
Chapter 14.Hazards of Anesthesia Machines & Breathing Systems
108
Chapter 14 Hazards of Anesthesia Machines and Breathing Systems Although enormous strides have been made in improving the safety of anesthesia apparatus, problems continue to be reported. Studies show that human error is more frequent than equipment failure ( 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 ). This chapter will examine hazards of anesthesia machines and breathing systems from the perspective of their effect on the patient. Many examples are given, but these should not be considered a complete listing of all possible dangers. Many hazards involve older apparatus that may have been modified and is no longer sold or serviced by the manufacturer. A discussion of anesthesia machine obsolescence is found in Chapter 5 . Hypoxia Hypoxic Inspired Gas Mixture Incorrect Gas Supplied Piping System The wrong gas may be supplied to the central oxygen supply ( 12 , 13 , 14 , 15 , 16 , 17 , 18 , 19 ). Crossovers between oxygen and other gases may occur in the piping system ( 20 , 21 , 22 , 23 ). During or following construction or repair, a pipeline may be filled with air or nitrogen rather than oxygen ( 24 , 25 ). A gas mixer, anesthesia machine, or ventilator may allow a crossover and contaminate one pipeline gas with the contents of the other ( 26 , 27 , 28 , 29 , 30 , 31 , 32 , 33 , 34 ). If the oxygen pressure is lower than the other gas, that gas may enter the oxygen pipeline. Inside the operating room, incorrect outlets may be installed ( 35 , 36 , 37 , 38 , 39 , 40 , 41 , 42 ). A terminal unit may accept an incorrect connector ( 43 , 44 , 45 , 46 , 47 , 48 ). An incorrect connector may be placed on a hose ( 49 , 50 , 51 , 52 , 53 , 54 , 55 ) or the pipeline inlet of the anesthesia machine ( 40 ). It may be possible to attach an oxygen tubing or hose to the outlet from an air flowmeter ( 56 , 57 , 58 , 59 ). If it is suspected that the pipeline oxygen system is delivering less than 100% oxygen, it is important to open an oxygen cylinder AND to disconnect the oxygen pipeline hose. If the pipeline hose is not disconnected, gas from the piping system
Transcript of Chapter 14.Hazards of Anesthesia Machines & Breathing Systems
Chapter 14 Hazards of Anesthesia Machines and Breathing Systems Although enormous strides have been made in improv ing the sa fety of anesthesia
apparatus, problems continue to be reported . Studies show that human error is
more frequent than equipment failure (1,2,3,4,5 ,6,7,8,9,10,11).
This chapter wi l l examine hazards of anesthesia mach ines and breathing sys tems
f rom the perspec tive of thei r ef fect on the pat ient. Many examples are g iven, bu t
these should not be considered a comple te l is ting of a ll possible dangers. Many
hazards involve older apparatus that may have been modif ied and is no longer sold
or serv iced by the manufacturer. A discuss ion of anes thesia machine obsolescence
is found in Chapter 5.
Hypoxia
Hypoxic Inspired Gas Mixture Incorrect Gas Supplied
Piping System The wrong gas may be supp lied to the central oxygen supply
(12,13,14,15,16,17,18,19). Crossovers between oxygen and other gases may occur
in the piping system (20,21,22,23). During or fo llowing construc tion or repair, a
pipel ine may be f i l led wi th air o r ni trogen rather than oxygen (24,25).
A gas mixer, anesthesia machine, or venti lator may allow a crossover and
contaminate one p ipeline gas with the contents of the other
(26,27,28,29,30,31,32,33,34). I f the oxygen pressure is lower than the other gas,
that gas may enter the oxygen pipeline.
Ins ide the operat ing room, incorrect outlets may be instal led
(35,36,37,38,39,40,41,42). A te rminal unit may accept an incorrect connector
(43,44,45,46,47,48). An incorrect connec tor may be placed on a hose
(49,50,51,52,53,54,55) o r the pipeline inlet of the anesthesia mach ine (40). I t may
be possible to attach an oxygen tubing or hose to the out le t from an air f lowmeter
(56,57,58,59).
I f i t is suspec ted that the pipe line oxygen system is del ivering less than 100%
oxygen, it is importan t to open an oxygen cylinder AND to disconnec t the oxygen
pipel ine hose. If the pipe line hose is no t disconnected, gas f rom the piping system

will s ti l l be delivered. If the cause of a low oxygen concentration is not obv ious and
the si tua tion is not corrected by disconnec ting the oxygen pipeline hose and
opening an oxygen cylinder, the pat ient should be venti la ted wi th room air by using
a manua l resuscitat ion bag (Chapter 10).
Cylinders I t is possible for a cyl inder labeled oxygen to contain another gas
(60,61,62,63,64,65). A cyl inder may be painted a color other than that normal ly
used for a part icular gas. Care shou ld be taken when using cy linders in o ther
countries, because four different colors (green, wh ite, b lue , and black) are used
around the world for oxygen (66). In a cylinder containing a mix ture of two gases,
incomplete mix ing may result in a hypoxic mix ture being del ivered (67,68). Such a
cylinder may require 45 minutes of rotating before mix ing is complete.
Despite almost universal use of the Pin Index Safe ty System, reports of incorrect
cylinders be ing connected to yokes continue to appear
(69,70,71,72,73,74,75,76,77,78,79,80,81,82). An incorrect yoke block may be
inserted (83 ,84). A pin may become unsc rewed from the yoke (85).
Crossovers in the Anesthesia Machine Crossovers between oxygen and other gases can occur ins ide the anesthesia
machine and are espec ially likely if the machine piping has been al tered (49,86).
Hypoxic Mixture Set
Flow Control Valve Malfunction A f low control valve malfunc tion may resul t in more or less gas being del ivered. If
the oxygen flow control valve is damaged and the f low is decreased, hypoxia can
resul t (87,88,89). If the f low control valve for another gas malfunct ions in such a
way that excessive gas is del ivered, hypoxia could a lso resu lt .
Incorrect Flowmeter Setting Some older anes thesia machines do not have a minimum oxygen ratio device that
prevents the user from dia ling a hypoxic fresh gas mixture. On these machines, a
hypoxic mix ture can be caused by partly or fully clos ing the oxygen f low control
valve, whi le a llowing the nitrous oxide f low to cont inue (90,91,92,93). Absence of a
minimum oxygen rat io device is one of the cri teria fo r machine obsolescence
(Chapter 5). Unfortunately, many anesthes ia machines in serv ice s ti l l lack th is
device (94). There may be prob lems wi th the minimum oxygen rat io device
(95,96,97,98,99,100,101,102,103,104,105), or the machine may have add it ional
gases that are not incorpora ted into the minimum oxygen ratio device.
Oxygen f low can be inadvertent ly lowered (or the f low o f another gas increased) if
the f low control knob is inadverten tly ro tated by an i tem on the surface below (106)
or by a hose or wire al lowed to drape around it . With some f lowmeters , in and out
movement of the f low contro l valve can change the f low s ignif icant ly (107).
Someone helping to move the machine could grab a f low control valve knob and
change the f low (F ig. 14.1). Most new machines have a guard over o r around the
f low control valves to prevent this problem.
The abil i ty to deliver 100% ni trous oxide was found in an anesthesia machine where
the tub ing to the common gas outlet became k inked (108,109). In this case,
P.406
the ni trous ox ide regulator was set at a h igher pressure than the oxygen regulator,
which caused ni trous oxide to preferent ial ly pass through the tubing.
View Figure
Figure 14.1 A dangerous practice. The flow control knob may look like a good thing to grab to someone moving an anesthesia machine. Flows may be altered in the process.
Incorrect Flowmeter Reading On some older machines , the f lowmeter indicator can disappear f rom view at the
top of the tube when the flow of gas exceeds the maximum scale cal ib ration. Such
a flowmeter is very similar in appearance to one wi th the ind icator resting at the
bottom. I f the f lowmeter carries a gas o ther than oxygen, a hypox ic mixture may
resul t .
I f an ai r flowmeter is present on a machine, dialing ai r instead of oxygen can resul t
in a hypox ic mixture (110). To prevent this , most modern anes thesia machines do
not allow administra tion of ai r and nitrous oxide wi thout addi tional oxygen flow.
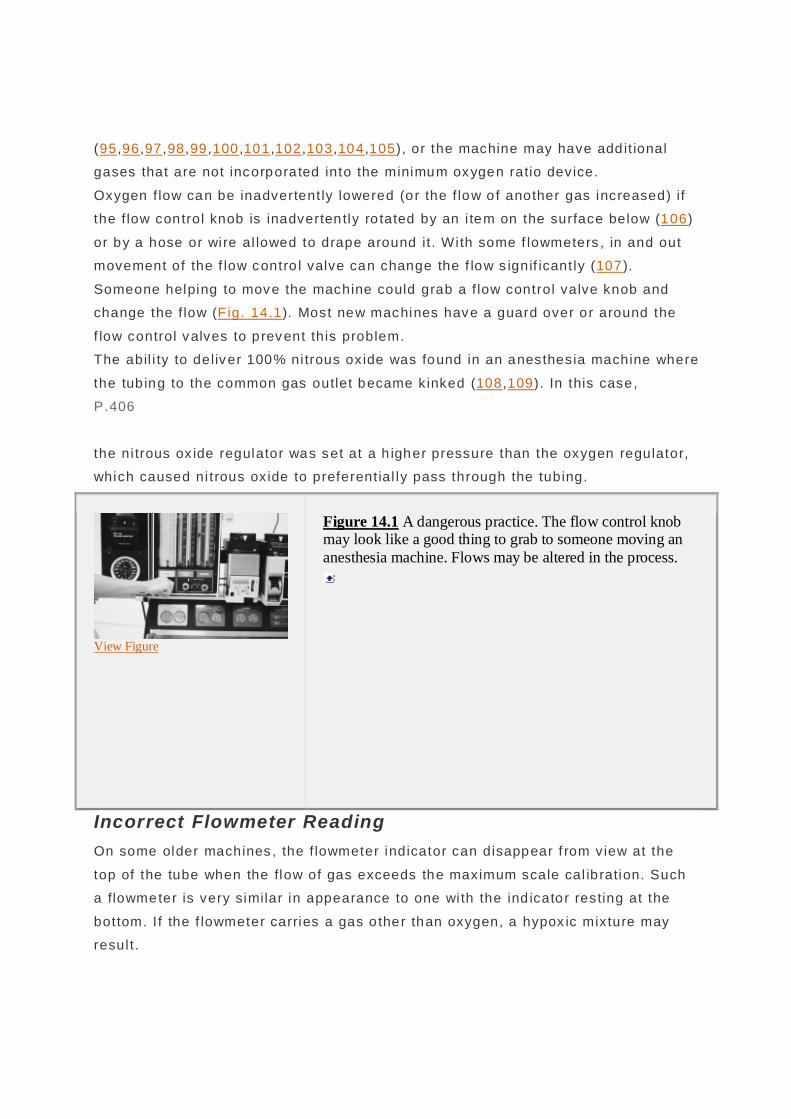
Inaccurate Flowmeter Causes of f lowmeter inaccuracy include di rt , grease, or o il on the indicator o r tube;
a stuck or damaged indicator; misalignment of the tube; stat ic e lec tricity; improper
ca libration ; the s top at the top of the tube fa ll ing down onto the indicator (Fig.
14.2); and transposi tion of indica tor, scale, or tube (111,112,113,114,115,116,117).
Oxygen Lost to Atmosphere I f there is a leak a t the top of the oxygen f lowmeter tube, oxygen wil l be
preferential ly los t, even if the oxygen flowmeter is downs tream of the other
f lowmeters (118,119,120,121,122,123). The posi t ion of the indica tor may not be
af fected. Of ten, the defect cannot be seen unti l the tube is d isassembled.
Other leaks in the anes thesia machine can resu lt in hypoxia, the magni tude of
which wi l l depend on the s ize of the leak and its locat ion
(121,122,124,125,126,127,128,129). I t is important to use a yoke p lug in any yoke
not containing a
P.407
cylinder so that gas wi l l not leak out of the yoke if the f low control valve to that
yoke is open.
Figure 14.2 The stop at the top of the flowmeter tube has broken off and fallen onto the indicator. The flowmeter will read less than the actual flow.
View Figure
Air Entrainment I f the pressure in the breathing system falls below atmospheric , ai r may be drawn
into the system through a leak or disconnect ion . Subatmospheric p ressure may be
caused by the pat ient 's insp iratory effort ; suct ion appl ied to an enteric tube
inadvertent ly placed in the tracheobronchial tree or to the work ing channel of a
f iberscope in the ai rway; a problem wi th a closed scavenging system interface; a
venti lato r wi th a hang ing bellows ; a piston venti lator; or a sides tream gas analyzer
wi th a low f resh gas f low (130,131,132,133,134,135,136,137). Ai r can enter the
breathing sys tem if the venti lator be llows is improperly connected or has a hole
(138,139,140,141,142,143,144) or the f resh gas f low is directed to the wrong ci rcui t
(145).
In many cases, ai r en trainment is manifested by a decrease in anesthet ic agent as
wel l as oxygen concentrat ions (135,146).
Hypoventilation
Causes Insufficient Gas in the Breathing System
Low Inflow Pipeline Problems Loss of pipel ine oxygen pressure was d iscussed in Chapter 2. Causes inc lude
damage during cons truct ion, debris in the l ine following instal lation, unannounced

system shutdown, pressure regulator malfunction , central supply sys tem
malfunct ion, a disrupted l ine between the central supply and the piping sys tem,
compressor fai lure resul t ing f rom an elec trical s torm, f i res, and a c losed isolat ion
valve (51,147,148,149,150,151,152,153,154,155,156,157,158,159). A station outlet
may become blocked or not accept a quick connector (159,160).
A hose may develop a leak, become b locked, or develop a kink tha t obs tructs gas
f low (152,161,162,163,164,165,166,167). The anesthesia machine may rol l over a
hose, occluding gas f low (164). The check valve at the pipeline inlet o f the
anesthesia mach ine may malfunc tion (168), or the f i l ter may become c logged,
reduc ing gas f low (169).
I f piped oxygen pressure is lost, an oxygen cylinder shou ld be opened and the
pipel ine hose disconnected from the wa ll to prevent f low from the cylinder into the
pipel ine. To minimize oxygen use, a gas-powered venti lato r should be turned OFF
(this is not necessary if an elec trically powered p is ton vent i lator is being used),
manual or spontaneous vent ilation ins ti tu ted , and the fresh gas f low lowered as
much as possible.
I f open ing an oxygen cylinder does not repressurize the anesthesia machine, then
there is a problem in the machine's high or intermedia te pressure system or the
cylinder is empty or not properly connected (164). A resusci tation bag should be
used to venti late the pat ient unti l another machine can be obtained.
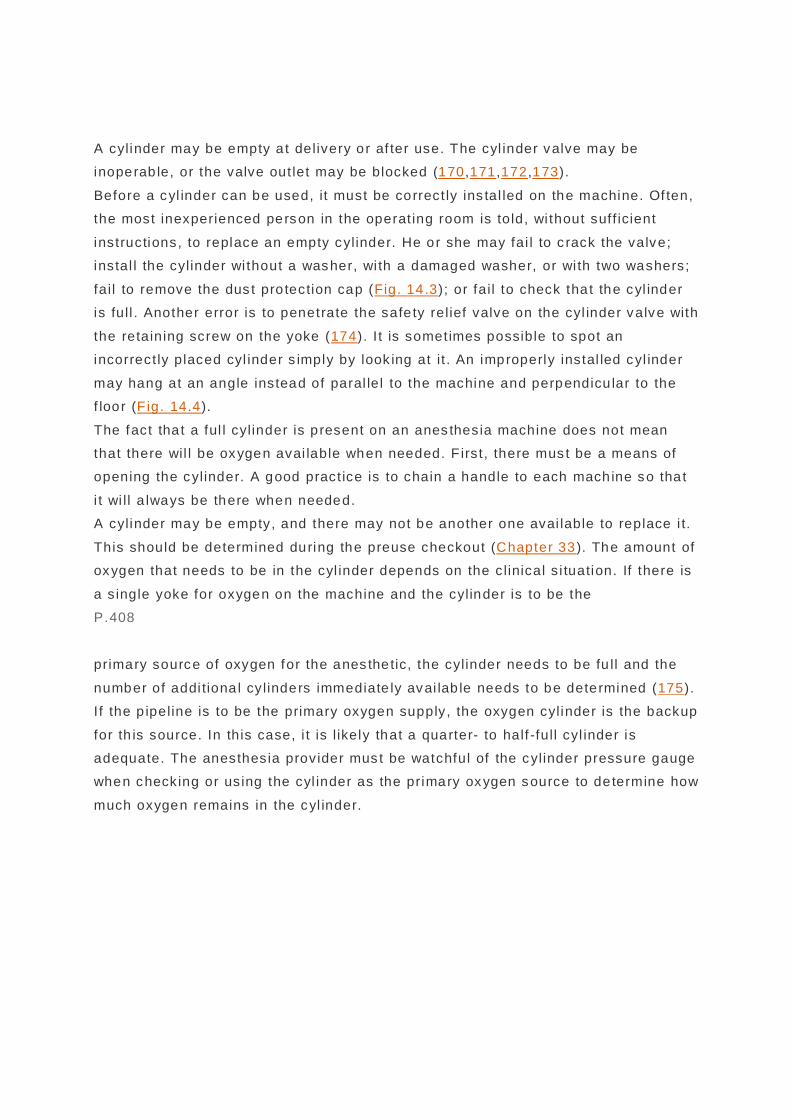
View Figure
Figure 14.3 Failure to remove the dust protection cap from a cylinder before installing it on a machine caused a portion of the cap to be pushed into the cylinder valve port, and this blocked the exit of gas from the cylinder.
Cylinder Problems
A cylinder may be empty a t delivery or af ter use. The cyl inder valve may be
inoperab le, or the valve out let may be blocked (170,171,172,173).
Before a cyl inder can be used, it must be correct ly ins tal led on the machine. Of ten,
the most inexperienced person in the operat ing room is told, wi thout suff icient
instructions, to replace an empty cylinder. He or she may fai l to c rack the valve;
instal l the cylinder wi thout a washer, wi th a damaged washer, or wi th two washers;
fail to remove the dus t pro tection cap (Fig. 14 .3); or fail to check tha t the cyl inder
is full . Another error is to penetrate the safe ty relief valve on the cyl inder valve with
the retaining screw on the yoke (174). I t is sometimes possible to spot an
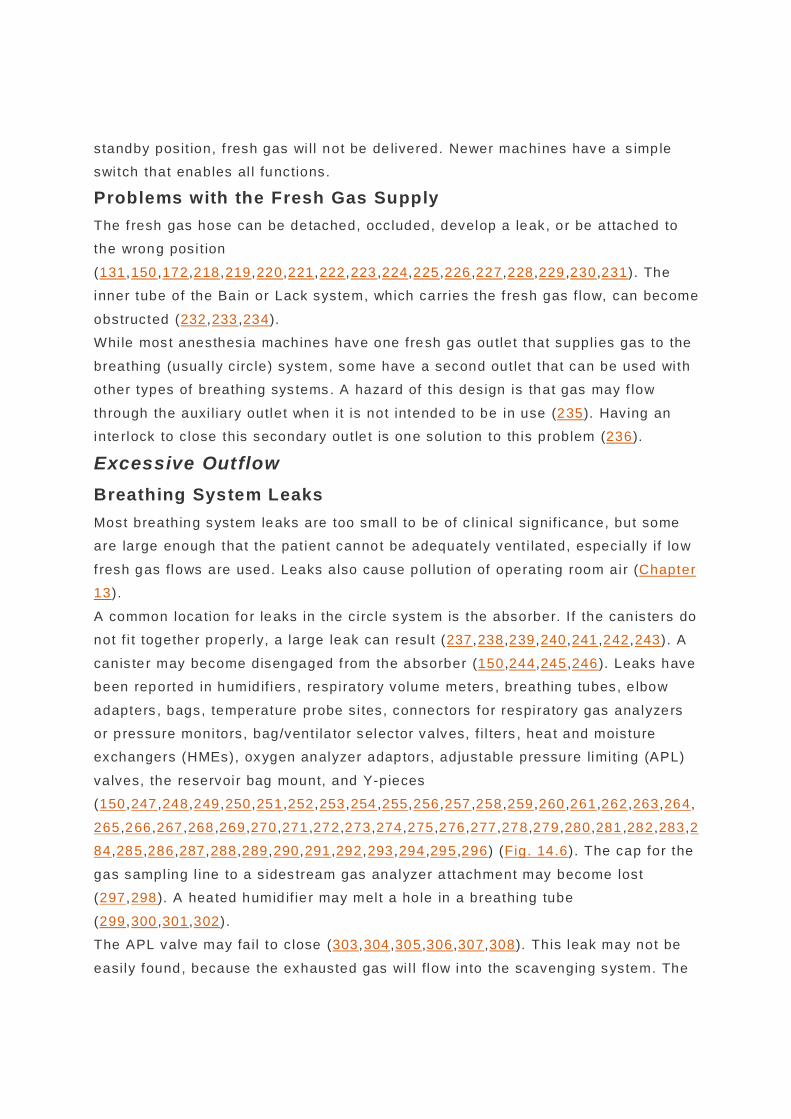
incorrect ly placed cyl inder s imply by look ing at it . An improperly instal led cyl inder
may hang at an angle instead of paral lel to the machine and perpendicu lar to the
f loor (F ig. 14.4).
The fact tha t a ful l cylinder is p resent on an anes thesia machine does not mean
that there wil l be oxygen avai lable when needed. F irst, there mus t be a means of
opening the cylinder. A good pract ice is to chain a handle to each mach ine so tha t
i t wi l l a lways be there when needed.
A cylinder may be empty, and there may not be another one avai lable to replace i t.
This should be determined during the preuse checkout (Chapter 33). The amount of
oxygen that needs to be in the cyl inder depends on the c linical s i tuation. If there is
a s ingle yoke for oxygen on the machine and the cylinder is to be the
P.408
primary source of oxygen for the anes thetic, the cylinder needs to be fu ll and the
number of addi tiona l cy linders immediate ly avai lab le needs to be determined (175).
I f the p ipeline is to be the primary oxygen supply, the oxygen cylinder is the backup
for th is source. In this case, i t is l ikely that a quarter- to half -full cyl inder is
adequate. The anesthesia provider mus t be watchful of the cylinder pressure gauge
when checking or us ing the cyl inder as the primary oxygen source to de termine how
much oxygen remains in the cyl inder.

View Figure
Figure 14.4 A sure sign that a cylinder is not correctly fitted in its yoke is that it hangs at an angle to the machine rather than perpendicular to the floor.
Anesthesia machines have a number of ways that warn the anesthesia provider tha t
the oxygen cyl inder has become exhausted. Many anesthesia providers do not
recognize when this occurs and furthermore do not know how to react to the
problem (176). This has been a ttributed in part to the fac t that anesthesia
technic ians usua lly maintain the cylinders on the machine and that many
anesthesia providers do not have experience wi th changing cy linders. This s lows
their react ion during an emergency si tuat ion .
Machine Problems
Obstruction Obstruct ion to gas f low in the anesthesia machine may be caused by problems in
the oxygen flush valve, f low control valve, yoke, or vaporizer connec tions
(117,177,178,179,180,181,182,183,184).
Leaks I f the check valve in the pipel ine inlet of the anesthesia machine fa ils , gas may flow
into the room (if the p ipeline hose is disconnected) or into the p iping system (if the
hose is connec ted) (185,186,187). Gas can be lost through a broken f lowmeter tube
or an open f low control valve with an opening to atmosphere upstream of the
f lowmeter (121).
Leaks can occur in the machine piping (188,189); at a loose or defect ive vaporizer
connec tion
(190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206); a

loose, defect ive, o r absent vaporizer f i l le r cap or d rain screw (207,208,209) (F ig.
14.5); or a defec t in the vaporizer itse lf (210). Vaporizer leaks do not manifest
themselves unt i l the vaporizer is turned ON. These can be
P.409
discovered if the vaporizer is turned ON during the checkout process (Chapter 33).
Some machines are designed so tha t when a vaporizer is removed, a manifold cap
must be placed where the vaporizer was s i tua ted. Fai lure to do so wil l resu lt in a
major leak. The pressure rel ief device on the mach ine may vent f resh gas if
downstream resistance causes the pressure to rise (211,212).
View Figure
Figure 14.5 When the block on the filling block is not in place, there will be a leak when the vaporizer is turned on.
Gas Supply Switched OFF The main ON-OFF switch on the machine may be accidental ly turned to the OFF
posit ion (213,214,215,216,217). Some mach ines have a two-posi t ion switch to turn
i t ON. One posit ion places the machine in standby, which enables only the
electrical portion of the machine, wh ile the other act ivates both the elec trical and
pneumatic port ions of the mach ine. If i t is not not iced tha t the switch is in the
standby posit ion, f resh gas wi l l not be de livered. Newer machines have a s imple
swi tch that enables al l functions.
Problems with the Fresh Gas Supply The f resh gas hose can be detached, occluded, develop a leak, o r be attached to
the wrong posi t ion
(131,150,172,218,219,220,221,222,223,224,225,226,227,228,229,230,231). The
inner tube of the Ba in or Lack system, which carries the f resh gas f low, can become
obstructed (232,233,234).
Whi le mos t anesthesia machines have one fresh gas outlet that supplies gas to the
breathing (usual ly c irc le) system, some have a second out let that can be used wi th
other types of breathing sys tems. A hazard of this design is that gas may f low
through the auxi l iary outlet when i t is not intended to be in use (235). Having an
inte rlock to c lose this secondary out le t is one solution to this problem (236).
Excessive Outflow Breathing System Leaks Most breathing system leaks are too small to be of c linical signif icance, but some
are large enough that the pat ient cannot be adequately vent i lated, especially if low
f resh gas flows are used. Leaks also cause pol lution of operat ing room air (Chapter
13).
A common location fo r leaks in the c i rc le system is the absorber. I f the can is ters do
not f i t together p roperly, a large leak can resul t (237,238,239,240,241,242,243). A
canis ter may become disengaged f rom the absorber (150,244,245,246). Leaks have
been reported in humid if iers , respiratory volume meters , breathing tubes, e lbow
adapters , bags, temperature probe s i tes, connectors for respiratory gas analyzers
or p ressure moni tors, bag/vent i la tor selector valves, f i l ters , heat and moisture
exchangers (HMEs), oxygen analyzer adaptors, adjustable pressure limi ting (APL)
valves, the reservoir bag mount, and Y-pieces
(150,247,248,249,250,251,252,253,254,255,256,257,258,259,260,261,262,263,264,
265,266,267,268,269,270,271,272,273,274,275,276,277,278,279,280,281,282,283,2
84,285,286,287,288,289,290,291,292,293,294,295,296) (Fig. 14.6). The cap for the
gas sampl ing l ine to a s ides tream gas analyzer a ttachment may become lost
(297,298). A heated humid if ie r may mel t a hole in a breathing tube
(299,300,301,302).
The APL valve may fail to c lose (303,304,305,306,307,308). This leak may not be
easily found, because the exhausted gas wi l l flow into the scavenging system. The

t ransfer tubing may need to be removed from the APL valve to de tec t the problem
(308,309). Mos t present bag/venti lator selec tor valves cause the APL valve to be
excluded f rom the system when swi tched to the automatic mode or when the
venti lato r is turned ON. With older machines where the APL valve is not excluded,
the user may forget to close i t when switching to automatic vent ilation .
View Figure
Figure 14.6 Parts of the breathing system may have holes in them when they are received from the manufacturer.
A leak may occur in a vent ilator (310,311) or in i ts a ttachment to the breathing
system (312,313,314). If the pilot l ine becomes d isconnected or k inked during
expirat ion, the spi l l valve ruptures or becomes stuck in the open posit ion, or the
exhaus t valve mal funct ions, gas can be lost (315,316,317,318,319). A large leak
wi l l occur if the bag/venti lator switch is placed in the venti lator pos it ion with no
connec tion to the venti lato r (320).
A defect ive nonrebreathing valve or misassembly of a manual resusci tator can
resul t in part or al l of the gas volume leaving the bag during inspirat ion and
escaping to a tmosphere (321,322,323).
Most leaks can be detected by the preuse check. Many reported leaks involve
equipment that was added after the checkout was performed (287,324). I t is
importan t that al l equipment that is to be used during a case be in place before the
preuse checkout is performed. Checking is discussed in more detail in Chapter 33.
Leaks may occur during an anesthetic (252). Such a leak may be evident by a low
expired volume or an inc rease in end-tidal carbon dioxide. With a s tanding bellows
venti lato r, the bel lows may not return to i ts fully expanded posi tion (325), and there
may be a change in the vent i lator sound. An airway pressure moni tor
P.410
may alarm wi th a leak but cannot be rel ied on, especial ly if the leak is no t large or
the alarm limi t is set low (258,326).
When a leak is suspected, a systematic search of the anes thesia machine and
breathing sys tem should be made, following the route of gas travel . It may be
easier to de tec t a leak if gloves are not worn (279). A leak can sometimes be
located by plac ing alcohol on the hands and moving the hands over components
whi le gas f low is occurring . The leaking gas evapora tes the alcohol and cools the
sk in.
Disconnections A disconnect ion is an unin tended separation of components (327). Disconnect ions
in b reath ing c ircui ts a re among the most common type of p reventable anes thetic
mishap involv ing equipment (1,2,11,238,328,329). Most b reathing system
connec tors are s lip fi t tings that rely on fr ic tion to hold them together. They wil l
come apart if suffic ient tens ion is app lied. If the connec tion is under a drape, th is
wi l l make it dif f icult to spot the disconnect ion (329,330).
Disconnec tions can occur anywhere in the breath ing system. The most common s ite
is between the breath ing system and tracheal tube connector or HME (1 ,331,332).
Disconnec tions are of ten associated wi th a third party interfering with the breathing
system and with surgery on the head and neck (238).
Disconnec tions can be made less f requent by making secure connec tions .
Connectors with lugs or other features that make them easy to grip may be easier
to t ighten. Push and twis t (wrung) connections are much stronger than those made
wi th a stra igh t push (333). Metal -to-metal or p las tic-to -plast ic joints are s tronger
than metal-to-plastic join ts (334).
Ant idisconnect devices for b reathing system components have been desc ribed
(327,335,336). Locking connectors use a mechan ical means to ensure that the
connec tors do not separate under any force tha t is common during use. Many
believe that they should not be used at the connec tion between the tracheal tube
connec tor and the breath ing system, reasoning tha t it is safer for such a union to
come apart under tension than for the tracheal tube to be pu lled out of the pat ient
(337). I t may be necessary to make a disconnection rap idly at this point for
suction ing or to re lieve a high pressure in the breathing system. Latch ing
connec tors are s imi lar but a re designed to “break away” wi th a certain

disconnection force (327). Adhes ive tape is sometimes used to prevent
disconnections. Unfortunate ly, tape can prevent the disconnect ion from being seen,
inhibi t reconnect ion, and cause an obstruc tion (327).
The anesthesia works tat ion standard (338) requires tha t the worksta tion be
provided wi th an a la rm tha t is activated in the event of a complete disconnect ion in
the breathing system. Alarms considered to comply wi th this requirement inc lude a
low airway pressure a larm, a low exhaled carbon d ioxide ala rm, and a low volume
alarm. These devices are discussed in Chapters 22 and 23. With spontaneous
breathing, no movement of the reservoir bag wi l l be seen if a disconnec tion occurs
(339).
Negative Pressure Applied to the Breathing System I f the a ir inlet valve of a closed scavenging inte rface or the opening to atmosphere
of an open interface becomes blocked or the inte rface is omitted, a subatmospheric
pressure may be transmitted across an open APL valve to the breathing system
(339,340,341,342,343,344).
I f suc tion is appl ied to the work ing channel of a f iberscope passed into the a irway
or to an enteric tube that has entered the trachea rather than the esophagus ,
respira tory gases wi l l be removed rap id ly f rom the lungs and breathing sys tem
(132,345,346,347).
Improper APL Valve Adjustment When manual ly control led or assis ted vent ilat ion is used, gas is vented from the
system during inspiration (unless a c losed system technique is used). Part of the
gas displaced f rom the bag goes to the pat ien t, and the rest is discharged from the
breathing sys tem. The person squeezing the bag may f ind it dif f icult to est imate
how much gas is entering the pat ien t and how much is escaping to a tmosphere.
Hypoventi lation can occur if too much gas escapes through the valve.
Blocked Inspiratory and/or Expiratory Pathway A partial o r complete block in the breathing sys tem can result in hypoventilation . In
most cases, the problem can be detected before the case has begun by having the
anesthesia provider o r the patien t breathe through the system (348). Lack of
obstruct ion to breathing, a satisfactory capnogram, and reservoir bag movement
should be seen. It is importan t that al l equipment that is planned to be used for the
case is in place in the system when the preuse checking is performed, as added
equipment may cause an obstruc tion (349,350,351,352).
Causes of b reathing system obstruction include manufacturing defec ts ; foreign
bodies (e.g., caps, plast ic wraps, tape); misconnect ions; blood; secret ions; or o ther
problems
(260,267,297,349,350,351,352,353,354,355,356,357,358,359,360,361,362,363,364,
365,366,367,368,369,370,371,372,373,374,375,376,377,378,379,380,381,382,383,3
84,385,386,387,388,389,390,391,392,393,394,395,396,397,398,399,400,401,402,40
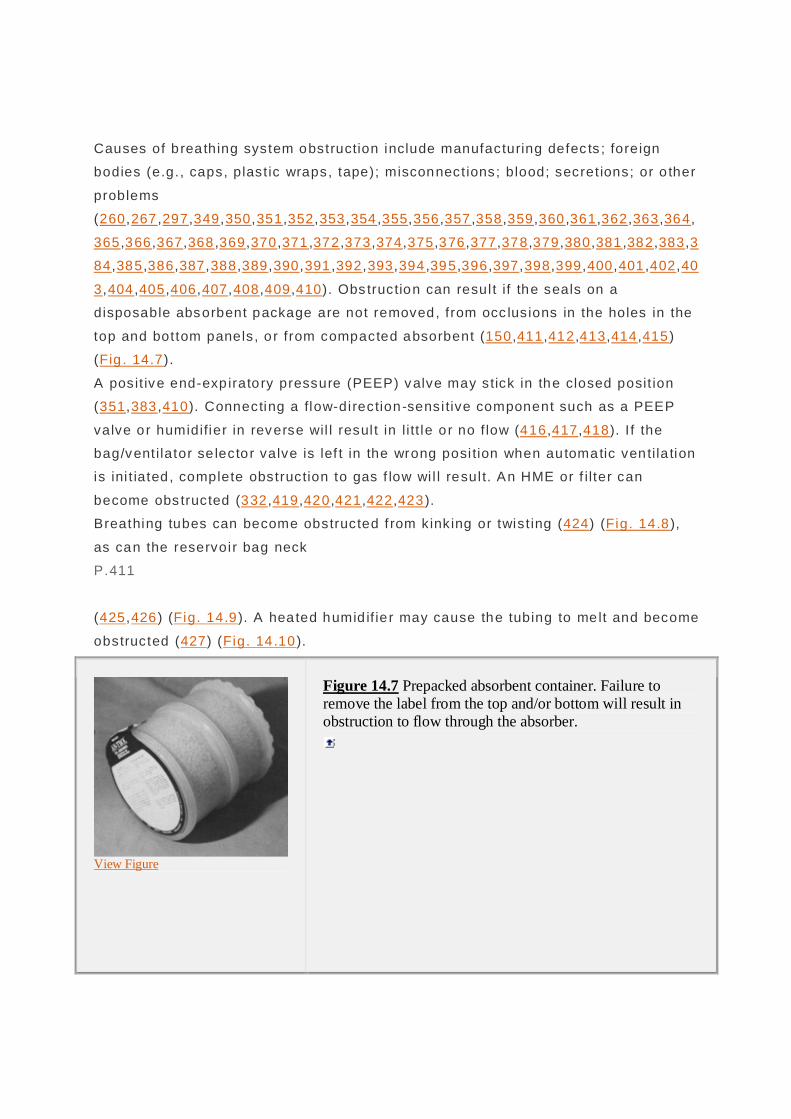
3,404,405,406,407,408,409,410). Obs truction can resul t if the seals on a
disposable absorbent package are not removed, from occ lusions in the holes in the
top and bottom panels, o r from compacted absorbent (150,411,412,413,414,415)
(Fig . 14.7).
A posit ive end-exp iratory pressure (PEEP) valve may stick in the closed posit ion
(351,383,410). Connecting a flow-direction-sensi tive component such as a PEEP
valve or humidifier in reverse wil l resul t in l i tt le o r no f low (416,417,418). I f the
bag/vent i lator se lector valve is lef t in the wrong posi tion when automatic venti la tion
is ini t iated , complete obstruction to gas f low wi l l resul t. An HME or f i l ter can
become obs tructed (332,419,420,421,422,423).
Breathing tubes can become obstructed f rom kinking or twist ing (424) (Fig. 14.8),
as can the reservoir bag neck
P.411
(425,426) (Fig. 14.9). A heated humid if ie r may cause the tubing to melt and become
obstructed (427) (Fig. 14 .10).
View Figure
Figure 14.7 Prepacked absorbent container. Failure to remove the label from the top and/or bottom will result in obstruction to flow through the absorber.

Ventilator Problems Hypoventi lation secondary to vent i la tor p rob lems is discussed in Chapter 12.
Causes inc lude cycling fai lu re, leaks of d riving or breathing sys tem gas,
inappropriate settings , and the venti la tor being turned OFF. If an anesthesia
machine is turned OFF and then turned ON aga in , the vent i lator may defau lt to
se tt ings that are d if ferent from those origina lly set (428).
View Figure
Figure 14.8 Kinking of a breathing tube.
Detection Vigilance aids used to detec t hypoventila tion inc lude ai rway pressure, resp iratory
volume, and carbon d ioxide moni tors. These are discussed in Chapters 22 and 23.
An oxygen analyzer may detect some disconnections (238,429,430) but shou ld not
be relied on, because i t is effective in on ly a l imi ted set of c i rcumstances . The low
temperature alarm on a heated humidif ier may s ignal loss of gas f low in the
breathing sys tem (238). Because any s ingle monitoring modal ity may fail to detec t
a problem, i t is advisab le to use more than one (428,431,432,433).
As stated previous ly, obstruct ions in the breathing system are best de tected by
breathing th rough the system before i t is used but af ter a ll components tha t wi l l be
used are in place. The checkout procedure is discussed in Chapter 33 .
Response to Hypoventilation

When hypoventilat ion occurs during mechanical vent ilat ion, the f i rs t s tep should be
to switch to manual vent i lat ion (434,435,436,437). The anesthesia provider can
then determine whether or not breathing sys tem resistance and compl iance is
normal and if there is adequate gas in the breathing system. I f manual venti lat ion
can be used to vent ilate the patien t sat is factori ly , the problem probably l ies wi th
the vent i la tor o r venti la tor c ircu it . If the problem cannot be d iagnosed or corrected
quick ly, manual venti lation can be cont inued or a backup anesthesia machine
brought in.
I f manua l venti la tion shows obs truct ion to venti la tion, the next s tep is to attach a
resusci tation bag to the ai rway device (mask, tracheal tube, or supraglo tt ic device).
I f i t remains dif ficul t to venti late the pat ien t, the problem is probably wi th the ai rway
device or wi th the pat ient. Compl ications related to supraglo tt ic a irways and
tracheal tubes are discussed in Chapters 17 and 19.
I f manua l venti la tion shows that there is gas f low into the breathing system, but i t is
not adequate to venti late the patient properly, the fresh gas flow should be
increased. I f increasing the fresh f low does not a llow adequate venti la tion, a
resusci tation bag should be used.
I f adequate vent i lation can be achieved by using a resusci tation bag, the tubing to
the bag should be connected to the anesthesia machine outlet , if poss ib le. Inspired
gas monitoring should be continued, if possible. This wi l l determine if the
resusci tation bag is being supp lied f rom the anes thesia machine or room air. I f the
resusci tation bag cannot be connected to the machine outlet or there is no f low
f rom the anesthesia machine, a source of oxygen should be connected to the
P.412
resusci tation bag and anesthes ia maintained by using intravenous agents .

View Figure
Figure 14.9 Twisting has caused this bag to become obstructed. Many bags have a guard in the neck to prevent this.
Af ter adequate vent ilation and anesthesia level have been established, the cause of
the problem can be invest igated. A second knowledgeable person should be sought
and serious considerat ion given to bringing in a second anesthesia machine, if this
has not al ready been done. Even if the problem can be found, i t may not be
possible to correct i t quick ly.
View Figure
Figure 14.10 Contact with a heated humidifier can cause a breathing tube to melt and become obstructed.
Hypercapnia

Hypoventilation Hypercapnia can be the resul t of hypoventilat ion, wh ich was discussed previously.
Inspired carbon dioxide wi l l be zero if hypoventilat ion is the sole cause of
hypercarbia. Other causes of hypercapnia mentioned below are associated wi th an
increased inspired carbon dioxide concentra tion.
Inadvertent Carbon Dioxide Administration A few anesthesia machines are equipped wi th a carbon dioxide cyl inder and
f lowmeter (438). This f lowmeter may be accidentally turned ON but no t not iced,
especial ly when the ind ica tor is at the top of the tube (439). An apparent ly OFF
f lowmeter may leak carbon dioxide into the breathing sys tem (440).
In one reported case, a ni trous oxide hose was connected to the carbon dioxide
stat ion outlet (441). A cylinder may be mis takenly f i l led with carbon dioxide (65).
Rebreathing without Carbon Dioxide Removal Absorbent Failure or Bypassed Absorbent I t is important to watch for the appearance of carbon dioxide in the insp ired gas .
The smaller canisters on some new machines have a shorter l ife span than the
larger ones on older machines. Hypercarbia can occur if channel ing allows gases to
bypass the absorbent (150,442).
Bypassed Absorber An absorber bypass allows some or all of the exhaled gases to bypass the
absorbent. Unintent ional activation
P.413
of this bypass can lead to hypercarbia. The absorber may be defec tive so that gas
f low is not di rected th rough the absorbent (443). Most new anesthesia breathing
systems tha t have small absorbers al low the canister(s) to be changed wi thout the
breathing sys tem integri ty being in terrupted. I t is possible that the anes thesia
provider may not no tice that a canister is loose or missing. Some anesthes ia
providers in tentiona lly remove the canister to allow carbon d ioxide to increase in
the breathing system at the end of a case. This may not be noticed by the nex t
anesthesia provider.

View Figure
Figure 14.11 Damaged unidirectional valve leaflet.
Unidirectional Valve Problems Correct movement o f gases in a ci rc le system depends on properly func tioning
unidi rect ional valves. If they do not c lose properly, rebreathing wil l occur. The disc
may become displaced, wet, s t icky, or damaged so that i t wi l l not seat properly
(150,444,445,446,447,448,449,450,451,452,453,454,455,456,457,458,459) (Fig.
14.11). The disc may not be replaced after removal for clean ing or serv icing. The
cage holding the disc may become dis lodged (460,461).
Unidi rectional valve prob lems can be discovered preoperat ively during the
breathing sys tem checkout (Chapter 33). Problems wi th the unidi rect ional valves
may be indicated by a respirometer indicat ing reversed flow (Chapter 23), a rise in
the inspired carbon dioxide above zero (Chapter 22) o r a capnogram wi th a slan ting
downstroke (Fig. 22.32). Pressure-volume loops (Chapter 23) may also indicate this
problem.

View Figure
Figure 14.12 Possible problems with the inner tube of the Bain system that can result in hypercarbia. The fresh gas supply tube can become detached (A), the inner tube can become kinked or develop a leak (B), and the inner tube may not extend to the patient port (C).
Problems with Nonrebreathing Valves Improperly assembled or s ticky nonrebreathing valves can resul t in part ial or total
rebreathing. Th is is discussed more ful ly in Chapter 9.
Inadequate Fresh Gas Flow to a Mapleson System In systems wi thout carbon d ioxide absorption, a low fresh gas f low can resul t in
dangerous rebreathing (Chapter 8). Reported causes include the fresh gas f low
being set too low; a leak or obs truction in the machine, common gas outlet , f resh
gas supply l ine , or a vaporizer; o r an empty cyl inder (263,462,463,464,465).
Problems with Coaxial Systems In Mapleson systems in which the fresh gases are delivered to the dista l end of the
system by an inner tube, rebreathing wi l l occur if the inner tube is avulsed,
damaged, k inked, or omitted; has a leak at the mach ine end; or does not extend to
the pat ient port (233,466,467,468,469,470,471,472,473,474,475,476) (F ig. 14.12).
I f the inner tube of a coaxial c i rc le system is displaced or develops a leak, an
increase in inspired carbon dioxide wi l l be seen, as previous ly exhaled gas wi l l be
reinhaled wi thout carbon d ioxide having been removed (477).
Excessive Dead Space An increase in dead space wi l l increase rebreathing. Th is increase is especial ly
importan t in small patien ts (478). An HME is placed between the pat ient port and
the breathing system. These come in a varie ty of s izes, and if a large one is used
on a patient wi th a small t idal volume, dangerous rebreathing may occur (479).

Often, a connector is added between the pat ien t port of the breathing sys tem and
the pat ient to move the breathing system away from the surgical field
P.414
(Fig . 14.13). These increase dead space and must be used wi th caut ion.
View Figure
Figure 14.13 Increased dead space between the breathing system and the patient can result in serious hypercarbia in pediatric patients and spontaneously breathing adults.
I f a disconnect ion occurs in a c losed space, such as under a plas tic drape over the
face during spontaneous breathing , exhaled gas containing carbon dioxide can
accumulate in that space and the inspired carbon diox ide level wi l l r ise (339).
Hypercarb ia is best detected using capnometry. Inspired carbon dioxide wi l l be zero
i f a c i rc le sys tem wi th properly function ing absorbent and un idirect ional valves is
used and hypoventilation is the sole cause of the hypercarbia. I f the hypercarbia is
not caused by added carbon diox ide and is the resul t of hypoventilat ion, increasing
the minute volume wi l l reduce the carbon diox ide in the breathing system. If the
carbon d ioxide absorbent or a un idi rectional valve is no t work ing properly ,
increasing the fresh gas flow wil l lower the carbon dioxide levels in the c i rc le
system. Hypercarbia when using a Mapleson system is usually the resul t of low
f resh gas flow, so inc reasing the f resh gas f low wi l l lower the inspired carbon
dioxide level. Chapters 8 and 9 discuss the Mapleson systems and c irc le sys tems.
Chapter 22 offers a ful ler discussion of carbon dioxide moni toring.
Hyperventilation A hole or tear in the vent i lator bel lows can cause inadverten t hypervent ilat ion
(138,139,480). This can be detected by an increased oxygen concentrat ion , if

oxygen is the driv ing gas (or a dec reased concentration if ai r is used); increased
venti lation as indica ted by a spirometer; or decreased end-t idal carbon dioxide.
These moni to rs are discussed in Chapters 22 and 23.
Excessive Airway Pressure In addi tion to interfering with venti la tion, a h igh pressure can cause barotrauma
and adverse effects on the cardiovascular sys tem. Neurologic changes and
otorrhagia have been reported (481,482). A hyperinf la ted lung may interfere with
surgery (483).
Modifying Factors The rate and extent of the pressure rise are important and wil l be affected by a
number of factors, includ ing the reservoir bag; the volume and compliance of the
system; the f resh gas f low; and use of a cuffed or uncuffed trachea l tube, face
mask, or supraglottic airway device.
The pressure in the breath ing system is normal ly l imited to 50 cm H2O by the
reservoir bag. Non-latex bags may allow s l igh tly higher pressures (484). When an
automatic vent i lator is in use, the bel lows buf fe rs increases in pressure. I f the bag
or bellows is excluded from the system, this buffering capaci ty is removed and
dangerously high pressures may be reached rapidly if there is coincidental
obstruct ion to the outflow of gases f rom, or high inflow in to, the system. Bag
exclusion is mos t commonly caused by an obstructed exp iratory l imb upstream of
the bag. The bag may become obs tructed at i ts neck (485) (Fig. 14 .9).
Unfortunately, an anesthesia provider who f inds a reservoir bag that is not f i l led
may incorrect ly assume that there is a leak in the system and operate the oxygen
f lush in an attempt to compensate (486). The high gas f low f rom the oxygen flush
can raise the pressure in the breathing system to dangerous levels very rapidly
when the bag is exc luded.
Protective Devices The anesthesia works tat ion standard requires that there be a dev ice to l imi t the
pressure in the breathing system to 125 cm H2O (338). These devices may
malfunct ion (487). In addi tion, there mus t be a means to continuously display the
pressure in the breathing system and a pressure moni tor tha t activates a high
prio ri ty alarm when the pressure in the breath ing system exceeds the operator-
adjustable l imi t for high pressure .
Some of the newer venti lato rs have pressure-controlled venti lat ion in which peak
ai rway pressure is lower than when volume control venti lat ion is used. Some of
these vent i lators automatica lly swi tch f rom the inspira tory to the expiratory phase
when the peak pressure th reshold is exceeded (488).
Another factor that can reduce the a irway pressure rise is an uncuffed tracheal tube
or a trachea l tube in which the cuff is not inf lated to a h igh pressure. Adjus ting cuff
pressure to 34 cm H2O or less wi l l a llow it to ac t as a safety valve fo r excessive
pressure in the a irway. The use
P.415
of a mask or supraglo tt ic ai rway dev ice wi l l also provide a means of pressure re lief .
Automatic disconnect ion of breathing sys tem components cannot be rel ied on to
provide pressure relief , because the pressures required for disconnection are fa r in
excess of those that cause lung inju ry (334).
Causes of Excessive Airway Pressure High Inflow I f the oxygen f lush valve s ticks in the ON posi tion, 35 to 75 L/minute of oxygen wil l
be de livered. Oxygen f lush valves on newer machines are designed to c lose
automatical ly but can fai l (489,490,491). It is possible for personnel to accidental ly
ac tua te some oxygen f lush valves. Other equipment may cause the f lush valve to
st ick in the ON posi tion (492,493,494,495). I f the oxygen f lush valve is act ivated
during inspira tion when a mechanical vent i lator is being used, a large volume of
gas wi l l be added to the inspired tidal volume, resul ting in a greatly increased
pressure wi th certain breathing system configurations (496,497). A vent i lator
control valve can malfunction, resul ting in a constant f low of d riv ing gas (498).
Low Outflow
Obstruction in the Expiratory Limb As noted previously, excluding the bag from the breathing sys tem resul ts in loss of
buffering capaci ty. Thus, breathing system obstruc tion in the expiratory l imb is
part icula rly hazardous if i t occurs ups tream of the reservoir bag. The expiratory
pathway can be obstructed by fore ign bodies (inc luding ampules, coins, plas tic
wraps, discs, tape, and caps) (361,499,500,501,502), water (503), or equ ipment
defec ts or misassembly
(383,410,497,504,505,506,507,508,509,510,511,512,513,514,515,516,517,518). A
PEEP valve may s tick or be placed backward (383,410,519,520,521,522,523).
The expiratory limb of a T-piece sys tem can become obstruc ted by the user's
f inger, k ink ing, external compression, misassembly, or adhesive tape
(524,525,526).
I f a pediatric breathing system with an adapter that has the f resh gas in le t
protrud ing near the end is used wi th a “low dead space” tracheal tube connector,
the fresh gas supp ly tube may c lose ly approximate or even press against the end o f
the connector, causing partial or complete obstruct ion of the exhalat ion pathway
(527,528,529). The same problem has been reported wi th a bronchoscope (530).
Obstruction at the Ventilator I f the venti lator sp il l valve becomes stuck, the pressure in the breathing system wi l l
r ise (317,531,532,533,534). The exi t of d riving gas f rom the bel lows housing may
be blocked (535).
Obstruction at the Adjustable Pressure-Limiting Valve APL valve omission, malfunct ion, or blockage may occur
(485,486,536,537,538,539,540,541). The user may fail to open the valve when
swi tching from automatic to spontaneous vent i lat ion if the APL valve is not
automatical ly excluded f rom the breathing sys tem during mechanical vent i lat ion and
automatical ly inc luded during manual or spontaneous venti la tion. With some APL
valves, subambient pressure from an act ive scavenging system wil l cause the valve
to c lose, p reventing excess gas f rom leaving the breath ing system
(542,543,544,545).
Obstruction in the Scavenging System The scavenging system is essent ially an extension of the breathing system. If
malfunct ions in the scavenging system occur, the pressure in the breathing system
may be affected. Obstruction in the transfer tubing between the APL valve in the
breathing sys tem or between the spi l l valve in the venti la to r and the interface can
prevent gas f rom leav ing the breathing sys tem (544,545,546,547,548,549,550,551).
The transfer tubing may be connected to an incorrec t s i te (552,553,554).
I f the pressure relief valve in a c losed ac tive scavenging interface (Chapter 13)
fails to open, sustained posi tive pressure in the breathing system can result . In one
reported case, a valve in tended for negative pressure rel ief ra ther than one fo r
posit ive pressure re lief was accidenta lly installed (555).

Problems with Nonrebreathing Valves in Resuscitators A sudden high inf low of gas or a quick squeeze or bump on the self-re fi l l ing bag of
a resusc itator may generate suff ic ient pressure to lock the nonrebreathing valve in
the inspiratory posi t ion (556). Continuing inf low wi l l cause a rise in pressure.
Incorrect nonrebreath ing valve assembly or malfunct ion may resu lt in obs truct ion to
exhalation (557,558,559,560).
Misconnected Oxygen Tubing Misconnection of oxygen tubing di rect ly to an indwel l ing tracheal or tracheos tomy
tube or supraglott ic airway device without provis ion fo r vent ing has occurred, of ten
wi th disastrous results (561,562,563,564,565,566,567,568,569) (Fig. 14 .14).
Another cause of increased pressure is connection to a T-piece wi th a c losed
expiratory l imb (570).
Unintentional Positive End-expiratory Pressure An external PEEP valve may remain in the c ircui t and not be removed, or an
integra l PEEP valve may be lef t in the ON posi t ion a t the end of a case and not
noticed by the nex t user (523,571) (Fig. 14 .15). With older b reathing systems, the
ai rway pressure gauge is loca ted on the absorber side of the unidi rect ional valves,
and PEEP cannot be observed on the gauge (483,523,572). Newer breathing
systems measure the pressure on the patien t s ide of the unidi rectional valve.
Inadvertent PEEP may be caused by water that is condensed in the tubing
connec ting the venti lator to the
P.416
breathing sys tem (573) o r an inadequate opening in the bag of a Mapleson F
system (574).

View Figure
Figure 14.14 A: The oxygen tubing is attached to the mask. B: The adapter has become detached from the mask and is attached to the tracheal tube connector. There is no way for the gas to escape.
Detection When an automatic venti la tor is used, i t is essential tha t the chest wal l motion ,
deflections on the breath ing system pressure gauge, t idal and minute volumes
registered on a resp irometer, and breath sounds be carefully moni tored. Observ ing
the ai rway pressure waveform, if available, can detect some problems . Pressure-
volume loops (Chapter 23) are also useful . The vent ilator may change sound wi th
stacked breaths. A continu ing or high airway pressure alarm may a le rt the operator
to this hazard . The capnograph (Chapter 22) may show an ascending l imb wi th a
prolonged rise time and no plateau.
Obs truct ions to the breathing system can be detected by performing a thorough
anesthesia mach ine
P.417
and breathing system check , including hav ing someone breathe through the sys tem
prio r to use (383). The procedure for preuse checking is discussed in Chapter 33.

View Figure
Figure 14.15 A: PEEP valve with 0 PEEP. B: Same valve with PEEP. Note the similarity in appearance.
Response I f there is a pressure bui ldup in the sys tem, a disconnect ion shou ld be made
IMMEDIATELY at the tracheal tube connec tor (575). T ime spent look ing for the
cause of the problem may resul t in ever-increasing pressure.
Venti la tion should be cont inued by us ing a resusci ta tion bag unti l the problem is
diagnosed and correc ted.
Inhalation of Foreign Substances A foreign body in the breath ing system can of fe r more risk than obstruction . In
some cases , it could migrate in to the pat ient 's respiratory trac t (576,577).
Absorbent Dust Inhaling absorbent dust can cause bronchospasm, laryngospasm, cough, decreased
compliance, and burns to the pat ient's face (578,579). Th is can be avoided by using
a fi l ter at the pat ient port, releasing breathing system pressure at the APL valve
when checking for leaks, tapp ing each canis ter to remove dus t before it is put into
the absorber, and not overf i l l ing can isters (581,582).
Medical Gases Contaminants Reported contaminants in medical gases inc lude water, o il , hydrocarbons , higher
ox ides of ni trogen, and metal l ic f ragments
(35,53,170,582,583,584,585,586,587,588,589,590,591). Bac teria may be found,
especial ly in compressed ai r (592,593,594,595).

Parts of Breathing System Components Part of a breathing system component may break and become detached. Reported
cases have involved parts of the sampl ing si te fo r an asp irat ing resp iratory gas
moni tor, an APL valve, an oxygen sensor, and HMEs
(297,388,596,597,598,599,600,601,602,603). Some manufac turers pla te the inside
surfaces of components wi th materials that may f lake off (604,605).
Other Foreign Bodies A number of other foreign bodies have been found in breathing sys tems
(377,378,379,381,396,400,499,500,501,502,577,606,607,608,609). Of ten, these
enter during c leaning.
Carbon Monoxide Dry absorbents contain ing sodium or potassium hydroxide can resul t in carbon
monoxide formation when
P.418
exposed to volat ile anesthet ic agents. Th is is discussed in detail in Chapter 9.
Anesthetic Agent Overdose An anesthet ic agent overdose can result in severe cardiovascular depression.
Chapter 6 offers a more complete discussion of overdose caused by vaporizer
malfunct ion.
Tipped Vaporizer I f a vaporizer charged wi th l iquid is tipped or agi tated, a very high concentra tion
may be de livered when the vaporizer is turned ON (610). Some newer vaporizers
have a “travel” setting that isolates the vaporizing chamber f rom the res t of the
vaporizer when the vaporizer is removed f rom the anesthesia mach ine.
Vaporizer or Nitrous Oxide Inadvertently Turned ON Previous vaporizer se tt ings by a colleague or serv ice technician can resu lt in the
vaporizer control dial being lef t in the ON pos it ion (611,612,613). Someone he lping
to move the machine may grasp a control dial , inadvertent ly turning it ON.
Inadvertent administrat ion of ni trous ox ide may occur if gas from the main
f lowmeters is used to supply supplementary oxygen (614).
Incorrect Agent in the Vaporizer

I f an agent is incorrect ly placed in a vaporizer designed for an agent wi th a lower
vapor pressure and/or a higher minimum alveolar concentrat ion (MAC) value, a
hazardous ly high concentrat ion may be delivered (615,616,617,618). An example is
plac ing isof lurane or halothane in a vaporizer designed for enf lurane.
Improper Vaporizer Installation I f a vaporizer not designed to be exposed to high gas flows is p laced in the f resh
gas supply tube between the anesthesia machine and the breathing system, there
wi l l be a h igher-than-usual f low of gas through the vaporizer when the oxygen f lush
is act ivated (619). Some vaporizers del iver a considerably higher-than-expected
vapor ou tput if connected so that gas f low is reversed, al though some wil l del iver a
normal concentrat ion (620,621).
Overfilled Vaporizer Most vaporizers are now designed so tha t they cannot be overf i lled. Many agent-
specif ic fi l ling devices prevent overf il l ing by connect ing the ai r intake in the bottle
to the ins ide of the vaporizing chamber. This safety feature can often be overridden
by s light ly unscrewing the bottle adapter and tu rning the concentra tion dial ON
during fi l ling (622,623,624). A drain has been added to some fi l ling devices to help
prevent overf i l l ing.
Vaporizer Interlock System Failure I f the vaporizer interlock system fa ils, i t is poss ib le to turn on more than one
vaporizer at a t ime (625,626).
An agent moni tor (Chapter 22) wil l measure the concentration of volati le agent in
the breathing system. When an overdose of anes thetic agent is suspected, the
patient should be disconnec ted f rom the breathing system and venti lated by using a
resusci tation bag and gas from a source other than the anes thesia machine out let.
Inadequate Anesthetic Agent Delivery Inadequate anes thetic agent delivery can cause serious morbidi ty and result in
patient awareness during the surgical p rocedure (627,628,629,630).
Decreased Nitrous Oxide Flow Pipel ine nitrous oxide may be lost as a resul t of leaks, a frozen regula tor, improper
maintenance, deplet ion of the system supp ly, and del iberate tampering with the
equipment (51,631,632,633). Cylinder supplies also can fail . An obstruc tion or leak

in the anesthes ia mach ine may cause decreased nitrous oxide f low (634). Another
potential problem is inadvertently us ing ai r instead of nitrous oxide (635).
Unexpectedly High Oxygen Concentration I f a connection between the n itrous oxide and oxygen sources occurs in the
pipel ine sys tem, a mixer, or the anesthesia machine, and the oxygen pressure is
higher than tha t of ni trous oxide, oxygen wil l f low into the ni trous oxide l ine
(636,637).
Accidental ac tivation of the oxygen f lush may occur (490,493,638,639,640,641).
Repeatedly using the oxygen f lush to keep the reservoir bag f i l led can lead to
patient awareness (491,642,643). Damage to the oxygen f lush valve can cause it to
leak oxygen into the f resh gas (644).
On some electronic machines, a machine problem wil l cause i t to switch into a “safe
mode” where only oxygen is delivered (645).
Air Entrainment As discussed earl ier in this chapter, a ir entrainment can cause dilu tion of inha led
anesthet ic agents.
P.419
Faulty Vaporizer Vaporizer leaks and prob lems wi th the mounting or interlock device are relatively
common
(630,646,647,648,649,650,651,652,653,654,655,656,657,658,659,660,661,662,663,
664). Such a leak of ten does not occur unt i l the vaporizer is turned ON. Therefore,
i t is essential that the preuse checking procedure for leaks be performed with the
vaporizers turned ON (Chapter 33).
Whi le the overf il led vaporizer has usually been associated with a h igher-than-
expected vapor ou tput, there is one reported case where it was associated with no
vapor ou tput (665).
Empty Vaporizer Another cause of underdosage is a vaporizer that runs empty (627). Cases have
been reported in wh ich a l iquid level was v is ible in the vaporizer s ight g lass
al though the vaporizer was empty (666). In one report, a fragment of rubber
obstructed the channel f rom the lower end of the l iquid level indica tor, showing a

l iquid level despi te the vaporizer being empty (667). Some electronic vaporizers wi l l
ac tivate an alarm when the l iquid level reaches a certain point.
Incorrect Agent in Vaporizer I f a vaporizer that is designed for use wi th a high ly vola ti le agent is fi l led wi th an
agent of low volati l i ty , the pat ient wi l l fail to receive the concentrat ion expec ted
(615,616). An example is plac ing enflurane in a vaporizer that is des igned fo r
isof lu rane.
Incorrect Vaporizer Setting An incorrect vaporizer sett ing can be a cause of anesthet ic underdosage. I t is
importan t to check se tt ings frequently during a case because they can be al tered
wi thout the operator's knowledge. It is not uncommon to forget to turn ON a
vaporizer af ter f i ll ing it during use. I f an anesthesia mach ine is tu rned OFF and
then tu rned ON again, the vaporizer sett ing may defaul t to zero (428).
Anesthetic Agent Breakdown The reac tion between some desiccated absorbents and sevoflurane (Chapter 9) can
be so rapid and ex tensive tha t it is dif f icul t to main tain a sat is factory inspired
concentration . If there is a large discrepancy between the vaporizer setting and the
agent level in the breathing sys tem, anesthetic breakdown shou ld be considered.
Inadvertent Exposure to Volatile Agents I t is possible that halothane-related hepati tis or mal ignant hyperthermia may be
triggered by small amounts of agent p resent in a machine and breathing system
even if the vaporizers are tu rned OFF (661,668,669,670,671,672,673,674). When a
patient wi th a history or suspicion of one of these ent i ties must be anesthetized,
the anes thesia machine should be prepared for use by removing all vaporizers i f
possible (673). Other necessary act ions inc lude changing the absorbent, replacing
the fresh gas supp ly hose, us ing new tub ings and bag, and f lushing wi th a high f low
of oxygen for a prolonged time (675,676,677,678,679,680).
Should an episode of malignant hyperthermia occur during adminis trat ion of
anesthesia and the department has a machine f rom which vaporizers have been
removed and tha t has been thoroughly flushed of vola ti le agents, i t should be
subst ituted fo r the machine in use. A fresh breathing system should be used. If the
department does not have such a mach ine, the fol lowing measures should be taken
to reduce the inhaled concentration of volati le anesthet ic (675,677):
• Change the breathing system hoses and bag.
• Change the fresh gas supply hose.
• Change the absorbent.
• Use very high oxygen f lows.
• Insert a charcoal f il ter on the inspiratory port of the absorber.
• Avoid using a contaminated vent i lator.
• Remove vaporizers from the machine if possible.
Inadvertent anes thetic agent exposure can occur i f the anesthesia machine is used
to deliver oxygen to a pa tient undergoing loca l or MAC anesthesia if the f resh gas
delivery port or the pat ient port of the breathing system is used to del iver oxygen to
a nasal cannula. If a vaporizer is inadvertently tu rned ON, the patient may become
deeply sedated or anes thetized wi th the agent (681,682). These problems can be
avoided by using the aux il ia ry f lowmeter on the anesthes ia machine, an oxygen
f lowmeter attached to the pipel ine system, or a cylinder as the oxygen source.
Physical Damage Older anesthes ia machines of ten have equ ipment added to the top of the machine.
This may resul t in the machine becoming top heavy. If the equipment contacts a
ce il ing column or other s tructure, equipment may be knocked onto the f loor or
personnel . Whi le newer anesthesia mach ines have a generally lower prof ile and
tend to include many of the moni to ring dev ices tha t are o ften placed on the top of
older machines , it is s ti l l poss ible to do physical damage to the machine.
Another hazard to anes thesia equipment is the presence of wires and tubings on
the f loor. These make i t more l ikely that the machine wi l l tip during movement,
spewing equipment to the floor. Many machines come
P.420
wi th op tiona l arms that hold breathing system hoses, tubings, and wires off the
f loor. A number of devices have been manufactured to move the impediments from
the machine wheels (683,684,685,686) (Fig. 14.16). The cas tors on a machine can
break , causing the anesthes ia machine to tip over (687).

View Figure
Figure 14.16 A: If the machine's wheels go over the hose, the machine will be tipped and the line blocked. B: This device allows easier movement of the machine by pushing hose out of the way. (Picture courtesy of CASTrGard.)
Electromagnetic Interference Over the past few decades, the number of wireless radio frequency (RF)
transmitters in medical fac il i ties has increased dramatica lly (688,689,690,691).
Wireless computer ne tworks , paging systems, handheld radios, cellula r telephones,
and o ther RF transmitters, wh ich are sources of electromagnetic energy, have
become prevalent in c linical envi ronments. In the future , it is l ikely that moni tors
and o ther devices wil l be connec ted to the data management system through a
wi reless connection. These produce electromagnetic radiat ion even when the
device is in standby mode, as they constantly send s ignals to the base station .
I t has long been recognized that equipment that emits radio waves can in terfere
wi th the operat ion of electronic medical equipment (electromagnetic in terfe rence or
EMI). The extent of the prob lem is unknown. Availab le c l inical data indicate that
serious malfunctions are rare (689). Equipment reported being affected inc ludes
moni tors , venti la to rs, and infusion pumps. The risk of interfe rence depends on
transmission power and f requency, dis tance to the transmitter, and immuni ty
(cons truction) of the medical dev ice.
The wide variety of RF transmitters and medica l dev ices used in and around heal th
care fac i li ties makes inte rac tions dif ficul t to predic t. A reas such as the operating
room and crit ical care areas , which have a h igh concentrat ion of electronic medical
devices, a re most l ikely to be affected by EMI. Diagnostic , moni toring, and
therapeutic equipment that is direct ly attached to pa tients is part icularly susceptible
to EMI.

To help prevent EMI, newer medical devices are manufac tured to enhance their
immuni ty to, or compatibil i ty wi th , external sources of electromagnetic energy.
Newer cel l phones and newer equipment offer better shielding to mitigate or
prevent electromechanical interference. Older med ical equipment is of more
concern because i t may not have been designed to be immune to the increasing ly
complex electromagnetic envi ronment that can be found in heal th care fac il i t ies.
For most RF transmitters , the f ield s trength dec reases wi th distance. I t follows that
in general , the greater the separat ion between a RF transmitter and a medical
device, the lower the RF exposure to the device, and the lower the potent ial for
EMI.
Careful considerat ion must be given to weighing the risks and benef i ts of wireless
equipment used in and around health care fac il i ties to determine whether i t can be
used safely and effec tively. Unless each medical device is tes ted for immuni ty to
each RF transmitter, i t is dif f icul t to identify which devices may be affec ted by a
part icula r transmitte r and what transmiss ion condi t ions are l ikely to cause
inte rference.
Since the time that cel lular telephones were introduced, health care organizat ions
have struggled to determine a prudent pol icy fo r their use in c linical settings . Some
faci li t ies have banned the use of cel lu lar telephones on their premises . Others
al low them to be used f ree ly, whereas others have banned the ir use in certain
areas or within a certain dis tance of medical equipment (688).
Al though appropriate medical device design and test ing for elec tromagnetic
compatibi l i ty (EMC) can
P.421
reduce potential EMI risks in the c linica l env ironment, they cannot ensure that a
device wil l no t experience problems. Under certain c ircumstances, EMI can st i l l
occur, even i f the dev ice conforms to current EMC standards. Therefore , di rec t or
c lose contact between the medical device and wire less communica tion devices
should be avoided. Wireless phones in public areas do not appear to cause
problems (690). Periodical test ing of wireless transmitt ing dev ices and medica l
equipment wi l l be required to ensure a safe env ironment.
Accident Investigation
Any t ime a pat ient has an unexplained problem, equipment malfunct ion or misuse
should be suspected, and the apparatus should not used again unt il this has been
disproved (692,693,694,695,696).
When there has been a patient injury, the health care fac il i ty safety off icer (or r isk
manager) should be contacted at once to superv ise investigat ion of the incident. An
es tablished pro tocol should be designed and followed so tha t all important areas
are systematical ly covered. All indiv iduals involved in the inc ident should document
their observations soon af te r the event whi le detai ls a re sti l l f resh in their minds.
This should be a s imple statement of facts, wi thout judgments about causali ty or
responsibi li ty .
The fol lowing quest ions need to be asked:
• What was the date and time of the prob lem?
• In what area did the problem occur?
• What monitors were being used?
• What were the set a larm l imits?
• What was the f irs t ind ica tion that there was a problem?
• At what t ime did the problem occur?
• Who f i rs t no ted the problem?
• What changes attracted attention? Were any alarms act ivated?
• What s igns or symptoms did the pat ient exhibit?
• Had there been any recent mod if ications to the electrical system or gas
pipel ines in tha t area?
• Was anyth ing al tered shortly before the inc ident?
• Was this the f i rs t case perfo rmed in tha t area on tha t day?
• Were there any problems during previous cases performed in that area on
that day or on the previous day?
• Were there any unusual occurrences in o ther areas on that day or on the
previous day?
• Had any equipment been moved in to that area recently? Were there any
problems noted in the room where it was prev iously used?
• What preuse anesthesia equipment checks were made?
• Who last f il led the vaporizers on the anesthes ia machine?
• I f a vaporizer was recent ly attached to the machine, were precautions taken
to prevent l iquid from being spi l led into the outf low trac t?

• Af ter the ini tial indica tion that a problem had occurred, what was the
sequence of events?
An importan t s tep involves construction of a t ime l ine, on wh ich all events are l is ted
in chronological order (692). This wi l l help to sort out events and may lead to
identif icat ion of miss ing data. Trend data f rom moni tors or a data management
system can help.
Numerous photographs should be taken of the area from various angles , wi th al l
equipment s i tuated where it was at the time of the inc ident. Each p iece of
equipment should be photographed separa tely.
Af ter pic tu res have been taken, al l suppl ies and equipment assoc iated wi th the
case should be saved and sequestered in a secure loca tion and labe led “DO NOT
DISTURB.” Settings should not be changed. Re levant identifying information such
as the manufac turer and lot and/or serial numbers shou ld be recorded.
I f af ter a ll this has been done i t appears possible that the equipment may be
implica ted in causing the problem, a thorough inspect ion of the equipment by an
uninvolved third party in the presence of the primary anesthes ia personnel ,
insurance carrier, heal th care faci l i ty safety off icer, pat ient representa tive, and
equipment manufacturers should be conducted. The invest igation should consist of
an in-depth examination of the equipment s imilar to the checking procedures
described earlier in this chapter. Vaporizers should be calibrated and checked to
determine if vapor is del ivered in the OFF pos it ion. An analys is shou ld be made of
the vaporizers ' contents, i f necessary. Following the investigation, a report should
be made, detail ing all facts, analyses, and conc lus ions.
I f a problem wi th the equ ipment is found, an a ttempt should be made to reconstruct
the accident, if this can be done without danger to anyone, and the equipment
should again be locked up unti l any li tiga tion is settled. If the invest igat ion reveals
no problems, the equipment can be re turned to serv ice with the consent of all
part ies .
Problem Reporting In the Uni ted Sta tes, the Center fo r Device and Radiological Heal th (CDRH) of the
Food and Drug Admin istration (FDA) receives postmarket adverse event reports
submitted by manufacturers, user fac il i ties , hea lth care
P.422

professionals , and consumers involv ing death, serious injury, or i l lness and produc t
malfunct ions (698,699). The FDA analyzes the reports to determine the impact on
the publ ic heal th and makes recommendations to manufacturers, heal th care
professionals , and consumers . MedWatch is the FDA's name for i ts medical
products report ing program. I t is a broad program that encompasses both voluntary
and mandatory report ing for medical products.
User facil i ties are required to report to the FDA medical device problems tha t have
or may have caused or contribu ted to death, serious i l lness, o r serious in ju ry.
Serious i l lness or in ju ry is def ined as life -threatening or resul ting in permanent
impairment of a body funct ion or permanent damage to a body structure or tha t
necessitates immedia te medica l or surgica l inte rvention to prevent damages to the
body.
User facil i ties mus t report a prob lem no later than 10 days after becoming aware of
i t. Failure to report accurately and in a timely manner can lead to c iv il o r even
criminal penalt ies. Problems resul ting in patient deaths are to be sent to the FDA
and to the equipment manufacturer. Serious i l lness or injury events are reported to
the manufacturer or, i f the manufacturer is not known, to the FDA. The
manufac turer has the respons ibil i ty to invest iga te the incident and, if appropriate,
report the inc ident to the FDA. Adverse events, inc lud ing those in which a dev ice
failed to performed as intended but did not resul t in a death or serious injury may
also be reported voluntari ly through the FDA's MedWatch program.
Reports sha ll not be admitted into evidence or otherwise used in a c iv il act ion
unless the fac i l i ty or personnel making the report knew that the information was
false. There are a number of ways that the information could become available,
including the Freedom of Information Act. It is therefore possible tha t th is
info rmation could be available for a c iv i l suit (698).
The user faci l i ty shou ld se t up a pro tocol for handl ing adverse inc idents in order
that they wi l l be properly reported in a timely fashion. Medical personnel need to
know who (the heal th care fac il i ty safety off icer, risk management, b iomedical
department, or other des ignated personnel) should receive the report.
References 1. Cooper JB, Newbower RS, Long CD, e t al . Preventab le anesthesia mishaps : a
study of human factors. Anesthesiology 1978;49:399–406.
[Fu ll text Link]

[CrossRef]
[Med line Link]
2. Cooper JB, Newbower RS, Kitz RJ. An analysis of major e rrors and equipment
failures in anesthesia management. Considerat ions fo r prevention and detection.
Anesthesiology 1984;60:34–42.
[Fu ll text Link]
[CrossRef]
[Med line Link]
3. Craig J, Wi lson ME. A survey of anaes thetic misadventures . Anaesthesia
1981;36:933–936.
[CrossRef]
[Med line Link]
4. Currie M. A prospective survey of anaes thetic crit ical events in a teaching
hospi tal. Anaesth In tens Care 1989;17:403–411.
[Med line Link]
5. Desmonts JM. Ro le of equipment fai lure in the causation of anaes thetic morbidity
and mortali ty: resul ts from the French national survey and comparison wi th the
Bos ton s tudy. Eur J Anaes th 1987;4:200–203.
6. Kumar V, Barcellos WA, Mehta MP, et al. Analys is of c ri tical incidents in a
teaching department for qua li ty assurance. A survey of mishaps during
anaesthesia . Anaesthesia 1988;43:879–883.
[Med line Link]
7. Short TG, O'Regan A, Lew J, et a l. Cri tical inc ident report ing in an anaesthet ic
department qual i ty assurance programme. Anaes thesia 1992;47:3–7.
8. Fast ing S , Gisvold SE. Equ ipment problems during anaesthesia—are they a
quali ty p roblem? Br J Anaes th 2002;89:825–831.
9. Grant LJ. Regulations and safety in medica l equipment design. Anaesthes ia
1998;53:1–3.
[Fu ll text Link]
[CrossRef]
[Med line Link]
10. Short TG, O'Regan A , Jauyasuriya JP, et al . Improvements in anaes thetic care
resul ting f rom a crit ical incident reporting programme. Anaesthes ia 1996;51:615–
621.
[Fu ll text Link]
[CrossRef]

[Med line Link]
11. Caplan RA, Vist ica MF, Posner KL, et al. Adverse anes thetic outcomes aris ing
f rom gas delivery equ ipment. A c losed c laims analys is. Anesthesiology 1997;87:
741–748.
[Fu ll text Link]
[CrossRef]
[Med line Link]
12. Sprague DH, Archer GW. In traoperat ive hypoxia from an erroneously f i l led
l iquid oxygen reservoir. Anesthesiology 1975;42:360–363.
[Fu ll text Link]
[CrossRef]
[Med line Link]
13. Hol land R. Foreign correspondence: “wrong gas” disaster in Hong Kong. APSF
News le tt 1989;4:26.
14. Bernstein D, Rosenberg A . Intraoperat ive hypoxia f rom nitrogen tanks wi th
oxygen f it t ings. Anesth Analg 1997;84:225–227.
[Fu ll text Link]
[CrossRef]
[Med line Link]
15. FDA Public Health Adv isory. Potent ia l fo r in jury from medical gas connections
of c ryogenic vessels, Augus t 9, 2001.
16. Smith FP. Mul t iple deaths f rom argon contamination of hosp ital oxygen supply.
J Forens ic Sci 1987;32:1098–1102.
[Med line Link]
17. Anonymous . O2-N2O mix -up leads to probe in to deaths of two patien ts. Biomed
Safe Stand 1981;11:123–124.
18. Anonymous . Argon-oxygen tank mixup causes th ree deaths at army hospital .
Biomed Safe Stand 1983;13:88–89.
19. Anonymous . Nitrogen in oxygen sys tem kil ls two. Biomed Safe Stand
2001;31:17.
20. Emmanuel ER, Teh JL. Dental anaesthet ic emergency caused by medical gas
pipel ine installat ion error. Aust Dent J 1983;28:79–81.
[Med line Link]
21. Sato T. Fatal pipe line accidents spur Japanese standards. APSF Newslett
1991;6:14.
22. Anonymous . Medical gas/vacuum sys tems. Technol Anesth 1987;7 :1–2.

23. Anonymous . Crossed gas lines alleged in O.R. death. Biomed Safe Stand
1989;19:4.
24. McAleavy JC. Bel ieve your moni to rs. Anesthesiology 1993;79:409–410.
[Fu ll text Link]
[CrossRef]
[Med line Link]
25. Elizaga AM, Frerichs RL. Nitrogen purging of oxygen pipel ines: an unusual
cause of intraoperative hypox ia . Anes th Ana lg 2000;91:242–243.
[Fu ll text Link]
[CrossRef]
[Med line Link]
26. Carley RH, Houghton IT, Park GR. A near d isaster f rom piped gases.
Anaesthesia 1984;39:891–893.
[CrossRef]
[Med line Link]
27. Karmann U, Roth F. Prevention of accidents associated wi th ai r-oxygen mixers.
Anaesthesia 1982;37:680–682.
[CrossRef]
[Med line Link]
28. Thorp JM, Rai l ton R. Hypox ia due to ai r in the oxygen pipel ine. Anaesthes ia
1982;37:683–687.
[CrossRef]
[Med line Link]
29. Ziecheck HD. Fau lty venti la tor check valves cause pipeline gas contamination .
Respir Care 1981;26:1009–1010.
30. Weightman WM, Fenton-May V, Saunders R, et al . Funct ional ly crossed
pipel ines. An intermit tent condi tion caused by a faul ty venti lator. Anaes thesia
1992;47:500–502.
[CrossRef]
[Med line Link]
31. Shaw R, Beach W, Metz le r M. Medical ai r contaminat ion with oxygen associated
wi th the Bear 1 and 2 vent ilators. Crit Care Med 1988;16:362.
[CrossRef]
[Med line Link]
32. Anonymous . Overv iew of oxygen-air proport ioners . Technol Anesth 2000;20:1–
3.

33. Kane W, Ridley JD, Sheehan MW, et al. Contaminat ion of the medical ai r supply
wi th oxygen. A c linica l engineering inc ident invest igat ion. J Cl in Eng 1990;15:295–
300.
[Med line Link]
34. Miyasaka K . Oxygen supp ly pressure should be the highest. Anaesth In tens
Care 1989;17:513–514.
[Med line Link]
35. Tingay MG, I ls ley AH, Will is RJ, e t al . Gas ident i ty hazards and major
contamination of medical gas system of a new hospi tal. Anaesth In tens Care
1978;6:202–209.
[Med line Link]
36. Anonymous . Nitrogen distribut ion systems. Technol Anesth 1989;9 :2.
37. Anonymous . Old-style Chemetron centra l gas outlets. Health Devices
1981;10(9):222–223.
38. Anonymous . Crossed connec tions in medical gas systems. Techno l Anes th
1984;5:3 .
39. Anonymous . Crossed N2O & O2 l ines blamed fo r outpatient surgery death .
Biomed Safe Stand 1992;22:14.
40. Downing JW. Safety of anaesthetic machines. South Af r Med J 1981;30:815.
[Med line Link]
41. Krenis LJ, Berkowitz DA. Errors in instal la tion of a new gas del ivery system
found af ter certif ication . Anes thesiology 1985;62:677–678.
[Fu ll text Link]
[CrossRef]
[Med line Link]
42. Lane GA. Medical gas out le ts—a hazard f rom interchangeable “quick connect”
couplers . Anesthesiology 1980;52:86–87.
[Fu ll text Link]
[CrossRef]
[Med line Link]
43. Scamman FL. An analys is of the factors leading to crossed gas l ines causing
profound hypercarbia during general anesthes ia. J Cl in Anesth 1993;5 :439–441.
[CrossRef]
[Med line Link]
44. Anonymous . Misconnect ion of O2 l ine to CO2 out le t claimed in death. Biomed
Safe Stand 1991;21:92–93.

45. Anonymous . Pat ients asphyxia ted by medical gas misconnect ions. Biomed Safe
Stand 2002;32:57–58.
46. Anonymous . Oxygen f lowmeters: report of death caused by misconnected
f lowmeter. Health Devices A lerts 2005;29:3.
47. Anonymous . Fatal gas l ine mix -up: how to avoid making the “gas tly” mistake.
Inst itute for Safe Medication Pract ices, December, 2004.
http :/ /www.ismp.org/MSAart ic les/GasPrin t.htm (accessed).
48. Barnow E, Browne G. Fau lty ni trous ox ide Schraeder valve. Anaes thesia
1997;52:392–393.
[Fu ll text Link]
[Med line Link]
49. Spurring PW, Shenol ikar BK. Hazards in anaes thetic equ ipment. Br J Anaes th
1978;50:641–645.
[CrossRef]
[Med line Link]
50. Robinson JS. A cont inuing saga of piped medica l gas supply. Anaes thesia
1979;34:66–70.
[CrossRef]
[Med line Link]
51. Feeley TW, Hedley-Whyte J. Bulk oxygen and ni trous oxide del ivery systems:
design and dangers. Anesthesiology 1976;44:301–305.
[Fu ll text Link]
[CrossRef]
[Med line Link]
52. Anonymous . The Westminster inquiry. Lancet 1977;2:175–176.
[CrossRef]
[Med line Link]
53. Dinnick OP. Medical gases—pipel ine problems. Eng Med 1979;8:243–247.
[CrossRef]
[Med line Link]
54. Neubarth J. Another hazardous gas supply misconnection. Anesth Analg
1995;80:206.
[Fu ll text Link]
[CrossRef]
[Med line Link]

55. Jardine DS. An epidemic of hypoxemia in two intensive care un its : cause and
human response. Anesthesiology 1992;77:1038–1043.
[Fu ll text Link]
[CrossRef]
[Med line Link]
56. O'Connor CJ, Hobin KF. Bypassing the diameter-indexed safety system.
Anesthesiology 1989;71:318–319.
[Fu ll text Link]
[CrossRef]
[Med line Link]
P.423
57. Anonymous . Pat ient receives air instead of oxygen: Canadian safe ty alert.
Biomed Safe Stand 1991;21:97–98.
58. Anonymous . Gas f lowmeters. Technol Anesth 1991;12:7–8.
59. Waite A, Macartney I . Ai r-oxygen f lowmeter confusion. Anaes thesia
2003;58:194–195.
[Fu ll text Link]
[CrossRef]
[Med line Link]
60. Boon PE. C-s ize cy linders . Anaesth Intens Care 1990;18:586–587.
[Med line Link]
61. Jawan B, Lee JH. Cardiac arrest caused by an incorrec tly f i l led oxygen cyl inder.
A case report. Br J Anaesth 1990;64:749–751.
[CrossRef]
[Med line Link]
62. Ward PM, Platt MW. Inappropria te f i l l ing of cyl inders. Anaesthesia
1992;47:544.
[CrossRef]
63. Boon PE. C-s ize cy linders . Anaesth Intens Care 1990;18:586–587.
[Med line Link]
64. Menon MRB, Lett Z. Incorrectly f i l led cyl inders. Anaesthes ia 1991;46:155–
156.
[CrossRef]
[Med line Link]

65. Hol land R. Foreign correspondence. Another “wrong gas” inc ident in Hong
Kong. APSF News le tt 1991;6:9.
66. Rende ll -Baker L . Problems with anes thetic gas machines and their so lu tions. In:
Rendel l-Baker L, ed . Problems with anes thetic and respiratory therapy equipment.
Int Anesth Cl in 1982;20(3):1–82.
67. Anonymous . Cylinders with unmixed helium/oxygen. Techno l Anes th
1990;10:4.
68. Orr IA, Hami l ton L. Entonox hazard. Anaesthes ia 1985;40:496.
[Med line Link]
69. Sim P. Entonox hazard: a reply. Anaes thesia 1985;40:496.
[Med line Link]
70. Anonymous . Misconnect ion of oxygen regulator to n itrogen cylinder could cause
death . Biomed Safe S tand 1988;18:90–91.
71. Anonymous . Nons tandard user modif icat ion of gas cy linder pin indexing.
Technol Anes th 1989;10:2.
72. Goebe l WM. Fai lu re of n itrous oxide and oxygen pin-indexing. Anesth Prog
1980;27:188–191.
[Med line Link]
73. Jayasuriya JP. Another example of Murphy's law—mix up of p in index valves.
Anaesthesia 1986;41:1164.
[CrossRef]
74. Mead P. Hazard wi th cyl inder yoke. Anaes th In tens Care 1981;9:79–80.
75. Anonymous . Medical gas safety: read the labels! They're the only sure identif ie r
of gas cyl inder contents. Technol Anesth 2001;21:1–3.
76. Anonymous . Hazard: improper attachment of an anesthesia gas cy linder to the
yoke. Med Devices Surveil lance 1990;4 :S5—S6.
77. Eul iano TY, Lampotang, Hardcast le JF. Pat ient s imulator identi fies faul ty H-
cylinder. J Clin Monit 1995;11:394–395.
[CrossRef]
[Med line Link]
78. Arapal li N, Jones N. Oxygen or ai r? Anaesthesia 2001;56:1205.
79. Anonymous . Medical gas cyl inders. Technol Anesth 2002;22:10.
80. Chamley D, Trethowen L. Pin index failu re. Anaes th Intens Care 1993;21:128–
129.
[Med line Link]
81. Thomas AN, Hurs t W, Saha B. Interchangeab le oxygen and ai r connectors.
Anaesthesia 2001;56:1205–1206.
[Fu ll text Link]
[Med line Link]
82. Saha B, Thomas AN, Tufchi A. Interchangeab le oxygen and carbon dioxide in
oxygen cylinders . Anaesthesia 2005;60:827–828.
[Fu ll text Link]
[CrossRef]
[Med line Link]
83. MacMi llan RR, Marshall MA. Fai lu re of the pin index system on a Cape Waine
venti lato r. Anaes thesia 1981;36:334–335.
[CrossRef]
[Med line Link]
84. Ful le r WR, Kel ly R, Russe ll WJ. Pin-index ing failure . Anaesth Intens Care
1985;13:440–441.
[Med line Link]
85. Youatt G, Love J. A funny yoke: tale of an unscrewed pin. Anaes th Intens Care
1981;9:178.
[Med line Link]
86. Bonsu AK, Stead AL. Accidental c ross-connexion of oxygen and ni trous ox ide in
an anaesthet ic machine. Anaes thesia 1983;38:767–769.
[CrossRef]
[Med line Link]
87. Beudoin MG. Oxygen needle valve obs truct ion. Anaesth In tens Care
1988;16:130–131.
[Med line Link]
88. Khal i l SN, Neuman J. Fai lure of an oxygen flow control valve. Anesthesiology
1990;73:355–356.
[Fu ll text Link]
[CrossRef]
[Med line Link]
89. Rung GW, Schneider AJL. Oxygen f lowmeter failure on the North American
Drager Narkomed 2a anesthesia machine. Anes th Analg 1986;65:211–212.
[Med line Link]
90. Anonymous . Oxygen deprivation a lleged in $2.5 mil l ion negligence su it . Biomed
Safe Stand 1981;11:53.
91. McGarry PMF. Anaes thetic machine standard. Can Anaesth Soc J
1978;25:436.
[Med line Link]
92. Wyant GM. Some dangers in anaesthesia. Can Anaes th Soc J 1978;25:71–72.
[Med line Link]
93. Jenk ins IR. A “too c lose to door” knob. Anaesth In tens Care 1991;19:614.
[Med line Link]
94. Saunders DI, Meek T. Almost 30% of anaes thetic machines in UK do not have
anti -hypoxia device. BMJ 2001;323:629.
[Fu ll text Link]
[Med line Link]
95. Richards C. Failure of a nitrous oxide-oxygen proport ioning device .
Anesthesiology 1989;71:997–999.
[Fu ll text Link]
[CrossRef]
[Med line Link]
96. Goodyear CM. Failure of ni trous oxide-oxygen proportioning device.
Anesthesiology 1990;72:397–398.
[Fu ll text Link]
[CrossRef]
[Med line Link]
97. Lohmann G. Faul t wi th an Ohmeda Excel 410 machine. Anaesthesia
1991;46:695.
[CrossRef]
[Med line Link]
98. Kidd AG, Hal l I. Faul t wi th an Ohmeda Exce l 210 anaesthet ic machine.
Anaesthesia 1994;49:83.
[CrossRef]
[Med line Link]
99. Ishikawa S, Nakazawa K, Maki ta K. Hypox ic gas f low caused by mal funct ion of
the proportioning system of anes thesia machines. Anes th Analg 2002;94:1672.
[Fu ll text Link]
[CrossRef]
[Med line Link]
100. Dav ies R. Faul t wi th an Ohmeda Excel 210 anaesthesia machine. Anaesthes ia
1994;49:83.
[CrossRef]
101. Paine GF, Kochan JJI. Failure of the chain-l ink mechan ism of the Ohmeda
Excel 210 anes thesia machine. Anesth Analg 2002;94:1374.
[Fu ll text Link]
[CrossRef]
[Med line Link]
102. Sharma ML. Problem with Ohmeda Excel 210 SE anesthet ic machine. Can J
Anesth 2002;49:438–439.
103. Cheng CJC, Garewal DS. A fai lure of the chain-l ink mechanism on the Ohmeda
Excel 210 anes thetic machine. Anes th Ana lg 2001;92:913–914.
[Fu ll text Link]
[CrossRef]
[Med line Link]
104. Ferguson S, Whi te E. An unusual and dangerous anaes thetic machine fai lu re.
Anaesthesia 1997;52:283–284.
[Fu ll text Link]
[Med line Link]
105. Gordon PC, Janes MFM, Lapham H, et al . Fai lu re of the proport ioning system
to prevent hypoxic mixture on a Modulus II Plus anesthes ia mach ine.
Anesthesiology 1995;82:598–599.
[Fu ll text Link]
[CrossRef]
[Med line Link]
106. Henl ing CE, Diaz JH. The c luttered anesthesia machine—a cause for hypoxia.
Anesthesiology 1983;58:288–289.
[Fu ll text Link]
[CrossRef]
[Med line Link]
107. Linton RAF, Foster CA, Spencer GT. A potent ia l hazard of oxygen f lowmeters.
Anaesthesia 1982;37:606–607.
[CrossRef]
[Med line Link]
108. Walpitagama R. Del ivery of 100% ni trous oxide by Ulco El i te 615 anaes thetic
machine. Anaesth Intens Care 2005;33:693.
[Med line Link]

109. Brooks M, Sc rimshaw K. Delivery of 100% nitrous oxide by Ulco El ite 615
anaesthetic machine—reply. Anaesth Intens Care 2005;33:693–694.
110. Russell WJ. The danger of ai r on anaesthetic machines . Anaesth Intens Care
1988;16:499.
111. Battig CG. Unusual fai lure of an oxygen flowmeter. Anesthesiology
1972;37:561–562.
[Fu ll text Link]
[CrossRef]
[Med line Link]
112. Chadwick DA. Transposi tion of rotameter tubes . Anes thesiology
1974;40:102.
[Fu ll text Link]
[CrossRef]
[Med line Link]
113. Hodge EA. Accuracy of anaesthetic gas f lowmeters. Br J Anaes th
1979;51:907.
[CrossRef]
[Med line Link]
114. Kel ley JM, Gabel RA. The improperly cal ib rated f lowmeter—another hazard.
Anesthesiology 1970;33:467–468.
[Fu ll text Link]
[CrossRef]
115. Thomas D. In terchangeable rotameter tubes . Anaesth Intens Care
1983;11:385–386.
[Med line Link]
116. Szocik JF. Preoperat ive hypoxemia. Anesth Analg 1993;76:681–682.
[Fu ll text Link]
[CrossRef]
[Med line Link]
117. Ai tkenhead AR. The pattern of l i t iga tion aga inst anaesthet is ts . Br J Anaesth
1994;73:10–21.
[CrossRef]
[Med line Link]
118. Chung DC, J ing QC, Prins L , et al . Hypoxic gas mixtures delivered by
anaesthetic machines equipped wi th a downstream oxygen f lowmeter. Can Anaes th
Soc J 1980;27:527–530.

[Med line Link]
119. Dudley M, Walsh E. Oxygen loss f rom rotameter. Br J Anaes th 1986;58:1201–
1202.
[CrossRef]
[Med line Link]
120. Russell WJ. Hypoxia from a select ive oxygen leak. Anaesth In tens Care
1984;12:275–276.
[Med line Link]
121. McHale S. A crit ical inc ident wi th the Ohmeda Excel 410 machine. Anaes thesia
1991;46:150.
[CrossRef]
[Med line Link]
122. Powell J . Leak f rom an oxygen flow meter. Br J Anaesth 1981;53:671.
[CrossRef]
[Med line Link]
123. Wishaw K. Hypoxic gas mixture wi th Quantif lex monitored dial mixer and
induction room safety. Anaesth Intens Care 1991;19:127.
[Med line Link]
124. Lenoir RJ, Easy WR. A hazard associated with removal of carbon diox ide
cylinders. Anes thesiology 1988;43:892–893.
125. McQui l lan PJ , Jackson IJB. Potent ial leaks f rom anaesthet ic machines.
Anaesthesia 1987;42:1308–1312.
[CrossRef]
[Med line Link]
126. Will iams AR, Hil ton PJ. Selec tive oxygen leak . A potent ial cause of pat ient
hypoxia. Anaes thesia 1986;41:1133–1134.
[CrossRef]
[Med line Link]
127. Wilson A. Dangerous leak. Anaesth Intens Care 1990;18:575.
[Med line Link]
128. Stoneham MD, Ismail F, Sansome AJ. Leakage of fresh gas from vacant CO2
cylinder yoke. Br J Anaesth 1993;48:730–731.
129. Russell EC, Derbyshire DR. More hidden leaks. Anaesthes ia 2001;56:597–
598.
[Fu ll text Link]
[CrossRef]
[Med line Link]
130. Lan ier WL. In traoperat ive ai r entrainment wi th Ohio Modulus anesthes ia
machine. Anesthesiology 1986;64:266–268.
[Fu ll text Link]
[CrossRef]
[Med line Link]
131. Ghanooni S, Wilks DH, F inestone SC. A case report of an unusual
disconnection. Anes th Ana lg 1983;62:696–697.
[Fu ll text Link]
[CrossRef]
[Med line Link]
132. Eisenk raft , JB. Complica tions of anes thesia delivery systems. ASA Annual
Ref resher Courses, 1996, New Orleans.
133. Walker T. Another p rob lem wi th a ci rc le system. Anaesthesia 1996;51:89.
[Fu ll text Link]
[CrossRef]
[Med line Link]
134. Beh T. A design fau lt of the Drager Cato anaes thesia workstation . Anaesth
Intens Care 2006;34:125.
[Med line Link]
135. Murphy E, Wi ll is S . Awareness and hypoxia risk wi th Drager Cato and Fabius
anaesthesia machines. Anaes th Intens Care 2004;32:721–722.
[Med line Link]
136. Mostello LA, Patel RI. Di lu tion of anesthetic gases by a new l ight source for
bronchoscopy. Anes thesiology 1986;65:445.
[Fu ll text Link]
[CrossRef]
[Med line Link]
137. Sandberg WS, Kaiser S. Novel breath ing c ircui t archi tecture : new
consequences of old problems. Anesthesio logy 2004;100:755–756.
[Fu ll text Link]
[CrossRef]
[Med line Link]
138. Rigg D, Joseph M. Spl i t venti lato r bellows. Anaesth In tens Care
1985;13:213.
[Med line Link]

139. Waterman PM, Pautler S, Smith RB. Accidental vent ilator-induced
hyperventi lat ion. Anesthes iology 1978;48:141.
[Fu ll text Link]
[CrossRef]
[Med line Link]
140. Baraka A, Muallem M. Awareness during anaes thesia due to a venti lato r
malfunct ion. Anaesthesia 1979;34:678–679.
[CrossRef]
[Med line Link]
141. Longmuir J , Craig DB. Inadvertent inc rease in insp ired oxygen concentration
due to defect in venti lato r bel lows. Can Anaesth Soc J 1976;23:327–329.
[Med line Link]
142. Love JB. Misassembly of a Campbel l venti la tor causing leakage of the driv ing
gas to a pat ient. Anaes th Intens Care 1980;8:376–377.
143. Marsland AR, So lomos J . Venti la tor malfunc tion detec ted by O2 analyser.
Anaesth Intens Care 1981;9 :395.
[Med line Link]
144. Whi te DC, Royston BD. Oxygen di lu tion in “trunk” venti lation of c ircle sys tems
(part 2). Br J Anaes th 1994;73:720P–721P.
145. Dalley P, Robinson B, Wel ler J , et a l. The use of high f idel ity human patient
s imulat ion and the introduction of new anaesthesia de livery sys tems. Anesth Analg
2004;99:1737–1741.
[Fu ll text Link]
[CrossRef]
[Med line Link]
146. Jarv is DA, Russell WJ. Drager Jul ian workstation . Anaesth Intens Care
2000;28:229.
[Med line Link]
147. Raphael DT. The low-pressure alarm condition: safe ty considerat ions and the
anesthesiologist 's response. APSF News le tt 1998–1999;13:33–40.
148. Russell WG. Oxygen supply a t risk. Anaes th Intens Care 1985;13:216–217.
[Med line Link]
149. Johnson DL. Centra l oxygen supply versus mother nature. Respir Care
1975;20:1043–1044.
[Med line Link]
150. Webb RK, Russell WJ, Klepper I , et a l. Equipment fai lure : an analys is of 2000
incident reports. Anaes th Intens Care 1993;21:673–677.
[Med line Link]
151. Stoller JK, Stefanak M, Orens D, et al. The hospi tal oxygen supply: an “O2K”
problem. Respir Care 2000;45:300–305.
[Med line Link]
152. Ewart IA. An unusual cause of gas pipe line failure. Anaesthesia
1990;45:498.
[CrossRef]
[Med line Link]
153. Braida AL, Mand ly M, Papadimos TJ. Dis ruption of the oxygen supply to a
heart-lung machine. Anaesthesia 2004;59:1254–1255.
[Fu ll text Link]
[CrossRef]
[Med line Link]
154. Anonymous . Plumber severs oxygen pipe. Biomed Safe Stand 1995;25(1):1.
155. Anonymous . Mystery of turned-off hosp ital oxygen supply so lved by Denver
police. B iomed Safe Stand 1987;17:18–19.
156. Anonymous . Did accidental O2 shutdown cause patien t death? Biomed Safe
Stand 1995;25:105–107.
157. Black AE. Extraordinary oxygen pipel ine fai lure . Anaesthesia 1990;45:599.
[CrossRef]
[Med line Link]
158. Anonymous . Medical gas delivery manifo ld could fai l. Biomed Safe Stand
1996; 26 :12.
159. Anderson B, Chamley D. Wal l ou tlet oxygen fai lu re. Anaes th Intens Care
1987;15:468–469.
[Med line Link]
160. Chung DC, Hunter DJ . The quick -mount pipel ine connector. Fai lu re of a “fa il -
safe” device. Can Anaesth Soc J 1986;33:666–668.
[Med line Link]
161. Lacoumenta S, Hall GM. A burst oxygen pipeline. Anaesthesia 1983;38:596–
597.
[CrossRef]
[Med line Link]

162. Muir J , Davidson-Lamb R. Apparatus fa ilure—cause for concern . Br J Anaesth
1980;52:705–706.
[CrossRef]
[Med line Link]
163. Cra ig DB, Cull igan J. Sudden interrup tion of gas flow through a Schrader
oxygen coupler unit . Can Anaesth Soc J 1980;27:175–177.
[Med line Link]
164. Anderson WR, Brock-Utne JG. Oxygen pipel ine supply failure. A coping
stra tegy. J Clin Monit 1991;7:39–41.
[CrossRef]
[Med line Link]
P.424
165. Will iams DJ . Occlusion of oxygen pipeline supp ly. Anaesth Intens Care
1999;27:321–322.
166. Anonymous. Anesthesia outle t hoses could have gas-f low restric t ion. Biomed
Safe Stand 1996;26:61.
167. McDade W, Ballan tyne JC. Potent ial r isk associa ted wi th anesthesia machines
wi th s ingle oxygen cylinders . J Clin Anes th 1996;8:260–261.
[CrossRef]
[Med line Link]
168. Varga DA, Guttery JS, Grundy BL. Intermit ten t oxygen delivery in an Ohmeda
Uni trol anes thesia machine due to a faul ty O-ring check valve assembly. Anes th
Analg 1987;66:1200–1201.
[Fu ll text Link]
[CrossRef]
[Med line Link]
169. Okutomi T, Watanabe S, Goto F. Oxygen f low reduction due to dus t partic le
blockage of the oxygen f i l ter. Anesth Analg 1993;76:915–917.
[Fu ll text Link]
[CrossRef]
[Med line Link]
170. Fee ley TW, Bancrof t ML, Brooks RA, et al . Potential hazards of compressed
gas cyl inders: a rev iew. Anesthesiology 1978;48:72–74.
[Fu ll text Link]

[CrossRef]
[Med line Link]
171. Blogg CE, Colv in MP. Apparent ly empty oxygen cylinders . Br J Anaesth
1977;49:87.
[CrossRef]
172. Singleton RJ, Lucbrook GL, Webb RK, et al. Physical in juries and
environmental safety in anaesthesia: an ana lysis of 2000 inc ident reports . Anaesth
Intens Care 1993;21:659–663.
[Med line Link]
173. Gordon P, Ozinsky J, Burger R. Safety of medica l gas cy linders wi th f inger
control valves. S Af r Med J 1993;83:915.
[Med line Link]
174. Mil l iken RA. An explosion hazard due to an imperfect design . Arch Surg
1972;105:125–127.
[Med line Link]
175. McDade W, Ballan tyne JC. Potent ial r isk associa ted wi th anesthesia machines
wi th s ingle oxygen cylinders . J Clin Anes th 1996;8:260–261.
[CrossRef]
[Med line Link]
176. Savoidell i GL, Naik VN, Joo HS, et al . Management of s imulated oxygen
supply fai lure : is there a gap in curriculum? Anes thesiology 2005;103:A1231.
177. Fi tzpatrick G, Moore KP. Malfunction in a needle valve. Anaesthesia
1988;43:164.
[Med line Link]
178. McMahon DJ, Holm R, Batra MS. Yet another machine faul t. Anesthesiology
1983;58:586–587.
[Fu ll text Link]
[CrossRef]
[Med line Link]
179. Boscoe MJ, Baxter RCH. Fa ilure of anaesthet ic gas supp ly. Anaesthesia
1983;38:997–998.
[CrossRef]
[Med line Link]
180. From R, George GP, Tinker JH. Foregger 705 malfunct ion resul ting in loss of
gas f low. Anesthesiology 1984;61:321–322.
[Fu ll text Link]

[CrossRef]
[Med line Link]
181. Ong B-C, bin Katijo J, Tan B-L, et al. Acute fai lure of oxygen del ivery.
Anesthesiology 2001;95:1038–1039.
[Fu ll text Link]
[CrossRef]
[Med line Link]
182. Chandradeva K. A serious inc ident wi th the Blease Frontl ine Gen ius
anaesthetic machine. Anaes thesia 2004;59:627.
[Fu ll text Link]
[CrossRef]
[Med line Link]
183. Hawk ins J . A serious inc ident wi th the Blease Front l ine Genius anaesthetic
machine. A reply. Anaesthesia 2004;59:627–628.
[Fu ll text Link]
[CrossRef]
[Med line Link]
184. Shankar SR, Stacey RGW, Raval ia A. Time to recheck the checkl is t?
Anaesthesia 1999;54:1023.
185. Bamber PA. Possible safety hazard on anaesthet ic machines. Anaes thesia
1987;42:782.
[CrossRef]
[Med line Link]
186. Heine JF, Adams PM. Another potent ial fai lure in an oxygen delivery system.
Anesthesiology 1985;63:335–336.
[Fu ll text Link]
[CrossRef]
[Med line Link]
187. Will iams C, D iaz-Navarro C. Anaesthetic machine checklis ts . Anaesthesia
2001;56:1006–1007.
[Fu ll text Link]
[CrossRef]
[Med line Link]
188. Nutta ll GA, Baker RD. Internal common gas line disconnec t. Anesthes io logy
1993;79:605–607.
[Fu ll text Link]
[CrossRef]
[Med line Link]
189. Kua JSE, Tan I . A rare cause of oxygen failure. Anaesthesia 1994;49:650–
651.
[Med line Link]
190. Capan L, Ramanathan S, Cha lon J , et al . A possible hazard with use of the
Ohio ethrane vaporizer. Anesth Analg 1980;59:65–68.
[Fu ll text Link]
[CrossRef]
[Med line Link]
191. Forrest T, Ch ilds D. An unusua l vaporiser leak. Anaesthesia 1982;37:1220–
1221.
[CrossRef]
[Med line Link]
192. Pyles ST, Kaplan RF, Munson ES. Gas loss from Ohio Modu lus vaporizer
se lec tor-interlock valve. Anes th Ana lg 1983;62:1052.
[Fu ll text Link]
[CrossRef]
[Med line Link]
193. Loughnan TE. Gas leak associated wi th a selec tatec . Anaesth Intens Care
1988;16:501.
194. Van Besouw JP, Thurlow AC. A hazard o f free-stand ing vaporizers.
Anaesthesia 1987;42:671.
[CrossRef]
[Med line Link]
195. Qadri AM. Unusua l detect ion of an old problem. Anaesthes ia 1988;43:611.
[CrossRef]
[Med line Link]
196. Berry PD, Ross DG. Missing O-ring causes unrecognised large gas leak.
Anaesthesia 1992;47:359.
[CrossRef]
[Med line Link]
197. Patte rson KW, Kean PK. Hazard with a Boyle vaporizer. Anaesthesia
1991;46:152–153.
[CrossRef]
[Med line Link]

198. Wraigh t WJ. Another fa ilure of Selectatec block. Anaesthesia 1990;45:795.
[CrossRef]
[Med line Link]
199. Hogan TS. Selec tatec swi tch malfunction . Anaesthesia 1985;40:66–69.
[CrossRef]
[Med line Link]
200. Jove F, Mil l iken RA. Loss of anesthet ic gases due to defec tive safety
equipment. Anes th Ana lg 1983;62:369–370.
[Fu ll text Link]
[CrossRef]
[Med line Link]
201. Jab lonski J , Reynolds AC. A potent ial cause (and cure) of a major gas leak.
Anesthesiology 1985;62:842–843.
[Fu ll text Link]
[CrossRef]
[Med line Link]
202. Child res WF. Malfunc tion of Ohio Modu lus anesthesia machine.
Anesthesiology 1982;56:330.
[Fu ll text Link]
[CrossRef]
[Med line Link]
203. Carter JA, McAtteer P. A serious hazard associated with the Fluo tec Mark 4
vaporizer. Anaes thesia 1984;35:1257–1258.
[CrossRef]
[Med line Link]
204. Powell JF, Morgan C. Se lec ta tec gas leak. Anaesth In tens Care 1993;21:891–
892.
205. Jab lonski J , Reynolds AC. A potent ial cause (and cure) of a major gas leak.
Anesthesiology 1985;62:842.
[Fu ll text Link]
[CrossRef]
[Med line Link]
206. Tighe SQM, Jones DA. Anaes thetic machine checks during anaesthesia .
Anaesthesia 1993;48:88.
[Med line Link]
207. Anonymous . Anesthesia uni t vaporizers. Technol Anesth 1987;7:4.
208. Dolan PF. Vaporizer leak. Anesthesiology 1978;49:302.
[Fu ll text Link]
[CrossRef]
[Med line Link]
209. Cooper PD. A hazard wi th a vaporizer. Anaesthesia 1984;39:935.
[Med line Link]
210. Rosenberg M, Solod E, Bourke DL. Gas leak through a Fluotec Mark I II
vaporizer. Anesth Analg 1979;58:239–240.
[Fu ll text Link]
[CrossRef]
[Med line Link]
211. Beavis R. Boyles mach ine. Anaesth Intens Care 1983;11:80.
[Med line Link]
212. Kataria B, Price P, Slack M. Delayed fi l l ing of the breathing bag due to a
portable vaporizer. Anesth Analg 1987;66:1055.
[Fu ll text Link]
[CrossRef]
[Med line Link]
213. Pomykala Z, Schecter H. Design f low in an anesthesia mach ine.
Anesthesiology 1992;77:399–400.
[Fu ll text Link]
[CrossRef]
[Med line Link]
214. Maurer WG. A disadvantage of s imi lar machine contro ls. Anes thesiology
1991;75:167–168.
[Fu ll text Link]
[CrossRef]
[Med line Link]
215. Ng K, Ho V. Narkomed 4E power fai lu re. Anaes th Intens Care 1997;25:309.
[Med line Link]
216. Rona ld AL. Accidenta l swi tch-off o f an anaesthetic machine. Anaesthes ia
1999;54:504.
[Fu ll text Link]
[CrossRef]
[Med line Link]

217. Anonymous . Accidental swi tch-off of an anaesthet ic machine. A reply from the
manufac turer. Anaesthesia 1999;54:504–505.
218. Okel l RW. Chain of errors. Anaesthes ia 1989;44:703–704.
[CrossRef]
[Med line Link]
219. Edsell MEG, Erasmus PD. Use of the common gas outlet for supplementary
oxygen during Caesarean sec tion. Anaes thesia 2005;60:1152.
[Fu ll text Link]
[CrossRef]
[Med line Link]
220. McLean JS, Houston PL, Dumais R. Erroneous connection of the fresh gas
f low to the anesthes ia c i rcui t. Can J Anaesth 2003;50:93.
[Med line Link]
221. Friesen RM. Safety of anaesthet ic machines. Can J Anaesth 1989;36:364.
[Med line Link]
222. Goldman JM, Phelps RW. No flow anes thesia. Anesth Analg 1987;66:1339.
[Fu ll text Link]
[CrossRef]
[Med line Link]
223. Mantia AM. A defective Washington T-piece. An example of inevi table fai lu re
and lessons to be learned. Anesthesiology 1983;59:167–168.
[Fu ll text Link]
[CrossRef]
[Med line Link]
224. Mil l iken RA, Bizzarri DV. An unusua l cause of fai lu re of anesthet ic gas
delivery to a pat ient c ircui t. Anes th Ana lg 1984;63:1047–1048.
[Full text Link]
[CrossRef]
[Med line Link]
225. Anonymous . Anesthesia breathing c ircui ts & f resh gas elbows reca lled.
Biomed Safe Stand 1989;19:19.
226. Bissonnette B, Roy WL. Obstruct ion of fresh gas f low in an Ayre's T-piece.
Can Anaesth Soc J 1986;33:535–536.
[Med line Link]
227. Si lver L, Lopes N, Brock-Utne J. Rais ing the opera ting table causing a sudden
anesthesia system obstruc tion. Anesth Analg 1996;82:1107–1108.

[Fu ll text Link]
[CrossRef]
[Med line Link]
228. Miguel R, Vila H. Mach ine wars . Another cause of pressure loss in the
anesthesia mach ine. Anesthesiology 1992;77:398–399.
[Fu ll text Link]
[CrossRef]
[Med line Link]
229. Anonymous . Fi rm begins reca ll of 21,680 breathing ci rcui ts . Biomed Safe
Stand 2001;31:100.
230. Wilden J . Cri tica l inc ident involv ing the Draeger Cato venti lator. Anaesthesia
2002;57:930–931.
[Fu ll text Link]
[Med line Link]
231. Hay H. Oxygen delivery fa ilure resul ting from interfe rence with a Bain
breathing sys tem. Eur J Anaesthesiol 2000;17:591–593.
[CrossRef]
[Med line Link]
232. Goresky GV. Bain c ircui t delivery tube obs truct ions. Can J Anaes th
1990;37:385.
[Med line Link]
233. Ingl is MS. Tors ion of the inner tube. Br J Anaesth 1980;52:705.
[CrossRef]
[Med line Link]
234. Forrest PR. Defective anaesthet ic breath ing c ircui t . Can J Anaesth
1987;34:541–542.
[Med line Link]
235. Olympio MA. Common gas outlet concern leads to correc tive ac tion. APSF
News le tt 2004;19:34.
236. Abramovich A. Common gas outlet concern leads to correc tive ac tion.
Response. APSF Newsle tt 2004;19:34.
237. Kshatri AM, Kingsley CP. Defect ive carbon dioxide absorber as a cause for a
leak in a breathing ci rcui t. Anesthes io logy 1996;84:475–476.
[Fu ll text Link]
[CrossRef]
[Med line Link]

238. Russell WJ, Webb RK, van der Walt JH, et al . Problems wi th venti lat ion : an
analys is of 2000 inc ident reports. Anaesth Intens Care 1993;21:617–620.
[Med line Link]
239. Creasy D. Hidden connection. Anaesthes ia 2001;56:488–489.
[Fu ll text Link]
[CrossRef]
[Med line Link]
240. Ianchulev SA, Comunale ME. To do or not to do a preinduct ion check-up of the
anesthesia mach ine. Anesth Analg 2005;101:774–776.
[Fu ll text Link]
[CrossRef]
[Med line Link]
241. Jack T. A lack of concern. Br J Anaes th 1998;80:878–879.
[Med line Link]
242. Mark D. An unusual anesthesia machine leak. J Cl in Anesth 2000;12:87.
[CrossRef]
[Med line Link]
243. Ezaru CS. Preinduc tion check-up of the anesthesia mach ine. Anesth Analg
2006;102:1588–1589.
[Fu ll text Link]
[CrossRef]
[Med line Link]
244. Anonymous . Anesthesia machine owners alerted to potent ial breathing ci rcuit
leak. Biomed Safe Stand 1989;19:122.
245. Birch AA, Fisher NA. Leak o f soda l ime seal after anesthesia mach ine check . J
Cl in Anesth 1989;1:474–476.
[CrossRef]
[Med line Link]
246. Anderson TY. Failure to venti la te. Anaes th Intens Care 1993;21:898.
[Med line Link]
247. Anonymous . Anesthesia breathing c ircui t reca ll expanded by FDA. Biomed
Safe Stand 1997;27:164–166.
248. Anonymous . Airway adapter reca lled; a ir leak poss ible. B iomed Safe Stand
2000;30:140.
249. Anonymous . Breathing circu it adapters. Techno l Anes th 2000;21:6–7.
250. Anonymous . Bax ter-Adul t anesthesia breath ing c ircui ts with swivel wye
connec tors: may be cracked. Heal th Devices Alerts 2002;26:3.
251. Bader SO, Doshi KK, Grunwald Z. A novel leak from an unfamil iar component.
Anesth Analg 2006;102:975–976.
[Fu ll text Link]
[CrossRef]
[Med line Link]
252. Rossberg ML, Greenberg RS. Anesthes ia respiratory c i rcui t failure.
Anesthesiology 2002;97:762–763.
[Fu ll text Link]
[CrossRef]
[Med line Link]
253. Ferderbar PJ, Kettler RE, Jablonski J , et al. A cause of b reathing system leak
during c losed c ircui t anesthesia. Anesthesio logy 1986;65:661–663.
[Med line Link]
254. Brown MC, Burris WR, Hil ley MD. Breathing c ircui t mishap result ing from Y-
piece dis integrat ion. Anesthesiology 1988;69:436–437.
[Fu ll text Link]
[CrossRef]
[Med line Link]
255. Colavita RD, Apfelbaum JL. An unusual source of leak in the anesthesia
c i rcui t. Anesthes io logy 1985;62:208–209.
[Fu ll text Link]
[CrossRef]
[Med line Link]
256. Cull ingford D. Broken yoke. Anaes th Intens Care 1985;13:442.
257. Cooper MG, Vouden J, Rigg D. Circui t leaks . Anaesth Intens Care
1987;15:539–540.
258. Chung DC, Ho AMH, Tay BA. “Apnea-volume” warning during normal
venti lation of the lungs: an unusua l leak in the Narkomed 4 anesthesia system. J
Cl in Anesth 2001;13:40–43.
[CrossRef]
[Med line Link]
259. Dhar P, George I, Mankad A, et al . Flow transducer gas leak detec ted after
induction. Anesth Analg 1999;89:1587.
[Fu ll text Link]

[CrossRef]
[Med line Link]
260. Pandit JJ, Pa layiwa E. Dangers of some s ingle-use in-l ine carbon dioxide
ai rway adaptors. Anaesthesia 2005;60:622–623.
[Fu ll text Link]
[CrossRef]
[Med line Link]
261. Ferderbar PJ, Kettler RE, Jablonski J , et al. A cause of b reathing system leak
during c losed c ircui t anesthesia. Anesthes io logy 1986;65:661–663.
[Med line Link]
262. Kemen M, Desai K, Roizen MF, et al. Over f if ty percent of disposable ci rcu its
leak. Anesth Analg 1990;70:S194.
263. Lamarche Y. Anaesthetic breathing c i rcuit leak from c racked oxygen analyzer
sensor connector. Can Anaesth Soc J 1988;32:682–683.
[Med line Link]
264. Mantia AM. Faul ty Y-piece. Anes th Ana lg 1981;60:121–122.
[Fu ll text Link]
[CrossRef]
[Med line Link]
265. Lee O, Sommer RM. Pressure moni toring hose causes leak in anesthesia
breathing c i rcuit . Anesth Analg 1991;73:365.
[CrossRef]
[Med line Link]
266. Poulton TJ. Unusual corrugated tubing leak. Anesth Analg 1986;65:1365.
[Fu ll text Link]
[CrossRef]
[Med line Link]
267. Prasad KK, Chen L. Complica tions related to the use of a heat and moisture
exchanger. Anes thesiology 1990;72:958.
[Med line Link]
268. Pat i l AR. Mel ting of anesthesia c ircui t by humidif ie r. Anesth Prog 1989;36:63–
65.
[Med line Link]
269. Raja SN, Gel le r H. Another potent ial source of a major gas leak .
Anesthesiology 1986;64:297–298.
[Fu ll text Link]

[CrossRef]
[Med line Link]
270. Sos is MB, Payne MN. Another cause fo r a leak in a disposable breathing
c i rcui t. Anesthes io logy 1989;71:806.
[Fu ll text Link]
[CrossRef]
[Med line Link]
271. Shampaine EL, Helfaer M. A modest proposal for improved humidif ier design.
Anesth Analg 1991;72:130–131.
[Fu ll text Link]
[CrossRef]
[Med line Link]
P.425
272. Biro P. Unusual cause fo r a c irc le sys tem leak. Anesth Analg 1996;83:196.
[Fu ll text Link]
[CrossRef]
[Med line Link]
273. Denman W, Coll ier BB. An inappropriate use of tape. Anaesthesia
1990;45:794–795.
[CrossRef]
[Med line Link]
274. Edge G, Papee E. An unsuspected source of breathing sys tem fa ilure.
Anaesthesia 1994;49:827–828.
[Med line Link]
275. Feinglass NG, Dorsch JA. Disposable c ircui t disconnects . Anesthesiology
1993;79:1449–1450.
[Fu ll text Link]
[CrossRef]
[Med line Link]
276. Horton RG. Exhale spi l l valve fai lu re. Anaes th Intens Care 1994;22:233–234.
[Med line Link]
277. Koehli N. Defect ive feed mount. Anaesthesia 1992;47:354–355.
[CrossRef]
[Med line Link]

278. Lacoux PA, Chris t ie G. Leaking Datex sampling se t fo r the end-tidal CO2
moni tor. Anaes thesia 1992;47:173.
[CrossRef]
[Med line Link]
279. Lam WH, Evans JM. Rubber gloves and anaesthet ic gas leak. Anaes thesia
1996;51:1075.
[Fu ll text Link]
[CrossRef]
[Med line Link]
280. Malhotra V, Bradley E. Broken inner s leeve of a Y-connector: course of a
c i rcui t leak and a potent ial fore ign body aspirat ion. Anesth Analg 1993;76:1169–
1170.
[Fu ll text Link]
[CrossRef]
[Med line Link]
281. Need leman S, Kaplan RF. Unusual source of ai r leak in a pediatric anesthesia
breathing c i rcuit . Anesth Analg 1995;81:654.
[Fu ll text Link]
[CrossRef]
[Med line Link]
282. Reinhart DJ , Friz R. Undetected leak in corrugated c i rcui t tubing in
compressed conf iguration. Anesthes iology 1993;78:218.
[Fu ll text Link]
[CrossRef]
[Med line Link]
283. Richardson J, Bickford-Smith PJ. Covert breathing system fai lure . Anaesthesia
1993;48:541.
[CrossRef]
[Med line Link]
284. Wang J-S, Hung W-T, Lin C-Y. Leakage of d isposable breathing ci rcui ts . J Clin
Anesth 1992;4:111–115.
[CrossRef]
[Med line Link]
285. Yassin K, Gibbons JJ . A hidden leak in the ci rcle system. Anesth Analg
1991;73:236.
[Fu ll text Link]

[CrossRef]
[Med line Link]
286. Anonymous . Pediatric anesthesia breathing ci rcu it tubing could spl it & leak .
Biomed Safe Stand 1994;24:124–126.
287. Marshal l A. Leak ing catheter mount swivels. Anaesth In tens Care
2000;28:333–334.
[Med line Link]
288. Will iams N. A leaky c ircui t . Anaesthesia 1996;51:406–407.
[Fu ll text Link]
[CrossRef]
[Med line Link]
289. Tolhurst-Cleaver C. The hidden leak. Anaes thesia 2000;55:914.
[Full text Link]
[CrossRef]
[Med line Link]
290. Aldridge J . Leak on Datex Aest ive/5 anaes thetic machine. Anaesthesia
2005;60:420–421.
[Fu ll text Link]
[CrossRef]
[Med line Link]
291. Bader SO, Eps tein RH, Grunwald Z, e t al . Occu lt leak in an anesthesia
machine c ircui t ; a quanti ta tive assessment. Anes thesiology 2005;103:A1147.
292. Stevenson PH, McLeskey CH. Breakage of a reservoir bag mount, an unusual
anesthesia mach ine fai lu re. Anesthesio logy 1980;53:270–271.
[Fu ll text Link]
[CrossRef]
[Med line Link]
293. Mil l iken RA. Bag mount de tachment. A function of age? Anesthes iology
1982;56:154.
294. Newnan PTE. Another faul ty ca theter mount: now you see it now you don't .
Anaesthesia 2001;56:699–700.
[Fu ll text Link]
[CrossRef]
[Med line Link]
295. Anonymous . Anesthesia ai rway connector recalled: port could open. B iomed
Safe Stand 1991;21:117–118.

296. Gunter JB, Myers T, Win ST, et al . Catas trophic failure of Aes tiva 3000
absorber man ifold. Anesthesiology 2004;100:199–200.
[Fu ll text Link]
[CrossRef]
[Med line Link]
297. Gulat i MS. Less caps , less connec ting and instant moni toring. Anaesthes ia
2004;59:720–721.
[Fu ll text Link]
[CrossRef]
[Med line Link]
298. Carter JA. Less caps, less connecting and ins tan t moni to ring. A reply.
Anaesthesia 2004;59:721.
[Fu ll text Link]
299. Wood D, Boyd M, Campbell C. Insulat ion of heated wire ci rcui ts . Anes th Analg
1992;74:471.
[Fu ll text Link]
[CrossRef]
[Med line Link]
300. Mizutani AR, Ozaki G, Rusk R. Insulation of heated wire ci rcuits . In response.
Anesth Analg 1992;74:472.
[Fu ll text Link]
[CrossRef]
301. Sprague DH, Maccioli GA. Disposable c i rcui t tubing melted by heated
humidif ier. Anesth Analg 1986;65:1247.
[CrossRef]
[Med line Link]
302. Anonymous . Inappropriate Fisher & Paykel heater-wire adapter melts
Allegiance breathing ci rcui t. Health Devices 2000;29(2–3):86–87.
[Med line Link]
303. Arms trong P, Flick R. An intermitten t fault involv ing an Ulco anaes thetic
machine. Anaesth Intens Care 2001;29:204–205.
[Med line Link]
304. Brown CQ, Canada ED, Graney WF. Fa ilure of Bain ci rcu it b reathing system.
Anesthesiology 1981;55:716–717.
[Med line Link]

305. Breen DP. Failure o f a valve in a Ba in system. A dangerous design?
Anaesthesia 1990;45:417.
306. Mil ler DC, Coll ins JW, Wal lace L. Failure of the expiratory valve on a Bain
system. Anaesthesia 1990;45:992.
307. Nelson RA, Snowdon SL. Fai lure of an adjustable pressure l imi ting valve.
Anaesthesia 1989;44:788–789.
[CrossRef]
[Med line Link]
308. Fernandes MPP, Barker KF. Loose adhesive in anaesthetic c i rcui t.
Anaesthesia 2006;61:73–74.
[Fu ll text Link]
[CrossRef]
[Med line Link]
309. Magee C. Loose adhesive in anaesthetic c ircui t . A reply. Anaes thesia
2006;61:74.
[Fu ll text Link]
310. Judkins KC, Safe M. Routine serv ic ing of the Cape-Wane vent ilator.
Anaesthesia 1983;38:1102.
[CrossRef]
[Med line Link]
311. Ripp CH, Chapin JW. A be llow's leak in an Ohio anesthesia venti la tor. Anesth
Analg 1985;64:942.
[Fu ll text Link]
[CrossRef]
[Med line Link]
312. Hutchinson BR. An unusual leak. Anaesth In tens Care 1987;15:355.
[Med line Link]
313. Rolbin S. An unusual cause of venti la to r leak. Can Anaesth Soc J
1977;24:522–524.
[Med line Link]
314. Wolf S, Watson CB, Clark P. An unusual cause of leakage in an anesthesia
system. Anes thesiology 1981;55:83–84.
[Fu ll text Link]
[CrossRef]
[Med line Link]

315. Choi JJ, Gu ida J , Wu W. Hypoventilatory hazard of an anesthetic scavenging
device. Anesthesiology 1986;65:126–127.
[Fu ll text Link]
[CrossRef]
[Med line Link]
316. Eisenk raft JB, Sommer RM. F lapper valve malfunction. Anes th Ana lg
1988;66:1132.
[Med line Link]
317. Eisenk raft JB. Potential fo r barotrauma or hypoventi la tion wi th the Drager AV-
E venti la tor. J Clin Anesth 1989;1:452–456.
[CrossRef]
[Med line Link]
318. Sommer RM, Bhalla GS, Jackson JM, e t al . Hypoventila tion caused by
venti lato r valve rupture . Anes th Analg 1988;67:999–1001.
[CrossRef]
[Med line Link]
319. Khali l SN, Ghols ton TK, Binderman J, et al. Flapper valve malfunction in an
Ohio c losed scavenging system. Anes th Ana lg 1987;66:1334–1336.
[Fu ll text Link]
[CrossRef]
[Med line Link]
320. Anonymous . Risk of barotrauma and/or lack of venti la tion on venti latorless
anesthesia mach ines. Techno l Anesth 1994;14:2–3.
321. Munford BJ, Wishaw KJ. Cri tical inc idents with nonrebreathing valves. Anaesth
Intens Care 1990;18:560–563.
[Med line Link]
322. Oliver JJ, Pope R. Potential hazard with s i licone resusci tators . Anaesthesia
1984;39:933–934.
[CrossRef]
[Med line Link]
323. Anonymous . Valve component on resusci tat ion k i ts may leak. Biomed Safe
Stand 1989;19:35–36.
324. McDermott M, Dearlove OR. A defect in disposab le equ ipment. Anaesthesia
2001;56:1215.
[Fu ll text Link]
[Med line Link]

325. Graham DH. Advantages of s tanding bel lows venti la to rs and low-f low
techniques. Anesthesio logy 1983;58:486.
[Fu ll text Link]
[CrossRef]
[Med line Link]
326. Anonymous . Min i-set vent i lator a larms can be lethal . Technol Anes th
1999;20:1–2.
327. Adams AP. Breath ing system disconnect ions. Br J Anaes th 1994;73:46–54.
[CrossRef]
[Med line Link]
328. Heath ML. Accidents associated with equipment. Anaes thesia 1984;39:57–
60.
[CrossRef]
[Med line Link]
329. Dain SL. Breathing c i rcuit disconnect ions: averting ca tastrophes. Can J
Anesth 2001;48:840–843.
330. Brahams D. Two locum anaes thetis ts conv ic ted of manslaughter. Anaes thesia
1990;45:981–982.
[CrossRef]
[Med line Link]
331. Neufeld PD, Johnson DL. Results of the Canadian Anaes thetis ts ' Society
opinion survey on anaesthet ic equipment. Can Anaesth Soc J 1983;30:469–473.
[Med line Link]
332. Lawes EG. Hidden hazards and dangers associated with the use of HME/fi l ters
in b reath ing c ircui ts . The ir effect on tox ic metabo li te production , pulse oximetry and
ai rway res is tance. Br J Anaes th 2003;91:249–264.
[Fu ll text Link]
[CrossRef]
[Med line Link]
333. Tunsti l l SA. Detachment of swivel connector f rom breathing ci rcuit .
Anaesthesia 2005;60:1051–1052.
[Fu ll text Link]
[CrossRef]
[Med line Link]
334. Neufeld PD, Johnson DL, deVeth J. Safety of anaesthesia breathing c ircui t
connec tors. Can Anaes th Soc J 1983;30:646–652.

[Med line Link]
335. Blatt D. Breath ing c ircui t disconnects, leaks could be prevented wi th locking
pin. APSF Newslett 1995;10:20.
336. Condon HA. An ant idisconnexion device. Anaesthesia 1982;37:103–104.
[CrossRef]
[Med line Link]
337. Eck J, Jantzen J -PAH. To disconnect is be tter than to extubate.
Anesthesiology 1992;76:483–484.
[Fu ll text Link]
[CrossRef]
[Med line Link]
338. American Society fo r Testing and Materials . Part icular requirements for
anesthesia workstations and their components (ASTM F-1850-00). West
Conshohocken, PA: Author, 2000.
339. Coll ins L, Vaghadia H. Pat ien t disconnec t. Can J Anaesth 1998;45:1135.
[Med line Link]
340. Blackstock D, Forbes M. Analys is of an anaesthetic gas scavenging sys tem
hazard. Can J Anaesth 1989;36:204–208.
[Med line Link]
341. Morr ZF, Stein ED, Ork in LR. A possible hazard in the use of a scaveng ing
system. Anes thesiology 1977;47:302–303.
[Med line Link]
342. Mostafa SM, Sutcl if fe AJ . Ant ipol lut ion expiratory va lves. A potent ial hazard.
Anaesthesia 1982;37:468–469.
[CrossRef]
[Med line Link]
343. Patel KD, Dalal FY. A potential hazard of the Drager scavenging in terface fo r
wal l suct ion . Anesth Analg 1979;58:327–328.
[Fu ll text Link]
[CrossRef]
[Med line Link]
344. Jones D. An unusual cause of a leak from an anaesthet ic machine.
Anaesthesia 1995;50:751.
[CrossRef]
[Med line Link]

345. Hodgson CA, Mostafa SM. Riddle of the pers istent leak . Anaesthesia
1991;46:799.
[CrossRef]
[Med line Link]
346. St irt JA, Lewens te in LN. Circle system fai lure induced by gastric suct ion.
Anaesth Intens Care 1981;9 :161–162.
[Med line Link]
347. Lee T, Schrader MW, Wright BD. Pseudo-fai lure of mechanical venti la tor
caused by accidental endobronchial nasogastric tube insertion. Respir Care
1980;25:851–853.
348. Olympio MA, Stoner J. Tight mask f i t could have prevented “airway”
obstruct ion. Anesthesiology 1992;77:822–825.
[Fu ll text Link]
[CrossRef]
[Med line Link]
349. Sethi AK, Mohta M, Sharma P. Breath ing c ircui t obstruct ion by a foreign body.
Anaesth Intens Care 2004;32:139–141.
[Med line Link]
350. Chacon AC, Kuczkowski KM, Samnchez RA. Unusua l case of breathing c i rcu it
obstruct ion: p las tic packaging revis i ted. Anesthesiology 2004;109:753.
[Fu ll text Link]
[CrossRef]
[Med line Link]
351. Aarhus D, Soreide E, Ho ls t-Larsen H. Mechanica l obstruct ion in the
anaesthesia de livery-sys tem mimicking severe bronchospasm. Anaesthes ia
1997;52:992–994.
[Fu ll text Link]
[CrossRef]
[Med line Link]
352. Eckhout GVJ, Bhatia S. Another cause of diff icul ty in venti la ting a pat ient. J
Cl in Anesth 2003;15:137–139.
[CrossRef]
[Med line Link]
353. Anonymous . Occluded Y-p ieces led to breathing c i rcuit recall . Biomed Safe
Stand 1991;21:60.

354. Anonymous. Anesthesia uni t carbon d iox ide absorbents . Technol Anesth
1992;11:7.
355. Anonymous . Humidif iers, heat/moisture exchange. Technol Anesth
1991;12:6.
356. Anonymous . Potent ial for ai rf low obstruction in breath ing c ircui t adapter.
Biomed Safe Stand 1998;19:129,131.
357. Anonymous . Breathing circu it adapters. Techno l Anes th 1998;19:8.
358. Anonymous . Breathing circu it adapters. Techno l Anes th 2000;21:6.
359. Barto lacci R. C irc le absorpt ion system hazard . Anaesth Intens Care
1995;23:123–124.
[Med line Link]
360. Carter JA. Checking anaesthet ic equipment and the expert group on b locked
anaesthetic tub ing (EGBAT). Anaesthesia 2004;59:105–107.
[Fu ll text Link]
[CrossRef]
[Med line Link]
361. Dav ies JR. Misuse of adhes ive tape. Anaesthesia 1988;43:841.
362. Bennett MW, Nowicki RW. Faul ty Penlon c ircle absorber. Anaesthesia
2005;60:932–933.
[Fu ll text Link]
[CrossRef]
[Med line Link]
363. Anonymous . Breathing system components—Gilbeck humidi f iers. Anaes thesia
1991;46:612.
364. Anonymous . Breathing-c ircu it connectors blocked by plastic membrane.
Biomed Safe Stand 1991;21:91.
365. Anonymous . Valves, posit ive end expiratory pressure. Techno l Anes th
1991;12:11.
366. Anonymous . Videotape explains OR f i res . Technol Anesth 1992;13:7 .
367. Anonymous. SLE—model N 2188 and N5188 heated patien t c i rcuits : connector
may be blocked. Heal th Dev ices Alerts 2005;29:11–12.
368. Baker AJ, Hall R. Malfunct ion of Hudson electrochemical oxygen sensor.
Anaesth Intens Care 1989;17:516–517.
[Med line Link]
369. Cook WP, Gravenstein JS. Breathing ci rcu it occlus ion due to a defect ive
paediatric face mask. Can J Anaesth 1988;35:205–206.

[Med line Link]
370. Daley H, Amoroso P. Dangerous repairs. Anaesthesia 1991;46:997.
[CrossRef]
[Med line Link]
371. Franke l DZN. Adhesive tape obstructing an anesthet ic c i rcui t. Anesthesio logy
1983;59:256.
[Med line Link]
372. Gaines CY, Rees DI. Vent ilator malfunct ion—another cause. Anesthesiology
1984;60:260–261.
[Fu ll text Link]
[CrossRef]
[Med line Link]
373. Koga Y, Iwatsuki N, Takahashi M, et al. A hazardous defect in a humidifier.
Anesth Analg 1990;71:712.
[Fu ll text Link]
[CrossRef]
[Med line Link]
374. Prados W. A dangerous defect in a heat and moisture exchanger.
Anesthesiology 1989;71:804.
[Fu ll text Link]
[CrossRef]
[Med line Link]
375. Sabo BA, Olinder PJ, Smith RB. Obstruction of a breathing ci rcui t. Anesth Rev
1983;10:28–30.
P.426
376. Springman SR, Malischke P. A potent ia lly serious anesthesia sys tem
malfunct ion. Anesthesiology 1986;65:563.
[Fu ll text Link]
[CrossRef]
[Med line Link]
377. Will iams EL, Reede L . One cap too many. Anes th Ana lg 1987;66:1340–1341.
[Fu ll text Link]
[CrossRef]
[Med line Link]

378. Gal lacher BP, Kelly M, Mora RR. Failure to venti late due to glass ampule
f ragment occlusion of the breathing ci rcu it . Anesthesiology 1997;87:180.
[Fu ll text Link]
[CrossRef]
[Med line Link]
379. Krensavage TJ , Richards E. Sudden development of anesthesia c i rcui t
obstruct ion by an end-t idal CO2 cap in the gas sampling elbow. Anesth Analg
1995;81: 204–213.
380. Marshal l FPF. Kinked inner tube of coaxial breathing system. Br J Anaesth
1993;71:171.
[CrossRef]
[Med line Link]
381. Platt ND. Unusual cause of obstructed ai rway. Anaesthesia 1993;49:540–
541.
[CrossRef]
[Med line Link]
382. Wilkes PRH. Bain ci rcuit occluded by foreign body. Can J Anaesth
1994;41:137–139.
[Med line Link]
383. Anonymous . Inju ries—one fatal—high light the need fo r pre-use tes ting of
disposable breathing ci rcu its . Heal th Dev ices 2000;29:188–189.
384. Choi J , Cooper GM. Circui t obs truct ion. Br J Anaesth 2003;91:452.
[Fu ll text Link]
[CrossRef]
[Med line Link]
385. Le Poidev in R. Circui t obs truct ion—is there a foolproof way? Anaesthes ia
2002;57:1221–1223.
386. Nichols K, Thomas D, Barker CJ. Circuit obstruct ion mimics bronchospasm.
APSF News le tt 2004;19:35.
387. McKenna C. Expert pane l to look into b locked anaes thetic tubing inc idents.
BMJ 2002;325:183.
[CrossRef]
388. Carter JA. Less caps, less connecting and ins tan t moni to ring. A reply.
Anaesthesia 2004;59:721.
[Fu ll text Link]

389. Anonymous . MMS—anes thesia breathing c ircui ts : possible a irway obs truct ion.
Hea lth Devices Alerts 2005;29:5–6.
390. Anonymous . Breathing circu it adapters. Techno l Anes th 2005;25:12–13.
391. Ananthanarayan C, Urbach G, Tincombe C, et al . Breathing c i rcuit occlus ion
due to defect in swivel port connector. Can J Anaesth 1990;37:707.
[Med line Link]
392. Foreman MJ, Moyes DG. Anaesthet ic breath ing c ircui t obstruct ion due to
blockage of tracheal tube connector by a foreign body—two cases. Anaes th In tens
Care 1999;27:73–75.
[Med line Link]
393. Johnston P. Unusual cause of obstructed expiration. Anaesthesia
1989;44:704–705.
[CrossRef]
[Med line Link]
394. Stewart KG, Cohen A. An unexpec ted cause of total expira tory obs truction.
Anaesthesia 1988;43:810.
[CrossRef]
[Med line Link]
395. Randhawa N, Semenov RA, Pate l A. Coaxial breathing sys tem outer tube
occlusion: what goes in mus t come out. Anaesthesia 2002;57:716–717.
[Fu ll text Link]
[CrossRef]
[Med line Link]
396. King D, Emerson B. Breathing system obstruc tion from in travenous giv ing se t
caps. Anaesthesia 2002;57:505.
[Fu ll text Link]
[Med line Link]
397. Gooch C, Peutre ll J . A faulty Bain ci rcu it . Anaesthesia 2004;59:618.
[Fu ll text Link]
[CrossRef]
[Med line Link]
398. LePoidevin R. A fau lty Bain c ircui t . A reply. Anaes thesia 2004;59:618.
[Fu ll text Link]
[CrossRef]
[Med line Link]

399. Anonymous . End-t idal detec tors obstructed by plast ic caps . Biomed Safe
Stand 1995;25:11–12.
400. Wan YL, Swan M. Exot ic obstruc tion. Anaes th Intens Care 1990;18:274.
[Med line Link]
401. Sturges JE, Matthews PC. Unusua l cause of c i rcui t failure. Anaesthesia
2002;57:616–617.
[Fu ll text Link]
[Med line Link]
402. Thorpe CM. Plas tic in the anaesthet ic c i rcui t. Anaes thesia 2002;57:85–86.
[Fu ll text Link]
[Med line Link]
403. Gulat i MS. Less caps , less connec ting and instant moni toring. Anaesthes ia
2004;59:720–721.
[Fu ll text Link]
[CrossRef]
[Med line Link]
404. Ward MM, Co ll ins SJ. Another case of obs truct ion to an anaesthet ic c ircu it . Br
J Anaesth 2003;90:110–111.
[Full text Link]
[CrossRef]
[Med line Link]
405. Sch lager A, Furtner B, Mit te rschiff thale r G. Acute obs truct ion during manual
venti lation caused by an end-tidal rubber cap in the reservoir bag. Anes th Ana lg
1999;89:804–805.
[Fu ll text Link]
[CrossRef]
[Med line Link]
406. Warters RD, Lee C, Szmuk P, et al. A warm air b lanket causes in traoperat ive
ai rway obstruction . Anes thesiology 2001;94:169–170.
[Fu ll text Link]
[CrossRef]
[Med line Link]
407. Anonymous . Anesthesia breathing c ircui t parts recal led because of occluded Y
pieces. Biomed Safe Stand 1987;17:10–11.
408. Anonymous . Anesthesia gas sampling elbow c i rcui ts recalled due to potent ial
of occlusion . Biomed Safe S tand 1998;28:172–173.

409. Kurian J , Renwick N. An unusual case of airway obs truct ion. Br J Anaesth
2001;86:804–805.
[Med line Link]
410. Anonymous . Inju ries—one fatal—high light the need fo r pre-use tes ting of
disposable breathing ci rcu its . Technol Anesth 2000;20:2–3.
411. Feingold A. Carbon dioxide absorber packaging hazard. Anesthesiology
1976;45:260.
[Fu ll text Link]
[CrossRef]
[Med line Link]
412. Anonymous . Sodasorb prepack CO2 absorpt ion cartr idges. Heal th Dev ices
1988;17:35–36.
[Med line Link]
413. Anonymous . Sodasorb Prepac safety adv isory. Lexing ton, MA: WR Grace &
Co., March 6, 1992.
414. Norman PH, Daley MD, Walker JR, et a l. Obstruc tion due to retained carbon
dioxide absorber canister wrapping. Anesth Analg 1996;83:425–426.
[Fu ll text Link]
[CrossRef]
[Med line Link]
415. Ransom ES, Norfleet EA. Obstruction due to retained carbon dioxide absorber
canis ter wrapping. Anesth Analg 1997;84:703.
[Fu ll text Link]
[CrossRef]
[Med line Link]
416. Brosnan C, Khoo K. Incorrect ly s ited PEEP valve . Anaesthesia 2005;60:418.
[Fu ll text Link]
[CrossRef]
[Med line Link]
417. Cameron AE, Power I , Tierney B. Portex swivel connector hazard . Anaesthesia
1984;39:496.
[CrossRef]
[Med line Link]
418. Gaylard D, Sav il le G. Kinked inner tube of coax ial breathing system. Br J
Anaesth 1994;72:367.
[CrossRef]

[Med line Link]
419. Wise HJ. ABC: back to basics wi th anaesthet ic breath ing components.
Anaesthesia 2002;57:86.
[Fu ll text Link]
[Med line Link]
420. Will iams DJ , Stacey MRW. Rap id and complete occlusion of a heat and
moisture exchange f i l te r by pulmonary edema (Clinica l report). Can J Anaesth
2002;49:126–131.
[Med line Link]
421. Anonymous . Humidif iers, heat/moisture exchange. Technol Anesth
1991;12:5.
422. Garnerin P, Schif fer E, Van Gesse l E, et al. Root-cause analys is of an ai rway
f il te r occlusion: a way to improve the re liabil i ty of the respiratory ci rcu it . Br J
Anaesth 2002;89:633–635.
[Fu ll text Link]
[CrossRef]
[Med line Link]
423. Wal ton JS, Fears R, Burt N, et al. Intraoperative breath ing c ircui t obstruc tion
caused by a lbu terol nebul izat ion. Anesth Analg 1999;89:650–651.
[Fu ll text Link]
[CrossRef]
[Med line Link]
424. Crowhurst P. Mishaps wi th the Mera-F c i rcuit . Anaesth In tens Care
1987;15:121–122.
[Med line Link]
425. Boumphery S. A new cause of ai rway obstruction . Anaesthesia 2002;57:293–
294.
[Fu ll text Link]
[CrossRef]
[Med line Link]
426. Roe JA. A new cause of ai rway obstruc tion. Anaes thesia 2002;57:293–294.
[Fu ll text Link]
[CrossRef]
[Med line Link]
427. Shrof f PK, Skerman JH. Humidif ier malfunction—a cause of anes thesia c i rcuit
occlusion. Anesth Analg 1988;67:710–711.

[Fu ll text Link]
[CrossRef]
[Med line Link]
428. Weinberg L, Sawhney S, Skewes D. Safety warning with Datex-Ohmeda S/5
anaesthetic delivery un it design. Anaes th Intens Care 2004;32:719–720.
[Med line Link]
429. McGarrigle R, Whi te S. Oxygen analyzers can detec t disconnec tions . Anes th
Analg 1984;63:464–465.
[Fu ll text Link]
[CrossRef]
[Med line Link]
430. Meyer RM. A case for mon itoring oxygen in the expira tory l imb of the ci rc le.
Anesthesiology 1984;61:374.
431. Spurring PW, Small LFG. Breathing system disconnex ions and misconnexions.
Anaesthesia 1983;38:683–688.
[CrossRef]
[Med line Link]
432. Lev ins RA, Francis RI, Burnley SR. Failu re to detect disconnexion by
capnography. Anaesthesia 1989;44:79.
[CrossRef]
[Med line Link]
433. Slee TA, Pavlin EG. Fa ilure of low pressure ala rm associated with the use of a
humidif ier. Anesthesiology 1988;69:791–793.
[Fu ll text Link]
[CrossRef]
[Med line Link]
434. Raphael DT, Weller RS, Doran DJ. A response algorithm for the low-pressure
alarm condi tion . Anes th Ana lg 1988;67:876–883.
[Fu ll text Link]
[CrossRef]
[Med line Link]
435. Raphael DT. An algorithmic response for the breathing system low-pressure
alarm condi tions. Prog Anes thesiol 1997;11:219–244.
436. Raphael DT, Weller RS, Doran DJ. A response algorithm for the low-pressure
alarm condi tion . Anes th Ana lg 1988;67:876–883.
[Fu ll text Link]

[CrossRef]
[Med line Link]
437. Raphael DT. The low-pressure alarm condition: safe ty considerat ions and the
anesthesiologist 's response. APSF News le tt 1998—1999;13:33–40.
438. Barry JES, Adams A. Inadvertent administra tion of carbon dioxide. Surv
Anesth 1991;35:368–374.
439. Dinnick DP. Accidental severe hypercapnia during anaesthesia. Br J Anaesth
1968;40:36–45.
[CrossRef]
[Med line Link]
440. Todd DB. Dangers of CO2 cyl inders on anaesthet ic machines. Anaes th Intens
Care 1995;50:911–912.
441. Klein SL, Li lburn JK. An unusual case of hypercarbia during general
anesthesia. Anesthesio logy 1980;53:248–250.
[Fu ll text Link]
[CrossRef]
[Med line Link]
442. Whi tten MP, Wise CC. Design faul ts in commonly used carbon dioxide
absorbers. Br J Anaesth 1972;44:535–537.
[CrossRef]
[Med line Link]
443. Loughman E. Defec tive soda lime can isters. Anaesth In tens Care
1990;18:275.
[Med line Link]
444. Cozani tis DA. Damage to an OHMEDA exp iratory valve. Anaesth Intens Care
2000;28:585–586.
[Med line Link]
445. Parry TM, Jewkes DA, Smith M. A stick ing f lutter valve. Anaesthes ia
1991;46:229.
[CrossRef]
[Med line Link]
446. Nunn BJ , Rosewarne FA. Exp iratory valve fai lure . Anaesth Intens Care
1990;18:273–274.
[Med line Link]
447. Anonymous . Anesthesia gas absorber check valves may “s tick open.” Biomed
Safe Stand 1990;20:156.
448. Fogdall RP. Exacerbat ion of iatrogenic hypercarbia by PEEP. Anes thesiology
1979;51:173–175.
[Fu ll text Link]
[CrossRef]
[Med line Link]
449. Pyles ST, Berman LS, Mode ll JH. Exp iratory valve dysfunc tion in a semic losed
c i rc le anesthes ia c i rcui t—verif icat ion by ana lysis of carbon dioxide waveform.
Anesth Analg 1984;63:536–537.
[Fu ll text Link]
[CrossRef]
[Med line Link]
450. Kim JM, Kovac AL, Mathewson HS. Incompetency of unidirect ional dome
valves. A mul ti -hospi tal s tudy. Anesth Analg 1985;64:237.
451. Rosewarne F, Wel ls D. Three cases of valve incompetence in a c irc le system.
Anaesth Intens Care 1988;16:376–377.
[Med line Link]
452. Whalley DG. Malfunction ing unid irectional valves of Ohmeda series 5 and 5A
carbon d ioxide absorbers. Can J Anaesth 1988;35:668–669.
[Med line Link]
453. Dzwonczyk D, Dahl MR, Ste inhauser R. A defect ive unidi rec tional dome valve
was not discovered during normal testing . J Clin Eng 1991;16:485–490.
[Med line Link]
454. Hornbein TF, Glauber DT. Inadvertent inspiration of carbon dioxide.
Anesthesiology 1984;61:114.
[Med line Link]
455. Aung SM, Ramez-Salem M, Podraza AG, e t al . An unusual cause of carbon
dioxide rebreathing in a ci rc le absorber system. Anesth Analg 1994;78:1027–
1028.
[Fu ll text Link]
[CrossRef]
[Med line Link]
456. Thorning GP, Groba CB. Cri tical inc ident due to a corroded exp iratory valve.
Anaesthesia 2005;60:823–824.
[Fu ll text Link]
[CrossRef]
[Med line Link]

457. Dawood AM, Digger T. An apparently normal looking valve as a cause of
rebreathing. Anaesthesia 2002;57:929–930.
[Fu ll text Link]
[Med line Link]
458. Ki tagawa H, Sai Y, Nosaka S, et a l. A new leak test for spec ifying
malfunct ions in the exhalation and inhala tion check valve . Anes th Ana lg
1994;78:611.
[Fu ll text Link]
[CrossRef]
[Med line Link]
459. Yew WS, Hwang NC. Faul ty unidirect ional expiratory valve as a cause of
rebreathing. Anaesthesia 2003;58:1239–1240.
[Fu ll text Link]
[CrossRef]
[Med line Link]
460. Findlay G, Spi t tal M. A subt le cause of c i rc le sys tem failure (let ter). Br J
Anaesth 1995;75:667–668.
[Med line Link]
461. Anonymous . Check valve re ta iners may dislodge in carbon dioxide absorbers.
Biomed Safe Stand 20:108.
462. Chang JL, Larson CE, Bedger RC, e t al . An unusual malfunction of an
anesthet ic machine. Anesthesiology 1980;52:446–447.
[Fu ll text Link]
[CrossRef]
[Med line Link]
463. Berner MS. Profound hypercapnia due to disconnect ion wi thin an anaes thetic
machine. Can J Anaesth 1987;34:622–626.
[Med line Link]
464. Dunn AJ . Empty tanks and Ba in c i rcui ts . Can Anaesth Soc J 1978;25:337.
[Med line Link]
465. Skil ton R, Kumar R. A new source of gas leak f rom an Ohmeda Exce l 410
machine. Anaesthesia 1995;50:266–267.
[CrossRef]
[Med line Link]
466. Breen M. Letter to the edi tor. Can Anaes th Soc J 1975;22:247.
[Med line Link]

467. Hannal lah R, Rosales JK. A hazard connected wi th re-use of the Bain's c ircui t :
a case report. Can Anaesth Soc J 1974;21:511–513.
[Med line Link]
468. Naqv i NH. Tors ion of inner tube. Br J Anaes th 1981;53:193.
[CrossRef]
469. Peterson WC. Bain c i rcuit . Can Anaesth Soc J 1978;25:532.
470. Mansel l WH. Spontaneous breathing wi th the Bain c ircuit a t low f low rates: a
case report. Can Anaesth Soc J 1976;23:432–434.
[Med line Link]
471. Fukunaga AF. Torsion and disconnection of inner tube of coaxial breathing
c i rcui t. Br J Anaes th 1981;53:1106–1107.
[CrossRef]
472. Roberts PJ. Unattached inner coaxial tube. Anaesthesia 1987;42:1128.
[CrossRef]
473. Read PJH, Lukey R. Potent ial hazard of the Kendall “Bain” c ircui t. Anaes th
Intens Care 1989;17:510.
[Med line Link]
474. Wildsmith JAW, Grubb DJ. Defec tive and misused co-axial c ircui ts .
Anaesthesia 1977;32:293.
[CrossRef]
[Med line Link]
475. Bel l CT, Bell AJ. An unusua l communicat ion? Anaes thesia 1994;49:830.
476. Ghai B, Makkar JK, Bhat ia A. Hypercarbia and arrhythmias resul t ing f rom
faul ty Ba in ci rcui t: a report of two cases. Anesth Analg 2006;102:1903–1904.
[Fu ll text Link]
[CrossRef]
[Med line Link]
477. Jel l ish WS, Nolan T, Kleinman B. Hypercapnia re lated to a faul ty adul t co-axial
breathing c i rcuit . Anesth Analg 2001;93:973–974.
[Fu ll text Link]
[CrossRef]
[Med line Link]
P.427

478. Fox LM. Equipment deadspace in paediatric b reathing systems. Anaesthesia
1992;47:1101–1102.
[CrossRef]
[Med line Link]
479. Raju R. Humidifier-induced hypercarb ia. Anaesthesia 1987;42:672–673.
[CrossRef]
480. Podraza A, Salem MR, Harris TL, et al. Effects of bel lows leaks on anesthesia
venti lato r function. Anesth Analg 1991;72:S215.
481. Dogu TS, Davis HS. Hazards of inadverten tly opposed valves. Anesthesiology
1970;33:122–123.
[Fu ll text Link]
[CrossRef]
[Med line Link]
482. Weaver LK, Fairfax WR, Greenway L. Bilatera l otorrhag ia associated wi th
continuous posit ive ai rway pressure. Chest 1988;93:878–879.
[CrossRef]
[Med line Link]
483. Mayle LL, Reed SJ, Wyche MQ. Excess ive a irway pressures occurring
concurrently wi th use of the Fraser Harlake PEEP valve . Anes thesiol Rev
1990;17:41–44.
484. Blanshard HJ , Milne MR. La tex -f ree reservoir bags : exchang ing one potential
hazard for another. Anaesthesia 2004;59:177–179.
[Fu ll text Link]
[CrossRef]
[Med line Link]
485. Thompson PW. Prevention of the hazard of excessive airway pressure .
Anaesthesia 1979;34:593.
[CrossRef]
[Med line Link]
486. Newton NI, Adams AQ. Excessive ai rway pressure during anesthes ia.
Anaesthesia 1978;33:689–699.
[Med line Link]
487. Johnson T. A s ticking valve. Anaesthes ia 1993;48:89.
[Med line Link]
488. Brockwell RC. Understand ing your anesthesia machine (ASA Ref resher Course
#506). Park Ridge, IL: ASA, 2005.

489. Bai ley PL. Failed release of an activated oxygen flush valve. Anesthesiology
1983;59:480.
[Fu ll text Link]
[CrossRef]
[Med line Link]
490. Puttick N. Hazard from the oxygen f lush control . Anaesthesia 1986;41:222–
224.
[CrossRef]
[Med line Link]
491. McCrirrick A, Warwick JP, Thomas TA. Capnography and awareness .
Anaesthesia 1992;47:1102–1103.
[CrossRef]
[Med line Link]
492. Anderson EC, Rendel l-Baker L. Exposed O2 f lush hazard. Anesthesiology
1982;56:328.
[Fu ll text Link]
[CrossRef]
[Med line Link]
493. Cooper CMS. Capnography. Anaesthesia 1987;42:1238–1239.
[CrossRef]
[Med line Link]
494. Hanafiah Z, Se llers WFS. Nudg ing the emergency oxygen. Anaes thesia
1991;46:331.
[CrossRef]
[Med line Link]
495. Morris S, Barclay K. Oxygen f lush buttons: more cri t ical incidents. Anaesthesia
1993;48:1115–1116.
[Med line Link]
496. Andrews JJ. Unders tanding anes thesia venti lators (ASA Ref resher Course
#242). Park Ridge, IL: ASA, 1990.
497. Anonymous . Barotrauma f rom anesthes ia venti lators . Technol Anesth
1988;9:1–2.
498. Sprung J, Samaan F, Hensler T, et al . Excessive a irway pressure due to
venti lato r control valve malfunc tion during anes thesia for open heart surgery.
Anesthesiology 1990;73:1035–1038.
[Fu ll text Link]
[CrossRef]
[Med line Link]
499. Alston RP. Expiratory obstruc tion in a c i rc le system. Anaesthesia
1987;42:1120.
[CrossRef]
[Med line Link]
500. Bishay EG, Echiverri E, Abu-Zaineh M, e t al . An unusual cause for a irway
obstruct ion in a young hea lthy adu lt . Anesthesiology 1984;60:610–611.
[Fu ll text Link]
[CrossRef]
[Med line Link]
501. Hindman BJ, Sperring SJ. Part ial expiratory l imb obstruction by a foreign body
abutt ing upon an Ohio 5400 volume moni tor sensor. Anesthesiology 1986;65:349–
350.
[Med line Link]
502. Jack TM. An unusual cause of complete expiratory obstruc tion. Anaes thesia
1987;42:564.
[CrossRef]
[Med line Link]
503. Hi lgenberg JC, Burke BC. Posi tive end-expira tory pressure produced by water
in the condensat ion chamber. Anesth Analg 1985;64:541–543.
[Fu ll text Link]
[CrossRef]
[Med line Link]
504. Anonymous . Dryden anesthes ia breathing c i rcuits . Technol Anesth 1988;8:4–
5.
505. Register SD. Detection o f defective equipment by proper preanes thetic
checks . Anesthesiology 1985;62:546–547.
[Fu ll text Link]
[CrossRef]
[Med line Link]
506. Smith CE, Otworth JR, Kaluszyk P. Bi lateral tension pneumothroax due to a
defec tive anesthesia breathing c i rcu it f i l ter. J Clin Anes th 1991;3:229–234.
[CrossRef]
[Med line Link]

507. Anonymous . Anesthesia death re lated to “wet” oxygen f i l te rs . Biomed Safe
Stand 1993;12:11–12.
508. Barton RM. Detection of expiratory antibacteria l f i l te r occlus ion. Anesth Analg
1993;77:197.
[Fu ll text Link]
[CrossRef]
[Med line Link]
509. McEwan AI, Dowell L, Karis JH. Bila teral tension pneumothorax caused by a
blocked bac terial f i l te r in an anesthes ia breathing c i rcui t. Anesth Analg
1993;76:440–442.
[Med line Link]
510. Thomson AR, Gordon NH. One-way valve malfunct ion in a c i rc le system.
Anaesthesia 1995;50:920–921.
[CrossRef]
[Med line Link]
511. Hamad M, Morgan-Hughes NJ, Beechey AP. Expiratory obstruct ion caused by
inappropriate connection o f the expiratory l imb of a breathing ci rcu it . Anaesthes ia
2003;58:719–720.
[Fu ll text Link]
[CrossRef]
[Med line Link]
512. Johnson RA, Vries LAG. High ai rway pressures wi th s tick ing one-way valves in
a c i rc le system. Anaesthesia 1999;54:406.
[Fu ll text Link]
[CrossRef]
[Med line Link]
513. Flowerdew RMM. A hazard of scavenger port design . Can Anaesth Soc J
1981;28:481–483.
[Med line Link]
514. Holley HS, Eisenman TS. Hazards of an anesthetic scavenging device . Anes th
Analg 1983;62:458–460.
[Fu ll text Link]
[CrossRef]
[Med line Link]
515. Mann ES, Sprague DH. An easi ly overlooked malassembly. Anesthesiology
1982;56:413–414.
[Fu ll text Link]
[CrossRef]
[Med line Link]
516. Stevens IM. Hazardous misconnec tion. Anaes th Intens Care 1988;16:374–
375.
[Med line Link]
517. Tavakol i M, Habeeb A. Two hazards of gas scavenging. Anesth Analg
1978;57:286–287.
[Fu ll text Link]
[CrossRef]
[Med line Link]
518. Edwards ND. Another misconnec tion. Anesthes io logy 1988;43:1066.
519. Anagnos tou JM, Hults SL, Moorthy SS. PEEP valve barotrauma. Anesth Analg
1990;70:674–675.
[CrossRef]
[Med line Link]
520. Anonymous . Pos it ive end exp iratory pressure valves. Technol Anesth
1991;11:11.
521. Kacmarek RM, Dimas S, Reyno lds J , et al . Technical aspects of posit ive end-
expiratory pressure (PEEP). Part I I. PEEP with posi t ive-pressure venti lat ion. Respir
Care 1982;27:1490–1504.
[Med line Link]
522. Anonymous . PEEP valves in anesthesia c i rcui ts . Heal th Dev ices 1983;13:24–
25.
523. Cooper JB. Unidirectional PEEP valves can cause safety hazards . APSF
News le tt 1990;5:28–29.
524. Anonymous . Dupaco bag tail scaveng ing valves. Technol Anesth 1983;4(6):1–
2.
525. Prince GD, Nichols BJ. Kinked breath ing systems—again . Anaesthesia
1989;44:792.
[CrossRef]
[Med line Link]
526. Munro HM. An accident wi th the Lack system. Anaesthesia 1990;45:601–602.
[CrossRef]
[Med line Link]

527. Goldsmith M. FDA issues pedia tric respiratory device ale rt . JAMA
1983;250:2264.
[CrossRef]
[Med line Link]
528. Branson R, Lam AM. Increased resistance to breathing: a potent ially lethal
hazard across a coaxia l ci rcui t-connector coupling. Can J Anaesth 1987;34:S90–
S91.
529. Vi ll fo rth JC. FDA safety alert . Breathing sys tem connec tors. Rockv il le, MD:
U.S. Food and Drug Administration, September 2, 1983.
530. Sloan IA, Ironside NK. Internal mis-mating of breathing system components.
Can Anaesth Soc J 1984;31:576–578.
[Med line Link]
531. Hi lton PJ, Clement JA. Surg ical emphysema resu lting f rom a venti lator
malfunct ion. Anaesthesia 1983;38:342–345.
[CrossRef]
[Med line Link]
532. Anonymous . Pre-use tes ting prevents “helpful ” reconnect ion of anes thesia
components . Technol Anesth 1987;8 :1–2.
533. Henzig D. Ins idious PEEP f rom a defec tive venti lator gas evacuation outlet
valve. Anesthesiology 1982;57:251–252.
[Med line Link]
534. Chaney MA. Del ivery of excessive airway pressure to a patien t by the
anesthesia mach ine. Anesth Analg 1993;76:1166–1167.
[Fu ll text Link]
[CrossRef]
[Med line Link]
535. Roth S, Tweedie E, Sommer RM. Excessive airway pressure due to a
malfunct ioning anes thesia vent i lator. Anes thesiology 1986;65:532–534.
[Full text Link]
[CrossRef]
[Med line Link]
536. Burgess RW. Blockage of spi l l valve . Anaesth Intens Care 1986;14:327–328.
[Med line Link]
537. Primiano F Jr. Open ad jus table pressure l imited valve. Anes thesiology
1998;88: 552.
[Fu ll text Link]

[CrossRef]
[Med line Link]
538. Ki tsberg A, Wolf f T. Pi tfal ls of disposable equ ipment. Anaesthesia
1999;54:818–819.
539. De la Rocha AR. Danger in an unpopped valve. APSF Newslett 1987;3:5.
540. Harper NJN. A new APL valve hazard. Anaesthesia 2001;56:1119–1120.
[Fu ll text Link]
[Med line Link]
541. Smith N. The self-regulating bag. Anaesthesia 2001;56:276–277.
[Fu ll text Link]
[CrossRef]
[Med line Link]
542. Sharrock ME, Le ith DE. Potent ial pulmonary barotrauma when venting
anesthet ic gases to suct ion. Anesthesiology 1977;46:152–154.
[Fu ll text Link]
[CrossRef]
[Med line Link]
543. Rendel l-Baker L. Hazard o f blocked scavenging valve. Can Anaesth Soc J
1982;29:182–183.
[Med line Link]
544. O'Conner DE, Daniels BW, Pf itzner J. Hazards of anaesthet ic scavenging:
case reports and brief rev iew. Anaesth Intens Care 1982;10:15–19.
[Med line Link]
545. Mal loy WF, Wrightman AE, O'Sull ivan D, e t al . Bi lateral pneumothorax f rom
suction appl ied to a venti lator exhaust valve . Anes th Analg 1979;58:147–149.
[CrossRef]
[Med line Link]
546. Dav ies G, Tarnawsky M. Letters to the edi to r. Can Anaes th Soc J
1976;23:228.
[Med line Link]
547. Hami lton RC, Byrne J . Another cause of gas -scavenging-line obs truct ion.
Anesthesiology 1979;51:365–366.
[Fu ll text Link]
[CrossRef]
[Med line Link]

548. Hagerdal M, Lecky JH. Anesthet ic death of an experimenta l animal related to a
scavenging sys tem malfunct ion. Anesthesiology 1977;47:522–523.
[Fu ll text Link]
[CrossRef]
[Med line Link]
549. Carvalho B. Hidden hazards of scavenging. Br J Anaesth 1999;83:532–533.
[Med line Link]
550. Hwang N. Hidden hazards of scavenging. Br J Anaesth 2000;84:827.
[Med line Link]
551. Carvalho B. Hidden hazards of scavenging. Br J Anaesth 2000;84:827.
[Med line Link]
552. Hayes C. An in teres ting misconnexion. Anaes thesia 1991;46:508–509.
[CrossRef]
[Med line Link]
553. Sainsbury DA. Scavenging misconnec tion. Anaes th In tens Care 1985;13:215–
216.
[Med line Link]
554. Phi l lips S. Scavenging hazard. Anaes th Intens Care 1991;19:615.
[Med line Link]
555. Berry JM, Blanks S. Misplaced valve poses potential hazard. APSF News le tt
2004;19:8.
556. Anonymous . Improperly c leaned resusc itator valves may st ick & block a irway.
Biomed Safe Stand 1991;21:105–107.
557. Dolan PF, Shapiro S, S teinbach RB. Va lve misassembly—manual ly opera ted
resusci tation bag. Anesth Analg 1981;60:66–67.
[Fu ll text Link]
[CrossRef]
[Med line Link]
558. Kl ick JM, Bushnell LS, Bancrof t ML. Barotrauma, a po tential hazard of manual
resusci tators. Anesthesiology 1978;49:363–365.
[Fu ll text Link]
[CrossRef]
[Med line Link]
559. Jumper A, Desai S, Liu P, e t al . Pulmonary barotrauma result ing from a faul ty
Hope I I resusci tation bag. Anes thesiology 1983;58:572–574.
[Fu ll text Link]

[CrossRef]
[Med line Link]
560. Pauca AL, Jenkins TE. A irway obs truction by breakdown of a nonrebreathing
valve. How foolproof is foolproof? Anes th Analg 1981;60:529–531.
561. Katz L, Crosby JW. Accidenta l misconnections to endotracheal and
tracheos tomy tubes. Can Med Assoc J 1986;135:1149–1151.
[Med line Link]
562. Wasserberger J, Ordog GJ, Turner AF, et al . Ia trogenic pulmonary
overpressure accident. Ann Emerg Med 1986;15:947–951.
[CrossRef]
[Med line Link]
563. Onsiong MK. Potential hazard of Hudson facemask. Anaes thesia
1988;43:907.
[Med line Link]
564. Newton NI. Supp lementary oxygen—potential for d isaster. Anaesthesia
1991;46:905–906.
[CrossRef]
[Med line Link]
565. Dav ies JR. A false compatibil i ty. Anaes thesia 1991;46:991.
[CrossRef]
[Med line Link]
566. Dubinsky IL . Near death caused by acc idental misconnec tion to an
endotracheal tube. Can Med Assoc J 1987;137:1105–1106.
[Med line Link]
567. Wasserberger J, Ordog GJ. Why endotracheal and oxygen tub ing might be
misconnected. Can Med Assoc J 1988;139:372.
[Med line Link]
568. Grime PD, Mal ins TJ. Hazard warn ing . A case of post-operative pu lmonary
barotrauma. Br J Oral Max il lofac Surg 1991;29:183–184.
[CrossRef]
[Med line Link]
569. Onsiong MK. Potential hazard of Hudson facemask. Anaes thesia
1988;43:907.
[Med line Link]
570. Giesecke AH, Sk rivanek GD. Respiratory obstruc tion in the recovery room.
Anesth Analg 1992;75:639.

[Fu ll text Link]
[CrossRef]
[Med line Link]
571. Markovi tz BP, Si lverberg M, God inez RI. Unusual cause of an absent
capnogram. Anesthesiology 1990;71:992–993.
[Fu ll text Link]
[CrossRef]
[Med line Link]
572. Eisenk raft JB. Problems with anesthesia gas del ivery sys tems (ASA Refresher
Course). Atlanta: ASA, 2005.
573. Highley DA. Condensat ion . Anaesthesia 1994;49:1101.
[CrossRef]
[Med line Link]
574. Jones RM. Inadvertent PEEP in a paedia tric b reathing system. Anaesthesia
1996;51:203–204.
[Fu ll text Link]
[CrossRef]
[Med line Link]
575. Shankar H. High airway pressure mandates diagnosis and remedy. APSF
News le tt 2005;20:23.
576. Ramachandran K, Chadwick S, Robson G. A ‘fo reign body’ in the c ircui t f i l ter.
Anaesthesia 2003;58:186.
[Fu ll text Link]
[CrossRef]
[Med line Link]
577. Lack JA. Another ai rway foreign body. Anaesthesia 2002;57:189.
[Fu ll text Link]
[Med line Link]
578. Dav is R. Soda lime dust. Anaesth In tens Care 1979;8:390.
[Med line Link]
579. Lauria JI. Soda-l ime dus t contamination of b reathing c i rcui ts . Anes thesiology
1975;42:628–629.
[Fu ll text Link]
[CrossRef]
[Med line Link]
580. Good ie D, Stewart I . Ulco carbon dioxide absorber. Anaesth Intens Care
1991;19:609–610.
[Med line Link]
581. Sch il le r DJ. Rusty water in an oxygen f lowmeter. Anaes thesia 1986;41:1061.
[CrossRef]
[Med line Link]
582. Anonymous . Oxygen cyl inders recal led because of o il contaminat ion. Biomed
Safe Stand 1991;21:20.
583. Russell WJ. Indus trial gas hazard. Anaesth In tens Care 1985;13:106.
[Med line Link]
584. Eichorn JH, Bancrof t ML, Laasberg LH, e t al . Contaminat ion of medical gas
and water pipel ines in a new hospi tal building. Anesthesiology 1977;46:286–289.
[Fu ll text Link]
[CrossRef]
[Med line Link]
585. Gilmour IJ , McComb RC, Palahniuk RJ. Contamination of a hospi tal oxygen
supply. Anesth Analg 1998;71:302–304.
[Fu ll text Link]
[CrossRef]
[Med line Link]
586. Coveler LA, Lester RC. Contaminated oxygen cyl inder. Anes th Ana lg
1989;69:674–676.
[Fu ll text Link]
[CrossRef]
[Med line Link]
587. Clutton-Brock J. Two cases of poisoning by contaminat ion of ni trous oxide with
higher oxides of ni trogen during anaesthes ia. Br J Anaes th 1967;39:388–392.
[CrossRef]
[Med line Link]
588. Moss E, Nagle T. Medical ai r sys tems are complex , usually poorly unders tood.
APSF News le tt 1996;11:18–21.
P.428
589. Anonymous . Oxygen sys tem contamination probed in pat ient deaths. Biomed
Safe Stand 1996;26:57–58.
590. Moss E. Hospi tal deaths reportedly due to contaminated O2. APSF Newslett
1996;11:13–18.
591. Moss E. Dangers seen poss ib le f rom contaminated medical gases. APSF
News le tt 1993;8:6–7.
592. Bjerring P, Oberg B. Bac terial contamination of compressed air for medical
use. Anaesthesia 1986;41:148–150.
[CrossRef]
[Med line Link]
593. Bjerring P, Oberg B. Possible role of vacuum sys tems and compressed ai r
generators in c ross-infec tion in the ICU. Br J Anaesth 1987;59:648–650.
[CrossRef]
[Med line Link]
594. Oberg B, Bjerring P. Comparison of microbiologica l contents of compressed ai r
in two Danish hospi ta ls . Effec t of oil and water reduct ion in ai r-genera ting uni ts .
Acta Anaesthesiol Scand 1986;30:305–308.
[Med line Link]
595. Warren RE, Newsom SWB, Matthews JA, et al. Medical g rade compressed air.
Lancet 1986;1:1438.
[CrossRef]
[Med line Link]
596. Taylor BL, Rainbow C, Ford D. Debris in a breathing system. Anaesthesia
1989;44:702.
[CrossRef]
[Med line Link]
597. James PD, Gothard JWW. Possible hazard f rom the inserts of condenser
humidif iers. Anaes thesia 1984;39:70.
[CrossRef]
[Med line Link]
598. Oh T. Bagging a foreign body. Anaesth Intens Care 1978;6 :89–91.
[Med line Link]
599. Ross A . Oxygen analyser hazard . Anaesth Intens Care 1986;14:466–467.
[Med line Link]
600. Anonymous . Inte rsurgica l—adult , ped ia tric breathing ci rcui ts : risk of inhala tion
of manufacturing debris . Heal th Dev ices 2002;26:2 .
601. Anonymous . Dev ice safe ty alert. Anesthesia gas elbow component may
separate . Biomed Safe Stand 1989;19:90.

602. Paulus DA. Dri l l ing remnants in elbow adapters . Anes th Ana lg 1986;65:824.
[Fu ll text Link]
[CrossRef]
[Med line Link]
603. Anonymous . Heat and moisture exchangers and f i l te rs: components may enter
breathing sys tems and cause blockages. Heal th Dev ices Alerts 2004;28(36): 5–6.
604. Gold MI. Defec t in a T-f i t ting connect ion. Anesthesiology 1980;52:184.
[Fu ll text Link]
[CrossRef]
[Med line Link]
605. Wald A, Mercurio A. Bl is te ring of epoxy material of Narco Airshields vent i lator
Anesthesiology 1983;58:390.
606. Nimmagadda UR, Salem MR, Klowden AJ, et al . An unusual foreign body in
the lef t main bronchus af ter open heart surgery. Anesth Analg 1989;68:803–805.
[Fu ll text Link]
[CrossRef]
[Med line Link]
607. Si le r JN, Neumann G. Latex glove hazard. APSF Newslett 1992;7 :11.
608. Razvi SAH.A live “foreign body” in an anaes thetic c i rcuit .2005;60:102–103.
609. Singh B, Bhardwaj M. A l ive foreign body in the breathing c i rcui t. Anesth Analg
2006;102:1293.
[Fu ll text Link]
[CrossRef]
[Med line Link]
610. Scott DM. Performance of BOC Ohmeda Tec 3 and Tec 4 vaporizers fol lowing
t ipp ing. Anaesth Intens Care 1991;19:441–443.
[Med line Link]
611. Ri ley RH, Hammond KA, Currie MS. “Hazards” of oxygen therapy during sp inal
anaesthesia . Anaesthesia 1991;46:421.
[CrossRef]
[Med line Link]
612. Will iams L , Barton C, McVey JR, e t al . A v isual warning device for improved
safety. Anesth Analg 1986;65:1364.
[Fu ll text Link]
[CrossRef]
[Med line Link]

613. Currie M, Mackay P, Morgan C, et a l. The “wrong drug” p rob lem in
anaesthesia : an analys is o f 2000 incident reports . Anaesth Intens Care 1993:
21:596–601.
[Med line Link]
614. Woehl ick HJ. Hazards of supplying supplemental oxygen through main gas
f lowmeters. Anesthes io logy 1993;78:401–402.
615. Bruce DL, Linde HW. Vaporization of mixed anes thetic l iquids. Anesthesiology
1984;342–346.
616. Chilcoat RT. Hazards of mis-f il led vaporizers. Summary tables. Anesthes io logy
1985;63:726–727.
[Fu ll text Link]
[CrossRef]
[Med line Link]
617. Martin S. Hazards of agent-specific vaporizers. A case report of successful
resusci tation after massive isof lu rane overdose. Anesthesiology 1985;62:830–
831.
[Fu ll text Link]
[CrossRef]
[Med line Link]
618. Block FE, Schul te GT. Observations on use of wrong agent in an anes thesia
agent vaporizer. J Cl in Moni t 1999;15:57–61.
619. Kel ly DA. Free-s tanding vaporizers. Anaes thesia 1985;40:661–663.
[CrossRef]
[Med line Link]
620. Railton R, Ingl is MD. High halothane concentrations f rom reversed f low in a
vaporizer. Anaes thesia 1986;41:672–673.
[CrossRef]
[Med line Link]
621. Yee S, Old S. Any wh ich way but loose: the s ignif icance of gas f low di rec tion
through a vaporizer. Anaesthesia 2000;55:598–600.
622. Sinclai r A, Van Bergeb H. Vaporizer overf i l l ing. Can J Anaesth 1993;40:77–
78.
[Med line Link]
623. Cra ig DB. Vaporizer overf i ll ing. Can Anaesth Soc J 1993;40:1005–1006.
624. Daniels D. Overf i l l ing of vaporizers. Anaesthesia 2002;57:288.
[Fu ll text Link]
[CrossRef]
[Med line Link]
625. Buettner AU. Failure of vaporizer inte rlock mechanism. Anaesth Intens Care
2000;28:451–452.
[Med line Link]
626. Webb C, Ringrose D, S tone A . Faul ty interlock on Drager vaporisers .
Anaesthesia 2005;60:628–629.
[Fu ll text Link]
[CrossRef]
[Med line Link]
627. Amir M. Caught by a cage. Anaesth Intens Care 1992;20:389–390.
[Med line Link]
628. Lewyn MJ . Pat ient wins damages for inju ry secondary to “l ight” anesthesia.
Anesth Malprac Protector 1991;3 :109–113.
629. Anonymous . JCAHO sentinel event alert: p revent ing and manag ing the impact
of anesthesia awareness . Heal th Devices Alerts 2004;28(44):1–2.
630. Domino KB, Posner KL, Caplan RA, e t al . Awareness during anesthesia . A
c losed c laim ana lysis. Anesthesiology 1999;90:1053–1061.
[Fu ll text Link]
[CrossRef]
[Med line Link]
631. Francis RN. Failure o f ni trous ox ide supply to theatre pipel ine system.
Anaesthesia 1990;45:880–882.
[CrossRef]
[Med line Link]
632. Yogananthan S. Fai lu re of nitrous oxide supply. Anaesthes ia 1990;45:897.
[CrossRef]
633. Paul DL. Pipeline fa ilure. Anaesthesia 1989;44:523.
[CrossRef]
634. Comber REH. Penlon rotameter block fai lu re. Anaes th Intens Care
1990;18:141–142.
[Med line Link]
635. James RH. Rotameter sequence—a variant of “read the labe l.” Anaesthesia
1996;51:87–88.
[Fu ll text Link]
[CrossRef]

[Med line Link]
636. Cra ig DB, Longmuir J . An unusual fai lure of an oxygen fa il -safe device. Can
Anaesth Soc J 1971;18:576–577.
[Med line Link]
637. Puri GD, George MA, Singh H, et al . Awareness under anaesthes ia due to a
defec tive gas -loaded regulator. Anaesthesia 1987;42:539–540.
[CrossRef]
[Med line Link]
638. Brahams D. Anaesthes ia and the law. Awareness and pain during anaesthesia .
Anaesthesia 1989;44:352.
[CrossRef]
[Med line Link]
639. Judkins KC. BOC Boyle M anaes thetic machine—a modif ication. Anaesthesia
1983;38:387–388.
[CrossRef]
[Med line Link]
640. Paymaster NJ. Inadvertent administra tion of 100% oxygen during anaesthesia.
Br J Anaesth 1978;50:1268.
[CrossRef]
[Med line Link]
641. Dodd KW. Inadvertent administrat ion of 100% oxygen during anaesthesia . Br J
Anaesth 1979;51:573.
[CrossRef]
642. Longmuir J , Craig DB. Misadventure wi th a Boyle 's gas machine. Can Anaes th
Soc J 1976;23:671–673.
[Med line Link]
643. Peters KR, Wingard DW. Anesthes ia mach ine leakage due to misal igned
vaporizers . Anes th Rev 1987;14:36–39.
644. Mann DP, Der Ananian J , Alston TA. Oxygen flush valve booby trap.
Anesthesiology 2004;101:558.
[Fu ll text Link]
[CrossRef]
[Med line Link]
645. Aziz E, Sanders GM. Fai lu re of Datex AS/3 anaesthes ia delivery uni t.
Anaesthesia 2000;55:1214–1215.
[Fu ll text Link]

[CrossRef]
[Med line Link]
646. Ghai B, Makkar JK. An unusual cause of fau lty Tec 7 vaporizer. Anesth Analg
2005;101:1890–1891.
[Fu ll text Link]
[CrossRef]
[Med line Link]
647. Orme R, Grange C. Vaporizer failu re. Anaes thesia 1999;54:111–112.
648. Green M, Bugg N, Ho lt P . Failed inhalationa l induc tion—a faul ty vaporizer.
Anaesthesia 1995;50:85–86.
[CrossRef]
[Med line Link]
649. Lewis SE, Andrews JJ, Long GW. An unexpec ted Penlon Sigma El i te vaporizer
leak. Anesthesiology 1999;90:1221–1224.
[Fu ll text Link]
[CrossRef]
[Med line Link]
650. Ngan J , Cashen D, Nichols G. Sevoflurane vaporizers . Can J Anes th
1999;46:200.
651. Cartwright DP, Freeman MF. Vaporizers. Anaesthesia 1999;54:519–520.
[Fu ll text Link]
[CrossRef]
[Med line Link]
652. Cudmore J, Keogh J. Another Selecta tec switch malfunction. Anaesthesia
1990;45:754–756.
[CrossRef]
[Med line Link]
653. Lamberty JM, Lerman J. Intraoperat ive fai lure of a f luotec Mark I I vapourizer.
Can Anaesth Soc J 1984;31:687–689.
[Med line Link]
654. Mal tby JR. In traopera tive failure of a Fluotec Mark I I vapourizer. Can Anaesth
Soc J 1985;32:200.
[Med line Link]
655. Anonymous . Anesthesia uni t vaporizers. Technol Anesth 1997;17(10):9.
656. Duff PJ, Roll ison RA, Lee TW. Selectatec problems: again and aga in. Anaesth
Intens Care 1994;22:622.

[Med line Link]
657. Dwyer M, Hol land R, Shepherd L , et al. Vaporizer and Selecta tec leaks.
Anaesth Intens Care 1994;22:739.
[Med line Link]
658. Chambers JC, Hough MB. Awareness hazard using a Tec 6 vaporiser.
Anaesthesia 2005;60:942.
[Fu ll text Link]
[CrossRef]
[Med line Link]
659. Mit ton M. Awarenesss hazard using a Tec 6 vaporiser. A rep ly. Anaesthesia
2005;60:942.
[Fu ll text Link]
660. Garstang JS. Gas leak from Tec 5 isof lurane vaporizer. Anaesthesia
2000;55:915.
[Fu ll text Link]
[CrossRef]
[Med line Link]
661. Duncan JAT. Select-a-tec swi tch malfunc tion. Anaes thesia 1985;40:911–912.
[CrossRef]
[Med line Link]
662. Chum NL. A potential c ircui t leak wi th Tec 5 vaporizers. Anesthesiology
1997;87:1599.
[Fu ll text Link]
[CrossRef]
[Med line Link]
663. Vohra SB. Leaking vaporizer. Anaesthesia 2000;55:606–607.
[Fu ll text Link]
[CrossRef]
[Med line Link]
664. MacLeod DM, EcEvoy L, Walker D. Report of vaporizer malfunc tion.
Anaesthesia 2002;57:299–300.
[Fu ll text Link]
[CrossRef]
[Med line Link]
665. Fernando PM, Peck DJ . An uncommon cause of vaporizer failure. Anaesthes ia
2001;56:1009–1010.

[Fu ll text Link]
[CrossRef]
[Med line Link]
666. Barcroft JP. Is there l iquid in the vaporizer? Anaesthesia 1989;44:939.
667. Found P, Forrest AP. Vaporizer level obstruct ion detected by anesthetic vapor
analys is. Anesth Analg 1999;88:469.
[Fu ll text Link]
[CrossRef]
[Med line Link]
668. Varma RR, Whitesell RC, Iskandarani MM. Ha lothane hepati tis wi thout
halothane. Role of inapparent c ircui t contamination and i ts p revention. Hepatology
1985;5:1159–1162.
[CrossRef]
[Med line Link]
669. El lis FR, Clarks IMC, Modgil l EM, et al. New causes o f mal ignant
hyperpyrexia. Br Med J 1975;1:575.
[Med line Link]
670. Bridges RT. Vaporizers—serv iced and checked? Anaesthesia 1991;46:695–
697.
671. Cook TL, Eger EI, Behl RS. Is your vaporizer off? Anesth Analg 1977;56:793–
800.
672. Robinson JS, Thompson JM, Barratt RS. Inadvertent contamination of
anaesthetic c ircui ts with halothane. Br J Anaesth 1977;49:745–753.
[CrossRef]
[Med line Link]
673. Ri tchie PA, Chesh ire MA, Pearce NH. Decontaminat ion of halothane f rom
anaesthetic machines achieved by cont inuous f lushing wi th oxygen. Br J Anaesth
1988;60:859–863.
[CrossRef]
[Med line Link]
674. Stree ts C, Davies P. Shou ld we perform a sniff tes t? Anaesthes ia
2000;55:509–510.
675. Beebe JJ, Sessler KI. Preparat ion of anesthesia machines for patien ts
susceptible to mal ignant hyperthermia. Anes thesiology 1988;69:395–400.
[Fu ll text Link]
[CrossRef]

[Med line Link]
676. McGraw TT, Keon TP. Malignant hyperthermia and the c lean machine. Can J
Anaesth 1989;36:530–532.
[Med line Link]
677. Cooper JB, Phil ip JH. More on anes thesia machines and malignant
hyperpyrexia. Anesthesiology 1989;70:561–562.
[Fu ll text Link]
[CrossRef]
[Med line Link]
678. Samulksa HM, Ramaiah S, Nob le WH. Unintended exposure to halothane in
surgical pat ients. Halothane washout studies. Can Anaes th Soc J 1972;19:35–41.
[Med line Link]
679. Gil ly H, Weindlmayr-Goettel M, Koberl H, et al. Anaes thetic uptake and
washout characteris tics of patien t c i rcuit tub ing wi th special regard to curren t
decontaminat ion techniques . Acta Anaesthesiol Scand 1992;36:621–627.
[Med line Link]
680. Petroz GC, Lerman J. Preparation o f the Siemens KION anesthet ic machine
for patients suscept ib le to malignant hyperthermia. Anesthesiology 2002;96: 941–
946.
[Fu ll text Link]
[CrossRef]
[Med line Link]
681. Smith WQ. Inadvertent inhala tion anaesthesia during surgery under
retrobu lbar eye block. Br J Anaesth 1998;81:793–794.
[Med line Link]
682. Stone AGH. Supplementary oxygen during Caesarean section. Anaesthesia
2006;61:298.
[Fu ll text Link]
[CrossRef]
[Med line Link]
683. Sakai T, Mc Intyre JWR, Baba S, et al . Push and pul l: move your anesthesia
machine more eas ily. Anesth Analg 1994;79:196–197.
[Fu ll text Link]
[CrossRef]
[Med line Link]

684. Sakai T. Protecting anaesthetic tubing from occlus ion. Br J Anaesth
2001;87:324.
[Med line Link]
685. Dell R, Cochrane D. Protecting anaes thetic tubing from occlusion . Br J
Anaesth 2000;84:698.
[Med line Link]
686. Ayllon IR, Mi l ls GH. Protect ing anaesthetic tubing from occlusion: an inbui l t
so lut ion. Br J Anaes th 2000;85:498.
[Med line Link]
687. Catto DD. Medical device safety alert . Drager Serv ice , Telford, PA., Feburary,
2001.
688. Tri JL, Severson RP, Fir i AR, e t al . Cellu lar telephone interference wi th
medical equ ipment. Mayo Clin Proc 2005;80:1286–1290.
[Med line Link]
689. Lyznicki JM, Al tman RD, Wi ll iams, MA. Report of the American Medical
Associat ion (AMA) Counci l on Scientif ic Affa irs and AMA recommendations to
medical professiona l s taff on the use of wire less rad io-f requency equipment in
hospi tals . Biomed Ins trum Technol 2001;35:189–195.
[Med line Link]
690. Wal lin MKE, Marve T, Hakansson PK. Modern wire less te lecommunication
technologies and their electromagnetic compatibi l i ty wi th l i fe -supporting equipment.
Anesth Analg 2005;101:1393–1400.
[Fu ll text Link]
[CrossRef]
[Med line Link]
P.429
691. Lauder PG. Mobile phone use in hosp itals . Anaesthesia 2006;61:616.
[Fu ll text Link]
[CrossRef]
[Med line Link]
692. Arms trong JN, Davies JM. A systematic method for the investigat ion of
anaesthetic inc idents. Can J Anaesth 1991;38:1033–1035.
[Med line Link]

693. Eagle CJ, Davies JM, Reason J. Accident analys is of la rge-scale technological
disas ters applied to an anaes thetic complicat ion. Can J Anaesth 1992;39: 118–
122.
[Med line Link]
694. Cooper JB, Cul len DJ , Eichhorn JH, e t al . Administrat ive guidel ines fo r
response to an adverse anesthesia event. J Clin Anes th 1993;5:79–84.
[CrossRef]
[Med line Link]
695. Forsel l RD. The cl in ical engineer's role in inc ident investigation . Biomed Inst
Tech 1993;27:378–383.
696. Lee RB. Reply to guide lines and techniques for the inves tigat ion of anesthet ic
accidents. J Clin Anesth 1994;6:171–172.
[CrossRef]
[Med line Link]
697. Marders J . FDA encourages the reporting of med ical device adverse events:
f ree-hosing hazards . APSF News lett 2002;17:41.
698. Anonymous . Medical dev ice report ing under the Safe Medical Devices Ac t: A
guide for healthcare fac il i t ies. ECRI, Plymouth Meeting, PA., 1991.
P.430
Questions For the fol lowing quest ions, answer
• f A, B , and C are correct
• i f A and C are correct
• i f B and D are correct
• is D is correct
• i f A, B, C, and D are correct.
1. Hypercarbia due to an incompetent unidirectional valve can be distinguished from that due to exhausted absorbent by A. The shape of the carbon dioxide waveform
B. An increase in inspired carbon dioxide
C. Increas ing the f resh gas f low
D. Absence of heat in the absorber

View Answer2. Causes of air entrainment include A. Suction applied to an nasogas tric tube curled in the esophagus
B. Malfunct ion of the in terface of a c losed scavenging system
C. Use of a mainstream gas analyzer
D. A leak in the venti lato r bel lows
View Answer3. What course of action should be taken if a gas crossover in the pipeline system is suspected? A. Use the oxygen f lush on the machine to purge the crossed gas
B. Disconnect the pipel ine, and open an oxygen cylinder
C. Turn up the f lowmeter for the crossed gas, and tu rn off the oxygen flowmeter
D. Use a resusci ta tion bag to vent i late wi th room a ir
View Answer4. Color(s) which an oxygen cylinder may be painted include
A. Black
B. Whi te
C. Blue
D. Green
View Answer5. Safety mechanism(s) that prevent a hypoxic mixture being delivered because the flowmeters are incorrectly set include A. The oxygen failure safe ty valve
B. An oxygen analyzer
C. The oxygen pressure fa ilure a la rm
D. Proport ioning system
View Answer6. A lower-than-expected anesthetic level may be caused by
A. Sevoflu rane breakdown by desiccated absorbent
B. A leak in a venti lator bellows
C. Vaporizer leak
D. Air f rom a light source
View Answer7. Which measures should be taken in the event that the oxygen pipeline supply is lost? A. Use low f resh gas flows
B. Open an oxygen cyl inder
C. Disconnect the machine f rom the centra l supply
D. Turn the pis ton venti lator OFF
View Answer8. A leak in the breathing system should be suspected if
A. The end-tidal carbon dioxide begins to increase
B. There is a change in the venti la tor sound

C. A standing venti lator bellows fails to return to the top of i ts housing
D. The FiO2 decreases during controlled vent i la tion
View Answer9. Which situations would result in a negative pressure in the breathing system?
A. Nasogastric tube p laced in the trachea
B. Suction applied to a work ing channel of a f iberscope
C. Malfunction of valves in a closed scavenging interface
D. Loss of oxygen pressure to the machine.
View Answer10. An obstruction in the breathing system may cause A. An increase in the peak breathing system pressure
B. Ac tivat ion of the high pressure alarm
C. Hypoventi lat ion
D. Decreased movement of the vent ilator bellows
View Answer11. Which monitors are reliable detectors of a breathing system disconnection?
A. Carbon d ioxide
B. Airway pressure
C. Respirometer
D. Oxygen analyzer
View Answer12. Causes of carbon dioxide in the inspiratory gas include A. Absorbent being bypassed
B. Inadequate f resh gas flow to a c i rc le breathing system
C. An incompetent unidirect ional valve
D. Excess carbon dioxide produc tion
View Answer13. Excessive airway pressure may be caused by
A. Malfunct ion of the APL valve
B. Use o f the oxygen f lush during inspira tion wi th certain mechanical venti lators
C. Obs truction in the scavenging system
D. A unidi rect ional PEEP valve p laced in the expiratory l imb
View Answer14. Anesthetic agent overdosage may be caused by
A. Isof lurane in a halothane vaporizer
B. Reversed f low through a vaporizer
C. Enf lurane in an isof lurane vaporizer
D. Overf i l led vaporizer
View Answer


















