
CPQOL Cerebral CPQOL Palsy Cerebral Palsy Quality of Life ...

5Journal ofNeurology, Neurosurgery, and Psychiatry 1995;59:50-54
Cerebral and callosal organisation in a righthemisphere dominant "split brain" patient
Helmi L Lutsep, C Mark Wessinger, Michael S Gazzaniga
AbstractPatients described in previous reportswho have undergone corpus callosotomyfor control of seizures have been lefthemisphere dominant for language. Todetermine the hemispheric localisation(and possible coexistence) of languageand traditional right hemisphere skills inreversed dominance, the first right hemi-sphere dominant corpus callosotomypatient was studied. Localisation of cal-losal functions was also investigated, as
MRI showed 15 cm of spared callosalbody. The patient, KO, a 15 year old girlwith familial left handedness, underwenttwo stage callosotomy in 1988.Lateralised visually presented stimulirequiring same or different comparisons
between visual fields showed chance per-
formance. Oral naming and readingshowed better performance by the righthemisphere than the left, whereas bothhemispheres were proficient in auditorycomprehension. Active voice syntax was
above chance only in the right hemi-sphere. Face recognition was signifi-cantly better in the right hemispherethan in the left. Tasks requiring tactilecomparisons between hands showedabove chance performance except in theinstance in which the non-dominant righthand was stimulated first in a point local-isation task between hands. This case
showed hemispheric coexistence of lan-guage and traditional right hemisphericskills in a corpus callosotomy patient withreversed language dominance. Tactiletransfer was localised to the mid-poste-rior callosal body.
(3 Neurol Neurosurg Psychiatry 1995;59:50-54)
Center forNeuroscience,University ofCalifornia Davis,Davis, CA, USAH L LutsepC M WessingerM S GazzanigaCorrespondence to:Dr Michael S Gazzaniga,Center for Neuroscience,University of CaliforniaDavis, Davis, CA 95616,USA.
Received 15 July 1994and in final revised form28 March 1995.Accepted 30 March 1995
Keywords: corpus collosum; language; tactile recogni-tion; face recognition
The surgical corpus callosotomy procedurefor intractable epilepsy has provided a uniqueopportunity to study the functions of the indi-vidual cerebral hemispheres, and has allowedthe illucidation of the corpus callosum's rolein the interhemispheric transfer of informa-tion.' Thus far the complete callosotomy or
"split brain" patients have all been left hemi-sphere dominant for language.23 In thesepatients, visuospatial tasks, face recognition,or line orientation judgment tasks are per-
formed better by the right hemisphere.4-6 Theavailability of a callosotomy patient with righthemispheric language dominance allows us toexplore the hemispheric localisation of skillswhen dominance is reversed, and to deter-mine whether language and perceptual skillscan coexist in one hemisphere.The present case has been shown by MRI
to have 1-5 cm of callosal body remaining,allowing specific function localisation withinthe corpus callosum to be investigated.Although animal studies have shownsomatosensory interhemispheric fibres to runthrough the rostral part of the caudal half ofthe callosal body,7 in humans the transfer oftactile information has been generallylocalised by behavioural studies to the portionof corpus callosum posterior to the foramen ofMonro.8-" More precise correlations of func-tion with MRI localisation can be made in thiscase. Moreover, reports have suggested thatintegrity of tactile information transferdepends on direction,'"113 which is furtherinvestigated in this study.
In the present report, it is shown that lan-guage and perceptual skills may coexist in onehemisphere. Although both hemispheres dis-play certain language capabilities, complexgrammatical skills are localised to only onehemisphere. The mid-posterior body of thecorpus callosum is shown to be the primarysite of transfer of tactile information, andhypotheses for directional variability in tactileperformance are proposed.
Patient and methodsPATIENTThe patient, KO, a left handed girl with oneleft handed sibling, was a 15 year old highschool student at the time of testing. She dis-played infantile spasms during the first sixmonths of life. These subsided until the ageof 6 years at which time she developed star-ing spells and generalised tonic-clonic andatonic seizures. The seizures becameintractable on medical treatment. At the ageof 9 KO underwent anterior callosal section,followed eight months later by posteriorcallosotomy. Although she has developed anew seizure type consisting of unresponsive-ness and stiffening of only one side of thebody, left or right, her seizure patterns andfrequencies have not changed greatly since theoperations.
Bedside tests of disconnection showed poorverbal reporting of the right visual field during
50
group.bmj.com on March 5, 2012 - Published by jnnp.bmj.comDownloaded from
Cerebral and callosal organisation in a right hemisphere dominant "split brain" patient
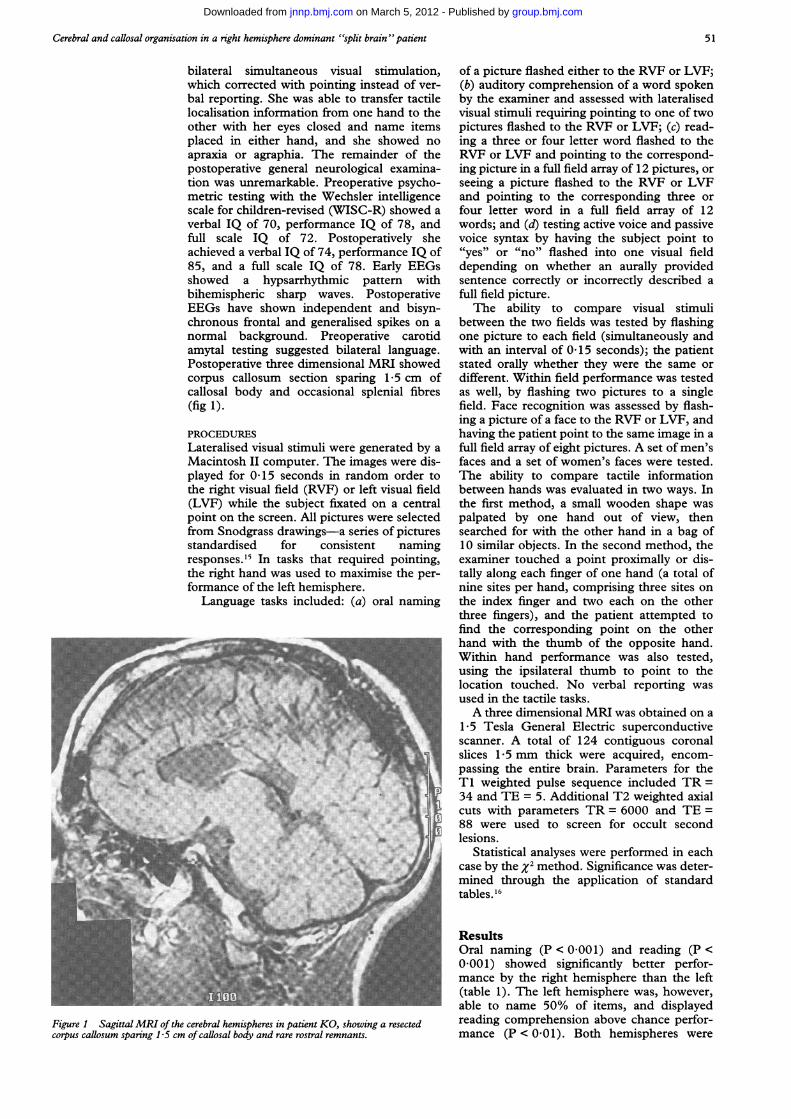
bilateral simultaneous visual stimulation,which corrected with pointing instead of ver-bal reporting. She was able to transfer tactilelocalisation information from one hand to theother with her eyes closed and name itemsplaced in either hand, and she showed noapraxia or agraphia. The remainder of thepostoperative general neurological examina-tion was unremarkable. Preoperative psycho-metric testing with the Wechsler intelligencescale for children-revised (WISC-R) showed averbal IQ of 70, performance IQ of 78, andfull scale IQ of 72. Postoperatively sheachieved a verbal IQ of 74, performance IQ of85, and a full scale IQ of 78. Early EEGsshowed a hypsarrhythmic pattern withbihemispheric sharp waves. PostoperativeEEGs have shown independent and bisyn-chronous frontal and generalised spikes on anormal background. Preoperative carotidamytal testing suggested bilateral language.Postoperative three dimensional MRI showedcorpus callosum section sparing 1-5 cm ofcallosal body and occasional splenial fibres(fig 1).
PROCEDURESLateralised visual stimuli were generated by aMacintosh II computer. The images were dis-played for 0 15 seconds in random order tothe right visual field (RVF) or left visual field(LVF) while the subject fixated on a centralpoint on the screen. All pictures were selectedfrom Snodgrass drawings-a series of picturesstandardised for consistent namingresponses.'5 In tasks that required pointing,the right hand was used to maximise the per-formance of the left hemisphere.
Language tasks included: (a) oral naming
Figure 1 SagittalMRI of the cerebral hemispheres in patient KO, showing a resectedcorpus callosum sparing 1 5 cm of callosal body and rare rostral remnants.
of a picture flashed either to the RVF or LVF;(b) auditory comprehension of a word spokenby the examiner and assessed with lateralisedvisual stimuli requiring pointing to one of twopictures flashed to the RVF or LVF; (c) read-ing a three or four letter word flashed to theRVF or LVF and pointing to the correspond-ing picture in a full field array of 12 pictures, orseeing a picture flashed to the RVF or LVFand pointing to the corresponding three orfour letter word in a full field array of 12words; and (d) testing active voice and passivevoice syntax by having the subject point to"yes" or "no" flashed into one visual fielddepending on whether an aurally providedsentence correctly or incorrectly described afull field picture.The ability to compare visual stimuli
between the two fields was tested by flashingone picture to each field (simultaneously andwith an interval of 0-15 seconds); the patientstated orally whether they were the same ordifferent. Within field performance was testedas well, by flashing two pictures to a singlefield. Face recognition was assessed by flash-ing a picture of a face to the RVF or LVF, andhaving the patient point to the same image in afull field array of eight pictures. A set of men'sfaces and a set of women's faces were tested.The ability to compare tactile informationbetween hands was evaluated in two ways. Inthe first method, a small wooden shape waspalpated by one hand out of view, thensearched for with the other hand in a bag of10 similar objects. In the second method, theexaminer touched a point proximally or dis-tally along each finger of one hand (a total ofnine sites per hand, comprising three sites onthe index finger and two each on the otherthree fingers), and the patient attempted tofind the corresponding point on the otherhand with the thumb of the opposite hand.Within hand performance was also tested,using the ipsilateral thumb to point to thelocation touched. No verbal reporting wasused in the tactile tasks.A three dimensional MRI was obtained on a
1.5 Tesla General Electric superconductivescanner. A total of 124 contiguous coronalslices 1-5 mm thick were acquired, encom-passing the entire brain. Parameters for theTi weighted pulse sequence included TR =34 and TE = 5. Additional T2 weighted axialcuts with parameters TR = 6000 and TE =88 were used to screen for occult secondlesions.
Statistical analyses were performed in eachcase by the x2 method. Significance was deter-mined through the application of standardtables. 16
ResultsOral naming (P < 0.001) and reading (P <0-001) showed significantly better perfor-mance by the right hemisphere than the left(table 1). The left hemisphere was, however,able to name 50% of items, and displayedreading comprehension above chance perfor-mance (P < 0-01). Both hemispheres were
51
group.bmj.com on March 5, 2012 - Published by jnnp.bmj.comDownloaded from

Lutsep, Wessinger, Gazzaniga
Table 1 Language results
RVFv RVFv LVFvRVF LVF LVF chance chance
Oral naming 18/36 35/36 P < 0001ReadingWord flashed, point picture 6/12 11/12Picture flashed, point word 4/12 10/12Total 10/24 21/24 P < 0-001 P < 0-01 P < 0-001
Auditory comprehension 33/36 36/36 NS P < 0-001 P < 0-001Active voice syntax 31/48 38/48 NS NS P < 0 005Passive voice syntax 12/24 15/24 NS NS NS
RVF = Right visual field; LVF = left visual field. Chance performance could not be determinedfor the oral naming and reading tasks. Chance was 18/36 for auditory comprehension; 24/48 foractive voice syntax; and 12/24 for passive voice syntax.
Table 2 Perceptual task results
Bilateral v RVF vRVF LVF Bilateral chance LVF
Picture comparisonNon-simultaneous 30/32 32/32 22/32 NS NSSimultaneous 15/16 16/16 8/16 NS NS
Face recognition 6/32 20/32 P < 0-001
RVF = Right visual field; LVF = left visual field. Chance performance was 16/32 for the non-simultaneous and 8/16 for the simultaneous picture comparison tasks; for the face recognitiontask chance was 4/32.
proficient in auditory comprehension of singlewords (P < 0-001). Active voice syntax(P < 0 005) was above chance only in theright hemisphere. Passive voice syntax taskscould not be mastered even after multiplepractice trials and full field training, renderingcomparisons of the two hemispheres unhelp-ful in this condition.
Face recognition was significantly better inthe right hemisphere than the left (P < 0-001;table 2). Tasks requiring picture same or dif-ferent comparisons between visual fieldsshowed chance performance (P > 0-10).
Tactile object comparison tasks betweenhands showed above chance performance ineach direction (P < 0-001; table 3). In thepoint matching task between hands, stimula-tion of the left hand and finding the corre-sponding point with the right showed abovechance performance (P < 0.005); stimulationof the right hand and matching with the leftshowed chance performance. There was nosignificant difference between the two direc-tional conditions of point matching. Withinhand performance was above chance in eachhand (P < 0-001), although more accuratewithin the left hand.
DiscussionThe language data (oral naming, auditorycomprehension, reading, and active voice syn-tax) indicate that patient KO is right hemi-sphere dominant for language. Although theleft hemisphere seems to have some capabilityfor speech production and comprehension,
only the dominant right hemisphere performsactive voice syntax. Face recognition is alsosignificantly better in the right hemisphere.Between field picture comparisons showvisual disconnection. Most of the betweenhand tactile comparisons (object comparisonsand point matching) do not show tactile dis-connection, although performance deterio-rates in the case in which the right hand isstimulated and the left hand finds the corre-
sponding point of stimulation.This and previous studies suggest that
unlike other language functions, complexgrammar skills are localised to only one hemi-sphere. Whereas callosotomy patients LB andNG have shown comprehension for nouns
and the affirmative or negative distinctionwith their non-dominant right hemispheres,active, passive, and future tenses as well as
plurals are not recognised.17 Callosotomypatients VP and JW both have complex righthemisphere lexicons, and VP's right hemi-sphere is also able to carry out verbal com-
mands and access speech."' 19 On the otherhand VP's right hemisphere is not able to per-
form the active and passive sentence taskdescribed in this paper, and JW's right hemi-sphere achieves an above chance performanceonly in the active condition.20 As in VP, thepresent case illustrates the ability of the non-
dominant, in this case left, hemisphere toaccess speech and to comprehend singlewords. Moreover, whereas the dominanthemisphere performs the active sentencegrammar task, the non-dominant hemispheredoes not. The non-redundant, fundamentalnature of grammar is further supported bytantalising evidence of its genetic inheritabil-ity, provided by the discovery of an autosomaldominant pattern of inheritance in a familywith poor grammar but otherwise generallyintact language functions.2' 22 Left hemidecor-tication also results in a deficiency in manipu-lation of grammatical structure by the isolatedright hemisphere, which shows basic lexicalcapabilities.23 Comprehension of passive nega-tive constructions, as well as use of morpho-logical markers and other grammaticalstructures, are impaired in hemidecorticationpatients. Performance on passives may, how-ever, be a misleading measure of linguisticcapabilities, as chance performance on
reversible passives in neurologically intactadolescents has been shown to be associatedwith low mental age to the degree seen inpatient KO.24 The chance performance ofboth of her hemispheres on this task is thusnot surprising.
It is of interest to learn whether cognitivefunctions characteristically associated with thenon-dominant hemisphere in patients with
Table 3 Tactile task results
Within Within Stimulate L, L- > R v Stimulate R, R- > L vR hand L hand find R chance find L chance
Object comparison 3/3 3/3 9/10 P < 0 001 10/10 P < 0 001Point matching 13/18 18/18 10/18 P < 0 005 6/18 NS
R = Right; L = left. Chance performance for the object comparison task was 1/10; for the point matching task, chance was 2/18.
52
group.bmj.com on March 5, 2012 - Published by jnnp.bmj.comDownloaded from
Cerebral and callosal organisation in a right hemisphere dominant "split brain" patient
left hemisphere language reside in the non-dominant hemisphere in right language domi-nant subjects as well. A left handed patientwith posterior section of the corpus callosumfor tumour of the third ventricle displayedlanguage in the right hemisphere and visu-ospatial drawing abilities in the left hemi-sphere.10 Although limited by the inability toconfirm all lesion locations with modem brainscanning capabilities, Hecaen et al, however,found a right hemispheric lesion dependencefor production of spatial function deficits aswell as cerebral ambilaterality of language rep-resentations in left handers with familial sinis-trality.2' Interestingly, in non-familial lefthanders, lesions causing spatial functiondeficits were not right hemisphere dependent.Patient KO has a clear right hemisphericsuperiority for face recognition, a traditionalright hemispheric specialised skill,6 whichplaces this function in her dominant (right)hemisphere along with language. Thus itseems that, especially in those subjects withfamilial left handedness, language and percep-tual skills may reside in the same hemisphere.Geschwind and Galaburda26 have suggestedthat certain right hemispheric skills rarely shiftto the left because the right hemisphere devel-ops earlier in utero. The right hemisphericfunctions may then be joined by language,which is more flexibly lateralised." Studies inhemidecorticated patients also provide evi-dence that language and visuospatial func-tions may coexist in the isolated righthemisphere.23 Likewise, only one of four stud-ied patients with right hemidecortication afterdisease acquired in childhood or later showed
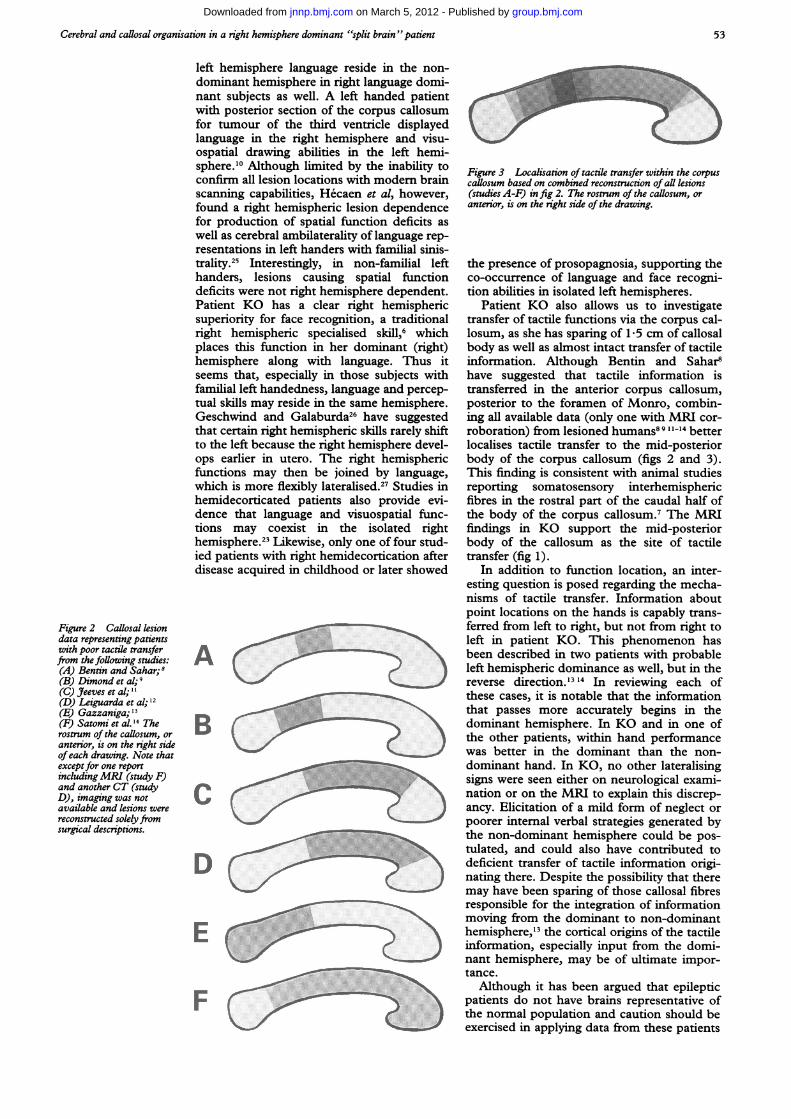
Figure 2 Callosal lesiondata representing patientswith poor tactile transferfrom thefoUowing studies:(A) Bentin and Sahar; 8(B) Dimond et al; 9(C) Jeeves et al; 11(D) Leiguarda et al;'2(E) Gazzaniga;"I(F) Satomi et al. 14 Therostrum of the callosum, oranterior, is on the right sideofeach drawing. Note thatexceptfor one reportincludingMRI (study F)and another CT (studyD), imaging was notavailable and lesions werereconstructed solelyfromsurgical descriptions.
A
B
C
D
E
F
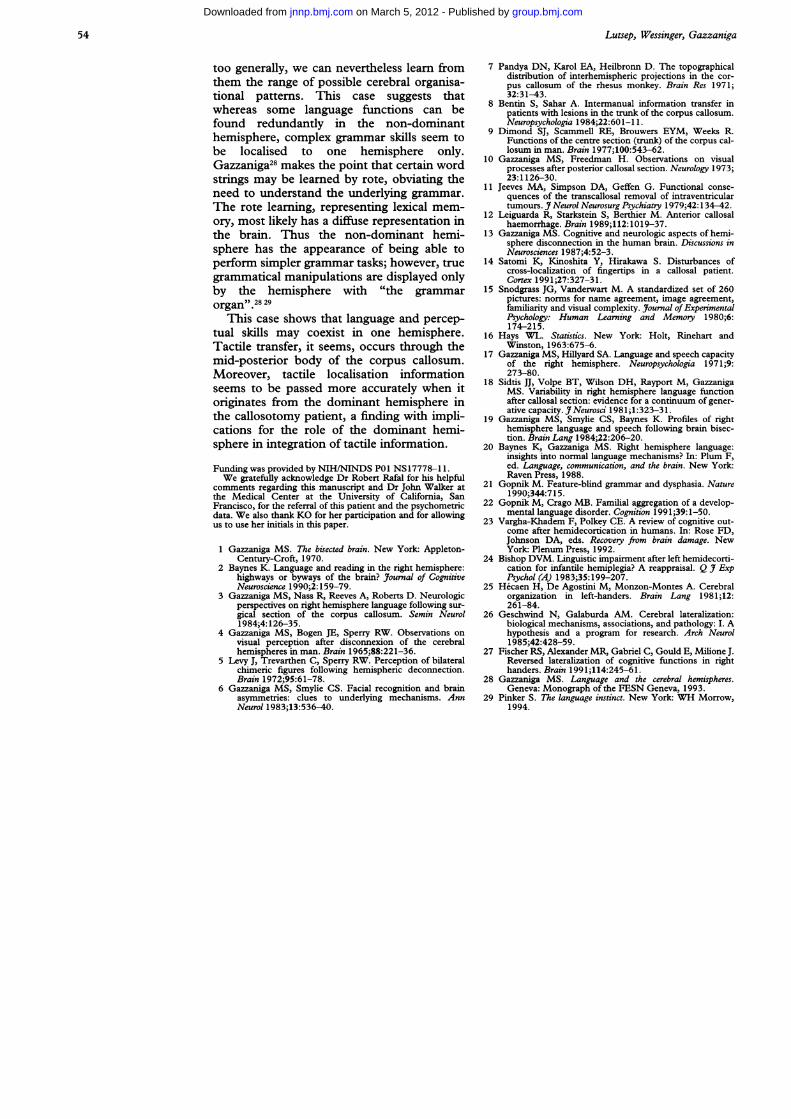
Figure 3 Localisation of tactile transfer within the corpuscallosum based on combined reconstruction of all lesions(studies A-F) infig 2. The rostrum of the caflosum, oranterior, is on the right side of the drawing.
the presence of prosopagnosia, supporting theco-occurrence of language and face recogni-tion abilities in isolated left hemispheres.
Patient KO also allows us to investigatetransfer of tactile functions via the corpus cal-losum, as she has sparing of 1-5 cm of callosalbody as well as almost intact transfer of tactileinformation. Although Bentin and Sahar8have suggested that tactile information istransferred in the anterior corpus callosum,posterior to the foramen of Monro, combin-ing all available data (only one with MRI cor-roboration) from lesioned humans8 9 11-14 betterlocalises tactile transfer to the mid-posteriorbody of the corpus callosum (figs 2 and 3).This finding is consistent with animal studiesreporting somatosensory interhemisphericfibres in the rostral part of the caudal half ofthe body of the corpus callosum.7 The MRIfindings in KO support the mid-posteriorbody of the callosum as the site of tactiletransfer (fig 1).
In addition to function location, an inter-esting question is posed regarding the mecha-nisms of tactile transfer. Information aboutpoint locations on the hands is capably trans-ferred from left to right, but not from right toleft in patient KO. This phenomenon hasbeen described in two patients with probableleft hemispheric dominance as well, but in thereverse direction.'3 14 In reviewing each ofthese cases, it is notable that the informationthat passes more accurately begins in thedominant hemisphere. In KO and in one ofthe other patients, within hand performancewas better in the dominant than the non-dominant hand. In KO, no other lateralisingsigns were seen either on neurological exami-nation or on the MRI to explain this discrep-ancy. Elicitation of a mild form of neglect orpoorer internal verbal strategies generated bythe non-dominant hemisphere could be pos-tulated, and could also have contributed todeficient transfer of tactile information origi-nating there. Despite the possibility that theremay have been sparing of those callosal fibresresponsible for the integration of informationmoving from the dominant to non-dominanthemisphere," the cortical origins of the tactileinformation, especially input from the domi-nant hemisphere, may be of ultimate impor-tance.
Although it has been argued that epilepticpatients do not have brains representative ofthe normal population and caution should beexercised in applying data from these patients
53
group.bmj.com on March 5, 2012 - Published by jnnp.bmj.comDownloaded from
Lutsep, Wessinger, Gazzaniga
too generally, we can nevertheless learn fromthem the range of possible cerebral organisa-tional patterns. This case suggests thatwhereas some language functions can befound redundantly in the non-dominanthemisphere, complex grammar skills seem tobe localised to one hemisphere only.Gazzaniga28 makes the point that certain wordstrings may be learned by rote, obviating theneed to understand the underlying grammar.The rote learning, representing lexical mem-ory, most likely has a diffuse representation inthe brain. Thus the non-dominant hemi-sphere has the appearance of being able toperform simpler grammar tasks; however, truegrammatical manipulations are displayed onlyby the hemisphere with "the grammarorgan" 28 29
This case shows that language and percep-tual skills may coexist in one hemisphere.Tactile transfer, it seems, occurs through themid-posterior body of the corpus callosum.Moreover, tactile localisation informationseems to be passed more accurately when itoriginates from the dominant hemisphere inthe callosotomy patient, a finding with impli-cations for the role of the dominant hemi-sphere in integration of tactile information.
Funding was provided by NIH/NINDS P01 NS17778-1 1.We gratefully acknowledge Dr Robert Rafal for his helpful
comments regarding this manuscript and Dr John Walker atthe Medical Center at the University of California, SanFrancisco, for the referral of this patient and the psychometricdata. We also thank KO for her participation and for allowingus to use her initials in this paper.
1 Gazzaniga MS. The bisected brain. New York: Appleton-Century-Croft, 1970.
2 Baynes K. Language and reading in the right hemisphere:highways or byways of the brain? Journal of CognitiveNeuroscience 1990;2:159-79.
3 Gazzaniga MS, Nass R, Reeves A, Roberts D. Neurologicperspectives on right hemisphere language following sur-gical section of the corpus callosum. Semin Neurol1984;4: 126-35.
4 Gazzaniga MS, Bogen JE, Sperry RW. Observations onvisual perception after disconnexion of the cerebralhemispheres in man. Brain 1965;88:221-36.
5 Levy J, Trevarthen C, Sperry RW. Perception of bilateralchimeric figures following hemispheric deconnection.Brain 1972;95:61-78.
6 Gazzaniga MS, Smylie CS. Facial recognition and brainasymmetries: clues to underlying mechanisms. AnnNeurol 1983;13:536-40.
7 Pandya DN, Karol EA, Heilbronn D. The topographicaldistribution of interhemispheric projections in the cor-pus callosum of the rhesus monkey. Brain Res 1971;32:31-43.
8 Bentin S, Sahar A. Intermanual information transfer inpatients with lesions in the trunk of the corpus callosum.Neuropsychologia 1984;22:601-1 1.
9 Dimond SJ, Scammell RE, Brouwers EYM, Weeks R.Functions of the centre section (trunk) of the corpus cal-losum in man. Brain 1977;100:543-62.
10 Gazzaniga MS, Freedman H. Observations on visualprocesses after posterior callosal section. Neurology 1973;23:1126-30.
11 Jeeves MA, Simpson DA, Geffen G. Functional conse-quences of the transcallosal removal of intraventriculartumours. J Neurol Neurosurg Psychiatry 1979;42: 134-42.
12 Leiguarda R, Starkstein S, Berthier M. Anterior callosalhaemorrhage. Brain 1989;112:1019-37.
13 Gazzaniga MS. Cognitive and neurologic aspects of hemi-sphere disconnection in the human brain. Discussions inNeurosciences 1987;4:52-3.
14 Satomi K, Kinoshita Y, Hirakawa S. Disturbances ofcross-localization of fingertips in a callosal patient.Cortex 1991;27:327-31.
15 Snodgrass JG, Vanderwart M. A standardized set of 260pictures: nonns for name agreement, image agreement,familiarity and visual complexity. Journal of ExperimentalPsychology: Human Learning and Memory 1980;6:174-215.
16 Hays WL. Statistics. New York: Holt, Rinehart andWinston, 1963:675-6.
17 Gazzaniga MS, Hillyard SA. Language and speech capacityof the right hemisphere. Neuropsychologia 1971 ;9:273-80.
18 Sidtis JJ, Volpe BT, Wilson DH, Rayport M, GazzanigaMS. Variability in right hemisphere language functionafter callosal section: evidence for a continuum of gener-ative capacity. JNeurosci 1981;1:323-31.
19 Gazzaniga MS, Smylie CS, Baynes K. Profiles of righthemisphere language and speech following brain bisec-tion. Brain Lang 1984;22:206-20.
20 Baynes K, Gazzaniga MS. Right hemisphere language:insights into normal language mechanisms? In: Plum F,ed. Language, communication, and the brain. New York:Raven Press, 1988.
21 Gopnik M. Feature-blind grammar and dysphasia. Nature1990;344:715.
22 Gopnik M, Crago MB. Familial aggregation of a develop-mental language disorder. Cognition 1991;39:1-50.
23 Vargha-Khadem F, Polkey CE. A review of cognitive out-come after hemidecortication in humans. In: Rose FD,Johnson DA, eds. Recovery from brain damage. NewYork: Plenum Press, 1992.
24 Bishop DVM. Linguistic impairment after left hemidecorti-cation for infantile hemiplegia? A reappraisal. Q J ExpPsychol (A) 1983;35:199-207.
25 Hecaen H, De Agostini M, Monzon-Montes A. Cerebralorganization in left-handers. Brain Lang 1981;12:261-84.
26 Geschwind N, Galaburda AM. Cerebral lateralization:biological mechanisms, associations, and pathology: I. Ahypothesis and a program for research. Arch Neurol1985;42:428-59.
27 Fischer RS, Alexander MR, Gabriel C, Gould E, Milione J.Reversed lateralization of cognitive functions in righthanders. Brain 1991;114:245-61.
28 Gazzaniga MS. Language and the cerebral hemispheres.Geneva: Monograph of the FESN Geneva, 1993.
29 Pinker S. The language instinct. New York: WH Morrow,1994.
54
group.bmj.com on March 5, 2012 - Published by jnnp.bmj.comDownloaded from
doi: 10.1136/jnnp.59.1.50 1995 59: 50-54J Neurol Neurosurg Psychiatry
H L Lutsep, C M Wessinger and M S Gazzaniga hemisphere dominant "split brain" patient.Cerebral and callosal organisation in a right
http://jnnp.bmj.com/content/59/1/50Updated information and services can be found at:
These include:
References http://jnnp.bmj.com/content/59/1/50#related-urls
Article cited in:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on March 5, 2012 - Published by jnnp.bmj.comDownloaded from


















