Cerebral circulation and brain stem syndromes
31
CEREBRAL CIRCULATION AND BRAINSTEM SYNDROMES Presenter – Dr.Goutham Moderator- Dr.SRIVANI MD
-
Upload
drrudra-naresh -
Category
Health & Medicine
-
view
501 -
download
0
Transcript of Cerebral circulation and brain stem syndromes

CEREBRAL CIRCULATION AND
BRAINSTEM SYNDROMES
Presenter – Dr.GouthamModerator- Dr.SRIVANI MD

THE BRAIN
•Large mass of nervous tissue located in cranialcavity.•Has four major regions.
Cerebrum (Cerebral hemispheres)
Diencephalon: Thalamus, Hypothalamus, Subthalamus & Epithalamus
Cerebellum
Brainstem: Midbrain, Pons & Medulla oblongata

BLOOD SUPPLY OF BRAIN• Brain Receives 17% of cardiac output• Consumes 20% of entire Oxygen used by the
body• 10 seconds of interruption in blood flow leads to
unconsciousness• Most neurologic disorders are due to vascular
lesions

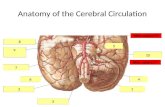
ANTERIOR AND POSTERIOR CIRCULATIONS• Anterior – Internal carotid arteries• Posterior – Vertebral arteries

ANTERIOR CIRCULATIONINTERNAL CAROTID artery Course it arises from the common carotid artery at the level of c4
vertebrae • Enters into Middle cranial fossa through carotid canal and
then enters through foramen lacerum into cavernous sinus Pierces dura and arachnoid maters.• It ends by Dividing into Anterior and Middle cerebral
arteries.

Branches of internal carotid artery1. Opthalmic artery
2. Posterior communicating artery
3. Anterior choroidal artery
4. Bifurcates into anterior cerebral artery and middle cerebral artery .

ANTERIOR CHOROIDAL ARTERY• Branch of internal carotid artery • Supplies posterior limb of internal capsule, retrolentiform and
sublentiform parts• Complete syndrome rare due to collaterals from MCA, PCA, and ICA• Syndrome comprises• c/l hemiplegia• c/l hemianaesthesia• c/l homonymous hemianopia

Anterior cerebral arterythe two anterior cerebral arteries joined together by anterior communicating artery.• Brain supplied by anterior cerebral artery Frontal poleMedial aspects of frontal and parietal lobes Basal gangliaCorpus callosum

Anterior Cerebral arteryA1 segment- proximal to anterior communicating artery it gives branches to anterior limb of internal capsule anteroinferior caudate anterior hypothalamus
A1 segment occlusion are rarely produces clinical syndrome because collateral flow through anterior communicating artery and collaterals from MCA and PCA

A2 SEGMENT• Part of anterior cerebral artery distal to anterior communicating
artery• supplies frontal pole , entire medial part of frontal and parietal lobe.
A2 SYNDROMELesion of A2 segment causes paralysis and sensory loss of C/L foot and
leg and involvement of paracentral lobule causes urinary incontinence.


MIDDLE CEREBRAL ARTERY • It arises from the internal carotid and continues into the later sulcus
where it then branches and projects to lateral cerebral cortex.

Middle cerebral ArteryM1 SEGMENT(proximal)-it gives deep penetrating or lenticulostriate branches which supplies Internal capsule, caudate nuclues, putamen and outer pallidus
M1 SYNDROME-occlusion of lenticulostriate branches-
Involvement of internal capsule produces contralateral hemiplegia.
Involvement of putamen, pallidus- leads to parkinsonian features.

Blood supply of internal capusle
Upper part ; lenticulo striate braches of MCALOWER PART : anterior chorodial artery

M2 Segment It has superior and inferior divisions supplies the entire superiolateral surface of cerebral hemispheres . Except• frontal pole• strip along the superiomedial frontal
and parietal cortex• medial temporal cortex• occipital lobe

M2 syndromes• If superior division involved• Brachial syndrome- weakness of hand and arm• Frontal opercular syndrome-Brocas aphasia with facial weakness with or without
arm weakness• proximal part of the superior division involved- clinical features of motor weakness,
sensory disturbances and brocas aphasia• If inferior division of M2 involved-• If dominant hemisphere- Wernickes aphasia without weakness with contralateral
homonymous superior quadrantanopia• If non dominant hemisphere- Hemispatial neglect , spatial agonosia without
weakness

Complete MCA syndrome• occulsion of both M1 AND M2 SEGEMENT IS COMPLETE MCA SYNDROME.
CLINICAL FEATURES • Contralateral hemiplegia• Contralateral hemianaesthesia• Contralateral homonymous hemianopia• If dominant hemisphere involved-Global aphasia• If non dominant hemisphere involved- Hemispatial neglect, and
constructional apraxia

CIRCLE OF WILLS o It is Formed by:
Two Anterior cerebral arteriesTwo Internal carotid arteriesTwo Posterior cerebral arteriesTwo Posterior communicating arteriesOne Anterior communicating artery

Branch of subclavian artery

• Structures Supplied by posterior circulation • Cerebellum• Medulla• Pons• Midbrain• Thalamus• Subthalamus• Hippocampus• Medial part of temporal lobe• Occipital lobe

Posterior cerebral artery
•P1 segment-proximal PCA supplies to - Midbrain, thalamus and subthalamus•P2 segment- distal PCA supplies to Temporal and occipital cortex.

P1 syndromes
•Due to the involvement of ipsilateral subthalamus, cerebral peduncles and midbrain

Posterior Cerebral Artery• P1 Syndromes
Syndrome Clinical features Localization
Claude’s syndrome 3rd nerve palsy contralateral ataxia
Rednucleus / cerebral peduncle
Weber’s syndrome 3rd nerve palsy hemiplegia Medial mid brain / cerebral peduncle
Benedikt’s syndrome 3rd Nerve palsy hemiplegiaAtaxia
Rednucleus / Medial mid brain
Subthalamic nucleus Contralateral hemiballismus
thalamic Déjerine-Roussy syndrome
contralateral hemisensory loss and agonizing pain
thalamus

P2 syndromes• ANTONS SYNDROME-bilateral occlusion in distal PCAs – bilateral
occipital lobe infarction- cortical blindness and patient often unaware and even deny it
• BALINTS SYNDROME-bilateral visual association areas- palinopsia and asimultagnosia

Blood supply of brain stem Structure Blood supply
Midbrain Posterior cerebral artery
Pons Basilar artery, superior cerebellar artery
Medulla Vertebral artery Posterior inferior cerebellar artery

Midbrain Syndromes

Syndrome Lesion location Structures involved Clinical features Comment
webers Midbrain base CN-3 fibers , cerebral peduncle
Ipsilateral 3-CN palsy,Contralateral hemiplegia
Usually vascular in origin
Claude’s Midbrain tegmentum
CN-3 fibers , red nucleus ,Superior cerebellar peduncle.
IpsilateraL 3-CN palsy,Rubral tremors,ContralateraL ataxia
Usually vascular in origin
Benedikt’s Midbrain tegmentum
CN-3 fibers , red nucleus ,Cerebral peduncle, Superior cerebellar peduncle
IpsilateraL 3-CN palsy, Rubral tremors,ContralateraL hemiplegia,Contralatera ataxia
Usually vascular in origin
Nothnagel’s Midbrain tectum(roof)
Ipsilateral OR BilateraL 3-CN, Superior cerebellar peduncle
3rd-CN palsy,Contralateral ataxia
Neoplastic in origin
Parineaud’s Midbrain dorsum Periaqueductal gray matter
Impaired upward gaze Usually due to mass lesion in the 3rd ventricle

Pontine syndromessyndrome Lesion
locationStructures involved Clinical features Comment
Millard-Gubler Pons Facial nerve nucleusCortico spinal tract
Ipsilateral facial nerve palsy,Contralateral hemiparesis
Usually vasucular
Foville’s Pons Facial nerve nucleusCortico spinal tractLateral gaze center
Ipsilateral facial nerve palsy,Contralateral hemiparesis,Horizontal gaze palsy.
Usually vasucular
Raymond’s Pons 6 th cranial nerve(abducence)Cortico spinal tract
Ipsilateral 6th nerve palsy,Contralateral hemiparesis,
Usually vasucular

Lateral medullary syndrome(Wallenburgs) Structure Clinical features
Spinothalamic tract Contralateral decreased pain and temperature
Spinocerebellar tract Ipsilateral ataxia
Sympathetic fibers Horners syndrome
Spinal trigeminal tract and nucleus(5th) Pain and numbness over Ipsilateral half of the face
Nucleus ambiguus Dysphagia,hoarseness
Vestibular nuclei Vertigo,nausea

Medial medullary syndromeStructure involved Clinical features
pyramid Contralateral hemiplegia
medial lemniscus contralateral loss of tactile and proprioception
hypoglossal nerve nucleus (12 th) Ipsilateral atrophy of half of tongue.

Thank u…