ch04
30
C H A P T E R zzzzzzzzzzzzzzzzzzzzzzzzzzz 4 Biomechanics of Fractures Biomechanics of Fractures zzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzz John A. Hipp, Ph.D. Wilson C. Hayes, Ph.D. Bone is a remarkable material with complex mechanical properties and a unique ability for self-repair, making it a fascinating structural material from both a clinical and an engineering perspective. Bone fails when overloaded, initiating a complex series of biologic and biomechanical events directed toward repair and restoration of function. Tremendous progress is being made in understanding, controlling, and enhancing the biologic aspects of fracture healing. The mechanical environment is always a crucial element of fracture healing, with strong interactions between biologic and mechanical factors. Clinical manage- ment of fractures must influence both the biologic and the mechanical conditions so that the original load-bearing capacity of the bone is restored as quickly as possible. There are thus three principal aspects of the biomechanics of fractures and their treatment: (1) biomechanical fac- tors that determine when and how a bone fractures, (2) biomechanical factors that influence fracture healing, and (3) control of the biomechanical environment by fracture treatments. The biomechanical factors that determine whether a bone fractures include the loads applied and the mechan- ical properties of bone and soft tissue. Humans engage in many activities, resulting in a broad range of loads. For normal bone, the loads that result in fracture are typically extremes; severely osteoporotic or pathologic bone may fracture during normal activities of daily living. In addition, the mechanical properties of bone vary over a wide range, and several pathologic processes can alter bone properties. Therefore, our first objective is to review the mechanical properties of bone, the changes in mechanical properties that accompany aging and certain disease processes, and the fracture risk for normal and diseased bone. Bone tissue has a unique ability for repair, frequently restoring its original load-bearing capacity in weeks to months. However, this repair process is influenced by the mechanical environment to which the healing bone is subjected, and bone healing fails under adverse condi- tions. The rate at which the load-bearing capacity is restored is affected by the stability of the fracture site. The second objective of this chapter is to review the bio- mechanics of fracture healing and the influence of the mechanical environment on the biology of fracture healing. Successful fracture treatment requires control of both the biologic and the mechanical aspects of fracture healing. Different approaches to fracture treatment control the mechanical environment in different ways and can influ- ence the rate at which load-bearing capacity is restored. The third objective of this chapter, therefore, is to review the biomechanics of fracture treatment, particularly in relation to the stability these approaches provide to healing fractures. Quantitative measurements that can help deter- mine the optimal fracture treatment would be of great clinical benefit. These measurements may help to promote a fracture-healing process that provides the most rapid restoration of load-bearing capacity. Quantitative measure- ments are being developed that may help determine the stability of a fracture and also the optimal timing for removal of fixation. The optimal treatment plan could be objectively selected by combining these measurements with known mechanical properties of a variety of fracture treatment approaches. The final objective is to review progress toward developing objective clinical tools for selecting and monitoring fracture treatment. BONE PROPERTIES AND FRACTURE RISK zzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzzz From a mechanical viewpoint, bone can be examined at two levels. At the first level, bone can be viewed as a material with mechanical properties that can be measured in the laboratory. These properties include the amount of deformation that occurs under load, the mechanism and rate at which damage accumulates in the bone, and the maximal loads that the material can tolerate before 90
Transcript of ch04

C H A P T E Rz z z z z z z z z z z z z z z z z z z z z z z z z z z4
Biomechanics of FracturesBiomechanics of Fractures
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
John A. Hipp, Ph.D.Wilson C. Hayes, Ph.D.
Bone is a remarkable material with complex mechanicalproperties and a unique ability for self-repair, making it afascinating structural material from both a clinical and anengineering perspective. Bone fails when overloaded,initiating a complex series of biologic and biomechanicalevents directed toward repair and restoration of function.Tremendous progress is being made in understanding,controlling, and enhancing the biologic aspects of fracturehealing. The mechanical environment is always a crucialelement of fracture healing, with strong interactionsbetween biologic and mechanical factors. Clinical manage-ment of fractures must influence both the biologic and themechanical conditions so that the original load-bearingcapacity of the bone is restored as quickly as possible.There are thus three principal aspects of the biomechanicsof fractures and their treatment: (1) biomechanical fac-tors that determine when and how a bone fractures,(2) biomechanical factors that influence fracture healing,and (3) control of the biomechanical environment byfracture treatments.
The biomechanical factors that determine whether abone fractures include the loads applied and the mechan-ical properties of bone and soft tissue. Humans engage inmany activities, resulting in a broad range of loads. Fornormal bone, the loads that result in fracture are typicallyextremes; severely osteoporotic or pathologic bone mayfracture during normal activities of daily living. Inaddition, the mechanical properties of bone vary over awide range, and several pathologic processes can alterbone properties. Therefore, our first objective is to reviewthe mechanical properties of bone, the changes inmechanical properties that accompany aging and certaindisease processes, and the fracture risk for normal anddiseased bone.
Bone tissue has a unique ability for repair, frequentlyrestoring its original load-bearing capacity in weeks tomonths. However, this repair process is influenced by themechanical environment to which the healing bone issubjected, and bone healing fails under adverse condi-tions. The rate at which the load-bearing capacity is
restored is affected by the stability of the fracture site. Thesecond objective of this chapter is to review the bio-mechanics of fracture healing and the influence ofthe mechanical environment on the biology of fracturehealing.
Successful fracture treatment requires control of boththe biologic and the mechanical aspects of fracture healing.Different approaches to fracture treatment control themechanical environment in different ways and can influ-ence the rate at which load-bearing capacity is restored.The third objective of this chapter, therefore, is to reviewthe biomechanics of fracture treatment, particularly inrelation to the stability these approaches provide to healingfractures. Quantitative measurements that can help deter-mine the optimal fracture treatment would be of greatclinical benefit. These measurements may help to promotea fracture-healing process that provides the most rapidrestoration of load-bearing capacity. Quantitative measure-ments are being developed that may help determine thestability of a fracture and also the optimal timing forremoval of fixation. The optimal treatment plan could beobjectively selected by combining these measurementswith known mechanical properties of a variety of fracturetreatment approaches. The final objective is to reviewprogress toward developing objective clinical tools forselecting and monitoring fracture treatment.
BONE PROPERTIES ANDFRACTURE RISKz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
From a mechanical viewpoint, bone can be examined attwo levels. At the first level, bone can be viewed as amaterial with mechanical properties that can be measuredin the laboratory. These properties include the amount ofdeformation that occurs under load, the mechanism andrate at which damage accumulates in the bone, and themaximal loads that the material can tolerate before
90
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 1/30 P 90 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 1/30 P 90 BLACK T

catastrophic failure. At a higher level, a bone can be viewedas a structure composed of a tissue organized into ageometry that has evolved for specific mechanical func-tions. Relevant structural properties include the amount ofdeformation that occurs during physiologic loading andthe loads that cause failure either during a single loadevent or during cyclical loading. Both the materialproperties of bone as a tissue and the structural propertiesof bone as an organ determine the fracture resistance ofbone and influence fracture healing. Thus, this sectionbegins by discussing the relevant mechanical properties ofbone as a material. This discussion is followed by a reviewof the structural properties of whole bones. The sectioncloses with a review of several important clinical applica-tions in which the biomechanics of fracture and the risk offracture have been studied.
Material Properties of Bone
CORTICAL BONE
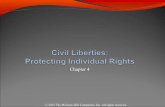
The mechanical properties of bone tissue are typicallydetermined by measuring the deformation of small,uniform specimens during application of simple, well-defined loads. Figure 4–1 illustrates a typical test thatinvolves subjecting a machined cortical bone specimen totensile loads. Dumbbell-shaped tensile specimens aretypically used, so that failure occurs in a reproduciblelocation. Two parameters are monitored during the tensiletest: the applied force and the displacement between twopoints along the long axis of the specimen. The resultingforce-displacement curve provides an indication of thestiffness and failure load of the bone specimen, but thedata are useful only for specimens with the same geometryas the one tested. To provide material property data thatcan be applied to any specimen geometry, the force anddisplacement data are converted to stress and strain. Thisconversion is a normalization process that eliminates the
influence of specimen geometry. The stress in the bonespecimen is calculated as the applied force divided bythe cross-sectional area, and the strain is measured as thepercentage change in length of a defined length of thespecimen.
A typical stress-strain curve for a tensile test of corticalbone is shown in Figure 4–2. The elastic modulus of bonetissue or structural materials such as stainless steel,titanium, or polymethyl methacrylate is determined fromthe slope of the initial, linear part of the curve. The pointat which the slope of the stress-strain curve decreases is theyield point of the bone, and the maximal recorded stress isthe ultimate strength of the tissue. After the bone hasyielded, the slope of the stress-strain curve drops to a newvalue termed the anelastic modulus.120 The area under thestress-strain curve reflects the capacity of bone to absorbenergy. The capacity to absorb energy increases with yieldstrength, but the greatest energy absorption is typicallyseen for bones with high ultimate strains, where substan-tial energy is absorbed during postyield deformation.Studies of bone under controlled loading conditionsprovide data to document the properties of cortical bone intension, compression, torsion, and bending.58
Bone is loaded cyclically during many activities of dailyliving, and the load required to cause bone to fail isdramatically lower if that load is applied repeatedly.The number of cycles of stress that bone can toleratedecreases as the stress level increases. This propertyof bone is measured using curves of the stress versusnumber of cycles to failure. These curves depend on thetype of loading (axial, bending, or torsion), the loadingrate, and the physical composition of the bone. Theinternal mechanisms in bone that determine its behaviorunder cyclical loading are beginning to be under-stood.21, 22, 56, 75, 76, 110, 127
Several factors influence the material properties ofcortical bone. For instance, the properties are dependenton the rate at which the bone tissue is loaded. Materialssuch as bone whose stress-strain characteristics aredependent on the applied strain rate are termed viscoelasticor time-dependent materials. However, the strain ratedependence of bone is relatively modest, with the elasticmodulus and ultimate strength of bone approximately
P
P
L1 L2A � Area
� � Strain �
� � Stress �
E � Elastic modulus
A � E � Axial rigidity
PA
L2 � L1
L1
FIGURE 4–1. Simple uniaxial tensile test with a dumbbell-shapedspecimen. P is the applied load and (L2 − L1)/L1 is the strain between twopoints along the specimen’s axis.
a
b
400
300
200
100
00.000 0.002 0.004 0.006 0.008 0.010
ST
RE
SS
(M
Pa)
Elastic modulus � Slope of line a
Anelastic modulus � Slope of line b
STRAIN
FIGURE 4–2. Typical stress-strain curve for human cortical bone showingthe curve regions where the elastic and anelastic moduli are calculated.
91CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 2/30 P 91 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 2/30 P 91 BLACK T

proportional to the strain rate raised to the 0.06 power20
(Figs. 4–3 and 4–4). Over a wide range of strain rates, theultimate compressive strength increases by a factor of 3,and the modulus increases by about a factor of 2.158
The stress-strain behavior of cortical bone is alsostrongly dependent on the orientation of bone microstruc-ture with respect to the loading direction.146 Severalinvestigators have shown that cortical bone is both
stronger and stiffer in the longitudinal direction (thepredominant orientation of osteons) than in the transversedirection. Materials such as bone whose mechanicalproperties depend on the loading direction are said to beanisotropic. The anisotropy and viscoelasticity of bonedistinguish it as a complex material, and both the strainrate and the loading direction must be specified whendescribing the material properties of bone tissue. Table 4–1
10�1
100
101
102
0 1
0.06 2
p
APPARENT DENSITY (g/cm2)
CO
MP
RE
SS
IVE
ST
RE
NG
TH
(m
n/m
2 )
S � 68 �
Strain rate � � 0.01 sec�1
Humantrabecular
Bovinetrabecular
Humantrabecular
Humancortical
Bovinecortical
FIGURE 4–3. Compressive strength as a func-tion of apparent density for human and bovinetrabecular and cortical bone. (Data from Car-ter, D.R.; Hayes, W.C. Science 194:1174–1176,1976.)
101
102
103
104
105
0.1 1
0.06 3
p
APPARENT DENSITY (g/cm2)
CO
MP
RE
SS
IVE
MO
DU
LUS
(m
n/m
2 )
E � 3790 �
Strain rate � � 0.01 sec�1
Humantrabecular
Bovinetrabecular
Humancortical
Bovinecortical
FIGURE 4–4. Compressive modulus as a func-tion of apparent density for human and bovinetrabecular and cortical bone. (Data from Car-ter, D.R.; Hayes, W.C. J Bone Joint Surg Am59:954–962, 1977.)
92 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 3/30 P 92 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 3/30 P 92 BLACK T

provides representative anisotropic material properties forhuman cortical bone, and ultimate strengths of corticalbone from adult femurs for longitudinal and transverseloads are summarized in Table 4–2.
TRABECULAR BONE
The major physical difference between trabecular boneand cortical bone is the increased porosity exhibited bytrabecular bone. This porosity is reflected by measure-ments of the apparent density (i.e., the mass of bone tissuedivided by the bulk volume of the test specimen, includingmineralized bone and marrow spaces). In the humanskeleton, the apparent density of trabecular bone rangesfrom approximately 0.1 to 1.0 g/cm3, whereas theapparent density of cortical bone is about 1.8 g/cm3. Atrabecular bone specimen with an apparent density of0.2 g/cm3 has a porosity of about 90%.
The compressive stress-strain properties of trabecularbone are markedly different from those of cortical boneand are similar to the compressive behavior of manyporous engineering materials that absorb energy onimpact.51, 145 Stress-strain curves (Fig. 4–5) for trabecularbone in compression exhibit an initial elastic regionfollowed by yield. The slope of the initial elastic regionranges from one to two orders of magnitude less than thatof cortical bone. Yield is followed by a long plateau regioncreated as more trabeculae fracture. The fractured trabec-
ulae begin to fill the marrow spaces at approximately 50%strain. Further loading of the specimen after the pores arefilled is associated with a marked increase in specimenmodulus.
Both the compressive strength and the compressivemodulus of trabecular bone are markedly influenced bythe apparent density of the tissue (see Figs. 4–3 and 4–4).Like cortical bone, trabecular bone is also anisotropic(material properties depend on the direction of loading).The regressions presented in Figures 4–3 and 4–4 includecortical bone with an apparent density of approximately1.8 g/cm3 as well as trabecular bone specimens fromseveral species representing a wide range of apparentdensities. These relationships suggest that the compressivestrength of all bone tissue in the skeleton is approximatelyproportional to the square of the apparent density.23 Theelastic modulus of trabecular bone tissue is approximatelyproportional to the cube of apparent density.20 Theexperimentally observed relationships are consistent withthe porous foam analogy for trabecular bone.51 Althoughthese relationships were initially derived from compressiontests, tensile tests of trabecular bone suggest that its tensilemodulus and tensile strength are slightly less than itscompressive strength.75 One interesting observation is thateven though the stiffness and strength of trabecular bonedepend on bone density and the direction of loading, for arange of bone densities, trabecular bone appears to fail atjust under 1% strain no matter what the direction ofloading.25
These relationships between mechanical properties andthe apparent density of bone tissue are important. First,they suggest that bone tissue can generate large changes inmodulus and strength through small changes in bonedensity. Conversely, subtle changes in bone density resultin large differences in strength and modulus. Thisconsideration is important when we note that bonedensity changes are usually not radiographically evidentuntil bone density has been reduced by 30% to 50%. Thepower law relationships of Figures 4–3 and 4–4 indicatethat such reductions in bone density result in nearly anorder of magnitude reduction in bone stiffness andstrength.
TABLE 4–2z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Ultimate Strength Values for Human Femoral Cortical Bone
Loading Mode Ultimate Strength (MPa)*
LongitudinalTension 135 (15.6)Compression 205 (17.3)Shear 71 (2.6)TransverseTension 53 (10.7)Compression 131 (20.7)
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z*Standard deviations in parentheses.Source: Data from Journal of Biomechanics, Volume number 8, Reilly,
D.T.; Burstein, A.H. The elastic and ultimate properties of compact bonetissue, pp. 393–405, Copyright 1975, with kind permission from ElsevierScience Ltd, The Boulevard, Langford Lane, Kidlington 0X5 1GB, UK.
TABLE 4–1z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Anisotropic Material Properties for Human Cortical Bone*
Loading Direction Modulus (GPa)
Longitudinal 17.0Transverse 11.5Shear 3.3
z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z*In comparison, moduli for common isotropic materials used in
orthopaedic implants are stainless steel, 207 GPa; titanium alloys, 127 GPa;bone cement, 2.8 GPa; ultrahigh-molecular-weight polyethylene, 1.4 GPa.
Source: Data from Journal of Biomechanics, Volume number 8, Reilly,D.T.; Burstein, A.H. The elastic and ultimate properties of compact bonetissue, pp. 393–405, Copyright 1975, with kind permission from ElsevierScience Ltd, The Boulevard, Langford Lane, Kidlington 0X5 1GB, UK.
0
40
80
120
160
200
0.00 0.05 0.10 0.15 0.20 0.25
STRAIN
ST
RE
SS
(M
Pa)
p � 0.3 g/cm3
p � 0.9 g/cm3
Trabecular bone
Cortical bone
Density p � 1.85 g/cm3
FIGURE 4–5. Compressive stress-strain curves for cortical and trabecularbone of different densities.
93CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 4/30 P 93 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 4/30 P 93 BLACK T

Structural Properties of Whole Bones
When the skeleton is exposed to trauma, some regions aresubjected to extreme loads. Fracture occurs when the localstresses or strains exceed the ultimate strength or strain ofbone in that region. Bone fracture can therefore be viewedas an event that is initiated at the material level and thenaffects the load-bearing capacity of bone at the structurallevel. The major difference between behavior at thematerial level and that at the structural level is related toinclusion of geometric features at the structural level andtheir exclusion at the material level. Thus, the structuralbehavior includes the effects of both bone geometry andmaterial properties, whereas material behavior occurswithout the effects of complex bone geometries. Anyattempt to predict the structural behavior of a skeletalregion must therefore reflect both the material propertiesof different types of bone in that region and the geometricarrangement of the bone.
Several aspects of bone cross-sectional geometry, suchas cross-sectional area and moment of inertia, are impor-tant in the structural properties. The cross-sectional area isstraightforward. When subjected to axial loads andassuming similar bone material properties, a large, thick-walled bone is more resistant to fracture simply becausethe internal forces are distributed over a larger surface area,resulting in lower stresses. The moment of inertiaexpresses the shape of the cross section and the particulardistribution of tissue or material with respect to appliedbending loads. The moment of inertia must be expressedin relation to a particular axis because bending can occurin many different planes. Equations for calculating themoment of inertia of several regular geometric crosssections are shown in Figure 4–6.123 From these equa-tions, it is apparent that the moment of inertia is highlysensitive to the distribution of area with respect to an axis.Material that is at a greater distance from the axis is more
efficient at resisting bending with respect to that axis. Asimple example of this principle is that a yardstick turnedon an edge is more resistant to bending than one turnedhorizontally. An I-beam is a particularly efficient cross-sectional shape for resisting bending in one directionbecause most of its area is distributed at a great distancefrom the bending axis.
If bones were subjected to bending in only onedirection, their cross-sectional area would probably haveevolved to something like an I-beam. Instead, long bonesare loaded by axial loads, bending in several planes, andtorsion. Under these conditions, a semitubular structureis most efficient. Diaphyseal bone cross-sectional geome-tries are roughly tubular in some regions but are veryirregular elsewhere. The moment of inertia for an irregularbone cross section can be determined from traces of theperiosteal and endosteal surfaces, using simple numericaltechniques.103 The moment of inertia partially deter-mines the risk of fracture. For example, small cross-sectional areas and moments of inertia of the femoral andtibial diaphysis predispose military trainees to stressfractures.12
Although bones are typically subjected to a variety ofcomplex loads, it is instructive to evaluate the strength ofa bone or fracture treatment method for simple, well-defined loads. Three types of loading are typicallyconsidered in laboratory experiments: axial loading, bend-ing, and torsion. For each load case, the behavior of thestructure is described by a rigidity term that is acombination of both material stiffness (represented by amodulus) and a geometric factor (area or moment ofinertia). Structures with high rigidity deform little under aload. For axial loads, the important parameters that governthe mechanical behavior of a structure are the cross-sectional area and the modulus of elasticity (see Fig. 4–1).The product of area and modulus is the axial rigidity. Forbending, the applied loads are expressed as a moment withdimensions of force times a distance. The importantstructural parameters in a bending test are the moment ofinertia and the elastic modulus (Fig. 4–7), and theirproduct is the bending (or flexural) rigidity. Torsional loadsare also expressed as a force times a distance. Thecross-sectional distribution of bone and the shear modulusof bone determine the torsional properties (Fig. 4–8).
Just as the moment of inertia describes the distributionof material about the bending axis for a cylindrical bone,the polar moment of inertia describes the distribution ofmaterial about the long axis of the structure being tested.The product of shear modulus and polar moment of inertiagives the torsional rigidity. For noncircular cross sectionsand for structures with cross sections that vary along thelength, a simple polar moment of inertia is not applicable.For these structures, various formulas and simple analyt-ical models can be used to calculate the structuralproperties under torsional loads.85, 123 The rigiditiesalready discussed describe how much a bone may deformunder a load. Alone, a quantitative estimate of rigidity maybe of limited use to a clinician who wants to know whethera bone would break when subjected to physiologicloading. Fortunately, there is evidence that a strongrelationship exists between bone stiffness and bonestrength.49
FIGURE 4–6. Some simple geometric cross sections and the correspondingformulas for calculating the moments of inertia with respect to the x-axis.
94 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 5/30 P 94 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 5/30 P 94 BLACK T

The various loading modes that occur in whole bonescan result in characteristic fracture patterns (Fig. 4–9).When loaded in tension, diaphyseal bone normallyfractures owing to tensile stresses along a plane that isapproximately perpendicular to the direction of loading.When loaded in compression, a bone typically fails alongplanes that are oblique to the bone’s long axis. Withcompressive loads, high shear stresses develop alongoblique planes that are oriented at about 45 degrees fromthe long axis. These maximal shear stresses are approxi-mately one half the applied compressive stress. However,because the shear strength of cortical bone is much lessthan the compressive strength (see Table 4–2), fractureoccurs along the oblique plane of maximal shear. Thus,compressive failures of bone occur along planes ofmaximal shear stress, and tensile fractures occur alongplanes of maximal tensile stress.
When a bone is subjected to bending, high tensilestresses develop on the convex side, whereas high
compressive stresses develop on the concave side. Theresulting fracture pattern is consistent with that observedduring axial compressive and tensile loading of wholebones. A transverse fracture surface occurs on the tensileside, whereas an oblique fracture surface is found on thecompressive side. Two fracture surfaces commonly occuron the compressive side, creating a loose wedge of bonethat is sometimes referred to as a butterfly fragment. Thefracture pattern is more complex when a bone is subjectedto torsion. Fractures usually begin at a small defect at thebone surface, and then the crack follows a spiral patternthrough the bone along planes of high tensile stress. Thefinal fracture surface appears as an oblique spiral thatcharacterizes it as a torsion fracture.
The fracture patterns discussed for idealized loadingconditions are consistent with some fractures seen clini-cally. With many traumatic loading conditions, however,bone is subject to a combination of axial, bending, andtorsional loading, and the resulting fracture patterns canbe complex combinations of the patterns previouslydescribed. In addition, high loading rates often result inadditional comminution of the fracture caused by thebranching and propagation of numerous fracture planes.Bone may tolerate higher loads if the loads are appliedrapidly,36 although the ability of bone to absorb energymay not change with loading rate. In addition, fracturescan be caused by a single load that is greater than theload-bearing capacity of the bone; these loads are com-monly called the ultimate failure load. Repeated applicationof loads smaller than the ultimate failure load can fatiguethe bone and eventually lead to failure. Fatigue failures ofbone are common in military training and in athletes. Fewdata exist about the loads that cause fatigue fractures.Fatigue fractures are believed to be associated with damageaccumulation within the bone. It is difficult to measure theactual fatigue properties of bone because repair of theaccumulated damage in the bone occurs in vivo but cannotbe reproduced in ex vivo experiments.
Engineering tools that were originally developed tostudy more traditional engineering problems provide newinsights into the structural mechanics of bone, skeletal
FIGURE 4–8. Simple torsion test of a cylinder. The angular deformation isindicated along with relevant formulas.
FIGURE 4–7. Representation of a four-point bending test of a beam. Theoriginal shape is shown by the dashedline, and the deformed shape is indicatedby the solid lines (deformations are exag-gerated).
95CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 6/30 P 95 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 6/30 P 95 BLACK T

fractures, and fracture treatments. Valuable insight into thebiomechanics of fractures can be obtained using simpleanalytical models that can be solved on paper with thehelp of a calculator.85, 142 However, the most commonlyapplied engineering tool is the finite element method.
The finite element method is a powerful engineeringmodeling tool that is routinely used to investigate complexstructures subject to varied loads and supports. Themethod involves forming a mathematical model of thebone from small elements of simple geometry (such asrectangles or tetrahedrons). Figure 4–10 shows represen-tative views of a finite element mesh used to model theproximal femur. The material properties of each elementare specified along with the applied loads and supportconditions. The model is then analyzed by a computer topredict the deformations and stresses within the struc-ture.88 Thus, the behavior of bone at both the material and
structural levels can be investigated using the finiteelement method. The finite element method allowsparametric investigation of material properties, geometry,and loading conditions and has been applied in manyorthopaedic biomechanical analyses.69 Several applica-tions of the finite element method in orthopaedic biome-chanics are discussed in this chapter. In particular, thefinite element method is being developed for understand-ing and predicting fracture risk and can provide betterinformation about bone strength than conventional bonedensity measurements.34
Age-Related and Pathologic BoneProperty Changes
With increasing age, the mechanical properties of bonetissue slowly degrade, and geometric changes provideadditional alterations in the structural characteristics ofbones. Age-related changes occur in both cortical andtrabecular bone, and changes in both regions can result inincreased fracture risk. Changes in bone mineral mass,density, mechanical properties, and histology associatedwith aging have been the subject of intensive investigation.The picture to emerge from this research is a progressivenet loss of bone mass with aging, beginning in the fifthdecade of life and proceeding more rapidly in women.122
Concurrent with this general loss of bone mass, bonetissue becomes more brittle and less able to absorb energy.The major clinical consequence of these skeletal changes isan age-related increase in fracture incidence.
At the tissue level, several age-related changes in thematerial properties of femoral cortical bone have beendemonstrated.19 A small decrease in elastic modulus
FIGURE 4–10. Different views of a finite element mesh of a proximalfemur. (From Lotz, J.C. Ph.D. dissertation, Massachusetts Institute ofTechnology, 1988.)
LOADING MODE
FRACTURE TYPE
Tension Compression Bending Torsion
Transverse Oblique Butterfly Spiral
FIGURE 4–9. Characteristic fracturestypically found for bones loaded tofailure with ‘‘pure’’ loading modes.
96 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 7/30 P 96 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 7/30 P 96 BLACK T

occurs with age (1.5% per decade), but the mostsignificant change occurs in the amount of strain that thebone tolerates before fracture. With aging, the ultimatestrain decreases by between 5% and 7% per decade. Theenergy required to fracture a bone is reflected in the areaunder the stress-strain curve. Because the elastic modulusdoes not change appreciably, the energy required forfailure is predominantly reduced by age-related decreasesin ultimate strain. Thus, with aging, the bone behavesmore like a brittle material, and the capacity of bone toabsorb the energy of a traumatic event decreases.
Studies of skeletal aging often do not consider theoverall geometry and distribution of bone tissue. Changeswith age in cross-sectional cortical geometry of the lowerlimb bones were studied at 11 locations along the length of103 femoral and 99 tibial cadaveric specimens. Resultsindicate that although both men and women undergoendosteal bone resorption and medullary expansion withaging, only men exhibit concurrent subperiosteal boneapposition and expansion. Consequently, men show littlechange in cortical area and some increase in secondmoments of inertia with age. Conversely, both the corticalarea and the second moments of inertia decrease with agein women. Thus, only men appear to remodel bone in away that compensates for loss of bone material strengthwith aging.11, 124
In a study of archaeologic bone specimens fromindividuals with high activity levels, both men and womenexhibited subperiosteal expansion and increases in secondmoments of area with aging.125 Together with observeddifferences in fracture incidence among living populations,these findings suggest that the relatively low activity levelsof modern civilization may not stimulate optimal boneremodeling throughout life and thus may contribute tohigher fracture risk in aged people. Reductions in thecross-sectional area of the tibia have also been observed inpatients after spinal cord injuries.39
The preceding discussion examined age-related changesin cortical bone. Trabecular bone plays an importantstructural role in many bones, and the age-related changesin trabecular bone contribute to the increased fracture riskin elderly people. Quantitative studies of trabecular bonemorphology in vertebral bodies demonstrated that thethickness of trabeculae decreases while the spacingbetween trabeculae increases.14, 133 These age-related mor-phologic changes significantly reduce the strength of thevertebral bodies, contributing to the observed increasedvertebral fracture incidence in elderly people.63, 72
Fracture Risk
A bone fails when the applied loads exceed the load-bearing capacity; hence, both the applied loads and theload-bearing capacity must be known to calculate fracturerisk. Most structures, such as a bridge or a building, aredesigned to withstand loads several times greater thanexpected. Similarly, the normal human skeleton cansupport loads much higher than expected during activitiesof daily living. The ratio of load-bearing capacity toload-bearing requirement is frequently termed the safety
factor. The inverse of this ratio has been termed the factorof risk for fracture.
For loads approximating the midstance phase of gait,the average load-bearing capacity of mature and osteopo-rotic human femurs ranges from 2000 to 10,000 N (472 to2250 pounds).45 Peak loads at the hip joint during themidstance phase of gait have been recorded as three to fivetimes body weight.13 Therefore, a 600-N (140-pound)individual who applies four times body weight to thefemur during walking has a femoral load-bearing capacitythat ranges from less than one to more than four times asstrong as needed, depending on the properties of thatindividual’s femur. For the tibia, axial loads while walkingare estimated to be two to four times body weight,101 andthe greatest bending moment applied during restrictedweight bearing is estimated to be about 79 Nm in men.84
Intact human tibias loaded in three-point bending failed at57.9 to 294 Nm, so the bending strength of the tibia is alsoone to four times the maximal applied bending loads. Themaximal torque that the tibia can tolerate was estimated tobe about 29 Nm. Under torsional loads, tibias failed at27.5 to 89.2 Nm, which is one to three times the maximalapplied torque. These calculations are valid only forparticular types of loading. Nevertheless, these estimatedfactors of risk may help determine when a healingfemoral fracture can tolerate moderate weight bearing orwhen a femur with a bone defect requires prophylacticstabilization.
There are several groups in whom fractures areprevalent and for whom prevention may be possible iffracture mechanisms and the patients at greatest risk canbe identified. One group is the growing elderly population,in which age-related fractures are prevalent. Another groupis cancer patients with metastatic bone disease, in whichprophylactic stabilization of impending fractures mayincrease patients’ quality of life. The next few sectionsdiscuss the fracture risk and methods for predictingfracture risk related to aging and metastatic bone lesions.
FRACTURE RISK WITH OSTEOPOROSIS
The epidemiology of age-related fractures suggests arelation between osteoporosis and increased fracturerisk63; consequently, risk factors associated with hip frac-tures have been the subject of much research. The effectsof age and gender have been documented, but these factorsare confounded by an increased propensity for trauma inthe elderly population.63 Fractures related to osteoporosisare commonly associated with falls, and the frequency offalls increases with age. In addition, falls are more commonin elderly women than in men, and fracture rates are alsogreater in women than in men.6, 54 Common sites forfall-related fractures are the proximal femur and distalforearm. Vertebral fractures are also frequently associatedwith traumatic loading such as occurs in backward falls,although relatively nontraumatic vertebral fractures maybe much more common than nontraumatic femoralfractures.
When age- and sex-specific incidence rates are com-pared for all major fractures of different skeletal regions,considerable variability is observed. This variability may bedue in part to varying proportions of cortical and
97CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 8/30 P 97 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 8/30 P 97 BLACK T

trabecular bone at different sites and to the difference inpattern of bone loss of these two types.94 Differences infracture risk may also be attributed to variations in overallbone geometry. For instance, the relatively short neck andsmaller femoral neck angle in Japanese women mayexplain their lower incidence of hip fracture comparedwith that in American women.104 The type and directionof loads during a fall (Fig. 4–11) are very different fromthose of loads during activities of daily living. Because thefemur is adapted to support activities of daily living, it maybe particularly sensitive to the abnormal loads during afall. These factors emphasize both the complex interac-tions that occur between age-related bone loss and skeletaltrauma and the need for improved understanding of thebiomechanics of fracture risk in specific skeletal sites.Reduced skeletal resistance to trauma and the increasedpropensity for falling are cofactors in determining hipfracture risk.54, 97 These considerations lead to the conclu-sion that both bone loss and trauma are necessary, but notindependently sufficient, causes of age-related hip frac-tures.
Fractures of the proximal femur are a significant publichealth problem and a major cause of mortality andmorbidity among elderly people,16, 111, 151 and attempts toreduce the incidence of age-related hip fractures haveprimarily focused on preventing or inhibiting excessivebone loss associated with osteoporosis. As a result, manynoninvasive measures of bone density have been devel-oped in the hope of identifying individuals with the
greatest fracture risk. Ex vivo studies have shown that theload-bearing capacity of the proximal femur can bepredicted from measurements of bone density and femoralgeometry.2, 90 An excellent correlation was found betweenthe ultimate failure load and quantitative computedtomographic (CT) measurements made at intertrochan-teric sites90 (Fig. 4–12). The best correlation was found forthe product of the average trabecular CT number and thetotal bone cross-sectional area. The use of this parametercould result in improved assessment of the degree ofosteoporosis and the associated risk of hip fracture.
Lotz and co-workers89 analytically studied the proximalfemur subjected to various load configurations, includingone-legged stance and fall. The finite element models (seeFig. 4–10) suggest that the joint load is transferred fromthe femoral head to the cortex of the calcar region throughthe primary compressive group of trabeculae during gait.These results contradict the current belief that loads aredistributed in proportion to the bone volume fractions.Instead, there is a shift in the distribution of load frommainly trabecular bone near the femoral head to corticalbone at the base of the femoral neck. This result, alongwith the observation that fractures of the proximal femurusually occur in the subcapital region,6 supports thehypothesis that fractures in osteoporotic bone result fromreduced strength of trabecular bone.98, 122
FRACTURE RISK WITH METASTATIC ANDBENIGN DEFECTS IN BONE
Metastatic lesions frequently occur in the axial andappendicular skeleton of patients with breast cancer,prostate cancer, and other cancers. Benign bone tumorsoccur in 33% to 50% of asymptomatic children evaluatedby random radiographs of long bones.129 These lesionscan represent a significant fracture risk. As reviewed by
FIGURE 4–11. Contact loads at the femoral head and greater trochanterrepresenting a fall to the side. (From Lotz, J.C. Ph.D. dissertation,Massachusetts Institute of Technology, 1988.)
Intertrochantericscan
Transcervicalscans
1 1
35
7
24
68
FIGURE 4–12. Quantitative computed tomography (QCT) scan locationsused to compare QCT data with in vitro failure strengths of proximalfemurs. (From Lotz, J.C. Ph.D. dissertation, Massachusetts Institute ofTechnology, 1988.)
98 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 9/30 P 98 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 9/30 P 98 BLACK T

Oda and Schurman,105 9% to 29% of skeletal metastasesseen by orthopaedic surgeons result in pathologic frac-tures. Prophylactic fixation of an impending fracture hasseveral advantages over treating a pathologic fracture,including relief of pain, decreased hospital stay, reducedoperative difficulty, reduced risk of nonunion, and reducedmorbidity. On the other hand, operations that do notreduce overall morbidity must be avoided. Clinicians arethus faced with the task of determining whether a defectrequires prophylactic stabilization.
Current clinical guidelines can provide contradictoryindications for prophylactic stabilization. Beals and col-leagues7 concluded that defects that have a dimensiongreater than 2.5 cm and that cause pain should bestabilized. Fidler47 suggested that defects that compromisemore than 50% of the cortex should be stabilized.However, many aspects of metastatic defect geometry andmaterial properties determine the structural consequencesof the lesion. In common sites of osseous metastases suchas the proximal femur, even experienced orthopaediconcologists cannot predict the strength reduction relatedto the defect from radiographs or from qualitativeobservation of CT examinations.67
Several ex vivo experiments have been reported thatspecifically addressed the structural consequences ofmetastatic defects in long bones:
1. McBroom and associates95 considered the structuralconsequences of transcortical holes in long bonessubjected to bending loads. They drilled holes ofvarious sizes through one cortex of canine femurs.Defect size was expressed as the hole diameter dividedby the bone diameter. The bones were tested to failureusing a four-point bending test.
2. Hipp and co-workers66 created endosteal defects incanine femurs that did not penetrate through the
cortical wall. The size of the endosteal defect wasexpressed as the average thickness of the cortical wall inthe area of the defect divided by the thickness of theintact cortical wall. The femurs were tested to failureusing a four-point bending test.
3. In another study, Hipp and colleagues65 createdtranscortical defects in sheep femora and tested thebones to failure using a torsion test.
For each of these ex vivo tests, finite element modelswere developed to complement the experimental data andto investigate parameters that can influence the structuralconsequences of metastatic lesions in bone. In all experi-ments, agreement was found between the finite ele-ment model predictions and the actual measurements ofstrength reductions related to the defects.
Existing guidelines for determining when to stabilizeprophylactically long bones with metastatic lesions canplace a bone at significant risk of fracture. On the basis ofour data, the strength of bones with simulated endostealmetastatic defects is proportional to defect size (Fig. 4–13)but is highly dependent on the type of loading. Forexample, a 65% reduction in bending strength wasdetermined for transcortical lesions destroying 50% of thecortex, whereas the same lesion was found to reducetorsional load-bearing capacity by 85%.
The finite element models show that the materialproperties of bone along the border of a defect cansignificantly increase the structural consequences of ametastatic defect. Many metastatic lesions are associatedwith bone resorption along the border of the lesion thatextends beyond the radiographically evident lysis. Thus,for osteolytic metastatic lesions, the structural conse-quences may be significantly greater than predicted fromplain radiographs. The finite element models also demon-strated that for endosteal defects, a critical geometric
0
20
40
60
80
100
0.0 0.2 0.4 0.6 0.8 1.0
REMAINING CORTICAL WALL
% IN
TA
CT
ST
RE
NG
TH
S � 99.6 � RCW � 2.0
Experimentaldata
Linear FEM
FIGURE 4–13. Percentage of intact bonebending strength (S) as a functionof endosteal defect size. Endosteal de-fect size is expressed as the ratio ofreduced wall thickness to intact corticalwall thickness. Both experimental andanalytical results are shown. FEM, fi-nite element model; RCW, remainingcortical wall. (Data from Hipp, J.A.;McBroom, R.J.; Cheal, E.J.; Hayes, W.C.J Orthop Res 7:828–837, 1989.)
99CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 10/30 P 99 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 10/30 P 99 BLACK T

parameter is the minimal cortical wall thickness. Forexample, a bone with an asymmetric defect that compro-mises 80% of the cortical wall at one point but only 20%of the wall on the opposite side is only 2% stronger intorsion than a bone with a defect that compromises 80% ofthe cortical wall around the entire circumference.
Even biplanar radiographs fail to detect critical geomet-ric parameters if the critical defect geometry is not alignedwith respect to the radiographic planes. In a retrospectivestudy of 516 metastatic breast lesions using anteroposte-rior radiographs, Keene and associates77 could not estab-lish a geometric criterion for lesions at risk of fracture,perhaps because critical geometric parameters were missedusing plain radiographs. Results of ex vivo experimentswith simulated defects suggest that CT scans at smallconsecutive scan intervals could facilitate evaluation of thefracture risk related to metastatic lesions.
Strength reductions related to vertebral defects can bedetermined from CT data.154, 155 These CT-based mea-surements require placing a phantom under the patientduring the examination so that CT attenuation data can beconverted to bone density. Known relations between bonedensity and bone modulus are then used to convert thebone density data to modulus. For each cross sectionthrough the vertebrae, the product of area and modulus issummed over the entire cross section, excluding posteriorelements. The lowest axial rigidity of all cross sections waslinearly related to the measured failure load.155
BIOMECHANICS OF FRACTUREHEALINGz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Fracture healing can be viewed as a staged process thatgradually restores the load-bearing capacity of bone,eventually returning it to approximately its originalstiffness and strength. The mechanical environment towhich a healing fracture is exposed profoundly affects thebiology and radiographic appearance of the fracture-healing process. This section addresses in vivo studies inwhich fracture healing was examined in controlled biome-chanical environments. These in vivo animal studies showthat the biomechanical environment provided by variousfracture treatment devices can alter the biology and therate of fracture healing.
Two general biologic mechanisms have been identifiedby which bone can repair itself. Close approximation andrigid immobilization of the fracture fragments result inlocalized remodeling at the fracture site, a process termeddirect cortical reconstruction. If a small gap exists betweenfracture fragments, direct cortical reconstruction is pre-ceded by radial filling of the gap with woven bone, aprocess termed gap healing. This intermediate process isfollowed by direct cortical reconstruction. It is likely thatin most clinical situations using rigid fixation, both gaphealing and direct cortical reconstruction are at work.
The conventional, more common mechanism of frac-ture repair is secondary osseous repair or natural healing.With less rigid immobilization, such as in casts or castbraces, fracture repair is characterized by callus formation.The periosteal callus forms from the fracture site hema-
toma with formation of a collar of fibrous tissue,fibrocartilage, and hyaline cartilage around the fracturefragments. Subperiosteal new bone is formed somedistance from the fracture site and, through a processsimilar to endochondral ossification, advances toward thecentral and peripheral regions of the callus. A similar, lessprolific response occurs at the endosteal surface. Overtime, the callus is remodeled from randomly orientedwoven bone to mature cortical bone. Direct corticalreconstruction and repair by callus formation alter thetemporal changes in mechanical properties of the fracturein unique patterns.
Healing by Direct CorticalReconstruction
Fundamental differences between direct cortical recon-struction and fracture healing by callus formation can beclearly seen in histologic preparations, as reviewed inChapter 2. With direct cortical reconstruction, there islittle evidence of resorption of fracture surfaces. If a smallgap exists between bone fragments, a layer of bone formswithin the gap. Once any gap has been filled, haversianremodeling directly crosses the fracture. The vascularsupply for the osteonal remodeling units is primarilyendosteal, although some periosteal contribution is alsoevident.118 In contrast, fracture healing by callus forma-tion typically involves resorption of fracture surfaces alongwith prolific woven bone formation originating primarilyfrom the periosteal surface, although some callus alsooriginates from the endosteal surface. After the fracture hasunited through the callus, osteonal remodeling occursacross the fracture, and the periosteal callus is remodeledand resorbed to some extent.112, 115, 118
Healing by Callus Formation
Formation of callus, especially periosteal callus, offersbasic mechanical advantages for a healing fracture. Refer-ring to Figures 4–6 and 4–7, the moment of inertia (andthus the bending rigidity) for a tubular structure dependson the fourth power of the radius. If we represent thefemoral shaft as a tubular structure with a normalmedullary diameter of 1.5 cm and a normal periostealdiameter of 3 cm, Figure 4–14A shows that the moment ofinertia increases by almost 10 times if the periostealdiameter is increased to 5 cm. Figure 4–14B shows thatreduction in endosteal diameter offers substantially lessimprovement. Although bone formed in a callus may notbe as strong or stiff as normal bone, the large increase inmoment of inertia provides a biomechanical advantage forperiosteal callus formation.
Biomechanical Stages of FractureHealing
For fracture healing involving periosteal callus, thebiomechanical stages of fracture healing have been studiedin animals. White and co-workers108, 109, 149, 150 used an
100 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 11/30 P 100 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 11/30 P 100 BLACK T

externally fixed rabbit osteotomy model to correlateradiographic and histologic information with the torsionalstiffness and failure strength at several postfracture timeperiods. They identified four biomechanical stages offracture healing (Fig. 4–15). The first indication ofincreasing stiffness occurred after 21 to 24 days. At thisstage the fracture exhibits a rubbery type of behaviorcharacterized by large angular deflections for low torques;the bone fails through the fracture site at low loads. Thisstage corresponds to bridging of the fracture gap by softtissues. At approximately 27 days, a sharp increase instiffness identifies the second stage, in which failures occurthrough the fracture site at low loads. Stiffness approachesthat of intact cortical bone. The third biomechanical stageis characterized by failure occurring only partially throughthe fracture site, with a stiffness similar to that of corticalbone but below normal strength. The final stage isachieved when the site of failure is not related to the
original experimental fracture, and the stiffness andstrength are similar to those of intact bone.
In a related study, Panjabi and colleagues107 comparedradiographic evaluation of fracture healing with the failurestrength of healing osteotomies. They applied nine differ-ent radiographic measures of fracture healing (Fig. 4–16).The best radiographic measure was cortical continuity(4 in Fig. 4–16), for which the correlation coefficientbetween the radiographic measure and bone strength wasr = .8. The lowest correlation between radiographic andphysical measurements was found for callus area (r = .17).The general conclusion of this study was that even underlaboratory conditions, radiographic information is notsufficient to decide accurately the biomechanical conditionof a healing fracture. This result is important becauseradiographic diagnosis is commonly applied to assessmentof fracture healing, although few studies have objectivelytested the predictive capability of this practice. Thus, the
0.00
0.60
1.20
1.80
2.40
3.00
0 4 6 82 10
ANGULAR DISPLACEMENT (DEGREES)
TO
RQ
UE
21 days
24 days
26 days
27 days
49 days
56 days
FIGURE 4–15. Angular displacement ofhealing osteotomies in rabbit femurs asa function of applied torque. Data areshown for animals tested after severalpostfracture time periods. (Data fromWhite, A.A., III; Panjabi, M.M.; South-wick, W.O. J Bone Joint Surg Am59:188–192, 1977.)
0
10
20
30
40
3 4 5
PERIOSTEAL DIAMETER (cm)
I (cm
4)
A
3
4
5
0 1 2
ENDOSTEAL DIAMETER (cm)
I (cm
4)
BFIGURE 4–14. A and B, Increase in moment of inertia afforded by changes in periosteal and endosteal diameters resulting from fracture callus.In both panels a tubular cross section is assumed. A constant 1.5-cm endosteal diameter is assumed in A and a constant 3-cm periostealdiameter in B.
101CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 12/30 P 101 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 12/30 P 101 BLACK T

methods for in vivo biomechanical assessment of fracturehealing previously discussed have particular clinical sig-nificance.
Several other animal experiments have shown similarbiomechanical stages of fracture healing,15, 37, 44 and thetime at which each stage of fracture healing is achieved isdependent on several factors. Using a canine model, Davyand Connolly37 experimentally produced fractures inweight-bearing bones (radii) and presumed non–weight-bearing bones (ribs). Healing bones were tested usingfour-point bending tests at 2 to 12 weeks. Both weight-bearing and non–weight-bearing bones healed with forma-tion of periosteal callus. For non–weight-bearing bones,bending strength increased more rapidly than stiffness,whereas stiffness increased more rapidly than strength inweight-bearing bones. This result also shows that thestiffness of a healing fracture does not necessarily correlatewith bone strength. Davy and Connolly further demon-strated that bone and periosteal callus geometry cantheoretically account for observed changes in fractureproperties. However, radiographic criteria have not beenshown to predict the strength or stiffness of a healingfracture. Under bending loads, the failure mechanismappears to be delamination of repair tissue from the bonefragments, suggesting that the adhesive bond betweenrepair tissue and bone fragments determines the structuralproperties.15
Whereas the mechanical environment clearly influencesthe morphology of the healing process, the conflictingresults of studies that investigated the effect of fixationrigidity on fracture healing leave the question of optimalfixation rigidity unsolved. Perren and co-workers113, 116
proposed a hypothesis that helps explain how fracturehealing is controlled by the local mechanical environment.They postulated that a tissue can be formed in theinterfragmentary region of a healing fracture only if the
involved tissues can tolerate the local mechanical strain.The tissues that are formed, in turn, contribute to thefracture rigidity, making possible the next step in tissuedifferentiation. For example, formation of granulationtissue may reduce the strain to a level at which fibrocarti-lage formation is possible.
Perren and co-workers further hypothesized thatthe fracture gap is widened by resorption of the boneends until the local tissue strain falls below a certainlimiting value. Resorption of fragment ends may reducethe strain sufficiently to permit completion of a bridgingcallus. Interfragmentary strain may influence fracturehealing in several ways. Local deformations may disruptvascularization and interrupt the blood supply todeveloping osteons. Deformation of cells may alter theirpermeability to macromolecules and increase biologicactivity. Strains may also induce changes in the electri-cal signals within the healing fracture site or elicit adirect cellular response. In all likelihood, a multifacto-rial relationship exists at various stages of the healingprocess.
DiGioia and associates40 examined the interfragmentarystrain hypothesis using computer models and comparedthe model results with the preliminary experimental dataof Mansmann and colleagues.30 Their results show thatcomplex three-dimensional strain fields exist within afracture gap and that the simple longitudinal strainsconsidered by Perren and co-workers underestimate thestrains experienced by the interfragmentary tissues. Theanalytical models show that the strain in tissue is greatestat the endosteal and periosteal surfaces of the bonefragments (Fig. 4–17). These are also the areas of earlybone resorption observed in experimental animals. Themodels also demonstrate the asymmetric distribution ofstrains that occur within the tissues at the gap betweenplated fracture fragments.
FIGURE 4–16. Radiographic measureswere compared with mechanical testsof partially healed fractures to evaluatethe efficacy of radiographic evaluationof fracture healing. (Data from Panjabi,M.M.; Walter, S.D.; Karuda, M.; et al.J Orthop Res 3:212–218, 1985.)
102 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 13/30 P 102 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 13/30 P 102 BLACK T

BIOMECHANICS OF FRACTURETREATMENTz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Many techniques are currently available for treatment ofskeletal fractures, and many factors are important inchoosing the best fixation. Many of these clinical factorsare discussed in other chapters, but one factor that iscrucial to all fractures is the need for sufficient stability toachieve fracture healing. Each method of fixation impartsa specific level of stability to a fracture and thus directlyinfluences fracture-healing biology.
When a fracture treatment method is evaluated, thehealing bone and the fracture treatment device should beconsidered as a mechanical system, with both the tissueand the device contributing to biomechanical behavior.59
The biomechanical behavior of the system can thus bealtered by changes in tissue properties (e.g., resorption atfracture surfaces, osteopenia under plates), changes to thefracture treatment device (e.g., dynamization of externalfixation), or changes in the mechanical connection be-tween device and tissue (e.g., pin or bone screw loosen-ing). In addition, bones are subject to diverse loads thatcan be a combination of axial, bending, and torsionalloads. Thus, the axial, bending, and torsional stability of afracture treatment method should be considered. Thissection addresses the basic mechanical characteristics offracture treatment techniques and the effect of each deviceon fracture healing.
Internal Fixation
INTRAMEDULLARY RODS
Intramedullary rods have several advantages in fracturetreatment, including restoration of bone alignment andearly recovery of weight bearing. The good clinical resultsand low rates of nonunion2 suggest that many currentclinical applications of these devices provide a mechanical
environment that facilitates fracture repair for selectedfractures. It is therefore useful to consider the stability ofthis treatment method as an example of a successfulmechanical construct.
Intramedullary rods are intended to stabilize a fractureby acting as an internal splint, forming a compositestructure in which both the bone and the rod contribute tofracture stability. This load-sharing property of rods isfundamental to their design and should be recognizedwhen they are used for fracture treatment.137 Conse-quently, intramedullary rod design must be evaluated withregard to both the structural properties of the rod and themechanics of the rod-bone interaction. Figure 4–18illustrates factors that determine the mechanical stability ofa femoral fracture stabilized by intramedullary fixation.
Complications that may occur with intramedullary rodsinclude rod migration, permanent deformation of the rod,and fatigue fractures. Delayed union and nonunion afterintramedullary nailing are also complications resultingfrom mechanical factors. Allen and co-workers2 identifiedseveral areas of potential weakness in intramedullary rods,including excessive flexibility, inadequate ability to trans-mit torsional loads, poor fixation of the rods within themedullary canal, and increased incidence of nonunion andimplant failure when proper reaming techniques are notemployed.
Several material and structural properties of intramed-ullary rods alter their axial, bending, and torsionalrigidities. These parameters include cross-sectional geom-etry, rod length, the presence of a longitudinal slot, and theelastic modulus of the material. The cross-sectionalgeometry can greatly affect all rigidities. Rods with thesame nominal outside diameter and similar shape butmade by different manufacturers varied in bending rigidityby more than a factor of 2 (Fig. 4–19A and B) and variedin torsional rigidity by more than a factor of 3 (Fig.4–19C).138 This variation was attributed to differences incross-sectional geometry. The data also show that there isnot always a simple relationship between rod size andrigidities. The rigidity increases significantly with roddiameter because the moment of inertia is approximatelyproportional to the fourth power of the rod radius (see Fig.4–6). However, the magnitude of change varies withdifferent manufacturers, in part because the wall thickness(with hollow rods) may be different for different roddiameters. Reaming increases the rod diameter that can beused but may reduce the strength of the bone and furthercompromise blood supply.
The unsupported length of intramedullary fixation isthe distance between implant–bone contact at the proxi-mal and distal segments of bone. This distance effectivelychanges as the fracture heals. During the initial stages of
Bone quality
Unsupported length
Distal lockingmechanism
Material and structuralproperties of the rod
Proximal fixationmechanism
Implant—bone contact(reamed/unreamed)
FIGURE 4–17. Representation of the strains experienced by tissues withina uniform osteotomy when the fractured bone is subjected to bendingloads. (Data from DiGioia, A.M., III; Cheal, E.J.; Hayes, W.C. J BiomechEng 108:273–280, 1986.)
Corticalbone
Plate
High shear stresses
FIGURE 4–18. Factors important in intramedullary fracture fixation.
103CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 14/30 P 103 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 14/30 P 103 BLACK T

fracture healing, two different unsupported lengths areimportant with intramedullary rods: the unsupportedlength in bending and the unsupported length in torsion.
Figure 4–20 illustrates the significance of unsupportedlength in bending. This length is determined by the pointsof bone–implant contact on the proximal and distal sidesof the fracture and can be different, depending on thedirection of bending. For a simple, well-reamed transversefracture, this distance is small, whereas for a severelycomminuted fracture, the unsupported length can begreat, resulting in increased deformation at the fracturesite.48 For bending loads, the rod is typically loaded inapproximately four-point bending (analogous to Fig. 4–7),and the nominal interfragmentary motion is proportionalto the square of the unsupported length. Therefore, a smallincrease in unsupported length can lead to a considerablylarger increase in interfragmentary motion.
With torsional loading, the unsupported length isdetermined by the points at which sufficient mechanical
interlocking occurs between bone and implant to supporttorsional loads. Simple rod designs that do not includeproximal or distal locking mechanisms have lower resis-tance to torsion. For rod designs that employ proximal anddistal locking mechanisms, the unsupported length istypically determined by the distance between the proximaland distal locking points. Mechanical interlocking mayalso occur between rod and bone at other places within themedullary canal. Relative motion between fracture frag-ments during torsional loading is roughly proportional tothe unsupported length (calculated according to Fig. 4–8).
Many rod designs have a longitudinal slot eitherpartially or fully along their length. The slot allows thecross section to be compressed like a stiff spring wheninserted into a medullary canal. This elastic compressioncan help promote a tight fit between rod and bone.10
However, with torsional loads the slot creates an ‘‘opensection’’ geometry that is theoretically 400 times less stiffthan a closed section.123 Reduced torsional rigidity can
0.0
2.5
5.0
12 14 1513 16
NOMINAL ROD DIAMETER (mm)
TO
RS
ION
AL
MO
DU
LUS
(N
� M
2 /de
g �
10�
2 )
C
0.0
0.1
0.2
12 14 1513 16
NOMINAL ROD DIAMETER (mm)
AP
FLE
XU
RA
L R
IGID
ITY
(N
� M
2 � 1
03 )
A
0.0
0.1
0.2
12 14 1513 16
NOMINAL ROD DIAMETER (mm)
ML
FLE
XU
RA
L R
IGID
ITY
(N
� M
2 � 1
03 )
B
OEC
DePuy
Howmedica
Zimmer
Synthes
FIGURE 4–19. Anteroposterior (AP) (A) and mediolateral (ML) (B) bending rigidities and torsional rigidities (C) of slotted intramedullary rods as a functionof nominal rod diameter for five commercially available rods from different manufacturers. Rods were oriented with the slot in the AP plane. (A–C, Datafrom Tencer, A.F.; Sherman, M.C.; Johnson, K.D. J Biomech Eng 107:104–111, 1985.)
104 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 15/30 P 104 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 15/30 P 104 BLACK T

have both positive and negative value. Reduction in rodstiffness allows the rod to conform to minor discrepanciesbetween rod and medullary geometry. Reduced rigiditymay also allow twisting of the rod during insertion, easinginsertion but compromising the use of external aimingdevices used to locate the distal locking points.78 With apartially slotted rod design, stress concentrations at theend of the slot where the cross section becomes continu-ous can result in failures at this location.12 However, thereported incidence of such device failures is small. Despitethe potential for intramedullary design variations to resultin substantial differences in strength and stiffness, many ofthe design variations seen in commercially available rodshave little effect on the gross mechanical properties.68
Intramedullary rod designs that provide mechanismsfor locking the rod proximally or distally have increasedthe indications for intramedullary rod use.55 Proximal anddistal locking mechanisms affect the torsional, axial, andbending properties of a fracture fixed with an intramedul-lary rod. The use of a locking mechanism on one side ofthe fracture only (proximal or distal) can increase theforces transmitted between fracture fragments during limbloading. The use of both proximal and distal locking canprevent axial displacement of bone along the rod andprovide additional torsional rigidity. Several different typesof distal locking mechanisms are currently available,including transverse screws and wings designed to engagecortical or cancellous bone. The strength of these lockingmechanisms depends in part on the quality of supportingbone.
Zych and co-workers160 compared four types ofintramedullary rods with distal locking mechanisms de-signed to engage cortical or cancellous bone. Intramedul-lary rods were used to fix osteotomies in 100 cadaverfemurs. Bone quality was radiographically graded, and
preparations were tested to failure in torsion with aconstant axial load or were subjected to 25 cycles ofreversing rotations. The authors concluded that fixationtorque was significantly lower in osteoporotic bones. Withosteoporotic bone, the amount of loosening is greatest withlocking mechanisms that engage cancellous bone ascompared with cortical bone, whereas for normal bone,cancellous and cortical locking mechanisms providesimilar resistance to loosening.
In combination, the presence of both proximal anddistal locking mechanisms helps control the axial stabilityof a fracture. Without both locking mechanisms, the bonecan glide axially along the implant. Thus, the combinationof proximal and distal locking can maintain axial separa-tion and bone length or facilitate application of compres-sion between bone fragments. The compression is lost ifresorption occurs at the points of contact between fracturefragments.
The mechanical interaction between bone and theimplant can also influence the torsional stability of anintramedullary fixed fracture. The mechanical interlockbetween implant and bone depends on the cross-sectionalgeometry of the bone and the geometry of the medullarycanal. The geometry of the medullary canal is frequentlychanged by reaming, in which case surgical techniqueestablishes the initial fit of implant in bone. For example,eccentric reaming can compromise mechanical stabilitywith intramedullary rods.156 Several tests have demon-strated that torsional resistance is a primary shortcomingof some intramedullary rods, with intramedullary rod–fixed femurs achieving only 13% to 16% of the torsionalstrength of intact femurs.
To improve torsional properties, designs incorporatingflutes and ribs to increase contact between rod and bone intorsion and designs that use screws or wings to engagecortical or cancellous bone have been developed. Forexample, Allen and associates2 showed that a flutedintramedullary rod can support 30% to 50% greater torquewithin the medullary canal than simpler cross sections.The use of proximal and distal locking mechanisms alsoaffects the torsional rigidity. Rotation of bone fragments atthe fracture site increases significantly as the lockingscrews are moved farther away from the fracture, consis-tent with the concept of decreased stability as the workinglength increases.50 Surgeons must also recognize that theentry portals used to insert intramedullary rods cansignificantly reduce the strength of the bone.136
FRACTURE HEALING WITHINTRAMEDULLARY RODS
The issue of ideal intramedullary rod flexibility is stilldebated. Using an osteotomized rabbit femur model,Wang and colleagues148 compared intramedullary rodswith 12% to 100% of the intact femoral bending stiffness.They found that rods with a stiffness equivalent to 20% to50% of that of an intact femur stimulated abundantexternal callus and resulted in improved return ofstructural properties as compared with rods with astiffness equivalent to 75% of normal. Similarly, Molsterand co-workers100 compared fracture healing in ratfemurs stabilized by a stiff stainless steel rod with femurs
Working length
FIGURE 4–20. The unsupported (or working) length of an intramedullarydevice can be much greater for a comminuted fracture than for a simpletransverse fracture.
105CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 9/5/02 14 P 16/30 P 105 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 9/5/02 14 P 16/30 P 105 BLACK T

stabilized by a flexible plastic rod. There was no significantdifference in radiographically determined time to unionbetween the groups. The torsional strength was also notstatistically different at 8 and 16 weeks, but the femursfixed with the flexible rod had more callus and signifi-cantly greater strength at 24 weeks. These studies supportthe contention that intramedullary rods should allow someamount of fracture mobility to stimulate callus formationand bone union.
The optimal fixation technique must allow transfer offorces between bone and implant without causing grossfailure of either the bone or the implant. For example,failure of bone has been observed with many rigidnail-plate devices used for fractures of the proximal femur.Sliding screws that allow load transmission between bonefragments as well as load transmission between bone andimplant reduce, but do not eliminate, penetration of theimplant into the femoral head. This penetration isassociated with (1) improper placement of the slidingscrew in the proximal femur and (2) osteoporotic bone.
Quantitative measurements of bone density in thefemoral head can help determine the load-bearing capacityof fractured proximal femurs after fixation with a slidinghip screw or with standard pins and screws130, 132 andmay also help identify when augmentation is required fordistal interlocking in osteoporotic bone. The load requiredto cause penetration of the sliding hip screw superiorlyinto the femoral head may be insufficient to supportactivities of daily living in osteoporotic patients. Forexample, hip screw penetration loads as low as 750 N havebeen recorded132 in osteoporotic femurs. Allowing forcontact forces of 3.3 times body weight during gait,31
load-bearing capacities greater than 1300 N would berequired in a very lightweight person. Quantitativemeasurements of bone density may therefore be beneficialto ensure that fixation does not fail because of failure ofbone around the fixation system, although sensitive andspecific guidelines have yet to be developed.
In combination with bone density measurements, newimplant designs can potentially reduce complications fromoverloading bone around the implant. For example, asliding hip screw that allows controlled injection of bonecement into surrounding osteoporotic bone can dramati-cally reduce translation of the hip screw into the femoralhead.32
BONE PLATES
As with intramedullary devices, several basic biomechan-ical principles are important in fracture fixation using boneplates. Figure 4–21 illustrates some important parameters.It is crucial to realize that the plate and the bone togetherform a mechanical construct, with some load supported bythe plate and some load passing between bone fragments.Therefore, changes in the plate, the bone, or the interfacebetween plate and bone can dramatically influence themechanical environment of a fracture. The interactionbetween plate and bone is also load dependent; the platemay improve stability for one type of loading much morethan for other types of loads.
The bending stiffness of a bone plate with a rectangularcross section is related to the third power of the plate
thickness, whereas the bending rigidity is directly propor-tional to the width or elastic modulus of the plate.Therefore, plate rigidity can be changed more by platethickness than by plate width or modulus, with thelimitation that thick plates may not be possible in regionswith limited overlying soft tissue thickness.
The mechanical properties of bone also affect thebehavior of the plate-bone system. For example, less stiffbone increases the load-sharing contribution of the plate.Also, osteoporosis, osteopetrosis, or other bone diseasesmay affect bone remodeling at the plate-bone or screw-bone interfaces and thus affect the mechanical perfor-mance of the plated bone. However, the role of boneproperties in fracture fixation with bone plates has yet tobe investigated. Most in vivo animal studies and ex vivostudies of plate fixation have examined the biomechanicsof plates applied to osteotomized bones in which reduc-tion and compression of bone fragments could beachieved. In cases of highly comminuted fractures or whenbone defects must be stabilized, adequate reduction andstability are more difficult to achieve. In these cases, themechanical demands on the plate are increased becauseload transmission between bone fragments may not bepossible and all loads must pass through the plate.
Loads can be transmitted between plate and bonethrough the bone screws and through mechanical inter-locking or frictional forces between the plate surface andthe bone. Hayes and Perren61 found frictional forces ofabout 0.37 (comparable to that of wood sliding on leather)between titanium or stainless steel plates and bone whentested ex vivo. Thus, significant forces may be transmittedbetween plate and bone under ideal conditions. Perren andassociates114 reviewed studies of coupling between platesand bone that suggest that after 1 year in vivo, thecoupling between plate and bone may be limited.
The concept of working length introduced with intra-medullary devices is also applicable to bone plates. Theworking length of the plate, especially in the bending-openconfiguration, is greater when the inner screws are notplaced (Fig. 4–22). Maximal plate deflection is approxi-mately proportional to the square of the working length(see Fig. 4–7), so large decreases in bending rigidity occurwhen the inner screws are not used.
Cheal and co-workers29, 40 investigated the biomechan-ics of plate fixation using a combined experimental and
FIGURE 4–21. Factors affecting the stability of a plated fracture.
106 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 17/30 P 106 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 17/30 P 106 BLACK T

theoretical approach. The experimental model consisted ofan intact Plexiglas tube with an attached six-hole stainlesssteel compression plate. Several parameters—includingfriction between plate and bone and screw pretensioninduced by tightening the bone screws—were investigatedusing finite element models (Fig. 4–23). Several load caseswere considered, including axial loads, off-axis loads, andbending. Excellent agreement was obtained between thetheoretical and the experimental models. The analyticalmodels showed that stress shielding of bone should belimited to the central region between the inner screws.This conclusion agrees with radiographic findings fromanimal studies of bone changes beneath plates.102, 144
Static preloads, applied by compression plate techniques,can negate any reduction in axial stress levels beneath theplate, but these preloads decay rapidly and have not beenshown to affect the long-term fracture-healing proc-ess.93, 131 For fractures fixed with compression plates,experimental studies show the importance of placing theplate on the tensile aspect of the bone because the platedbone is particularly weak under loads that bend open thefracture. Finally, the results show that the outer screwsreceived the highest stresses.
The location of the plate (tension versus compressiveside of the bone) is an important factor in the biomechan-ics of bone plates because application of a bone platechanges the moment of inertia of the plate-bone systemcompared with an intact bone. With uniform axial loads,the stress throughout a cross section of intact bone isrelatively constant. With application of a bone plate, acombination of bending and axial stresses is realized in thesame cross section of bone. Subjected to bending loads, aplated bone can be in a bending-open or bending-closedconfiguration (see Fig. 4–22). The placement of the platerelative to the loading direction determines the proportionof the loads supported by the plate.
Hayes and Perren60 used osteotomized, plated sheeptibias to test the composite plate-bone system in thebending-open and bending-closed directions, both withand without application of compression between bonefragments (four-point bending). Figure 4–24 shows typicalresults from these tests, which clearly show that thecomposite plate-bone system is more stiff in the bending-closed direction and that application of compression alsoincreases the stiffness. Minns and associates99 also showed
FIGURE 4–23. Three-dimensional finite element mesh of a compression-plated tube used to study analytically the mechanical performance ofplate-bone systems. Only one quarter of the plated tube needs to bemodeled owing to the symmetry of the problem. (Data from Cheal, E.J.;Hayes, W.C.; White, A.A., III; Perren, S.M. J Biomech 18:141–150,1985.)
Working length
Bendingclosed
Bendingopen(no inner screws)
Bendingopen(all screws)
Unloaded
a
a
a
FIGURE 4–22. Different bending con-figurations for a plated fracture. Thisfigure also illustrates the concept ofworking length with bone plates andthe value of using all screws.
107CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 18/30 P 107 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 18/30 P 107 BLACK T

that application of a compression plate on the side of thebone normally loaded in tension produces the stiffestfixation. Although experimental efforts have shown thatpreloading a fracture gap through compression plating canincrease fracture stability, Matter and colleagues93 demon-strated that a static preload does not necessarily affect thepattern of bone remodeling. Slatis and co-workers131
found that the only difference associated with staticpreloading was a more rapid appearance of morphologicchanges.
The local mechanics within an oblique or comminutedfracture are significantly more complicated than thoseassociated with a transverse osteotomy. Beaupre andassociates8 studied the mechanics of plate fixation wherethere is insufficient bone to support ideal compressionplate fixation. A theoretical model of an idealized platedbone system and strain gauge readings from various animalmodels showed that the amount of bending is usually notsufficient to place a plated bone in a bending-openconfiguration when a gap exists between the fracturefragments. The results suggest that if contact between bonefragments cannot be achieved, there are situations inwhich the risk of plate failure is reduced if the plate isapplied to the compression side of the bone. It should benoted, however, that these results have not been substan-tiated by in vivo studies of fracture healing with insuffi-cient bone support.
FRACTURE HEALING WITH BONE PLATES
The temporal changes in the biomechanics of fractures thatheal by direct cortical reconstruction in the presence ofrigid internal fixation have been reported by Hayes andRuff.62 Compression plate fixation was applied to experi-mental osteotomies in dogs. Groups of dogs were sacri-ficed between 8 and 52 weeks. In addition, several groupsof dogs were sacrificed 2 to 8 weeks after plate removal at20 weeks. After sacrifice, the plates were removed, and the
bones were tested to failure in bending. The bendingstrength of the experimental bone was compared with thebending strength of the contralateral intact bone.
Figure 4–25 shows the change in strength versus timefor the plated tibias expressed as percentage of intact bonestrength. The results demonstrate a gradual increase instrength from 8 to 20 weeks. At 20 weeks, the plated boneswere 80% as strong as the intact bones. From 20 to 30weeks, plated bone strength declined to approximately60% of intact strength. The data suggest that for thisanimal model, 20 weeks would be the optimal time forplate removal. When the plates were removed at 20 weeks,the bending strength fell slightly during the first 4 weeksafter plate removal (Fig. 4–26) but then increased. Eightweeks after plate removal, the experimental bones were asstrong as or stronger than the contralateral intact bones.
0.00
0.20
0.40
0.60
0.80
1.00
1.20
5 15 25 35 45 55
TIME FOLLOWING FRACTURE (wk)
BE
ND
ING
MO
ME
NT
RA
TIO
Plated/control
FIGURE 4–25. Bending moment at failure as a function of time afterfracture for canine tibial fractures treated with compression plates.Bending moment at failure is expressed as the ratio between the strengthof the plated bone and that of the intact control bone. (Data from Hayes,W.C.; Ruff, C.B. In: Uhthoff, H.K.; Jaworski, Z.F.G., eds. Twelfth AnnualApplied Basic Sciences Course. Ottawa, University of Ottawa, 1986,pp. 371–377.)
0
2
4
6
8
10
12
14
0 4 8 12 16 20
MID-SPAN DEFLECTION (mm)
BE
ND
ING
MO
ME
NT
(N
-m) Intact
Bend closedcompression
Bend closedno compression
Bend opencompression
Bend openno compression
FIGURE 4–24. Maximal deflectionversus bending moment for platedsheep tibias. Tibias were plated withor without compression and weretested in both bend-open and bend-closed configurations. (Data fromHayes, W.C. In: Heppenstall, R.B., ed.Fracture Treatment and Healing. Phil-adelphia, W.B. Saunders, 1980,pp. 124–172.)
108 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 19/30 P 108 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 19/30 P 108 BLACK T

The effect of plate stiffness on fracture healing is notclear. Akeson and co-workers1 compared the failurestrength of osteotomies at 4 months treated with stainlesssteel and less rigid composite internal fixation plates andfound no significant difference. In contrast, Bradley andassociates17 found increased structural strength and mate-rial strength after treatment of an osteotomy with a lessrigid fixation plate compared with treatment of anosteotomy with a more rigid fixation plate. The observa-tion that interfragmentary relative motion influences thefracture-healing pattern of cortical bone has led to severalstudies examining the healing of fractures treated withplates of varying stiffness.
Woo and colleagues157 noted that there are severalaspects of the structural properties of bone plates. Theyexamined the axial, bending, and torsional stiffness ofplates and designed two plates that allowed comparison ofplates with high axial stiffness and plates with highbending and torsional stiffness. They found axial stiffnessto be the dominant factor that controls stresses in bone.Plates that provide sufficient bending and torsionalstiffness to stabilize the bone and low axial stiffness totransfer stress to the bone performed best.
Terjesen and Apalset139 investigated bone healing ofrabbit tibial osteotomies fixed with plates that had 13%,17%, 61%, or 74% of the bending stiffness of intact bone.After 6 weeks of plate fixation, the amount of periostealcallus was inversely related to plate stiffness. Bones treatedwith the stiffest plate tended to have lower rigidity andstrength than bones treated with less stiff plates. Theauthors also noted that no relation was found between theamount of periosteal callus and bone strength at 6 weeks.
Rigid internal fixation depends on force transmissionbetween implant and bone and between fractured boneends. Bone necrosis between implant and bone or betweenbone fragments compromises fixation stability. To under-stand better the reaction of living bone to compressionplate fixation, Perren and Rahn116 designed a strain-
gauged, four-hole compression plate that enabled them tomonitor the compression applied to the bone fragments bythe plate. The plates were applied to both intact andosteotomized bones in sheep. The tensile stress in the platewas measured at weekly intervals for 12 weeks after plateapplication. Plate tension for the intact bone group isshown in Figure 4–27. There was a gradual decrease inplate tension over 12 weeks after a steeper decrease in thefirst few days following surgery. The general trends foundfor the osteotomized group were the same as those foundfor intact bones. These results show that rigid internalfixation can maintain compression between bone frag-ments for several weeks. This finding suggests that there isno pressure necrosis between bone fragments or at theinterface between implant and bone because if a layer ofbone 10 to 20 µm thick were resorbed, tensile forces in theplate would drop to zero.
Histologic analysis confirmed the radiographic indica-tion of direct cortical reconstruction. In spite of full weightbearing immediately after plate application, the osteoto-mies were bridged by direct haversian remodeling. Thehistologic pattern of bone remodeling suggests a mecha-nism for the slow decrease in plate tension. It is postulatedthat bone remodeling at the osteotomy site results in localreductions in bone stiffness, reducing the compressiveloads maintained by the plate.
Several studies have concluded that early porosisnoted beneath bone plates during the first 6 monthsis due to the plate’s shielding bone from functionalstresses.24, 102, 140, 143, 144, 152 Perren and co-workers114
suggested that early in fracture healing, the porosis notedbeneath bone plates is in fact due to disruption of theblood supply to the bone caused by the contact betweenbone and plate. Plate-bone contact has been shown toresult in porosis by 1 month after surgery. Perren andco-workers presented four arguments in support ofvascular disruption as the cause of porosis beneath boneplates81, 114:
1. The porosis beneath plates appears to be a temporary,intermediate stage in bone remodeling in response tosurgery.
0
250
500
750
1000
0 20 40 60 80
DAYS
PLA
TE
LO
AD
(N
)
FIGURE 4–27. Force applied by a bone plate to the bone as a function oftime after compression plating for plates applied to intact canine tibias invivo. (Data from Perren, S.M.; Huggler, A.; Russenberger, M.; et al. ActaOrthop Scand Suppl 125:19–28, 1969.)
0.00
0.40
0.80
1.20
1.60
2.00
0 2 4 6 8 10
WEEKS POSTPLATE REMOVAL
BE
ND
ING
MO
ME
NT
RA
TIO
Plated/control
FIGURE 4–26. Bending moment at failure as a function of time followingplate removal at 20 weeks for canine tibial fractures treated withcompression plates. Bending moment at failure is expressed as the ratiobetween the strength of the plated bone and that of the intact controlbone. (Data from Hayes, W.C.; Ruff, C.B. In: Uhthoff, H.K.; Jaworski,Z.F.G., eds. Twelfth Annual Applied Basic Sciences Course. Ottawa,University of Ottawa, 1986, pp. 371–377.)
109CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 20/30 P 109 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 20/30 P 109 BLACK T

2. The bone-remodeling pattern is better explained by thepattern of vascular disruption than by the stressdistribution beneath the plate.
3. In a comparative study of plastic plates and steel plates,more porosis was noted beneath the plastic plate, eventhough the steel plate should provide substantiallymore stress shielding.
4. Porosis beneath bone plates can be substantiallyreduced by using plates that provide for improvedcirculation.
External Fixation
Current external fixation devices provide a wide range offrame configuration and fracture stability options, makingexternal fixation adaptable to many clinical situations.External fixation devices also provide a convenient way toalter fixation rigidity during the course of healing and offerpotential for monitoring the biomechanical progression offracture healing. The stability provided by an externalfixation device depends on both the frame configuration
and the interaction between frame and bone fragments.Juan and associates73 showed that for several types ofexternal fixators, callus formation is essential to a stablefracture. Huiskes and Chao70 showed that external fixatorrigidities can be altered by several orders of magnitudethrough changes in frame configuration.
As shown in Figures 4–28 and 4–29, several geometric,material, and technical factors, as well as loading direc-tions, can play a role in the biomechanics of externallyfixed fractures. The relative contribution of several of thesefactors has been quantified using computer models.70
Most biomechanical studies of external fixators examinethe effect of various parameters on rigidity under severaltypes of loading. It must be strongly emphasized that if theclamps or other connectors used in an external fixationsystem become loose, the stability of the fixation is severelycompromised.41 These connections may also actually failunder relatively low loads.
The percutaneous pins are typically the weakestcomponent of an external fixation system. Several studieshave shown that high stresses can occur in the pins,possibly resulting in permanent deformation of the pin,
FIGURE 4–29. Various loading modes thatmust be considered when evaluating themechanical behavior of an externallyfixed fracture.
FIGURE 4–28. Factors affecting the stabilityof an externally fixed fracture.
110 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 21/30 P 110 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 21/30 P 110 BLACK T

especially when the fracture site is unstable.71, 74 Thebending rigidity of each pin is theoretically proportional tothe fourth power of the pin diameter, so increasing the pindiameter from 4 to 6 mm increases the bending stiffness ofeach pin by five times. Pin diameter has been shown to beone of the most important parameters that determinefixator stiffness.27 The bending stiffness of each pin is alsoproportional to the cube of the sidebar-to-bone distance,and small changes in the sidebar-to-bone distance causelarge changes in pin rigidity.
The relationship between pin diameter or sidebar-to-bone distance and fixator rigidity is more complicated inmost fixators where several fixation pins are used and thefractures are subject to a variety of loads. Figure 4–30illustrates this point using data from Chao and Hein26 fora standard Orthofix external fixator tested ex vivo using anartificial fracture model. In this model, a single-planeexternal fixator is mounted in a plane identified as
mediolateral. The axial stiffness data of Figure 4–30A showthat, for example, a four-pin Orthofix fixator with a 4-mmsidebar-to-bone span has an axial stiffness of about 3000N/cm. Thus, a 600-N (61-kg) individual bearing half his orher weight on the fixed limb would cause approximately 1mm of displacement at the fracture site if a gap existedbetween the bone fragments. Experimental studies havefound gap displacements up to 2 mm for a 600-N load,and these displacements are strongly dependent on thefixation system and the presence of callus.73 Directmeasurements of axial motion in externally fixed tibialdiaphyseal fractures showed that displacements reached amaximum of 0.6 mm after 7 to 12 weeks of healing.80
Comparing Figure 4–30B and C demonstrates that themediolateral bending stiffness is more than four times theanteroposterior bending stiffness for the unilateral single-plane Orthofix fixator. The figures also show that thestiffness increases with the number of pins and decreases
0
1000
2000
3000
6000
5000
4000
3 4 5
SIDEBAR TO BONE SPAN (cm)
ST
IFF
NE
SS
(N
/cm
)
AXIAL STIFFNESS
Four pins
Six pins
A
0
100
200
400
300
3 4 5
SIDEBAR TO BONE SPAN (cm)
RIG
IDIT
Y (
N �
M2 )
ML BENDING RIGIDITY
Four pins
Six pins
C
0
100
200
400
300
3 4 5
SIDEBAR TO BONE SPAN (cm)
ST
IFF
NE
SS
(N
� c
m/d
eg)
TORSIONAL STIFFNESS
Four pins
Six pins
D
0
10
20
30
90
50
60
70
80
40
3 4 5
SIDEBAR TO BONE SPAN (cm)
RIG
IDIT
Y (
N �
M2 )
AP BENDING RIGIDITY
Four pins
Six pins
B
FIGURE 4–30. A–D, Fixator stiffness as a function of the distance between bone and sidebar for four different loading configurations. Data for both four-pinand six-pin fixator configurations are shown. The bending stiffness data of Chao and Hein26 were converted to bending rigidities using the formulas fromFigure 4–7. (A–D, Data from Chao, E.Y.S.; Hein, T.J. Orthopedics 11:1057–1069, 1988.)
111CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 22/30 P 111 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 22/30 P 111 BLACK T

with sidebar-to-bone spacing under all loading configura-tions. However, the effect of sidebar-to-bone spacing ismost pronounced with axial loads. A six-pin fixator issignificantly more stiff than a four-pin fixator with axialand torsional loads, whereas the six-pin fixator is less rigidwith bending loads applied in the plane of the fixator.Chao and Hein26 attributed this to uneven clampingpressure on the pins, causing some pins to carry more loadthan others. If each pin carried the same load, the fixatorstiffness should increase by a factor of 6/4 when comparinga six-pin with a four-pin frame.70 The data of Figure 4–30show that this is not the case for the Orthofix fixator,reinforcing the hypothesis that some pins must besupporting more load than others and thus may be moresusceptible to pin loosening or pin failure.
External fixation is used both in situations wherecontact between bone fragments can be achieved (fracturereduction) and in cases where a gap remains initiallybetween bone fragments (e.g., limb lengthening, severelycomminuted fractures). These two situations providesubstantially different biomechanical requirements forexternal fixation. Bone contact allows load sharing be-tween bone and fixator for compressive, torsional, andcertain bending loads. Without bone contact, the externalfixator must support the full load, which can have asignificant effect on fracture healing. It is also possible toapply compression across a fracture gap using an externalfixator. The amount of compression that can be applieddepends in part on the rigidity of the external fixator.96
With transverse fractures, application of compressionacross the fracture site can greatly increase the stiffness ofthe frame-bone system.18
Fixation pin loosening is a common problem withexternal fixators. Clinical128 and analytical71 studies havedemonstrated that the pin-bone interface is potentially aweak link in the stability of an external fixation system.Loose pins can substantially decrease the stability of anexternally fixed fracture and lead to soft tissue problems.Commonly cited reasons for pin loosening include pindesign, pin placement, pin tract infection, necrosis re-lated to surgical trauma during pin placement, necro-sis related to unfavorable bone stress, and contactpressure at the pin-bone interface. Suggested solutions tothe pin-loosening problem include changes in surgicaltechnique,134 changes in pin properties and threaddesign,82, 91 and changes in frame rigidity.28 Rigorous invivo studies of suggested solutions have yet to be reported,however.
FRACTURE HEALING WITH EXTERNALFIXATION
Experimental evidence suggesting that fracture fixationrigidity significantly affects the biology of bone healing hasprompted several studies that compare bone healing withvarious external fixation rigidities. Wu and associates159
used a canine tibial osteotomy model to examine bonehealing with a rigid six-pin versus a less rigid four-pinunilateral frame. Union was achieved with all osteotomies,but the clinical characteristics of bone healing dependedon fixator rigidity. Bone union was clinically and biome-chanically evident earlier with the more rigid frame. There
was greater periosteal callus formation at 90 and 120 daysand a higher incidence of pin loosening with less rigidframes. However, at 120 days after osteotomy, the torsionalstrength and torsional stiffness were not statisticallydifferent for the different frame rigidities.
The fracture pattern noted during torsion testingsuggested that the more rigidly fixed osteotomies hadreached a more mature stage of fracture healing. Theincreased periosteal callus formation would provide tor-sional strength and stiffness for the less rigidly fixed tibias.Thus, although the repair tissue formed with less rigidlyfixed fractures may be weaker as a material, the geometricdistribution of the tissue provides structural stability.Histologic examination suggested that with the rigidframes, fracture healing occurred by direct cortical recon-struction, whereas with less rigid fixation, periosteal callusformation characteristic of secondary bone healing wasevident.
The same general conclusions were realized in a studyby Williams and co-workers153 that compared canine tibialosteotomies treated by one or two planes of externalfixation. The two-plane fixators were significantly morerigid in bending and torsion than the single-plane fixator,whereas the axial stiffness of the fixators was similar. Boneunion was achieved with both fixators. Higher fracture sitestiffness early in the fracture-healing process and less callusformation were noted with the more rigid two-planefixators. After 13 weeks, however, the stiffness andradiographic characteristics of healing fractures were thesame for the two external fixation frames. This studysupports that of Wu and associates159 in demonstratingthat osteotomy union can be achieved with a range ofexternal fixator rigidities, that stiffer external fixationframes result in more rapid return of fracture site stiffness,and that externally fixed osteotomies converge to similarbiomechanical levels during later stages of fracture healingwith various fixator rigidities.
Briggs and Chao18 demonstrated that external fixatorsthat apply compression across the fracture provide morerigid fixation than those without compression. Hart andcolleagues57 created tibial osteotomies bilaterally in dogs.Both sides were treated with external fixators, butcompression was applied on only one side. After 90 days,fracture healing was evaluated biochemically, histologi-cally, and biomechanically. All of the osteotomies hadhealed after 90 days. No significant differences were foundin blood flow, histology, or strength between the groups.Hart and colleagues concluded that although compressionincreases the rigidity of externally fixed transverse osteoto-mies, it has little effect on the biologic or biomechanicalstate of fracture healing at the time period studied.57
Goodship and Kenwright52 investigated the influenceof induced interfragmentary motion on the healing of tibialosteotomies in sheep. They compared rigid fixation of anosteotomy with a 3-mm gap with a similar situation withthe addition of a 1-mm axial deformation applied over17-minute periods daily. They found significant improve-ment in healing, as measured radiographically and byfracture stiffness, with the applied micromotion. Thisimprovement was evidently due to greater callus formationwith the controlled motion. Kenwright and co-workers79
extended this study to examine alternate levels of applied
112 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 23/30 P 112 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 23/30 P 112 BLACK T

micromotion and found that 2-mm deformations weredetrimental to healing, whereas 0.5-mm deformationsenhanced healing in later stages (8 to 12 weeks).Kenwright and associates79 used similar regimens ofmicromotion in a clinical study and found that fracturehealing occurred earlier than in patients who received rigidexternal fixation with no applied micromotion. Goodshipand associates53 also showed that increasing the externalfixation frame stiffness by moving the sidebars closer to thebone slowed down fracture healing in an ovine model oftibial fractures.
Although numerous studies have shown that therigidity of fracture fixation influences bone healing, mostof these studies used experimental designs in whichfixation rigidity was held constant throughout the study.Consideration of the interfragmentary strain hypothesis ofPerren and co-workers leads immediately to the hypothe-sis that rigid fixation may be desirable early during healingto reduce the strain levels to a point at which bone cellscan survive. After osseous union has begun, it might bedesirable to increase load transfer across the fracture site inorder to stimulate bone remodeling. This concept is incommon clinical practice where increased weight bearingis prescribed after a period of reduced weight bearing.External fixators provide a convenient method for alteringfixation rigidity during the course of healing. This factprompted several studies in which fixation rigidity wasaltered during the course of fracture healing.4, 5, 42, 80
Dynamization is a term used to describe mechanismsthat decrease the stiffness of a fixation device or mecha-nisms that allow increased motion between fracturefragments. A few devices specifically allow motion alongone axis (axial dynamization). Dynamization is intended toaccelerate fracture healing by allowing more load transferacross the fracture site after the initial stages of fracturehealing.
To examine the effect of destabilization on unstableosteotomies, Egger and associates42 externally fixed bilat-eral oblique osteotomies in adult canine tibias. In this case,a 2-mm gap was left between fracture fragments. After 6weeks, the rigidity of fixation was reduced on one side.After 12 weeks, the ‘‘destabilized’’ tibia had significantlygreater torsional strength, but not stiffness, than the tibiawith constant rigid fixation. The difference was attributedto more advanced bone remodeling of the initial bone-healing response. It is also noteworthy that the differenceswere not radiographically evident.
Egger and co-workers43 investigated the effect ofreducing fixator stability in a canine tibial obliqueosteotomy model at various times after osteotomy. Desta-bilization of fixation stability was accomplished by con-verting a trilateral external fixation frame to a unilateralframe at 1, 2, 4, or 6 weeks after osteotomy. Reduction inexternal fixation rigidity at 1, 2, or 4 weeks resulted inincreased callus formation with decreased torsionalstrength as compared with osteotomies treated withcontinuous rigid fixation. However, destabilization ofexternal fixation after 6 weeks increased torsional strengthby 30%, although it had little effect on torsional strength,energy absorption, or pin loosening. The increase instrength was attributed to more rapid maturation of theinitial direct cortical reconstruction response. Finally, the
incidence of pin loosening increased when fixation rigiditywas reduced, which was attributed to higher stresses at thepin-bone interface.
Dynamization increases the load that is transferredacross the fracture and may allow increased micromotionbetween fragments. The effect of micromotion on fracturehealing is not clear. Kershaw and colleagues80 have shownin a prospective clinical study that imposing micromotionreduced healing time for tibial diaphyseal fractures. Incontrast, Aro and associates5 applied Orthofix unilateralfixators to transverse osteotomies bilaterally in dogs. After15 days, axial motion was allowed on one side whilerigid fixation was maintained contralaterally. After 90days, the periosteal callus was more uniformly distributedon the side where axial freedom was allowed; however,the torsional stiffness and strength were the same for bothbones.
In a sheep model of fracture healing, micromotion atan osteotomy site was controlled by applying rigid orsemirigid external fixators. The difference in fracturesite micromotion was approximately 25% between thegroups. A 25% increase in micromotion resulted in a400% increase in regional blood flow at the osteotomysite.147 There was also substantially more callus in theosteotomies treated with semirigid external fixation.Despite the pronounced difference in blood flow andhistology, no differences in failure torque or torsionalstiffness could be attributed to fixator rigidity ormicromotion. Similar results were found by Steen andco-workers135 in a study in which axial compression wasallowed 2 weeks after a 3-week limb-lengthening period.The torsional strength of fixators with and withoutdelayed reduction in external fixator stiffness wasstatistically equal. Steen and co-workers attributed thisresult to insufficient differences in the rigidity of thefixators. Dynamization also had no effect in a rabbitmodel of fracture healing.117
Further studies are needed to determine what types offractures benefit from delayed reduction in fixationrigidity, what magnitude of reduction in rigidity is optimal,what is the optimal time to change rigidity, and howrigidity or other parameters can be noninvasively moni-tored.
Comparative Studies of Healing withDifferent Types of Fixation
The preceding discussions have examined the widerange of fracture fixation stability that can be obtainedwith various treatments and the different types of healingthat occur with rigid versus less rigid fixation. However,the relative merits of the different healing patterns arewidely debated, and little quantitative evidence isavailable for comparison on other than clinical grounds.Micromovement between bone fragments facilitates frac-ture healing, but the acceptable range of micromotionand the optimal range of micromotion have not beendetermined.
Although nonmechanical clinical aspects of a fracturemay dictate the best fracture treatment approach, there are
113CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 24/30 P 113 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 24/30 P 113 BLACK T

cases in which several options exist, and mechanicalconsiderations are important in selecting a fixationmethod. Several animal studies have compared fracturehealing with different types of fixation (e.g., plates versusrods, internal fixation versus external fixation).
Rand and colleagues119 compared compression platesand reamed, fluted intramedullary rods using the caninetransverse tibial osteotomy model. They evaluated bloodflow, fracture site morphology, and bone strength atvarious times up to 120 days after fracture. Clinical unionwas evident in all dogs after 42 days. Blood flow to thefracture site reached higher levels and remained highlonger in osteotomies treated with reaming and intramed-ullary rods. There was significantly more new boneformation with intramedullary fixation, with most of thenew bone formed in periosteal callus. With compressionplating, most of the new bone formed endosteally. Platedbones were significantly stronger and stiffer than rod-fixedbones at 42 and 90 days but not at 120 days. The studydemonstrated different healing mechanisms with the twotreatments studied, but the time required to establishnormal strength and stiffness was not different.
Sarmiento and co-workers126 compared rigid compres-sion plating with functional braces for closed nondis-placed fractures and found that fractures treated withfunctional braces produced abundant callus and hadgreater torsional strength than rigidly fixed fractures.However, Lewallen and associates,86 using a canine tibialmodel, radiographically, histologically, and biomechani-cally compared osteotomies fixed by compression platingwith those stabilized by external fixators. Initially, theless rigid, externally fixed osteotomies were significantlyless stiff than those fixed by the more rigid compres-sion plating. Dogs applied more load sooner to thecompression-plated leg than to the contralateral externallyfixed limb. After 120 days, bone union occurred in mostanimals independent of fixation method. However,compression-plated bones were significantly stronger andstiffer in torsion than those that were externally fixed.Histologically, the total amount of new bone was similarfor the two fixation methods, but there was significantlymore resorbed bone and intracortical porosity withexternally fixed bones and more intracortical new bone onthe compression-plated side. Also, there was greater bloodflow to externally fixed osteotomy sites, consistent withother results suggesting increased bone remodeling withthe less stable fixation.
Terjesen and Svenningsen141 utilized transverse tibialosteotomies in rabbits to compare fracture healing withmetal plates with that with plaster casts and toexamine the role of limb loading in fracture healingwith different treatments. Four types of fracture treatmentwere studied: plate fixation, plate fixation with a longplaster cast, a long plaster cast, and a short plaster cast.The long plaster casts were intended to restrict loads onthe healing bone. Callus area, bending strength, andbending stiffness were evaluated after 6 weeks. Fracturesthat were treated with the long plaster cast, both with andwithout plating, were significantly weaker and less stiff.More periosteal callus developed with both long and shortcast treatments than with plated fractures. The authorsconcluded that weight bearing and muscular activity are
more effective than fixation stiffness at promoting boneunion.
MONITORING FRACTURE HEALINGz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Because bones are structural members whose functions areto support the body and permit the skeletal motionsnecessary for survival, it seems natural that fracturehealing should be evaluated by the return of prefracturestiffness and strength. Instead, however, clinical assess-ments of fracture healing are typically made by impreciseradiographic criteria, by subjective assessments of pain,and by comparison with previous clinical experience. As aresult, little is known about the return of stiffness andstrength to healing bones. Noninvasive imaging techniquesmay also allow objective assessment of fracture healing,92
but the sensitivity and specificity of these techniques arelargely unknown.
Several research groups have proposed or implementednoninvasive methods for monitoring the biomechanicalprogression of fracture healing. The general approach is toapply loads across the fracture gap and measure theresultant deflections. Many of these methods are directedtoward externally fixed fractures because the externalfixation pins provide a direct mechanical connection to thefractured bone (assuming that the pins have not loosened).As the fracture heals, the slope of the load-versus-displacement curve increases, representing a return to theoriginal stiffness of the bone. The goal is to monitor theload-versus-displacement curve to determine whetherthe union is proceeding normally. There are two advan-tages of this information. First, in the case of delayedunion, corrective action can be taken earlier than would bepossible if using radiographic information alone. Second,the biomechanics of the fracture treatment can be ‘‘finetuned’’ to provide the optimal mechanical environment forfracture healing.
One clinical objective of fracture treatment is to restorethe load-bearing capacity of the bone. In the laboratory,bone from animal models of fracture healing can beremoved, and both the stiffness and the load-bearingcapacity can be measured. In contrast, only the stiffness ofhealing bones can be measured in patients. It is thereforeimportant to understand the relationships between stiff-ness and load-bearing capacity of healing fractures. Henryand co-workers64 demonstrated that caution is neededwhen using bone stiffness to determine the strength of ahealing fracture. They utilized a rabbit osteotomy model,and fractures were fixed by intramedullary rodding,plating, or no surgical intervention. Bones were testedusing four-point bending 5 to 10 weeks after osteotomy.All fracture treatments resulted in similar biomechanicalresults, so the data were pooled. Figure 4–31 shows therelationship between bone strength and bone stiffness 5weeks after osteotomy. Both strength and stiffness valuesare expressed as the ratio of fractured bone to intact bone.The regression line for the data indicates a slope of about0.5, suggesting that bone strength returns more slowlythan bone stiffness.
Proposed methods for monitoring externally fixed
114 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 25/30 P 114 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 25/30 P 114 BLACK T

fracture healing can be divided into two groups: methodsthat involve application of quasistatic loads across thefracture and methods that utilize dynamic or vibration-type loads. Beaupre and associates9 demonstrated theapplication of fracture site monitoring using static loads. AHoffman-Vidal external fixation system was applied to anidealized fracture model ex vivo. The model consisted ofPlexiglas cylinders representing a long bone with neoprenediscs of various stiffness placed between the ends of thecylinders representing the healing fracture gap. Loads wereapplied to the fixation pins, and the deflection across thefracture gap was monitored. They also utilized ananalytical (finite element) model of the external fixator inwhich changes in the fracture site stiffness could be
altered. Both the experimental and the analytical resultsdemonstrated that the stiffness of a fracture gap could beevaluated using this method.
The relationships between external fixator pin displace-ment and the mechanical properties of the fracture site arenonlinear3, 9, 117 and dependent on the applied loadcharacteristics.41 Thus, it is important to document therelationship between pin displacement and fracture sitestiffness for each external fixator frame configurationbefore interpreting the data. For most loading configura-tions, there is a relatively steep decrease in pin displace-ment with initial increases in fracture site stiffness (0% to10% of intact bone stiffness). During later stages of fracturehealing, the decrease in pin displacement is small, withlarge increases in fracture site stiffness (Fig. 4–32). It mayalso be difficult to separate the effect of loosening ofconnectors in the external fixation system41 from theeffects of fracture healing.
Evans and colleagues46 developed a displacementtransducer that clamps on to the external support of aunilateral fixation system. Axial and bending loads aremanually applied to the limb while the reaction force andframe deflection are monitored. Using this system, curvesof limb load versus sidebar deflection can be monitored atvarious times after fracture. Changes in the slope of theload-deflection curve provide an indication of the biome-chanical progression of fracture healing. Although theauthors did not verify the relationship between fracturesite stiffness and transducer signal, they applied the systemfor monitoring numerous tibial fractures. Utilizing thissystem, they collected clinical data to determine when anexternal fixator can be safely removed.
Fracture site monitoring using dynamic tests typicallyinvolves applying an oscillating or impulse load across thefracture gap and monitoring the acceleration or displace-
0
1
2
3
4
5
6
7
0 10 20 30 40 50 60
PERCENTAGE INTACT BONE STIFFNESS
PIN
DIS
PLA
CE
ME
NT
(m
m)
Bilateralframe
Unilateralframe
445 N axial load
A
0
1
2
0 10 20 30 40 50 60
PERCENTAGE INTACT BONE STIFFNESS
PIN
DIS
PLA
CE
ME
NT
(m
m)
45 N bending load
B
Bilateralframe
Unilateralframe
FIGURE 4–32. A and B, Analytical results for an idealized model of an externally fixed fracture. The pin displacement during application of distractionand bending loads to the bone is shown as a function of fracture site stiffness. (A and B, Data from An, K.N.; Kasman, R.A.; Chao, E.Y.S. Eng Med17:11–15, 1988.)
0.00
0.25
0.50
0.75
1.00
0.00 0.25 0.50 0.75 1.00 1.25 1.50
STIFFNESS (FRACTURED/INTACT)
ST
RE
NG
TH
(F
RA
CT
UR
ED
/INT
AC
T)
0.45 � X � 0.05
FIGURE 4–31. Bone strength versus fracture stiffness for rabbit tibialosteotomies after 5 weeks of healing with several different fracturetreatment methods. (Data from Henry, A.N.; Freeman, M.A.R.; Swanson,S.A.V. Proc R Soc Med 61:902–906, 1968.)
115CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 26/30 P 115 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 26/30 P 115 BLACK T

ment of the bone at one or more locations. An example ofa dynamic system for monitoring fractures is the boneresonance analysis method, developed and tested byCornelissen and co-workers35 for monitoring tibial frac-tures. This technique is designed to measure the lowestresonant frequency of a fractured tibia. The basis for themethod is that the resonant frequency of a tibia decreasessignificantly with fracture and then increases as thefracture heals. Small, 30- to 300-Hz, cyclical axial loads areapplied to the medial malleolus and below the tibialtuberosity, and the acceleration of a point along theanterior surface of the tibia is monitored. The resonantfrequency of the limb is determined as the vibrationfrequency that results in the greatest tibial mobility. Inclinical practice, the resonant frequency of the fracturelimb is monitored during the course of fracture healing.This technique requires that loads be transmitted acrosssoft tissues. With the presence of joints and variablemuscle tension, interpretation of bone resonance analysistest results is complicated. For this reason the absolutevalues of measured resonant frequencies are not reliable,and the data must be analyzed for temporal changes inresonant frequencies. Comparative measurements usinga normal contralateral limb serve as a reference. Nosignificant difference between resonant frequencies ofnormal left and right limbs were observed in tests of morethan 50 normal individuals.
Tibial refractures after external fixation occur in 3% to11% of patients.38, 83, 121 Quantitative measurement ofstructural properties can help determine the optimal timeto remove the fixator and may thereby reduce therefracture rate.121 In a consecutive series of 117 patientswith diaphyseal tibial fractures, unilateral external fixationwas removed when radiographic and clinical findingssuggested that union had occurred. In 8 of these patients(7%), refracture occurred. In the next 95 patients, externalfixation was removed when the bending rigidity of thelower leg was greater than 15 Nm/degree, and none ofthese patients experienced refracture.121 The sensitivity ofthe stiffness measurement was 100%, but the specificitywas 78% (44 of 160 patients had a stiffness below 15Nm/degree but did not experience refracture).
Several potential difficulties must be considered. Forexample, Churches and associates33 demonstrated thatfixation pin loosening significantly alters the stability of anexternally fixed fracture. Pin loosening could also lead tomisleading results if pin displacements are used to monitorfracture biomechanics. Thus, it is important to monitorpin loosening in studies in which pin displacements areemployed to monitor fracture healing. Similarly, none ofthe connections in the external fixation system can beallowed to loosen because this leads to misleadingresults.41 In addition, few studies have adequately charac-terized the sensitivity of the monitoring techniques todetermine the resolution of the in vivo biomechanicalmeasurements and how clinical alterations in frameconfigurations affect data over the treatment period.Finally, additional clinical data are required for biome-chanical characterization of ‘‘normal’’ fracture healingpatterns in humans as standard curves are needed toidentify abnormal temporal sequences in fracture healing.
SUMMARYz z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z z
Biomechanical studies of the material and structuralproperties of bones have provided a basic understandingof bone properties and the alterations that can accom-pany aging and bone pathologic abnormalities. This infor-mation has been applied in several experimental andanalytical studies that are enhancing our ability to pre-dict fracture risk associated with aging and metastatic bonedisease. This basic understanding of bone biomechanicsalso facilitates understanding of the fracture treatmentbiomechanics because the mechanical properties of boneand the mechanical properties of the fracture treat-ment together determine the biomechanics of a fixationsystem.
Two basic types of fracture-healing biologies have beenidentified, and it has been well established that biome-chanical factors influence fracture healing. Numerousanimal studies have demonstrated that the return of bonestiffness and strength can be altered by fixation rigidity.However, a consensus has not been reached on theoptimal fixation rigidity for different types of fractures oron how fixation rigidity should be altered as the fractureheals. The literature, however, does provide informationthat can facilitate clinical management of orthopaedicfractures.
Selection of the optimal form of fracture managementinvolves balancing sometimes conflicting requirements.Several studies have demonstrated that a wide range offixation stabilities are available through numerous internaland external fixation device designs and applications.Frequently, several basic mechanical principles can be usedto understand the degree of fixation rigidity provided byeach treatment method. When specific biomechanicalfixation requirements can be identified, sufficient engi-neering tools are available to choose a treatment method.One application of biomechanical analyses of fracturetreatment is in monitoring the biomechanical progressionof fracture healing. Methods are being developed that willallow noninvasive biomechanical monitoring. Furtherresearch may provide noninvasive and objective measuresfor selecting treatment methods, altering treatment duringthe course of healing, and determining the time forremoval of the fixation for optimal return of normal weightbearing.
REFERENCES
1. Akeson, W.H.; Woo, S.L.Y.; Rutherford, L.; et al. The effects ofrigidity of internal fixation plates on long bone remodeling: Abiomechanical and quantitative histiological study. Acta OrthopScand 47:241–249, 1976.
2. Allen, W.C.; Heiple, K.G.; Burstein, A.H. A fluted femoralintramedullary rod. J Bone Joint Surg Am 60:506–515, 1978.
3. An, K.N.; Kasman, R.A.; Chao, E.Y.S. Theoretical analysis offracture healing monitoring with external fixators. Eng Med17:11–15, 1988.
4. Aro, H.; Chao, E. Bone-healing patterns affected by loading,fracture fragment stability, fracture type, and fracture site compres-sion. Clin Orthop 293:8–17, 1993.
5. Aro, H.T.; Kelly, P.J.; Lewallen, D.G.; Chao, E.Y.S. The effects ofphysiologic dynamic compression on bone healing under externalfixation. Clin Orthop 256:260–273, 1990.
116 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 27/30 P 116 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 27/30 P 116 BLACK T

6. Backman, S. The proximal end of the femur. Acta Radiol StockhSuppl 146:1–166, 1957.
7. Beals, R.K.; Lawton, G.D.; Snell, W.E. Prophylactic internal fixationof the femur in metastatic breast cancer. Cancer 28:1350–1354,1971.
8. Beaupre, G.S.; Carter, D.R.; Dueland, R.T.; et al. A biomechanicalassessment of plate fixation, with insufficient bony support.J Orthop Res 6:721–729, 1988.
9. Beaupre, G.S.; Hayes, W.C.; Jofe, M.H.; White, A.A., III. Monitoringfracture site properties with external fixation. J Biomech Eng105:120–126, 1983.
10. Beaupre, G.S.; Schneider, E.; Perren, S.M. Stress analysis of apartially slotted intramedullary nail. J Orthop Res 2:369–376,1984.
11. Beck, T.; Ruff, C.; Bissessur, K. Age-related changes in femalefemoral neck geometry: Implications for bone strength. CalcifTissue Int 53:S41–S46, 1993.
12. Beck, T.; Ruff, C.; Mourtada, F.; et al. Dual-energy x-rayabsorptiometry–derived structural geometry for stress fractureprediction in male U.S. Marine Corps recruits. J Bone Miner Res11:645–653, 1996.
13. Bergmann, G.; Graichen, F.; Rohlmann, A. Hip joint loading duringwalking and running, measured in two patients. J Biomech26:969–990, 1993.
14. Bergot, C.; Laval-Jeantet, A.M.; Preteux, F.; Meunier, A. Measure-ment of anisotropic vertebral trabecular bone loss during agingby quantitative image analysis. Calcif Tissue Int 43:143–149,1988.
15. Black, J.; Perdigon, P.; Brown, N.; Pollack, S.R. Stiffness andstrength of fracture callus. Relative rates of mechanical maturationas evaluated by a uniaxial tensile test. Clin Orthop 182:278–288,1984.
16. Boyce, W.J.; Vessey, M.P. Rising incidence of fracture of the proximalfemur. Lancet 1:150–151, 1985.
17. Bradley, G.W.; McKenna, G.B.; Dunn, H.K.; et al. Effects of flexuralrigidity of plates on bone healing. J Bone Joint Surg Am61:866–872, 1979.
18. Briggs, B.T.; Chao, E.Y.S. The mechanical performance of thestandard Hoffmann-Vidal external fixation apparatus. J Bone JointSurg Am 64:566–573, 1982.
19. Burstein, A.H.; Reilly, D.T.; Martens, M. Aging of bone tissue:Mechanical properties. J Bone Joint Surg Am 58:82–86, 1976.
20. Carter, D.R.; Hayes, W.C. Bone compressive strength: The influenceof density and strain rate. Science 194:1174–1176, 1976.
21. Carter, D.R.; Hayes, W.C. Compact bone fatigue damage. I. Residualstrength and stiffness. J Biomech 10:325–327, 1977.
22. Carter, D.R.; Hayes, W.C. Compact bone fatigue damage. II. Amicroscopic examination. Clin Orthop 127:265–274, 1977.
23. Carter, D.R.; Hayes, W.C. The compressive behavior of bone as atwo-phase porous structure. J Bone Joint Surg Am 59:954–962,1977.
24. Carter, D.R.; Shimaoka, E.E.; Harris, W.H.; et al. Changes inlong-bone structural properties during the first 8 weeks of plateimplantation. J Orthop Res 2:80–89, 1984.
25. Chang, W.C.; Christensen, T.M.; Pinilla, T.P.; Keaveny, T.M. Uniaxialyield strains for bovine trabecular bone are isotropic and asymmet-ric. J Orthop Res 17:582–585, 1999.
26. Chao, E.Y.S.; Hein, T.J. Mechanical performance of the standardOrthofix external fixator. Orthopedics 11:1057–1069, 1988.
27. Chao, E.Y.S.; Kasman, R.A.; An, K.N. Rigidity and stress analysis ofexternal fixation devices—A theoretical approach. J Biomech15:971–983, 1982.
28. Chao, E.Y.S.; An, K.N. Stress and rigidity and external fixationdevices. In: Gallagher, R.H.; Simon, B.R.; Johnson, P.C.; Gross, J.F.,eds. Finite Elements in Biomechanics. New York, John Wiley &Sons, 1982, pp. 195–222.
29. Cheal, E.J.; Hayes, W.C.; White, A.A., III; Perren, S.M. Stressanalysis of compression plate fixation and its effects on long boneremodeling. J Biomech 18:141–150, 1985.
30. Cheal, E.J.; Mansmann, K.A.; DiGioia, A.M., III; et al. Role ofinterfragmentary strain in fracture healing: Ovine model of ahealing osteotomy. J Orthop Res 9:131–142, 1991.
31. Cheal, E.; Spector, M.; Hayes, W. Role of loads and prosthesismaterial properties on the mechanics of the proximal femur aftertotal hip arthroplasty. J Orthop Res 10:405–422, 1992.
32. Choueka, J.; Koval, K.; Kummer, F.; et al. Biomechanical compari-son of the sliding hip screw and the dome plunger. J Bone JointSurg Br 77:277–283, 1995.
33. Churches, A.E.; Tanner, K.E.; Harris, J.D. The Oxford externalfixator: Fixator stiffness and the effects of bone pin loosening. EngMed 14:3–11, 1985.
34. Cody, D.D.; Gross, G.J.; Hou, F.J.; et al. Femoral strength is betterpredicted by finite element models than QCT and DXA. J Biomech32:1013–1020, 1999.
35. Cornelissen, P.; Cornelissen, M.; Van der Perre, G.; et al. Assessmentof tibial stiffness by vibration testing in situ. II. Influence of softtissues, joints and fibula. J Biomech 19:551–561, 1986.
36. Courtney, A.; Wachtel, E.; Myers, E.; Hayes, W. Effects of loadingrate on strength of the proximal femur. Calcif Tissue Int 55:53–58,1994.
37. Davy, D.T.; Connolly, J.F. The biomechanical behavior of healingcanine radii and ribs. J Biomech 15:235–247, 1982.
38. de Bastiani, G.; Aldegheri, R.; Brivio, L.R. The treatment of fractureswith a dynamic axial fixator. J Bone Joint Surg Br 66:538–545,1984.
39. de Bruin, E.D.; Herzog, R.; Rozendal, R.H.; et al. Estimation ofgeometric properties of cortical bone in spinal cord injury. ArchPhys Med Rehabil 81:150–156, 2000.
40. DiGioia, A.M., III; Cheal, E.J.; Hayes, W.C. Three-dimensionalstrain fields in a uniform osteotomy gap. J Biomech Eng108:273–280, 1986.
41. Drijber, F.P.; Finlay, J.B.; Dempsey, A. Evaluation of linear finite-element analysis models: Assumptions for external fixation devices.J Biomech 25:849–855, 1992.
42. Egger, E.; Gottsauner-Wolf, F.; Palmer, J.; et al. Effects of axialdynamization on bone healing. J Trauma 34:185–192, 1993.
43. Egger, E.L.; Lewallen, D.G.; Norrdin, R.W.; et al. Effects ofdestabilizing rigid external fixation on healing of unstable canineosteotomies. Trans Orthop Res Soc 34:302, 1988.
44. Ellsasser, J.C.; Moyer, C.F.; Lesker, P.A.; Simmons, D.J. Improvedhealing of experimental long bone fractures in rabbits by delayedinternal fixation. J Trauma 15:869–876, 1975.
45. Esses, S.I.; Lotz, J.C.; Hayes, W.C. Biomechanical properties of theproximal femur determined in vitro by single-energy quantitativecomputed tomography. J Bone Miner Res 4:715–722, 1989.
46. Evans, M.; Kenwright, J.; Cunningham, J.L. Design and perfor-mance of a fracture monitoring transducer. J Biomed Eng 10:64–69,1988.
47. Fidler, M. Prophylactic internal fixation of secondary neoplasticdeposits in long bones. Br Med J 10:341–343, 1973.
48. Frankle, M.; Cordey, J.; Sanders, R.W.; et al. A biomechanicalcomparison of the antegrade inserted universal femoral nail withthe retrograde inserted universal tibial nail for use in femoral shaftfractures. Injury 30(Suppl 1):A40–A43, 1999.
49. Fyhrie, D.P.; Vashishth, D. Bone stiffness predicts strength similarlyfor human vertebral cancellous bone in compression and forcortical bone in tension. Bone 26:169–173, 2000.
50. George, C.J.; Lindsey, R.W.; Noble, P.C.; et al. Optimal location of asingle distal interlocking screw in intramedullary nailing of distalthird femoral shaft fractures. J Orthop Trauma 12:267–272, 1998.
51. Gibson, L.J. Cancellous bone. In: Gibson, L.T.; Ashby, M.F., eds.Cellular Solids. New York, Pergamon Press, 1988, pp. 316–331.
52. Goodship, A.E.; Kenwright, J. The influence of induced micro-movement upon the healing of experimental tibial fractures. J BoneJoint Surg Br 67:650–655, 1985.
53. Goodship, A.; Watkins, P.; Rigby, H.; Kenwright, J. The role offixator frame stiffness in the control of fracture healing: Anexperimental study. J Biomech 26:1027–1035, 1993.
54. Greenspan, S.; Myers, E.; Maitland, L.; et al. Fall severity and bonemineral density as risk factors for hip fracture in ambulatory elderly.JAMA 271:128–133, 1994.
55. Grosse, A.; Christie, J.; Taglang, G.; et al. Open adult femoral shaftfracture treated by early intramedullary nailing. J Bone Joint Surg Br75:562–565, 1993.
56. Guo, X.; McMahon, T.; Keaveny, T.; et al. Finite element modelingof damage accumulation in trabecular bone under cyclic loading.J Biomech 27:145–155, 1994.
57. Hart, M.B.; Wu, J.J.; Chao, E.Y.; Kelly, P.J. External skeletal fixationof canine tibial osteotomies. Compression compared with nocompression. J Bone Joint Surg Am 67:598–605, 1985.
117CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 28/30 P 117 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 28/30 P 117 BLACK T
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=5125680&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3404329&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3745226&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6527162&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7922790&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7096379&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6746689&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3141014&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1639829&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6692620&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8459454&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2857223&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1177333&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2816516&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1249116&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3347037&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6491803&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=9619462&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3405906&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8408085&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8264067&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3988783&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1984043&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8132682&dopt=Abstract

58. Hayes, W.C. Biomechanical measurements of bone. In: Burstein, A.,ed. CRC Handbook of Engineering in Medicine and Biology:Section B. Instruments and Measurements. Cleveland, CRC Press,1978, pp. 333–372.
59. Hayes, W.C. Biomechanics of fracture healing. In: Heppenstall, R.B.,ed. Fracture Treatment and Healing. Philadelphia, W.B. Saunders,1980, pp. 124–172.
60. Hayes, W.C.; Perren, S.M. Flexural rigidity of compression platefixation. Med Biol Eng 2:242–244, 1971.
61. Hayes, W.C.; Perren, S.M. Plate-bone friction in the compressionfixation of fractures. Clin Orthop 89:236–240, 1972.
62. Hayes, W.C.; Ruff, C.B. Biomechanical compensatory mechanismsfor age-related changes in cortical bone. In: Uhthoff, H.K.; Jaworski,Z.F.G., eds. Twelfth Annual Applied Basic Sciences Course. Ottawa,University of Ottawa, 1986, pp. 371–377.
63. Hayes, W.; Myers, E. Biomechanics of fractures. In: Riggs, B.;Melton, L., eds. Osteoporosis: Etiology, Diagnosis, and Manage-ment, 2nd ed. New York, Raven Press, 1995, pp. 93–114.
64. Henry, A.N.; Freeman, M.A.R.; Swanson, S.A.V. Studies of themechanical properties of healing experimental fractures. Proc R SocMed 61:902–906, 1968.
65. Hipp, J.A.; Edgerton, B.C.; An, K.N.; Hayes, W.C. Structuralconsequences of transcortical holes in long bones loaded in torsion.J Biomech 23:1261–1268, 1990.
66. Hipp, J.A.; McBroom, R.J.; Cheal, E.J.; Hayes, W.C. Structuralconsequences of endosteal metastatic lesions in long bones.J Orthop Res 7:828–837, 1989.
67. Hipp, J.A.; Springfield, D.; Hayes, W. Predicting pathologic fracturerisk in the management of metastatic bone defects. Clin Orthop312:120–135, 1995.
68. Hora, N.; Markel, D.C.; Haynes, A.; Grimm, M.J. Biomechanicalanalysis of supracondylar femoral fractures fixed with modernretrograde intramedullary nails. J Orthop Trauma 13:539–544,1999.
69. Huiskes, R.; Chao, E.Y.S. A survey of finite element analysis inorthopedic biomechanics: The first decade. J Biomech 16:385–409,1983.
70. Huiskes, R.; Chao, E.Y.S. Guidelines for external fixation framerigidity and stresses. J Orthop Res 4:68–75, 1986.
71. Huiskes, R.; Chao, E.Y.S.; Crippen, T.E. Parametric analysis ofpin-bone stresses in external fixation. J Orthop Res 3:341–349,1985.
72. Jacobsen, S.; Cooper, C.; Gottlieb, M.; et al. Hospitalization withvertebral fracture among the aged: A national population-basedstudy, 1986–1989. Epidemiology 3:515–518, 1992.
73. Juan, J.A.; Prat, J.; Vera, P.; et al. Biomechanical consequences ofcallus development in Hoffmann, Wagner, Orthofix, and Ilizarovexternal fixators. J Biomech 25:995–1006, 1992.
74. Kasman, R.A.; Chao, E.Y. Fatigue performance of external fixatorpins. J Orthop Res 2:377–384, 1984.
75. Keaveny, T.; Guo, X.; Wachtel, E.; et al. Trabecular bone exhibitsfully linear elastic behavior and yields at low strains. J Biomech27:1127–1136, 1994.
76. Keaveny, T.; Wachtel, E.; Guo, X.; Hayes, W. Mechanical behavior ofdamaged trabecular bone. J Biomech 27:1309–1318, 1994.
77. Keene, J.S.; Sellinger, D.S.; McBeath, A.A.; Engber, W.D. Metastaticbreast cancer in the femur: A search for the lesion at risk of fracture.Clin Orthop 203:282–288, 1986.
78. Kempf, I.; Karger, C.; Willinger, R.; et al. Locked intramedullarynailing—Improvement of mechanical properties. In: Perren, S.M.;Schneider, E., eds. Biomechanics: Current Interdisciplinary Re-search. Boston, Martinus Nijhoff, 1985, pp. 487–492.
79. Kenwright, J.; Richardson, J.B.; Goodship, A.E.; et al. Effect ofcontrolled axial micromovement on healing of tibial fractures.Lancet 2:1185–1187, 1986.
80. Kershaw, C.; Cunningham, J.; Kenwright, J. Tibial external fixation,weight bearing, and fracture movement. Clin Orthop 293:28–36,1993.
81. Klaue, K.; Fengels, I.; Perren, S.M. Long-term effects of plateosteosynthesis: Comparison of four different plates. Injury31(Suppl 2):51–62, 2000.
82. Klip, E.; Rosma, R. Investigations into the mechanical behavior ofbone-pin connections. Eng Med 7:43–46, 1978.
83. Krettek, C.; Haas, N.; Tscherne, H. The role of supplementallag-screw fixation for open fractures of the tibial shaft treated withexternal fixation. J Bone Joint Surg Am 73:893–897, 1991.
84. Laurence, M.; Freeman, M.A.R.; Swanson, S. Engineering consid-erations in the internal fixation of fractures of the tibial shaft. J BoneJoint Surg Br 51:754–768, 1969.
85. Levensteon, M.; Beaupre, G.; Van der Muelen, M. Improved methodfor analysis of whole bone torsion tests. J Bone Miner Res9:1459–1469, 1994.
86. Lewallen, D.G.; Chao, E.Y.S.; Kasman, R.A.; Kelly, P.J. Comparisonof the effects of compression plates and external fixators on earlybone-healing. J Bone Joint Surg Am 66:1084–1091, 1984.
87. Liew, A.S.; Johnson, J.A.; Patterson, S.D.; et al. Effect of screwplacement on fixation in the humeral head. J Shoulder Elbow Surg9:423–426, 2000.
88. Lotz, J.C.; Cheal, E.J.; Hayes, W.C. Fracture prediction for theproximal femur using finite element models: Part I: Linear models.J Biomech Eng 113:353–360, 1991.
89. Lotz, J.; Cheal, E.; Hayes, W. Stress distributions within theproximal femur during gait and falls: Implications for osteoporoticfracture. Osteoporos Int 5:252–261, 1995.
90. Lotz, J.C.; Hayes, W.C. The use of quantitative computedtomography to estimate risk of fracture of the hip from falls. J BoneJoint Surg Am 72:689–700, 1990.
91. Manley, M.T.; Hurst, L.; Hindes, R.; et al. Effects of low-moduluscoatings on pin-bone contact stresses in external fixation. J OrthopRes 2:385–392, 1984.
92. Markel, M.; Chao, E. Noninvasive monitoring techniques forquantitative description of callus mineral content and mechanicalproperties. Clin Orthop 293:37–45, 1993.
93. Matter, P.; Brenwald, J.; Perren, S.M. The effect of static compres-sion and tension on internal remodeling of cortical bone. Helv ChirActa 42(Suppl 12):1–57, 1975.
94. Mazess, R.B. On aging bone loss. Clin Orthop 165:239–252, 1982.95. McBroom, R.J.; Cheal, E.J.; Hayes, W.C. Strength reductions from
metastatic cortical defects in long bones. J Orthop Res 6:369–378,1988.
96. McCoy, M.T.; Chao, E.Y.S.; Kasman, R.A. Comparison of mechan-ical performance in four types of external fixators. Clin Orthop180:23–33, 1983.
97. Melton, L.J., III. Epidemiology of hip fractures: Implications of theexponential increase with age. Bone 18:121S–125S, 1996.
98. Melton, L.J., III; Khosla, S.; Atkinson, E.J.; et al. Relationship ofbone turnover to bone density and fractures. J Bone Miner Res12:1083–1091, 1997.
99. Minns, R.J.; Bremble, G.R.; Campbell, J. A biomechanical study ofinternal fixation of the tibial shaft. J Biomech 10:569–579, 1977.
100. Molster, A.O.; Gjerdet, N.R.; Langeland, N.; et al. Controlledbending instability in the healing of diaphyseal osteotomies in therat femur. J Orthop Res 5:29–35, 1987.
101. Morrison, J.B. The mechanics of the knee joint in relation to normalwalking. J Biomech 3:51–61, 1969.
102. Moyen, B.J.L.; Lahey, P.J.; Weinberg, E.H.; Harris, W.H. Effects onintact femora of dogs of the application and removal of metal plates:A metabolic and structural study comparing stiffer and moreflexible plates. J Bone Joint Surg Am 60:940–947, 1978.
103. Nagurka, M.L.; Hayes, W.C. Technical note: An interactive graphicspackage for calculating cross-sectional properties of complexshapes. J Biomech 13:59–64, 1980.
104. Nakamura, T.; Turner, C.J.; Yoshikawa, T.; et al. Do variations in hipgeometry explain differences in hip fracture risk between Japaneseand white Americans? J Bone Miner Res 9:1071–1076, 1994.
105. Oda, M.A.S.; Schurman, D.J. Monitoring of pathological fractures.In: Stoll, B.A.; Parbhoo, S., eds. Bone Metastasis. New York, RavenPress, 1983, pp. 271–288.
106. Panagiotopoulos, E.; Fortis, A.P.; Lambiris, E.; Kostopoulos, V. Rigidor sliding plate. A mechanical evaluation of osteotomy fixation insheep. Clin Orthop 358:244–249, 1999.
107. Panjabi, M.M.; Walter, S.D.; Karuda, M.; et al. Correlations ofradiographic analysis of healing fractures with strength: A statisticalanalysis of experimental osteotomies. J Orthop Res 3:212–218,1985.
108. Panjabi, M.M.; White, A.A., III; Southwick, W.O. Temporal changesin the physical properties of healing fractures in rabbits. J Biomech10:689–699, 1977.
109. Panjabi, M.M.; White, A.A., III; Wolf, J.W. A biomechanicalcomparison of the effects of constant and cyclic compression onfracture healing in rabbit long bones. Acta Orthop Scand 50:653–661, 1979.
118 SECTION I • General Principles
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 29/30 P 118 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 29/30 P 118 BLACK T
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6480637&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=4646262&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1762430&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7492864&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2292605&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2795323&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8339505&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7075066&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3357085&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6352706&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3950810&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8777076&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=4032105&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1420517&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3819909&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1517275&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6527163&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7798281&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7354095&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3955991&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7942154&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=2877327&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=9973997&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8339493&dopt=Abstract

110. Parfitt, A. Bone age, mineral density, and fatigue damage. CalcifTissue Int 53(Suppl):S82–S85, 1993.
111. Parker, M.J.; Pryor, G.A.; Myles, J. 11-year results in 2,846patients of the Peterborough Hip Fracture Project: Reducedmorbidity, mortality and hospital stay. Acta Orthop Scand 71:34–38, 2000.
112. Perren, S.M.; Boitzy, A. Cellular differentiation and bone biome-chanics during the consolidation of a fracture. Anat Clin 1:13–28,1978.
113. Perren, S.M.; Cordey, J. The concept of interfragmentary strain. In:Uhthoff, H.K., ed. Current Concepts of Internal Fixation ofFractures. New York, Springer-Verlag, 1980, pp. 63–77.
114. Perren, S.M.; Cordey, J.; Rahn, B.A.; et al. Early temporary porosisof bone induced by internal fixation implants. Clin Orthop232:139–151, 1988.
115. Perren, S.M.; Huggler, A.; Russenberger, M.; et al. The reaction ofcortical bone to compression. Acta Orthop Scand Suppl 125:19–28,1969.
116. Perren, S.M.; Rahn, B.A. International symposium on fixation offractures. Biomechanics of fracture healing. Can J Surg 23:228–232,1980.
117. Prat, J.; Juan, J.; Vera, P.; et al. Load transmission through the callussite with external fixation systems: Theoretical and experimentalanalysis. J Biomech 27:469–478, 1994.
118. Rahn, B.A.; Gallinaro, P.; Baltensperger, A.; Perren, S.M. Primarybone healing: An experimental study in the rabbit. J Bone Joint SurgAm 53:783–786, 1971.
119. Rand, J.A.; An, K.N.; Chao, E.Y.S.; Kelly, P.J. A comparison of theeffect of open intramedullary nailing and compression-platefixation on fracture-site blood flow and fracture union. J Bone JointSurg Am 63:427–442, 1981.
120. Reilly, D.T.; Burstein, A.H. The elastic and ultimate properties ofcompact bone tissue. J Biomech 8:393–405, 1975.
121. Richardson, J.; Cunningham, J.; Goodship, A.; et al. Measuringstiffness can define healing of tibial fractures. J Bone Joint Surg Br76:389–394, 1994.
122. Riggs, B.L.; Wahner, H.W.; Seeman, E.; et al. Changes in bonemineral density of the proximal femur and spine with aging.Differences between the postmenopausal and senile osteoporosissyndromes. J Clin Invest 70:716–723, 1982.
123. Roark, R.J.; Young, W.C. Tables of cross-sectional formulae. In:Formulas for Stress and Strain, 5th ed. New York, McGraw-Hill,1975, pp. 59–72.
124. Ruff, C.B.; Hayes, W.C. Age changes in geometry and mineralcontent of the lower limb bones. Ann Biomed Eng 12:573–584,1984.
125. Ruff, C.B.; Hayes, W.C. Bone mineral content in the lower limb:Relationship to cross-sectional geometry. J Bone Joint Surg Br66:1024–1031, 1984.
126. Sarmiento, A.; Mullis, D.L.; Latta, L.L.; et al. A quantitativecomparative analysis of fracture healing under the influence ofcompression plating vs. closed weight-bearing treatment. ClinOrthop 149:232–239, 1980.
127. Seireg, A.; Kempke, W. Behavior of in vivo bone under cyclicloading. J Biomech 2:455–461, 1969.
128. Seligson, D.; Stanwyck, T. The general technique of externalfixation. In: Seligson, D.; Pope, M., eds. Concepts in ExternalFixation. New York, Grune & Stratton, 1982, pp. 9–108.
129. Silverman, F.N. Essentials of Caffey’s pediatric x-ray diagnosis.Pediatr Radiol 1989; 1216.
130. Sjostedt, A.; Zetterberg, C.; Hansson, T.; et al. Bone mineral contentand fixation strength of femoral neck fractures. Acta Orthop Scand65:161–165, 1994.
131. Slatis, P.; Karaharju, E.; Holmstrom, T.; et al. Structural changes inintact tubular bone after application of rigid plates withand without compression. J Bone Joint Surg Am 60:516–522,1978.
132. Smith, M.D.; Cody, D.D.; Goldstein, S.A.; et al. Proximal femurbone density and its correlation to fracture load and hip-screwpenetration load. Clin Orthop 283:244–251, 1992.
133. Snyder, B.D.; Edwards, W.T.; Hayes, W.C. Trabecular changes withvertebral osteoporosis. Letter. N Engl J Med 319:793–794, 1988.
134. Spiegel, P.; Vanderschilden, J. Minimal internal and minimalexternal fixation in the treatment of open extremity fractures. In:Seligson, D.; Pope, M., eds. Concepts in External Fixation. NewYork, Grune & Stratton, 1982, pp. 267–278.
135. Steen, H.; Fjeld, T.O.; Bjerkreim, I.; et al. Limb lengthening bydiaphyseal corticotomy, callus distraction, and dynamic axialfixation. An experimental study in the ovine femur. J Orthop Res6:730–735, 1988.
136. Strothman, D.; Templeman, D.C.; Varecka, T.; Bechtold, J. Retro-grade nailing of humeral shaft fractures: A biomechanical study ofits effects on the strength of the distal humerus. J Orthop Trauma14:101–104, 2000.
137. Tarr, R.R.; Wiss, D.A. The mechanics and biology of intramedullaryfracture fixation. Clin Orthop 212:10–17, 1986.
138. Tencer, A.F.; Sherman, M.C.; Johnson, K.D. Biomechanical factorsaffecting fracture stability and femoral bursting in closed intramed-ullary rod fixation of femur fractures. J Biomech Eng 107:104–111,1985.
139. Terjesen, T.; Apalset, K. The influence of different degrees ofstiffness of fixation plates on experimental bone healing. J OrthopRes 6:293–299, 1988.
140. Terjesen, T.; Benum, P. The stress-protecting effect of metal plateson the intact rabbit tibia. Acta Orthop Scand 54:810–818, 1983.
141. Terjesen, T.; Svenningsen, S. The effects of function and fixationstiffness on experimental bone healing. Acta Orthop Scand59:712–715, 1988.
142. Turner, C.; Burr, D. Basic biomechanical measurements of bone: Atutorial. Bone 14:595–608, 1993.
143. Uhthoff, H.K.; Dubuc, F.L. Bone structure changes in the dog underrigid internal fixation. Clin Orthop 81:165–170, 1971.
144. Uhthoff, H.K.; Finnegan, M. The effects of metal plates onpost-traumatic remodelling and bone mass. J Bone Joint Surg Br65:66–71, 1983.
145. Vajjhala, S.; Kraynik, A.M.; Gibson, L.J. A cellular solid model formodulus reduction due to resorption of trabeculae in bone.J Biomech Eng 122:511–515, 2000.
146. VanBuskirk, W.C.; Ashman, R.B. The elastic moduli of bone. In:Cowin, S.C., ed. Mechanical Properties of Bone. New York,American Society of Mechanical Engineers, 1981, pp. 131–144.
147. Wallace, A.L.; Draper, E.R.C.; Strachan, R.K.; et al. The vascularresponse to fracture micromovement. Clin Orthop 301:281–290,1994.
148. Wang, G.J.; Reger, S.I.; Mabie, K.N.; et al. Semirigid rod fixation forlong-bone fractures. Clin Orthop 192:291–298, 1985.
149. White, A.A., III; Panjabi, M.M.; Southwick, W.O. Effects ofcompression and cyclical loading on fracture healing—A quantita-tive biomechanical study. J Biomech 10:233–239, 1977.
150. White, A.A., III; Panjabi, M.M.; Southwick, W.O. The fourbiomechanical stages of fracture repair. J Bone Joint Surg Am59:188–192, 1977.
151. White, B.; Fisher, W.; Laurin, C. Rate of mortality for elderlypatients after fracture of the hip in the 1980s. J Bone Joint Surg Am69:1335–1340, 1987.
152. Williams, D.F.; Gore, L.F.; Clark, G.C.F. Quantitative microradiog-raphy of cortical bone in disuse osteoporosis following fracturefixation. Biomaterials 4:285–288, 1983.
153. Williams, E.A.; Rand, J.A.; An, K.N.; et al. The early healing of tibialosteotomies stabilized by one-plane or two-plane external fixation.J Bone Joint Surg Am 69:355–365, 1987.
154. Windhagen, J.; Hipp, J.A.; Hayes, W.C. Postfracture instability ofvertebrae with simulated defects can be predicted from computedtomography data. Spine 25:1775–1781, 2000.
155. Windhagen, H.; Hipp, J.A.; Silva, M.J., et al. Predicting failure ofthoracic vertebrae with simulated and actual metastatic defects.Clin Orthop 344:313–319, 1997.
156. Winquist, R.A.; Hansen, S.T.; Clawson, D.K. Closed intramedullarynailing of femoral fractures. J Bone Joint Surg Am 66:529–539,1984.
157. Woo, S.L.Y.; Lothringer, K.S.; Akeson, W.H.; et al. Less rigidinternal fixation plates: Historical perspectives and new concepts.J Orthop Res 1:431–439, 1984.
158. Wright, T.M.; Hayes, W.C. Tensile testing of bone over a wide rangeof strain rates: Effects of strain rate, microstructure and density. MedBiol Eng Comput 14:671–680, 1976.
159. Wu, J.J.; Shyr, H.S.; Chao, E.Y.S.; Kelly, P.J. Comparison ofosteotomy healing under external fixation devices with differentstiffness characteristics. J Bone Joint Surg Am 66:1258–1264, 1984.
160. Zych, G.A.; Greenbarg, P.E.; Milne, E.L.; et al. Mechanics of distallocking IM nail fixation in osteopenic and normal femora. TransOrthop Res Soc 13:406, 1988.
119CHAPTER 4 • Biomechanics of Fractures
#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 30/30 P 119 COLOR T#6818 @ l 1/ id/CLS b k /GRP d /JOB b /DIV h04 7/16/02 13 P 30/30 P 119 BLACK T
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3769275&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3999706&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6670503&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6991087&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8188727&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8274302&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=5133037&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=1206042&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8156689&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7119111&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3967436&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6534224&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6640055&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3818701&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=9372783&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6707031&dopt=Abstract
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=6491792&dopt=Abstract