
Cesarean Delivery on Maternal Request
41
Cesarean Delivery on Maternal Request Presented by: Barbara Hughes, CNM, MS, MBA, FACNM Colorado Perinatal Care Council July 31, 2009
-
Upload
adriano-minor -
Category
Documents
-
view
83 -
download
4
description
Cesarean Delivery on Maternal Request. Presented by: Barbara Hughes, CNM, MS, MBA, FACNM Colorado Perinatal Care Council July 31, 2009. Background and Process. Increasing Rate of Cesarean Delivery NIH Role CDMR: What is it? Identifying the Key Questions What did the evidence say? - PowerPoint PPT Presentation
Transcript of Cesarean Delivery on Maternal Request

Cesarean Delivery on Maternal Request
Presented by:Barbara Hughes, CNM, MS, MBA, FACNMColorado Perinatal Care CouncilJuly 31, 2009


Background and Process
Increasing Rate of Cesarean Delivery
NIH Role
CDMR: What is it?
Identifying the Key Questions
What did the evidence say?
What were the recommendations?
What’s YOUR Opinion?

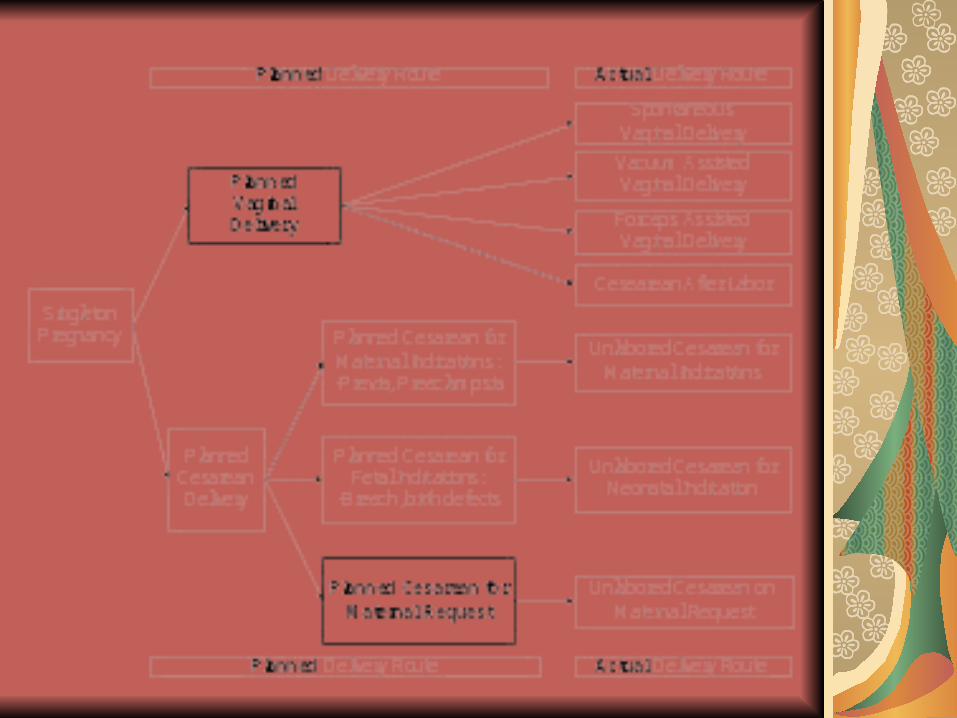
Definition of Cesarean Delivery on Maternal Request (CDMR)
Primary cesarean delivery
Singleton pregnancy
At term
On maternal request
No maternal or neonatal indications

Conference SponsorsNational Institute of Child Health and Human Development, NIH (NICHD)Office of Medical Applications of Research, NIH (OMAR)
Co-SponsorsNational Institute of Diabetes and Digestive and Kidney Diseases, NIHNational Institute of Nursing Research, NIHOffice of Research on Women’s Health
Also supported by:The Agency for Healthcare Research and Quality (AHRQ)

State-of-the-Science ConferenceNIH consensus and state-of-the-science statements
are prepared by independent panels of health professionals and public representatives on the basis of
(1) the results of a systematic literature review prepared under contract with the Agency for Healthcare Research and Quality (AHRQ),
(2) presentations by investigators working in areas relevant to the conference questions during a 2-day public session,
(3) questions and statements from conference attendees during open discussion periods that are part of the public session, and
(4) closed deliberations by the panel during the remainder of the second day and morning of the third. This statement is an independent report of the panel and is not a policy statement of the NIH or the Federal Government.
Who was on the Panel???OB/GYN PhysiciansMFMUrogynecologistUrologistAnesthesiologistEpidemiologistBio-statisticianNeonatologistPsychiatristDean of Law SchoolNurse-MidwifePatient Representative

The Assignment...
National Institute of Child Health and Human Development (NICHD) and the Office of Medical Applications of Research (OMAR) of the National Institutes of Health (NIH) convened a State-of-the-Science Conference from March 27 to 29, 2006, to assess the available scientific evidence relevant to four key questions:
What are the Key Questions (KQs)?
KQ1: What is the trend and incidence of cesarean delivery over time in the US and in other developed countries?KQ2: What is the effect of approach to delivery (i.e. cesarean delivery on maternal request compared to planned vaginal delivery), on maternal and infant short-term and long-term outcomes?KQ3: What are the factors affecting the magnitude of the benefits and harms in KQ2?KQ4: What future research directions need to be considered to get evidence for making appropriate decisions regarding CDMR versus planned vaginal delivery?
Key Question 1
What Is The Trend and Incidence of Cesarean Delivery Over Time in the United States and in Other Countries?

Total and primary cesarean rate and (VBAC): United States, 1989-2004 (29.1% in 2004)
0
5
10
15
20
25
30
35
Per
10
0
1995 20044
Total cesarean2
Primary cesarean3
VBAC1
Year1Number of vaginal births after previous cesarean per 100 live births to women with a previous cesarean delivery 2Percentage of all live births by cesarean delivery3Number of primary cesarean deliveries per 100 live births to women who have not had a previous cesarean 4Based on preliminary data NOTE: Due to changes in data collection from implementation of the 2003 revision of the U.S. Standard Certificate of Live Birth, there may be small discontinuities in rates of primary cesarean delivery and VBAC in 2003 and 2004. See “Technical Notes.”
1989 1991 1993 1997 2001 20031999
What is the IDEAL Rate of CD?
Healthy People 2010 = 15%
Upon what basis was this rate determined?
Does the cesarean section rate influence maternal and child health?

The Evidence
Evidence-based Practice Center (EPC) Report:
RTI International—University of North Carolina at Chapel Hill Evidence-based Practice Center (RTI-UNC EPC)
NUMEROUS additional articles
Speakers
Audience Participants

Planned Vaginal Delivery
Planned Cesarean Delivery
? ?

Key Question 2
What Are the Short-Term (Under One Year) and Long-Term Benefits and Harms to Mother and Baby Associated With Cesarean by Request Versus Attempted Vaginal Delivery?

Quality and Relevance of the Evidence
For the evidence obtained from the EPC report, the panel utilized an evidence quality grading scale provided within the document:
Level I—strong,
Level II—moderate,
Level III—weak
Level IV—absent

What did we have to work with?
No Level I evidence was found! 3 outcomes had Level II evidence
(Mom) Hemorrhage, LOS
(Baby)Respiratory morbidity
The remaining outcomes were Level III or IV
Interpretation of many outcome variables was confounded by a lack of appropriate comparison groups, a lack of consistency in outcome definitions, and the frequent use of composite outcomes & proxies.

Maternal Outcomes With Moderate-Quality Evidence (2)
Hemorrhage. The frequency of postpartum hemorrhage associated with planned CD is less than that reported with the combination of PVD and unplanned CD.
Maternal length of hospital stay is higher for CD, planned or otherwise, than for vaginal delivery. But...

Benefits & Harms: SummaryWith the exception of 3 outcome
variables with moderate-quality evidence (maternal hemorrhage, maternal length of stay, and neonatal respiratory morbidity)... all of the remaining outcome assessments considered by the panel were based on weak evidence.
This significantly limits the reliability of judgments regarding whether an outcome measure favors either CDMR or PVD.

Key Question 3
What Factors Influence Benefits and Harms?

What factors influence benefits & harms?
Patient specific factorsAge
Childbearing plans/family size
Obesity
Accuracy of gestational age assessment
Psychological factors

What factors influence benefits & harms?
Cultural & Societal IssuesCultural beliefs and practices
Personal philosophy of birth
Increasing societal acceptance
Media

What factors influence benefits & harms?
Provider Type and Professional Resources
Obstetrical providers...OB/GYN Physicians
MFM Physicians
Family Medicine Physicians
Certified Nurse-Midwives
What factors influence benefits & harms?
Provider Type and Professional Resources
Provider’s View of CDMR...Training
Practice environment
Experience
Personal philosophy
Medicolegal issues
What factors influence benefits & harms?
Provider Type and Professional ResourcesGeographical locationLevel of perinatal servicesAvailability of anesthesiaHospital resources (OR & Staff)Unpredictability of timing
Complex issuesPotential for biased recommendations

What factors influence benefits & harms?Ethical Issues
Provider/Patient relationshipEthical principles
AutonomyBeneficenceFirst, DO NO HARM
“If a woman requests information...”Shared decision making processWhen a provider cannot support a request for CDMR, “...it is appropriate to refer the woman to another provider.”

Summary of factors that influence benefits and harms...
Birth is an inherently normal process
The majority of women would like to achieve a spontaneous vaginal delivery and should supported in their efforts to achieve that goal
The available evidence and data comparing risks and benefits of PVD and CDMR are sparse and provide few clear conclusions

Key Question 4
What future research directions need to be considered to get evidence for making appropriate decisions regarding cesarean delivery on request or attempted vaginal delivery?

Future research directions
Surveys of women, providers, insurers and healthcare facilities regarding CDMRCreate mechanisms to identify CDMR
CPT CodeBirth Certificate
Increase research devoted to strategies to predict and influence the likelihood of successful vaginal birth, especially in the first pregnancy
Future research directions
Study of large, prospective cohorts, including long-term follow-up of mothers and children
Study of critical outcomes
Case-control studies
Randomized Trials?

Future research directions
Future studies should determine whether there are modifiable factors in the management of labor that can decrease maternal and neonatal complications.
Furthermore, an attempt should be made to identify subgroups of women at higher risk for complications that would benefit most from planned CDMR.

Studies comparing CDMR & PVD should consider the following key outcomes...
MaternalMaternal deathPlacental abnormalities including previa & acretaPelvic floor disordersPsychological factors

Studies comparing CDMR & PVD should consider the following key outcomes...
NeonatalNeonatal death
Neonatal encephalopathy
CP
Brachial plexus injury
Respiratory outcomes
Neurodevelopmental outcomes
Other birth injuries

Studies comparing CDMR & PVD should consider the following key outcomes...
Cost analysis of CDMR

Conclusions...The incidence of CD without medical/obstetrical indications is rising in the United States, and a component of this is due to CDMR. Given the tools available, the magnitude of the CDMR component is difficult to quantify.
There is insufficient evidence to evaluate fully the benefits and risks of CDMR as compared to PVD, and more research is needed.

Conclusions...
Until quality evidence becomes available, any decision to perform a CDMR should be carefully individualized and consistent with ethical principles.
Given that the risks of placenta previa and acreta rise with each CD, CDMR is not recommended for women desiring several children.

Conclusions...
CDMR should not be performed prior to 39 weeks or without verification of lung maturity, because of the significant danger of neonatal respiratory complications.
Request for CDMR should not be motivated by unavailability of effective pain management. Efforts must be made to assure availability of pain management services for all women.

Conclusions...
NIH or another appropriate Federal agency should establish and maintain a Web site to provide up-to-date information on the benefits and risks of all modes of delivery.

What is YOUR opinion???



















