CHAPTER 134 OXYGEN THERAPY AND BASIC RESPIRATORY CARE · P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1:...
14
P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3 CHAPTER 134 ■ OXYGEN THERAPY AND BASIC RESPIRATORY CARE ELAMIN M. ELAMIN J. MICHAEL JAEGER ANDREW C. MILLER THE CHEMISTRY OF OXYGEN Oxygen in air exists in a diatomic molecular form (O 2 , molec- ular weight [MW] 16 g/mol) that, at standard temperature and pressure, is a colorless, odorless gas. The diatomic molecular state is the form that we administer to our patients as a res- piratory gas, either pure oxygen or in mixtures with air or helium (heliox), and is that form most commonly referred to as oxygen. While the gaseous state of oxygen is most clinically relevant, it can be found in a liquid and solid state as well under appropriate conditions. However, molecular oxygen has additional chemical states that expand its impact on human physiology. The diatomic form (“oxygen”) is essential for aer- obic metabolism in animals but is toxic to obligate anaerobic organisms (a fact exploited in hyperbaric oxygen therapy). The triatomic form, ozone, is produced continuously by ultravio- let (UV) radiation in the upper layers of the atmosphere, and serves to shield the earth’s surface from UV radiation. However, ozone is also produced by the immune system as an antimi- crobial defense. Finally, singlet oxygen (several different forms exist) is a high-energy state of molecular oxygen in which all the electron spins are paired, resulting in extreme instability and exceptional reactivity toward common organic molecules. Such oxygen-free radicals, as they are collectively termed, have varied and increasingly important physiologic roles; therefore, their role in both normal and pathologic processes must be recognized and understood to allow the correct application of oxygen therapy. In this chapter, we will discuss the various modalities for oxygen delivery in the critical care setting. In addition, we will address oxygen’s diverse physiologic and possible pathologic effects, but in our discussion of oxygen-free radicals, we will confine it to their role in oxidative lung injury, while being cognizant of their potential impact on all tissues. OXYGEN THERAPY DEVICES Oxygen therapy is one of the basic modes of respiratory care. Yet, despite the fact that oxygen has been delivered to patients with lung disease for almost a century, it is commonly delivered in imprecise concentrations. Because oxygen is “invisible,” it has often been downgraded to a position considerably less than the powerful drug that it is. Delivery devices for oxygen therapy are typically classified into two groups: variable flow or fixed-flow equipment. The term variable flow relates to the fact that as the patient’s respi- ratory pattern changes, delivered oxygen is diluted with room air. This results in a widely inconsistent and fluctuating fraction of inspired oxygen concentration (FiO 2 ). In fact, despite some commonly published figures for delivered FiO 2 at given flow rates, the actual FiO 2 delivered to the patient by various devices is neither precise nor predictable. Variable flow devices include nasal catheter, nasal cannulae, transtracheal oxygen catheter, and various oxygen masks. Fixed-flow equipment, on the other hand, provides the en- tire patient’s inspired gas with a precisely controlled FiO 2 ; when applied appropriately, the FiO 2 delivered to the patient is therefore constant, regardless of ventilatory pattern. Fixed- flow devices include air-entrainment masks, large-volume aerosol systems, and large-volume humidifier systems. The following describes various oxygen delivery equipment and their proper placement, possible problems, and overall per- formance. Variable Flow Equipment Nasal Catheter Description. The nasal catheter is the simplest oxygen delivery device. It is a soft, plastic, blind-end tube with numerous side holes at the distal tip. Nasal catheters typically come in French sizes, which is a reference to the outside diameter (OD) of the device. A French (Fr) size is three times the OD in millimeters, with typical adult sizes being 12 Fr to 14 Fr. Oxygen is delivered to the nasal catheter from a bubble humidifier through the oxygen tubing. Placement. Before use, the catheter should be liberally lubri- cated with a water-soluble lubricant. The catheter is placed in the external naris and advanced along the floor of the nasal cavity into the oropharynx, stopping just behind the uvula. The appropriate size can be determined by inspection of the external naris and by measurement of the distance between the tip of the nose to the ipsilateral external ear. To achieve proper placement, use a tongue blade and flash- light to observe the posterior pharynx, and then advance the catheter into the nasopharynx until it appears below the uvula. After identifying the catheter tip, withdraw the catheter until the tip of the catheter is no longer seen. Once proper place- ment is achieved, the catheter should be secured to the nose with tape. Problems. Pain and discomfort during insertion have been de- scribed. In the presence of nasal pathologic conditions, includ- ing nasal polyps, deviated septum, and nasal congestion, place- ment may be particularly traumatic or impossible. Bleeding 2043
Transcript of CHAPTER 134 OXYGEN THERAPY AND BASIC RESPIRATORY CARE · P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1:...

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
CHAPTER 134 ■ OXYGEN THERAPYAND BASIC RESPIRATORY CAREELAMIN M. ELAMIN � J. MICHAEL JAEGER � ANDREW C. MILLER
THE CHEMISTRY OF OXYGEN
Oxygen in air exists in a diatomic molecular form (O2, molec-ular weight [MW] 16 g/mol) that, at standard temperature andpressure, is a colorless, odorless gas. The diatomic molecularstate is the form that we administer to our patients as a res-piratory gas, either pure oxygen or in mixtures with air orhelium (heliox), and is that form most commonly referred toas oxygen. While the gaseous state of oxygen is most clinicallyrelevant, it can be found in a liquid and solid state as wellunder appropriate conditions. However, molecular oxygen hasadditional chemical states that expand its impact on humanphysiology. The diatomic form (“oxygen”) is essential for aer-obic metabolism in animals but is toxic to obligate anaerobicorganisms (a fact exploited in hyperbaric oxygen therapy). Thetriatomic form, ozone, is produced continuously by ultravio-let (UV) radiation in the upper layers of the atmosphere, andserves to shield the earth’s surface from UV radiation. However,ozone is also produced by the immune system as an antimi-crobial defense. Finally, singlet oxygen (several different formsexist) is a high-energy state of molecular oxygen in which allthe electron spins are paired, resulting in extreme instabilityand exceptional reactivity toward common organic molecules.Such oxygen-free radicals, as they are collectively termed, havevaried and increasingly important physiologic roles; therefore,their role in both normal and pathologic processes must berecognized and understood to allow the correct application ofoxygen therapy.
In this chapter, we will discuss the various modalities foroxygen delivery in the critical care setting. In addition, we willaddress oxygen’s diverse physiologic and possible pathologiceffects, but in our discussion of oxygen-free radicals, we willconfine it to their role in oxidative lung injury, while beingcognizant of their potential impact on all tissues.
OXYGEN THERAPY DEVICES
Oxygen therapy is one of the basic modes of respiratory care.Yet, despite the fact that oxygen has been delivered to patientswith lung disease for almost a century, it is commonly deliveredin imprecise concentrations. Because oxygen is “invisible,” ithas often been downgraded to a position considerably less thanthe powerful drug that it is.
Delivery devices for oxygen therapy are typically classifiedinto two groups: variable flow or fixed-flow equipment. Theterm variable flow relates to the fact that as the patient’s respi-ratory pattern changes, delivered oxygen is diluted with room
air. This results in a widely inconsistent and fluctuating fractionof inspired oxygen concentration (FiO2). In fact, despite somecommonly published figures for delivered FiO2 at given flowrates, the actual FiO2 delivered to the patient by various devicesis neither precise nor predictable. Variable flow devices includenasal catheter, nasal cannulae, transtracheal oxygen catheter,and various oxygen masks.
Fixed-flow equipment, on the other hand, provides the en-tire patient’s inspired gas with a precisely controlled FiO2;when applied appropriately, the FiO2 delivered to the patientis therefore constant, regardless of ventilatory pattern. Fixed-flow devices include air-entrainment masks, large-volumeaerosol systems, and large-volume humidifier systems.
The following describes various oxygen delivery equipmentand their proper placement, possible problems, and overall per-formance.
Variable Flow Equipment
Nasal CatheterDescription. The nasal catheter is the simplest oxygen deliverydevice. It is a soft, plastic, blind-end tube with numerous sideholes at the distal tip. Nasal catheters typically come in Frenchsizes, which is a reference to the outside diameter (OD) of thedevice. A French (Fr) size is three times the OD in millimeters,with typical adult sizes being 12 Fr to 14 Fr. Oxygen is deliveredto the nasal catheter from a bubble humidifier through theoxygen tubing.
Placement. Before use, the catheter should be liberally lubri-cated with a water-soluble lubricant. The catheter is placed inthe external naris and advanced along the floor of the nasalcavity into the oropharynx, stopping just behind the uvula.The appropriate size can be determined by inspection of theexternal naris and by measurement of the distance between thetip of the nose to the ipsilateral external ear.
To achieve proper placement, use a tongue blade and flash-light to observe the posterior pharynx, and then advance thecatheter into the nasopharynx until it appears below the uvula.After identifying the catheter tip, withdraw the catheter untilthe tip of the catheter is no longer seen. Once proper place-ment is achieved, the catheter should be secured to the nosewith tape.
Problems. Pain and discomfort during insertion have been de-scribed. In the presence of nasal pathologic conditions, includ-ing nasal polyps, deviated septum, and nasal congestion, place-ment may be particularly traumatic or impossible. Bleeding
2043

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
2044 Section XIII: Respiratory Disorders
can occur resulting from mucosal irritation. For this reason,patients with coagulation disorders should not have a nasalcatheter placed.
When in place, routine changing of the catheter is requiredto prevent blockage of the side holes with secretions in additionto subsequent reduction of oxygen flow.
Performance. Nasal catheters have been used for adults as wellas infants (1). In adults, nasal catheters provide a relatively lowFiO2. The increase in FiO2 through the nasal catheter is directlyrelated to gas flow, and is enhanced at low flow rates by usingthe nasopharynx and oropharynx as a reservoir for oxygen.Accordingly, at flow rates of 6 to 10 L/minute, an FiO2 of0.69 to 0.82 can be delivered to the patient (2). However, likeall variable performance equipment, delivered FiO2 will varywith a change in respiratory rate or tidal volume.
The major advantage of using a nasal catheter is that it canbe securely placed in obtunded patients. However, due to along list of disadvantages, including discomfort, difficulty ininsertion, and bleeding, nasal catheters are infrequently usedtoday.
Nasal CannulaDescription. The nasal cannula is the most frequently utilizedoxygen delivery device. It consists of a blind-end tube withtwo protruding “nasal prongs” that rest in the external naris.Cannulae come in a variety of designs for more comfortableor subtle application. Regardless of the design, the principleof oxygen delivery is the same. Cannulae are connected to anoxygen flowmeter through oxygen tubing without a humidifi-cation device for flow less than 4 L/minute and with a bubblehumidifier for higher flow rates to prevent nasal drying (3).
Placement. Nasal cannulae are easily placed regardless of thetype and brand.
Problems. The nasal cannula is relatively problem free. How-ever, short-term use can result in drying of the nasal mucosa,while long-term use can cause pressure sores above the ears, un-der the chin, and above the upper lip. Gauze or foam paddingcan be placed between the cannula and irritation sites to limitthis complication.
Performance. A nasal cannula is used with oxygen flow ratesof 1 to 6 L/minute in adults and as low as 1/16 L/minute ininfants. The exact FiO2 delivered with a nasal cannula has beenmeasured and estimated using a variety of methods and, asexpected, yielded a variety of results.
An earlier method to predict FiO2 through variable per-formance equipment and using a host of assumptions demon-strated a wide range of FiO2 values delivered by nasal cannulaat any given constant flow of oxygen (4). Another study in FiO2
delivery through the nasal cannula utilized a model of the respi-ratory system (5). The model consisted of a lung placed insidea rigid container and attached to a rubber test lung throughtubing that approximated tracheal volume. A ventilator pro-ducing a sine wave was connected to the container, and inspira-tory flow varied from 12 to 40 L/minute at a constant rate andvolume. The study illustrated that delivered FiO2 varied 13%to 40% at a given oxygen flow when inspiratory flow variedfrom 12 to 40 L/minute.
The nasal cannula is commonly used as the first means todeliver oxygen to patients requiring long-term therapy. In the-ory, the nasal cannula increases FiO2 by 0.04 for every liter ofoxygen flow. Flow is typically set between 1 and 6 L/minute.Flow above 6 L/minute adds little to increased FiO2, and mayinduce patient discomfort, including nasal mucosa dryness andbleeding.
Oxygen-conserving Devices
The wide use of nasal cannulae led to recognition of an impor-tant device limitation. Since there is lack of synchronizationbetween the patient ventilation and continuous flow of oxy-gen through the cannula, there is wasted oxygen flow to theroom during expiration. In an attempt to eliminate this wasteand reduce the cost of oxygen delivery, several device modifica-tions have been developed. However, the mechanism of oxygenconservation has centered on two main concepts.
Reservoir CannulaDescription. These devices use a mechanical reservoir or an in-creased anatomic reservoir that fills with 100% oxygen duringexhalation and empties the oxygen into the lungs early in in-spiration. This was achieved through the use of a collapsiblechamber that empties on inspiration and fills during exhala-tion.
Moustache-style Cannula. This is among the most widelyavailable reservoir devices. The cannula contains a soft, inflat-able reservoir with a volume of approximately 20 mL. Duringpatient exhalation, oxygen flow fills the expandable reservoir.Then, during early inspiration, the patient inspires first fromthe reservoir, causing the reservoir to begin to empty, and fromthe continuous flow once the reservoir is depleted.
Placement. The reservoir cannula rests directly beneath thenose.
Problems. The moustache-style cannula is larger, heavier, andmore obvious than the traditional cannula. Hence, it is moreobtrusive, and many patients in need of O2 therapy at homemay prefer not to wear it in public.
Performance. As expected, the reservoir cannula can achieveoxygenation equivalent to a conventional nasal cannula, but ata lower flow rate.
Pendant Reservoir Cannula
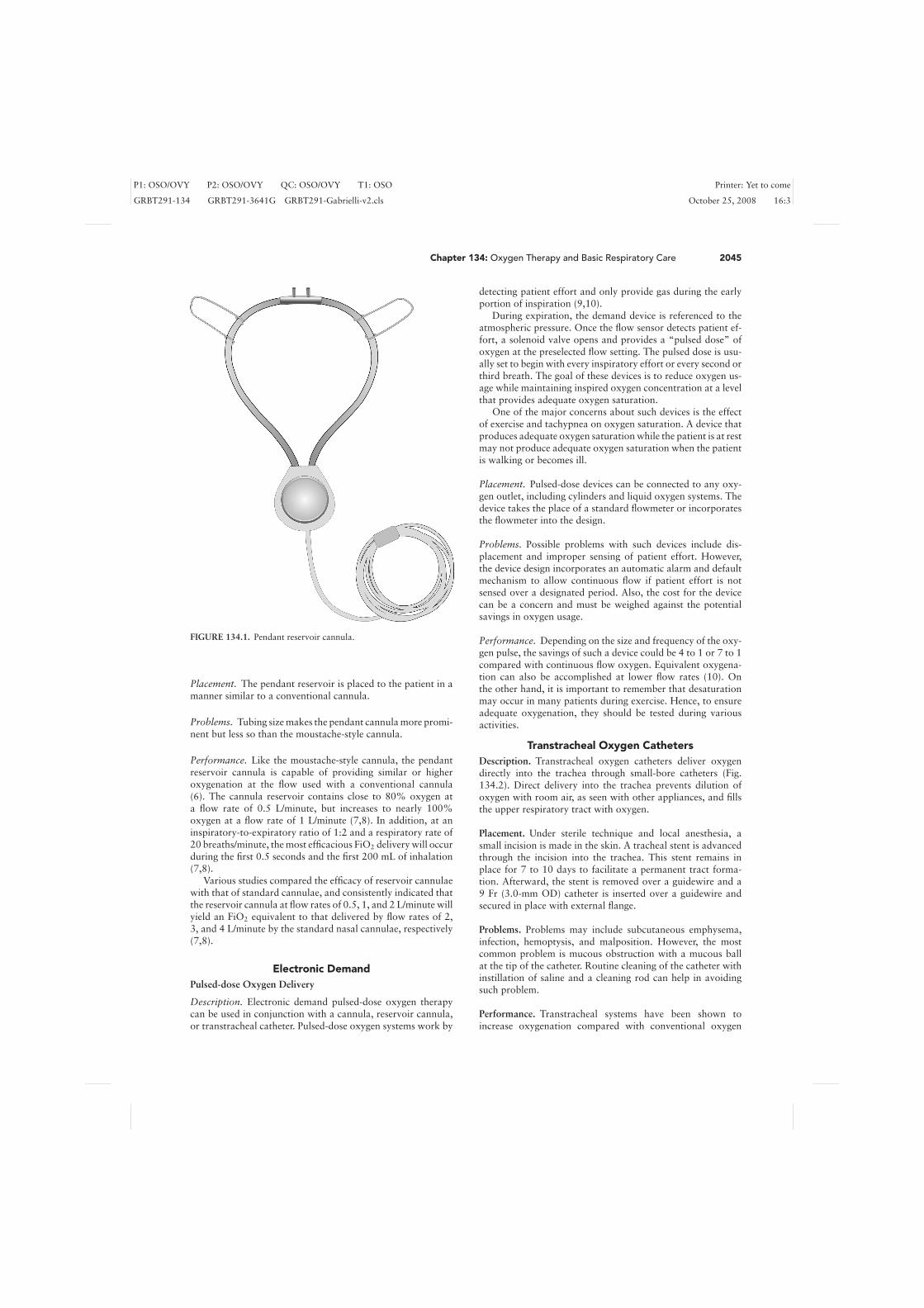
Description. The pendant reservoir cannula (Fig. 134.1) usesa pendant-like reservoir that is worn on the chest with a larger-diameter cannula and connecting tubing. The pendant containsan inflatable reservoir with a volume of approximately 40 mLthat forces gas up the cannula tubing during expiration. Sub-sequently, during early inspiration, the gas stored in the tubingacts as a reservoir of oxygen, but as inspiration continues, thecannula begins to function like a conventional cannula.
Overall, most of the benefit appears to be derived from theoversized tubing between the patient and the pendant (6).
P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
Chapter 134: Oxygen Therapy and Basic Respiratory Care 2045
FIGURE 134.1. Pendant reservoir cannula.
Placement. The pendant reservoir is placed to the patient in amanner similar to a conventional cannula.
Problems. Tubing size makes the pendant cannula more promi-nent but less so than the moustache-style cannula.
Performance. Like the moustache-style cannula, the pendantreservoir cannula is capable of providing similar or higheroxygenation at the flow used with a conventional cannula(6). The cannula reservoir contains close to 80% oxygen ata flow rate of 0.5 L/minute, but increases to nearly 100%oxygen at a flow rate of 1 L/minute (7,8). In addition, at aninspiratory-to-expiratory ratio of 1:2 and a respiratory rate of20 breaths/minute, the most efficacious FiO2 delivery will occurduring the first 0.5 seconds and the first 200 mL of inhalation(7,8).
Various studies compared the efficacy of reservoir cannulaewith that of standard cannulae, and consistently indicated thatthe reservoir cannula at flow rates of 0.5, 1, and 2 L/minute willyield an FiO2 equivalent to that delivered by flow rates of 2,3, and 4 L/minute by the standard nasal cannulae, respectively(7,8).
Electronic DemandPulsed-dose Oxygen Delivery
Description. Electronic demand pulsed-dose oxygen therapycan be used in conjunction with a cannula, reservoir cannula,or transtracheal catheter. Pulsed-dose oxygen systems work by
detecting patient effort and only provide gas during the earlyportion of inspiration (9,10).
During expiration, the demand device is referenced to theatmospheric pressure. Once the flow sensor detects patient ef-fort, a solenoid valve opens and provides a “pulsed dose” ofoxygen at the preselected flow setting. The pulsed dose is usu-ally set to begin with every inspiratory effort or every second orthird breath. The goal of these devices is to reduce oxygen us-age while maintaining inspired oxygen concentration at a levelthat provides adequate oxygen saturation.
One of the major concerns about such devices is the effectof exercise and tachypnea on oxygen saturation. A device thatproduces adequate oxygen saturation while the patient is at restmay not produce adequate oxygen saturation when the patientis walking or becomes ill.
Placement. Pulsed-dose devices can be connected to any oxy-gen outlet, including cylinders and liquid oxygen systems. Thedevice takes the place of a standard flowmeter or incorporatesthe flowmeter into the design.
Problems. Possible problems with such devices include dis-placement and improper sensing of patient effort. However,the device design incorporates an automatic alarm and defaultmechanism to allow continuous flow if patient effort is notsensed over a designated period. Also, the cost for the devicecan be a concern and must be weighed against the potentialsavings in oxygen usage.
Performance. Depending on the size and frequency of the oxy-gen pulse, the savings of such a device could be 4 to 1 or 7 to 1compared with continuous flow oxygen. Equivalent oxygena-tion can also be accomplished at lower flow rates (10). Onthe other hand, it is important to remember that desaturationmay occur in many patients during exercise. Hence, to ensureadequate oxygenation, they should be tested during variousactivities.
Transtracheal Oxygen CathetersDescription. Transtracheal oxygen catheters deliver oxygendirectly into the trachea through small-bore catheters (Fig.134.2). Direct delivery into the trachea prevents dilution ofoxygen with room air, as seen with other appliances, and fillsthe upper respiratory tract with oxygen.
Placement. Under sterile technique and local anesthesia, asmall incision is made in the skin. A tracheal stent is advancedthrough the incision into the trachea. This stent remains inplace for 7 to 10 days to facilitate a permanent tract forma-tion. Afterward, the stent is removed over a guidewire and a9 Fr (3.0-mm OD) catheter is inserted over a guidewire andsecured in place with external flange.
Problems. Problems may include subcutaneous emphysema,infection, hemoptysis, and malposition. However, the mostcommon problem is mucous obstruction with a mucous ballat the tip of the catheter. Routine cleaning of the catheter withinstillation of saline and a cleaning rod can help in avoidingsuch problem.
Performance. Transtracheal systems have been shown toincrease oxygenation compared with conventional oxygen

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
2046 Section XIII: Respiratory Disorders
FIGURE 134.2. Transtracheal oxygen catheter.
therapy with a nasal cannula at equivalent flow rates, or canprovide equivalent oxygenation at lower flow rates (11).
Patient acceptance is also reportedly improved because ofthe relatively hidden appearance of the equipment. Reducedoxygen usage, reduced costs, and increased life of portable gassources have all been reported with transtracheal oxygen ther-apy. The use of transtracheal oxygen therapy can reduce re-quired oxygen flow by close to 50% (12). The latter may evenbe enhanced with the additional use of demand pulsed-doseoxygen that can further increase the savings.
Masks
Simple MaskDescription. The simple mask is a disposable, lightweightplastic that increases FiO2 by increasing the available reservoirby adding the volume of the mask. Oxygen is delivered to themask through standard oxygen tubing at a flow rate of 5 to12 L/minute. The mask allows room air to be drawn in aroundthe mask edges and through side ports. A bubble humidifiermay be used to provide comfort, especially with prolonged use.
Placement. Simple masks are held in place over the patient’snose and mouth with an adjustable elastic strap.
Problems. Patients wearing a mask may complain of claustro-phobia or pain at the site of mask application. Also, it caninterfere with eating and drinking.
Performance. Since it is a variable performance device, the ac-tual FiO2 delivered varies with mask fit, oxygen flow, and cer-tainly patient respiratory effort. This was first suggested in astudy by Bethune and Coffis (13), who investigated the relationof the flow and rebreathing of carbon dioxide (CO2). They wereable to demonstrate that, at flow rates of 1 to 8 L/minute and
tidal volume of 500 mL, an FiO2 of 0.21 to 0.60 can be deliv-ered. However, at the same flow rates but at a tidal volume of1,000 mL, only an FiO2 of 0.21 to 0.43 was delivered. It is gen-erally stated that a minimum flow of 5 L/minute is necessaryto prevent rebreathing of CO2 (14).
Partial Rebreathing Reservoir MaskDescription. Partial rebreathing reservoir masks are simplemasks that are fitted with an additional 600- to 800-mL reser-voir that extend below the patient’s chin. Oxygen flow is pro-vided from a bubble humidifier at a flow that keeps the reservoirbag at least half full during inspiration (usually 8–15 L/minute).In addition, during expiration, the first third of expired gas en-ters the reservoir bag, hence the term, partial rebreather. Thisis gas from the anatomic reservoir, so it is high in oxygen andcontains little CO2. As the bag fills from the oxygen flow andfirst third of expiration, the remaining expired gas exits theexhalation openings of the mask.
Placement. The partial rebreathing reservoir mask is held inplace over the patient’s nose and mouth with an adjustableelastic strap.
Problems. As stated above, flow must be adjusted as patientdemand changes to ensure minimal FiO2 delivery.
Performance. At flow rates of 6 to 10 L/minute, the partial re-breathing mask delivered FiO2 values from 0.35 to 0.70 (15).
Nonrebreathing Reservoir MaskDescription. The Nonrebreathing Reservoir Mask incorpo-rates one-way valves over one of the mask side ports and abovethe reservoir bag. The one-way valve over the reservoir bag pre-vents expired gas from entering into the bag. In addition, theone-way valve over the side port limits further entrainment ofroom air during inspiration, except if gas flow is inadvertentlydisconnected.
Placement. The nonrebreathing mask is held in place over thepatient’s nose and mouth with an adjustable elastic strap.
Problems. In addition to previously mentioned shortcomingsof masks, the combined effects of time and moisture can causeone-way valves to stick in either the open or closed position.
Performance. The nonrebreathing mask requires minimumoxygen flow of 10 to 15 L/minute to prevent the reservoirbag from collapsing during inspiration. With that flow rate,it is estimated that an FiO2 of 0.60 to 0.80 is delivered with anonrebreathing mask (15). A FiO2 of 0.57 to 0.70 is deliveredwhen oxygen flow can be set greater than the patient minuteventilation. Contrary to common belief, FiO2 values near 1.0cannot be achieved using the commonly available disposablenonrebreathing masks.
Fixed-performance Devices
Air-entrainment MasksDescription. An air-entrainment mask consists of the mask, ajet nozzle, and entrainment ports. Oxygen under pressure is

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
Chapter 134: Oxygen Therapy and Basic Respiratory Care 2047
TABLE 134.1
AIR-ENTRAINMENT MASK FiO2 SETTINGS ANDMINIMUM OPTIONAL OXYGEN FLOW RATES FORVARIOUS SETTINGS
Minimum oxygen Entrainment Total flowFiO2 setting flow (L/min) ratio O2:Air (L/min)
0.24 4 1:25 1040.28 4 1:10 440.31 6 1:7 480.35 8 1:5 480.40 8 1:3 320.50 12 1:1.7 320.60 12 1:1 240.70 12 1:0.6 19
delivered through the jet nozzle just below the mask. As gastravels through the jet nozzle, its velocity increases dramati-cally. On exiting the nozzle, the gas at high velocity entrains ordrags ambient air into the mask. This is due not to the Venturiprinciple, but rather to the viscous shearing forces betweenthe gas traveling through the nozzle and the stagnant ambi-ent air (16). Accordingly, the delivered FiO2 is dependent onthe size of the nozzle and entrainment ports, and the rate ofoxygen flow. On average, an air-entrainment mask has six toeight FiO2 settings as well as minimum optional oxygen flowrates for various settings (Table 134.1). To provide additionalsystem humidity, an aerosol collar can be applied around theentrainment ports. The dry oxygen will then entrain air froman aerosol system, increasing the humidity delivered to the pa-tient. However, the addition of aerosol particles to room airmay increase gas density, which will reduce entrained volume,and may slightly increase the delivered FiO2.
Placement. The mask is secured to the patient’s face with anadjustable, elastic band.
Problems. The most important problem associated with theair-entrainment mask is obstruction of the entrainment portby various objects. This decreases total flow perceptibly andincreases FiO2.
Performance. The air-entrainment mask requires FiO2 values<0.30 to maintain total flow 30% greater than peak inspira-tory flow and continue to function as a fixed-performance sys-tem (17). At higher FiO2, the total flow falls below 40 L/minute,and the air-entrainment mask becomes a variable performancedevice. The latter may occur if patient demand for flow in-creases and room air is drawn in around the mask (18).
To accommodate such a demand, masks with larger volumes(volume ≥ 300 mL) and extension tubes between the jet and themask will act as reservoirs for blended gas, keeping deliveredFiO2 values more constant (19).
Overall, the air-entrainment mask is intended for patientswith high or changing ventilatory demands, such as patientswith chronic lung disease who may hypoventilate when ex-posed to high FiO2 values.
The OxyMaskDescription. The OxyMask is a recently introduced oxygenface mask for both hospital and home use. It uses a small dif-
FIGURE 134.3. The OxyMask.
fuser to concentrate and direct oxygen toward the mouth ornose. This unique design enables the OxyMask to deliver oxy-gen more efficiently than a Venturi mask, especially in patientswith chronic hypoxemia (20).
Placement. The OxyMask is an “open oxygen” system thatdoes not require physical contact with the patient’s face. The de-vice resembles a hands-free telephone headset, with the speakerportion replaced with “an oxygen diffuser” for precise andcomfortable oxygen delivery (Fig. 134.3). The oxygen diffusercan be directed toward the nose or mouth; however, it doesnot come in contact with either one. Consequently, the Oxy-Mask will not interfere with various activities such as eatingand talking (21).
Performance. A recent study compared the OxyMask ver-sus the Venturi mask in 26 oxygen-dependent patients withchronic, stable respiratory disease in a randomized, single-blind, cross-over design (20). Oxygen delivery was titrated tomaintain an oxygen saturation (SaO2) 4% to 5% and 8% to9% above baseline for two separate 30-minute periods of sta-ble breathing. Oxygen flow rate, partial pressure of inspiredand expired oxygen (PO2) and carbon dioxide (PCO2), minuteventilation, heart rate, nasal and oral breathing, SaO2, andtranscutaneous PCO2 were recorded. The study reported loweroxygen flow rates, higher inspired PO2, and lower expired PO2
while using the OxyMask. In addition, minute ventilation andinspired and expired PCO2 were significantly higher while us-ing the OxyMask, whereas transcutaneous PCO2, heart rate,and the ratio of nasal to oral breathing did not change sig-nificantly throughout the study. The study concluded thatoxygen is delivered safely and more efficiently by the Oxy-Mask than by the Venturi mask in stable oxygen-dependentpatients.
Similar results were obtained in the early postoperative pe-riod, during which OxyMask delivered adequate levels of oxy-gen for most patients, with no patient experiencing an oxygendesaturation event less than 97.88% 4 minutes post extubation(21). In addition, patients and clinicians praised the OxyMaskfor its comfort and ease of use, allowing nurses to performfacial care without interrupting oxygen therapy.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
2048 Section XIII: Respiratory Disorders
Large-volume Aerosol and Humidifier SystemsDescription. Large-volume aerosol systems use air-entrain-ment nebulizers alone or in tandem to provide gas to facemasks, T-pieces, and tracheostomy collars. Nondisposableaerosol systems usually offer FiO2 values of 0.40, 0.60, and1.0, whereas disposable systems offer continuous adjustments,with six to eight settings calibrated from 0.28 to 1.0. Thesesystems use a constant jet nozzle with a changeable size en-trainment port to modify FiO2.
Placement. Placement varies with the device used. Most sys-tems use an elastic band that attaches the device around thehead or neck, while the T-piece connects directly to the artifi-cial airway.
Problems. The most common problem with the system is inad-equate flow. Other common problems include the presence ofwater condensation in the delivery tubing that prevents roomair entrainment and increases delivered FiO2. In general, if mistfrom the aerosol escapes the oxygen delivery device during in-spiration, flow is generally considered sufficient.
Performance. Under conditions of high patient ventilatory de-mand, these systems become variable performance devices (22).With decreased flow, room air becomes entrained in the mask,and therefore, despite the increase in set FiO2 values, deliveredFiO2 decreases. Accordingly, when precise FiO2 values are nec-essary at a high flow rate, a high-volume humidifier system ispreferred. If delivery of oxygen is required in excess of 100L/minute, a blender, air–oxygen flowmeter, or even a Venturisystem can be used and directed through a heated humidifier.A reservoir is usually placed between the humidifier and thepatient.
MIXING AIR AND OXYGEN
Oxygen Flowmeters and Blenders
Various commercially available oxygen flowmeters (Fig. 134.4)can be used to deliver precise oxygen concentrations. Gas isdelivered from air and oxygen flowmeters and passes througha humidifier before being delivered to the nasal cannula ormask.
Air–oxygen blenders (Fig. 134.5) are more expensive com-pared with using two flowmeters, but with a 50-psig (pounds-force per square inch gauge) source, they can deliver moreprecise FiO2 values. In general, blenders have three sepa-rate compartments where different functions are performed:the alarm, pressure-balancing, and proportioning compart-ments.
Air and oxygen enter the alarm compartment from two sep-arate inlets. If the pressure differences between the two inletsare greater than 10 psig, the accuracy of FiO2 will be compro-mised and a high-pitched alarm will sound (23). The pressure-balancing compartment will then use a diaphragm to balancethe air and oxygen pressures. Finally, at the proportioning com-partment, air and oxygen at similar pressures are adjusted inproportion to the desired FiO2.
FIGURE 134.4. Oxygen and air flowmeters.
Postextubation Respiratory Therapy
Postextubation pulmonary complications are major causes ofmorbidity and mortality among intensive care unit (ICU) pa-tients, especially after thoracic or upper abdominal surgeries.During normal respiration, healthy individuals inspire ap-proximately ten times each hour and take large intermittentbreaths—“sighing”—that are three times the normal tidal vol-ume (24). However, postoperatively, such deep breaths are ab-sent and replaced with a shallow, monotonous breathing pat-tern that decreases ventilation to the dependent lung regions,contributing—with the use of postoperative higher FiO2—to the development of atelectasis. Factors such as residual
FIGURE 134.5. Oxygen blender.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
Chapter 134: Oxygen Therapy and Basic Respiratory Care 2049
anesthetic effects and incisional pain promote decreased restinglung volume. Furthermore, assuming a prolonged postopera-tive recumbent position, the diaphragmatic movement is lim-ited and the functional residual capacity (FRC) decreased (25).The diminishing expiratory lung volume decreases lung com-pliance and eventually increases the elastic work of breathing.To minimize this work, patients take shallow, frequent breaths,which may further decrease lung volume (25). The primary goalof postoperative respiratory therapy is to increase FRC, reduc-ing pulmonary atelectasis and their related complications.
A slight elevation of temperature and decrease in breathsounds over the lung bases may be useful in diagnosing at-electasis. However, these means are insensitive in detecting de-creases in FRC. In addition, the large decline in the amount ofair that can be maximally forced out of the lungs after a max-imal inspiration (forced vital capacity [FVC]) and the forcedexpiratory volume in the first second (FEV1) that occur afterupper abdominal operations are patient effort dependent andcannot accurately predict a decrease in FRC. The same can betrue regarding the interpretations of portable chest roentgenog-raphy in ICU patients, which is useful for identifying patientswith atelectasis but does not predict FRC.
The use of postextubation positive pressure devices has beenpart of respiratory therapy management since intermittent pos-itive pressure breathing (IPPB) was first introduced over 50years ago (26). In addition to the incentive spirometer (IS), thereare many positive pressure devices from which to choose; theseinclude IPPB, continuous positive airway pressure (CPAP), pos-itive expiratory pressure (PEP), and nasal intermittent positivepressure ventilation. In this section, we will review the physi-ologic effects and indications relating to the use of the IS andIPPB. However, the use of CPAP and noninvasive intermittentpositive pressure ventilation will be discussed in detail else-where in the textbook.
Incentive SpirometerDescription. Compared to the many therapeutic maneuversand devices that have been used to prevent postoperative pul-monary complications, the IS has gained the most popularityfor its simplicity, and currently is a common mode of postop-erative respiratory therapy worldwide.
The IS is designed to mimic natural sighing or yawning byencouraging the patient to maximally inflate the lungs and sus-tain that inflation. This is accomplished by using a device thatprovides patients with visual or other positive feedback whenthey inhale at a predetermined flow rate or volume and inspi-ratory time, the latter usually targeted at 3 seconds (27). Theprolonged and forced lung inflations open collapsed alveoli,preventing or resolving atelectasis. Since the re-expanded alve-oli remain inflated during expiration, the FRC increases.
Placement. The IS mouthpiece is placed in the mouth with thelips tightly sealed around it. The IS should be used five to tenbreaths per session, or at a minimum every hour while awake(i.e., 100 times a day) (27).
Problems. The IS use may lead to discomfort secondary to in-adequate incisional pain control and hypoxia secondary to in-terruption of prescribed oxygen therapy if a face mask or shieldis being used. Furthermore, the IS is generally ineffective un-less closely supervised or performed as ordered. In addition,
although uncommon, it might result in barotrauma in patientswith severely emphysematous lungs.
Performance. Four trials with 443 participants contributed toa recent Cochrane Database of Systematic Review about thebenefits of the IS (28). In that review, there was no significantdifference in pulmonary complications (atelectasis and pneu-monia) between treatment with the IS and treatment with otherpositive pressure breathing techniques (CPAP, bilevel positiveairway pressure [BiPAP], and IPPB), regardless of preoperativepatient education. In addition, patients treated with the IS hadworse pulmonary function and arterial oxygenation comparedwith positive pressure breathing (CPAP, BiPAP, IPPB). How-ever, in view of the small number of patients in the includedstudies and the multiple methodologic and reporting shortcom-ings, these results should be interpreted cautiously.
Intermittent Positive Pressure BreathingDescription. IPPB is used in clinical practice, primarily to im-prove the lung volumes and to decrease the work of breathing.However, its role in clearing excessive secretions from the lungsis questionable and controversial. Commercially available de-vices are most commonly used for the delivery of IPPB. In gen-eral, all these devices are powered by compressed gas—eitherair or oxygen (29). Short-term humidification can be addedto the driving gas. Since IPPB is a pressure-cycled device, theoperator can select the pressure and flow rate of the gas andthe sensitivity for the patient to trigger the system. Upon in-spiration, a negative pressure is generated in the circuit, andinspiratory flow proceeds until the preset pressure is attainedwhen flow ceases and the patient expires passively. The opera-tor should adjust the machine settings until a desired maximalvolume is delivered to the patient, in general “eyeballed” to 1inch of chest excursion or approximately 6 to 8 mL/ideal bodyweight in kilograms (30,31).
Placement. The patient is connected to IPPB through a mouth-piece. The patient needs to be cooperative and spontaneouslybreathing to trigger the machine using the mouthpiece. Occa-sionally, a full face mask may be used for less conscious pa-tients, as it is generally tolerated only for a brief period oftime.
Problems. IPPB has been shown to increase tidal volume, andconsequently minute ventilation, by passively ventilating thepatient and hence improving arterial blood gases (29). How-ever, this may lead to a decline in cardiac output as a result ofincreased intrathoracic pressure during delivery and decreasedvenous return.
Performance. A large body of literature has been published ex-amining the efficacy of IPPB in different patient populations.The efficacy of IPPB in the management of chronic obstructivepulmonary disease (COPD) was found to be mainly unsup-ported (29). This can be partly explained by an inappropriatechoice of patient populations, the frequency of IPPB used, andother confounding effects of concurrent chest physiotherapytechniques (32).
Another largely studied use of IPPB was in the preven-tion or management of postoperative respiratory complications(33). The comparative efficacy of IPPB with IS, deep breathingexercises, blow bottles, and physiotherapy has been studied.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
2050 Section XIII: Respiratory Disorders
Although this literature is overwhelmed by various method-ologic problems, their outcomes demonstrated that the use ofIPPB conferred no added benefit to patients following abdom-inal or cardiac surgery when compared to the other modalities(29). However, it is conceivable that in patients with excessivesecretions, IPPB may need to be combined with gravity-assisteddrainage and chest wall vibrations for more effective upwardclearing of secretions (29).
The use of IPPB has declined over the past two decades,partly due to controversial research outcomes and partly asa result of the introduction of newer modes of positive pres-sure support. However, IPPB may still have a role—thoughreduced—in the management of patients with reduced lungvolumes and respiratory insufficiency who cannot cooperatewell with the use of IS.
OXYGEN: THE PHYSIOLOGICIMPACT
The Fate of Oxygen in the Body
The predominant metabolic pathway for oxygen is as an elec-tron acceptor in oxidative phosphorylation within the mito-chondria (34). Oxidation of glucose and fatty acids shuttleselectrons to special molecular carriers, which are either pyri-dine nucleotides or flavins within the mitochondria. The re-duced forms of these carrier proteins, in turn, donate theirhigh-potential electrons to molecular oxygen by means of anelectron transport chain located in the inner membrane of thedouble-enveloped mitochondria. The transmembrane protongradient generated as a by-product of this electron exchange
and associated liberation of a large amount of free energy drivesthe synthesis of adenosine triphosphate (ATP) from adenosinediphosphate (ADP) and inorganic phosphate (Pi). Of the fourprotein complexes that form the electron transport chain, com-plex IV, also known as cytochrome c oxidase, is responsible forthe transfer of four electrons, along with four hydrogen ions,to reduce molecular oxygen to two molecules of water. Cy-tochrome c oxidase has an extremely complex structure andcontains 13 subunits, two heme groups (cytochrome a and cy-tochrome a3), and multiple metal ion cofactors (three atoms ofcopper, one of magnesium, and one of zinc).
Although the transfer of four electrons and four protonsreduces oxygen to water, the transfer of one or two electronsproduces superoxide anion (●O2
–) and peroxide (O22–), respec-
tively. This occurs in about 1% to 2% of all cases (35). Super-oxide anions need an additional electron to make them morestable, so they steal an electron from the nearest source such asmitochondrial DNA, the mitochondrial membrane (lipid per-oxidation), protein, reductants such as vitamins C or E, ornonenzymatic antioxidants such as glutathione or thioredoxin.If too much mitochondrial damage occurs, the cell undergoesapoptosis, or programmed cell death (Fig. 134.6). The majorityof superoxide anions produced is converted to hydrogen per-oxide in the mitochondrial matrix or cytosol by one of threeversions of superoxide dismutase. Hydrogen peroxide (H2O2)is a more stable compound; however, it also can cause cellulardamage as a result of its further reduction to hydroxyl radicals(●OH) by a series of iron-catalyzed reactions (36).
Oxygen-free radicals are produced in pulmonary smoothmuscle cells, endothelial cells, alveolar cells, and leukocytesresiding in the lungs. They are produced by both enzymaticand nonenzymatic (auto-oxidation) reactions. Enzymes capa-ble of forming superoxide radicals include xanthine oxidase,
INTRACELLULAREndoplasmic
Reticulum
Mitochondria
ONOO–
ONO
GSSG
NADP–
G6PD
GR
GRx
GPx
H2O2
O2–
H2O
eGPX
H2O2
GPx
H2O
O2–
TrxS2
Trx(SH)2
NADPH
CAT
CuZnSOD
GSH
NADP
CatalaseTRXPRXGRX ATP
NADP–
PARPActivation
ssDNABreaks
MnSODECSOD
GSH
ECSOD
Prx
EXTRACELLULAR
NADP/NADPHOxidases
CapillaryMembrane& Tissue
injury
ANDREW C. MILLER MD
FIGURE 134.6. Oxidant and antioxidant systems.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
Chapter 134: Oxygen Therapy and Basic Respiratory Care 2051
arachidonic acid peroxidases, nitric oxide synthase, nicoti-namide adenine dinucleotide phosphate (NADPH) oxidase,and nicotinamide adenine dinucleotide (NADH) oxidase(37,38). All of these enzymes are essential to the biochemicalfunction of the cell. Phagocytic cells in the lung, such as neu-trophils and alveolar macrophages, can form large quantitiesof superoxide anions during “respiratory bursts” (39,40). Themost significant sources of free radicals in lung tissue are themitochondria and endoplasmic reticulum, the sites of many ofthe aforementioned enzyme reactions.
The Antioxidants
To combat the excess accumulation of intracellular oxygen rad-icals, a system of enzymatic and nonenzymatic antioxidants ex-ists in the lungs to prevent their formation and to facilitate theeradication of these reactive species (41,42). There are threeprimary enzymatic antioxidant systems, although other com-pounds serve as opportune scavengers. First is superoxide dis-mutase (SOD), which is found both intra- and extracellularly(42,43). It is present in the cytosol and the mitochondria onthe plasma membrane surface, and in the extracellular plasma(44). The cytosolic form of SOD (CuZnSOD), which containszinc and copper, is associated with pulmonary and endothelialvascular smooth muscle cells (45). The manganese-containingmitochondrial form (MnSOD) is abundant in pulmonary arte-rial smooth muscle and endothelium, and is felt to be the most
active defense during times of pulmonary oxidative stress, cat-alyzing the dismutation of ●O2
– to H2O2.Catalase and the glutathione antioxidant systems are the
primary mechanisms for the reduction of hydrogen peroxide.Catalase is a hemoprotein found in peroxisomes that catalyzesthe reduction of hydrogen peroxide to water. Its limited cellu-lar distribution suggests that it has a specific role in managinghydrogen peroxide excess during inflammatory responses. Thesulfur-containing antioxidant, glutathione, has a much broaderdistribution than catalase, and has been measured in the cytosolat millimolar concentrations (46). Exogenously administeredglutathione has little effect on intracellular levels. However,N-acetylcysteine is a glutathione analogue capable of cross-ing the plasma membrane and enhancing glutathione activity,which may account for its purported beneficial effects in var-ious forms of cellular injury. Glutathione peroxidase plays arole in eliminating lipid peroxidases formed from free radical–altered lipid membranes (46). Glutathione peroxidase enhancesthe reduction of H2O2 by first oxidizing glutathione (in its re-duced form, GSH) and donating the pair of electrons to hydro-gen peroxide to form water. The oxidized glutathione disulfide(GSSG) is subsequently reduced in a reaction that transfers theprotons from NADPH + H+ (Fig. 134.7) (47). Glutathione re-ductase activity is dependent on NADPH generated from thehexose monophosphate shunt (48). The activity of the glu-tathione peroxidase enzyme in humans is also dependent onthe trace element selenium. The absence of selenium in the dietwill markedly reduce the efficacy of the glutathione peroxidasesystem.
ROS ROS
ROS
ROS ROS
ROS
DeathReceptor
Alveoli Alveoli
Caspase-8 Activation
Cell Membrane
BH-1-BH3Proteins
Activation
BH3 ProteinsActivation
PUMA, Bik, Bid,Bmt, Bim, Hrk,
Bad, Bcl-G
Bax, Bak
Mitochondria
Cytochromec release
STAT
NuclearMembrance
Stress Genes (HO1, HSP)
Fas, P53, Bax
GADD45/153, p21
Cell DeathGenes
IkB/NFkB NFkB
Caspase-3/7 Activation
Caspase-9 Activation
Pro-inflammatory Genes (IL-8, TNFα
Survival Genes(Bcl-2, IL-6, IL-11, MnSOD)
Andrew C. Miller MD
Hyperoxic CellDeath
FIGURE 134.7. Hyperoxic cell death.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
2052 Section XIII: Respiratory Disorders
Other elements with antioxidant capacity include the lipid-soluble vitamin E and the water-soluble vitamin C. VitaminE (a-tocopherol) is a plasma membrane constituent thoughtto play a role in inhibiting oxidative cell membrane injury,possibly by interfering with surfactant synthesis (49). Its de-ficiency in critically ill patients may lead to a susceptibilityto pulmonary oxygen toxicity. Vitamin C, or ascorbic acid,is found primarily in the extracellular space and, given its wa-ter solubility, is best suited to protecting the respiratory airwaymucosa from pollutant oxidants. Other purported nonenzy-matic antioxidants include uric acid, β-carotene, taurine, al-bumin, and bilirubin. Newly discovered families of proteins,the thioredoxins, are located in the inner mitochondrial mem-brane of the airway epithelium. They may scavenge reactiveoxygen species in response to oxidative stress and activateother intramitochondrial antioxidant systems such as MnSOD(50).
Pulmonary Oxygen Toxicity
It may appear paradoxical that oxygen could be a pulmonarytoxin at nearly any concentration (51). The lung is well-prepared to cope with the insult when relatively low partialpressures of oxygen (e.g., 160 mm Hg at standard temperatureand pressure (STP)) are breathed by virtue of the presence ofabundant antioxidants. However, when these defense mecha-nisms are overwhelmed or depleted by prolonged exposure toan elevated PO2, a progressive and potentially lethal inflam-matory reaction takes place in the lungs (52).
Reactive oxygen species are cytotoxic to nearly all cells thatconstitute the respiratory system. This toxicity stems from twoprimary mechanisms. The first major mechanism, already men-tioned, is lipid peroxidation, and the second is DNA damage.
Polyunsaturated fatty acids are a major constituent of theplasma membrane and mitochondrial membrane envelope.Hydroxyl-free radicals derived from molecular oxygen destroythese fatty acids by cleaving hydrogen atoms. Protonated hy-droxyl radicals form the radical intermediates, peroxides andperoxyradicals. Peroxides and peroxyradicals subsequently re-move hydrogen atoms from other fatty acids, initiating a de-structive chain reaction that renders the plasma membraneporous (53,54).
Cellular DNA is at risk in the presence of reactive oxygenspecies. Hydroxyl radicals also damage DNA by directly hy-droxylating guanine (55). Additionally, oxidant stress depletesnicotinamide nucleotides and disrupts the cellular cytoskele-ton (56). Free radical attacks on DNA are known to producenearly 100 lesions that include oxidation of bases and sugars,depurination, depyrimidation, and phosphodiester single- anddouble-strand breaks (57). It is controversial whether DNAstrand breaks result directly from the attack of reactive oxygenspecies on DNA or are a consequence of nucleases activatedduring programmed cell death. Regardless, the reactive lipidcompounds formed during lipid peroxidation by hydroxyl-freeradicals are capable of cross-linking DNA proteins, compro-mising structural integrity (58). Such reactions induce cell deathby a combination of apoptosis and cell necrosis, and interferewith protein synthesis and cell replication (59–61). Superox-ides may also modify gene transcription by the activation ofa potent regulator of gene transcription, the ubiquitous nu-clear factor-κB (NF-κB) (62). It is unclear what impact this has
on any specific protein synthesis, although one study providedsome evidence of a negative feedback mechanism by inducingthe expression of superoxide dismutase (63).
An additional primary target of oxygen-free radicals ispulmonary artery smooth muscle, resulting in vasoconstric-tion. Pulmonary artery smooth muscle contractility is affectedthrough a variety of pathways, although most involve eitherthe release of calcium from the sarcoplasmic reticulum or itssequestration via the enhanced activity of ATP-dependent Ca2+
uptake transporters. Superoxide anions also destroy nitric ox-ide produced by endothelial cells, in effect eliminating one ofthe most potent vasodilatory regulators in the lung (35).
A bimodal response to oxygen toxicity is seen in the lung.Initially, there is a proliferative phase where pulmonary arteryendothelial cells replicate rapidly in response to the presenceof superoxide anions. Superoxide anion production and releaseby these stimulated endothelial cells is far greater than that ofquiescent endothelium. Thus begins a vicious cycle of super-oxide radical generation and increased levels of exposure ofsurrounding lung parenchyma resulting in further DNA strandbreakage, depletion of ATP, and enhanced membrane lipid per-oxidation (64). This produces the inhibitory phase of endothe-lial proliferation. Other pulmonary cells such as bronchial andtype I alveolar epithelial cells are also early victims in oxidantinjury. Type I alveolar cells are replaced by hyperplasia of typeII alveolar epithelial cells, resulting in the typical thickeningof the alveolar epithelium seen in electron micrographs. Claracells, which are nonciliated epithelial cells distributed through-out the airways and rich in cytochrome P450, are particularlysensitive to oxidant stress (65).
The Clinical Manifestations ofPulmonary Oxygen Toxicity
It is common to treat hypoxemia with supplemental oxygen toincrease the inspired PO2. However, the clinical consequencesof continuous exposure to high partial pressures of inspired O2
(PiO2) are directly related to the inflammatory reactions result-ing from the cellular injury described above. While studies inanimal models have clearly shown the damage to alveolar ep-ithelial and vascular endothelial cells, the results in humanshave been less conclusive. It is very likely that, in additionto species differences, there are genetic, environmental, andpathologic processes that modify the susceptibility to oxygen-related lung damage in humans that have not yet been eluci-dated.
Initial attempts to delineate the threshold for oxygen toxi-city had their basis in military diving applications and duringattempts to develop cabin atmospheres for manned space flightand undersea habitats in the 1960s and 1970s. In a series of ex-periments in hyperbaric chambers during this period, healthydivers were subjected to 28 to 30 days of breathing air underincreased ambient pressure, with a target PiO2 0.51, 0.57, and0.81 atmospheres (66). Of note, the air at sea level provides aPiO2 of 0.21 ATM. The results of many such studies suggestedthat the threshold for signs and symptoms of pulmonary oxy-gen toxicity occurred at approximately a PiO2 of 0.60 (67,68);thus arose the clinical dictum that an FiO2 of <60% should bethe limit for prolonged oxygen therapy (69). However, it maynot be accurate to extrapolate such studies in healthy divers

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
Chapter 134: Oxygen Therapy and Basic Respiratory Care 2053
to sick patients with pre-existing parenchymal disease or thesystemic inflammatory response syndrome (SIRS).
Normal individuals breathing 100% O2 experience symp-toms of tracheobronchitis within 12 to 24 hours (69). Thisinitial phase of oxygen toxicity is marked by a decline in tra-cheobronchial clearance of particulates, substernal chest dis-comfort, tachypnea, and a nonproductive cough. Associatedsystemic symptoms include malaise, nausea, headache, andanorexia. While the decrease in particulate clearance may be-gin as early as 6 hours after such exposures, by 24 hours thevital capacity begins to decline significantly. Within 48 hoursof exposure to 100% oxygen, decrements in static lung compli-ance and carbon monoxide–diffusing capacity are measurable.In a study of patients with irreversible brain damage and venti-lated with 100% FiO2, the alveolar-arterial gradient increasedrapidly after 40 to 60 hours. Continued exposure of the lungs tohigh partial pressures of oxygen ultimately contributed to thedevelopment of the acute respiratory distress syndrome (ARDS)accompanied by severe dyspnea and subsequent pulmonary fi-brotic changes. Chest radiographic findings are nonspecific andshow increased interstitial markings or alveolar consolidationsimilar to a number of other causes of diffuse alveolar damage.
Hypercapnia
The wisdom of administering high partial pressures of oxygento patients with chronic hypercarbia continues to be a source ofdebate among clinicians. The concern has been that the patientwith CO2 retention (e.g., COPD) relies predominantly on a hy-poxic ventilatory drive and that increasing PaO2 by the admin-istration of oxygen will result in depression of this stimulus anda dangerous drop in minute ventilation with a rise in PaCO2.PaCO2 has been observed to rise in a subset of these patientssuffering acute exacerbations of their COPD when treated with100% O2 (60). However, there have been several studies in bothstable COPD and those with acute exacerbations that demon-strate only a transient decline in minute ventilation inadequateto explain the accompanying rise in CO2 (70–72). Another ex-planation for a rise in PaCO2 includes rightward displacementof the CO2–hemoglobin dissociation curve in the presence ofincreased oxygen saturation, and a consequent reduction incarboxyhemoglobin formation and transport—the Haldane ef-fect. More likely, there are relative increases in dead space ven-tilation via alterations in hypoxic pulmonary vasoconstriction.Hanson et al. modeled ventilation and perfusion in a computersimulation of the lung, and demonstrated that it was possi-ble to account for the change in PaCO2 by oxygen-inducedrelaxation of hypoxic pulmonary vasoconstriction (73). Thispulmonary vascular response to hypoxia is capable of redirect-ing blood flow from alveoli that are poorly ventilated to thosewith a higher PaO2. Blunting this response by artificially in-creasing the PaO2 prevents appropriate matching between ven-tilation and pulmonary perfusion, and permits a rise in CO2.A recent study examined a cohort of CO2-retaining COPD pa-tients recovering from an acute exacerbation after they hadbeen weaned from mechanical ventilation to a baseline FiO2 of0.3 to 0.4 (72). Patients were re-exposed to an FiO2 of 0.7 for20 minutes, and no statistically significant changes in respira-tory rate, tidal volume, dead space, or PaCO2 were reported.Robinson et al. compared two groups of patients with acuteCOPD exacerbations, dividing them into CO2-retaining and
nonretaining groups (74). They found only modest declines inminute ventilation, with a rise in PaCO2 averaging about 3mm Hg in the CO2 retainer group upon exposure to 100%O2 face mask. The dispersion of alveolar ventilation/perfusionratios increased nearly equally in both groups upon oxygenexposure, suggesting that hypoxic pulmonary vasoconstrictionwas affected equally in both groups. From these experiments,one must conclude that the mechanisms generating hypercap-nia in individuals with COPD treated with supplemental oxy-gen are varied and complex. Close monitoring of respiratoryparameters, including arterial oxygenation and carbon diox-ide, is mandatory when oxygen therapy is employed to reversesevere hypoxemia.
Absorption Atelectasis
An individual spontaneously breathing a high inspired con-centration of oxygen results in replacement of nitrogen withoxygen within the alveoli. This may cause absorption atelec-tasis secondary to oxygen diffusing into the alveolar capillaryblood more rapidly than nitrogen can diffuse into the alveoliand inhaled oxygen can replace the lost volume (75). This maybe more theoretical than practical, certainly in the short termwhere nitrogen will continue to diffuse into the blood from alltissues, and to some degree into the alveoli to re-establish anequilibrium. Nonetheless, it is potentially a problem in thoseregions of the lung experiencing low ventilation/perfusion ra-tios and subjected to large compressive forces (e.g., lower lobesfrom abdominal contents or weight of the heart in the supine in-dividual). The rate of alveoli collapse may potentially be greaterin those circumstances where there are increased metabolic de-mands and rates of oxygen uptake. Although the mechanismhas not been fully elucidated, decrements in vital capacity of upto 20% have been recorded after exposure to 100% oxygen inpatients, although oxygen-induced tracheobronchitis was pre-sumed (76).
SUMMARY
The management of airway, breathing, and oxygen therapyin critically ill patients continues to be a challenging task. Acomprehensive understanding of the various oxygen deliverymodalities is of utmost importance in not only delivering thehighest quality of care to the critically ill patients, but alsoavoiding major oxygen therapy–related consequences, includ-ing increased morbidity and even mortality.
References
1. Guilfojie T, Dabe K. Nasal catheter oxygen therapy for infants. Respir Care.1981;26:35–39.
2. Kory RC, Bergman JC, Sweet RD, et al. Comparative evaluation of oxygentherapy techniques. JAMA. 1962;179:123–128.
3. AARC Clinical Practice Guideline: Oxygen Therapy for Adults in the AcuteCare Facility—2002 Revision & Update. Respir Care. 2002;47(6):717–720.
4. Shapiro BA, Harrison RA, Kacmarek RM, et al. Oxygen therapy. In: ShapiroBA, Harrison RA, Kacmarek RM, et al., eds. Clinical Application of Respi-ratory Care. 3rd ed. Chicago, IL: Year Book Medical Publishers; 1985;176–191.
5. Ooi R, Joshi P, Soni N. An evaluation of oxygen delivery using nasal prongs.Anesthesia. 1992;47:591–593.
P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
2054 Section XIII: Respiratory Disorders
6. Domingo C, Roig J, Coll R, et al. Evaluation of the use of three differ-ent devices for nocturnal oxygen therapy in COPD patients. Respiration.1996;63(4):230–235.
7. Tiep BL, Nicotra B, Carter R, et al. Evaluation of a low-flow oxygen-conserving nasal cannula. Am Rev Respir Dis. 1984;130:500–502.
8. Tiep BL, Lewis ML. Oxygen conservation and oxygen-conserving devices inchronic lung disease: a review. Chest. 1987;92:263–273.
9. Garrod R, Bestall JC, Paul E, et al. Evaluation of pulsed dose oxygen de-livery during exercise in patients with severe chronic obstructive pulmonarydisease. Thorax. 1999;54:242–244.
10. Fuhrman C, Chouaid C, Herigault R, et al. Comparison of four demandoxygen delivery systems at rest and during exercise for chronic obstructivepulmonary disease. Respir Med. 2004;98(10):938–944.
11. Blackmon GM, Johnson MC II, Plotkin E. Rapidly progressive extensive sub-cutaneous emphysema associated with an implantable intratracheal oxygencatheter. Chest. 1998;113(3):834–836.
12. Jackson M, King MA, Wells FC, et al. Clinical experience and physi-ologic results with an implantable intratracheal oxygen catheter. Chest.1992;102:1413–1418.
13. Bethune DW, Coffis JM. Evaluation of oxygen therapy equipment. Thorax.1967;22:221–225.
14. Jensen AG, Johnson A, Sandstedt S. Rebreathing during oxygen treatmentwith face mask. Acta Anaesth Scand. 1991;35:289–291.
15. Banjer NR, Govan JR. Long term transtracheal oxygen delivery through mi-crocatheter in patients with hypoxaernia due to chronic obstructive airwaysdisease. BMJ. 1986;293:111–114.
16. Redding JS, McAffee DD, Gross CW. Oxygen concentrations received fromcommonly used delivery systems. South Med J. 1978;71(2):169–172.
17. Woolner DF, Larkin J. An analysis of the performance of a variable Venturi-type oxygen mask. Anaesth Intens Care. 1980;8:44–51.
18. Campbell EJM, Minty KB. Controlled oxygen therapy at 60% concentration.Lancet. 1976;2:1199–1203.
19. Cox D, Gifibe C. Fixed performance oxygen masks. Anaesthesia.1981;36:958–964.
20. Beecroft JM, Hanly PJ. Comparison of the OxyMask and Venturi mask in thedelivery of supplemental oxygen: pilot study in oxygen-dependent patients.Can Respir J. 2006;13(5):247–252.
21. Futrell JW Jr, Moore JL. The OxyArmTM: a supplemental oxygen deliverydevice Anesth Analg. 2006;102:491–494.
22. Foust GN, Potter WH, Wilson MD, et al. Shortcomings of using two jetnebulizer in tandem with an aerosol face mask for optimal oxygen therapy.Chest. 1991;99:1346–1351.
23. Barnes TA. Equipment for mixed gas and oxygen therapy. Respir Care ClinN Am. 2000;6(4):545–595.
24. Zikria BA, Spencer JL, Kinney JM, et al. Alterations in ventilatory func-tion and breathing patterns following surgical trauma. Ann Surg. 1974;179:1–7.
25. Stock MC, Downs JB, Gauer PK, et al. Prevention of postoperativepulmonary and conservative therapy complications with CPAP, incentivespirometry, and conservative therapy. Chest. 1985;87:151–157.
26. Motley H, Cournand A, Richards D. Observations of the clinical use ofintermittent positive pressure. J Aviation Med. 1947;18:417.
27. Marini JJ, Baker WL, Lamb VJ. Breath stacking increases the depth andduration of chest expansion by incentive spirometry. Am Rev Respir Dis.1990;141:343–346.
28. Freitas ERFS, Soares BGO, Cardoso JR, et al. Incentive spirometry forpreventing pulmonary complications after coronary artery bypass graft.Cochrane Database of Systematic Reviews 2007;3:CD004466. DOI:10.1002/14651858. CD004466.pub2.
29. Denehy L, Berney S. The use of positive pressure devices by physiotherapists.Eur Respir J. 2001;7:821–829.
30. Webber BA, Pryor JA. Physiotherapy skills: techniques and adjuncts. In Web-ber BA, Pryor JA, ed. Physiotherapy for Respiratory and Cardiac Problems.London: Churchill Livingstone; 1993:113–172.
31. Bott J, Keilty S, Noone L. Intermittent positive pressure breathing—a dyingart? Physiotherapy. 1992;78:656–660.
32. Ali J. Effect of post-operative intermittent positive pressure breathing on lungfunction. Chest. 1984;85:192–196.
33. Oikkonen M, Karjalainen K, Kahara V, et al. Comparison of incentivespirometry and intermittent positive pressure breathing after coronary arterybypass graft. Chest. 1991;99:60–65.
34. Stryer L. Oxidative phosphorylation. In Biochemistry. 4th ed. New York,W.H. Freeman and Co., 1995, 529–558.
35. Zhang DX, Gutterman DD. Mitochondrial reactive oxygen species-mediated signaling in endothelial cells. Am J Physiol Heart Circ Physiol.2006;292:H2023.
36. Halliwell B, Gutteridge JM. Role of free radicals and catalytic metal ions inhuman disease: an overview. Methods Enzymol. 1990;186:1.
37. Marshall C, Mamary AJ, Verhoeven AJ, et al. Pulmonary artery NADPH-oxidase is activated in hypoxic pulmonary vasoconstriction. Am J Resp CellMol Biol. 1996;15:633.
38. Kukreja RC, Contos HA, Hess ML, et al. PGH synthase and lipoxyge-nase generate superoxide in the presence of NADH or NADPH. Circ Res.1986;59:612.
39. Cross AR, Jones OT. Enzyme mechanisms of superoxide production.Biochim Biophys Acta. 1991;1057:281.
40. Forman HJ, Torres M. Reactive oxygen species and cell signaling: respiratoryburst in macrophage signaling. Am J Respir Crit Care Med. 2002;166:S4.
41. Comhair SAA, Erzurum SC. Antioxidant responses to oxidant-mediated lungdiseases. Am J Physiol Lung Cell Mol Physiol. 2002;283:L246.
42. Kinnula VL, Crapo JD. Superoxide dismutases in the lung and human lungdiseases. Am J Respir Crit Care Med. 2003;167:1600.
43. Bowler RP, Crapo JD. Oxidative stress in airways: is there a role for extra-cellular superoxide dismutase? Am J Respir Crit Care Med. 2002;166:S38.
44. Sandstrom J, Karlsson K, Edlund T, et al. Heparin-affinity patterns and com-position of extracellular superoxide dismutase in human plasma and tissues.Biochem J. 1993;294:853.
45. McCord JM, Fridovich I. Superoxide dismutase: an enzymic function forerythrocuprein (hemocuprein). J Biol Chem. 1969;244:6049.
46. Ross D, Norbeck K, Moldeus P. The generation and subsequent fate of glu-tathionyl radicals in biological systems. J Biol Chem. 1985;260:15028.
47. Deneke SM, Fanburg BL. Regulation of cellular glutathione. Am J PhysiolLung Cell Mol Physiol. 1989;257:L163.
48. Meister A, Anderson ME. Glutathione. Am Rev Biochem. 1983;52:711.49. Kolleck I, Sinha P, Rustow B. Vitamin E as an antioxidant of the lung:
mechanisms of vitamin E delivery to alveolar type II cells. Am J Respir CritCare Med. 2002;166:S62.
50. Das KC, Guo XL, White CW. Induction of thioredoxin and thioredoxinreductase gene expression in lungs of newborn primates by oxygen. Am JPhysiol Lung Cell Mol Physiol. 1991;276:L530.
51. Davies K. Oxidative stress: the paradox of aerobic life. Biochem Soc Symp.1995;61:1.
52. Valko M, Leibfritz D, Moncol J, et al. Free radicals and antioxidants innormal physiological functions and human disease. Int J Biochem Cell Biol.2007;39(1):44.
53. Doelman CJ, Bast A. Oxygen radicals in lung pathology. Free Radic BiolMed. 1990;9:381.
54. Van der Vliet A, Smith D, O’Neill CA, et al. Interactions of peroxynitritewith human plasma and its constituents: oxidative damage and antioxidantdepletion. Biochem J. 1994;303:295.
55. Finkel T, Holbrook NJ. Oxidants, oxidative stress and the biology of ageing.Nature. 2000;408:239.
56. Rahman I, Biswas SK, Kode A. Oxidant and antioxidant balance in theairways and airway diseases. Eur J Pharmacol. 2006;533:222–239.
57. O’Reilly MA. DNA damage and cell cycle checkpoints in hyperoxic lunginjury: braking to facilitate repair. Am J Physiol Lung Cell Mol Physiol.2001;281(2):L291–305.
58. Wiseman H, Halliwell B. Damage to DNA by reactive oxygen and nitrogenspecies: role in inflammatory disease and progression to cancer. Biochem J.1996;313:17.
59. Mantell LL, Lee PJ. Signal transduction pathways in hyperoxia-induced lungcell death. Mol Genet Metab. 2000;71(1–2):359–370.
60. Nanavaty UB, Pawliczak R, Doniger J, et al. Oxidant-induced cell death inrespiratory epithelial cells is due to damage and loss of ATP. Exp Lung Res.2002;28:591.
61. Volkert MR, Landini P. Transcriptional responses to DNA damage. CurrOpin Microbiol. 2001;4:178.
62. Shreck R, Baeuerle PA. Assessing oxygen radicals as mediators in activationof inducible eukaryotic transcription factor NF-kappa B. Methods Enzymol.1994;234:151.
63. Demple D. Study of redox-regulated transcription factors in prokaryotes.Methods. 1997;11:267.
64. Li PF, Dietz R, von Harsdorf R. Differential effect of hydrogen peroxide andsuperoxide anion on apoptosis and proliferation of vascular smooth musclecells. Circulation. 1997;96:3602.
65. Cho M, Chichester C, Plopper GC, et al. Biochemical factors important inClara cell selective toxicity in the lung. Drug Metab Rev. 1995;27:369.
66. Dougherty JJH, Frayre RL, Miller DA, et al. Pulmonary function duringshallow habitat air dives (SHAD I, II, III). In: Schilling CW, Beckett MW,eds. Underwater Physiology VI: Proceedings of the Sixth Symposium onUnderwater Physiology. Bethesda, MD: FASEB; 1978:193.
67. Morgan TE Jr, Ulvedal F, Welch BE. Observations in the SAM two-manspace cabin simulator. II Biomedical aspects. Aerospace Med. 1961;32:591.
68. Clark JM, Lambertsen CJ. Pulmonary Oxygen Tolerance in Man and Deriva-tion of Pulmonary Oxygen Tolerance Curves. Institute for EnvironmentalMedicine Report. Philadelphia: University of Pennsylvania; 1970:1.
69. Clark JM, Thom SR. Oxygen under pressure. In: Brubakk AO, NeumanTS, eds. Bennett and Elliott’s Physiology and Medicine of Diving. 5th ed.Edinburgh: Saunders; 2003:358.
70. Aubier M, Murciano D, Milic-Emili J, et al. Effects of the administrationof O2 on ventilation and blood gases in patients with chronic obstructivepulmonary disease during acute respiratory failure. Am Rev Respir Dis.1980;122:747.
71. Sassoon CSH, Hassell KT, Mahutte CK. Hyperoxic-induced hypercap-nia in stable chronic obstructive pulmonary disease. Am Rev Respir Dis.1987;135:907.
72. Crossley DJ, McGuire GP, Barrow PM, et al. Influence of inspired oxygen

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
Chapter 134: Oxygen Therapy and Basic Respiratory Care 2055
concentration on deadspace, respiratory drive, and PaCO2 in intubatedpatients with chronic obstructive pulmonary disease. Crit Care Med.1997;25:1522.
73. Hanson CW, Marshall BE, Frasch HF, et al. Causes of hypercarbia withoxygen therapy in patients with chronic obstructive pulmonary disease. CritCare Med. 1996;24:23.
74. Robinson TD, Freiberg DB, Regnis JA, et al. The role of hypoventilation and
ventilation-perfusion redistribution in oxygen-induced hypercapnia duringacute exacerbations of chronic obstructive pulmonary disease. Am J RespirCrit Care Med. 2000;161:1524.
75. Duggan M, Kavanagh BP. Pulmonary atelectasis: a pathogenic perioperativeentity. Anesthesiology. 2005;102:838.
76. Carvalho CR, de Paula P, Schettino G, et al. Hyperoxia and lung disease.Curr Opin Pulm Med. 1998;4:300.

P1: OSO/OVY P2: OSO/OVY QC: OSO/OVY T1: OSO Printer: Yet to come
GRBT291-134 GRBT291-3641G GRBT291-Gabrielli-v2.cls October 25, 2008 16:3
2056