Aviation sector---Jet Airways & Qatar Airways Market Analysis

The upper airway is a complex structure that serves as the conduit from the external environment to the
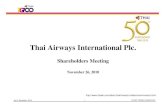
intrathoracic airways and lungs. The anatomic regions of the upper airway (Figure 50-1) include the nasal cavity,nasopharynx, velopharynx behind the soft palate, orophar-ynx, hypopharynx, and larynx. This conduit has a variety of functions, including the filtering and conditioning of air, olfaction, mastication and deglutition, phonation,coughing, and protection of the lower airways and lungsfrom large particulate material.1–6 This chapter focuses onthe physiology and pathophysiology of the respiratory-related functions of the upper airway. The discussion ofother upper airway functions is limited to their interactionwith respiratory function.
ANATOMY AND PHYSIOLOGY OF THE UPPER AIRWAY
NOSE
To enter the upper airway, air flows rapidly upward through theanterior nares or nasal vestibules, which are 1 cm–diameterchannels in the anterior portion of the nose. Coarse hairs or vibrissae within the vestibules serve to filter largerparticulate matter. The air then encounters the nasal sep-tum, which divides the nasal passage into two fossae. Thelateral walls of the fossae contain irregular projectionsknown as the turbinates, which create turbulent flow andreduce flow rate. This prolongs contact of the inspired airwith the nasal mucosa, which at this level is richly suppliedwith a system of subepithelial capillaries and venoussinusoids, along with submucosal glands and goblet cells.The rich vascularization of the mucosa provides forhumidification and temperature conditioning of the inspired air. Production of a mucous layer by glandularstructures provides for trapping of particulate matter. Nasal secretions produced by the highly vascular mucosa arerich in immunoglobulins, cytokines, and other cytolyticsubstances, and there is extensive mucosal production of
nitric oxide by the nose and paranasal sinuses; all of thesehave potent antimicrobial activity. There is thus consider-able filtering, temperature conditioning, and humidificationof the air traversing the nasal fossae, which have an impor-tant protective function for the lower airways.
Although the nose accounts for over 50% of upper airwayflow resistance in normal, awake persons, it is the preferredroute of breathing during resting ventilation. As ventilatorydrive increases, some dilatation of the nares and vasocon-striction of the nasal mucosa may help to reduce airflowresistance, but as demands increase, the mouth opens andthe lower-resistance oropharyngeal route is recruited,although at the cost of reduced conditioning of the inspiredair. Other functions of the nose include olfaction and a con-tribution to phonation, in that the nose acts as a resonatingchamber for some components of speech.
PHARYNX
This structure consists of the nasopharynx, oropharynx, andhypopharynx. Inspired air exits the nasal passages posteri-orly through 2.5 �1.5 cm openings known as the choanaeand enters the nasopharynx. The nasopharynx extends fromthe choanae down to the lower margin of the soft palate. Thesegment of the nasopharynx immediately behind the softpalate has been termed the velopharynx. The mucosa of theposterior nasopharyngeal wall contains a collection of lym-phoid tissue termed the single pharyngeal or adenoid tonsil.This structure can hypertrophy and produce nasal obstruc-tion, which often contributes to obstructive sleep apnea(OSA) in children. As with the palatine tonsils between the anterior and posterior tonsillar pillars lower down, theadenoid tends to involute after puberty.
The muscular structures in the wall of the nasopharynxand soft palate play a major role in speech, swallowing, andbreathing. These muscles act to partition airflow betweenthe oral and nasal routes, particularly under conditions ofincreased ventilatory drive. The palatal muscles are alsoimportant in the maintenance of airway patency.
CHAPTER 50
PHYSIOLOGY OF THE UPPERAIRWAYS AND UPPER AIRWAY
OBSTRUCTION IN DISEASE
R. John Kimoff

582 Sleep Disordered Breathing
The oropharynx lies behind the oral cavity and extendsfrom the soft palate superiorly to the tip of the epiglottisinferiorly. The lateral walls include the anterior (palatoglos-sal) and posterior (palatopharyngeal) tonsillar pillars, whichmerge superiorly into the soft palate and between which liethe fossae of the palatine tonsils. The posterior pharyngealwall is largely composed of the pharyngeal constrictor mus-cles, whereas the posterior aspect or base of the tongue liesanteriorly. This structure serves as the main conduit for bothsolids and liquids from the mouth to the esophagus and forthe flow of air through to the larynx. The coordination ofthese various neuromuscular functions is achieved throughreflex control involving neural afferents in the pharyngealmucosa; these project to pontomedullary centers, whichintegrate this information and regulate swallowing andrespiratory functions.
Swallowing is characterized by initial elevation of the lar-ynx, followed by active contraction of the oropharynx, lead-ing to shortening and constriction of the pharynx to activelypropel food toward the esophagus. The normal coordinationof this action in humans is such that swallowing occursalmost exclusively during late expiration in seated humansand is accompanied by respiratory inhibition, that is, pro-longation of expiratory time, and other processes, such asvocal cord closure and laryngeal elevation, that assist inprotecting the laryngeal aperture.7–9
In contrast to the passage of food during swallowing, air-flow through the oropharynx is passive, being driven by thenegative intrathoracic pressure generated by the respiratorypump muscles. However, whereas the nasal and laryngealsegments of the upper airway are supported by bony andcartilaginous structures, the pharynx is a collapsible mus-cular tube. There is clear evidence that the stability andpatency of this structure during breathing depend upontonic and phasic activation of muscles surrounding theairway, which act to stiffen and dilate the pharynx during
inspiration.10–13 These muscles include the genioglossusmuscle, which positions and stabilizes the tongue, palatalmuscles such as the tensor and levator palatini and thepalatoglossus and palatopharyngeus muscles, and musclesthat stablilize the hyoid bone, such as the geniohyoid andsternohyoid muscles. If the dilating musculature is notsufficiently activated, collapse of this segment will occurduring inspiration, due to a suction effect of the negativeintraluminal pressure associated with inspiratory airflow.Thus, in generating inspiratory impulses, the brainstem res-piratory controller produces a sequential wave of respiratorymuscle activation, with initial activation of pharyngeal dila-tors, which stiffen and dilate this conduit. Subsequently,laryngeal activation leads to opening of the glottic aper-ture, chest wall muscle activation that stiffens andexpands the chest wall, and diaphragmatic activation.14–16
Pharyngeal caliber is also modulated by important reflexmechanisms that regulate within-breath levels of phasicmuscle activation. Both tonic and phasic activity of pharyn-geal dilators and the protective reflexes are reduced duringsleep, which leads to increased airflow resistance duringsleep in normal subjects and can contribute to collapse ofthe upper airway in patients with OSA.
The hypopharynx extends downward from the uppermargin of the epiglottis to the lower border of the cricoidcartilage, serving as the conduit from the oropharynx to thelaryngeal inlet and esophagus. The piriform recesses lie oneach side of the hypopharynx. These recessess serve todirect food boluses down and away from the larynx in tran-sit to the esophagus. During swallowing, as noted above,there is laryngeal constriction and a movement of theepiglottis in order to protect the laryngeal aperture.
LARYNX
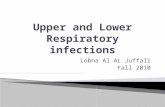
The structure of the larynx, and in particular the cartilagi-nous skeleton and musculature, is illustrated in Figure 50-2,which also illustrates the action of the musculature on glot-tic patency.3,17–19 In addition to the thyroid, cricoid, and ary-tenoid cartilages, the epiglottic cartilage, which descends toprotect the laryngeal aperture during swallowing, is alsoconsidered to be part of the laryngeal apparatus. The larynxplays an integral role in all upper airway functions, includ-ing respiration, phonation, cough, swallowing, and vomit-ing. As with the pharyngeal structures, these activities areinitiated and coordinated by brainstem centers, with modu-lation by afferent neural inputs from the airway itself. In thecase of the larynx, there is a rich sensory array of mucosalsensory receptors, which respond to changes in airflow,pressure, temperature, and laryngeal position. Impulsesfrom these receptors are conveyed centrally through thesuperior laryngeal nerve to modulate laryngeal function andbreathing pattern. Motor innervation of the laryngeal mus-culature is conveyed through the recurrent laryngeal nerves,with the exception of the cricothyroid muscle, which is sup-plied by the external branch of the superior laryngeal nerve.The recurrent laryngeal nerves arise from the vagus nervewithin the thorax and travel superiorly along the media-stinal structures to the larynx. On the right, the recurrentlaryngeal nerve arises at the level of the subclavian artery,
FIGURE 50-1 Anatomy of the upper airway.

Physiology of the Upper Airway and Upper Airway Obstruction in Disease 583
and on the left, the nerve arises at the level of the aortic arch. Disease processes, including intrathoracic disease, thatdisrupt the recurrent laryngeal nerve therefore lead to vocal cord paralysis and laryngeal dysfunction, which hasimplications for all of the other functions of the larynx.
Although protective closure of the larynx during swal-lowing is part of the integrated deglutition process, there isalso a more basic laryngeal protective response called the“glottic closure reflex.” This is characterized by a short-latency activation of the adductor muscles to rapidly closethe glottic aperture in response to stimulation of the laryn-geal mucosa by tactile or chemical stimuli. This is thereforea critical response that protects against aspiration of foreignmaterial into the upper airway. It is of note that, in contrastto the situation in many mammalian species, the humanreflex is not crossed, so that damage to the superior laryn-geal nerve on one side can result in failure of ipsilateral vocalfold closure, thereby increasing the risk of aspiration.17
Although the glottic closure reflex represents a crucial pro-tective mechanism, the response may become exaggerated insome disease conditions, leading to laryngospasm or pro-longed glottic closure following withdrawal of the incitingstimulus.
With respect to the respiratory function of the larynx,during inspiration the posterior cricoarytenoid muscle, theonly vocal cord abductor muscle, is activated to widen the glottic aperture.18,19 There is simultaneous activation of the cricothyroid muscle, which acts to lengthen the vocalfold. The concurrent lengthening and abduction of the
folds lead to an increase in glottic cross-sectional area, thusreducing resistance to inspiratory airflow. The posteriorcricoarytenoid muscle relaxes during expiration, whereasthe cricothyroid muscle may remain active, to maintain thelength of the cords. Under some conditions, there is activecontraction of the adductor muscles to narrow the apertureand produce expiratory “braking.” This strategy is adoptedin an attempt to maintain end-expiratory lung volume. Thisoccurs, for example, in neonates with respiratory distresssyndrome and is manifested as expiratory grunting due toglottic closure. An extreme instance of prolonged glotticclosure appears to occur in apnea of prematurity, in whichexperimental evidence has demonstrated that apneas areassociated with active glottic closure.20
In some patients, laryngeal function becomes disturbedsuch that there is intermittent inspiratory closure of thevocal cords. This condition has been variously termed vocalcord dysfunction syndrome, paradoxical vocal cord motion,and laryngismus stridulus.21–23 The clinical presentationmay mimic both asthma and organic upper airway obstruc-tion and may be acute and lead to endotracheal intuba-tion. Spirometric flow–volume curves are very helpful inmaking the diagnosis (see below). A substantial proportionof affected individuals also have asthma; patients withoutasthma are often women who have been misdiagnosed asasthmatic. This syndrome typically occurs in the absence ofany evident structural laryngeal disease, and the mecha-nisms responsible are unclear. However, psychogenic factorsappear to play a role as the dysfunction is intermittent, maybe worse in times of emotional stress, and, even if sustainedduring wakefulness, tends to disappear during sleep.Furthermore, psychiatric disorders are common amongaffected individuals. Treatment approaches include patienteducation, psychotherapy as needed, and referral to a speechpathologist.
The larynx also plays a major role in phonation.Although sound can be produced passively by creating air-flow through the larynx, the generation of speech or songrequires finely controlled activation of laryngeal muscles.These muscles act to shape and position the vocal cords togenerate speech and modulate the spatial relationshipbetween the cricoid and thyroid cartilages to vary the pitchof the sound produced. Further modulation of sound isproduced superiorly in the pharynx and nasal cavity.Breathing during speech is characterized by rapid inspiration,followed by prolonged expiration, during which the subglot-tic pressure is maintained relatively constant as the finemotor actions of the laryngeal apparatus produce sound.24
Stuttering appears to represent an example of an alteredinteraction between laryngeal and respiratory functionduring speech, the mechanisms for which remain poorlyunderstood.25
CLINICAL PHYSIOLOGY OF UPPER AIRWAYOBSTRUCTION
CLINICAL DESCRIPTION
Obstruction of the upper airway can occur in various clini-cal contexts and disease states, although it is much less
FIGURE 50-2 Laryngeal skeleton and musculature, illustrating theactions of the major muscles.

584 Sleep Disordered Breathing
common than obstructive disease of the lower airway, suchas asthma or chronic obstructive pulmonary disease(COPD). Unfortunately, the clinical presentation of the twomay be very similar (dyspnea and noisy breathing), so thatthe less common diagnosis of upper airway obstruction maybe missed if a careful clinical evaluation and appropriatetesting are not performed. A missed diagnosis, particularlyin the context of acute or severe upper airway obstruction,may have devastating consequences for the patient asappropriate treatment may be delayed beyond the point ofsevere airway compromise and respiratory arrest.
A hallmark clinical feature of upper airway obstruction isdyspnea with stridor, a loud, constant-pitch inspiratorysound that indicates obstruction of the extrathoracic airway.Severe extrathoracic or variable intrathoracic large airwayobstruction may also cause expiratory prolongation and awheeze-like sound, making it difficult to distinguish fromdisease of the lower airways. Other symptoms associatedwith upper airway obstruction include cough, hoarseness,dysphagia, and orthopnea, depending upon the location andnature of the obstructing lesion. Although it is beyond thescope of this chapter to provide an exhaustive description ofcauses of upper airway obstruction, a list of commonpathologies is provided in Table 50-1.
PHYSIOLOGIC TESTING FOR UPPER AIRWAY
OBSTRUCTION
Forced expiratory and inspiratory spirometry with recordingof the flow–volume curve is the most important physiologic
tool for the diagnosis of upper airway obstruction.26–35
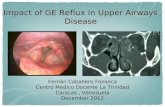
Examples of normal and pathologic flow–volume curves areshown in Figure 50-3. Normally, there is an initial rapid risein expiratory flow to a peak value that is dependent oneffort, lung elastic recoil, and flow in the large airways. Aslung volume decreases, flow becomes effort-independentand determined by the balance between lung recoil and flowresistance in progressively smaller airways. During forcedinspiration, flow is effort dependent throughout, with thepeak value occurring at midinspiration. Peak expiratoryflow rate is considerably larger than peak inspiratory flowrate because of the effects of lung elastic recoil. However, at50% of vital capacity, forced inspiratory flow (FIF50) issomewhat greater than forced expiratory flow (FEF50), duein part to normal expiratory dynamic compression of theairways. Thus, the normal FIF50/FEF50 ratio is slightlygreater than 1.
Obstructing lesions of the upper airways may be eitherfixed or variable; that is, lesions produce narrowing thatvaries with pressures acting across the airways during inspi-ration and expiration (Figure 50-4). In the case of variableintrathoracic large airway obstruction (see Figure 50-3B),during expiration, pleural pressure is more positive thanintratracheal pressure, leading to dynamic compression ofthe airway and thereby increased airway narrowing andreduced expiratory flow. However, during inspiration, thereis a net distending pressure across the large airway, so thatpatency of the lumen tends to increase, yielding a relativepreservation of inspiratory flow rate. The FIF50/FEF50 ratiowill therefore be well above 1, typically in the range of 2 to 3.
In the case of variable extrathoracic upper airwayobstruction (see Figure 50-3C), the pressure surroundingthe airway is atmospheric, so that during inspiration, thereis a net negative transmural pressure, which tends to worsen
FIGURE 50-3 Flow–volume curves: upper airway obstruction. A,Normal flow–volume curve. B, Variable intrathoracic obstructiondue to a tracheal tumor. C, Variable extrathoracic obstruction dueto a laryngeal tumor. D, Fixed upper airway obstruction due tolarge tracheal tumor. Solid line � air; dotted line � helium. Note theimprovement in both inspiratory and expiratory flow with helium.
loV ( )L
Flow(L/s)
Flow(L/s)
Flow(L/s)
A B
C D
Flow(L/s)
loV ( )L
loV ( )L
EF F 05
FIF 05
loV ( )L
8
6
4
2
0
-2
-4
-6
-8
8
6
4
2
0
-2
-4
-6
-8
8
6
4
2
0
-2
-4
-6
-8
8
6
4
2
0
-2
-4
-6
-8
Table 50-1 Causes of Upper Airway Obstruction
InfectiousAcute epiglottitisLaryngotracheobronchitis (croop)Ludwig’s anginaRetropharyngeal abscess
Allergic/immuneEdema associated with anaphylaxisAngioneurotic edemaRelapsing polychondritisRheumatoid arthritisSjögren’s syndrome (adenopathy)Wegener’s granulomatosis
TumorsBenignMalignant
Laryngeal carcinomaBronchogenic carcinomaLymphomaOther metastatic disease
VascularRight-sided aortic archDouble aortic archInnominate artery syndromeAberrant left pulmonary artery
Tracheal abnormalitiesNeuromuscularVocal cord dysfunctionForeign body aspirationTraumaInhalation
Smoke/burnChemical

Physiology of the Upper Airway and Upper Airway Obstruction in Disease 585
airway narrowing and reduce inspiratory flow. In contrast,during expiration, the positive pressure within the airwayproduces a transmural distending pressure and reduces theextent of narrowing, resulting in increased expiratory rela-tive to inspiratory flow. Thus, the FIF50/FEF50 ratio will beless than 1.
The anatomy of many upper airway lesions, however, is such that the degree of obstruction is not materiallyinfluenced by the pressures acting across the airway, withresultant comparable reductions in both inspiratory andexpiratory flow (see Figure 50-3D). In this case, the FIF50/FEF50 ratio may be close to 1.
From Figure 50-3, it can be seen that inspection of theflow–volume curve and recognition of the characteristicchanges in pattern are crucial to the recognition of upperairway obstruction. It is important to emphasize that onecannot rely solely upon tabular data from simple spirometryto exclude the diagnosis of upper airway obstruction.Because flow in the medium and small airways contributessignificantly to forced expiratory volume in 1 second(FEV1), substantial large airway obstruction may be presentbefore significant changes in FEV1 occur. When concomi-tant airway disease, such as COPD, is present, the sensitiv-ity of spirometry for the detection of upper airwayobstructing lesions is even lower. Peak expiratory flow rateis much more sensitive for the presence of expiratory largeairway obstruction, and a hallmark finding in tabular data isa reduction in peak expiratory flow rate (as percent pre-dicted) that is out of proportion to other changes in flowrates, particularly FEV1. However, assessment of the inspira-tory flow pattern is also crucial.
The characteristic flattening of the flow–volume curve inupper airway obstruction reflects the presence of pathologicflow limitation. Flow limitation is defined as a state in whichincreasing effort does not result in increasing airflow. Thus,flow is reduced and constant over a range of lung volumes,producing the flattened shape of the curves depicted inFigure 50-3. The turbulent flow occurring in the context ofa high driving pressure during inspiration is responsible forproducing the sound of stridor in extrathoracic airwayobstruction. As noted above, intrathoracic obstruction canresult in prolonged expiratory flow and low-pitched wheeze,
and increased breath sounds can be heard during bothinspiration and expiration, again due to turbulent flowresulting from fixed airway obstruction.
Turbulence due to airway narrowing can be reduced byadministration of a helium–oxygen (Heliox) mixture, whichis less dense than air. This can be used diagnostically incases where it is unclear whether changes in flow–volumecurves are due to large airway obstruction. The standard cri-terion for identifying a large airway component is the detec-tion of an increase with helium of more than 50% in eitherpeak expiratory or inspiratory flow.34 Heliox administrationis also a useful, albeit temporary, therapeutic adjunct in theclinical management of upper airway obstruction.
Mediastinal masses may cause intrathoracic large airwayobstruction that varies with body position. Owing to gravi-tational factors, intrathoracic large airway obstructionresulting from anterior mediastinal masses may be moreprominent when the patient is supine. Airway obstructioncan worsen with the chest wall relaxation that occurs on theinduction of anesthesia, so that preoperative and postopera-tive airway management in such patients requires carefulattention. The positional variation of large airway obstruc-tion can be evaluated by assessing changes in peak flow ratesduring seated versus supine spirometry.36
In the context of acute, severe extrathoracic upper air-way obstruction (eg, epiglottitis, foreign body aspiration, oracute laryngeal injury), inspiratory intrathoracic drivingpressures may become extremely negative, and this, in turn,may lead to the development of “negative-pressure pul-monary edema.”37,38 This is believed to be due to a combi-nation of increased venous return leading to increasedpulmonary blood volume and negative pericapillary intersti-tial tissue pressure caused by large negative intrapleuralpressures, resulting in forces that favor fluid transudationinto the interstitium. In some patients, left ventricular (LV) dysfunction is believed to also contribute because of increased LV wall transmural pressure, that is, afterload,resulting from the negative intrapleural pressure. Manage-ment of this condition primarily involves management ofthe upper airway obstruction.
PATHOPHYSIOLOGY OF UPPER AIRWAY COLLAPSE DURING SLEEP: OBSTRUCTIVESLEEP APNEA
CLINICAL DESCRIPTION
OSA is characterized by repeated episodes of upper airwayobstruction during sleep. This important condition is highlyprevalent in the adult population, being estimated to affect2 to 9% of women and 4 to 15% of men, depending on the precise definitions used and the population understudy.39,40 OSA also occurs in the pediatric age group,although with considerably lower prevalence. OSA is associ-ated with considerable morbidity, increased health careresource utilization, and, probably, increased mortal-ity.12,13,40–42 Apneic episodes are characterized by upper air-way closure and progressively increasing respiratory effortsdriven by chemoreceptor and mechanoreceptor stimuli,which then provoke arousal from sleep and reopening of the
Inspiration Expiration
00
–
–
––
––
–
–Ppl < Ptr
Ptr < Patm Ptr < Patm
0
++
+
+
+
+++
Ppl < Ptr
0
FIGURE 50-4 Forces acting across the airways that determinespirographic patterns in cases of variable intrathoracic and extra-thoracic upper airway obstruction. Patm � atmospheric pressure;Ppl � pleural pressure; Ptr � tracheal pressure.

586 Sleep Disordered Breathing
airway. These events result in sleep fragmentation, repetitivehypoxemia, and swings in heart rate, blood pressure, andcardiac output, which are responsible for the clinical seque-lae of OSA. The latter include excessive daytime sleepiness,impaired concentration, cognitive functions and memory,and mood disturbances. There is a rapidly growing body ofdata linking OSA to increased cardiovascular risk, includinghypertension, cardiac ischemic events, arrhythmia, cere-brovascular accidents, congestive heart failure, and pul-monary hypertension. Severe OSA can also be associatedwith changes in ventilatory control and hypoventilationduring wakefulness, typically in the context of underlyinglung dysfunction. There is also growing evidence of a linkbetween OSA and asthma. These issues are discussed furtherbelow and in a subsequent chapter.
OSA should be suspected clinically in patients with ahistory of heavy habitual snoring and excessive daytimesleepiness. Sleep testing is performed to establish thediagnosis. The current “gold standard” test is completeovernight polysomnography performed in a sleep laboratory.This test involves recording of the electroencephalogram,electrooculogram and submental electromyogram forsleep–wake staging, pulse oximetry, determination of airflow
with an oronasal thermistor or through nasal pressure (currently the method of choice), determination of respira-tory effort with inductance plethysmography, piezoelectricsensors or mercury strain gauges around the thorax andabdomen or with an esophageal balloon (typically reservedfor research studies or special clinical cases), determinationof body position with mercury switch or video recording,recording of sound (snoring) with a microphone, anddetection of periodic limb movements with leg electromyo-graphic electrodes. A typical polysomnographic tracing froma patient with severe OSA is shown in Figure 50-5.
The raw data tracings from the sleep study are scored by atechnologist to identify sleep–wake state for each consecutive30-second period (epoch) of the night, according to standardcriteria.43 The respiratory signals are scored to identify apneas(�10 seconds of complete cessation of airflow) and hypop-neas (event lasting �10 seconds, with reduced airflow associ-ated with oxygen desaturation and/or brief arousal fromsleep), and whether these are obstructive or central in nature(associated or not with ongoing respiratory effort duringevents).44 Summary data are generated in both tabular andgraphic form to describe the physiology of sleep, breathing,and other events through the night (Figure 50-6). Although
FIGURE 50-5 Representative tracing from a polysomnographic recording in a patient with obstructive sleep apnea, showing three sequen-tial obstructive events, one apnea and two hypopneas. Note that the severity of event-associated oxygen desaturation correlates with theextent of flow reduction during these events. The flow signal is a nasal pressure recording, with inspiration in the upward direction, andillustrates the upper airway flow limitation (flattening) during hypopneas. Note the partial rib cage paradox in the thoracic respiratoryinductance plethysmography signal.
OC
OC
EMGC4-A1
C3-A2
EKG+ 100.0
+ 90.0
+ 80.0
LEGS
SaO2
Flow
Chest(respitrace)
Abdomen(respitrace)
Snore
Snore
Stage 1 Stage 1 Stage 1
Arc
Stage 1Wake Stage 2 Stage 2 Stage 2
Snore
Obstructive HypopneaObstructive Hypopnea wObstructive Apnea

Physiology of the Upper Airway and Upper Airway Obstruction in Disease 587
the polysomnogram therefore provides extensive physiologicinformation, which is useful in the clinical setting, this is atime- and cost-intensive testing procedure of limited availa-bility. Owing to the prevalence of OSA and issues of limitedaccess to full polysomnography, there is a growing relianceon simplified tests that record oximetry alone, or oximetrywith airflow and respiratory effort channels, to establish thediagnosis.
MECHANISMS OF UPPER AIRWAY COLLAPSE
DURING SLEEP
As described above, the pharyngeal airway can be consid-ered as a collapsible tube, the patency of which is deter-mined by a balance between forces tending to close theairway, such as intraluminal suction pressure during breath-ing, and forces acting to maintain airway patency, notablythe activation of upper airway dilator muscles. The currentbroad conception of OSA pathophysiology is that upper air-way anatomic dimensions are reduced in affected patients,leading to compensatory activation of upper airway dilators.Muscle activity is therefore adequate during wakefulness tomaintain airway patency, but at sleep onset, when upperairway tonic and phasic activity are reduced and protectivereflexes are inhibited, airway closure supervenes.12,13,42
The evidence supporting these concepts, as well as otherpotential factors contributing to the pathophysiology ofOSA, is considered in the following sections. A schematic ofthe mechanisms contributing to upper airway collapse dur-ing sleep is shown in Figure 50-7.
Upper Airway Anatomy in OSA Upper airway collapse dur-ing sleep in OSA occurs predominantly in the retropalatal andretroglossal airway, that is, the velopharynx and oropharynx.
OX
IME
TR
Y 100
21:00 22:00 23:00 00:00 01:00 02:00 03:00 04:00 05:0050
SN
OR
ING
1000
21:00 22:00 23:00 00:00 01:00 02:00 03:00 04:00 05:00-1000
BO
DY
PO
S
21:00 22:00 23:00 00:00 01:00 02:00 03:00 04:00 05:00
Out of BedUpright
RightLeft
ProneSupine
STA
GIN
G
21:00 22:00 23:00 00:00 01:00 02:00 03:00 04:00 05:00
Stage 4
Stage 3
Stage 2Stage 1
WakeRem
RE
SP
IRAT
OR
Y
21:00 22:00 23:00 00:00 01:00 02:00 03:00 04:00 05:00
Ap CHp CAp M
Ap O
Hp OUAWR
FIGURE 50-6 Composite hypnogram from a patient with severeobstructive sleep apnea and hypopnea. Individual apneas andhypopneas are indicated by vertical bars on the “Respiratory”graph. The patient was awake from 1:45 am to 3:15 am, so that no respiratory disturbance occurred during that time. Note that in this patient the severity of respiratory disturbance is influencedby sleep stage and body position. Oxygen desaturation is moresevere during rapid eye movement (REM) than during non-REM sleep, in part due to increased length of events related toincreased arousal threshold during REM. During stage 2, non-REM sleep apneas predominate when the patient is supine (eg, 10 pm), whereas hypopneas predominate when the patient is on the side (eg, 1 am), due to gravitational effects on upper air-way caliber. This results in positional effects on event-associatedoxygen desaturation.
Factors Affecting Upper Airway Calibre
Patency Collapse
Anatomic Configuration(bony structure, soft tissue)
Airway Collapsibility (Pcrit)
Extraluminal Tissue Pressure
Lung Volume
Surface Tension
Intraluminal Pressure
Increased Dilator MuscleActivation
Adaptation Injury, Dysfunction
Sleep-related decrements in muscle activity
Dilator Reflex Responses
Denervation (Sensory, Motor)
Inflammation, Edema
Less Negative More Negative
Lower Higher
Less Positive More Positive
Normal Sleep-relatedDecrement
Blunted (latency, amplitude)
Normal Reduced Dimensions
Traction on UA Reduced EELV, Less Traction
Normal Increased
Mild Marked vs. HeightenedCompensatory Levels During W
Altered Airway Calibre,Tissue Characteristics,
Neuromuscular fxn
Absent Neural, Muscular Dysfunction
Absent
FIGURE 50-7 Schematic of mechanismscontributing to upper airway collapse duringsleep in obstructive sleep apnea.

588 Sleep Disordered Breathing
There is abundant evidence that the airway dimensions arereduced in OSA patients in comparison with normal controlsubjects. Techniques that have been used to study airwaysize include cephalometry, fluoroscopy, acoustic reflection,videoendoscopy, computed tomography, and magneticresonance imaging (MRI). The accumulated data indicatethat both reductions in the dimensions of the bony cranio-facial framework and increases in the size of soft tissuestructures surrounding the airway may contribute toreduced airway dimensions. Alterations in craniofacialproportions that have been described include reducedlength of the mandibular ramus, inferior positioning of the hyoid bone, and retroposition of the maxilla.45 In addi-tion to circumferential narrowing, increased airway lengthmay also be a factor. Increased distance between the hyoidbone and the mandibular plane found in cephalometricstudies and increased airway length found in a recent MRImodeling analysis appear to be associated with an increasedlikelihood of upper airway collapse.46
Increases in soft tissue dimensions that have been foundin imaging studies include enlargement of the soft palate,tongue, parapharyngeal fat pads, and lateral pharyngealwalls. These increases contribute to anatomic narrowingand may also contribute to increased tissue pressure, whichfavors airway collapse. The increased tissue volume proba-bly reflects changes that also affect mechanical characteris-tics of the tissues, leading to altered airway biomechanics(see below). Several mechanisms appear to contribute tothese soft tissue changes. Upper airway edema has beenfound clinically, histologically, and by MRI scanning.47–49
This may result from upper airway trauma during obstruc-tive events, hypoxemia, systemic inflammation, or a combi-nation of factors. Mucosal edema improves with nasalcontinuous positive airway pressure (CPAP) treatment ofOSA.48 Increased deposition of fat in the upper airway inobese patients contributes to narrowing, particularly in theregion of the parapharyngeal fat pads, but elsewhere in theupper airway as well.45 Weight gain is also associated withincreased amounts of fat-free tissue, some of which is mus-cle, such that obesity may contribute to increased upper air-way muscle mass. The latter may also be due to loading withhypertrophy or muscle injury and edema, which is discussedfurther below. Genetic factors probably also play a role indetermining soft-tissue volume, in a manner analogous tocraniofacial structure.
Lung Volume Effects on Upper Airway Size Studies inboth humans and animals have shown that upper airwaycaliber is influenced by changes in lung volume, such thatdecreased lung volume is associated with decreased upperairway dimensions and increased airflow resistance.50–52
This appears to be due to effects of tracheal tug on upper air-way length and/or wall characteristics.51,52 OSA patientsappear to have greater lung volume dependence of upperairway caliber than normal subjects.53 Assumption ofthe recumbent position is associated with reduced end-expiratory lung volume, and obese patients have particularlymarked reductions in supine functional residual capacity.Furthermore, lung volume may also decrease during the
course of obstructive apnea. These reductions in lungvolume would therefore contribute to reduced upper airwaycaliber, further increasing the predisposition to collapse.
Mechanical Properties of the Upper Airway The cross-sectional area of the pharynx is determined by the interac-tion between the mechanical characteristics of thisstructure, that is, compliance of the wall, and the transmuralpressure.12,13 The passive mechanical properties of the upperairway in OSA have received considerable attention.Schwartz and colleagues54,55 have modeled the upper airwayas a Starling resistor and produced an extensive literatureassessing the collapsibility of the pharyngeal airway underpassive conditions. This typically involves the application of a range of positive and negative airway pressures, withextrapolation from steady-state pressure–flow relationshipsto determine the pressure associated with airway closure, orcritical pressure, Pcrit. During sleep, Pcrit values are about�13 cm H2O in normal subjects, about �6 cm H2O in snor-ers, and about �2 cm H2O in patients with predominantlyobstructive hypopnea; in apneic patients, the upper airwayclosing pressure is positive, often in the range �10 to�15 cm H2O. Isono and colleagues56 have studied thestatic properties of the human pharynx under conditions of general anesthesia and muscle paralysis. These authorsfound that for OSA versus control subjects, the average andmaximal velopharyngeal cross-sectional areas were smaller,closing pressures were higher, and area–pressure compliancecurves were shifted down and to the right, indicative ofincreased collapsibility. Other authors have also shownreduced distensibility of the upper airway in OSA.Collectively, these data point to the presence of a smaller,more collapsible, and less distensible, that is, less compliant,airway in OSA.
During active breathing, the transmural pressure acrossthe pharynx is another major determinant of cross-sectionalarea. The transmural pressure is determined by the balancebetween the intraluminal pressure, which is negative duringinspiration, and the extraluminal or tissue pressure. Thelatter is determined by the volume and mechanical charac-teristics of tissues surrounding the airways and by the levelof activation of surrounding constrictor and dilator muscles.Muscle activation will be considered in the followingsection. No direct measurements have been made of inter-stitial tissue pressure in humans, although measurements in anesthetized pigs showed positive extraluminal pressuresthat correlated with airway obstructive events. The occur-rence of airway collapse under passive conditions withoutnegative intraluminal pressure54,55 suggests that positivetissue pressures probably also exist in humans.
Surface tension contributes to pharyngeal collapsi-bility.12,57,58 This may be particularly important at the pointwhere generation of an opening pressure is required toseparate mucosal surfaces that have come into contactduring complete airway collapse. However, surface forceswill also influence the distensibility of the rounded pha-ryngeal structure throughout the respiratory cycle. Upperairway surface lining fluid from OSA subjects showsincreased surface tension in comparison with that of fluid

Physiology of the Upper Airway and Upper Airway Obstruction in Disease 589
from control subjects.58 Topical application of artificialsurfactant renders the upper airway less collapsible and can produce reductions in the severity of obstructive eventsduring sleep in OSA patients.57
Neural Control of Pharyngeal Motor Activity As dis-cussed earlier in this chapter, the tonic and phasic activationof dilatory musculature surrounding the pharyngeal airwayis critical to the prevention of airway collapse as negativeintraluminal pressure during inspiration causes a decrease intransmural pressure. Results from several groups have indi-cated that the activity of upper airway dilators is greater inOSA patients than in normal subjects, and this is believed torepresent a compensatory mechanism for the inherentanatomic compromise of the airway in such patients.59,60
There are several major inputs influencing the activationof pharyngeal dilator muscles by the brainstem respiratorycontroller.13,61–63 As noted above, the normal integrated pat-tern of central respiratory output is such that there is preac-tivation of upper airway musculature before activation of thelower pump muscles occurs.14,15 Perturbations in this pat-tern, with delayed activation of upper airway dilators in rela-tion to chest wall and diaphragm activation, have beenreported in some patients with OSA, and this is believed tocontribute to upper airway instability.15 Central output toupper airway motor neurons is also influenced by chemo-receptor stimulation, so that fluctuations in carbon dioxidelevel may destabilize output to the dilator muscles.
Most important for sleep apnea, however, is the influenceof sleep-related decrements in pharyngeal motor output.Whereas the upper airway may be narrowed during wakeful-ness in OSA, obstruction occurs only during sleep, empha-sizing the importance of state-dependent influences onupper airway control. Sleep onset in normal subjects is ini-tially associated with reduced tonic and phasic activity of thegenioglossus, geniohyoid, and palatal muscles. However,phasic muscle activity tends to recover as sleep is estab-lished, whereas muscles with a predominantly tonic patternof activation tend to show further losses of activity as sleepdeepens.13,42 It is therefore believed that reduced tonic acti-vation is an important factor contributing to upper airwaycollapse. However, both phasic and tonic muscle activitymay be potently inhibited during rapid eye movement(REM) sleep,64 accounting in part for the increased severityof OSA during REM versus non-REM sleep. A key observa-tion in OSA patients is that the fall in upper airway dilatorelectromyographic activity associated with sleep onsetappears to be substantially greater than in controls.65 Thus,upper airway dilator activity is greater during wakefulness,representing a compensation for upper airway size andmechanics, but appears to be lost at sleep onset.
The activity of upper airway dilators is also modulated by reflex inputs. The available evidence indicates that themost important local stimulus for activation of these mus-cles is intrapharyngeal negative pressure.13,66 Reflex activa-tion by pulses of negative pressure applied to the upperairway has been described for the genioglossus, levatorpalatini, and palatoglossus muscles. This negative pressurereflex is impaired for the levator palatini and palatoglossus
muscles in OSA versus control subjects. Furthermore, evenin normal individuals, there is a decrease in the activity ofthis reflex at sleep onset. Thus, an important modulatinginfluence on upper airway caliber is attenuated during sleep,and this is believed to predispose to upper airway collapse.
The afferent inputs to the negative pressure reflex arisefrom the mucosa of the oropharynx and larynx.66–68 Theimportance of mucosal afferents to upper airway motor con-trol has been demonstrated in studies involving topicalapplication of anesthetic to interfere with mucosal sensoryreceptor activity. Topical upper airway anesthesia leads toreduced dilator muscle activity and increased pharyngealairflow resistance during wakefulness and sleep and caninduce apnea and hypopnea in normal subjects, increase thefrequency of obstructive events in snorers, and lead todelayed end-apneic arousal and increased apnea duration inOSA subjects.67–69 Recently, we showed the presence of animpairment in mucosal mechanosensory function in theoropharynx of snorers and OSA patients, which partiallyimproved in OSA patients following CPAP treatment.67 Theseverity of oropharyngeal sensory impairment correlateswith the latency of the palatoglossus and genioglossusmuscle reflex responses to pulses of negative pressuredelivered to the upper airway, as described by Mortimoreand Douglas.70 Therefore, the afferent neural impairmentappears to contribute to impaired dilator reflex responsive-ness, which probably has important implications for upperairway function. Additional studies using endoscopicsensory testing have also demonstrated impaired laryngealsensation in OSA patients versus controls.68 Within the OSA group, there appeared to be two subgroups, one with normal sensation and another with abnormal sensa-tion, the severity of which correlated with the apnea–hypopnea index. Thus, in some patients, an impairment of mucosal sensory function appears to contribute to OSA pathophysiology.
Although the mechanisms underlying impaired upperairway sensation remain unclear, histologic studies havedemonstrated neural changes consistent with injury andrepair that could represent the basis for mucosal sen-sorineural dysfunction.49,68 An accumulating body of datapoints to the presence of significant cellular inflammation in upper airway tissue.49,68 As noted above, this may berelated to tissue injury resulting from vibration-associatedtrauma, hypoxemia, or other factors, including the state of systemic inflammation, which has been associated withboth OSA and obesity. Inflammatory mechanisms ormechanical trauma may account for the neural injuryobserved in the upper airway mucosa, although furtherinvestigation is required to establish the precise mechanismsinvolved.
Pharyngeal Muscle Function in OSA There is accumu-lating evidence that OSA is associated with changes in thestructure and function of the upper airway dilator muscles.Some of these changes appear to be adaptive in nature,whereas others are more consistent with injury and may leadto impaired contractile function, thus contributing to upperairway dysfunction. As noted above, upper airway dilator

590 Sleep Disordered Breathing
activity is increased in OSA patients during wakefulness.Whereas sleep-related decrements in upper airway muscleactivity contribute to upper airway collapse, the terminationof obstructive events is associated with massive activation ofupper airway dilators, which, it should be noted, occursunder hypoxic conditions. Thus, the evidence suggests that,overall, upper airway muscle activity is substantiallyincreased in OSA. This raises the possibility that these mus-cles could undergo secondary changes as a direct conse-quence of their increased activity level.71 Skeletal muscle iswell recognized to alter its phenotype in order to adapt tothe prevailing demands placed upon it, thereby maximizingmuscle efficiency. Properties such as muscle fiber size, con-tractile protein isoform profile, and metabolic enzyme con-tent can be readily modified, with resultant changes inmuscle performance. However, when excessive contractiledemands are placed upon muscle, it is well documented that the structural integrity of the muscle cell can bephysically disrupted by the forces produced during musclecontraction. This activity-induced injury is particularlyprominent when the forces opposing muscle contractionresult in muscle lengthening during activation, or so-calledeccentric contraction.71,72
Eccentric contractions of upper airway dilator muscleshave been demonstrated during airway occlusion andprogressive hypercapnia in anesthetized cats.73 Because similar events occur in human OSA, it has been hypothe-sized that eccentric contractions also occur in pharyngealdilators in this condition,71 through at least two possi-ble mechanisms: (1) muscles that are mechanically linked could contract against one another, as has been demon-strated for the sternohyoid and geniohyoid muscles duringairway occlusion in anesthetized animals, and (2) largenegative intraluminal pressures associated with pharyngealobstruction, which could act to forcibly lengthen the oppos-ing dilator muscles.71,72
Petrof and colleagues,72 using the English bulldog, whichsuffers from OSA, found that the sternohyoid muscle, animportant upper airway dilator muscle, showed evidence offiber-type shift but also changes consistent with activity-induced muscle injury, consisting of abnormal fiber mor-phology (central nucleation, fissured and moth-eatenappearance), inflammatory cell infiltrates, and increasedamounts of connective tissue. Muscle injury was also foundin the geniohyoid muscle, another pharyngeal dilator. Asubsequent MRI study using the bulldog model74 showedchanges consistent with muscle edema or fibrosis in four offive pharyngeal muscles examined. These changes were notseen in limb muscles or in control animals. Thus, there iscompelling evidence for muscle injury in this animal modelof OSA.
Studies on human OSA tissues have also shown evidenceof both adaptation and injury. Several smaller studies haveshown histologic changes consistent with injury.71 However,studies by Series and colleagues75,76 on the musculus uvulaemuscle did not show pathologic evidence of injury butdemonstrated an increase in the proportion of fast-twitch(type IIa) fibers and the activity of enzymes of anaerobicmetabolism in OSA patients. The force-generating capacity
of the muscle was the same in OSA patients and controlsubjects when normalized for muscle cross-sectional area,but in a subsequent study, changes in the musculus uvulaemuscle correlated with upper airway collapsibility. Patientswith the most easily collapsible upper airway also showedthe greatest increases in force production, type IIa fiberprevalence, anaerobic metabolism, and susceptibility tomuscle fatigue. Carrera and Barbé77 studied genioglossusmuscles from OSA patients and from controls; they alsoreported a shift to type II fiber type and specifically demon-strated increased fatigability of the genioglossus muscle inOSA. Thus, even in the absence of morphologic injury,adaptive changes induced by the contraction history of the upper airway muscles may also have adverse functionalconsequences.
In the discussion on pharyngeal motor control in the pre-ceding section, it was noted that there is evidence for anupper airway afferent neuropathy in OSA, based on bothsensory testing data and pathologic findings. There is evi-dence to suggest that there may, in fact, be a more diffuseupper airway neuropathy in OSA that also affects efferentnerves and may lead to muscle denervation. Woodson andcolleagues47 reported demyelination in upper airway tissuespecimens. Histologic evidence of motor denervation, suchas fiber type grouping and grouped atrophy, has also beenfound in several recent studies.50,78 In a recent study ofhuman upper airway surgical specimens from OSA and con-trol subjects, we demonstrated increased nerve tissue prolif-eration within the muscle compartment, revealed by specificantibody to neural tissue (PGP 9.5), and also found groupsof myocytes expressing neural cell adhesion molecule, asensitive marker of muscle denervation.49 These findingssuggest that denervation-related changes may contribute toupper airway muscle function in OSA.
As discussed above, the edema and inflammatory cellinfiltration of the upper airway mucosa described by severalgroups suggest that inflammatory mechanisms may con-tribute to upper airway dysfunction in OSA, leading, forexample, to neuropathic changes.49 In the study just citedfrom the author’s laboratory,49 we demonstrated increasedinflammatory cell infiltration in OSA upper airway muscle.Furthermore, preliminary data from our laboratory haverevealed increased expression of tumor necrosis factor-� andinterleukin-1� in muscle tissue from patients with severeOSA versus those with mild OSA. It is now well establishedthat cytokines can lead directly to muscle dysfunction.79
Thus, inflammatory changes in the upper airway may alter muscle function directly by this means or conceivablyby contributing to neuropathy, which, in turn, may lead tomuscle denervation. It is likely that muscle adaptation and injury are ongoing in a dynamic process in OSA, thatdifferent muscle groups within the upper airway may beaffected differently, and that the extent of change and phys-iologic consequences for muscle function may vary betweenOSA patients. Further work will be required to further elu-cidate the contribution of upper airway muscle denervation and injury to the pathophysiology of this disorder, as well asto determine whether muscle changes may represent apotential therapeutic target in OSA.

Physiology of the Upper Airway and Upper Airway Obstruction in Disease 591
OSA and Ventilatory Control There is a growingunderstanding of the effects of chemoreceptor sensitivityand ventilatory control instability on the pathogenesis ofperiodic breathing and central apnea.80,81 Differences in thecontrol of breathing between wakefulness and sleep (eg, thehigher ventilatory setpoint and ventilatory chemosensitivityduring wakefulness) lead to respiratory instability duringthe transition from wakefulness to sleep, accounting forapneas and hypopneas, which may be seen at sleep onset innormal subjects. Furthermore, recent work has shown thatventilatory responses are heightened at the instant of arousalfrom sleep in comparison to stable wakefulness.62 Thus,instability of the sleep–wake state per se may destabilizebreathing. The state changes associated with apneas andhypopneas, that is, microarousal at the termination ofevents, followed by the rapid return to sleep, thereforerepresent a situation of inherently unstable respiratory con-trol. Numerous investigators have postulated that alteredchemoreceptor sensitivity or instability of other respiratorycontrol mechanisms may therefore contribute to the patho-genesis of OSA. An early observation in support of thishypothesis was the occurrence of periodic breathing duringsleep immediately following tracheostomy for OSA.82
A large body of data has been generated concerningchanges in classic chemoreceptor responses in OSA,although there have been rather inconsistent findings. Someauthors have reported heightened hypoxic sensitivity, whichwas postulated to contribute to respiratory instability,whereas others have reported blunted hypoxic sensitivity.83
Hypercapnic ventilatory responsiveness has been reportedto be normal or decreased in OSA and, if reduced, mayimprove following treatment with nasal CPAP.83
Recently, Younes and colleagues used proportional assistventilation (PAV) to evaluate ventilatory control stability inOSA patients.84 With the upper airway stabilized duringsleep by nasal CPAP, increasing levels of PAV (controllergain) were applied up to the point at which periodic breath-ing was elicited. It was found that patients with severe OSA were much more susceptible to the development ofperiodic breathing than patients with mild-to-moderateOSA, indicating increased endogenous loop gain in thesevere group. The mechanisms underlying this ventilatoryinstability, and its precise role in the pathogenesis of OSA,remain to be established.
Although the role of changes in chemoreceptor sensitiv-ity in the pathogenesis of OSA remains unclear, there isstrong evidence that severe OSA may produce secondarychanges in ventilatory control, namely hypoventilation dur-ing wakefulness. This occurs in a subset of OSA patientswho appear to be the group at risk for decompensation andrespiratory failure in the context of intercurrent medical ill-ness, or in some cases simply because of inexorable progres-sion of the changes associated with sleep-disorderedbreathing. Most patients with OSA and daytime hypoxemiaand/or hypercapnia have some underlying lung dysfunction,such as COPD or obesity-related or neuromuscular restric-tive impairment.83,85,86 OSA patients with hypercapnia havebeen described as demonstrating impaired ventilatory recov-ery after apnea.87 This may represent a blunting or failure of
load compensation mechanisms in such patients and maycontribute to a “resetting” of the chemoreceptors, leading toawake hypoventilation. Daytime blood gases typicallyimprove dramatically or normalize following effective treat-ment of OSA, supporting the concept that the nocturnalrespiratory disturbance leads to the development of awakehypoventilation.
OSA and Asthma There is growing evidence of a linkbetween OSA and asthma. In a recent study at McGill,88 26consecutive refractory asthmatic subjects were evaluated incomparison with 21 age-matched and gender-matched con-trol subjects with moderate asthma. The prevalence of OSAin both groups was dramatically increased over populationnormal values, with a tendency for OSA to be more preva-lent among subjects with severe asthma (16/26, 62%) thanamong those with moderate asthma (10/21, 48%) and forOSA to be somewhat more severe among the refractoryasthma group. These findings, together with evidence fromother case series, suggest that OSA may contribute to wors-ened asthma control. For example, Chan and colleagues89
studied nine patients with severe asthma and snoring orOSA who suffered frequent nocturnal asthma attacks despitemaximum bronchodilator therapy. CPAP treatment of upperairway obstruction during sleep improved asthma control,as reflected in asthma symptoms, bronchodilator use, andpeak flow rates.
There are several mechanisms by which OSA and asthmacould interact. There is evidence that stimulation of upperairway mechanoreceptors during snoring and apneas canlead to reflex bronchoconstriction. Alternatively, gastro-esophageal reflux occurs frequently in OSA patients and is awell-recognized exacerbating factor in asthma. Treatment ofasthma with corticosteroids may contribute to OSA byincreasing obesity and/or pharyngeal myopathy.90 Finally, asnoted above, there are considerable data documenting upperairway inflammation in OSA and growing evidence that thisplays a role in OSA pathophysiology. The links between rhi-nosinus inflammation and lower airway inflammation inasthma are well documented (termed the “united airwayhypothesis”). It may therefore be that pharyngeal involve-ment represents part of a continuum of airway inflammatoryinvolvement. There may thus be a reciprocal interactionbetween these disease processes, such that worsening ofOSA may contribute to worsened asthma control and viceversa. This concept is supported by the clinical data citedabove concerning the effects of OSA treatment on asthmacontrol. Research efforts are ongoing to further evaluate themechanisms of the OSA–asthma interaction and to moresystematically assess the effects of OSA treatment on asthmacontrol.
PHYSIOLOGIC ASPECTS OF DIAGNOSTIC TESTING
FOR OSAIn recent years, recording of nasal pressure has emerged as a sensitive indicator of upper airway narrowing.Introduction of a standard nasal oxygen cannula into thenares, with connection of the tubing end to a differentialpressure transducer referenced to atmosphere, provides for

592 Sleep Disordered Breathing
a semiquantitative assessment of nasal airflow. Of greaterinterest is the fact that the shape of the inspiratory pressurecurve during tidal respiratory cycles shows flattening indica-tive of flow limitation as upper airway narrowing occurs, inthe same way that forced maximal curves reveal extratho-racic upper airway obstruction, as discussed earlier in thischapter.91,92 This technique provides for the detection ofsubtle episodes of upper airway narrowing.
Respiratory effort was traditionally measured by using anesophageal catheter to estimate pleural pressure. This inva-sive approach has largely been replaced by techniquesinvolving the use of sensors on the rib cage and abdomen todetect respiratory effort and movement. The most sensitiveof these is respiratory inductance plethysmography, whichprovides data on changes in thoracoabdominal motionresulting from partial or complete upper airway obstruction.Partial or complete rib cage paradoxical motion is often seenduring apneas and hypopneas and can provide confirmatoryevidence of increasing respiratory effort in the context ofupper airway obstruction.
PHYSIOLOGY OF TREATMENT APPROACHES TO OSAThere are several treatments aimed at compensating for the anatomic predisposition to upper airway collapse.Mandibular advancement splints, for example, act to advancethe lower jaw in relation to other craniofacial structures,
thereby increasing the anteroposterior oropharyngealdimension.93 This approach does not compensate for otherfactors contributing to upper airway collapse during sleep,and there are limitations to its anatomic effects. Oral appli-ances are therefore effective in mild-to-moderate apnea buttypically do not alleviate moderate-to-severe OSA. Surgicalinterventions are also aimed at compensating for reducedupper airway dimensions. In childhood OSA, hypertrophyof the adenoid and, to a lesser extent, the palatine tonsils isoften a major factor contributing to airway compromise, sothat adenoidectomy–tonsillectomy is a mainstay of treat-ment for OSA in the child. Maxillomandibular advancementsurgery may be beneficial in the context of craniofacialinsufficiency, for example, the marked micrognathia associ-ated with Pierre–Robin syndrome. This approach may alsobe useful for nonobese adults with similar but more subtlecraniofacial disproportion. Surgical intervention in general,however, has a much more limited role in adult OSA.94
Tracheostomy is highly effective as it bypasses the site ofairway obstruction. However, there are adverse social as well as medical aspects of chronic tracheostomy, whichseverely limit the applicability of this intervention. A variety of approaches directed at reducing or stiffening soft palate tissue have been applied to adult OSA. These include conventional uvulopalatopharyngo-plasty, laser-assisted uvuloplasty, radiofrequency-controlled
Clinical Suspicion of OSA
Polysomnography (PSG) Readily Available
No
PortableMonitor
Yes
PSG
RDI < 10 RDI 10-30 RDI > 30 AHL < 10 AHL 10-30 AHL > 30
Daytime Sleepiness Daytime Sleepiness
No No No NoYes Yes Yes Yes
PSGStop W/U Clinical F/U Treat TreatConsiderOtherDx +/orRepeatPSG
Stop W/U Clinical F/U TreatTreat
Treatment Decision
CPAP CPAP Alternaitve (oralappliance surgery)
Titration PSG
Clnical F/U
Sleep Hx, F/U, PSG
PSG on Treatment
AHI > 10
AdjustTreatment orCPAP Trial
Persistent orRecurrent Sx
AHI < 10
Daytime Sleepiness Daytime Sleepiness
FIGURE 50-8 Approach todiagnosis and managementof obstructive sleep apnea.

Physiology of the Upper Airway and Upper Airway Obstruction in Disease 593
thermoablation (somnoplasty), and other procedures.Overall, the results of these interventions have been highly disappointing in the context of moderate-to-severe OSA.This is undoubtedly due to the limited anatomic effects of these interventions, combined with the role of factorsother than anatomic predisposition to upper airway collapseduring sleep.
The treatment of choice for OSA is nasal CPAP.95,96 CPAPfunctions as a pneumatic splint for the upper airway. Asealed mask is applied over the nose, and a continuouspositive pressure is applied to the mask from a blower unitto distend the airway. The pressure required to maintainairway patency is determined by anatomic, mechanical, neu-romuscular, and state-dependent factors, such that a greaterpressure may be required for the supine position than for thelateral decubitus position and during REM than during non-REM sleep. Traditionally, CPAP titration has been per-formed in the sleep laboratory, with manual adjustment todetermine the minimum pressure required to maintain air-way patency in all sleep stages and body positions. Thispressure is then prescribed for home treatment. Morerecently, automated CPAP devices have become available,which continuously monitor the amplitude and contour ofairflow with a pneumotachograph in the CPAP unit. Amicroprocessor then evaluates the adequacy of these signalsand adjusts the pressure to respond to inspiratory flowlimitation and/or reduced airflow. The concept is that this isa more physiologic approach that should match the treat-ment delivered to the dynamic changes in upper airwaycaliber determined by the factors described above. An algo-rithm for the diagnosis and management of OSA is shown inFigure 50-8.
UPPER AIRWAY IN CENTRAL SLEEP APNEA
Central sleep apnea is encountered in a variety of clinicalconditions. It may be present as part of primary or sec-ondary hypoventilation syndromes (hypercapnic centralapnea) due to central nervous system (CNS) lesions orneuromuscular disease involving the respiratory muscles.Alternatively, nonhypercapnic forms of central apneainclude idiopathic central sleep apnea and Cheyne–Stokesrespiration (CSR) during sleep, which may occur in thesetting of congestive heart failure, renal failure, or CNSlesions.97
Although the upper airway is not believed to play a pri-mary role in most of these conditions, there is evidence thatupper airway instability and collapse are associated withcentral apnea and may contribute to its pathophysiology.Badr and colleagues have shown, using video-endoscopy, thatupper airway collapse occurs in the context of hyperventila-tion-induced central apnea during sleep, even in normalsubjects.98 Thus, the loss of respiratory drive due to inducedhypocapnia leads to airway closure, confirming the impor-tance of respiratory drive to upper airway muscles in main-taining airway patency. Conversely, there is evidence thatupper airway collapse may induce central apneas. Theclinical correlate of this is that patients with snoring andsome obstructive apneas or hypopneas during REM sleep
may demonstrate central events during non-REM sleep.Furthermore, some patients with predominant central apnearespond to nasal CPAP treatment, suggesting that upperairway closure contributes to these events.99 These findingsmay in part be explained by evidence indicating that stimu-lation of upper airway mechanoreceptors may result inreflex inhibition of inspiratory drive. Thus, stimulation oflaryngeal receptors in experimental animals has beenreported to induce apnea.97,100 Furthermore, we found thatinhibition of upper airway mucosal receptors with the use oftopical anesthesia resulted in increased respiratory effortduring obstructive apneas in OSA patients. This points tothe loss of an inhibitory influence on respiratory drive, withattenuation of airway sensory receptor function.69
There has been considerable recent interest in CSRduring sleep in the setting of chronic congestive heartfailure. Sleep-disordered breathing is common among stable heart failure patients, occurring in up to 40%,101,102
with CSR representing the most common form. CSR isbelieved to both result from and lead to worsening of heart failure through complex mechanisms and has beenshown to be associated with reduced survival for a givenlevel of cardiac dysfunction. Treatment with nasal CPAP in this group leads to improvements in CSR, ventricularfunction, and quality of life.102 A multicenter trial (CAN-PAP) is currently under way to determine the effects of CPAP on mortality in heart failure patients with CSR. Themechanisms by which CPAP leads to improvement in CSRremain unclear. However, recent work at McGill, involvingthe forced oscillation technique to assess upper airwaypatency, has demonstrated that upper airway closure isfrequent even during pure central events in heart failurepatients with CSR.103 Furthermore, overlap between OSAand CSR has been described in this population.104
Thus, upper airway instability may also contribute to thepathogenesis of CSR.
SUMMARY AND CONCLUSIONS
This chapter has examined the normal structure andfunction of the upper airway, with an emphasis on thephysiologic aspects of the integration of breathing with thevariety of other upper airway functions. The most seriousclinical disturbance of upper airway function is anatomic or functional obstruction with airflow compromise. We have considered the physiologic basis for both the clinicalpresentation and approach to diagnostic testing for thevarious forms of upper airway obstruction. Finally, we have considered sleep-disordered breathing and in particularOSA, a very common but, for many individuals, no lessserious form of variable extrathoracic upper airwayobstruction occurring during sleep. The research that has been directed at understanding the mechanisms under-lying OSA has led to major advances in our knowledge ofupper airway structure and function. Although considerableprogress has been made, ongoing work aimed at furtherelucidating the mechanisms of OSA will undoubtedlybroaden our understanding of upper airway function ingeneral.

594 Sleep Disordered Breathing
REFERENCES
1. Proctor D. Form and function of the upper airways and thelarynx. In: Macklem P, Mead J, editors. Handbook of physi-ology. Section 3. The respiratory system, mechanics ofbreathing. Bethesda, MD: American Physiological Society;1986. p. 63–74.
2. Isaacs RS, Sykes JM. Anatomy and physiology of the upperairway. Anesthesiol Clin North Am 2002;20:733–45, v.
3. Proctor DF. The upper airways. II. The larynx and trachea. AmRev Respir Dis 1977;115:315–42.
4. Doyle DJ, Arellano R. Upper airway diseases and airway man-agement: a synopsis. Anesthesiol Clin North Am 2002;20:767–87, vi.
5. Cauna N. Blood and nerve supply of the nasal lining. In:Proctor DF, Anderson IB, editors. The nose. Oxford: ElsevierBiomedical Press; 1982. p. 44–69.
6. Thach B, Brouillette R. The respiratory function of pharyngealmusculature: relevance to clinical obstructive apnea. In:Euler C, Lagercrantz H, editors. Central nervous controlmechanisms in breathing. Oxford: Pergamon Press; 1979. p.483–94.
7. McFarland DH, Lund JP. Modification of mastication andrespiration during swallowing in the adult human. JNeurophysiol 1995;74:1509–17.
8. McFarland DH, Lund JP, Gagner M. Effects of posture on thecoordination of respiration and swallowing. J Neurophysiol1994;72:2431–7.
9. Broussard DL, Altschuler SM. Central integration of swallowand airway-protective reflexes. Am J Med 2000;108 Suppl4a:62S–7S.
10. Remmers JE, DeGroot WJ, Sauerland EK, Anch AM.Pathogenesis of upper airway occlusion during sleep. JAppl Physiol 1978;44:931–8.
11. Kuna ST, Sant’Ambrogio G. Pathophysiology of upper airwayclosure during sleep. JAMA 1991;266:1384–9.
12. Wheatley JR, Amis TC. Mechanical properties of the upperairway. Curr Opin Pulm Med 1998;4:363–9.
13. Fogel RB, Malhotra A, White DP. Sleep. 2: pathophysiology ofobstructive sleep apnoea/hypopnoea syndrome. Thorax2004;59:159–63.
14. Strohl KP, Hensley MJ, Hallett M, et al. Activation of upper air-way muscles before onset of inspiration in normal humans.J Appl Physiol 1980;49:638–42.
15. Hudgel DW, Harasick T. Fluctuation in timing of upper airwayand chest wall inspiratory muscle activity in obstructivesleep apnea. J Appl Physiol 1990;69:443–50.
16. Patrick GB, Strohl KP, Rubin SB, Altose MD. Upper airway anddiaphragm muscle responses to chemical stimulation andloading. J Appl Physiol 1982;53:1133–7.
17. Sasaki CT, Weaver EM. Physiology of the larynx. Am J Med1997;103:9S–18S.
18. Suzuki M, Kirchner JA. The posterior cricoarytenoid as an inspi-ratory muscle. Ann Otol Rhinol Laryngol 1969;78:849–64.
19. Wyke B. Respiratory activity of intrinsic laryngeal muscles. Anexperimental study. In: Wyke BD, editor. Ventilatory andphonatory control systems. London: Oxford UniversityPress; 1974. p. 408–21.
20. Fortier PH, Reix P, Arsenault J, et al. Active upper airway closureduring induced central apneas in lambs is complete at thelaryngeal level only. J Appl Physiol 2003;95:97–103.
21. Cormier YF, Camus P, Desmeules MJ. Non-organic acute upperairway obstruction: description and a diagnostic approach.Am Rev Respir Dis 1980;121:147–50.
22. Newman KB, Mason UG III, Schmaling KB. Clinical features ofvocal cord dysfunction. Am J Respir Crit Care Med 1995;152(4 Pt 1):1382–6.
23. Macklem P, Rector W, Wang K. Upper airway obstruction inasthma. Johns Hopkins Med J 1980;147:233–7.
24. Proctor DF. Modifications of breathing for phonation. In:Macklem PT, Mead J, editors. Handbook of physiology.Bethesda (MD): American Physiological Society; 1986. p.597–604.
25. Johnston S, Yan S, Sliwinski P, Macklem PT. Modified Campbelldiagram to assess respiratory muscle action in speech.Respirology 1999;4:213–22.
26. Kryger M, Bode F, Antic R, Anthonisen N. Diagnosis of obstruc-tion of the upper and central airways. Am J Med 1976;61:85–93.
27. Miller RD, Hyatt RE. Evaluation of obstructing lesions of thetrachea and larynx by flow–volume loops. Am Rev RespirDis 1973;108:475–81.
28. Hyatt RE. Evaluation of major airway lesions using theflow–volume loop. Ann Otol Rhinol Laryngol 1975;84(5 Pt 1):635–42.
29. Gibson GJ, Pride NB, Empey DW. The role of inspiratorydynamic compression in upper airway obstruction. Am RevRespir Dis 1973;108:1352–60.
30. Owens GR, Murphy DM. Spirometric diagnosis of upper airwayobstruction. Arch Intern Med 1983;143:1331–4.
31. Kashima HK. Documentation of upper airway obstruction inunilateral vocal cord paralysis: flow–volume loop studies in43 subjects. Laryngoscope 1984;94:923–37.
32. Vincken WG, Gauthier SG, Dollfuss RE, et al. Involvement ofupper-airway muscles in extrapyramidal disorders. A causeof airflow limitation. N Engl J Med 1984;311:438–42.
33. Vincken W, Elleker G, Cosio MG. Detection of upper airwaymuscle involvement in neuromuscular disorders using theflow–volume loop. Chest 1986;90:52–7.
34. Orr JB. Helium–oxygen gas mixtures in the management ofpatients with airway obstruction. Ear Nose Throat J 1988;67:866–9.
35. Ernst A, Feller-Kopman D, Becker HD, Mehta AC. Centralairway obstruction. Am J Respir Crit Care Med 2004;169:1278–97.
36. Hnatiuk OW, Corcoran PC, Sierra A. Spirometry in surgery foranterior mediastinal masses. Chest 2001;120:1152–6.
37. Kanter RK, Watchko JF. Pulmonary edema associated with upper airway obstruction. Am J Dis Child 1984;138:356–8.
38. Kollef MH, Pluss J. Noncardiogenic pulmonary edema follow-ing upper airway obstruction. 7 cases and a review of theliterature. Medicine (Baltimore) 1991;70:91–8.
39. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructivesleep apnea: a population health perspective. Am J RespirCrit Care Med 2002;165:1217–39.
40. Flemons WW. Clinical practice. Obstructive sleep apnea. N Engl J Med 2002;347:498–504.
41. Cistulli PA, Sullivan CE. Pathophysiology of sleep apnea. In:Saunders NA, Sullivan CE, editors. Sleep and breathing.New York: Marcel Dekker; 1994. p. 405–48.
42. Ayappa I, Rapoport DM. The upper airway in sleep: physiologyof the pharynx. Sleep Med Rev 2003;7:9–33.
43. Rechtschaffen A, Kales A. A manual of standardized terminol-ogy, technique and scoring system for sleep stages ofhuman sleep. Los Angeles: Los Angeles Brain InformationService, Brain Information Institute, UCLA; 1968.
44. Sleep-related breathing disorders in adults: recommenda-tions for syndrome definition and measurement tech-niques in clinical research. The Report of an AmericanAcademy of Sleep Medicine Task Force. Sleep 1999;22:667–89.
45. Schwab RJ. Pro: sleep apnea is an anatomic disorder. Am J Respir Crit Care Med 2003;168:270–1.

Physiology of the Upper Airway and Upper Airway Obstruction in Disease 595
46. Malhotra A, Huang Y, Fogel RB, et al. The male predispositionto pharyngeal collapse: importance of airway length. Am J Respir Crit Care Med 2002;166:1388–95.
47. Woodson BT, Garancis JC, Toohill RJ. Histopathologic changesin snoring and obstructive sleep apnea syndrome.Laryngoscope 1991;101:1318–22.
48. Ryan CF, Lowe AA, Li D, Fleetham JA. Three-dimensionalupper airway computed tomography in obstructive sleep apnea. A prospective study in patients treated byuvulopalatopharyngoplasty. Am Rev Respir Dis 1991;144:428–32.
49. Boyd JH, Petrof BJ, Hamid Q, et al. Upper airway muscle inflam-mation and denervation changes in obstructive sleepapnea. Am J Respir Crit Care Med 2004;170:541–6.
50. Series F, Cormier Y, Desmeules M. Influence of passivechanges of lung volume on upper airways. J Appl Physiol1990;68:2159–64.
51. Van de Graaff WB. Thoracic traction on the trachea: mecha-nisms and magnitude. J Appl Physiol 1991;70:1328–36.
52. Rowley JA, Permutt S, Willey SJ, et al. Effect of tracheal andtongue displacement on upper airway airflow dynamics. J Appl Physiol 1996;80:2171–8.
53. Hoffstein V, Zamel N, Phillipson EA. Lung volume dependenceof pharyngeal cross-sectional area in patients with obstruc-tive sleep apnea. Am Rev Respir Dis 1984;130:175–8.
54. Schwartz AR, Smith PL, Wise RA, et al. Induction of upper air-way occlusion in sleeping individuals with subatmosphericnasal pressure. J Appl Physiol 1988;64:535–42.
55. Gleadhill IC, Schwartz AR, Schubert N, et al. Upper airway col-lapsibility in snorers and in patients with obstructivehypopnea and apnea. Am Rev Respir Dis 1991;143:1300–3.
56. Isono S, Remmers JE, Tanaka A, et al. Anatomy of pharynx inpatients with obstructive sleep apnea and in normalsubjects. J Appl Physiol 1997;82:1319–26.
57. Jokic R, Klimaszewski A, Mink J, Fitzpatrick MF. Surface tensionforces in sleep apnea: the role of a soft tissue lubricant: a randomized double-blind, placebo-controlled trial. Am J Respir Crit Care Med 1998;157(5 Pt 1):1522–5.
58. Kirkness JP, Madronio M, Stavrinou R, et al. Relationshipbetween surface tension of upper airway lining liquid andupper airway collapsibility during sleep in obstructivesleep apnea hypopnea syndrome. J Appl Physiol 2003;95:1761–6.
59. Mezzanotte WS, Tangel DJ, White DP. Waking genioglossalelectromyogram in sleep apnea patients versus normalcontrols (a neuromuscular compensatory mechanism). J Clin Invest 1992;89:1571–9.
60. Suratt PM, McTier RF, Wilhoit SC. Upper airway muscle activa-tion is augmented in patients with obstructive sleep apneacompared with that in normal subjects. Am Rev Respir Dis1988;137:889–94.
61. Horner RL. Motor control of the pharyngeal musculature andimplications for the pathogenesis of obstructive sleepapnea. Sleep 1996;19:827–53.
62. Horner RL. Impact of brainstem sleep mechanisms on pharyn-geal motor control. Respir Physiol 2000;119:113–21.
63. Horner RL. The neuropharmacology of upper airway motorcontrol in the awake and asleep states: implications forobstructive sleep apnoea. Respir Res 2001;2:286–94.
64. Wiegand L, Zwillich CW, Wiegand D, White DP. Changes inupper airway muscle activation and ventilation duringphasic REM sleep in normal men. J Appl Physiol 1991;71:488–97.
65. Mezzanotte WS, Tangel DJ, White DP. Influence of sleep onseton upper-airway muscle activity in apnea patients versusnormal controls. Am J Respir Crit Care Med 1996;153(6 Pt 1):1880–7.
66. Malhotra A, Fogel RB, Edwards J, et al. Local mechanisms drive genioglossus activation in obstructive sleep apnea.Am J Respir Crit Care Med 2000;161:1746–9.
67. Kimoff RJ, Sforza E, Champagne V, et al. Upper airway sensa-tion in snoring and obstructive sleep apnea. Am J RespirCrit Care Med 2001;164:250–5.
68. Nguyen ATD, Jobin V, Payne R, et al. Laryngeal and velopha-ryngeal sensory impairment in obstructive sleep apnea.Sleep. [In press]
69. Cala SJ, Sliwinski P, Cosio MG, Kimoff RJ. Effect of upper airway anesthesia on apnea lengthening across the night in obstructive sleep apnea. J Appl Physiol 1996;81:2618–26.
70. Mortimore IL, Douglas NJ. Palatal muscle EMG response tonegative pressure in awake sleep apneic and controlsubjects. Am J Respir Crit Care Med 1997;156:867–73.
71. Petrof BJ, Hendricks JC. Muscle factors in obstructive sleepapnea. In: Pack AI, editor. Sleep apnea: pathogenesis,diagnosis, and treatment. New York: Marcel Dekker; 2002.p. 217–34.
72. Petrof BJ, Pack AI, Kelly AM, et al. Pharyngeal myopathy ofloaded upper airway in dogs with sleep apnea. J ApplPhysiol 1994;76:1746–52.
73. van Lunteren E, Haxhiu MA, Cherniack NS. Effects of trachealairway occlusion on hyoid muscle length and upper airwayvolume. J Appl Physiol 1989;67:2296–302.
74. Schotland HM, Insko EK, Panckeri KA, et al. Quantitative mag-netic resonance imaging of upper airway musculature in ananimal model of sleep apnea. J Appl Physiol 1996;81:139–46.
75. Series F, Cote C, Simoneau J-A, et al. Physiologic, metabolic,and muscle fiber type characteristics of musculus uvulae insleep apnea hypopnea syndrome and in snorers. J ClinInvest 1995;95:20–5.
76. Series F, Simoneau JA, St Pierre S. Muscle fiber area distribu-tion of musculus uvulae in obstructive sleep apnea andnon-apneic snorers. Int J Obes Relat Metab Disord 2004;24:410–5.
77. Carrera M, Barbé F, Savelda J, et al. Patients with obstructivesleep apnea exhibit genioglossus dysfunction that isnormalized after treatment with continuous positive airwaypressure. Am J Respir Crit Care Med 1999;159:1960–6.
78. Edstrom L, Larsson H, Larsson L. Neurogenic effects on thepalatopharyngeal muscle in patients with obstructive sleepapnoea: a muscle biopsy study. J Neurol NeurosurgPsychiatry 1992;55:916–20.
79. Wilcox P, Milliken C, Bressler B. High-dose tumor necrosisfactor � produces an impairment of hamster diaphragmcontractility. Am J Respir Crit Care Med 1996;153:1611–5.
80. Phillipson EA, Bowes G. Control of breathing during sleep. In: Cistulli PA, Widdicombe JG, editors. Handbook of phys-iology. Vol 2. The respiratory system, control of breathing.Section 3. Part 1. Bethesda, MD: American PhysiologicalSociety; 1986. p. 649–80.
81. Dempsey JA, Smith CA, Eastwood PR, et al. Sleep-inducedrespiratory instabilities. In: Pack AI, editor. Sleep apnea:pathogenesis, diagnosis and treatment. New York: MarcelDekker; 2002. p. 57–98.
82. Onal E, Lopata M. Periodic breathing and the pathogenesis ofocclusive sleep apnea. Am Rev Respir Dis 1982;126:676–80.
83. Kimoff RJ, Brooks D, Horner RL, et al. Ventilatory and arousalresponses to CO2 and hypoxia during application of acanine model of obstructive sleep apnea. Am J Respir CritCare Med 1997;156:886–94.
84. Younes M, Ostrowski M, Thompson W, et al. Chemical controlstability in patients with obstructive sleep apnea. Am J Respir Crit Care Med 2001;163:1181–90.

596 Sleep Disordered Breathing
85. Bradley TD, Rutherford R, Lue F, et al. Role of diffuse airwayobstruction in the hypercapnia of obstructive sleep apnea.Am Rev Respir Dis 2004;134:920–4.
86. Krieger J, Sforza E, Apprill M, et al. Pulmonary hypertension,hypoxemia, and hypercapnia in obstructive sleep apneapatients. Chest 1989;96:729–37.
87. Ayappa I, Berger KI, Norman RG, et al. Hypercapnia and ven-tilatory periodicity in obstructive sleep apnea syndrome.Am J Respir Crit Care Med 2002;166:1112–5.
88. Shannon J, Pepe C, Ernst P, et al. High prevalence of obstruc-tive sleep apnea (OSA) in severe and moderate asthma.Am J Respir Crit Care Med 2004;169:A542.
89. Chan CS, Woolcock AJ, Sullivan CE. Nocturnal asthma: role ofsnoring and obstructive sleep apnea. Am Rev Respir Dis1988;137:1502–4.
90. Yigla M, Tov N, Solomonov A, et al. Difficult-to-control asthma and obstructive sleep apnea. J Asthma 2003;40:865–71.
91. Montserrat JM, Farre R, Ballester E, et al. Evaluation of nasalprongs for estimating nasal flow. Am J Respir Crit Care Med1997;155:211–5.
92. Condos R, Norman RG, Krishnasamy I, et al. Flow limitation asa non-invasive assessment of residual upper-airway resist-ance during continuous positive airway pressure therapy ofobstructive sleep apnea. Am J Respir Crit Care Med1994;150:475–80.
93. Ferguson KA. The role of oral appliance therapy in thetreatment of obstructive sleep apnea. Clin Chest Med2003;24:355–64.
94. Li KK. Surgical management of obstructive sleep apnea. ClinChest Med 2003;24:365–70.
95. Sullivan CE, Issa FG, Berthon-Jones M, Eves L. Reversal ofobstructive sleep apnoea by continuous positive airwaypressure applied through the nares. Lancet 1981;1:862–5.
96. Verse T, Pirsig W, Stuck BA, et al. Recent developments in thetreatment of obstructive sleep apnea. Am J Respir Med2003;2:157–68.
97. Bradley TD, Phillipson EA. Central sleep apnea. Clin ChestMed 1992;13:493–505.
98. Badr MS, Toiber F, Skatrud JB, Dempsey J. Pharyngeal narrow-ing/occlusion during central sleep apnea. J Appl Physiol1995;78:1806–15.
99. Hoffstein V, Slutsky AS. Central sleep apnea reversed bycontinuous positive airway pressure. Am Rev Respir Dis1987;135:1210–2.
100. Lee JC, Stoll BJ, Downing SE. Properties of the laryngealchemoreflex in neonatal piglets. Am J Physiol 1977;233:R30–6.
101. Bradley TD, Floras JS. Sleep apnea and heart failure: part II:central sleep apnea. Circulation 2003;107:1822–6.
102. Sin DD, Logan AG, Fitzgerald FS, et al. Effects of continuouspositive airway pressure on cardiovascular outcomes inheart failure patients with and without Cheyne–Stokesrespiration. Circulation 2000;102:61–6.
103. Jobin V, Rigau J, Farre R, et al. Evaluation of upper airwaypatency during Cheyne–Stokes respiration using the forcedoscillation technique. Am J Respir Crit Care Med 2002;165:A247.
104. Tkacova R, Niroumand M, Lorenzi-Filho G, Bradley TD.Overnight shift from obstructive to central apneas inpatients with heart failure: role of PCO2 and circulatorydelay. Circulation 2001;103:238–43.