glioblastoma multiforme. J Neurosurg 1988;68:698-704.
301. Halperin EC, Bentel G, Heinz ER, et al. Radiation therapy treat-ment planning in supratentorial glioblastoma multiforme: an analysis based on postmortem topographic anatomy with CT correlations. Int J Radiat Oncol Biol Phys 1989;17:1347-1350.
302. Kelly PJ, Daumas-Duport C, Kispert DB, et al. Imaging-based stereotaxic serial biopsies in untreated intracranial glial neo-plasms. J Neurosurg 1987;66:865-874.
303. Choucair AK, Levin VA, Gutin PH, et al. Development of mul-tiple lesions during radiation therapy and chemotherapy in pa-tients with gliomas. J Neurosurg 1986;65:654-658.
304. Kopelson G, Linggood R. Infratentorial glioblastoma: the role of neuraxis irradiation. Int J Radiat Oncol Biol Phys 1982;8: 999-1003.
305. Nelson DF, Nelson JS, Davis DR, et al. Survival and prognosis of patients with astrocytoma with atypical or anaplastic features. J Neurooncol 1985;3:99-103.
306. Walker MD, Green SB, Byar DP, et al. Randomized comparisons of radiotherapy and nitrosoureas for the treatment of malignant glioma after surgery. N Engl J Med 1980;303:1323-1329.
307. Prados MD, Gutin PH, Phillips TL, et al. Highly anaplastic astrocytoma: a review of 357 patients treated between 1977 and 1989. Int J Radiat Oncol Biol Phys 1992;23:3-8.
308. Wood JR, Green SB, Shapiro WR. The prognostic importance of tumor size in malignant gliomas: a CT scan study by the Brain Tumor Cooperative Group. J Clin Oncol 1988;6:338-343.
309. Wisoff JH, Boyett JM, Berger MS, et al. Current neurosurgi-cal management and the impact of the extent of resection in the treatment of malignant gliomas of childhood: a report of the Children’s Cancer Group Trial no. CCG-945. J Neurosurg 1998;89:52-59.
310. Garden AS, Maor MH, Yung WKA, et al. Outcome and patterns of failure following limited-volume irradiation for malignant as-trocytomas. Radiother Oncol 1991;20:99-110.
311. Fine HA, Dear KB, Loeffler JS, et al. Meta-analysis of radiation therapy with and without adjuvant chemotherapy for malignant gliomas in adults. Cancer 1993;71:2585-2597.
312. Murray KJ, Nelson DF, Scott C, et al. Quality-adjusted survival analysis of malignant glioma. Patients treated with twice-daily radiation (RT) and carmustine: a report of Radiation Therapy Oncology Group study 83-02. Int J Radiat Oncol Biol Phys 1995;31:453-459.
313. Sneed PK, Gutin PH, Larson DA, et al. Patterns of recurrence of glioblastoma multiforme after external irradiation fol-lowed by implant boost. Int J Radiat Oncol Biol Phys 1994;29: 719-727.
314. Hochberg FH, Pruitt A. Assumptions in the radiotherapy of glioblastoma. Neurology 1980;30:907-911.
315. Wallner KE, Galicich JH, Krol G, et al. Patterns of failure fol-lowing treatment for glioblastoma multiforme and anaplastic astrocytoma. Int J Radiat Oncol Biol Phys 1989;16:1405-1409.
316. Loeffler JS, Alexander E III, Hochberg FH, et al. Clinical pat-terns of failure following stereotactic interstitial irradiation for malignant gliomas. Int J Radiat Oncol Biol Phys 1990;19: 1455-1462.

PART 10 Central Nervous System868
317. Agbi CB, Bernstein M, Laperriere N, et al. Patterns of recur-rence of malignant astrocytoma following stereotactic intersti-tial brachytherapy with 125I implants. Int J Radiat Oncol Biol Phys 1992;23:321-326.
318. Laramore GE, Diener-West M, Griffin TW, et al. Randomized neutron dose searching study for malignant gliomas of the brain: results of an RTOG study. Int J Radiat Oncol Biol Phys 1988;14:1093-1102.
319. Loeffler JS, Alexander E III, Wen PY, et al. Results of stereotactic brachytherapy used in the initial management of patients with glioblastoma. J Natl Cancer Inst 1990;82:1918-1921.
320. Scharfen CO, Sneed PK, Wara WM, et al. High activity iodine-125 interstitial implant for gliomas. Int J Radiat Oncol Biol Phys 1992;24:583-591.
321. Prados MD, Gutin PH, Phillips TL, et al. Interstitial brachytherapy for newly diagnosed patients with malignant gliomas: the UCSF experience. Int J Radiat Oncol Biol Phys 1992;24:593-597.
322. Stelzer KJ, Laramore GE, Griffin TW, et al. Fast neutron radio-therapy: the University of Washington experience. Acta Oncol 1994;33. 275-280.
323. Larson DA, Gutin PH, McDermott M, et al. Gamma knife for glioma: selection factors and survival. Int J Radiat Oncol Biol Phys 1996;36:1045-1053.
324. Pickles T, Goodman GB, Rheaume DE, et al. Pion radiation for high grade astrocytoma: results of a randomized study. Int J Ra-diat Oncol Biol Phys 1997;37:491-497.
325. Sneed PK, Prados MD, McDermott MW, et al. Large effect of age on survival of patients with glioblastoma treated with radiothera-py and brachytherapy boost. Neurosurgery 1995;36:898-904.
326. Wen PY, Alexander E III, Black PM, et al. Long-term results of stereotactic brachytherapy used in the initial treatment of pa-tients with glioblastomas. Cancer 1994;73:3029-3036.
327. Shrieve DC, Alexander E III, Wen PY, et al. Comparison of stere-otactic radiosurgery and brachytherapy in the treatment of recur-rent glioblastoma multiforme. Neurosurgery 1995;36:275-284.
328. Mehta MP, Masciopinto J, Rozental J, et al. Stereotactic radio-surgery for glioblastoma multiforme: report of a prospective study evaluating prognostic factors and analyzing long-term sur-vival advantage. Int J Radiat Oncol Biol Phys 1994;30:541-549.
329. Buatti JM, Friedman WA, Bova FJ, et al. Linac radiosurgery for high grade gliomas: the University of Florida experience. Int J Radiat Oncol Biol Phys 1995;32:205-210.
330. Nelson DF, Diener-West M, Weinstein AS, et al. A randomized comparison of misonidazole sensitized radiotherapy plus BCNU and radiotherapy plus BCNU for treatment of malignant glioma after surgery: final report of an RTOG study. Int J Radiat Oncol Biol Phys 1986;12:1793-1800.
331. Urtusan R, Band P, Chapman JD, et al. Radiation and high-dose metronidazole in supratentorial glioblastomas. N Engl J Med 1976;294:1364-1367.
332. Miralbell R, Mornex F, Greiner R, et al. Accelerated radiother-apy, carbogen, and nicotinamide in glioblastoma multiforme: report of European Organization for Research and Treatment of Cancer Trial 22933. J Clin Oncol 1999;17:3143-3149.
333. Hegarty TJ, Thornton AF, Diaz RF, et al. Intraarterial bromode-oxyuridine radiosensitization of malignant gliomas. Int J Radiat Oncol Biol Phys 1990;19:421-428.
334. Sullivan FJ, Herscher LL, Cook JA, et al. National Cancer In-stitute (phase II) study of high-grade glioma treated with ac-celerated hyperfractionated radiation and iododeoxyuridine: results in anaplastic astrocytoma. Int J Radiat Oncol Biol Phys 1994;30:583-590.
335. Groves MD, Maor MH, Meyers C, et al. A phase II trial of high-dose bromodeoxyuridine with accelerated fractionation radiotherapy followed by procarbazine, lomustine, and vincris-tine for glioblastoma multiforme. Int J Radiat Oncol Biol Phys 1999;45:127-135.
336. Prados MD, Scott C, Sandler H, et al. A phase 3 randomized study of radiotherapy plus procarbazine, CCNU, vincristine (PCV) with or without BrdU for the treatment of anaplastic astrocytoma: a preliminary report of the Radiation Therapy Oncology Group study 9404. Int J Radiat Oncol Biol Phys 1999;45:1109-1115.
337. Saroja KR, Mansell J, Hendrickson FR, et al. Failure of acceler-ated neutron therapy to control high grade astrocytomas. Int J Radiat Oncol Biol Phys 1989;17:1295-1297.
338. Fitzek MM, Thornton AF, Rabinov JD, et al. Accelerated proton/photon irradiation to 90 cobalt gray equivalent for glioblastoma multiforme: results of a phase II prospective trial. J Neurosurg 1999;91:251-260.
339. Leibel SA, Gutin PH, Wara WM, et al. Survival and quality of life after interstitial implantation of removable high-activity iodine 125 sources for treatment of patients with recurrent malignant gliomas. Int J Radiat Oncol Biol Phys 1989;17:1129-1139.
340. Selker RG, Shapiro WR, Green S, et al. A randomized trial of interstitial radiotherapy (IRT) boost for the treatment of newly diagnosed malignant glioma (glioblastoma multiforme, ana-plastic astrocytoma, anaplastic oligodendroglioma, malignant mixed glioma). Brain Tumor Cooperative Group study 87-01 [abstract]. Paper presented at the 45th Meeting of the Congress of Neurological Surgeons. San Francisco: CA, October 14-18, 1995.
341. Florell RC, MacDonald DR, Irish W, et al. Selection bias, sur-vival, and brachytherapy for glioma. J Neurosurg 1992;76: 179-183.
342. Loeffler JSI, Alexander E III, Shea WM, et al. Radiosurgery as part of the initial management of patients with malignant glio-mas. J Clin Oncol 1992;10:1379-1385.
343. Sankaria JN, Mehta MP, Loeffler JS, et al. Radiosurgery in the initial management of malignant gliomas: survival comparison with the Radiation Therapy Oncology Group recursive parti-tioning analysis. Int J Radiat Oncol Biol Phys 1995;32:931-942.
344. Nelson DF, Curran WJ Jr, Scott C, et al. Hyperfractionated radiation therapy and BIS-chlorethyl nitrosourea in the treat-ment of malignant glioma: possible advantage observed at 72 Gy in 1.2 Gy bid fractions: report of the Radiation Therapy Oncology Group protocol 8302. Int J Radiat Oncol Biol Phys 1993;25:193-207.
345. Fallia C, Olmi P. Hyperfractionated and accelerated radiation therapy in central nervous system tumors (malignant glio-mas, pediatric tumors, and brain metastases). Radiother Oncol 1997;43:235-246.
346. Brada M, Sharpe G, Rajan B, et al. Modifying radical radiothera-py in high grade gliomas: shortening the treatment through ac-celeration. Int J Radiat Oncol Biol Phys 1999;43:287-292.
347. Levin VA, Maor MH, Thall PF, et al. Phase II study of acceler-ated fractionation radiation therapy with carboplatin followed by vincristine chemotherapy for the treatment of glioblastoma multiforme. Int J Radiat Oncol Biol Phys 1995;33:357-364.
348. Halperin EC. Multiple-fraction-per-day external beam radio-therapy for adults with supratentorial malignant gliomas. J Neu-rooncol 1992;14:255-262.
349. Fulton DS, Urtasun RC, Scott-Brown I, et al. Increasing radia-tion dose intensity using hyperfractionation on patients with malignant glioma: final report of a prospective phase I-II dose response study. J Neurooncol 1992;14:63-72.
350. Shapiro WR, Green SB, Burger PC, et al. Randomized trial of three chemotherapy regimens and two radiotherapy regimens in postoperative treatment of malignant glioma: Brain Tumor Cooperative Group Trial no. 8001. J Neurosurg 1989;71:1-9.
351. Levin VA, Silver P, Hannigan J, et al. Superiority of post- radiotherapy adjuvant chemotherapy with CCNU, procar-bazine, and vincristine (PCV) over BCNU for anaplastic gliomas: NCOG 6G61 final report. Int J Radiat Oncol Biol Phys 1990;18: 321-324.
352. Medical Research Council Brain Tumour Working Party. Ran-domized trial of procarbazine, lomustine, and vincristine in the adjuvant treatment of high-grade astrocytoma: a Medical Research Council Trial. J Clin Oncol 2001;19:509-518.
353. Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987-996.
354. Athanassiou H, Synodinou M, Maragoudakis E, et al. Rand-omized phase II study of temozolomide and radiotherapy com-pared with radiotherapy alone in newly diagnosed glioblastoma multiforme. J Clin Oncol 2005;23:2372-2377.

33 The Brain and Spinal Cord 869
355. Hegi ME, Diserens AC, Gorlia T, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med 2005;352:997-1003.
356. del Rowe J, Scott C, Werner-Wasik M, et al. Single-arm, open-label phase II study of intravenously administered tirapazamine and radiation therapy for glioblastoma multiforme. J Clin Oncol 2000;18:1254-1259.
357. Valtonen S, Timonen U, Toivanan P, et al. Interstitial chem-otherapy with carmustine-loaded polymers for high-grade gliomas: a randomized double-blind study. Neurosurgery 1997;41:44-49.
358. Nakagawa K, Aoki Y, Fujimaki T, et al. High-dose conformal ra-diotherapy influenced the pattern of failure but did not improve survival in glioblastoma multiforme. Int J Radiat Oncol Biol Phys 1998;40:1141-1149.
359. Sheline GE. Radiotherapy for high grade gliomas. Int J Radiat Oncol Biol Phys 1990;18:793-803.
360. Yung WKA, Janus TJ, Maor M, et al. Adjuvant chemotherapy with carmustine and cisplatin for patients with malignant glio-mas. J Neurooncol 1992;12:131-135.
361. Heideman RL, Kuttesch J, Gajjar AJ, et al. Supratentorial malig-nant gliomas in childhood: a single institution perspective. Can-cer 1997;80:497-504.
362. Finlay JL, Boyett JM, Yates AJ, et al. Randomized phase III trial in childhood high-grade astrocytoma comparing vincristine, lomustine, and prednisone with the eight-drugs-in-1 regimen. J Clin Oncol 1995;13:112-123.
363. Mork SJ, Lindegaard K-F., Halvorsen TB, et al. Oligodendro-glioma: incidence and biological behavior in a defined popula-tion. J Neurosurg 1985;63:881-889.
364. Jenkins RB, Blair H, Ballman KV, et al. A t(1;19)(q10;p10) me-diates the combined deletions of 1p and 19q and predicts a bet-ter prognosis of patients with oligodendroglioma. Cancer Res 2006;66:9852-9861.
365. Brandes AA, Tosoni A, Cavallo G, et al. Correlations between O6-methylguanine DNA methyltransferase promoter methyla-tion status, 1p and 19q deletions, and response to temozolomide in anaplastic and recurrent oligodendroglioma: a prospective GICNO study. J Clin Oncol 2006;24:4746-4753.
366. Shaw EG, Scheithauer BW, O’Fallon JR, et al. Oligodendro-gliomas: the Mayo Clinic experience. J Neurosurg 1992;76: 428-434.
367. Shaw EG, Scheithauer BW, O’Fallon JR. Management of supratentorial low-grade gliomas. Oncology 1993;7:97-107.
368. Sheline GE, Boldney E, Karisburg P, et al. Therapeutic consider-ations in tumors affecting the central nervous system: oligoden-drogliomas. Radiology 1964;82:44-49.
369. Chin HW, Hazel JJ, Kim TH, et al. Oligodendrogliomas. I. A clinical study of cerebral oligodendrogliomas. Cancer 1980;45: 1458-1466.
370. Lindegaard K-F., Mork SJ, Eide GE, et al. Statistical analysis of clinicopathological features, radiotherapy, and survival in 270 cases of oligodendroglioma. J Neurosurg 1987;67:224-230.
371. Reedy PD, Bay JW, Hahn JF. Role of radiation therapy in the treatment of cerebral oligodendroglioma: an analysis of 57 cases and a literature review. Neurosurgery 1983;67:224-230.
372. Allison RR, Schulsinger A, Vongtama V, et al. Radiation and chemotherapy improve outcome in oligodendroglioma. Int J Radiat Oncol Biol Phys 1997;37:399-403.
373. Ludwig CL, Smith MT, Godfrey AD, et al. A clinicopathologi-cal study of 323 patients with oligodendrogliomas. Ann Neurol 1986;19:15-21.
374. Cairncross JG, MacDonald DR. Successful chemotherapy for recurrent malignant oligodendroglioma. Ann Neurol 1988;23: 460-464.
375. Cushing H, Eisenhardt L. Meningiomas: Their Classification, Regional Behavior, Life History, and Surgical End Results. Springfield, IL: Charles C Thomas, 1938.
376. Glaholm J, Bloom HJG, Crow JH. The role of radiotherapy in the management of intracranial meningiomas: the Royal Marsden Hospital experience with 186 patients. Int J Radiat Oncol Biol Phys 1990;18:755-761.
377. Dziuk T, Woo S, Butler B, et al. Malignant meningioma: an indication for initial aggressive surgery and adjuvant radiotherapy. J Neurooncol 1998;37:177-188.
378. Jaaskelainen J, Haltia M, Servo A. Atypical and anaplastic men-ingiomas: radiology, surgery, radiotherapy, and outcome. Surg Neurol 1986;25:233-242.
379. Mirimanoff RO, Rosoretz DE, Linggood RM, et al. Meningioma: analysis of recurrence and progression following neurosurgical resection. J Neurosurg 1985;62:18-24.
380. Goldsmith BJ, Wara WM, Wilson CB, et al. Postoperative irradiation for subtotally resected meningiomas. A retrospective analysis of 140 patients treated from 1967 to 1990. J Neurosurg 1994;80:195-201.
381. Petty AM, Kun LE, Meyer GA. Radiation therapy for incom-pletely resected meningiomas. J Neurosurg 1985;62:502-507.
382. Wara WM, Sheline GE, Newman H, et al. Radiation therapy of meningiomas. AJR Am J Roentgenol 1975;123:453-458.
383. Carelia RJ, Ransohoff J, Newall J. Role of radiation therapy in the management of meningioma. Neurosurgery 1982;10:332-339.
384. Forbes AR, Goldberg ID. Radiation therapy in the treatment of meningioma: the Joint Center for Radiation Therapy experience, 1970 to 1982. J Clin Oncol 1984;2:1139-1143.
385. Maguire PD, Clough R, Friedman AH, et al. Fractionated exter-nal-beam radiation therapy for meningiomas of the cavernous sinus. Int J Radiat Oncol Biol Phys 1999;44:75-79.
386. Lunsford L. Contemporary management of meningiomas: radia-tion therapy as an adjuvant and radiosurgery as an alternative to surgical removal? J Neurosurg 1994;80:187-190.
387. Kondziolka D, Flickinger JC, Perez B. Judicious resection and/or radiosurgery for parasagittal meningiomas: outcomes from a multicenter review. Neurosurgery 1998;43:405-413.
388. Kondziolka D, Levy EI, Niranjan A, et al. Long-term outcomes after meningioma radiosurgery: physician and patient perspec-tives. J Neurosurg 1999;91:44-50.
389. Shafron DH, Friedman WA, Buatti JM, et al. Linac radiosur-gery for benign meningiomas. Int J Radiat Oncol Biol Phys 1999;43:321-327.
390. Smith JL, Vuksanovic MM, Yates BM, et al. Radiation therapy for primary optic nerve meningiomas. J Clin Neuroophthalmol 1981;1:85-89.
391. Borovich B, Doron Y, Braun J, et al. Recurrence of intracra-nial meningiomas: the role played by regional multicentricity. Clinical and radiological aspects. J Neurosurg 1986;65(Pt 2): 168-171.
392. Roche P-H, Regis J, Dufour H, et al. Gamma knife radiosurgery in the management of cavernous sinus meningiomas. J Neuro-surg 2000;93:68-73.
393. Ojemann SG, Sneed PK, Larson DA, et al. Radiosurgery for malignant meningioma: results in 22 patients. J Neurosurg 2000;93:62-67.
394. Deen HC Jr, Scheithauer BW, Ebersold MJ. Clinical and path-ologic study of meningiomas of the first two decades of life. J Neurosurg 1982;56:317-322.
395. Drake JM, Hendrick EB, Becker LE, et al. Intracranial meningi-omas in children. Pediatr Neurosci 1986;12:134-139.
396. Snow RB, Lavyne MH. Intracranial space-occupying lesions in AIDS patients. Neurosurgery 1985;16:148-153.
397. So YT, Beckstead JH, Davis RL. Primary central nervous system lymphoma in AIDS: a clinical and pathologic study. Ann Neurol 1986;20: 566-S72.
398. Reni M, Ferreri AJ, Garancini MP, et al. Therapeutic manage-ment of primary central nervous system lymphoma in immuno-competent patients: results of a critical review of the literature. Ann Oncol 1997;8:227-234.
399. Jack CR, Reese DF, Scheithauer BW. Radiographic findings in 32 cases of primary CNS lymphoma. AJR Am J Roentgenol 1986;146:271-276.
400. Hochberg FH, Miller DC. Primary central nervous system lym-phoma. J Neurosurg 1988;68:835-853.
401. Murray K, Kun L, Cox J. Primary malignant lymphoma of the central nervous system. J Neurosurg 1986;65:600-607.

PART 10 Central Nervous System870
402. Socie G, Piprot-Chauffat C, Schlienger M, et al. Primary lym-phoma of the central nervous system: an unresolved therapeutic problem. Cancer 1990;65:322-326.
403. Nelson DF, Martz KL, Bonner H, et al. Non-Hodgkin’s lympho-ma of the brain: can high-dose, large-volume radiation therapy improve survival? Report on a prospective trial by the Radiation Therapy Oncology Group: RTOG 8315. Int J Radiat Oncol Biol Phys 1992;23:9-17.
404. Loeffler JS, Ervin TJ, Mauch P, et al. Primary lymphomas of the central nervous system: patterns of failure and factors that influ-ence survival. J Clin Oncol 1985;3:490-494.
405. Laperriere NJ, Cerezo L, Milosevic MF, et al. Primary lympho-ma of brain: results of management of a modern cohort with radiation therapy. Radiother Oncol 1997;43:247-252.
406. Glass J, Gruber ML, Cher L, et al. Preirradiation methotrexate chemotherapy of primary central nervous system lymphoma: long-term outcome. J Neurosurg 1994;81:188-195.
407. Abrey LE, DeAngelis LM, Yahalom J. Long-term survival in pri-mary CNS lymphoma. J Clin Oncol 1998;16:859-863.
408. Abrey LE, Yahalom J, DeAngelis LM. Treatment for pri-mary CNS lymphoma: the next step. J Clin Oncol 2000;18: 3144-3150.
409. Schultz C, Scott C, Sherman W, et al. Preirradiation chemo-therapy with cyclophosphamide, doxorubicin, vincristine, and dexamethasone for primary CNS lymphomas: initial report of Radiation Therapy Oncology Group Protocol 88-06. J Clin On-col 1996;14:556-564.
410. O’Neill BP, Wang C-H., O’Fallon JR, et al. Primary central nerv-ous system non-Hodgkin’s lymphoma (PCNSL): Survival ad-vantages with combined initial therapy? A final report of the North Central Cancer Treatment Group study 86-72-52. Int J Radiat Oncol Biol Phys 1999;43:559-563.
411. Ferreri AJM, Reni M, Villa E. Therapeutic management of pri-mary central nervous system lymphoma: lessons from prospec-tive trials. Ann Oncol 2000;11:927-937.
412. DeAngelis LM, Seiferheld W, Schold SC, et al. Combination chemotherapy and radiotherapy for primary central nervous system lymphoma: Radiation Therapy Oncology Group Study 93-10. J Clin Oncol 2002;20:4643-4648.
413. Posner JB. Management of central nervous system metastases. Semin Oncol 1977;4:81-91.
414. Pickren JW, Lopez G, Tsukada Y, et al. Brain metastases: an autopsy study. Cancer Treatment Symposia 1983;2:295-313.
415. Gaspar L, Scott C, Rotman M, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group brain metastases trials. Int J Radiat Oncol Biol Phys 1997;37:745-751.
416. Swift PS, Phillips T, Martz K, et al. CT characteristics of patients with brain metastases treated in Radiation Therapy Oncology Group study 79-16. Int J Radiat Oncol Biol Phys 1993;25: 209-214.
417. Smalley SR, Laws ER Jr, O’Fallon JR, et al. Resection for solitary brain metastasis: role of adjuvant radiation and prognostic vari-ables in 229 patients. J Neurosurg 1992;77:531-540.
417a. Borgelt G, Gelber R, Kramer S, et al. The palliation of brain metastases: final results of the first two studies by the Radia-tion theraphy Oncology Group. Int J Radiat Oncol Biol Phys. 1980;6:11-9.
418. Shaw EG. Radiotherapeutic management of multiple brain me-tastases: “3000 in 10” whole brain radiation is no longer a “no brainer.” Int J Radiat Oncol Biol Phys 1999;45:253-254.
419. Auchter RM, Lamond JP, Alexander E III, et al. A multi- institutional outcome and prognostic factor analysis of radiosur-gery for resectable single brain metastasis. Int J Radiat Oncol Biol Phys 1996;35:27-35.
420. Patchell RA, Tibbs PA, Walsh JW, et al. A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med 1990;322:494-500.
421. Alexander E III, Moriarty TM, Davis RB, et al. Stereotactic radio-surgery for the definitive, noninvasive treatment of brain metas-tases. J Natl Cancer Inst 1995;87:34-40.
422. Flickinger JC, Kondziolka D, Lunsford LD, et al. A multi- institutional experience with stereotactic radiosurgery for resectable single brain metastasis. Int J Radiat Oncol Biol Phys 1994;28:797-802.
423. Smalley SR, Laws ER Jr, O’Fallon JR, et al. Resection for solitary brain metastasis: role of adjuvant radiation and prognostic vari-ables in 229 patients. J Neurosurg 1992;77:531-540.
424. Aoyama H, Shirato H, Tago M, et al. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. JAMA 2006;295:2483-2491.
425. Choi KN, Withers HR, Rotman M. Intracranial metastases from melanoma: clinical features and treatment by accelerated frac-tionation. Cancer 1985;56:1-9.
426. Weltman E, Salvajoli JV, Brandt RA, et al. Radiosurgery for brain metastases: a score index for predicting prognosis. Int J Radiat Oncol Biol Phys 2000;46:1155-1161.
427. Mork SJ, Loken AC. Ependymoma: a follow-up study of 101 cases. Cancer 1977;40:907-915.
428. McCormick PC, Torres R, Post KD, et al. Intramedullary epend-ymoma of the spinal cord. J Neurosurg 1990;72:523-532.
429. Reimer R, Onofrio BM. Astrocytomas of the spinal cord in chil-dren and adolescents. J Neurosurg 1985;63:669-675.
430. Kopelson G, Linggood RM, Leinman GM, et al. Management of intramedullary spinal cord tumors. Radiology 1980;135: 473-479.
431. Chun HC, Schmidt-Ullrich RK, Wolfson A, et al. External beam radiotherapy for primary spinal cord tumors. J Neurooncol 1990;9:211-217.
432. Guidetti B, Mercuri S, Vagnozzi R. Long-term results of the sur-gical treatment of 129 intramedullary spinal gliomas. J Neuro-surg 1981;54:323-330.
433. Cooper PR, Epstein F. Radical resection of intramedullary spinal cord tumors in adults: recent experience in 29 patients. J Neuro-surg 1985;63:492-499.
434. Epstein J. Spinal cord astrocytomas of childhood. Prog Exp Tumor Res 1987;30:135-153.
435. Epstein FJ, Farmer J-P., Freed D. Adult intramedullary astrocyto-mas of the spinal cord. J Neurosurg 1992;77:355-359.
436. Epstein F, McCleary EL. Intrinsic brain-stem tumors of child-hood: surgical indications. J Neurosurg 1986;64:11-15.
437. Epstein F. Intraaxial tumors of the cervicomedullary junction in children. Concepts Pediatr Neurosurg 1987;7:117.
438. Kopelson G, Linggood RM, Kleinman GM, et al. Management of intramedullary spinal cord tumors. Radiology 1980;135: 473-479.
439. O’Sullivan C, Jenkin RD, Doherty MA, et al. Spinal cord tumors in children: long-term results of combined surgical and radiation treatment. J Neurosurg 1994;81:507-512.
440. Kopelson G. Radiation tolerance of the spinal cord previously damaged by tumor and operation: long term neurological improvement and time-dose-volume relationships after irradia-tion of intraspinal gliomas. Int J Radiat Oncol Biol Phys 1982;8: 925-929.
441. Shaw EG, Evans RG, Scheithauer BW, et al. Radiotherapeutic management of adult intraspinal ependymomas. Int J Radiat Oncol Biol Phys 1986;12:323-327.
442. Garcia DM. Primary spinal cord tumors treated with surgery and postoperative irradiation. Int J Radiat Oncol Biol Phys 1985;11:1933-1939.
443. Bryne TN. Spinal cord compression from epidural metastases. N Engl J Med 1992;327:614-619.
444. Rodichok LD, Harper GR, Ruckdeschel JC, et al. Early diagnosis of spinal epidural metastases. Am J Med 1981;70:1181-1188.
445. Young RF, Post EM, King GA. Treatment of spinal epidural metastases. J Neurosurg 1980;53:741-748.
446. Sorensen PS, Borgesen SE, Rohde K, et al. Metastatic epidural spinal cord compression: results of treatment and survival. Can-cer 1990;65:1502-1508.
447. Latini P, Maranzano E, Ricci S, et al. Role of radiotherapy in metastatic spinal cord compression: preliminary results from a prospective trial. Radiother Oncol 1989;15:227-233.

33 The Brain and Spinal Cord 871
448. Sundaresan N, Galicich JH, Lane JM, et al. Treatment of neo-plastic epidural cord compression by vertebral body resection and stabilization. J Neurosurg 1985;63:676-684.
449. Siegal T, Seigal T. Surgical decompression of anterior and pos-terior malignant epidural tumors compressing the spinal cord: a prospective study. Neurosurgery 1985;17:424-432.
450. Herbert SH, Solin LJ, Rate WR, et al. The effect of palliative radiation therapy on epidural compression due to metastatic malignant melanoma. Cancer 1991;67:2472-2476.
451. Olsen ME, Chernik NL, Posner JB. Infiltration of the leptome-ninges by systemic cancer. Arch Neurol 1974;30:122-137.