Cellular responses to amyloid-beta protofibrils
72
ACTA UNIVERSITATIS UPSALIENSIS UPPSALA 2018 Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1405 Cellular responses to amyloid-beta protofibrils Focus on astrocytes, extracellular vesicles and antibody treatment ELISABETH NIKITIDOU ISSN 1651-6206 ISBN 978-91-513-0173-0 urn:nbn:se:uu:diva-334358
Transcript of Cellular responses to amyloid-beta protofibrils

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2018
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1405
Cellular responses to amyloid-betaprotofibrils
Focus on astrocytes, extracellular vesicles andantibody treatment
ELISABETH NIKITIDOU
ISSN 1651-6206ISBN 978-91-513-0173-0urn:nbn:se:uu:diva-334358

Dissertation presented at Uppsala University to be publicly examined in Rudbecksalen,Rudbecklaboratoriet, Dag Hammarskjölds väg 20, Uppsala, Friday, 9 February 2018 at09:15 for the degree of Doctor of Philosophy. The examination will be conducted in English.Faculty examiner: Professor Gunnar K. Gouras (Department of Experimental MedicalScience, Lund University).
AbstractNikitidou, E. 2018. Cellular responses to amyloid-beta protofibrils. Focus on astrocytes,extracellular vesicles and antibody treatment. Digital Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine 1405. 70 pp. Uppsala: Acta UniversitatisUpsaliensis. ISBN 978-91-513-0173-0.
Knowledge about the cellular mechanisms behind the initiation and propagation of Alzheimer’sdisease (AD) is limited. Decades of research have focused on neuronal abnormalities in AD,but recently more attention has been given to the glial cells. Being the most numerous glial celltype in the brain, astrocytes are important for many functions, but their role in AD is poorlyunderstood. The aim with this thesis was to clarify the involvement of astrocytes in AD byusing a co-culture system of primary neurons and glia. The co-cultures were exposed to solubleamyloid-beta (Aβ) aggregates, i.e. protofibrils that are known to be particularly harmful.
In Paper I, the capacity of astrocytes to ingest and degrade Aβ protofibrils was investigated.We found that astrocytes effectively ingested Aβ, but were ineffective in degrading the material.The intracellular accumulation of Aβ in astrocytes resulted in lysosomal dysfunction, highintracellular load of partly N-terminally truncated Aβ and extracellular vesicle (EV) mediatedneuronal cell death.
Cells can communicate by releasing cargo into EVs, but the role of EVs in the spreading ofAβ pathology is unclear. In Paper II, the protein content of EVs released specifically followingAβ protofibril exposure was analyzed. We found markedly increased levels of apolipoproteinE (apoE) in EVs from Aβ protofibril exposed co-cultures, suggesting a role for intercellulartransfer of apoE in Aβ pathology.
Passive immunotherapy has been suggested as a promising therapeutic strategy for AD. InPaper III, we investigated if the Aβ protofibril-selective antibody mAb158 could affect Aβclearance in the co-culture. The mAb158 treatment reduced Aβ accumulation in astrocytes andrescued neurons from Aβ-induced cell death.
In Paper IV, we explored the effect of EVs, isolated from Aβ protofibril exposed co-cultureson cultured neurons. In addition to increased cell death, we found that such EVs had a strongnegative impact on the synapses, dendrites and mitochondria of the neurons.
Taken together, this thesis contributes with important knowledge about the role of astrocytesin Aβ pathology, the vesicle-mediated spreading of Aβ and the effects of anti-Aβ antibodytreatment.
Keywords: Alzheimer’s disease, Amyloid-beta, Protofibrils, Astrocytes, Extracellularvesicles, Antibody, Neurons, Degradation
Elisabeth Nikitidou, Department of Public Health and Caring Sciences, Geriatrics, Box 609,Uppsala University, SE-75125 Uppsala, Sweden.
© Elisabeth Nikitidou 2018
ISSN 1651-6206ISBN 978-91-513-0173-0urn:nbn:se:uu:diva-334358 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-334358)

To my wonderful familyfor your endless love and support


The good life is one inspired by loveand guided by knowledge.
Bertrand Russel

Supervisors: Anna Erlandsson, PhD, Associate Professor Department of Public Health and Caring Sci-ences, Uppsala University, Uppsala, Sweden Martin Ingelsson, MD, PhD, Professor Department of Public Health and Caring Sci-ences, Uppsala University, Uppsala, Sweden
Faculty opponent: Gunnar K. Gouras, MD, PhD, Professor
Department of Experimental Medical Science, Wallenberg Neuroscience Center, Lund Univer-sity, Lund, Sweden
Examining committee: Susanne Frykman, PhD, Associate Professor Department of Neurobiology, Care Sciences and Society, Karolinska Institute, Stockholm, Sweden Finn Hallböök, PhD, Professor Department of Neuroscience, Uppsala Univer-sity, Uppsala, Sweden Kina Höglund, PhD, Associate Professor Department of Psychiatry and Neurochemistry, Institute of Neuroscience and Physiology, Sahlgrenska Academy, Gothenburg University, Gothenburg, Sweden
Chairman: Stina Syvänen, PhD, Associate Professor Department of Public Health and Caring Sci-ences, Uppsala University, Uppsala, Sweden

List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Söllvander S, Nikitidou E, Brolin R, Söderberg L, Sehlin D, Lannfelt
L, Erlandsson A. (2016) Accumulation of amyloid-β by astrocytes re-sult in enlarged endosomes and microvesicle-induced apoptosis of neurons. Molecular Neurodegeneration 11(1):38
II Nikitidou E, Khoonsari PE, Shevchenko G, Ingelsson M, Kultima K, Erlandsson A. (2017) Increased release of apolipoprotein E in extra-cellular vesicles following amyloid-β protofibril exposure of neu-roglial co-cultures. Journal of Alzheimer’s disease 60(1):305-321
III Söllvander S, Nikitidou E, Zyśk M, Söderberg L, Sehlin D, Lannfelt L, Erlandsson A. The Aβ protofibril selective antibody mAb158 pre-vents accumulation of Aβ in astrocytes and rescues neurons from Aβ-induced cell death. Submitted
IV Nikitidou E, Ingelsson M, Erlandsson A. Extracellular vesicle-medi-ated amyloid-β toxicity in cortical neurons. Manuscript
Reprints were made with permission from the respective publishers.

Cover artwork The front cover is designed in collaboration with my dear brother-in-law and talented neuroscientist Marco Ledri.

Contents
Popular science summary ............................................................................. 13
Populärvetenskaplig sammanfattning ........................................................... 15
Introduction ................................................................................................... 17 Alzheimer’s disease .................................................................................. 17 Familial Alzheimer’s disease ................................................................... 18 Sporadic Alzheimer’s disease .................................................................. 19 Apolipoprotein E ...................................................................................... 20 APP processing ........................................................................................ 20 Aβ aggregation ......................................................................................... 22 Aβ toxicity ................................................................................................ 23 The amyloid cascade hypothesis .............................................................. 23 Diagnosis and treatment of Alzheimer’s disease ...................................... 24 Aβ immunotherapy in Alzheimer’s disease ............................................. 24 Inflammation in Alzheimer’s disease ....................................................... 25 Astrocytes ................................................................................................. 26 Astrocytes in Alzheimer’s disease ........................................................... 26 Aβ clearance ............................................................................................. 27 Extracellular vesicles ................................................................................ 29 Extracellular vesicles in Alzheimer’s disease .......................................... 30
Aim of the thesis ........................................................................................... 31 Specific aims ............................................................................................ 31
Experimental procedures .............................................................................. 32 Model systems for Alzheimer’s disease ................................................... 32 Neural cell culture model ......................................................................... 32 Synthetic Aβ42 protofibrils ....................................................................... 34 Immunofluorescence and other staining techniques ................................. 35 Microscopy techniques ............................................................................. 36 Differential ultracentrifugation ................................................................. 37 Enzyme-linked immunosorbent assay ...................................................... 38 Mass spectrometry analysis ...................................................................... 39 Western blot analysis ............................................................................... 40 Immunoprecipitation ................................................................................ 41

Results and comments ................................................................................... 42 Cellular uptake and accumulation of Aβ42 protofibrils ............................ 42 Incomplete clearance of Aβ42 protofibrils by astrocytes .......................... 43 Formation of enlarged endosomes in astrocytes following Aβ42 protofibril exposure .................................................................................. 44 Secondary neuronal toxicity following Aβ42 protofibril exposure ........... 45 Spreading mechanisms of Aβ pathology by the secretion of extracellular vesicles ................................................................................ 46 Antibody-mediated effects on astrocytic Aβ42 protofibril clearance ........ 48 Future perspectives ................................................................................... 50
Concluding remarks ...................................................................................... 52
Acknowledgements ....................................................................................... 53
References ..................................................................................................... 57

Abbreviations
Aβ ABCA1 AD ADL AICD Aph-1 apoE APP BACE1 bFGF2 cAMP CNPase CNS CSF CTF DAPI DLB ECL EGF ELISA EVs FITC FTD GFAP HFIP HRP ICC ILVs IP LAMP1 LAMP2 LC-MS LDLR LRP
Amyloid-beta ATP-binding cassette transporter 1 Alzheimer’s disease Activities of daily living APP intracellular domain Anterior pharynx defective Apolipoprotein E Amyloid precursor protein Beta-site APP cleaving enzyme 1 Basic fibroblast growth factor 2 Cyclic adenosine monophosphate 2',3'-Cyclic-nucleotide 3'-phosphodiesterase Central nervous system Cerebrospinal fluid Carboxyterminal fragment 4',6-diamidino-2-phenylindole Dementia with Lewy bodies Enhanced chemiluminescence Epidermal growth factor Enzyme-linked immunosorbent assay Extracellular vesicles Fluorescein isothiocyanate Frontotemporal dementia Glial fibrillary acidic protein 1,1,1,3,3,3,-Hexafluoro-2-propanol Horseradish peroxidase Immunocytochemistry Intraluminal vesicles Immunoprecipitation Lysosomal-associated membrane protein 1 Lysosomal-associated membrane protein 2 Liquid chromatography-mass spectrometry Low density lipoprotein receptor Low density lipoprotein receptor-related protein

LTP MHC MMSE MS MVBs MVs NaOH NFTs NMDA PBS Pen-2 PET PiB PSEN1 PSEN2 p-tau PVDF Rab ROS SDS TEM TUNEL V-ATPase VLDL
Long-term potentiation Major histocompatibility complex Mini-mental state examination Mass spectrometry Multivesicular bodies Microvesicles Sodium hydroxide Neurofibrillary tangles N-methyl-D-aspartate Phosphate-buffered saline Presenilin enhancer Positron emission tomography Pittsburgh compound B Presenilin 1 Presenilin 2 Hyperphosporylated tau Polyvinylidene fluoride Ras-related protein Reactive oxygen species Sodium dodecyl sulfate Transmission electron microscopy Terminal deoxynucleotidyl transferase dUTP nick end labeling Vacuolar-type ATPase Very low density lipoprotein

13
Popular science summary
Dementia is the diagnostic term for a variety of symptoms, caused by many different diseases and injuries in the brain. Alzheimer's disease (AD) is the most common cause of dementia, which accounts for 60-80% of all dementia cases in the world. In AD, the brain tissue becomes atrophic due to an abnor-mal extent of neuronal cell death. This gradual process is ongoing for many years, before the first clinical symptoms arise. The symptoms vary depending on which brain region that is affected, but the parietal and temporal lobes are particularly diseased. The parietal lobe is a brain area that is important for our orientation skills, practical ability, and writing and counting skills, while the temporal lobe is important for learning, memory storage, language functions and emotional regulation. In AD, these and many other brain functions are impaired. At present, there is unfortunately no cure for the disease, but the symptoms can be relieved in some cases by medication. About 1-5% of all AD cases are caused by hereditary mutations in different genes, but the ma-jority have an unknown cause. Research is conducted worldwide to investigate the underlying disease mechanisms in order to develop therapies for treating AD. A suggested explanation to why the neurons die in the AD brain is based on the storage of the deleterious protein, amyloid-beta (Aβ), between neurons in the form of plaques. In addition, another protein called tau is accumulated inside the neurons and forms tangles, which can induce their death. There is a theory that strongly supports that formation of Aβ occurs first and then drives the disease by the formation of tangles. Increasing evidence indicates that it is not the plaques that are deleterious to neurons, but rather the soluble precur-sors of the plaques, so-called Aβ oligomers and protofibrils. Research has so far mainly focused on the neuronal impact in AD, but more attention has started to be given to the different glial cells of the brain. Astro-cytes, the most common type of glial cells, have previously been considered to function primarily as support cells for the neurons. However, it has been found that astrocytes have several important functions, both in the healthy and the diseased brain. Their functions include regulating the brain’s pH, blood flow and chemical environment, nurturing neurons and contributing to the for-mation of the blood-brain barrier. Astrocytes also respond to brain damage by forming a so-called glial scar, as well as helping in the degradation of foreign particles and harmful proteins such as Aβ. The aim of this thesis was to increase the knowledge about the role of astro-cytes in the uptake and degradation of Aβ protofibrils, and to study whether

14
astrocytes may contribute to the Aβ pathology by spreading Aβ and other pro-teins via vesicles. To our help, we cultured neurons, astrocytes and oligoden-drocytes from neural stem cells isolated from embryonic mouse brains. The differentiated cells in the mixed co-culture were exposed to synthetic Aβ pro-tofibrils to study the cellular responses. In the first study, we found that astrocytes effectively engulf Aβ protofibrils, but that they are ineffective and slow in degrading the ingested material, which are instead stored in the cell’s garbage stations called lysosomes. We also noted that oligodendrocytes, which belong to the brain’s glial cells, accumu-late Aβ protofibrils to a certain extent, while the neurons do not. No neuronal cell death occurred directly after the Aβ protofibril exposure. However, the high load of Aβ protofibrils in astrocytes resulted in the astrocytes releasing the partially degraded material into vesicles in the cell medium, which in turn induced neuronal cell death. In the second study, we analyzed and compared the protein content of the vesicles that were secreted specifically after Aβ protofibril exposure with ves-icles secreted from untreated cell cultures. The amount of released vesicles did not differ, but we found five proteins that showed markedly altered levels in vesicles from Aβ protofibril exposed cell cultures, compared to untreated cell cultures. The most prominent protein of them was apolipoprotein E, known to transport cholesterol between cells and to be strongly linked with AD. In the third study, we investigated how the degradation of Aβ protofibrils in astrocytes is affected by treatment with the Aβ protofibril-selective antibody mAb158, which in humanized form (BAN2401) is currently in clinical trials for AD. We found that the Aβ accumulation in astrocytes ceased when the cell cultures were treated with mAb158 and the neurons were rescued from dying. In the fourth study, we investigated how the neurons are affected by treat-ment with vesicles isolated from Aβ protofibril-exposed cell cultures. In ad-dition to increased neuronal cell death, we found a significant negative impact on the neurons’ dendrites, synapses and mitochondria (the energy stations of the cell). In summary, we have been able to demonstrate that astrocytes have an im-portant role in the Aβ pathology and that vesicle-mediated spreading of Aβ may accelerate the disease. Our results also indicate that immunotherapy against Aβ can affect different pathological processes in both astrocytes and neurons.

15
Populärvetenskaplig sammanfattning
Demens är den diagnostiska benämningen för en rad symptom som kan bero på många olika sjukdomar och skador i hjärnan. Den vanligaste orsaken till demens är Alzheimers sjukdom (AD), som utgör 60-80% av alla demenssjuk-domar i världen. Vid AD börjar hjärnvävnaden gradvis förtvina, till följd av att nervcellerna dör i onormal omfattning. Denna process sker smygande och under en längre tid innan de första kliniska symptomen uppkommer. Sympto-men varierar beroende på vilken del av hjärnan som drabbats, men framför allt påverkas parietal- och temporalloberna. Parietalloben är ett hjärnområde som är viktig för vår orienteringsförmåga, praktiska förmåga samt skriv- och räk-neförmåga, medan temporalloben är viktig för inlärning, minneslagring, språkfunktioner och emotionell reglering. Vid AD försämras dessa och många andra hjärnfunktioner. Sjukdomen går dessvärre i nuläget inte att bota, men symptomen kan i vissa fall lindras med mediciner. Cirka 1-5% av alla AD fall orsakas av ärftliga mutationer i olika gener, men majoriteten har en okänd orsak. Forskning pågår världen över för att förstå de bakomliggande sjuk-domsmekanismerna i hopp om att utveckla terapier för att kunna behandla sjukdomen. En huvudsaklig förklaring till att nervcellerna dör i AD hjärnan tros bero på att ett skadligt protein, amyloid-beta (Aβ), lagras mellan nervcel-ler i form av plack. Dessutom ansamlas även små trådar, av proteinet tau, i s.k. tangles inuti nervcellerna, vilka också kan bidra till att de dör. Det finns en stark teori om att Aβ uppkommer först och därefter driver sjukdomsförlop-pet genom bildandet av tangles. Alltmer forskning tyder på att det inte är placken som är giftiga för nervcellerna, utan de lösliga förstadierna till placken, s.k. Aβ oligomerer och protofibriller. Forskningen har hittills främst varit inriktad på nervcellernas påverkan i AD, men alltmer uppmärksamhet har börjat ges till hjärnans olika gliaceller. Astro-cyter, den vanligaste typen av gliaceller, har tidigare ansetts fungera huvud-sakligen som stödjeceller åt nervcellerna. Det har dock visat sig att astrocyter har flera viktiga funktioner, både i den friska och sjuka hjärnan. Deras funkt-ioner innefattar att reglera hjärnans pH, blodflöde och kemiska miljö, ge nä-ring åt nervceller och bidra till uppbyggandet av blod-hjärnbarriären. Astro-cyter reagerar även på sjukdomar och hjärnskador genom att bilda ett så kallat gliaärr, samt hjälper till i nedbrytningen av främmande partiklar och skadliga proteiner såsom Aβ. Syftet med den här avhandlingen var att öka kunskapen om astrocyters roll i upptaget och nedbrytningen av Aβ protofibriller samt studera om astrocyter

16
bidrar till Aβ patologin genom att sprida Aβ och andra proteiner i vesiklar. Till vår hjälp odlade vi nervceller, astrocyter och oligodendrocyter från neu-rala stamceller som isolerats från embryonala mushjärnor. De färdigutveck-lade cellerna i den gemensamma cellkulturen behandlades med syntetiska Aβ protofibriller för att studera det cellulära svaret. I den första studien fann vi att astrocyter effektivt tar upp Aβ protofibriller, men att de är ineffektiva och långsamma på att bryta ner materialet, som istäl-let lagras i cellens sopstationer som kallas lysosomer. Vi noterade även att oligodendrocyter, vilka också tillhör hjärnans gliaceller, lagrar Aβ protofibril-ler i viss utsträckning, medan nervcellerna inte gör det. Ingen nervcellsdöd infann sig direkt efter exponeringen av Aβ protofibriller. Den höga belast-ningen av Aβ protofibriller i astrocyter resulterade dock i att astrocyterna släppte ut det delvis nedbrutna materialet i vesiklar i cellmediet, vilka i sin tur inducerade nervcellsdöd. I den andra studien analyserade och jämförde vi proteininnehållet från ve-siklar som utsöndrades specifikt efter Aβ protofibrill-behandling med vesiklar som utsöndrades från obehandlade cellkulturer. Mängden vesiklar skiljde sig inte åt, men vi fann fem proteiner som visade markant förändrade nivåer i vesiklar från Aβ protofibrill-behandlade cellkulturer jämfört med obehandlade cellkulturer. Det mest framträdande proteinet av dem var apolipoprotein E, känd för att transportera kolesterol mellan celler och som är starkt kopplad till AD. I den tredje studien undersökte vi hur nedbrytningen av Aβ protofibriller i astrocyter påverkas genom behandling med den Aβ protofibrill-selektiva an-tikroppen mAb158, som i humaniserad form (BAN2401) just nu befinner sig i klinisk prövning för behandling av AD. Vi fann att Aβ ackumuleringen i astrocyter upphörde när cellkulturerna behandlades med mAb158 och nerv-cellerna räddades från att dö. I den fjärde studien undersökte vi hur nervcellerna påverkas av behandling med vesiklar isolerade från Aβ protofibrill-behandlade cellkulturer. Utöver ökad nervcellsdöd fann vi kraftig negativ påverkan på nervcellernas utskott, synapser och mitokondrier (cellens energistationer). Sammanfattningsvis har vi kunnat påvisa att astrocyter har en viktig roll i Aβ patologin och att vesikel-medierad spridning av Aβ skulle kunna påskynda sjukdomsförloppet. Våra resultat tyder också på att immunterapi mot Aβ kan påverka olika patologiska processer i både astrocyter och nervceller.

17
Introduction
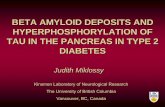
Alzheimer’s disease It is estimated that more than 46.8 million people worldwide are affected by dementia and, according to the World Alzheimer Report 2016, the number of cases are expected to reach 131.5 million by 2050 [1]. Dementia has therefore become an important health and socioeconomic issue in our society. The most common cause of dementia is Alzheimer’s disease (AD), which constitutes 60-80% of all dementia cases [2]. Other forms of dementia include vascular dementia, dementia with Lewy bodies (DLB) and frontotemporal dementia (FTD). Alzheimer’s disease is an irreversible, progressive neurodegenerative disorder that was first described by the German psychiatrist and neuropa-thologist Alois Alzheimer in 1906. He observed and clinically investigated a 55-year old patient named Auguste Deter, who was suffering from severe memory loss, disorientation and other cognitive impairments. Following her death, Alois Alzheimer examined the autopsied brain and discovered neuro-pathological lesions in the form of dense amyloid plaques around neurons and neurofibrillary tangles (NFTs) inside the neurons (Figure 1) [3]. The extracel-lular amyloid plaques and intraneuronal NFTs were later shown to consist of amyloid-beta (Aβ) fibrils and hyperphosphorylated tau (p-tau), respectively [4]. They represent the two major neuropathological hallmarks of AD.
Figure 1. The neuropathological hallmarks of AD consist of extracellular amyloid plaques (green, A) and intracellular NFTs (red, B). Pictures kindly provided by Paul O’Callaghan.

18
Moreover, AD is characterized by vascular damage from extensive plaque deposition, neuroinflammation, gradual loss of neurons and degeneration of axons and dendrites that lead to enlarged ventricles and brain atrophy [5]. In most cases, the NFTs initially involve the medial temporal lobe structures (e.g. hippocampus and entorhinal cortex) and then extend to the temporal, parietal and frontal lobes as the disease progresses [6]. Consequently, this will give rise to various behavioral, psychological and cognitive symptoms affecting learning, memory, language and other higher executive functions in AD pa-tients [7, 8]. The severity of symptoms will gradually worsen as the disease progresses and affected individuals will also suffer from impaired movements and end up completely dependent on their caregivers in the late stage of the disease [9]. Due to heterogeneity in the rate of progression among AD pa-tients, it may be difficult for clinicians to give an accurate prognosis after a clinical diagnosis of AD [10] and the life expectancy can vary between 3-20 years [11], with the definite cause of death usually being pneumonia or is-chemic heart disease [12]. Based on the age of onset, AD is divided into fa-milial or sporadic AD, which helps us better understand the development and severity of the disease.
Familial Alzheimer’s disease Early-onset or familial AD generally affects individuals under the age of 65 years and constitutes 1-5% of all AD cases [13]. It is associated with a more rapid rate of disease progression because of inheritance factors. In familial AD, the cause is a mutation with an autosomal dominant inheritance pattern. The first gene to be identified in familial AD was the amyloid precursor protein (APP) gene on chromosome 21, discovered in 1987 by Kang and col-leagues [14]. The APP is an integral, transmembrane glycoprotein (cell-sur-face receptor) with a large extracellular domain and a small cytosolic domain [15]. Alternative splicing of the mammalian APP gene produces different isoforms; whereas the APP695 isoform is primarily expressed in the brain the APP751 and APP770 isoforms are mainly expressed in the periphery [16, 17]. The physiological role of APP is only partly understood, but it has been sug-gested to be important for neuronal function, including neuronal migration, neurite outgrowth, synapse formation and synaptic plasticity [18, 19]. Point mutations (insertion, deletion or substitution to a single nucleotide base) in the APP gene lead to an improper post-translational proteolytic processing of APP, resulting in enzymatic cleavage of the APP fragment to form Aβ by β- and γ-secretases [20]. More than 16 disease-causing mutations located at or in the vicinity of the β- and γ-secretase cleavage sites or within the APP sequence have been discovered in various families around the world [21, 22]. Among them is the Swedish mutation, discovered in 1992 and caused by two base pair transversions at the β-secretase cleavage site, which results in an increased

19
total Aβ production [23]. The London mutation is instead caused by mutations in the γ-secretase cleavage sites, which leads to an increased production of the 42-amino acid Aβ sequence compared to the 40-amino acid Aβ sequence (Aβ42/Aβ40 ratio) [24]. Increased formation of soluble Aβ protofibrils due to a mutation located within the Aβ sequence was found in the Arctic mutation in 2001 [25]. Interestingly, it was found a few years ago that a group of individ-uals on Iceland with a missense mutation (amino acid substitution) in the APP gene, referred to as the Icelandic mutation, are protected against developing AD [26]. An important parallel to familial AD was the discovery that Down’s syndrome trisomy 21 individuals, who have an extra copy of chromosome 21 on which the APP gene is located, most often develop amyloid pathology and AD-like symptoms before the age of 35 years [27, 28]. Other mutations located outside the APP gene locus are missense mutations in the Presenilin 1 (PSEN1) and Presenilin 2 (PSEN2) genes located on chro-mosome 14 and 1, respectively. These genes encode for the catalytic subunits of γ-secretase and lead to an increased Aβ42/Aβ40 ratio [29-32]. Although mu-tations only represent a small percentage of all AD cases, they have enabled generation of suitable animal models for AD and increased the understanding of the disease pathogenesis.
Sporadic Alzheimer’s disease The majority of AD patients (>95%) have a late-onset, sporadic disease vari-ant that affects individuals over the age of 65 years [13]. The cause of this form of the disease is unclear, but several factors have been reported to in-crease the risk of developing sporadic AD and it may likely be multifactorial, resulting from a combination of different factors [33]. Aside from the clear risk factor of age, many epidemiological studies have found lifestyle-related associations linked to the cardiovascular system, including hypertension, hy-percholesterolemia, atherosclerosis, coronary heart disease, smoking, obesity and diabetes [34-39]. In addition, patients with a history of stroke, traumatic brain injury and chronic neuroinflammation are at higher risk of developing AD, probably due to a decreased clearing capacity and a greater Aβ-related burden [40-42]. Other studies have found that people with a higher educational level may be protected against developing AD because of a higher cognitive reserve, but it is unclear whether such a factor affects the disease process or not [43-45]. Nevertheless, time spent in engaging in mental, physical and lei-sure activities has been associated with a reduced risk of dementia in cogni-tively healthy individuals over 65 years [46].

20
Apolipoprotein E The strongest genetic risk factor for sporadic AD is the association with the apolipoprotein E (apoE) genotype [47, 48]. The apoE gene is located on chro-mosome 19 and encodes a 299-amino acid protein with a native molecular mass of ~34 kDa [49]. In peripheral tissues, apoE is primarily produced by the liver and macrophages, while in the central nervous system (CNS) it is pri-marily produced by astrocytes and to some extent by microglia, oligodendro-cytes and ependymal layer cells [50-53]. Under certain conditions, such as excitotoxic injury, neurons are also able to generate apoE [54, 55]. The phys-iological function of apoE mainly relates to packaging and transporing cho-lesterol and other lipids, as well as binding to cell surface apoE receptors [56]. Upon production in the CNS, apoE is secreted by astrocytes [51, 57] where cholesterol and other lipids are transferred to apoE predominantly via ATP-binding cassette transporter 1 (ABCA1), a brain lipid regulator protein ex-pressed on astrocytes, microglia and neurons [58, 59]. The transport to cells is mediated by the interaction of apoE with abundant cell surface receptors, in-cluding the low density lipoprotein receptor (LDLR), low density lipoprotein receptor-related protein 1 and 2 (LRP1 and LRP2) and very low density lipo-protein (VLDL), followed by endocytosis [60]. The apoE gene shows a genetic polymorphism in humans and exists in three major isoforms; ε2, ε3 and ε4. Despite a single amino acid substitution among the apoE isoforms, this will result in differences in several functional proper-ties, including their ability to bind lipids, receptors and Aβ [61, 62]. The apoE ε3 allele (~78%) is the most frequent in the general population, followed by ε4 (~14%) and ε2 (~8%) [63, 64]. Individuals with one or two copies of the apoE ε4 allele have a significantly higher risk of developing AD and with a lower age of onset, while the apoE ε2 allele seems to be protective [47, 65, 66]. There is evidence that apoE co-deposits with Aβ in amyloid plaques of AD patients, particularly amongst apoE ε4 carriers [67] and astrocytic apoE has been shown to be important for the uptake and degradation of Aβ [68]. However, it is up to date not entirely clear why apoE ε4 carriers have an in-creased risk of developing AD.
APP processing Since APP is a protein, it will be degraded and recycled. Processing of the APP occurs by proteolytic cleavage with the enzymes α-, β- and γ-secretase in either the non-amyloidogenic or the amyloidogenic pathway (Figure 2). In the non-amyloidogenic pathway, APP is first cleaved by α-secretase, a member of the ADAM family of proteases, within the Aβ domain (at the Lys16-Leu17 bond). This cleavage prevents the formation of Aβ [69, 70] and results in extracellular release of a large soluble N-terminal ectodomain

21
known as sAPPα, whereas the carboxyterminal fragment (CTF) APP-CTF83, remains bound to the plasma membrane. It has been shown that sAPPα has a neuroprotective role, preventing neurons from excitotoxicity and promoting neurite outgrowth, synaptogenesis and cell adhesion [71, 72]. The plasma membrane-bound fragment APP-CTF83 is then further cleaved by γ-secre-tase, which is a tetrameric protease complex consisting of the four subunits presenilin, nicastrin, anterior pharynx defective (Aph-1) and presenilin en-hancer (Pen-2) [73]. This cleavage will result in the release of a small extra-cellular P3 fragment (with unknown physiological function) that is rapidly de-graded, as well as the generation of an amino-terminal APP intracellular do-main (AICD) [74]. In the amyloidogenic pathway, APP is instead first cleaved by the mem-brane-bound aspartyl protease β-secretase (also known as beta-site amyloid precursor protein cleaving enzyme 1, BACE1), causing the extracellular re-lease of a large N-terminal ectodomain called sAPPβ, while leaving the C-terminal fragment APP-CTF99 bound to the plasma membrane [73]. The function of sAPPβ is poorly understood, but it has been suggested to be im-portant for synaptic pruning during CNS development [75]. The APP-CTF99 is then further cleaved by γ-secretase, resulting in the production and extra-cellular release of Aβ, as well as the generation of intracellular AICD that is released in the cytosol.
Figure 2. APP processing. The APP transmembrane protein can be processed in two different pathways. In the non-amyloidogenic pathway, APP is first cleaved by α-secretase with a subsequent cleavage by γ-secretase. In the amyloidogenic pathway, APP is instead cleaved by β-secretase with a subsequent cleavage by γ-secretase, re-sulting in formation of the Aβ peptide.

22
Aβ aggregation Various Aβ peptides with different chain lengths are produced, depending on the γ-secretase cleavage site. The majority of Aβ produced following APP pro-cessing consists of the 4 kDa Aβ40 monomer along with a minor portion of the Aβ42 monomer, but additional shorter or longer Aβ variants have been observed [76, 77]. Although the Aβ42 has only two additional amino acids, its hydropho-bic structure makes it more prone to aggregate and more toxic to neurons than Aβ40 [78]. In addition, Aβ42 has been found to be the predominant component of the amyloid plaques [79, 80]. Depending on conformational changes, mono-meric Aβ can either enter an off-pathway, preventing Aβ to aggregate into fibrils by forming soluble end-stage oligomers, or an on-pathway with gradually in-creased fibrillization. The Aβ monomers will then adopt a β-hairpin structure and start to assemble and aggregate into small soluble oligomers, including Aβ dimers, trimers, tetramers and protofibrils (Figure 3) [81-83]. Protofibrils are described as elongated, curvilinear >70 kDa intermediates of up to 200 nm in length and with a general diameter of 4-10 nm [25, 84-87]. As the end-stage of the Aβ aggregation process, insoluble Aβ fibrils are deposited as plaques. Inter-estingly, it has been shown that small soluble Aβ aggregates have the ability to seed high-molecular weight Aβ aggregates into insoluble Aβ fibrils and thus induce the deposition of Aβ, suggesting that the seeding propagation of Aβ may contribute to the progression of AD [88, 89].
Figure 3. The Aβ aggregation pathway. The Aβ monomers aggregate and form solu-ble oligomers that act as building blocks for protofibrils. Elongation of protofibrils generates insoluble Aβ fibrils, the main component of amyloid plaques. Plaque im-age kindly provided by Paul O’Callaghan.

23
Aβ toxicity The cause of neurodegeneration in AD has been a central question for many years, but it is well known that Aβ plays an important role. However, which Aβ species that cause the neurological damage, directly or indirectly, has been debated. For many years, it was considered that insoluble fibrillar Aβ found in the plaques were the main neurotoxic species, but recently the research has shifted more towards the soluble forms of Aβ as the main causative agents. One of the strongest arguments supporting this theory is the lack of correlation between the amount of Aβ plaques in human AD brains and the severity of AD-like symptoms [86, 90, 91], whereas other studies have suggested that the concentration of soluble Aβ oligomers correlates with the pathological picture [84, 86, 92-95]. However, it should not be excluded that fibrillar Aβ may have a partial role in AD [96]. Oligomeric Aβ have been found to bind with high affinity to synapses and impair neurotransmission by rapidly inhibiting long-term potentiation (LTP) in rodent hippocampal slice preparations [97, 98]. Moreover, injection of various Aβ oligomers directly into the rodent brain leads to cognitive impairments [99, 100]. In addition to synaptic dysfunction, Aβ oligomers also cause mitochondrial dysfunction and oxidative stress [101].
The amyloid cascade hypothesis In 1992, Hardy and Higgins proposed a theory on the causative mechanisms of progression in AD, known as the amyloid cascade hypothesis, wherein they postulate that Aβ is the causative agent that initiates a sequence of events that ultimately lead to dementia [102]. The main support of the amyloid cascade hypothesis is based on the discovery of the genetic factors described above (related to APP, PSEN1, PSEN2 and apoE), which all promote and increase Aβ deposition in AD before the onset of neuroinflammation, NFT pathology, neuronal loss and dementia [103]. Moreover, mutations in the tau gene on chromosome 17 are known to cause FTD, but without the appearance of am-yloid plaques, thus indicating that tau pathology itself can cause neuronal loss but that tau pathology is a downstream process of Aβ pathology [104]. Since most AD cases occur in a sporadic fashion, Hardy and Higgins propose that other external factors, such as head trauma, may trigger Aβ deposition and in this way lead to downstream pathological processes [102]. Since the amyloid cascade hypothesis was first published, the focus of research has shifted from amyloid plaques to the soluble oligomeric Aβ forms as the main neurotoxic species in AD, since they predict the disease progression more accurately than the Aβ plaque burden [81, 83, 86, 105, 106].

24
Diagnosis and treatment of Alzheimer’s disease Standardized diagnostic criteria for AD were first published in 1984 [107]. In order to give a valid clinical diagnosis of AD, it is necessary to rule out other conditions that can also cause dementia. The typical dementia of AD is char-acterized by a reduction of multiple cognitive functions, such as prominent episodic memory impairment, deficits in spatiotemporal cognition and execu-tive functions, aphasia and apraxia that combined will adversely affect the pa-tient’s activities of daily living (ADL) [108]. To assess the cognitive status of the patient, the Mini-Mental State Examination (MMSE) is often used, which tests various neuropsychological parameters, including orientation, memory, language, construction and abstract reasoning [109]. Additional diagnostic criteria for AD involve physical and neurological examination, blood- and se-rological tests to rule out other causes of the symptoms and analysis of Aβ42, total-tau and p-tau in cerebrospinal fluid (CSF) [110]. The decreased CSF lev-els of Aβ42 are suggested to be related to the increased aggregation of Aβ pep-tides in the AD brain, whereas the increased tau levels are suggested to reflect the extracellular leakage of the microtubule-associated tau protein following neuronal cell death of the AD brain. Detection of fibrillar Aβ from amyloid plaques can further be visualized by positron emission tomography (PET) im-aging with the radioligand Pittsburgh Compound B (PiB) [111]. At present, there is no curative treatment for AD, but pharmacological treat-ment is often used in an attempt to alleviate the symptoms. Acetylcholinester-ase inhibitors are most often used in early-to-moderate AD to increase acetyl-choline levels in the brain and thus improve memory. In moderate-to-severe AD, N-methyl-D-aspartate (NMDA) receptor antagonists can be used to re-duce excitotoxicity [112, 113].
Aβ immunotherapy in Alzheimer’s disease Antibody-based immunotherapy against Aβ has been proposed as a therapeu-tic strategy for AD and several clinical trials have been performed, using both active and passive immunization. In active immunization trials, synthetic in-tact Aβ42 or conjugated Aβ42 fragments have been used to activate the immune system to produce endogenous antibodies against Aβ [114, 115]. Unfortu-nately, all active immunization trials to date have failed, presumably due to reduced responsiveness of the immune system to produce the right kind of antibodies in older individuals as well as severe side effects, such as menin-goencephalitis [116, 117]. Passive immunization with direct administration of anti-Aβ antibodies has instead become the more common strategy to target the soluble Aβ aggregates. Two large phase III clinical trials using the monoclonal antibodies Bapi-neuzumab (targeting the N-terminal region of Aβ) from Pfizer/Janssen and

25
Solanezumab (targeting the central region of Aβ) from Eli Lilly both failed to improve cognition or functional ability in mild-to-moderate AD. In addition, the extent of adverse effects, such as cerebral microbleeds, were rather high [118, 119]. Antibodies targeting soluble oligomeric forms of Aβ aggregates are currently being investigated in clinical trials. The BAN2401 monoclonal antibody, targeting Aβ protofibrils was developed by BioArctic AB and is currently in a phase 2b clinical trial conducted by Eisai Pharmaceutical [120]. The murine version of BAN2401, called mAb158, has been shown to reduce brain levels of Aβ protofibrils and prevent Aβ deposition in mouse models of AD. Another monoclonal antibody targeting soluble aggregated forms of Aβ is Aducanumab by Biogen, which was recently reported to slow down cogni-tive decline in a phase I study and a large phase III clinical study is currently underway for the treatment of AD [121]. However, the underlying mecha-nisms of how Aβ antibodies affect the Aβ deposition, mediate their therapeutic effects and the role of different cell types for its action remain to be elucidated.
Inflammation in Alzheimer’s disease The neuroinflammatory aspects of AD have been widely studied, but it still remains unclear whether inflammation is the cause, a contributor or merely a consequence of the disease. According to the amyloid cascade hypothesis, the immune system is activated following Aβ accumulation. Regardless, it is well known that there is an ongoing neuroinflammation in the AD brain, mani-fested by activation of microglia, astrocytes, T-cells and the complement sys-tem. Moreover, there is a release of proinflammatory cytokines and chemo-kines, e.g. IL-1β, IL-6 and TNF-α, production of immunoglobulins and upreg-ulation of microglial cell surface markers, e.g. major histocompatibility (MHC) complex II, CD36, CD14, CD11c and Fc receptors [122-126]. Free radicals such as reactive oxygen species (ROS) are also generated in the AD brain [127-134]. Overproduction and release of ROS and other cytotoxic fac-tors lead to oxidative stress, mitochondrial dysfunction, cell damage and neu-rotoxicity in AD [135]. During neuroinflammation, some microglia have an immunosuppressive role by producing anti-inflammatory cytokines and neu-rotrophic growth factors [136]. Microglia and astrocytes are, as the brain’s resident immune cells, important for maintaining homeostasis by removing misfolded proteins such as Aβ [137]. Their activation in the early stages of AD suggests an initial protective role in preclinical AD, but during the course of the disease, microglia and astrocytes may be less efficient in their task and may instead switch to a hypersensitive proinflammatory state [138]. The in-terplay between microglia and astrocytes may also be important in the disease. It was recently reported that activated microglia induce a specific subpopula-tion of astrocytes, termed A1 astrocytes, by secreting IL-1α, TNF-α and C1q. Activation prevented A1 astrocytes to promote neuronal survival, outgrowth,

26
synaptogenesis and phagocytosis. The presence of A1 astrocytes in several neurodegenerative post-mortem brains, including AD, suggests that astrocytes may also contribute to neuronal cell death [139].
Astrocytes Astrocytes, named after their star-like appearance, were long considered as mere support cells for neurons, but the knowledge has advanced and it is now well known that they are specialized glial cells with many important functions in the CNS. Their role includes buffering of ions [140], pH [141] and neuro-transmitters [142, 143], regulation of cerebral blood flow [144], water transport by aquaporin channels [145], metabolic support for neurons [146], modification of synapse signaling [147], contribution to the glymphatic clear-ance pathway [148] and the blood-brain barrier [149]. The population of glial cells in relation to neurons in the human brain has been debated. Quantitative data from brain tissue analyses have shown conflicting results throughout the years, due to the samples analyzed (various distribution of cells in different parts of the brain) and histological counting methods. It was long proposed that the glia/neuron ratio was 10:1, but recent studies suggest about a 1:1 ratio [150]. Although the number of astrocytes varies uniformly in different brain areas of mammalian species, the proportion of astrocytes is estimated to be 20-40% of the total mammalian brain cell number, making it the most abun-dant glial cell type in the brain [151]. Based on morphology and anatomic location in the brain, astrocytes are divided into fibrous or protoplasmic astro-cytes. Fibrous astrocytes connect to other cells by their long fiber-like pro-cesses and are present in the white matter, but the majority of astrocytes are protoplasmic, displaying short branches in the grey matter [152]. Unlike neu-rons, astrocytes are electrically non-excitable neural cells that instead possess excitability based on movements of Ca2+ ions between intracellular compart-ments and Ca2+ fluxes across the plasma membrane [153]. Astrocytes respond to almost all neurotransmitters, neuromodulators and hormones by cellular changes in cytosolic Ca2+ or cyclic adenosine monophosphate (cAMP) [154].
Astrocytes in Alzheimer’s disease Astrocytes respond to lesions and pathogenic insults through a process re-ferred to as reactive astrogliosis. During reactive astrogliosis, astrocytes be-come hypertrophic, start to proliferate and upregulate their intermediate fila-ments (glial fibrillary acidic protein (GFAP), nestin and vimentin) [155]. In AD, reactive astrocytes are frequently found around amyloid plaques in both transgenic AD mice [156-158] and in human post-mortem brains [159, 160]. Being the most numerous glial cell type in the brain, astrocytes may have a

27
great impact on the degradation and clearance of Aβ and the role of astrocytes in the maintenance of brain homeostasis may be severely affected in AD. It has been suggested that in the early stages of AD, astrocytes have a more neu-roprotective role and the ability to phagocytose Aβ aggregates for degradation. However, with increased brain atrophy in the later stages of AD, astrocytes have been implicated to contribute to the neuroinflammation and Aβ pathol-ogy by failure of Aβ clearance [161]. In addition, Aβ has also been found to affect astrocytes by inducing Ca2+ oscillations, which may contribute to the neurotoxicity [162, 163].
Aβ clearance There are various mechanisms to clear Aβ from the brain, including degrada-tion by the ubiquitin-proteasome pathway [164], clearance by the blood-brain barrier interstitial fluid bulk flow [165], CSF absorption [166], and endocytic pathways by phagocytosis and pinocytosis [167]. Phagocytosis is primarily conducted by microglia in the brain, but also astrocytes, neurons and oligoden-drocytes possess phagocytic abilities. In fact, it has previously been reported that astrocytes can engulf whole dead cells, Aβ aggregates, synapses and α-synuclein [168-172]. However, astrocytes have been found to store, rather than degrade, ingested whole dead cells [173]. The reason behind the slow digestion was found to be poor lysosomal acidification, due to high levels of Rab27a in astrocytes. The Rab27a is known to reduce the acidity of lysosomes by Nox2 recruitment, in order to preserve antigens for presentation, as astro-cytes express MHC class II. There are different uptake mechanisms of Aβ by the cells. Receptor-medi-ated phagocytic internalization occurs by interaction of specific receptors on the phagocytic cell with ligands on the surface of the Aβ peptide, which then triggers actin filaments of the phagocyte to zipper up around the particle and engulf it [174]. Pinocytosis, on the other hand, occurs in all cell types and involves the invagination of particles into endocytic vesicles upon stimulation by growth factors or other signals and can be divided into four subgroups based on the uptake mechanisms; macropinocytosis, clathrin-mediated endo-cytosis, caveolae-mediated endocytosis and clathrin/caveolae-independent endocytosis (Figure 4) [175]. In microglia, soluble Aβ have been shown to be internalized mainly through pinocytosis and fibrillar Aβ through receptor-me-diated phagocytosis [176]. The uptake mechanisms of Aβ by astrocytes is poorly understood, but both macropinocytosis and receptor-mediated phago-cytosis have been suggested as engulfment mechanisms [177, 178].

28
Figure 4. Endocytic cellular pathways. Extracellular material can be taken up by en-docytosis through various mechanisms, including receptor-mediated phagocytosis and micropinocytosis. After internalization, the material is transported to early endo-somes, where it can either be recycled back to the plasma membrane or be degraded by the endosomal-lysosomal pathway. In this pathway, the pH will subsequently drop causing activation of degrading enzymes. Important proteins of the endosomal-lysosomal pathway are Rab5, Rab7, LAMP-1 and LAMP-2. Exosomes are derived from MVBs, whereas MVs bud directly from the plasma membrane.
Following internalization, the cargo first arrives to the early endosomes, the main sorting stations in the endocytic pathway, characterized by the presence of the Ras-related proteins Rab4 and Rab5 [179]. The majority of cargo, in-cluding most receptor proteins, is returned to the plasma membrane via recy-cling endosomes. Cargo destined for degradation, such as Aβ, will follow the endosomal-lysosomal pathway. In the early endosomes, formation of intralu-minal vesicles (ILVs) begins, and in the late endosomes (also known as mul-tivesicular bodies, MVBs) the proteins are sorted between the endosomal membrane and ILVs, characterized by the replacement of Rab4 and Rab5 to

29
the late endosomal markers Rab7 and Rab9. During the maturation process from early endosomes to lysosomes the vacuolar-type ATPase (V-ATPase) proton pump will subsequently drop the pH from around 6.2 in early endo-somes to 5.5 and 5.0 in late endosomes and lysosomes, respectively, by deliv-ering and increasing the concentration of acid hydrolases (degrading enzymes) [180, 181]. Except for the Rab proteins, the lysosomal-associated membrane proteins LAMP-1 and LAMP-2 are also involved in the maturation process of early endosomes to mature lysosomes, the end-stage where the waste material is degraded by proteolytic activity with lysosomal enzymes [182]. Studies have shown the endosomal-lysosomal pathway to be heavily affected in the AD brain, before Aβ and tau pathology begin, by dysregulation of pH and cellular indigestion, which may lead to impaired clearance of Aβ [183, 184].
Extracellular vesicles Intercellular communication is essential for all multicellular organisms. Ex-tracellular vesicles (EVs) is one form of intercellular communication, deliver-ing various proteins, lipids, nucleic acids and sugar molecules between cells. The EVs can be isolated from a wide range of fluids, including cell culture medium, blood, CSF, saliva, breast milk and urine [185-187] by different tech-niques, including differential ultracentrifugation, density gradient centrifuga-tion, size-exclusion chromatography, filtration and polymer-based precipita-tion [188]. Differential ultracentrifugation is commonly used and consists of several steps. First, a low-speed centrifugation is applied to remove cells and cell debris, then by a higher speed spin to remove any remaining cell remnants, followed by high-speed ultracentrifugation. Characterization of EVs is based on size, properties and cellular origin of the vesicles. Microvesicles or ecto-somes (MVs) are produced by direct budding from the plasma membrane and range in size from 100-1000 nm. Exosomes are small membranous vesicles (20-100 nm) that are formed when late endosomes/MVBs fuse with the plasma membrane by involvement of Rab11, Rab27 and Rab35 (Figure 4) [189-192]. The EVs are released from various cells in the brain, including mi-croglia, astrocytes and neurons, and the uptake of released EVs is suggested to occur mainly by phagocytosis, alternatively by macropinocytosis or mem-brane fusion [193-196]. Typical EV protein markers are the tetraspanins CD9, CD63 and CD81; the lipid rafts flotillin-1, flotillin-2 and caveolin-1, and the intravesicular markers alix, TSG101 and syndecan. Although several EV iso-lation protocols have been developed, there is currently a challenge within the research community to fully characterize different EV populations in practice, due to limitations in the purity of the isolated EVs, the risk of contamination of other EVs or cell remnants, and the lack of explicit protein markers for the different EVs. However, smaller EVs, such as exosomes, are isolated at higher

30
speed of centrifugation and longer ultracentrifugation step than larger EVs, such as MVs.
Extracellular vesicles in Alzheimer’s disease Extracellular vesicles have been implicated to contribute to the pathogenesis of AD and other neurodegenerative disorders by transmitting protein aggre-gates, and they have also been proposed to take part in cell-to-cell transfer of prions [197, 198]. Specifically, Aβ, APP and its cleaving products have been found to be sorted in MVBs and released by exosomes into the extracellular space in transgenic AD animal models, suggesting that exosomes promote ag-gregation of neurotoxic Aβ in amyloid plaques [199-201]. The EV proteins alix and flotillin-1 have also been found to be enriched in amyloid plaques in the human AD brain and in a transgenic AD mouse model [202, 203]. More-over, there is a significant correlation between the amount of microglial MVs and atrophy of the hippocampus in AD patients [204]. However, it should be mentioned that exosomes have also been suggested to have neuroprotective roles, e.g. by acting on extracellular Aβ to promote uptake and clearance by microglia [205]. Since the EV content mirrors the intracellular environment, it could contribute with important information about ongoing pathological processes and may be a useful source for biomarkers, reflecting the progres-sion of various diseases, including AD.

31
Aim of the thesis
The overall aim of this thesis was to increase the knowledge of astrocytes in Aβ pathology, focusing on Aβ clearance and Aβ-induced toxicity by the se-cretion of EVs. All the included studies have been performed using a co-cul-ture system of primary neurons, astrocytes and oligodendrocytes.
Specific aims I To clarify the role of astrocytes in Aβ pathology by studying uptake,
degradation and toxicity of Aβ42 protofibrils.
II To analyze the protein content of EVs, specifically released following Aβ42 protofibril exposure.
III To investigate if Aβ degradation in astrocytes can be enhanced by treatment with the Aβ protofibril-selective antibody mAb158.
IV To examine the mechanisms behind the neurotoxicity, mediated by EVs released following Aβ42 protofibril exposure.

32
Experimental procedures
Model systems for Alzheimer’s disease Epidemiological and population-based studies on AD patients are important for evaluating data, in order to find common denominators and risk factors of the disease. However, experimental studies on humans are limited due to var-ious ethical issues. The existence of both in vitro and in vivo models in AD research has been beneficial and enabled researchers to study various aspects of the disease. Many transgenic animal models of AD have been developed to study the disease in vivo thanks to the genetic discoveries linked to AD. Also, new ways of studying AD pathology have been made possible by breeding rodents carrying more than one AD mutation. One such example are mice ex-pressing the APP gene with both the human Arctic and Swedish mutations (tg-ArcSwe). The tg-ArcSwe mice develop an early (4-8 months) and prominent Aβ pathology, with elevated soluble Aβ aggregates such as Aβ protofibrils, and amyloid plaques [206-208]. Animal models are useful for studying the disease phenotype and for the development of new drugs and treatments, as they allow behavioral and functional analyses. On the other hand, cell culture models are a more direct way to study cellular and molecular processes of individual cells, which could increase our understanding of some aspects of the disease. Moreover, cell culture models are easily reproduced and require reduced number of experimental animals. However, one limitation is that cell culture models do not reflect the complexity of the brain.
Neural cell culture model Throughout this thesis, we have used an in vitro cell culture model, consisting of primary astrocytes, neurons and oligodendrocytes. In order to obtain these, cerebral cortices from C57/BL6 mice of embryonal day 14 (E14) were dis-sected and the dissociated cells were cultured in serum-free medium. Neural stem cells were expanded as neurospheres in DMEM/F12-GlutaMAX cell culture medium supplemented with B27 and growth factors (epidermal growth factor, EGF and basic fibroblast growth factor 2, bFGF2) and passaged every second or third day. The neurospheres were dissociated and plated as a mon-olayer on coated coverslips or cell culture dishes in medium with growth fac-tors, in order to let them recover from the passage. After 24 h incubation, the

33
neural stem cells were differentiated in mitogen-free medium for 7 days, with medium changes performed every second or third day. The differentiated neu-ral cultures were quantified after immunocytochemistry (ICC) and consisted of ~70% astrocytes, ~25% neurons and ~5% oligodendrocytes (Figure 5) [209]. Microglia originate from the hematopoietic stem cell line and were therefore not present in our cultures. This enabled us to fully study the capacity of astrocytes as scavenger cells without the presence of professional phago-cytes.
Figure 5. Mixed neural cell cultures from embryonal cortical stem cells. Differentia-tion of the neural stem cells leads to development into a co-culture of astrocytes, neurons and oligodendrocytes. GFAP, βIII-tubulin, CNPase (all green), DAPI blue. Scale bar: 20 µm.
After the differentiation period, cultured cells were exposed to synthetic Aβ42 protofibrils or left untreated, and were followed over time. In Paper I and Paper III, cells were exposed to Aβ42 protofibrils for 24 h prior to fixation or cell lysis, or were washed thoroughly in culture medium without Aβ42 proto-fibrils and incubated for an additional 6 or 12 days prior to fixation or cell lysis. In order to study the effect of mAb158 in Paper III, Aβ42 protofibrils were pre-incubated for 5 min with the hybridoma-produced murine mAb158 (IgG2a) antibody or the recombinantly produced mAb158, RmAb158 (IgG2c)

34
antibody, with or without the N297D mutation prior to addition to the cultures. To analyze the release and protein content of EVs in Paper II, cells were con-stantly exposed to Aβ42 protofibrils for 2 or 5 days prior to medium collection and ultracentrifugation in order to maximize the EV content. The time points in Paper II were based on the finding in Paper I that formation of enlarged endosomes start to appear after 2-3 days. In Paper I and Paper IV, primary cortical E14 neurons were cultured 12 days in vitro (12DIV) in neurobasal medium. The neuronal cultures were treated with EVs isolated 6 and 12 days after Aβ42 protofibril exposure of neuroglial co-cultures (Aβ42 protofibril-EVs) or EVs from untreated neuroglial co-cultures (Control-EVs). The viabil-ity and cellular effects of the neurons in response to EV treatment were inves-tigated.
Synthetic Aβ42 protofibrils Throughout this thesis, we have used synthetic Aβ to study the cellular re-sponses. Since the quality of Aβ and its propensity to aggregate varies between different manufacturers and lots, we consistently used the same lot of Aβ in all experiments throughout each study. Due to the hydrophobicity of Aβ, it has a propensity to stick to glass and plastic surfaces in tubes, plates, pipette tips and chromatography columns. However, this may be avoided by addition of small amounts of detergents. Fluorescent HiLyteTM Fluor 555-labeled Aβ42 (Aβ42-555) peptides or unlabeled Aβ42 peptides were used as starting material to prepare Aβ42 protofibrils. In many laboratories, organic compounds such as 1,1,1,3,3,3,-Hexafluoro-2-propanol (HFIP) are used to dissolve and mon-omerize Aβ. However, we and other research groups routinely use sodium hydroxide (NaOH) to dissolve the lyophilized Aβ peptide, since increase in the pH of Aβ (pH ~10.5-11) followed by neutralization with PBS avoids the Aβ to pass its isoelectric point. This will lead to formation of peptide solutions with higher yields of low-molecular weight Aβ and lower levels of pre-exist-ing aggregates [210-212]. After dissolution, both Aβ42-555 and unlabeled Aβ42 peptides were centrifuged for 5 min at 17 900 x g to remove any insoluble aggregates. All solutions and material used to prepare Aβ42 protofibrils were sterile and final aliquots were stored at -70oC. The expected concentration of Aβ was routinely analyzed and confirmed in our laboratory, using the proto-fibril specific ELISA, based on mAb158 [206]. We defined Aβ protofibrils as curvilinear structures with a size larger than 75 kDa, based on cryo-TEM stud-ies [206] and HPLC-SEC analysis using a Superdex 75 column (>95% purity of Aβ42 protofibrils), respectively. The HiLyteTM Fluor 555-label did not dis-turb the protofibril conformation of Aβ42 protofibrils.

35
Immunofluorescence and other staining techniques Immunofluorescence staining techniques are based on the direct or indirect binding of antibodies, chemically conjugated with a fluorophore to a specific antigen of interest, thus enabling visualization of the specimen under a fluo-rescence microscope. In direct immunofluorescence, the primary antibody is labeled with a fluorophore. However, in all the papers we have used indirect immunofluorescence, in which we have selected primary antibodies that bind to the antigen of interest and then added fluorescent secondary antibodies to detect the primary antibody. All cells used for ICC were cultured on coated coverslips and were fixed in 4% paraformaldehyde (PFA). A list of all primary antibodies used in the papers are shown in Table I. Specific markers were used in all papers to stain the three cell types present in the mixed co-culture. As-trocytes were stained with the intermediate filament protein GFAP, neurons with the microtubule-associated protein βIII-tubulin and oligodendrocytes with the myelin-associated enzyme protein 2',3'-Cyclic-nucleotide 3'-phos-phodiesterase (CNPase). It is important to keep in mind that GFAP does not stain the whole cell, but only approximately 15% of the astrocyte, leading to underestimation of actual astrocyte size [213]. Various Aβ antibodies (mAb1C3, 6E10, mAb158 and a polyclonal Aβ42 antibody) were used in the papers. Although they target different epitopes on Aβ, they all stained Aβ equally well. Vectashield mounting medium containing 4',6-diamidino-2-phe-nylindole (DAPI), which binds strongly to A-T rich regions in the DNA, was used to visualize the cell nuclei.
Table 1. List of all primary antibodies used for ICC in the different papers of this thesis.

36
To study degradation of Aβ by the endosomal-lysosomal pathway, we per-formed additional stainings in Paper I against the lysosomal-associated mem-brane proteins LAMP-1 and LAMP-2, as well as the early and late endosomal proteins Rab5 and Rab7, respectively. To investigate if the lysosomes in the Aβ42 protofibril accumulating astrocytes were acidic or not, we performed ex-periments using LysoTracker® Red DND-99, which is a dye that labels acidic organelles in live cells. In Paper II, we used antibodies against apoE to study the expression of this protein in the three different cell types and in combina-tion with the EV marker CD9 and trans-golgi subcellular marker GM-160. The treatment effect of mAb158 was evaluated by analysis of the intensity and area of Aβ inclusions in Paper III. Phalloidin is a phallotoxin produced by the death cap mushroom Amanita phalloides and binds actin filaments of cells. Fluorescein isothiocyanate (FITC) conjugated phalloidin was used in Paper III in combination with Aβ42 antibodies to visualize the cell contours in the presence of Aβ. In order to visualize and analyze the amount of apoptotic cells following EV treatment of cortical neuronal cultures in Paper I and Paper IV, terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) assay was used. This assay detects DNA fragmentation by labeling 3′-hy-droxyl termini generated during apoptosis. However, it is important to be aware of that fragmented DNA may also be visualized by necrotic cells. Therefore, it should not be excluded that TUNEL assay may also stain for necrosis [214]. Neurons were transfected with CellLight® Mitochondria-GFP for 24 h in Paper IV to visualize mitochondria in live cells.
Microscopy techniques Studies of cellular expression, cellular responses, EV release, co-localization, Aβ42 accumulation and clearance were possible by the use of different micros-copy techniques. Following ICC, images of cells were captured using conven-tional fluorescence microscopy. For detailed analysis on co-localization of Aβ42 protofibrils and mAb158 in astrocytes, confocal microscopy was used in Paper I and Paper III. This technique allows scanning across the layers of the specimen to make up a z-stack that can be used to create a three-dimen-sional image. In order to dynamically study mechanisms of Aβ protofibril clearance over time in the co-cultures, we used time-lapse microscopy in Paper I and Paper III. For this purpose, cells were cultured in time-lapse culture dishes with a glass bottom and experiments were performed at 37oC in humidified 5% CO2 in air using a Nikon Biostation Live Cell Recorder. Images were captured every 10 minutes up to 5 days and were combined to a sequential movie. EV-secreting cells and EVs in Paper I, Paper II and Paper IV were visu-alized by transmission electron microscopy (TEM). This technique can be uti-lized to study very small cellular structures down to nanometer range. It uses

37
a beam of electrons to pass through an ultra-thin specimen and only electrons that pass through the specimen will convert into light and create an image. Compared to a regular light microscope, TEM creates images with very high resolution and magnification, due to the lower wavelength of electrons than light. The EV-secreting cells were fixed in 2.5% glutaraldehyde and following ultracentrifugation, EVs were resuspended in PBS before preparation of TEM.
Differential ultracentrifugation One of the most common methods used to isolate EVs from a solution is by differential ultracentrifugation. It requires centrifugation in multiple steps, first at low speed to eliminate cell debris, then at higher spin speed to remove larger vesicles and debris and finally at high speed in the 100 000 x g range. Therefore, ultracentrifugation must always be performed in high vacuum to reduce friction of rotor and air. Differential ultracentrifugation was used in Paper I, Paper II and Paper IV to isolate EVs from the cell culture media of mixed co-cultures (Figure 6). The ultracentrifugation protocol was the same in all three papers, with an initial low-spin speed of 300 x g for 5 min, followed by 2000 x g for 10 min and finally 135 000 x g for 1.5 h at 4oC. Although the EV pellets are not visible by eye after ultracentrifugation, using a swinging bucket rotor (SW28) will make the EVs sediment to the bottom center during ultracentrifugation. The EVs were resuspended in PBS, lysis buffer with pro-tease inhibitors or neurobasal medium depending on the experimental set-up. Analysis of EVs was performed by TEM, mass spectrometry (MS) analysis, western blot analysis and immunoprecipitation (IP). In Paper I and Paper IV, we aimed to investigate the viability and the cellular effects of primary cortical neurons following treatment with EVs isolated from Aβ42 protofibril exposed co-cultures. For this purpose, neuroglial co-cultures were either exposed to Aβ42 protofibrils for 24 h or left untreated, followed by thorough washes in medium to remove any residual Aβ. Cells were kept in the Aβ-free medium and the cell culture medium was collected after 6 and 12 days, pooled, centrifuged in two steps, ultracentrifuged, resuspended in neurobasal medium and added to cortical neurons. In Paper II, we focused more on ana-lyzing the protein content of EVs released by the co-cultures specifically in re-sponse to Aβ42 protofibril exposure. Co-cultures were constantly exposed to Aβ42 protofibrils or left untreated in order to maximize the protein release. In order to discriminate between exosomes and larger MVs in Paper II, we per-formed experiments in which the samples (following the two initial centrifuga-tion steps) were first ultracentrifuged for 30 min at 10 000 x g at 4oC (to pellet MVs). The supernatant was then ultracentrifuged a second time for 1.5 h at 135 000 x g at 4oC (to pellet exosomes). The cellular effects of EV treatment on primary cortical neurons were investigated in closer detail in Paper IV.

38
Figure 6. Experimental set-up for isolation of EVs by differential ultracentrifuga-tion. The collected media was centrifuged in two steps prior to ultracentrifugation. The EV pellets, containing a mixture of larger MVs and exosomes, were resus-pended in PBS, lysis buffer or neurobasal medium depending on the method of anal-ysis. Scale bar: 100 nm.
Enzyme-linked immunosorbent assay Enzyme-linked immunosorbent assay (ELISA) is an immunological technique used for identifying and quantifying the concentration of specific antigens in a sample by using antibodies. Its high sensitivity allows detection of antigens in very low ranges, depending on the interaction between antigen and anti-body. A commonly used type of ELISA in laboratories is the sandwich ELISA. In the first step of a sandwich ELISA, a capture antibody is immobi-lized on a microplate surface. The surface is then blocked to prevent non-spe-cific binding with other proteins of the sample, which are added in the next step. Only antigens that are recognized by the antibody will be captured, while the remaining non-bound proteins are washed away. A biotinylated secondary antibody, linked with a detection enzyme e.g. horseradish peroxidase (HRP), is then added. The addition of a substrate e.g. Enhanced K-blue® substrate will lead to a detectable signal in the presence of antigen due to a measurable color change.

39
In our studies, we have used sandwich ELISAs to specifically measure total Aβ (Aβ1-x and Aβx-42 ELISAs) in Paper I and Paper III, and Aβ protofibrils (mAb158 ELISA) in Paper I. It is important to consider the aggregation state of Aβ when measuring synthetic or biological Aβ. The hydrophobic C-termi-nus of Aβ is often hidden in the core of Aβ aggregates, leading to underesti-mation of actual Aβ levels in C-terminus dependent ELISAs. To circumvent this issue, samples containing Aβ can be boiled in sodium dodecyl sulfate (SDS) to break up the Aβ aggregates into monomeric forms. In this way, the C-terminus of Aβ is accessible to allow detection of total Aβ. Prior to ELISA, all samples (except lysate pellets) in the Aβ1-x and Aβx-42 ELISAs were dena-tured by boiling in SDS and then further diluted to decrease the SDS concen-tration, in order to avoid interference from SDS. No SDS treatment or boiling was performed in samples analyzed with the mAb158 ELISA. As capture an-tibodies in the Aβ1-x and Aβx-42 ELISAs we used the Aβ N-terminal specific mAb82E1 and polyclonal Aβ42 antibody, respectively. The biotinylated mAb4G8, specific for the mid-region of Aβ, was used as detection antibody. In the mAb158 ELISA, the monoclonal mAb158 antibody was used as both the capture and detection antibody. The mAb158 ELISA is designed to spe-cifically measure larger Aβ protofibrils and does therefore not detect Aβ mon-omers or low molecular weight Aβ oligomers. However, more than one epitope has to be present to be detected in the mAb158 ELISA.
Mass spectrometry analysis Mass spectrometry is a common tool for protein identification and quantifica-tion. The mass spectrometer consists of an ion source, a mass analyzer and an ion detection system. To enable analysis of proteins by MS, the proteins are first ionized, then separated according to their (or their fragments) mass to charge ratio (m/z) and finally detected by the system. This allows detection of a large scale of proteins with a relatively high specificity and sensitivity [215]. By coupling a liquid chromatography to the mass spectrometer (LC-MS) and separate the molecules in an additional dimension (retention time), one can further enhance MS sensitivity. In Paper II, we performed a type of LC-MS analysis called shotgun MS based label free (LF) quantification analysis, to study the expression and relative levels of proteins in EVs. Following differ-ential ultracentrifugation, the lysed proteins in the EV samples were first di-gested to peptides by trypsin/Lys-C and then run through the LC-MS. The peptide sequences were identified using a search engine against Uni-Prot/Swiss-Pro human database (in combination with a decoy database), con-taining more than 20 000 human protein sequences. The protein identification was then inferred from the peptide sequences. A lower limit of the false dis-covery rate for proteins had to be selected (p<0.05) in order for them to be considered present in the samples.

40
Western blot analysis Western blot analysis is a molecular biology technique used for immunode-tection of proteins by visualizing the size of your protein of interest. For quan-titative data of protein concentration, ELISA is preferred as it is more reliable than western blot analysis. However, an advantage over ELISA is that western blot analysis allows one to detect the size of the proteins, which makes it pos-sible to be more confident about the specificity of the antibodies. In our stud-ies, the proteins were first denatured by heating in SDS (LDS sample buffer) and dithiothreitol (reducing agent) to give them a negative charge that was proportional to their molecular weight. After sample loading onto a SDS-pol-yacrylamide (SDS-PAGE) gel, an electric field was applied across the gel to enable migration of the negatively charged proteins towards the positive elec-trode, thus separating the proteins according to their molecular weight. All proteins on the gel were transferred to a polyvinylidene fluoride (PVDF) membrane or nitrocellulose membrane (used for Aβ detection) by applying an electrical field, making the proteins migrate towards the positive electrode. The membrane was then blocked to prevent non-specific binding with other proteins of the samples and the primary antibody specific against the protein of interest was added to the membrane. Following overnight incubation, a HRP-conjugated secondary antibody was added and the protein of interest was visualized by enhanced chemiluminescence (ECL). Development by ECL is an indirect method for detecting proteins bound on a membrane. It utilizes a combination of a chemiluminiscent substrate and a strong oxidizing agent to form excited intermediates. When these excited intermediates decay to a lower energy level, they release a strong blue emission at 450 nm wavelength. By applying ECL, it produces intense, prolonged light emission and low back-ground noise. It is also possible to use secondary antibodies directly conju-gated to fluorescent dyes for visualization and quantitative analysis of pro-teins. By using fluorophores with different excitation and emission spectra, differentiation of proteins can be performed on the same membrane. In Paper II, we performed western blot analysis to study the amount of re-leased EVs with various antibodies (flotillin-1, TSG101 and CD9). Moreover, antibody against apoE was used to visualize and quantitatively analyze apoE levels from the EV lysates compared to flotillin-1 levels. In order to evaluate the clearance of Aβ42 in Paper III, we performed western blot analysis on medium samples from untreated and Aβ42 protofibril exposed co-cultures with or without preincubation of mAb158. Western blot analysis on neuronal cell lysates was performed following EV treatment with synaptophysin antibodies in Paper IV to study the intracellular expression of the synaptic marker syn-aptophysin.

41
Immunoprecipitation Immunoprecipitation is a technique used for isolating and concentrating a spe-cific protein of interest by precipitating the protein antigen out of a solution, e.g. by a magnetic particle concentrator. First, antibodies are added in the so-lution to allow specific binding to the antigen. In order to precipitate the anti-gen-antibody complex, a superparamagnetic bead is added to bind to the anti-body, thus enabling precipitation by the magnetic particle concentrator. In Pa-per II, we immunoprecipitated apoE from lysed and intact EVs to investigate the localization of apoE. Dynabeads™ with recombinant Protein G coupled to the surface were used as magnetic beads. After extensive washes in washing buffer, premixed LDS sample buffer and reducing agent were added together with elution buffer to the samples for further investigation by western blot analysis.

42
Results and comments
Being the most numerous glial cell type in the brain, astrocytes have many important functions in the brain, but their role in AD is poorly understood. Insufficient lysosomal degradation has been suggested to be the main cause of sporadic AD [181, 216]. The ineffective degradation may lead to spreading of AD pathology, due to Aβ secretion from the phagocytic cells [217]. Many studies have been focusing on the role of microglia in AD, but the importance of astrocytes has not been thoroughly investigated. Our research group has recently shown that astrocytes effectively engulf whole dead cells, but store, rather than degrade the ingested material [173]. In this thesis, we were inter-ested in investigating the role of astrocytes in Aβ pathology and clearance. Since soluble Aβ aggregates, including protofibrils, have been suggested to be the most neurotoxic Aβ species, we focused on examining the cellular re-sponses of Aβ42 protofibrils.
Cellular uptake and accumulation of Aβ42 protofibrils In order to investigate the uptake and accumulation of Aβ42 protofibrils by the major cell types in the brain, we performed experiments in Paper I, using mixed co-cultures of primary cortical astrocytes (70%), neurons (25%) and oligodendrocytes (5%). The cell cultures were exposed to Aβ42-555 protofi-brils for 24 h, fixed and stained with antibodies against the three cell types to study the amount of intracellular Aβ. Astrocytes, neurons and oligodendro-cytes were stained with GFAP, βIII-tubulin and CNPase, respectively. We found that astrocytes contained large deposits of Aβ42-555, while neurons had almost no detectable levels of intracellular Aβ. Accumulation of Aβ42-555 was also noted in the oligodendrocytes (Figure 7). Interestingly, the Aβ42-555 in-clusions frequently co-localized with DAPI-stained condensed nuclei. The in-tracellular deposits of Aβ42-555 in astrocytes was further confirmed by confo-cal microscopy. To verify that the 555-label was still bound to Aβ after en-gulfment, we exposed parallel co-cultures with unlabeled Aβ and stained them with four different Aβ antibodies (mAb1C3, 6E10, mAb158 and a polyclonal Aβ42 antibody). The immunostainings revealed that all antibodies displayed the same staining pattern as the labeled Aβ42-555 protofibrils, indicating that the 555-label was still bound to Aβ in the detected intracellular Aβ deposits. To follow the engulfment of Aβ42 protofibrils over time, we performed time-

43
lapse experiments, in which we recorded the cell culture during the 24 h Aβ42-555 protofibril exposure. Our results showed that already after 30 min, astro-cytes had accumulated Aβ42-555 and the intensity of the staining increased during the 24 h time period. Immunostainings of brain sections from 14-month-old tg-ArcSwe mice in Paper I demonstrated that reactive astrocytes were tightly localized around the amyloid plaques and Aβ co-localized with astrocytes, confirming that our findings in the cell cultures reflected cellular processes of Aβ pathology in vivo.
Figure 7. Cellular uptake and accumulation of Aβ42 protofibrils. Following 24 h Aβ42-555 protofibril exposure, astrocytes (A) contained large deposits of Aβ42-555, whereas neurons did not (B). Accumulation of Aβ42-555 was noted in oligodendro-cytes (C). GFAP, βIII-tubulin, CNPase (all green), Aβ42-555 (red), DAPI (blue). Scale bar: 20 µm.
Incomplete clearance of Aβ42 protofibrils by astrocytes To follow the degradation of ingested Aβ42 protofibrils, the co-cultures in Pa-per I were washed after the 24 h incubation with Aβ42-555 protofibrils and were cultured for additional 6 or 12 days prior to fixation and immunostaining. Our results demonstrated that astrocytes effectively engulfed Aβ42 protofi-brils, but that the ingested material was only partially degraded within 12 days. The oligodendrocytes contained large or medium-sized Aβ42-555 inclusions that did not significantly change over time. Intensity- and area measurements of the intracellular Aβ42-555 confirmed that astrocytes degraded the Aβ42-555 protofibrils to some degree, although very slowly. In contrast to our results with Aβ42-555 protofibrils, cell cultures exposed to synthetic Aβ40-555 mono-mers showed no accumulation of Aβ in astrocytes. To investigate the intracellular localization of ingested Aβ42 protofibrils in Paper I, immunostainings with the lysosomal marker LAMP-1 were per-formed. Only a limited co-localization between Aβ42 and LAMP-1 was found directly after exposure (24 h), but the co-localization increased over time. At 12 days after Aβ42 protofibril removal, most of the intracellular Aβ deposits

44
co-localized with LAMP-1, indicating that Aβ42 protofibrils were transported to lysosomal compartments within the astrocytes. However, to clarify if the astrocytic lysosomes were acidic enough to degrade the ingested Aβ42 proto-fibrils, additional experiments using the LysoTracker® dye, that labels acidic organelles in live cells, were performed. Interestingly, we found that although the lysosomes were LAMP-1 positive, the Aβ42-containing lysosomes did not stain with the LysoTracker® dye, indicating that Aβ42 protofibrils stored in astrocytes were located in immature lysosomes. We aimed to find out if the Aβ42 stored in the immature lysosomes were partially degraded. For this pur-pose, we analyzed cell culture lysates using three different sets of sandwich ELISAs (the N-terminal dependent Aβ1-x, the protofibril specific mAb158 ELISA and the N-terminal independent Aβx-42 ELISA). The ELISA results showed that a high proportion of the intracellularly stored Aβ was N-termi-nally truncated, indicating that ingested Aβ42 protofibrils were partially de-graded by the astrocytes and processed in a way that could alter their proper-ties and toxicity.
Formation of enlarged endosomes in astrocytes following Aβ42 protofibril exposure Time-lapse recording of cell cultures after Aβ42 protofibril exposure in Paper I revealed an interesting finding. The accumulation of Aβ induced formation of enlarged, dynamic vacuoles in the astrocytes after 2-3 days (Figure 8). The vacuoles were built up successively over time and increased in size (up to ~50 µm in diameter) by fusing with adjacent vacuoles. The giant vacuoles eventu-ally shrank or collapsed, but concurrently, formation of new vacuoles ap-peared in the astrocytes, without causing astrocytic death.
Figure 8. Formation of enlarged endosomes in astrocytes following Aβ42 protofibril exposure. Time-lapse recording taken 5 days after Aβ42 protofibril exposure showed formation of large dynamic vacuoles (white asterisks) that fused inside the astro-cytes. The vacuoles were identified to be enlarged early endosomes. Scale bar: 10 µm.

45
Immunostainings with the specific endosomal markers Rab5 (early endosomal marker) and Rab7 (late endosomal marker) identified the giant vacuoles to be enlarged early endosomes. Thus, these data indicate that the accumulation of Aβ induced severe endosomal-lysosomal defects in the phagocytic astrocytes.
Secondary neuronal toxicity following Aβ42 protofibril exposure To investigate how Aβ42 protofibril exposure affected the viability of astro-cytes, neurons and oligodendrocytes in Paper I, the number of each cell type was manually quantified directly after 24 h exposure, as well as 6 and 12 days after Aβ42 protofibril removal. The total number of living cells was compared to the cell number in parallel, unexposed cell cultures. A significant increase in astrocytes and oligodendrocytes was observed after 12 days, indicating that Aβ42 protofibril exposure triggered proliferation of glial cells. However, the number of neurons significantly decreased in the Aβ42 protofibril exposed cul-tures (Figure 9). This was noted after 12 days and not directly after Aβ42 pro-tofibril removal, indicating that the neuronal cell death was due to a secondary mechanism, most likely connected to the incomplete astrocytic clearance of Aβ42 protofibrils.
Figure 9. Secondary neuronal toxicity following Aβ42 protofibril exposure. The number of astrocytes increased 12 days (24 h + 12 days) after Aβ42 protofibril expo-sure (A). Neuronal cell death was observed 12 days (24 h + 12 days) after Aβ42 pro-tofibril exposure and not directly after exposure (B). Data is presented as relative number of each cell type.

46
Spreading mechanisms of Aβ pathology by the secretion of extracellular vesicles Failure of proper Aβ42 protofibril clearance and the formation of enlarged en-dosomes in astrocytes following Aβ42 protofibril exposure made us hypothe-size that astrocytes may try to get rid of the ingested material by secreting it into EVs. To identify if this was a possible mechanism for the secondary neu-ronal toxicity, we isolated EVs from the cell culture medium by differential ultracentrifugation in Paper I and added these to cortical neuronal cultures. Neurons were fixed after 48 h and the number of apoptotic TUNEL-labeled neurons was quantified. Our results revealed that Aβ42 protofibril-EVs signif-icantly induced neuronal cell death compared to Control-EVs, demonstrating that Aβ42 protofibril accumulation induced secretion of EVs with neurotoxic content. There was no difference in the amount of released EVs between ex-posed and unexposed co-cultures, indicating that the toxicity was due to their content. Interestingly, Aβ1-x and Aβx-42 ELISA analysis of the EV content demonstrated that EVs contained N-terminally truncated Aβ42, suggesting spreading of Aβ pathology by the secretion of EVs. The presence of Aβ in EVs gave us a hint that additional proteins might be altered in response to Aβ42 protofibril exposure, which may be of interest from a biomarker point of view. To elucidate the protein content of the EVs in re-sponse to Aβ42 protofibril exposure, we performed LC-MS analysis of the lysed EVs in Paper II. In order to detect early changes of protein levels at the time of formation of enlarged endosomes and maximize the protein content, co-cultures were constantly exposed to Aβ42 protofibrils for 2 (day 0-2) or 5 (day 2-5) days prior to ultracentrifugation. The LC-MS analysis of the EV content revealed a total of 807 unique proteins, of which five displayed altered levels in Aβ42 protofibril exposed cultures. These proteins were apoE, CNPase, clathrin heavy chain 1, 60S ribosomal protein L4 and cytoplasmic dynein 1 heavy chain 1, all known to be involved in central cellular processes but not known to be directly linked to each other. In particular, we noted that apoE stood out among these proteins and it was the only protein that was in-creased at both time points. We selected to further study apoE due to this fact and because of its strong link to AD. Western blot analysis revealed that the EV release did not change markedly in response to Aβ42 protofibril exposure, but a threefold increase in apoE levels was found in Aβ42 protofibril-EVs com-pared to Control-EVs, both at day 0-2 and day 2-5 (Figure 10A). The apoE was mainly situated inside the EVs, particularly in the exosome fraction (Fig-ure 10B), indicating an endosomal origin. Immunoreactivity of apoE was seen mainly in astrocytes and neurons following Aβ42 protofibrils, suggesting a re-lease of EVs mainly from the secretory astrocytes. The role of apoE in EVs in the spreading of Aβ pathology remains to be further investigated.

47
Figure 10. Increased release of apoE in EVs isolated from Aβ42 protofibril exposed co-cultures. At both day 0-2 and day 2-5, western blot analysis of lysed EVs from Aβ42 protofibril exposed co-cultures (+) demonstrated a threefold increase of apoE, compared to control cultures (-). The EV markers flotillin-1, TSG101 and CD9 showed that the amount of EVs did not change markedly in response to exposure (A). Apolipoprotein E was primarily situated in the exosome fraction, indicating an endosomal origin (B).
To investigate the cellular effects of Aβ42 protofibril-EVs on neurons in closer detail, we performed immunostaining and TUNEL assays of neurons, after 2 and 4 days of EV incubation in Paper IV. Consistent with the results from Paper I, we found significantly less viable neurons and an increased number of apoptotic cells. Moreover, addition of Aβ42 protofibril-EVs resulted in loss of neuronal synapses and dendrites in the living neurons (Figure 11A-B). However, western blot analysis with specific antibodies against the synaptic marker synaptophysin revealed no altered intracellular levels of the protein in presence of Aβ42 protofibril-EVs, compared to Control-EVs. This result sug-gests that there is a reorganization of the existing synaptophysin rather than a change in protein levels. Furthermore, TEM analysis and the CellLight® Mi-tochondria-GFP dye, that labels mitochondria in live cells, demonstrated se-vere mitochondrial impairment in neurons after treatment with Aβ42 protofi-bril-EVs, as seen by their disrupted mitochondrial network and mitochondrial swelling (Figure 11C-D). These results indicate a possible role of EVs in the progression of Aβ-induced pathology.

48
Figure 11. Neuronal effects after Aβ42 protofibril-EV treatment. Cortical neurons displayed long branches of dendrites and synapses after treatment with Control-EVs (A), whereas Aβ42 protofibril-EVs had detrimental effects on the neurons (B). In ad-dition, mitochondria from neurons treated with Control-EVs exhibited healthy mito-chondria (C), but Aβ42 protofibril-EVs induced mitochondrial impairment and swell-ing (red asterisks) (D). Synaptophysin (red), βIII-tubulin (green), DAPI (white). Scale bars: A-B: 20 µm, C-D: 2 µm.
Antibody-mediated effects on astrocytic Aβ42 protofibril clearance The humanized version of the murine Aβ protofibril selective antibody mAb158, called BAN2401, is currently evaluated in phase 2b clinical trials for AD. Although the mAb158 antibody has previously been shown to reduce the levels of pathogenic Aβ and prevent Aβ deposition in tg-ArcSwe mice, the cellular mechanisms of mAb158 and other therapeutic Aβ antibodies remain elusive. In Paper III, we aimed to investigate if mAb158 (IgG2a) could affect the Aβ42 protofibril clearance by astrocytes in the mixed co-culture. Co-cul-tures were exposed to Aβ42-555 protofibrils for 24 h in the presence or absence of mAb158 prior to fixation, or cultured for an additional 6 or 12 days after removal of Aβ42-555 protofibrils and mAb158 prior to fixation. Our ICC data demonstrated that preincubation of Aβ42-555 protofibrils with mAb158 almost abolished the accumulation of astrocytic Aβ42-555 protofibrils, already at 24 h

49
(Figure 12). A reduced effect on astrocytic Aβ accumulation was seen when mAb158 was added 1 h prior to Aβ42-555 protofibril exposure. However, the effect of mAb158 was lost when added 3 days after the Aβ42-555 protofibril exposure, indicating that the preformed extracellular antigen-antibody complex is crucial for the effect to occur. Time-lapse and confocal microscopy confirmed that Aβ42-555 protofibrils and mAb158 co-localized inside the astrocytes and that the intracellular accumulation of Aβ was much weaker at 24 h in presence of mAb158, compared to Aβ42-555 protofibrils only. Similar to mAb158, co-incubation with the mAb1C3 antibody, binding pan-Aβ, also lowered the Aβ42-555 accumulation in astrocytes. To investigate further if the effect was specific for Aβ antibodies, co-cultures were exposed to Aβ42 protofibrils together with the irrelevant antibody Ly-128 (IgG1) or the irrelevant antibody MOPC-173 (IgG2a). The Ly-128 did not reduce the intracellular Aβ and MOPC-173 had a significantly lower effect on the Aβ accumulation, as compared to mAb158, indicating that the effect was mainly specific for Aβ antibodies.
Figure 12. The mAb158 antibody prevents accumulation of Aβ in astrocytes. Accu-mulation of Aβ42-555 protofibrils was notable in astrocytes at 24 h (A). However, antibody treatment almost abolished the accumulation of astrocytic Aβ42-555 proto-fibrils (B). Scale bar: 20 µm.
The intracellular concentration of Aβ42 was significantly reduced after mAb158 treatment in Paper III, as demonstrated by ELISA analysis. Western blot analysis showed an increased clearance of Aβ42 from the cell culture me-dium in the presence of mAb158, indicating that Aβ was not secreted as much by the cells after mAb158 treatment. Importantly, in Paper I and Paper IV, we found that Aβ42 protofibril exposure resulted in increased neuronal cell death by the secretion of Aβ-containing EVs, but mAb158 treatment in Paper III rescued the neurons from Aβ-induced toxicity. However, the effect of

50
mAb158 was not observed when the antibody was added 3 days after Aβ42 protofibril removal. We sought to elucidate the mechanism mediating the Aβ clearance by astro-cytes. To investigate if the mAb158 effect on Aβ protofibril accumulation is Fcγ receptor dependent or Fcγ receptor independent, we used the recombi-nantly produced mAb158 antibody, N297D (IgG2c), which has a mutation on the glycosylation site, leading to loss of receptor-binding and reduced C1q binding. We found that mAb158 with the N297D mutation (asparagine re-placed by aspartic acid) showed almost as good clearing effect of Aβ in the astrocytes, as the mAb158 without the mutation. Moreover, studies were per-formed to investigate if the antigen-binding sites of the mAb158 antibody, called F(ab’)2, could mediate Aβ clearance in the absence of an Fc region. The divalent F(ab’)2 fragment of an antibody is generated by pepsin digestion to remove the Fc region while leaving intact some of the hinge region, thus preventing the fragment to bind to any of the Fcγ receptors. The F(ab’)2 frag-ment of mAb158 also significantly reduced the accumulation of Aβ in astro-cytes, suggesting that the effect of mAb158 on Aβ42 protofibril clearance is mainly a Fcγ receptor independent mechanism. In order to investigate the influence of the proteosomal and endosomal-lysosomal pathway on mAb158-mediated Aβ clearance in astrocytes, we preincubated co-cultures with the proteosomal inhibitor mg-132 or the ly-sosomal inhibitor bafilomycin for 30 min prior to Aβ42 protofibril exposure in the presence or absence of mAb158. The inhibitors were also present during the 24 h exposure. Neither mg-132 nor bafilomycin had any effect on the mAb158-mediated reduction of Aβ deposits in astrocytes, demon-strating that inhibition of the proteosomal or lysosomal pathway did not have an impact on the reduced Aβ accumulation. Taken together, our re-sults indicate that the majority of the antigen-antibody complexes may be degraded by another, not yet described mechanism.
Future perspectives Based on the results of this thesis, one major issue that still remains to be clarified is why the neurons die following Aβ42 protofibril-EV treatment. The EVs may contain other cargo aside from N-terminally truncated Aβ that may induce toxicity. Immunocytochemistry against Aβ42 should be performed in order to assess if EVs transport the Aβ into the neurons. Furthermore, it re-mains unclear if apoE from EVs promote or counteract the Aβ pathology. Nevertheless, it would be of interest to evaluate the biomarker potential of apoE in EVs isolated from human AD CSF samples, including apoE ε4 carri-ers, in order to reflect the in vivo role of apoE in EVs. Whether neurons in culture could be rescued from EV-induced cell death by inhibition of the cel-lular uptake, e.g. by the endocytic inhibitor Dynasore is a relevant question.

51
In addition, this may provide useful insights into the mechanistic action of EVs, i.e. if EVs are required to be endocytosed in order to cause cellular dam-age or if the toxic action occurs extracellularly. The positive effect of mAb158 on the reduction of Aβ accumulation in astrocytes was evident, but the exact mechanism mediating the clearance effect remains unclear. It is likely that mAb158 not only affects the Aβ accumulation, but may also limit the spread-ing of Aβ pathology by EVs. Although our experiments showed that mAb158 still had an effect on the Aβ clearance, regardless of the inhibition of either the proteosomal or endosomal-lysosomal pathway, full blocking is not guar-anteed by the inhibitors. Experiments using different parts of the mAb158 an-tibody still resulted in increased Aβ clearance. In addition, Aβ was cleared rapidly from both the cell culture medium and intracellularly by mAb158 treatment, but only when the antigen and antibody were present at the same time to allow formation of antigen-antibody complexes. Time-lapse recording showed low background signals without increased amount of Aβ complexes floating in the medium. It would therefore be interesting to examine if there are other ways to activate astrocytes to clear Aβ. One hypothesis that may be worth investigating is if the antigen-antibody complexes are able to stimulate the astrocytes to respond by releasing certain molecules that may help clear Aβ already in the extracellular space, thus limiting the uptake by the astro-cytes.

52
Concluding remarks
The work presented in this thesis has increased our understanding of the cel-lular responses to Aβ42 protofibrils, the spreading of Aβ pathology by the se-cretion of EVs and the mechanisms of antibody treatment in a mixed cell cul-ture model exposed to Aβ42 protofibrils. In Paper I, we showed that astrocytes effectively engulf Aβ42 protofibrils, but store, rather than degrade the ingested material. The incomplete degrada-tion of Aβ42 protofibrils resulted in formation of enlarged endosomes in astro-cytes and induced secondary neuronal cell death by the release of N-terminally truncated Aβ in EVs. Our results demonstrate that astrocytes are highly in-volved in Aβ pathology, by accumulating and spreading toxic Aβ species. In Paper II, we found that the release of EVs did not vary in response to Aβ42 protofibril exposure, but the protein content in EVs changed markedly. Specifically, a threefold increase of apoE was confirmed in Aβ42 protofibril-EVs, compared to Control-EVs. This increase of apoE in EVs may be a “de-fense” mechanism of the cells to fibrillize soluble Aβ to less toxic fibrils, but this needs to be further addressed. In Paper III, we demonstrated that mAb158 reduced the astrocytic Aβ pro-tofibril accumulation and rescued neurons from Aβ-induced cell death. Anti-gen binding was crucial for the effect to occur and increased clearance of Aβ was confirmed from both the extracellular and intracellular space. In the AD brain, this type of passive immunization targeting Aβ pathology might en-hance Aβ clearance and thus preserve the functionality of astrocytes. In Paper IV, we showed that spreading of Aβ-induced pathology by the secretion of EVs has detrimental effects on neurons. The Aβ42 protofibril-EVs induced neuronal cell death, destroyed synapses and dendrites and caused mi-tochondrial impairment. These findings may be involved in the neuroinflam-matory process and exacerbation of AD pathology. Taken together, the work presented in this thesis demonstrates a chain of cellular events that occur in response to Aβ42 protofibril exposure, eventually leading to neuronal cell death. Aβ protofibril-selective antibodies may consti-tute a promising therapeutic strategy against AD. By preventing vesicle-me-diated spreading of Aβ, progression of neurodegeneration may be limited.

53
Acknowledgements
This thesis work has been carried out at the division of Molecular Geriatrics at the Department of Public Health and Caring Sciences, Rudbeck Laboratory, Uppsala University. I am grateful for the financial support from the Swedish Research Council, Alzheimer Foundation, Magnus Bergvall Foundation, Gamla Tjänarinnor Foundation, Åke Wiberg Foundation, Åhlén Foundation, Stohnes Foundation, Hedlund Foundation, Dementia Association Foundation, Swedish Geriatric Foundation, Uppsala Berzelii Technology Centre for Neu-rodiagnostics and Uddeholm Foundation (Värmlands Nation). The day before I moved to Uppsala to start my PhD, I read two interesting quotes that left an impression on me. The first quote was the following: It is not because things are difficult that we do not dare, it is because we do not dare that they are difficult. The second quote was: You cannot cross the ocean unless you have the courage to leave the shore. In retrospect, I am very happy I left the shore because, despite a few headwinds at times, it took me on an amazing and unforgettable PhD journey. A journey that has now reached its final destination. This journey would not have been possible or the same with-out a few people. I would like to take the opportunity to acknowledge them here. The first person I would like to thank is my supervisor Anna for allowing me to sail with you. As a captain, you have guided me through this journey with great enthusiasm and wisdom. You have believed in me, supported me, en-couraged me and helped me to grow as a researcher. I have learned a lot from you during these years we have worked together and I am extremely grateful for all the time and effort you have invested in me. On top of that, you are a very nice person. Martin, my co-supervisor, I have always felt your strong support and that you have been there for me whenever I have needed you. You are, in many ways, an inspiring leader with a great passion for science. I appreciate that I got to visit the memory clinic at Akademiska hospital to see the important clinical work you do with the patients. I am grateful for our stimulating discussions, regardless of whether they have been in the office or in an airplane on our way

54
to a conference. Considering everything I have learned from you, it was my pleasure to introduce you to the world of Sudoku. I would like to express my gratitude towards my talented colleagues and col-laborators, who have contributed in the different papers. Sofia, it has been a pleasure working with you and I have appreciated our good teamwork. Dag, our “ELISA king”, thank you for sharing your knowledge and for teaching me that sometimes it is the mistake that saves the analysis. Payam, Ganna and Kim, I am grateful for your excellent work on mass spectrometry and your warm support in my work. Robin, thanks for introducing me to the ultracen-trifuge and for all the fun Midsummer parties in Flogsta. Marlena, thanks for being such a friendly and helpful colleague. Linda S, I appreciate that you let me come to BioArctic AB to do some lab work, it was a success! I have en-joyed getting to know you and the other colleagues there. Lasse, thank you for many inspiring talks. As the former head of the group, you made me feel very welcome when I joined the group. I would like to thank previous and current members of the Molecular Geriat-rics group for creating such a nice and friendly work atmosphere. We have also had some fantastic lab dinners, after works, kick-offs, game nights, movie nights, housewarming parties, birthday parties etc. Stina, I am grateful that you gave me “one bad and one good news” prior to my PhD, showing me that things may not always have only two outcomes, but that there could be a third (really good) opportunity. Energetic Joakim, you bring so much positivity to our group and it is always fun to talk to you. Sweet Ximena, thanks for helping me with administrative issues, for continuously finding new ways to improve our work environment and for our deep lunch conversations. My technical hero Vilmantas, thank you for helping me fix my computer issues. Linn, I am grateful for all your help and support during the past months and your calming and caring aura has a positive effect on me. Emma, I appreciate our friendship and all the great times we have shared together, including singing karaoke during a pub crawl. Gabriel, thanks for all the fun memories from our confer-ences and summer school trips. Anna L, you started in our group the same week as me and we soon became good friends. Sharon, there is never a dull moment with you. Thanks for all the good laughs and for being there ready to give me an astrocyte hug. I am happy I got to do this PhD journey with my friends Leire and Tsong. We have followed and supported each other since day one and it warms my heart to know that we have many wonderful memories together. This journey would not have been the same without you, so thank you both for everything. During my time in the lab, I have had the pleasure to meet a few people from the IGP department. Mi amiga Verónica, you have always been there to give

55
me your good advice and honest opinion. It is easy, spontaneous, relaxing and unpretentious to be with you. Thanks for contributing in making my time in Uppsala beyond pleasant. My friend Matko, I treasure our memories together, including our dinners out, picnics in Sunnersta, Zumba classes (“Zumba let’s go!”) and our summer excursion to Öregrund was priceless. Argyris, thanks for being there for me and cheering me up with your fun personality. I am going to miss our coffee breaks. I would also like to thank Eric, Diego, Chi-ara, Miguel, Kiki, Ross and Emma Y for nice conversations, fun masquerade planning and awesome parties. Mary, my Greek-Italian friend, we found each other even before we both moved to Uppsala and I am grateful that fate brought us together. Valia, I am happy to have you as my friend and I will never forget that time when we queued for an hour out in the freezing winter weather to enter Värmlandsklub-ben, only to leave after fifteen minutes. My ambitious Julia, I hope that we someday can go back to that rooftop bar in Stockholm for delicious drinks and nice view. My wonderful Loreto, we started off as neighbors, but I believe I have found a lifelong friend. I appreciate your genuineness, kindness and thoughtfulness. Our fun trips to Czech Republic, Spain and Germany were amazing and I am sure that more trips will follow. You are simply the best! Thanks also to my other fun former neighbor Zain, for encouraging me to step out of my comfort zone. In the beginning of this journey, I did not know many people in Uppsala, so to have Athina and Frank there for me meant a lot. I appreciate you welcom-ing me and making me feel like home. A little bit more than halfway into my PhD, I met a relative whom I did not know I had in Uppsala. Angelo, indeed, your name reflects your character. Since the moment I met you, life in Uppsala has been quite an adventure. Thank you for enriching it in many ways. To Christina and Uncle Jimmy, I appreciate your kindness and generosity. Some people followed me long before I started this journey. I would like to apologize that I might not always have had much time for you, but you have always been in my mind. I would like to thank my childhood friends Katerina and Helena, for all the creative games we came up with, all the sleepovers and fun trips. You are special to me and I appreciate our long-lasting friendship. My beloved god-parents Jenny and Ilias, I value the memories we have together, not the least

56
from my time in the USA. Thanks to all family friends for always being there, in good and in difficult times, and for all the great parties! Thank you to both my grandparents for your brave decision to come to Swe-den. My wonderful grandparents Elisabeth and Panagiotis, everything you do and say is with love. Thank you for always wanting my best and for always letting the family come in first hand. I would like to honor my grandparents Garifalia and Michail, for encouraging and supporting me in my education. My strong grandmother Garifalia, you gave me special meaning in pursuing my doctoral studies in the field of Alzheimer’s disease and thinking of you during my work has kept me motivated to always do my best. My dear grand-father Michail, your comforting words that everything will be alright, όλα να πάνε καλά, will always continue to echo inside me. Thank you to my aunts Poppi, Mirro and Katerina, for your motherly love and to all my cousins for fun times together! Marco, my fantastic brother-in-law, you are like a brother to me. Thank you for all your help and support over the years, especially dur-ing my thesis work. I owe you many pizzas! My little fighter and adorable niece Valentina, you are a ray of sunshine who brings so much joy and posi-tive energy into my life. I am excited to follow your, and your sibling’s, own magical journey. To my beautiful and wise sister Litsa, we have a special bond that only sisters can have. Throughout my entire life, you have been my best friend, my role model, my mentor and my protector always looking out for me to make sure that I am well. Thank you for being someone I can always lean on and trust. You are an incredible woman with a big heart and I am extremely happy to have you in my life. Finally, I could not have done the big journey without my extraordinary par-ents, Parthéna and Grigorios. Your immense support and unconditional love means everything to me. Mom, thank you for being my best teacher and friend in life. Dad, thank you for encouraging me to always follow my heart, to fight for my dreams and to never give up. It is an honor for me to defend my thesis the same day as you did 27 years ago. Mom and dad, I am forever grateful for everything that you have done for me and I love you both infinitely.

57
References
1. Prince, M., et al., World Alzheimer Report 2016. Improving healthcare for people living with dementia. Coverage, quality and costs now and in the future. 2016: https://www.alz.co.uk/research/WorldAlzheimerReport2016.pdf.
2. Association, A.s., 2017 Alzheimer's disease facts and figures, in Alzheimers Dement 13:325-373. 2017: https://www.alz.org/documents_custom/2017-facts-and-figures.pdf.
3. Alzheimer, A., et al., An English translation of Alzheimer's 1907 paper, "Uber eine eigenartige Erkankung der Hirnrinde". Clin Anat, 1995. 8(6): p. 429-31.
4. Ittner, L.M. and J. Gotz, Amyloid-beta and tau--a toxic pas de deux in Alzheimer's disease. Nat Rev Neurosci, 2011. 12(2): p. 65-72.
5. Pini, L., et al., Brain atrophy in Alzheimer's Disease and aging. Ageing Res Rev, 2016. 30: p. 25-48.
6. Braak, H. and E. Braak, Evolution of neuronal changes in the course of Alzheimer's disease. J Neural Transm Suppl, 1998. 53: p. 127-40.
7. Serra, L., et al., Are the behavioral symptoms of Alzheimer's disease directly associated with neurodegeneration? J Alzheimers Dis, 2010. 21(2): p. 627-39.
8. Mega, M.S., et al., The spectrum of behavioral changes in Alzheimer's disease. Neurology, 1996. 46(1): p. 130-5.
9. Yan, J.H., et al., Alzheimer's disease and mild cognitive impairment deteriorate fine movement control. J Psychiatr Res, 2008. 42(14): p. 1203-12.
10. Komarova, N.L. and C.J. Thalhauser, High degree of heterogeneity in Alzheimer's disease progression patterns. PLoS Comput Biol, 2011. 7(11): p. e1002251.
11. Wattmo, C., E. Londos, and L. Minthon, Response to cholinesterase inhibitors affects lifespan in Alzheimer's disease. BMC Neurol, 2014. 14: p. 173.
12. Brunnstrom, H.R. and E.M. Englund, Cause of death in patients with dementia disorders. Eur J Neurol, 2009. 16(4): p. 488-92.
13. Reitz, C. and R. Mayeux, Alzheimer disease: epidemiology, diagnostic criteria, risk factors and biomarkers. Biochem Pharmacol, 2014. 88(4): p. 640-51.
14. Kang, J., et al., The precursor of Alzheimer's disease amyloid A4 protein resembles a cell-surface receptor. Nature, 1987. 325(6106): p. 733-6.

58
15. Dyrks, T., et al., Identification, transmembrane orientation and biogenesis of the amyloid A4 precursor of Alzheimer's disease. EMBO J, 1988. 7(4): p. 949-57.
16. Golde, T.E., et al., Expression of beta amyloid protein precursor mRNAs: recognition of a novel alternatively spliced form and quantitation in Alzheimer's disease using PCR. Neuron, 1990. 4(2): p. 253-67.
17. van der Kant, R. and L.S. Goldstein, Cellular functions of the amyloid precursor protein from development to dementia. Dev Cell, 2015. 32(4): p. 502-15.
18. Sosa, L.J., et al., The physiological role of the amyloid precursor protein as an adhesion molecule in the developing nervous system. J Neurochem, 2017. 143(1): p. 11-29.
19. Dawkins, E. and D.H. Small, Insights into the physiological function of the beta-amyloid precursor protein: beyond Alzheimer's disease. J Neurochem, 2014. 129(5): p. 756-69.
20. Weggen, S. and D. Beher, Molecular consequences of amyloid precursor protein and presenilin mutations causing autosomal-dominant Alzheimer's disease. Alzheimers Res Ther, 2012. 4(2): p. 9.
21. Tang, Y.P. and E.S. Gershon, Genetic studies in Alzheimer's disease. Dialogues Clin Neurosci, 2003. 5(1): p. 17-26.
22. Ryan, N.S. and M.N. Rossor, Correlating familial Alzheimer's disease gene mutations with clinical phenotype. Biomark Med, 2010. 4(1): p. 99-112.
23. Mullan, M., et al., A pathogenic mutation for probable Alzheimer's disease in the APP gene at the N-terminus of beta-amyloid. Nat Genet, 1992. 1(5): p. 345-7.
24. Goate, A., et al., Segregation of a missense mutation in the amyloid precursor protein gene with familial Alzheimer's disease. Nature, 1991. 349(6311): p. 704-6.
25. Nilsberth, C., et al., The 'Arctic' APP mutation (E693G) causes Alzheimer's disease by enhanced Abeta protofibril formation. Nat Neurosci, 2001. 4(9): p. 887-93.
26. Jonsson, T., et al., A mutation in APP protects against Alzheimer's disease and age-related cognitive decline. Nature, 2012. 488(7409): p. 96-9.
27. Glenner, G.G. and C.W. Wong, Alzheimer's disease and Down's syndrome: sharing of a unique cerebrovascular amyloid fibril protein. Biochem Biophys Res Commun, 1984. 122(3): p. 1131-5.
28. Schupf, N., et al., Specificity of the fivefold increase in AD in mothers of adults with Down syndrome. Neurology, 2001. 57(6): p. 979-84.
29. Schellenberg, G.D., et al., Genetic linkage evidence for a familial Alzheimer's disease locus on chromosome 14. Science, 1992. 258(5082): p. 668-71.
30. Campion, D., et al., Mutations of the presenilin I gene in families with early-onset Alzheimer's disease. Hum Mol Genet, 1995. 4(12): p. 2373-7.

59
31. Levy-Lahad, E., et al., Candidate gene for the chromosome 1 familial Alzheimer's disease locus. Science, 1995. 269(5226): p. 973-7.
32. Rogaev, E.I., et al., Familial Alzheimer's disease in kindreds with missense mutations in a gene on chromosome 1 related to the Alzheimer's disease type 3 gene. Nature, 1995. 376(6543): p. 775-8.
33. Bird, T.D., Alzheimer Disease Overview, in GeneReviews(R), M.P. Adam, et al., Editors. 1993: Seattle (WA).
34. Mayeux, R., Epidemiology of neurodegeneration. Annu Rev Neurosci, 2003. 26: p. 81-104.
35. Kivipelto, M., et al., Midlife vascular risk factors and Alzheimer's disease in later life: longitudinal, population based study. BMJ, 2001. 322(7300): p. 1447-51.
36. Halling, A. and J. Berglund, Association of diagnosis of ischaemic heart disease, diabetes mellitus and heart failure with cognitive function in the elderly population. Eur J Gen Pract, 2006. 12(3): p. 114-9.
37. Anstey, K.J., et al., Smoking as a risk factor for dementia and cognitive decline: a meta-analysis of prospective studies. Am J Epidemiol, 2007. 166(4): p. 367-78.
38. Kivipelto, M., et al., Obesity and vascular risk factors at midlife and the risk of dementia and Alzheimer disease. Arch Neurol, 2005. 62(10): p. 1556-60.
39. Holscher, C., Diabetes as a risk factor for Alzheimer's disease: insulin signalling impairment in the brain as an alternative model of Alzheimer's disease. Biochem Soc Trans, 2011. 39(4): p. 891-7.
40. Guo, Z., et al., Head injury and the risk of AD in the MIRAGE study. Neurology, 2000. 54(6): p. 1316-23.
41. Plassman, B.L., et al., Documented head injury in early adulthood and risk of Alzheimer's disease and other dementias. Neurology, 2000. 55(8): p. 1158-66.
42. Zhou, J., et al., Association between stroke and Alzheimer's disease: systematic review and meta-analysis. J Alzheimers Dis, 2015. 43(2): p. 479-89.
43. Stern, Y., et al., Influence of education and occupation on the incidence of Alzheimer's disease. JAMA, 1994. 271(13): p. 1004-10.
44. Sando, S.B., et al., Risk-reducing effect of education in Alzheimer's disease. Int J Geriatr Psychiatry, 2008. 23(11): p. 1156-62.
45. Lindsay, J., et al., Risk factors for Alzheimer's disease: a prospective analysis from the Canadian Study of Health and Aging. Am J Epidemiol, 2002. 156(5): p. 445-53.
46. Scarmeas, N., et al., Influence of leisure activity on the incidence of Alzheimer's disease. Neurology, 2001. 57(12): p. 2236-42.
47. Corder, E.H., et al., Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer's disease in late onset families. Science, 1993. 261(5123): p. 921-3.
48. Poirier, J., et al., Apolipoprotein E polymorphism and Alzheimer's disease. Lancet, 1993. 342(8873): p. 697-9.

60
49. Mahley, R.W., Apolipoprotein E: cholesterol transport protein with expanding role in cell biology. Science, 1988. 240(4852): p. 622-30.
50. Zhang, J. and Q. Liu, Cholesterol metabolism and homeostasis in the brain. Protein Cell, 2015. 6(4): p. 254-64.
51. Pitas, R.E., et al., Astrocytes synthesize apolipoprotein E and metabolize apolipoprotein E-containing lipoproteins. Biochim Biophys Acta, 1987. 917(1): p. 148-61.
52. Bao, F., et al., Expression of apolipoprotein E in normal and diverse neurodegenerative disease brain. Neuroreport, 1996. 7(11): p. 1733-9.
53. Diedrich, J.F., et al., Neuropathological changes in scrapie and Alzheimer's disease are associated with increased expression of apolipoprotein E and cathepsin D in astrocytes. J Virol, 1991. 65(9): p. 4759-68.
54. Xu, P.T., et al., Sialylated human apolipoprotein E (apoEs) is preferentially associated with neuron-enriched cultures from APOE transgenic mice. Neurobiol Dis, 1999. 6(1): p. 63-75.
55. Xu, Q., et al., Profile and regulation of apolipoprotein E (ApoE) expression in the CNS in mice with targeting of green fluorescent protein gene to the ApoE locus. J Neurosci, 2006. 26(19): p. 4985-94.
56. Corona, A. and G. Landreth, Lipidated APOE has effects on cognitive function that are independent of amyloid-beta pathology. Brain, 2015. 138(Pt 12): p. 3470-2.
57. Fagan, A.M., et al., Unique lipoproteins secreted by primary astrocytes from wild type, apoE (-/-), and human apoE transgenic mice. J Biol Chem, 1999. 274(42): p. 30001-7.
58. Wahrle, S.E., et al., ABCA1 is required for normal central nervous system ApoE levels and for lipidation of astrocyte-secreted apoE. J Biol Chem, 2004. 279(39): p. 40987-93.
59. Kim, W.S., et al., Role of ABCG1 and ABCA1 in regulation of neuronal cholesterol efflux to apolipoprotein E discs and suppression of amyloid-beta peptide generation. J Biol Chem, 2007. 282(5): p. 2851-61.
60. Rebeck, G.W., et al., The generation and function of soluble apoE receptors in the CNS. Mol Neurodegener, 2006. 1: p. 15.
61. Liu, M., et al., Apolipoprotein E gene polymorphism and Alzheimer's disease in Chinese population: a meta-analysis. Sci Rep, 2014. 4: p. 4383.
62. Liu, C.C., et al., Apolipoprotein E and Alzheimer disease: risk, mechanisms and therapy. Nat Rev Neurol, 2013. 9(2): p. 106-18.
63. Corbo, R.M. and R. Scacchi, Apolipoprotein E (APOE) allele distribution in the world. Is APOE*4 a 'thrifty' allele? Ann Hum Genet, 1999. 63(Pt 4): p. 301-10.
64. Farrer, L.A., et al., Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease. A meta-analysis. APOE and Alzheimer Disease Meta Analysis Consortium. JAMA, 1997. 278(16): p. 1349-56.

61
65. Raber, J., Y. Huang, and J.W. Ashford, ApoE genotype accounts for the vast majority of AD risk and AD pathology. Neurobiol Aging, 2004. 25(5): p. 641-50.
66. Martins, C.A., et al., APOE alleles predict the rate of cognitive decline in Alzheimer disease: a nonlinear model. Neurology, 2005. 65(12): p. 1888-93.
67. Nishiyama, E., et al., Distribution of apolipoprotein E in senile plaques in brains with Alzheimer's disease: investigation with the confocal laser scan microscope. Brain Res, 1997. 750(1-2): p. 20-4.
68. Koistinaho, M., et al., Apolipoprotein E promotes astrocyte colocalization and degradation of deposited amyloid-beta peptides. Nat Med, 2004. 10(7): p. 719-26.
69. Esch, F.S., et al., Cleavage of amyloid beta peptide during constitutive processing of its precursor. Science, 1990. 248(4959): p. 1122-4.
70. Sisodia, S.S., et al., Evidence that beta-amyloid protein in Alzheimer's disease is not derived by normal processing. Science, 1990. 248(4954): p. 492-5.
71. Furukawa, K., et al., Increased activity-regulating and neuroprotective efficacy of alpha-secretase-derived secreted amyloid precursor protein conferred by a C-terminal heparin-binding domain. J Neurochem, 1996. 67(5): p. 1882-96.
72. Mattson, M.P., Cellular actions of beta-amyloid precursor protein and its soluble and fibrillogenic derivatives. Physiol Rev, 1997. 77(4): p. 1081-132.
73. Lichtenthaler, S.F., alpha-secretase in Alzheimer's disease: molecular identity, regulation and therapeutic potential. J Neurochem, 2011. 116(1): p. 10-21.
74. Chow, V.W., et al., An overview of APP processing enzymes and products. Neuromolecular Med, 2010. 12(1): p. 1-12.
75. Nikolaev, A., et al., APP binds DR6 to trigger axon pruning and neuron death via distinct caspases. Nature, 2009. 457(7232): p. 981-9.
76. Findeis, M.A., The role of amyloid beta peptide 42 in Alzheimer's disease. Pharmacol Ther, 2007. 116(2): p. 266-86.
77. Sun, X., W.D. Chen, and Y.D. Wang, beta-Amyloid: the key peptide in the pathogenesis of Alzheimer's disease. Front Pharmacol, 2015. 6: p. 221.
78. Yan, Y. and C. Wang, Abeta42 is more rigid than Abeta40 at the C terminus: implications for Abeta aggregation and toxicity. J Mol Biol, 2006. 364(5): p. 853-62.
79. Suzuki, N., et al., An increased percentage of long amyloid beta protein secreted by familial amyloid beta protein precursor (beta APP717) mutants. Science, 1994. 264(5163): p. 1336-40.
80. Gravina, S.A., et al., Amyloid beta protein (A beta) in Alzheimer's disease brain. Biochemical and immunocytochemical analysis with antibodies specific for forms ending at A beta 40 or A beta 42(43). J Biol Chem, 1995. 270(13): p. 7013-6.

62
81. Shankar, G.M., et al., Amyloid-beta protein dimers isolated directly from Alzheimer's brains impair synaptic plasticity and memory. Nat Med, 2008. 14(8): p. 837-42.
82. Townsend, M., et al., Effects of secreted oligomers of amyloid beta-protein on hippocampal synaptic plasticity: a potent role for trimers. J Physiol, 2006. 572(Pt 2): p. 477-92.
83. Walsh, D.M., et al., Naturally secreted oligomers of amyloid beta protein potently inhibit hippocampal long-term potentiation in vivo. Nature, 2002. 416(6880): p. 535-9.
84. Walsh, D.M., et al., Amyloid beta-protein fibrillogenesis. Structure and biological activity of protofibrillar intermediates. J Biol Chem, 1999. 274(36): p. 25945-52.
85. Caughey, B. and P.T. Lansbury, Protofibrils, pores, fibrils, and neurodegeneration: separating the responsible protein aggregates from the innocent bystanders. Annu Rev Neurosci, 2003. 26: p. 267-98.
86. McLean, C.A., et al., Soluble pool of Abeta amyloid as a determinant of severity of neurodegeneration in Alzheimer's disease. Ann Neurol, 1999. 46(6): p. 860-6.
87. Walsh, D.M., et al., Amyloid beta-protein fibrillogenesis. Detection of a protofibrillar intermediate. J Biol Chem, 1997. 272(35): p. 22364-72.
88. Hu, X., et al., Amyloid seeds formed by cellular uptake, concentration, and aggregation of the amyloid-beta peptide. Proc Natl Acad Sci U S A, 2009. 106(48): p. 20324-9.
89. Sowade, R.F. and T.R. Jahn, Seed-induced acceleration of amyloid-beta mediated neurotoxicity in vivo. Nat Commun, 2017. 8(1): p. 512.
90. Dickson, D.W., et al., Correlations of synaptic and pathological markers with cognition of the elderly. Neurobiol Aging, 1995. 16(3): p. 285-98; discussion 298-304.
91. Lue, L.F., et al., Soluble amyloid beta peptide concentration as a predictor of synaptic change in Alzheimer's disease. Am J Pathol, 1999. 155(3): p. 853-62.
92. Lambert, M.P., et al., Diffusible, nonfibrillar ligands derived from Abeta1-42 are potent central nervous system neurotoxins. Proc Natl Acad Sci U S A, 1998. 95(11): p. 6448-53.
93. Naslund, J., et al., Correlation between elevated levels of amyloid beta-peptide in the brain and cognitive decline. Jama-Journal of the American Medical Association, 2000. 283(12): p. 1571-1577.
94. Lesne, S., L. Kotilinek, and K.H. Ashe, Plaque-bearing mice with reduced levels of oligomeric amyloid-beta assemblies have intact memory function. Neuroscience, 2008. 151(3): p. 745-9.
95. Martins, I.C., et al., Lipids revert inert Abeta amyloid fibrils to neurotoxic protofibrils that affect learning in mice. EMBO J, 2008. 27(1): p. 224-33.
96. Stern, E.A., et al., Cortical synaptic integration in vivo is disrupted by amyloid-beta plaques. J Neurosci, 2004. 24(19): p. 4535-40.

63
97. Moreth, J., et al., Globular and protofibrillar abeta aggregates impair neurotransmission by different mechanisms. Biochemistry, 2013. 52(8): p. 1466-76.
98. Barghorn, S., et al., Globular amyloid beta-peptide oligomer - a homogenous and stable neuropathological protein in Alzheimer's disease. J Neurochem, 2005. 95(3): p. 834-47.
99. Cleary, J.P., et al., Natural oligomers of the amyloid-beta protein specifically disrupt cognitive function. Nat Neurosci, 2005. 8(1): p. 79-84.
100. Reed, M.N., et al., Cognitive effects of cell-derived and synthetically derived Abeta oligomers. Neurobiol Aging, 2011. 32(10): p. 1784-94.
101. Carrillo-Mora, P., R. Luna, and L. Colin-Barenque, Amyloid beta: multiple mechanisms of toxicity and only some protective effects? Oxid Med Cell Longev, 2014. 2014: p. 795375.
102. Hardy, J.A. and G.A. Higgins, Alzheimer's disease: the amyloid cascade hypothesis. Science, 1992. 256(5054): p. 184-5.
103. Reitz, C., Alzheimer's disease and the amyloid cascade hypothesis: a critical review. Int J Alzheimers Dis, 2012. 2012: p. 369808.
104. Karran, E., M. Mercken, and B. De Strooper, The amyloid cascade hypothesis for Alzheimer's disease: an appraisal for the development of therapeutics. Nat Rev Drug Discov, 2011. 10(9): p. 698-712.
105. Mucke, L. and D.J. Selkoe, Neurotoxicity of amyloid beta-protein: synaptic and network dysfunction. Cold Spring Harb Perspect Med, 2012. 2(7): p. a006338.
106. Esparza, T.J., et al., Amyloid-beta oligomerization in Alzheimer dementia versus high-pathology controls. Ann Neurol, 2013. 73(1): p. 104-19.
107. McKhann, G., et al., Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology, 1984. 34(7): p. 939-44.
108. Albert, M.S., et al., The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement, 2011. 7(3): p. 270-9.
109. Benson, A.D., et al., Screening for Early Alzheimer's Disease: Is There Still a Role for the Mini-Mental State Examination? Prim Care Companion J Clin Psychiatry, 2005. 7(2): p. 62-69.
110. Zetterberg, H., Cerebrospinal fluid biomarkers for Alzheimer's disease: current limitations and recent developments. Curr Opin Psychiatry, 2015. 28(5): p. 402-9.
111. Marcus, C., E. Mena, and R.M. Subramaniam, Brain PET in the diagnosis of Alzheimer's disease. Clin Nucl Med, 2014. 39(10): p. e413-22; quiz e423-6.

64
112. Massoud, F. and S. Gauthier, Update on the pharmacological treatment of Alzheimer's disease. Curr Neuropharmacol, 2010. 8(1): p. 69-80.
113. Reisberg, B., et al., Memantine in moderate-to-severe Alzheimer's disease. N Engl J Med, 2003. 348(14): p. 1333-41.
114. Schenk, D., et al., Immunization with amyloid-beta attenuates Alzheimer-disease-like pathology in the PDAPP mouse. Nature, 1999. 400(6740): p. 173-7.
115. Morgan, D., et al., A beta peptide vaccination prevents memory loss in an animal model of Alzheimer's disease. Nature, 2000. 408(6815): p. 982-5.
116. Orgogozo, J.M., et al., Subacute meningoencephalitis in a subset of patients with AD after Abeta42 immunization. Neurology, 2003. 61(1): p. 46-54.
117. Gilman, S., et al., Clinical effects of Abeta immunization (AN1792) in patients with AD in an interrupted trial. Neurology, 2005. 64(9): p. 1553-62.
118. Salloway, S., et al., Two phase 3 trials of bapineuzumab in mild-to-moderate Alzheimer's disease. N Engl J Med, 2014. 370(4): p. 322-33.
119. Doody, R.S., et al., Phase 3 trials of solanezumab for mild-to-moderate Alzheimer's disease. N Engl J Med, 2014. 370(4): p. 311-21.
120. Lannfelt, L., et al., Perspectives on future Alzheimer therapies: amyloid-beta protofibrils - a new target for immunotherapy with BAN2401 in Alzheimer's disease. Alzheimers Res Ther, 2014. 6(2): p. 16.
121. Sevigny, J., et al., The antibody aducanumab reduces Abeta plaques in Alzheimer's disease. Nature, 2016. 537(7618): p. 50-6.
122. Coraci, I.S., et al., CD36, a class B scavenger receptor, is expressed on microglia in Alzheimer's disease brains and can mediate production of reactive oxygen species in response to beta-amyloid fibrils. Am J Pathol, 2002. 160(1): p. 101-12.
123. Liu, Y., et al., LPS receptor (CD14): a receptor for phagocytosis of Alzheimer's amyloid peptide. Brain, 2005. 128(Pt 8): p. 1778-89.
124. Kamphuis, W., et al., Transcriptional profiling of CD11c-positive microglia accumulating around amyloid plaques in a mouse model for Alzheimer's disease. Biochim Biophys Acta, 2016. 1862(10): p. 1847-60.
125. Okun, E., M.P. Mattson, and T.V. Arumugam, Involvement of Fc receptors in disorders of the central nervous system. Neuromolecular Med, 2010. 12(2): p. 164-78.
126. Perlmutter, L.S., et al., MHC class II-positive microglia in human brain: association with Alzheimer lesions. J Neurosci Res, 1992. 33(4): p. 549-58.

65
127. Parajuli, B., et al., Oligomeric amyloid beta induces IL-1beta processing via production of ROS: implication in Alzheimer's disease. Cell Death Dis, 2013. 4: p. e975.
128. Strohmeyer, R., et al., Microglial responses to amyloid beta peptide opsonization and indomethacin treatment. J Neuroinflammation, 2005. 2: p. 18.
129. Bhaskar, K., et al., Microglial derived tumor necrosis factor-alpha drives Alzheimer's disease-related neuronal cell cycle events. Neurobiol Dis, 2014. 62: p. 273-85.
130. Eikelenboom, P. and F.C. Stam, Immunoglobulins and complement factors in senile plaques. An immunoperoxidase study. Acta Neuropathol, 1982. 57(2-3): p. 239-42.
131. Frautschy, S.A., et al., Microglial response to amyloid plaques in APPsw transgenic mice. Am J Pathol, 1998. 152(1): p. 307-17.
132. Griffin, W.S., et al., Brain interleukin 1 and S-100 immunoreactivity are elevated in Down syndrome and Alzheimer disease. Proc Natl Acad Sci U S A, 1989. 86(19): p. 7611-5.
133. Tooyama, I., et al., Reactive microglia express class I and class II major histocompatibility complex antigens in Alzheimer's disease. Brain Res, 1990. 523(2): p. 273-80.
134. Pekny, M. and M. Pekna, Astrocyte reactivity and reactive astrogliosis: costs and benefits. Physiol Rev, 2014. 94(4): p. 1077-98.
135. Massaad, C.A., Neuronal and vascular oxidative stress in Alzheimer's disease. Curr Neuropharmacol, 2011. 9(4): p. 662-73.
136. Colton, C.A., Heterogeneity of microglial activation in the innate immune response in the brain. J Neuroimmune Pharmacol, 2009. 4(4): p. 399-418.
137. Tremblay, M.E., et al., The role of microglia in the healthy brain. J Neurosci, 2011. 31(45): p. 16064-9.
138. Solito, E. and M. Sastre, Microglia function in Alzheimer's disease. Front Pharmacol, 2012. 3: p. 14.
139. Liddelow, S.A., et al., Neurotoxic reactive astrocytes are induced by activated microglia. Nature, 2017. 541(7638): p. 481-487.
140. Kofuji, P. and E.A. Newman, Potassium buffering in the central nervous system. Neuroscience, 2004. 129(4): p. 1045-56.
141. Obara, M., M. Szeliga, and J. Albrecht, Regulation of pH in the mammalian central nervous system under normal and pathological conditions: Facts and hypotheses. Neurochemistry International, 2008. 52(6): p. 905-919.
142. Sattler, R. and J.D. Rothstein, Regulation and dysregulation of glutamate transporters. Handb Exp Pharmacol, 2006(175): p. 277-303.
143. Lajtha, A., S. Berl, and H. Waelsch, Amino acid and protein metabolism of the brain. IV. The metabolism of glutamic acid. J Neurochem, 1959. 3(4): p. 322-32.

66
144. Anderson, C.M. and M. Nedergaard, Astrocyte-mediated control of cerebral microcirculation. Trends Neurosci, 2003. 26(7): p. 340-4; author reply 344-5.
145. Amiry-Moghaddam, M. and O.P. Ottersen, The molecular basis of water transport in the brain. Nat Rev Neurosci, 2003. 4(12): p. 991-1001.
146. Escartin, C. and N. Rouach, Astroglial networking contributes to neurometabolic coupling. Front Neuroenergetics, 2013. 5: p. 4.
147. Bezzi, P. and A. Volterra, A neuron-glia signalling network in the active brain. Curr Opin Neurobiol, 2001. 11(3): p. 387-94.
148. Jessen, N.A., et al., The Glymphatic System: A Beginner's Guide. Neurochem Res, 2015. 40(12): p. 2583-99.
149. Abbott, N.J., L. Ronnback, and E. Hansson, Astrocyte-endothelial interactions at the blood-brain barrier. Nat Rev Neurosci, 2006. 7(1): p. 41-53.
150. von Bartheld, C.S., J. Bahney, and S. Herculano-Houzel, The search for true numbers of neurons and glial cells in the human brain: A review of 150 years of cell counting. J Comp Neurol, 2016. 524(18): p. 3865-3895.
151. Herculano-Houzel, S., The glia/neuron ratio: how it varies uniformly across brain structures and species and what that means for brain physiology and evolution. Glia, 2014. 62(9): p. 1377-91.
152. Zhang, Y. and B.A. Barres, Astrocyte heterogeneity: an underappreciated topic in neurobiology. Curr Opin Neurobiol, 2010. 20(5): p. 588-94.
153. Verkhratsky, A., J.J. Rodriguez, and V. Parpura, Calcium signalling in astroglia. Mol Cell Endocrinol, 2012. 353(1-2): p. 45-56.
154. Kimelberg, H.K. and M. Nedergaard, Functions of astrocytes and their potential as therapeutic targets. Neurotherapeutics, 2010. 7(4): p. 338-53.
155. Pekny, M., U. Wilhelmsson, and M. Pekna, The dual role of astrocyte activation and reactive gliosis. Neurosci Lett, 2014. 565: p. 30-8.
156. Heneka, M.T., et al., Focal glial activation coincides with increased BACE1 activation and precedes amyloid plaque deposition in APP[V717I] transgenic mice. J Neuroinflammation, 2005. 2: p. 22.
157. Daschil, N. and C. Humpel, Green-Fluorescent Protein(+) Astrocytes Attach to Beta-Amyloid Plaques in an Alzheimer Mouse Model and Are Sensitive for Clasmatodendrosis. Front Aging Neurosci, 2016. 8: p. 75.
158. Holcomb, L., et al., Accelerated Alzheimer-type phenotype in transgenic mice carrying both mutant amyloid precursor protein and presenilin 1 transgenes. Nat Med, 1998. 4(1): p. 97-100.
159. Thomason, L.A., et al., Reactive astrocytes associated with plaques in TgCRND8 mouse brain and in human Alzheimer brain express phosphoprotein enriched in astrocytes (PEA-15). FEBS Lett, 2013. 587(15): p. 2448-54.

67
160. Pike, C.J., B.J. Cummings, and C.W. Cotman, Early association of reactive astrocytes with senile plaques in Alzheimer's disease. Exp Neurol, 1995. 132(2): p. 172-9.
161. Rodriguez-Arellano, J.J., et al., Astrocytes in physiological aging and Alzheimer's disease. Neuroscience, 2016. 323: p. 170-82.
162. Abramov, A.Y., L. Canevari, and M.R. Duchen, Changes in intracellular calcium and glutathione in astrocytes as the primary mechanism of amyloid neurotoxicity. J Neurosci, 2003. 23(12): p. 5088-95.
163. Peters, O., et al., Astrocyte function is modified by Alzheimer's disease-like pathology in aged mice. J Alzheimers Dis, 2009. 18(1): p. 177-89.
164. Hong, L., H.C. Huang, and Z.F. Jiang, Relationship between amyloid-beta and the ubiquitin-proteasome system in Alzheimer's disease. Neurol Res, 2014. 36(3): p. 276-82.
165. Deane, R., A. Sagare, and B.V. Zlokovic, The role of the cell surface LRP and soluble LRP in blood-brain barrier Abeta clearance in Alzheimer's disease. Curr Pharm Des, 2008. 14(16): p. 1601-5.
166. Alvira-Botero, X. and E.M. Carro, Clearance of amyloid-beta peptide across the choroid plexus in Alzheimer's disease. Curr Aging Sci, 2010. 3(3): p. 219-29.
167. Sokolowski, J.D. and J.W. Mandell, Phagocytic clearance in neurodegeneration. Am J Pathol, 2011. 178(4): p. 1416-28.
168. Lee, S.J., B.R. Seo, and J.Y. Koh, Metallothionein-3 modulates the amyloid beta endocytosis of astrocytes through its effects on actin polymerization. Mol Brain, 2015. 8(1): p. 84.
169. Chang, G.H., N.M. Barbaro, and R.O. Pieper, Phosphatidylserine-dependent phagocytosis of apoptotic glioma cells by normal human microglia, astrocytes, and glioma cells. Neuro Oncol, 2000. 2(3): p. 174-83.
170. Chung, W.S., et al., Astrocytes mediate synapse elimination through MEGF10 and MERTK pathways. Nature, 2013. 504(7480): p. 394-400.
171. Fellner, L., et al., Toll-like receptor 4 is required for alpha-synuclein dependent activation of microglia and astroglia. Glia, 2013. 61(3): p. 349-60.
172. Jones, R.S., et al., Amyloid-beta-induced astrocytic phagocytosis is mediated by CD36, CD47 and RAGE. J Neuroimmune Pharmacol, 2013. 8(1): p. 301-11.
173. Loov, C., et al., Engulfing astrocytes protect neurons from contact-induced apoptosis following injury. PLoS One, 2012. 7(3): p. e33090.
174. Allen, L.A. and A. Aderem, Mechanisms of phagocytosis. Curr Opin Immunol, 1996. 8(1): p. 36-40.
175. Conner, S.D. and S.L. Schmid, Regulated portals of entry into the cell. Nature, 2003. 422(6927): p. 37-44.

68
176. Lee, C.Y. and G.E. Landreth, The role of microglia in amyloid clearance from the AD brain. J Neural Transm (Vienna), 2010. 117(8): p. 949-60.
177. Liddelow, S. and D. Hoyer, Astrocytes: Adhesion Molecules and Immunomodulation. Curr Drug Targets, 2016. 17(16): p. 1871-1881.
178. Zhang, H., et al., Activated scavenger receptor A promotes glial internalization of abeta. PLoS One, 2014. 9(4): p. e94197.
179. Laifenfeld, D., et al., Rab5 mediates an amyloid precursor protein signaling pathway that leads to apoptosis. J Neurosci, 2007. 27(27): p. 7141-53.
180. Poteryaev, D., et al., Identification of the switch in early-to-late endosome transition. Cell, 2010. 141(3): p. 497-508.
181. Appelqvist, H., et al., The lysosome: from waste bag to potential therapeutic target. J Mol Cell Biol, 2013. 5(4): p. 214-26.
182. Scott, C.C. and J. Gruenberg, Ion flux and the function of endosomes and lysosomes: pH is just the start: the flux of ions across endosomal membranes influences endosome function not only through regulation of the luminal pH. Bioessays, 2011. 33(2): p. 103-10.
183. Cataldo, A.M., et al., Abeta localization in abnormal endosomes: association with earliest Abeta elevations in AD and Down syndrome. Neurobiol Aging, 2004. 25(10): p. 1263-72.
184. Cataldo, A.M., et al., Endocytic pathway abnormalities precede amyloid beta deposition in sporadic Alzheimer's disease and Down syndrome: differential effects of APOE genotype and presenilin mutations. Am J Pathol, 2000. 157(1): p. 277-86.
185. Keller, S., et al., Body fluid derived exosomes as a novel template for clinical diagnostics. J Transl Med, 2011. 9: p. 86.
186. Thery, C., et al., Isolation and characterization of exosomes from cell culture supernatants and biological fluids. Curr Protoc Cell Biol, 2006. Chapter 3: p. Unit 3 22.
187. Lasser, C., et al., Human saliva, plasma and breast milk exosomes contain RNA: uptake by macrophages. J Transl Med, 2011. 9: p. 9.
188. Li, P., et al., Progress in Exosome Isolation Techniques. Theranostics, 2017. 7(3): p. 789-804.
189. Cocucci, E., G. Racchetti, and J. Meldolesi, Shedding microvesicles: artefacts no more. Trends Cell Biol, 2009. 19(2): p. 43-51.
190. Johnstone, R.M., Exosomes biological significance: A concise review. Blood Cells Mol Dis, 2006. 36(2): p. 315-21.
191. Hsu, C., et al., Regulation of exosome secretion by Rab35 and its GTPase-activating proteins TBC1D10A-C. J Cell Biol, 2010. 189(2): p. 223-32.
192. Ostrowski, M., et al., Rab27a and Rab27b control different steps of the exosome secretion pathway. Nat Cell Biol, 2010. 12(1): p. 19-30; sup pp 1-13.
193. Morelli, A.E., et al., Endocytosis, intracellular sorting, and processing of exosomes by dendritic cells. Blood, 2004. 104(10): p. 3257-66.

69
194. Fitzner, D., et al., Selective transfer of exosomes from oligodendrocytes to microglia by macropinocytosis. J Cell Sci, 2011. 124(Pt 3): p. 447-58.
195. Potolicchio, I., et al., Proteomic analysis of microglia-derived exosomes: metabolic role of the aminopeptidase CD13 in neuropeptide catabolism. J Immunol, 2005. 175(4): p. 2237-43.
196. Faure, J., et al., Exosomes are released by cultured cortical neurones. Mol Cell Neurosci, 2006. 31(4): p. 642-8.
197. Fevrier, B., et al., Cells release prions in association with exosomes. Proc Natl Acad Sci U S A, 2004. 101(26): p. 9683-8.
198. Lim, Y.J. and S.J. Lee, Are exosomes the vehicle for protein aggregate propagation in neurodegenerative diseases? Acta Neuropathol Commun, 2017. 5(1): p. 64.
199. Rajendran, L., et al., Alzheimer's disease beta-amyloid peptides are released in association with exosomes. Proc Natl Acad Sci U S A, 2006. 103(30): p. 11172-7.
200. Vingtdeux, V., et al., Alkalizing drugs induce accumulation of amyloid precursor protein by-products in luminal vesicles of multivesicular bodies. J Biol Chem, 2007. 282(25): p. 18197-205.
201. Perez-Gonzalez, R., et al., The exosome secretory pathway transports amyloid precursor protein carboxyl-terminal fragments from the cell into the brain extracellular space. J Biol Chem, 2012. 287(51): p. 43108-15.
202. Kokubo, H., et al., Part of membrane-bound Abeta exists in rafts within senile plaques in Tg2576 mouse brain. Neurobiol Aging, 2005. 26(4): p. 409-18.
203. Kokubo, H., C.A. Lemere, and H. Yamaguchi, Localization of flotillins in human brain and their accumulation with the progression of Alzheimer's disease pathology. Neurosci Lett, 2000. 290(2): p. 93-6.
204. Joshi, P., et al., Extracellular vesicles in Alzheimer's disease: friends or foes? Focus on abeta-vesicle interaction. Int J Mol Sci, 2015. 16(3): p. 4800-13.
205. Yuyama, K., et al., Sphingolipid-modulated exosome secretion promotes clearance of amyloid-beta by microglia. J Biol Chem, 2012. 287(14): p. 10977-89.
206. Englund, H., et al., Sensitive ELISA detection of amyloid-beta protofibrils in biological samples. J Neurochem, 2007. 103(1): p. 334-45.
207. Lord, A., et al., The Arctic Alzheimer mutation facilitates early intraneuronal Abeta aggregation and senile plaque formation in transgenic mice. Neurobiol Aging, 2006. 27(1): p. 67-77.
208. Lord, A., et al., Amyloid-beta protofibril levels correlate with spatial learning in Arctic Alzheimer's disease transgenic mice. FEBS J, 2009. 276(4): p. 995-1006.

70
209. Lindstrom, V., et al., Extensive uptake of alpha-synuclein oligomers in astrocytes results in sustained intracellular deposits and mitochondrial damage. Mol Cell Neurosci, 2017. 82: p. 143-156.
210. Teplow, D.B., Preparation of amyloid beta-protein for structural and functional studies. Methods Enzymol, 2006. 413: p. 20-33.
211. Fezoui, Y., et al., An improved method of preparing the amyloid beta-protein for fibrillogenesis and neurotoxicity experiments. Amyloid, 2000. 7(3): p. 166-78.
212. Jan, A., D.M. Hartley, and H.A. Lashuel, Preparation and characterization of toxic Abeta aggregates for structural and functional studies in Alzheimer's disease research. Nat Protoc, 2010. 5(6): p. 1186-209.
213. Bushong, E.A., et al., Protoplasmic astrocytes in CA1 stratum radiatum occupy separate anatomical domains. J Neurosci, 2002. 22(1): p. 183-92.
214. Grasl-Kraupp, B., et al., In situ detection of fragmented DNA (TUNEL assay) fails to discriminate among apoptosis, necrosis, and autolytic cell death: a cautionary note. Hepatology, 1995. 21(5): p. 1465-8.
215. Chandramouli, K. and P.Y. Qian, Proteomics: challenges, techniques and possibilities to overcome biological sample complexity. Hum Genomics Proteomics, 2009. 2009.
216. Nixon, R.A., D.S. Yang, and J.H. Lee, Neurodegenerative lysosomal disorders: a continuum from development to late age. Autophagy, 2008. 4(5): p. 590-9.
217. Dinkins, M.B., et al., Exosome reduction in vivo is associated with lower amyloid plaque load in the 5XFAD mouse model of Alzheimer's disease. Neurobiol Aging, 2014. 35(8): p. 1792-800.


Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1405
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-334358
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2018