Challenges in bringing the bench to bedside in drug development for sle
11
1036 | DECEMBER 2004 | VOLUME 3 www.nature.com/reviews/drugdisc REVIEWS Systemic lupus erythematosus (SLE) is a chronic, relapsing and remitting inflammatory disorder, the hallmark of which is a diverse but characteristic set of AUTOANTIBODIES that can bind to both intracellular and extracellular structures. Although SLE is considered a prototypic autoimmune disease, it is remarkable in its heterogeneity, and can potentially involve virtually any organ. The molecular basis for the underlying immunological disarray can differ between patients, and the pathophysiological disorders that have been described in this disease span both affector and effector arms of the immune system. It is therefore not surprising that the clinical manifestations of lupus are diverse, that the temporal sequence of organ involvement is often unpredictable, and that flares can remit without consequence or leave permanent damage in their wake. Clinical manifestations of lupus SLE can involve any organ system (most commonly joints, skin and kidneys) in many different ways, and the heterogeneous nature of lupus can result in a diag- nostic challenge for physicians. SLE patients can present with a broad spectrum of clinical and laboratory mani- festations, including fever, fatigue, inflammatory rash, oral ulcers, arthralgia and arthritis, nephritis, serositis, anaemia, leukopaenia and thrombocytopaenia. Further- more, central nervous system involvement in SLE patients (neuropsychiatric lupus) has multiple clinical presentations, including headache, cerebrovascular disease, cognitive dysfunction, psychosis, seizures, trans- verse myelitis, chorea, cranial and peripheral neuro- pathies, pseudotumour cerebri and demyelinating syndromes 1,2 . The American College of Rheumatology (ACR) proposed the SLE Classification Criteria in 1982 (REF. 3), which were revised and updated in 1997 (REF. 4). On the basis of these classification criteria, for the purpose of identifying patients in clinical SLE studies, a patient should have four or more of the eleven manifes- tations serially or simultaneously (BOX 1). Patients with less than four manifestations are often diagnosed as having ‘lupus-like disease’. The nature of lupus Lupus does not have a single ‘nature’; indeed, the disease is characterized by its diverse pathology and varied clinical expression. Despite several characteristic patterns of illness that define a few recognizable subgroups of patients, each patient is unique and there is no currently identified means to predetermine the course of ill- ness in any given individual. This unpredictability CHALLENGES IN BRINGING THE BENCH TO BEDSIDE IN DRUG DEVELOPMENT FOR SLE Joan T. Merrill*, Doruk Erkan ‡ , and Jill P. Buyon § Abstract | It is now widely accepted that the current standard of care for systemic lupus erythematosus (SLE) patients is inadequate. There has not been a new medication approved for this disease in thirty years. Attempts to develop and test new drugs have been ongoing since the mid-1990s, but have encountered formidable obstacles. Current models for lupus pathogenesis have provided a theoretical framework for understanding how heterogeneous genetic defects might combine in various ways to increase susceptibility to SLE in different individuals, and could have important implications for new drug development. With the current burst of drug discovery and increased public awareness of SLE, the impetus to overcome these obstacles has never been greater. *Clinical Pharmacology Research Program, Oklahoma Medical Research Foundation, 825 Northeast 13 t h Street Oklahoma City, Oklahoma 73104, USA. ‡ Division of Rheumatology, Hospital for Special Surgery, Weill Medical College of Cornell University, 535 East 70th Street, New York, New York 10021, USA. § Division of Rheumatology, Hospital for Joint Diseases, New York University School of Medicine, 301 East 17th Street, New York, New York 10001, USA. Correspondence to D.E. e-mail: [email protected] doi:10.1038/nrd1577 AUTOANTIBODY Antibody against patients’ own cellular antigens.
Transcript of Challenges in bringing the bench to bedside in drug development for sle

1036 | DECEMBER 2004 | VOLUME 3 www.nature.com/reviews/drugdisc
R E V I E W S
Systemic lupus erythematosus (SLE) is a chronic,relapsing and remitting inflammatory disorder, thehallmark of which is a diverse but characteristic set ofAUTOANTIBODIES that can bind to both intracellular andextracellular structures. Although SLE is considered aprototypic autoimmune disease, it is remarkable in itsheterogeneity, and can potentially involve virtuallyany organ. The molecular basis for the underlyingimmunological disarray can differ between patients,and the pathophysiological disorders that have beendescribed in this disease span both affector and effectorarms of the immune system. It is therefore not surprisingthat the clinical manifestations of lupus are diverse,that the temporal sequence of organ involvement isoften unpredictable, and that flares can remit withoutconsequence or leave permanent damage in their wake.
Clinical manifestations of lupusSLE can involve any organ system (most commonlyjoints, skin and kidneys) in many different ways, andthe heterogeneous nature of lupus can result in a diag-nostic challenge for physicians. SLE patients can presentwith a broad spectrum of clinical and laboratory mani-festations, including fever, fatigue, inflammatory rash,oral ulcers, arthralgia and arthritis, nephritis, serositis,
anaemia, leukopaenia and thrombocytopaenia. Further-more, central nervous system involvement in SLEpatients (neuropsychiatric lupus) has multiple clinicalpresentations, including headache, cerebrovasculardisease, cognitive dysfunction, psychosis, seizures, trans-verse myelitis, chorea, cranial and peripheral neuro-pathies, pseudotumour cerebri and demyelinatingsyndromes1,2. The American College of Rheumatology(ACR) proposed the SLE Classification Criteria in 1982(REF. 3), which were revised and updated in 1997 (REF. 4).On the basis of these classification criteria, for thepurpose of identifying patients in clinical SLE studies, apatient should have four or more of the eleven manifes-tations serially or simultaneously (BOX 1). Patients withless than four manifestations are often diagnosed ashaving ‘lupus-like disease’.
The nature of lupusLupus does not have a single ‘nature’; indeed, the diseaseis characterized by its diverse pathology and variedclinical expression. Despite several characteristic patternsof illness that define a few recognizable subgroups ofpatients, each patient is unique and there is no currentlyidentified means to predetermine the course of ill-ness in any given individual. This unpredictability
CHALLENGES IN BRINGING THE BENCH TO BEDSIDE IN DRUGDEVELOPMENT FOR SLEJoan T. Merrill*, Doruk Erkan‡, and Jill P. Buyon§
Abstract | It is now widely accepted that the current standard of care for systemic lupuserythematosus (SLE) patients is inadequate. There has not been a new medication approvedfor this disease in thirty years. Attempts to develop and test new drugs have been ongoingsince the mid-1990s, but have encountered formidable obstacles. Current models for lupuspathogenesis have provided a theoretical framework for understanding how heterogeneousgenetic defects might combine in various ways to increase susceptibility to SLE in differentindividuals, and could have important implications for new drug development. With the currentburst of drug discovery and increased public awareness of SLE, the impetus to overcomethese obstacles has never been greater.
*Clinical PharmacologyResearch Program,Oklahoma Medical ResearchFoundation, 825 Northeast13th Street Oklahoma City,Oklahoma 73104, USA.‡Division of Rheumatology,Hospital for Special Surgery,Weill Medical College ofCornell University, 535 East70th Street, New York,New York 10021, USA.§Division of Rheumatology,Hospital for Joint Diseases,New York University Schoolof Medicine, 301 East 17thStreet, New York, New York10001, USA.Correspondence to D.E.e-mail: [email protected]:10.1038/nrd1577
AUTOANTIBODY
Antibody against patients’ owncellular antigens.

NATURE REVIEWS | DRUG DISCOVERY VOLUME 3 | DECEMBER 2004 | 1037
R E V I E W S
TH2 CELLS
A subset of CD4 cells that aremainly involved in stimulatingB cells.
POLYCLONAL
Multiple clones with diversespecificity.
APOPTOSIS
Programmed cell death.
CYTOKINES
Proteins produced by cells tointeract with other cells.
production and the attack of self in an unregulatedmanner11,12. A number of new treatments have beendesigned to suppress POLYCLONAL B-cell responses whileleaving other required immune functions intact.
It is well established that lupus can arise by manymolecular routes. Evidence from murine and humanstudies have demonstrated abnormalities at varioussteps of immune regulation, including defects in pro-teins that regulate T cells, B cells and multiple intra-cellular and extracellular communication pathways— any of which can contribute, directly or indirectly,to autoantibody spreading in SLE13–15.
In addition, recent studies in both animal modelsand humans indicate that defective activation-inducedcell death and subsequent reduced clearance of the after-math might be fundamental to the pathogenesis oflupus16,17. Growing interest in the mechanisms underlyingthe programmed elimination (APOPTOSIS) and disposal ofimmune cells has led to the insight that this process isintrinsic to immune regulation and the maintenance ofimmune tolerance17,18. Immune regulation exists as a deli-cate balance that serves opposing forces: the survival ofbeneficial immune-recognizing cells and the deletionof harmful autoreactive cells19. Interestingly, apoptoticcells are considered the source of DNA, histones andnucleoprotein complexes that drive the production ofpathological autoantibodies in lupus. These structurescome under immune surveillance when they rise to thesurface of apoptotic cells, which might be a function,and not merely a coincidental side effect, of programmedcell death17.
Physiological autoantibodies are part of a normalimmune repertoire, and have functions crucial forimmune regulation. These include the opsonization ofapoptotic cells to promote their clearance, broadeningof the immune repertoire to fight recalcitrant infec-tions, restraint of tumour growth, and modulation ofT-cell functions20–23. In a healthy person, an autoanti-body repertoire exists just as it does in the lupus patient,but in this more well-ordered environment the activitiesof these antibodies are held in check, so that auto-immune responses have a net beneficial effect. In SLE,where numerous immune regulating systems havebroken down, autoantibodies are unleashed in anuncontrolled manner, indicating that this is an illness ofdegree rather than simply one of aberrant immunefunction (FIG. 1). Anti-double-stranded DNA (anti-dsDNA) antibodies are important in the pathogenesisof SLE, and the presence of these antibodies is one ofthe ACR SLE classification criteria. However, not allanti-dsDNA antibodies are pathogenic, and those thatare tend to be immunoglobulin (Ig) G isotype and havemultiple somatic mutations in their variable regions24.
CYTOKINES and immune complexes are also importantin lupus pathogenesis. For example, there is substantialevidence that interferon-α (IFNα) plays a significantrole in the pathogenesis of lupus and thus the IFNαpathway is a promising target for therapeutic interven-tion in SLE patients25. A detailed discussion of the role ofcytokines and immune complexes in SLE can be foundin two recent review articles26,27.
makes treatment selection and outcome measurementintrinsically problematic.
Knowledge of the genetics and pathophysiology oflupus, although still work in progress, has advancedsufficiently in recent years to explain how such diagnosticand clinical complexity might arise. It is evident from anumber of investigations in murine genome systems, aswell as in multiplex human families, that an underlyingpredisposition to disordered immune interactions isprobably inherited through a polygenic mechanism5–10.
This is not surprising, because in a well-regulatedimmune response an intricate system is in place to con-serve homeostasis, and involves a balance betweeninflammatory triggers, modulating mechanisms andimmune clearance. The latter serves to remove debrisfrom inflammatory foci which, if left unattended, canresult in irreversible scarring of an organ and perpet-uation of an aberrant immune response. Althoughimmune abnormalities in lupus are multifaceted, a hall-mark of the disorder is unchecked autoantibodyspreading, which can arise from a classic kind of T
H2
response. The consequence is pathological autoantibody
Box 1 | The 1997 Revised Criteria for Classification of SLE*
• Malar rash: fixed erythema, flat or raised, over the malar eminences, tending to sparethe nasolabial folds.
• Discoid rash: erythematosus raised patches with adherent keratotic scaling andfollicular plugging; atrophic scarring can occur in older lesions.
• Photosensitivity: skin rash as a result of unusual reaction to sunlight, by patient historyor physician observation.
• Oral ulcers: oral or nasopharyngeal ulceration, usually painless, observed by physician.
• Arthritis: non-erosive arthritis involving two or more peripheral joints, characterizedby tenderness, swelling or effusion.
• Serositis: (i) pleuritis — convincing history of pleuritic pain or rubbing heard by aphysician or evidence of pleural effusion; or (ii) pericarditis — documented byelectrocardiogram or rub or evidence of pericardial effusion.
• Renal disorder: (i) persistent proteinuria greater than 0.5 grams per day or greater than3+ if quantitation is not performed; or (ii) cellular casts — can be red cell,haemoglobin, granular, tubular or mixed.
• Neurological disorder: (i) seizures — in the absence of offending drugs or knownmetabolic derangements — for example, uraemia, ketoacidosis or electrolyteimbalance; (ii) psychosis in the absence of offending drugs or known metabolicderangements — for example, uraemia, ketoacidosis or electrolyte imbalance.
• Haematological disorder: (i) haemolytic anaemia with reticulocytosis; (ii) leukopaenia— less than 4,000 per mm3 total on two or more occasions; (iii) lymphopaenia — lessthan 1,500 per mm3 on two or more occasions; or (iv) thrombocytopaenia — less than100,000 per mm3 in the absence of offending drugs.
• Immunological disorder: (i) anti-DNA — antibody to native DNA in abnormal titre;(ii) anti-Sm — presence of antibody to Sm nuclear antigen; or (iii) positive finding ofantiphospholipid antibodies based on either an abnormal serum level of ummuno-globulin G (IgG) or IgM anticardiolipin antibodies, a positive test result for lupusanticoagulant using a standard method, or a false-positive serological test for syphilisknown to be positive for at least 6 months and confirmed by Treponema pallidumimmobilization or fluorescent treponemal antibody absorption test.
• Antinuclear antibody — an abnormal titre of antinuclear antibody byimmunofluorescence or an equivalent assay at any point in time and in the absenceof drugs known to be associated with ‘drug-induced lupus’ syndrome.
*Information taken from REFS 3 and 4.

1038 | DECEMBER 2004 | VOLUME 3 www.nature.com/reviews/drugdisc
R E V I E W S
Hispanic and African-American ethnicity, as well aspoverty, might contribute to poor outcomes in nephritisand in other manifestations of lupus — a fact that isacknowledged widely but has been studied minimally30.The prognosis for lupus patients with severe manifesta-tions is currently worse than for many forms of cancer.For this reason, therapies more specifically targeted tothe immune dysregulation of SLE are urgently required.Appropriate randomized trials to better optimize andcompare current therapies in wide empirical use forlupus should be an additional priority.
Aggressive global immune-suppression strategies willprobably always have some place in the management ofSLE patients with acute life-threatening manifestations.However, these treatments remain highly problematicin practical use, and are associated with significantmorbidity, which can be out of proportion to the degreeof illness being treated, and, indeed, unacceptably danger-ous regardless of the clinical urgency. For subgroups ofpatients with mild to moderate or even severe symp-toms, suboptimal treatment, particularly in minoritypopulations, has become the compromise.
Several attempts have been made to test new immune-modulating drugs in the past decade, but none have ledto an FDA-approved treatment for global use in lupus,although there are now several pending applications forlimited use or provisional status. The following is a reviewof recently developed drugs to examine the impedimentsfaced in proving clinical efficacy, and what approachescan be taken to address these impediments (TABLE 3).
Impediments to drug development for lupusLimits to disease activity indices. Several formally vali-dated measures of lupus disease activity are now availablefor use (TABLES 4,5), including SLAM (Systemic LupusActivity Measure), SLEDAI (Systemic Lupus Erythe-matosus Disease Activity Index), LAI (Lupus ActivityIndex), ECLAM (European Consensus Lupus ActivityMeasurement) and BILAG (British Isles Lupus ActivityGroup)34. Primary outcome measurements in multi-centre trials have frequently relied heavily on these tools.Three of the most widely used indices — SLEDAI,SLAM and BILAG — have been validated with regardto uniformity of scoring by different investigators, andassociation with change in disease activity in patientswith SLE in several studies34–39.
In summary, current models of lupus pathogenesisprovide a theoretical framework for understanding howheterogeneous genetic defects might combine in variousways to increase susceptibility to SLE in different individ-uals, and could have important implications for new drugdevelopment. Because lupus is a heterogeneous disorder,in which immune responses can go awry for disparatereasons, mechanistic approaches to treatment either needto target broadly relevant common pathways, or willrequire biological sophistication in the selection of appro-priate subgroups of patients, along with optimization ofadministration and dosing.Attempts should be made tocreate gentler immune-modulating therapies for therestoration of balance in immune networks, rather thanto completely suppress them as current therapies do.
The management of lupus: where do we stand?The introduction of corticosteroids in the 1950s and theaddition of immune-suppressive treatments duringthe next 50 years occurred on a largely empirical basis.This led to gradual improvements in disease manage-ment and quality of life for lupus patients, but unaccept-able side effects. TABLE 1 contains an overview of currenttreatments for SLE, and some of their major toxicities.TABLE 2 compares medications approved by the FDA forSLE with the list of commonly used medications. Manydrugs currently in use remain understudied, unavailableor hard to obtain on standard insurance plans, and sub-standard with regard to evidence-based informationabout optimal administration, dosing and monitoring.
Furthermore, patients with SLE might have intrin-sically increased risks for infection that are furtheramplified by immunosuppressive therapies, particularlycyclophosphamide and high-dose glucocorticoids28,29.Although currently used pharmacological agents haveimproved the prognosis in patients with lupus during thepast 40 years, there is a general consensus that the degreeof control remains suboptimal and that levels of adversereactions are unacceptable29–32. For example, a retro-spective review of 53 paediatric patients with lupusnephritis receiving state-of-the-art treatment found that5-year renal survival for class IV nephritis in children isonly 82.4%33. In an additional study of 128 patientswith proliferative glomerulonephritis, the percentageof patients who did not double their serum creatinineat 5 years was only 67.0%, and at 10 years was 58.9%30.
Table 1 | Current treatments for SLE
Treatment Efficacy (mild/moderate flare) Efficacy (severe flare) Toxicity
Corticosteroids Usually effective (lower doses) Sometimes effective (higher doses) High
NSAIDs Sometimes effective Not effective Moderate
Antimalarials Sometimes effective/long-term use Not effective Low
Azathioprine Usually effective Sometimes effective Moderate
Methotrexate Usually effective Unknown Moderate
Leflunomide Unknown Unknown Moderate
Cyclosporine Not used Sometimes effective High
Cyclophosphamide Not used Sometimes effective High
NSAIDs, non-steroidal anti-inflammatory drugs; SLE, systemic lupus erythematosus.

NATURE REVIEWS | DRUG DISCOVERY VOLUME 3 | DECEMBER 2004 | 1039
R E V I E W S
monthly visits, two thirds of the area under the curveof disease activity during the study period will beblacked out when using the SLEDAI. Several seriousmanifestations of SLE are not included, such ashaemolytic anaemia. Estimates of sensitivity to changeof the different instruments has varied with the stan-dard used, but SLEDAI, not surprisingly, has beenfound to be the least sensitive to change39. A benefit ofSLEDAI is its relative simplicity.
BILAG is the optimal instrument in wide use forlupus trials in the United States because it combinesthe strengths of SLAM (sliding scale for severity) with thestrengths of SLEDAI (weighting for the perceived seri-ousness of a manifestation). Within each organ systemassessed there are various gradations of severity thatcan be applied, rendering this instrument more practicalthan SLEDAI in real-life terms (a patient with severethrombocytopaenia will score higher than a patientwith mild arthritis). Furthermore, this instrumentlends itself to the observation of patterns in individualorgan systems. This provides a major advantage becauseit enables the assessment of medications that might onlybe effective for certain organ manifestations, such asskin flares.
The effectiveness of all of the SLE disease-activityinstruments are further limited by the need for intensiveinvestigator training and continuous quality assuranceprogrammes to ensure consistency and reproducibilityin their use. It remains unclear whether some of theearlier clinical trials in lupus might have fallen short ofdemonstrating efficacy due to intrinsic and/or adminis-trative flaws in the assessment tools. In fact, it hasbecome a standard in designing current clinical trials toinclude training and subsequent validation of the investi-gators in the use of these instruments. Furthermore,guidelines for the use of these instruments are nowincluded in the investigator procedures manuals.
SLICC Damage Index and quality-of-life instruments.In addition, a cumulative damage index has been devel-oped and validated as the Systemic Lupus InternationalCooperating Clinics (SLICC)/ACR Damage Index42,43.In an inception cohort of patients with lupus followedfor at least 15 years, the mean SLICC Damage Indexincreased less than two points after 15 years of follow-up.Despite evidence that damage accumulates very slowly,this instrument has had widespread use in clinical trialsbut, as predicted, has provided little added value to the
The sensitivity to change and responsiveness of SLEactivity indices have been addressed in a small numberof studies. These efforts indicate that the most widelyused systems (SLEDAI, SLAM and BILAG) are sensitiveto change in adults40 and children41. However, littleresearch has been done on the responsiveness of thesemeasures40 to therapy.
SLAM reflects patients’ subjective experiences betterthan the other indices39. Unfortunately, SLAM is weightedonly by the severity of individual symptoms withoutconsideration for the significance of the manifestationinvolved. Therefore, a patient with largely subjectiveconstitutional complaints such as fatigue, headache andarthralgia might score an equal value as a patient withactive nephritis, severe thrombocytopaenia or cognitivedysfunction. This renders global scoring problematic.
SLEDAI is the most objective of the instruments,relying almost entirely on verifiable data. However, it hasseveral limitations relevant to use in clinical trials as aprimary outcome measure. It is weighted only by theperceived importance of an organ system, rather than bygraded severity within that organ system. For example, alife-threatening platelet count receives a lower score thanisolated low complements or a mildly active discoidlesion in the scalp. It is an all-or-none instrument,scored in the presence (or persistence) of any symp-toms, whether they are improving or worsening. Thisnarrows the gap between an effective drug and placeboin a drug study. If two patients enter the study withmoderate arthritis and one has partial improvementand the other worsens, the scores remain identical.SLEDAI captures only signs and symptoms that haveoccurred within a ten-day window. In a study assessing
Table 2 | Medications to treat SLE
Medication Frequency of use in SLE FDA approval for SLE
Corticosteroids High Yes
Hydroxychloroquine High Yes
Aspirin Low Yes
Azathioprine High No
Methotrexate High No
Cyclophosphamide High in severe SLE No
Other NSAIDs/DMARDs Moderate No
DMARDs, disease-modifying antirheumatic drugs; FDA, Food and Drug Administration; NSAIDs,non-steroidal anti-inflammatory drugs; SLE, systemic lupus erythematosus.
Table 3 | Drugs in recent or current development for SLE
Approach Mechanism Example Developer(s)
Hormonal therapy Weak androgen Prasterone Genelabs, Inc.
Proliferation inhibition Purine synthesis inhibitor Mycophenolate Roche/Aspreva
Tolerization attempt Surrogate antigen Abetimus sodium La Jolla Pharmaceutical
Tolerization attempt Surrogate antigen LJP 1082 La Jolla Pharmaceutical
B-cell regulation CD154 antagonism IDEC 131, BG9588 IDEC and Biogen
B-cell regulation BLyS antagonism Lymphostat B Human Genome Sciences
B-cell depletion Antibody to CD20 Rituximab Genentech/Biogen/IDEC/Roche
BLyS, B-lymphocyte stimulator; SLE, systemic lupus erythematosus.

1040 | DECEMBER 2004 | VOLUME 3 www.nature.com/reviews/drugdisc
R E V I E W S
Biomarkers. The availability of validated biologicalmarkers in SLE will be an important advance in theassessment of new treatments for SLE and the optimiza-tion of their use. Specifically, a credible set of biomarkersmight be predictive of whether a given patient isappropriate for a treatment, provide a characteriza-tion of disease activity and help to guide therapy. It islikely that only a limited set of promising candidates canbe reproducibly validated. It is equally likely that only asubset of those markers will be validated as surrogateendpoints (defined as markers that are detected early inthe course of therapy, respond appropriately to therapy
assessment in studies of relatively short duration.Although measurement of cumulative damage isimportant in assessing long-term effects of drugs, it isless valuable in Phases I–III of human trials.
There is no health status or disability instrumentspecific to SLE. However, the Medical Outcomes Survey(SF-36) is a widely accepted measurement to of healthstatus and health-related quality of life in lupus patientsbecause of its widespread use, and previous internationalvalidation, for many rheumatic diseases42. Interestingly,data from the SF-36 might prove more sensitive tochange than the lupus-specific activity indices.
High-riskpolymorphism:Gene 1
Gene 3:strongamelioration
Gene 2:weakamelioration
Gene 5:strongexacerbation
Gene 4:weakexacerbation
T cell
B cell
H1-specificT cell
B cell
MacrophageApoptotic cell
Membrane blebwith antigens
a
b
c
IL-4
CD40L
CD40
Nucleosome
DNA
H1
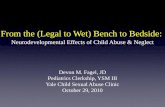
Figure 1 | Immune system in SLE. a | Systemic lupus erythematosus (SLE) risk probably evolves as a net effect of multipleinteracting genes and environmental influences. In a classic TH2 type immune response, invading antigen is recognized bysurface immunoglobulin on a B cell and presented to a T cell. Signals pass between the B and T cells, leading to stimulation ofgerminal centres and the generation of an antibody response directed against the perceived pathogen. Several processes cancontribute to the diversity (and hence the versatility) of an immune response. If an immune response persists too long, the resultis an increased degree of immunoglobulin rearrangement and/or hypermutation leading to new antibody specificities that couldbe more effective in eliminating a recalcitrant invader. Eventually this can lead to increased production of autoantibodies thathave the capacity to bind to self-antigens and stimulate (or perpetuate) inflammation in target organs. b | Autoantibodies arenot necessarily an aberrant element in the immune response. As cells undergo programmed death, antigens that are normallysequestered from immune surveillance inside the cell translocate to the surface in membrane blebs. These are recognized ascommon lupus autoantigens. Autoantibodies may develop in service to the organism, opsonizing the dead cell via these newlyexposed surface antigens to facilitate immune clearance by phagocytosis. Circulating antibodies specific for antigens thatcome up with the membrane blebs on apoptotic cellmembranes attach to the Fc receptors on macrophages and cause theingestion of the apoptotic debris, which dampens the immune response. In SLE there is defective phagocytosis. This mightlead to persistent autoantibody production. These antibodies continue to permutate and spread their binding capabilities tomore and more self-structures, perpetuating the immune response to pathologica levels. c | This figure depicts an example ofhow, in SLE patients, a B cell might recognize, internalize and process the material in the nucleosome followed by thepresentation of self antigen to a T cell. Modified, with permission, from REF. 126 © (1999) Current Biology Ltd.

NATURE REVIEWS | DRUG DISCOVERY VOLUME 3 | DECEMBER 2004 | 1041
R E V I E W S
later-phase trials, of understanding the best ways toadminister new therapies, of saving significant develop-ment costs, and providing the FDA with better data forassessing investigational treatments.
In addition, a biomarker validation effort that isindependent of drug development efforts could addressserious design limitations intrinsic to current pharma-ceutical trials. The largest investigational drug trialsbeing envisioned for lupus at this time will recruit nomore than 300–350 patients, which is under-poweredfor biomarker subset analysis. Furthermore, the back-ground medications in investigational drug trials in SLEare quite variable. The assumption is that if a patient isflaring through prednisone, azathioprine or mycopheno-late mofetil (CellCept; Roche), then the medications arenot effective in that given situation and their influence isconsidered inconsequential. From a clinical perspective,this might be valid. However, with respect to biomarkersthis might not be the case. A better understanding of therelationships between the various agents used in SLEand their effects on different biomarkers versus diseaseactivity is a pressing concern in the translation of theserecently discovered, potentially important markers tothe support of novel drug development.
Given the heterogeneity of lupus and its relative rarity,which limits the number of patients available for thegrowing number of clinical trials being planned, it seemsextremely unlikely that in the near future industry-sponsored trials can reduce the background therapies toa common denominator. This would pose a formidablerecruitment problem, in that most of the multicentrestudies currently being designed would no longer befeasible. Therefore, data from biomarker validationstudies could be of great value to investigators planningtrials by providing validated objective outcome measuresand a reasonable idea of whether given backgroundtherapies will or will not cause confounding resultswhen using these biomarkers as tools.
Finally, despite the fact that biomarkers have beenactively studied in the context of several clinical trialsfor lupus in the past decade, no publications regardingbiomarkers have yet emerged from any industry-sponsored trials since 1994. This is probably due to acombination of factors, including company priorities inpreparing data for the FDA, and loss of interest whentrials do not demonstrate the predicted efficacy.Therefore, an independent biomarker validation effortcould provide a timely addition to an under-studiedfield at a point when drug development for systemiclupus is rapidly expanding.
Limitations to currently used lupus therapiesThere is no doubt that corticosteroids, which were life-saving 50 years ago, remain a staple in lupus treatment,predominately because they have a dramatic and nearlyimmediate impact on lupus flares. Unfortunately, thesehighly effective drugs are also a major cause of morbidityand mortality28,59–61.
Other widely used treatments for lupus are the anti-malarials, particularly hydroxychloroquine. This classof drug is effective for milder manifestations62–65, with
and are predictive of longer-term outcomes). Thosemarkers that meet criteria for surrogate endpoints willimprove the efficiency of clinical trials, in some casesdecreasing the time frame of the trial. In longer trials, sur-rogate endpoints could be used to optimize therapeuticregimens early in the study.
To date, not a single candidate biomarker has beenuniformly validated for any aspect of SLE. Potentialcandidate biomarkers have been summarized by theSLE Biomarkers Working Group (BOX 2). These includethe type-1 interferon system44,45, anti-dsDNA antibodiesand complement46–48, vascular cell-adhesion molecule 1(VCAM1)49,50, B-lymphocyte stimulator (BLyS)51–56 andsoluble CD27 levels57,58.
Previous studies to assess these potential biomarkersin human lupus have generated ambiguous results, whichis probably due to small sample sizes, absence of controlsand restriction to single centres. Disparate definitions oflupus disease activity or flare and variable, sometimesundefined, background therapies ongoing in the patientsunder study limit the generalizability of these studies.Moreover, meaningful conclusions have been thwarted byinconsistencies in laboratory testing methods, absence ofuniform subpopulations under study and substandardapplication of the clinical activity indices. The biomarkersproposed by the Biomarkers Working Group as mostlikely to be validated in a rigorous prospective clinical trialemerged, despite the shortcomings stated.
Validation of these biomarkers would be comple-mentary to ongoing pharmaceutical studies, and allowsthe external reassessment of findings from sponsored,drug-specific trials, and an improved ability to deter-mine the general applicability of published outcomes.One major goal of such a study would be to determinewhether any of these candidate markers can serve as anearly surrogate for longer-term outcomes. If so, thiscould increase the chances of redesigning more efficient
Box 2 | Biomarkers for SLE: pitfalls in proof
Biomarkers proposed by the systemic lupuserythematosus (SLE) Biomarkers Working Group
• Type-1 interferon system
• Anti-dsDNA and complement
• Vascular cell adhesion molecule 1
• B-lymphocyte stimulator (BLyS)
• Soluble CD27
Problems impeding past human SLE biomarkerevaluation
• Insufficient sample size
• Absence of controls in some studies
• Single-centre studies
• Disparate definitions of flare
• Variable background therapies
• Inconsistencies in laboratory techniques
• Heterogeneity of study populations
• Imprecise use of disease indices

1042 | DECEMBER 2004 | VOLUME 3 www.nature.com/reviews/drugdisc
R E V I E W S
profile is equivalent. Methotrexate in relatively modestdoses is now widely used for cutaneous and articularmanifestations79.
Cyclosporine has been used in moderate to severesystemic lupus for a number of years, although notwidely. Formal study of this medication in human trialsis scant80,81. Depending on the individual patient,cyclosporine would not be recommended as a first-lineagent, because less toxic medications seem to be as effec-tive, at least in the short term. Its current place seems tobe in treating recalcitrant membranous nephritis.
Supporting therapies with anticoagulants andother vascular regulators are an integral part of themanagement of patients with SLE. The antiphospho-lipid syndrome — which might exist as an independentdiagnosis, but which is a frequent manifestation oflupus — is an important cause of arterial and venousthromboses, pregnancy loss and thrombotic manifes-tations, which can coexist with classic lupus nephritisand contribute to poor outcomes. A number of treat-ments, including steroids, aspirin, heparin, statins andimmunoglobulin, alone or in combination, have beenassessed in clinical series82.
Several other agents are worthy of mention, partic-ularly for use in various forms of cutaneous lupus,either alone or in combination with the more com-monly used agents listed above. These include dapsone(which might be the drug of choice for bullous lupus),thalidomide (helpful in refractory cases of discoidlupus) and retinoids (which have particular efficacy inhypertrophic LE)83.
Finally, high-dose chemotherapy and stem-celltransplantation, as well as immune ablation withouttransplantation, have been examined in a limited num-ber of patients and could be efficacious in patients withsevere SLE84,85. However, the sporadic and unpredictablenature of life-threatening manifestations of SLE, and thefrequency with which severe organ damage is irreversibleonce it occurs, restricts the potential of this intervention.
New treatment options for lupus patientsHormonal therapy: dehydroepiandrosterone (Prasterone).Deficiency of the weak androgen dehydroepiandros-terone (DHEA) has been associated with lupus86. Thereis trial evidence indicating DHEA might be steroid-sparing in patients with active disease, improve patients’perceptions of health and functionality, improve bonedensity in lupus patients and increase the time toflare86–88. However, difficulties with the design andexecution of these studies could have contributed toan inability to differentiate this drug from placebo inprimary outcomes.
Hormonal therapy: purine pathway inhibition revisitedwith a newer agent — mycophenolate mofetil. Myco-phenolate mofetil (MMF) is an approved immuno-suppressive agent for the prevention of organ transplantrejection, which targets the purine pathway at a pointintermediate to the activities of methotrexate and aza-thioprine. Several preliminary studies have indicated thatit might be useful in the treatment of lupus nephritis89–94.
the added benefit of modulating dyslipoproteinaemiaand improving bone-mineral density in SLE patients62–64,two problems exacerbated by steroid use.
The use of cyclophosphamide in lupus nephritisdates back to the 1960s, and the results of a controlledtrial were first reported in 1971 (REF. 66). Prolonged follow-up of a National Institutes of Health-based cohort ofpatients suggested that long-term therapy with cyclo-phosphamide enhances renal survival in patients withproliferative lupus nephritis. Furthermore, it is thefirst-line treatment for severely ill lupus patients withorgan-threatening or life-threatening disease, such aslupus vasculitis. Despite significant toxicity associatedwith cyclophosphamide, it clearly reduces morbidity andmortality in lupus patients. Nausea and vomiting, hairloss, leukopaenia, infections, gonodal failure, bladdertoxicity and, rarely, malignancies are some of the well-documented side effects of cyclophosphamide. Fibrosisof ovarian follicles is age- and dose-dependent67–69, andtherefore a serious issue in the treatment of all women ofchild-bearing potential. In addition, this treatment isassociated with a relatively high relapse rate.
Azathioprine is a purine analogue that is widelyused for the long-term management of moderate tosevere manifestations, frequently as a ‘steroid-sparing’agent70–77. On the basis of limited evidence, azathio-prine has also been used extensively for maintenancetherapy, once renal remission has been achieved,although its use as induction therapy in nephritis hasbeen disappointing to date73–77. Individualized patienttherapy based on genetic background and monitoringof active metabolites is potentially possible with thisdrug, and could provide the optimal means by which tosafely and effectively prescribe it in the near future.
Leflunomide, like several other drugs that are mar-keted for rheumatoid arthritis, has come into occasionaluse in lupus patients, although there are only limitedpublished data in support of this practice78. There are nodata to indicate that it is any more effective than the morecommonly prescribed methotrexate, and the side-effect
Table 4 | Overview of SLE disease activity measurement instruments
Instrument Ranking priority Problem
SLEDAI Generally weighs importance Within organ, degree and change of organ not factored
SLAM Degree of symptom Importance of organ not factored
BILAG Importance of organ and degree Complexity of instrumentof symptom
BILAG, British Isles Lupus Activity Group; SLAM, Systemic Lupus Activity Measure; SLE, systemiclupus erythematosus; SLEDAI, Systemic Lupus Erythematosus Disease Activity Index.
Table 5 | Strength of instruments used as specific outcome measures
Instrument Strength Best use
SLEDAI More specific to lupus Entry criteria, equivalence or broad outcomes
SLAM Most sensitive Reflects patients’ subjective responses
BILAG Most accurate global measure By qualified investigators
BILAG, British Isles Lupus Activity Group; SLAM, Systemic Lupus Activity Measure; SLE, systemiclupus erythematosus; SLEDAI, Systemic Lupus Erythematosus Disease Activity Index.

NATURE REVIEWS | DRUG DISCOVERY VOLUME 3 | DECEMBER 2004 | 1043
R E V I E W S
generated a significant anti-idiotypic response withoutevidence of lupus flares, which would be a concern duringattempts to stimulate a network response
B cells or B-cell regulation: antagonists of CD154. Patientswith active lupus nephritis exhibit high B-cell germinalcentre activity, reflecting interactions between CD40 andits ligand, CD 154 (REF. 100). Signalling through CD40 isknown to have an important role in B-cell proliferationand in classical pathways of autoantibody production inhuman SLE101. However, the interactions of this moleculeare complicated102–104 and the consequence of circulatingCD154 (exacerbating or ameliorating the inflammatoryresponse) remains to be determined.
Absence of predicted consequences notwithstanding,interactions between CD40 and CD154 probably con-tribute to development and activity in several animalmodels105–110. In a preliminary sub-study involving 5patients with SLE nephritis who were treated with anti-CD154, the frequency of B cells producing immuno-globulin G (IgG) anti-DNA was reduced, and thesechanges persisted for several months after treatment111.
Two companies have initiated developmental pro-grammes for antibodies to CD154 as potential therapiesfor SLE. In Phase I and II trials, the humanized mono-clonal anti-CD154 antibody IDEC-131 (Biogen Idec) waswell tolerated, but efficacy compared with placebowas, unfortunately, not demonstrated112,113.
During the same time period, Biogen was studyinga different anti-CD154 therapy for several indications,including lupus nephritis. The lupus programme wasput on hold after a Phase II study was interrupted dueto thromboembolic events that had occurred in sev-eral protocols. Of the 18 patients for whom efficacycould be evaluated, 2 had a 50% reduction in protein-uria. A decrease in anti-dsDNA antibodies was alsoobserved, along with increased C3 concentrations andimproved haematuria, indicating that, despite therisks involved, the drug has appropriate biologicaleffects114. The mechanism responsible for these multi-ple thrombotic events has not yet been defined.Possibilities include signalling effects involving mono-cytes or platelets or a formulary issue unrelated to thebiology of anti-CD154.
A major unanswered question is why one antibody toCD154 was ineffective but apparently safe, whereasanother (targeting the same molecule) achieved a biologi-cal effect but was accompanied by unacceptable throm-botic side effects. Of possible relevance is that the Biogenproduct was delivered at twice the maximal dose used inthe IDEC trial, and that these two antibodies target dif-ferent epitopes on CD154. It is unfortunate that bothdevelopment programmes were terminated, becauseunderstanding these events might lead to a safe and highlyeffective treatment for lupus via modulation of CD154.
B cells or B-cell regulation: BLyS antagonism. Elevatedlevels of BLyS have been implicated in the pathogenesis ofautoimmune diseases. This molecule is secreted bymonocytes and affects B-cell activation, with stimulatoryeffects on antibody development in response to several
In a single-centre study from Miami91, 59 patients withproliferative nephritis received induction therapywith cyclophosphamide and corticosteroids, and weresubsequently randomized to maintenance with quarterlycyclophosphamide, oral azathioprine or oral MMF.During maintenance therapy, a significantly greaternumber of patients died or progressed to renal failure inthe cyclophosphamide group than in the other twogroups. Additionally, morbidity was higher, includinginfections and hospitalizations, in those patients receivingcyclophosphamide91. These data support the use of eitherazathioprine or MMF in the maintenance phase, onceremission has been induced.
Targeted immune modulation: abetimus sodium.Abetimus sodium (LJP 394/Riquent; La Jolla) is a syn-thetic molecule consisting of four double-strandedoligodeoxyribonucleotides attached to a proprietarycarrier platform consisting of non-immunogenic poly-ethylene glycol. The goal is to introduce a surrogateantigen for pathological antibodies, which is intended tocrosslink immunoglobulin on susceptible B cells. It ishypothesized that this might tolerize the B cells to furtherantigenic stimulus95.
In the process of seeking out the appropriate B-celltarget, the potentially tolerizing molecule is likely toencounter circulating antibody.A possible factor, then, inconsidering the optimal strategy for dosing and adminis-tration of this therapy is to identify whether circulatingantibodies would saturate the toleragen, restricting thedegree to which tolerization is practical. To date, nohuman evidence of tolerization has been produced,despite the finding that the therapy seems promising anddepletes levels of the circulating targeted antibodies96,97.
Phase I, II and III studies have been completed,which have collectively involved nearly 1,000 patients98.Importantly, no significant toxicity has been observedwith this treatment, and there is no evidence that it isimmune-depleting. In patients with a history of lupusnephritis and elevated anti-DNA (Farr assay) withhigh affinity to abetimus, the treatment significantlydecreases anti-DNA antibodies, improves quality of lifeand produces a trend towards reducing the incidence ofrenal flares98 as compared with placebo groups.Althoughunambiguous efficacy remains unproven, and there islittle evidence to date of its toleragenicity, the availabledata indicate that there should be strong interest inpursuing further work with this treatment, possibly byusing anti-DNA antibody depletion as a biologicalmarker for a dose-optimizing strategy.
La Jolla Pharmaceutical Co. has completed a Phase Itrial of an additional toleragen, aimed at a linear,extended epitope segment of β
2glycoprotein I, a major
target antigen for the antiphospholipid syndrome. Otheragents that involve surrogates to deflect autoantibodiesfrom their targets are also in development. One approachis to generate anti-idiotypic responses to pathogenic anti-body structures. In a preliminary study, nine stablepatients with a history of lupus nephritis were injectedwith the murine anti-dsDNA antibody Mab 3E10 (REF. 99).Immunization with this antibody seems to be safe and

1044 | DECEMBER 2004 | VOLUME 3 www.nature.com/reviews/drugdisc
R E V I E W S
However, several potential biological pitfalls merit con-cern with the use of these novel agents. First, humanantibody responses to immunoglobulin and receptortherapies might be more frequent and dangerous inlupus patients. Second, manipulation of the delicatebalance that exists between various elements of complexinflammatory signalling pathways might have unpre-dictable effects, particularly in patients in which theunderlying defects in these pathways remain incom-pletely identified. Last, multiple interfaces betweeninflammatory mediators and coagulation proteins orother vascular regulators have been described in recentyears but are not yet well understood. Therefore, cautionis advised in the study of selective response modifiers ina population already at increased risk for thrombosis,vasculitis and atherosclerosis.
The major impediments to successful drug devel-opment for lupus will be solved when the communitycan successfully integrate emerging knowledge on agenetic and molecular level about the nature of theimmune dysfunction, with adequate definitions ofdisease flare and remission. A crucial component of thisprocess will be the validation and strategic use of acomprehensive set of biological markers to optimizeadministration of investigational immune-modulatingagents and to assess their effectiveness. Methods ofselecting and evaluating lupus patients in recent multi-centre clinical trials have been challenging. Patientselection for new treatments could be made far morerational, and the administration of both establishedand investigational treatments optimized, by using amore effective set of objective guidelines, some sectionsof which, such as the BILAG instrument, are alreadyin the public domain. However, other parts of thesolution are urgently overdue, particularly the assess-ment and validation of biomarkers in collaborativecohort studies and within the context of ongoingequivalence and efficacy trials.
Although these concepts merit some considerationfor any disease and any drug development programme,they are so crucial to understanding the multifacetedmanifestations of SLE that this has become an imme-diate problem. Current treatments for this chronic,disabling and potentially life-threatening disease arenot evidence-based. Accordingly, most of the medica-tions now used to treat moderate to severe lupus flaresare not FDA-approved treatments, and have neverbeen studied to the degree which would warrantapproval. These are certainly urgent concerns for lupuspatients and their physicians.
signals. Elevated serum BLyS and BLyS mRNA seem to becommon in SLE, but not healthy controls51,52. SurfaceBLyS expression on SLE peripheral blood mononuclearcells is also increased51,53 and serum BLyS levels have beencorrelated with anti-dsDNA titres in some patients51.Overexpression of BLyS in mice has been observed tolead to SLE-like disease52, and treatment of such micewith a BLyS antagonist can ameliorate disease progres-sion and enhance survival, indicating that BLyS might bean attractive therapeutic target for human lupus.
Several unresolved issues remain, including thepotential homeostasis conferred by a family of mole-cules related to BLyS52–55, which might form into func-tional units with BLyS. This could introduce somecomplexity into the identification of the optimal regi-men for BLyS antagonism, as well as in the identificationof those SLE patients most likely to benefit fromBLyS-antagonist therapy.
Several companies are currently testing BLyS antago-nists. The furthest advanced in human SLE trials is themonoclonal antibody LymphoStat-B (Human GenomeSciences)56 LymphoStat-B is known to bind with highaffinity to human BLyS and inhibits binding of BLySto all of its known receptors, inhibiting BLyS-inducedB-cell proliferation in vitro and in a murine model56.In a cynomolgus monkey model, administration ofLymphoStat-B decreased B cells in the spleen and inmesenteric lymph nodes56.
B cells or B-cell regulation: B-cell-depleting therapy. Anumber of case reports and series have suggested thatrituximab (Rituxan; Genentech/Biogen Idec), the CD20antagonist which has proven highly effective for B-celllymphomas, might be useful for lupus-like syndromes, inparticular autoimmune thrombocytopaenia97,98,115–125.
There have been several case series in lupuspatients115–119. In some, B-cell depletion was not found tocorrelate with responsiveness, although various defini-tions for depletion have been used. In one open-labelstudy, at 2 months post-treatment, B-cell percentageswere highly correlated with both serum rituximab leveland FcγRIIIa genotype116, indicating that much remainsto be learned before we can optimize responses to thispotentially promising agent in individual patients.
ConclusionsTargeted immune therapies raise both hopes and con-cerns. It is proposed, with good reason, that furtherdevelopment of targeted immune-modulating therapieswill lead to safer and more specific treatments for SLE.
1. Boumpas, D. T. et al. Systemic lupus erythematosus:emerging concepts. Part 1: renal, neuropsychiatric,cardiovascular, pulmonary, and hematologic disease. Ann. Intern. Med. 122, 940–950 (1995).A review article on the pathogenesis, diagnosis andmanagement of dermatological and jointmanifestations of SLE.
2. Boumpas, D. T. et al. Systemic lupus erythematosus:emerging concepts. Part 2: dermatologic and joint disease,the antiphospholipid antibody syndrome, pregnancy andhormonal therapy, morbidity and mortality, andpathogenesis. Ann. Intern. Med. 123, 42–53 (1995).
A review article on the pathogenesis, diagnosis andmanagement of visceral manifestations of SLE.
3. Tan, E. M. et al. The 1982 revised criteria for theclassification of systemic lupus erythematosus. ArthritisRheum. 25, 1271–1277 (1982).This paper describes the 1982 revised classificationcriteria for SLE.
4. Hochberg, M. C. Updating the American College ofRheumatology revised criteria for the classification of systemiclupus erythematosus. Arthritis Rheum. 40, 1725 (1997).Provides an updated version of the 1982 revisedclassification criteria for SLE.
5. Mohan, C., Yu, Y., Morel, L., Yang, P. & Wakeland, E. K.Genetic dissection of SLE pathogenesis: Sle3 on murinechromosome 7 impacts T cell activation, differentiation, andcell death. J. Immunol. 162, 6492–6502 (1999).
6. Morel, L. et al. Multiplex inheritance of componentphenotypes in a murine model of lupus. Mamm. Genome.10, 176–181 (1999).
7. Alarcon-Riquelme, M. E. & Prokunina, L. Finding genes forSLE: complex interactions and complex populations. J. Autoimmun. 21, 117–120 (2003).
8. Namjou, B. et al. Stratification of pedigrees multiplex forsystemic lupus erythematosus and for self-reported

NATURE REVIEWS | DRUG DISCOVERY VOLUME 3 | DECEMBER 2004 | 1045
R E V I E W S
rheumatoid arthritis detects a systemic lupus erythematosussusceptibility gene (SLER1) at 5p15. 3. Arthritis Rheum. 46,2937–2945 (2002).
9. Tsao, B. P. et al. Linkage and interaction of loci on 1q23 and16q12 may contribute to susceptibility to systemic lupuserythematosus. Arthritis Rheum. 46, 2928–2936 (2002).
10. Olson, J. M. et al. A genome screen of systemic lupuserythematosus using affected-relative-pair linkage analysiswith covariates demonstrates genetic heterogeneity. GenesImmun. 3 (Suppl. 1), S5–S12 (2002).
11. Arbuckle, M. R., Reichlin, M., Harley, J. B. & James, J. A.Shared early autoantibody recognition events in thedevelopment of anti-Sm B/B’ in human lupus. Scand. J.Immunol. 50, 447–455 (1999).
12. James, J. A. & Harley, J. B. A model of peptide-inducedlupus autoimmune B cell epitope spreading is strain specificand is not H-2 restricted in mice. J. Immunol. 160, 502–508(1998).
13. Kammer, G. M., Laxminarayana, D. & Khan, I. U.Mechanisms of deficient Type I protein kinase A activity inlupus T lymphocytes. Int. Rev. Immunol 23, 225–244 (2004).
14. Takeuchi, T., Tsuzaka, K. & Abe, T. Altereed expression ofthe T cell receptor–CD3 complex in sle. Int. Rev. Immunol23, 273–291 (2004).
15. Grammer, A. C. & Lipsky, P. E. B cell abnormalities in systemiclupus erythematosus. Arthritis Res. Ther. 5 (Suppl. 4), S22–27(2003).
16. Kim, S. J., Gershov, D., Ma, X., Brot, N. & Elkon, K. B.Opsonization of apoptotic cells and its effect onmacrophage and T cell immune responses. Ann. NY Acad.Sci. 987, 68–78 (2003).
17. Ravirajan, C. T., Pittoni, V. & Isenberg, D. A. Apoptosis inhuman autoimmune diseases. Int. Rev. Immunol. 18,563–589 (1999).
18. Grodzicky, T. & Elkon, K. B. Apoptosis: a case where toomuch or too little can lead to autoimmunity. Mt Sinai J. Med.69, 208–219 (2002).
19. Baumler, C., Kim, G. O. & Elkon, K. B. Growth regulation ofactivated lymphocytes: defects in homeostasis lead toautoimmunity and/or lymphoma. Rev. Immunogenet. 2,283–290 (2000).
20. Kay, M. M. & Goodman, J. Immunoregulation of cellularlifespan: physiologic autoantibodies and their peptideantigens. Cell. Mol. Biol. 49, 217–243 (2003).
21. Gardner-Thorpe, J., Ito, H., Ashley, S. W. & Whang, E. E.Autoantibody-mediated inhibition of pancreatic cancer cellgrowth in an athymic (nude) mouse model. Pancreas 27,180–189 (2003).
22. Stafford, H. A., Anderson, C. J. & Reichlin, M. Unmaskingof anti-ribosomal P autoantibodies in healthy individuals.J. Immunol. 155, 2754–2761 (1995).
23. Bouvet, J. P. et al. Induction of natural autoantibody activityfollowing treatment of human immunoglobulin withdissociating agents. J. Autoimmun. 16, 163–172 (2001).
24. Rahman, A. Autoantibodies, lupus and the science ofsabotage. Rheumatology (Oxford) 43, 1326–1336 (2004).
25. Crow, M. K. & Kirou, K. A. Interferon-α in systemic lupuserythematosus. Curr. Opin. Rheumatol. 16, 541–547 (2004).
26. Illei, G. G., Tackey, E., Lapteva, L. & Lipsky, P. E. Biomarkersin systemic lupus erythematosus. I. General overview ofbiomarkers and their applicability. Arthritis Rheum. 50,1709–1720 (2004).The first part of a review article on the biomarkers thatcan be used to predict prognosis, characterizedisease activity and guide therapy in SLE patients.
27. Illei, G. G., Tackey, E., Lapteva, L. & Lipsky, P. E. Biomarkersin systemic lupus erythematosus: II. Markers of diseaseactivity. Arthritis Rheum. 50, 2048–2065 (2004).The second part of a review article on the biomarkersthat can be used to predict prognosis, characterizedisease activity and guide therapy in SLE patients.
28. Badsha, H. & Edwards, C. J. Intravenous pulses ofmethylprednisolone for systemic lupus erythematosus.Semin. Arthritis Rheum. 32, 370–377 (2003).
29. Kang, I. & Park, S. H. Infectious complications in SLE afterimmunosuppressive therapies. Curr. Opin. Rheumatol. 15,528–534 (2003).
30. Barr, R. G. et al. Prognosis in proliferative lupus nephritis: therole of socio-economic status and race/ethnicity. Nephrol.Dial. Transplant. 18, 2039–2046 (2003).
31. Cortes-Hernandez, J. et al. Predictors of poor renaloutcome in patients with lupus nephritis treated withcombined pulses of cyclophosphamide andmethylprednisolone. Lupus 12, 287–296 (2003).
32. Isenberg, D. & Leckie, M. J. Biological treatments forsystemic lupus erythematosus. Scand. J. Rheumatol. 31,187–191 (2002).
33. Bogdanovic, R. et al. Lupus nephritis in childhood: a reviewof 53 patients followed at a single center. Pediatr. Nephrol.19, 36–44 (2004).
34. Gladman, D. D. Indicators of disease activity, prognosis,and treatment of systemic lupus erythematosus. Curr. Opin.Rheumatol. 6, 487–492 (1994).
35. Gladman, D. D. et al. Sensitivity to change of 3 systemiclupus erythematosus disease activity indices: internationalvalidation. J. Rheumatol. 21, 1468–1471 (1994).
36. Hay, E. M. et al. The BILAG index: a reliable and validinstrument for measuring clinical disease activity insystemic lupus erythematosus. Q. J. Med. 86, 447–458(1993).
37. Gladman, D. D. et al. Crosscultural validation and reliability of3 disease activity indices in systemic lupus erythematosus.J. Rheumatol. 19, 608–611 (1992).
38. Bencivelli, W. et al. Disease activity in systemic lupuserythematosus: report of the Consensus Study Group of theEuropean Workshop for Rheumatology Research. III. Clin.Exp. Rheumatol. 10, 549–554 (1992).
39. Ward, M. M., Marx, A. S., Barry, N. N. Comparison of thevalidity and sensitivity to change of 5 activity indices insystemic lupus erythematosus. J. Rheumatol. 27, 664–670(2000).
40. Corzillius, M., Fortin, P. & Stucki, G. Responsiveness andsensitivity to change of SLE disease activity measures.Lupus 8, 655–9 (1999).
41. Brunner, H. I., Feldman, B. M., Bombardier, C. &Silverman, E. D. Sensitivity of the Systemic LupusErythematosus Disease Activity Index, British Isles LupusAssessment Group Index, and Systemic Lupus ActivityMeasure in the evaluation of clinical change in childhood-onset systemic lupus erythematosus. Arthritis Rheum. 42,1354–1360 (1999).
42. Stoll, T. et al. Consistency and validity of patientadministered assessment of quality of life by the MOS SF-36; its association with disease activity and damage inpatients with systemic lupus erythematosus. J. Rheumatol.24, 1608–1614 (1997).
43. Stoll, T., Stucki, G., Malik, J., Pyke, S. & Isenberg, D. A.Association of the Systemic Lupus InternationalCollaborating Clinics/American College of RheumatologyDamage Index with measures of disease activity and healthstatus in patients with systemic lupus erythematosus. J. Rheumatol. 24, 309–313 (1997).
44. Baechler, E. C. et al. Interferon-inducible gene expressionsignature in peripheral blood cells of patients with severelupus. Proc. Natl Acad. Sci. USA 100, 2610–2615 (2003).
45. Bennett, L. et al. Interferon and granulopoiesis signatures insystemic lupus erythematosus blood. J. Exp. Med. 197,711–723 (2003).
46. Nagy, G., Brozik, M., Tornoci, L. & Gergely, P. Diagnosticvalue of combined evaluation of neopterin and anti-DNAantibody levels for assessment of disease activity insystemic lupus erythematosus. Clin. Exp. Rheumatol. 18,699–705 (2000).
47. Mollnes, T. E. et al. Complement activation in patients withsystemic lupus erythematosus without nephritis.Rheumatology (Oxford) 38, 933–940 (1999).
48. Nagy, G. et al. Usefulness of detection of complementactivation products in evaluating SLE activity. Lupus 9,19–25 (2000).
49. Horak, P. et al. Clinical utility of selected disease activitymarkers in patients with systemic lupus erythematosus.Clin. Rheumatol. 20, 337–344 (2001).
50. Belmont, H. M., Buyon, J., Giorno, R. & Abramson, S.Up-regulation of endothelial cell adhesion moleculescharacterizes disease activity in systemic lupuserythematosus. The Shwartzman phenomenon revisited.Arthritis Rheum. 37, 376–383 (1994).
51. Stohl, W. et al. B lymphocyte stimulator overexpression inpatients with systemic lupus erythematosus: longitudinalobservations. Arthritis Rheum. 48, 3475–3486 (2003).
52. Stohl, W. SLE — systemic lupus erythematosus: a BLySful,yet BAFFling, disorder. Arthritis Res. Ther. 5, 136–138(2003).
53. Kawasaki, A., Tsuchiya, N., Fukazawa, T., Hashimoto, H. &Tokunaga, K. Analysis on the association of human BLYS(BAFF, TNFSF13B) polymorphisms with systemic lupuserythematosus and rheumatoid arthritis. Genes Immun. 3,424–429 (2002).
54. Roschke, V. et al. BLyS and APRIL form biologically activeheterotrimers that are expressed in patients with systemicimmune-based rheumatic diseases. J. Immunol. 169,4314–4321 (2002).
55. Seshasayee, D. et al. Loss of TACI causes fatallymphoproliferation and autoimmunity, establishing TACIas an inhibitory BLyS receptor. Immunity 18, 279–288(2003).
56. Baker, K. P. et al. Generation and characterization ofLymphoStat-B, a human monoclonal antibody thatantagonizes the bioactivities of B lymphocyte stimulator.Arthritis Rheum. 483, 253–265 (2003).
57. Swaak, A. J., Hintzen, R. Q., Huysen, V., van den Brink, H. G.& Smeenk, J. T. Serum levels of soluble forms of T cellactivation antigens CD27 and CD25 in systemic lupuserythematosus in relation with lymphocytes count anddisease course. Clin. Rheumatol. 14, 293–300 (1995).
58. Font, J. et al. Elevated soluble CD27 levels in serum ofpatients with systemic lupus erythematosus. Clin. Immunol.Immunopathol. 81, 239–243 (1996).
59. Stojanovich, L., Stojanovich, R., Kostich, V. & Dzjolich, E.Neuropsychiatric lupus favourable response to low dose i. v.cyclophosphamide and prednisolone (pilot study). Lupus12, 10–15 (2003).
60. Zonana-Nacach, A., Barr, S. G., Magder, L. S. & Petri, M.Damage in systemic lupus and its association withcorticosteroids. Arthritis Rheum. 43, 1801–1808 (2000).
61. Fisher, D. E. & Bickel, W. H. Corticosteroid-inducedavascular necrosis. A clinical study of seventy-sevenpatients. Bone Joint Surg. Am. 53, 859–873 (1971).
62. Tam, L. S., Gladman, D. D., Hallett, D. C., Rahman, P. &Urowitz, M. B. Effect of antimalarial agents on the fastinglipid profile in systemic lupus erythematosus. J. Rheumatol.27, 2142–2145 (2000).
63. Borba, E. F. & Bonfa, E. Longterm beneficial effect ofchloroquine diphosphate on lipoprotein profile in lupuspatients with and without steroid therapy. J. Rheumatol.28, 780–785 (2001).
64. Lakshminarayanan, S., Walsh, S., Mohanraj, M. &Rothfield, N. Factors associated with low bone mineraldensity in female patients with systemic lupuserythematosus. J. Rheumatol. 28, 102–108 (2001).
65. Levy, R. A. et al. Hydroxychloroquine (HCQ) in lupuspregnancy: double-blind and placebo-controlled study.Lupus 10, 401–404 (2001).
66. Steinberg, A. D. et al. Cyclophosphamide in lupus nephritis:a controlled trial. Ann. Intern. Med. 75, 165–171 (1971).
67. Flanc, R. S. et al. Treatment of diffuse proliferative lupusnephritis: a meta-analysis of randomized controlled trials.Am. J. Kidney Dis. 43, 197–208 (2004).A systematic review of randomized controlled trials,which assessed the benefits and harm of currenttreatments for diffuse proliferative lupus nephritis.
68. Miller, J. J., Williams, G. F. & Leissring, J. C. Multiple latecomplications of therapy with cyclophosphamide,including ovarian destruction. Am. J. Med. 50, 530–535(1971).
69. Brook, C. G. & Evans, P. R. Psychosis in systemic lupuserythematosus (SLE) and the response tocyclophosphamide. Proc. R. Soc. Med. 62, 912 (1969).
70. Bardana, E. J. Jr, Porter, G. A., Pirofsky, B., Gourley, R. T. &Bayrakci, C. Azathioprine in steroid-insensitive nephropathy.Am. J. Med. 49, 789–800 (1970).
71. Drinkard, J. P. et al. Azathioprine and prednisone in thetreatment of adults with lupus nephritis. Clinical, histological,and immunological changes with therapy. Medicine(Baltimore) 49, 411–432 (1970).
72. El Hachmi, M., Jadoul, M., Lefebvre, C., Depresseux, G. &Houssiau, F. A. Relapses of lupus nephritis: incidence, riskfactors, serology and impact on outcome. Lupus 12,692–696 (2003).
73. Chan, T. M. et al. Treatment of membranous lupus nephritiswith nephrotic syndrome by sequential immunosuppression.Lupus 8, 545–551 (1999).
74. Contreras, G. et al. Sequential therapies for proliferativelupus nephritis. N. Engl. J. Med. 350, 971–980 (2004).
75. Mok, C. C., Ho, C. T., Chan, K. W., Lau, C. S. & Wong, R. W.Outcome and prognostic indicators of diffuse proliferativelupus glomerulonephritis treated with sequential oralcyclophosphamide and azathioprine. Arthritis Rheum. 46,1003–1013 (2002).
76. Abu-Shakra, M. & Shoenfeld, Y. Azathioprine therapy forpatients with systemic lupus erythematosus. Lupus 10,152–153 (2001).
77. Armenti, V. T. et al. Report from the National TransplantationPregnancy Registry (NTPR): outcomes of pregnancy aftertransplantation. Clin. Transpl. 1, 121–130 (2002).
78. Remer, C. F., Weisman, M. H. & Wallace, D. J. Benefits ofleflunomide in systemic lupus erythematosus: a pilotobservational study. Lupus 10, 480–483 (2001).
79. Sato, E. I. Methotrexate therapy in systemic lupuserythematosus. Lupus 10, 162–164 (2001).
80. Hu, W. et al. Cyclosporine A in treatment of membranouslupus nephropathy. Chin. Med. J. 116, 1827–1830 (2003).
81. Dammacco, F. et al. Cyclosporine-A plus steroids versussteroids alone in the 12-month treatment of systemic lupuserythematosus. Int. J. Clin. Lab. Res. 30, 67–73 (2000).
82. Merrill, J. T. Regulation of the vasculature: clues from lupus.Curr. Opin. Rheumatol. 14, 504–509 (2002).
83. Fabbri, P., Cardinali, C., Giomi, B. & Caproni, M.Cutaneous lupus erythematosus: diagnosis andmanagement. Am. J. Clin. Dermatol. 4, 449–465 (2003).

1046 | DECEMBER 2004 | VOLUME 3 www.nature.com/reviews/drugdisc
R E V I E W S
84. Traynor, A. E. et al. Treatment of severe systemic lupuserythematosus with high-dose chemotherapy andhaemopoietic stem-cell transplantation: a phase I study.Lancet 356, 701–707 (2000).
85. Hashimoto, N. et al. Autologous hematopoietic stem celltransplantation for refractory antiphospholipid syndromecausing myocardial necrosis. Bone Marrow Transplant.33, 863–866 (2004).
86. Merrill, J. T. Dehydroepiandrosterone, a sex steroidmetabolite in development for systemic lupuserythematosus. Expert Opin. Investig. Drugs 12, 1017–1025(2003).
87. Petri, M. A. et al. Effects of prasterone on corticosteroidrequirements of women with systemic lupus erythematosus:a double-blind, randomized, placebo-controlled trial.Arthritis Rheum. 46, 1820–1829 (2002).
88. Chang, D. M., Lan, J. L., Lin, H. Y. & Luo, S. F. Dehydro-epiandrosterone treatment of women with mild-to-moderatesystemic lupus erythematosus: a multicenter randomized,double-blind, placebo-controlled trial. Arthritis Rheum. 46,2924–2927 (2002).
89. Ding, L., Zhao, M., Zou, W., Liu, Y. & Wang, H. Mycopheno-late mofetil combined with prednisone for diffuse proliferativelupus nephritis: a histopathological study. Lupus 13,113–118 (2004).
90. Li, L., Wang, H. & Lin, S. Mycophenolate mofetil treatmentfor diffuse proliferative lupus nephritis: a multicenter clinicaltrial in China. Zhonghua Nei Ke Za Zhi. 41, 476–479(2002).
91. Contreras, G. et al. Sequential therapies for proliferativelupus nephritis. N. Engl. J. Med. 350, 971–80 (2004).
92. Harzallah, K. et al. Efficacy of mycophenolate mofetil onrecurrent glomerulonephritis after renal transplantation.Clin. Nephrol. 59, 212–216 (2003).
93. Zhao, M. et al. Clinical observations of mycophenolatemofetil therapy in refractory primary nephrotic syndrome.Nephrology 8, 2–10 (2003).
94. Buratti, S., Szer, I. S., Spencer, C. H., Bartosh, S. & Reiff, A.Mycophenolate mofetil treatment of severe renal disease inpediatric onset systemic lupus erythematosus. J. Rheumatol.28, 2103–2108 (2001).
95. Coutts, S. M., Plunkett, M. L., Iverson, G. M., Barstad, P. A.& Berner, C. M. Pharmacological intervention in antibodymediated disease. Lupus 5, 158–159 (1996).
96. Merrill, J. T. LJP 1082: a toleragen for Hughes syndrome.Lupus 13, 335–338 (2004).
97. Weisman, M. H., Bluestein, H. G., Berner, C. M. & de Haan, H. A. Reduction in circulating dsDNA antibodytiter after administration of LJP 394. J. Rheumatol. 24,314–318 (1997).
98. Wallace, D. J. & Tumlin, J. A. LJP 394 (abetimus sodium,Riquent) in the management of systemic lupuserythematosus. Lupus 13, 323–327 (2004).
99. Spertini, F. et al. Idiotypic vaccination with a murine anti-dsDNA antibody: phase I study in patients with nonactivesystemic lupus erythematosus with nephritis. J. Rheumatol.26, 2602–2608 (1999).
100. Grammer, A. C. et al. Abnormal germinal center reactions insystemic lupus erythematosus demonstrated by blockadeof CD154-CD40 interactions. J. Clin. Invest. 112,1506–1520 (2003).
101. Harigai, M. et al. Responsiveness of peripheral blood B cellsto recombinant CD40 ligand in patients with systemic lupuserythematosus. Lupus 8, 227–233 (1999).
102. Uhm, W. S. et al. Cytokine balance in kidney tissue fromlupus nephritis patients. Rheumatology (Oxford) 42,935–938 (2003).
103. Kuroiwa, T., Schlimgen, R., Illei, G. G. & Boumpas, D. T.Monocyte response to Th1 stimulation and effector functiontoward human mesangial cells are not impaired in patientswith lupus nephritis. Clin. Immunol. 106, 65–72 (2003).
104. Kato, K. et al. The soluble CD40 ligand sCD154 in systemiclupus erythematosus. J. Clin. Invest. 104, 947–955 (1999).
105. Higuchi, T. et al. Cutting edge: ectopic expression of CD40ligand on B cells induces lupus-like autoimmune disease.J. Immunol. 168, 9–12 (2002).
106. Quezada, S. A. et al. Distinct mechanisms of action of anti-CD154 in early versus late treatment of murine lupusnephritis. Arthritis Rheum. 48, 2541–2554 (2003).
107. Kairaitis, L. et al. Blockade of CD40-CD40 ligand protectsagainst renal injury in chronic proteinuric renal disease.Kidney Int. 64, 1265–1272 (2003).
108. Wang, X. et al. Effects of anti-CD154 treatment on B cells inmurine systemic lupus erythematosus. Arthritis Rheum. 48,495–506 (2003).
109. Kalled, S. L., Cutler, A. H. & Burkly, L. C. Apoptosis andaltered dendritic cell homeostasis in lupus nephritis arelimited by anti-CD154 treatment. J. Immunol. 167,1740–1747 (2001).
110. Brams, P. et al. A humanized anti-human CD154monoclonal antibody blocks CD154-CD40 mediatedhuman B cell activation. Int. Immunopharmacol. 1,277–294 (2001).
111. Huang, W. et al. The effect of anti-CD40 ligand antibody onB cells in human systemic lupus erythematosus. ArthritisRheum. 46, 1554–1562 (2002).
112. Davis, J. C. Jr, Totoritis, M. C., Rosenberg, J., Sklenar, T. A.& Wofsy, D. Phase I clinical trial of a monoclonal antibody against CD40-ligand (IDEC-131) in patients withsystemic lupus erythematosus. J. Rheumatol. 28, 95–101(2001).
113. Kalunian, K. C., Davis, J. C. Jr, Merrill, J. T., Totoritis, M. C. &Wofsy, D. Treatment of systemic lupus erythematosus byinhibition of T cell costimulation with anti-CD154: arandomized, double-blind, placebo-controlled trial. ArthritisRheum. 46, 3251–3258 (2002).
114. Boumpas, D. T. et al. A short course of BG9588 (anti-CD40ligand antibody) improves serologic activity and decreaseshematuria in patients with proliferative lupusglomerulonephritis. Arthritis Rheum. 48, 719–727 (2003).
115. Leandro, M. J., Edwards, J. C., Cambridge, G.,Ehrenstein, M. R. & Isenberg, D. A. An open study of B lymphocyte depletion in systemic lupus erythematosus.Arthritis Rheum. 46, 2673–2677 (2002).
116. Anolik, J. H. et al. The relationship of FcγRIIIa genotype todegree of B cell depletion by rituximab in the treatment ofsystemic lupus erythematosus. Arthritis Rheum. 48,455–459 (2003).
117. Weide, R., Heymanns, J., Pandor, F. A. & Koppler, H.Successful long-term treatment of systemic lupuserythematosus with rituximab maintenance therapy. Lupus12, 779–782 (2003).
118. Anolik, J., Sanz, I. & Looney, R. J. B cell depletion therapy insystemic lupus erythematosus. Curr. Rheumatol. Rep. 5,350–356 (2003).
119. Eisenberg, R. SLE — rituximab in lupus. Arthritis Res. Ther.5, 157–159 (2003).
120. Kneitz, C., Wilhelm, M. & Tony, H. P. Effective B celldepletion with rituximab in the treatment of autoimmunediseases. Immunobiology 206, 519–527 (2002).
121. Shanafelt, T. D., Madueme, H. L., Wolf, R. C. & Tefferi, A.Rituximab for immune cytopenia in adults: idiopathic throm-bocytopenic purpura, autoimmune hemolytic anemia, andEvans syndrome. Mayo Clin. Proc. 78, 1340–1346 (2003).
122. Zaja, F. et al. B-cell compartment as the selective target forthe treatment of immune thrombocytopenias.Haematologica 88, 538–546 (2003).
123. Cate, R. et al. Anti-CD20 monoclonal antibody (rituximab)for refractory autoimmune thrombocytopenia in a girl withsystemic lupus erythematosus. Rheumatology (Oxford)43, 244 (2004).
124. Saito, K. et al. Successful treatment with anti-CD20monoclonal antibody (rituximab) of life-threatening refractorysystemic lupus erythematosus with renal and centralnervous system involvement. Lupus 12, 798–800 (2003).
125. Fra, G. P., Avanzi, G. C. & Bartoli, E. Remission of refractorylupus nephritis with a protocol including rituximab. Lupus12, 783–787 (2003).
126. Janeway, C., Travers, P., Walport, M. & Capra, J. D.Immunobiology: The immune System in Health and Disease4th edn (Current Biology, London, 1999).
AcknowledgementsThe authors would like to thank T. Roehrig for her technicalassistance with the manuscript.
Competing interests statementThe authors declare competing financial interests: see Web versionfor details.
Online links
DATABASESThe following terms in this article are linked online to:Entrez Gene:http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=geneBLyS | CD27 | CD40 | CD154 | VCAM1OMIM: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=OMIMSLEAccess to this interactive links box is free online.