Chang 2001
4
76 5. Gherardi R, Gray F, Poirier J. Neurinomes et neurofibromes, t~lt- ments histologiques distinctifs. Arch Anat Cytol Pathol 1985; 33: 297-301. 6. Le Viet D, Lantieri L, Loy S. Tumeurs extirpables des nerfs ptriphtriques. Ann Chir Plast Esthet 1993; 38: 172-9. 7. White W, Shiu MH, Rosenblum MK, Erlandson RA, Woodruff JM. Cellular schwannoma. A clinicopathologic study of 57 patients and 58 tumors. Cancer 1990; 66: 1266-75. 8. Carstens PH, Schrodt GR. Malignant transformation of a benign encapsulated neurilemoma. Am J Clin Pathol 1969; 51: 144-9. 9. Harrison DH, Morgan BD. The instep island flap to resurface plan- tar defects. Br J Plast Surg 1981; 34: 315-18. 10. Eren S, Matejic B, Hettich R. Indication, technique, and results of plantaris medialis neurovascular island flaps. Ann Plast Surg 1992; 28: 152-9. 11. Evans GRD, Robb GL. Cutaneous foot malignancies: outcome and options for reconstruction. Ann Plast Surg 1995; 34: 396-401. 12. Shanahan RE, Gingrass RP. Medial plantar sensory flap for cover- age of heel defects. Plast Reconstr Surg 1979; 64: 295-8. 13. Masquelet AC, Romana MC. The medialis pedis flap: a new fascio- cutaneous flap. Plast Reconstr Surg 1990; 85: 765-72. 14. Hayashi A, Maruyama Y. Lateral calcaneal V-Y advancement flap for repair of posterior heel defects. Plast Reconstr Surg 1999; 103: 577-80. 15. Gumener R, Zbrodowski A, Montandon D. The reversed fasciosub- cutaneous flap in the leg. Plast Reconstr Surg 1991; 88:1034-41. British Journal of Plastic Surgery 16. Jeng SE Wei FC. Distally based sural island flap for foot and ankle reconstruction. Plast Reconstr Surg 1997; 99: 744-50. 17. De Sofas X, Torossian JM, Perez Ortiz N, Guinard D, Moutet E Le lambeau neuro-cutan6 de nerf saph~ne externe. Ann Chit Plast Esthet 1996; 41: 121-6. The Authors J. M. Torossian MD, Chief Resident J. L. Beziat MD, Professor, Head Department of Plastic and Maxillofacial Surgery, M. Salle MD, Chief Resident Department of Anatomy and Cytopathology, Htpital de la Croix-Rousse, 103 Grande-Rue de la Croix-Rousse, 69317 Lyon Cedex 04, France. 17. Augey MD, Head Department of Dermatology, Centre Hospitalier 'Lucien Hussel', BP 127, 38209 Vienne Cedex, France. Correspondence to Dr J. M. Torossian. Paper received 2 June 1999. Accepted 24 November 1999. British Journal of Plastic Surgery (2001), 54 2001 The British Association of Plastic Surgeons doi: 10.1054/bjps.2000.3482 A challenging treatment for an ischaemic ulcer in a patient with Buerger's disease: vascular reconstruction and local flap coverage H. Chang, T. Hasegawa*, K. Motekit and K. Ishitobit Department of Plastic and Reconstructive Surgery, Kyorin University School of Medicine; *Department of Plastic and Reconstructive Surgery and t Vascular Surgery, Tokyo Saiseikai Central Hospital, Tokyo, Japan SUMMARY. An ischaemic heel ulcer in a patient with Buerger's disease was reconstructed using an in situ saphenous vein graft combined with a local flap. The bypass was sufficient to restore blood supply to the ischaemic limb but a flap was necessary to cover the persistent heel ulcer, which remained after revascularisation. One month after bypass surgery the ulcer was debrided and the resulting defect was covered with a lateral supramalleolar flap. The postopera- tive course was uneventful and the flap donor site healed well. When treating ischaemic ulcers in a patient with Buerger's disease, vascular reconstruction should be considered first in order to salvage the limb. After revascularisa- tion, a local flap can be used to cover a persistent defect but very few local flaps have been reported. This report is the first published case of successful local flap transfer after bypass surgery in a patient with Buerger's disease. We think that a local flap is one possible treatment for a non-healing ulcer after revascularisation. 2001 The British Association of Plastic Surgeons Keywords: Buerger's disease, ischaemic ulcer, in situ saphenous vein graft, revascularisation, local flap. Case report A 63-year-old woman was referred to us for wound coverage. She had been diagnosed with Buerger's disease at the age of 62. There was no evidence of diabetes, hyperlipidaemia or hyperten- sion and she did not smoke. At the time of admission, she pre- sented with painful ulceration and calcaneal-bone exposure on the left heel (Fig. 1). The toes were cold and pale but there was Presented in part at the 40th Annual Meeting of the Japan Society of Plastic and Reconstructive Surgery, Miyazaki City, Japan, April 1997, and at the 67th Anniversary Scientific Meeting of ASPRS, PSEF and ASMS, Boston, MA, USA, October 1998. no sign of gangrene or ulceration. Previously, she had undergone left lumbar sympathectomy, which reduced the wound pain, but the size of the ulcer increased. Preoperative digital subtraction angiography revealed segmental defects of the anterior and pos- terior tibial arteries. Blood supply to the distal arteries was by collateral vessels that showed a 'corkscrew' appearance (Fig. 2). There was no evidence of arteriosclerotic lesions such as calcifi- cation of the vessel wall. She underwent careful debridement of the heel ulcer but growth of granulation tissue was not adequate for wound coverage. Two of the infrapopliteal arteries were occluded but distal run-off was fair. Femorocrural bypass was indicated to salvage the limb and provide effective healing of the ischaemic ulcer.
-
Upload
edhobiondi -
Category
Documents
-
view
283 -
download
1
description
med
Transcript of Chang 2001
-
76
5. Gherardi R, Gray F, Poirier J. Neurinomes et neurofibromes, t~lt- ments histologiques distinctifs. Arch Anat Cytol Pathol 1985; 33: 297-301.
6. Le Viet D, Lantieri L, Loy S. Tumeurs extirpables des nerfs ptriphtriques. Ann Chir Plast Esthet 1993; 38: 172-9.
7. White W, Shiu MH, Rosenblum MK, Erlandson RA, Woodruff JM. Cellular schwannoma. A clinicopathologic study of 57 patients and 58 tumors. Cancer 1990; 66: 1266-75.
8. Carstens PH, Schrodt GR. Malignant transformation of a benign encapsulated neurilemoma. Am J Clin Pathol 1969; 51: 144-9.
9. Harrison DH, Morgan BD. The instep island flap to resurface plan- tar defects. Br J Plast Surg 1981; 34: 315-18.
10. Eren S, Matejic B, Hettich R. Indication, technique, and results of plantaris medialis neurovascular island flaps. Ann Plast Surg 1992; 28: 152-9.
11. Evans GRD, Robb GL. Cutaneous foot malignancies: outcome and options for reconstruction. Ann Plast Surg 1995; 34: 396-401.
12. Shanahan RE, Gingrass RP. Medial plantar sensory flap for cover- age of heel defects. Plast Reconstr Surg 1979; 64: 295-8.
13. Masquelet AC, Romana MC. The medialis pedis flap: a new fascio- cutaneous flap. Plast Reconstr Surg 1990; 85: 765-72.
14. Hayashi A, Maruyama Y. Lateral calcaneal V-Y advancement flap for repair of posterior heel defects. Plast Reconstr Surg 1999; 103: 577-80.
15. Gumener R, Zbrodowski A, Montandon D. The reversed fasciosub- cutaneous flap in the leg. Plast Reconstr Surg 1991; 88:1034-41.
British Journal of Plastic Surgery
16. Jeng SE Wei FC. Distally based sural island flap for foot and ankle reconstruction. Plast Reconstr Surg 1997; 99: 744-50.
17. De Sofas X, Torossian JM, Perez Ortiz N, Guinard D, Moutet E Le lambeau neuro-cutan6 de nerf saph~ne externe. Ann Chit Plast Esthet 1996; 41: 121-6.
The Authors
J. M. Torossian MD, Chief Resident J. L. Beziat MD, Professor, Head
Department of Plastic and Maxillofacial Surgery,
M. Salle MD, Chief Resident
Department of Anatomy and Cytopathology, Htpital de la Croix-Rousse, 103 Grande-Rue de la Croix-Rousse, 69317 Lyon Cedex 04, France.
17. Augey MD, Head
Department of Dermatology, Centre Hospitalier 'Lucien Hussel', BP 127, 38209 Vienne Cedex, France.
Correspondence to Dr J. M. Torossian.
Paper received 2 June 1999. Accepted 24 November 1999.
British Journal of Plastic Surgery (2001), 54 9 2001 The British Association of Plastic Surgeons doi: 10.1054/bjps.2000.3482
A challenging treatment for an ischaemic ulcer in a patient with Buerger's disease: vascular reconstruction and local flap coverage
H. Chang, T. Hasegawa*, K. Motek i t and K. Ishitobit
Department of Plastic and Reconstructive Surgery, Kyorin University School of Medicine; *Department of Plastic and Reconstructive Surgery and t Vascular Surgery, Tokyo Saiseikai Central Hospital, Tokyo, Japan
SUMMARY. An ischaemic heel ulcer in a patient with Buerger's disease was reconstructed using an in situ saphenous vein graft combined with a local flap. The bypass was sufficient to restore blood supply to the ischaemic l imb but a flap was necessary to cover the persistent heel ulcer, which remained after revascularisation. One month after bypass surgery the ulcer was debrided and the resulting defect was covered with a lateral supramalleolar flap. The postopera- tive course was uneventful and the flap donor site healed well. When treating ischaemic ulcers in a patient with Buerger's disease, vascular reconstruction should be considered first in order to salvage the limb. After revascularisa- tion, a local flap can be used to cover a persistent defect but very few local flaps have been reported. This report is the first published case of successful local flap transfer after bypass surgery in a patient with Buerger's disease. We think that a local flap is one possible treatment for a non-healing ulcer after revascularisation. 9 2001 The British Association of Plastic Surgeons
Keywords: Buerger's disease, ischaemic ulcer, in situ saphenous vein graft, revascularisation, local flap.
Case report
A 63-year-old woman was referred to us for wound coverage. She had been diagnosed with Buerger's disease at the age of 62. There was no evidence of diabetes, hyperlipidaemia or hyperten- sion and she did not smoke. At the time of admission, she pre- sented with painful ulceration and calcaneal-bone exposure on the left heel (Fig. 1). The toes were cold and pale but there was
Presented in part at the 40th Annual Meeting of the Japan Society of Plastic and Reconstructive Surgery, Miyazaki City, Japan, April 1997, and at the 67th Anniversary Scientific Meeting of ASPRS, PSEF and ASMS, Boston, MA, USA, October 1998.
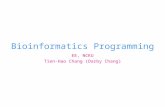
no sign of gangrene or ulceration. Previously, she had undergone left lumbar sympathectomy, which reduced the wound pain, but the size of the ulcer increased. Preoperative digital subtraction angiography revealed segmental defects of the anterior and pos- terior tibial arteries. Blood supply to the distal arteries was by collateral vessels that showed a 'corkscrew' appearance (Fig. 2). There was no evidence of arteriosclerotic lesions such as calcifi- cation of the vessel wall. She underwent careful debridement of the heel ulcer but growth of granulation tissue was not adequate for wound coverage.
Two of the infrapopliteal arteries were occluded but distal run-off was fair. Femorocrural bypass was indicated to salvage the limb and provide effective healing of the ischaemic ulcer.
-
Lipomatosis of the parotid gland in a child 77
ligated AVI
unligated A'
Figure 1--Ulceration of the left heel of a 63-year-old woman. Part of the calcaneal bone was exposed.
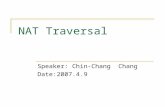
Figure 3--Diagram of the femoroposterior tibial bypass surgery using an in situ saphenous vein graft (ISVG). The superficial femoral artery and all of the infrapopliteal arteries are occluded but distal run-off is fair. Femoral to posterior tibial artery and dorsalis pedis artery bypasses were performed. (FA: femoral artery; DFA: deep femoral artery; SFA: superficial femoral artery; AVF: arteriovenous fistula; PA: peroneal artery; ATA: anterior tibial artery; PTA: posterior tibial artery.)
Figure 2---Preoperative digital subtraction angiogram of the left lower extremity of a 63-year-old woman, showing typical findings of Buerger's disease. The anterior and posterior tibial arteries have seg- mental occlusions. The distal arteries are visualised by collateral ves- sels that show a "corkscrew' appearance.
Revascularisation consisted of bypass from the femoral artery to the dorsalis pedis artery and the posterior tibial artery using an in situ saphenous vein graft. In the in situ saph'enous vein graft technique, the ipsilateral great saphenous vein is used to bypass the distal arteries (Fig. 3). The great saphenous vein and the femoral vessels were exposed through a groin incision and the great saphenous vein was divided at the femorosaphenous junc- tion. The proximal valves were incised using valve scissors under direct vision. The outflow arteries, the posterior tibial and dor- salis pedis arteries, were prepared for graft anastomosis through a separate incision. The proximal saphenous vein was anasto- mosed end-to-side to the patent femoral artery. The distal saphe- nous vein and outflow arteries were exposed for anastomosis.
The remaining valves in the saphenous vein were incised with a valvulotome via the distal transected vein. Active blood flow from the graft was confirmed. The graft was anastomosed end- to-side to the dorsalis pedis artery and a branch of the graft was anastomosed to the posterior tibial artery. When both proximal and distal anastomoses were completed, most tributaries of the graft, arteriovenous fistulae, were identified by Doppler and lig- ated under direct vision. Finally, the patency of the outflow arteries was confirmed by Doppler.
Four days postoperatively, the graft to the dorsalis pedis artery was occluded but the bypass to the posterior tibial artery was patent. After vascular reconstruction, the heel ulcer showed good wound healing with fair growth of granulation tissue, but the calcaneal bone was not covered completely.
One month postoperatively the heel ulcer was not completely healed and the calcaneal bone was still exposed. Surgical debridement was performed and the resulting defect measured 4 x 4 cm. A lateral supramalleolar flap was planned to cover the soft tissue defect (Fig. 4). The perforator of the peroneal artery was identified about 5 cm above the lateral malleolus and the flap was transferred to the heel defect by a 180 ~ rotation (Fig. 5). Most of the donor defect was closed primarily and a small split- thickness skin graft was applied to the remainder.
The postoperative course was uneventful and the donor site healed well. The patient had no wound problems in the follow- ing 2 years and currently ambulates without difficulty (Fig. 6).
-
78 British Journal of Plastic Surgery
Figure 4--Marking of the lateral supramalleolar flap. The flap transfer was performed 1 month after vascular reconstruction. Pulsation of the nutrient vessel, and the perforator of the posterior peroneal artery, were confirmed about 5 cm above the lateral malleolus by Doppler.
Discussion
Buerger's disease or thromboangiitis obliterans is a rare peripheral vascular disease that is defined as a segmental, inflammatory and obliterative disease of medium-sized and small arteries, t-4 The clinical criteria for diagnosis of Buerger's disease are smoking history, onset before the age of 50 years, infrapopliteal arterial occlusive lesions, upper limb involvement or phlebitis migrans and absence of atheroscterotic risk factors. Angiographic findings, such as tapering or abrupt occlusion of peripheral arteries and the corkscrew appearance of collaterals, serve as sup- porting evidence. 3,4 In our case, the patient was a non- smoker and had late onset, but in all other respects her clinical manifestations and the digital subtraction angio- graphy findings fit the diagnosis of Buerger's disease well.
The common initial symptom of Buerger's disease is an ischaemic ulcer in the lower limb) These ulcers are commonly accompanied by severe pain and usually prove intractable to medical therapy. Once conservative treat- ments, such as abstinence from smoking, nerve block or medication, fail, surgical procedures such as sympathec- tomy or amputation may be necessary.
In patients with Buerger's disease, coverage of lower extremity defects is complicated by poor local vascularity. Spontaneous healing by formation of granulation tissue is often limited and the use of skin grafts or local flaps for wound closure is restricted. Free flaps can provide immediate soft tissue coverage and neovascularisation, 5
Figure 5--The insetting of the flap. The flap was rotated by 180 ~ about the pedicle.
but acceptable recipient vessels for microvascular anasto- moses are difficult to find in these ischaemic limbs.
In atherosclerotic patients with ischaemic lesions, the use of a bypass graft for free flap transfer has been encouraged. 6-8 Vascular bypass surgery can improve limb ischaemia by increasing arterial perfusion, which improves wound healing and makes it more likely that suitable recipient vessels for the flaps can be found. The role of vascular bypass surgery in patients with Buerger's disease remains controversial because of the high inci- dence of graft failure. 3'9 However, in selected cases where a preoperative angiogram shows fair run-off and bypass surgery can provide blood flow to the distal lower extrem- ity, revascularisation is indicated to salvage the limb. 3'4'9 After revascularisation, spontaneous healing of ulcers may occur and skin-graft coverage of granulation tissue may be possible, but flap surgery is necessary in most cases. Blood flow in the revascularised lower extremity usually stabilises several weeks after bypass surgery. Here, the bypass surgery was successful except for early postoperative occlusion of the graft to the dorsalis pedis artery. Perfusion of the ischaemic limb became stable, but growth of granulation tissue over the exposed calcaneal bone was not sufficient for skin grafting a month after revascularisation. Since we considered that early dis- charge from hospital was desirable for the patient, wound coverage with a flap transfer was performed.
Several surgical modalities have been reported for the treatment of non-healing ulcers in patients with Buerger's disease including saphenous vein grafts, 9,1~ omental
-
Lipomatosis of the parotid gland in a child 79
raised. In this case, however, the flap did not show any congestion.
We consider that limb salvage with an in situ saphe- nous vein bypass graft followed by secondary local flap reconstruction is a valuable alternative in selected cases of Buerger's disease.
Figure 6~Sofi-tissue contour of the heel, 2 years postoperatively.
grafts 11,12 and free muscle flaps without bypass. 5 A con- ventional cross leg flap 13 may be an alternative but it has disadvantages such as donor site morbidity and decreased quality of life for the patient. To our knowledge, this is the first described case of 'local flap' reconstruction of an ischaemic ulcer after revascularisation in a patient with Buerger's disease. The use of a local flap should be con- sidered carefully because of donor site morbidity and the unreliability of flap nutrition even after bypass surgery. The authors were able to use the supramalleolar flap 14 because the preoperative angiogram showed a patent posterior peroneal artery and strong pulsation of its perforating branch was confirmed by Doppler after revas- cularisation.
By comparison with the conventional reverse vein graft, the in situ saphenous vein graft provides improved long-term patency. 15 We believe that in this case the in situ saphenous vein graft provided sufficient blood flow to the nutrient vascular pedicle of the flap as well as to the ischaemic limb. After the bypass surgery, pulsation of the distal arteries was confirmed and the growth of gran- ulation tissue over the ulcer increased. In addition, stronger pulsation of the feeding artery to the flap, the perforating branch of the peroneal artery, was confirmed by postoperative Doppler study, which enabled us to plan the flap transfer. Unligated arteriovenous fistulae can help the bypass graft remain patent by maintaining con- tinuous blood flow through the graft. On the other hand, the venous pressure of the revascularised leg can be ele- vated by shunt flow through the arteriovenous fistulae and venous congestion is possible when local flaps are
References
1. Mishima Y. Thromboangiitis obliterans (Buerger's disease). Int J Cardiol 1996; 54(Suppl.): S 185-7.
2. Suzuki S, Yamada I, Himeno Y. Angiographic findings in Buerger disease. Int J Cardiol 1996; 54(Suppl.): S189-95.
3. Shionoya S. Buerger's disease: diagnosis and management. Cardiovasc Surg 1993; 1: 207-14.
4. Shionoya S. Buerger's disease (thromboangiitis obliterans). In Rutherford RB, ed. Vascular Surgery. 4th ed. Philadelphia: WB Saunders, 1989: 235-45.
5. Van Landuyt K, Monstrey S, Tonnard P, Vermassen E Free flap coverage of a gangrenous forefoot in a patient with Buerger's disease: a case report. Ann Hast Surg 1996; 36: 154-7.
6. Dabb RW, Davis RM. Latissimus dorsi free flaps in the elderly: an alternative to below-knee amputation. Hast Reconstr Surg 1984; 73: 633-40.
7. Colen LB. Limb salvage in the patient with severe peripheral vas- cular disease: the role of microsurgical free-tissue transfer. Plast Reconstr Surg 1987; 79: 389-95.
8. Ciresi KF, Anthony JP, Hoffman WY, Bowersox JC, Reilly LM, Rapp JM. Limb salvage and wound coverage in patients with large ischemic ulcers: a multidisciplinary approach with revascu- larization and free tissue transfer. J Vasc Surg 1993; 18: 648-55.
9. Sasajima T, Kubo Y, Izumi Y, Inaba M, Goh K. Plantar or dorsalis pedis artery bypass in Buerger's disease. Ann Vasc Surg 1994; 8: 248-57.
10. Sasajima T, Kubo Y, Inaba M, Goh K, Azuma N. Role of infra- inguinal bypass in Buerger's disease: an eighteen-year experience. Eur J Vasc Endovasc Surg 1997; 13: 186-92.
11. Talwar S, Jain S, Porwal R, Laddha BL, Prasad P. Free versus pedicled omental grafts for limb salvage in Buerger's disease. Aust N Z J Surg 1998; 68: 38-40.
12. Singh I, Ramteke VK. The role of omental transfer in Buerger's disease: New Delhi's experience. Aust N Z J Surg 1996; 66: 372-6.
13. Yoshimura M, Shimada T, Matsuda M, Hosokawa M, Imura S. A new method for repairing skin defects of the lower leg under unsatisfactory conditions: utilization of peroneal island flap from the opposite sound leg. Plast Reconstr Surg 1990; 85: 123-6.
14. Masquelet AC, Beveridge J, Romana C, Gerber C. The lateral supramalleolar flap. Plast Reconstr Surg 1988; 81: 74-81.
15. Bergamini TM, Towne JB, Bandyk DF, Seabrook GR, Schmitt DD. Experience with in situ saphenous vein bypasses during 1981 to 1989: determinant factors of long-term patency. J Vasc Surg 1991; 13: 137-49.
The Authors
Hak Chang MD, Plastic Surgeon
Department of Plastic and Reconstructive Surgery, Kyorin University School of Medicine, 6-20-2 Shinkawa, Mitaka City, Tokyo 181-8611, Japan.
Tokio Hasegawa MD, Plastic Surgeon, Department of Plastic and Reconstructive Surgery Katsuhiko Moteki MD, Vascular Surgeon, Department of Vascular Surgery Kozo Ishitobi MD, Vascular Surgeon, Department of Vascular Surgery
Tokyo Saiseikai Central Hospital, 1-4-17 Mita, Minatoku, Tokyo 108-0073, Japan.
Correspondence to Hak Chang MD.
Paper received 28 March 2000. Accepted 25 September 2000, after revision.