Changes in urinary amino acid fractional excretion in neonates undergoing total parenteral nutrition
8
Early Human Development, 18 (1988) 31-44 Elsevier Scientific Publishers Ireland Ltd. EHD 00905 Changes in urinary amino acid fractional excretion in neonates undergoing total parenteral nutrition Mark Rosenthal Leicester Royal Infirmary, Leicester. U.K. Accepted for publication 21 November 1987 Summary The paper examines the possible reasons why there was a different weight gain pattern in two groups of sick neonates fed two different amino acid solutions during a prospective double-blind trial of otherwise identical total parenteral nutrition. During the 13-month study period, 14 neonates (eight less than 32 weeks gestation) received Vamin as their amino acid source, and 18 (eight less than 32 weeks gestation) received a new amino acid solution, Paedmin. The older group of neonates gained weight far better when fed Vamin (P< 0.003), neonates of less than 32 weeks gestation gained weight better when fed Paedmin (P < 0.004). These differences in weight gain were reflected in differences in plasma amino acid concentration in that the levels were lower in the groups gaining weight less well; and in urinary fractional excretion where the groups gaining weight less well had a markedly higher fractional excretion and total urinary loss of amino acids (P < 0.001). It is suggested that these differences in amino acid handling of two different amino acid solutions may lead to differences in weight gain. neonates; amino acids; urinary fractional excretion Introduction Since 1944, when total parenteral nutrition (TPN) was first undertaken on a child [9], there have been studies observing amino acid patterns during this period. These Address for correspondence: Dr. M. Rosenthal, 20 Hawthorn Road, Gatley, Cheadle, Cheshire, SK8 4NB, U.K. 0378-3782/88/$03.50 0 1988 Elsevier Scientific Publishers Ireland Ltd. Published and Printed in Ireland
-
Upload
mark-rosenthal -
Category
Documents
-
view
212 -
download
0
Transcript of Changes in urinary amino acid fractional excretion in neonates undergoing total parenteral nutrition

Early Human Development, 18 (1988) 31-44 Elsevier Scientific Publishers Ireland Ltd.
EHD 00905
Changes in urinary amino acid fractional excretion in neonates undergoing total parenteral
nutrition
Mark Rosenthal
Leicester Royal Infirmary, Leicester. U.K.
Accepted for publication 21 November 1987
Summary
The paper examines the possible reasons why there was a different weight gain pattern in two groups of sick neonates fed two different amino acid solutions during a prospective double-blind trial of otherwise identical total parenteral nutrition. During the 13-month study period, 14 neonates (eight less than 32 weeks gestation) received Vamin as their amino acid source, and 18 (eight less than 32 weeks gestation) received a new amino acid solution, Paedmin. The older group of neonates gained weight far better when fed Vamin (P< 0.003), neonates of less than 32 weeks gestation gained weight better when fed Paedmin (P < 0.004). These differences in weight gain were reflected in differences in plasma amino acid concentration in that the levels were lower in the groups gaining weight less well; and in urinary fractional excretion where the groups gaining weight less well had a markedly higher fractional excretion and total urinary loss of amino acids (P < 0.001). It is suggested that these differences in amino acid handling of two different amino acid solutions may lead to differences in weight gain.
neonates; amino acids; urinary fractional excretion
Introduction
Since 1944, when total parenteral nutrition (TPN) was first undertaken on a child [9], there have been studies observing amino acid patterns during this period. These
Address for correspondence: Dr. M. Rosenthal, 20 Hawthorn Road, Gatley, Cheadle, Cheshire, SK8 4NB, U.K.
0378-3782/88/$03.50 0 1988 Elsevier Scientific Publishers Ireland Ltd. Published and Printed in Ireland

38
have pointed towards worrying plasma concentrations of certain amino acids during TPN [2,11], made recommendations about altering the composition of the amino acid solutions [ 11, recognised a dose/response relationship of intake to plasma levels [3] and compared the efficacy of differing amino acid solutions upon nitrogen retention in the neonate [4]. In order to improve intact survival in this very vulnerable age group, it is important to determine the reasons why neonates gain weight during TPN so that this growth can be optimised.
Evidence is put forward, based on observations reported previously [7] from a study comparing a current standard amino acid solution for neonates in the U.K., Vamin (Kabivitrum, Sweden) with a new amino acid solution, Paedmin (Pfrimmer, F.R.G.) suggesting that urinary amino acid fractional excretion may have a role.
Patients and methods
During a continuous 13-month period, all 32 neonates who received TPN for longer than 48 h were studied in a prospective double-blind manner.
The amino acid solution was either Paedmin (n = 18) or Vamin (n = 14) at a rate of 2.5 g protein/kg per day from day 1 of TPN (Table I), the choice randomly determined by drawn card in pharmacy. In all other respects, their parenteral nutrition was identical. Each patient received 20% Intralipid plus Vitlipid
TABLE I
Characteristics of amino acids with % content in each of the TPN solutions.
Vamin vso)
Paedmin Wsl
Amino acid type
Charge Essential
Glutamic acid 11.1 Isoleucine 5.4 Leucine 1.3 Methionine 2.4 Phenylalanine 6.0 Tryptophan 0.9 Tyrosine 0.5 Valine 6.5 Cysteine 2.2 Arginine 3.2 Alanine 6.0 Aspartic acid 5.6 Glycine 5.1 Histidine 2.7 Lysine 4.9 Proline 12.7 Berine 12.9 Threonine 4.5
15.3 Acidic 4.5 Neutral 5.0 Neutral 1.6 Neutral 2.6 Neutral 0.7 Neutral 0.4 Neutral 4.2 Neutral 0.4 Neutral 4.1 Basic
24.6 Neutral 1.3 Acidic
12.3 Neutral 1.1 Basic 3.3 Basic 8.1 Imino 0.0 Neutral 3.3 Neutral
No Yes Yes YeS YfS Yes Yes Yes Yes Yes No No No Yes Yes No No Yes
100% 100%
39
(Kabivitrum, Sweden) at 0.5 g/kg per day on day 1 of TPN rising to 3 g/kg per day by day 6, made up to a total volume of 150 ml/kg per day with a 10% dextrose/ electrolyte/trace element/water soluble vitamin mixture.
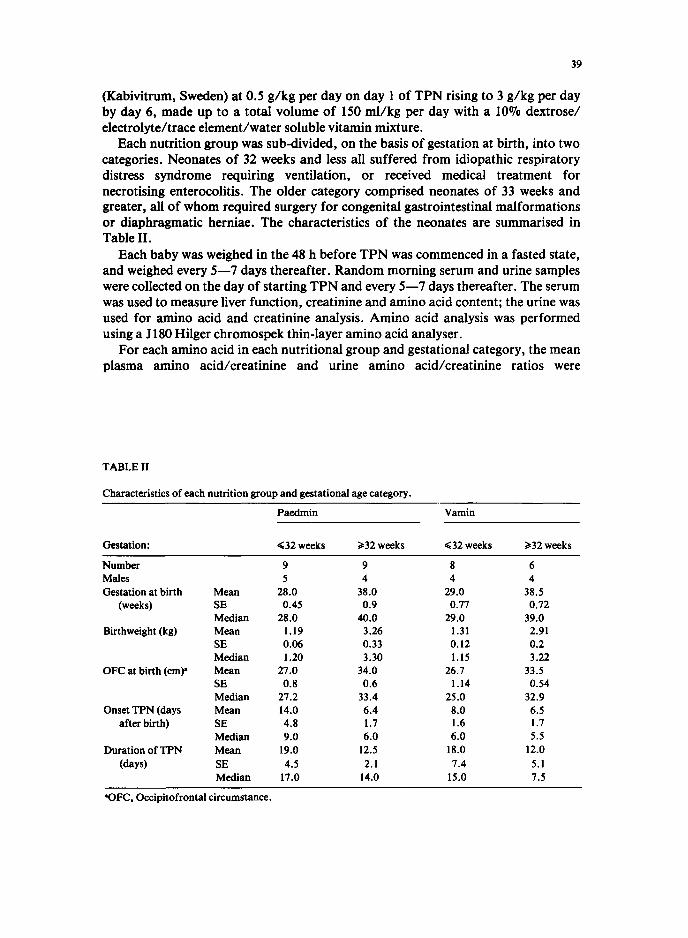
Each nutrition group was sub-divided, on the basis of gestation at birth, into two categories. Neonates of 32 weeks and less all suffered from idiopathic respiratory distress syndrome requiring ventilation, or received medical treatment for necrotising enterocolitis. The older category comprised neonates of 33 weeks and greater, all of whom required surgery for congenital gastrointestinal malformations or diaphragmatic herniae. The characteristics of the neonates are summarised in Table II.
Each baby was weighed in the 48 h before TPN was commenced in a fasted state, and weighed every 5-7 days thereafter. Random morning serum and urine samples were collected on the day of starting TPN and every 5-7 days thereafter. The serum was used to measure liver function, creatinine and amino acid content; the urine was used for amino acid and creatinine analysis. Amino acid analysis was performed using a J 180 Hilger chromospek thin-layer amino acid analyser.
For each amino acid in each nutritional group and gestational category, the mean plasma amino acid/creatinine and urine amino acidicreatinine ratios were
TABLE II
Characteristics of each nutrition group and gestational age category.
Paedmin Vamin
Gestation: (32 weeks 232 weeks (32 weeks 232 weeks
Number Males Gestation at birth
(weeks)
Birthweight (kg)
OFC at birth (cmp
Onset TPN (days after birth)
Duration of TPN (days)
Mean SE Median Mean SE Median Mean SE Median Mean SE Median Mean SE Median
9 9 8 6 5 4 4 4
28.0 38.0 29.0 38.5 0.45 0.9 0.77 0.72
28.0 40.0 29.0 39.0 1.19 3.26 1.31 2.91 0.06 0.33 0.12 0.2 1.20 3.30 1.15 3.22
27.0 34.0 26.7 33.5 0.8 0.6 1.14 0.54
27.2 33.4 25.0 32.9 14.0 6.4 8.0 6.5 4.8 1.7 1.6 1.7 9.0 6.0 6.0 5.5
19.0 12.5 18.0 12.0 4.5 2.1 7.4 5.1
17.0 14.0 15.0 7.5
*FC, Occipitofrontal circumstance.

determined as well as mean plasma amino acid concentrations in both the fasted and TPN fed states; from these the mean fractional excretion (FE) was determined using the formula:
where U = urine, P = plasma, aa = amino acid concentration and cr = creatinine concentration. Statistical comparisons are made using Kendal’s coefficient of concordance W, Spearman’s rank correlation coefficient R, Fisher’s exact test plus Fisher’s test for combining independent tests of significance [lo] and analysis of variance.
Results
Figure 1 shows the comparative weight changes expressed as percentage change from pre-TPN weight for all the neonates. Neonates of 32 weeks and less fed Paedmin had a less marked and shorter period of weight loss followed by a similar weight gain velocity to those fed Vamin (P < 0.004). Neonates of 33 weeks and greater showed a marked weight gain when fed Vamin, but an overall weight loss when fed Paedmin (P < 0.003).
The fractional excretions and plasma concentrations of each amino acid are shown in Figs. 2 and 3 respectively. During TPN (Fig. 2), there is a remarkably consistent hierarchical order of FE for the 16 amino acids (coefficient of
Fig. 1. Weight changes during TPN expressed as mean ( f S.E.M.) percentage weight change from pre- TPN weight in neonates of gestations at birth less than 32 weeks (A) and greater than 33 weeks (B). -, Paedmin as protein source; - - - -, Vamin-fed neonates.

36
32.
16
Fig. 2. Mean fractional excretion in neonates of less than 32 weeks gestation (A) and greater than 33 weeks gestation (B) in fasted and fed (Paedmin or Vamin) state for the 16 amino acids measured. See text for statistical analysis.
concordance, W = 0.947, P 4 0.001) and is present regardless of gestation and nutrition. There is an overall tendency for the non-essential amino acids (Gly, Ser, Asp, Ala, Glu) to have a higher FE than expected by chance (P< 0.07).
There is also a very strong hierachical order for the plasma amino acid concentrations which is the same whether fasted or fed, preterm or term (Fig. 3, coefficients of concordance, W = 0.88 for preterm group and 0.96 for term group, both P 4 0.001). There is, however, no correlation between plasma amino acid rank and its equivalent FE rank (Spearman’s R = 0.05 for Vamin, and 0.17 for Paedmin, NS).
In neonates of 33 weeks and greater, babies fed Vamin showed a rise in FE for five amino acids (Glu, Val, Ile, His, Lys) and a fall in 11; those fed Paedmin showed a rise for 14 and a fall for two (Met, Leu) when comparing fasted to fed state (P < 0.001). During TPN, neonates fed Paedmin had 14/16 amino acids (except Ile, Leu) with a higher FE than babies fed Vamin (P < 0.001) but Paedmin-fed babies had lower plasma concentrations for 13/16 (except Glu, Ile, Thr) amino acids. Differences were also observed in the total urinary and serum amino acid values:

42
700-
5 600- z a s ‘g 500-
6 c ; 400-
e ‘I : ; 300- 1
h zoo-
loo-
o-
@
I I Pm-TPN Vamin
I Paedmin
700-
600-
500-
4w-
300-
zoo-
loo-
OA
Fig. 3. Mean plasma amino acid concentrations in neonates of 32 weeks gestation and less (A) and 33 weeks gestation and greater (B) in a fasted or fed (Paedmin or Vamin) state for the 16 amino acids measured. See text for statistical analysis.
total urinary loss of amino acids was 45% more in Paedmin-fed neonates (5018 ~ol/mmol creatinine vs. 3547 mol/ mmol Cr for Vamin) whereas total plasma values were 20% less (49.5 mol/mmol Cr for Paedmin vs. 61.6 @ol/mmol Cr for Vamin). Babies in this gestation category fed Paedmin gained weight poorly.
In neonates of 32 weeks and less, those babies fed Vamin show an increase in PE for all 16 amino acids (P < 0.001) compared to the fasting state (compare term babies). Neonates fed Paedmin show a rise in FE for ten amino acids, but a fall for six (Leu, Ile, Val, Met, Glu, Gly) when compared to the fasting state. This is a different FE pattern to that of Vamin (P < 0.02). During TPN, 13 amino acids in the Vamin-fed group have a higher PE than those fed Paedmin (P < 0.02, except Thr, Ser, Tyr), but in the Vamin-fed group, plasma amino acid concentrations were lower for nine amino acids and greater by less than 20 @01/l in five of the other seven (Val, Ile, Leu, Tryp, Ser, Cys, His). Total urinary loss of amino acids was 27% less in Paedmin-fed neonates (6635 pol/mmol Cr vs. 9116 pmol/mmol Cr) and total plasma amino acids were 5% greater in this group (50.6 @ol/mmol Cr vs. 48.2 l.unol/mmol Cr for Vamin). Neonates fed Vamin gained weight less well than those fed Paedmin.
Discussion
The results show that differences in weight gain in groups of neonates fed different amino acid profiles with the same total protein intake were associated both
43
in magnitude and direction by differences in fractional excretion, total urinary loss and total plasma concentrations of amino acids. From this study, it cannot be concluded with certainty that the different amino acid handling in the two age groups is either due to changing organ maturity as gestation advances, instead of, for example, the metabolic effects of surgery, which only occurred in the older group, though the former is suggested as being more likely.
There are eight recognised separate reabsorptive mechanisms for amino acids in the mammalian kidney, the most capacious of which involves the neutral amino acids [8]. L-Ala, Leu, Ile, Met, Phe, Tyr, VaI, Gln, Tryp, are thought to share one high capacity system (for which they have a strong affinity) with His, Ser and Thr which have a lower affinity. This is borne out by the present study in that His, Ser and Thr tend to have higher fractional excretions than the other amino acids using this system (Fig. 2). It is likely that the system is not fully developed in especially the preterm neonate resulting in competition among the higher affinity amino acids leading to a raised fractional excretion.
The greater FE of aspartate than glutamate during TPN confirms the work of Doolan et al. [5] in adults, and O’Brian and Butterfield [6] in well neonates suggesting a different affinity in the two amino acids for the same transport mechanism.
In the neonate, where absorbtive capacities are more likely to be easily saturated, a raised plasma amino acid concentration will lead to an increased filtered load (the product of the glomerular filtration rate and the plasma amino acid concentration) [8]. This will tend to both increase its own fractional excretion and possibly increase the fractional excretion of the other amino acids sharing the same absortive mechanism by competition for binding sites. Whether in the human neonate this leads to a reduction back to the original ‘normal’ plasma concentration from the original higher level, or because of the complex competitive interactions in the renal tubule, actually leads to excess loss is not known. From the data, however, it may appear so, in that the higher fractional excretions are associated with lower plasma amino acid levels.
The hierachical order of plasma amino acid concentrations is consistent with other studies: the correlation between plasma amino acid rank in Vamin-fed babies in the present study with those of Anderson et al. [2] was R = 0.93 (P B 0.001) as was the correlation between Paedmin or Vamin-fed babies in the present study with Chessax’s study [4] (R > 0.80, P< 0.001).
If these changes in FE actually lead to differences in weight gain (and are not merely an association), then the composition of neonatal amino acid solutions may be altered and then tested in an objective way by growth and fractional excretion measurements. This may improve the neonate’s chances of survival when suffering from conditions requiring TPN.
Acknowledgements
My thanks to Dr. M. Levene for allowing me to report these findings on his patients, and Mr. E. Layward for the amino acid analysis; Dr. D.A. Price, Professor LB. Houston and Dr. R.J. Postlethwaite for their advice.

44
References
8
9
10
11
Abitol. C.L., Feldman, D.B., Ahman, P. and R&man, D. (1975): Plasma amino acid patterns during supplemental intravenous nutrition of low birth weight infants. J. Pediatr., 86,766771. Anderson, GE., Bucher, D., Friis-Hansen, B., Nexo, E. and Oleson, H. (1983): Plasma amino acid concentrations in newborn infants during parenteral nutrition. J. Parent. Ent. Nutr., 7,369-373. Anderson, G.H., Bryan, H., Jeejeebhoy, K.N. and Corey. P. (1977): Dose-response relationships between amino acid intake and blood levels in newborn infants. Am. J. Clin. Nutr., 30, 1110-l 121. Chessax. P., Zebiche, H., Pineault, M.. Lepage, D. and Dallaire. L. (1985): Effect of amino acid composition of parenteral solutions on nitrogen retention and metabolic response in very low birth weight infants. J. Paediatr., 106, 111-117. Doolan, P.D., Harper, H.A., Hutchin, M.E. and Alpen, E.L. (1955): Renal clearance of 18 individual amino acids in human subjects. J. Clin. Invest., 202,577-583. O’Brian, D. and Butterfield, L.J. (1963): Further studies on renal tubular conservation of free amino acids in early infancy. Arch. Dis. Child,. 38,437-442. Rosenthal, M., Sinha, S., Layward, E. and Levene. M. (1987): A double blind comparison of a new parenterai amino acid solution in neonatal total parenteral nutrition. Early Hum. Dev., 15, 137- 146. Silbemagl, S. (1985): Amino acids and oligopeptides. In: The Kidney: Physiology and Pathophysiology. Editors: D.W. Seldin and B. Giebisch. Raven Press, New York. Stegink, L.D. (1983): Amino acids in Parenteral nutrition. Solution infused - Lessons learned. Am. J. Dis. Child., 137,1008-1016. Wallis, W.A. (1942): Compounding probabilities from independent significance tests. Econometrics, 10,229-248. Wong, P. and Pildes, R. (1974): Plasma amino acids in low birth weight infants treated with intravenous amino acid infusion. Biol. Neonate, 25,300-306.