Preparing a Written Report Prepared by: R Bortolussi MD FRCPC and Noni MacDonald MD FRCPC.
Upload
abby-cordingleyCategory
view
215download
5
Cervical Screening Guidelines
- for now and the future -
Meg McLachlin, MD, FRCPC
Faculty/Presenter Disclosure
• Faculty: Dr. C. McLachlin• Program: 51st Annual Scientific Assembly
• Relationships with commercial interests:– None
Disclosure of Commercial Support
• This program has received financial support from no one in the form of nothing
• This program has received in-kind support from no one in the form of nothing.
• Potential for conflict(s) of interest:– none

Mitigating Potential Bias
• None identified


Cervical Screening Guidelines - for now and the future
• Status of Cervical Screening in Ontario
• Guidelines – Context, Start, Stop and Interval
• Future Directions– Role of HPV testing

Available at www.cancercare.on.ca/ pcs/screening/cervscreening/OCSP/

Incidence rates, by age group, 1981-2007
Cancer Care Ontario (Ontario Cancer Registry, 2010).

Cervical Screening Participation Rate
Ontario Cancer Plan target 2010: 85%
2000-2002 2003-2005 2006-2008 2009-20110
10
20
30
40
50
60
70
80
90
100

Ontario Cervical Screening Program Report (2003–2008)
Other Key Messages Quality of Screening
• Unsatisfactory Pap test rate (0.5%) is much lower than in many other jurisdictions > most likely due to Ontario’s predominant use of liquid-based cytology.
Screening History • In 2008, 37.9% of women (20-69 yrs) diagnosed
with cervical cancer had not had a Pap test six months to 10 years before their diagnosis date.
What has changed?
- Recognition of the potential harms of overscreening - especially in young women
- Emerging evidence regarding the role of primary HPV testing
Potential Harms of Screening Adolescents
• High rates of low-grade, mostly transient abnormalities
• 90% will clear infection within 2 years
• Unnecessary anxiety from detection and treatment
• Treatment linked to adverse future pregnancy outcomes
• No protective effect with screening

Screening Initiation
• Start screening at age 21 for women who are or ever have been sexually active women
• Sexual activity includes intercourse, as well as digital or oral sexual activity involving the genital area with a partner of either gender.
• Women who are not sexually active by 21 years of age should delay cervical cancer screening until sexually active.
• Regardless of sexual activity, there is no evidence to support screening women under 21 years of age.

Screening Interval
• Cytology screening every 3 years
• No incremental benefit of annual cytology screening over triennial for the average risk population
• Any visual cervical abnormalities and/or abnormal symptoms must be investigated regardless of cytology findings


Screening Cessation
• Stop screening at age 70 if adequate and negative screening history (3 or more negative tests in past 10 years)
• Low incidence in women with negative history
• Potential discomfort of procedure
• Difficulties visualizing squamocolumnar junction
• Aligns with most Canadian provinces
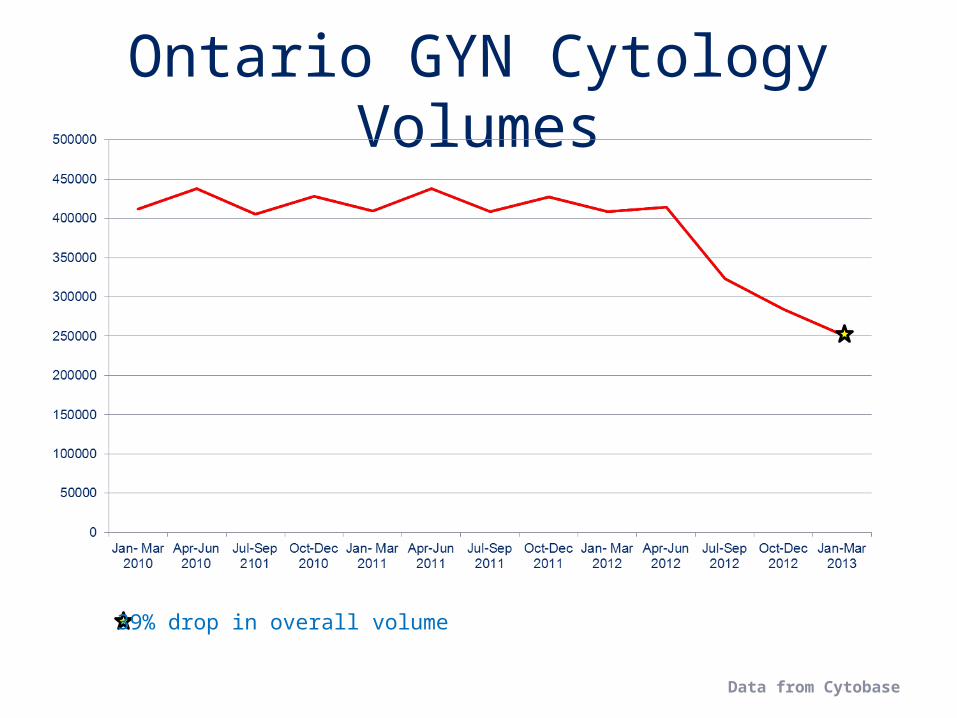
Ontario GYN Cytology Volumes
39% drop in overall volume
Data from Cytobase
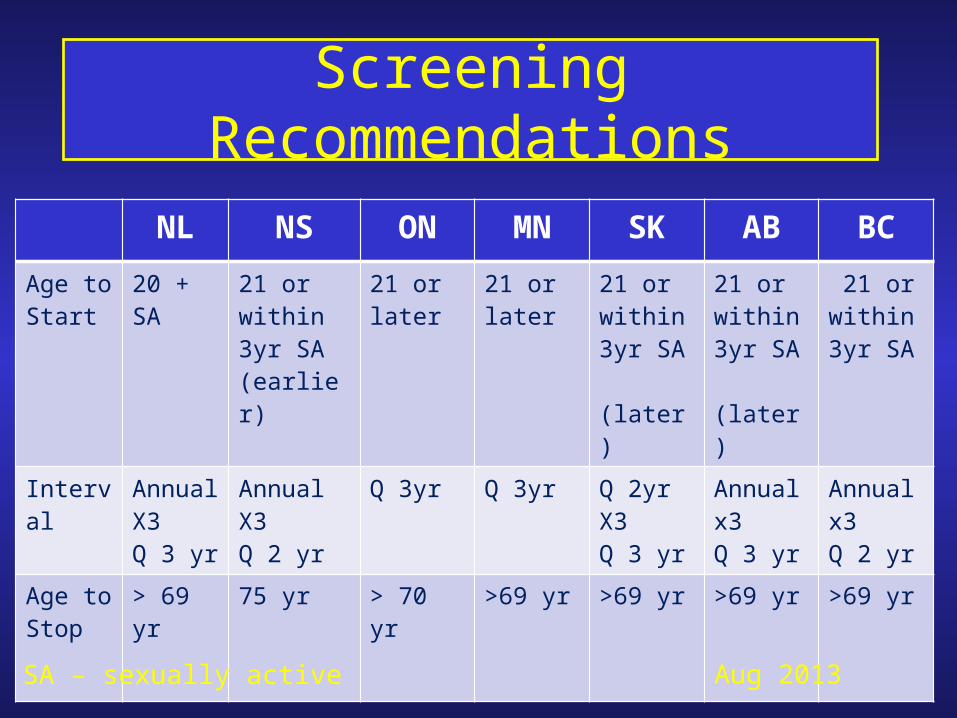
NL NS ON MN SK AB BC
Age to Start
20 + SA 21 or within 3yr SA (earlier)
21 or later
21 or later
21 or within 3yr SA (later)
21 or within 3yr SA (later)
21 or within 3yr SA
Interval Annual X3Q 3 yr
Annual X3Q 2 yr
Q 3yr Q 3yr Q 2yr X3Q 3 yr
Annual x3Q 3 yr
Annual x3Q 2 yr
Age to Stop
> 69 yr 75 yr > 70 yr >69 yr >69 yr >69 yr >69 yr
Screening Recommendations
SA – sexually active Aug 2013
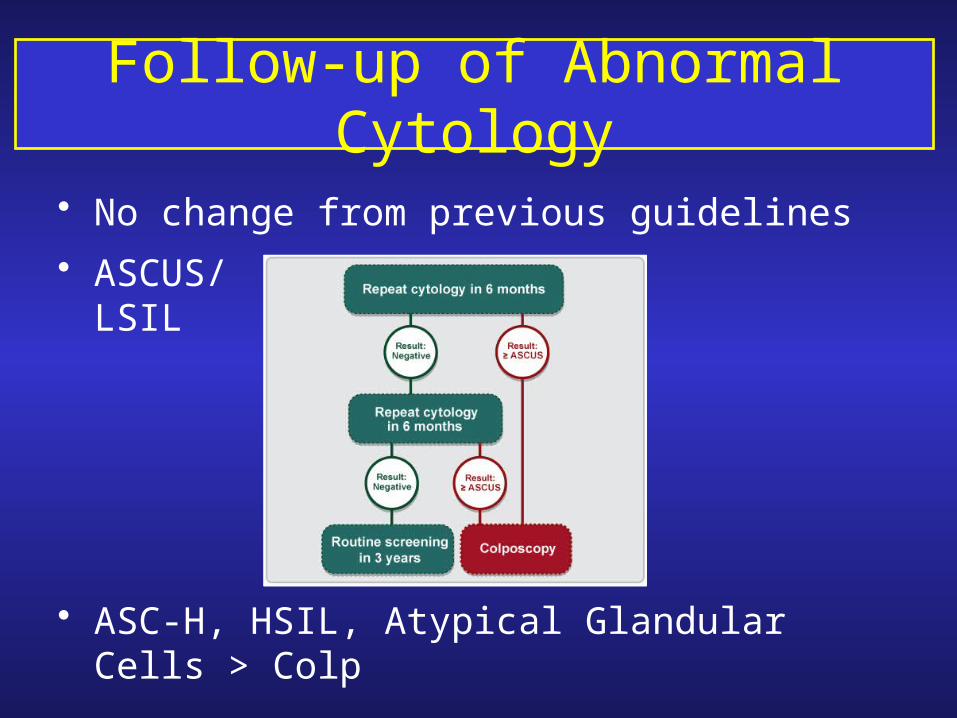
Follow-up of Abnormal Cytology
• No change from previous guidelines
• ASCUS/LSIL
• ASC-H, HSIL, Atypical Glandular Cells > Colp
Amendments to the Schedule of Benefits for Physician Services
• The cervical screening fee code (G365) has been amended to reflect CCO’s new guidelines
• Routine cervical screening is insured once every 33 months
• Payment rules for G394 (additional) have been amended to allow payment for:
follow-up of abnormal pap smear; or
inadequate pap smear; or
annually in a patient who is immunocompromised, or
a patient with a history of oncogenic HPV-typing; or
the patient is a member of a vulnerable group
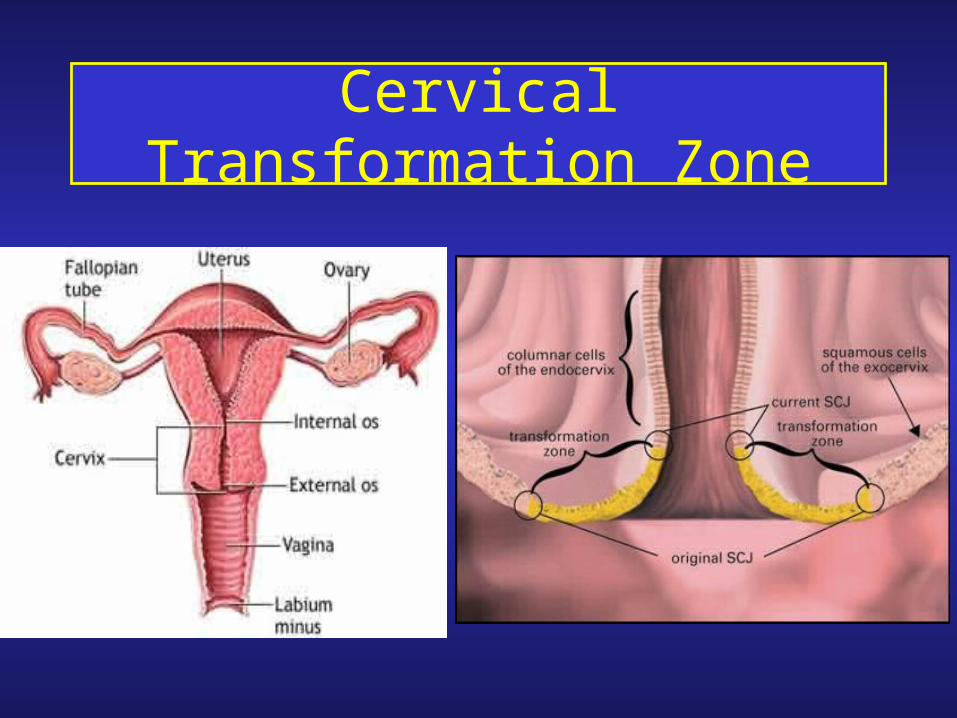
Cervical Transformation Zone

Transformation Zone
• Women whose cervical cytology is satisfactory for evaluation and negative for intraepithelial lesion or malignancy but transformation zone components are lacking should be retested at their regular screening interval. Absence of T-zone components alone does not require earlier re-screening.
• Women with abnormal cervical cytology should be managed as per guidelines regardless of the presence or absence of T zone components.
If cytology is normal, screening should be done every 3 years.
The absence of T zone is NOT a reason to repeat a Pap test earlier than the recommended interval.

Endometrial Cells
Benign Endometrial Cells
• BEC in pre-menopausal women who are asymptomatic require no action
• BEC in post-menopausal women require investigation, including adequate endometrial tissue sampling
• any woman with abnormal vaginal bleeding requires investigation, which should include endometrial tissue sampling
Recommendation:Endometrial cells in Pap tests from premenopausal women who are asymptomatic require no action. Postmenopausal women and/or women with abnormal vaginal bleeding require investigation including adequate endometrial tissue sampling.
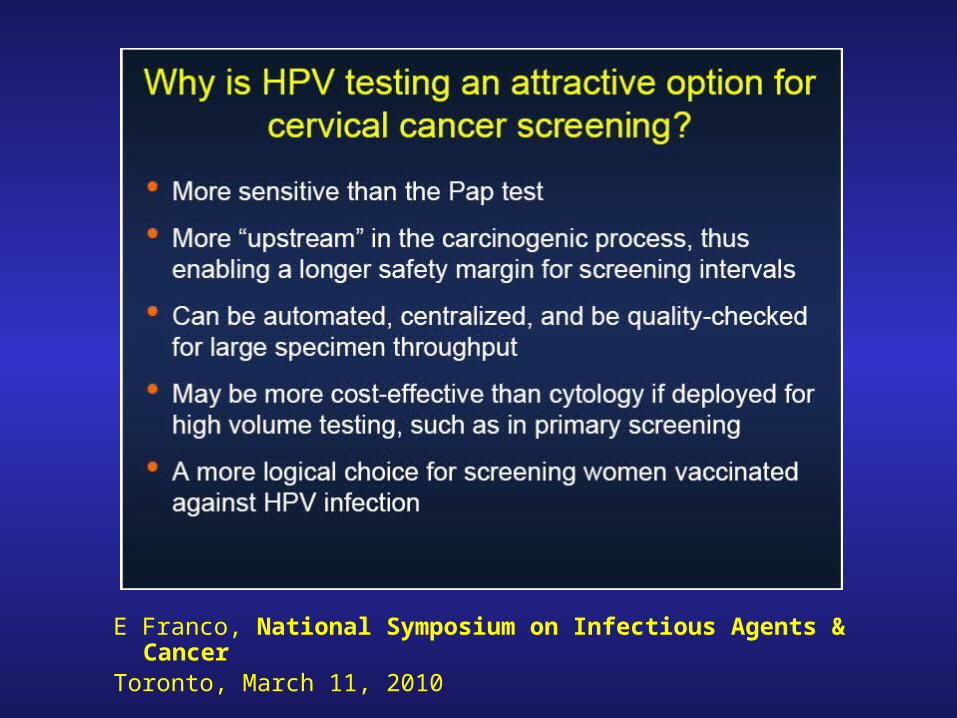
E Franco, National Symposium on Infectious Agents & CancerToronto, March 11, 2010

PositiveNegative
High risk HPV DNA testing
Repeat
HPV DNA at
X year intervals
Positive
ColposcopyRepeat hrHPV testing at 12
months
Positive Negative
Cytology
Negative
Cervical Sample (Pap)
adapted from Cuzick et al. 2008
Primary Cervical Screening with HPV testing

Organizing the Program• 1º HPV screening must be implemented
only within an organized program
• OCSP organization underway
• Prescribed registry status
• Data collection – Cytobase and health claims data
• Patient correspondence
Evidence: Correspondence• Recalls and reminders increase screening
attendance and are cost-effective
• Correspondence on abnormal test results may increase follow-up adherence
• Follow-up rates increase with personalized reminders
30

Timelines & Status Overview
31
Category Type
OCSP Timelines Status
Privacy Notice
NoticeWomen age 21-69 with a
current ResultAug 15, 2013 COMPLETE
Invitation Invitation Women age 30-69 Nov 2013 In progress
Invitation Reminder
Invitation reminders Nov 2013 In progress
Recall RecallWomen age 21-69 due
for screeningOct 2013 In progress
Recall Reminder Recall reminders Oct 2013 In progress
Result Notification
Normal Result Normal Pap test results Sept 19, 2013 On Target
Unsatisfactory Result
Unsatisfactory Pap test results
Sept 19, 2013 On Target
Abnormal ResultAbnormal Pap test
resultsSept 19, 2013 On Target
Abnormal Follow-up (Reminder)
Abnormal follow-up Nov 2013 In progress