Cesarean Section Primary.pptx
33
CESAREAN SECTION When, Why and How Matthew Snyder, DO, Maj, USAF, MC Nellis AFB, NV
-
Upload
andreas-berkat-elloirahmatdi -
Category
Documents
-
view
22 -
download
2
Transcript of Cesarean Section Primary.pptx

CESAREAN SECTIONWhen, Why and How
Matthew Snyder, DO, Maj, USAF, MCNellis AFB, NV

OVERVIEW
Indications Instruments Procedure Post-operative management Post-partum counseling
C/S INDICATIONS - FETAL
Fetal Macrosomia (over 5000g, GDM – 4500g)
Multiple Gestations Fetal Intolerance to Labor Malpresentation / Unstable Lie – Breech
or Transverse presentation

C/S INDICATIONS - FETAL
Non-reassuring Fetal Heart Tracing Repetitive Variable Decelerations Repetitive Late Decelerations Fetal Bradycardia Fetal Tachycardia Cord Prolapse

C/S INDICATIONS - MATERNAL
Elective Repeat C/S Maternal infection (active HSV, HIV) Cervical Cancer/Obstructive Tumor Abdominal Cerclage Contracted Pelvis
Congenital, Fracture Medical Conditions
Cardiac, Pulmonary, Thrombocytopenia

C/S INDICATIONS – MATERNAL/FETAL
Abnormal Placentation Placenta previa Vasa previa Placental abruption
Conjoined Twins Perimortem Failed Induction / Trial of Labor

C/S INDICATIONS – MATERNAL/FETAL
Arrest Disorders Arrest of Descent (no change in station
after 2 hours, <10 cm dilated)
Arrest of Dilation (< 1.2 cm/hr nullip; < 1.5 cm/hr multip)
Failure of Descent (no change in station after 2 hours, fully dilated)

C/S INDICATIONS – MATERNAL/FETAL

SURGICAL INSTRUMENTS
Uses: Adson: Skin Bonney: Fascia DeBakey: soft
tissue, bleeders Russians: uterus

SURGICAL INSTRUMENTS
Uses: Allis-Adair: tissue,
uterus Pennington:
tissue, uterus
These are suitable for hemostasis use

SURGICAL INSTRUMENTS
Uses: Kocher clamp:
fascia, thicker tissues
SURGICAL INSTRUMENTS
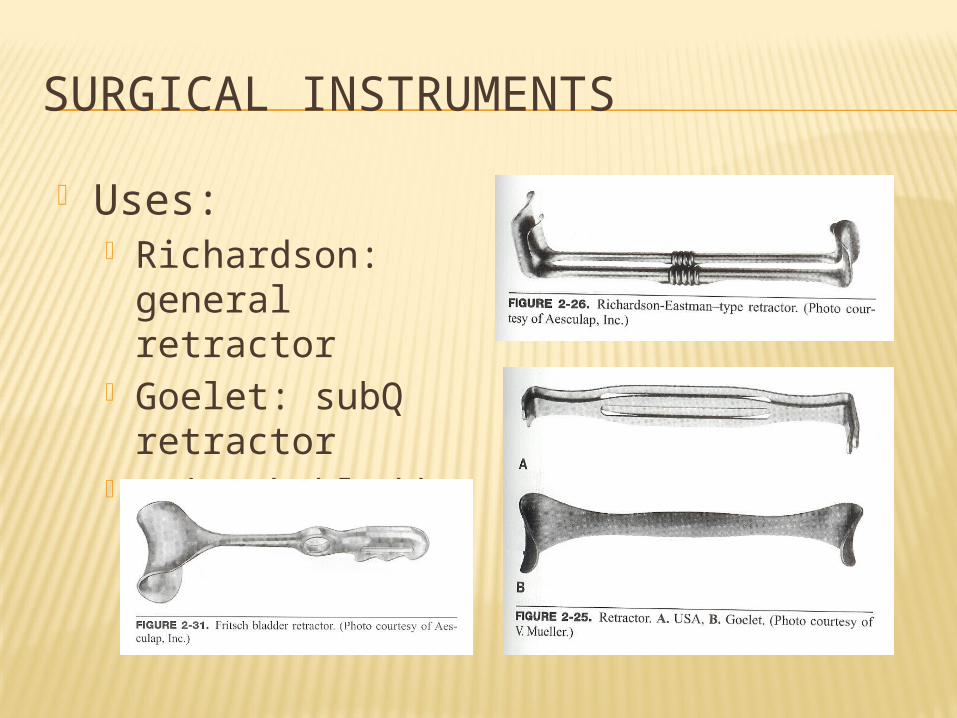
Uses: Richardson:
general retractor Goelet: subQ
retractor Fritsch bladder
blade

SURGICAL INSTRUMENTS
Uses: Mayo, curved:
fascia Metzenbaum,
curved: soft tissue Bandage scissors:
cord cutting, uterine extension

CESAREAN SECTION: INCISION TO UTERUS Preparation:
Ensure SCDs applied Setup bovie and suction Test pt by pinching on either side of
incision and around navel with Allis clamp Lap sponge in other hand

CESAREAN SECTION: INCISION TO UTERUS Determined by previous mode of delivery/hx
and body habitus – Pfannenstiel most common – 3 cm (2 fingerbreadths) above symphysis

CESAREAN SECTION: INCISION TO UTERUS Be cautious of the Superficial Epigastric
vessels

CESAREAN SECTION: INCISION TO UTERUS Rectus fascia incised in midline and
extended bil. with Mayo scissors/scalpel Elevate superior and inferior edges of
rectus fascia with Kocher clamps, dissect muscle from fascia at linea alba.

CESAREAN SECTION: INCISION TO UTERUS Separate rectus fascia to enter
peritoneum Bluntly with finger Using two hemostats to elevate
peritoneum and incise with Metzenbaum scissors
**Be careful of adhesions!!! – transilluminate at all times!!!**

CESAREAN SECTION: UTERINE INCISION TO DELIVERY Vesicoperitoneum reflexion entered with
Metz and extended bil. for bladder flap
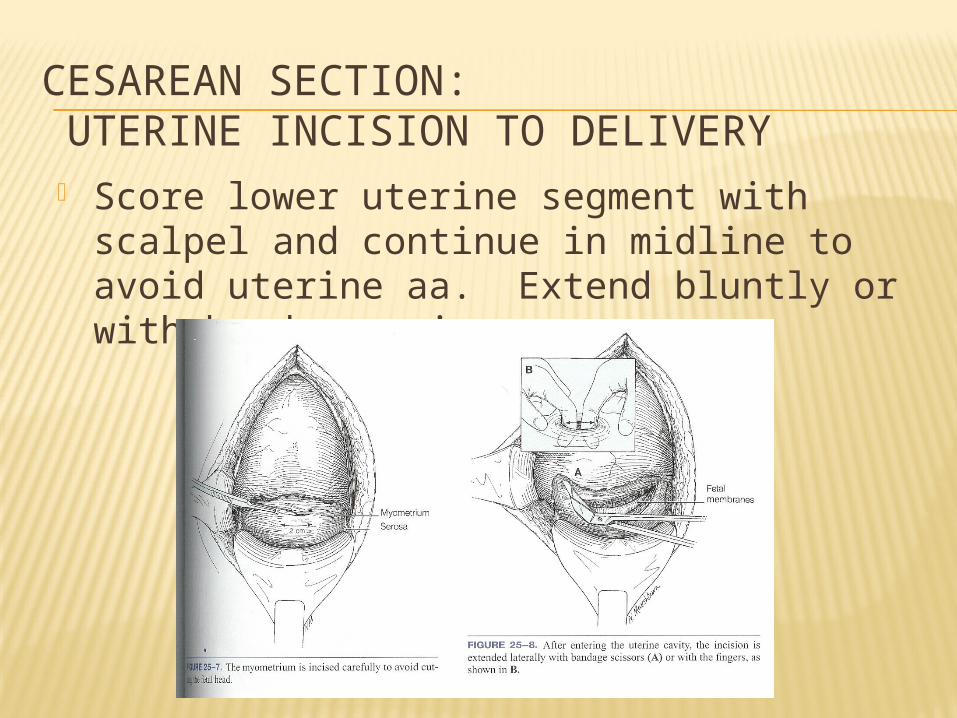
CESAREAN SECTION: UTERINE INCISION TO DELIVERY Score lower uterine segment with scalpel
and continue in midline to avoid uterine aa. Extend bluntly or with bandage scissors.

CESAREAN SECTION: UTERINE INCISION TO DELIVERY Once delivering hand inserted, bladder
blade removed Bring head up to incision by flexing fetal
head, without flexing wrist to avoid uterine incision extensions
Once infant delivered, collect cord gases if desired and cord blood sample
Deliver placenta manually or with uterine massage

CESAREAN SECTION: UTERINE CLOSURE If exteriorized, use a
moist lap sponge to wrap uterus and retract once placenta is delivered
Close uterine incision with locking suture (usually 0-Vicryl or 1-Chromic)
Perform imbricating stitch

CESAREAN SECTION: CLOSURE Examine adnexa, irrigate rectouterine
pouch and/or gutters and re-examine uterine incision
Ensure hemostasis of rectus then close fascia with non-locking suture to avoid vessel strangulation
Close subcut. space if over 2 cm, then skin
If needed, clear lower uterine segment and vagina of clots once skin is closed and dressed

POST-OPERATIVE CARE
Pt. must urinate within four hours of Foley removal, otherwise replace Foley for another 12 hours
Any fever post-op MUST be investigated Wind: Atelectasis, pneumonia Water: UTI Walking: DVT, PE, Pelvic thromboembolism Wounded: Incisional infection,
endomyometritis, septic shock

POST-OPERATIVE CARE
In the first 12-24 hours, the dressing may become soaked with serosanguinous fluid – if saturated, replace dressing otherwise no action needed
After Foley is removed (usually within 12 hours post-op), encourage ambulation of halls, not just room
Dressing may be removed in 24-48 hours post-op (attending specific), use maxipad
Ensure pt. is tolerating PO intake, urinating well and has flatus before discharge
Watch for post-op ileus

DELAYED COMPLICATIONS
Subsequent Pregnancies Uterine rupture/dehiscence Abnormal placental implantation (accreta,
etc) Repeat Cesarean section
Adhesions Scaring/Keloids
WOUND DEHISCENCE
Noted by separation of wound usually during staple removal or within 1-2 weeks post-op
Must explore entire wound to determine depth of dehiscence (open up incision if needed) – if through rectus fascia, back to the OR
If dehiscence only in subQ layer, debride wound daily with 1:1 sterile saline/H2O2 mixture and pack with gauze
May use prophylactic abx – Keflex, Bactrim, Clinda
KEY: Close f/u and wound exploration

POST-PARTUM COUNSELING:PHARM Continue PNV Colace Motrin 800 mg q8 Percocet 1-2 tabs q4-6 for
breakthrough OCP (start 4-6 wks post-partum)

POST-PARTUM COUNSELING:ACTIVITY No lifting objects over baby’s wt. Continue ambulation No strenuous activity NOTHING by vagina (sex, tampons,
douches, bathtubs, hot tubs) for 6 wks!!

POST-PARTUM COUNSELING:INCISION CARE Only showers – light washing If pt has steristrips, should fall off in 7-
10 days, otherwise use warm, wet washcloth to remove
If pt has staples – removal in 3-7 days outpt.
Most attendings will have pt f/u in office in about 2 wks for wound check

POST-PARTUM COUNSELING:NOTIFY MD/DO Fever (100.4)/Chills HA Vision changes RUQ/Epigastric pain Mastitis sx Increasing abd. pain Erythema/Induration/ increasing swelling around
incision
Purulent drainage Serosanguinous drainage over half dollar size on pad Wound separation Purulent vaginal discharge Vaginal bleeding over 1 pad/hr or golf ball size clots Calf tenderness

SUMMARY
Indications Surgical Technique Post-operative management Post-operative Complications Post-partum counseling

REFERENCES
Cunningham, F., Leveno, Keith, et al. Williams Obstetrics. 22nd ed., New York, 2005.
Gabbe, Steven, Niebyl, Jennifer, et al. Obstetrics: Normal and Problem Pregnancies. 4th ed., Nashville, 2001.
Gilstrap III, Larry, Cunningham, F., et al. Operative Obstetrics. 2nd ed., New York, 2002.
www.uptodateonline.com