CATHETER ASSOCIATED URINARY TRACT INFECTION IN THE ...
74
CATHETER ASSOCIATED URINARY TRACT INFECTION IN THE INTENSIVE CARE UNIT: INCIDENCE, RISK FACTORS AND MICROBIOLOGIC PROFILE. A DISSERTATION SUBMITTED TO THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA, IN PART FULFILMENT OF THE REQUIREMENT FOR THE AWARD OF FELLOWSHIP OF THE COLLEGE IN ANAESTHESIA. BY NWACHUKWU, MARTHA UGOCHI. MBBS (NIG.) 1991. i
Transcript of CATHETER ASSOCIATED URINARY TRACT INFECTION IN THE ...

CATHETER ASSOCIATED URINARY TRACT INFECTION IN THE INTENSIVE
CARE UNIT: INCIDENCE, RISK FACTORS AND MICROBIOLOGIC PROFILE.
A DISSERTATION SUBMITTED TO THE NATIONAL POSTGRADUATE MEDICAL
COLLEGE OF NIGERIA, IN PART FULFILMENT OF THE REQUIREMENT FOR
THE AWARD OF FELLOWSHIP OF THE COLLEGE IN ANAESTHESIA.
BY
NWACHUKWU, MARTHA UGOCHI.
MBBS (NIG.) 1991.
i

DEDICATION
This dissertation is dedicated to the Almighty God who makes all things beautiful in His time. It
is also dedicated to my Lord and Saviour Jesus Christ, who ransomed me with His Precious
Blood.
iv
ACKNOWLEDGEMENT
I heartily wish to appreciate my project supervisors: Dr H. A. Ezike, Dr Ajuzieogu Obinna and
Dr (Mrs) Onyeka Tonia for their encouragement, support and painstaking efforts in guiding the
various aspects of this research work and proof-reading the manuscripts with admirable
promptness.
My gratitude also goes to the other consultant Anaesthetists who read through and made
necessary corrections in the work especially Drs Onyekwulu F. and Amucheazi A. I also wish to
appreciate Dr. P. Ufoegbunam who counseled me on the choice of research topic and provided
me with appropriate impetus for this work.
I am indebted to the resident doctors who assisted in the collection of some of the samples
especially Dr Solomon Akponye, who rendered this assistance as a friend indeed. I appreciate the
Medical Laboratory Scientists in both microbiology laboratories of the tertiary institutions where
I carried out my investigations for their understanding in receiving urine samples even at call
hours.
Finally, I wish to thank immensely, my husband Dr. Nwachukwu, E.N. and children - Daniel,
David and Deborah for their patience, understanding, love, care and many prayers while this
work persisted. May the good Lord reward you all for your sacrifice and labour of love on my
behalf.
v

TABLE OF CONTENTS
Title Page
Title page i
Declaration page ii
Attestation page iii
Dedication iv
Acknowledgement v
Table of contents vi
List of tables viii
List of figures ix
List of Abbreviations x
Summary 1
Chapter 1: Introduction 3
Aims and Objectives 6
Chapter 2: Literature Review 7
Chapter 3: Patients, Materials and Methods 18
Chapter 4: Results 23
Tables 26
Figures 30
Chapter 5 Discussion 36
vi

Conclusions 44
Recommendations 46
Limitations of the study 47
References 48
Appendices 57
Appendix I : Data collection form 57
Appendix 11: Patient informed consent 60
Appendix 111: UNTH Ethics Committee approval 62
Appendix 1V: FMC Ethics Committee approval 63
Appendix V: Registration of dissertation 64
vi
LIST OF TABLES
Table Title Page
Table1. Distribution of duration of admission/catheterization with CAUTI status 26
Table II .Antibiotic sensitivity pattern of bacterial isolates 27
Table III. Antibiotic resistant pattern of bacterial isolates 28
Table IV. Distribution of ICU fomites with their isolated organisms. 29

vii
LIST OF FIGURES
Figure Title Page
Figure1. Incidence of Catheter Associated Urinary Tract Infection 30
Figure2. Age group distribution of patients with their CAUTI status 31
Figure3. Gender distribution of patients with their CAUTI status 32
Figure4. Distribution of patients with comorbidities and CAUTI status 33
Figure 5.Clinical specialty distribution of subjects and CAUTI status 34
Figure 6.Distribution of various microbial isolates 35
viii
LIST OF ABBREVIATIONS
ABUTI -Asymptomatic bacteremia urinary tract infection
ASB- Asymptomatic bacteriuria
BMI- Body Mass Index
CAUTI-Catheter -Associated Urinary Tract Infection
CDC- Centre for Disease Control.
CFU- Colony Forming Unit
CONS- Coagulase Negative Staphylococcus.
CVP-Central Venous Pressure.
DA-HAI Device–Associated Hospital Acquired Infection.
ECG-Electrocardiography.
E coli- Escherichia coli.
EEG- Electroencephalography.
E R-Emergency Room.
FMC- Federal Medical Centre.
HAI-Hospital Acquired Infection.
HDU- High Dependency Unit.
HIV- Human Immunodeficiency Virus.
ICU-Intensive Care Unit.
ix
INICC- International Nosocomial Infection Control Consortium.
IUC-Indwelling Urethral Catheter
KISS-The Hospital Infection Surveillance.(German)
MRSA- Methicillin Resistant Staphylococcal Aureus
NHSN- NationalHealthcare Safety Network.
OR- Operating Room.
P aeruginosa- Pseudomonas aeruginosa
SPSS- Statistical Package for Social Sciences
SUTI- Symptomatic Urinary Tract Infection.
UCH- University College Hospital.
UICP- Universal Infection Control Precautions
UNTH- University of Nigeria Teaching Hospital.
USA-United States of America.
UTI- Urinary Tract Infection.
VRE- Vancomycin Resistant Enterococcus.
x

SUMMARY
Patients in the intensive care units often require the insertion of various invasive devices such as
peripheral venous lines, urinary catheters and tracheal tubes for therapy and monitoring. These
devices predispose them to a high risk of acquiring nosocomial infections. Catheter-associated
urinary tract infection (CAUTI) is one of the commonest types of hospital-acquired infection
(HAI) in the ICU, and increases cost, morbidity and mortality. This prospective observational
study was aimed at determining the incidence of catheter- associated urinary tract infection with
its risk factors and microbiologic profile among critically ill patients in two Intensive care units
in South East Nigeria. The study was conducted over a seven -month period in the Intensive
Care Units of University of Nigeria Teaching Hospital (UNTH) Ituku Ozalla , Enugu State and
Federal Medical Centre(FMC), Umuahia, Abia State. Both hospitals have four- bedded ICUs but
UNTH also has a four-bedded High Dependency Unit (HDU). Patients admitted into these ICUs
with indwelling urinary catheters inserted in the Emergency room(ER), Operating Room (OR) or
ICU who met the inclusion criteria were enrolled for the study.
The first catheter urine sample was collected aseptically from each patient and sent for
microscopy, culture and sensitivity (mcs) to ascertain the baseline urine status. The patients
whose base line samples had microbial growth were excluded as the study was aimed at UTI
acquired in the ICU. A total of ninety six patients were enrolled, 26 patients either had microbial
growth in their first samples or demised before the collection of the second sample and had to be
excluded from the study. Seventy patients concluded the study. A total of 25 (35.71%) of the 70
subjects had microbial growth in their second or third sample giving an incidence of 36%.Four
(13.79%) of 29 whose duration of admission/catheterization was 48 hours to 72 hours had
CAUTI, while 21(51.22%) of 41 whose duration of admission was up to 5-7days had CAUTI.
Twenty eight (28) organisms were isolated and include Candida species, 12(42.87);
Staphylococcus aureus, 4(14.29);Klebsiella species,3(10.71%); Escherichia coli 2(7.14%); others
7(25.00%). The bacterial isolates were mostly susceptible to Nitrofurantoin. The organisms
showed a high resistance to the antibiotics tested.
1
The most predominant organism grown from ICU fomites was Staphylococcus aureus and the
fomite most affected was the suction machine. This study showed a high incidence of CAUTI in
ICU with duration of admission /catheterization as the only statistically significant risk factor. It
also confirmed the presence of pathogens on ICU fomites which could be continuous sources of
cross-infection affecting both patients and health care givers. Institution guidelines for the care
and monitoring of urethral catheterization are therefore desirable and urinary catheters should be
removed once they are no longer needed. Nitrofurantoin can be used for the empirical treatment
of UTI in our environment while awaiting urine microscopy, culture and sensitivity results.

2

CHAPTER ONE
INTRODUCTION
The Intensive Care Unit (ICU) is an area of the hospital where facilities are concentrated for
treatment of critically ill patients1.The purpose of the ICU is to provide a level of care
unattainable in other areas of the hospital for patients suffering an acute illness from which they
have a realistic chance of recovery. In addition to nursing care, observation and monitoring, the
patient may also require mechanical ventilation and cardiovascular support. In some centres,
separate ICUs exist for specialized fields of medicine such as coronary care, neurosurgery,
paediatrics, and transplant surgery. However in the majority of hospitals, as obtainable in the
developing countries, a general ICU deals with critically ill patients from various specialties.1
Nosocomial infections, also called health care acquired or health care-associated infections
(HAI) is defined by the Centre for Disease Control (CDC) as a localized or systemic condition
resulting from an adverse reaction to the presence of an infectious agent(s) or its toxin(s) without
any evidence that the infection was present or incubating at the time of admission to the acute
care setting.2 Patients admitted into the ICU are especially susceptible to nosocomial infections
in view of the significant risk factors such as the use of invasive devices like central venous
catheterization, urethral catheterization, mechanical ventilation; stress ulcer prophylaxis, and
increased ICU stay.3-6 Nosocomial infections result in increased morbidity and mortality,
prolonged hospital stay and increased medical expenses.1
Hourly measurement of urine output is a routine procedure for the critically ill patient, the
amount of urine formed each hour being an indicator of the fluid status and renal function and a
reduction in the volume to less than a critical value is a matter of concern.7 An adequate urine
flow should be more than 500mls/24 hours per m2 or more than 20mls/hour/m2. Accurate hourly
measurements of urine output is therefore essential for evaluation of fluid status and renal
perfusion.7 The indwelling urethral catheter is passed to enable this urine monitoring. The
presence of an indwelling urethral catheter is often complicated by catheter-associated urinary
tract infection.
3

Catheter-Associated Urinary Tract Infection (CAUTI) is urinary tract infection in a patient who
had an indwelling urinary catheter (IUC) in place at the time of or within 48 hours prior to
infection onset.8 Catheter associated urinary tract infection complicates 14 -100% of all catheters
passed depending on the duration of use.9 They account for 32% of all health care associated
infections in the intensive care units in the United States of America9 and has been associated
with a three-fold increased risk for mortality in hospital-based studies with estimates of more
than 50,000 excess deaths occurring per year in the United State of America(USA) as a result of
these infections.10 Chukwuocha in Owerri, South East of Nigeria found a prevalence of 44% of
bacteriuria among catheterized patients in various hospital wards11. In a study conducted at the
University College Hospital (UCH) Ibadan, Western Nigeria, CAUTI accounted for 43.96% of
HAI.12 Rosenthal et al. in a study of 55 ICUs in 8 developing countries discovered that CAUTI
was responsible for 29% of device-associated nosocomial infections, giving prevalence of
4.2%.13 Catheter-associated urinary tract infection can lead to such complications as cystitis,
pyelonephritis, gram negative bacteriuria, prostatitis, epididimytis and orchitis in the male;
endocarditis, vertebral osteomyelitis, septic arthritis, endolphthalmitis, and meningitis in all
patients14.These complications associated with CAUTI cause discomfort to the patient,
prolonged hospital stay, increased cost and mortality.14The daily rate of bacteriuria in
catheterized patients increases by about 5% with the incidence directly related to the duration of
catheterization.15 Among the patients with bacteriuria, 10 to 25% will develop symptoms of
urinary tract infection such as suprapubic or loin pain16. Bacteraemia results from catheter-
related bacteriuria in approximately 3% of patients and invariably represents a serious
complication.15 Risk factors for acquiring CAUTI include, duration of catheterization, female
sex (because of the short and wide urethra and its proximity to the anus), extended ICU stay,
colonization of the drainage bag, diarrhea, diabetes mellitus, renal insufficiency and errors in
catheter care.15The predominant organisms causing CAUTI in ICU are enteric gram negative
bacilli, enterococci, pseudomonas aeruginosa and Candida species.16
4

ICU treatment is quite expensive both in the developed and developing countries of the world.
Okafor estimated the daily ICU cost in Eastern Nigeria at about $85 (about 13,000 naira).17 The
cost is further increased when there is an added burden of CAUTI which is reasonably
preventable. Estimates from one university hospital in Kuwait based on data for almost twenty
years showed that CAUTI led to approximately $204,000 in additional expenses per year,18
despite their importance, there have been very few studies focused on CAUTI in the critically ill.
No study has been done evaluating CAUTI in the Intensive care unit in South Eastern Nigeria.
This study therefore, was aimed at determining the incidence and risk factors associated with
CAUTI and the microbiologic profile with their sensitivity pattern in the ICUs of two tertiary
health care facilities in South Eastern Nigeria.
5
AIMS AND OBJECTIVES
AIM:
The aim of this prospective study was to determine the incidence of Catheter- Associated
Urinary Tract Infection (CAUTI), the risk factors and microbiologic profile among critically ill
patients on admission in two Intensive Care Units (ICUs) in South East of Nigeria.
SPECIFIC OBJECTIVES:
The specific objectives were the following:
1. To determine the incidence of CAUTI in the ICU.
2. To determine the risk factors associated with CAUTI in the ICU.
3. To determine the microbiologic profile of CAUTI in the ICU.
4. To determine the antibiotic sensitivity pattern of CAUTI in the ICU.
5. To determine the resident microorganisms in the ICU.
6
CHAPTER TWO
LITERATURE REVIEW
Definition of Catheter Associated Urinary Tract Infection (CAUTI)
Urinary tract infection (UTI) is an inflammatory response to the colonization of the urinary tract,
(which may involve the bladder (cystitis), renal pelvis (pyelitis),or renal parenchyma
(pyelonephritis)) from a bacteria or fungal pathogen.19 Catheter-associated urinary tract infection
(CAUTI) is urinary tract infection in a patient who had an indwelling urinary catheter in place at
the time of or within 48 hours prior to onset of infection.8 An ICU- acquired UTI was defined
using a modification of the criteria of Costel 20and colleagues as those patients with a positive
urine culture (at least 105colony forming units/ml(cfu/ml) of one or two organisms first identified
on ICU day 3 (48 hours) or later.20 Patients with positive urine culture within 48 hours of ICU
discharge were also considered to have ICU-acquired UTIs. Asymptomatic bacteriuria is the
isolation of a specified quantitative count of bacteria in an appropriately collected urine
specimen obtained from an individual without symptoms and signs of UTI.21Acute
uncomplicated UTI is a symptomatic bladder infection characterized by frequency, urgency,
dysuria, or suprapubic pain in a woman with normal genitourinary tract and is associated with
both genetic and behavioral determinants.22 Uncomplicated urinary tract infections rarely occur
in men and urinary infection in men is usually considered complicated.22 Pyuria is the presence
of increased numbers of polymorph nuclear leucocytes in the urine and is evidence of an
inflammatory response in the urinary tract23
Epidemiology of Catheter-Associated Urinary Tract Infection
Prevalence and Incidence
Device-Associated Hospital Acquired Infection (DA-HAI) rates in the ICU of countries with
limited resources are 3-5 times higher than rates in the high-income countries as reported from
hospitals by International Nosocomial Infections Control Consortium (INICC).24
7

In a prospective study conducted in an adult surgical ICU of a tertiary University Hospital in
Lebanon, incidence of CAUTI was 13.07 per 1000 urinary catheter days which was about ten-
fold higher than the US rate of 1.5 CAUTI rate per 1000 urinary catheter days determined by the
CDC/NHSN25and 2.5CAUTI rate determined by KISS.26 Prevalence of asymptomatic bacteriuria
in patients with short-term urethral catheterization is 9-23%, while that for long term
catheterization is 100 %.27
Daily risk of developing CAUTI is 3-7% in acute hospital settings.28Abaeze in Abeokuta,
Western Nigeria in a cross-sectional study with 200 catheterized patients, in a tertiary health
institution, found an incidence of CAUTI as 40%29 This rate was quite high compared to what
was obtainable in developed countries as the United States where a surveillance study of CAUTI
in the ICUs gave incidences of 3.1-7.4 per 1000 catheter days.30Abaeze however, attributed the
high incidence to the possibility of non-observance of sterile precautions during catheterization
and technical errors by health care givers. The mode of collection of the samples was not
mentioned as samples collected from the drainage bag will yield a higher incidence and health
care givers involved in urethral catheterization are usually trained and are aware that it is a sterile
procedure. This high incidence could also be as a result of the non-ICU location of the patients as
catheter care is not optimal on the general wards. The study also failed to mention the cut off for
significant bacteriuria as the incidence will be lower if ≥105 is used as against ≥103. They were
also silent on their criteria for diagnosis (symptomatic or asymptomatic or both. Karina et al.31
in a prospective study of medical patients in both ICU and non ICU wards, also recorded a very
high incidence (51.4%) in the Philippines General Hospital31.This high incidence could have
been as a result of a lower (≥103) cut-off for significant bacteriuria used in this study, though
their criterion for using that was based on some recommendations that for complicated UTI as in
catheterized patients, levels below 103 can be representative of true infection. The researchers
failed to mention if their result included both symptomatic and asymptomatic cases. However,
Alavaren et al.28 studying in the same region,-the Philippines, among 178 non-ICU medical and
surgical adult patients, also using ≥103as the value for significant bacteriuria, had a lower
incidence of 24.7%. This is probably because they excluded patients with confirmed UTI and
their study was conducted on non-critically ill patients, as infection rates are higher among the
critically ill. 8

Indranil Bagchi et al.32 studying 220 adult patients without recent history of UTI in both medical
and surgical wards and ICUs in a tertiary health facility in Maharashtra India found an incidence
of 29.09% which is slightly higher than Alavaren’s result.28 They also excluded patients with
recent UTI showing that excluding patients with UTI from the study, can reduce the incidence of
CAUTI. Duo-shuang33in a cohort study in the ICU in China, found an incidence rate for CAUTI
as 15.8. This rate is lower than others cited 28,29,31,32 probably because it is an ICU-specific study
as ICU patients although critically ill, usually attract better nursing care including better urinary
catheter care as patient to nurse ratio is smaller.
Pathogenesis
Urinary tract infection is inflammatory responses to the colonization of the urinary tract from a
bacterial or fungal pathogen.19 Most bacteria causing CAUTI gain access to the urinary tract
either extraluminally or intraluminally.34 Extra luminal contamination may occur during
insertion from contamination of the catheter from any source. It is also thought to occur when the
microorganisms ascend from the perineum along the surface of the catheter. It is commoner in
women because of the shorter length of the urethra and its proximity to the anus.35 Intraluminal
contamination occurs by ascent of bacteria from a contaminated catheter drainage tube or urine
drainage bag.36 There are three main catheter-associated entry points for bacteria.(1)The urethral
meatus, with the introduction of bacteria during insertion of the catheter.(2)The junction
(connection) of the catheter with the drainage bag especially when a break in the close catheter
system occurs and (3)the drainage port of the collection. All these mechanisms involved in the
pathogenesis of colonization and infection of the urinary tract combine to make CAUTI very
difficult to prevent in patients with indwelling catheter in place for more than two weeks.
Catheter-associated bacteriuria may be symptomatic or asymptomatic. 20-30% of patients with
bacteriuria will present with symptoms of CAUTI.37-38
Most CAUTI involve multiple organisms and resistant bacteria from catheter-associated
biofilms, and include enterobacteriaciae other than E coli, (e.g. klebsiella, enterobacter, proteus
and citrobacter), pseudomonas aeruginosa, enterococci, staphylococci and Candida.
9

The infecting organism depends on the hospital unit35. The predominant organisms causing
CAUTI in ICU are the enteric gram-negative bacilli, enterococci, Candida species and P.
aeruginosa.35 Candiduria is especially common in individuals on broad spectrum antibiotic
therapy,35 because of increased use of antibiotics, resistant microorganisms particularly
Pseudomonas aeruginosa and Candida albicans are too frequently involved in device- associated
nosocomial infections35.
Broad spectrum antibiotic use is likely to contribute to colonization by candida species by
suppressing endogenous bacterial flora, primarily in the gut and lower genital tract and possibly
in the superficial area adjacent to the urethral meatus. It may interfere with phagocyte function
and antibody formation with subsequent impaired host defense mechanism against candida
infections.39-41 Candiduria is increasingly becoming an important subgroup of nosocomial UTI
(10-15%) and almost all are caused by candida albicans.40-42The prevalence varies in hospital
settings and is most prevalent among patients in the Intensive care units, more especially surgical
ICU, leukaemia and bone marrow transport units.43,44 Previous studies showed that the common
risk factors were urinary tract instrumentation, previous surgical procedures, recent use of
antibiotics, advanced age, female sex, diabetes mellitus, immunosuppressive therapy and
prolonged hospital stay.40,42-44,46-48 In a recent case controlled study, it was shown that the risk
factor to develop candiduria was increased by 12-fold after urinary catheterization, six fold each
after use of broad spectrum antibiotics and presence of urinary tract abnormalities, four-fold
following abdominal surgeries, two-fold in the presence of diabetes mellitus and one-fold with
the use of corticosteroids.39The study found no significant difference between the groups
compared in terms of female sex and age.39
Catheter -Associated Biofilms
Catheters are a good medium for bacterial growth because once they gain access to the urinary
tract, bacteria produce various adhesions including hair-like fimbrae that allow them to attach
firmly to the catheter wall. These bacteria up-regulate their expression of certain genes resulting
in altered phenotypes that ultimately lead to biofilms (living layers of organisms).49
10

Urine contains protein that adheres to and primes the catheter surface. Microorganisms bind this
protein layer and attach to the surface. Such bacteria are different from fleeting planktonic
bacteria (bacteria that float in urine). Indwelling urinary catheter biofilms may initially be
comprised of a single organism, but can lead to multiorganism biofilms because the presence of
biofilms inhibits antimicrobial activity.49 The presence of urinary catheter biofilms has important
implications for antimicrobial resistance, diagnosis, prevention and treatment of CA-UTIs.49
Clinical Presentation of CAUTI
From the Centre for Disease Control Criteria, CAUTI may present as symptomatic urinary tract
infection (SUTI) or Asymptomatic Bacteriuria (ASB).24-25 SUTI must meet the following
criteria; 1. Patient had an indwelling urinary catheter in place at the time of specimen collection,
or onset of symptoms and signs and at least one of the following signs or symptoms with no
other recognized cause. Fever (>380C), suprapubic tenderness, costovertebral angle pain or
tenderness and positive urine culture of ≥105 colony forming units (cfu)/ml with no more than
two species of organisms, or patient had an indwelling urinary catheter removed within 48 hours
prior to urine collection or onset of symptoms and at least one of the following signs or
symptoms with no other recognized cause; fever (>380C), urgency, frequency, dysuria,
suprapubic tenderness, costovertebral angle pain or tenderness. A positive urine culture of ≥ 103
and<105 colony forming units (cfu)/ml with >2 species of microorganisms.24-25
Asymptomatic Bacteremic UTI (ABUTI):Patient with an indwelling urinary catheter or had one
in ICU in the past 48 hours with no symptom but has a positive urine culture >105 cfu/ml with
not more than two species of uropathogenic organisms and a positive blood culture with at least
one matching uropathogen microorganism to urine culture.24
11

Risk Factors
Various studies have identified the significant risk factors for CAUTI as being, the female
gender,35prolonged duration of catheterization29and prolonged duration of ICU
admission.29Alavaren et al28 in their study identified risk factors, as open drainage system,
prolonged catheterization and daily meatal care. In this study, open drainage system was used in
31.5% while closed drainage was used in 68.5%. Bacteriuria was present in 88.5% of those on
open drainage by the 3rd day and 100% on the 6th day, while among those with closed drainage
system, only 38% had bacteriuria on the 6th day of catheterization. Daily meatal care and
application of antimicrobial ointments and solutions theoretically should prevent or delay onset
of infection. This study showed that bacteriuria was higher in patients with daily meatal care
compared to those without catheter care. This could have resulted from the fact that mobilization
of catheter during catheter care irritates the bladder mucosa there by encouraging
microorganisms to ascend and invade the mucosal epithelium and proliferate50. The average
daily incidence of bacteriuria was 9.5%. This increasing incidence of bacteriuria with increasing
duration was valid up to the 6th day of catheterization beyond which 100% of the patients had
bacteriuria. Ekrem Temiz51 in Zongudal Kaemas University Hospital found that immune
suppression, previous antibiotic usage and the presence of other site nosocomial infection were
risk factors for acquiring CAUTI. In the absence of other site infection, the female gender and
duration of catheterization were the risk factors for CAUTI alone. Karina Billote Domingo31 in
the Philippines studying both ICU and non-ICU medical patients with indwelling Foley catheters
inserted within 24 hours (in the emergency room) of admission found duration of catheterization,
the female gender and diabetes mellitus as unalterable risk factors for CAUTI. In their study,
bacteriuria developed at an average of 4.1 days. After two days of catheterization, 20.6% of the
patients had acquired CAUTI, 36% after 4 days and 46.7% after 7days. Duration of
catheterization was the most significant risk factor. Increasing duration of catheterization
increases the likelihood of microbes ascending to the bladder either via the intra or extra luminal
route. The female gender probably because of the anatomy was the next risk factor leading to
easier access of the perineal flora to the bladder along the catheter as it traverses the shorter
female urethra. 12
Diabetes mellitus was the third risk factor.Diabetics are at an increased risk of acquiring
infections because of increased prevalence of perineal colonization by potential pathogens and an
increased ability of the urine to support microbial growth31. Indranil Bagchi et al32 in their study
found increasing age, female gender, diabetes mellitus and duration of catheterization as risk
factors for CAUTI in ICU. This study revealed that maximum incidence occurred in people
above 75 years of age with an incidence of 66.67%( 2 out of 3) while the minimum incidence
was found in the age group 18-25 years with an incidence of 11.76% (2 out of 17).In the same
study, CAUTI occurred in 36 out of 105 females (34.29%) while the incidence in males was
24.35% (28 out of 115) showing that females were more vulnerable to acquiring CAUTI than
males as already indicated. The study also found that out of the 64 cases of CAUTI, 10 (15.63%)
were detected on the third day, 22 (34.38%) within 5 days and 32 (50%) within 7 days. The 50%
incidence on the 7th day is close to Domingo’s 46.7% on the same day in their study31. Indranil’s
study40 also showed that 14 (21.88%) out of the 64 cases of CAUTI recorded were diabetic
patients. In that same study,only 10 diabetic patients were free from CAUTI showing that
diabetes mellitus predisposes a patient to developing CAUTI.
Microorganisms involved in Catheter associated urinary tract infection.
Abaeze et al29 in Abeokuta, Western Nigeria and Indranil et al32 in India, in their various studies
isolated E coli as the commonest organism causing CAUTI both in ICU and non ICU settings
while Taiwo et al52 in Osogbo, Western Nigeria and Mahshid53in Iran found Klebsiella species as
the commonest organisms causing CAUTI. Mindy et al 54 in Singapore and Duo-shuang33 in
China isolated Candida species as the commonest organisms in their independent studies.
Abaeze et al29 in their study with 200 patient samples showed that 82 (41%) yielded bacterial
growth while 118 (59%) were sterile. 29(37.37%) of the isolates were E coli, 17(20.73%) were
Klebsiella Pneumoniae, 13(15.85%) were Staphylococcus aureus, 10(12.2%) were Pseudomonas
aeruginosa, 8(9.75%) were Proteus mirabilis while 5(6.1%) were Candida albicans. The
commonest organisms in this study were enterobacteriaceae group (E. coli and Klebsiella) which
are organisms in the bowel and may have ascended into the urinary tract following
contamination.
13

The most sensitive drug was ofloxacin with a sensitivity of 52.9% for Klebsiella pneumonia and
13.8% for E coli. Gentamycin was the next sensitive drug with a sensitivity of 41.17% for
Klebsiella and 13.79% for E coli. Augmentin had the highest (41.17%) sensitivity for E coli, the
commonest organism and 12.5% for Proteus mirabilis probably because these drugs are not
easily abused. The commonly used antibiotics (Cotrimoxazole and Amoxycillin) had 100%
resistance likely because of inappropriate uses and abuse. In Indranil’s study32 of 200 adult
patients in the ICU in Maharashtra India, 64 patients developed CAUTI with 66 isolates. 72.73%
were caused by gram negative bacilli, 16.67% by gram positive cocci, and 10.6% by fungal,
23(34.85%) were caused by E coli, 13(19.7%) by Klebsiella, 8(12.2%) by
Pseudomonas,7(10.6%) by Candida, 4(6.06%) by Enterococcus, 4(6.06%) by CONS, 2(3.03%)
by Citrobacteria and Proteus. In this study, all gram negative isolates were sensitive to
Imipenem, E coli and pseudomonas species showed maximum sensitivity to Piperacillin and
Tazobactam. Klebsiella showed maximum sensitivity to Ceftazidime. All gram positive isolates
were sensitive to Vancomycin. CONS, Staphylococcus aureus and enterococcus species showed
maximum sensitivity towards Linezolidine and Ciprofloxacin. Both groups of isolates showed
the least sensitivity to Ampicillin likely because the common antibiotics like Ampicillin are often
abused. In Taiwo’s study52 122 patient samples were studied out of which 108 had significant
bacteriuria with 126 microbial isolates. Klebsiella was the commonest organism isolated
46(36.6%), Pseudomonas was the next 34(27.0%), E. coli was the third 26(20.6), Staphylococcus
aureus 12(9.5%), Candida 4(3.2%).Many of these organisms are part of the patient’s endogenous
bowel flora, and some may have been acquired from cross contaminations from other patients or
the hands of health care givers. Isolating 126 organisms from 108 patient samples implies that
some infections were either monomicrobial or polymicrobial. The organisms were most sensitive
to Ciprofloxacin (83.3%) and Pefloxacin (66.7%) and exhibited multiple resistance to commonly
used antibiotics such as Ampicillin (100%), Gentamycin (90.9%), Tetracycline (89.9%),
Cotrimoxazole (87.3%). The emergence of multiresistant pathogens could be as a result of
prophylactic antibiotic use or abuse of commonly used antibiotics as all the patients were on
prophylactic antibiotic.
14

ICU Resident Organisms
Studies, 55,56 have shown that hospital surfaces and frequently used medical equipments become
contaminated by a variety of pathogenic and non-pathogenic organisms. In a study by Kramer et
al56 in which literature was systematically reviewed in Medline, cited articles were assessed and
standard text books on the topic were reviewed, they discovered that most gram positive bacteria
such as Enterococcus specie including Vancomycin Resistant Enterococcus (VRE),
Staphylococcus aureus including Methicillin Resistant Staph aureus (MRSA),and Streptococcus
pyogenes survive for months on dry surfaces. Many gram negative organisms such as E coli,
Klebsiella, Pseudomonas aeruginosa, Acinobacter, and Shigella specie can also survive for
months on dry surfaces. Candida albicans which is the most important nosocomial fungal
pathogen can survive for four months on surfaces. These imply that the most common
nosocomial pathogens can survive or persist for prolonged periods in hospital surfaces and
formites,56 thereby becoming continuous sources of infection transmission if no regular
preventive measure is applied.56 The mode of transmission from inanimate surfaces to
susceptible patients can be direct or indirect through the hand of the health care worker, but this
can be reduced to 50% through compliance with hand hygiene.56 Sung-on Teng and colleagues
in Taiwan determining the degree of bacterial contamination of patient’s files in the surgical ICU
and surgical ward and found that 90 % (81 out of 90) of charts in ICU and 72.2 %( 65 out of 90)
from surgical wards were contaminated with pathogenic or potential pathogenic bacteria
(p=0.0023).57 Coagulase negative staphylococci (CONS) were the most commonly isolated
bacteria both in surgical ICU( n=40, 44.44%) and surgical ward( n=48, 53.33%). Several
bacteria isolated from the chart had the same antibiogram as that isolated from the patient.57
Contaminated patients’ charts, can therefore serve as a source of cross infection. In surgical ICU,
Klebsiella pneumonia isolated from two of three charts was also isolated from corresponding
patients. Compliance with hand hygiene by health workers is critical to reducing this. Hand
washing remains the cornerstone of Infection control in the ICU.58 In a study conducted by
Tamberker58 in Amravati India, 400 swab samples were collected from the hands of 100 students
15
before and after hand washing and analyzed to see the effect of hand washing on
microbial flora of the hand. Prior to hand washing the hands of all the students were found to
harbor pathogens which include Staphylococcus species 23%, E coli 20%, Klebsiella 10%,
Micrococcus specie 9%, Proteus sp, Citrobacter and Streptococcus 7% each Enterobacter 6%,
Enterococcus 4%, Pseudomonas 3%, Salmonella species 2%. After hand washing there was 54%
reduction in microbial flora. Salmonella had 100% reduction, Staphylococcus 88%. E coli 59%,
Enterococcus 59%, Proteus 55%, Streptococcus 54%, Citrobacter 45% and Klebsiella 39%.This
indeed shows that compliance to hand washing by health care personnel reduces transmission of
nosocomial infections.
Infection Control in the Intensive Care Unit
Infection control is an application of scientific and epidemiological principles for infection
prevention and reduction. Hand washing, aseptic techniques and environment cleaning are
perhaps the most important infection control measures. Infection control programs have become
a requirement for hospital accreditation by the Joint Commission on Accreditation of Healthcare
Organizations59. The first formal US infection control hospital surveillance project initiated it as
a result of the 1950s Staphylococcus aureus pandemic. The Institute for Healthcare Initiatives
(IHI) is a not-for-profit organization reports how greater than 100,000 annual deaths can be
avoided by quality initiative infection control measures. Infection control consists of standard
precautions with or without transmission-based isolation precautions depending upon site/type of
infection. The infection control committee typically includes an infection control practitioner
(physician or nurse), trained ICU epidemiologist, and infectious disease or microbiology
specialist. The committee aims to develop infection control policies, educate hospital personnel,
provide wound-infection feedback to surgeons, and investigate suspected outbreaks. Standard
(universal) precautions are recommended for all hospitalized patients and consist of hand
hygiene and respiratory hygiene with cough etiquettes. This also includes safe disposal of
instruments and soiled linens. Hand hygiene, perhaps the most effective method for infection
control, can be done with 60-95% alcohol-based hand rub or soap.
16

Hand hygiene is recommended before clean/ aseptic procedures, before and after touching a
patient or patient surroundings, and after body fluid exposure.60 Infection control bundles
example, urinary catheter bundles can be used to reduce the incidence of CAUTI and this
includes;
Daily surveillance regarding further need of catheter
Proper securing of catheter on body
Maintenance of closed sterile drainage tubes
Aseptic techniques for obtaining urine samples
Meticulous Hand hygiene
Avoidance of prophylactic antibiotics and regular urine culture.
17

CHAPTER THREE
PATIENTS, MATERIALS AND METHODS
Study Locations
This study was conducted on critically ill patients admitted into the Intensive Care Units (ICUs)
of the University of Nigeria Teaching Hospital (UNTH), Ituku Ozalla, Enugu State and Federal
Medical Centre (FMC), Umuahia, Abia State. Both hospitals are tertiary health institutions with
multidisciplinary Intensive Care Units in the South East, Nigeria.
UNTH is a 450-bedded hospital in Enugu state serving Enugu, Anambra, Ebonyi, Abia, Imo and
some states in the South South zone of Nigeria. FMC Umuahia is a 304-bedded hospital in Abia
State and serves Abia, Imo, Ebonyi and Akwa Ibom States. Both hospitals have four-bedded
ICUs. UNTH in addition has a 4 bedded- high dependency unit to which patients are stepped-
down before they are discharged to the ward.
Ethical Clearance
Ethical clearance was obtained from Health Ethics Research Committees (HERC) of both
hospitals. Informed consent was obtained from the patients or relatives for the study. One
patient declined the collection of her third sample and was allowed to opt out.
Study Design
This was a prospective cross-sectional descriptive study in which patients who met the inclusion
criteria were included.
Sample Size Estimation
The sample size was calculated using the formula for determining the minimum sample size for
the prevalence rate of a condition in a population, assuming a confidence level of 95% and
degree of accuracy of 0.05.
18

The formula is as follows:
n=Z2 P (1-P)/d2
Where:
n= the desired sample size when the population is greater than 10,000.
z=1.96 (a standard normal deviate, usually set at 1.96, which corresponds to the 95% confidence
level).
P=the proportion in the target population estimated to have a particular characteristic. This is the
proportion of catheterized ICU patients estimated to have CAUTI. From a previous study carried
out in the ICU of 8 developing countries, the prevalence of CAUTI among critically ill patients
admitted into the ICU was 4.2%44. So P =4.2% was assumed ( i.e. 0.042).
1-P=1-0.042=0.958
d=0.05(degree of accuracy desired)
Therefore substituting the figures into the formula, the minimum sample size was n=Z2P (1-P)/d2
=1.962 x 0.042 x0.958/0.052 = 61.83 approximately 62. An attrition of 10% gave 6.18
approximately 6 giving a sample size of 68.
96 patients who met the inclusion criteria were initially enrolled into the study. 26 patients had to
be excluded as some of them demised while some had microbial growth in their first samples
leaving only 70.
Inclusion Criteria
Adult patients (18 years and above) admitted into the ICU with IUC inserted in the ICU or
elsewhere without signs and symptoms of UTI.
19

Exclusion Criteria
Paediatric patients (less than 18 years)
Patients with features of UTI prior to ICU admission as this was an incidence study based on
ICU- acquired infection.
Patients whose ICU admission was anticipated to be very brief (24 hours or less)
Patients with renal impairment.
Patients who demised before their second sample could be collected.
Procedure
A total of 96 patients were enrolled into the study. Twenty six (26) patients were excluded
while 70 were recruited. The researcher aseptically collected urine specimens from the
disinfected urinary catheter ports into sterile containers some of which contained boric acid (to
prevent multiplication of bacteria). The samples were sent to the microbiology laboratories for
microscopy, culture and sensitivity. The first sample was collected within 24 hours of ICU
admission from 96 patients. The second was collected at 48 to 72 hours (day 3-day 4) of
admission while the third sample was collected on day 5-7 of ICU admission. Only two samples
were collected from 29 patients while those from whom only baseline samples were collected
either because of their demise or presence of microbial growth were excluded from the study.
Forty one (41) patients also had their third samples collected on days 5-7 of ICU admission.
Patients discharged from the ICU before 72 hours of admission were followed up on the ward to
collect the second sample (as ICU- acquired CAUTI may still be incubating).
Urine specimen was cultured with the semi-quantitative method in the microbiology laboratories
of both hospitals. Significant bacteriuria was regarded as the growth of ≥103colony forming units
(cfu) /ml of urine. The results of full blood counts and blood culture of patients with evidence of
systemic infection (requested by the managing physicians) were reviewed to rule out bacteremia
though bacteremia was outside the scope of this study.
20

Swabs of regularly used equipments in the ICU (such as suction machines, mechanical
ventilators, patient’s monitors, beds and side tables) were also taken and sent for microscopy,
culture and sensitivity to determine the resident organisms in these ICUs. This was done twice
(in the first and last months) during data collection in both ICUs. A data collection form was
used to document the patient’s demographic characteristics and results of the investigations.
Statistical Analysis
Data were collected on forms specifically designed for the study. Data were presented in tables
expressed as mean (±SD) and figures (pie and bar charts). Statistical association was determined
using the Chi-square test for categorical variables and Student’s t-test for numerical variables. A
p-value of <0.05 was considered significant. Statistical analyses were performed using Statistical
Package for Social Sciences (SPSS) version 20, 2011.
Risk factors were determined with multinomial logistic regression analysis
21
CHAPTER FOUR
RESULTS
The baseline urine sample was collected from all 96 patients but only results of 70 patients were
analysed. The second samples were collected from the seventy recruited patients 48-72 hours of
ICU admission. Twenty nine (41.43%) of the 70 patients studied had only their second samples
collected 48 to 72 hours of ICU admission, while 41(58.57%) patients whose ICU admission
was longer also had their third samples collected on or after the 5th day (5-7 days) of ICU
admission. A total of 25 (35.71%) of the 70 patients recruited had microbial growth in their
samples giving a CAUTI incidence of 35.71%.
Table 1 shows the effect of duration of catheterization and admission on CAUTI status. In this
study, 29 of the 70 patients recruited exited after the collection of the second sample. Four
(13.73%) of the 29 patients developed CAUTI while 25(86.21%) did not. Twenty one (51.22%)
of the 41 patients whose third samples were collected were positive for CAUTI on or after the
fifth day of catheterization and admission while 20(48.75%) did not acquire CAUTI. The
incidence of CAUTI in this study was 35.71%. Duration of catheterization and admission was
the only statistically significant factor in this study with a p-value of 0.001 and x2 as 10.363.
Table II shows the antibiotic sensitivity pattern of isolated bacteria. Nitrofurantoin had the
highest sensitivity being sensitive to 11(68.75%) of 16 organisms, the quinolones were sensitive
to 6(37.50%) organisms while Augmentin and the cephalosporins were sensitive to 3(18.75%)
each. Imipenem was sensitive to only one (50%) of two organisms tested. Staphylococcus
aureus, E coli, Lactose fermenting organisms isolated were all susceptible to Nitrofurantoin
(100%). Klebsiella was only 33.3% sensitive to Nitrofurantoin, quinolones and Imipenem.
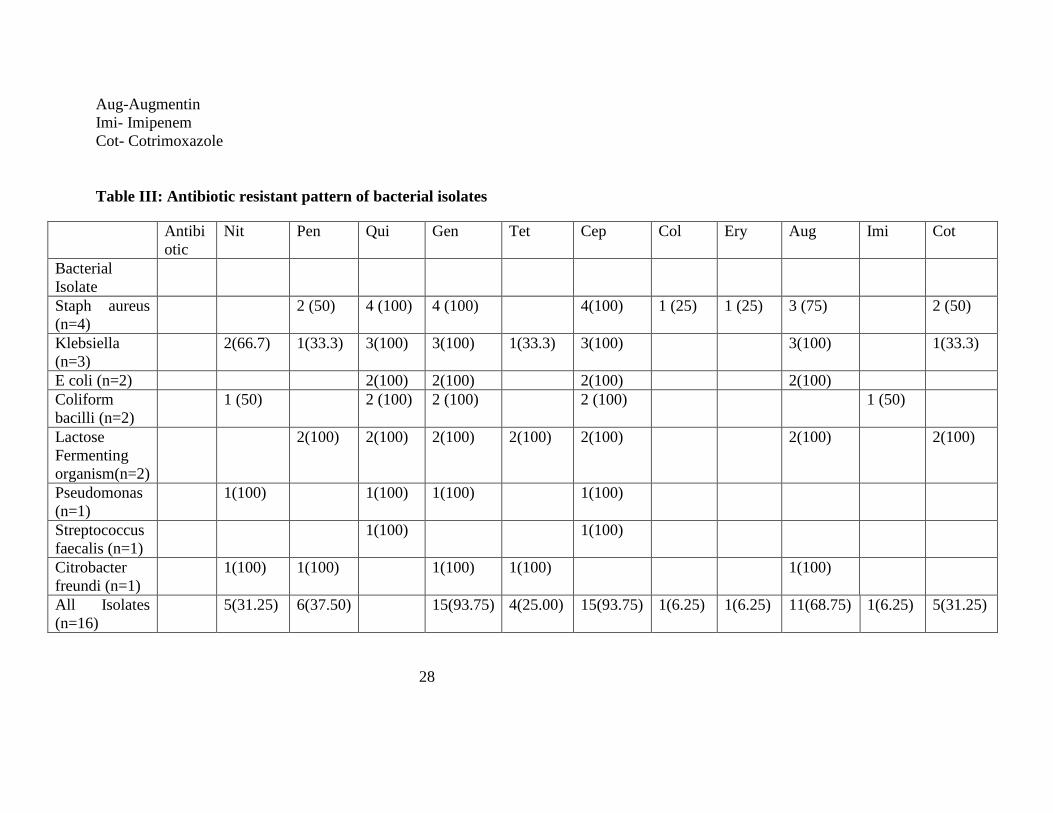
Table III shows the antibiotic resistant pattern of isolated bacteria. Staphylococcus aureus,
Klebsiella species and E coli were all 100% resistant to the Quinolones, Gentamicin and
Cephalosporins. They were also 75% and 100% each respectively to Augmentin. Pseudomonas
species were resistant to all the four antimicrobials tested. Fifteen (93.75%) of the sixteen
bacteria isolated were resistant to both Gentamycin and cephalosporins.
23
Eleven (68.50%) were resistant to Augmentin while 5(31.25%) were resistant to Nitrofurantoin.
All six organisms tested against the penicillins were resistant to them.
The isolated candida species were not tested against any antifungal drug for sensitivity and
resistance pattern.
Table IV shows various ICU fomites and the microorganisms isolated. A total of thirteen (13)
microorganisms were isolated: Staphylococcus aureus,7(53.85%);Klebsiella species,
2(15.39%);Staphylococcus epidermidis,1(7.69%); Coliform bacilli,1(7.69%); Proteus, 1(7.69%);
spore forming organism,1(7.69%).There was growth on six(60%) of the ten fomites. Three
fomites had mixed organisms while the other three had single organisms. Multiparameter
patients’ monitors had no growth on both cultures. Swabs from patients’ beds side tables and
suction machines showed microbial growth on both cultures. The ventilators and bedside tables
showed growth on one of the two swabs taken.
Figure 1 is a pie chart showing the incidence of catheter-associated urinary tract infection.
Twenty five (36%) of the 70 patients recruited had microbial growth while 45(64%) were free
from CAUTI.
Figure 2 is a bar chart representing the age group distribution of the patients with their CAUTI
status. The age range of patients studied was 18-75 years with a mean age of 36.99, (Standard
Error of mean-SEM of 1.881 and standard deviation-SD of 15.740). The most frequent age group
was 18-27 with 24 patients and 8(33.33%) being CAUTI positive. Age group 28-37 had a
frequency of 21 with 7 (33.33%) being CAUTI positive. 38-47 years had a frequency of 6 with
4(66.67) being CAUTI positive giving the highest occurrence of CAUTI. Only four patients
were of 68-77 age group and all were free from CAUTI.
Figure 3 is a bar chart showing gender distribution of respondents with their CAUTI status. In
this study, 49(70%) of the 70 patients studied were males while 21(30.00%) were females with a
male to female ratio of 2.33:1.00. Fourteen (28.57%) of the 49 male patients had CAUTI as well
as 11(52.38%) of the 21 female patients.
24
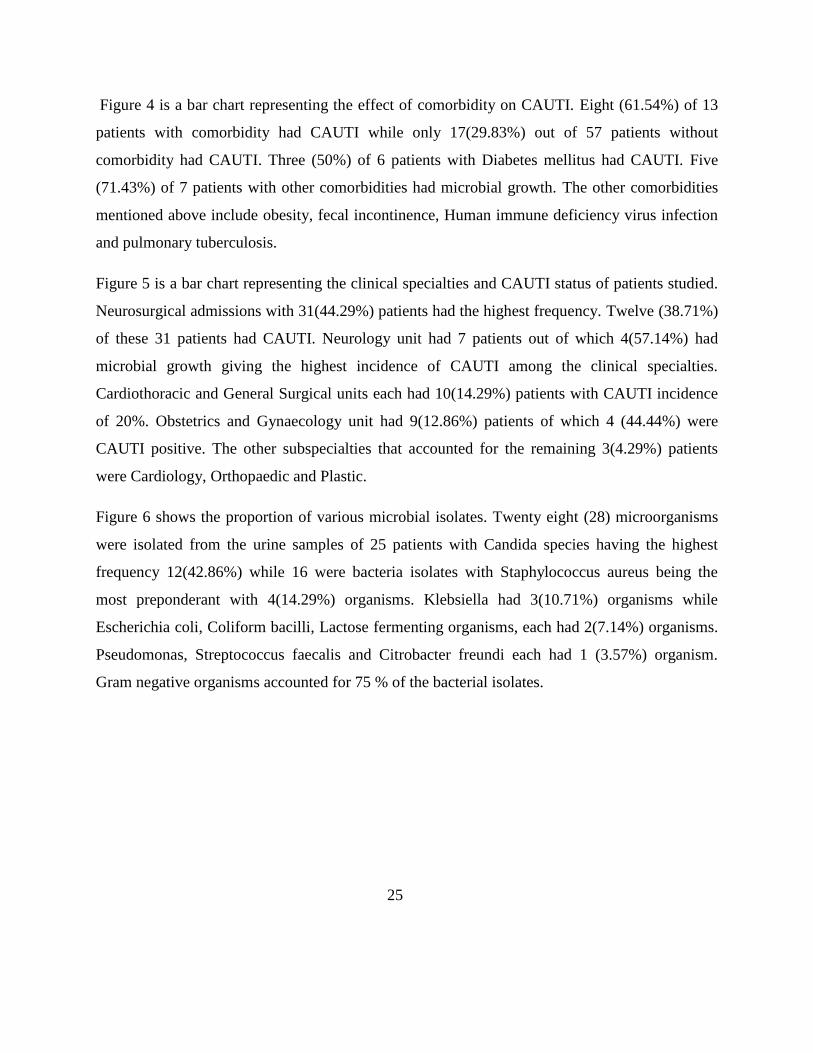
Figure 4 is a bar chart representing the effect of comorbidity on CAUTI. Eight (61.54%) of 13
patients with comorbidity had CAUTI while only 17(29.83%) out of 57 patients without
comorbidity had CAUTI. Three (50%) of 6 patients with Diabetes mellitus had CAUTI. Five
(71.43%) of 7 patients with other comorbidities had microbial growth. The other comorbidities
mentioned above include obesity, fecal incontinence, Human immune deficiency virus infection
and pulmonary tuberculosis.
Figure 5 is a bar chart representing the clinical specialties and CAUTI status of patients studied.
Neurosurgical admissions with 31(44.29%) patients had the highest frequency. Twelve (38.71%)
of these 31 patients had CAUTI. Neurology unit had 7 patients out of which 4(57.14%) had
microbial growth giving the highest incidence of CAUTI among the clinical specialties.
Cardiothoracic and General Surgical units each had 10(14.29%) patients with CAUTI incidence
of 20%. Obstetrics and Gynaecology unit had 9(12.86%) patients of which 4 (44.44%) were
CAUTI positive. The other subspecialties that accounted for the remaining 3(4.29%) patients
were Cardiology, Orthopaedic and Plastic.
Figure 6 shows the proportion of various microbial isolates. Twenty eight (28) microorganisms
were isolated from the urine samples of 25 patients with Candida species having the highest
frequency 12(42.86%) while 16 were bacteria isolates with Staphylococcus aureus being the
most preponderant with 4(14.29%) organisms. Klebsiella had 3(10.71%) organisms while
Escherichia coli, Coliform bacilli, Lactose fermenting organisms, each had 2(7.14%) organisms.
Pseudomonas, Streptococcus faecalis and Citrobacter freundi each had 1 (3.57%) organism.
Gram negative organisms accounted for 75 % of the bacterial isolates.
25

TABLE 1; Distribution of duration of Admission/ Catheterization and CAUTI Status
---------------------------------------------------------------------------------------------------------------------
DURATION CAUTI STATUS OF SUBJECTS Total
Positive (+) Negative (-)
48-72 hours (day 3-4) 4 (13.79%) 25(86.21%) 29(100.00%)
Day 5-7 21(51.22%) 20(48.78) 41(100.00%)
--------------------------------------------------------------------------------------------------------------------
TOTAL 25(35.71) 45(64.29%) 70(100.00%)
--------------------------------------------------------------------------------------------------------------------
X2 =10.363a while the p value =0.001
26

Table II: Antibiotic sensitivity pattern of bacterial isolates
Antibiotic Nit (%) Pen Qui Gen Tet Cep Col Ery Aug Imi Cot
Bacterial Isolate
Staph aureus (n=4) 4(100) 1(25.0) 1 (25.0)
Klebsiella (n=3) 1(33.3) 1 (33.3) 1 (33.33)
E coli (n=2) 2(100) 2 (100)
Coliform bacilli (n=2) 1(50) 2 (100) 1(50)
Lactose Fermenting
organism(n=2)
2(100) 2 (100)
Pseudomonas (n=1)
Streptococcus faecalis (n=1) 1(100) 1(100)
Citrobacter freundi n=1 1(100)
All Isolates n=16 11(68.75) 6 (37.50) 3(18.75) 3(18.75) 1(6.25)
Nit- Nitrofurantoin
Pen- Penicillins
Qui -Quinolones
Tet- Tetracycline
Gen-Gentamycin
Cep- Cephalosporins
Col- Colistin
Ery- Erythromycin
27
Aug-Augmentin
Imi- Imipenem
Cot- Cotrimoxazole
Table III: Antibiotic resistant pattern of bacterial isolates
Antibi
otic
Nit Pen Qui Gen Tet Cep Col Ery Aug Imi Cot
Bacterial
Isolate
Staph aureus
(n=4)
2 (50) 4 (100) 4 (100) 4(100) 1 (25) 1 (25) 3 (75) 2 (50)
Klebsiella
(n=3)
2(66.7) 1(33.3) 3(100) 3(100) 1(33.3) 3(100) 3(100) 1(33.3)
E coli (n=2) 2(100) 2(100) 2(100) 2(100)
Coliform
bacilli (n=2)
1 (50) 2 (100) 2 (100) 2 (100) 1 (50)
Lactose
Fermenting
organism(n=2)
2(100) 2(100) 2(100) 2(100) 2(100) 2(100) 2(100)
Pseudomonas
(n=1)
1(100) 1(100) 1(100) 1(100)
Streptococcus
faecalis (n=1)
1(100) 1(100)
Citrobacter
freundi (n=1)
1(100) 1(100) 1(100) 1(100) 1(100)
All Isolates
(n=16)
5(31.25) 6(37.50) 15(93.75) 4(25.00) 15(93.75) 1(6.25) 1(6.25) 11(68.75) 1(6.25) 5(31.25)
28
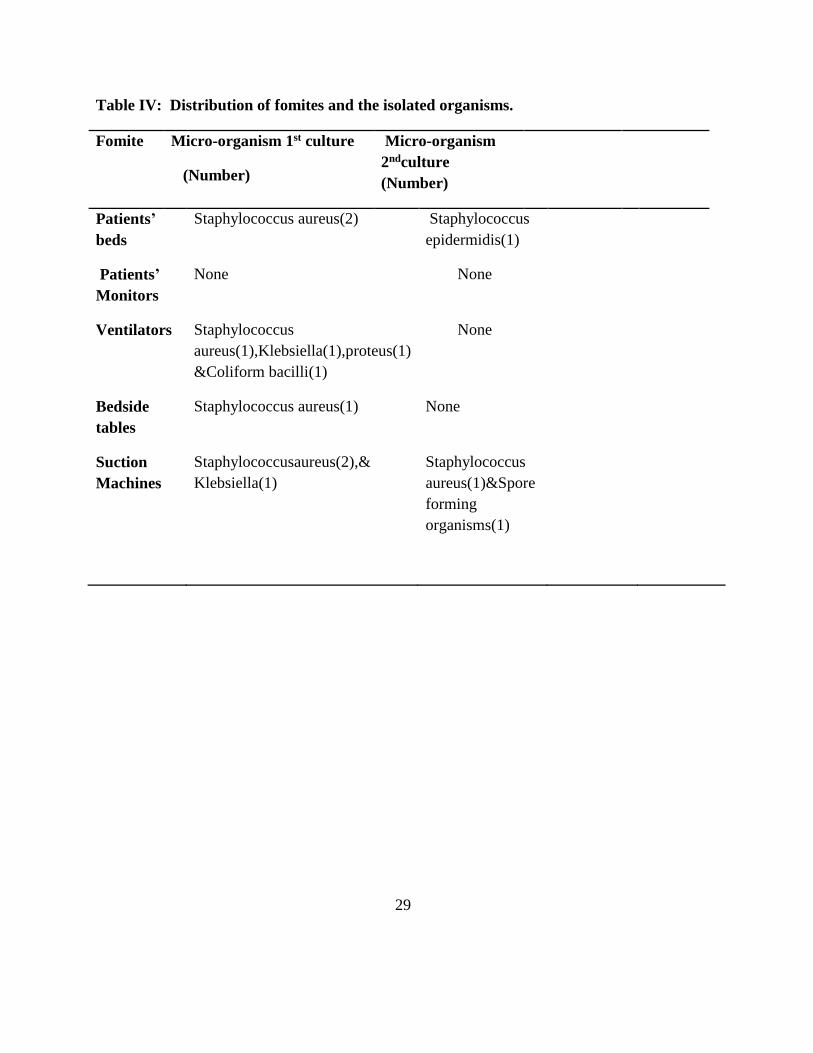
Table IV: Distribution of fomites and the isolated organisms.
Fomite Micro-organism 1st culture
(Number)
Micro-organism
2ndculture
(Number)
Patients’
beds
Staphylococcus aureus(2) Staphylococcus
epidermidis(1)
Patients’
Monitors
None None
Ventilators Staphylococcus
aureus(1),Klebsiella(1),proteus(1)
&Coliform bacilli(1)
None
Bedside
tables
Staphylococcus aureus(1) None
Suction
Machines
Staphylococcusaureus(2),&
Klebsiella(1)
Staphylococcus
aureus(1)&Spore
forming
organisms(1)
29
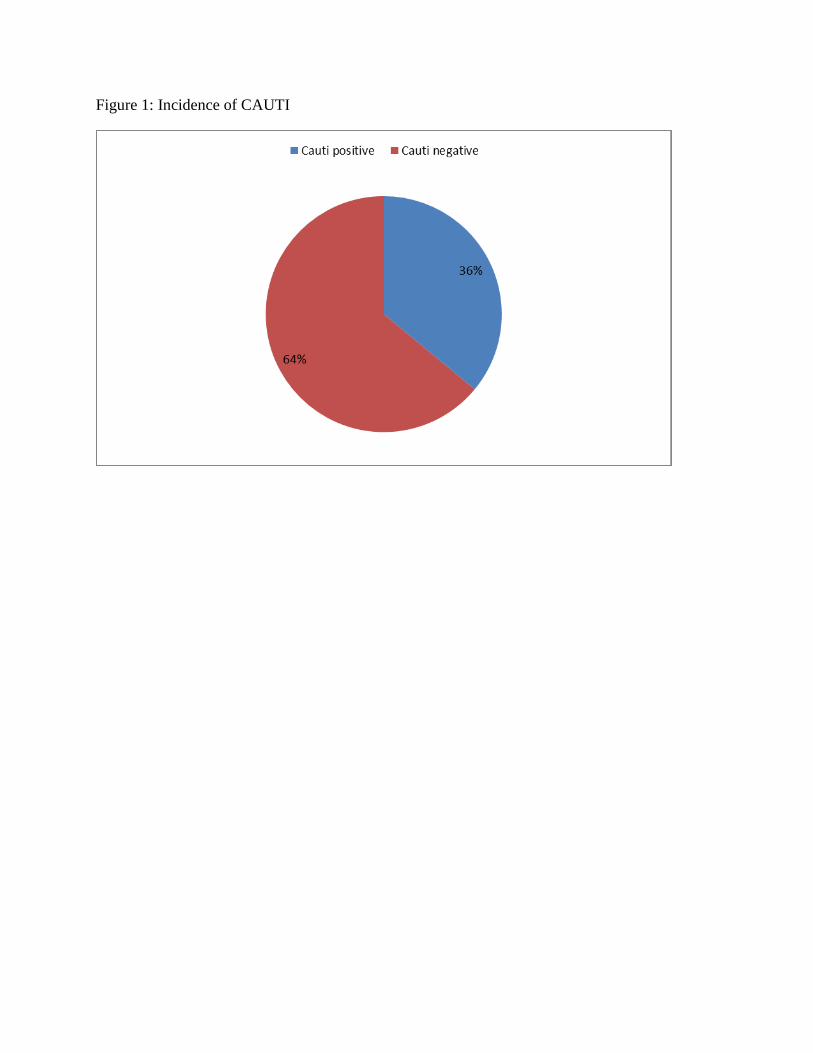
Figure 1: Incidence of CAUTI
30
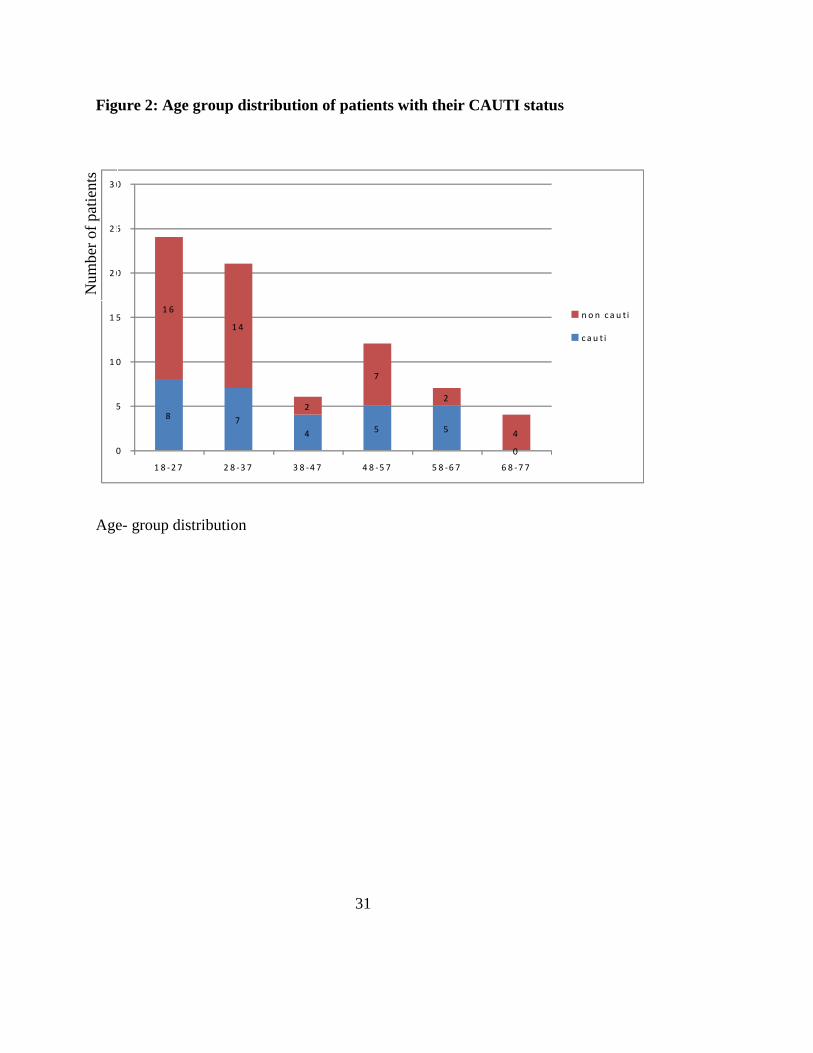
Figure 2: Age group distribution of patients with their CAUTI status
8 7
4 5 5
0
1 6
1 4
2
7
2
4
0
5
1 0
1 5
2 0
2 5
3 0
1 8 -2 7 2 8 -3 7 3 8 -4 7 4 8 -5 7 5 8 -6 7 6 8 -7 7
n o n c a u t i
c a u t i
Age- group distribution
31
Num
ber
of
pat
ients

Figure 3: Gender distribution of patients and CAUTI status
3 5
1 0
1 4
1 1
5
1 0
1 5
2 0
2 5
3 0
3 5
4 0
4 5
5 0
M a le F e m a le
C a u t i
N o c a u t i
Gender
32
Num
ber
of
pat
ients
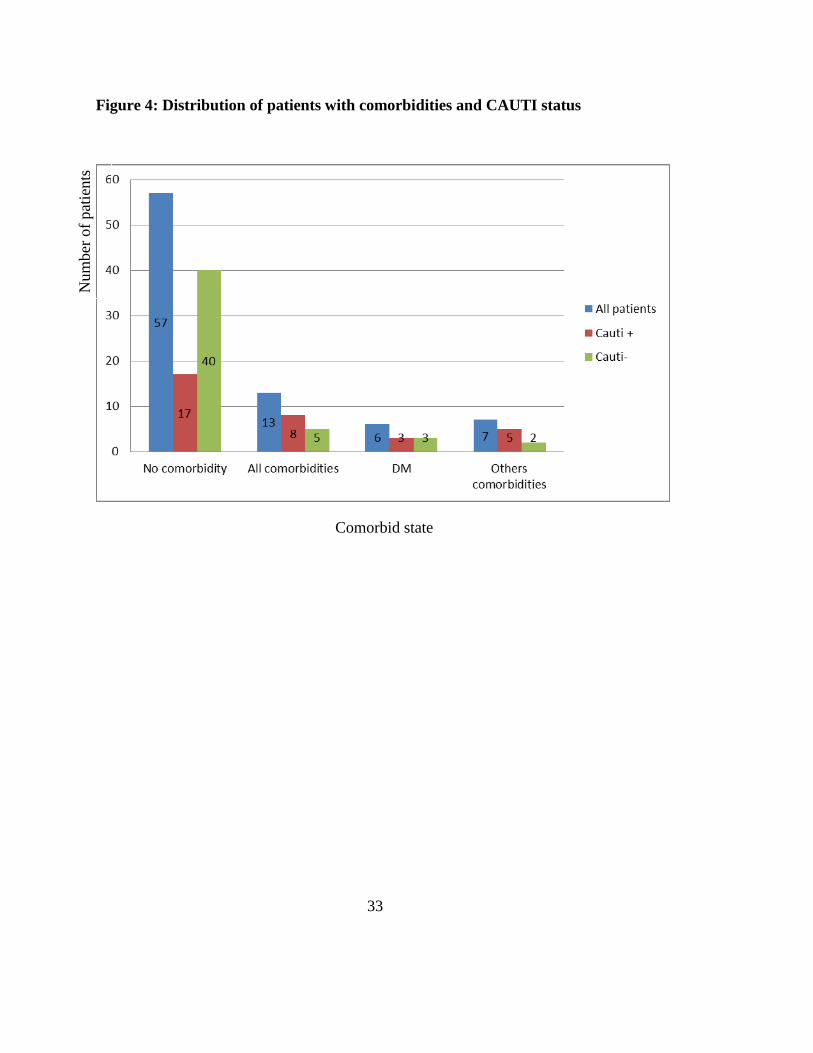
Figure 4: Distribution of patients with comorbidities and CAUTI status
Comorbid state
33
Num
ber
of
pat
ients

Figure 5: Clinical specialty distribution of subjects and CAUTI status
31 7 9 23
12 4
4 5
19 3
5 18
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Neurosurg Neurology O& G others
cauti-
cauti+
all patients
Clinical specialty
34
Per
centa
ge

Figure 6: Distribution of various microbial isolates
35
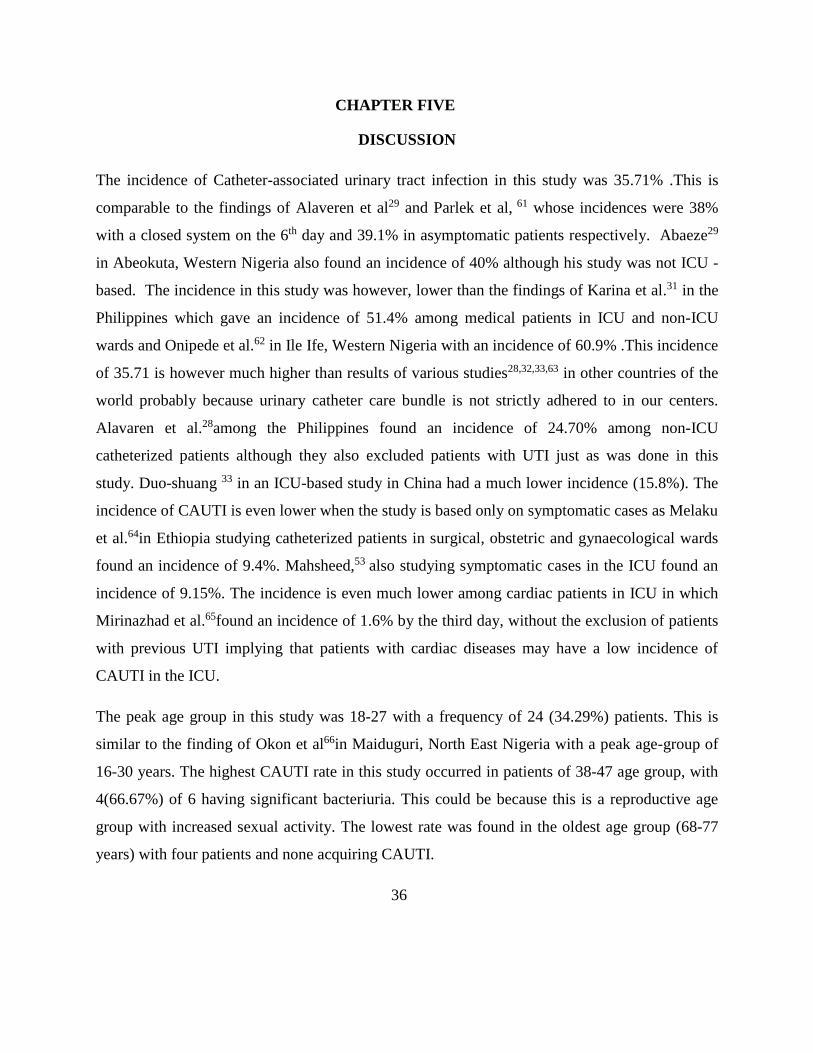
CHAPTER FIVE
DISCUSSION
The incidence of Catheter-associated urinary tract infection in this study was 35.71% .This is
comparable to the findings of Alaveren et al29 and Parlek et al, 61 whose incidences were 38%
with a closed system on the 6th day and 39.1% in asymptomatic patients respectively. Abaeze29
in Abeokuta, Western Nigeria also found an incidence of 40% although his study was not ICU -
based. The incidence in this study was however, lower than the findings of Karina et al.31 in the
Philippines which gave an incidence of 51.4% among medical patients in ICU and non-ICU
wards and Onipede et al.62 in Ile Ife, Western Nigeria with an incidence of 60.9% .This incidence
of 35.71 is however much higher than results of various studies28,32,33,63 in other countries of the
world probably because urinary catheter care bundle is not strictly adhered to in our centers.
Alavaren et al.28among the Philippines found an incidence of 24.70% among non-ICU
catheterized patients although they also excluded patients with UTI just as was done in this
study. Duo-shuang 33 in an ICU-based study in China had a much lower incidence (15.8%). The
incidence of CAUTI is even lower when the study is based only on symptomatic cases as Melaku
et al.64in Ethiopia studying catheterized patients in surgical, obstetric and gynaecological wards
found an incidence of 9.4%. Mahsheed,53 also studying symptomatic cases in the ICU found an
incidence of 9.15%. The incidence is even much lower among cardiac patients in ICU in which
Mirinazhad et al.65found an incidence of 1.6% by the third day, without the exclusion of patients
with previous UTI implying that patients with cardiac diseases may have a low incidence of
CAUTI in the ICU.
The peak age group in this study was 18-27 with a frequency of 24 (34.29%) patients. This is
similar to the finding of Okon et al66in Maiduguri, North East Nigeria with a peak age-group of
16-30 years. The highest CAUTI rate in this study occurred in patients of 38-47 age group, with
4(66.67%) of 6 having significant bacteriuria. This could be because this is a reproductive age
group with increased sexual activity. The lowest rate was found in the oldest age group (68-77
years) with four patients and none acquiring CAUTI.
36

Nineteen (37.26%) of 51 who were below 47 years had CAUTI while 6(31.58%) of 19 patients
who were above 47 also had CAUTI implying that CAUTI acquisition could be age-related as
already. In Kulkarni’s63study, 84% of the patients above 40 years had CAUTI which differs
from the findings of this study in which more of the younger age group acquired CAUTI and
four patients who were above 67 years old, although male were CAUTI-free. This is uncommon,
as elderly men are prone to prostatic hypertrophy with bladder outlet obstruction, which is a
major predisposing factor to the development of asymptomatic bacteriuria. In Abaeze’s study29,
the most affected age-group was 26-35years with 31.50% while the least affected age-group was
also the elderly 86-95 years (5.00%).This is somewhat similar to the findings of this study
probably because both were Nigerian-based studies and CAUTI distribution could be
geographical.
Significant bacteriuria occurred in 11 (52.40%) of 21 females and 14 (28.57%) of 49 males
This higher incidence of CAUTI in the female gender has been well documented.11,35,67,68 The
anatomy of the female urogenital tract predisposes her to the acquisition of CAUTI (the short
and wide urethra, which is close to the anus makes it susceptible to faecal contamination.) The
female urine is also said to have more suitable pH and osmolality for the growth of E coli.69
Certain studies have also shown a male preponderance to CAUTI. Mahshed et al53 had 75% of
CAUTI cases as male, Taiwo et al.52 also had a male preponderance. Older men are prone to
bladder outlet obstruction secondary to prostatic hyperplasia and malignancy and this
predisposes them to the acquisition of urinary tract infection.
Duration of catheterization was the only risk factor in this study which was statistically
significant. It is known as the most important modifiable risk factor in the acquisition of
CAUTI.15 Studies have shown that the daily risk for acquiring CAUTI is 3-6% and cumulatively
increases the longer the catheter remains in situ35,36 . By the 30th day of catheterization, infection
rates are close to 100%.9 This study showed that 4 (13.79%) patients had significant bacteriuria
by the 4th day while 25(35.71%) had acquired CAUTI by the 7th day. This is similar to the
findings of Karina et al.31 and Indranil et al.32 in which bacteriuria was 46.7% and 50%,
37
respectively by the 7th day but higher than the findings of Taiwo et al.52 who found an incidence
of 20% by the 7th day. This higher incidence may have resulted from the fact that this study was
ICU-based and CAUTI is commoner among critically ill patients. The result here is however
lower than that of Kulkarni et al.63in which 15(34.09%) had significant bacteriuria by the 3rd day
and 29 (65.90%) by the 7th day.
Neurosurgical unit had the highest frequency of admissions with 31(44.29%) patients, probably
because patients with severe traumatic brain injury are usually unconscious and are admitted into
the ICU for airway management and ventilatory support. They also had a high incidence of
CAUTI as 12(38.71%) had significant bacteriuria. This could be because unconscious patients
are usually catheterized for a longer duration predisposing them to the acquisition of CAUTI.
Neurology patients had the highest incidence of CAUTI with 4 (57.14%) of 6 having significant
bacteriuria probably because they are often incontinent and perineal care may not be optimal
leading to extra luminal ascent of bacteria into the bladder. Cardiology had the lowest in
frequency of admissions with only one patient (1.43%) who was also CAUTI-free.
Cardiothoracic unit had a total of 10(14.28%) patients with just 2 (20.00%) having significant
bacteriuria. Patients in cardiac ICU have been documented to have low incidence of CAUTI.66
Obese and faecal incontinent patients had 100% CAUTI each although the number was
insufficient to draw conclusions. Patients with Human immunodeficiency Virus (HIV) had
66.67% with significant bacteriuria. Diabetes mellitus is a known risk factor for the acquisition
of CAUTI. The 50% incidence of CAUTI in hyperglycaemic patients in this study is higher than
the finding in Kulkarni’s63 study which had 39% incidence. In patients with diabetes mellitus,
impaired granulocyte function, increased adherence of uropathogens to the bladder epithelium
and the effect of glucosuria on the growth of uropathogens in diabetic patients contribute to a
higher urinary tract infection prevalence.70The immunocompromised state which is characteristic
of these patients allows bacteriuria to easily extend into the upper urinary tract. Patients with
diabetes especially those admitted into the ICU with indwelling urethral catheters are more
susceptible to the development of urosepsis, thus these patients require strict blood glucose
monitoring to prevent occurrence and progression.70
38
The only obese patient in this study was a polytraumatised female who was also CAUTI positive,
It is documented that the incidence of UTI is 2.5-5 fold higher among obese individuals (BMI
≥30 kg/m2) than among the non-obese. Obese females are even at a higher risk.71.Obesity has
been shown to predispose to UTI after traumatic injury.72,73 Patients with faecal incontinence in
this study also showed 100% CAUTI incidence, probably because meatal contamination
occurred leading to extra luminal ascent of pathogens into the urinary tract. Patients who were
HIV seropositive showed an incidence of 66.67% of bacteriuria in this study. This was high and
could be as a result of immunosuppression, however Asharak et al 74and Park75 in their different
studies showed no significant association between HIV infection and UTI. Park75however found
an association between the viral load and UTI. It should however be noted that the number of
comorbid patients in this study was too small to draw a conclusion. A study with a larger sample
size should give a more reliable result.
Consistent with some other studies both in the developed76 and developing33,77 countries of the
world, Candida specie was the most frequent pathogen isolated in this study accounting for
42.87%. This is similar to the finding in a multicenter study in ICUs in Turkey which had
candida as the commonest pathogen responsible for CAUTI with a frequency of 44.9%.78 Risk
factors for Candiduria (as prevalent in this study) include the presence of indwelling urinary
catheters, use of antibiotics (as all our patients were on various antibiotics), older age, previous
surgery and the presence of diabetes mellitus39. Candiduria may not be associated with
candidaemia and most cases are asymptomatic and are usually benign and do not require local or
systemic antifungal therapy. The infection needs to be confirmed by a second sterile sample.
Mortality can be high particularly in debilitating patients. In a recent case control study39, it was
shown that the risk of developing candiduria was increased by 12-fold after urinary
catheterization, six fold after use of broad spectrum antibiotics, and urinary tract abnormalities.
The prevalence of candiduria varies in hospital settings and is most prevalent among patients in
ICU especially surgical ICU and in leukaemia and bone marrow transplant units43,44.In a
multicenter study in ICUs in Turkey the most common pathogens responsible for CAUTI were
Candida species with a frequency of 44.9% which is quite close to that found in this study.78
39

The most prevalent bacterial isolates in this study were Staphylococcus aureus with a frequency
of 4(25.00%), Klebsiella species with a frequency of 3(18.75), E coli, coliform bacilli and
lactose fermenting organisms with frequencies of 2(12.5%) each. This differs from previous
studies which had E coli37,40,73, Klebsiella52,53 and Pseudomonas79 as the commonest organisms.
Most of these organisms are part of the patients’ endogenous bowel flora and some may have
been acquired through cross contamination from fomites or health care givers. The presence of
Staphylococcus aureus could mean a systemic infection affecting the urinary tract from the
haematogenous route.
All the patients in our ICUs were on various antibiotics prophylactically. A total of nineteen
antibiotics belonging to different classes were tested in this study against sixteen bacterial
pathogens. Nitrofurantoin had the highest sensitivity being sensitive to 11(68.75%) organisms.
This is similar to the findings of Awolude80 in Ibadan, Western Nigeria, Okon et al.66 in Northern
Nigeria and Kalkurni63 where most of the organisms were highly sensitive to Nitrofurantoin
among other antibiotics. This finding differs from that of Onyegbule81 et al. where the pathogens
were more sensitive to Augmentin. It also differs from Taiwo’s finding48 where most of the
organisms were poorly sensitive to Nitrofurantoin. This implies that Nitrofurantoin would be
effective for empirical antibiotic therapy in our environment. Imipenem was sensitive to 1 of 2
organisms tested.This is similar to Kulkarni’s63finding.This study also showed 50.00% resistance
to Imipenem. The quinolones showed sensitivity to 6 (37.50%) of the bacterial isolates, E coli
was susceptible to only 30% of the antibiotics tested, it was however 100% susceptible to
nitrofurantoin. Fifteen (93.75%) of 16 isolated bacteria were resistant to both Gentamicin and
Cephalosporins. While 11(68.75%) were resistant to Augmentin. All four Staphylococcus
aureus, all three Klebsiella, and both E coli isolates were resistant to the quinolones, Gentamicin
and Cephalosporins. This high resistance pattern is similar to that of Duo-shuang33 where
resistance was 88.00%. Multiresistant pathogens are common in CAUTI as a result of the
presence of biofilms. Staphylococcus aureus was susceptible to only 4 (26.67%) of 15 antibiotics
groups tested. It was 100% susceptible to Nitrofurantoin, 25% sensitive to, Gentamicin and
Augmentin each. Pseudomonas was resistant to all antibiotics tested.
40

This is similar to the finding of Duo-shuang33where Pseudomonas showed absolute resistance to
Ciprofloxacin, Amikacin, Ceftazidine and even Imipenem. All six pathogens tested against the
penicillins including Amoxicillin were resistant to it while Amoxicillin with Clavulinic acid
(Augmentin) gave a sensitivity of 15.39% confirming that augmenting Amoxicillin with
Clavulinic acid improves its efficacy.
Antibiotic resistance is a problem in the Intensive Care Unit especially as related to the
challenge of biofilms in catheter-associated urinary tract infection. Biofilms provide a sustained
reservoir for microorganisms that after detachment can infect the patient. These biofilms cause
further problems if the bacterium (e g P mirabilis) produces the enzyme urease.82The urine
becomes alkaline causing the production of ammonium ions followed by crystallization of
calcium and magnesium phosphate within the urine. These crystals are then incorporated into the
biofilm resulting in encrustation and blockade of the catheter over a period of time. The complex
structures of the biofilms promote bacterial proliferation and protect the bacteria from
destruction by cleaners, antiseptics, antibiotics, and the host’s immune system.82 Bacteria within
a biofilm exhibit greater ability to communicate and exchange genetic information than do free-
floating (planktonic) bacteria. This communication is hypothesized to promote antibiotic
resistance and spread of the biofilm to other surfaces of the catheter and urinary epithelium.
Biofilms can begin to develop within the first 24 hours after catheterization and has been
reported to grow so thick as to block a catheter lumen.83 The presence of urinary catheter
biofilms has important implications for antimicrobial resistance, diagnosis, prevention and
treatment of CAUTI. In those patients who need an IUC for long term bladder management,
prevention of complications relies on adherence to catheter care policies.84,85,86,87,88
Antibiotic use in ICU should be based on escalation and de-escalation mechanism whereby the
provision of effective initial antibiotic is achieved while avoiding unnecessary antibiotic use that
would promote development of resistance. It is a key element within antimicrobial stewardship
programs and treatment paradigm for serious sepsis. The embodiment of de-escalation is that
based on microbiology results around day three therapy.
41
The empiric antibiotics that were started are stopped or reduced in number and or narrowed in
spectrum. De-escalation is clinically effective and appropriate.89
Six different species of pathogens that were isolated from fomites had a preponderance of
Staphylococcus aureus with 7 (53.85%) of 13 pathogens. This is similar to Ike’s90 study
conducted on fomites in ICU in Jos, Nigeria, where staphylococcus aureus was the most
preponderous isolate. This is quite significant as Staphylococcus aureus including Methicillin
Resistant Staphylococcus Aureus (MRSA), Enterococcus species including Vancomycin
Resistant Enterococcus (VRE) and Streptococcus pyogenes, are known to persist for months on
dry surfaces and so can be sources of cross infection in the ICU56. The gram negative organisms,
Klebsiella (15.39%), coliform bacilli (7.69%), isolated are also known to survive for months on
dry surfaces. Proteus vulgaris, Vibrio cholera, Bordetella pertussis and Haemophilis influenza
are known to persist for days on fomites. Spore forming bacteria which constituted 7.69% of the
isolates are also known to persist for months on fomites becoming continuous sources of
infection if appropriate preventive measures are not adopted.56The mode of transmission of
infection can be direct or indirect through the hand of health care givers but this is reduced by
50% through compliance to hand hygiene.56 The isolation of Staph aureus as the most prevalent
organism both from patient’s samples and fomites suggest the possibility of cross infection.
Candida species, though the most prevalent organisms isolated from the patients in this study
were absent from the fomites, probably because the disinfection methods which include use of
soap and water for organic decontamination, antiseptics like alcohol, chlorhexidine, and iodine,
used in these centers were effective against them. Gram negative bacteria have been described to
persist longer than gram positive bacteria.91Humid conditions improved the persistence of some
types of bacteria such as Chlamydia trachomatis92and E coli93.Staph aureus is known to persist
longer at low humidity94.Methicillin Resistance Staphylococcus Aureus ( MRSA) has improved
survival under low temperature (40 or 60).94 Some authors described a longer persistence on
plastics95,96 while others see a survival advantage on steel.97 Longer persistence has been
described with higher innocular96,in the presence of protein,91Serum91and Sputum98.These could
be the reason why suction machines and ventilators had the highest growth of organisms, as the
42

suction bottles often contain fluid with organic matter which may not be discarded immediately
after each use, encouraging the growth of microorganisms.
The humidifiers attached to ventilators also do contain moisture. Patients on mechanical
ventilators are prone to acquiring ventilator associated pneumonia which is a common
nosocomial infection in ICU. The absence of microbial growth on patient’s monitors and
minimal growth on side tables could be explained that disinfection of such surfaces was easier
and organic matter could easily be visualized and removed and such surfaces disinfected.
Infection control in ICU
Isolation, the separation of an infectious patient from other people is probably the oldest form of
infection control still practiced.99The aim of isolation precaution is to reduce the risk of the
spread of infection, before and after diagnosis, to susceptible individuals including health care
workers. Health care givers are required to adopt the universal infection control precautions
(UICP). This requires clinical staff to wear, and change gloves in clearly defined clinical
situations.100They are also required to make a risk assessment of when additional protective
clothing is required. Additional protective clothing comes into play for infections spread by
droplets or airborne, and some that spread by contact. The universal infection control precautions
involve hand washing and the use of gloves when handling blood, body fluids, and contaminated
materials. These precautions are to be applied to all patients receiving care in a hospital,
regardless of their diagnosis or presumed infection status. If used wisely it can limit the need for
single room isolation.
A single room with shut doors is intended to prevent the transmission of organisms spread by the
airborne route and to prevent gross contamination of the environment outside of the room with
certain organisms spread by contact.101,99 For non-air-borne infections requiring a single room, it
is preferable to keep the door closed. Confinement to a single room can be an unpleasant
experience .While it is necessary to restrict the patient, it also discourages staff from entering the
room. The patient can feel deprived of human contact, so a single room should not be used if
airborne transmission is unlikely or if there is little risk of heavy environmental contamination.
43

The architectural design of the ICU has little influence on the infection rate and the dry
environment example walls, and ceilings do not require any particular attention.102
44

CONCLUSION
It was evident in this study that incidence of Catheter- associated urinary tract infection in the
Intensive Care Unit in South Eastern Nigeria was 35.71%. Duration of catheterization was found
to be a major risk factor for CAUTI and was statistically significant. The most prevalent
organism associated with CAUTI in the ICUs studied was Candida species while the commonest
bacteria was Staphylococcus aureus which was also the most predominant isolate from fomites.
The most sensitive antibiotic against CAUTI in these ICUs was Nitrofurantoin which can be
used empirically while awaiting the result of culture and sensitivity although treatment for
asymptomatic bacteriuria is discouraged. The Suction machine was the highest source of
microbes in the ICU.
45

RECOMMENDATIONS
Institution guidelines for the placement of urinary catheters in the ICU should be implemented
and surveillance studies frequently conducted to ensure compliance.
Each patient on admission in the ICU should have a dedicated suction machine to minimize
cross-infection to other patients. Diligent decontamination of the suction machines by discarding
the fluid in bottle after each suctioning section and the use of single use suction catheters would
help to reduce the number of pathogens present on the suction apparatus thereby reducing
nosocomial infections.
There should be strict compliance to disinfecting the ventilator corrugated tubings after each
patient use to minimise cross-infection to the next patient using the ventilator. Disposable
corrugated tubings should be used for each patient.
Training and re-training of health care-givers on hand hygiene compliance would reduce the
incidence of HAI in the ICU.
There should be regular surveillance of nosocomial infection in the ICU.
46

LIMITATIONS OF THE STUDY
The sample of our study was relatively small. A similar study with a larger sample size would be
desirable.
All our patients were on antibiotics and this may have affected the result of the study.
47
REFERENCES
1. Aitkenhead A R. Principles of Intensive care. In: Nimmo W S. Smith G, editors. Anaesthesia.
Oxford: Blackwell Scientific Publications, 1990.1267-1300.
2. Garnes J S, Jarvis W R, Emori T G, Horan T C, Hughes J M. CDC Definitions for nosocomial
infection. Am J Infect Control 1988; 16:128-140.
3. Vincent J L, Bilian D J, Suter PM, Bruining H A, White J, Nicholas Chanoin M H, Wolff M,
Spencer R C, Hemmer M. The prevalence of nosocomial infection in intensive care units
in Europe. Results of the European prevalence of infection in intensive care unit (EPIC)
study. EPIC International Advisory Committee. JAMA 1995; 274:639-644.
4. Ak O, Batirel A, Ozer S, Colacoglu S. Nosocomial infections and risk factors in the intensive
care unit of a teaching and research hospital. A Prospective cohort study. Med Sc.
Monit.2011; 17: 24-29.
5. Esen S, Leblebicioglu H. Prevalence of nosocomial infections at Intensive Care Units in
Turkey. A multicenter one day point prevalence study. Scan J Infect Dis 2004;36:144-
148
6. Legras A. Malvy D, Quinioux A I, Villers D, Bouachour G, Robert R, Thomas R. Nosocomial
infections: Prospective Survey of incidence in five French Intensive care units. Intensive
care Med. 1998; 24: 1040-1046.
7. Ledoux D, Luckart H, Cardiac Surgery. Cardiac Nursing 4th ed. Philadelphia; Lippincot
Williams and W Wilkins; 2000:580-613.
8. Allen Bridson K. Using the National Health Care Safety Network (NHSN) for CAUTI
Surveillance.2011;[email protected];accessed on 18th July, 2012.
9. Apisarnthanark A, Rutjunawech S, Wichansaw, Wakuns et al. Initial inappropriate Urinary
catheter use in a tertiary Care Centre; Incidence, risk factors and outcomes. Am J Infect
control. 2007; 39 (9):594-599.
10. Platt R, Polk BF, Murdock B, Rosner B. Mortality associated with nosocomial urinary tract
infection. N Engl J of Med. 1982; 307, 637-642.
11. Chukwuocha U M, Dozie U W, Nwawume I O. Bacteriuria in patients with indwelling
Urethral catheter in Owerri Municipality. Afr J Microbiol Res. 2011; 5(9):990-995.
48

12. Ige I A , Asuzu M C. Hospital acquired infections in a Nigerian Tertiary Health Facility.
An audit of surveillance reports. Nig Med. J 2011; 52:239-247.
13. Rosenthal ND, Maki DG, Salomao R, Morero CA, Meyta Y, Hignera F, Cuella LE, Arican
OA, Abougal Leblebicioglu H; International Nosocomial Infection control. Device
associated nosocomial infection in 55 ICUs of 8 developing countries. Annals Intern
Med. 2006 Oct 17; 145(8):582-591.
14. Klevens RM, Edward JR. Richard CL Jr, Horan T C,Gaynes R P,Pollock D A, et al.
Estimating health care associated Infections and deaths in US hospitals 2002. Public
health reports 2007; 122(2): 160-166.
15. Markler A. Urinary catheter care in the intensive care unit. Nurs Crit care 2004; 9(1):21-
27.
16. Saint S, Wiese J Amory JK, et al. Are physicians aware of which of their patients have
indwelling urinary catheters? Am J med 2000; 109: 476-480.
17.Okafor UV Challenges in Critical Care Services in Sub-Saharan Africa. Perspectives from
Nigeria. Indian J Crit Care Med 2009; 13:25-27.
18.Kruger JN, Kaeser DL, Wenzel RP. Nosocomial UTI; Secular trends, treatment and
economics in a university hospital. J Urology 1983; 130:102-106
19. Schaeffer A I, Schaeffer E M, Wein A J, Kavouissi LR, Novick AC, Partin A W, Peters CA,
eds. Infections of the urinary tract. Urology 9th edition. Philadelphia PA. Sanders,
2007:223-303.
20. Costel EE, Mitchell S, Kaiser AB. Abbreviated surveillance of nosocomial urinary tract
infections, a new approach. Infect Control 1985;6: 11-13.
21. Rubin RH, Shapino ED, Andriole VT, Davis R J. Stamm W E. Evaluation of new anti-
infective drugs for the treatment of urinary tract infection. Clin Infect Dis.
1992;15(supple1):216-227.
22. Hootom TM, Bradly S F, Cardenas D D,Colgan R, Geerlings S E,Rice J C, et al. Diagnosis,
Prevention and treatment of CA-UTI in adults: 2009 International clinical practice
guidelines from the infective Disease society of America. Clin infect Dis 2010; 50(5):
625-663.
23. Stamm W E. Measurement of pyuria and its relation to bacteriuria. Am J of Med. 1983;
75(supple IB): 53-58.
49
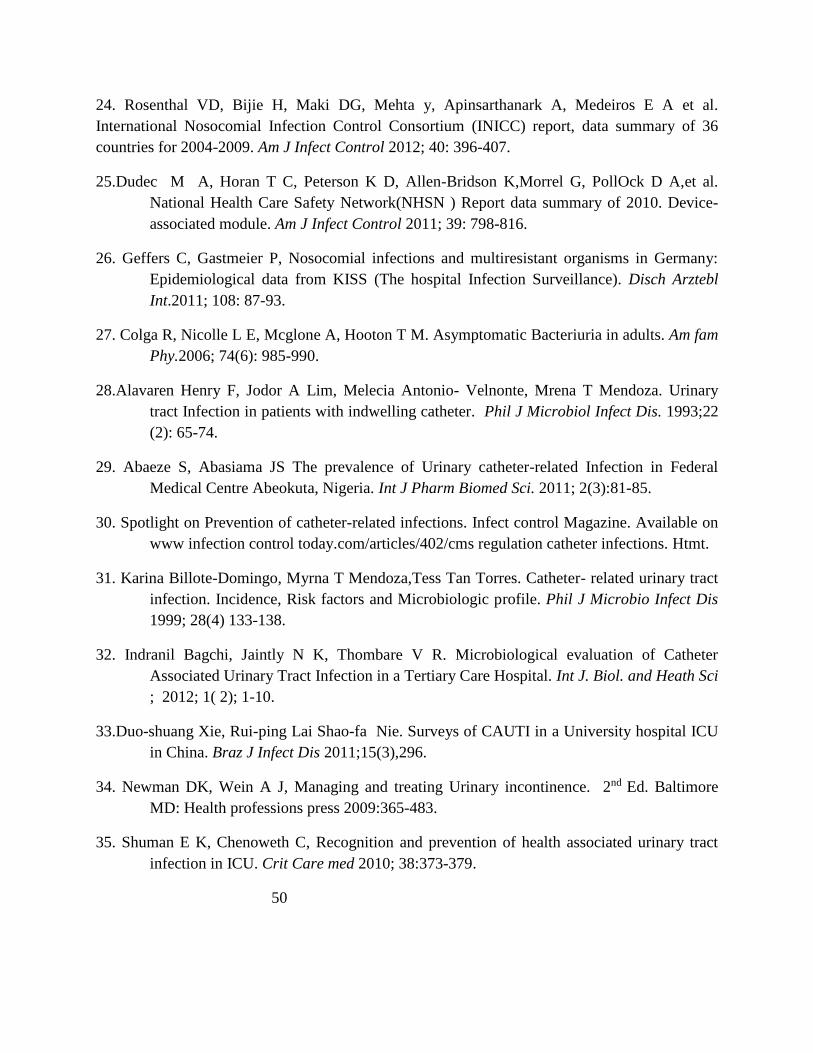
24. Rosenthal VD, Bijie H, Maki DG, Mehta y, Apinsarthanark A, Medeiros E A et al.
International Nosocomial Infection Control Consortium (INICC) report, data summary of 36
countries for 2004-2009. Am J Infect Control 2012; 40: 396-407.
25.Dudec M A, Horan T C, Peterson K D, Allen-Bridson K,Morrel G, PollOck D A,et al.
National Health Care Safety Network(NHSN ) Report data summary of 2010. Device-
associated module. Am J Infect Control 2011; 39: 798-816.
26. Geffers C, Gastmeier P, Nosocomial infections and multiresistant organisms in Germany:
Epidemiological data from KISS (The hospital Infection Surveillance). Disch Arztebl
Int.2011; 108: 87-93.
27. Colga R, Nicolle L E, Mcglone A, Hooton T M. Asymptomatic Bacteriuria in adults. Am fam
Phy.2006; 74(6): 985-990.
28.Alavaren Henry F, Jodor A Lim, Melecia Antonio- Velnonte, Mrena T Mendoza. Urinary
tract Infection in patients with indwelling catheter. Phil J Microbiol Infect Dis. 1993;22
(2): 65-74.
29. Abaeze S, Abasiama JS The prevalence of Urinary catheter-related Infection in Federal
Medical Centre Abeokuta, Nigeria. Int J Pharm Biomed Sci. 2011; 2(3):81-85.
30. Spotlight on Prevention of catheter-related infections. Infect control Magazine. Available on
www infection control today.com/articles/402/cms regulation catheter infections. Htmt.
31. Karina Billote-Domingo, Myrna T Mendoza,Tess Tan Torres. Catheter- related urinary tract
infection. Incidence, Risk factors and Microbiologic profile. Phil J Microbio Infect Dis
1999; 28(4) 133-138.
32. Indranil Bagchi, Jaintly N K, Thombare V R. Microbiological evaluation of Catheter
Associated Urinary Tract Infection in a Tertiary Care Hospital. Int J. Biol. and Heath Sci
; 2012; 1( 2); 1-10.
33.Duo-shuang Xie, Rui-ping Lai Shao-fa Nie. Surveys of CAUTI in a University hospital ICU
in China. Braz J Infect Dis 2011;15(3),296.
34. Newman DK, Wein A J, Managing and treating Urinary incontinence. 2nd Ed. Baltimore
MD: Health professions press 2009:365-483.
35. Shuman E K, Chenoweth C, Recognition and prevention of health associated urinary tract
infection in ICU. Crit Care med 2010; 38:373-379.
50
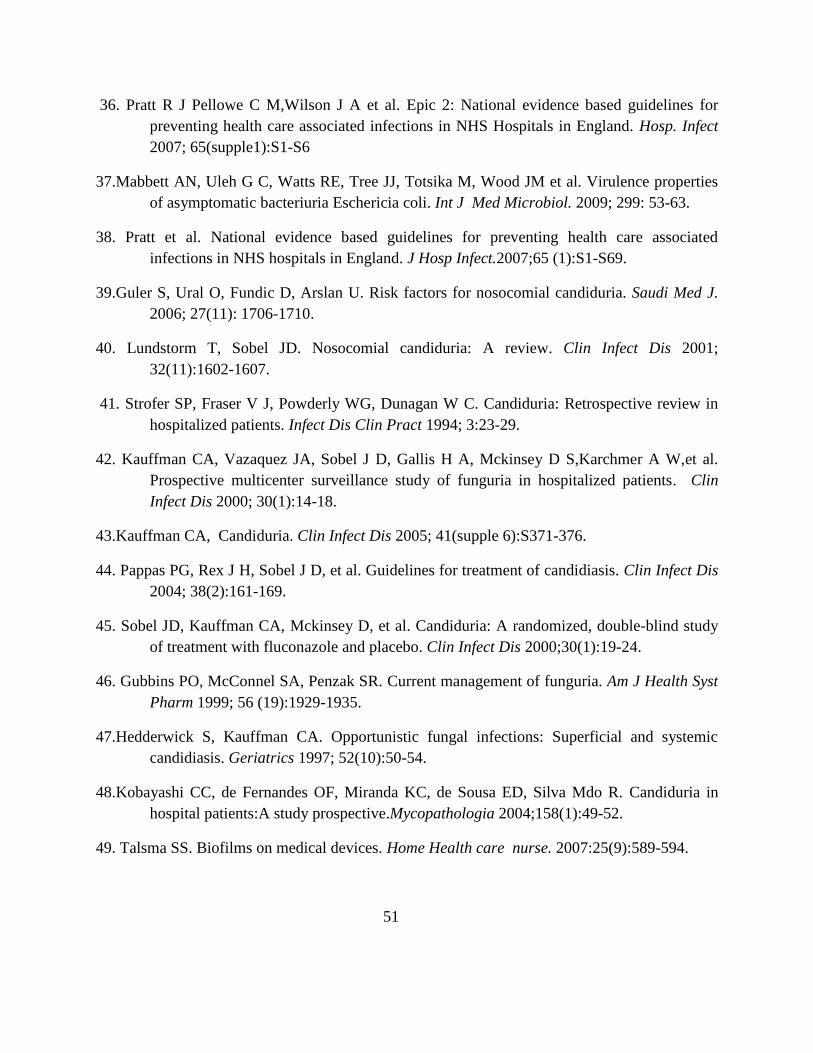
36. Pratt R J Pellowe C M,Wilson J A et al. Epic 2: National evidence based guidelines for
preventing health care associated infections in NHS Hospitals in England. Hosp. Infect
2007; 65(supple1):S1-S6
37.Mabbett AN, Uleh G C, Watts RE, Tree JJ, Totsika M, Wood JM et al. Virulence properties
of asymptomatic bacteriuria Eschericia coli. Int J Med Microbiol. 2009; 299: 53-63.
38. Pratt et al. National evidence based guidelines for preventing health care associated
infections in NHS hospitals in England. J Hosp Infect.2007;65 (1):S1-S69.
39.Guler S, Ural O, Fundic D, Arslan U. Risk factors for nosocomial candiduria. Saudi Med J.
2006; 27(11): 1706-1710.
40. Lundstorm T, Sobel JD. Nosocomial candiduria: A review. Clin Infect Dis 2001;
32(11):1602-1607.
41. Strofer SP, Fraser V J, Powderly WG, Dunagan W C. Candiduria: Retrospective review in
hospitalized patients. Infect Dis Clin Pract 1994; 3:23-29.
42. Kauffman CA, Vazaquez JA, Sobel J D, Gallis H A, Mckinsey D S,Karchmer A W,et al.
Prospective multicenter surveillance study of funguria in hospitalized patients. Clin
Infect Dis 2000; 30(1):14-18.
43.Kauffman CA, Candiduria. Clin Infect Dis 2005; 41(supple 6):S371-376.
44. Pappas PG, Rex J H, Sobel J D, et al. Guidelines for treatment of candidiasis. Clin Infect Dis
2004; 38(2):161-169.
45. Sobel JD, Kauffman CA, Mckinsey D, et al. Candiduria: A randomized, double-blind study
of treatment with fluconazole and placebo. Clin Infect Dis 2000;30(1):19-24.
46. Gubbins PO, McConnel SA, Penzak SR. Current management of funguria. Am J Health Syst
Pharm 1999; 56 (19):1929-1935.
47.Hedderwick S, Kauffman CA. Opportunistic fungal infections: Superficial and systemic
candidiasis. Geriatrics 1997; 52(10):50-54.
48.Kobayashi CC, de Fernandes OF, Miranda KC, de Sousa ED, Silva Mdo R. Candiduria in
hospital patients:A study prospective.Mycopathologia 2004;158(1):49-52.
49. Talsma SS. Biofilms on medical devices. Home Health care nurse. 2007:25(9):589-594.
51

50.Newman D. The indwelling urinary catheter. Principles for best practice. J Wound ostomy
and continence Nursing. 2007; 24(6):655-661.
51.Ekrem Temiz, Nihal Piskin,Hande Aydemir,Nefise Oztopak, Deniz Akduman,Guven Celebi
and Kokturk. Factors associated with catheter associated urinary tract Infections and
the effects of other Concomitant nosocomial infections in intensive care. Scand. J of
Infect Dis 2012; Vol 44 (5) 344-349.
52.Taiwo SS, Aderuomu A. Catheter associated Urinary tract infection Aetiological agents and
antimicrobial susceptibility in Ladoke Akintola University Teaching Hospital Oshogbo
Nigeria. AJ BR 2006;9:141-148.
53 . Mahshid Talebi Taher, Ali Golespin pour, Symptomatic nosocomial urinary tract infection
in ICU patients. Identification of microbiologic resistance pattern. Iranian J of Clin
Infect. Dis 2009; 4(1):25-29.
54. Mindy K X, Joice Y C Lee, Ian Y J Wee, Helen M L Oh. Evaluation of ICU-acquired UTI
in Singapore. Ann Acad Med Singapore 2010; 39: 460-465.
55. Sehulster L.M, Chrinn RYW, Ardurin M.I et al. Guidelines for environmental Infection
Control in healthcare facilities 2003.Recommendations from CDC and the Health Care
Infection Control Practices Advisory Committee.
56. Kramer A, SwebbleL, Kampt G, How long do nosocomial pathogens persist on inanimate
surfaces? A systemic review. BMC Infect Dis 2006; 6:130.
57. Sing-on Teng, Wensenlee, Tsong-Yih O, Yu-chia Hsieh,Wuan-Lee, Yi-Chun Lin. Bacterial
contamination of patients’ medical charts in a surgical ward and the intensive care unit :
impact on nosocomial infections. J Microbiol Immunol Infect .2009; 42:86-91.
58. Tambekar D H,Shirsat S D. Handwashing; A cornerstone to prevent transmission of
Diarrhoeal Infection. Asian J of Med Sci (2009)1(3):100-103
59. Blouin AS. Helping to solve health care most critical safety and quality problems. J Nurs
Care Qual. 2010; 25: 95-99.
60.Boyce JM, Pittet D, et al. Guideline for Hand Hygiene in Health-Care Settings:
recommendations of the Healthcare Infection Control Practices Advisory Committee
and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Infect Control Hosp
Epidemiol 2002; 23:3-40.
52
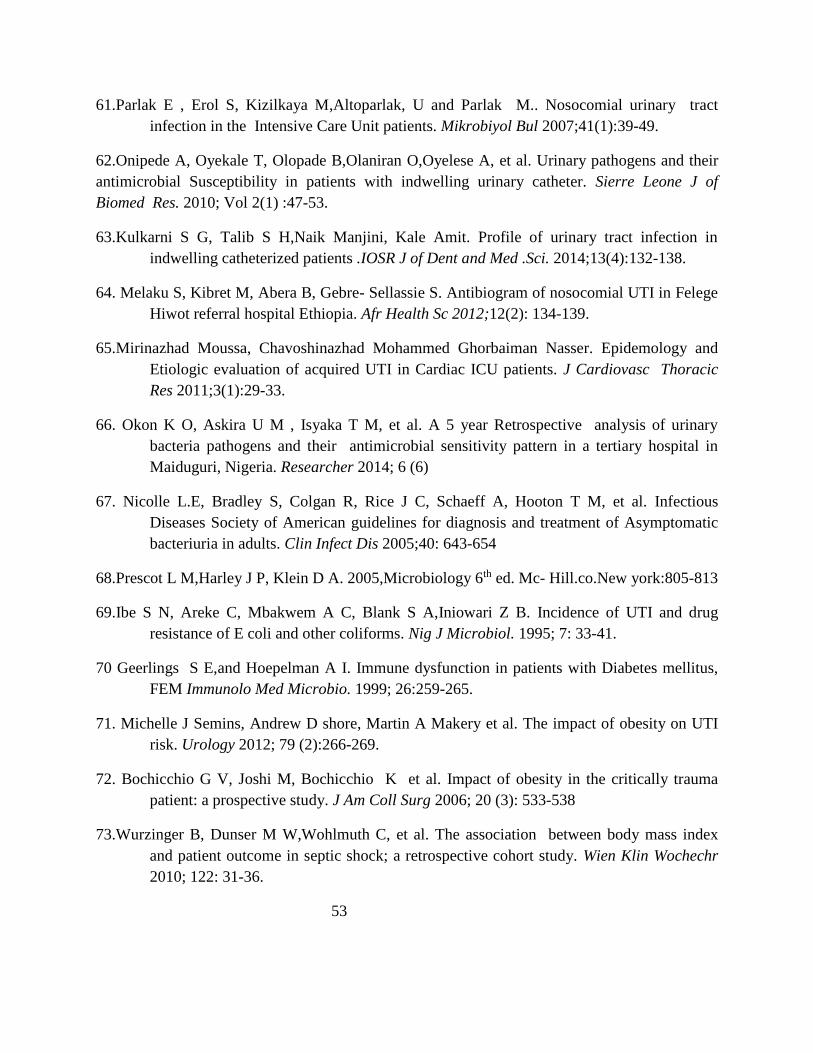
61.Parlak E , Erol S, Kizilkaya M,Altoparlak, U and Parlak M.. Nosocomial urinary tract
infection in the Intensive Care Unit patients. Mikrobiyol Bul 2007;41(1):39-49.
62.Onipede A, Oyekale T, Olopade B,Olaniran O,Oyelese A, et al. Urinary pathogens and their
antimicrobial Susceptibility in patients with indwelling urinary catheter. Sierre Leone J of
Biomed Res. 2010; Vol 2(1) :47-53.
63.Kulkarni S G, Talib S H,Naik Manjini, Kale Amit. Profile of urinary tract infection in
indwelling catheterized patients .IOSR J of Dent and Med .Sci. 2014;13(4):132-138.
64. Melaku S, Kibret M, Abera B, Gebre- Sellassie S. Antibiogram of nosocomial UTI in Felege
Hiwot referral hospital Ethiopia. Afr Health Sc 2012;12(2): 134-139.
65.Mirinazhad Moussa, Chavoshinazhad Mohammed Ghorbaiman Nasser. Epidemology and
Etiologic evaluation of acquired UTI in Cardiac ICU patients. J Cardiovasc Thoracic
Res 2011;3(1):29-33.
66. Okon K O, Askira U M , Isyaka T M, et al. A 5 year Retrospective analysis of urinary
bacteria pathogens and their antimicrobial sensitivity pattern in a tertiary hospital in
Maiduguri, Nigeria. Researcher 2014; 6 (6)
67. Nicolle L.E, Bradley S, Colgan R, Rice J C, Schaeff A, Hooton T M, et al. Infectious
Diseases Society of American guidelines for diagnosis and treatment of Asymptomatic
bacteriuria in adults. Clin Infect Dis 2005;40: 643-654
68.Prescot L M,Harley J P, Klein D A. 2005,Microbiology 6th ed. Mc- Hill.co.New york:805-813
69.Ibe S N, Areke C, Mbakwem A C, Blank S A,Iniowari Z B. Incidence of UTI and drug
resistance of E coli and other coliforms. Nig J Microbiol. 1995; 7: 33-41.
70 Geerlings S E,and Hoepelman A I. Immune dysfunction in patients with Diabetes mellitus,
FEM Immunolo Med Microbio. 1999; 26:259-265.
71. Michelle J Semins, Andrew D shore, Martin A Makery et al. The impact of obesity on UTI
risk. Urology 2012; 79 (2):266-269.
72. Bochicchio G V, Joshi M, Bochicchio K et al. Impact of obesity in the critically trauma
patient: a prospective study. J Am Coll Surg 2006; 20 (3): 533-538
73.Wurzinger B, Dunser M W,Wohlmuth C, et al. The association between body mass index
and patient outcome in septic shock; a retrospective cohort study. Wien Klin Wochechr
2010; 122: 31-36.
53
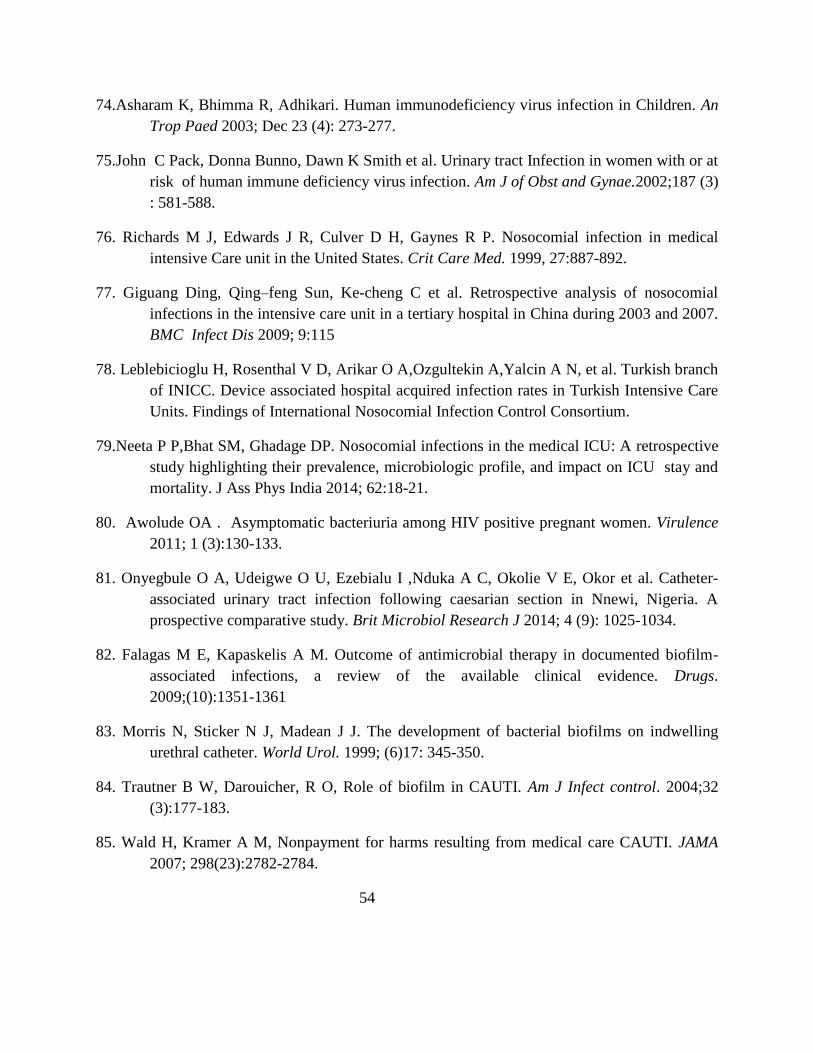
74.Asharam K, Bhimma R, Adhikari. Human immunodeficiency virus infection in Children. An
Trop Paed 2003; Dec 23 (4): 273-277.
75.John C Pack, Donna Bunno, Dawn K Smith et al. Urinary tract Infection in women with or at
risk of human immune deficiency virus infection. Am J of Obst and Gynae.2002;187 (3)
: 581-588.
76. Richards M J, Edwards J R, Culver D H, Gaynes R P. Nosocomial infection in medical
intensive Care unit in the United States. Crit Care Med. 1999, 27:887-892.
77. Giguang Ding, Qing–feng Sun, Ke-cheng C et al. Retrospective analysis of nosocomial
infections in the intensive care unit in a tertiary hospital in China during 2003 and 2007.
BMC Infect Dis 2009; 9:115
78. Leblebicioglu H, Rosenthal V D, Arikar O A,Ozgultekin A,Yalcin A N, et al. Turkish branch
of INICC. Device associated hospital acquired infection rates in Turkish Intensive Care
Units. Findings of International Nosocomial Infection Control Consortium.
79.Neeta P P,Bhat SM, Ghadage DP. Nosocomial infections in the medical ICU: A retrospective
study highlighting their prevalence, microbiologic profile, and impact on ICU stay and
mortality. J Ass Phys India 2014; 62:18-21.
80. Awolude OA . Asymptomatic bacteriuria among HIV positive pregnant women. Virulence
2011; 1 (3):130-133.
81. Onyegbule O A, Udeigwe O U, Ezebialu I ,Nduka A C, Okolie V E, Okor et al. Catheter-
associated urinary tract infection following caesarian section in Nnewi, Nigeria. A
prospective comparative study. Brit Microbiol Research J 2014; 4 (9): 1025-1034.
82. Falagas M E, Kapaskelis A M. Outcome of antimicrobial therapy in documented biofilm-
associated infections, a review of the available clinical evidence. Drugs.
2009;(10):1351-1361
83. Morris N, Sticker N J, Madean J J. The development of bacterial biofilms on indwelling
urethral catheter. World Urol. 1999; (6)17: 345-350.
84. Trautner B W, Darouicher, R O, Role of biofilm in CAUTI. Am J Infect control. 2004;32
(3):177-183.
85. Wald H, Kramer A M, Nonpayment for harms resulting from medical care CAUTI. JAMA
2007; 298(23):2782-2784.
54

86.Gould C V, Umschield C A, Agarwal R K, Kuntz G, Pegnez D A. Healthcare infection
control practices Advisory committee. Guideline for prevention of CAUTI,2009. Infect
Control Hosp Epidermiol. 2010; 31 (4):319-326.
87. Gray M L, securing the indwelling urinary catheter. Am J of Nurs.2008; 108(12):44-50.
88. Lo Nicolle L, Classen D. Strategies to prevent CAUTI in acute care hospitals. Infect control
Hosp Epidermiol.2008;29(supple1) S41-S50.
89.Masterton R G. Crit care clin 2011; 27(1): 149-162.
90.Ikeh E I ,Erdoo I. Bacterial flora on fomites in a Nigerian Multidisciplinary Intensive Care
Unit. Lab Medicine 2011;42:411-413.
91.Hirai Y; Survival of bacteria under dry conditions from a view point of nosocomial infections.
J Hosp Infect.1991;19: 191-200.
92.Novak K D,Kowalski R P, Karenchak L M, Gordon Y J: Chlamydia trachomatis can be
transmitted by a non porous plastic surface in vitro. Cornea 1995;14: 523-526.
93.William A P, Avery L M, Killham K, Jones DL,: Persistence of Escherichia coli 0157 on
farm surfaces under different environmental conditions. J Applied Microbiol 2005;98:
1075-1083.
94. Noyce J O, Michels H, Keenl C W:Potential use of copper surfaces to reduce survival of
Methicillin Resistant Staphylococcus Aureus in the health care environment. J Infect
Cont 2006;63: 289-297.
95. Perez J L, Gomez E, Sauca G. Survival of gonococci from urethral discharge on formites.
Eur J Clin Microbiol and Infect Dis 1990;1:54-55.
96. Neely, A N. A survey of gram negative bacterial survival on hospital fabrics and plastics. J of
Burn Care and Rehab 2000;21: 523-527.
97. Webster C, Towner K J, Humphret S H, Survival of Acinobacter on three clinically related
inanimate surfaces. Infect Control Hosp Epidem 2000
98. Smith C R; Survival of tubercle bacilli: the viability of dried tubercle bacilli in unfiltered
roomlight and in the refrigerator. Am Rev of Tubercl.1942;5: 334-345.
99. Meers P, Jacobson W, McPherson M, Hospital infection control for Nurses.1st ed. London:
Chapman and Hall,1992.
55
100. Centers for disease control. Update: universal precautions for prevention of transmission of
immunodeficiency virus, hepatitis B virus, and other blood borne pathogens in health
care settings. MMWR 1988; 37:377-388.
101. Hospital Acquired Infection Control. 1st ed. Oxford University Press,1992.
102. Heubner J,Frank U, Kappstein, I . Influence of architectural design on nosocomial
infections in intensive care units: a 2 year analysis. Int Care Med 1988;15: 179-183.
56

APPENDIX I
Data collection form
Study Title;
Catheter associated urinary tract infection in ICU; Incidence, Risk factors and Microbiological
profile.
Date;
A. Patient’s demography and physical Data
Name;--------------------------------------------------
Hosp no;-------------------------------------------
Age in years;-----------------------------------------
Sex ; --------------------------------------------------
Diagnosis;-------------------------------------------------------------
B. ICU Admission.
Date of admission into ICU-----------------------------------------
Indication for ICU admission-------------------------------------------
Source of admission; A/E ; Theatre; Ward
Antibiotic therapy: Yes ; No
Baseline vital signs on admission; Pulse rate Bp Temp.-
C. Urethral catheterization history;
Date of 1st catheterization –; Place of catheterization:
Date of 1st change of catheter (if changed)
- Reason for change of catheter.
57
D. Co- morbid state
Diabetes mellitus Yes ; No
Immuno compromised Yes ; No
Steroid Therapy Yes ; No
Antibiotics Yes ; No
E. Urine culture
1st sample ; ( Within 24 hours of ICU admission)
Results: Growth ; Yes ; No
Organisms grown; Sensitivity pattern;
2nd sample (48 to 72 hours of ICU admission)
Results: Growth Yes ; No
Microorganisms grown with sensitivity pattern.
3rd sample (5-7days of ICU admission).
Exact day; Day 5; Day 6 ; Day 7
Results: Growth; No Yes
Microorganisms grown with sensitivity pattern;
E. Evidence of bacteremia: Yes; No
If yes
Vital sign changes; Pulse - Temp.-
Blood culture result: Growth Yes No
Microorganisms and their sensitivity pattern.
58
Full blood count
WBC; Total : Differentials
ICU FORMITES FOR CULTURE. Organism (s) grown
Suction Machine:
Ventilator:
Side table:
Patient’s bed:
Patient’s monitor;
59
APPENDIX II
Patient Informed Consent
Dear patient,
You are being asked to participate in a research study. In order to decide whether or not you
should agree to be part of this research study, you should understand enough about the research
to make an informed judgment.
This consent form gives detailed information about the study which the investigator will discuss
with you. Once you understand this you will be asked to sign this form if you wish to participate.
The research being proposed to you is;
Catheter associated urinary tract infection in the ICU; incidence, risk factors and
microbiologic profile.
Purpose of the study:
The purpose of this study is to ascertain how the use of an indwelling urinary catheter in the ICU
contributes to acquiring urinary tract infection.
Description of the Study Procedures;
You are admitted into the ICU because you are critically ill and your body needs close
monitoring for a good outcome. Among these includes the insertion of a urinary catheter to
monitor your urine output which help us to know how your kidneys are functioning. This
catheter will be allowed to stay as long as it is needed. There may be need to change it whenever
we deem fit for your own good. Your urine sample will be examined about three times to check
for evidence of urinary tract infection contracted while in the ICU.
Risks; Your participation in this study will not expose you to further risks outside your illness.
Confidentiality: All the information obtained will be treated as confidential.
60

Benefits: You will not be required to pay an extra cost for the investigations.
The result of the study will also help in better management of yourself and other patients in the
ICU.
You are at liberty to withdraw from this research if you so wish.
Feedback: The researcher will be available at any time to answer your questions on this
research. You can reach the researcher.Dr (Mrs.) Nwachukwu, M. U. Department of
Anaesthesia. UNTH Ituku-Ozalla/FMC, Umuahia.08034224246.
Response: I have read and understood the above and further explanations have cleared my
doubts. I fully understand the nature, risks and benefits of the study and hereby consent to take
part in it.
--------------------------------------- ----------------------------------------------
Name and signature of patient Name and signature of Researcher
Date -------------------------------- Date ---------------------------------
Name and signature of witness. Date ---------------------------------
61

APPENDIX III
62

APPENDIX IV
6
3

APPENDIX V
64