
CDPH Ryan White Part A Early Intervention Services (EIS ...
67
CDPH Ryan White Part A Early Intervention Services (EIS) Learning Collaborative Series Kick-Off Meeting Tuesday, June 28, 2016
Transcript of CDPH Ryan White Part A Early Intervention Services (EIS ...
CDPH Ryan White Part A Early Intervention Services (EIS)
Learning Collaborative Series Kick-Off Meeting
Tuesday, June 28, 2016

Agenda
• Welcome • PHIMC & CDPH QM Collaboration• Learning Collaborative History, Structure, & Requirements• EIS Site Visit Recap & Data Overview • EIS Quality Improvement Projects: Standards, Indicators, & Goals• PDSA Overview• Talk to Your Partner • Meet Your Coach & Team Discussion• Close
Goals for Today’s Meeting
1) Review the CDPH Learning Collaborative structure and purpose.
2) Brainstorm quality improvement projects ideas.
3) Agency introductions to assigned coaches and teams.
4) Leave with developed quality improvement projects ideas.
The Learning Collaborative Binder
• Agenda
• LC Agency Contact List
• Coaching Assignments & Teams
• Quality Improvement Projects
• HRSA EIS Program Monitoring Standards
• CDPH EIS Standards of Care
• NHAS Indicators
• QM EIS Audit Tool
• PHIMC Aggregate Data Presentation
• TRN’s EMA Aggregate Data Report
• LC Evaluation

PHIMC Mission and Vision
Public Health Institute of Metropolitan Chicago (PHIMC) enhances the capacity of public health and health care systems in Illinois to promote health equity and expand access to services.

How We Work
PHIMC leads efforts to strengthen the public health infrastructure in Illinois through:
• Organizational Development
• System Transformation
• Fiscal Management
• Program Implementation
How does PHIMC fit into Ryan White Part A?
• Technical assistance provider partnering with CDPH to implement Ryan White Quality Management (RW QM) across the Chicago EMA.
• Prior to March 2015, MATEC was lead on this project for 14 years.
• MATEC contracted primarily with Training Resources Network- Ms. Susan Thorner’s consulting agency.
The CDPH RWQM Program is….
A partnership between PHIMC and the Chicago Department of Public Health’s Quality Management (QM) Unit to provide training, technical assistance, and capacity building support to Ryan White Part A funded agencies in an effort to maintain sustainable internal QM infrastructure across the Chicago EMA.

How is RWQM Implemented?
• QM Site Visit Implementation
• Learning Collaboratives
• Webinars
• Support core MATEC Trainings
• Generating QM Newsletter/Online QM Resources
• Participation in Community Planning Efforts, i.e. CAHISC and the MAG
• Updating CDPH Standards of Care
• Audit Tool Creation & Data Collection
• Sub-recipient and CAHISC member surveys
• Conflict Resolution Training & Grievance Access
PHIMC and CDPH collaborate on the following items:

What is Quality Management (QM)vs.
Quality Assurance (QA) or Quality Improvement (QI)?
• Quality Management: All functions to evaluate and improve quality
i.e. QM committee + QM plan + QM site visits from funder, etc.
• Quality Assurance: Checking Boxesi.e. Program Monitoring Site Visits
• Quality Improvement: Enhancing Servicesi.e. Increasing percentage of AOMC clients receiving STI screening

What is a “Learning Collaborative”?
• Model developed by the Institute for Healthcare Improvement (IHI) in 1994, later adopted by NQC & HRSA
• Since 2000, NY State Health Department has tested LC model with RW Parts A-D
• In 2008, NQC published LC guide for RW providers nationwide
• Implementing quality improvement & identifying best practices
• Designed for clinical carehttp://nationalqualitycenter.org/files/planning-and-implementing-a-successful-learning-collaborative-pdf/
What is a CDPH Ryan White Part A Learning Collaborative (LC)?
• One Ryan White core service category selected based on CDPH Quality Management site visits from previous year.
• At least four LCs occur in given grant period (March 1st- Feb 28th).
• Agencies that received QM site visit in previous year are required to attend.
• Open to all CDPH RW Part A funded agencies.
Who should attend an CDPH RW Part A LC?
• CDPH Ryan White Part A-funded agencies
• Designated members of RW quality improvement team ORagency staff implementing the service category in question
• For 2016 EIS focused series, this may include:- Member of RW QI team
- Program Managers
- EIS specialists
- LTC staff
- Anyone else instrumental in implementing EIS

What are the requirements for LC participants?
• Register and attend four Learning Collaboratives.
• Complete and present on one quality improvement project for your agency by January 25, 2017.
• Work with and report to assigned coach as necessary.
Translating Ryan White Service Category into an Learning Collaborative Format
1) Review standards of care
2) Evaluate data
3) Convene planning session that includes providers for input
4) Identify quality improvement project areas (measurable indicators)
5) Create space for providers and experts to share best practices
6) Solicit provider input throughout
2016 Early Intervention Services (EIS) Learning Collaborative Series: Foundation
Note: This is the first CDPH Part A EIS focused Learning Collaborative.
• Partially informed by 2015 QM EIS site visits.
• Planning session convened on 5/24/16 including providers from 5 agencies.
• Local provider input and focus.
This year’s number one goal is to structure a learning collaborative that allows RW providers to be the experts.
2016 Early Intervention Services (EIS) Learning Collaborative Series: Structure
• Four provider meetings
• Quality Improvement Tips, Tricks, Trends
• Best Practices Presentations from EIS Providers
• Built in time to meet with coaches & team
CDPH 2015 EIS Site Visit Overview
• 20 agencies site visited in 2015
• 4/20 previously funded by CDPH
• 16/20 newly funded
• Pilot Year
• Not required: EIS Quality Improvement Plan
• Required: 1 EIS Quality Improvement Project
Before We Review the Data….
• EIS is brand new!
• Site visit audit tool has room for improvement.
• Training Resources Network (TRN) led audit tool creation and data report generation.
• Site visit data scores are not punitive measures, but indicators of potential areas of improvement.

Katie Morin, PHIMC Data Strategist
Tuesday, June 28, 2016
EIS Technical Assistance Site VisitAggregate Data Report Back
TA Site Visit Overview
• TA Site Visits September to October 2015• Conducted by CDPH, PHIMC, & TRN
• 20 Agencies (4 Previously Funded 16 Newly Funded)• 222 Charts Reviewed
• For Sites funded prior to 3/1/2015 the review covered March 1, 2014 to February 28, 2015.
• For Sites funded after 3/1/2015 the review covered March 1, 2015 to August 31, 2015.
• Final Report and figures compiled by TRN • All compilations are based on the average of the percentages in the
EMA report, not the raw data.
Quality Assurance Measures
QA Measures:• Largely a compliance check
• Does not have the most direct impact on linkage, retention and suppression.
CQI Measures:• More direct impact on linkage, retention and suppression.

84%
51%
61%
96%
63%
30%
Documentation of Consent Forms Documentation of Initial Intake Documentation of Signed Service Plan Documentation of Completed and SignedMedical Assessment/Evaluation
Documentation ofRisk Assessment
Documentation ofCase Closure
Chicago EMA Documentation of Completion of Forms
QA Data Conclusions
QA Highlights• 96% Completed and Signed Medical Evaluations• 84% Signed Client Consent Forms
QA Opportunities for improvement• 51% Documentation of Initial Intake• 61% Signed Service Plans • 63% Documentation of Risk Assessment • 30% Documentation of Case Closure
Quality Improvement Measures
• All compilations are based on the average of the percentages across all providers in the EMA report, not the raw data.
Data is divided into the following: • Documentation of HIV Testing and Counseling
• Documentation of Referral Services
• Documentation of Health Education and Literacy
• Documentation of Linkage & Retention

94%
80%
93%
65%
Documentation of confirmed HIV status in the chart Documentation that the meaning of a positive HIV test wasexplained to the patient
Documentation of referral for appointment with medicalprovider discussed and provided
Documentation of referral for medical case managementdiscussed and provided
Documentation of HIV Testing and Counseling

83%
CHICAGO EMA AGGREGATE
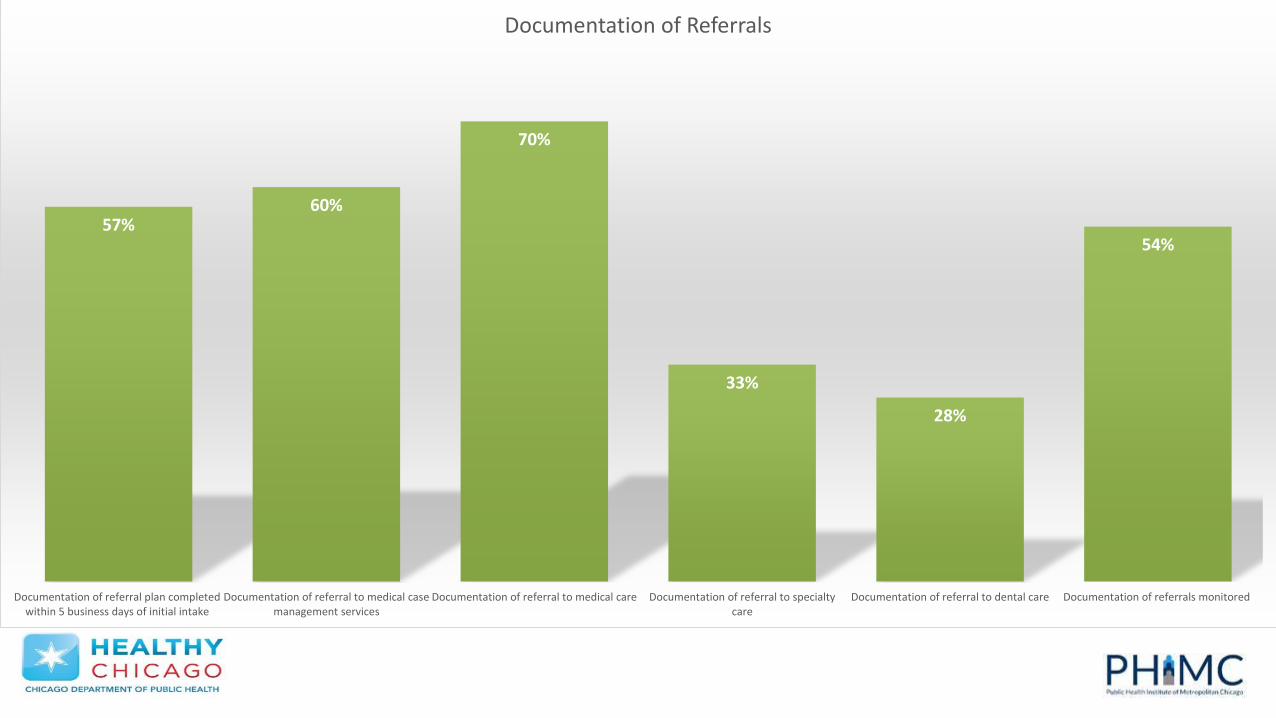
57%60%
70%
33%
28%
54%
Documentation of referral plan completedwithin 5 business days of initial intake
Documentation of referral to medical casemanagement services
Documentation of referral to medical care Documentation of referral to specialtycare
Documentation of referral to dental care Documentation of referrals monitored
Documentation of Referrals
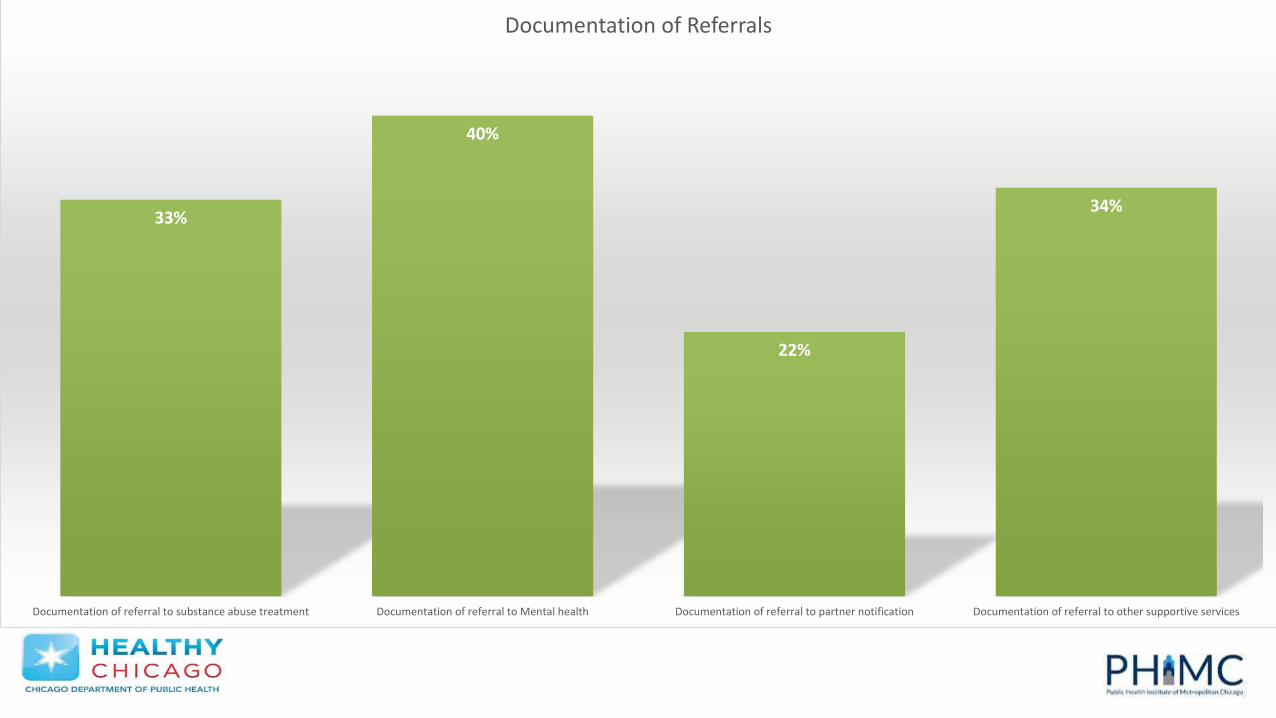
33%
40%
22%
34%
Documentation of referral to substance abuse treatment Documentation of referral to Mental health Documentation of referral to partner notification Documentation of referral to other supportive services
Documentation of Referrals
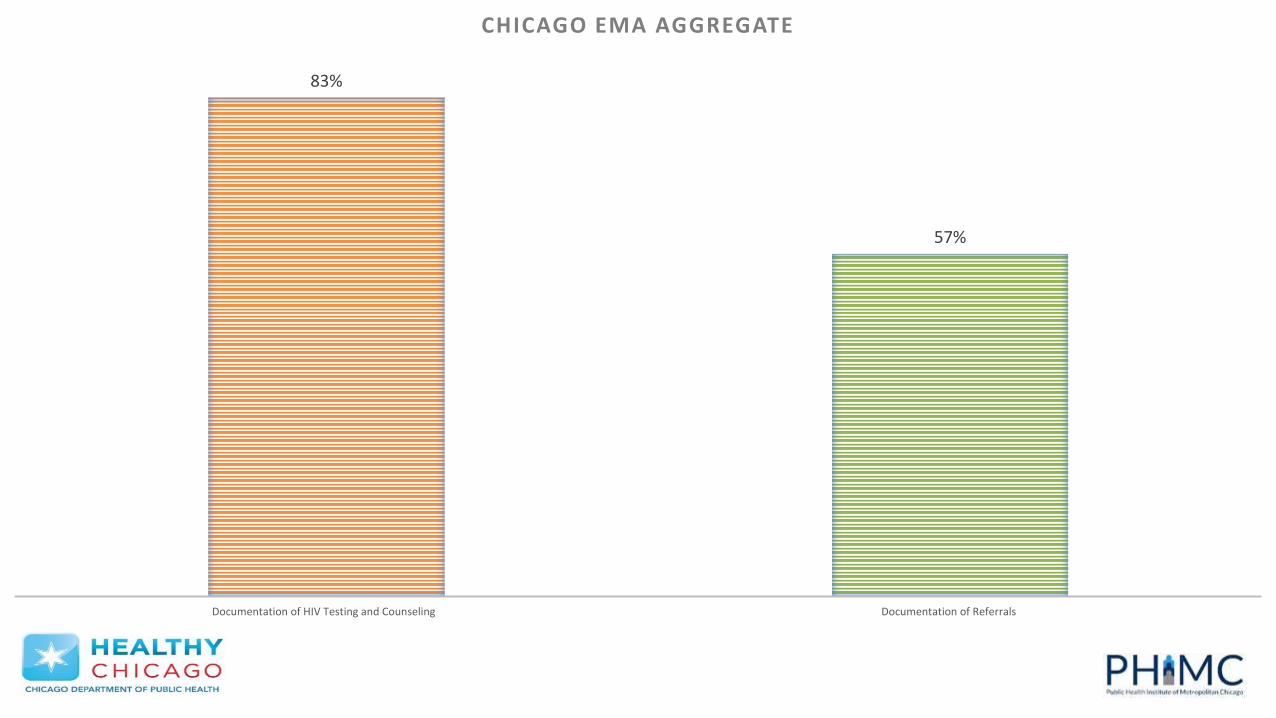
83%
57%
Documentation of HIV Testing and Counseling Documentation of Referrals
CHICAGO EMA AGGREGATE
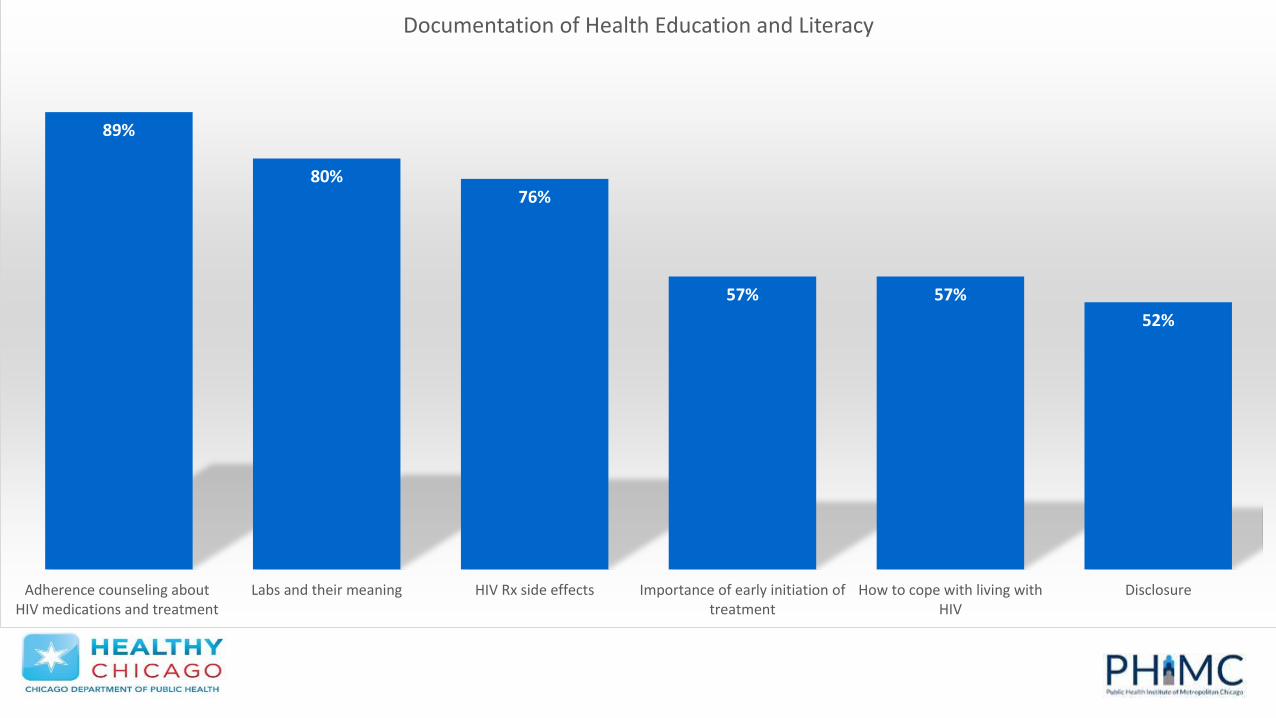
89%
80%76%
57% 57%
52%
Adherence counseling aboutHIV medications and treatment
Labs and their meaning HIV Rx side effects Importance of early initiation oftreatment
How to cope with living withHIV
Disclosure
Documentation of Health Education and Literacy
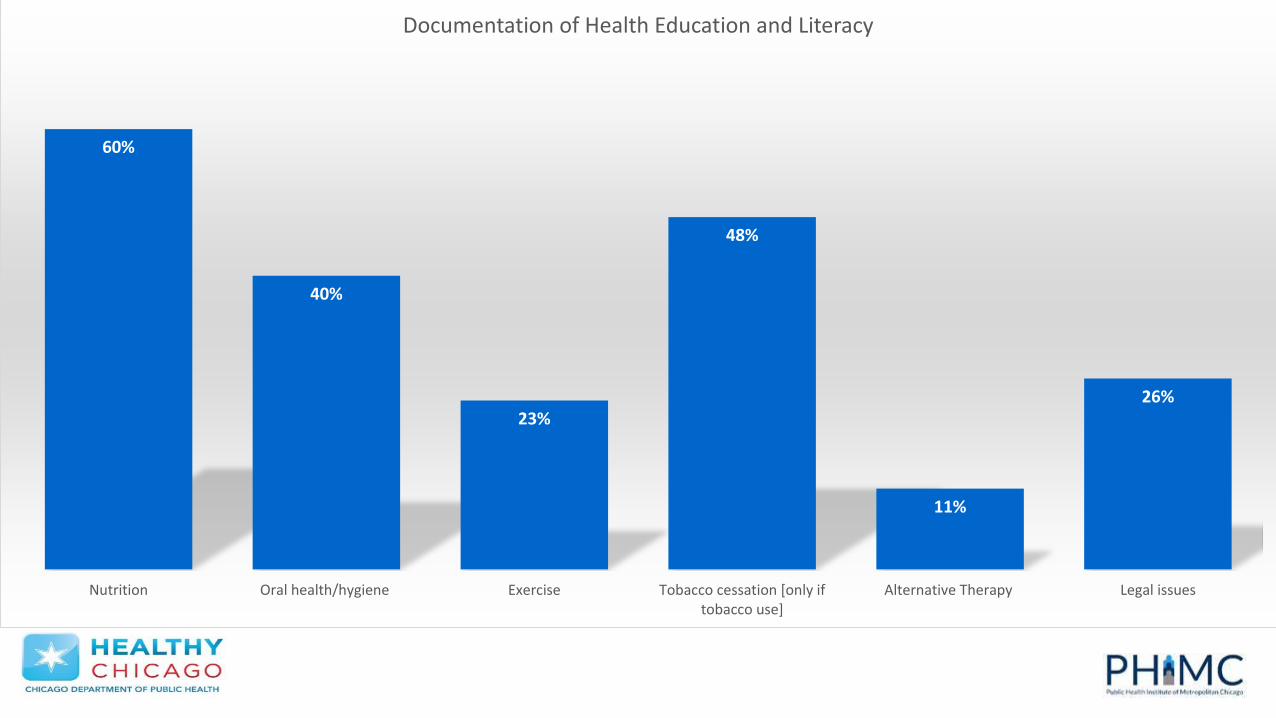
60%
40%
23%
48%
11%
26%
Nutrition Oral health/hygiene Exercise Tobacco cessation [only iftobacco use]
Alternative Therapy Legal issues
Documentation of Health Education and Literacy
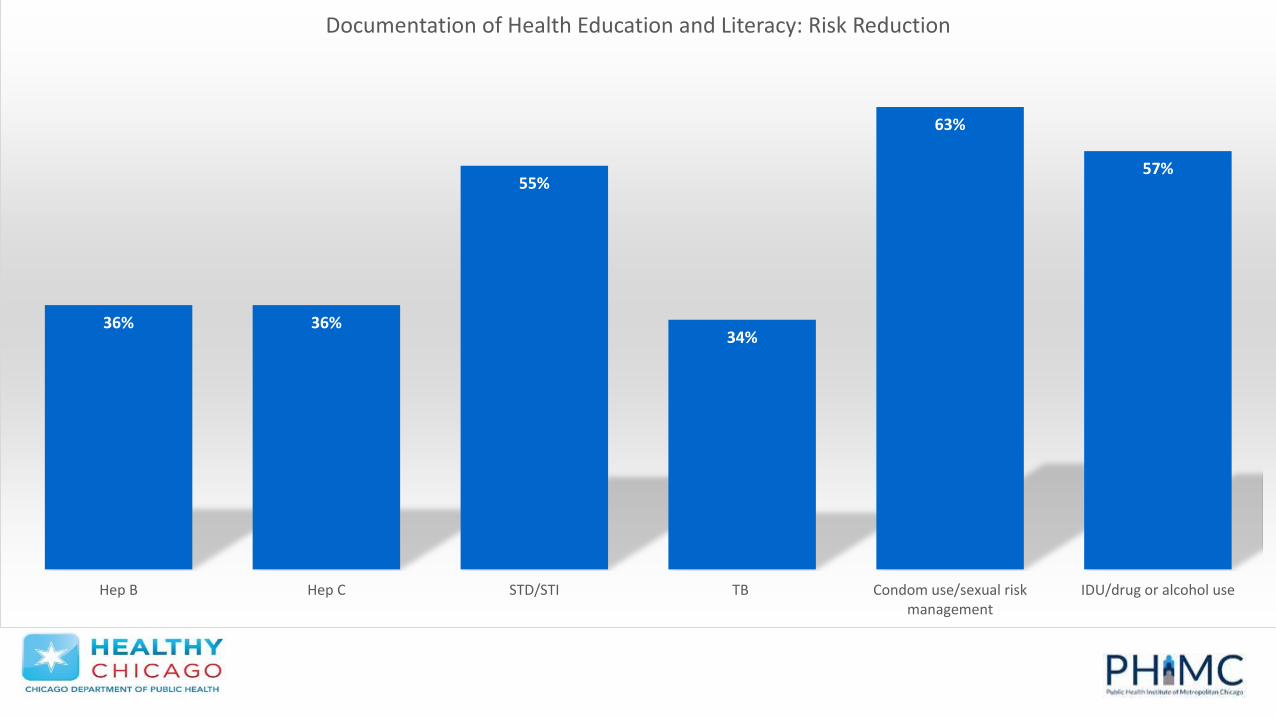
36% 36%
55%
34%
63%
57%
Hep B Hep C STD/STI TB Condom use/sexual riskmanagement
IDU/drug or alcohol use
Documentation of Health Education and Literacy: Risk Reduction
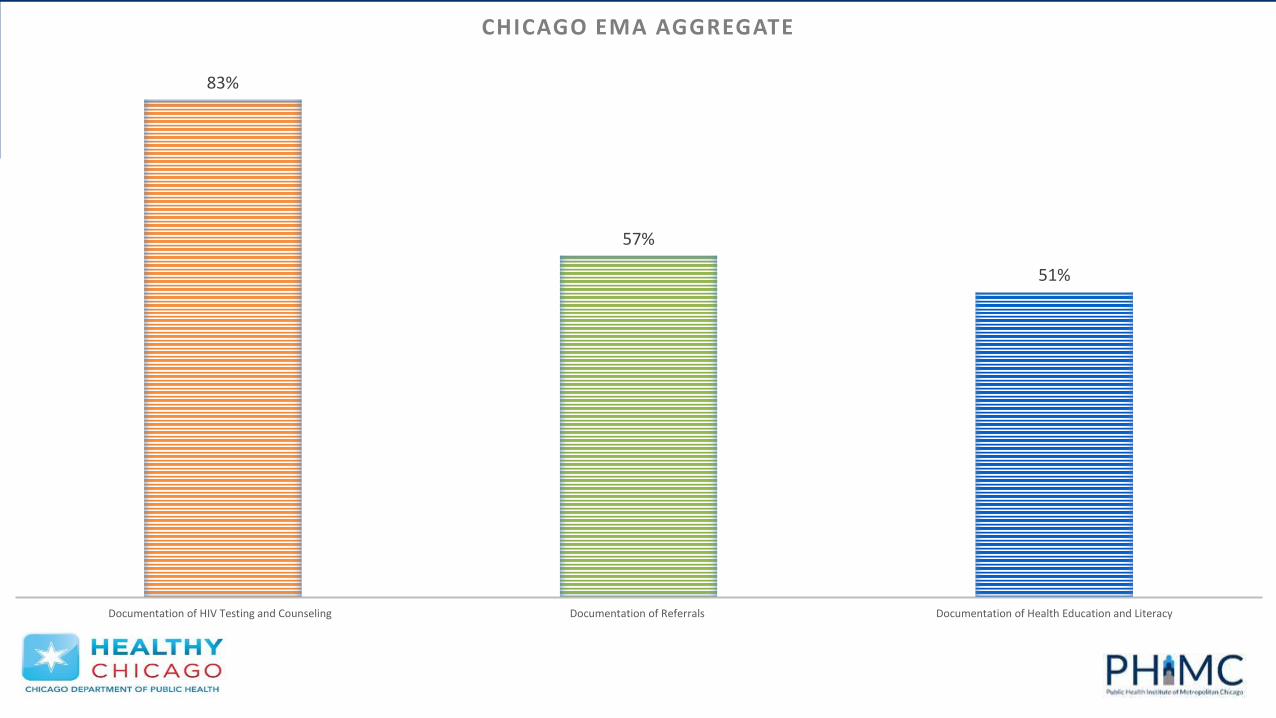
83%
57%
51%
Documentation of HIV Testing and Counseling Documentation of Referrals Documentation of Health Education and Literacy
CHICAGO EMA AGGREGATE

65%
72%
Reasons the patient did not have at least two medical visits Follow-up telephone calls, letters &/or home visit) for missed appointments
Linkage and Retention Efforts
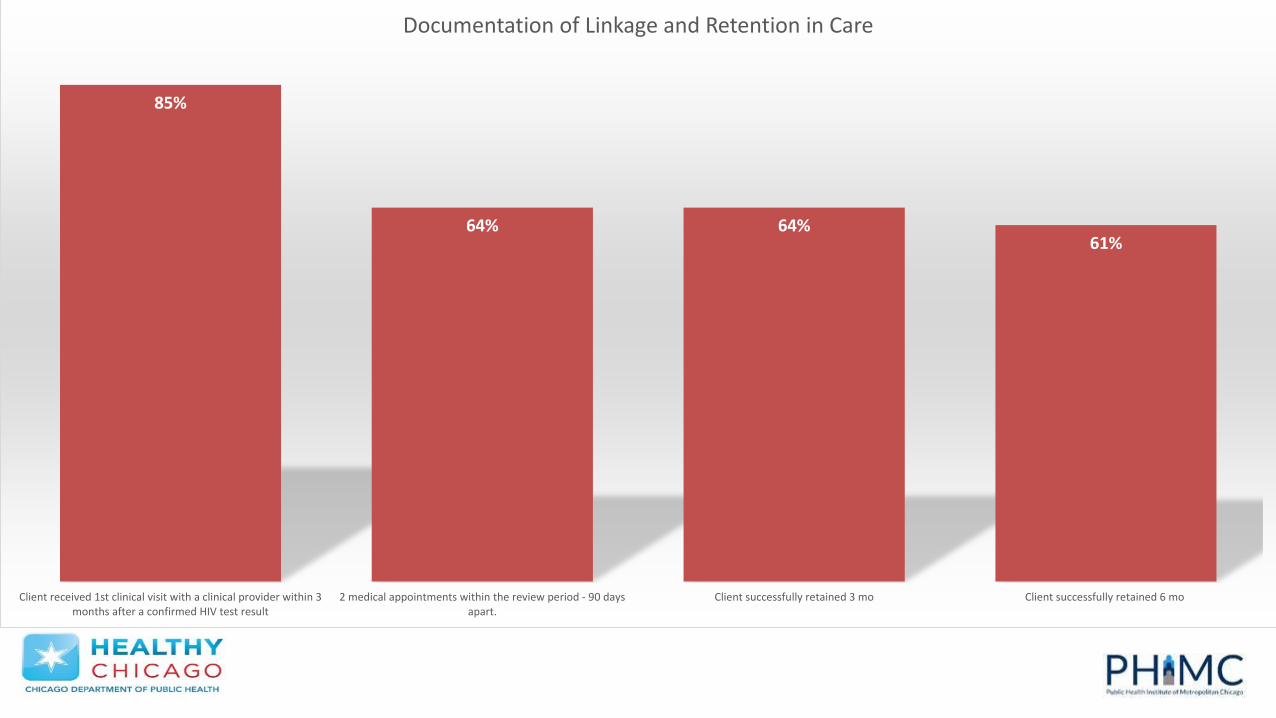
85%
64% 64%61%
Client received 1st clinical visit with a clinical provider within 3months after a confirmed HIV test result
2 medical appointments within the review period - 90 daysapart.
Client successfully retained 3 mo Client successfully retained 6 mo
Documentation of Linkage and Retention in Care
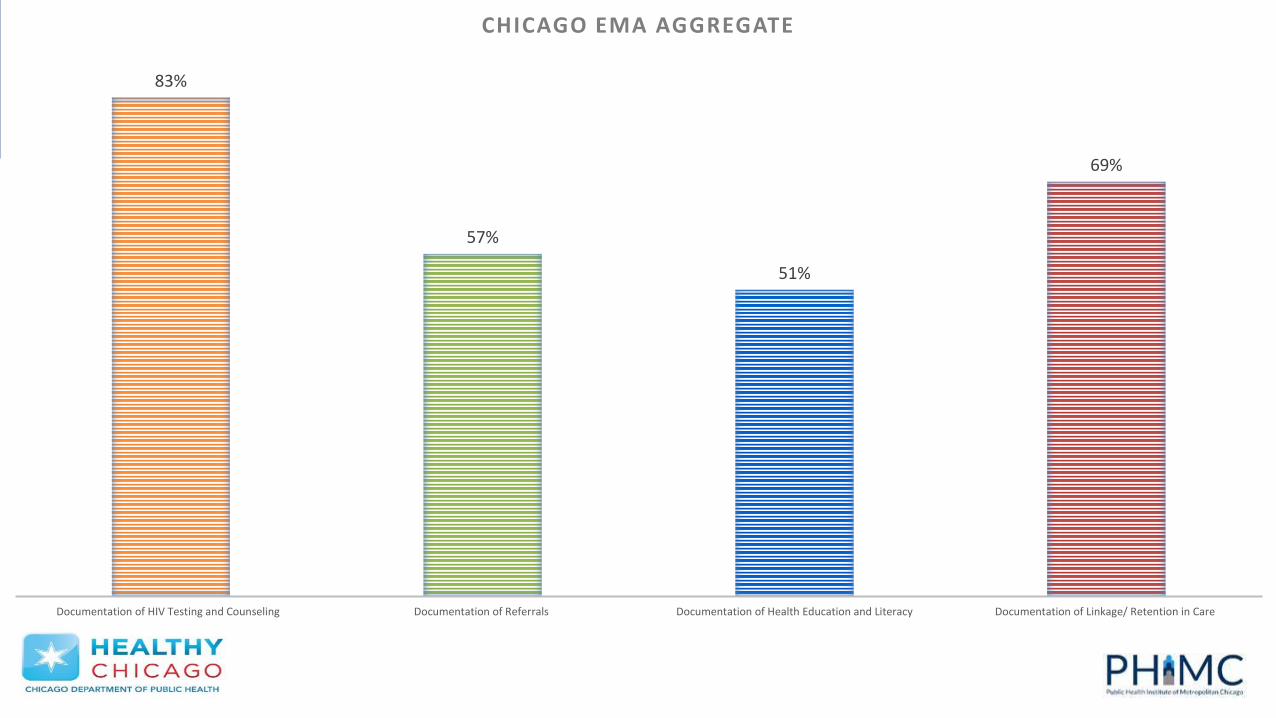
83%
57%
51%
69%
Documentation of HIV Testing and Counseling Documentation of Referrals Documentation of Health Education and Literacy Documentation of Linkage/ Retention in Care
CHICAGO EMA AGGREGATE

Quality Improvement Data: Highlights
HIV Testing and Counseling • 93% Referral for appointment with medical provider discussed and
provided • 80% Documentation that the meaning of a positive HIV test was
explained to the patient
Health Education and Literacy • 89% Adherence Counseling Provided • 80% Meaning of Labs Explained
Linkage and Retention in Care• 85% Attended Clinical Visit within 3 months
Quality Improvement Data: Opportunities for Improvement
HIV Testing and Counseling:• 65% Referrals to medical case management
Referrals • Documentation of referrals overall fell short of the 80% or the “good”
measure• Example 54% Monitoring of referrals
Quality Improvement Data: Opportunities for Improvement
Health Education and Literacy• Documentation of health education and literacy fell short of the 80% or
“good” measure in several areas. • Example 57% Importance of early initiation of treatment
Linkage and Retention in Care • 64% client successfully retained 3 months.
Questions?
Acknowledging the challenges with utilizing EIS in an LC format
• Brand new service category• Limited data • Standards of care do not include measurable indicators• Intervention contains non-clinical/social components
What We Know: The 4 Buckets of Early Intervention Services (EIS)
• HIV Counseling and Testing
• Linkage to Care
• Referrals
• Health Literacy

Applying the NHAS Indicators to EIS
NHAS Indicator 4: Increase percentage of newly diagnosed person
linked to HIV medical care within one month of their diagnosis to at
least 85%.
NHAS Indicator 5: Increase the percentage of person with diagnosed
HIV infection who are retained in HIV medical care to at least 90%.
NHAS Indicator 6: Increase the percentage of persons with diagnosed
HIV infection who are virally suppressed to at least 80%.
Steps to selecting an EIS Quality Improvement Project
Step 1: Select an NHAS indicator.
Step 2: Select one of the buckets of EIS.
Step 3: Identify small-scale projects.
Step 4: Conduct PDSA.

Break

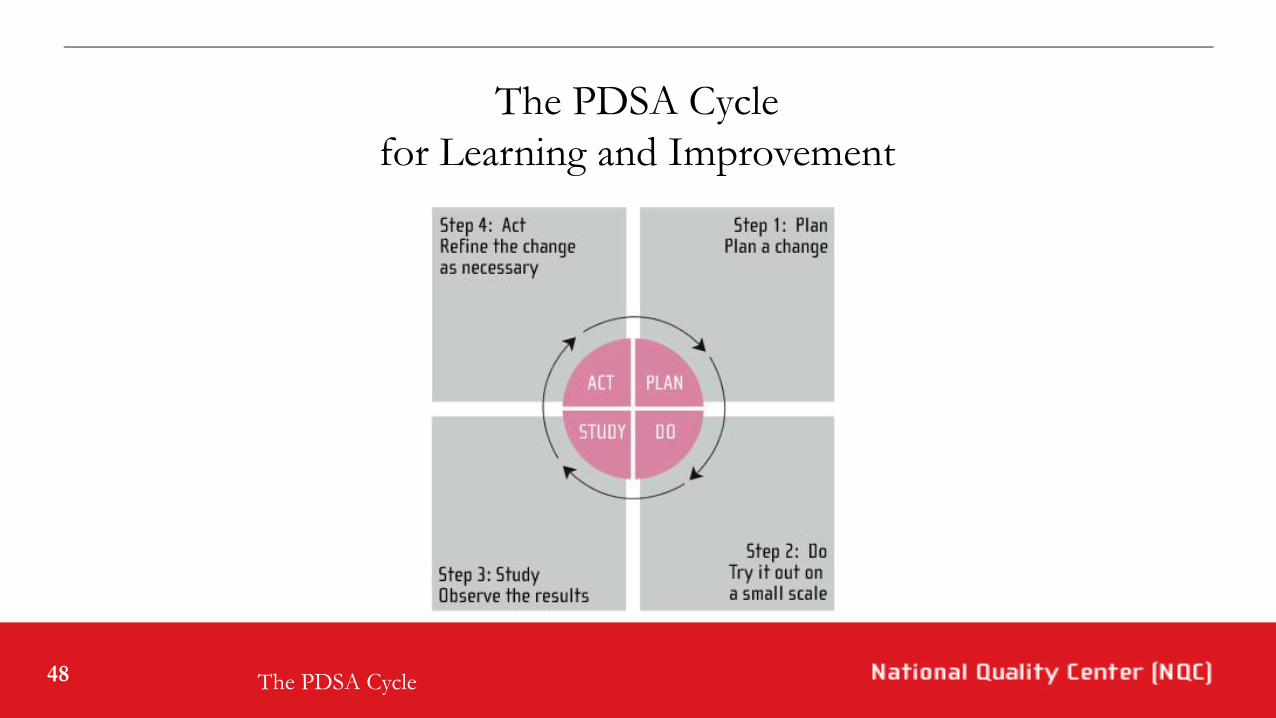
The PDSA Cycle or
How Can We Accelerate Improvements in
HIV Care?
The Quality Academy
Tutorial 13
48
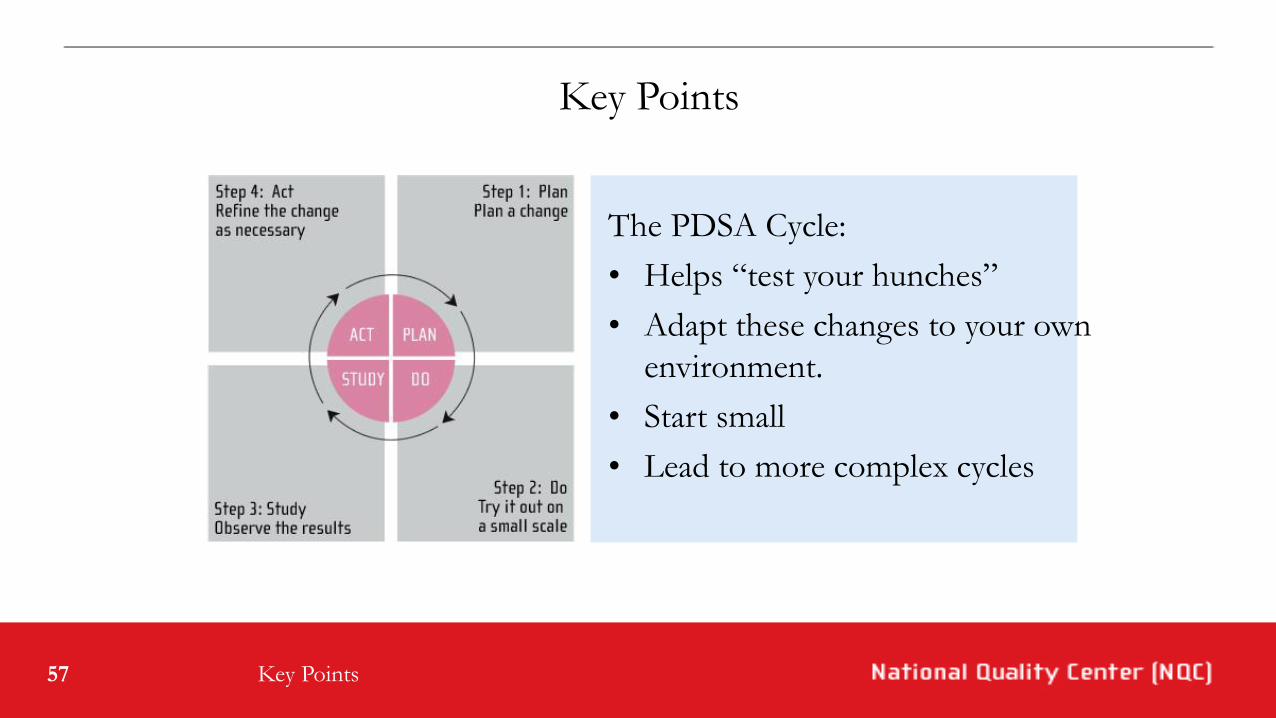
The PDSA Cycle
for Learning and Improvement
The PDSA Cycle

49
Plan
The PDSA Cycle
1. Clarify your Objective
2. Make a prediction
• Formulate theory
• Objective + specificity
3. What is to be done
• Who
• What
• Where
• When
• How

50
Do
The PDSA Cycle
1. Carry out the plan
2. Document your
observations
• Expected
• Unexpected
3. Begin analysis
51
Study
The PDSA Cycle
Complete
Compare
Summarize
52
Act
The PDSA Cycle
1. Adjustments
• Changes to previous test?
• What adjustments?
• Expand last cycle?
2. New cycles
• What are you planning?
• What are you going to test?

53
At the Beginning, Test on a Small Scale
• “What change could you implement by next Tuesday?”
• Use the “Rule of 1”:
• 1 facility
• 1 office
• 1 provider
• 1 patient
Applying PDSA
54
Scale Down the Time Frame
• Years
• Quarters
• Months
• Weeks
• Days
• Hours
• Minutes
Drop down two
levels! (years to
months, weeks
to hours)
Applying PDSA

55
Keep the First Tests Simple
• Volunteers at first
• Useful, not perfect, data
• Use “huddles” to report
Applying PDSA
56
Build Each Cycle on Its Predecessor
“The shorter the timeframes between test cycles, the more tests can be conducted and therefore, more opportunities for learning will emerge.”
HIVQUAL Workbook
Applying PDSA
57
Key Points
The PDSA Cycle:
• Helps “test your hunches”
• Adapt these changes to your own
environment.
• Start small
• Lead to more complex cycles
Key Points

58
Resources
• http://www.IHI.org/IHI/Improvement/ ImprovementMethodsprovides information on improvement methods, strategies, and changes.
• Moen, Ronald, Thomas Nolan; “Process Improvement” Quality Progress, 1987, p62.
• Langley, Gerald, Kevin Nolan and Thomas Nolan; “The Foundation of Improvement,” Quality Progress, June 1994, p. 81.
• Langley, Gerald, Kevin Nolan, Thomas Nolan, Cliff Norman, and Lloyd Provost; The Improvement Guide. San Francisco, CA; Jossey-Bass, 1996.
• Nolan, Kevin; “ASQs Accelerating Change Collaborative Series: A Challenge for Industry,” Quality Progress, Jan 1999, p55.
Resources
59
The Quality Academy
For further information, contact:
National Quality Center
New York State Dept. of Health
90 Church Street, 13th floor
New York, NY 10007-2919
Work: 212.417.4730
Fax: 212.417.4684
Email: [email protected]
Or visit us online at NationalQualityCenter.org
In Closing
60
QUESTIONS?

Talk to Your Neighbor
• EIS Challenges and Successes
• Quality Improvement Project Brainstorm
Meet with Your Coach & Team
Team 1: Charlotte Detournay
Austin CBC
Michael Reese
Regional Care Association
Team 2: Silas Hyzer
Loyola Medical Center
Lurie Children’s Hospital
Mount Sinai
Team 5: Katie Morin
Access Community Health Network
Erie Family Health Center
Heartland Health Outreach
Howard Brown Health Center
Team 6: Barbara Schechtman
South Suburban HIV/AIDS Regional
Clinics
Provident Hospital
Core Center
Team 3: Rod Kaup
AIDS Healthcare Foundation
Lawndale Christian Community Health
Center
Open Door Clinic
South Shore Hospital
Team 4: Laura Kuever (Jenny Epstein)
Lake County Health Department
University of Illinois, Chicago
University of Chicago

Small Group Discussion Questions
1. Introductions & Outstanding Questions
2. Share one productive Ryan White quality improvement project experience you've had. What made it productive?
3. What do you find is the biggest challenge in implementing quality improvement projects at your agency? Why?
4. Brainstorm and share potential EIS QIPs.
5. How can coach be most supportive to you and your agency?

Upcoming Learning Collaboratives
• Tuesday, September 20th, 9:30 AM- 12:30 PM
• Thursday, November 17th, 9:30 AM- 12:30 PM
• Wednesday, January 25th, 9:30 AM- 12:30 PM
Other Upcoming CDPH QM activities
• QM Webinar 1 “Conducting Quality Improvement Projects for Ryan White Part A Early Intervention Services (EIS) in the Chicago EMA” coming up on Tuesday, July 26th 12:00 pm- 1:00 pm
• Online QM Resource Hub in progress
• 2016 QM site visits: mental health, psycho-social, and substance abuse residential
• QM site visit orientation in August 2016
Questions?

Thank You!
Ayla Karamustafa, Quality and Prevention Manager
Public Health Institute of Metropolitan Chicago
Katie Morin, Data Strategist
Public Health Institute of Metropolitan Chicago
Barbara Schechtman, Quality Management Consultant
Public Health Institute of Metropolitan Chicago


















