
Centers for Disease Control and Prevention Global AIDS Program Prevention Interventions for People...
40
Centers for Disease Control and Prevention Global AIDS Program Prevention Interventions for People Living with HIV: 5 HIV Prevention Steps and Tools for Implementation Pamela Bachanas, PhD Washington, DC August, 2008
-
date post
20-Dec-2015 -
Category
Documents
-
view
229 -
download
0
Transcript of Centers for Disease Control and Prevention Global AIDS Program Prevention Interventions for People...

Centers for Disease Control and PreventionGlobal AIDS Program
Prevention Interventions for People Living with HIV: 5 HIV Prevention
Steps and Tools for Implementation
Pamela Bachanas, PhDWashington, DC
August, 2008
Prevention for People Living with HIV
• Scale up of care and treatment programs in SSA have been an extraordinary success – 2.5 million people on ARVs
• However, in 2007 alone, 2.5 million people were newly infected with HIV, most of whom will eventually need ARVs
• Effective and efficient HIV prevention interventions are critically needed

Prevention for People Living with HIV
• Traditional focus of prevention efforts have been on preventing acquisition among HIV- individuals
• To have a significant impact on slowing the spread of the epidemic, prevention efforts must also be directed toward individuals living with HIV who can transmit the virus

HIV prevalence, Kenya, 2006
HIV negative, 94%
HIV positive, 6%
Only HIV+ individuals can transmit HIV
►Focusing on ~1.3m HIV-infected people rather than ~21.6m uninfected people is an efficient, targeted prevention approach
HIV Prevention in Care and Treatment
• Due to increasing availability of HIV treatment, many HIV+ persons are accessing health care settings and clinics, providing an opportunity to reach a large number of infected persons with prevention messages and interventions
• Health care providers in HIV clinic settings meet with patients regularly and can deliver consistent, targeted prevention messages and strategies during routine visits
• Providers are considered authority figures and trusted sources of health information

HIV Prevention in Care and Treatment
• For any disease, preventive information on infection control is regarded as quality standard of care
• Health care providers can also address biomedical prevention strategies, such as reproductive health and STI management
• Given clinic burden and complexity of patients’ needs, many patients need more in-depth counseling on prevention issues (e.g. disclosure, alcohol use). Incorporating counselors (including PLWHA) into clinic settings is essential for a comprehensive prevention program

Prevention for People Living with HIV
• Multiple approaches to prevention are needed; integration of prevention into care and treatment settings is critical
• Integrating prevention services into care and treatment can be overwhelming and can require a great deal of effort and resources
• However, we can’t afford not to do it
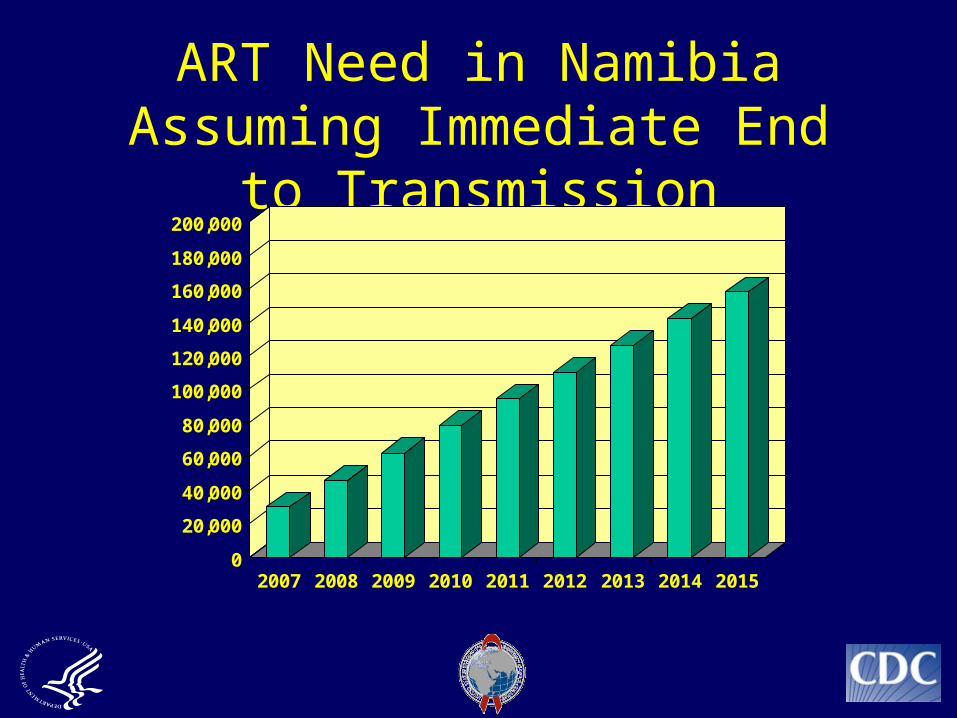
ART Need in Namibia Assuming Immediate End to Transmission
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
200,000
2007 2008 2009 2010 2011 2012 2013 2014 2015

ART Need in Namibia Assuming Ongoing Transmission
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
2007 2008 2009 2010 2011 2012 2013 2014 2015

Prevention for People Living with HIV
• The question isn’t can we do prevention in care and treatment…
• The question is how do we do prevention in care and treatment…
– What are the specific interventions– How can they be implemented most efficiently
(task shifting, etc,)

Step 1 – Give prevention recommendations to every
patient at every visit

Critical Need for Prevention Interventions with PLWHA
• Vast majority of PLWHA are married in Kenya (70%), Malawi (82%), & Uganda (57%) [DHS & AIS data]
• Rates of partner testing among PLWHA very low
• Rates of disclosure of serostatus to partner(s) low and challenging
• Condom use in stable relationships very low

HIV status of spouses of HIV-infected persons in Kenya, DHS,
2003
►In Kenya, 50% of married HIV+ persons (450,000) have an HIV-negative spouse
HIV DISCORDANT:
One partner positive, one partner negative: 50%CONCORDANT POSITIVE:
Both partners HIV-infected: 50%

38%
13%
49%
Spouse with long-standing infection
Spouse withrecent infection
Spouse wasuninfected
Nature of Incident Infection, Uganda Sero-behavioral Survey, 2004-5
Note: among 79 couples

CONDOM USE IN REGULAR PARTNERSHIPS

Discordant Couple Interventions:Couple Counseling and Testing
963 discordant couples in Lusaka (Allen et al., 2003)
53 discordant couples in Kigali (Allen et al., 1992)
149 discordant couples in Kinshasa (Kamenga et al., 1991)
Self-reported condom use increased from 3% to 80% after 1 year
Self-reported condom use increased from 4% to 57% after 1 year
Self-reported condom use increased from <5% to 77% after 1 year

Step 1 – Give prevention recommendations to every patient
at every visit• Providers and counselors must assess
whether each patient’s partner has been tested; test or refer to counselor for testing
• Provider- and/or counselor-assisted disclosure
• Counselor who can conduct rapid testing available in clinic and community settings
• Children of HIV+ moms tested

Step 1 – Give prevention recommendations to every patient
at every visit
• Discordant couples identified and counseled– Positive partners linked to care and treatment– Negative partners counseled on prevention practices to stay
negative (condoms!)
• Provider delivers brief messages on patient self-protection & partner protection– Consequences of unprotected sex
• Provider assesses patient for alcohol use that affects adherence or risky behavior– Refer drinkers to counselor

HIV Acquisition among Male Partners of HIV + Female Partners By Circumcision
Status In Rakai
0
8.2
0
27.7
0
27.7
0
5
10
15
20
25
30
Acq
uis
itio
n/1
00p
y
<10,000 10,000-49,999 >50,000
CircumcisedUncircumcised
Female viral loadQuinn et al; NEJM 2000; 342:921-9

Step 2 – Assess adherence to ARVs
• Provide adherence support or refer to counselor for support

Step 3 – STI Management Integrated into HIV Clinics
STI Management Integrated into HIV Care
• In HIV+ individuals, STIs have been shown to increase genital HIV shedding, increasing likelihood of HIV transmission.
• STIs have been associated with increased genital HIV shedding in persons on ARVs with suppressed plasma viral loads.
• Genital ulcer disease has the strongest association with HIV transmission; high rates of HIV/HSV co-infection.
• Urethritis, vaginitis, and bacterial vaginosis have also been associated with transmission and acqusition.

STI Management Integrated into HIV Care
• Assess for signs and symptoms of STIs at every visit and treat as indicated
• Treating STIs in HIV+ persons is important for care, as STIs can be more severe and more difficult to treat in immunocompromised individuals
• Treating STIs in HIV+ persons is important for prevention; may reduce chances of transmission of HIV
• Treating partners of patients with STIs may reduce reinfection and stop the spread of the STI

Step 4 - Family Planning Services and Safer Pregnancy Counseling in
Care and Treatment (through Wrap-Around Programs)

Family Planning
• Many women on ARVs resume sexual activity and have unintended pregnancies (Bunnell et al., 2006)
• Preventing unintended pregnancy in HIV+ women who do not want children can avert the need for and costs associated with (Sweat et al., 2004)– PMTCT– care for HIV+ children – support for orphans
• Other HIV+ women on treatment desire children (Nakayiwa et al., 2006); they require counseling on safe timing of pregnancy and referrals to PMTCT

Unmet need for family planning among HIV-infected women (Bunnell, 2007)
Kenya Malawi Uganda
Last pregnancy unplanned/unwanted
54% 40% 49%
HIV-infected women who do not want more children
41% 50%
-Unmet need for contraception among those who do not want more children
64%
79%
-

Step 4 – Assess pregnancy status & intentions
• Inquire about pregnancy status/intentions every visit
Through wrap-around funding:• Provide basic contraceptives in HIV clinic (pills,
injectables) and refer to FP for other contraceptives
• Provide basic counseling on safer conception, pregnancy, and delivery for HIV+ women desiring pregnancy in the HIV care and treatment setting

Step 5 – Give patient condoms at every visit!!

Lay Counselors in Care and Treatment Clinics

Lay Counselors
• Given clinic burden and complexity of patients’ needs, many patients need more in-depth counseling on prevention issues than providers can manage
• Task shifting some responsibilities to lay counselors may be a cost-effective and supportive way to meet clinic and patient needs for services
• Training lay counselors to expand and reinforce prevention messages delivered by providers and to provide more in-depth counseling on specific prevention issues is critical for prevention efforts

HIV Prevention for People Living with HIV/AIDS: An Intervention Toolkit for HIV Care and Treatment Settings
Overhead 5-10

The 5 HIV Prevention Steps Intervention
• 1-day Provider Training– Sensitizes providers to their
critical role in influencing patients’ risk behaviors
– Teaches them skills for delivering behavioral prevention messages
– Provides overview and rationale for biomedical interventions
– Allows providers to practice delivering prevention messages to patients

Family Planning and Safer Pregnancy Counseling
• 2 day provider training• Trains providers to integrate FP services into
routine care and treatment of HIV+ women and partners of male patients
• Pills, injectables• Safer pregnancy counseling• Flip chart for health care providers – technical
resource

Management of Sexually Transmitted Infections in People
Living with HIV/AIDS• 2 day provider training
• Management of STIs in PLWHA as part of routine care– Assessment questions, exams, syndromic
management
• Partner management

HIV Prevention and Adherence Counseling for PLWHA
• 2 week training on prevention and adherence counseling for lay counselors (many of whom are PLWHA)
• 2 week training on counseling and testing for lay counselors (where permitted by national guidelines
• Flip chart for group education on prevention and adherence topics
• Individual counseling guide

Prevention for People Living with HIV in Care and Treatment Settings
• Kenya• Namibia• Nigeria• Haiti• Ethiopia
• Tanzania• Rwanda• Cote d’ Ivoire• Botswana• South Africa (?)

Preventionfor PLWHA
PMTCT/ANC
Primary Care
CCCFamily Planning
Integrating HIV Prevention into Integrating HIV Prevention into Clinic SettingsClinic Settings
TB
Male Circumcision
Testing and counseling
Preventionfor PLWHA
Community counseling centers
Community Health Workers
VCTPLWHA support
networks
Integrating HIV Prevention into Integrating HIV Prevention into Community SettingsCommunity Settings
FBO servicesHome-based
Care

Thank you!

Discussion Questions
• How can Track 1 partners assist MOH and USG in developing and scaling up national programs?
• How can Track 1 partners strengthen role as technical leaders and TA providers in this area?
• How can efforts be coordinated to reduce duplication of program development and increase implementation efforts?
• What are challenges and barriers to implementation and scale-up?


















