Challenges of glucose control in ckd
63
Diabetes and Kidney Diabetes and Kidney Dr.Sampathkumar MD,DNB,DM,FRCP MMHRC 1
-
Upload
drk-sampath-kumar -
Category
Health & Medicine
-
view
182 -
download
2
description
The incidence of Chronic KidneyDisease[ CKD ] has reached epidemic proportions. Diabetes tops the list of causes of CKD.Both hypo and hyperglycemia can complicate advanced renal disease. The topic is discussed in this presentation
Transcript of Challenges of glucose control in ckd

Diabetes and KidneyDiabetes and Kidney
Dr.SampathkumarMD,DNB,DM,FRCP
MMHRC
1

2 sides of the coin 2 sides of the coin
2

ALL patients with Diabetes and ALL patients with Diabetes and Proteinuria/Renal failure have Proteinuria/Renal failure have
diabetic renal disease .diabetic renal disease .You may be wrong 50% of the
times !
3
Common Pitfall

Indications for Renal Biopsy Indications for Renal Biopsy
4

Diabetic N along with Infection Diabetic N along with Infection related GN related GN

Endocap. Prolif to 100% crescentsEndocap. Prolif to 100% crescents

Progressive grades of CKDProgressive grades of CKD
7

Filtration Pressure +15 mm Hg Filtration Pressure +15 mm Hg
8

Diabetic glomerular diseaseDiabetic glomerular diseaseFlitration Pressure +35Flitration Pressure +35
9
80 mm

Renal and cv risk increases once Renal and cv risk increases once microalbuminuria crosses 6 mg/gmicroalbuminuria crosses 6 mg/g
Albuminuria Renal risk CV event
0-10 1 1
10-20 2.34 1.9
20-30 12.4 9.8
10

New classification of albumin New classification of albumin excretionexcretion
11

12

13

Traditional Vs Novel Traditional Vs Novel
14

Non Proteinuric nephropathyNon Proteinuric nephropathy
15

16
CKD

17
This patient develops KWD within 5 years though his Hb A1 c was 6.5 %

Insulin dynamics in CKDInsulin dynamics in CKD
18

19

20

Insulin half life in CKDInsulin half life in CKD
21


23

24

Use of OHAs in CKDUse of OHAs in CKD
25

Metformin Controversy Metformin Controversy in CKD….in CKD….
26

Pharmacokinetics of MetforminPharmacokinetics of Metformin
27

MALA- Metformin Associated MALA- Metformin Associated Lactic Acidosis Lactic Acidosis • Decreased Utilisation vs hepatic dysfn
ANAEROBIC GLYCOLYSIS
SHOCK STATES
LIVER DYSFNTYPE B
METFORMIN
•2-10 per 100,000 patients receiving metformin /year•MALA accounts for 0.1-1% total patients admitted to ICU•Mortality is high – 30-50%
Balance

2 sites where Metformin acts2 sites where Metformin acts
29

Hypotension rather than Hypotension rather than metformin level which metformin level which determined Lactate accumulationdetermined Lactate accumulation
30
Conclusion from this study

31

SFU in CKDSFU in CKD
• Depends on Renal or Hepatic metabolism
• Depends also on whether metabolites have hypoglycemic effects
32

33

34

35

36

37

Drug exposure(AUC) in renal impairment compared to patients Drug exposure(AUC) in renal impairment compared to patients with normal renal functionwith normal renal function
Drug Mild RI Moderate RI Severe RI Hemodialysis
Metformin NA NA NA NA
GlibenclamideM1+M2
NA NA -45% NA
GlimepirideM2
NA -55%+100%
-55%+400%
NA
Repaglinide NA +19% +32% +32%
Pioglitazone NA -17% to -43% 17% to -43% NA
Sitagliptin +61% +126% +277% +350%
Vildagliptin +40% +71% +100% NA
Saxagliptin(Active metabolite)
+16%+67%
+41%+192%
+108%+347%
NANA
Alogliptin +70% +110% +220% +280%
Linagliptin +29% +56% +41% +54%
Exenatide -19% -3% NA +227%
A.J Scheen. Expert Opinion on Drug Metabolism and Toxicology: 2013

Linagliptin in a recent study lowered albuminuria on top of Linagliptin in a recent study lowered albuminuria on top of standard ACEi/ARB therapy in patients with T2DMstandard ACEi/ARB therapy in patients with T2DM
39
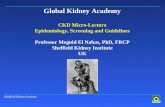
Linagliptin significantly lowers albuminuria on top of recommended standard treatment for diabetic nephropathy
1. Inclusion criteria: Stable ACE/ARB background; albuminuria 30−3000 mg/g creatinine; GFR > 30.*Albuminuria-lowering evidence for linagliptin will emerge from MARLINA 1218.89.
**ADA 2012, 953-P
Adjusted mean change in albuminuria(24 weeks)1
24 weeks’ treatmentEffect of linagliptin on albuminuria in humans*
n
95% CI
59
-20%, +23%
168
-42%, -22%
Placebo Linagliptin
-4%
-33%
-29%p < 0.05
Albuminuria:
Early marker for renal damage
Marker for endothelial dysfunction
Cardiovascular risk factor
Lowering of albuminuria is associated with kidney & CV protection
Definitions
Microalbuminuria
UACR ≥ 30 mg/g creatinine < 300 mg/g creatinine
Macroalbuminuria
UACR ≥ 300 mg/g creatinine
-29% in albuminuria vs placeboafter 24 weeks’ treatment**
Proven renal safety with potential for additional kidney benefit– Mean GFR remains unchanged after treatment initiation with linagliptin up
to 24 weeks
-29% in albuminuria vs placeboafter 24 weeks’ treatment**
Albuminuria Lowering by Linagliptin is independent of the Improvement in Glucose
Linagliptin significantly lowers albuminuria on top of recommended standard treatment for diabetic nephropathy
1. Inclusion criteria: Stable ACE/ARB background; albuminuria 30−3000 mg/g creatinine; GFR > 30.*Albuminuria-lowering evidence for linagliptin will emerge from MARLINA 1218.89.
**ADA 2012, 953-P
Adjusted mean change in albuminuria(24 weeks)1
24 weeks’ treatmentEffect of linagliptin on albuminuria in humans*
n
95% CI
59
-20%, +23%
168
-42%, -22%
Placebo Linagliptin
-4%
-33%
-29%p < 0.05
Albuminuria:
Early marker for renal damage
Marker for endothelial dysfunction
Cardiovascular risk factor
Lowering of albuminuria is associated with kidney & CV protection
Definitions
Microalbuminuria
UACR ≥ 30 mg/g creatinine < 300 mg/g creatinine
Macroalbuminuria
UACR ≥ 300 mg/g creatinine
-29% in albuminuria vs placeboafter 24 weeks’ treatment**
Proven renal safety with potential for additional kidney benefit– Mean GFR remains unchanged after treatment initiation with linagliptin up
to 24 weeks
-29% in albuminuria vs placeboafter 24 weeks’ treatment**
Possible mechanism: The reno-
protective effect of linagliptin as
studies in preclinical modelInhibition of podocyte damage and
Inhibition of myofibroblast
transformation
Increased GLP-1 receptor
expression

40

41

Extreme Hyperglycemia in CKDExtreme Hyperglycemia in CKD
42

Case HistoryCase History
• 67 yrs old male in altered sensorium• Type 2 Diabetes, CAD • On OHA for the past 5 y• Fever,Dysuria – 7 d• Pain abdoment -1 d• Altered sensorium – 12 h• On Glimepride, Metformin ,Metoprolol,
Losartan, eplerenone,Asprin,atorvastatin

Phy ExaminationPhy Examination
• Significant volume depletion• FEBRILE -101,RR 19 /PM• BP -100/70• JVP-Collapsed• S1,S2 FAINT, Lung Bases - clear• Abdomen- Left Lumbar area tender • Catheter draining turbid urine• Drowsy, Neck supple,No FND,Plantar –
Flexor Bil

LabLab
• Urine – Pus cells +++, Bacteria ++• Hb – 9.8, TC – 18,300. P 84,L14,E2• B.Sugar- 604, B Urea – 87,S.Creat-2.3• Na -147,K – 6.2,Cl – 112, HCO3 – 18.PCO2- 35,pO2 -90• Ketone body – neg• ABG - P H – 7.32
Pyuria Hyperglycemia Azotemia HyperNa,HyperK,Met.Acidosis

3 major grades of insulin deficits 3 major grades of insulin deficits

WHY IS HE NOT WHY IS HE NOT KETONEMICKETONEMIC

Calculated osm

ECF hyperosmolality produces ICF ECF hyperosmolality produces ICF dehydrationdehydration
RF PREVENTS GLYCOSURIA

ICF ECF
Na , GK, P
Urea Water
Ethanol
Insulin lack and hyperosmolality drives K outside

60 kg / 10% Deficit/Na 147 60 kg / 10% Deficit/Na 147
6 / 3L
1 L/I hr
0.45%Sal.
H2O /po

Insulin therapy Insulin therapy

53


Hemodialysis for severe Hemodialysis for severe hyperglycemia in CKDhyperglycemia in CKD
55
Extreme hyperglycemia with ketoacidosis and hyperkalemia in a patient on chronic hemodialysis.Hemodial Int. 2008 Oct ;12 Suppl 2:S43-7.

56

CAPD patientCAPD patient
• Dialysate contains • Glucose in high• Concentration
• Hyperglycemia severe and common
57

Icodextrin use in diabetic patientIcodextrin use in diabetic patient• Icodextrin is
Polymer of Glucose• False high reading of
Blood Glucose if • GDH/PQQ strips
are used • Risk of iatrogenic
hypoglycemia due to misdiagnosis and over reaction
58

Renal Transplantation.Renal Transplantation.
59

Post transplant DiabetesPost transplant Diabetes
• Tacrolimus• Cyclosporine• Steroids• CMV• HCV • Metabolic syndrome
60

45 yrs female , Renal TX in 45 yrs female , Renal TX in MMHRC at 1999.Presents with MMHRC at 1999.Presents with proteinuria , edemaproteinuria , edema
61

Arteriolar hyalinosisArteriolar hyalinosis
62

63
Hypoglycemia Vs Hyperglycemia in Hypoglycemia Vs Hyperglycemia in CKD- Tight rope walk!CKD- Tight rope walk!
If he falls your reputation also falls !!