CDC Autism Study, March 2012

of 24
-
Upload
the-salt-lake-tribune -
Category
Documents
-
view
220 -
download
0
Transcript of CDC Autism Study, March 2012
-
8/2/2019 CDC Autism Study, March 2012
1/24
Surveillance Summaries / Vol. 61 / No. 3 March 30, 2012
U.S. Department of Health and Human Services
Centers for Disease Control and Prevention
Morbidity and Mortality Weekly Report
Prevalence of Autism Spectrum Disorders
Autism and Developmental Disabilities MonitoringNetwork, 14 Sites, United States, 2008
-
8/2/2019 CDC Autism Study, March 2012
2/24
-
8/2/2019 CDC Autism Study, March 2012
3/24
Surveillance Summaries
MMWR / March 30, 2012 / Vol. 61 / No. 3 1
Corresponding author: Jon Baio, EdS, National Center on BirthDeects and Developmental Disabilities, CDC, 1600 Cliton Road,MS E-86, Atlanta, GA 30333. Telephone: 404-498-3873; Fax: 404-498-3550; E-mail:[email protected].
Prevalence of Autism Spectrum Disorders Autism andDevelopmental Disabilities Monitoring Network,
14 Sites, United States, 2008Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators
Abstract
Problem/Condition: Autism spectrum disorders (ASDs) are a group o developmental disabilities characterized by impairmentin social interaction and communication and by restricted, repetitive, and stereotyped patterns o behavior. Symptoms typicallyare apparent beore age 3 years. The complex nature o these disorders, coupled with a lack o biologic markers or diagnosis andchanges in clinical deinitions over time, creates challenges in monitoring the prevalence o ASDs. Accurate reporting o data isessential to understand the prevalence o ASDs in the population and can help direct research.
Period Covered: 2008.
Description of System: The Autism and Developmental Disabilities Monitoring (ADDM) Network is an active surveillance systemthat estimates the prevalence o ASDs and describes other characteristics among children aged 8 years whose parents or guardianreside within 14 ADDM sites in the United States. ADDM does not rely on proessional or amily reporting o an existing ASD
diagnosis or classiication to ascertain case status. Instead, inormation is obtained rom childrens evaluation records to determinethe presence o ASD symptoms at any time rom birth through the end o the year when the child reaches age 8 years. ADDMocuses on children aged 8 years because a baseline study conducted by CDC demonstrated that this is the age o identiied peakprevalence. A child is included as meeting the surveillance case deinition or an ASD i he or she displays behaviors (as described ona comprehensive evaluation completed by a qualiied proessional) consistent with the American Psychiatric Associations Diagnosticand Statistical Manual-IV, Text Revision (DSM-IV-TR) diagnostic criteria or any o the ollowing conditions: Autistic DisorderPervasive Developmental DisorderNot Otherwise Speciied (PDD-NOS, including Atypical Autism); or Asperger Disorder. Theirst phase o the ADDM methodology involves screening and abstraction o comprehensive evaluations completed by proessionaproviders at multiple data sources in the community. Multiple data sources are included, ranging rom general pediatric healthclinics to specialized programs or children with developmental disabilities. In addition, many ADDM sites also review andabstract records o children receiving special education services in public schools. In the second phase o the study, all abstractedevaluations are reviewed by trained clinicians to determine ASD case status. Because the case deinition and surveillance methodshave remained consistent across all ADDM surveillance years to date, comparisons to results or earlier surveillance years can bemade. This report provides updated ASD prevalence estimates rom the 2008 surveillance year, representing 14 ADDM areas inthe United States. In addition to prevalence estimates, characteristics o the population o children with ASDs are described, aswell as detailed comparisons o the 2008 surveillance year indings with those or the 2002 and 2006 surveillance years.
Results: For 2008, the overall estimated prevalence o ASDs among the 14 ADDM sites was 11.3 per 1,000 (one in 88) childrenaged 8 years who were living in these communities during 2008. Overall ASD prevalence estimates varied widely across all sites(range: 4.821.2 per 1,000 children aged 8 years). ASD prevalence estimates also varied widely by sex and by racial/ethnic groupApproximately one in 54 boys and one in 252 girls living in the ADDM Network communities were identiied as having ASDsComparison o 2008 indings with those or earlier surveillance years indicated an increase in estimated ASD prevalence o 23%when the 2008 data were compared with the data or 2006 (rom 9.0 per 1,000 children aged 8 years in 2006 to 11.0 in 2008 orthe 11 sites that provided data or both surveillance years) and an estimated increase o 78% when the 2008 data were compared
with the data or 2002 (rom 6.4 per 1,000 children aged 8 years in 2002 to 11.4 in 2008 or the 13 sites that provided data or bothsurveillance years). Because the ADDM Network sites do not make up a nationally representative sample, these combined prevalenceestimates should not be generalized to the United States as a whole.
Interpretation: These data conirm that the estimatedprevalence o ASDs identiied in the ADDM networksurveillance populations continues to increase. The extentto which these increases relect better case ascertainment as aresult o increases in awareness and access to services or true
mailto:[email protected]:[email protected] -
8/2/2019 CDC Autism Study, March 2012
4/24
Surveillance Summaries
2 MMWR / March 30, 2012 / Vol. 61 / No. 3
increases in prevalence o ASD symptoms is not known. ASDs continue to be an important public health concern in the UnitedStates, underscoring the need or continued resources to identiy potential risk actors and to provide essential supports or personwith ASDs and their amilies.
Public Health Action: Given substantial increases in ASD prevalence estimates over a relatively short period, overall and withinvarious subgroups o the population, continued monitoring is needed to quantiy and understand these patterns. With 5 bienniasurveillance years completed in the past decade, the ADDM Network continues to monitor prevalence and characteristics o
ASDs and other developmental disabilities or the 2010 surveillance year. Further work is needed to evaluate multiple actorscontributing to increases in estimated ASD prevalence over time. ADDM Network investigators continue to explore these actorswith a ocus on understanding disparities in the identiication o ASDs among certain subgroups and on how these disparitiehave contributed to changes in the estimated prevalence o ASDs. CDC is partnering with other ederal and private partners ina coordinated response to identiy risk actors or ASDs and to meet the needs o persons with ASDs and their amilies.
Introduction Autism spectrum disorders (ASDs) are a group o
developmental disabilities characterized by impairments insocial interaction and communication and by restricted,
repetitive, and stereotyped patterns o behavior (1). Symptomstypically are apparent beore age 3 years. Since the early 1990s,elevated public concern about continued reported increasesin the number o children receiving services or ASDs andreports o higher-than-expected ASD prevalence estimates haveunderscored the need or systematic public health monitoringo ASDs (2). Tracking the prevalence o ASDs over time posesunique challenges because o the complex nature o thesedisorders, a lack o biologic markers or diagnosis, and changesin clinical deinitions over time.
In 2000, CDC established the Autism and DevelopmentalDisabilities Monitoring (ADDM) Network to collect data that
would provide estimates o the prevalence o ASDs and otherdevelopmental disabilities in the United States (2). Initial reportsrom the ADDM Network provided ASD prevalence estimatesrom six sites or the 2000 surveillance year (3) and rom 14 sitesor the 2002 surveillance year (4). Estimates o ASD prevalenceamong children aged 8 years were similar or both surveillanceyears. Data combined rom all sites in each respective surveillanceyear yielded overall ASD prevalence estimates o 6.7 per 1,000children aged 8 years in 2000 (range: 4.59.9) and 6.6 per1,000 in 2002 (range: 3.310.6), or one in every 150 childrenaged 8 years.
The subsequent ADDM Network report provided data on
estimated ASD prevalence among children aged 8 years or2004 (eight sites) and 2006 (11 sites) (5). When data romall sites were combined, overall estimated ASD prevalence was 8.0 per 1,000 children aged 8 years in 2004 (range:4.69.8), or one in every 125 children, and 9.0 per 1,000 in2006 (range: 4.212.1), or one in every 110 children aged8 years. ASD prevalence estimates or the 2002 and 2006surveillance years were compared (5). All 10 ADDM sites
that provided data or both surveillance years reported anincrease in estimated ASD prevalence (range: 27%95%). By2006, the combined estimated prevalence o ASDs in ADDMNetwork sites approached 1% o children aged 8 years, a4-year increase o 57% among sites that provided data or
both the 2002 and 2006 surveillance years (5). Some o theincrease in estimated ASD prevalence might be attributed toimproved identiication, particularly among certain subgroup(e.g., children without intellectual disability and Hispanicchildren). These data indicated the importance o continuingto monitor trends in ASD prevalence and o accelerating thepace o research into risk actors and eective interventions.
Certain studies rom the United States, Europe, and Asiahave reported ASD prevalence estimates based on nationasurvey data, statewide administrative data, or communityscreening approaches (610). Results rom these studiesare generally consistent with those reported by the ADDM
Network, although some international prevalence estimatesare higher. In the United States, parent-reported data romthe 2007 National Survey o Childrens Health indicated anoverall estimated prevalence o 11.0 per 1,000 children aged317 years (6), and data rom the National Health InterviewSurvey demonstrated a nearly ourold increase in estimatedASD prevalence between the 19971999 and the 20062008surveillance periods (7). A British study that employed both aquestionnaire and direct screening methods estimated an ASDprevalence o close to 1% o children aged 59 years duringthe 2003 and 2004 school years (8,9). A recent study basedon population screening and direct assessment in South Koreaestimated overall ASD prevalence o 26.4 per 1,000 childrenaged 712 years in 2006 (10).
This report provides updated ASD prevalence estimatesrom the ADDM Network or the 2008 surveillance yearrepresenting 14 sites in the United States. In addition toprevalence estimates, characteristics o the population ochildren with ASDs are described. This report is intended tocommunicate the latest available ASD prevalence estimates
-
8/2/2019 CDC Autism Study, March 2012
5/24
Surveillance Summaries
MMWR / March 30, 2012 / Vol. 61 / No. 3 3
rom the ADDM Network and to provide basic comparisons with estimates or earlier ADDM surveillance years. Moreocused eorts are underway to analyze available data onmultiple actors inluencing the identiication o children withASDs and potential changes in risk actors over time.
Methods
Study SitesThe Childrens Health Act o 2000 (11) authorized CDC to
create the ADDM Network, the only collaborative network toestimate the prevalence o ASDs in the United States. ADDMhas multiple goals: 1) to obtain as complete a count as possibleo the number o children with ASDs in each project area, 2) toreport comparable population-based ASD prevalence estimatesrom dierent sites and determine i these rates are changingover time, 3) to study whether autism is more common amongsome groups o children than among others, and 4) to providedescriptive data on the population o children with ASDs.Since the ADDM Networks inception in 2000, CDC hasunded grantees in 14 states (Alabama, Arizona, Arkansas,Colorado, Florida, Maryland, Missouri, New Jersey, NorthCarolina, Pennsylvania, South Carolina, Utah, West Virginia,and Wisconsin). The ADDM Network implements a multisite,multiple-source, records-based surveillance methodology basedon a model originally implemented by CDCs Metropolitan Atlanta Developmental Disabilities Surveillance Program(MADDSP) (12). The case deinition and surveillance
methods, which have been described in detail previously(25,12,13), have remained consistent over time, enablingcomparisons across multiple surveillance years. ADDM ocuseson children aged 8 years because a baseline ASD prevalencestudy conducted by MADDSP demonstrated that this is the ageo identiied peak prevalence (12). MADDSP represents oneADDM site in Georgia, and the remaining ADDM projectsare administered through state health departments or throughuniversities working on behal o their state health departmentsto collect or receive inormation used or protecting publichealth. Sites were selected through a competitive objectivereview process on the basis o their ability to conduct active,
records-based surveillance o ASDs; they were not selectedto be a nationally representative sample. Each ADDM siteparticipating in the 2008 surveillance year unctioned as apublic health authority under the HIPAA Privacy Rule andmet applicable local Institutional Review Board and privacy/conidentiality requirements under 45 CFR 46 (14).
Case AscertainmentADDM is an active surveillance system that does not rely
on proessional or amily reporting o an existing diagnosis orclassiication to ascertain ASD case status. Case determinationis completed in two phases. The irst phase involves screening
and abstraction o records at multiple data sources in thecommunity. All abstracted evaluations then are compiled andreviewed by trained clinicians to determine ASD case status inthe second phase o the study. In the irst phase, a broad netis cast to screen thousands o records and identiy a subset ochildren with general symptoms o ASDs, whereas a much morestrict case deinition is applied during the second phase o thestudy. Because childrens records are screened at multiple datasources, developmental assessments completed by a wide rangeo health and education providers are included. Data sourceare categorized as either 1) education source type, includingevaluations to determine eligibility or special education
services or 2) health source type, including diagnostic anddevelopmental assessments rom psychologists, neurologistsdevelopmental pediatricians, physical therapists, occupationatherapists, speech/language pathologists, and other providers Agreements to access records are made at the institutionalevel in the orm o contracts, memoranda, or other ormalagreements. All ADDM Network sites have agreements in placeto access records at health sources; however, our ADDM sites(Alabama, Florida, Missouri, and Wisconsin) have not beengranted access to records at education sources, and in one site(Colorado), parents are notiied directly about the study andmay request that their childrens education records be excluded
In the irst phase o the study, ADDM Network sites identiysource records to review based on a childs year o birth andeither 1) eligibility classiications in special education or2) International Classiication o Diseases, Ninth Revision(ICD-9) billing codes (Box) or select childhood disabilitiesor psychological conditions. Childrens records are screenedto conirm year o birth and residency in the surveillancearea at some time during the surveillance year. For childrenmeeting age and residency requirements, the source iles arescreened or certain behavioral or diagnostic descriptionsdeined by ADDM as triggers or abstraction (e.g., childdoes not initiate interactions with others, preers to play aloneor engage in solitary activities, or has received a documentedASD diagnosis). I abstraction triggers are ound, evaluationinormation rom birth through the current surveillance yearis abstracted into a single composite record or each child.
In the second phase o the ADDM methodology, theabstracted composite evaluation iles are de-identiied and
-
8/2/2019 CDC Autism Study, March 2012
6/24
Surveillance Summaries
4 MMWR / March 30, 2012 / Vol. 61 / No. 3
reviewed systematically by trained clinicians to determineASD case status using a coding scheme based on the AmericanPsychiatric Associations Diagnostic and Statistical Manual-IV,Text Revision (DSM-IV-TR) (1) criteria or ASDs. A child isincluded as meeting the surveillance case deinition or ASD i
he or she displays behaviors at any time rom birth through theend o the year when the child reaches age 8 years, as describedon a comprehensive evaluation by a qualiied proessional, thatare consistent with the DSM-IV-TR diagnostic criteria orany o the ollowing conditions: Autistic Disorder; PervasiveDevelopmental DisorderNot Otherwise Speciied (PDD-NOS, including Atypical Autism); or Asperger Disorder.
Descriptive CharacteristicsIn addition to coding DSM-IV-TR diagnostic
criteria or determining ASD case status, clinicianreviewers systematically record additional indingsrom each abstracted evaluation. For example
reviewers note any concerns regarding the childsdevelopment by age 3 years, with speciic ocuson the development o social, language, andimaginative play skills as well as any mention oregression or plateau in skill development. Thediagnostic conclusions rom each evaluation recordalso are summarized or each child, includingnotation o any ASD diagnosis by subtypewhen available. Children are considered to havea previously documented ASD classiication ithey received a diagnosis o Autistic DisorderPDD-NOS, Asperger Disorder, or ASD that was
documented in an abstracted evaluation or by anICD-9 billing code at any time rom birth throughthe end o the year when they reached age 8 yearsor i they received special education services underan autism eligibility during the surveillance year.
Inormation on childrens unctional skills alsois abstracted rom source records, when availableincluding scores on tests o intellectual abilityChildren are classiied as having intellectuadisability i they had an intelligence quotient (IQ)score o 70 on their most recent test available in therecord. Borderline intellectual ability is deined as
having an IQ score o 7185, and average or above-average intellectual ability is deined as having anIQ score o >85. In the absence o a speciic IQscore, an examiners statement about the childsintellectual ability, i available, is used to classiythe child in one o these three levels.
Quality AssuranceAll sites ollow the same quality assurance standard
established by the ADDM Network. For Phase 1, screeningand abstraction o source records are monitored or accuracy
on a periodic basis. In Phase 2, ongoing inter-rater reliabilitychecks are conducted on a blinded, random sample o 10% orecords undergoing clinician review. For the 2008 surveillanceyear, when comparison samples rom all sites are combined,inter-rater agreement on case status (conirmed ASD versus notASD) was 90.2% (k = 0.8); this exceeds the minimal qualityassurance standards established by the ADDM Network orall surveillance years.
BOX. Core list of International Classification of Diseases, Ninth Revision billingcodes used by all Autism and Developmental Disabilities Monitoring Networksites to identify records for review at health sources
299.0 Autistic disorder299.1 Childhood disintegrative disorder
299.8 Other speciied pervasive developmental disorders299.9 Unspeciied pervasive developmental disorder315.30 Developmental speech or language disorder315.31 Expressive language disorder315.32 Mixed receptive-expressive language disorder315.4 Developmental coordination disorder315.5 Mixed development disorder315.8 Other speciied delays in development315.9 Unspeciied delay in development317.0 Mild mental retardation318.0 Moderate mental retardation318.1 Severe mental retardation
318.2 Proound mental retardation319.0 Unspeciied mental retardation330.8 Other speciied cerebral degenerations in childhood348.3 Encephalopathy, not elsewhere classiied348.8 Other conditions o brain348.9 Unspeciied condition o brain759.5 Tuberous sclerosis759.83 Fragile X syndrome771.0 Congenital rubella783.42 Delayed milestonesV79.2 Screening, mental retardationV79.3 Screening, developmental handicaps in early childhood
V79.8 Screening, other speciied mental disorders anddevelopmental handicaps
V79.9 Screening, unspeciied mental disorder anddevelopmental handicap
-
8/2/2019 CDC Autism Study, March 2012
7/24
Surveillance Summaries
MMWR / March 30, 2012 / Vol. 61 / No. 3 5
Analytic MethodsPopulation denominators or calculating ASD prevalence
estimates were obtained rom CDCs National Center orHealth Statistics (NCHS) vintage 2009 bridged-race postcensalpopulation estimates or calculating vital rates (15). NCHS
provides estimated population counts by state, county,single year o age, race, ethnic origin, and sex. Populationdenominators or the 2008 surveillance year were compiledrom the postcensal estimates o children aged 8 years living inthe counties under surveillance by each ADDM site (Table 1).
For two sites (Arizona and Utah), partial counties wereincluded in the 2008 surveillance area, so geographic boundarieswere deined by the school district(s) included in the surveillancearea. Counts o children residing in outlying school districts weresubtracted rom the county-level postcensal denominators usingschool enrollment data rom the U.S. Department o EducationsNational Center or Education Statistics (16). Enrollment counts
o students in third grade during the 200809 school year werenoted to dier rom NCHS postcensal population estimates; thisdierence was attributable primarily to children being enrolledout o the customary grade or their age, in private schools,or home-schooled. Because these dierences varied by raceand sex within the applicable counties, a race- and sex-speciicadjustment actor based on enrollment data was applied to theNCHS data to derive school districtspeciic denominators orthese two states.
For comparison o prevalence estimates across multipletime points, population estimates also were obtained romthe NCHS vintage 2009 bridged-race postcensal population
estimates (15) using the number o children aged 8 years livingin the surveillance counties during 2002, 2006, and 2008.These population estimates dier slightly rom those used inprevious ADDM reports but represent the most recent availabledata (17) or evaluating changes in the prevalence o ASDsacross multiple time points.
The race/ethnicity o each child whose records wereabstracted was determined rom inormation contained insource records or, i not ound in the source ile, rom birthcertiicates (when available). Race- or ethnicity-speciicprevalence estimates were calculated or ive populations: non-Hispanic white, non-Hispanic black, Hispanic, Asian/PaciicIslander, and American Indian/Alaska Native. Prevalenceresults are reported as the total number o children meetingthe ASD case deinition per 1,000 children aged 8 years inthe population in each race/ethnicity group. ASD prevalencealso was calculated separately or males and emales, as wellas within each level o intellectual ability. Overall prevalenceestimates include all children identiied with ASDs regardless
o sex, race/ethnicity, or level o intellectual ability and thus arenot aected by the availability o data on these characteristics
Conidence intervals (CIs) or prevalence estimates werederived under the assumption that the observed counts ochildren identiied with ASDs are random variables drawn roman underlying Poisson distribution. For the current report
chi-square tests, rate ratios (RRs), and percentage dierenceswere calculated to compare prevalence estimates within andacross sites and between surveillance years. A maximum valueo p
-
8/2/2019 CDC Autism Study, March 2012
8/24
Surveillance Summaries
6 MMWR / March 30, 2012 / Vol. 61 / No. 3
Funding or most ADDM Network sites participating in the2008 surveillance year was awarded or a 4-year cycle during20062010, during which time data were collected or the2006 and 2008 surveillance years. However, three additionalsites (Arkansas, New Jersey, and Utah) were unded during20092010 to collect data or the 2008 surveillance yearonly. These three sites also had participated in the ADDM
2002 surveillance year and were able to compare their 2008prevalence results to those rom 2002. However, because only 1year o unding was available to complete the study, these threesites covered smaller surveillance areas in 2008 compared withother sites and with the earlier surveillance year(s) in whichthese three returning sites participated. This enabled the threesites to complete surveillance year 2008 on the same timelineas other ADDM Network sites. However, this abbreviated
timeline required that population denominators or eacho the three returning sites be ewer than 10,000 childrenpotentially yielding less representative prevalence estimatesor Arkansas, New Jersey, and Utah. Results rom the ADDM2004 surveillance year were not compared with 2008 resultsbecause only eight o the 14 sites completed both studies, andthe 2004 surveillance year represented a smaller scale, optiona
eort based on available resources.Seven o the 14 sites participating in the 2008 surveillanceyear included a dierent mix o counties or school districts in2008 compared with 1 or more previous surveillance yearsFor these sites, numerators and denominators or between-yearcomparisons were restricted systematically to residents o the coresurveillance area that were common across all surveillance years ina given analysis (i.e., 2008-to-2002 ratios, 2008-to-2006 ratios
TABLE 1. Number* and percentage of children aged 8 years, by race/ethnicity and site Autism and Developmental Disabilities MonitoringNetwork, 14 sites, United States, 2008
Site Site/Institution Surveillance area
TotalWhite,
non-HispanicBlack,
non-Hispanic Hispanic API AI/AN
No. No. (%) No. (%) No. (%) No. (%) No. (%)
Alabama Univ of Alabama at
Birmingham
32 counties in north and
central Alabama
36,566 24,516 (67.0) 9,295 (25.4) 2,112 (5.8) 489 (1.3) 154 (0.4)
Arizona Univ of Arizona Part of 1 county in
metropolitan Phoenix
32,601 15,022 (46.1) 1,804 (5.5) 14,227 (43.6) 893 (2.7) 655 (2.0)
Arkansas Univ of Arkansas for
Medical Sciences
1 county (Pulaski) in
metropolitan Little Rock
4,940 2,371 (48.0) 2,112 (42.8) 296 (6.0) 123 (2.5) 38 (0.8)
Colorado Colorado Dept of Public
Health and Environment
1 county (Arapahoe) in
metropolitan Denver
7,725 3,990 (51.7) 1,051 (13.6) 2,233 (28.9) 387 (5.0) 64 (0.8)
Colorado Colorado Dept of Public
Health and Environment
6 counties in metropolitan
Denver (excludes Arapahoe)
29,336 16,923 (57.7) 1,390 (4.7) 9,660 (32.9) 1,179 (4.0) 184 (0.6)
Florida Univ of Miami 1 county (MiamiDade) in
south Florida
29,366 7,013 (23.9) 6,328 (21.5) 15,540 (52.9) 445 (1.5) 40 (0.1)
Georgia CDC 5 counties including
metropolitan Atlanta
50,427 18,725 (37.1) 20,690 (41.0) 7,875 (15.6) 2,958 (5.9) 179 (0.4)
Maryland Johns Hopkins Univ 6 counties in suburban
Baltimore
27,022 18,337 (67.9) 5,796 (21.4) 1,347 (5.0) 1,467 (5.4) 75 (0.3)
Missouri Washington Univ
St. Louis
5 counties including
metropolitan St. Louis
25,668 17,718 (69.0) 6,153 (24.0) 891 (3.5) 816 (3.2) 90 (0.4)
New Jersey Univ of Medicine and
Dentistry of New Jersey
1 county (Union) in
metropolitan Newark
7,082 3,096 (43.7) 1,601 (22.6) 2,050 (28.9) 322 (4.5) 13 (0.2)
North Carolina Univ of North Carolina
Chapel Hill
11 counties in central
North Carolina
36,913 21,038 (57.0) 9,414 (25.5) 4,977 (13.5) 1,353 (3.7) 131 (0.4)
Pennsy lvania Univ of Pennsylvani a 1 metropolitan count y
(Philadelphia)
18,440 5,180 (28.1) 9,060 (49.1) 3,067 (16.6) 1,067 (5.8) 66 (0.4)
South Carol ina Medical Univ of
South Carolina
23 counties in Coastal and
Pee Dee regions
23,769 12,506 (52.6) 9,566 (40.2) 1,285 (5.4) 295 (1.2) 117 (0.5)
Utah Univ of Utah Part of 1 county in
northern Utah
2,123 899 (42.3) 116 (5.5) 902 (42.5) 171 (8.1) 35 (1.6)
Wisconsin Univ of
WisconsinMadison
10 counties in south
eastern Wisconsin
34,451 22,479 (65.2) 5,818 (16.9) 4,720 (13.7) 1,264 (3.7) 170 (0.5)
Abbreviations: API = Asian/Pacific Islander; AI/AN = American Indian/ Alaska Native.
* Total numbers of children aged 8 years in each surveillance area were obtained from CDCs National Center for Health Statistics vintage 2009 postcensal population estimates. Denominator excludes school districts that were not included in the surveillance area, calculated from National Center on Education Statistics enrollment counts of third graders duringthe 20082009 school year.
Colorado health and education source type surveillance area. Expanded Colorado health source type only surveillance area.
-
8/2/2019 CDC Autism Study, March 2012
9/24
Surveillance Summaries
MMWR / March 30, 2012 / Vol. 61 / No. 3 7
and statistics that include all 3 surveillance years). Numeratorsor these comparisons were selected based on the childs countyo residency or, or sites with surveillance areas deined by schooldistricts, based on the childs census block group o residencywithin school district boundaries. Denominators or between-year comparisons were based on county-level NCHS postcensal
estimates or the core surveillance area that was included duringboth surveillance years in a given comparison. For sites withsurveillance areas deined by school districts, only those schooldistricts included in both surveillance years were included whendenominators or between-year comparisons were calculated.For these sites, county-level population estimates were adjustedaccording to school enrollment data in the same manner asdenominators or the 2008 surveillance year were computedbut urther restricted to the school districts included in bothsurveillance years in a given comparison. Sites adjusting theirdenominators in this manner included Arizona or both the2008-to-2006 and the 2008-to-2002 comparisons, as well asNew Jersey and Utah or the 2008-to-2002 comparisons (schooldistricts were used in deining surveillance areas or New Jerseyin 2002 and Utah in 2008). Comparisons between surveillanceyears were not aected by any changes in sites agreements toaccess education records because no sites had access to educationsources or one surveillance year but not or the other.
ResultsThe 14 ADDM sites that provided data or the 2008
surveillance year covered a total population o 337,093 children
aged 8 years, which represented 8.4% o the U.S. populationo children that age in 2008 (13). A total o 48,247 sourcerecords or 38,253 children were reviewed at education andhealth sources. O these, the source records o 6,739 childrenmet the criteria or abstraction, which was 17.5% o thetotal number o children whose source records were reviewedand 2% o the total population under surveillance (range:1.0% [Alabama]6.3% [Utah]). During clinician review,3,820 children (57%) were conirmed as meeting the ASDsurveillance case deinition (range: 30% [Arkansas]74%[North Carolina]). The number o evaluations abstractedor each child ultimately identiied as having an ASD varied
(median: 5; range: 3 [Florida and North Carolina]10 [Utah].
Overall ASD Prevalence EstimatesWhen data rom all 14 ADDM sites in the 2008 surveillance
year were combined, overall estimated ASD prevalence was11.3 per 1,000 (one in 88) children aged 8 years (range:4.8 [Alabama]21.2 [Utah]) (Table 2). Overall estimated
prevalence o ASDs was signiicantly lower in Alabama (4.8 per1,000) than in any other site. Utah had the highest estimated ASD prevalence (21.2 per 1,000), which was signiicantlyhigher than all other sites except Arizona and New JerseyThe overall estimated ASD prevalence in New Jersey (20.5per 1,000) was signiicantly higher than in any other site
except Utah.On average, estimated ASD prevalence was signiicantly
higher in ADDM sites that had access to education sourcescompared with sites that relied solely on health sources toidentiy cases (RR: 1.5; 95% CI = 1.41.7; p
-
8/2/2019 CDC Autism Study, March 2012
10/24
Surveillance Summaries
8 MMWR / March 30, 2012 / Vol. 61 / No. 3
site that identiied approximately the same estimated ASDprevalence among non-Hispanic white children, non-Hispanicblack children, and Hispanic children. Estimates or Asian/Paciic Islander children ranged rom 2.2 to 19.0 per 1,000
although wide conidence intervals suggest that these indingsshould be interpreted with caution.
TABLE 2. Estimated prevalence* of autism spectrum disorders (ASDs) per 1,000 children aged 8 years, by sex and race/ethnicity Autism andDevelopmental Disabilities Monitoring Network, 14 sites, United States, 2008
Site Total no.Total no.
with ASDs
Sex
Male-to-femaleprev ratio
Total Male Female
Prev 95% CI Prev 95% CI Prev 95% CI
Alabama 36,566 174 4.8 (4.15.5) 8.1 (7.09.5) 1.1 (0.71.8) 7.2
Arizona 32,601 507 15.6 (14.317.0) 25.1 (22.827.6) 5.4 (4.46.7) 4.6Arkansas 4,940 52 10.5 (8.013.8) 17.5 (13.023.6) 3.6 (1.97) 4.8
Colorado 7,725 91 11.8 (9.614.5) 20.1 (16.125.0) 2.9 (1.65.3) 6.8Colorado** 29,336 188 6.4 (5.67.4) 10.4 (8.912.2) 2.2 (1.63.1) 4.7
Florida 29,366 211 7.2 (6.38.2) 11.3 (9.713.1) 2.9 (2.13.9) 3.9
Georgia 50,427 601 11.9 (11.012.9) 19.6 (18.021.4) 3.8 (3.14.6) 5.2Maryland 27,022 336 12.4 (11.213.8) 20.5 (18.323.1) 3.9 (2.95.1) 5.3
Missouri 25,668 357 13.9 (12.515.4) 21.6 (19.224.3) 5.9 (4.77.4) 3.7
New Jersey 7,082 145 20.5 (17.424.1) 34.2 (28.740.7) 5.8 (3.89.1) 5.8North Carolina 36,913 525 14.2 (13.115.5) 23.1 (21.025.3) 5.1 (4.16.2) 4.5
Pennsylvania 18,440 245 13.3 (11.715.1) 22.2 (19.425.4) 4.3 (3.15.8) 5.2
South Carolina 23,769 264 11.1 (9.812.5) 18.3 (16.120.9) 3.5 (2.64.8) 5.2Utah 2,123 45 21.2 (15.828.4) 31.7 (22.444.8) 11.7 (6.820.1) 2.7
Wisconsin 34,451 267 7.8 (6.98.7) 11.7 (10.213.4) 3.7 (2.94.7) 3.2
Total 337,093 3,820 11.3 (11.011.7) 18.4 (17.719.0) 4.0 (3.74.3) 4.6
See table footnotes below.
TABLE 2. (Continued) Estimated prevalence* of autism spectrum disorders (ASDs) per 1,000 children aged 8 years, by sex and race/ethnicity Autism and
Developmental Disabilities Monitoring Network, 14 sites, United States, 2008
Site
Race/Ethnicity Prev ratio
White, non-Hispanic Black, non-Hispanic Hispanic API White-to-black
White-to-Hispanic
Black-to-HispanicPrev 95% CI Prev 95% CI Prev 95% CI Prev 95% CI
Alabama 5.0 (4.26.0) 4.0 (2.95.5) 1.4 (0.54.4) 4.1 (1.016.4) 1.3 3.5 2.8
Arizona 20.7 (18.523.1) 16.1 (11.223.1) 8.9 (7.510.6) 19.0 (11.830.6) 1.3 2.3 1.8
Arkansas 13.5 (9.519.1) 7.1 (4.311.8) 10.1 (3.331.4) 1.9 1.3 0.7Colorado 14.8 (11.519.1) 10.5 (5.818.9) 6.7 (4.111.1) 2.6 (0.418.3) 1.4 2.2 1.6
Colorado** 7.3 (6.18.7) 6.5 (3.412.4) 3.5 (2.54.9) 0.9 (0.16.0) 1.1 2.1 1.8
Florida 4.6 (3.26.5) 3.0 (1.94.7) 8.2 (6.99.8) 2.2 (0.316) 1.5 0.6 0.4
Georgia 11.8 (10.313.5) 11.9 (10.513.5) 7.1 (5.59.2) 15.9 (11.921.1) 1.0 1.7 1.7
Maryland 12.9 (11.414.7) 11.7 (9.314.9) 5.9 (311.9) 8.2 (4.614.4) 1.1 2.2 2.0
Missouri 14.6 (12.916.5) 9.3 (7.112) 9.0 (4.518) 9.8 (4.919.6) 1.6 1.6 1.0New Jersey 21.0 (16.526.8) 20.6 (14.729) 20.0 (14.727.2) 3.1 (0.422) 1.0 1.0 1.0
North Carolina 14.6 (13.116.4) 15.4 (13.118.1) 7.6 (5.610.5) 11.8 (7.219.3) 1.0 1.9 2.0
Pennsylvania 14.3 (11.417.9) 12.7 (10.615.2) 9.1 (6.313.2) 8.4 (4.416.2) 1.1 1.6 1.4South Carolina 10.2 (8.612.2) 9.9 (8.112.1) 7.0 (3.613.5) 1.0 1.5 1.4
Utah 40.0 (28.955.5) 25.9 (8.380.2) 4.4 (1.711.8) 1.5 9.0 5.8
Wisconsin 8.6 (7.59.9) 5.0 (3.57.2) 3.8 (2.46.1) 2.4 (0.87.4) 1.7 2.3 1.3Total 12.0 (11.512.5) 10.2 (9.510.9) 7.9 (7.28.6) 9.7 (8.111.6) 1.2 1.5 1.3
Abbreviations: CI = confidence interval; API = Asian/Pacific Islander.* Per 1,000 children aged 8 years. All children are included in the total regardless of race or ethnicity. Overall prevalence also includes children for whom race/ethnicity was unknown. All sites identified statistically significantly higher prevalence among males compared with females (p
-
8/2/2019 CDC Autism Study, March 2012
11/24
Surveillance Summaries
MMWR / March 30, 2012 / Vol. 61 / No. 3 9
Previously Documented ASD Classification Among all children meeting the ASD surveillance case
deinition, approximately 79% had a previously documentedASD classiication (range: 67% [Colorado]87% [Pennsylvaniaand Wisconsin]). The median age o earliest known ASDdiagnosis documented in childrens records (Table 3) variedby diagnostic subtype (Autistic Disorder: 48 months; ASD/PDD: 53 months; Asperger Disorder: 75 months). O the2,627 children with a diagnostic subtype on record, 516 (20%)had dierent subtypes noted across multiple evaluations,suggesting instability in the initial subtype diagnosed orapproximately one in ive children. The age o earliest knowndiagnosis or all subtypes combined is not reported because osubstantial variability in the median age at the earliest knownASD diagnosis by subtype, the proportion o children withineach subtype category across the dierent ADDM sites, andthe subtype noted across multiple evaluations or each child.
Special Education EligibilitySites with access to education records collected inormation
about the eligibility categories under which special educationservices were received in public schools (Table 4). Widevariation existed in the proportion o children with a primaryeligibility category o autism (range: 39% [Colorado]72%[North Carolina]). In Colorado, autism is a subcategory ophysical disability, so the primary eligibility might have beendocumented as autism or physical disability, depending on theschool district. Other common special education eligibilitiesincluded intellectual disability, health or physical disabilityspeech and language impairment, and speciic learningdisability, with these proportions also varying by site.
Intellectual AbilityData on intellectual ability are reported or the seven sites
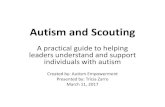
having inormation available or at least 70% o children whomet the ASD case deinition (Figure 2). When data rom theseseven sites were combined, 38% o children with ASDs were
FIGURE 1. Estimated prevalence (per 1,000 population) of autism spectrum disorders (ASDs) among children aged 8 years, by access to educationrecords and population size covered Autism and Developmental Disabilities Monitoring Network (ADDM), 14 sites, United States, 2008
* 95% confidence intervals. Overall weighted ASD prevalence. Expanded Colorado health source type only surveillance area.
Colorado health and education source type surveillance area.** Size of dot represents total population of children aged 8 years residing in the surveillance area.
Alabama
Wisconsin
Florida
Colorado
Missouri
Pennsylvania
Georgia
North Carolina
Arizona
Maryland
South Carolina
Colorado
New Jersey
Arkansas
Utah
Prevalence
ADDMs
ite
Approximate
population size**
2,500
10,000
22,500
40,000
ADDM site type
Health onlysource type
Education andhealth source type
2520151050 30
*
-
8/2/2019 CDC Autism Study, March 2012
12/24
-
8/2/2019 CDC Autism Study, March 2012
13/24
Surveillance Summaries
MMWR / March 30, 2012 / Vol. 61 / No. 3 11
Evaluation of Missing Records andExpanded ICD-9 Codes
Underascertainment o ASDs because o missing recordsvaried by site. The majority o sites estimated that the totalnumber o children identiied with ASDs might potentiallyhave increased 85
IQ 7185
IQ 70
0
10
20
30
40
50
60
70
80
90
100
M F M F M F M F M F M F M F M F
Arizona Arkansas Georgia New Jersey N. Carolina S. Carolina Utah Total
Percentage
-
8/2/2019 CDC Autism Study, March 2012
14/24
Surveillance Summaries
12 MMWR / March 30, 2012 / Vol. 61 / No. 3
2006 and 2008, and one site identiied a lower ASD prevalenceamong emales in 2008 compared with 2006.
Changes in estimated ASD prevalence during 20062008also varied by race within individual ADDM sites and whencombining data rom all sites. The combined estimates
indicated a 16% increase in ASD prevalence among non-Hispanic white children (10.011.5 per 1,000), a 42% increaseamong non-Hispanic black children (7.010.0 per 1,000)and a 29% increase among Hispanic children (6.17.9 per1,000). The percentage increase was statistically signiicant
TABLE 5. Estimated prevalence of autism spectrum disorders (ASDs) per 1,000 children aged 8 years, by sex and race/ethnicity comparisoof select earlier surveillance years to 2008, with rate ratio and percentage of prevalence change* Autism and Developmental DisabilitiesMonitoring Network, 14 sites, United States, 2002, 2006, and 2008
Alabama Arizona Arkansas Colorado Florida Georgia Maryland MissouriNew
JerseyNorth
Carolina PennsylvaniaSouth
Carolina Utah WisconsinAll sites
combined
Total ASD
2002 3.3 7.9 10.6 6.2 7.5 7.0 7.2 11.1 6.6 5.2 6.1 8.3 5.1 6.4
2008 4.8 15.6 10.5 11.8 11.9 12.1 13.9 20.3 12.7 13.3 11.1 21.2 7.8 11.4Rate ratio 1.5 2.0 1.0 1.9 1.6 1.7 1.9 1.8 1.9 2.6 1.8 2.6 1.5 1.8
(95% CI) (1.31.7) (1.92.1) (0.61.4) (1.52.3) (1.51.7) (1.51.9) (1.72.1) (1.52.1) (1.72.1) (2.42.8) (1.62) (2.13.1) (1.31.7) (1.71.9)
% change 45.6 97.1 -0.3 88.8 58.3 74.1 92.7 83.4 93.6 156.1 83.0 157.0 51.7 78.5
2006 6.0 15.8 7.4 4.0 10.1 9.1 12.1 10.2 8.4 8.8 7.7 9.0
2008 4.8 15.6 11.8 7.2 11.9 12.4 13.9 12.4 13.3 11.1 7.8 11.0
Rate ratio 0.8 1.0 1.6 1.8 1.2 1.4 1.1 1.2 1.6 1.3 1.0 1.2
(95% CI) (0.61) (0.91.1) (1.31.9) (1.62) (1.11.3) (1.21.6) (0.91.3) (11.4) (1.41.8) (1.11.5) (0.81.2) (1.11.3)
% change -20.4 -1.8 60.1 79.8 18.0 36.7 14.9 21.0 58.6 26.0 0.8 22.6
Male
2002 5.0 12.9 17.4 10.8 12.3 10.6 11.2 18.2 10.8 8.5 9.3 15.6 7.8 10.2
2008 8.1 25.1 17.5 20.1 19.6 20.2 21.6 33.9 20.6 22.2 18.3 31.7 11.7 18.6
Rate ratio 1.6 2 1.0 1.9 1.6 1.9 1.9 1.9 1.9 2.6 2.0 2.0 1.5 1.8
(95% CI) (1.31.9) (1.82.2) (0.61.4) (1.52.3) (1.51.7) (1.72.1) (1.72.1) (1.62.2) (1.72.1) (2.42.8) (1.82.2) (1.42.6) (1.31.7) (1.71.9)
% change 61.5 95.3 0.5 86.2 59.7 90.9 93.6 86.2 91.7 160.0 97.7 103.3 49.4 81.6
2006 9.0 24.5 11.3 6.9 16.5 15.5 19.3 16.8 13.2 14.6 13.0 14.5
2008 8.1 25.1 20.1 11.3 19.6 20.6 21.6 19.9 22.2 18.3 11.7 17.9
Rate ratio 0.9 1.0 1.8 1.6 1.2 1.3 1.1 1.2 1.7 1.3 0.9 1.2(95% CI) (0.71.1) (0.91.1) (1.42.2) (1.41.8) (1.11.3) (1.11.5) (0.91.3) (11.4) (1.51.9) (1.11.5) (0.71.1) (1.11.3)
% change -9.5 2.4 77.2 62.7 18.6 32.4 12.4 18.2 67.8 25.8 9.7 23.0
Female
2002 1.4 2.7 3.7 1.4 2.6 3.2 3.0 3.5 2.1 1.8 2.8 0.9 2.3 2.4
2008 1.1 5.4 3.6 2.9 3.8 3.6 5.9 5.7 4.6 4.3 3.5 11.7 3.7 4.0
Rate ratio 0.8 2.0 1.0 2.1 1.4 1.1 1.9 1.6 2.2 2.4 1.3 12.7 1.6 1.6
(95% CI) (0.21.4) (1.62.4) (0.11.9) (13.2) (1.11.7) (0.61.6) (1.52.3) (0.92.3) (1.72.7) (1.92.9) (0.81.8) (10.714.7) (1.22) (1.51.7)
% change -18.7 102.6 -2.7 110.0 44.6 13.2 93.4 62.8 115.1 138.0 28.4 1168.5 61.9 63.2
2006 2.8 6.4 3.3 0.9 3.4 2.4 4.8 3.4 3.3 2.6 2.3 3.2
2008 1.1 5.4 2.9 2.9 3.8 3.9 5.9 4.6 4.3 3.5 3.7 3.8
Rate ratio 0.4 0.8 0.9 3.1 1.1 1.6 1.2 1.4 1.3 1.4 1.6 1.2
(95% CI) (0.10.9) (0.51.1) (0.11.7) (2.53.7) (0.81.4) (1.22) (0.91.5) (11.8) (0.81.8) (0.91.9) (1.22) (1.11.3)
% change -60.1 -15.6 -10.9 212.0 11.9 63.7 23.8 37.4 28.3 34.7 59.1 20.8
White, non-Hispanic
2002 3.3 9.9 10.5 6.7 8.8 7.1 7.6 15.1 6.5 7.6 6.1 15.1 5.8 7.0
2008 5.0 20.7 13.5 14.8 11.8 12.1 14.6 20.4 12.7 14.3 10.2 40.0 8.6 11.9
Rate ratio 1.5 2.1 1.3 2.2 1.3 1.7 1.9 1.4 2.0 1.9 1.7 2.7 1.5 1.7
(95% CI) (1.21.8) (1.92.3) (0.81.8) (1.82.6) (1.11.5) (1.51.9) (1.72.1) (11.8) (1.72.3) (1.52.3) (1.42) (2.13.3) (1.31.7) (1.61.8)
% change 54.0 109.3 28.2 122.4 34.2 71.0 91.6 35.3 96.0 87.5 69.0 165.5 47.8 69.5
2006 5.8 18.3 6.6 3.3 12.0 9.2 13.7 12.0 10.3 7.3 8.7 10.0
2008 5.0 20.7 14.8 4.6 11.8 12.9 14.6 12.2 14.3 10.2 8.6 11.5
Rate ratio 0.9 1.1 2.2 1.4 1.0 1.4 1.1 1.0 1.4 1.4 1.0 1.2
(95% CI) (0.71.1) (0.91.3) (1.72.7) (0.91.9) (0.81.2) (1.21.6) (0.91.3) (0.81.2) (11.8) (1.11.7) (0.81.2) (1.11.3)
% change -13.3 13.1 123.1 39.0 2.0 40.3 6.7 1.7 38.2 40.9 1.3 15.6
Black, non-Hispanic
2002 3.4 7.0 9.6 5.6 6.7 6.7 4.7 6.4 7.2 4.1 5.5 0 3.6 5.5
2008 4.0 16.1 7.1 10.5 11.9 12.6 9.3 20.6 14.2 12.7 9.9 25.9 5.0 10.5
Rate ratio 1.2 2.3 0.7 1.9 1.8 1.9 2.0 3.2 2.0 3.1 1.8 NA** 1.4 1.9
(95% CI) (0.71.7) (1.63) (0.11.4) (0.83.0) (1.62) (1.52.3) (1.62.4) (2.53.9) (1.62.4) (2.83.4) (1.52.1) NA (0.91.9) (1.82.0)
% change 17.8 128.7 -26.2 88.6 77.9 87.2 97.6 222.3 98.3 207.3 79.2 NA 37.2 91.1
2006 6.7 16.8 12.1 1.5 9.3 7.8 5.1 7.4 7.4 7.4 3.7 7.0
2008 4.0 16.1 10.5 3.0 11.9 11.7 9.3 14.2 12.7 9.9 5.0 10.0
Rate ratio 0.6 1.0 0.9 2.0 1.3 1.5 1.8 1.9 1.7 1.3 1.4 1.4
(95% CI) (0.21) (0.51.5) (0.11.7) (1.22.8) (1.11.5) (1.11.9) (1.42.2) (1.52.3) (1.42) (11.6) (0.82) (1.31.5)
% change -40.6 -4.5 -13.7 96.1 27.8 50.8 80.9 91.2 72.4 34.7 36.4 42.1
See table footnotes on page 13.
-
8/2/2019 CDC Autism Study, March 2012
15/24
Surveillance Summaries
MMWR / March 30, 2012 / Vol. 61 / No. 3 13
or all three racial/ethnic groups. Alabama identiied a lowerprevalence among non-Hispanic black children in 2008, andArizona identiied a lower prevalence among Hispanic childrenin 2008 compared with 2006 results.
In the our sites with IQ test data available on at least 70%o children with ASDs in both the 2006 and 2008 surveillanceyears, the estimated prevalence o ASD with intellectualdisability increased 12% on average (4.24.7 per 1,000), whilethe prevalence o ASD with borderline intellectual ability
increased 22% (2.32.8 per 1,000), and the prevalence o ASDwith average or above-average intellectual ability increased 13%(3.94.4 per 1,000).
Comparison Between 2002 and 2008Prevalence Estimates
Thirteen ADDM sites completed both the 2002 and 2008surveillance years, with all but one (Arkansas) identiying a
TABLE 5. (Continued) Estimated prevalence of autism spectrum disorders (ASDs) per 1,000 children aged 8 years, by sex and race/ethnicit comparison of select earlier surveillance years to 2008, with rate ratio and percentage of prevalence change* Autism and DevelopmentaDisabilities Monitoring Network, 14 sites, United States, 2002, 2006 and 2008
Alabama Arizona Arkansas Colorado Florida Georgia Maryland MissouriNew
JerseyNorth
Carolina PennsylvaniaSouth
Carolina Utah WisconsinAll sites
combined
Hispanic
2002 1.9 4.4 5.6 2.8 4.6 0 1.6 6.4 4.2 4.6 4.3 0 0.3 3.7
2008 1.4 8.9 10.1 6.7 7.1 4.3 9.0 20.1 6.9 9.1 7.0 4.4 3.8 7.7Rate ratio 0.8 2.0 1.8 2.4 1.5 NA 5.5 3.1 1.7 2.0 1.6 NA 13.2 2.1
(95% CI) (0.12.6) (1.72.3) (0.54.1) (1.33.5) (1.02.0) NA (3.47.6) (2.43.8) (0.92.5) (1.42.6) (0.32.9) NA (11.215.0) (1.92.3)
% change -26.3 102.3 80.4 139.3 54.3 NA 462.5 214.1 64.3 97.8 62.8 NA 1,166.7 109.2
2006 0.6 11.4 4.4 4.9 4.8 6.2 2.6 5.9 7.7 4.7 1.7 6.1
2008 1.4 8.9 6.7 8.2 7.1 5.9 9.0 6.7 9.1 7.0 3.8 7.9
Rate ratio 2.3 0.8 1.5 1.7 1.5 1.0 3.5 1.1 1.2 1.5 2.2 1.3
(95% CI) (0.14.6) (0.61) (0.62.4) (1.42) (1.11.9) (0.12) (25) (0.51.7) (0.61.8) (0.42.6) (1.33.1) (1.21.4)
% change 132.8 -21.7 53.8 67.8 48.1 -3.9 246.7 12.3 18.7 47.7 122.8 29.1
IQ < 70
2002 2.8 3.5 3.4 3.7 3.0 3.3 1.8 3.2
2008 4.9 3.6 4.6 4.9 4.1 5.1 2.4 4.6
Rate ratio 1.7 1.0 1.3 1.3 1.4 1.6 1.3 1.5
(95% CI) (1.42) (0.31.7) (1.11.5) (0.81.8) (1.11.7) (1.31.9) (0.12.6) (1.41.6)
% change 73.2 3.4 33.7 33.9 39.1 56.6 29.0 45.4
2006 5.9 3.5 3.8 3.9 4.2
2008 4.9 4.6 4.1 5.1 4.7
Rate ratio 0.8 1.3 1.1 1.3 1.1(95% CI) (0.61.0) (1.11.5) (0.81.4) (11.6) (1.01.2)
% change -17.8 32.6 6.8 31.5 11.9
IQ = 7185
2002 1.6 3.3 1.3 1.9 1.4 0.7 0 1.4
2008 3.5 3.0 2.5 4.4 3.3 2.3 3.3 2.9
Rate ratio 2.2 0.9 2.0 2.4 2.3 3.6 NA 2.2
(95% CI) (1.92.5) (0.21.6) (1.72.3) (1.73.1) (1.92.7) (34.2) NA (2.02.4)
% change 119.6 -8.2 96.9 135.1 130.5 255.4 NA 116.8
2006 3.3 2.1 1.9 1.6 2.3
2008 3.5 2.5 3.2 2.3 2.8
Rate ratio 1.0 1.2 1.7 1.5 1.2
(95% CI) (0.71.3) (0.91.5) (1.32.1) (1.11.9) (1.01.4)
% change 3.9 20.8 66.5 47.1 21.7
IQ >85
2002 2.9 3.5 2.3 3.4 1.9 1.7 4.1 2.4
2008 6.5 2.6 4.0 8.3 4.8 2.0 12.3 4.7
Rate ratio 2.3 0.7 1.7 2.4 2.5 1.2 3.0 1.9
(95% CI) (2.12.5) (0.11.4) (1.51.9) (1.92.9) (2.12.9) (0.81.6) (2.23.8) (1.82.0)
% change 127.3 -25.3 75.2 142.5 152.1 16.1 196.6 92.9
2006 5.5 3.7 4.1 2.1 3.9
2008 6.5 4.0 4.6 2.0 4.4
Rate ratio 1.2 1.1 1.1 1.0 1.1
(95% CI) (1.01.4) (0.91.3) (0.81.4) (0.61.4) (1.01.2)
% change 18.4 8.6 13.1 -4.3 12.8
Abbreviations: CI = confidence interval; NA = not available.* Rate ratios and percentage change calculated with 2008 as the numerator and either 2002 or 2006 as the denominator. Data not reported. Rate ratio statistically significant at p
-
8/2/2019 CDC Autism Study, March 2012
16/24
Surveillance Summaries
14 MMWR / March 30, 2012 / Vol. 61 / No. 3
signiicantly higher prevalence o ASDs in 2008 compared with2002 (Table 5). When data rom all sites were combined, ASDprevalence estimates among children aged 8 years increased78% during 20022008 (rom 6.4 to 11.4 per 1,000). Thecombined increase across all sites was 82% or males (10.218.6 per 1,000) and 63% or emales (2.44.0 per 1,000)
during this 6-year period. The combined estimates indicateda 70% increase among non-Hispanic white children (7.011.9per 1,000), a 91% increase among non-Hispanic black children(5.510.5 per 1,000), and a 110% increase among Hispanicchildren (3.77.7 per 1,000) during 20022008.
In the seven sites with IQ test data available on at least 70%o children with ASDs in both the 2002 and 2008 surveillanceyears, estimated prevalence o ASD with intellectual disabilityincreased 45% on average (3.24.6 per 1,000), while theestimated prevalence o ASD with borderline intellectual
ability increased 117% (1.42.9 per 1,000), and the estimatedprevalence o ASD with average or above-average intellectuaability increased 93% (2.44.7 per 1,000).
When data rom all 13 sites participating in the 2002 and2008 surveillance years were combined, the proportion ochildren meeting the ASD surveillance case deinition who
had a comprehensive evaluation completed by age 36 monthsincreased over time, rom 32% or children born in 1994 to41% or children born in 2000 (i.e., children identiied in the2002 and 2008 surveillance years, respectively). During thistime, the proportion with an earliest known ASD diagnosisby age 36 months increased rom 12% or children born in1994 to 18% or children born in 2000.
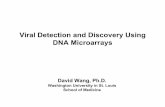
FIGURE 3. Proportion of children identified with autism spectrum disorders (ASDs) by previous ASD classification on record as of age 8 yearsby state and year Autism and Developmental Disabilities Monitoring Network, United States, 14 sites, 2002,* 2006, and 2008
* N = 2,682 N = 2,757 N = 3,820
Percentage
50
55
60
65
70
75
80
85
90
95
100
02 06 08
AL AR AZ CO FL GA MD MO NC NJ PA SC UT WI
Previous ASD classication on record Suspicion of ASD noted No mention of ASD
02 08 02 06 08 02 06 08 02 06 08 02 06 08 02 06 08 02 06 08 02 08 02 06 08 02 06 08 02 06 0802 0806 08
-
8/2/2019 CDC Autism Study, March 2012
17/24
Surveillance Summaries
MMWR / March 30, 2012 / Vol. 61 / No. 3 15
Previously Documented ASDClassification: 2002, 2006, and 2008
The proportion o children meeting the ASD surveillancecase deinition who had a documented ASD classiicationin their records increased over time in seven o the 10 sites
completing all 3 surveillance years (Figure 3). For these 10ADDM sites combined, and restricting analysis to residentso the core surveillance areas that were common across all 3surveillance years, the proportion o surveillance cases with aprevious ASD classiication increased rom 72% in 2002 to77% in 2006 and to 79% in 2008.
DiscussionThe results provided in this report suggest that three topics
require urther exploration. First, estimated ASD prevalencecontinues to rise in most ADDM Network sites, indicatingan expanded need or programs serving children with ASDs.Second, a wide range o ASD prevalence was estimatedacross ADDM Network sites. Finally, estimated prevalencevaried widely by sex and race/ethnicity. To address such widevariation in ASD prevalence estimates (over time, acrosssites, and between sex and racial/ethnic groups) a numbero actors should be considered, primarily those ocusing onascertainment.
Temporal Changes in ASD PrevalenceWhile ASD prevalence estimates in the overall population
increased 23% or the 2-year period 20062008, and 78%during the 6-year period 20022008, the largest increases overtime were noted among Hispanic children and non-Hispanicblack children and among children without co-occurringintellectual disability. Better identiication in these speciicgroups explains only part o the overall increase, however,as estimated ASD prevalence increased in all groups whendata were stratiied by sex, race/ethnicity, and intellectualability. Previous reports rom the ADDM Network havediscussed underascertainment in racial and ethnic minoritygroups, and ADDM data have revealed ASD as one o the ewdevelopmental disabilities or which a positive correlation existsbetween socioeconomic status (SES) and identiied prevalenceo the condition (18). Further investigation is needed to betterunderstand potential ascertainment bias and disparities byrace/ethnicity and SES in access to diagnostic and treatmentservices or children with ASDs. I these gaps are decreasing,continued ASD prevalence increases might be expected overalland among speciic groups.
Children meeting the surveillance case deinition or ASD arenot required to have an existing ASD diagnosis or classiicationon record, but examiners diagnostic impressions do actorprominently in ascertainment methods and can inluencetemporal changes in ASD prevalence. Approximately 79% oall children meeting the surveillance case deinition in 2008
had a documented ASD classiication in their records, thehighest proportion ever reported or any ADDM Networksurveillance year. This oers evidence that providers inthese communities are increasingly more likely to documentthe presence o ASDs and acilitate access to services thatare speciic to the needs o children with ASDs. Also, theproportion o children with an earliest known ASD diagnosisby age 36 months increased over time. However, 21% o thechildren meeting the ASD surveillance case deinition do nohave any documented ASD classiication in their records, andthose who do are not being identiied early enough. In areaswhere autism-speciic interventions are available to children who qualiy on the basis o diagnosis, early screening anddiagnosis improves access to services during the most criticaldevelopmental periods. Limitations in the data and reportindings in terms o the earliest known diagnosis suggestthat the diagnostic inormation obtained rom evaluationrecords might not capture the exact age o each childs earliestdiagnosis. Given this and the instability o diagnostic subtypesover time, the median age o earliest known diagnosis or anyspeciic ASD should be interpreted cautiously. Nonethelessthe data indicate that many children with ASDs do not receivea diagnosis until they reach preschool or kindergarten age
missing opportunities or earlier therapies that potentiallycould improve communication and socialization while theseskills are developing. Because the data or this report werecollected on children born during 19942000, uture reportsrom the ADDM Network might demonstrate greater progressin early identiication stemming rom policy changes initiatedin recent years, including state-based insurance reorm andthe expansion o services or children with ASDs occurringin many states.
Variation in ASD Prevalence by Site, Sex,and Race/Ethnicity
For the 2008 surveillance year, a wider range o site-speciicASD prevalence estimates was identiied than in previouADDM Network surveillance years. Variation in estimated ASD prevalence was associated primarily with sites havingaccess to education records and also appeared to be associated with improved identiication among children withouintellectual disability. On average, estimated ASD prevalencewas signiicantly higher in ADDM sites that had access to
-
8/2/2019 CDC Autism Study, March 2012
18/24
Surveillance Summaries
16 MMWR / March 30, 2012 / Vol. 61 / No. 3
education sources compared with sites thatrelied solely on health sources to identiy cases,and ASD prevalence in the one Coloradocounty where project sta had access to bothhealth and education sources was almosttwice as high as in the six counties where only
health records were accessed. Such dierencescannot be attributed solely to source access,as other actors (e.g., demographic dierencesand service availability) also might haveinluenced these indings. In general, however,having access to education records continuesto be associated with higher identiied ASDprevalence when comparing across or withinmost ADDM Network sites.
The two sites with the highest ASDprevalence estimates in 2008 (Utah andNew Jersey) identiied higher proportions ochildren with IQ >70 compared with any siteparticipating in 2008 or previous ADDMNetwork surveillance years. Among the sevensites reporting data on intellectual ability, ASDprevalence was typically higher in sites havinga greater percentage o children with IQ >70(Figure 4). Because testing practices and otheractors that inluence these indings mightvary across sites, urther analysis is needed tounderstand this pattern in 2008 and earlierADDM surveillance years.
The availability o childrens recordsalso was identiied as a potential source ounderascertainment and variation in ASDprevalence estimates among sites. When asensitivity evaluation algorithm was appliedto counts o records that could not be locatedor review, estimated ASD prevalence in some sites mighthave been much higher i all childrens records had beenavailable or review. In other sites, however, the impact omissing records was considered negligible, so record availabilitylikely accounted or at least some o the variation across sites.Because nearly hal o the missing records in Florida were
rom a program serving children aged birth to 3 years, 26% isconsidered a liberal estimate, and the actual yield rom theseearly childhood records might have been smaller. In Alabama,the vast majority o missing records was rom acilities that werein the process o converting rom paper to electronic records orhad storage limitations during the period o data collection, sothe large number o missing records might have had a one-timeeect on the 2008 surveillance data or this site.
The estimated prevalence o ASDs was signiicantly higheramong boys (one in 54) than among girls (one in 252), witha male-to-emale RR o 4.6 or all sites combined. Althoughthe ADDM site with the highest ASD prevalence had thelowest male-to-emale ratio while the site with the lowest ASDprevalence had the highest male-to-emale ratio, improvedidentiication among emales compared with males did not
appear to be associated with between-site dierences inoverall ASD prevalence. Much wider variation existed in sitesprevalence estimates or males than or emales.
ASD prevalence estimates also varied widely by race/ethnicityacross and within most sites, with only one site (New Jersey)identiying approximately the same ASD prevalence amongnon-Hispanic white, non-Hispanic black, and Hispanicchildren. Most ADDM Network sites continue to identiy
FIGURE 4. Variation in estimated prevalence (per 1,000 population) of autism spectrumdisorders (ASDs) among children aged 8 years, by Intelligence Quotient (IQ) score Autismand Developmental Disabilities Monitoring Network, seven sites,* United States, 2008
* Includes sites having information on IQ score available for at least 70% of children who met the ASDcase definition.
Total population aged 8 years.
Prev
alence
15
10
5
20
25
0
NewJersey
ArizonaNorthCarolina
GeorgiaSouthCarolina
UtahArkansas
N = 7,082N = 32,601N = 36,913N = 50,427 N = 2,123N = 23,769N* = 4,940
IQ >70IQ unknown
IQ 70
-
8/2/2019 CDC Autism Study, March 2012
19/24
Surveillance Summaries
MMWR / March 30, 2012 / Vol. 61 / No. 3 17
higher ASD prevalence estimates among non-Hispanic whitechildren compared with other racial/ethnic groups, and with noclearly documented dierences between these groups in knownrisk actors or ASDs, disparities in prevalence estimates suggestunderascertainment among Hispanic and non-Hispanic blackchildren. However, these disparities in identiication appear
to be diminishing in many sites, and urther work is neededto evaluate how identiication among certain racial/ethnicpopulations is associated with dierences in ASD prevalencebetween sites and over time.
LimitationsThe data provided in this report are subject to at least two
limitations. First, increases in awareness and access to serviceshave improved the ability o the ADDM Network to identiychildren with ASD over time, and this likely contributes to theincrease in estimated prevalence. The proportion o the increase
that is attributable to such changes in case ascertainment orattributable to a true increase in prevalence o ASD symptomscannot be determined. Ongoing monitoring is an importanttool to learn why more children are being identiied with ASDsand can provide important clues in the search or risk actors.
Second, the surveillance areas were not selected to berepresentative o the United States as a whole, nor were theyselected to be representative o the states in which they arelocated. Limitations regarding population size, surveillanceareas, and the consistency o these attributes were considered when analysts evaluated comparisons across multiple timepoints. Although the two ADDM sites reporting the highest
prevalence estimates in 2008 also reported among the highestprevalence estimates in 2002, the most recent results romNew Jersey and Utah are based on subregions o their 2002surveillance areas, with smaller populations compared withthose areas and with most other ADDM sites. The estimatedprevalence in these subregions possibly was inluenced byactors unique to these smaller communities and might notrelect the number and characteristics o children with ASDsin the larger areas covered by these ADDM sites in 2002.Similarly, ive other ADDM sites covered dierent surveillanceareas in 2008 compared with 2002 and/or 2006. Althoughcomparisons with earlier surveillance years were careullyrestricted to comparable surveillance areas, caution is advisedwhen interpreting results. For example, the addition o oneNorth Carolina county in 2008 resulted in a nearly 15%increase in the overall prevalence o ASDs in that site comparedwith their indings when this new county was excluded romthe prevalence estimate. Although this county was excludedrom calculations when the 2008 results were compared withthose rom earlier surveillance years, the impact o this single
county highlights the relative dierences across subregions oany given ADDM site.
Future Analyses to Address LimitationsFor dierences in ASD prevalence, across sites and within
subregions o each site to be understood better, urtherexploration o geographic variation in multiple contextuaand potential risk actors is needed. This involves in-depthanalysis o known characteristics in the population o childrenidentiied with ASDs (e.g., intellectual ability, SES, and birthcharacteristics), as well as geographic dierences aectingthe population as a whole. These results point to a need orgeospatial analyses o both physical and social environmentsincluding occupational and socioeconomic characteristics othe population, state policy dierences potentially aectingaccess to services (e.g., insurance reorm, per capita educationaspending, and immigration policy), and geographic dierence
in environmental exposures that potentially might aectneurodevelopment.
Another important consideration or uture analyses is thechanging clinical deinition o ASDs over time. Although theADDM methods have always been based on the DSM-IV-TR(1) diagnostic criteria, proposed changes to the deinitiono Autism Spectrum Disorder in the orthcoming revisedDiagnostic and Statistical Manual o Mental Disorders(DSM-5) might aect prevalence estimates and complicatetemporal comparisons (19). The proposed revised diagnosticcriteria or Autism Spectrum Disorder would combine threesubgroups currently under the DSM-IV-TR heading o
Pervasive Developmental Disorders into one category andmight require a child to display more pronounced symptomto receive a diagnosis. Because the ADDM methods includeinormation on a broad range o symptoms, the ADDMNetwork is well-positioned to adopt the proposed DSM-5deinition into its ongoing study and, at the same time, obtaincomparison estimates based on the DSM-IV-TR deinitionCDC and ADDM Network investigators are exploring thedata to understand how the proposed changes might aectthe current prevalence estimates and will continue to prioritizethese comparisons so as to understand trends better over timeThis inormation is crucial to increasing knowledge o thiscomplex spectrum o behaviors.
Ongoing EffortsAlthough multiple actors inluence the identiication o
children with ASDs and dierences in prevalence estimateacross sites, the data provided in this report indicate the need orurther exploration o possible associations between overall ASDprevalence and improved identiication among children withou
-
8/2/2019 CDC Autism Study, March 2012
20/24
Surveillance Summaries
18 MMWR / March 30, 2012 / Vol. 61 / No. 3
intellectual disability, children in all racial/ethnic populations,and both males and emales, including potential interactionsbetween these actors. ADDM Network investigators continueto explore a broad variety o potential risk and ascertainmentactors to understand dierences in ASD prevalence estimatesbetween sites and over time.
With 5 surveillance years completed to date, and datacollection underway or the 2010 surveillance year, the ADDMNetwork has compiled extensive data on the prevalence andcharacteristics o ASDs and other developmental disabilities.These data cover large populations or obtaining prevalenceestimates and provide depth and breadth o inormationon topics not captured in national health surveys. The ADDM record-review methodology enables reporting odata on intellectual ability, speciic ASD subtype diagnosisand educational classiication, within- and between-statecomparisons, and linkage to other datasets or explorationo potential risk actors such as birth characteristics andsocioeconomic disparities as well as examination o healthservices utilization. Currently, the ADDM Network iscollecting inormation on children who were aged 8 years in2010 and or the irst time also is monitoring ASDs amongchildren aged 4 years. In 2012, ADDM sites will begincollecting inormation or the 2012 surveillance year.
ConclusionASDs continue to be an important public health concern.
The indings provided in this report conirm that prevalence
estimates o ASD continue to increase in the majority oADDM Network communities, and ongoing public healthsurveillance is needed to quantiy and understand thesechanges over time. Further work is needed to evaluate multipleactors aecting ASD prevalence over time. ADDM Networkinvestigators continue to explore these actors in multiple ways,with a ocus on understanding disparities in the identiicationo ASDs among certain subgroups and evaluating temporalchanges in the prevalence o ASDs. CDC also is engagedwith other ederal, state, and private partners in a coordinatedresponse to identiy risk actors or ASDs and meet the needs opersons with ASDs and their amilies. Additional inormation
is available at http://www.cdc.gov/autism .
Acknowledgments
Data in this report were provided by ADDM Network SurveillanceYear 2008 investigators: Martha Wingate, DrPH, Beverly Mulvihill,PhD, University o Alabama at Birmingham; Russell S. Kirby, PhD,
University o South Florida, Tampa; Sydney Pettygrove, PhD, ChriCunni, MD, F. John Meaney, PhD, University o Arizona, TucsonEldon Schulz, MD, University o Arkansas or Medical SciencesLittle Rock; Lisa Miller, MD, Colorado Department o Public Healthand Environment, Denver; Cordelia Robinson, PhD, University oColorado at Denver and Health Sciences Center; Gina Quintana
Colorado Department o Education, Denver; Marygrace Yale KaiserPhD, University o Miami, Coral Gables, Florida; Li-Ching LeePhD, Johns Hopkins University, Rebecca Landa, PhD, KennedyKrieger Institute, Baltimore, Maryland; Craig Newschaer, PhDDrexel University, Philadelphia, Pennsylvania; John ConstantinoMD, Robert Fitzgerald, MPH, Washington University in St. LouisMissouri; Walter Zahorodny, PhD, University o Medicine andDentistry o New Jersey, Newark; Julie Daniels, PhD, University oNorth Carolina, Chapel Hill; Ellen Giarelli, EdD, Drexel UniversityPhiladelphia, Pennsylvania; Jennier Pinto-Martin, PhD, Universityo Pennsylvania; Susan E. Levy, MD, The Childrens Hospital oPhiladelphia, Pennsylvania; Joyce Nicholas, PhD, Jane CharlesMD, Medical University o South Carolina, Charleston; Judith
Zimmerman, PhD, University o Utah, Salt Lake City; MatthewJ. Maenner, PhD, Maureen Durkin, PhD, DrPH, University oWisconsin, Madison; Catherine Rice, PhD, Jon Baio, EdS, Kim VanNaarden Braun, PhD, Keydra Phillips, MPH, Nancy DoernbergMarshalyn Yeargin-Allsopp, MD, Division o Birth Deects andDevelopmental Disabilities, National Center on Birth Deects andDevelopmental Disabilities, CDC.
Data collection was coordinated at each site by ADDM Networkproject coordinators: Anita Washington, MPH, Yasmeen WilliamsMPH, Kwin Jolly, MS, Research Triangle Institute, Atlanta, GeorgiaNeva Garner, University o Alabama at Birmingham; Kristen ClancyMancilla, University o Arizona, Tucson; Allison Hudson, Universityo Arkansas or Medical Sciences, Little Rock; Andria Ratchord
MSPH, Colorado Department o Public Health and EnvironmentDenver; Yolanda Castillo, MBA, Colorado Department o EducationDenver; Claudia Rojas, Yanin Hernandez, University o Miami, CoraGables, Florida; Kara Humes, Rebecca Harrington, MPH, JohnsHopkins University, Baltimore, Maryland; Rob Fitzgerald, MPH
Washington University in St. Louis, Missouri; Josephine ShenoudaMS, University o Medicine and Dentistry o New Jersey, NewarkPaula Bell, University o North Carolina, Chapel Hill; Rachel ReisUniversity o Pennsylvania, Philadelphia; Lydia King, PhD, MedicaUniversity o South Carolina, Charleston; Amanda Bakian, PhD
Amy Henderson, University o Utah, Salt Lake City; Carrie ArnesonMS, University o Wisconsin, Madison; Susan Graham SchwartzMSPH, CDC. Additional assistance was provided by project staincluding data abstractors, clinician reviewers, epidemiologists, anddata management/programming support. Ongoing ADDM Networksupport was provided by Joanne Wojcik, Victoria Wright, NationaCenter on Birth Deects and Developmental Disabilities, CDC, RitaLance, Northrop Grumman, contractor to CDC.
http://www.cdc.gov/autismhttp://www.cdc.gov/autism -
8/2/2019 CDC Autism Study, March 2012
21/24
Surveillance Summaries
MMWR / March 30, 2012 / Vol. 61 / No. 3 19
References
1. American Psychiatric Association. Diagnostic and statistical manual omental disorders. 4th ed. Washington, DC: American Psychiatric
Association; 2000.2. Rice CE, Baio J, Van Naarden Braun K, Doernberg N, Meaney F J,
Kirby RS, or the ADDM Network. A public health collaboration orthe surveillance o autism spectrum disorders. Paediatr Perinat Epidemiol
2007;21:17990.3. CDC. Prevalence o autism spectrum disordersAutism and
Developmental Disabilities Monitoring Network, six sites, United States,2000. MMWR 2007;56(No. SS-1):111.
4. CDC. Prevalence o autism spectrum disordersAutism andDevelopmental Disabilities Monitoring Network, 14 sites, United States,2002. MMWR 2007;56(No. SS-1):1228.
5. CDC. Prevalence o autism spectrum disordersAutism andDevelopmental Disabilities Monitoring Network, United States, 2006.MMWR 2009;58(No. SS-10).
6. Kogan MD, Blumberg SJ, Schieve LA, et al. Prevalence o parent-reported diagnosis o autism spectrum disorder among children in theU.S., 2007. Pediatrics 2009;124:1395403.
7. Boyle CA, Boulet S, Schieve LA, et al. Trends in the prevalence odevelopmental disabilities in U.S. children, 19972008. Pediatrics
2011;127:103442.8. Baron-Cohen S, Scott FJ, Allison C, et al. Prevalence o autism-spectrumconditions: UK school-based population study. Br J Psychiatry2009;194:5009.
9. Fombonne E. Estimated prevalence o autism spectrum conditions inCambridgeshire is over 1%. Evid Based Ment Health 2010;13:32.
10. Kim YS, Leventhal BL, Koh YJ, F, et al. Prevalence o autism spectrumdisorders in a total population sample. Am J Psychiatry 2011;168:90412.
11. HR 4365, 106th Cong, 19992000. Childrens Health Act o 2000Available at http://www.govtrack.us/congress/bill.xpd?bill=h106-4365Accessed March 14, 2012.
12. Yeargin-Allsopp M, Rice C, Karapurkar T, Doernberg N, Boyle CMurphy C. Prevalence o autism in a US metropolitan area. JAMA2003;289:4955.
13. Van Naarden Braun K, Pettygrove S, Daniels J, et al. Evaluation o amethodology or a collaborative multiple source surveillance networkor autism spectrum disordersAutism and Developmental DisabilitiesMonitoring Network, 14 sites, United States, 2002. MMWR 2007;56(No. SS-1):2940.
14. US Department o Health and Human Services. Code o FederaRegulations. Title 45. Public Welare CFR 46. Available at http://www.hhsgov/ohrp/humansubjects/guidance/45cr46.html. Accessed March 14, 2012
15. CDC. Estimates o the July 1, 2000July 1, 2009, United States residenpopulation rom the vintage 2009 postcensal series by year, county, agesex, race, and Hispanic origin. Available at http://www.cdc.gov/nchs/nvss/bridged_race/data_documentation.htm#vintage2009 . AccessedMarch 14, 2012.
16. US Department o Education. Common core o data. Available at http:/nces.ed.gov/ccd/bat. Accessed March 14, 2012.
17. Lazarus C, Autry A, Baio J, Avchen RN, Van Naarden Braun K. Impacto postcensal versus intercensal population estimates on prevalence o
selected developmental disabilitiesmetropolitan Atlanta, Georgia19911996. Am J Ment Retard 2007;112:4626.
18. Durkin MS, Maenner MJ, Meaney FJ, et al. Socioeconomic inequalityin the prevalence o autism spectrum disorder: evidence rom a U.Scross-sectional study. PLoS One 2010;5:e11551.
19. American Psychiatric Association. DSM-5 development: autismspectrum disorder. Available at http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=94 . Accessed March 14, 2012.
http://www.govtrack.us/congress/bill.xpd?bill=h106-4365http://www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.htmlhttp://www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.htmlhttp://www.cdc.gov/nchs/nvss/bridged_race/data_documentation.htm#vintage2009http://www.cdc.gov/nchs/nvss/bridged_race/data_documentation.htm#vintage2009http://nces.ed.gov/ccd/bathttp://nces.ed.gov/ccd/bathttp://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=94http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=94http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=94http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=94http://nces.ed.gov/ccd/bathttp://nces.ed.gov/ccd/bathttp://www.cdc.gov/nchs/nvss/bridged_race/data_documentation.htm#vintage2009http://www.cdc.gov/nchs/nvss/bridged_race/data_documentation.htm#vintage2009http://www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.htmlhttp://www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.htmlhttp://www.govtrack.us/congress/bill.xpd?bill=h106-4365 -
8/2/2019 CDC Autism Study, March 2012
22/24
-
8/2/2019 CDC Autism Study, March 2012
23/24
-
8/2/2019 CDC Autism Study, March 2012
24/24
DEPARTMENTOFHEALTHANDHUMA
NSERVICES
Ce
ntersorDiseaseControlandPreve
ntion(CDC)
Atlanta,GA30333
OfcialBusiness
Pe
naltyorPrivateUse$300
Re
turnServiceRequested
U.S. Government Printing Ofce: 2012-523-218/73183 Region IV ISSN: 1546-0738
TheMorbidity and Mortality Weekly Report (MMWR) Series is prepared by the Centers or Disease Control and Prevention (CDC) and is available ree ocharge in electronic ormat. To receive an electronic copy each week, visit MMWRs ree subscription page at http://www.cdc.gov/mmwr/mmwrsubscribe.html.Paper copy subscriptions are available through the Superintendent o Documents, U.S. Government Printing Oice, Washington, DC 20402;telephone 202-512-1800.
Address all inquiries about theMMWRSeries, including material to be considered or publication, to Editor,MMWRSeries, Mailstop E-90, CDC, 1600Cliton Rd., N.E., Atlanta, GA 30333 or to [email protected].
All material in theMMWRSeries is in the public domain and may be used and reprinted without permission; citation as to source, however, is appreciated.
Use o trade names and commercial sources is or identiication only and does not imply endorsement by the U.S. Department o Health and Human Services.
Reerences to non-CDC sites on the Internet are provided as a service toMMWRreaders and do not constitute or imply endorsement o these organizationsor their programs by CDC or the U.S. Department o Health and Human Services. CDC is not responsible or the content o these sites. URL addresseslisted inMMWRwere current as o the date o publication.
Surveillance Summaries
http://www.cdc.gov/mmwr/mmwrsubscribe.htmlhttp://www.cdc.gov/mmwr/mmwrsubscribe.htmlhttp://www.cdc.gov/mmwr/mmwrsubscribe.htmlmailto:[email protected]:[email protected]://www.cdc.gov/mmwr/mmwrsubscribe.htmlhttp://www.cdc.gov/mmwr/mmwrsubscribe.html