Changing power relationships between nurses: a case-study of early changes towards patient-centred...
12
Journal of Clinical Nursing 1993; 2: 219-229 Changing power relationships between nurses: a case-study of early changes towards patient-centred nursing ANGIE TITCHEN MSc, MCSP Research and Developmental Fellow, National Institute for Nursing,* Radclijfe Infirmary, Oxford 0X2 6HE, UK ALISON BINNHI MA, RGN, RM, Dip.N Senior Sister, John Radclijfe Hospital, Headington, Oxford, UK Accepted for publication 20 January 1993 Summary • This case-study provides a description and interpretation of the traditional power relationship between a sister and staff nurses, in an acute general medtcal ward. • The ways in which the nurses changed that power relationship, with the introduction of team nursing are explored. • The paper describes, from the sister's and nurses' perspectives, the difficulties associated with the devolution of authority, from sister to team leaders, and the resulting confusion about the new relationship between them. • Three themes emerged in the changing power relationships and these are presented and examined. Keywords: patient-centred nursing, power relationships, devolution of authority, primary nursing, team nursing. Introduction Patient-centred nursing, where care is tailored specifically to each patient's needs, has aroused much interest and is being widely promoted in the UK by the nursing profes- sion, as a desirable alternative to traditional nursing. However, very little is known about this kind of nursing or about the processes involved when nurses change their work organization method and power relationships in order to create a structure which offers an opportunity to practise in a patient-centred way. In 1989, Alison Binnie was appointed as a senior sister, in an acute medical unit, to lead the change from tra- * The National Institute Jor Nursing was formerly the Institute oJ Nursing at O.xjord. ditional nursing to patient-centred nursing. Alison approached the Institute of Nursing at Oxford*, to pro- pose the setting up of a collaborative study which would both support and investigate this major change in practice. Angie Titchen, an educationalist and researcher with a physiotherapy background, was appointed by the Institute as research associate to the project. Our 'value position' at the outset and throughout the research was one of deep commitment to patient-centred nursing. The aim of our action research project, entitled Patient- Centred Nursing in Practice, was to help nurses in two medical wards to change gradually from traditional nurs- ing to patient-centred nursing (using the work organiza- tion method known as primary nursing), and also to study the complex organizational, professional and personal changes considered necessary for such a major shift in 219
-
Upload
angie-titchen -
Category
Documents
-
view
214 -
download
2
Transcript of Changing power relationships between nurses: a case-study of early changes towards patient-centred...

Journal of Clinical Nursing 1993; 2: 219-229
Changing power relationships between nurses: a case-study of earlychanges towards patient-centred nursing
ANGIE TITCHEN MSc, MCSPResearch and Developmental Fellow, National Institute for Nursing,* Radclijfe Infirmary,
Oxford 0X2 6HE, UK
ALISON BINNHI MA, RGN, RM, Dip.NSenior Sister, John Radclijfe Hospital, Headington, Oxford, UK
Accepted for publication 20 January 1993
Summary
• This case-study provides a description and interpretation of the traditionalpower relationship between a sister and staff nurses, in an acute general medtcalward.
• The ways in which the nurses changed that power relationship, with theintroduction of team nursing are explored.
• The paper describes, from the sister's and nurses' perspectives, the difficultiesassociated with the devolution of authority, from sister to team leaders, and theresulting confusion about the new relationship between them.
• Three themes emerged in the changing power relationships and these arepresented and examined.
Keywords: patient-centred nursing, power relationships, devolution of authority,primary nursing, team nursing.
Introduction
Patient-centred nursing, where care is tailored specificallyto each patient's needs, has aroused much interest and isbeing widely promoted in the UK by the nursing profes-sion, as a desirable alternative to traditional nursing.However, very little is known about this kind of nursing orabout the processes involved when nurses change theirwork organization method and power relationships inorder to create a structure which offers an opportunity topractise in a patient-centred way.
In 1989, Alison Binnie was appointed as a senior sister,in an acute medical unit, to lead the change from tra-
* The National Institute Jor Nursing was formerly the Institute oJ
Nursing at O.xjord.
ditional nursing to patient-centred nursing. Alisonapproached the Institute of Nursing at Oxford*, to pro-pose the setting up of a collaborative study which wouldboth support and investigate this major change in practice.Angie Titchen, an educationalist and researcher with aphysiotherapy background, was appointed by the Instituteas research associate to the project. Our 'value position' atthe outset and throughout the research was one of deepcommitment to patient-centred nursing.
The aim of our action research project, entitled Patient-Centred Nursing in Practice, was to help nurses in twomedical wards to change gradually from traditional nurs-ing to patient-centred nursing (using the work organiza-tion method known as primary nursing), and also to studythe complex organizational, professional and personalchanges considered necessary for such a major shift in
219

220 A. Titchen and A. Binnie
practice style. The purpose of the project is to provide UKnurses with a 'map' of the processes involved in the changefrom traditional to patient-centred nursing and to suggestthe kind of strategies that are likely to be effective inachieving the change. I'his paper focuses on the findingswhich clarified the nature of the traditional power relation-ship between the sister and the staff nurses and how thisrelationship was changed to lay the foundations for prim-ary nursing.
Befot-c the ch-angcs were introduced, the organization ofthe nursing work in the two study wards involved one, or apair o( nurses (depending upon how many nurses were onduty), being allocated (on a shift by shift basis) the care ofpatients located in each half of the ward. Nurses allocatedto the patietits at one 'ctid' of the ward stayed at that 'end'for several consecutive shifts whenever possible, but thiswas not predictable. The sister, or the tnost senior nurse onduty in the former's absence, was 'in charge'.
In 1989, team nursing was established. The ward nurseswere grouped into three permanent teams and the dutyrota was organized to ensure that there was always aminitnum of one nurse from each team on duty. Patientswere allocated to a team on admission and were nursed bythis same small group of nurses throughout their stay.Whilst the traditiotial 'in charge' role was abandoned, onenurse was still nominated 'co-ordinator' for the shift, andwas expected to retain an overview of ward activities and toco-ordinate liaison between team nurses and tnetnbers ofother disciplines. This structural change created the op-portunity for patient-centred nursing to being to emerge,because nurses had tnore clearly defined responsibilitiesfor a smaller caseload of patients. Predictable continuity,guaranteed by the system, meant that much closer andmore sustained relationships could begin to developbetween nurses and their patients. The establishment ofthe team system was seen as the first step towards primarynursing.
Changing the way in which nurses worked meant thatnew roles and power relationships had to be negotiated. Ifnurses were to be allocated responsibility fbr patient care,decision making and leading the nursing teatns, then theymust be authorized to act withiti the sphere of theirresponsibility (Manthey, 1980).
In practice, changing the work organizational designand devolving authority for decision making resulted,initially, in confusion for the tiurses. l'"or example, theywere unclear about the extent of their new respon.sibiliticsor how far to tnove into areas of work previously utider-taken by the person 'in charge'. One of us, A.T., docu-mented this confusion in a case-study, carried out in one ofthe study wards, 5 months after team nursing was intro-
duced. Although A.T. collected, analysed and interpretedthe data, A.B. shared the planning and writing up of thecase-study. The work was to provide a starting point forthe action research, by identifying how the nurses madesense of their experience on the ward before and during theeary days of the chatige and their needs for personal andprofessional developtnent. A.T. describes the researchproject and its t-esults.
The ease-study
At the beginning of the rcseai-ch, a theoretical frameworkof patient-centred nursing was devised frotn our personalexperience and from the literature on primary nursing. Weeventually rejected much of the etnpirical work reported itithe literature, on the grounds that it is mttthodologicallyflawed, finding support in the litetature for this view(Giovannetti, 1986). We decided, tlietcfore, to start withouta thcotetical ftamcwork, that is, without identifyitig vati-ables and possible telationships between them (which inturn suggest research questions and data collection methods).
The aim of the approach adopted was to gain a pheno-menological utiderstanding of the situation the nurses weretrying to change and of their early experiences of theinnovation. An attempt to understand the nature of wardlife and the processes of nursing and learning frotn theperspective of the participants was being made. Theapproach described by Schutz (1962) was used, whichfollowed well-established tesearch procedures developedby Benner (1984), Bt-own & Mclntyre (1988) and Mac-Leod (1990). Having previously made t)ur personal theor-etical understandings of the substantive area explicit, Iattempted to 'bracket' (Schutz, 1962; Otnery, 1983) orsuspend them during data collection, by adopting the roleof 'sttanger' who goes into the situation, naively, andwithout pteconceptions of what might be found. This rolehad sotne credibility with the nutses iti the study wardbecause I do not have a nut-sing background. The nursesexpected me to have some general insights into what wasliappenitig because of my clinical experience, but they didnot make the assumption that I would be familar with theordinary and taken-for-granted knowledge of the practis-ing nurse. Success, or otherwise, at 'bracketing' wastnonitored and tecorded (Titchen & Mcfntyrc, 1992).
1 he aims of the case-study were to:1 describe the early change to tcatn nursing from theperspective of patients, nurses and hospital staff",2 capture nurses' perceptions and feelings about
• traditional nursing before the change,• the experience of the initial changes,• further changes that were planned.

Changing power relationships between nurses 221
Only the data which relate to the changitig power relation-ship between the sister/senior sister and the staff nurses arepresented in this paper.
The aim was not to give a full, literal description of theexisting state of affairs in the case-study ward, but toattempt to clarify the basic structures or otganizationalfeatures and the underlying change processes taking placein the ward. Becher & Kogan (1980) stated that the valueof seeking to identify fundamental components and inter-connections is, that if the initiative is successful, it willhave 'wider relevance and a more enduring validity thanthe literal depiction of the contemporary scene'. The basicpremise of the investigation was, therefore, the study of thestructutes and processes frotn a phenomenological per-spective. My task was to interpret the participants' percep-tions and feelings by usitig abstractions or constructs,drawn, where appropriate, from my own ktiowledge,crnpirical work and the social sciences. Thus, I wasattempting to genctate a theorized account or social theoryabout the initial changes from traditional to patient-centred nursing. Theorization, through linking the find-ings to substantive social science theory and existingempirical work, plus a rich description of this particular
situation, enables readers of the research, to make de-cisions about whether the findings can be generalized andapplied to their situations.
Methodology
The fiekiwork was carried out over a 14-week period, usingparticipant observation, in-depth interviews and review ofdocutnentation, for exatnple, minutes of ward meetingsand care plans. By combining a number of data sourcesand research methods, it was possible to cross-check thedata (Titchen & Bimiie, 1992a). A very thorough atidrigorous phenomenological approach to the qualitativedata analysis was devised and is described elsewhere(Titchen & Mclntyre, 1992).
The themes
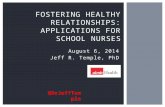
In total 11 themes were identified in the study (Fig. 1),three of which are presented here, because they relate tothe construct 'changing power relationships betweennurses'. The theme titles are derived from the first-orderconstructs of the participants in the situation, for example.
7.
6.
3.
4.
10.
8. Working relationships
11. The vision
1. In charge 2. Thrown at us
Communication
We needed more support
What the hell am I supposed to be doing?
Make it up as you go along
Change for the better—perhaps not yet
9. A bit of eachsystem really
5. She's not my patient
Figure 1 The cctiinil and marginal themes as |)crccivcd by the participani.s in the .situation.

222 A. Titchen and A. Binnie
'In charge', and from my second-order constructs, forexample, 'Old Cultural Norms' which are derived from myexperience, tny knowledge of the social sciences, and theetnpirical and theoretical literature (Titchen & Mclntyre,1992).
Theme 1,'/« Charge^: Old Cultural Norms, presents theinitial power relationship between the sister and the nursesin the traditional ward setting. The staff nurses perceivedthat the locus of control lay with the sister and decisionmaking was centralized and autocratic. In Theme 2,'Thrown at us'': Initial Top-down Change Strategy, theinitiation of the change to team nursing was perceived bythe nurses as 'top-down', but welcome. Theme 3, 'Whatthe Hell am I Supposed to he DoingV: Role Ambiguitydescribes the confusion which occurred when new roleswere not clarified or negotiated and power and authoritywere not devolved explicitly.
A tentative proposition which connects the concerns andissues arising from the three themes was generated.
If there is an attempt to change the powerrelationship between staff nurses and the sister (bymoving from the cultural norm of autocratic,centralized decision tnaking, to a norm ofdecentralized decision making), nurses willexperience role ambiguity, if authority is notexphcitly and publicly devolved by the sister.
The proposition was used to develop a tentative guidingprinciple for effecting role clarity which was tested later inthe research.
My interpretations of and theorizations from the dataare presented in italic typeface. The names of the teamleaders and sister have been changed to protect theiridentities. The pronouns 'she' or 'her' arc used because allthe nurses were female.
THEME 1 IN CHARGE : OLD CULTURAL NORMS
The elements of this theme are cultural norms prevailingon the ward before, and in the early days of, the changes(see Fig. 2).
' / have the keys, 1 therefore have the power': autocraticdectsion maieing
The nurses with experience of the ward, before the changeto team nursing, perceived that, at that time, a traditionalhierarchy was in place:S.N. (There was an ethos of) f have the keys, I therefore
have the power. . . . A hierarchical sort of structurewas in force then.
Staff nurses' decisions
1 have the keys, 1therefore have thepower
Sister knew everything
Task allocation
Communication
Figure 2 Theme 1. '/?; charge
Decisions on ward organization, patient care and dischargeplanning were made by the person 'in charge', i.e. thesister or the most senior nurse on duty in her absence. Thesister, unlike the senior staff nurse, had responsibility fordecision making beyond the length of her 'in charge' shift.
There was evidence that the nurses tended to accept theauthority of the person 'in charge' to make key decisions asthe norm.S.R. Nurses are fairly disciplined and if I say we are going
to do it, they do it..S.N. It was working quite well because that's how I'd
worked where I came frotn before. So to tne, it wasnormal.
S.N. I don't think I ever thought about how I could change(things) or whatever, because I didn't feel that I was ina situation to do anything about it.
The norm on t/te tvcird was one of a hureaucratic hierarchy.Weber (1947) first characterized a htireaucrcuy with twomain features— a division of labour and a hierarchicalmanagement. Within a traditional hierarchy, power is vestedin a positton within the organization and not in an individual.McMahon's (1990) study confirms my finding that in wardswith a hierarchical management, power rested tinth the 'incharge' position, regardless of who held it at any parttcttlartime. Traditionally, this person holds the ward keys (McMa-hon, 1991). I suggest that the keys symbolize the authoritywhich IS invested in the person holding them and convey thelegitimate capacity to exercise potver.

Changing power relationships between nurses 223
The concept of porver has been studied by marty disciplines
and from many perspectives. There are stibscquently many
meanings of the term 'power' and no agreed definition.
Perhaps the most freijnently c/uoted defittition tn the nursing
Itteratttre is that by the sociologist Max Weber:
'. . . tbe probability that one actor within a socialrelationship will be in a position to carry his ownwill despite resistance, regardless of the basis onwbich that probability rests.' (Weber, 1947, p. 152.)
Hokanson Hawks (1991) in her concept analysis of power,
suggested that power appears to be associated with effective-
ness Cpofper to') or tpith forcefulness ('power over'). The
language used by the sister and the staff mirse in the first ttvo
quotes above, suggests that the sister, or the person 'in charge'
m her absence, had 'potver over' the staff nurses, whilst the last
quote stiggests the staff mirse's perceived lack of 'power to'
change the status quo.
The staff' ntirses had been socialized into accepting their
place tpitltin the hierarchy and did not expect to have any
control over their working lives. This finding supports evi-
dence in Binnie's (19S8) study. Lukes (1986, cited in
Robinson, 1991) argued that power concerns the complex and
subtle ways in which institutions—political, industrial and
educational—influence peoples' thinking and perceptions.
Consequently, '. . . they accept their role in the existing order
of things, either because they see it as natural and unchange-
able, or because they value it as divinely ordained and
beneficial'.
Three months before the fieldwork began, I attended award meeting to talk about tbe project and to observe therest of the meeting. At this point, ward meetings were stillvery new and unfiimiliar. I made the following observationof the style of leadership of the sister, Lorraine.I'lELDNOTE. Lorraine's style of leadership appears essen-
tially autocratic. She made all the final decisions,without asking the others what they thought. Discus-sion in the group tended to be between Lorraine andthe individual nurse and not between nurse and nurse.No-one was asked to be responsible for carrying outthe decisions made.
The nurses did not always agree with Lorraine's de-cisions or the task routines on the ward, but, on the whole,they did not challenge her.S.N. A lot of people cotne onto the ward . . . talking loudly
and sister would say, 'be quiet' or 'it is rest time'. Imean, gosb, that went out with the Ark, but still, youknow, we have our rest periods and they haven'tchanged and I don't think things like that will, withouta lot of special encouragement.
Before the change to team nursing, Mary, an exper-ienced staff nurse, felt that tnost of the nurses did not see
Lorraine as open to new ideas or change. Mary gave anexample where she had decided to apply a particulardressing to a patient's bed sore. Her colleague was nothappy about this decision, but wben Mary pressed her for'a rationale for not liking it', the nurse responded, 'Sisterdoesn't like it'. Mary concluded that her colleagues were'frightened' to approach sister and suggest new things. Shefelt that their fears were unfounded because when shepresented her research-based rationale for using the dress-ing, Lorraine accepted her argument. Mary thought thatthe nurses were unable to overcome their 'fear of sister'because the old ward structure maintained the position ofthe sister at the top of the ward hierarchy. The studentsand junior nurses felt that they had come to expect atraditional sister to be a bit of an 'ogre' and that Lorrainewas 'a bit of the old school'.
The result of authority being invested in one person wasthat the staff nurses considered that responsibility forpatient care decision making was withheld from them, ifthey were not 'in charge'. They (and the senior students)wanted more responsibility and had started to grumble, forexample, a staff nurse said, 'Nobody's willing to give youany responsibility'.
The nurses' grtimbling may suggest that they trere exper-
iencing 'role deprivatioit'. In other words, they had been
professionally prepared to do more than they were betng
allowed to do in the ward. In a study hy Kramer (1968),
nurses who were employed in roles in which they could not
fulfill their professional expectations, experienced role depri-
vation. Binnie's (1988) study gives further exatnples of staff
nurses feeling frtistrated and demotivated hy the absence of
personal atithority for clinical decision making.
When I asked Anna, one of the team leaders, about herprevious experiences of nursing, she explained that, asnurses became more senior, they moved further away from'the bedside'. A sister was even further removed fromactual patient contact and, yet, she was the person makingthe decisions about tiursing care. Anna implied that shesaw this situation as being inappropriate.
Before team nursing tpas established on the ward, there was
a cultural norm of autocratic, autonomous decision making hy
the person 'in charge', for ward organization and patient care.
The organizational theory upon which such decision tnaking
was hased was one of centralized decision making. According
to Goodman (1965, cited in Manthey, 1980), this kind of
decision tnaking is only approriate in organizations where the
product of the functions is ittanimatc and where the tasks, to
achieve the functions, are predictahle, repetittvc and automa-
tic. In organizations where hutnan beings arc involved, the
tasks to achteve the functions are not predictable, repcttttvc or
automatic. For the most efficient and economical way of

224 A. 'f'itchcti and A. Binnie
working, control and decision maktng shottld lie at the level ofaction. By seeing the tnapproprtalcness of nursing caredecisions betng made by nurses tvho are not directly involved,and hy complaining thai they are not being given responsi-bility, the nur.ses were inferring ihat decentralized decisionmaking is more appropriate for patient care.
It appears that the norms of centralized deciston makingand not challenging routine and ritual were maintainedthrough a fear of sisters, in general, and through a fear of thissister, in particular. Studies by MacCiuire (1901) andRei'ans (1964) produced evidence that the legacy of the'dragon' sister and ihe /earful student remained. Manthey(I9H()) suggested that nursing is still influenced by its'ptinishmenl-oriented heritage'. I suggest that these staffnurses were afraid that they would be punished or repri-manded if they challenged the system.
'Sister knew everything': knowledge = power
The nurses reported that the person 'in charge' was theonly nurse in the ward who knew 'what was going on' withevery patient. She was expected to cotnmunicate withrelatives, doctors and health professionals and most of thecotnmunications from, and to, the nurses went throughher. The person 'tn charge' being the centre of communicationfor the ward replicates Pembrey's (1980) and McMahon's(1990) ftndings. This person was seen by the nurses as verypowerful, because she possessed a whole t-ange of ktiow-lcdge and was the nurse to whom people turned, lorinfortnation, to sort out problems and to get things done.
Because doctors and health professionals had heen social-ized to expect that the sister's role was to communicate withthem, they did so, which meant that she knew about eachpatient.
The sister's power, in particular, was accepted unques-tionably by the staff nurses, and she was seen to maintainher power by not handing on information to the nut-ses.S.N. (Tradit:ional experience elsewhere) It tends to be that
the doctors talk to Sister and it dcpctids what she islike (whether) she will pool that information. If shedoesn't, you are left at the bottom to run the baths.
7he sister's philosophy ahout sharing information with thenurses strongly influences the working life off he staff nurse.The sister is the gcUekeeper lo knowledge and controls commu-nication channels. If she does not share the knowledge with thestaff nurses, they are disempowered and reduced to carryingout routine tasks.
Knowledge gave the person 'in charge' 'power to' acteffectively and 'power over' the nurses, because she had theinformation upon which to base decisions winch the staff nurseswould carry out.
l l ie sister's control of knowledge and communicationpersisted, to sotne extent, in the early days of the change toteam nursing. The nutses found that when Lorraine wasacting as co-ordinator, she often withheld infonnationuntil the shift handover. The nurses felt that she was stillworkitig partly as though she were 'in charge' and not fullyperforming the new liaison role. The delay in the informa-tion being handed on tnade it difficult for the tiurses toorganize and plan their work and to respond quickly torequests from doctors and health professionals. Lorrainesaid that she waited until the shift handover to pass oninfortnation because she saw it as the quickest and tnostefficient way of doing so.
In the old system, betng 'in charge' gave access to importantinformation and implied authority to make decisions aboutpatient care. Thus the 'in charge' role, invested mainly in thesister, was a source of power. The rest of the nursing team,denied information and dependent upon instructions frontahove, were effectively disempowered. In the new system, whenthe sister withheld inforntation until the next shift handover,the nurses also fell disempowered. This information was notwithheld intentionally to diseinpower (he nurses, it was thestster's attempt to manage her time efficiently and reflected hertask-orientated leadership style (Fiedler, 1971). This situa-tion shows how power can have unintended effects on thepeople around the person holding the power.
The hierarchical communication structure was beginning tobe replaced by a spread of information throughout theorganization, thus it was beginning to take on the features oj a.lateral or organic structure (Burns Q> Stalker, 1961). In thetransition period, the sister tended, at times, to slip hack intoihe old mind-set and old power relationships.
THt'MI' 2 'TitROWN AT US': INITIAL TOI'-DOWN CHANGE
STRATKCfY
The eletnents of Theme 2 are shown in Figute 3.
'Have a go at this and see what happens': facilitatingownership of change
In retrospect, the nurses saw the initiation of the change asbeing imposed from above 'thrown at us' by the seniorsister and the sister. It seemed that the idea had beentossed to thetn and that they had been 'left to their owndevices to battle it out', without enough support. At theirfirst ward meeting, they remembered discussing the pro-posal, welcoming it and coming to a consensus decisionthat they would try it. This decision wa.s described inslightly different ways, 'Let's give it a go' (indicating thatthey were owning the idea) rcjircscnted all but one of the

Chatiging power relationships between nurses
Organizationalchanges camefirst
Have a go at this and see whathappens
1 didn't know what to expect
Initial shannbles and confusion
It just sort of happened— overnight
Figure 3 Theme 2. ^'Thrown at us.'
nurses' views, whilst 'I supposed we accepted it we werequite happy to try it' (ittdicatcd acceptance oj sotttconc else'sidea, tpith a hint of resignation) was the idiosyticraticresponse from the one nurse who was not happy with thechanges at the outset. The rest of the nurses were verypositive and enthusiastic about the prospect of change.
Nurses, not at the tneeting, had no recollection of theiropinion ever being sought. Although they supported thechange, they would have preferred to have been consulted.S.N. It would have been nice for the whole ward, all the
staff and students, to have sat down and discussed it.The senior sister was very clear that her leadetship was notabout getting people to follow her blindly. Rather, sheaimed to enable people to initiate and carry forwardchanges themselves.
S.S. I recognize that that kind of leadership stems fromwell-established, trusting relationships. I wanted toallow people to get to know me, to see me as non-threatening but helpful. Whilst I knew I would needto generate enthusiasm and ideas, I wanted to helppeople come up with their own ideas initially — to getinvolved with the development work and take thingsforward themselves. . .
A.T. What would you have done if they had not wanted to
make the changes?S.S. I would have accepted their decision and gone on
working on their dissatisfactions with the old system,until they started to push for change thetnselves.
The initiation of the change was perceived hy the ntirscs as
'top-dottm' (Ottaway, 1976) hut tpclcomc. They satr that the
decision to suggest change cantc front the scntor ststcr. Hotp-
evcr, it is clear from her articulation of her change strategy
that the settlor .<:istcr did not ttHutt to impose change hy ustng a
'top-dowtt' approach or 'tnanagctncnt cdtct' (Manthey,
1980). She presented the proposal for change to the staff
nurses and sought a conscttsus dcctsion. She tpatttcd to create a
clitnatc for a 'hottotn-up' approach which involves the partici-
pation of the people who ipill he affected hy the change. Such
an approach cnahlcs people to have control over thctr tporktng
lives. The senior .s'w/cr adopted a participative (Schcin, 1980)
attd relationship-orientated (Fiedler, 1971) .^tylc ofmanagc-
tncnt (as opposed to task-oricntatcd) and attctnptcd to foster
trttst and ownership of the change through consensus decision
makittg. Her tnind-sct was one of giving support without
pressure. Manthey (1980) argued that this tnind-sct will
facilitate the introduction of primaty nursing and promote a
clitnatc for success. She urges nurses in higher level positions
not to exert pressure and trams that this strategy may he a
difftcttlt one to achieve.
The senior sister cnahled participative dcctsion tnaktng hy
providing the structure, i.e. the tpard tneeting. However,
hcyond this point, there trcre no dccision-tnaking and fccdhack
loops. The decision to go ahead tpith the change tfas tnade hy
the nttrscs who happened to he on duty on the day oj the ward
tneeting. It tpas only months later, after stajf nttrses had
experienced having sotne control over their iporking lives, that
they could reflect that a truly dctnocratic decision would have
involved everyone in the tvard. Nevertheless, the nurses fell
that they otrncd the change right frotn the heginning.
THEME .1 ' W H A T THE ttELL AM t SUPPOSED TO BE
DOING?': ROLE AMBIGUITY
The elements of Theme 3 are shown in Figure 4.
7'w cottfuscd'
The nurses and the sister were confused, to varyingdegrees, about their own and others' new or modified roles.As the data are very rich, I have litnited illustrativeexamples to the team leader and sister roles.
The role of the teatn leader
Confusion over what was expected of the team leadersseemed to be linked to the lack of clarity in the lines olresponsibility and accountability, and in particular, theextent of their authority for tnanagement of staff andnursing care.

226 A. Titchen and A. Binnie
I'm confused
Help with developingthe roles
Nurses pushiing outthe boundaries/Sisterletting go
'Using' a seniorstaff nurse'Fait accompli'
Patient careDecision making
Figure 4 Theme 3. ''Whcii the hell am I supposed to be doing?'
6/9/89. Team leaders meeting: the teamleaders felt that their new role had 'just evolved' andthat it was not 'really recognized' . . . they said thatthey did not feel that they had 'the authority to act as aleader'.
At a staff development interview, Anna, the least confidentteam leader, told the sister and senior sister how insecureshe had been feeling:s.N. They said, 'and how can we help you?' and I said,
'Well quite a lot actually—what the hell am I meant tobe doing?' And then they said, 'Oh yes, we have beenthinking about this and we will have to meet andeverything', and then it did get arranged and we had ameeting of team leaders.
At this meeting, the senior sister described the team leaderrole as she saw it:FIELDNOTE 6/9/89. The senior sister talked about the
team leader role and the boundaries of authority, i.e.they could push almost as far as primary nursing butthat the sister had the veto. The team leader shoulddecide whether they or their team is capable of makingparticular decisions. Problems that they felt unable todeal with should be taken to the sister.
Although authority had been explicitly devolved at this
meeting, Anna was still not clear. She was fearful that she
would make 'a dog's dinner of it', l^his team leader was
describing role ambiguity which exists where individuals have
inadequate information about their role, that is, the objectives
associated with the role, its scope and responsibilities and
others' expectations of it (Harre & Lamb, 1986). Moreover,
Anna did not feel that the devolution of authority to theteam leaders had been made public enough, by the sisterand senior sister, to be recognized by her team (only theteam leaders were present when authority was explicitlydevolved).S.N. I was new . . . you don't want to rock the boat and be
seen as 'who the hell does she think she is, marchingon here and telling us what to do'.
The team leader wanted her new role to be legitimized so that
the team members' expectations of her and their behaviour
towards her would change. Banton (1965) argued that role
change is not always easy. He said that it requires individuals
to be aware of lhe rights and obligations of the new role and
their behaviottr to be changed accordingly. It is also necessary
for other people to recognize the role change and to modify
their behaviour towards the person in a corresponding way.
This team leader wanted her team to recognize her change of
role.
In the first kw months of the change, there was anadditional uncertainty about tfie new relationship betweenthe team leaders and the sister. The least confident teamleader, Anna, was afraid of offending the sister by over-stepping the mark, but she was not sure where the markwas.S.N. I just sort of drifted along for a while, trying to suss
out in my mind exactly what my role was, and then,again, I felt awkward because Sister was still calledSister and she was at the top and how much can you —are you meant to organize your own little team,without treading on her toes, or is she expecting you toget on with it and she is just going to supervise?
Team leader role ambiguity and unclear role boundaries led to
an uncertain relationship between the leaders and the sister.
Although authority for leading the teams had been devolved
from the sister to the team leaders, the extent of the authority
and power to act had not been made explicit. Manthey (1980)
stated that when individuals have been allocated, and have
accepted, responsibility, they must be authorized to act within
the sphere of their responsibility. Lack of congruence between
authority and responsibility will lead to poorly understood
decision-making lines. One team leader wanted to clarify the
decision-making lines between herself and the sister, but she
saw the potential for conflict. She wanted to avoid this cottfltct
but was not sure how to negotiate her new role boundaries.
The nurses felt that the new roles should have beenclarified at the outset of the development. They saw it asthe responsibility of the sister and senior sister to stateclearly what the new roles were and a.s the responsibility ofthe nurses to explore these roles at their teatn meetings.The nurses said that neither of these things happened.

Changing power relationships between nurses 227
At this time, the senior sister was not entirely clearabout the new nursing roles. However, she did not explainto the nurses that there was no blueprint for these newroles, either from the literature or from her previousexperience. Neither did she make explicit that the researchwas about describing the new roles, based on the nurses'experience.
Bant on (1965) suggested that 'clusters of rights and
ohligations constittite roles'. Fvery social relationship consists
of a patr of roles, for example, teatn leader and team meniher.
Within the relationship, obligations are reciprocal, i.e. one
individual's obligation is herlhis partner's right, and vice
versa. I suggest that the senior sister should have made her
position clear hy artictilating her own lack of clarity ahout
ohligations and rights of the netp roles and reciprocal relation-
ships and that one of the expected otitcomes of the action
research was their clarification.
The role of the sister
The stafl" nurses were aware that the sister's role hadchanged considerably with the introduction of team nurs-ing and they admired their sister, Lorraine, for beingwilling to make the changes:S.N. She's gone miles and I admire that and for accepting a
loss of power and authority,S.N. Lorraine had the most changes to go through from her
own little notch at the top, and I quite admire her forgoing through all that change and sort of letting go ofher authority.
They felt that these were difficult changes for her to make.Mary, a team leader, witnessed 'her problems of coming toterms with her new role'.S.N. She loses her keys—the keys with the power and she's
found it very difficult to slot in.Mary, who had establisbed a collegiate relationship withthe sister, saw her working hard to trust the nurses'competency.S.N. You have to trust your colleagues and a favourite
saying of hers is 'but they are trained nurses', alwaysreassuring herself, 'but they are trained nurses andsenior nurses' and she's been reminding herself eachtime.
Nevertheless, the nurses sensed that Lorraine did notreally know how to develop her new role:S.N. She doesn't know where she is going, I don't think. . . .
She actually enjoys the role of team leader and that's abit of a problem for her.
The staff nurses were recognizing their new rights oj
devolved power and authority. The sister was perceived hy the
team leaders to be promoting a power shift in her relationship
with them, therefore fulfilling her obligations. She was seen to
be trying to get used to a collegiate relationship with the staff
nurses, based on trtist, respect and democratic decision making,
thus attempting to meet the obligations of the new role. This
was considered not be easy for her.
Lorraine was aware of the need for her role to changeconsiderably to enable the development of patient-centrednursing on the ward. She admitted to a feeling of confu-sion.S.R. I feel a bit confused really. I know what I ought to be
doing and I know what I would like to be doing, and Ithink the changes are for the better. I think it isrecognized that the sister's role is the most difficultone, having been in control of 20 patients and knowingexactly what was going on. . . . Relinquishing a certainamount of responsibility. . . . I should be here for thenurses, rather than for the patients.
Lorraine talked openly about her uncertainty in her newrelationship with the team leaders.t IELDNOTE 6/9/89. Team leaders meeting. Lorraine said
that she was uncertain—she didn't know how much toleave the team leaders to their 'own devices and howmuch to interfere'. She asked them, 'what do you wantfrom me?'
The sister's question, 'What do you want frotn me?' was
evidence of the shift towards detnocratic decision making.
The sister was aware of her new ohligations. She recognized
the need to devolve authority for patient care to the nurses and
to enahle the staff ntirses to take on their new respottsibilities.
However, she did not appear to have a clear .strategy for
overcotning the constraints tphich prevented her from fully
tneeting these netv obligatioits.
Sister letting golnurses pushing out the boundaries
Initially, authority was devolved from the sister to the staffnurses in several interconnecting ways. The nurses startedto push otit at the botindaries of their responsibility. Lorraine
began to let go of her atithority, either in response to the
ntirses' pushing or as a deliberate strategy. The nurses' stories
of 'the plastic drawsheet' and 'the handover' illustrate this
intercomtectedness.
'The Plastic Drawsheet'
In the old system, Lorraine would 'never tolerate plasticdrawsheets'.N.A. God forbid anyone who brought one on. They were
immediately turfed off.Mary described how, early in the development, 'with

228 A. Titchen and A. Binnic
discussions in the right atmosphere (at a ward meeting),the plastic drawsheet came in'.S.N. They wetit round and round the garden before they
decided to confront Lorraine. There was no problem inthe end, because she said that she didn't like them, butit was up to the team leaders to decide for their team.And that was sensible, you know. . . . They are usedvery sensibly on the ward now and she's happy withthat.
This story illustrates how the sister was beginning to make
space for the team leaders lo make clinical decisions and to
trust their clinical judgements.
' The Handover'
In the early days of team nursing when Lorraine wasacting as co-ordinator, she handed over to the next shift.Anna perceived the inconsistency of this action (whichwould have been carried out in the old system by the nurse'in charge') with the new way of working.S.N. I think it wasn't really sort of malicious, but Sister still
wanted to hand over at the end of the shift and I said,'Well, (laughs) why don't we hand over our ownteams, you know, we've been looking after them? Firstof all, it was fbr quickness, 'I'll just hand them overtype of thing'. But you feel that if you have got yourown little team to look after, then how on earth doesanyone else know what you have been doing on thatshift?
Lorraine remembered the same incident:S.R. We tried the co-ordinator just handing over in the
office . . . and the nurses staying out on the ward, butthen we decided, well I was on holiday, they decidedthat the nurse would handover her own patients.
Lorraine accepted the change the nurses had made andthen tried to help them become 'more business-like' andsuccinct in their reporting.
'The stories show the shifting locus of control—how the
sister began to devolve her authority in response to the nurses
pushing for change, by allowing them to make nursing care or
organizational decisions. She was nudged, gently, by the
nurses who had identified inconsistency between old routines
and the new philosophy and who were no longer afraid to
suggest new ideas because it was legitimate for them to do so.
The new philosophy and structure had been agreed by
consensus, but, to make them work, the nurses still had lo take
the initiative to challenge the status cjuo.
If a power holder is reluctant lo devolve power, and is
challenged by subordinates, that person can retain it by
isolating. Ignoring, ridiculing and maktng those challenging
feel guilty and unworthy (Robinson, 1991). The second story
shows how the sister did not use a/iy of these behaviours, when
a decision was made in her absence. She, thus, demonstrated
her acceptance of a changing power relationship and commit-
ment to the development.
Conclusion
Evidence of the 'in charge' role and centtalized decision-making suggests that a traditional, bureaucratic hierarchywas in place on the study ward before the change to teamnursing. The person 'in charge', usually the sister, was thefocus for communication with other disciplines and was,therefore, the gatekeeper to information. Exclusive accessto information placed her in a powerful position anddisempowered the nurses as practitioners. Although thestaff nurses had been socialized to accept this hierarchyand their place within it, they recognized the inappropri-ateness of centralized decision making wheti dealing withhuman beings. They demonstrated a traditional fear of thesister's autocratic role by not challenging it, whilst grum-bling about not having personal tespotisibility for makingdecisions about patient care. Their dissatisfaction suggeststhat they were experiencing role deprivation.
A 'top-down' strategy for initiating team nursing wasadopted by the senior sister because the nurses were notyet ready for a 'bottom-up' approach, that is, to putforward a proposal thetnselves. The evidence presentedhere supports this view and also shows how a ward clitnatebegan to develop which enabled 'bottom-up' pushing atthe boundaries.
The team leader role was not made sufficiently explicitand authority was not publicly established which led touncertainty and the fear of treading on toes. This evidenceillustrates the importance of specifically defining the extentof authority and of legitimizing a tiew role, so thatexpectations on all sides are clear. The devolution ofauthority from the sister to the staff nurses was a gradualprocess. Some initiative came from the sister, but devolu-tion was increasingly nudged along by the nurses. In time,new, more collegiate relationships were established.
This work highlights the complexity of devolving auth-ority and decision making and facilitating a change in rolesand power relationships when moving frotn ttaditionalnursing to team nursing. The elements of decentralizeddecision making (clear assignment and acceptance of re-sponsibility, authority proportionate to responsibility, andaccountability) were not yet fully established on the studyward, 6 months after the changes began.
Evidence has been presented from which I tentativelygenerated the proposition: if there is an attempt to changethe power relationship between staff nurses and the sister

Changing power relationships between nurses 229
(by moving frotn the cultural nortn of autocratic, centra-lized decision making, to a norm of participative, decentra-lized decision making), nutses ate likely to experience roleambiguity, if authority is not explicitly and publiclydevolved by the sister.
The guiding principle derived from this proposition wasthat when there is an attempt to change the powerrelationship between staff nutses and the sister, as wouldoccur with the development of pritnary nursing, the sistermust, explicitly and publicly, devolve authority to the staffnurses, in order to avoid serious role atnbiguity. In theaction research which followed this case-study, we testedthis priticiple and addressed the issues raised in this paper(Titchen & Binnie, 1992b).
Acknowledgments
We would like to thank warmly all the participants in thisstudy for expressing their views so openly during thefieldwork, and for cotnnienting on this paper which trig-gered metiiories of the first painful steps towards patient-centred nursitig.
References
Banton M. (1965) Roles: an Introduclion to the Study of Social
Relations. Tavistoek Publications f.td, London.Bcchei- T. & Kogan M. (1980) Process and Structure in Higher
Education. Ileinemann, f^oiidon.Benner P. (1984) From Novice to Expert: Excellenee and Power in
Clinieal Nursing Practice. Addison-Wesley Publishing Company,f^ondon.
Binnie A. (1988) 'The working lives of staff nurses: a sociologicalperspective. MA dissertation in Sociological Researeh in HealthCare, Warwick University.
Brown S. & Mclntyre D. (1993) Making SeiLw of Teaching. OpenUniversity Press, Milton Keynes.
Burns T. & Stalker G. (1961) 'The Management of Innovation.Tavistoek Publications, f^ondon.
Fiedler F. (1971) Validation and extension of the contingency modelof leadership effectiveness: A review of empirical findings. Psy-chological Bulletin 76, 128 14S.
Giovannetti P. (1986) F.valuation of primary nursing. In Annual
Review of Nursing Research (Werley 11., Fitzpatrick J. & TauntonR., eds). Springer-Verlag, New York, pp. 127-151.
Goodman P. (1965) People or Personnel: Decentralization and the
Mixed System. Random 1 louse, Toronto.
I Iarre R. & Lamb R. (1986) 'The Dictionary of Personality and SocialPsychology. Basil Blackwell, Oxford, pp. 292-29.1
Hokanson Hawks J. (1991) Power: a concept analysis. Journal ofAdvanced Nursing, 16, 75-1—762.
Kramer M. (1968) Nurse role deprivation -a symptom of neededchange. Social Science and .Medicine 2(4), 461—174.
Lukes S. (1986) Poiver: A Radical View. MacMillan, London.MaeGuire J. (1961) From Student to Nurse. Part I: the Induction
Period. Oxford Area Nurse Training Committee.Macf.eod M. (1990) Experience in everyday nursing practice: a study
oj'experienced' ward sisters. PhD thesis. University of Edinburgh,Edinburgh.
McMahon R. (1990) Power and eollegial relations among nurses onwards adopting primary nursing and hierarchical ward manage-ment structures. Journal of .-Idvanced Nursing 15, 232-239.
McMahon R. (1991) Power and communication issues in primarynursing. In Primary Nursing in Perspective (Ersscr S. & TuttonE., eds). Scutari Press, Harrow, pp. 217-226.
Manthey M. (1980) A theoretical framework for primary nursing.Journal of Nursing .Administration June, 11-15.
Omery A. (1983) Phenomenology: a method for nursing researeh.Advances in Nursing Science January, 49-63.
Ottaway R.N. (1976) A change strategy to implement new norms,new styles and new environment in the work organisation.Personnel.Review 5(1), 13-18.
Pembrey S. (1980) 'The Ward Sister—Key to Nursing. Royal Collegeof Nursing, London.
Rabinow P. & Sullivan M. (1979) Interpretive Social Science.University of California Press, Berkeley.
Revans R. (1964) Standards for .Morale, Cause and Effect in Hos-pitals. NufReld Provincial Hospitals Trust. Oxford UniversityPress, Oxford.
Robinson J. (1991) Power, politics and policy analysis in nursing. InNursing; a Knowledge Base for Practice (Perry A. & Jolley M,eds). Edward Arnold, London, pp. 271-307.
Schein E. (1980) Organizational P.<:yehology. Prentice Hall, Engle-wood Cliffs, New Jersey.
Schutz A. (1962) Collected Papers Vols 1-3. Kluwcr AcademicPress, Dordrecht, The Netherlands.
Titcben A. & Binnie A. (1992a) Patient-Centred Nursing in Prac-tice: .4 Case Study of the Initial Changes Towards PrimaryNursing. Institute of Nursing, Oxford.
Titchen A. & Binnie A. (1992b) If'hat the Hell am I Suppo.<ed to beDoing?: Putting Practice into 'Theory and Back .Again. Institute otNursing, Oxford.
Titchen A. & Mclntyre D. (1992) A Phenomenological .-Ipproach toQiialitative Data .Analysis in Nursing Research. Institute of Nurs-ing, Oxford.
Weber M. (1947) The Theory oj Social and Economic Organization.Free Press of Glencoe, New York.