
Cath Lab in Cardiac Arrest - American Heart Associationwcm/@gra/documents/... · 1 Khaled M. Ziada,...
42
1 Khaled M. Ziada, MD Director, Cardiovascular Catheterization Laboratories Gill Heart Institute, University of Kentucky Utilizing the Cath Lab for Cardiac Arrest UK/AHA Strive to Revive Symposium May 2013
Transcript of Cath Lab in Cardiac Arrest - American Heart Associationwcm/@gra/documents/... · 1 Khaled M. Ziada,...

1
Khaled M. Ziada, MD
Director, Cardiovascular Catheterization LaboratoriesGill Heart Institute, University of Kentucky
Utilizing the Cath Lab for Cardiac Arrest
UK/AHA Strive to Revive SymposiumMay 2013
2
Presenter Disclosure Information
KHALED M. ZIADA, MD
Gill Foundation Professor of Interventional Cardiology
FINANCIAL DISCLOSURE
No relevant financial relationships to disclose.

3
Cardiac Arrest - Definition
� Ineffective cardiac contractions resulting in hemodynamic collapse
� Essentially a catastrophic arrhythmic event
� Pulseless ventricular tachycardia
� Ventricular fibrillation
� Pulseless electrical activity (PEA)
� Asystole

4
Cardiac Arrest – Rhythm Sequence
Akhtar M et al. Ann Intern Med 1991; 114: 499
5
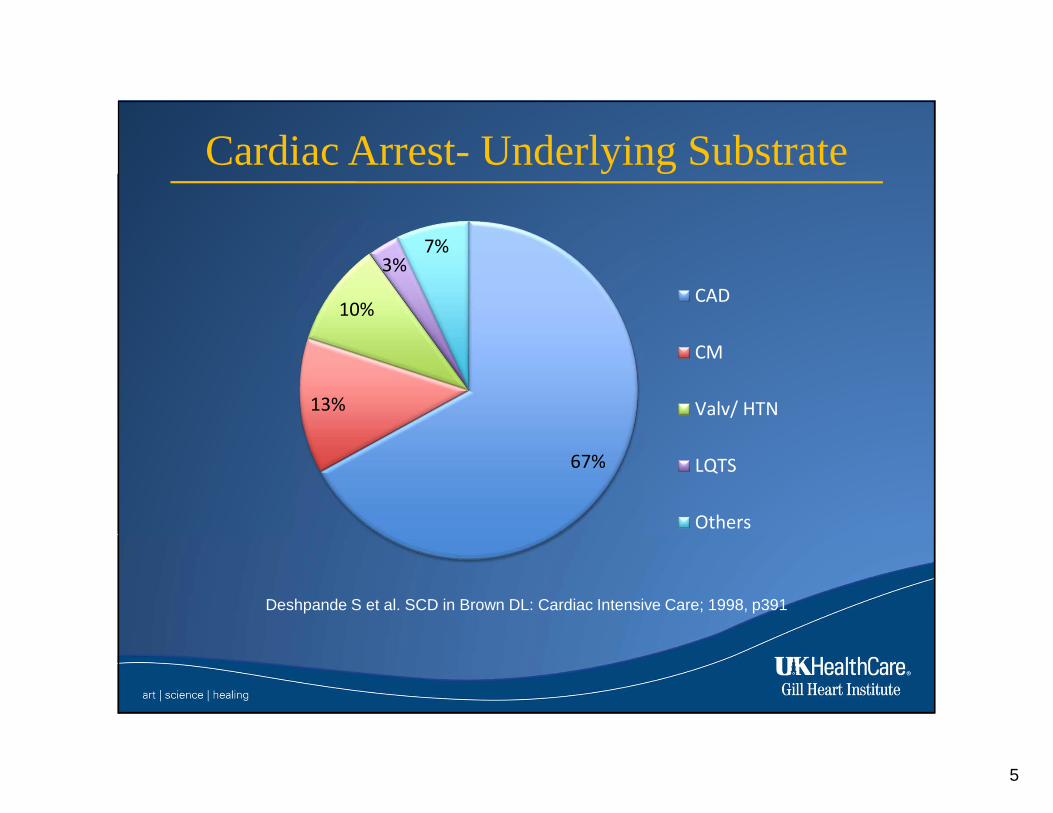
Cardiac Arrest- Underlying Substrate
67%
13%
10%
3%7%
CAD
CM
Valv/ HTN
LQTS
Others
Deshpande S et al. SCD in Brown DL: Cardiac Intensive Care; 1998, p391

6
How Can the Cath Lab Help?
CADSTEMI
Cardiogenic shock
NSTEMI & chronic CAD
Anomalies
Therapeutic Hypothermia
Pulmonary Embolism
ThrombolysisReferral to
surgery
IVC filter
Monitoring and
Resuscitation

7
Cardiac Arrest- Relationship to MI
1. Mylotte D et al. JACC 2013; 6:115-25.2. Myerburg RJ et al. SCD. In Zipes D: Cardiac Electrophysiology 2004; p 720
� STEMI presenting with resuscitated arrest 4-5% 1
� Resuscitated arrest showing new ST elevation 20% 2
� Resuscitated arrest with evidence of healed MI 40-75% 2

8
Arrest and Shock in STEMI
29.6%
Mylotte D et al. JACC 2013; 6:115-25.

9
Arrest, Shock and Mortality in STEMI
� 30-day mortality with cardiogenic shock 40-50%
� 30-day mortality with resuscitated arrest 40-50%
� 30 day mortality with arrest and shock 60-70%
10
Acute STEMI Care is A Team Sport

11
In STEMI Patients, Time is Muscle
12
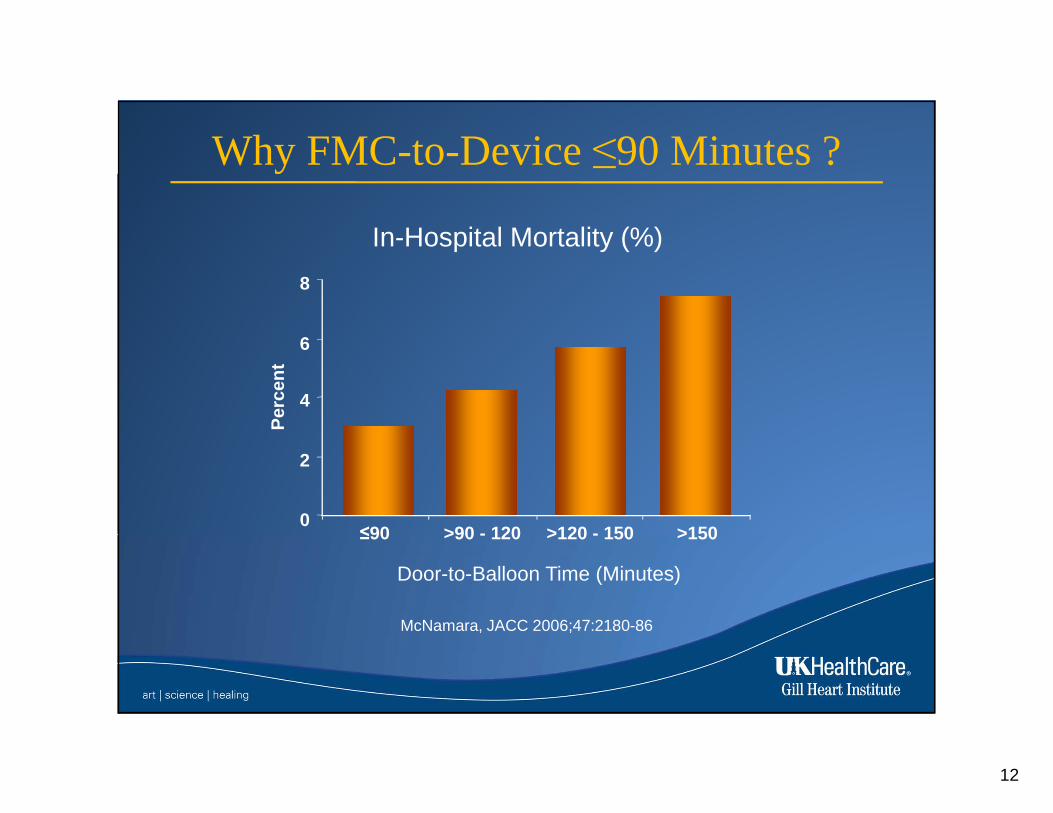
Why FMC-to-Device ≤90 Minutes ?
McNamara, JACC 2006;47:2180-86
Per
cen
t
0
2
4
8
≤90 >90 - 120 >120 - 150
Door-to-Balloon Time (Minutes)
6
>150
In-Hospital Mortality (%)

13
Timely Reperfusion is the Goal
14
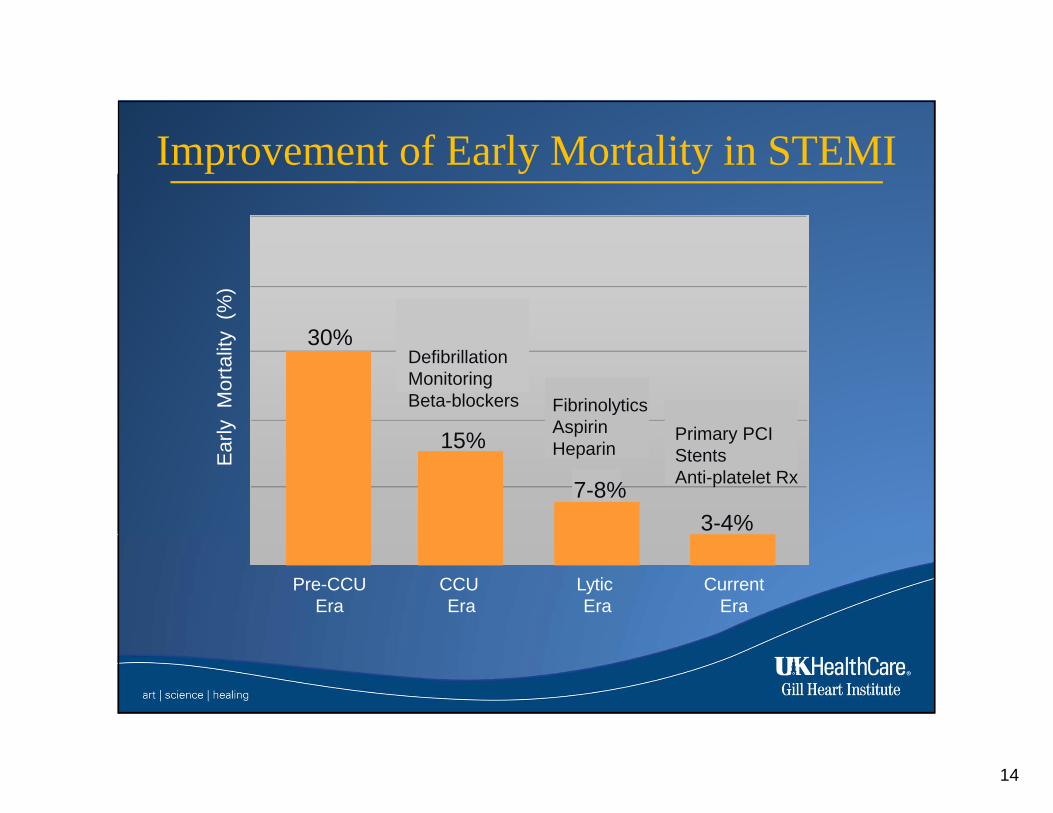
Improvement of Early Mortality in STEMI
Ear
ly
Mor
talit
y (
%)
Pre-CCUEra
30%
CCU Era
DefibrillationMonitoringBeta-blockers
15%
Lytic Era
FibrinolyticsAspirinHeparin
CurrentEra
Primary PCIStentsAnti-platelet Rx
3-4%
7-8%
15
Cardiac Arrest in Context of STEMI
Therapeutic hypothermia should be started as soon as possible in comatose patients with STEMI and out-of-hospital cardiac arrest caused by VF or pulseless VT, including patients who undergo primary PCI.
Immediate angiography and PCI when indicated should be performed in resuscitated out-of-hospital cardiac arrest patients whose initial ECG shows STEMI.
I IIa IIb III
I IIa IIb III
ACC/AHA STEMI Guidelines, 2013

16
Evidence for Early Transfer to Cath Lab
Strote J et al. Am J Cardiol 2012; 109: 451.
� Retrospective propensity matched analysis
� 240 patients with resuscitated out of hospital arrest in the Seattle area
� Prior to routine application of hypothermia
� Improved hospital survival, but no significant difference in neurologic status

17
Acute Management and Long Term Outcome
Dumas F et al. JACC 2012; 60:21-27.
Five Year Survival
� 1001 patients who were discharged from hospital with resuscitated out of hospital arrest
� 38% underwent PCI
� 25% underwent hypothermia
� Adjusted RRR of death was reduced with PCI (by 54%) and hypothermia (by 30%)
18
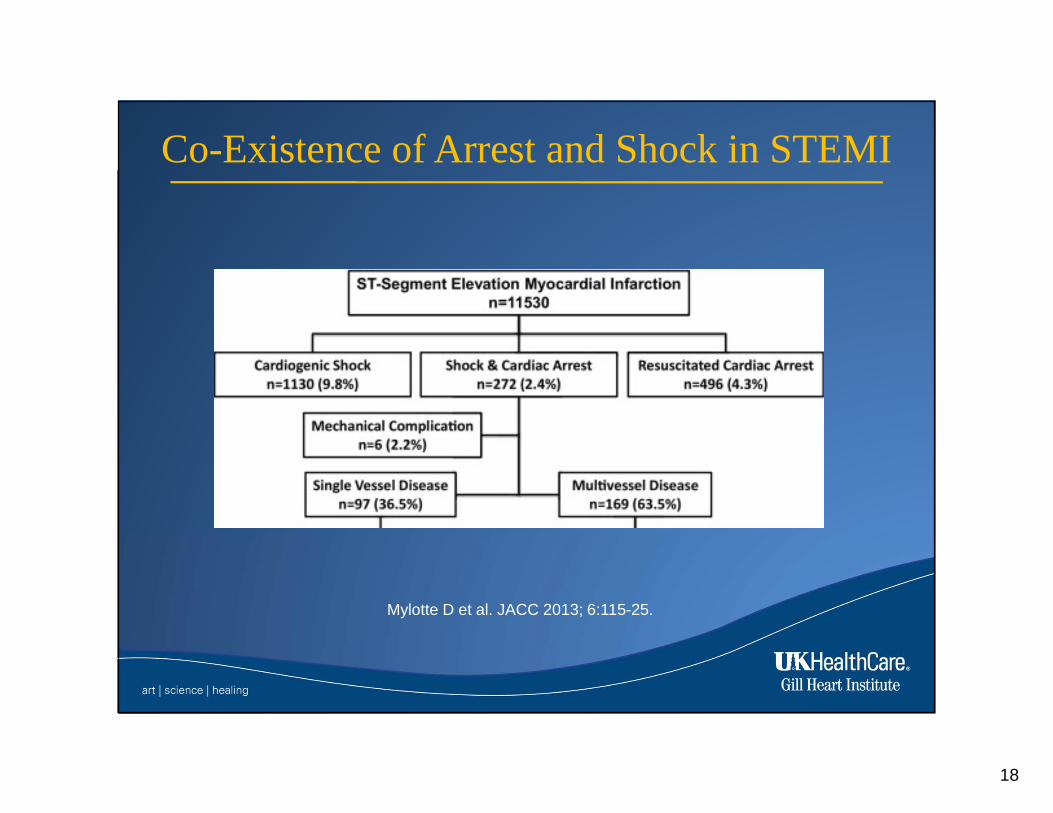
Co-Existence of Arrest and Shock in STEMI
Mylotte D et al. JACC 2013; 6:115-25.

19
MV PCI for STEMI, Arrest and Shock
Mylotte D et al. JACC 2013; 6:115-25.
Six Months Survival
Single vs. Multi-vessel Disease Culprit only vs. Multi-vessel PCI

20
Advanced Support for Cardiogenic Shock
Is There Evidence to Support Mechanical Support?

21
Intra-Aortic Balloon Counter-pulsation
o Mainstay of hemodynamic support for cardiogenic shock pts
o Main mechanisms of action:
● Improve cardiac index
● Reduce afterload
● Reduce LVEDP & PCWP
● Improve coronary perfusion
o Indicated for CS (class IB ACC/AHA and IC ESC guidelines)
o Most commonly used support system

22
IABP – Cardiogenic Shock
The SHOCK Trial
Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock?*
Hochman, J.S. et al. N Engl J Med 1999;341:625-34
* IABP was used in 86% of patients in each group

23
IABP – Acute MI without Shock
Shock II Trial
Randomized Comparison of IABP vs. OMT in Addition to Revascularization in Patients with Acute Myocardial Infarction Complicated by Cardiogenic Shock
Thiele H et al. N Engl J Med 2012, 367: 1287-96
o 600 pts with AMI + CS
o >95% revascularization
o 1:1 randomization to IABP+OMT vs. OMT alone
o Primary Endpoint: All-cause mortality at 30 days
Mor
talit
y (%
)
Time After Randomization (Days)
24
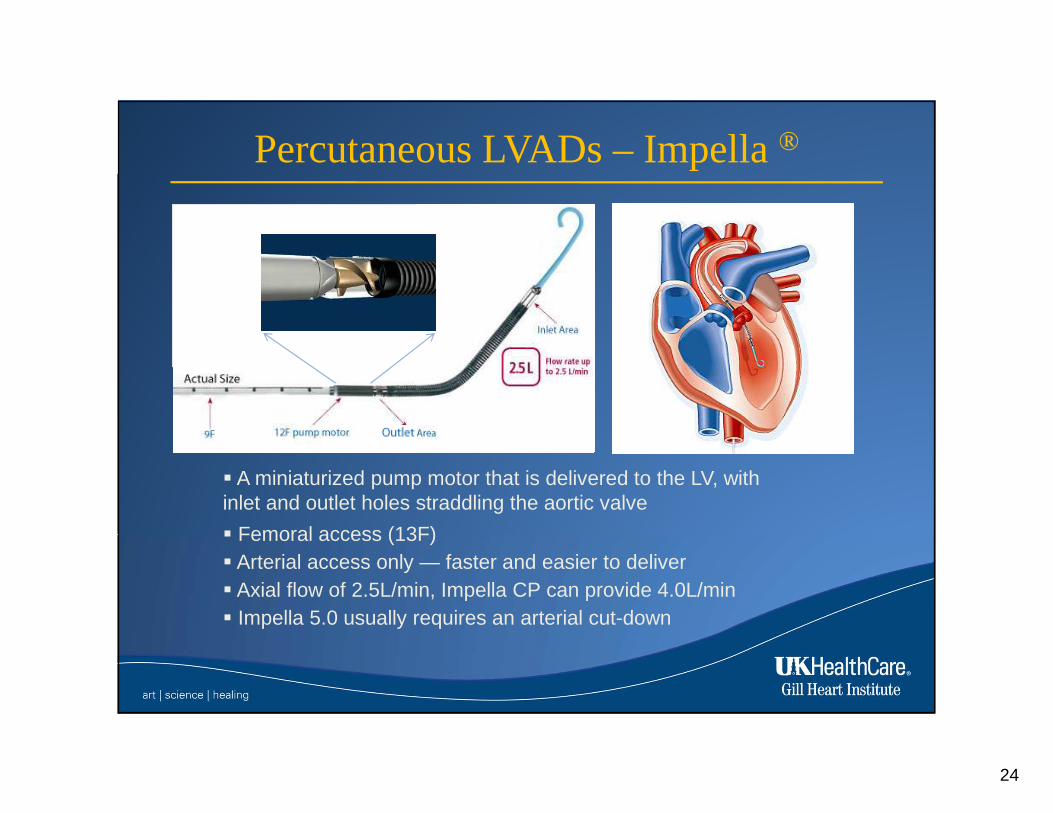
� A miniaturized pump motor that is delivered to the LV, with inlet and outlet holes straddling the aortic valve
� Femoral access (13F)� Arterial access only — faster and easier to deliver� Axial flow of 2.5L/min, Impella CP can provide 4.0L/min� Impella 5.0 usually requires an arterial cut-down
Percutaneous LVADs – Impella®

25
Percutaneous LVADs – Impella®
The PROTECT II Trial: Post-hoc Analysis 1
25
Log rank test, p=0.04
Death, Stroke, large MI, TVR
IABP
IMPELLA
All Patients,
Counting
Only
Large MIs
(N=426)

26
Percutaneous LVADs – Impella®
Caudal –High OM
Cranial -Mid LAD
Baseline Angiograms

27
Percutaneous LVADs – Impella®
Final Angiograms
Caudal –High OM
Cranial -Mid LAD
28
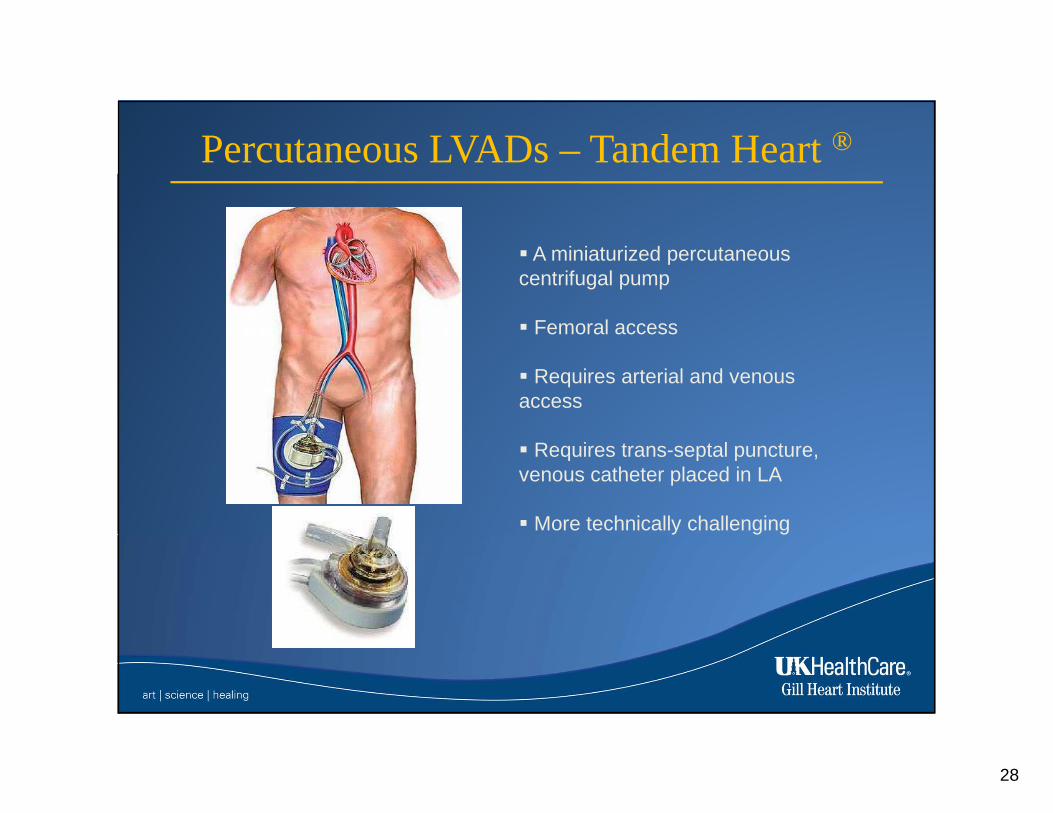
� A miniaturized percutaneous centrifugal pump
� Femoral access
� Requires arterial and venous access
� Requires trans-septal puncture, venous catheter placed in LA
� More technically challenging
Percutaneous LVADs – Tandem Heart ®
29
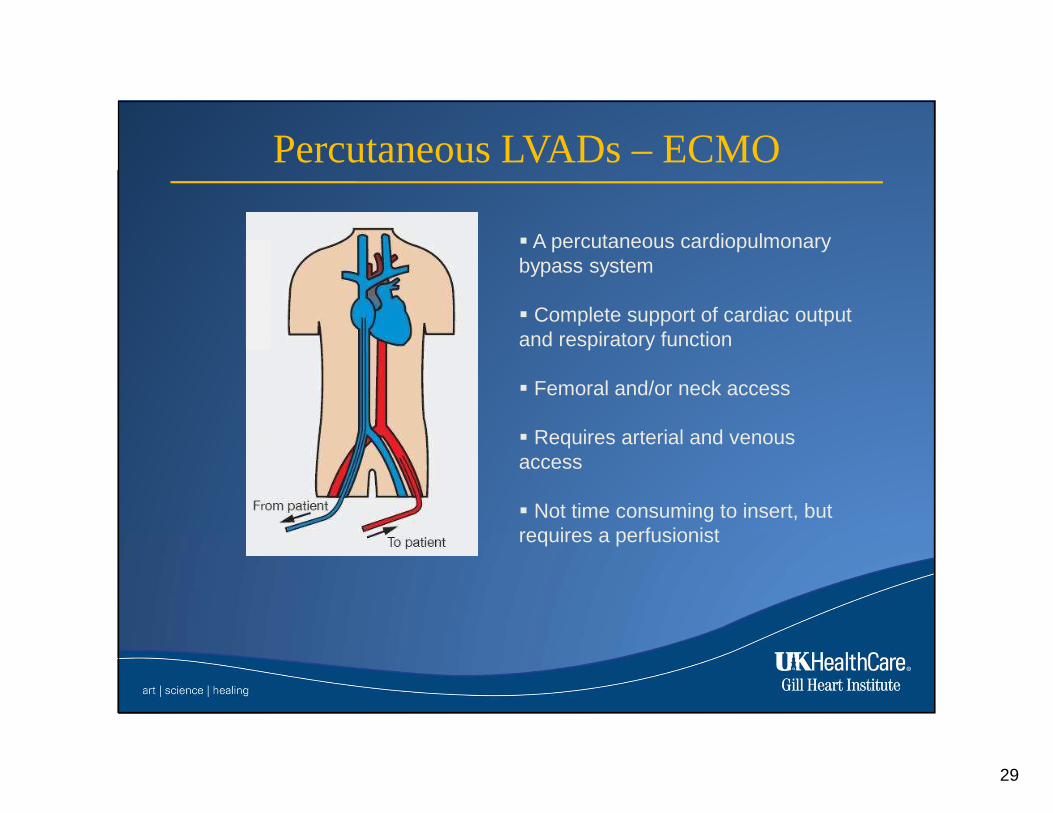
� A percutaneous cardiopulmonary bypass system
� Complete support of cardiac output and respiratory function
� Femoral and/or neck access
� Requires arterial and venous access
� Not time consuming to insert, but requires a perfusionist
Percutaneous LVADs – ECMO

30
Non-Coronary Arrest in the Cath Lab
� Massive and submassive PE
� Hypertrophic cardiomoypathy
� Anomalous coronary arteries
� anomalous LM arising from R cusp
� Functional conditions
� Long QT syndromes
� Electrolyte disturbances

31
Pulmonary Embolism

32
Pulmonary Thrombolysis
33
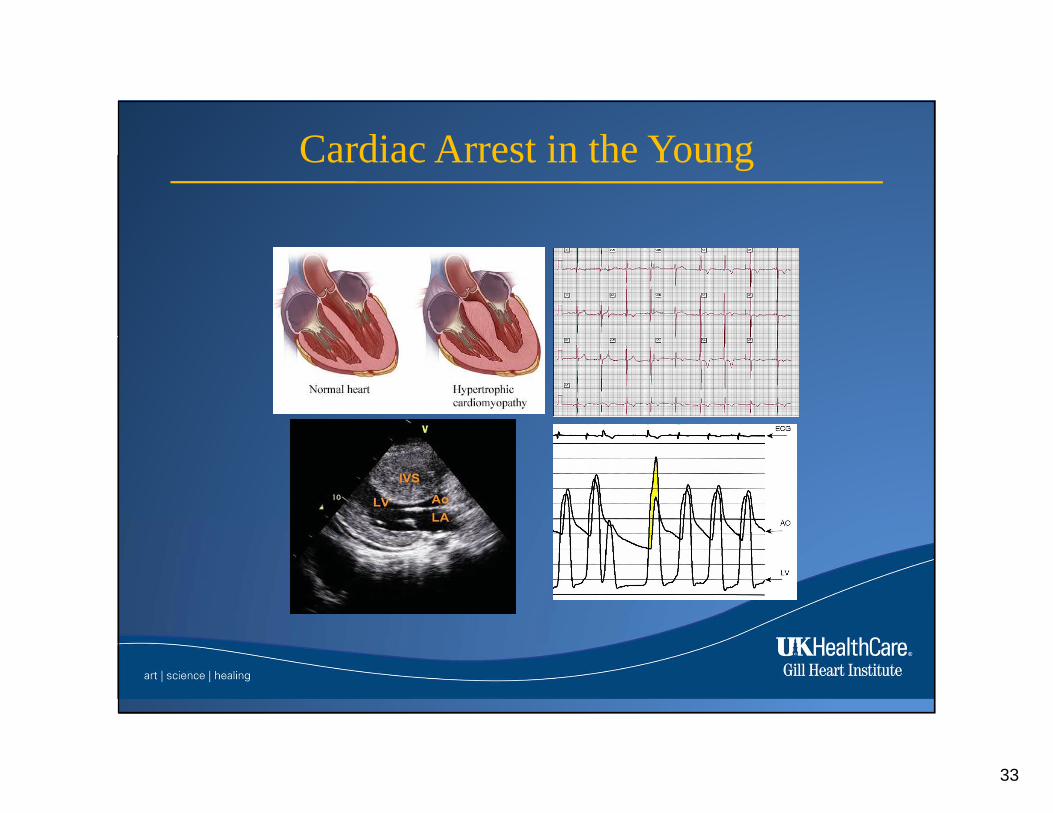
Cardiac Arrest in the Young

34
Cardiac Arrest in the Young
Lim M J et al. Circulation 2005;111:e108-e109
RVOT
Aorta

35
Impact of Therapeutic Hypothermia
77 VT-VF patients, with No Cardiogenic Shock

36
Impact of Therapeutic Hypothermia

37
Hypothermia – Making the Guidelines

38
Cardiac Arrest in Context of STEMI
Therapeutic hypothermia should be started as soon as possible in comatose patients with STEMI and out-of-hospital cardiac arrest caused by VF or pulseless VT, including patients who undergo primary PCI.
Immediate angiography and PCI when indicated should be performed in resuscitated out-of-hospital cardiac arrest patients whose initial ECG shows STEMI.
I IIa IIb III
I IIa IIb III
ACC/AHA STEMI Guidelines, 2013

39
Endovascular Induction of Hypothermia

40
Endovascular Induction of Hypothermia

41
Induction of Hypothermia with ECMO

42

















