CCEB Whole Body Vibration as an Anabolic Bone Therapy in Children Mary B. Leonard, MD, MSCE The...
40
CCEB CCEB Whole Body Vibration as an Anabolic Whole Body Vibration as an Anabolic Bone Therapy in Children Bone Therapy in Children Mary B. Leonard, MD, MSCE Mary B. Leonard, MD, MSCE The Children’s Hospital of Philadelphia The Children’s Hospital of Philadelphia Center for Clinical Epidemiology and Center for Clinical Epidemiology and Biostatistics Biostatistics
-
Upload
silvia-davidson -
Category
Documents
-
view
215 -
download
0
Transcript of CCEB Whole Body Vibration as an Anabolic Bone Therapy in Children Mary B. Leonard, MD, MSCE The...
CCEBCCEB
Whole Body Vibration as an Anabolic Whole Body Vibration as an Anabolic Bone Therapy in ChildrenBone Therapy in Children
Mary B. Leonard, MD, MSCEMary B. Leonard, MD, MSCEThe Children’s Hospital of PhiladelphiaThe Children’s Hospital of PhiladelphiaCenter for Clinical Epidemiology and Center for Clinical Epidemiology and
BiostatisticsBiostatistics
2000 NIH Osteoporosis 2000 NIH Osteoporosis Consensus Conference StatementConsensus Conference Statement
• Peak Bone Mass is a critical determinant of Peak Bone Mass is a critical determinant of life-long skeletal healthlife-long skeletal health
• Maximizing peak bone mass is a priority Maximizing peak bone mass is a priority
• The NIH called for research strategies to The NIH called for research strategies to identify and intervene in disorders that identify and intervene in disorders that compromise attainment of peak bone mass compromise attainment of peak bone mass in children with chronic diseasein children with chronic disease
– Especially corticosteroid therapyEspecially corticosteroid therapy

Rethinking OsteoporosisRethinking Osteoporosis
Bone strength is a function of bone Bone strength is a function of bone density (g/cmdensity (g/cm33) and bone quality) and bone quality
Bone quality refers to geometry, Bone quality refers to geometry, micro-architecture, turnover, micro-micro-architecture, turnover, micro-damage repair, and mineralizationdamage repair, and mineralization
Osteoporosis Prevention, Diagnosis & Therapy Osteoporosis Prevention, Diagnosis & Therapy NIH Consensus Conference 2000NIH Consensus Conference 2000
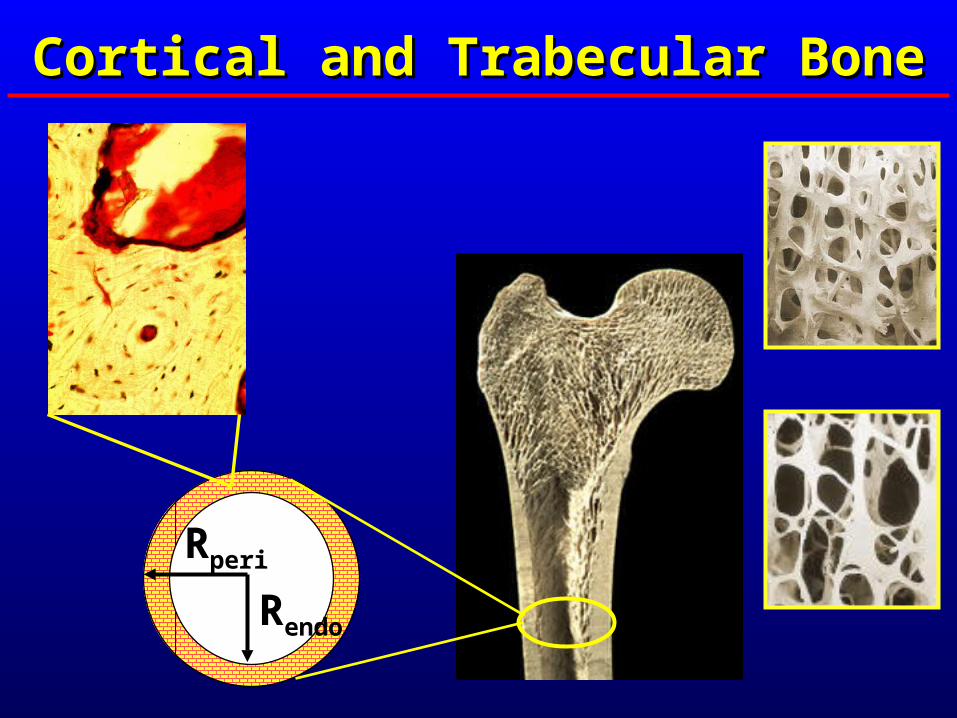
Cortical and Trabecular BoneCortical and Trabecular Bone
Rperi
Rendo
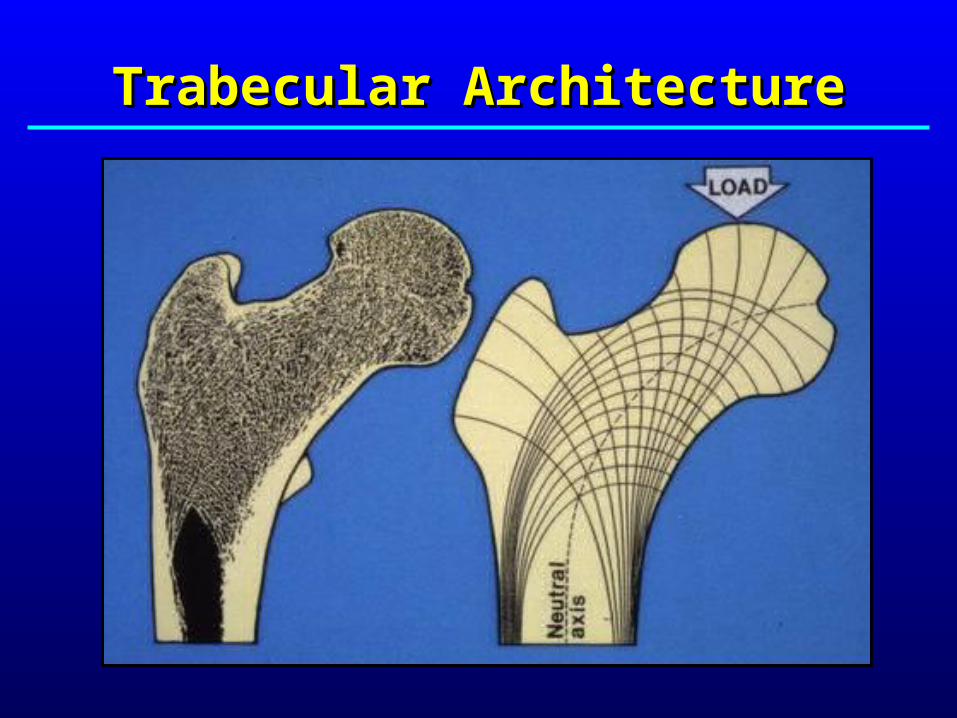
Trabecular ArchitectureTrabecular Architecture
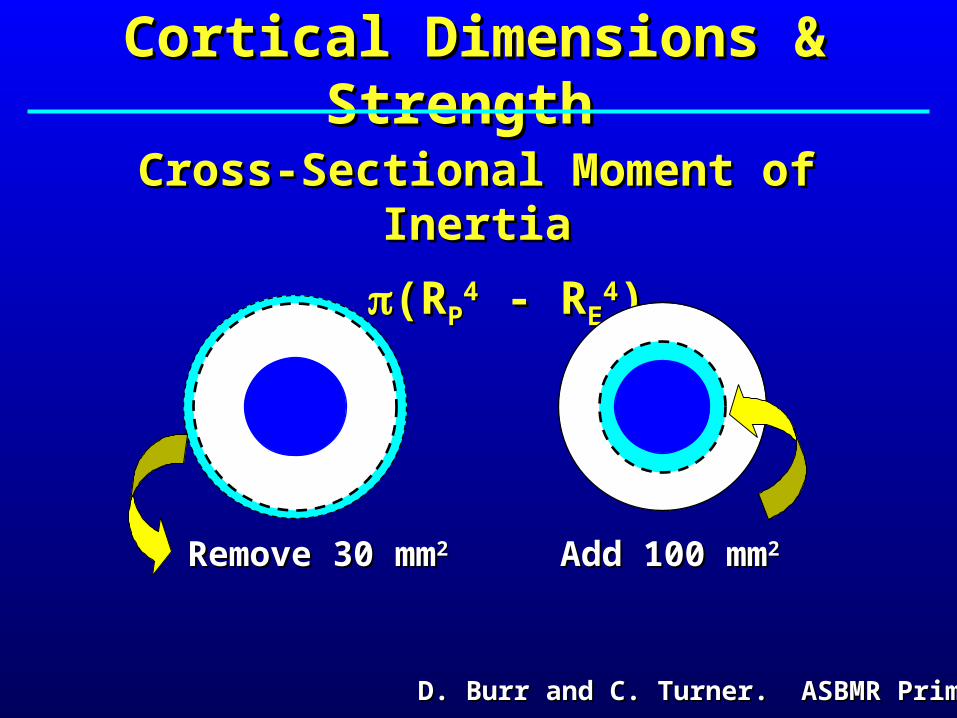
Cortical Dimensions & StrengthCortical Dimensions & Strength
Cross-Sectional Moment of InertiaCross-Sectional Moment of Inertia
(R(RPP44 - R - REE
44))
Remove 30 mmRemove 30 mm22 Add 100 mmAdd 100 mm22
D. Burr and C. Turner. ASBMR PrimerD. Burr and C. Turner. ASBMR Primer

Skeletal Skeletal RemodelingRemodeling
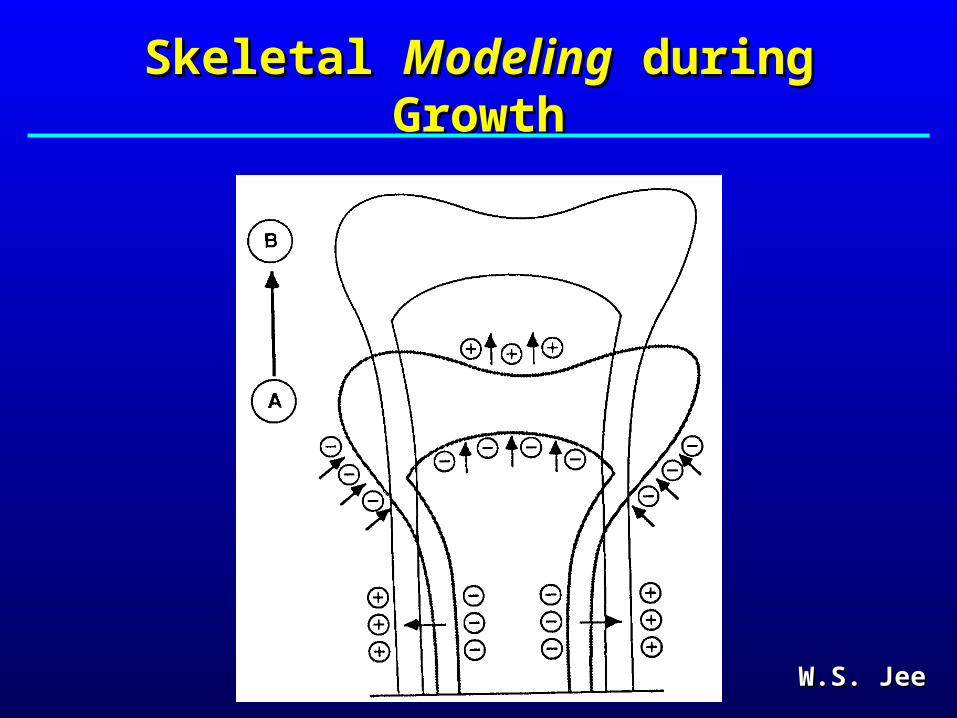
Skeletal Skeletal ModelingModeling during Growth during Growth
W.S. JeeW.S. Jee

Changes in Cortical & Trabecular Changes in Cortical & Trabecular Bone with GrowthBone with Growth
• Trabecular Bone Volume FractionTrabecular Bone Volume Fraction– Increases during Tanner stages III – VIncreases during Tanner stages III – V
– Increases are greater in blacks than whites Increases are greater in blacks than whites
trabecular thickness and material densitytrabecular thickness and material density
• Cortical Density and DimensionsCortical Density and Dimensions– Density increases with age, F > MDensity increases with age, F > M
– During puberty boys develop greater periosteal radius During puberty boys develop greater periosteal radius and girls develop relatively smaller endosteal radiusand girls develop relatively smaller endosteal radius
– CSMI greater in blacks than whitesCSMI greater in blacks than whites
Gilsanz V, et al. NEJM 1991, J Clin Endo Metab 1997, J Clin Endo Metab 1998.Gilsanz V, et al. NEJM 1991, J Clin Endo Metab 1997, J Clin Endo Metab 1998.Seeman E. Lancet 2002. Rauch and Schoenau JBMR 2001.Seeman E. Lancet 2002. Rauch and Schoenau JBMR 2001.
Threats to Bone Health in Children Threats to Bone Health in Children with Crohn Diseaseswith Crohn Diseases
• Decreased muscle forces / loadingDecreased muscle forces / loading• MalnutritionMalnutrition
– Calcium, Vitamin D, Vitamin K, ZincCalcium, Vitamin D, Vitamin K, Zinc
• Delayed puberty Delayed puberty • Alternations in GH / IGF axisAlternations in GH / IGF axis• MedicationsMedications
– GlucocorticoidsGlucocorticoids
• Inflammatory Cytokines Inflammatory Cytokines – IL-6, TNF-IL-6, TNF-
Glucocorticoid-Induced OsteoporosisGlucocorticoid-Induced Osteoporosis
• Glucocorticoids are widely used in pediatricsGlucocorticoids are widely used in pediatrics
• GlucocorticoidsGlucocorticoids
– Bone formation Bone formation
– Bone resorption then Bone resorption then ? ? Bone resorption Bone resorption
• Glucocorticoids are associated with increased Glucocorticoids are associated with increased fracture rates in children fracture rates in children
• Assessment of GC effects may be confounded by Assessment of GC effects may be confounded by – effects of the underlying diseaseeffects of the underlying disease
– altered growth, maturation and body compositionaltered growth, maturation and body composition
– limitations of DXA techniqueslimitations of DXA techniques

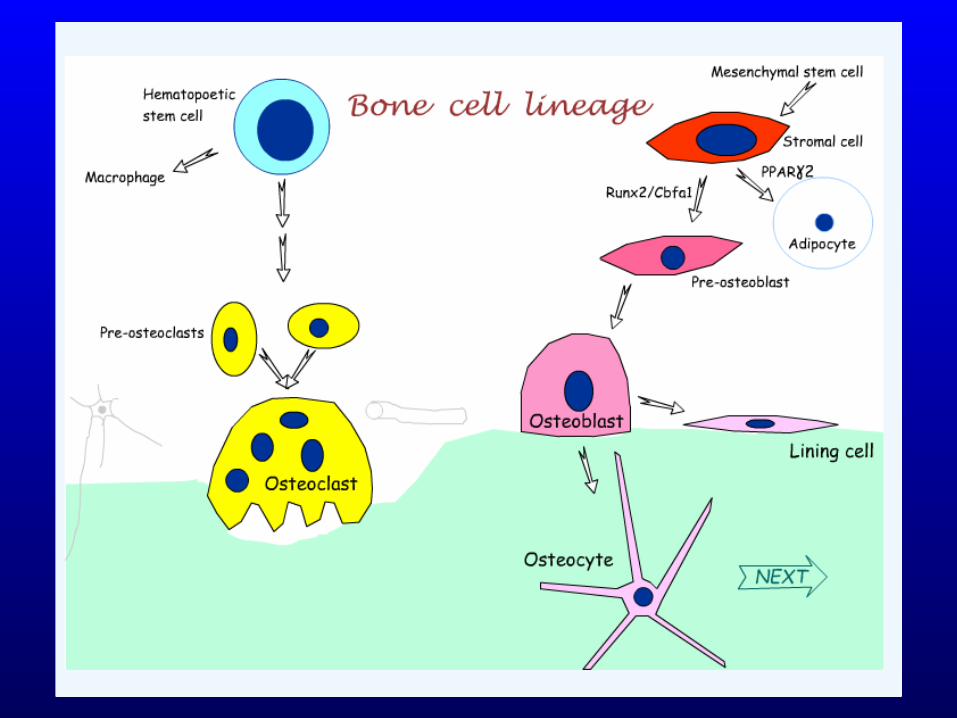
Glucocorticoid Effects
Decrease Bone Formation• Shift cellular differentiation of stem cells away from osteoblasts • Inhibit osteoblast production of bone matrix• Promote osteoblast apoptosis• Impair osteocytes
Increase Bone Resorption• Promote osteoclastogenesis by RANKL and OPG expression in osteoblasts
Glucocorticoid & Cytokine Effects Glucocorticoid & Cytokine Effects on Bone Cellson Bone Cells
TNF- Effects
Decrease Bone Formation• Shift cellular differentiation of stem cells away from osteoblasts• Inhibit collagen synthesis by osteoblasts• Promote osteoblast apoptosis• Impair osteocytes
Increase Bone Resorption• Promote osteoclastogenesis by RANKL and OPG expression in osteoblasts

Models of Glucocorticoid-Induced Models of Glucocorticoid-Induced Osteoporosis in ChildrenOsteoporosis in Children
Crohn DiseaseCrohn Disease
Steroid Dependent Nephrotic Steroid Dependent Nephrotic SyndromeSyndrome
Juvenile Idiopathic ArthritisJuvenile Idiopathic Arthritis
Renal TransplantRenal Transplant
Crohn DiseaseCrohn Disease
• Chronic inflammatory bowel diseaseChronic inflammatory bowel disease
• Insidious onsetInsidious onset
• May result in abscesses, granulomas or fistulas May result in abscesses, granulomas or fistulas
• 85% of children present with weight loss85% of children present with weight loss
• Growth failure and pubertal delay are commonGrowth failure and pubertal delay are common
• Treated with systemic glucocorticoids, steroid Treated with systemic glucocorticoids, steroid enemas, 5-ASA, methotrexate and other enemas, 5-ASA, methotrexate and other immunomodulatorsimmunomodulators
• Associated with fractures in children and adultsAssociated with fractures in children and adults

Crohn Disease & Bone Mineral ContentCrohn Disease & Bone Mineral Content
DXA Scans in 104 children DXA Scans in 104 children and young adults with CDand young adults with CD
Age: 4 – 25 yrAge: 4 – 25 yr
CD duration: 4.0 CD duration: 4.0 ++ 3.4 yr 3.4 yr
Median cumulative Median cumulative glucocorticoid exposure: glucocorticoid exposure: 10,300 mg10,300 mg
Burnham, et al. J Bone Miner Res 2004Burnham, et al. J Bone Miner Res 2004
4.5
5.0
5.5
6.0
6.5
7.0
7.5
8.0
8.5
4.5 4.6 4.7 4.8 4.9 5.0 5.1 5.2 5.3
Ln
(W
ho
le B
od
y B
MC
)
Control
Crohn
Ln (Height)

Standard Deviation Scores Standard Deviation Scores (Z-Scores)(Z-Scores)
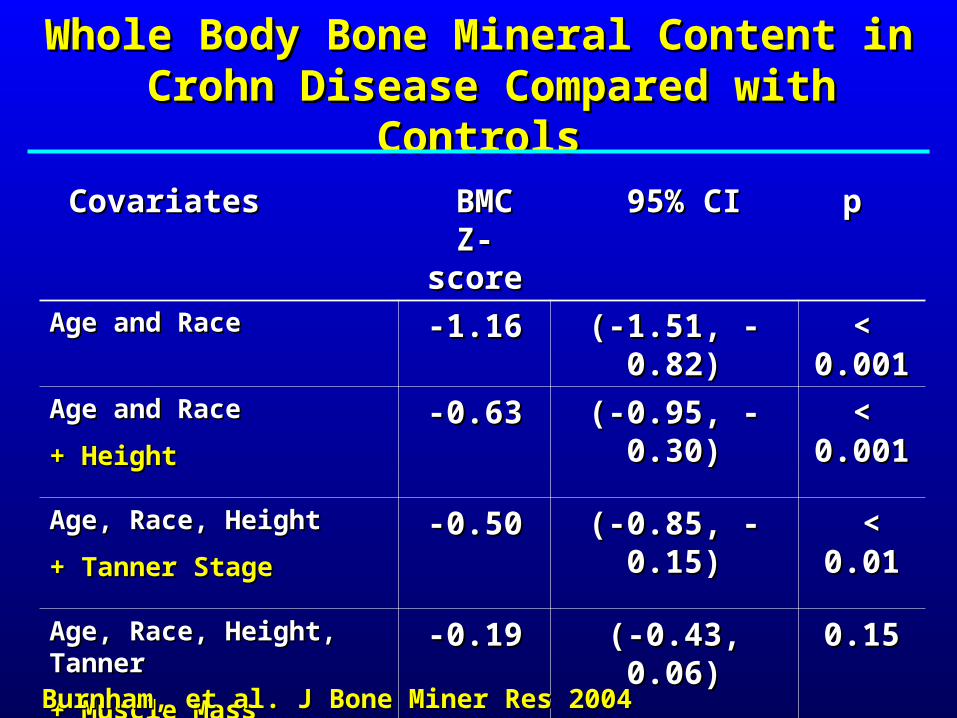
Whole Body Bone Mineral Content in Whole Body Bone Mineral Content in Crohn Disease Compared with ControlsCrohn Disease Compared with Controls
CovariatesCovariates BMC Z-BMC Z-scorescore
95% CI95% CI p p
Age and RaceAge and Race -1.16-1.16 (-1.51, - 0.82)(-1.51, - 0.82) < 0.001< 0.001
Age and RaceAge and Race
+ Height+ Height
-0.63-0.63 (-0.95, - 0.30)(-0.95, - 0.30) < 0.001< 0.001
Age, Race, HeightAge, Race, Height
+ Tanner Stage+ Tanner Stage
-0.50-0.50 (-0.85, - 0.15)(-0.85, - 0.15) < 0.01< 0.01
Age, Race, Height, TannerAge, Race, Height, Tanner
+ Muscle Mass+ Muscle Mass
-0.19-0.19 (-0.43, 0.06)(-0.43, 0.06) 0.150.15
Burnham, et al. J Bone Miner Res 2004 Burnham, et al. J Bone Miner Res 2004

Inflammatory CachexiaInflammatory Cachexia
• Lean mass deficits without fat mass deficitsLean mass deficits without fat mass deficits
• Muscle active cytokines (TNF-Muscle active cytokines (TNF-, IL-6, IL-1, IL-6, IL-1))
– inhibit myogenic differentiationinhibit myogenic differentiation
– stimulate muscle protein degradation stimulate muscle protein degradation
– induce myoblast apoptosisinduce myoblast apoptosis
• Note: Glucocorticoids increase myostatin, a Note: Glucocorticoids increase myostatin, a negative regulator of muscle massnegative regulator of muscle mass
Burnham, et al. AJCN 2005Burnham, et al. AJCN 2005Thayu, et al IBD 2007 Thayu, et al IBD 2007
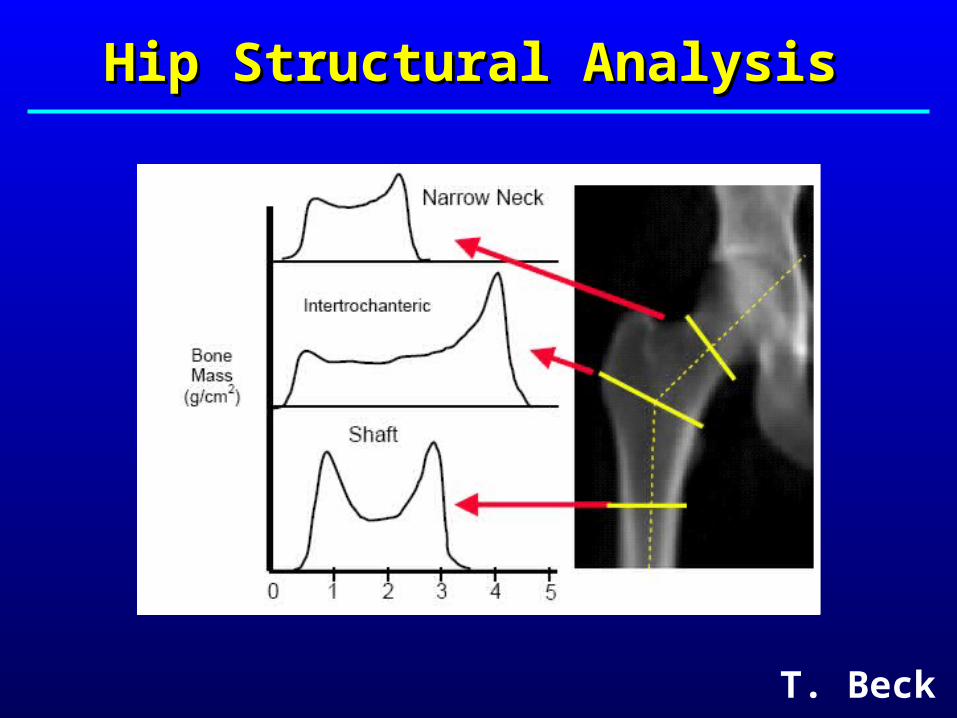
Hip Structural AnalysisHip Structural Analysis
T. Beck
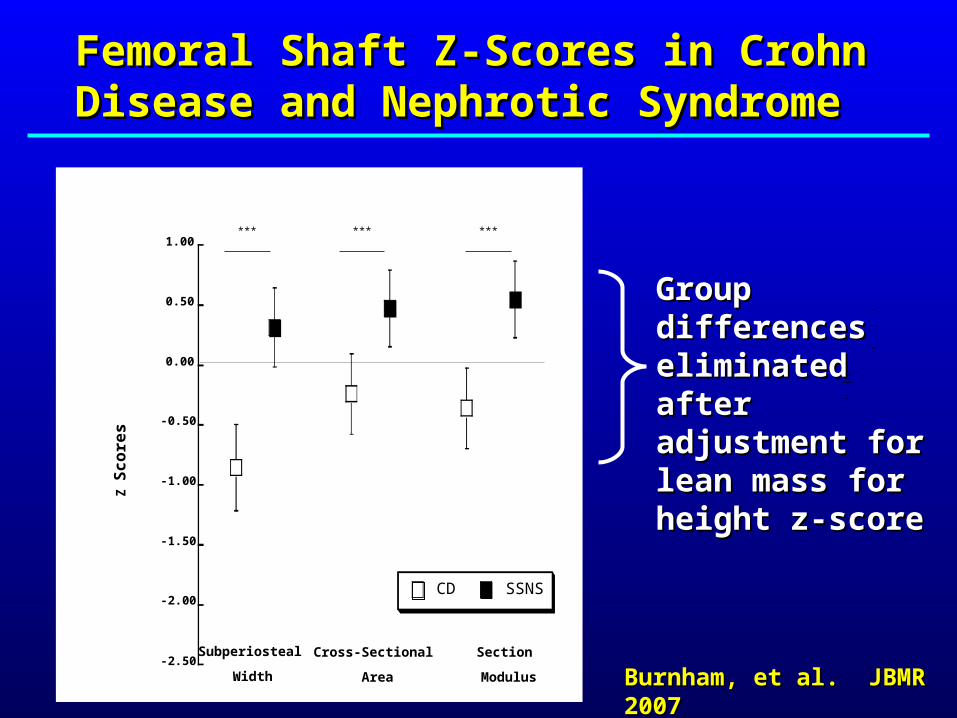
Femoral Shaft Z-Scores in Crohn Femoral Shaft Z-Scores in Crohn Disease and Nephrotic Syndrome Disease and Nephrotic Syndrome
Burnham, et al. JBMR 2007Burnham, et al. JBMR 2007
Z S
co
res
-2.50
-2.00
-1.50
-1.00
-0.50
0.00
0.50
1.00
CD SSNS
Subperiosteal
Width
Cross-Sectional
Area
Section
Modulus
*** ******
Group differences Group differences eliminated after eliminated after adjustment for adjustment for lean mass for lean mass for height z-scoreheight z-score
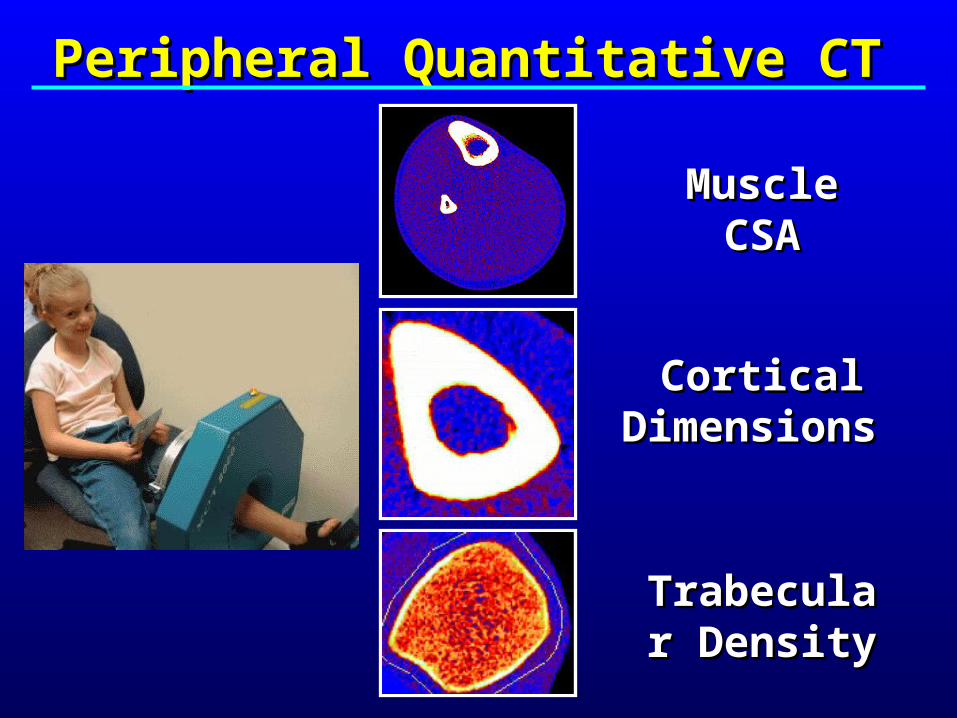
Peripheral Quantitative CTPeripheral Quantitative CT
Muscle Muscle CSACSA
Cortical Cortical Dimensions Dimensions
Trabecular Trabecular DensityDensity
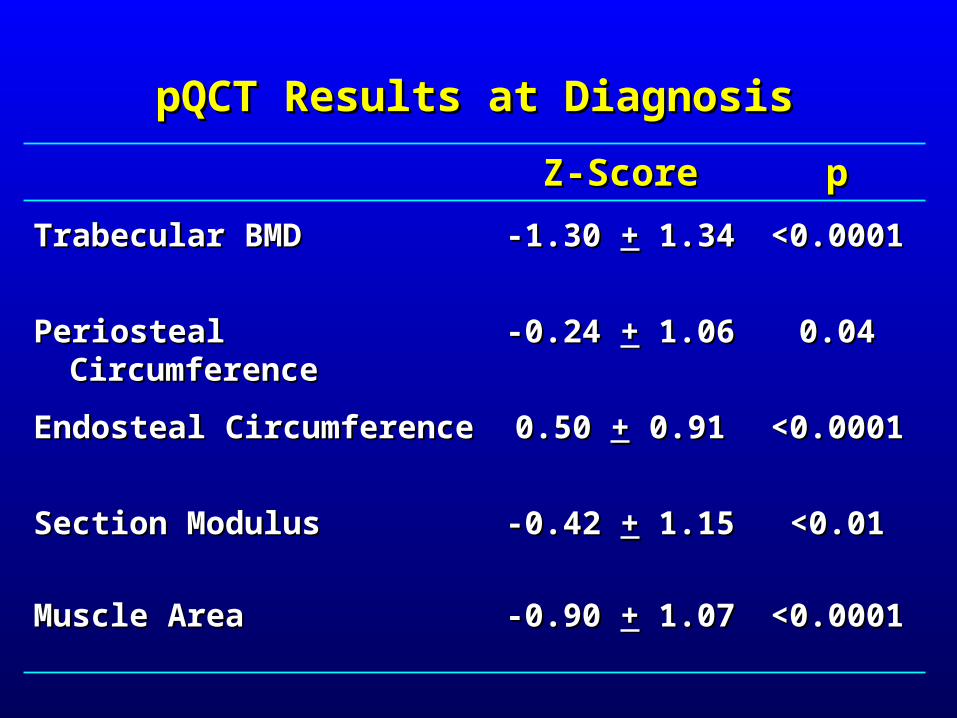
pQCT Results at DiagnosispQCT Results at Diagnosis
Z-ScoreZ-Score pp
Trabecular BMDTrabecular BMD -1.30-1.30 ++ 1.34 1.34 <0.0001<0.0001
Periosteal CircumferencePeriosteal Circumference -0.24-0.24 ++ 1.061.06 0.040.04
Endosteal CircumferenceEndosteal Circumference 0.50 0.50 ++ 0.91 0.91 <0.0001<0.0001
Section ModulusSection Modulus -0.42-0.42 ++ 1.151.15 <0.01<0.01
Muscle AreaMuscle Area -0.90-0.90 ++ 1.071.07 <0.0001<0.0001

Treatment OptionsTreatment Options
• Treat the underlying disease!Treat the underlying disease!
• Calcium and Vitamin D supplementsCalcium and Vitamin D supplements
• Osteoporosis medications?Osteoporosis medications?
– Antiresorptive agentsAntiresorptive agents
– Anabolic agentsAnabolic agents
• Weight bearing physical activityWeight bearing physical activity

High Impact Physical Activity in ChildhoodHigh Impact Physical Activity in ChildhoodIncreases Bone Density and DimensionsIncreases Bone Density and Dimensions

Control Triple Jumper
Midshaft
Distal
Area +30%
Density +67%
Athlete StudiesAthlete Studies
Rachel Wetzsteon Heinonen et al. Bone, 2003
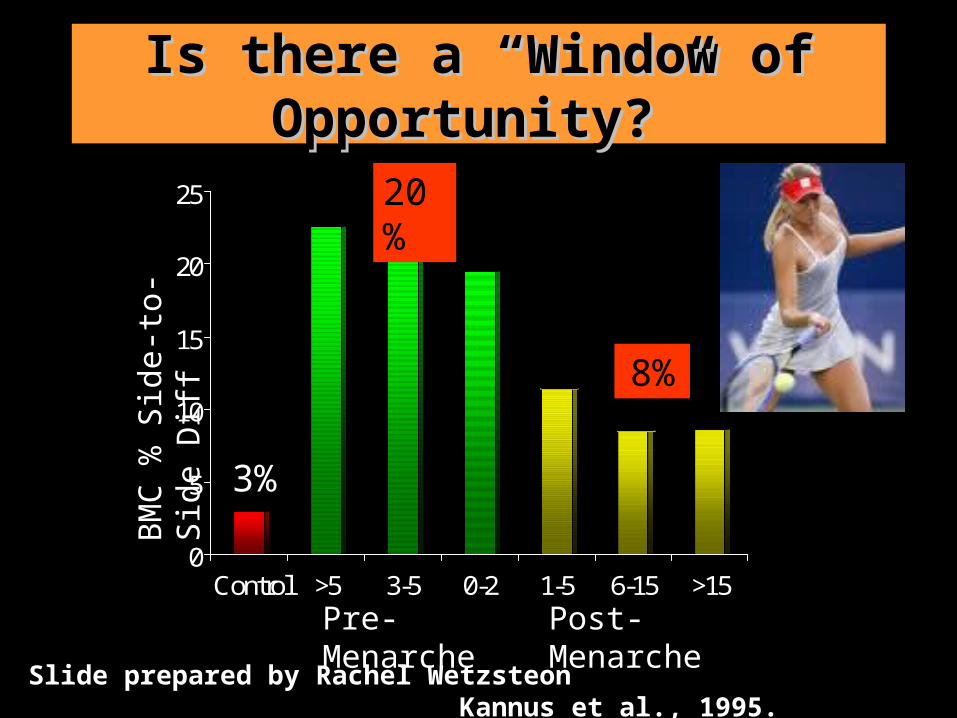
Is there a “Window of Is there a “Window of Opportunity?”Opportunity?”
0
5
10
15
20
25
Control >5 3-5 0-2 1-5 6-15 >15
Slide prepared by Rachel Wetzsteon Kannus et al., 1995.
Pre-Menarche Post-Menarche
3%
20%
8%
BMC
% S
ide-
to-S
ide
Diff
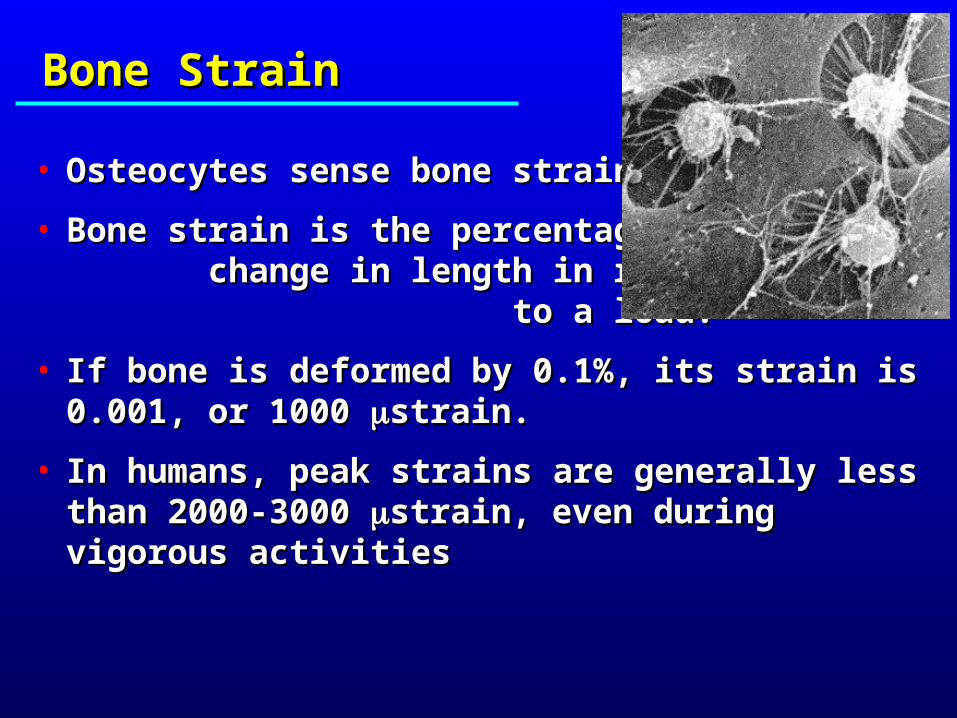
Bone StrainBone Strain
• Osteocytes sense bone strainOsteocytes sense bone strain
• Bone strain is the percentage change Bone strain is the percentage change in length in response to a load. in length in response to a load.
• If bone is deformed by 0.1%, its strain is 0.001, or If bone is deformed by 0.1%, its strain is 0.001, or 1000 1000 strain. strain.
• In humans, peak strains are generally less than In humans, peak strains are generally less than 2000-3000 2000-3000 strain, even during vigorous activitiesstrain, even during vigorous activities

Bone can be maintained with a few Bone can be maintained with a few large loading cycles, or thousands of large loading cycles, or thousands of extremely small onesextremely small ones
maintain
resorb
anabolic
Qin et. al., 1998
Low Magnitude Mechanical Low Magnitude Mechanical Stimuli are Anabolic to BoneStimuli are Anabolic to Bone
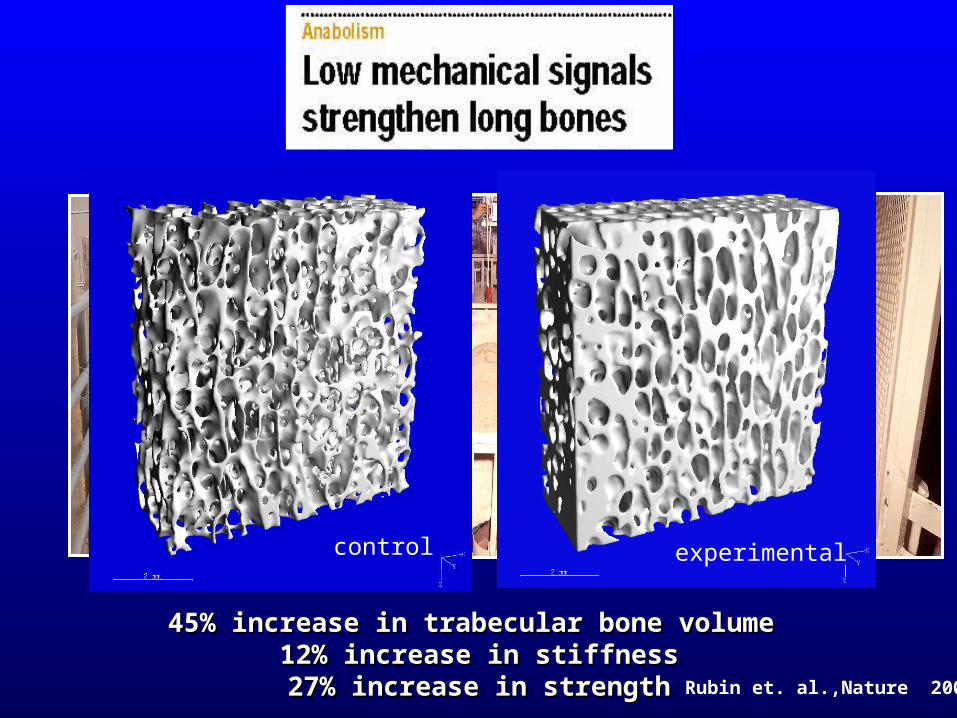
45% increase in trabecular bone volume 45% increase in trabecular bone volume 12% increase in stiffness12% increase in stiffness27% increase in strength27% increase in strength Rubin et. al.,Nature 2001
experimental control

But, wait!But, wait!There’s more to the story….There’s more to the story….
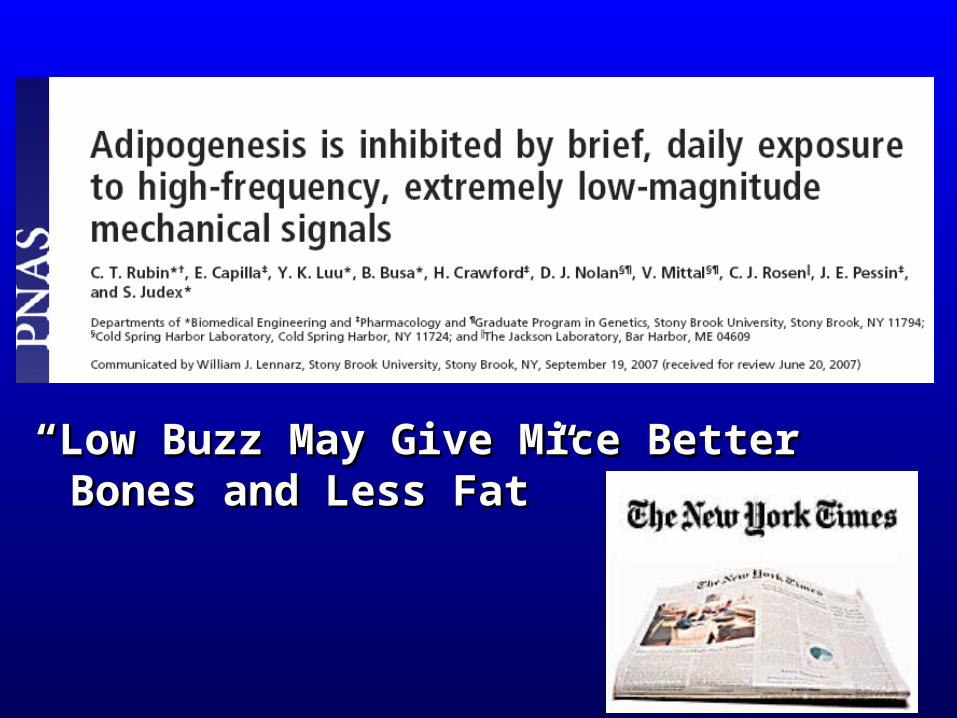
““Low Buzz May Give Mice Better Bones and Low Buzz May Give Mice Better Bones and Less Fat” Less Fat”
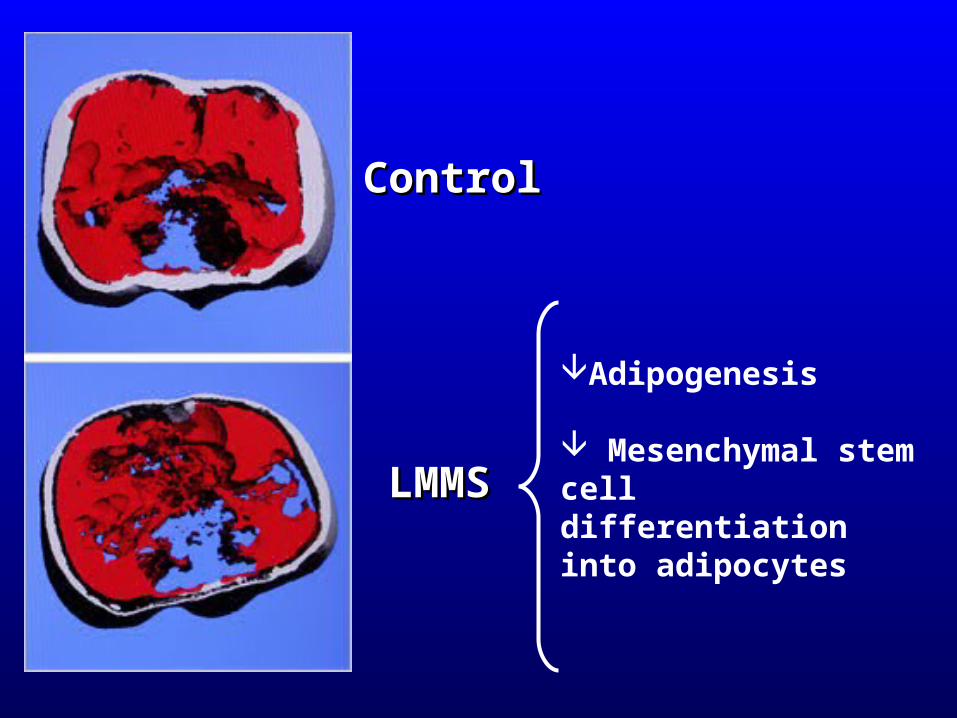
ControlControl
LMMSLMMS
Adipogenesis
Mesenchymal stem cell differentiation into adipocytes

“I’ve got him on vibrate”
AcknowledgementsAcknowledgements• Project StaffProject Staff
– Krista Howard and Kristin FrinoKrista Howard and Kristin Frino
• NIHNIH– NIDDK, NIDDK and NIAMS NIDDK, NIDDK and NIAMS
• CHOP IBD Center and GI DivisionCHOP IBD Center and GI Division– Robert Baldassano and Meena ThayuRobert Baldassano and Meena Thayu– Meena Thayu, MD Meena Thayu, MD
• CHOP Nutrition and Growth LabCHOP Nutrition and Growth Lab– Babette S. Zemel, PhDBabette S. Zemel, PhD
• SUNY and Juvent, IncSUNY and Juvent, Inc– Clint Rubin, PhDClint Rubin, PhD