Changes to Oncology Coding 2008- 2009 Bobbi Buell Version 5.0 December 2008.
59
Changes to Oncology Coding 2008- 2009 Bobbi Buell Version 5.0 December 2008
-
Upload
myron-wood -
Category
Documents
-
view
216 -
download
0
Transcript of Changes to Oncology Coding 2008- 2009 Bobbi Buell Version 5.0 December 2008.

Changes to Oncology Coding 2008- 2009
Bobbi Buell
Version 5.0
December 2008

Disclaimer
Payers differ on their guidelines. Please verify coding for each payer and claim.
This is not legal or payment advice. This content is abbreviated for Medical Oncology. It does not
substitute for a thorough review of code books, regulations, and Carrier guidance.
This information is good for the date of the information and may contain typographical errors.
CPT is the trademark for the American Medical Association. All Rights Reserved.

Session Objectives
Discuss ICD-9-CM Changes for 2009 Discuss CPT Changes for 2009 Discuss HCPCS Coding for 2009 Discuss ESA Coding Now Discuss Coding for PQRI 2009 Discuss Coding for E-Prescribing 2009 Review some E/M Changes for 2008 Review Consult Coding Discuss What You Need to Do Next

General References
Physician Payment Rule = http://www.cms.hhs.gov/PhysicianFeeSched/PFSFRN/list.asp#TopOfPage
Hospital Outpatient Rule = http://www.cms.hhs.gov/HospitalOutpatientPPS/HORD/list.asp#TopOfPage
ICD-9-CM Codes = http://www.cms.hhs.gov/ICD9ProviderDiagnosticCodes/07_summarytables.asp#TopOfPage

Coding Issues

Cancer ICD-9-CM Codes 10/1/08 199.2 Malignant neoplasm associated with transplant organ 203.02 Multiple myeloma, in relapse 203.12 Plasma cell leukemia, in relapse 203.82 Other immunoproliferative neoplasms, in relapse 204.02 Acute lymphoid leukemia, in relapse 204.12 Chronic lymphoid leukemia, in relapse 204.22 Subacute lymphoid leukemia, in relapse 204.82 Other lymphoid leukemia, in relapse 204.92 Unspecified lymphoid leukemia, in relapse 205.02 Acute myeloid leukemia, in relapse 205.12 Chronic myeloid leukemia, in relapse 205.22 Subacute myeloid leukemia, in relapse 205.32 Myeloid sarcoma, in relapse 205.82 Other myeloid leukemia, in relapse 205.92 Unspecified myeloid leukemia, in relapse 206.02 Acute monocytic leukemia, in relapse 206.12 Chronic monocytic leukemia, in relapse 206.22 Subacute monocytic leukemia, in relapse 206.82 Other monocytic leukemia, in relapse 206.92 Unspecified monocytic leukemia

Cancer ICD-9-CM Codes 10/1/08 207.02 Acute erythremia and erythroleukemia, in relapse 207.12 Chronic erythremia, in relapse 207.22 Megakaryocytic leukemia, in relapse 207.82 Other specified leukemia, in relapse 208.02 Acute leukemia of unspecified cell type, in relapse 208.12 Chronic leukemia of unspecified cell type, in relapse 208.22 Subacute leukemia of unspecified cell type, in relapse 208.82 Other leukemia of unspecified cell type, in relapse
208.92 Unspecified leukemia, in relapse

Cancer ICD-9-CM Codes 10/1/2008 209.00 Malignant carcinoid tumor of the small intestine, unspecified portion 209.01 Malignant carcinoid tumor of the duodenum 209.02 Malignant carcinoid tumor of the jejunum 209.03 Malignant carcinoid tumor of the ileum 209.10 Malignant carcinoid tumor of the large intestine, unspecified portion 209.11 Malignant carcinoid tumor of the appendix 209.12 Malignant carcinoid tumor of the cecum 209.13 Malignant carcinoid tumor of the ascending colon 209.14 Malignant carcinoid tumor of the transverse colon 209.15 Malignant carcinoid tumor of the descending colon 209.16 Malignant carcinoid tumor of the sigmoid colon 209.17 Malignant carcinoid tumor of the rectum 209.20 Malignant carcinoid tumor of unknown primary site 209.21 Malignant carcinoid tumor of the bronchus and lung 209.22 Malignant carcinoid tumor of the thymus 209.23 Malignant carcinoid tumor of the stomach 209.24 Malignant carcinoid tumor of the kidney 209.25 Malignant carcinoid tumor of foregut, not otherwise specified 209.26 Malignant carcinoid tumor of midgut, not otherwise specified 209.27 Malignant carcinoid tumor of hindgut, not otherwise specified 209.29 Malignant carcinoid tumor of other sites
New Cancer ICD-9 Codes 10/1/2008 209.30 Malignant poorly differentiated neuroendocrine carcinoma, any site 238.77 Post-transplant lymphoproliferative disorder (PTLD) 289.84 Heparin-induced thrombocytopenia (HIT) 999.81 Extravasation of vesicant chemotherapy 999.82 Extravasation of other vesicant agent 999.88 Other infusion reaction 999.89 Other transfusion reaction V07.51 Prophylactic use of selective estrogen receptor modulators (SERMs) V07.52 Prophylactic use of aromatase inhibitors V07.59 Prophylactic use of other agents affecting estrogen receptors and estrogen levels V13.51 Personal history of pathologic fracture V87.41 Personal history of antineoplastic chemotherapy V87.42 Personal history of monoclonal drug therapy V87.49 Personal history of other drug therapy

Other ICD-9-CM Changes
Secondary Diabetes Mellitus (249.xx) New types of headaches (339.xx) A gaggle of new PAP and anal smear codes
(795.xx-796.xx) V87.xx for exposure to toxic (and potentially
carcinogenic) substances

Funniest 2009 ICD-9-CM Codes
339.43 Primary Thunderclap Headache 339.82 Headache Associated With Sexual Activity 339.85 Primary Stabbing Headache 372.74 Pingueculitis 611.81 Ptosis of Breast

Changed Codes of Note 203.00 Multiple myeloma, without mention of having achieved remission 203.10 Plasma cell leukemia, without mention of having achieved remission 203.80 Other immunoproliferative neoplasms, without mention of having achieved remission 204.00 Acute lymphoid leukemia, without mention of having achieved remission 204.10 Chronic lymphoid leukemia, without mention of having achieved remission 204.20 Subacute lymphoid leukemia, without mention of having achieved remission 204.80 Other lymphoid leukemia, without mention of having achieved remission 204.90 Unspecified lymphoid leukemia, without mention of having achieved remission 205.00 Acute myeloid leukemia, without mention of having achieved remission 205.10 Chronic myeloid leukemia, without mention of having achieved remission 205.20 Subacute myeloid leukemia, without mention of having achieved remission 205.30 Myeloid sarcoma, without mention of having achieved remission 205.80 Other myeloid leukemia, without mention of having achieved remission 205.90 Unspecified myeloid leukemia, without mention of having achieved remission

Changed Codes of Note (2009) 206.00 Acute monocytic leukemia, without mention of having achieved remission 206.10 Chronic monocytic leukemia, without mention of having achieved remission 206.20 Subacute monocytic leukemia, without mention of having achieved remission 206.80 Other monocytic leukemia, without mention of having achieved remission 206.90 Unspecified monocytic leukemia, without mention of having achieved remission 207.00 Acute erythremia and erythroleukemia, without mention of having achieved remission
207.10 Chronic erythremia, without mention of having achieved remission 207.20 Megakaryocytic leukemia, without mention of having achieved remission 207.80 Other specified leukemia, without mention of having achieved remission 207.20 Megakaryocytic leukemia, without mention of having achieved remission 207.80 Other specified leukemia, without mention of having achieved remission \ 208.00 Acute leukemia of unspecified cell type, without mention of having achieved remission 208.10 Chronic leukemia of unspecified cell type, without mention of having achieved remission 208.20 Subacute leukemia of unspecified cell type, without mention of having achieved remission 208.80 Other leukemia of unspecified cell type, without mention of having achieved remission 208.90 Unspecified leukemia, without mention of having achieved remission
V45.71 Acquired absence of breast and nipple

CPT Changes 2009
CPT decided to ‘go green this year and changed the numbering for the Hydration and Therapeutic codes so they are in the same section as the Chemo codes. All Hydration and Therapeutic codes will be “963”
codes instead of “907” codes. 90761 = 96361 90767 = 96367 90772 = 96372 ETC.
Source: CPT 2009 Crosswalk available at http://www.asco.org

CPT Changes 2009
The Chemotherapy Section name has changed to “Chemotherapy or Highly Complex Drug or Highly Complex Biologic Agent” Administration The word “highly complex” used with frequency Will payers change admin codes on some drugs? CMS leaves this up to the MACs and Carriers. Other payers may be more strict with drug
administration, but let’s wait and see what the AMA says.
Descriptor Source: CPT 2009

HCPCS Changes 2009 (1/1/2009)
New Codes:
J0641 INJECTION, LEVOLEUCOVORIN CALCIUM, 0.5 MGJ1267 INJECTION, DORIPENEM, 10 MGJ1453 INJECTION, FOSAPREPITANT, 1 MGJ1459 INJECTION, IMMUNE GLOBULIN (PRIVIGEN), INTRAVENOUS, NON-LYOPHILIZED (E.G.

HCPCS Changes
New Codes
J8705 TOPOTECAN, ORAL, 0.25 MG
J9033 INJECTION, BENDAMUSTINE HCL, 1 MG
J9207 INJECTION, IXABEPILONE, 1 MG
J9330 INJECTION, TEMSIROLIMUS, 1 MG

HCPCS Changes
Changed Descriptors
J1572 INJECTION, IMMUNE GLOBULIN, (FLEBOGAMMA/FLEBOGAMMA DIF), INTRAVENOUS,
J2788 INJECTION, RHO D IMMUNE GLOBULIN, HUMAN, MINIDOSE, 50 MICROGRAMS (250 I.U.)
J2790 INJECTION, RHO D IMMUNE GLOBULIN, HUMAN, FULL DOSE, 300 MICROGRAMS (1500 I.U.)
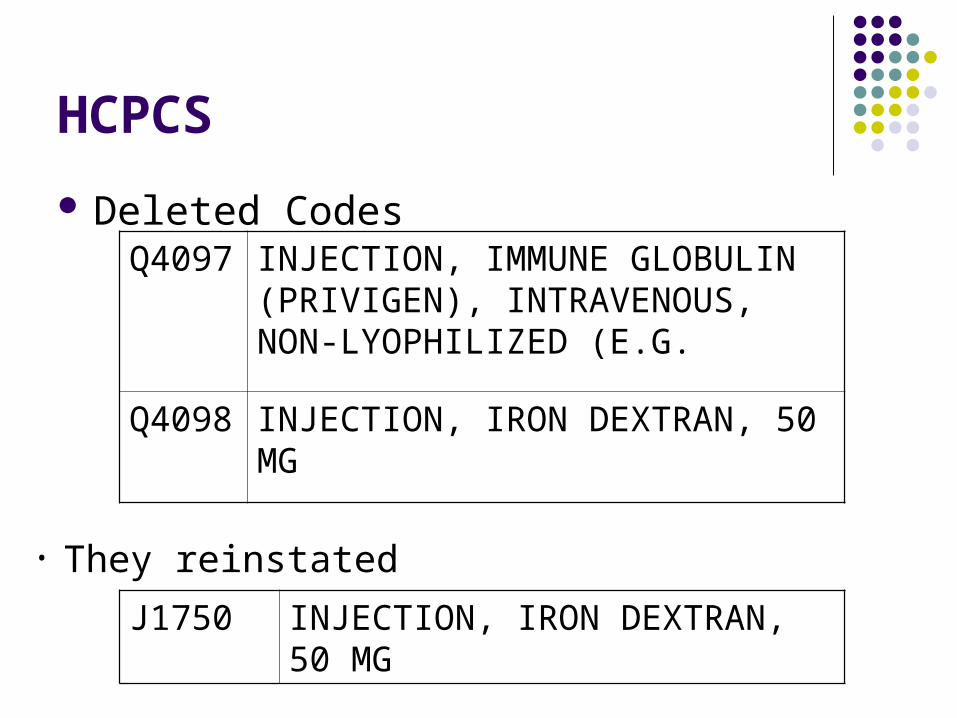
HCPCS
Deleted CodesQ4097 INJECTION, IMMUNE GLOBULIN
(PRIVIGEN), INTRAVENOUS, NON-LYOPHILIZED (E.G.
Q4098 INJECTION, IRON DEXTRAN, 50 MG
J1750 INJECTION, IRON DEXTRAN, 50 MG
• They reinstated

MIPPA Legislation - PQRI
The Medicare Improvements for Patients and Providers Act (MIPPA), passed in July 2008, contained several new authorities and requirements for quality reporting and PQRI for 2009 and beyond.
Section 131 directly impacts PQRI Section 132 contains the new electronic
prescribing incentive provisions.

MIPPA Legislation – PQRI, Section 131
PQRI 2009 incentive provided and raised to 2% Eligible professionals shall be paid 2% incentive of
estimated allowable charges submitted not later than 2 months after the end of the reporting period for 2009 quality measures.
Adds qualified audiologists in the definition of eligible professionals.
No effect on 2007 or 2008 incentive payments.

Registries CMS received over 55 self-nomination requests for
registries to become “qualified” to submit quality data for possible incentive payment on behalf of their clients.
32 registries have been selected for “production” (eligible to earn a payment incentive for their providers)
The final list of “qualified” registries is posted on the PQRI website at: http://www.cms.hhs.gov/PQRI/20_Reporting.asp#TopOfPage and go to the first download (“2008 List of Qualified Registries”)

Registries
Becoming a “qualified” registry is not a guarantee by CMS that the registry will be successful submitting data on behalf of their clients.
These registries, however, have gone through a complete evaluation of their measure calculations and a test that their system can successfully communicate with our data warehouse.

6 Registry-Based Options
Reporting Period: Reporting Period:January 1, 2008 - July 1, 2008 – December 31, 2008 December 31, 2008
Individual Measures: Individual Measures:80% of applicable cases 80% of applicable casesMinimum 3 measures Minimum 3 measures
One Measures Group: One Measures Group:30 consecutive patients 15 consecutive patients OR OR80% of applicable cases 80% of applicable cases
Do You Want to Use a Registry?
Must be a registered registry with CMS and approved for submission.
Must successfully report in 2008. This can be a mystery right now. Not really known until after 3/31/2009.
May charge you, so is it cheaper than doing it claim by claim?

Hematology-Oncology Measures 2009 MDS And Acute Leukemias Cytogenetic Testing MDS Documentation of Iron Stores Multiple Myeloma: Treatment With Bisphosphonates CLL Baseline Flow Cytometry Hormonal Therapy for Stage IC-III ER/PR + Breast Cancer Chemotherapy for Stage III Colon Cancer Patients Breast Cancer Patients Who Have pT and pN category and histological grade for their cancer Colorectal Cancer Patients Who Have pT and pN category and histological grade for their cancer Inappropriate use of bone scan for staging low risk cancer patients Adjuvant hormonal therapy for high-risk prostate cancer patients Three-dimensional radiotherapy for patients with prostate cancer. Melanoma: Follow Up Aspects of Care (2009) Melanoma: Continuity of Care (2009) Melanoma: Coordination of Care (2009) Oncology Med/Rad: Plan of Care for Pain (2009) Oncology Med/Rad: Pain Quantified (2009) Oncology: Radiation Dose Limits to Normal Tissues (2009) Oncology Recording of Clinical Stage for Lung and Esophageal Cancer (2009) Notice #73 and #74 are gone

PQRI Coding 2008 (until 12/31/08) Coding Example--Measure #71 Hormonal Therapy for Stage IC-III. ER/PR + Breast CA
Report once per reporting period for all females 18 and over having breast cancer seen during the reporting period.
Numerator Coding for patients receiving tamoxifen and AIs and have Stage 1C-III, ER/PR+; coding now depends upon the submission of three numerator codes in some cases. Tamoxifen/AI Prescribed (Three CPT II Codes [4179F & 33xxF & 3315F] are required to
report) Tamoxifen/ AI Not Prescribed for Medical, Patient, or System Reasons (Three CPT II
Codes [4179F-1-3P & 33xxF & 3315F ] Tamoxifen/ AI Not Prescribed due to Stage or ER/PR Negative [3302F OR 3303F OR
3312F or 3316F] Tamoxifen/ AI Not Prescribed; Reason Not Specified (Three CPT II Codes [4179F-8P &
33xxF & 3315F] are required to report) No documentation of cancer stage or ER/PR status [3305F-8P or 3316F-8P ONLY]
Denominator Coding Patient is 18 years old or older Breast Cancer Dx Codes (174.0-174.6, 174.8, 174.9) E/M codes (99201-99205, 99212-99215)

PQRI Coding 2008 Huh? What?????
Level II CPT Codes CPT II 4179F = Tamoxifen or AI
prescribed CPT II 33xx = AJCC Cancer Stage I C-
Stage IV C CPT II 3305-8P = No stage documented CPT II 3315 F = ER+ or PR+ breast
cancer CPT II 3316F = ER/PR negative breast
cancer Modifiers
-1P = Not qualified for medical reasons -2P = Not qualified for patient reasons -3P = Not qualified for system reasons -8P = Reasons not otherwise specified
PQRI Errors
Errors from 2007 1,711,975 (12.15%) of QDC submission attempts had a
missing NPI. 2,662,023 (18.89%) of QDC submission attempts occurred
with an incorrect HCPCS code. 1,963,196 (13.93%) of QDC submission attempts occurred
with an incorrect Dx code. 1,019,422 (7.24%) of QDC submissions had an incorrect
HCPCS and Dx code. 700,201 (4.97%) had only the QDC code and no other line
items were billed.
“Physician Quality Reporting Initiative 2007 Reporting Experience” available at http://www.cms.hhs.gov/pqri/

Oncology-Specific Errors
Measure % OK HCPCS Wrong
Dx Wrong QDC Only NPI Problem
#71 Breast Cancer with drug tx
83.70% 5.61% 4.04% 5.87% 13.38%
#73 Plan of Chemotherapy
25.16% 52.70% 12.40% 8.00% 5.68%
#72 Stage III Colon Cancer
56.25% 7.38% 12.00% 4.68% 9.31%
“Physician Quality Reporting Initiative 2007 Reporting Experience” available at http://www.cms.hhs.gov/pqri/

Hem-Onc Specific ErrorsMeasure % OK HCPCS
WrongDx Wrong QDC Only NPI
Problem
#70 Baseline Flow in CLL
77.31% 7.13% 10.35% 3.28% 12.50%
#67 MDS Baseline Cytogenetic Testing
66.63% 9.05% 9.47% 3.67% 10.31%
#69 Multiple Myeloma Tx With Biphosphonates
73.02% 12.21% 8.28% 4.46% 12.40%
#74 RT Recommended Breast Ca
15.45% 58.15% 1.03% 7.47% 7.31%
“Physician Quality Reporting Initiative 2007 Reporting Experience” available at http://www.cms.hhs.gov/pqri/

MIPPA Legislation – Successful Electronic Prescriber, Section 132
The MIPPA provides for a 2% incentive payment to eligible professionals who successfully prescribe (as defined by the statute) their patient’s medications electronically beginning in 2009.
The legislation specifically refers to the electronic prescribing measure currently in 2008 PQRI (measure #125).
E-Prescribing measure will be removed from PQRI for 2009 and added to the E-Prescribing incentive program as a stand-alone benefit.
The Secretary has the authority to update the specifications of the electronic prescribing measure in the future.
2008 PQRI – E-Prescribing Measure
Electronic Prescribing Structural Measure (measure #125) qualifies as one of three required measures in PQRI to earn an incentive payment.
Requirement for 2008 PQRI is to report the measure on 80% or more of eligible patients BUT this goes to 50% in 2009.
No separate incentive for successful E-Prescribing in 2008 PQRI
Electronic Prescribing Measure in 2008 PQRI
Currently eligible professionals (EPs) can report that they electronically prescribe (eRx) medications using a qualified program as defined in PQRI measure #125 Adoption/Use of e-Prescribing by reporting one of the G-codes in the measure
You must have and regularly use an electronic prescribing program to report the measure
The electronic prescribing program must meet ALL of the requirements listed in PQRI measure #125
If you have not adopted an electronic prescribing system that meets the specifications of the measure you cannot report on this measure.

Free E-Prescribing in Oncology!
That’s right! Just for cancer
practices! www.oncologyerx.com For more information,
contact me!

Qualified Electronic Prescribing Systems – 2009 The measure assesses eligible professional’s use of
electronic prescribing using a qualified system. As a qualified system, the program must be able to
perform the following tasks: Communicate with the patient’s pharmacy; Help the physician identify appropriate drugs and
provide information on lower cost alternatives for the patient;
Provide information on formulary and tiered formulary medications; and
Generate alerts about possible adverse events, such as improper dosing, drug-to-drug interactions, or allergy concerns.
Successful Reporting of the eRx Measure for 2009
The measure is intended to be reported on for EVERY patient visit in the denominator.
Successful reporting is defined as reporting the measure on at least 50% of eligible patients or an amount of electronic submission of claims under Part D. Limitation: CPT codes that make up the denominator
MUST account for at least 10% of the provider’s total allowed charges for Medicare Part B covered services OR a parameter of claims NOT submitted to Part D (not in 2009).
Reporting of E-Rx in 2009
To get paid the incentive, you must have an e-prescribing system, report a visit and choose a code (not out yet) to state that the patient:
They did not prescribe any medications during the visit; They used e-prescribing for any medications prescribed
during the visit; or They did not use e-prescribing for a prescription because
the law prohibits electronic prescribing for the specific type of drug, such as a controlled substance.

Coding for E-Prescribing 2009
You must use a QUALIFIED E-prescribing system AND Have an encounter with one of these codes
90801, 90802, 90803, 90804, 90805, 90806, 90807, 90808, 90809, 92002, 92004, 92012, 92014, 96150, 96151, 96152, 99201, 99202, 99203, 99204, 99205, 99211, 99212, 99213, 99214, 99215, 99241, 99242, 99243, 99244, 99245, G101, G0108, G0109.
Notice some from original guidelines were removed.

Coding for E-prescribing 2008-2009
Report on all eligible patients: G8443--All prescriptions created during the encounter were
generated using an e-prescribing system. G8445--No prescriptions were generated during the encounter.
Provider does have access to a qualified e-prescribing system. G8446--Provider does have access to a qualified e-prescribing
system. Some or all prescriptions generated were printed or phoned in as required by state regulation, patient request, or pharmacy being able to receive electronic transmission.
Future Penalties for Not Electronically Prescribing
Eligible professionals who are not successfully using electronic prescribing by 2012 will be penalized 1% of their covered Medicare Part B charges. This means that these providers will be paid at 99% for their
covered Medicare Part B fee schedule services. Limitation applies as for incentives Fee reduction is prospective, providers will have to
electronically prescribe by a date to be determined to be sure their fees are not reduced in 2012.
This date will not be before 2010. Hardship exemption on a case-by-case basis for small
practices.

Future Penalties for Not Electronically Prescribing
In 2013 - 1.5% deducted from their covered Medicare Part B services. Professionals will be paid at 98.5% of the
physician fee schedule for covered services. In 2014 and beyond penalty will increase to
2%. Professionals will receive 98% of the physician
fee schedule for the covered services they provide.

Part D Information
The Secretary has the authority to change the requirements for successful E-Prescribing in the future.
The MIPPA legislation allows for future use of Part D data in lieu of claims-based reporting by eligible professionals.
Should You Go For It?
Let’s say you are a singlesingle Medical Oncologist AND you want to know whether or not to go for the incentive for your NPI Your E/M revenue is $325,000 Your drug administration revenue, plus other
procedures is $275,000 Your Medicare % is 50% Your PQRI plus E-Rx bonus would be $12,000.
Info Sources for ESAs… View the policy itself at
http://www.cms.hhs.gov/mcd/viewdecisionmemo.asp?id=203 View CMS FAQs
http://www.cms.hhs.gov/mcd/ncpc_view_document.asp?id=12 View ASCO FAQs
http://www.ascofoundation.org/portal/site/ASCO/menuitem.5d1b4bae73a9104ce277e89a320041a0/?vgnextoid=24be6e7507523110VgnVCM100000ed730ad1RCRD
View CMS Transmittals R1412, R1413, R80NCD at http://www.cms.hhs.gov/Transmittals/2008Trans/list.asp
View American Society of Hematology Guidelines (ASH) at http://www.hematology.org/policy/practice/01242008.cfm

ESA/Anemia Billing Summary If the patient has cancer and is on chemotherapy, submit the “most
recent” hemoglobin must be <10 (or Hct < 30%). Bill the H or H results and use -EA. Follow Carrier guidelines for diagnosis coding.
If the patient is on Radiotherapy, submit the latest H or H result, use -EB, and get denied.
If the patient does not have chemotherapy-induced anemia (or ESRD), submit the latest H or H, use -EC, and follow your Carrier’s guidelines for coding and billing.
If the patient has cancer and is on an anemia drug which is not self-administered, submit the latest H or H result. All other guidelines are at Carrier discretion.

Medicare: Hospital Discharge Day
Transmittal #1460, CR #5794, effective 4/1/2008 A Hospital Discharge Day service (99238-99239) is a face-to-
face service between the attending physician and the patient. Only the attending physician of record shall report 99238-99239.
Other providers shall report subsequent hospital services (99231-99233), if they perform concurrent services.
Reporting of the service is on the calendar day of the visit, even if it differs from the discharge date.
Report only one discharge service (99238-99239) per patient per stay. Do NOT report discharge services and subsequent services the same date.
Discharge services may be billed for pronouncement of death on the date of death.

Medicare: Inpatient/ Observation
Transmittal #1466, CR 5791 Initial Hospital Observation Services (CPT codes 99218-99220) and Observation Care Discharge
Services (99217) When the observation care is less than 8 hours on the same calendar date report
an Initial Observation Care code. Do not report an Observation Care Discharge Service.
When the patient is admitted for observation care and discharged on a different calendar date report an Initial Observation Care and an Observation Care Discharge.
In those rare instances when a patient is held in observation care status for more than two calendar dates report an Office or Other Outpatient Visit (CPT 99211-99215) for a visit before the discharge date.
The medical record must include documentation that: Satisfies E/M guidelines for admission to and discharge from observation care to inpatient
hospital care. Identifies the billing physician/NPP was present and personally performed the services Indicates the number of hours that the patient remained in the observation care status Identifies the admission and discharge notes were written by the billing physician/NPP

Medicare Inpatient/ Observation Observation or Inpatient Care Services (including Admission and Discharge
Services) (CPT codes 99234-99236) When a patient is admitted to observation or inpatient hospital care for a
minimum of 8 hours but less than 24 hours and discharged on the same calendar date report an Observation or Inpatient Hospital Care Services code (Including Admission and Discharge Services). Do not report an additional discharge service.
The medical record must include documentation that: States the stay for hospital treatment or observation care status
involves 8 hours but less than 24 hours. Identifies the billing physician/NPP was present and personally
performed the services. Identifies the admission and discharge notes were written by the billing
physician/NPP.
Transmittal #1466, CR 5791
Medicare: Prolonged Services On April 14, 2008, CMS issued Transmittal 1490CP, Change Request 5972,
Effective Date is June 2, 2008(meaning that’s when you are responsible for it) with an Implementation Date of July 7, 2008
These services (99354-99355) are payable when billed on the same day (and, on the same claim) as the companion evaluation and management codes. Again, the time for the service refers to the typical/average time units associated with the companion evaluation and management service as noted in the CPT code.
Each additional 30 minutes of direct face-to-face patient contact following the first hour of prolonged services may be reported by CPT code 99355.
Prolonged service of less than 30 minutes total duration on a given date is not separately reported because the work involved is included in the total work of the evaluation and management codes. So, using our 99213 example, you would not report anything of less than 45 minutes, as that time frame is 30 minutes past the average visit time per CPT.

Medicare Prolonged Services Code 99355 or 99357 may be used to report each additional 30 minutes beyond the first hour of prolonged
services, based on the place of service. These codes may be used to report the final 15 – 30 minutes of prolonged service on a given date, if not otherwise billed. Prolonged service of less than 15 minutes beyond the first hour or less than 15 minutes beyond the final 30 minutes is not reported separately.
Companion Codes must be correct in terms of pairing with Prolonged Services or claims for these codes will not be paid… The companion evaluation and management codes for 99354-99355 are the Office or Other Outpatient visit
codes (99201 - 99205, 99212 –99215), the Office or Other Outpatient Consultation codes (99241 – 99245), the Domiciliary, Rest Home, or Custodial Care Services codes (99324 – 99328, 99334 – 99337), the Home Services codes (99341 - 99345, 99347 – 99350); and/or
The companion evaluation and management codes for 99356-99357 are the Initial Hospital Care codes (99221 - 99223, 99231 – 99233), the Inpatient Consultation codes (99251 – 99255); Nursing Facility Services codes (99304 -99318).
There is a requirement for physician (or NPP) presence. Physicians may count only the duration of direct face-to-face contact between the physician and the patient (whether the service was continuous or not) beyond the typical/average time of the visit code billed to determine whether prolonged services can/cannot be billed and to determine the prolonged services codes that are allowable.
Documentation is required in the medical record regarding the duration and content of the medically necessary evaluation and management service and prolonged services billed. According to the Transmittal “the start and end times of the visit shall be documented in the medical record along with the date of service.)”
Counseling/coordination of care can necessitate use of Prolonged Services---but you must use the highest level of the code set involved first, e.g. 99215, 99245.
Medicare will not pay prolonged services codes 99358 and 99359, which do not require any direct patient face-to-face contact (e.g., telephone calls).

Medicare Consultations (Medicare) Transmittal 788, CR #4215, December 2005
No shared visits for consultations in either office or hospital. Either the NPP or MD should charge for the consult. This is black and white in the transmittal.
3 R’s have been more formalized and one has been added… REQUEST from another physician for consultant’s opinion must be
clearly documented in BOTH the receiving and referring physician charts.
Referring MDs must have it in their plan of care, but there is no need for you to check every record.
The REASON for the consult must be clearly documented in the medical record.
Opinion RENDERED by the consultant with RECOMMENDATIONS for treatment.
REPORT goes back to the referring physician. 99211 may not be used for a consult.

Consultations
Consultations (Cont’d) Consultations may be billed based on time for
counseling/coordination of care, but an opinion must be rendered.
Also, if care is continuous before the consult for the same/original problem, an additional consult may not be billed.
Only ONE consultation may be billed per inpatient stay.

Consultations
Transfer of Care A transfer of care occurs when a physician or NPP requests that another physician or
NPP take over the responsibility for managing the patient’s complete care for the condition, and does not expect to continue treating or caring for the patient for that condition.
When this transfer is arranged, the requesting provider is not asking for an opinion or advice to personally treat this patient and is not expecting to continue treating the patient for the condition. The receiving physician or NPP shall document this transfer of the patient’s care in the patient’s medical record or plan of care.
If a transfer of care occurs, report the appropriate new or established patient visit code should be billed based on place of service.
51 Specialty Societies have objected to this language (including the AMA, ASCO, and ASH), but this Transmittal is still in effect and has been the Medicare rule since 1/1/2006.
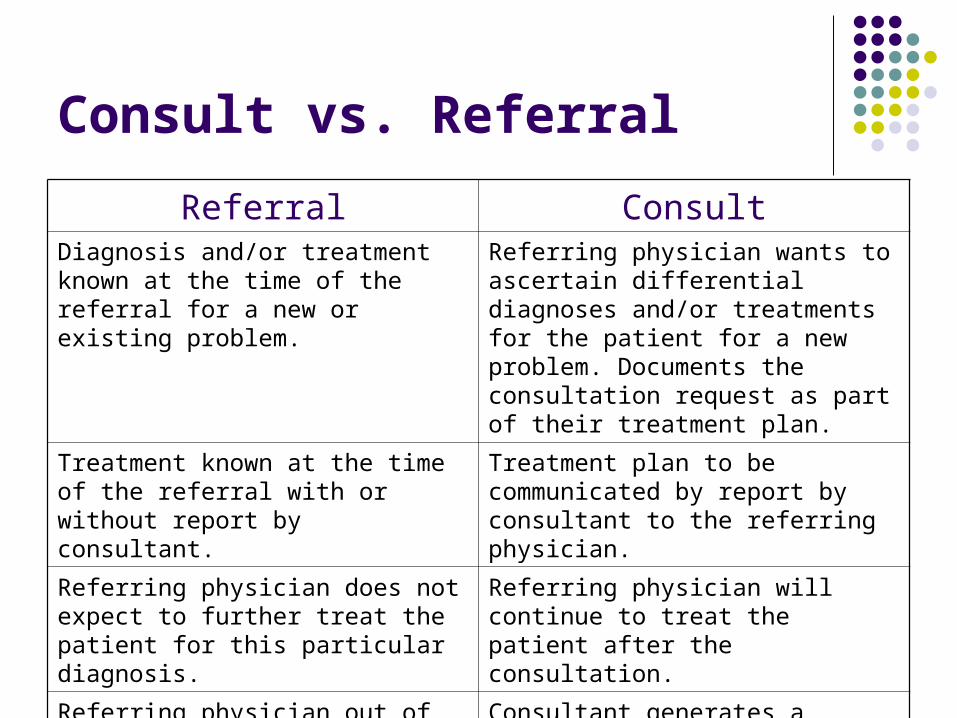
Consult vs. Referral
Referral ConsultDiagnosis and/or treatment known at the time of the referral for a new or existing problem.
Referring physician wants to ascertain differential diagnoses and/or treatments for the patient for a new problem. Documents the consultation request as part of their treatment plan.
Treatment known at the time of the referral with or without report by consultant.
Treatment plan to be communicated by report by consultant to the referring physician.
Referring physician does not expect to further treat the patient for this particular diagnosis.
Referring physician will continue to treat the patient after the consultation.
Referring physician out of the picture. Consultant generates a report with their opinion and plan for treatment and may update the referring physician periodically .

Modifier -JW
Transmittal on Drug Waste--Transmittal 1478, CR 5923 Contractors “may” require Modifier -JW to denote waste on
single-dose vials or packages. Contractors may use it to pay you for appropriate waste
that is unused and discarded. Effective April 17, 2008.

Strategies for Success
Analyze the reasons for rejected, denied, or delayed claims and fix it. If you do not have an EOB analyzer, you are behind the curve.
Really consider doing PQRI and e-prescribing---4% is nothing to sneeze at.
Enforce contracts with private payers. Check out the AMA Report Card, if you think they are being straight with you.
Audit chemo prospectively; peer review E&M. Physicians must review consults before it is too late! Transmittal 788, CR 4215 (2005).
Look at your billing profiles. Give $$ back before the RACs collect it for you!
Participate in the struggle!

Contact Info
Contact [email protected] [email protected] 800-795-2633
Newsletter is free! Education for your staff--check it out at
http://www.eexpertpartners.com/payperview.html

Thank You!