
Changes, Challenges & Choices - Indiana MGMA · ProAssurance Indemnity is an approved provider of...
33
Under Pressure Changes, Challenges & Choices A Risk Resource Seminar Presented by
Transcript of Changes, Challenges & Choices - Indiana MGMA · ProAssurance Indemnity is an approved provider of...

Under Pressure Changes, Challenges &
Choices
A Risk Resource Seminar
Presented by

Risk Resource Regional Office 2600 Professionals Drive
Post Office Box 150 Okemos, Michigan 48805–0150
800.292.1036
Hayes V. Whiteside, MD Chief Medical Officer
Senior Vice President, Risk Resource [email protected]
800.282.6242, ext. 2670
www.ProAssurance.com
Course Objectives
Participation in this seminar will better enable participants to: • Communicate in ways that promote good interpersonal relationships with patients,
families, physicians, allied healthcare professionals, and practice staff; • Demonstrate conduct that results in effective information exchange with patients, families,
physicians, allied healthcare professionals, and practice staff; and • Identify at least one personal bias that influences daily operational decisions.
Accreditation Statement
ProAssurance Indemnity is an approved provider of continuing nursing education by the Alabama State Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on Accreditation. Alabama Board of Nursing Provider Number ABNP0161 (valid through August 5, 2017). 2.0 ASNA/2.4 ABN contact hours will be awarded for successful completion of this activity.
Successful Completion of this CNE
In order to receive contact hour credit for CNE activity, you must:
• Be present for the entire activity • Complete and submit the evaluation form • Include nursing license # on evaluation form
DISCLAIMER. Information in this presentation is neither an official statement of position, nor should it be considered as professional legal advice to individuals or organizations.

Presenters
Kathi Burton, MS, HRM, FASHRM, is a Risk Resource Manager for ProAssurance. She has a master’s degree in safety management with a clinical internship in radiological safety. She is also a Fellow of the American Society of Healthcare Risk Management and a Certified Healthcare Risk Manager. Phone: 800.282.1036, ext. 6204 e-mail: [email protected] Mark J. Hakim, MA, MBA, is Director, Risk Resource for ProAssurance. He obtained a master’s degree in exercise physiology from Michigan State University and his MBA from University of Detroit Mercy. He has an extensive background in exercise physiology and cardiology and has managed occupational and employee health programs. Phone: 800.282.1036, ext. 6225 e-mail: [email protected] Aaron R. Hamming, JD, is a Risk Resource Advisor for ProAssurance. He obtained a Bachelor’s in Comparative Political Systems from Western Michigan University and his law degree from the Thomas M. Cooley School of Law. His private-practice background included litigation and appellate practice, and he is a member of both the Michigan and the Grand Rapids Bar Associations. He has also surveyed hospitals as a senior examiner for the Michigan Quality Council. Phone: 800.282.1039, ext. 6292 e-mail: [email protected] Laurette Salzman, MBA, CPHRM, is a Senior Risk Resource Advisor for ProAssurance. She obtained a master’s degree in business administration from Upper Iowa University. She has extensive experience in hospital and clinic operations, training and education, and healthcare risk management consultation. Phone: 800.279.8331, ext. 8304 e-mail: [email protected] Jeremy Wale, JD, is a Risk Resource Advisor for ProAssurance. He obtained his law degree with honors from Thomas M. Cooley Law School, where he was a published legal scholar and editor of the Law Review. Mr. Wale regularly writes about risk management topics for our insureds’ benefit. Phone: 800,282.1036, ext. 6368 e-mail: [email protected]

ProAssurance’s Approach to
Risk Management and the
Defense of Claims ProAssurance is committed to the improvement of the American Judicial System. Improvement is made possible when all participants have a thorough understanding of the system and its underlying premises and procedures. Improvement is also made possible when the participants receive regular instruction in the details of the operation of the dispute resolution mechanisms afforded by our society. Our system is an adversary system. Its effectiveness is dependent upon honest advocacy. Dishonest advocacy, frequently seen among too many lawyers today, will ultimately destroy the very fabric of our system. Many plaintiffs’ lawyers are honest, hard working, and ethical attorneys trying to do the best for their clients. However, like all professions, the legal profession has its share of bad apples, and these lawyers are willing to resort to devious means to obscure the truth from a jury and to erect barriers which will prevent a jury from understanding the truth of your position. Today’s program and the following materials are offered to improve your understanding of how the system works. An enhanced understanding of our judicial system will relieve your misgivings about the system and improve your confidence. Unfortunately, some lawyers seek to utilize your misgivings in a way that serves to prevent the system from treating you fairly. This is often demonstrated by their reference to bits and pieces of a medical record rather than the complete picture, or their reliance on half-truths or their propensity to take matters out of context. It is also apparent that certain of these lawyers seek to ignore and hide the many dilemmas and difficult clinical conditions which health care professionals face every day and which inevitably shape the life and death decisions that must be made without the benefit of hindsight. These tactics, employed all too often by some lawyers today, serve to distort the truth in professional liability actions. Your highest obligation in your professional responsibility is to tell the truth. It is the highest moral, legal, and ethical obligation you have. You should always, in all circumstances, tell the truth in fulfilling that obligation. Once a jury understands the truth, they will always reach the right result. It is only in those circumstances in which an unsuspecting jury is misled by a plaintiff’s attorney that a jury can be misled in returning a verdict that does not represent the truth. Nothing about today’s program or the following materials is designed to alter your basic obligations to your patients. You would not take that advice even if it were offered to you. However, we do hope these materials will help alleviate the natural feelings of frustration which a health care professional feels when wrongly accused of injuring a patient. Plaintiffs’ attorneys seek to utilize these feelings to avoid the truth. Hopefully, these materials will help instill in you a respect for the system and an understanding of how it operates so that when you are unfairly accused of wrongdoing you will be in a position to defend yourself.

1
• Practice of medicine increasingly difficult
– Technology
– Patients
– Physicians
– Other clinicians
– Regulations
Under Pressure
New Reimbursement Models
Hospital Consolidations
Affordable Care Act
Physician Shortage
Physician Burnout
State Regulations
Obamacare
ACOs
EHRs
? ? ?
Physician↓
Patient
• Allied healthcare professionals
• Patient portals
• Patient experience
• Communication
Under Pressure

2
Allied Healthcare Professionals
• Advanced practice nurses
– Nurse practitioners
– Nurse anesthetists
– Nurse midwives
• Physician assistants
Allied Healthcare Professionals
• Growing numbers in healthcare
– Both NPs & PAs nearly doubled in 10 years
• American Association of Nurse Practitioners 2014
data = 205,000 NPs
• National Commission on Certification of Physician
Assistants 2013 data = 95,583 PAs
Allied Healthcare Professionals
NP Fact Sheet. American Association of Nurse Practitioners Web site. http://www.aanp.org/all-
about-nps/np-fact-sheet. Updated March, 2015. Accessed March 26, 2015.
2013 Statistical profile of certified physician assistants: An annual report of the National
Commission on Certification of Physician Assistants. July, 2014. Available at
http://www.nccpa.net/Upload/PDFs/2013StatisticalProfileofCertifiedPhysicianAssistants-
AnAnnualReportoftheNCCPA.pdf.

3
• Why AHPs growing in numbers?
– Aging patient population
– Larger patient population through legislation
(Affordable Care Act)
– Number of new physicians not meeting demand
Allied Healthcare Professionals
Allied Healthcare Professionals
• Paid claims against physicians have fluctuated, but
reported paid claims against AHPs have steadily risen
Profession 1993 1998 2003 2008 2013
Physician (MD or
DO)
14,51
1
14,39
6
15,12
4
10,85
99,205
Nurse practitioner 90 119 172 263 299
Physician assistant 29 58 112 124 160
National Practitioner Data Bank. Generated using the Data Analysis Tool at
http://www.npdb.hrsa.gov/analysistool. March 25, 2015.
• Friction between physicians & nurses?
– IOM suggests NPs & nurses can fill missing
physician gap
– AMA immediate response - physicians have more
education & training
• Physician-led healthcare teams best
Allied Healthcare Professionals
The future of nursing: Leading change, advancing health. “Key Messages of the Report.” Pg. 21-
30. Washington, DC: The National Academies Press, 2011.
Patchin R. AMA Responds to IOM report on future of Nursing. American Medical Association
Web site. http://www.ama-assn.org/ama/pub/news/news/nursing-future-workforce.page.
October 5, 2010. Accessed March 26, 2015.
4
• Patient viewpoint?
– Small majority of patients prefer seeing a
physician (if given a choice)
• Numbers change depending on immediate availability
of physician, type of complaints, race, sex, & patient’s
socioeconomic status
Allied Healthcare Professionals
Dill M, Pankow S, Erikson C, Shipman S. Survey shows consumers open to a greater role for
physician assistants and nurse practitioners. Health Affairs. 2013;32(6):1135-1142.
• State specific
• Laws differ for NPs & PAs
• NPs typically require collaboration
• PAs require supervision
– Usually requires immediate availability of
physician (in-person, phone, or other
telecommunications method)
AHP Regulations
• Trend for NPs & PAs - more stringent on
entry into practice & less stringent on scope
of practice
• Compliance with state regulations does not
insulate AHP or physician working with AHP
from professional liability claims or
allegations
AHP Regulations (cont’d)
Gadbois E, Miller E, Tyler D, Intrator O. Trends in state regulation of nurse practitioners and
physician assistants, 2001 to 2010. Med. Care Res. Rev. April, 2015;72:200-219.

5
• AHP rarely sole defendant
• Risks for physicians
– Vicarious liability
– Negligent training/supervision
– Bad outcome for common patient
Medical Professional Liability
Failure to:
• Timely diagnose
• Timely refer to supervising/collaborating
physician or specialist
• Improper performance
Common Allegations - AHPs
• Assuming too much responsibility
• Inadequate supervision
• Absence of/deviation from written protocols
• Exceeding scope of authorized practice or
prescriptive authority
• Failure/delay in seeking collaboration or
referral
Liability Concerns

6
• True collaboration = more than having or
following agreement or protocol
• Review of care = more than signing-off on
documentation
• Encourage communication, collaboration &
questions
Risk Mitigation Strategies
Allied Healthcare
Professionals
Case Study 1
• 61YOM (5’10”, 163 lbs.) c/o abd pressure;
mild mid-sternal pain
– HTN, hypercholesterolemia, family hx MI
– Zestril, ASA, Viagra & Vitamin E
• Examined by PA
– BP 140/78, P 99, & R 16
– Normal physical exam
• Bowel sounds slightly ↑& tender to palp in
epigastric areas
AHP Case Study 1

7
• EKG: non-specific ST-T waves changes
– Compared to prior EKG - no acute changes
• Prevacid & return for lab work
• Supervising physician did not evaluate pt
– Concurred with PA’s EKG interpretation
Case Study 1 (cont’d)
• Wife awakened by agonal respirations
– Called 911 & began CPR
• Paramedics arrived
– Pulseless, apneic, no BP, pupils fixed & dilated
– Resuscitation unsuccessful
• Death certificate: COD - MI
Case Study 1 (cont’d)
• Multifocal CAD – 80-90% stenosis of LCX
– 80% multifocal stenosis of LAD
– 40-50% stenosis of RCA
– Slight LVH; no evidence of aneurysm
• Bilateral pulm congestion, negative for PE
• Acute gastritis, normal esophagus, small bowel & pancreas
• Diverticulosis of sigmoid & rectal colon
Autopsy Report

8
• Lawsuit filed against practice & physician
• Allegation:
– Failure to evaluate, dx, & treat heart disease
resulting in MI & death
• Discussion
• Outcome: __________________
Case Study 1 (cont’d)
Allied Healthcare
Professionals
Case Study 2
• 50YOF (5’7”, 220 lbs.) GYN exam by NP
– Smoking 30 yrs - 1 ppd, seizures, GERD, anxiety, gall bladder surgery, hysterectomy & HTN
– Tegretol, Premarin, Ativan, Maxzide, Pravachol, Adalat, & ketoprofen
• Normal BP & GYN exam
– Hemorrhoids
– R knee pain & swelling
– Reminder for annual GYN exam
AHP Case Study 2

9
• Complaints of rectal bleeding
– “On & off” blood on paper & in toilet
– Constipation, alternating with normal BMs, abd
pain, gas, bloating, & post-BM sensation
– BP 152/86, wt 234 lbs
• External & internal hemorrhoids
– Negative FOBT
• Assessment: hemorrhoids & IBS
AHP Case Study 2 (cont’d)
3 Months later
• Treated by GI for acid reflux
– Denied hematemesis, hematochezia, & melena
– Prilosec & follow-up in 6 months or earlier
AHP Case Study 2 (cont’d)
• Returned to NP c/o cysts on R wrist
– Dx - benign ganglion cyst: referred to surgeon
– Did not ask about hemorrhoids/rectal bleeding
• Presented to new physician for physical
– No complaints
– Colonoscopy & mammogram
AHP Case Study 2 (cont’d)

10
• Colonoscopy– Sigmoid mass consistent with Ca, multiple colon
polyps, diverticulosis, & suboptimal prep
• Biopsy– Moderately differentiated adenocarcinoma with
desmoplasia
– Adenomatous polyp with severe atypism
• CT – Low density nodule in L lower liver
– Consistent with cavernous hemangioma
– No definite tumor identified
AHP Case Study 2 (cont’d)
• Repeat colonoscopy
– Multiple polyps
– Rare diverticulosis
– Sigmoid colon mass at 15 cm
• Referred to general surgeon
– Resection of sigmoid colon & rectum
– Partial omentectomy
– Diverting transverse loop colostomy
AHP Case Study 2 (cont’d)
• Chemotherapy
• Lawsuit filed against NP & physician
– Delayed Dx of colon CA resulting in additional
surgery, tx & recurrence
• Discussion
• Outcome: ____________________
AHP Case Study 2 (cont’d)

11
• Patient fails to respond to treatment
• Unexplained physical findings
• Computer EKG interpretation differs from AHP’s interpretation
• EKGs performed due to symptoms
• Potentially serious or life-threatening conditions
• Emergencies after initial care
• Patient requests to see physician
Suggestions for Physician Consultation
• Familiarity with applicable state laws
• Verify AHP’s credentials upon hiring or
supervising/collaborating
– Recheck periodically
– Some states require annual review of
collaboration agreement
• Develop written collaborative care guidelines
Risk Mitigation Strategies
• Delegate functions/responsibilities
consistent with both physician’s & AHP’s
competence & expertise
• Periodically discuss AHP care with pts
– Ask for honest, constructive feedback
Risk Mitigation Strategies

12
• Survey private payers for their AHP reimbursement guidelines
• Schedule one-on-one time for AHP with physician
• Develop & document scheduling protocols for staff
• Load appointment parameters into schedule
• Instruct billing office to train AHP
• Marketing & communication plan to introduce AHP
• Include professional development into compensation
Suggestions When New AHPs
Join Your Practice
Toth C. Seven surefire ways to start a nonphysician practitioner off right. J Med Pract Manage.
2014;29(4):214-215.
Patient Portals
• Secure online website – 24 hr pt access to PHI
• Secure user name & password to access health info
• May allow pts to:– Exchange secure emails w/ clinicians
– Request Rx refills
– Make payments
– Schedule appointments
– Update contact info
– View ed materials
– Download/complete forms
What is a Patient Portal? (HealthIT.gov)
http://www.healthit.gov/providers-professionals/faqs/what-patient-portal

13
• 2009 American Recovery & Reinvestment
Act (ARRA)
• Main components of “Meaningful Use”
– Use certf’d EHR in meaningful manner
– Electronic exchange of health info―improve
quality of care
– Use certf’d EHR to submit quality/other
measures
Why Use a Patient Portal?
http://www.hrsa.gov/healthit/meaningfuluse/MU%20Stage1%20CQM/whatis.html
“Simply making services available doesn’t
cut it. Unless you are engaging patients you
won’t meet meaningful use requirements.
Messaging and other mechanisms need to
be part of your practice.”
http://www.kevinmd.com/blog/2013/04/build-patient-portal.html
• Stage 2 MU engagement requirements of
clinical summaries
– Pt-specific education resources
– Timely access to health info
– Reminders for preventive follow-up care, etc.
– Secure electronic messaging
Connection Between Portal & MU
How to optimize patient portals for patient engagement and meet meaningful use requirements:
National Learning Consortium Fact Sheet. HealthIT.gov Web site.
http://www.healthit.gov/sites/default/files/nlc_how_to_optimizepatientportals_for_patienteng
agement.pdf. May, 2013. Accessed February 12, 2015.

14
• What features/services will be offered?
• Plan for marketing, enrollment, training & pt
assistance
• Pilot test portal w/ clinicians at clinical sites
• Promote/facilitate portal use
• Develop P&Ps for response times
System Implementation
Health IT.gov National Learning Consortium Fact Sheet, May 2013
http://www.healthit.gov/sites/default/files/nlc_how_to_optimizepatientportals_for_patient
engagement.pdf
• Simplify process – register pts at clinic
• Educate pts re appropriate portal communications
• Engage pts w/ interactive decision tools,
personalized messages, etc.
• Offer all at once or phase-in
• ID pts that benefit most from portal use, e.g.,
chronic conditions
• Encrypt PHI
Ambulatory Settings System
Implementation (cont’d)
HealthIT.gov National Learning Consortium Fact Sheet, August 2012
http://www.healthit.gov/providers-professionals/implementation-resources/using-
patient-portals-ambulatory-care-settings-fact
• Assume portal info is discoverable
• Adopt P&Ps for pt portals
• Establish timeframes for messages
• Establish allowed subject
matter/transactions, e.g., Rx refills
• Confirm all “To” fields are correct before
sending
Physician/Pt Communication Guidelines
Haddad P. Patient portals: what physicians need to know. Michigan State Medical Society Legal
Alert, Health Law Update. November, 2011.

15
• Have pts create auto-reply to acknowledge
clinicians’ messages
• Have pts indicate transaction category in
subject line of message
• Create auto-reply to receipt of messages
• Retain electronic communications w/ pts
Physician/Pt Communication Guidelines
(cont’d)
Haddad P. Patient portals: what physicians need to know. Michigan State Medical Society Legal
Alert, Health Law Update. November, 2011.
• Use std block text at end of messages to pts
• Include clinician’s full name & contact info
• Emphasize importance of alternative
communication in emergencies
Physician/Pt Communication Guidelines
(cont’d)
Haddad P. Patient portals: what physicians need to know. Michigan State Medical Society Legal
Alert, Health Law Update. November, 2011.
• Beth Israel Deaconess Med Ctr, Geisinger
Health System, HarborView Med Ctr
– Does allowing pt access to clinical notes ↑ pt
engagement?
– 1st determined what want to make available
– Most open-notes environments start w/ basic pt
portal
– Add capabilities, including clinical notes
– Determine elements pts would benefit from seeing
Online Patient Portals:
“Unveiling the Doctor’s Note”
http://www.amednews.com/article/20121231/business/121239994/4/

16
• Suppress certain notes until phys talks to pt
• Consider tip sheets & ed sessions for clinicians
• Post launch – 82% physicians found notes
useful (↑5%)
• Most pts felt access was beneficial
Online Patient Portals:
“Unveiling the Doctor’s Note” (cont’d)
http://www.amednews.com/article/20121231/business/121239994/4/
• 82.6% pts felt more in control of their care
• 81% remembered care plan better
• 82% understood health condition better
• 71 % took better care of self
Online Patient Portals:
“Unveiling the Doctor’s Note” Results
http://www.amednews.com/article/20121231/business/121239994/4/
• 70% took meds more consistently
• 31% concerned re privacy
• 7% worried more
• 5% found notes more confusing than helpful
• 1.6% felt offended
Online Patient Portals:
“Unveiling the Doctor’s Note” (cont’d)
http://www.amednews.com/article/20121231/business/121239994/4/
Source: Inviting Patients to Read their Doctors’ Notes: A Quasi-experimental Study and a
Look Ahead.” Annals of Internal Medicine, Oct 2.
http://www.amednews.com/article/20121231/business/121239994/4/
17
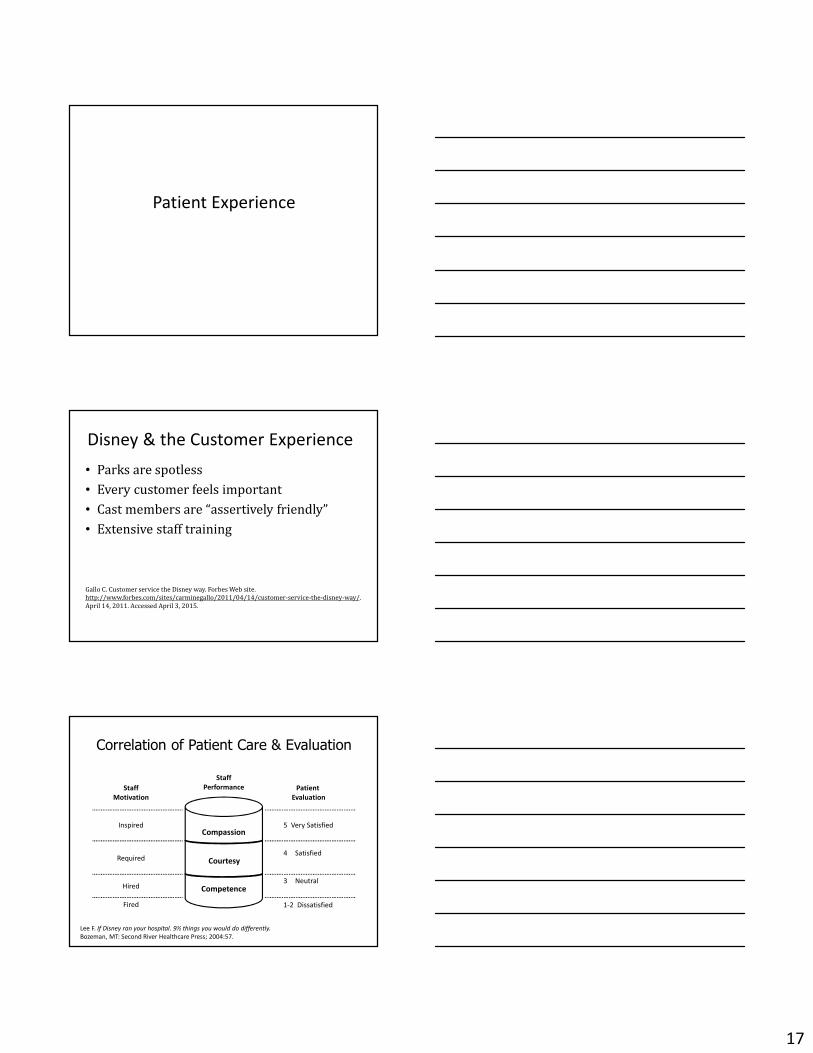
Patient Experience
• Parks are spotless
• Every customer feels important
• Cast members are “assertively friendly”
• Extensive staff training
Disney & the Customer Experience
Gallo C. Customer service the Disney way. Forbes Web site.
http://www.forbes.com/sites/carminegallo/2011/04/14/customer-service-the-disney-way/.
April 14, 2011. Accessed April 3, 2015.
Correlation of Patient Care & Evaluation
Competence
Courtesy
Compassion
Staff
Motivation
Inspired
Required
Hired
Fired
Staff
Performance Patient
Evaluation
5 Very Satisfied
4 Satisfied
3 Neutral
1-2 Dissatisfied
Lee F. If Disney ran your hospital. 9½ things you would do differently.
Bozeman, MT: Second River Healthcare Press; 2004:57.

18
• ↑ Reimbursement
• ↑ Reviews – more referrals
• ↑ Patient health?
Positive Patient Experience
• Higher pt satisfaction scores may
– Lower readmission rates
– Lower mortality
– Shorter LOS
– Lower inpatient mortality after acute MI
Patient Satisfaction May Promote Healing
ECRI, Risk Management News, Higher Patient Satisfaction Aligns with Higher Surgical Quality, Study
Finds, January 7, 2015 citing Tsai, Thomas C., Orav, E. John, Jha, Ashish K., Patient Satisfaction and
Quality of Surgical Care in US Hospitals, Annals of Surgery, January 2015, 261:1, p2-8.
Glickman, et al., Patient Satisfaction and Its Relationship with Clinical Quality and Inpatient
Mortality in Acute Myocardial Infarction, Circulation, 2010; 3:188-195, originally published online
February 23, 2010.
• Good communication facilitates:
– Pt understanding
– Builds trust
– Increases likelihood of agreement on treatment
• Increased confidence in your recommendations
– ↑ Compliance
– Improved self-care
Patient Satisfaction May Promote Healing

19
• ↑ Reimbursement
• ↑ Reviews – more referrals
• ↑ Patient health
• ↓Malpractice risk?
Positive Patient Experience
• What Prevents Lawsuits?
• Good patient outcomes
• Good patient experiences
• What Mitigates Lawsuits?
• Competent care
• Good documentation
Risk Management

20
“[R]isk is predicted by the practitioner’s
inability to communicate effectively and
establish and maintain rapport with patients,
especially in the face of an adverse event.”
Communication & Lawsuits
Hickson G, Jenkins AD. Identifying and addressing communication failures as a means of
reducing unnecessary malpractice claims. NC Med J. 2007;68(5):362-364.
Communication
• Assist physician if uncomfortable speaking to pt
• Talk in private area
– No interruptions
• Convey kindness, calmness, & empathy
• Start with open ended question
– “Tell me what’s going on”
– Listen without interruption
Angry Patients—Talking it Through
O’Brien J. The patient relationship and service recovery guide: A colorful approach to
handling upset and angry patients. Am J Orthop.2015;44(1):43-46.

21
• Acknowledge person’s feelings without accepting
or assigning blame
• Avoid becoming judgmental or defensive
• Once concern has been voice - ask what would it
take to resolve
– If issue can be resolved immediately – do it
– If not – look into it & follow up
• Provide your name & contact info for follow-up
Talking it Through (cont’d)
O’Brien J. The patient relationship and service recovery guide: A colorful approach to
handling upset and angry patients. Am J Orthop.2015;44(1):43-46.
• Surgeons with more dominant & less
concerned tone of voice were more likely to
have been sued
• Not just “what” you say, but also “how”
– Avoid dominance
– Sympathy
Surgeon’s Tone of Voice:
A Clue to Malpractice History
Surgeon’s Tone of Voice: A Clue to Malpractice History. Ambady et al., Surgery 2002.
• Eye contact
• Greet patient by name
• Sit down
• Empathize in difficult situations
• Get to know pt when possible
• Open ended questions
• Focus on conversation
• Factual & timely documentation
Patient Communication

22
• Communication � increased satisfaction
• Expressed satisfaction with process when
they “have the opportunity to express their
point of view fully and . . . the decision maker
is perceived as having listened to and
considered their side’s arguments.”
Learn From Convicted Felons?
Casper J. Tyler T. Fisher B. Procedural justice in felony cases. Law & Soc’y Rev.
1988;22(3):483-507.
• Make patients feel respected
• Use informed consent process to build
physician-patient relationship
• Let patients know you care about their
feedback
Improving Physician-Patient
Communication
Hickson G, Jenkins AD. Identifying and addressing communication failures as a means of
reducing unnecessary malpractice claims. NC Med J. 2007;68(5):362-364.
1. Provide clear recommendations - Most patients want clear and up-to-
date information about your recommended work-up and treatment plans.
2. Elicit patient beliefs/questions - Patients often have concerns or firm
beliefs that may hinder acceptance of your recommendations. Eliciting &
addressing these can relieve patient anxiety, promote acceptance of your
recommendations, and improve satisfaction with their visit.
3. Provide empathy, partnership and legitimation - Patients are more
likely to adhere to recommendations if they feel understood, supported and
included as a partner with their physicians.
4. Confirm agreement/overcome barriers - Finding common ground,
understanding the patient’s perspective and identifying and addressing
potential barriers will help you and your patient agree on a plan of action.
Key Skills for Choosing Wisely® Conversations
Choosing Wisely® is a registered trademark of ABIM Foundation.

23
Jury Expectations
Jury
The 4 Questions Jurors Ask
1. Whom can I trust in this lawsuit?
2. If I were in a medical crisis, would I be in
safe hands with this physician?
3. Under the circumstances, did the physician
do the best that he or she could?
4. Did the physician make the proper medical
decision?
Crawford L. Why winners win: decision making in medical malpractice cases.
J Am Orthop Surg. 2007;15(suppl 1):S70-S74.
Competence
Courtesy
Compassion
Patient
Evaluation
5 Very Satisfied
4 Satisfied
3 Neutral
1-2 Dissatisfied
Jury
Evaluation
Was the physician caring?
Did the physician do the
best for the patient under
the circumstances?
Is the physician competent?
Physician
Performance
(Adapted from) Lee F. If Disney ran your hospital. 9½ things you would do differently.
Bozeman, MT: Second River Healthcare Press; 2004:57.

24
New Reimbursement Models
Hospital Consolidations
Affordable Care Act
Physician Shortage
Physician Burnout
State Regulations
Obamacare
ACOs
EHRs
? ? ?
Physician↓
Patient
Less
Control
More
Control
Mini-Max Principal
The lowest level of performance by any
employee, allowed to continue without
corrective action, becomes the highest level
of performance that can be required of any
other employee in a similar position with
the employer.
Nelson R. Re-orient your practice from thinking “patient” to thinking “consumer.”
Presented at: ProAssurance Risk Resource conference; February 17, 2015; Tucson, AZ.
• Can they multitask successfully without getting angry
or frustrated easily?
• Are they able to actively listen to people, i.e. do they
take the time? Are they defensively preparing
responses before hearing the issue? Do they care about
your client population?
• Do conditions enable staff to work easily & efficiently?
• What staff are located in the front? What staff are
located in the back?
First Points of Contact
Nelson R. Re-orient your practice from thinking “patient” to thinking “consumer.”
Presented at: ProAssurance Risk Resource conference; February 17, 2015; Tucson, AZ.

25
• Interference
• Repetitive inefficiency
• Incommunicado
• Appointment delays
• Office waits
• Rudeness
Director of First Impressions
Nelson R. Re-orient your practice from thinking “patient” to thinking “consumer.”
Presented at: ProAssurance Risk Resource conference; February 17, 2015; Tucson, AZ.
• Name one thing about today’s visit that could be
improved, what would it be?
– Make it easier to get appointment
– Waiting time
– Friendlier physicians
– Friendlier nurses
– Friendlier staff
– Improved parking
– Telephone service
One Question Survey
74
Nelson R. Re-orient your practice from thinking “patient” to thinking “consumer.”
Presented at: ProAssurance Risk Resource conference; February 17, 2015; Tucson, AZ.
• Medical practice is increasingly complex
• Think patients as consumers
• Destination—excellent customer service
• It’s important to think how we get there
– Training
– Teamwork
– Tools
– Patient communication
Concluding Thoughts

INDIANA PHYSICIAN ASSISTANTS
Disclaimer: This information is provided for general guidance and should not be considered legal advice. Laws in this area are evolving and may have changed since this information was compiled. Please contact your local legal counsel for the most up-to-date information regarding the practice of Physicians Assistants in Indiana.
Definition A PA must meet the qualifications for licensure; including graduating from an approved PA or surgical assistant program, passing the certifying exam, and maintaining National Commission on Certification of Physician Assistants certification. (IC § 25-27.5-2-10) (844 IAC § 2.2-1-5) Scope of Practice A PA must engage in a dependent practice with physician supervision. A PA may perform, under the supervision of the supervising physician, the duties and responsibilities that re delegated by the supervising physician and that are within the supervising physician’s scope of practice, including prescribing and dispensing drugs (except for Schedule I controlled substances (IC § 25-27.5-5-4)) and medical devices. A patient may elect to be see, examined, and treated by the supervising physician (IC §25-27.5-5-2) PA shall notify supervising physician immediately if the PA determines that a patient should be seen by a physician. The supervising physician must then schedule a patient exam in a timely manner, or arrange for another physician to see the patient. (IC § 25-27.5-5-2) A PA is the agent of the supervising physician in the performance of all practice-related activities (IC § 25-27.5-5-3) It is the obligation of each team of a physician and PA to ensure that:
• the PA’s scope of practice is identified; • that the delegation of medical tasks is appropriate to the PA’s level of competence and
within the supervising physician’s scope of practice; and • that the relationship with, and access to the supervising physician is defined.
(IC § 25-27.5-6-3) The supervising physician may delegate to a PA the authority to provide volunteer work, including charitable work and migrant health care. (IC § 25-27.5-6-6) Prescribing
• A PA may prescribe, dispense, and administer drugs and medical devices to the extent delegated by the supervising physician. A PA may prescribe controlled substances if; he/she has practiced for at least one (1) year after graduating, and practiced for at least 1800 hours.
• A PA may request, receive, and sign for professional samples that are within the PA’s delegated prescribing privileges.
• A PA must document at least 30 contact hours of pharmacology from a committee approved educational program to prescribe drugs.
• A PA may not prescribe, administer, or monitor general anesthesia, regional anesthesia, or deep sedation. A PA may administer moderate sedation in limited circumstances, as outlined by the Board.
Updated April 20, 2015

• A PA may not prescribe or dispense ophthalmic devices. (IC § 25-27.5-5-4) All prescribing authority must be expressly delegated in writing by the supervising physician, in the supervisory agreement. The writing must include the drugs or classes or drugs that the PA may prescribe, as well as the protocols the PA must follow when prescribing. A physician may delegate to the PA the authority to prescribe only those medications that are within the physician’s scope of practice. (IC § 25-27.5-5-6) (844 IAC § 2.2-1.1-16) Controlled Substances Prescribing
• A PA may not prescribe more than a 30-day supply of controlled substances, and a physician must issue any refills for the initial prescription.
• A PA prescribing controlled substances must obtain both Indiana and DEA controlled substance registrations. When completing a prescription, a PA must include their signature, “PA-C,” state license number, and DEA number. (IC § 25-27.5-5-6)
Licensing application requirements are located at (844 IAC § 2.2-2-1) Supervision
• Supervision means that a physician or physician designee is overseeing the activities of, and accepting responsibility for, medical services rendered by a PA, and: o The supervising physician or the physician designee is physically present at the location
where the PA performs services, OR o The supervising physician or designee is immediately available for consultation via
telecommunication and available to see the patient within 24 hours if requested, AND is within a reasonable travel distance from the facility to personally ensure proper care.
• Supervision also includes the use of protocols, guidelines, and standing orders developed or approved by the supervising physician. (IC § 25-27.5-2-14)
A physician may not supervise more than two PAs. (IC § 25-27.5-6-2) Supervision by the physician or the physician designee must be continuous but it does not require the physical presence of the physician. (IC § 25-27.5-6-1) The supervising physician and the PA must maintain a written supervisory agreement, signed by the supervising physician(s) and the PA that:
• includes the tasks delegated to the PA; • describes the supervisory plan for the PA, including emergency procedures that the PA must
follow; • specifies the names of the drug or drug classification and medical devices the PA is
delegated to prescribe and the protocol the PA shall follow in prescribing a drug; • includes the name, address, and phone number of the supervising physician(s); and • includes a description of the setting or settings in which the PA will be working. (IC § 25-27.5-5-2) (844 IAC § 2.2-1.1-16)
A PA’s supervisory agreement must be submitted to the Board and include all of the tasks being delegated by the supervising physician. (IC § 25-27.5-5-2(F)) A supervising physician may temporarily designate responsibility for the supervision of a PA to a physician designee for when the supervising physician is unavailable. (IC § 25-27.5-2-11)
Updated April 20, 2015

Chart review The supervising physician or the physician designee shall review charts within 72 hours as follows:
o First year of PA practice, 100%. o Second year of PA practice, 50%. o Third year of PA practice, and thereafter 25%. o This schedule resets only if the PA changes specialty. (IC § 25-27.5-6-1)
Physician registration (844 IAC § 2.2-2-2) The supervising physician must register his or her intent to supervise a PA to the board on a board-approved form. The following information must be contained on the form:
• Name, business address, and telephone number of the supervising physician; • Name business address, telephone number, and certification number of the PA; • Current license number of the physician; • A statement that the physician will not be supervising more than two PAs; • A description of the setting in which the PA will practice, including specialty where
applcicable; • A statement that the supervising physician:
o Will exercise continuous supervision over the PA; o Shall review all patient encounters maintained by the PA within 24 hours after the
PA has seen a patient; o At all times retain professional and legal responsibility for the care rendered by the
PA; and • A detailed description of the performance evaluation process.
The supervising physician must notify the board within 15 days of the termination of the supervisory relationship. The notification must provide the reason for the termination. Identification A PA must wear a nametag identifying the individual as a PA while they are engaged in professional activities. A PA must also inform patients that he or she is a PA. A PA shall not portray himself or herself as a licensed physician. A PA’s current license must be available for inspection at the primary place of business. (IC § 25-27.5-5-5) (844 IAC § 2.2-2-5) Physician liability A supervising physician must submit a statement to the board that the physician retains professional and legal responsibility for the care rendered by the PA. (IC § 25-27.5-6-4(3)) If a PA is an employee of a physician, physician group, or other legal entity, the PA remains the legal responsibility of the supervising physician, this includes when the PA provides care in a facility. If a PA is a facility employee, the supervising physician has legal responsibility for PA’s actions. (IC § 25-27.5-6-7)
Updated April 20, 2015
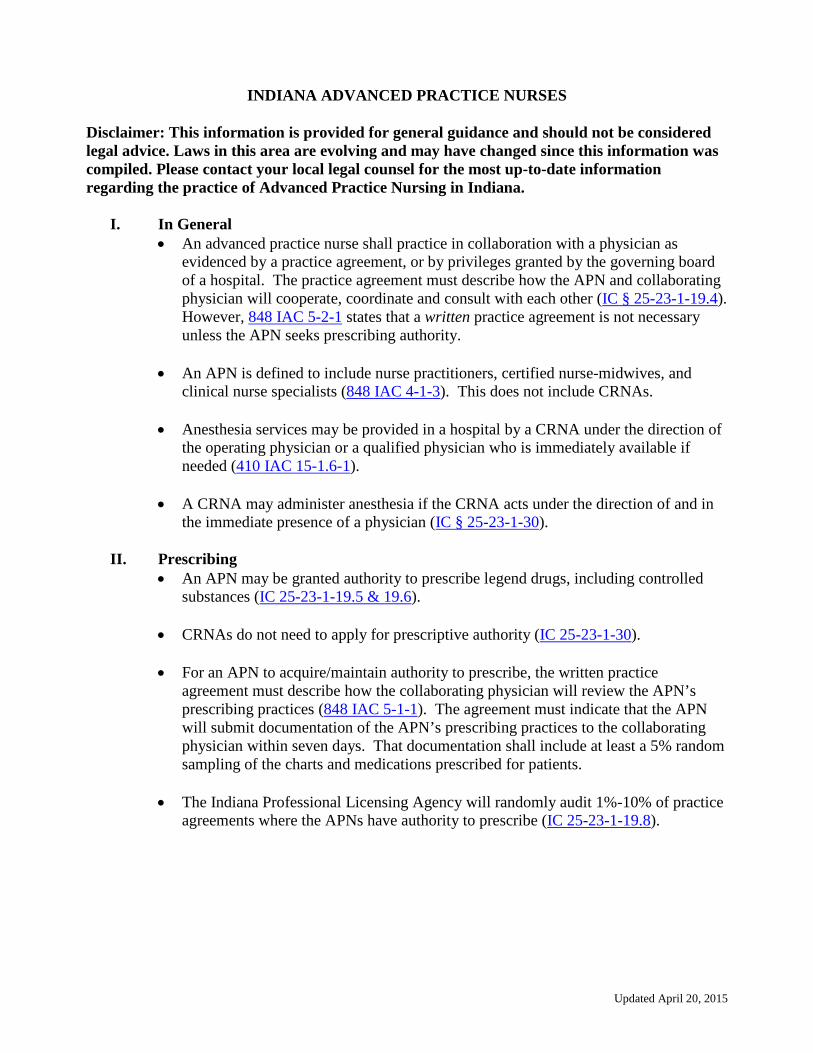
INDIANA ADVANCED PRACTICE NURSES
Disclaimer: This information is provided for general guidance and should not be considered legal advice. Laws in this area are evolving and may have changed since this information was compiled. Please contact your local legal counsel for the most up-to-date information regarding the practice of Advanced Practice Nursing in Indiana.
I. In General • An advanced practice nurse shall practice in collaboration with a physician as
evidenced by a practice agreement, or by privileges granted by the governing board of a hospital. The practice agreement must describe how the APN and collaborating physician will cooperate, coordinate and consult with each other (IC § 25-23-1-19.4). However, 848 IAC 5-2-1 states that a written practice agreement is not necessary unless the APN seeks prescribing authority.
• An APN is defined to include nurse practitioners, certified nurse-midwives, and
clinical nurse specialists (848 IAC 4-1-3). This does not include CRNAs. • Anesthesia services may be provided in a hospital by a CRNA under the direction of
the operating physician or a qualified physician who is immediately available if needed (410 IAC 15-1.6-1).
• A CRNA may administer anesthesia if the CRNA acts under the direction of and in
the immediate presence of a physician (IC § 25-23-1-30).
II. Prescribing • An APN may be granted authority to prescribe legend drugs, including controlled
substances (IC 25-23-1-19.5 & 19.6).
• CRNAs do not need to apply for prescriptive authority (IC 25-23-1-30).
• For an APN to acquire/maintain authority to prescribe, the written practice agreement must describe how the collaborating physician will review the APN’s prescribing practices (848 IAC 5-1-1). The agreement must indicate that the APN will submit documentation of the APN’s prescribing practices to the collaborating physician within seven days. That documentation shall include at least a 5% random sampling of the charts and medications prescribed for patients.
• The Indiana Professional Licensing Agency will randomly audit 1%-10% of practice
agreements where the APNs have authority to prescribe (IC 25-23-1-19.8).
Updated April 20, 2015


















