
IUBS REPRODUCTIVE BIOLOGY IN - Current Issue | Biology International

chapter 3
Principles of ReproductiveBiology and Development

CONTENTS
PageIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Measurement of Reproductive Function: Relation to Workplace Hazards . . . . . . . . . . . . . . 44
Normal Reproductive Biology and Development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Hormonal Control Mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44Male Reproductive Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46Female Reproductive Function . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48Embryogenesis and Fetal Growth . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49The Pregnant Woman . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49Coping with Pregnancy Loss. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52Lactation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53Sexual Development: Puberty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
Abnormal Development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54Historical Perspective. . . . ., . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54Terminology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55Mutagens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56Impaired Embryogenesis and Fetal Growth . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Mechanisms of Action of Reproductive and Developmental Toxicants . . . . . . . . . . . . . . . . 57
Reproductive Dysfunction in the Population as a while . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
Summary and Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
Chapter 3 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
List of TablesTable No. Page3-1.Measures of Reproductive Function Readily Obtainable Prior to Fertilization. . . . . . . 4S3-2. Measures of Reproductive Function Readily Obtainable After Fertilization . . . . . . . . . 453-3. Stages of Embryonic and Fetal Development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 513-4. Principles of Teratogenesis and Timing of Embryonic and Fetal Toxicity . . . . . . . . . . 57
List of FiguresFigure Ale. Page3-1.The Male Reproductive System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 473-2. Relation Between Oocyte Number and Age in Women.... . . . . . . . . . . . . . . . . . . . . . . 483-3,The Female Reproductive System . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . so3-4.Relation Between Age, Oocyte Number, and Menopause . . . . . . . . . . . . . . . . . . . . . . . . 513-5. Embryogenesis and Fetal Growth: Three Trimesters of Gestation . . . ., .. ...,., . . . 523-6. The Percentage of Normal Women Who Conceive per Menstrual Cycle
and the Outcome of the Pregnancies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . , . . . . . S33-7. Percentage of Surviving and Lost Human Embryos and Fetuses at Different
Stages of Pregnancy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 543-8.Mechanisms of Action of Reproductive Toxins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58

Chapter 3
Principles of ReproductiveBiology and Development
INTRODUCTION
Normal reproductive function comes about onlyas a consequence of interactions among multiplephysiological systems. In the narrowest sense, re-production is the union of sperm and ovum toform a new biological entity. Yet the union of ga-metes is merely a signal event in the continuumof physiological processes comprising normal re-productive function, Prior to fertilization, for ex-ample, the maturation of sperm and egg dependson the coordinated secretion of multiple hor-mones. At coitus, synchronized neural reflexesand appropriate reproductive behaviors are re-quired to bring gametes together. After concep-tion, embryonic growth depends on the integrityof the zygote and a remodeling of the maternalcirculatory system. The later growth and devel-opment of the offspring are a function of bothprenatal and postnatal nutrition.
For purposes of this report, reproductivefunction is used in the broadest sense possible.It encompasses:
●
●
●
●
●
●
●
●
●
the functional and structural integrity of thesperm and ova;differentiation and development of the inter-nal and external reproductive organs and en-docrine glands;activation of the adult reproductive systemat puberty;senescence of the adult reproductive system(e.g., menopause);behaviors associated with or subserving re-production (e.g., libido);maternal and paternal prenatal events;embryonic and fetal events (e.g., organo-genesis);maternal postnatal events (e.g., lactation); andchild health and development.
The significance of some aspects of reproduc-tive function not overtly related to fertility is oftenunderestimated; because they are held to bestrictly private matters, many of these subjectstend to go undiscussed. In fact, an individual’s re-productive function and, should it occur, repro-ductive dysfunction, can be of extraordinary per-sonal importance. Impotence, menstrual pain, andloss of libido exemplify instances of reproductivedysfunction that can have substantial impact onindividual well-being and human relationships.
Concern about reproductive processes is notlimited to the brief periods in an individual’s life-time during which reproduction may actually oc-cur. Reproductive function is an integral part ofeveryday human health and well-being. Before,during, and after the childbearing years, repro-ductive hormones may act, for example, on suchvariables as resistance to heart disease and can-cer, immune function, complexion, bone mineralcontent, and feeling and mood. Threats to repro-ductive function can take place at nearly any pointduring an individual’s lifespan. In fact, the mostinsidious hazards to reproductive function maybe those whose immediate effects are apparentlybenign, but whose ill effects surface at a laterdate.
Viewed from this perspective, the bounds oftypical reproductive function and the task ofdefining atypical reproductive function seem im-possibly broad in scope. Yet, by using an arrayof well-defined endpoints, it is possible to assesshuman reproductive function in both a qualita-tive and a quantitative manner.
43

44 . Reproductive Health Hazards in the Workplace
MEASUREMENT OF REPRODUCTIVE FUNCTION:RELATION TO WORKPLACE HAZARDS
For the couple desiring to reproduce, it may beargued that the only meaningful index of repro-ductive function is the ability to produce a healthybaby when they wish to do so. At any given time,the couple either can, or cannot, procreate. But,for the purposes of this report, this final commondenominator of successful procreation must bedissected into numerous constituent factors in or-der to: 1) examine the nature of reproductivefunction and dysfunction, and 2) relate reproduc-tive dysfunction to a potential workplace hazard.Multiple endpoints of reproductive function fur-ther serve to define the reproductive status andphysiological well-being of the majority of the pop-ulation who are, at any given time, not pro-creating,
Endpoints used for measuring reproductivefunction may be divided into two groups: 1) thoseserving as indices of reproductive function inde-pendent of fertilization, and 2) those serving assuch indices after fertilization. There are closeparallels between male and female reproductiveprocesses up to the point at which sperm and eggmature. Thereafter, most of the reproductiveprocesses related to procreation occur in the fe-male, as the fetal-placental-maternal system ex-hibits many stages without counterpart in themale.
Table 3-1 lists measures by which reproductivefunction may be assessed in adult men and wom-en. The measures listed are limited to those thatare readily observable in a relatively noninvasivefashion. In order to have broad applicability ina workplace or outpatient setting, such measuresare obtainable by one or more of the followingmeans:
● a detailed patient history,● a physical examination,● blood samples,● semen samples l o r. urine samples.
Table 3-1 illustrates the disparity between theease with which male and female reproductiveparameters can be assessed. That is, sperm arereadily accessible, while eggs are not Table 3-2lists measures by which reproductive functionmay be assessed in the adult woman and her off-spring during pregnancy and after birth. Again,the measures listed are limited to those readilyobtainable in the relatively noninvasive fashionjust described. A comprehensive discussion of themethods used to assess reproductive function, in-cluding more sophisticated methods than thoselisted in these tables, appears in chapter 5.
NORMAL REPRODUCTIVE BIOLOGY AND DEVELOPMENT
Hormonal Control Mechanisms
In both men and women, the hypothalamus, anarea at the base of the brain, serves as a funda-mental neural regulator of the body’s reproduc-tive function. It receives neural and hormonal in-put from the brain and endocrine glands and re-sponds to these stimuli by secreting luteinizinghormone-releasing hormone (LHRH) and otherhormones. The hypothalamus releases LHRH intotiny blood vessels which surround the pituitarygland, With a target so nearby, LHRH is releasedin minute amounts and breaks down quickly. As
a consequence, this vital reproductive hormone—a telling indicator of reproductive function—ispossible but difficult to detect in peripheral bloodcirculation.
LHRH acts on cells of the anterior pituitarygland to promote secretion of two hormones, lu -teinizing hormone (LH) and follicle-stimulatinghormone (FSH). LH and FSH, known as gonado-tropin, direct hormone and gamete productionby the testes and ovaries. As the gonads releasehormones in response to stimulation by LH andFSH, these gonadal hormones act at the hypothal-

Ch. 3—Principles of Reproductive Biology and Development ● 4 5
Table 3-1.—Measures of Reproductive Function Readily ObtainablePrior to Fertilization
Affected individual
Endpoint Male (Both) Female
Sexual function: Erection LibidoEjaculation Behavior
Endocrine system: Luteinizing hormone Cervical mucusFollicle-stimulating quality
hormoneSteroid hormones
(androgens,estrogens, andprogestins)
Germ cells: Sperm numberSperm motilitySperm shape
(morphology)Chromosomal
integrityFertilizing ability
Fecundity: Testicular integrity Integrity of external Ovarian integritySemen quality genitalia Blockage of oviduct
Menstrual regularityAmenorrheaAnovulatory cycles
Secondary sexual Breast developmentcharacteristics: Facial and axillary hair
growthSebaceous glands
Reproductive lifespan: Age at puberty Age at menopauseSOURCE: Office of Technology Assessment.
Table 3.2.—Measures of Reproductive Function Readily Obtainable After Fertilization
Affected individual
Endpoint Female (Both) Offspring
Endocrine system: Human chorionicgonadotropin
Steroid hormones,especiallyprogesterone
Health duringpregnancy: Hemorrhage Fetal death Morphology
Toxemia Spontaneous Chromosomalabortion aberrations
Perinatal period: Premature birth DeathPostmature birth: Chromosomal
aberrationsBirth defectsBirth weightApgar score
Postnatal period: Lactation Infant deathChildhood morbidityChildhood
malignanciesDevelopmentBehavior
Reproductive lifespan: Age at menopause Age at pubertySOURCE: Office of Technology Assessment.

—-
46 . Reproductive Health Hazards in the Workplace
amus and pituitary gland to reduce the secretionof LH and FSH. In this way, a feedback loop oper-ates, involving the hypothalamus, pituitary gland,and gonads. A defect at any point in the hypo-thalamic-pituitary -gonadal axis or in the metabo-lism of their modulator hormones will interruptthe normal pattern of reciprocal hormone secre-tion among these organs.
The moment-to-moment secretion of LH andFSH is best described as episodic, or pulsatile, witha frequency of 1 to 2 hours under normal condi-tions. The pattern of episodic gonadotropin secre-tion represents endocrine signaling from thehypothalamic-pituitary unit to the gonads, thusdirecting normal ovarian and testicular activity(6,14,58). In addition, larger alterations in the pat-tern of gonadotropin pulses are correlated withdramatic changes in reproductive function, as inthe peripubertal period, at menopause, and in cer-tain pathological conditions. The pattern of hor-mone secretion is difficult to detect when the plas-ma concentration of gonadotropins is low, as inprepubertal individuals.
Normal, premenopausal, adult women (but notmen) exhibit a second cyclic mode of hormonesecretion. This cyclic secretion is marked by aperiodic, synchronous burst of LH and FSH re-lease, known as the preovulatory LH surge. Es-trogens secreted by the cells in the ovaries actupon the brain to trigger the preovulatory surge.Thus, coordination of both neural and ovarian sig-nals is required for normal ovulation to occur.
In order to map the pattern of LH and FSH se-cretion—and thus judge hypothalamic-pituitaryfunction-it is necessary to draw serial blood sam-ples at frequent intervals. A single blood sam-ple yields no information about the pattern ofgonadotropin secretion, although it can sometimes identify gross abnormalities in hormonel e v e l s
The episodic nature of LH and FSH secretionis a consequence of episodic release of LHRH fromthe hypothalamus. In this way, intrinsic proper-ties of the central nervous system mediate gonad-otropin secretion and, ultimately, gonadal func-tion. It is through the central nervous system thatpsychological, emotional, sensory, and environ-
mental stimuli can profoundly influence repro-ductive function.
Male Reproductive Function
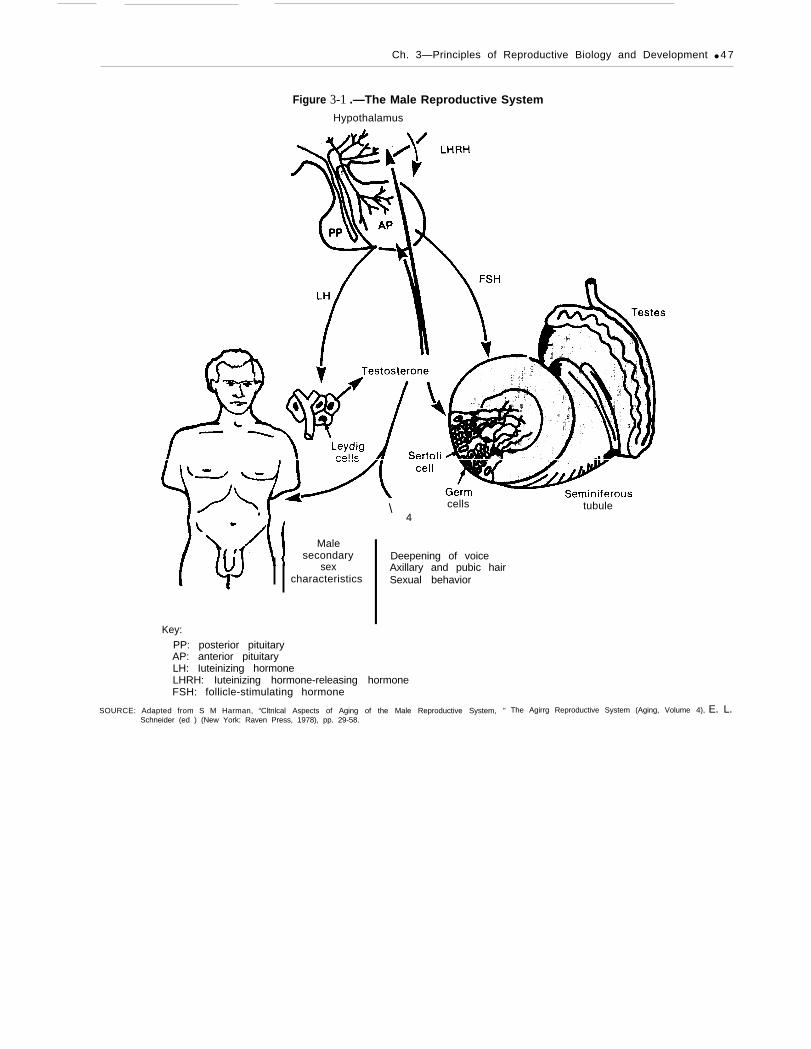
In the male, the testes are the target of the LHand FSH released by the pituitary gland (figure3-l). The testes serve two functions, producingboth gametes (sperm) and hormones, notably tes-tosterone. Sperm develop in the loops of seminif-erous tubules within the testes; these tubulesmake up the bulk of the testes. Testosterone isproduced by the Leydig cells, which are scatteredthroughout the testes and lie outside the semi-niferous tubules. Damage to the sperm-producingtubules does not necessarily affect testosteroneproduction by the Leydig cells. However, a defi-cit in testosterone production by the Leydig cellsis likely to be accompanied by impaired spermproduction because of feedback to the pituitaryand hypothalamus.
Sperm are produced continuously in the testesbeginning at puberty and continuing throughoutlife. A decline in sperm production may occur asmen age, becoming apparent in the sixth decadeand beyond (22,41). Such an age-related declinein sperm production is not observed in all studypopulations (44), and the response of the testesto aging is variable (41).
Sperm production begins with division of spermprecursor cells, the spermatogonia, within theseminiferous tubules. Spermatogonia are gener-ally thought of as falling into two broad catego-ries—those in a self-renewing pool and those ina proliferating pool of cells. Most spermatogoniaare in the latter. These spermatogonia divide toproduce two daughter cells that are destined tobecome spermatozoa. A few more spermatogoniaexist in a pool of cells that renew themselves.These spermatogonia produce two daughter cellsthat can either remain in the population or com-mit to the proliferating pool of cells.
When spermatogonia are damaged or killed bya toxic agent (e.g., ionizing radiation) reproduc-tive function in the male maybe greatly impaired.There is some evidence that a third type of sper-matogonium that rarely divides under normal cir-
Ch. 3—Principles of Reproductive Biology and Development ● 4 7
Figure 3-1 .—The Male Reproductive System
Hypothalamus
Malesecondary
sexcharacteristics
\ cells4
I Deepening of voiceAxillary and pubic hairSexual behavior
Key:
PP: posterior pituitaryAP: anterior pituitaryLH: Iuteinizing hormoneLHRH: Iuteinizing hormone-releasing hormoneFSH: follicle-stimulating hormone
tubule
SOURCE: Adapted from S M Harman, “Cltnlcal Aspects of Aging of the Male Reproductive System, ” The Agirrg Reproductive System (Aging, Volume 4), E. L.Schneider (ed ) (New York: Raven Press, 1978), pp. 29-58.

48 ● Reproductive Health Hazards in the Workplace
cumstances may begin to actively divide to replen-ish the population of spermatogonial cells, andin this way, the testes may regain sperm-produci-ng capacity. Although it may be temporary, in-terruption of fertility can have lifelong conse-quences in that timing of procreation can becrucial. The gonad itself may be the target of toxicagents (e.g., DBCP). In such cases, depending uponthe extent of exposure, gonadal damage can beirreversible.
The final stages of sperm maturation take placeduring passage of the sperm from the testesthrough the long, coiled epididymis. Maturationinvolves changes in motility, metabolism, andmorphology. Sperm then leave the body in thesemen, a fluid comprised of secretions of the semi-nal vesicles, prostate, and glands adjacent to theurethra. Ejaculation is a two-part spinal reflex thatinvolves: 1) emission, the movement of the semeninto the urethra; and 2) ejaculation proper, thepropulsion of the semen out of the urethra at thetime of orgasm.
The process of forming sperm from primitivestem cells in the seminiferous tubules consumesan estimated 64 to 74 days; the sperm take an ad-ditional 9 to 12 days to pass through the epidi-dymis. For this reason, changes in the sperm-pro-ducing activities of seminiferous tubules are gen-erally not immediately reflected in ejaculatedsemen.
Testosterone has a number of actions. It dif-fuses into the seminiferous tubules to promotesperm development. Testosterone is also secretedinto the general circulation, where it acts at thehypothalamic-pituitary unit to modulate the re-lease of LH. (FSH release by the pituitary glandis modulated by a protein factor called inhibin,which is secreted from the seminiferous tubules.)Testosterone acts to promote growth and devel-opment of male sexual organs, causing an increasein size of the penis, prostate, Cowper’s gland, andseminal vesicles, and promoting secretory activi-ty of the latter three glands. Male secondary sexcharacteristics (e.g., increased muscle mass, beardgrowth, deep voice, and underarm and pubic hair)are all developed and maintained by testosterone.Sex drive in men increases in puberty as testoster-one rises, usually decreases in the event of cas-
tration, and is restored by exogenous testoster-one in ‘men with dysfunctional testes.
Female Reproductive Function
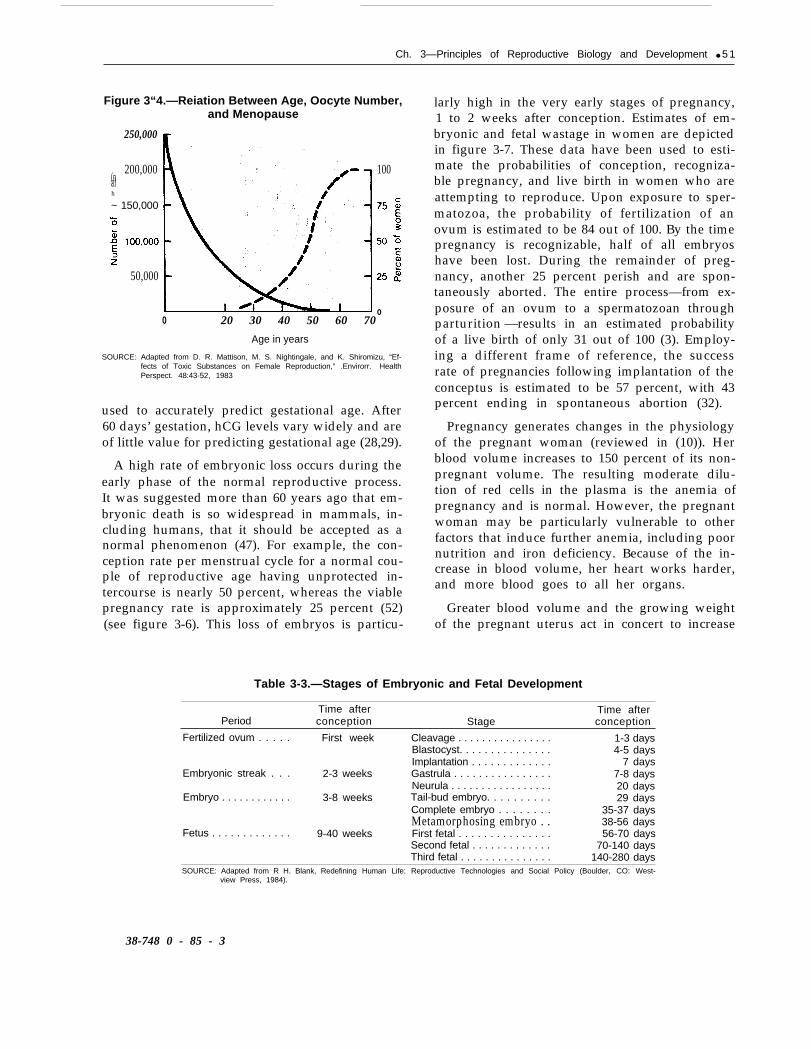
In the female, the target organs of LH and FSHare the ovaries. Within each ovary are primitivegerm cells, called oocytes. The number of oocytesin the ovaries is fixed prenatally and is greatestduring the fetal stage of development, when itreaches several million. After peaking in the sev-enth month of gestation, the number of oocytesdecreases to fewer than 1 million at birth, andcontinues to decline markedly throughout life (fig-ure 3-2). Only about 400 oocytes are actuallyovulated during the period of female fertility.In contrast to the continuing renewal of germcells throughout an adult male’s life, no newoocytes are formed after the fetal stage in thefemale.
The female menstrual cycle averages 28 to 29days, but may range from 21 to 50 days (13). Eachmonth, LH and FSH stimulate growth of a selectedgroup of ovarian follicles–small spheres of cellsthat surround a developing egg. Concomitant withthe growth in size and number of follicular cellsis the production of estrogenic hormones by theseovarian cells. Estrogens are responsible for thethickening of the uterine lining, or endometrium.Estrogens also stimulate and maintain secondarysex characteristics (e.g., growth of breasts, devel-opment of a flared pelvis, and distribution of body
Figure 3.2.-Relation Between Oocyte Number
2 2 4 6 8“ 10 20 30 40 50 60 70Birth
Months YearsSOURCE: Adapted from D. R. Mattison, M. S. Nightingale, and K. Shiromizu, “Ef-
fects of Toxic Substances on Female Reproduction,” Environ, Hea/thPerspect. 48:43-52, 1983.

Ch. 3—Principles of Reproductive Biology and Development ● 4 9
fat to hips and thighs), and induce cyclical alter-ations in cervical mucus.
Follicular growth continues throughout the fol-licular phase of the menstrual cycle. One domi-nant follicle then prevails, while the 20 or moreother follicles at the same stage of developmentbegin to degenerate. At ovulation, the dominantfollicle ruptures in response to a surge of LH andFSH, and the ovum travels down the oviduct tothe uterus. Fertilization of the ovum by a spermusually takes place in the oviduct, within 24 to36 hours after ovulation. The follicular cells ofthe dominant follicle remaining in the ovary forma temporary endocrine organ called the corpusIuteum.
During the second half of the menstrual cycle,the luteal phase, the corpus luteum produces highlevels of progesterone in addition to estrogens.These hormonal changes prepare the uterus fora possible pregnancy. If a fertilized egg does notreach the uterus and begin to implant, the corpusIuteum regresses, the uterine lining is discharged,and menstruation occurs. (Figure 3-3 summarizesthe female reproductive cycle.) The luteal phaseusually consumes about 14 days. Variability in thelength of the overall menstrual cycle, from 21 to50 days, typically results from varying durationof the follicular phase, rarely from variations inthe luteal phase, although shortening of the lu-teal phase may profoundly affect the ability tosupport implantation of the fertilized egg (seechapter 5).
Menopause, the cessation of menstrual cyclic-ity, occurs when the ovary is virtually depletedof oocytes, and is marked by diminished produc-tion of ovarian estrogens, bursts of LHRH release,sudden body-temperature fluctuations, and otherchanges of a longer term. It occurs, on average,at about age 50 (figure 3-4). The destruction ofoocytes at any time from the fetal period throughadulthood may lead to premature ovarian failure,and premature menopause. As oocytes age, thechances of developmental abnormalities in off-spring increase.
Embryogenesis and Fetal Growth
If fertilization of the ovum occurs (24 to 36hours after ovulation), cell division is initiated and
continues during the next 3 to 4 days as the earlyembryo, called a blastocyst, passes down theoviduct. The blastocyst implants in the lining ofthe uterus 6 to 7 days after ovulation. During thesecond and third weeks following conception,extraembryonic membranes are laid down andthe development of the three layers of cells (endo-derm, mesoderm, and ectoderm) occurs. Thus,by the time the first menstrual period is missed,the embryo is in the primitive “streak” stage,
The embryonic period takes place betweenweeks 3 and 8 to 9 of pregnancy I This is a criti-cal phase of development, during which cell dif-ferentiation proceeds at an accelerated pace. Dur-ing this period, the brain, eyes, heart, upper andlower limbs, and other organs are formed.
The fetal period is considered to have begunafter the major organs have developed. It extendsfrom approximately 8 or 9 weeks of gestationalage until birth. This period is both a time of fetalgrowth and continued biochemical and physio-logical maturation of tissues and organs. Early inthe fetal period, during weeks 9 to 11, the exter-nal genitalia differentiate, The growth and devel-opment of the nervous system occurs largely inthe later fetal stages, during the second and thirdtrimesters of pregnancy. It is important to notethat the growth of nerve cells, or neurons, andthe formation of connections between neurons,called synapses, continue in humans even afterbirth. Table 3-3 summarizes the timing of embry -onic and fetal development, and figure 3-5 placesthe periods of embryogenesis, organ-system de-velopment, and fetal growth in the perspectiveof a full-term pregnancy.
The Pregnant Woman
If a fertilized egg reaches the uterus and be-gins to implant, the nascent placenta produces thehormone hCG, human chorionic gonadotropin.This hormone signals the corpus luteum to con-tinue producing progesterone and estrogens inorder to maintain the uterine endometrial lining.
‘References to time during pregnanqy are often made in two ways.If the time from conception, or time of gestation, is enumerated(as in this text), a full term pregnancy spans about 38 weeks. If preg-nancy is timed from the last menstrual period, about 2 weeks areadded, making a term pregnancv equal to about 40 weeks.

—
50 ● Reproductive Health Hazards in the Workplace
Figure 3-3.—The Female Reproductive System
Breast developmentAxillary and pubic hairSexual behavior
Key:LH: Iuteinizing hormoneFSH: follicle-stimulating hormoneLHRH: Iuteinizing horm~ne-releasing hormone
SOURCE: Adapted from E. K. Sllbergeld and D. Mattison, personal communication, 19S4.
Secretion of hCG is the earliest biochemicalchange indicative of pregnancy. Chorionic gonad-otropin has been detected in plasma and urineas early as 6 to 9 days after conception; that is,very soon after implantation of the primitive em-bryo into the uterine endometrium, Under invitro conditions, hCG secretion has been detectedat 7 days after fertilization, in the absence of im-plantation (15), suggesting that hCG release by thedeveloping embryo occurs even prior to implan-tation. In a spectacular demonstration of the diag-
nostic value of hCG measurement, doubly ele-vated hCG levels in blood have been used todiagnose the occurrence of twins, just 2 to 3weeks after conception (23).
During the first 60 days of gestation, the secre-tion of hCG doubles approximately every 2 days(5). This leads to an exponential rise in maternalplasma hCG concentration with very little indi-vidual variation. Maternal plasma hCG levels dur-ing the first 60 days of pregnancy can thus be
Ch. 3—Principles of Reproductive Biology and Development ● 5 1
Figure 3“4.—Reiation Between Age, Oocyte Number,and Menopause
250,000
200,000(nalh
~ 150,000
50,000
0 20 30 40 50 60 70
Age in years
100
o
SOURCE: Adapted from D. R. Mattison, M. S. Nightingale, and K. Shiromizu, “Ef-fects of Toxic Substances on Female Reproduction,” .Envirorr. HealthPerspect. 48:43-52, 1983
used to accurately predict gestational age. After60 days’ gestation, hCG levels vary widely and areof little value for predicting gestational age (28,29).
A high rate of embryonic loss occurs during theearly phase of the normal reproductive process.It was suggested more than 60 years ago that em-bryonic death is so widespread in mammals, in-cluding humans, that it should be accepted as anormal phenomenon (47). For example, the con-ception rate per menstrual cycle for a normal cou-ple of reproductive age having unprotected in-tercourse is nearly 50 percent, whereas the viablepregnancy rate is approximately 25 percent (52)(see figure 3-6). This loss of embryos is particu-
larly high in the very early stages of pregnancy,1 to 2 weeks after conception. Estimates of em-bryonic and fetal wastage in women are depictedin figure 3-7. These data have been used to esti-mate the probabilities of conception, recogniza-ble pregnancy, and live birth in women who areattempting to reproduce. Upon exposure to sper-matozoa, the probability of fertilization of anovum is estimated to be 84 out of 100. By the timepregnancy is recognizable, half of all embryoshave been lost. During the remainder of preg-nancy, another 25 percent perish and are spon-taneously aborted. The entire process—from ex-posure of an ovum to a spermatozoan throughparturition —results in an estimated probabilityof a live birth of only 31 out of 100 (3). Employ-ing a different frame of reference, the successrate of pregnancies following implantation of theconceptus is estimated to be 57 percent, with 43percent ending in spontaneous abortion (32).
Pregnancy generates changes in the physiologyof the pregnant woman (reviewed in (10)). Herblood volume increases to 150 percent of its non-pregnant volume. The resulting moderate dilu-tion of red cells in the plasma is the anemia ofpregnancy and is normal. However, the pregnantwoman may be particularly vulnerable to otherfactors that induce further anemia, including poornutrition and iron deficiency. Because of the in-crease in blood volume, her heart works harder,and more blood goes to all her organs.
Greater blood volume and the growing weightof the pregnant uterus act in concert to increase
Table 3-3.—Stages of Embryonic and Fetal Development
Time after Time afterPeriod conception Stage conception
Fertilized ovum . . . . . First week Cleavage . . . . . . . . . . . . . . . . 1-3 daysBlastocyst. . . . . . . . . . . . . . . 4-5 daysImplantation . . . . . . . . . . . . . 7 days
Embryonic streak . . . 2-3 weeks Gastrula . . . . . . . . . . . . . . . . 7-8 daysNeurula . . . . . . . . . . . . . . . . . 20 days
Embryo . . . . . . . . . . . . 3-8 weeks Tail-bud embryo. . . . . . . . . . 29 daysComplete embryo . . . . . . . . 35-37 daysMetamorphosing embryo . . 38-56 days
Fetus . . . . . . . . . . . . . 9-40 weeks First fetal . . . . . . . . . . . . . . . 56-70 daysSecond fetal . . . . . . . . . . . . . 70-140 daysThird fetal . . . . . . . . . . . . . . . 140-280 days
SOURCE: Adapted from R H. Blank, Redefining Human Life: Reproductive Technologies and Social Policy (Boulder, CO: West-view Press, 1984).
38-748 0 - 85 - 3
52 ● Reproductive Health Hazards in the Workplace
pressure on the leg veins during pregnancy. Sit-ting or standing in one position may become un-comfortable, and the risk of developing varicoseveins in the legs is increased. The weight of theenlarging uterus also increases strain on the lowerback. The pregnant woman’s kidneys serve to filter wastes from both her blood and that of thefetus. The increased blood flow to the kidneysand pressure on the bladder can cause the preg-nant woman to urinate more frequently, particu-larly as pregnancy progresses.
Coping With Pregnancy LOSS
Embryonic or fetal loss causes maternal and pa-ternal grief reactions. The grief pattern seen par-allels that which has been described in facingdeath in adulthood (25), namely:
● shock,● disorganization,● volatile emotions,● guilt,● loss,

Ch. 3—Principles of Reproductive Biology and Development ● 5 3
Figure 3-6.—The Percentage of Normal Women WhoConceive per Menstrual Cycle and the Outcome of.
1 000/0
lmplantat ion>
These Pregnancies
ally supportive counseling sessions are consideredan essential part of care for couples who experi-ence a pregnancy loss (30).. -
1 k
Notpregnant
(55%0)
Pregnant(45”/0)
aln ~ome pregnancies clinical diagnosis is not made but the woman does have
a transient increase in serum human chorionic gonadotropin (hCG) levels
SOURCE Adapted from M. R Soules, “The In Vitro Fertilization Pregnancy Rate:Let’s Be Honest With One Another, ” fertility& Sterility43(4)’511 -513,1985
● relief, and. reestablishment of an emotional balance.
A 1984 study found that the strongest stage ofgrief in pregnancy loss was guih. This stage tookthe longest time to begin to resolve, and was theone in which the couples needed the most sup-port and assistance. Women stated that if onlythey had not jogged, or had sexual intercourse,or fallen, or if they had eaten better, the sponta-neous abortion might not have happened. Othershad to deal with previous events that representedhigher risks, such as medical illnesses or heavycigarette smoking (3o).
Although society is sensitive toward the cou-ple who experiences pregnancy loss, there is atendency not to express this sympathy. There are,for example, no accepted rituals for mourning anearly pregnancy loss. Wakes and funerals are un-common for a nonviable fetus. Indepth, emotion-
Lactation
The breast is a complex organ that both syn-thesizes and excretes. When feeding a growinginfant, the mother typically produces a liter ofmilk per day, containing protein, fat, carbohy-drate, minerals, vitamins, hormones, and antibod-ies. All nutrient components are fully digestible.The product is delivered sterile, on demand, andwith the carbohydrate and protein suspended ina mineral/aqueous system. The fat is excreted asa milk-fat globule, Because breast milk is a mix-ture of both water and fat, it can serve as a vehi-cle for a wide variety of substances present inmaternal tissue or blood. Many constituents pres-ent in maternal blood plasma may be present inbreast milk. Chemical or drug excretion intobreast milk may be accomplished by binding tomilk protein or to the surface of milk fat glob-ules. It is also possible that fat-soluble chemicals(e.g., DDT, PCB, most insecticides) maybe trappedentirely within the milk-fat globule (2,19,61).
Sexual Development: puberty
Puberty is the period of transition between thejuvenile state and adulthood. During this stage ofdevelopment, secondary sex characteristics ap-pear and mature, the adolescent growth spurt oc-curs, profound psychologic effects are observed,and fertility is achieved. These changes are in parta consequence of maturation of the hypothalamic-pituitary-gonadotropin unit, stimulation of the sexorgans, and secretion of sex steroid hormones(17). A complex biological and maturational event,puberty actually spans several years, and is notwell understood in terms of its onset.
Most American girls (98.8 percent) enter pu-berty between age 8 and age 13, with a mean ageof 11 years (43). They complete their secondarysexual development in an average of 4.2 years,with a range of 1.5 to 6 years (32). Menarche (thefirst menstrual period) occurs fairly late in thematurational process and is the salient event forthe pubertal girl. The first menstrual period ap-pears at an average age of 12.8 years (56).

54 ● Reproductive Health Hazards in the Workplace
Figure 3-7.—Percentage of Surviving and Lost Human Embryos and Fetuses at Different Stagesof Pregnancy
0 1 2 6 10 14 18 22 26 30 34 38 B
Weeks after ovulation
Some sign of puberty is first shown by 98.8 per- complete secondary sexual development in ancent of normal American boys between 9 and 14 average of 3.5 years, with a range of 2 to 4.5 yearsyears, with a mean age of 11.6 years (43). Boys (33).
ABNORMAL DEVELOPMENT
Historical Perspective by the pharmaceutical industry, using animal
Since the 1950S) tests of the effects of selectedmodels. The prospective sires and dams are usu-ally exposed to the test chemical by diet, and
chemicals on reproduction have been conducted measurements are made of reproductive end-
This section reviews abnormal development of the embryo/fetus; points (e.g., pregnancy rate; successful parturi-a discussion of abnormal reproductive function from puberty tion; number, viability, and growth rate of off-through adulthood appears in ch. 5. spring).

Ch, 3—Principles of Reproductive Biology and Development ● 5 5
As a consequence of the thalidomide tragedyin the early 1960s (see chapter 2), intensive ef-forts were mounted to detect substances capa-ble of producing structural abnormalities in de-veloping fetuses. The ability to detect skeletal andexternal malformations was emphasized, becausetechniques were available to detect those typesof effects (60). These efforts were placed in a prac-tical context as awareness grew that nearly allsubstances or agents are capable of adversely af-fecting the conceptus, if the dose is sufficientlygreat (24).
Methodologic advances since the 1960s havepermitted detection of soft-tissue deficits andsome functional deficits. These include alterationsin central nervous system function (7), intestinalfunction (11), and respiratory function (42). Asa result, the concept of teratology has evolved intoa broad concept that includes structural and func-tional aspects of reproductive and developmen-tal capability.
Terminology
The field of developmental toxicology is evolv-ing rapidly, and its vocabulary is consequently ina state of flux. In late 1984, the EnvironmentalProtection Agency (57) summarized the relevantterminology as follows:
●
●
Developmental toxicity is the induction ofadverse effects on development occurring upto the time of puberty. The four principalmanifestations of developmental toxicity are:1) death of the conceptus, 2) structural ab-normality, 3) altered growth, and 4) function-al deficiency.Embryotoxicity and fetotoxicity refer toany toxic effect on the conceptus occurringas a result of prenatal exposure. The distin-guishing feature between the terms is theperiod during which the insult occurs. Theseterms include malformation, altered growth,and in-utero death.—Altered growth is a significant alteration
in fetal or neonatal organ or body weight.A change in body weight may or may notbe accompanied by a change in skeletalmaturation. Altered growth can be inducedat any stage of development, may be rever-sible, or may result in a permanent change.
—Functional teratogenesis refers to aera-tions or delays in the postnatal abilities ofthe individual or organ system, followingexposure to an agent during critical peri-ods of prenatal or postnatal development.
—A malformation is defined as a permanentstructural deviation that is generally incom-patible with or severely detrimental to nor-mal postnatal survival or development.These types of defects are also called tera-togenic effects. A variation is defined asa divergence beyond the usual range ofstructural constitution, but which may nothave as severe an effect as a malformationon survival or health. Distinguishing be-tween malformations and variations is dif-ficult, since there exists a continuum of re-sponses from the normal to the extremedeviant. Other terminology that is oftenused, but no better defined, includesanomaly, deformation, and aberration.
Developmental toxicants thus induce functionalteratogenesis, structural malformations, alteredgrowth, or variations. Toxicants can act duringeither the embryonic or fetal periods, and can killthe embryo or fetus. Developmental toxicantsmay be equally toxic to both the parents and theembryo/fetus. If exposure occurs at, or sufficient-ly near to, the adult toxic dose, both the embryo/fetus and pregnant woman are likely to be harmed’(21,27),
A teratogen can be defined in several ways. Asindicated, the EPA defines teratogenic effects asfunctional alterations or delays in postnatal abil-ities and structural malformations that are gen-erally incompatible with or severely detrimentalto normal postnatal survival or development. Ateratogen can also be defined as a substance thatadversely affects the embryo at doses below thosenecessary to produce overt signs of toxicity in thepregnant woman (53). Yet another definitionstates that a teratogen is an agent that producesa malformation at any dose (2 I).
Thalidomide remains the premier, but not sole,example of a chemical—a pharmacologic in this
%ome substances may be equally toxic to woman and embryo.If exposure occurs at, or sufficiently near to, the adult toxic dose,both the embryo and woman will be affected. The woman may re-cover, but the embryo can be irrevocably damaged (19).

56 ● Reproductive Health Hazards in the Workplace
instance—uniquely hazardous to the developingembryo. It has a marked selectivity for a particu-lar target in humans, the limb buds of the con-ceptus. Thalidomide is able to injure the con-ceptus at dose levels so small as to be essentiallyharmless to the pregnant woman. However, mostdevelopmental toxicants can affect the woman aswell.
The evolution of the concept of developmentaltoxicity and teratogenicity over the past 20 yearshas implications for public policy. For example,the Toxic Substances Control Act (TSCA; PublicLaw 94-469), written in 1976, classifies somechemicals as “teratogens)” thereby implying theexclusion of substances that may cause other de-velopmental effects. Section 4(b) of TSCA statesthat testing standards may be prescribed for car-cinogenesis, mutagenesis, and teratogenesis bythe Administrator of the Environmental Protec-tion Agency. Section 4(e) requires the Adminis-trator to develop a list of chemicals for priorityattention. The chemicals listed are those knownor suspected to cause or contribute to cancer,gene mutation, or birth defects. Section 1O(C) re-quires coordination between the Administratorand the Secretary of the Department of Healthand Human Services for research on rapid screen-ing techniques for carcinogenic, mutagenic, andteratogenic effects of chemicals.
The wording of these sections of TSCA is gen-erally consistent with contemporary understand-ing of cancer and mutations. However, insertionof the words “developmental toxicants” wouldclarify the existing statute with regard to contem-porary understanding of the word “teratogen.”
Mutagens
A mutagen is an agent capable of altering thestructure of deoxyribonucleic acid (DNA), the ge-netic material of a cell, The basic process of muta-genesis may be spontaneous or induced by someagent, and may involve the alteration of a singlecell. If the event occurs in a sperm progenitor oregg cell, the cell may die or the mutation may betransmitted to progeny of the affected parent.This kind of mutation, called a germ cell muta-tion, may be expressed, for example, as fetal wast-
age, sterility, structural or functional defect, orinherited disease. If the event occurs in a cellother than a sperm or an egg, the result may becell death or the formation of daughter cells thatproduce altered gene products or tumors. Thistype of mutation is called a somatic cell mutation(46). Mutations in somatic cells imply the existenceof a germ cell genetic hazard if the inducing agentalso reaches the gonads. Mutations may or maynot be harmful either to the affected individualor to the progeny.
Impaired Embryogenesis andFetal Growth
During its earliest phase, prior to implantationand beginning organogenesis, the fertilized ovum(table 3-3) is largely resistant to certain types oftoxicants. That is, toxic insults occurring duringthe preimplantation stages that do not kill the em-bryo usually do not have an adverse outcome.During this early embryonic period—the first 3weeks of pregnancy—the most probable effectsof toxic influences on the embryo are severe dam-age and death, followed by spontaneous abortion(16).
After implantation, the organs develop rapidlyin a complex series of overlapping and interde-pendent events. The embryonic period is the pri-mary, although not the sole, period for the induc-tion of congenital malformations. During embryo-genesis, the rate of cell division and the timeddifferentiation of primordial cells into organ sys-tems confer a period of increased vulnerabilityto toxic effects. This is the period during whichmost structural teratogens act; functional terato-gens may act later on, as well. The expression ofteratogenicity varies with dose and with timingof exposure during gestation (51).
During the fetal stages and extending into earlypostnatal life, major functional and tissue matu-ration occurs. An agent acting during this periodof time can markedly disrupt these processes.Such insults would be expressed not as majorgross anatomical abnormalities, but rather as dec-rements of anticipated function (21). For this rea-son, most damage occurring in fetal stages is likelyto be regarded as a type of functional injury,rather than as the gross malformations or devel-

Ch. 3—Principles of Reproductive Biology and Development ● 5 7
opmental disruptions that may occur during theearlier embryonic period (16).
The major organs are already formed by thebeginning of the fetal stages, after which it is toolate to cause gross morphological abnormalities.For example, after the palatine shelves have al-ready fused with one another to form the palate,cleft palate cannot be induced by any agent. Nev-ertheless, a substantial amount of developmentcontinues after the embryonic stages, and in-uteroexposure of the fetus has been established as ca-pable of producing altered postnatal functionalcapabilities. Such alterations have been producedin numerous organ systems (e.g., central nervoussystem, gastrointestinal tract, and cardiovascularsystem) (21).
Exposure of the developing nervous system totoxic influences may result in enduring behavioraldeficits or abnormalities. Behavioral teratogene-sis may thus be induced during organogenesis,in the later fetal stages of pregnancy, and evenpost-partum. Ingestion of mercury, alcohol, or ad-dicting drugs, for example, can cause behavioraldeficits or abnormalities in later fetal stages.
The exact nature and severity of induced im-pairments to embryogenesis and fetal growth de-pend on such factors as the time of exposure, theseverity of exposure, and the nature of the sub-stance itself (see table 3-4), Although it is gener-
Table 3.4.—Principies of Teratogenesis andTiming of Embryonic and Fetai Toxicity
●
●
●
●
●
●
●
●
Teratogens often adversely affect only a portion of ex-posed individuals; large individual differences in suscep-tibility exist.
Susceptibility to embryotoxins depends on the geneticmakeup of the embryo and the environmental conditionsand lifestyle variables surrounding the parents.
Toxic agents may be devastating to the embryo but harm-less to the parents.
A toxic agent may produce defects at different levels ofbiological organization resulting in biochemical, phys-iological, or behavioral anomalies that may not be ap-parent at birth.
A toxic agent may affect the embryo even when givenprior to conception either to the mother or to the father.
The kind of effect a genetic or environmental toxinproduces depends on the stage of development duringwhich it acts.
The same toxic agent may disrupt the developmentalprogram and produce a congenital malformation at onestage, but merely injure an organ or produce no effectat all at another stage.
The earlier in the formation of a structure a toxic agentacts, the more complete is the damage to that structure.
SOURCE: Adapted from A. S. Goldman, “Critical Periods of Prenatal Toxic in-sults,” Drug and Chemical Risks to the Fetus and Newborn, R. H.Schwartz and S. J. Yaffe (eds.) (New York: Alan R. Llss, Inc., 1980).
ally not possible to examine a defective newbornand determine precisely when, during pregnancy,a malformation occurred, it is often possible todetermine a gestational age beyond which it couldnot have been precipitated (2 I).
MECHANISMS OF ACTION OF REPRODUCTIVE ANDDEVELOPMENTAL TOXICANTS
The mechanisms of reproductive and develop-mental toxicity can be reduced ultimately to someeffect that interrupts the normal functioning ofa cell, tissue, organ, or organism (8), A toxicant,whether a chemical, physical, or biological agent(see chapter 4), acts by interrupting biologicalprocesses, including the transfer of energy andinformation necessary for normal reproductivefunction and development.
the toxin interacts with a critical cell or subcel-lular component, disrupting an event necessaryfor normal reproductive function. If this inter-action goes unrepaired, the toxic effect—alteredreproductive function–will be produced. The tox-ic effect may be highly specific and affect onlya single function of a single cell type. Or it maybe broad and nonspecific, with multiple sites oftoxicity within the organism. Within each target,
Following exposure, for example, to a toxicthis multistep process precedes the occurrenceof reproductive toxicity (34).
chemical, the compound must be distributed tothe target organ ie.g., hypothalamus, pituitary Metabolism of the chemical by the liver or kid-gland, gonad, uterus, epididymis, or liver), where neys, for example, may result in toxicity that isit exerts its toxic effect, Within the target organ, more or less apparent. In some cases, a compound
58 . Reproductive Health Hazards in the Workplace
may be metabolized and cleared from the body,and no adverse effect will occur. In other cases,metabolic products may be more toxic or long-lived than the original toxin.
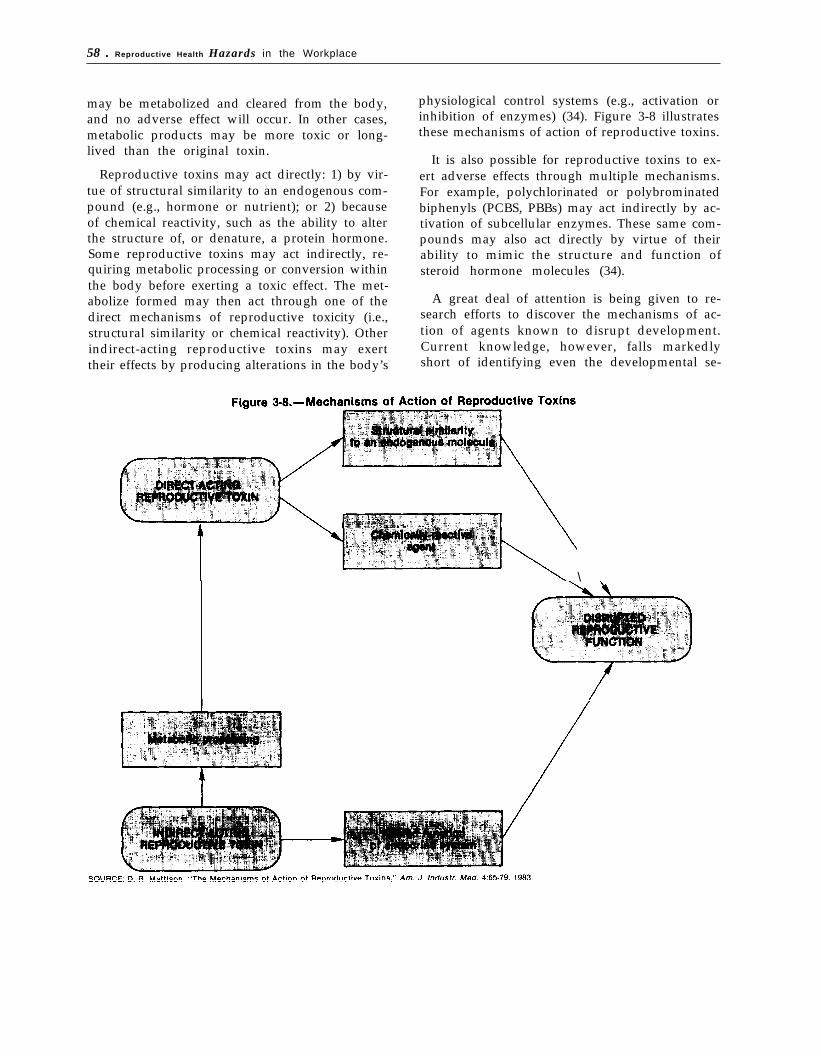
Reproductive toxins may act directly: 1) by vir-tue of structural similarity to an endogenous com-pound (e.g., hormone or nutrient); or 2) becauseof chemical reactivity, such as the ability to alterthe structure of, or denature, a protein hormone.Some reproductive toxins may act indirectly, re-quiring metabolic processing or conversion withinthe body before exerting a toxic effect. The met-abolize formed may then act through one of thedirect mechanisms of reproductive toxicity (i.e.,structural similarity or chemical reactivity). Otherindirect-acting reproductive toxins may exerttheir effects by producing alterations in the body’s
physiological control systems (e.g., activation orinhibition of enzymes) (34). Figure 3-8 illustratesthese mechanisms of action of reproductive toxins.
It is also possible for reproductive toxins to ex-ert adverse effects through multiple mechanisms.For example, polychlorinated or polybrominatedbiphenyls (PCBS, PBBs) may act indirectly by ac-tivation of subcellular enzymes. These same com-pounds may also act directly by virtue of theirability to mimic the structure and function ofsteroid hormone molecules (34).
A great deal of attention is being given to re-search efforts to discover the mechanisms of ac-tion of agents known to disrupt development.Current knowledge, however, falls markedlyshort of identifying even the developmental se-
\

Ch. 3—Principles of Reproductive Biology and Development ● 5 9
quences leading to some adverse effects, muchless the precise cellular and molecular mecha-nisms involved in disruptions of normal structureand function of either the reproductive systemor in-utero development (21). Nevertheless, it ispossible to enumerate general developmentalmechanisms that can be disrupted and lead toaltered development. These include:
●
●
●
●
●
faulty cell or tissue differentiation;excessive, or in some cases inadequate, celldeath during development;improper cellular migration;faulty intercellular communication; anddisrupted metabolism, manifested as alteredrespiration, absorption, excretion, or se-cretion.
Three issues are central to understanding themechanisms of action of reproductive and devel-opmental toxicants; these issues also illustrate theoverall complexity of reproductive toxicology (34).They are:
● Species differences: Differences in repro-ductive toxicology among species are a reflec-tion of variations among species. In mecha-nisms of hormonal control, for example,there are differences in anatomy, metabo-lism, and pharmacokinetics.Q In some in-stances, these species differences are poorlyunderstood. A reproductive toxin in one spe-cies may not be toxic in another (including
4Pharmacokinetics refers to the study of the action of a chemicalin the body over a period of time. It includes the processes of ab-sorption, distribution, localization in tissues, transformation intoother chemicals with biological activity, and excretion.
humans) because of differences in reproduc-tive or toxicological mechanisms. The tera-togenicity of thalidomide is an instructive ex-ample of species susceptibility in that rat andmouse are relatively insensitive, while rab-bit, human, and nonhuman primates are sen-sitive (49). Another example is the differenceexhibited by rats and mice in sensitivity tooocyte destruction by aromatic hydrocarbons(e.g., benzo(a)pyrene) (36).Gender differences: This issue is crucial be-cause of the differences in anatomy and bio-logical control mechanisms for reproductionin the male and female. Because of the easeof accessibility of gametes and gonads in themale, more suspect compounds have beenscreened in animal studies and demonstratedtoxic to males than to females. Whether thisrepresents an actual gender difference in ga -metic or gonadal toxicity or is simply an ar-tifact of experimental designs is as yet un-known. More parameters are accessible forevaluating sperm, for example, than more-difficult-to-obtain oocytes (table 3-l).Time frame for toxicity: Knowledge of thewindow of sensitivity during which a struc-ture or function may be affected by repro-ductive and developmental toxicants is of crit-ical importance. A developing organ such asthe ovary (35) may be susceptible to theharmful effects of a reproductive toxin, yetthe same agent may have no effect on the de-veloped organ. Little is known, for example,about differences between the immatureoocyte and the mature, preovulatory oocytewith respect to susceptibility to reproductivetoxins.
REPRODUCTIVE DYSFUNCTION IN THE POPULATION AS A WHOLE5
In 1982, approximately 2,4 million marriedAmerican couples, or 8.4 percent of those inwhich the wives were of childbearing age (I5 to44) were unintentionally infertile, The epidemio-logic profile of infertile couples reveals: 1) agreater proportion of infertile couples among
This section is a summary of the detailed analysis of reproduc-tive impairment in the general population that appears in app. A,
blacks than whites, 2) a tendency to have experi-enced one or no live births, and 3) a tendency forthe woman to be age 30 or over with less thana high school education. Although the overall in-fertility rate among married couples (excludingthose who have been surgically sterilized) has notchanged since the 1960s, subgroups of couplesin which the wife is age 20 to 24 or black haveexperienced substantial increases in infertility

60 Reproductive Health Hazards in the Workplace
(39,40). It is important to note that many infer-tile couples are only temporarily affected and mayeventually bear a viable infant irrespective ofmedical treatment (12).
The causes of infertility are often complex, dif-ficult to pinpoint, and variable among individuals.Infertility is attributed in roughly equal propor-tions to men and women among married couples(18). The known and suspected causal factors ofinfertility can be categorized as:
environmental, including pollutants;pathological, including infectious diseases;heritable, such as genetic syndromes;iatrogenic, or medication-induced, includ-ing contraceptive and therapeutic drugs;nutritional;ascribed, including race, maternal or pater-nal age; andsociobehavioral, including “recreational”drugs, stress, and exercise.
Analysis of these factors reveals large gaps inscientific knowledge of the causes of infertility,and even sparser knowledge about possible syn-ergism with occupational factors.
Infant mortality rates in the United States arehigher than those of many developed countries.The proportion of infant deaths due to birth de-fects has risen to more than 20 percent, because:1) the rate of birth defects has not fallen as rap-idly as the overall infant death rate, and 2) im-provements in prenatal and postnatal care havereduced the infant death toll from other causes.The overall infant death rate for blacks is almosttwice that for whites, and more than three timeshigher for infant deaths that are due specificallyto low birth weight or prematurity. Although theoverall rate of birth defects is lower among blacksthan whites, the proportion of black infants oflow birth weight is almost twice that of white in-fants, probably because of: 1) the higher propor-tion of preterm black infants, and 2) the higherproportion of black mothers possessing risk fac-tors for bearing low birth-weight infants.
Birth defects afflict about 7 percent of live-borninfants in the United States (31). About one-halfof these birth defects are apparent at birth; theremainder become clinically apparent within 1
year. Some of the most common defects involvethe cardiovascular system and the male urogeni-tal system. Many of the more common birth de-fects, such as Down syndrome or neural tube de-fects, have a substantial impact on the individual,family, and society because of the severity of theirphysiological and functional effects. Single neu-ral tube defects (those with no major associateddefects) decrease in incidence following a gradientacross the United States from East to West andare most common in white and female newborns(26). Several other defects, including Down syn-drome and clubfoot, are most common in theNortheast.
The causes of the majority of birth defects areunknown. Individuals may be affected differentlyby a given causal agent, and some may not be af-fected at all. Age, health, and personal habits ofboth male and female, and extent of prenatal carein the female are some of the characteristics thatcan influence the risk of adverse fetal effects. At-tempts to isolate and identify work-related repro-ductive hazards must take these variables into ac-count (50). The timing and extent of fetal exposureto the agent during gestation may also vary itseffect.
Sociobehavioral factors have received much at-tention in the quest to understand the causes ofbirth defects. Alcohol is teratogenic when con-sumed by the mother in large amounts (definedvariably) and can result in ‘(fetal alcohol syn-drome)” characterized by central nervous systemdysfunction, mental retardation, growth deficien-cy, and facial deformities (54). Among neonatesof alcoholic mothers, 83.3 percent had birth weightsunder the tenth percentile compared with 2.3 per-cent in a nonalcoholic sample (55). In a prospec-tive study of the relationship between birthweight and alcohol consumption during the firsttrimester of pregnancy in 31,604 pregnancies, theauthors found that consuming at least one to twodrinks daily was associated with a significantlyincreased risk of producing a growth-retarded in-fant. Conversely, consuming less than one drinkdaily had minimal to no effects on intrauterinegrowth and birth weight. The authors note that“an occasional drink has only a trivial effect onintrauterine growth” (38). Conclusions regarding

Ch. 3—Prjncjples of Reproductive Biology and Development 61
the effects of alcohol consumption, although prob-ably valid for heavy drinkers, may be tentativebecause of the difficulty of assessing all possibleimpacts on prenatal development. These includefactors often associated with excessive alcoholconsumption such as smoking, heavy coffee con-sumption, abuse of drugs, lower socioeconomicstatus, and poor nutrition. In addition, moststudies do not control for the father’s consump-tion of alcohol or other paternal risk factors.
Cigarette smoke and nicotine are also harmful,carrying an increased risk of: 1) prematurity; 2)low birth weight, due partly to fetal malnutritionresulting from depression of placental circulationor maternal appetite; and 3) perinatal death(45,54). A pregnant woman who smokes two packsof cigarettes a day may reduce the oxygen sup-ply to her fetus by 25 percent (l). Effective Octo-ber 1985, new warning statements were required(Public Law 98-474) on the packages and adver-tising of all cigarette brands sold in the UnitedStates (59). Two of these statements call specificattention to the hazards imposed by maternalsmoking upon the offspring, for example:
SURGEON GENERAL’S WARNING: Smokingby Pregnant Women May Result in Fetal Injury,Premature Birth, and Low Birth Weight.
Data on the effects of passive smoking-inhalationof the spouse’s or co-worker’s smoke by the preg-nant woman-on the fetus are not available.
In sum, more complete knowledge of causal fac-tors for both male and female infertility and birthdefects in the population at large is needed to ac-curately isolate and identify reproductive hazardsspecific to the workplace. Epidemiological surveil-lance using incidence data is capable of detect-ing only unusually high rates of infertility or birthdefects in certain worker populations, and onlyafter many people have been affected. Even then,epidemiological data are often not sensitiveenough to pick up more subtle changes (see chap-ter 5), and national prevalence data may not pin-point locally high rates of infertility and birthdefects. Furthermore, many indicators of repro-ductive impairment, such as early spontaneousabortion, are difficult to detect and are thereforeunderreported.
SUMMARY AND CONCLUSIONS
The complexity of the continuum called repro-ductive biology and development is masked bya tendency to focus on discrete components ofthe process, such as the sperm cell or the egg cellor the embryo. Reproductive function also encom-passes pregnancy, lactation, child health and de-velopment, puberty, adult behavior, reproductivesenescence, and the integration of reproductivephysiology with the overall health of the individ-ual. Failure to recognize the integral role of eachof these components as part of reproductive func-tion leads to an underestimation of the sensitiv-ity of normal reproductive biology and develop-ment to perturbation.
Reproductive function in adult men and womencan be assessed by relatively simple means, in-cluding a detailed patient history, a physical ex-amination, blood samples, semen samples, andurine samples. When only these means are em-ployed, a disparity exists between the ease with
which male and female reproductive parameterscan be assessed. Sperm are readily accessible,while eggs are not. However, evaluation of thecauses of particular aspects of reproductive dys-function is difficult. Diagnostic techniques are dis-cussed in chapter 5.
Embryonic loss is a normal part of the repro-ductive process. Only one-quarter to one-third ofall embryos conceived develop to become live-born infants. The remainder are lost at some stagebetween fertilization and the end of pregnancy.Data such as these are hard to obtain, and esti-mates vary, because the loss of embryos is par-ticularly high in the early stages, before clinicaldiagnosis of pregnancy is made.
The terminology of the evolving field of devel-opmental toxicology is rapidly changing. The fourprincipal manifestations of developmental toxic-ity are: 1) death of the conceptus, 2) structural

62 ● Reproductive Health Hazards in the Workplace
abnormality, 3) altered growth, and 4) functionaldeficiency. Structural abnormalities and altera-tions or delays in postnatal abilities are teratogeniceffects. Insertion of the term “developmental tox-icant” for the term ‘(teratogen” in the languageof TSCA would clarify the existing statute to co-incide with contemporary understanding of theword “teratogen. ”
The complexity of reproduction and develop-ment is mirrored by the complexity of biologicalmechanisms underlying toxicology, which involveabsorption, distribution within the body, metab-olism (toxification and/or detoxification), excre-tion, and repair (34).
Toxicants may produce their adverse reproduc-tive or developmental effects by one of severalmechanisms. Some agents may act directly, eitherby virtue of direct chemical action, or by struc-tural similarity to endogenous molecules (e.g., hor-mone mimics or antagonists). Other agents inter-rupt reproductive processes indirectly, either by
metabolic processing to a direct-acting toxicant(e.g., metabolic activation to form an active chem-ical), or by altering the normal endocrine balance(e.g., increased steroid hormone clearance) (34).
The causes of the unintentional infertility be-ing experienced by some 2.4 million U.S. marriedcouples are varied and difficult to pinpoint. More-over, for some couples, infertility is a temporaryphenomenon. The known and suspected causesof infertility can be grouped as environmental,pathological, heritable, iatrogenic (i.e., medication-induced), nutritional, and sociobehavioral. Birthdefects afflict about 7 percent of live-born infants.As in the case of infertility, the causes of manybirth defects are often unknown or speculative.Analysis of reproductive impairment in the popu-lation as a whole (see appendix A to this chapter)provides a background against which to identifyany increased incidence of reproductive dysfunc-tion that may be workplace-related.
CHAPTER 3 REFERENCES
Ch. 3—Principles of Reproductive Biology and Development ● 6 3

46
47$
48.
49.
50.
51
52.
58.
59.
60.


















