Challenging Cases in Cancer: Early Breast Cancer Clifford A. Hudis, MD Chief, Breast Cancer Medicine...
42
Challenging Cases in Cancer: Early Breast Cancer Clifford A. Hudis, MD Chief, Breast Cancer Medicine Service Attending Physician Memorial Sloan-Kettering Cancer Center New York, NY
-
Upload
patience-mathews -
Category
Documents
-
view
215 -
download
0
Transcript of Challenging Cases in Cancer: Early Breast Cancer Clifford A. Hudis, MD Chief, Breast Cancer Medicine...

Challenging Cases in Cancer: Early Breast Cancer
Clifford A. Hudis, MDChief, Breast Cancer Medicine Service
Attending Physician
Memorial Sloan-Kettering Cancer Center
New York, NY

Case 1
• 57-year old woman with calcifications on her yearly screening mammogram is found to have 1.3 cm of invasive ductal carcinoma
• The tumor is strongly positive for both the estrogen and progesterone receptors and negative for HER2
• After undergoing a lumpectomy with clear margins and a sentinel node procedure yielding negative nodes, she seeks an opinion regarding treatment to improve her overall survival
• She has already planned radiation therapy

Case 1
• Which adjuvant therapy has been shown to offer the greatest impact on overall survival for patients with node-negative, hormone-receptor positive invasive breast cancer?1. Tamoxifen
2. Anastrozole
3. Letrozole
4. Tamoxifen followed by Exemestane
5. Tamoxifen followed by Anastrozole
6. Tamoxifen followed by Letrozole
7. Combination chemotherapy alone
8. Combination chemotherapy AND options 1, 2, 3, 4, 5 or 6
9. Clinical Trial

Case 1
• Which adjuvant therapy has been shown to offer the greatest impact on overall survival for patients with node-negative, hormone-receptor positive invasive breast cancer?1. Tamoxifen
2. Anastrozole
3. Letrozole
4. Tamoxifen followed by Exemestane
5. Tamoxifen followed by Anastrozole
6. Tamoxifen followed by Letrozole
7. Combination chemotherapy alone
8. Combination chemotherapy AND options 1, 2, 3, 4, 5 or 6
9. Clinical trial
Recommended Approach:
• Clinical trial

Effect of Tamoxifen on Breast Cancer Recurrence
Effect of Tamoxifen on Breast Cancer Death
Early Breast Cancer Trialists' Collaborative Group. Lancet. 2005; 365:1687-1717

Selective vs. NonselectiveAromatase Inhibition
Federman, DD: The Adrenal. Dale DC, Federman DD, eds. In: Scientific American Medicine. Section 3. Subsection IV. ©1997 Scientific American Inc. All rights reserved.
Multiple steps involving P-450 enzymes and production of steroid intermediates
Cholesterol
Cortisol AndrostenedioneAldosterone
Testosterone
Estrone Estradiol
Selective Inhibitors
Nonselective Inhibitors

Steroidal and Non-steroidal Aromatase InhibitorsDifferences in Structure and Function
Androstenedione
O
NH2
H
C2H5
ON
Aminoglutethimide
Steroidal Inactivators Androgen Substrate
Non-steroidal Inhibitors
CH3
CH3
CH3
CH3NC CN
AnastrozoleLetrozole
N
O
CH2
O
Exemestane
NC CN
N
NN
O
ONN
Formestane
O
OH
O

* Note that some patients from the original newly diagnosed population are lost due to recurrence or adverse events prior to randomization
TRIALS
• ATAC• BIG 01-98• TEAM
• BIG 01-98
• IES• ITA• ARNO95/ABCSG8*
DIRECT COMPARISON
SWITCHING
*
SEQUENCING
EXTENDED ADJUVANT
• MA.17
Adjuvant AI Hormonal Therapy Trial Designs

All women were:
• Postmenopausal
• 84% HR +
• 61% node -
• 21% Rx chemotx
RecruitmentJuly 1996-March 2000
Anastrozole + Tamoxifen (N=3,125)
Tamoxifen (N=3,116)
Surgery± RT ± chemo
Anastrozole (N=3,125)
5 years
ATAC Design

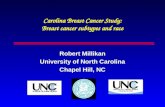
ATAC: Recurrence (HR +ve)Median follow up 68 months
Patients (%)
Follow-up time (years)
0
5
10
15
20
25
0 1 2 6
Absolute difference: 1.7% 2.4% 2.8% 3.7%
At risk: A 2618 2540 2448 2355 2268 2014 830T 2598 2516 2398 2304 2189 1932 774
Anastrozole (A)
Tamoxifen (T)
3
HR
0.74
0.79
HR +ve
ITT
95% CI
(0.64, 0.87)
(0.70, 0.90)
P-value
0.0002
0.0005
4 5
CI = confidence intervals; HR = hazard ratioITT = intent-to-treat ATAC Trialists’ Group. Lancet 2005;365:60-62

ATAC: Overview of Adverse Events* (%)
*Adverse events on treatment or within 14 days of discontinuation
Drug-related:
AEs
SAEs
AEs leading to withdrawal
P-value
< 0.0001
0.0001
0.0002
Tamoxifen(N=3,094)
68.4
9.0
14.3
Anastrozole(N=3,092)
60.9
4.7
11.1
ATAC Trialists’ Group. Lancet 2005;365:60-62

* Patients 1 fracture occurring before recurrence, including patients no longer on treatment
ATAC: Pre-specified Adverse Events (%)
T
40.9
10.2
13.2
0.8
2.8
4.5
29.4
7.7
5.1
A
35.7
5.4
3.5
0.2
2.0
2.8
35.6
11.0
1.3
Hot flashes
Vaginal bleeding
Vaginal discharge
Endometrial cancer
Ischemic cerebrovascular
Venous thromboembolic
Joint symptoms
Fractures*
Hysterectomy
P-value
< 0.0001
< 0.0001
< 0.0001
0.02
0.03
0.0004
< 0.0001
< 0.0001
< 0.0001
ATAC Trialists’ Group. Lancet 2005;365:60-62

ATAC: Overall SurvivalCurves Shown for HR+ Patients
Includes non breast cancer deaths
At risk:
A 2618 2566 2505 2437 2377 2117 867
T 2598 2549 2502 2430 2333 2080 855
Follow-up time (years)
0
5
10
15
20
25
0 1 2 3 4 5 6
Pa
tient
s (%
)
Anastrozole (A)
Tamoxifen (T)
HR
0.97
0.97
HR+
95% CI
(0.83–1.14)
(0.85-1.12)
P-value
0.7
0.7ITT
A
296
411
T
301
420
ATAC Trialists’ Group. Lancet 2005;365:60-62

BIG 01-98 (FEMTA)
TamoxifenTamoxifen
TamoxifenTamoxifen
LetrozoleLetrozole
LetrozoleLetrozole
LetrozoleLetrozoleRR
AA
NN
DD
OO
MM
II
ZZ
EE
TamoxifenTamoxifen
2 Years2 Years 3 Years3 Years
5 Years5 Years
ER+ and/or ER+ and/or PgR+ PgR+ Postmenopausal Postmenopausal women s/p women s/p surgery surgery ±± chemo, chemo, ±± RT RT
Primary Endpoints: DFS, DDFS, OS

BIG 01-98 Primary Core Analysis
• Compares Letrozole versus Tamoxifen
• Includes all patients
• Letrozole: Arms B and D
• Tamoxifen: Arms A and C
• Excludes events and FU beyond switch for C & D
Tamoxifen
Letrozole
Tamoxifen Letrozole
Letrozole Tamoxifen
A
B
C
D
2-Arm Option
4-Arm Option

TAM
0
20
40
60
80
100
0 1 2 3 4 5
Pe
rce
nt a
live
an
d d
ise
ase
-fre
e
Years from randomization
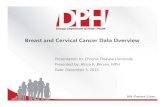
97.797.6
YearlyDFS (%)
95.193.4
90.589.0
86.884.6
84.081.4
No. at Risk
38923896
29642926
12611238
892866
40034007
567544
LET
N HR (95% CI) P Value
8010 0.81 (0.70-0.93) 0.003
BIG 01-98: Disease-free Survival

Updated Safety Analysis of BIG 01-98 Trial: Cardiovascular Adverse Events During Adjuvant
Letrozole (Let) vs. Tamoxifen (Tam) Therapy
Tamoxifen
Letrozole
Letrozole
BIG 1-98: N = 7963Let - HR: 19% lower for DFS, 27% reduced risk for distant
recurrence compared to Tam.
Grade 3-5 Adverse Event
Number of Events With
Letrozole
(N = 3,975)
Number of Events With Tamoxifen
(N = 3,988)
Relative Risk P
Any CardiacAny Cardiac 9696 5757 1.631.63 .0036.0036
Ischemic Heart DiseaseIschemic Heart Disease 4545 2929 1.461.46 .12.12
HypertensionHypertension 5757 4848 1.181.18 .40.40
CVA/TIACVA/TIA 4747 4747 0.980.98 .94.94
ThromboembolicThromboembolic 3535 9292 0.380.38 < .0001< .0001
Cardiovascular AEs higher for Let, but relatively rare.Patients at risk for thromboembolism should avoid tamoxifen
Coates et al, ASCO 2007, Abstract 521

ABCSG 8 – ARNO 95:Combined Analysis Trial Structure
Primarysurgery+/- RTx
TAM 3 yearsN=1,606
Total patientsN=3,224
ABCSG 8N=2,262
+ARNO 95
N=962
ANA 3 yearsN=1,618
+ TAM 2 years
100% HR positive 74% node negative0% Rx chemotx
Jakesz et al, Lancet 2005;366:455–462

ABCSG 8 – ARNO 95: Event-free Survival 28 Months Median Follow-up
Events = locoregional recurrences, distant metastases, contralateral breast ca
Event-free survival (%)
0
75
80
85
90
95
100
0 1 2 3 4 5
ANA vs TAM P=0.0009 HR 0.60 [95% CI 0.44-0.81]
EFS time in years
ANA
TAM
At risk:
1606 343 176TAMANA 1618
12171243
858874
593623 375 178

ABCSG 8 – ARNO 95: Overall Survival
Number Deaths 3 yrs. OS
(%)
TAM 1,606 59 96.4
ANA 1,618 45 97.1
ANA vs TAM P =0.16 HR 0.76 95% CI 0.52-1.12
Jakesz et al, Lancet 2005;366:455–462

IES Trial Design
Diagnosis
2-3 years2-3 years study
treatment
Total 5 years endocrine therapy
Tamoxifen
RANDOMIZE
Exemestane
5,162*
Tamoxifen
5,294*
Post Treatment Follow-up
10335*
Start of study
* Total women years Coombes et al, ASCO 2006, # LBA527

0
10
20
30
4050
60
70
80
90
100
0 1 2 3 4 5
Time since randomization (years)
% s
urvi
ving
dis
ease
free
0
10
2030
40
50
60
7080
90
100
0 1 2 3 4 5
Time since randomization (years)
% s
urvi
ving
dis
ease
free
IES: Disease-free Survival
yearyear
% abs. diff.% abs. diff.
(95% CI)(95% CI)
2.52.5 55
3.23.2 3.43.4
(1.6 – 4.9)(1.6 – 4.9) (0.1 – 6.8)(0.1 – 6.8)
En
d o
f E
nd
of
trea
tmen
t tr
eatm
ent
ER+/UnknownER+/Unknown
HR = 0.75 (95% CI: 0.65-0.87)HR = 0.75 (95% CI: 0.65-0.87)Log-rank test: Log-rank test: P P = 0.0001= 0.0001
E = 339 / 2296E = 339 / 2296
T = 438 / 2306T = 438 / 2306
E = 354 / 2352E = 354 / 2352
En
d o
f E
nd
of
trea
tmen
ttr
eatm
ent
ITTITT
HR = 0.76 (95% CI: 0.66-0.88)HR = 0.76 (95% CI: 0.66-0.88)Log-rank test: Log-rank test: PP = 0.0001 = 0.0001
T = 454 / 2372T = 454 / 2372
2.52.5 55
3.43.4 3.53.5
(1.8 – 5.1)(1.8 – 5.1) (0.1 – 6.9)(0.1 – 6.9)
Coombes et al, Lancet. 2007 Mar 17;369(9565):906.

0
10
20
30
4050
60
70
80
90
100
0 1 2 3 4 5
Time since randomization (years)
Wom
en a
live
(%)
0
1020
3040
50
6070
8090
100
0 1 2 3 4 5
Time since randomization (years)W
omen
aliv
e (%
)
IES: Overall Survival
yearyear
% abs. diff. % abs. diff.
(95% CI)(95% CI)
2.52.5 55
0.80.8 1.21.2
(-0.4 – 1.9)(-0.4 – 1.9) (-1.5 – 3.9)(-1.5 – 3.9)
En
d o
fE
nd
of
trea
tmen
ttr
eatm
ent
HR = 0.85 (95% CI: 0.71-1.02)HR = 0.85 (95% CI: 0.71-1.02)Log-rank test: Log-rank test: PP = 0.08 = 0.08
E = 222 / 2352E = 222 / 2352
T = 261 / 2372T = 261 / 2372
ITTITT
En
d o
fE
nd
of
trea
tmen
ttr
eatm
ent
HR = 0.83 (95% CI: 0.69-1.00)HR = 0.83 (95% CI: 0.69-1.00)Log-rank test: Log-rank test: P = P = 0.050.05
E = 210 / 2296E = 210 / 2296
T = 251 / 2306T = 251 / 2306
ER+/UnknownER+/Unknown
2.52.5 55
0.70.7 1.61.6
(-0.4 – 1.9)(-0.4 – 1.9) (-1.2 – 4.3)(-1.2 – 4.3)
Coombes et al, Lancet. 2007 Mar 17;369(9565):906.

Primary Endpoint: Disease-free Survival
n = 2,575
n = 2,582
All Postmenopausal Patients and Disease-free
Tamoxifen Placebo
Letrozole
4.5 - 6 years initial adjuvant 5 years extended adjuvant
0 – 3
months
NCIC CTG Intergroup Trial MA.17 Design
Goss PE, et al, NEJM. 349;19 November 6, 2003.

No. at risk (letrozole) 2575 2308 1327 1110 624 9 0
No. at risk (placebo) 2582 2298 1295 610 180 11 0
P P < .001< .001
Letrozole Placebo
0
20
40
60
80
100
Time From Randomization (Months)
0 10 20 30 40 50 60
Per
cent
age
MA.17: Disease-free Survival
Goss PE, et al. J NEJM. 349;19 November 6, 2003.

Adjuvant Endocrine Trials: Efficacy
StrategyStrategy RCTsRCTs PtsPts UpdateUpdate Median FU Median FU (mo.)(mo.) AIAI
Efficacy [HR, Efficacy [HR, PP]]
DFS/EFSDFS/EFS OSOS
Up-FrontUp-FrontATACATAC 6,1866,186 Lancet 2006Lancet 2006 6868 ANAANA 0.87 (0.01)0.87 (0.01) 0.97 (0.7)0.97 (0.7)
BIG-1-98BIG-1-98 4,9224,922 JCO 2007JCO 2007 5151 LETLET 0.82 (0.007)0.82 (0.007) 0.91 (>0.05)0.91 (>0.05)
““Early” Early” SwitchSwitch
ITA-1ITA-1 380380 JCO 2001JCO 2001 6161 AGTAGT NR (0.6)NR (0.6) NR (0.005)NR (0.005)
ITA-2ITA-2 448448 Ann Oncol Ann Oncol 20062006 6464 ANAANA 0.57 (0.005)0.57 (0.005) 0.56 (0.1)0.56 (0.1)
IESIES 4,7424,742 Lancet 2007Lancet 2007 5656 EXEEXE 0.76 (0.0001)0.76 (0.0001) 0.85 (0.08)0.85 (0.08)
ABCSG8/ARNOABCSG8/ARNO 3,2243,224 Lancet 2005Lancet 2005 2828 ANAANA 0.60 (0.0009)0.60 (0.0009) NR (0.16)NR (0.16)
““Extended” Extended” SwitchSwitch
MA.17MA.17 5,1575,157 JNCI 2005JNCI 2005 3030 LETLET 0.58 (0.001)0.58 (0.001) 0.82 (0.3)0.82 (0.3)
ABCSG 6aABCSG 6a 856856 ASCO 2005ASCO 2005 6060 ANAANA 0.64 (0.047)0.64 (0.047) NRNR
NSABP B-33NSABP B-33 1,5981,598 SABCS 2006SABCS 2006 3030 EXEEXE 0.68 (0.07)0.68 (0.07) 1.20 (0.64)1.20 (0.64)

AI’s & Hazard Rate Inflections:Does the Timing of Hormone Therapy Influence
the Change in the RATE of Events?
5 10
YEARS
% DFS
ATAC/BIG 01-98
MA.17
IES/ARNO 8-ABCSG 95

Local/regional
recurrence
Distant metastasis
Deathfrom any
cause
Invasive Contra-lateral breast cancer
Second primary invasive cancer (non-
breast)
Ipsi-lateral DCIS
Contra-lateral DCIS
Ipsi-lateral LCIS
Contra-lateral LCIS
BIG 1-98 X X X X X
MA-17 X X X X X X X
ATAC X X X X X X
IES X X X X
ARNO X X X
NOTE: EFS (Event-free Survival) used by ARNODCIS = Ductal Carcinoma in situLCIS = Lobular Carcinoma in situ
Hudis et al, JCO, Vol 25, No 15 (May 20), 2007: pp. 2127-2132
Example of Inconsistent Definitions of Disease-free Survival

Early Breast Cancer Trialists’ Collaborative Group, Sept 2000 (*Lancet 1998)
Comparison (N)
CMF vs. Nil (12,000)
CMF+ vs. Nil (3,200)
Other vs. Nil (12,000)
*CMF/Tam vs. Tam (640) < 50
*CMF/Tam vs. Tam (9,192) 50+
Anthracyclines+ vs. CMF (13,600)
Longer vs. Shorter (6,100)
Recurrence
+24 ± 3
+20 ± 5
+24 ± 3
+ 21 ± 13
+19 ± 3
+11 ± 3
+6 ± 4
Death
+15 ± 3
+12 ± 5
+16 ±3
+25 ± 14
+ 11 ± 4
+16 ± 3
2 ± 4
PolyChemotherapy:56/64 Available Trials
10,000 Deaths / 28,000 Enrolled

Case 2
• 45-year old woman with calcifications on her yearly screening mammogram is found to have 1.3 cm of invasive ductal carcinoma (infiltrating carcinoma) metastatic to 3 lymph nodes
• She has had a lumpectomy and is planning radiation therapy
• The tumor is weakly positive for both the estrogen and progesterone receptors but also positive by both IHC and FISH for HER2
• She seeks an opinion regarding treatment to prevent recurrence and improve her overall survival

Case 2
• Which adjuvant chemotherapy would you recommend in addition to hormone therapy?
1. CMF x 6 + trastuzumab
2. AC x 4 + trastuzumab
3. FEC/CEF/CAF/FAC + trastuzumab
4. AC x 4 followed by a taxane x 4 + trastuzumab
5. AC x 4 followed by paclitaxel x 4 (all q 2 weeks) + trastuzumab
6. TAC x 6 followed by trastuzumab
7. Carbo/docetaxel + trastuzumab
8. Trastuzumab alone

H Trastuz
DoxorubCyclophPaclitaxDocetaxCBDCA
Adjuvant Trastuzumab
NSABP B-31
NCCTG 9831
H…x 52
H…x 52
H…x 52
H…x 52
H…x 52
BCIRG 006
H…x 1 years
H…x 2 years
No therapy
StandardChemoRx
HERA

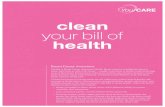
B-31/N9831 Survival
ACACTHTH94%94%
91%91%
87%87%
92%92%ACACTT
NN DeathsDeathsACACTT 1,6791,679 9292ACACTHTH 1,6721,672 6262
HR = 0.67, 2P = 0.015HR = 0.67, 2P = 0.015
Years From Randomization
Romond et al, ASCO 2005

Disease-free Survival: Adjuvant Trastuzumab
Romond EH, et al. N Engl J Med. 2005;353:1673-1684.
N9831
Years From Randomization
0 1 2 3 4 5
50
60
70
80
90
100
78%
87%86%
68%
HR: 0.55; 2P = .0005
ACT 807 90ACTH 808 51
0 1 2 3 4 5
50
60
70
80
90
100 B-31
HR: 0.45; 2P = 1x10-9
74%
87%85%
66%
Pat
ien
ts (
%)
N EventsTreatment
872 171864 83
ACTACTH
ACTACTH
Treatment N Events

100
80
60
40
20
0
Patients(%)
Months from randomization
Observation
No. at risk
1703 1627 1498 1190 794 407 146
1698 1606 1424 1042 677 354 126
1-year trastuzumab
59
90
Events HR 95% CI P value
0.63 0.45, 0.87 0.0051
3-yearOS
92.4
89.2
12 360 186 24 30
Smith et al., Proc ASCO 2006
HERA: Overall Survival (censored)Median 2-year FU

Disease-free Survival: 2nd Interim Analysis
Absolute DFS benefitsAbsolute DFS benefits(from years 2 to 4):(from years 2 to 4):
ACACTH vs. ACTH vs. ACT: 6%T: 6%TCH vs. ACTCH vs. ACT: 5%T: 5%
% D
ise
ase
Fre
e
0.5
0.60.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5
PatientsPatients EventsEvents
1,0731,073 192192 ACAC→→TT1,0741,074 128128 ACAC→→THTH1,0751,075 142142 TCHTCH
81%
87%
86%
77%
83%
82%87%
93%
92%
HR (ACHR (AC→→TH vs. ACTH vs. AC→→T) = T) = 0.61 [0.48;0.76]0.61 [0.48;0.76] P P < 0.0001< 0.0001
HR (TCH vs. ACHR (TCH vs. AC→→T) = T) = 0.67 [0.54;0.83]0.67 [0.54;0.83] P P = 0.0003= 0.0003
Year from randomization

Overall Survival: 2nd Interim Analysis
HR (AC→TH vs AC->T) = HR (AC→TH vs AC->T) = 0.59 [0.42;0.85]0.59 [0.42;0.85] P P = 0.004= 0.004HR (TCH vs AC→T) = HR (TCH vs AC→T) = 0.66 [0.47;0.93]0.66 [0.47;0.93] P P = 0.017= 0.017
% S
urvi
val
% S
urvi
val
0.50.5
0.60.6
0.70.7
0.80.8
0.90.9
1.01.0
00 11 22 33 44 55
PatientsPatients EventsEvents1,0731,073 8080 AC→TAC→T1,0741,074 4949 ACAC→→THTH1,0751,075 5656 TCHTCH
97%97%
99%99%
93%93%
97%97%
95%95%92%92%
91%91%
86%86%
Year from randomizationYear from randomization
98%98%

Summary of Results from 5 Adjuvant Trastuzumab Trials
Recurrence Recurrence TrialTrial ControlControl Exp ArmExp Arm Conc ? N=; FU=Conc ? N=; FU= HR, % HR, % MortalityMortality
B31+N9831B31+N983111 AC + PAC AC + PAC Same +Same + YY 3351; 2y 3351; 2y 4747 3333 all Q3W x 4all Q3W x 4 Tras 1y Tras 1y
N9831N9831 AC + PACAC + PAC Same +Same + NN 3585; 1.5y3585; 1.5y 1313 1515 Post CPost C11 all Q3W x 4all Q3W x 4 Tras 1yTras 1y
HERA HERA 22 Any PriorAny Prior Same +Same + NN 3387; 1y3387; 1y 4646 2424 adjuvant CTadjuvant CT Tras 1yTras 1y
BCIRG OO6BCIRG OO633 AC + DAC + D Same +Same + YY 3222; 2y3222; 2y 5151 ------all Q3W X 4all Q3W X 4 Tras 1yTras 1y
CbD +CbD + YY 3222; 2y3222; 2y 3939 ------Tras 1yTras 1y
FinHerFinHer44 D or V + D or V + Same +Same + YY 1010; 3y1010; 3y 5858 5959FEC x 3 FEC x 3 Tras 9W Tras 9W
1.1. Romond EH. N Engl J Med 2005:353:1673-1684Romond EH. N Engl J Med 2005:353:1673-16842.2. Piccart-Gebhart MJ et al. Presented at: ASC0 41Piccart-Gebhart MJ et al. Presented at: ASC0 41stst Annual Meeting; May 13-17, 2005 Annual Meeting; May 13-17, 2005
3.3. Slamon D et al. Presented at: 28Slamon D et al. Presented at: 28thth Annual San Antonio Breast Cancer Symposium; December 8-11, 2005 Annual San Antonio Breast Cancer Symposium; December 8-11, 20054.4. Joensuu H et al, Breast Cancer Res Treat. 2005;94(suppl 1):S5. Abstract 2. Joensuu H et al, Breast Cancer Res Treat. 2005;94(suppl 1):S5. Abstract 2.
CbD = carbloplatin, docetaxel; CT = chemotherapy; D = docetaxel; HR = hazard ratio; Tras = trastuzumab; V = vinorelbineCbD = carbloplatin, docetaxel; CT = chemotherapy; D = docetaxel; HR = hazard ratio; Tras = trastuzumab; V = vinorelbine

q 2 wk (w/G-CSF) q 3 wk
7/481 (1.5%)
5/487 (1%) 12/488 (2.5%)
12/473 (2.5%)*
Grade 3 Post-Rx Cardiac Events:36/1929 (2%)
No association with schedule or regimen( * plus one cardiac death w/Rx)
Hudis et al, SABCS 2005

Trastuzumab is Safe With Dose-Dense: AC→ TPreliminary Results Of MSKCC Pilot: 04-126
N = 70
Dang, et al, SABCS. 2006 (abstr 2101).
HHHHHHHHHH x 52 doses (weeks)

Dose-Dense AC→Paclitaxel (T) + H: Results
Multi-gated radionuclide angiography scan (MUGA) obtained at baseline and at months 2, 6, 9, and 18
MUGA at:
Baseline Month 2 Month 6 Month 9 Month 18
Median LVEF (%) 68 67 66 65 66
Range 55-81 58-79 52-75 53-75 55-75
Dang, et al, SABCS. 2006 (abstr 2101).
LVEF=left ventricular ejection fraction.
CHF in 1 patient of 70

Summary
• Targeting of the estrogen receptor through deprivation of estrogen shows a clear and consistent advantage in post-menopausal women for the use of aromatase inhibitors
• Role of chemotherapy
• Targeted therapies can improve survival in early-stage breast cancer
• Dose-Dense Chemotherapy