Changes of the Marginal Monkeys - steinerbio.com · 316 Steiner,Pearson,Ainamo Figure2....
7
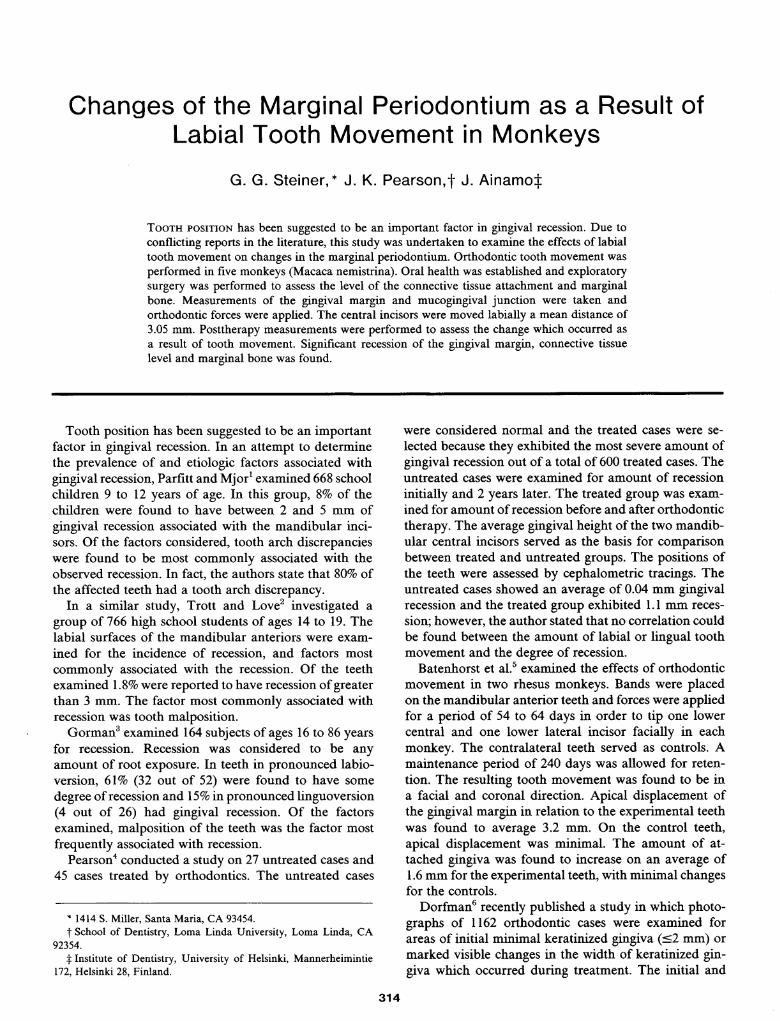
Changes of the Marginal Periodontium as a Result of Labial Tooth Movement in Monkeys G. G. Steiner,* J. K. Pearson,f J. Ainamo^ Tooth position has been suggested to be an important factor in gingival recession. Due to conflicting reports in the literature, this study was undertaken to examine the effects of labial tooth movement on changes in the marginal periodontium. Orthodontic tooth movement was performed in five monkeys (Macaca nemistrina). Oral health was established and exploratory surgery was performed to assess the level of the connective tissue attachment and marginal bone. Measurements of the gingival margin and mucogingival junction were taken and orthodontic forces were applied. The central incisors were moved labially a mean distance of 3.05 mm. Posttherapy measurements were performed to assess the change which occurred as a result of tooth movement. Significant recession of the gingival margin, connective tissue level and marginal bone was found. Tooth position has been suggested to be an important factor in gingival recession. In an attempt to determine the prevalence of and etiologic factors associated with gingival recession, Parfitt and Mjor1 examined 668 school children 9 to 12 years of age. In this group, 8% of the children were found to have between 2 and 5 mm of gingival recession associated with the mandibular inci- sors. Of the factors considered, tooth arch discrepancies were found to be most commonly associated with the observed recession. In fact, the authors state that 80% of the affected teeth had a tooth arch discrepancy. In a similar study, Trott and Love2 investigated a group of 766 high school students of ages 14 to 19. The labial surfaces of the mandibular anteriors were exam- ined for the incidence of recession, and factors most commonly associated with the recession. Of the teeth examined 1.8% were reported to have recession of greater than 3 mm. The factor most commonly associated with recession was tooth malposition. Gorman3 examined 164 subjects of ages 16 to 86 years for recession. Recession was considered to be any amount of root exposure. In teeth in pronounced labio- version, 61% (32 out of 52) were found to have some degree of recession and 15% in pronounced linguoversion (4 out of 26) had gingival recession. Of the factors examined, malposition of the teeth was the factor most frequently associated with recession. Pearson4 conducted a study on 27 untreated cases and 45 cases treated by orthodontics. The untreated cases * 1414 S. Miller, Santa Maria, CA 93454. t School of Dentistry, Loma Linda University, Loma Linda, CA 92354. Institute of Dentistry, University of Helsinki, Mannerheimintie 172, Helsinki 28, Finland. were considered normal and the treated cases were se- lected because they exhibited the most severe amount of gingival recession out of a total of 600 treated cases. The untreated cases were examined for amount of recession initially and 2 years later. The treated group was exam- ined for amount of recession before and after orthodontic therapy. The average gingival height of the two mandib- ular central incisors served as the basis for comparison between treated and untreated groups. The positions of the teeth were assessed by cephalometric tracings. The untreated cases showed an average of 0.04 mm gingival recession and the treated group exhibited 1.1 mm reces- sion; however, the author stated that no correlation could be found between the amount of labial or lingual tooth movement and the degree of recession. Batenhorst et al.5 examined the effects of orthodontic movement in two rhesus monkeys. Bands were placed on the mandibular anterior teeth and forces were applied for a period of 54 to 64 days in order to tip one lower central and one lower lateral incisor facially in each monkey. The contralateral teeth served as controls. A maintenance period of 240 days was allowed for reten- tion. The resulting tooth movement was found to be in a facial and coronal direction. Apical displacement of the gingival margin in relation to the experimental teeth was found to average 3.2 mm. On the control teeth, apical displacement was minimal. The amount of at- tached gingiva was found to increase on an average of 1.6 mm for the experimental teeth, with minimal changes for the controls. Dorfman6 recently published a study in which photo- graphs of 1162 orthodontic cases were examined for areas of initial minimal keratinized gingiva (<2 mm) or marked visible changes in the width of keratinized gin- giva which occurred during treatment. The initial and 314
Transcript of Changes of the Marginal Monkeys - steinerbio.com · 316 Steiner,Pearson,Ainamo Figure2....
Changes of the Marginal Periodontium as a Result ofLabial Tooth Movement in Monkeys
G. G. Steiner,* J. K. Pearson,f J. Ainamo^
Tooth position has been suggested to be an important factor in gingival recession. Due to
conflicting reports in the literature, this study was undertaken to examine the effects of labialtooth movement on changes in the marginal periodontium. Orthodontic tooth movement was
performed in five monkeys (Macaca nemistrina). Oral health was established and exploratorysurgery was performed to assess the level of the connective tissue attachment and marginalbone. Measurements of the gingival margin and mucogingival junction were taken andorthodontic forces were applied. The central incisors were moved labially a mean distance of3.05 mm. Posttherapy measurements were performed to assess the change which occurred as
a result of tooth movement. Significant recession of the gingival margin, connective tissuelevel and marginal bone was found.
Tooth position has been suggested to be an importantfactor in gingival recession. In an attempt to determinethe prevalence of and etiologic factors associated withgingival recession, Parfitt and Mjor1 examined 668 schoolchildren 9 to 12 years of age. In this group, 8% of thechildren were found to have between 2 and 5 mm ofgingival recession associated with the mandibular inci-sors. Of the factors considered, tooth arch discrepancieswere found to be most commonly associated with theobserved recession. In fact, the authors state that 80% ofthe affected teeth had a tooth arch discrepancy.
In a similar study, Trott and Love2 investigated a
group of 766 high school students of ages 14 to 19. Thelabial surfaces of the mandibular anteriors were exam-
ined for the incidence of recession, and factors mostcommonly associated with the recession. Of the teethexamined 1.8% were reported to have recession of greaterthan 3 mm. The factor most commonly associated withrecession was tooth malposition.
Gorman3 examined 164 subjects of ages 16 to 86 yearsfor recession. Recession was considered to be anyamount of root exposure. In teeth in pronounced labio-version, 61% (32 out of 52) were found to have some
degree of recession and 15% in pronounced linguoversion(4 out of 26) had gingival recession. Of the factorsexamined, malposition of the teeth was the factor mostfrequently associated with recession.
Pearson4 conducted a study on 27 untreated cases and45 cases treated by orthodontics. The untreated cases
* 1414 S. Miller, Santa Maria, CA 93454.t School of Dentistry, Loma Linda University, Loma Linda, CA
92354. Institute of Dentistry, University of Helsinki, Mannerheimintie
172, Helsinki 28, Finland.
were considered normal and the treated cases were se-
lected because they exhibited the most severe amount ofgingival recession out of a total of 600 treated cases. Theuntreated cases were examined for amount of recessioninitially and 2 years later. The treated group was exam-
ined for amount of recession before and after orthodontictherapy. The average gingival height of the two mandib-ular central incisors served as the basis for comparisonbetween treated and untreated groups. The positions ofthe teeth were assessed by cephalometric tracings. Theuntreated cases showed an average of 0.04 mm gingivalrecession and the treated group exhibited 1.1 mm reces-
sion; however, the author stated that no correlation couldbe found between the amount of labial or lingual toothmovement and the degree of recession.
Batenhorst et al.5 examined the effects of orthodonticmovement in two rhesus monkeys. Bands were placedon the mandibular anterior teeth and forces were appliedfor a period of 54 to 64 days in order to tip one lowercentral and one lower lateral incisor facially in eachmonkey. The contralateral teeth served as controls. Amaintenance period of 240 days was allowed for reten-tion. The resulting tooth movement was found to be ina facial and coronal direction. Apical displacement ofthe gingival margin in relation to the experimental teethwas found to average 3.2 mm. On the control teeth,apical displacement was minimal. The amount of at-tached gingiva was found to increase on an average of1.6 mm for the experimental teeth, with minimal changesfor the controls.
Dorfman6 recently published a study in which photo-graphs of 1162 orthodontic cases were examined forareas of initial minimal keratinized gingiva (<2 mm) or
marked visible changes in the width of keratinized gin-giva which occurred during treatment. The initial and
314
Volume 52Number 6 Changes ofMarginal Periodontium 315
final cephalograms from these cases were also examinedfor changes in tooth position in order to determine ifthere was any correlation between mandibular incisortooth movement and changes seen in keratinized gingivaduring orthodontic therapy. The results indicated thatthose 16 patients who demonstrated marked gingivalrecession had no consistent buccal or lingual tooth move-ment. However, in the eight patients exhibiting an in-crease in keratinized gingiva, there was a significantamount of lingual tooth movement.
Thus, the studies by Parfitt and Mjor,1 Trott andLove,2 Gorman,3 and Batenhorst et al.5 seem to indicatethat tooth malposition is often associated with gingivalrecession. This is contrary to the findings of Pearson.4Further, Dorfman6 found no strong correlation betweenlabial tooth movement and loss of keratinized gingiva.Due to the conflicting results reached by previous au-
thors, this study was undertaken to examine the effectsof labial tooth movement on changes of the marginalperiodontium.
MATERIALS AND METHODS
Animals
Five adult female monkeys (Macaca nemistrina) were
used as experimental subjects. The maxillary and man-
dibular central incisors were subjected to labial ortho-dontic movement and the canines served as untreatedcontrol teeth. The lateral incisors were not analyzed inan effort to separate the moved and unmoved teeth bya reasonable dimension.
Oral HygieneThe teeth of each subject were initially thoroughly
scaled and polished. Throughout orthodontic therapy,each monkey received oral hygiene care according totwo different methods. One arch was swabbed withChlorhexidine and flossed while the opposing arch wasbrushed with a soft toothbrush* and toothpaste^ andflossed (Fig. 1).Amalgam Marker
An amalgam marker was placed on the facial surfaceof each anterior tooth. The marker was placed above thegingival margin but below the orthodontic brackets. Allmeasurements were taken from the apical extent of theamalgam marker.
Parameters
Tooth Movement (TM). The amount of labial toothmovement was calculated by comparing an initial mea-
surement from the mesial fossa of the second bicuspid tothe incisai edge of the central incisor with this same
measurement after orthodontic tooth movement.
* Pycopay, Block Drug Corp., Jersey City, NJ 07302.t Ultrabright toothpaste, Colgate Palmolive Corp., New York, NY.
RIGHT QUADRANT LEFT OUADRANT
MAXILLA Chlorhexidine exploratoryswab surgeryChlorhexidine
swab
MANDIBLE mechanical exploratorycleaning surgerymechanical
cleaning
Figure 1. Diagram distribution of the variables oral hygiene and preor-thodontic exploratory surgery on animals 1, 3, 5. The remaining animals(2, 4) received identical treatment but in opposite quadrants and arches.
Gingival Margin (GM). Measurements were madefrom the apical extent of the amalgam marker on thetooth to the gingival margin. The measurements were
taken using dividers and were transferred to a recordsheet by punching holes in the paper. The distancebetween the two points was later read with a comparator.
Mucogingival Junction (MGJ). Where there was anydoubt of the exact location of the mucogingival junction,the mucosa was swabbed with Schiller's iodine solution7which stains the nonkeratinized oral mucosa dark brown.The iodine solution does not stain the keratinized gin-gival area. Measurements were then made from theapical extent of the amalgam marker to the mucogingivaljunction. Dividers were used as above.
Width of Keratinized Gingiva (KG). The width ofkeratinized gingiva was calculated by subtracting thedistance between the alloy and the gingival margin fromthe distance between the alloy and the mucogingivaljunction.
Connective Tissue Level (CTL). The level of the con-
nective tissue attachment was determined by measuringfrom the apical extent of the amalgam marker to themost coronal extent of the connective tissue fibers sub-sequent to the careful elevation of a labial full thicknessflap (Fig. 2). Toluidine blue was applied and used todelineate the level of the collagen fibers on the toothsurface8 (Fig. 3). The preorthodontic exploratory surgerywas performed on either right or left quadrants. Themeasurements for the connective tissue level on the teethin the quadrants which received preorthodontic explor-atory surgery served also as initial readings for contra-lateral teeth. Prior to surgery, the distance from theincisai edge to the apical extent of the amalgam markerwas measured with dividers. During surgery the mea-
surement was made from the amalgam marker to theconnective tissue level (Fig. 4). These two numbers were
added and then used as initial measurements for thecontralateral teeth. In this manner measurements couldbe obtained for the teeth which were not operated on
surgically before the orthodontic tooth movement. Theassumption was made that contralateral teeth wouldhave similar anatomy.
Marginal Bone Level (MBL). The level of the marginalbone was also assessed during the preorthodontic ex-
ploratory surgery in a similar manner as for the connec-

316 Steiner, Pearson, Ainamo
Figure 2. Preorthodontic exploratory surgery.
Figure 3. Application of toluidine blue. The stained areas include plaqueand collagen fibers. The unstained area between collagen fibers andplaque indicates previous epithelial attachment.
five tissue (Fig. 5). Figure 1 describes the quadrantswhich received preorthodontic exploratory surgery. Thepostorthodontic surgery included all anterior teeth. Mea-surements were then taken on all central incisors andcuspids. Dividers were used as described above.
Orthodontics
Edgewise orthodontic applicances were used toachieve tooth movement. Segment wires were positionedin each quadrant from first molar to lateral incisor toinclude the second bicuspid and cuspid. The centralswere then bracketed to 16 X 22 elgiloy wire run throughtubes located on each segment wire (Fig. 6). Activationof the appliance was achieved by the use of open coilwire to provide approximately 50 gm of force in thelabial direction (Fig. 7). The appliances were checkedweekly to insure bodily movement, and to prevent extru-sion. Bodily movement of the right and left centralincisors in both arches was continuous until dehiscencein the alveolus was believed to have occurred. Thepresence of a dehiscence was evaluated by palpation andlateral cephalograms. Orthodontic forces were thus ap-plied for a period of 13 weeks. A stabilization period of
J. Periodontol.June, 1981
3 weeks followed (Fig. 8). The experimental design isoutlined in Figure 9.
Statistical MethodTo compare displaced central incisors and untreated
control cuspids for dependent variables (gingival margin,mucogingival junction, keratinized gingiva, connectivetissue level and marginal bone level) a general analysisof variance program (BMD08V) was used. The variablesof classification included orthodontic movement, animaldifferences and maxilla/mandible. Left/right was con-sidered to be two duplications nested within animals. Afixed constant model was used on each variable ofclassification except for left/right.
A general linear hypothesis program (BMDX64) wasused to test for the relationship between tooth movementand changes in the dependent variables. The programwas adjusted for animal differences, maxillary/mandib-ular differences and interaction between maxillary andmandibular arches. Design variables were animal andmaxilla/mandible. Tooth movement served as the co-
variate.In order to determine if mechanical cleaning versus
Chlorhexidine treatment and initial exploratory surgeryversus no surgery had any effect on the changes foundin the dependent variables, the general linear hypothesis
Figure 4. Measurement of the level of connective tissue attachment.

Volume 52Number 6 Changes ofMarginal Periodontium 317
Figure 5. Measurement of the level of the marginal bone.
Figure 6. Orthodontic appliance used to create labial displacement of thecentral incisors.
program (BMDX64) was again used. Animals, maxilla/mandible, mechanical cleaning/chlorhexidine, surgery/nonsurgery, served as design variables. Interactions were
not included in the model.
RESULTS
The changes in pre- and postexperimental data includ-ing mean and standard deviations for all dependentvariables can be found on Table 1. Figure 10 and Table1 demonstrate the difference between the pre-experimen-
Figure 7. Tooth and gingival relationships prior to orthodontic therapy.
Figure 8. After orthodontic therapy.
EXPERIMENTAL DESIGN
Procedures
Surgery on rightquadrants of monkeys1 3 and 5. Surgery onleft quadrants ofmonkeys 2 and 4
weeks
Orthodontic forcesapplied
Measurements
Marker to marginalbone level and connective tissue level
Weekly measurementsfrom amalgam markerto gingival marginand mucogingival
junction
13 weeks
Stabilization
Flap surgery on allanterior teeth
3 weeks
Final measurements ofgingival marginmucogingival junctionconnective tissue leveland marginal bone level
Figure 9. Experimental design.

318 Steiner, Pearson, AinamoJ. Periodontol.
June, 1981
Table 1Changes in dependent variables during 16 weeks of orthodontic therapy, comprising 13 weeks of labial movement ofcentral incisors and a subsequent 3week stabilization periodThe abbreviations are for amount of labial movement (TM), change in width of keratinized gingiva (KG), and change in distance from amalgammarker to gingival margin (GM), mucogingival junction (MGJ), level of connective tissue (CTL) and marginal bone level (MBL). Allmeasurements are in millimeters.
Displaced incisors Control cuspidsAnimal
Tooth TM GM MGJ KG CTL MBL Tooth GM MGJ KG CTL MBL
92425
89
2425
89
2425
89
2425
89
2425
2.02.52.03.0
4.04.03.04.0
2.02.03.53.5
2.52.04.03.5
2.53.54.03.5
0.30.50.60.9
1.31.51.61.4
1.10.60.81.3
0.61.01.51.3
1.20.80.61.2
0.80.40.60.5
2.01.41.61.4
1.10.30.91.8
0.11.10.90.0
1.31.01.81.4
0.5-0.1
0.0-0.4
0.7-0.1
0.00.0
0.0-0.3
0.10.5
-0.5-0.1-0.6-1.3
0.10.21.20.3
0.20.50.70.8
3.73.04.13.7
1.51.61.61.3
1.91.51.61.3
1.91.92.42.2
8.17.97.23.1
0.10.52.72.8
7.56.36.25.0
1.00.67.87.4
10.26.89.17.6
6112227
6112227
6112227
6112227
6112227
-0.2-0.20.00.3
0.30.20.00.2
0.10.20.30.7
0.50.00.10.8
0.30.1
-0.20.5
-0.3-0.40.20.8
0.30.20.00.2
0.00.20.70.6
0.40.20.30.2
0.20.30.10.2
-0.1-0.20.20.5
0.0-0.1
0.30.0
-0.10.00.4
-0.1
-0.10.20.30.6
-0.10.20.3
-0.1
-1.5-0.10.91.2
2.30.82.21.3
-1.50.00.0
-1.7
1.41.40.51.0
2.41.40.7
-0.1
0.30.81.36.4
1.3-1.1
3.73.0
1.41.20.51.2
2.30.31.73.1
-0.21.20.5
-0.1
MeanSD
3.050.8
1.010.4
1.020.6
0.010.5
1.931.1
5.483.1
0.200.3
0.230.3
0.100.2
0.890.8
1.521.0
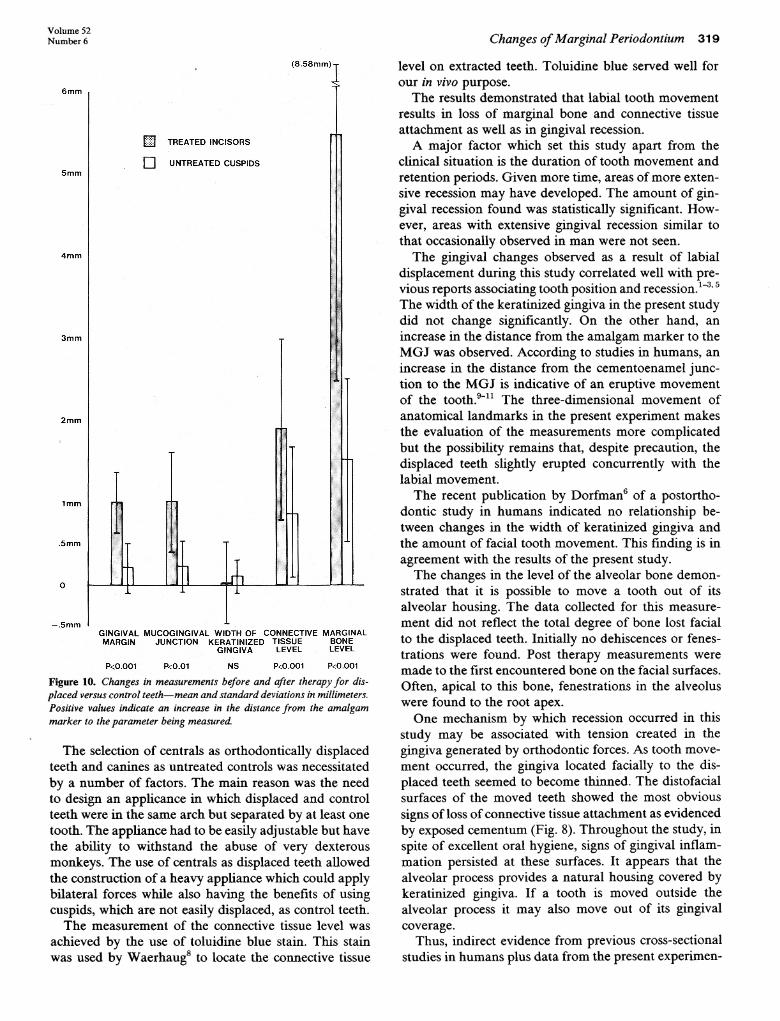
tal and postexperimental measurements for all displacedincisors and orthodontically untreated control cuspids.Upon comparison of displaced and control teeth, therewere significant differences in the distance from theamalgam marker to the gingival margin, the mucogin-gival junction, the connective tissue level and the mar-
ginal bone level. However, there was no difference in thewidth of the keratinized gingiva (Table 2).
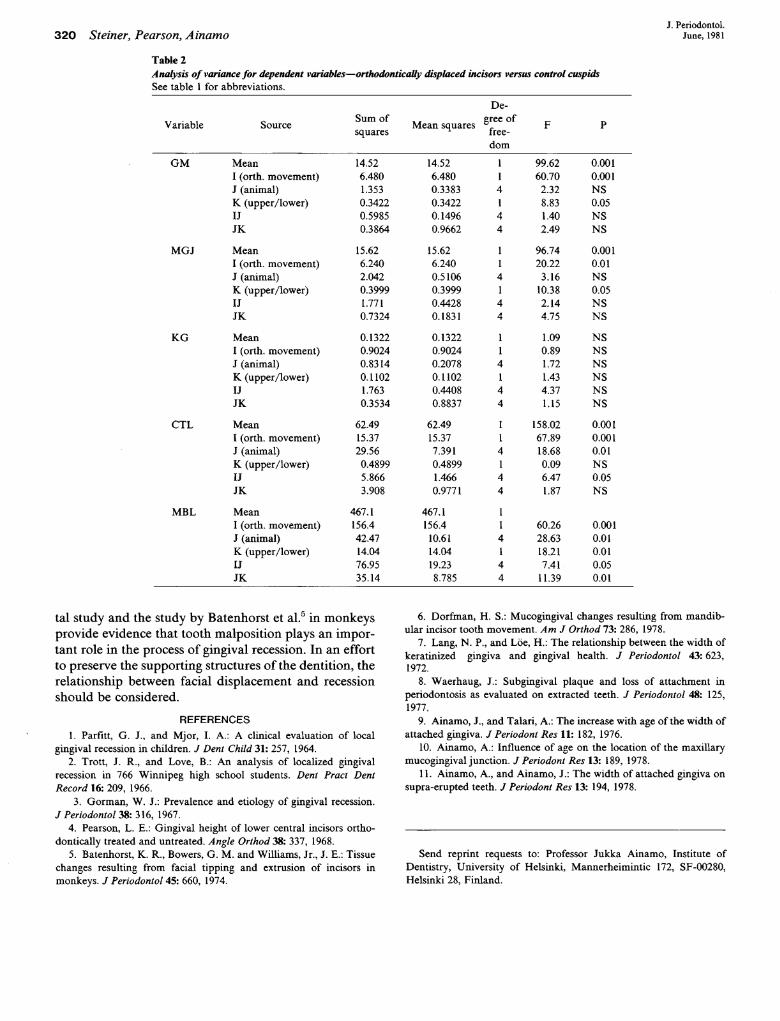
The statistical data (Table 2) demonstrate a significantrecession of the gingival margin (P < 0.001) in displacedincisors over untreated control cuspids. Difference be-tween the recession of the upper and lower teeth indi-cated an increased amount of recession associated withthe lower arch (P < 0.05). A similar difference was foundin the distance from the amalgam marker to the muco-
gingival junction, except that in this respect the differ-ence between displaced versus control teeth was onlysignificant to the 0.01 level.
The analysis of the difference between displaced anduntreated control teeth in relation to the connective tissuelevel found a loss of connective tissue attachment sig-nificant to the 0.001 level. Significant differences werefound between the reactions of various animals (P <
0.01) and the interaction between animals and orthodon-tic movement (P < 0.05). The change in the height ofthe facial alveolar bone was significantly different to the
0.001 level when comparing displaced versus controlteeth. Significant differences were also found betweenthe changes observed in different animals, in maxillaryand mandibular arches, and in interactions of these twovariables (P < 0.01).
The amount of recession of the gingival margin andchanges in the distance between the amalgam markerand the mucogingival junction, the connective tissuelevel and the marginal bone level were all found to benot statistically significantly related to the amount oftooth movement.*
The displaced teeth that were brushed and flossed hadno changes different from those in the teeth which wereswabbed with Chlorhexidine.*
The teeth that received pre-experimental exploratorysurgery had the same changes in the measurements forthe gingival margin, mucogingival junction, connectivetissue level and marginal bone level as had the contra-lateral nonsurgically treated teeth.*
DISCUSSIONThis study was designed to analyze the relationship
between labial tooth movement and changes of the mar-
ginal periodontium.* Statistical method and data available upon request.
Volume 52Number 6 Changes ofMarginal Periodontium 319
(8.58mm) T
W] TREATED INCISORS
UNTREATED CUSPIDS
DL 04
GINGIVAL MUCOGINGIVAL WIDTH OF CONNECTIVE MARGINALMARGIN JUNCTION KERATINIZED TISSUE BONE
GINGIVA LEVEL LEVEL
P<0.001 P<0.01 NS P<0.001 P<0.001
Figure 10. Changes in measurements before and after therapy for dis-placed versus control teeth—mean and standard deviations in millimeters.Positive values indicate an increase in the distance from the amalgammarker to the parameter being measured.
The selection of centrals as orthodontically displacedteeth and canines as untreated controls was necessitatedby a number of factors. The main reason was the needto design an applicance in which displaced and controlteeth were in the same arch but separated by at least one
tooth. The appliance had to be easily adjustable but havethe ability to withstand the abuse of very dexterousmonkeys. The use of centrals as displaced teeth allowedthe construction of a heavy appliance which could applybilateral forces while also having the benefits of usingcuspids, which are not easily displaced, as control teeth.
The measurement of the connective tissue level was
achieved by the use of toluidine blue stain. This stainwas used by Waerhaug8 to locate the connective tissue
level on extracted teeth. Toluidine blue served well forour in vivo purpose.
The results demonstrated that labial tooth movementresults in loss of marginal bone and connective tissueattachment as well as in gingival recession.
A major factor which set this study apart from theclinical situation is the duration of tooth movement andretention periods. Given more time, areas of more exten-sive recession may have developed. The amount of gin-gival recession found was statistically significant. How-ever, areas with extensive gingival recession similar tothat occasionally observed in man were not seen.
The gingival changes observed as a result of labialdisplacement during this study correlated well with pre-vious reports associating tooth position and recession.1"3,5The width of the keratinized gingiva in the present studydid not change significantly. On the other hand, anincrease in the distance from the amalgam marker to theMGJ was observed. According to studies in humans, anincrease in the distance from the cementoenamel junc-tion to the MGJ is indicative of an eruptive movementof the tooth.9-11 The three-dimensional movement ofanatomical landmarks in the present experiment makesthe evaluation of the measurements more complicatedbut the possibility remains that, despite precaution, thedisplaced teeth slightly erupted concurrently with thelabial movement.
The recent publication by Dorfman6 of a postortho-dontic study in humans indicated no relationship be-tween changes in the width of keratinized gingiva andthe amount of facial tooth movement. This finding is inagreement with the results of the present study.
The changes in the level of the alveolar bone demon-strated that it is possible to move a tooth out of itsalveolar housing. The data collected for this measure-
ment did not reflect the total degree of bone lost facialto the displaced teeth. Initially no dehiscences or fenes-trations were found. Post therapy measurements were
made to the first encountered bone on the facial surfaces.Often, apical to this bone, fenestrations in the alveoluswere found to the root apex.
One mechanism by which recession occurred in thisstudy may be associated with tension created in thegingiva generated by orthodontic forces. As tooth move-
ment occurred, the gingiva located facially to the dis-placed teeth seemed to become thinned. The distofacialsurfaces of the moved teeth showed the most obvioussigns of loss of connective tissue attachment as evidencedby exposed cementum (Fig. 8). Throughout the study, inspite of excellent oral hygiene, signs of gingival inflam-mation persisted at these surfaces. It appears that thealveolar process provides a natural housing covered bykeratinized gingiva. If a tooth is moved outside thealveolar process it may also move out of its gingivalcoverage.
Thus, indirect evidence from previous cross-sectionalstudies in humans plus data from the present experimen-
320 Steiner, Pearson, AinamoJ. Periodontol.
June, 1981
Table 2Analysis of variance for dependent variables-See table 1 for abbreviations.
orthodontically displaced incisors versus control cuspids
Variable Source
De-Sum of ., eree of
Mean squares.squares free-dom
GM Mean1 (orth. movement)J (animal) (upper/lower)IJJK
MGJ MeanI (orth. movement)J (animal) (upper/lower)IJJK
KG MeanI (orth. movement)J (animal) (upper/lower)IJJK
CTL MeanI (orth. movement)J (animal) (upper/lower)IJJK
MBL MeanI (orth. movement)J (animal) (upper/lower)IJJK
14.526.4801.3530.34220.59850.3864
15.626.2402.0420.39991.7710.7324
0.13220.90240.83140.11021.7630.3534
62.4915.3729.56
0.48995.8663.908
467.1156.442.4714.0476.9535.14
14.526.4800.33830.34220.14960.9662
15.626.2400.51060.39990.44280.1831
0.13220.90240.20780.11020.44080.8837
62.4915.377.3910.48991.4660.9771
467.1156.4
10.6114.0419.238.785
114144
114I44
114144
114144
114144
99.6260.70
2.328.831.402.49
96.7420.22
3.1610.382.144.75
1.090.891.721.434.371.15
158.0267.8918.680.096.471.87
60.2628.6318.217.41
11.39
0.0010.001NS0.05NSNS
0.0010.01NS0.05NSNS
NS SNSNSNSNS
0.0010.0010.01NS0.05NS
0.0010.010.010.050.01
tal study and the study by Batenhorst et al.5 in monkeysprovide evidence that tooth malposition plays an impor-tant role in the process of gingival recession. In an effortto preserve the supporting structures of the dentition, therelationship between facial displacement and recessionshould be considered.
REFERENCES1. Parfitt, G. J., and Mjor, I. .: A clinical evaluation of local
gingival recession in children. J Dent Child 31: 257, 1964.2. Trott, J. R., and Love, B.: An analysis of localized gingival
recession in 766 Winnipeg high school students. Dent Pract DentRecord 16: 209, 1966.
3. Gorman, W. J.: Prevalence and etiology of gingival recession.J Periodontol 38: 316, 1967.
4. Pearson, L. E.: Gingival height of lower central incisors ortho-dontically treated and untreated. Angle Orthod 38: 337, 1968.
5. Batenhorst, . R., Bowers, G. M. and Williams, Jr., J. E.: Tissuechanges resulting from facial tipping and extrusion of incisors inmonkeys. J Periodontol 45: 660, 1974.
6. Dorfman, H. S.: Mucogingival changes resulting from mandib-ular incisor tooth movement. Am J Orthod 73: 286, 1978.
7. Lang, N. P., and Löe, H.: The relationship between the width ofkeratinized gingiva and gingival health. / Periodontol 43: 623,1972.
8. Waerhaug, J.: Subgingival plaque and loss of attachment inperiodontosis as evaluated on extracted teeth. J Periodontol 48: 125,1977.
9. Ainamo, J., and Talari, .: The increase with age of the width ofattached gingiva. J Periodont Res 11: 182, 1976.
10. Ainamo, .: Influence of age on the location of the maxillarymucogingival junction. J Periodont Res 13: 189, 1978.
11. Ainamo, ., and Ainamo, J.: The width of attached gingiva on
supra-erupted teeth. J Periodont Res 13: 194, 1978.
Send reprint requests to: Professor Jukka Ainamo, Institute ofDentistry, University of Helsinki, Mannerheimintic 172, SF-00280,Helsinki 28, Finland.

![INSTITUTEOFAERONAUTICALENGINEERING · Figure3 4. (a)Deriveshapefunctionandstiffnessmatrixfor2Dtrusselement. [7M] (b)ForthecantileverbeamsubjectedtotheuniformloadwasshowninFigure4,determinethever-](https://static.fdocuments.in/doc/165x107/5e89f388fdf1fb7ddc317bc7/instituteofaeronauticalengineering-figure3-4-aderiveshapefunctionandstiffnessmatrixfor2dtrusselement.jpg)