
Cath Lab Essentials : LV Assist Devices for Hemodynamic ... · PDF fileGoals To compare and...
37
Pranav M. Patel, MD, FACC, FSCAI Chief, Division of Cardiology Associate Professor of Medicine & Biomedical Engineering University of California, Irvine Division of Cardiology Cath Lab Essentials : LV Assist Devices for Hemodynamic Support (IABP, Impella, Tandem Heart)
Transcript of Cath Lab Essentials : LV Assist Devices for Hemodynamic ... · PDF fileGoals To compare and...

Pranav M. Patel, MD, FACC, FSCAI Chief, Division of Cardiology
Associate Professor of Medicine & Biomedical Engineering University of California, Irvine
Division of Cardiology
Cath Lab Essentials : LV Assist Devices for
Hemodynamic Support
(IABP, Impella, Tandem Heart)
Goals
To compare and contrast mechanical LV
assistance and percutaneous support devices in
terms of their designs and ideal applications
Review current indications for commonly used
devices
Describe the factors that should be considered
when choosing the most appropriate devices

Causes of Cardiogenic Shock
Predominant LV Failure
74.5%
Acute Severe MR
8.3%
VSD
4.6%
Other
7.5%
Shock Registry
JACC 2000 35:1063

Physiology of Cardiogenic Shock: A Downward Spiral
Myocardial ischemia
Damaged heart muscle
Cardiac output
[ CO]
Blood pressure [ BP]
CO & BP
Myocardial ischemia
Venous return
15
14
13
12 11
10
9
8
7 4
5
6
1
2
3
Myocardial Infarction
Death
Coronary artery perfusion
NO synthesis
CO
BP SVR
Inflammatory activation
Myocardial perfusion (blush )
Vasodilation
[SVR ]
Hemodynamic support
Reperfusion of IRA :
PCI or CABG Reducing
inflammatory
response: ?

Emergency revascularisation - SHOCK
Trial
47%50%
53%56%
63%66%
0%
10%
20%
30%
40%
50%
60%
70%
30 days (n=302) 6 months (n=301) 12 months (n=299)
Mo
rta
lity
(%
)
ERV
IMS
85% of survivors NYHA Class I/II at 12 months after early revascularization or
initial medical stabilization
Hochman JAMA 2000;285:190
p=0.11
p=0.03
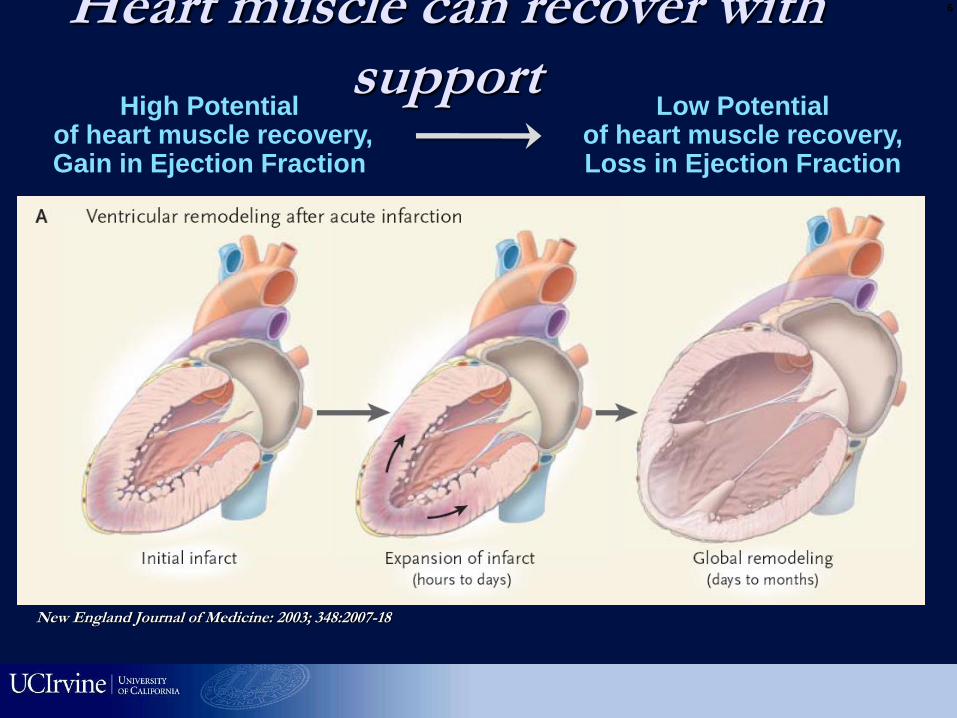
New England Journal of Medicine: 2003; 348:2007-18
Heart muscle can recover with support
High Potential of heart muscle recovery, Gain in Ejection Fraction
Low Potential of heart muscle recovery, Loss in Ejection Fraction
6

Cardiac Support in Cath lab
Hemodynamic Principles
IABP TandemHeart Impella Hemopump ECMO CPS
90’s 80’s 70’s 00’s

Intra-Aortic Balloon Pump
•Introduced in 1968 (Kantrowitz)
•First “true percutaneous” support device
•Cheapest, commonest (20% of all cardiogenic shock cases), CO 0.5L/min
•Stabilize pt, but not full support
•No outcome benefit
Diastolic pressure
CO
MAP
LV Wall Tension
PCWP
Oxygen Demand
LV Volume
Coronary Blood Flow
Hemodynamic Effects:
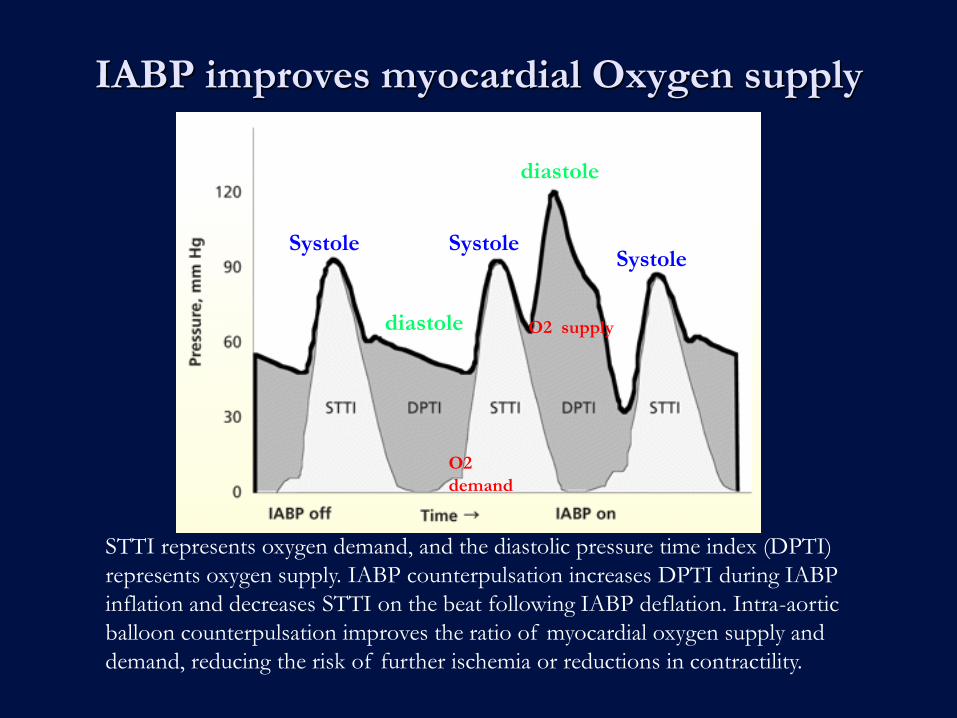
IABP improves myocardial Oxygen supply
STTI represents oxygen demand, and the diastolic pressure time index (DPTI)
represents oxygen supply. IABP counterpulsation increases DPTI during IABP
inflation and decreases STTI on the beat following IABP deflation. Intra-aortic
balloon counterpulsation improves the ratio of myocardial oxygen supply and
demand, reducing the risk of further ischemia or reductions in contractility.
O2
demand
O2 supply
Systole Systole Systole
diastole
diastole

Onset systole
deflate Adjust timing
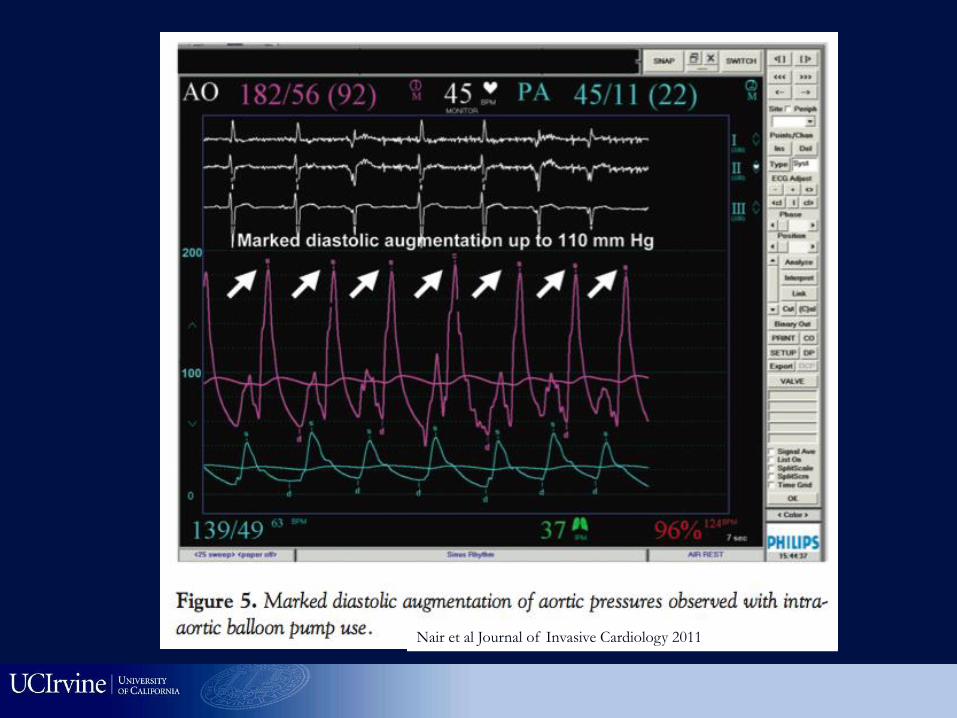
Nair et al Journal of Invasive Cardiology 2011
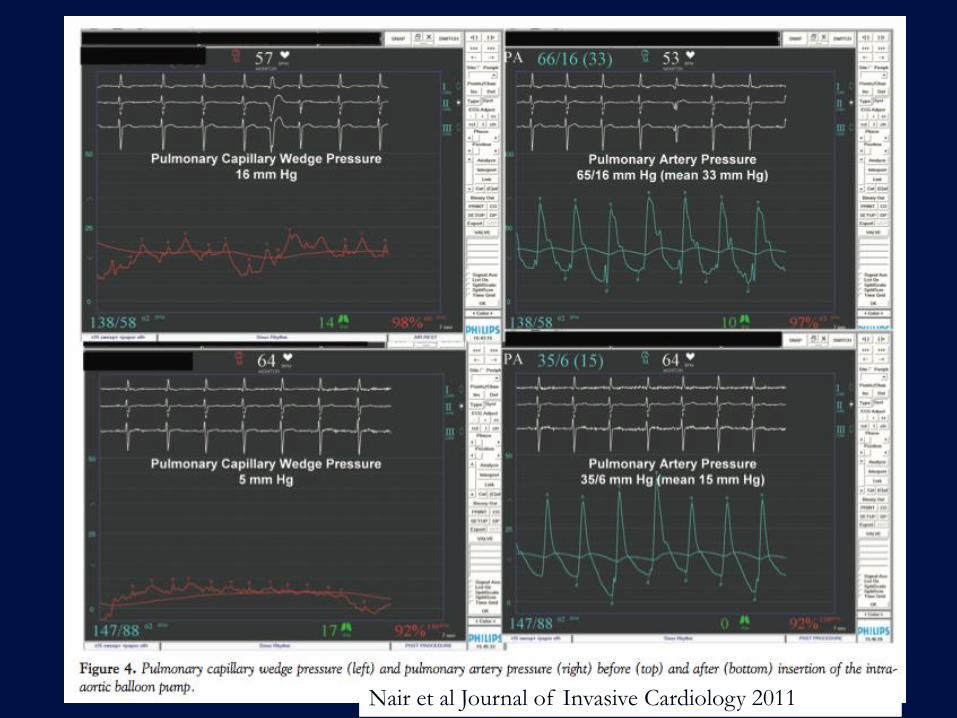
Nair et al Journal of Invasive Cardiology 2011
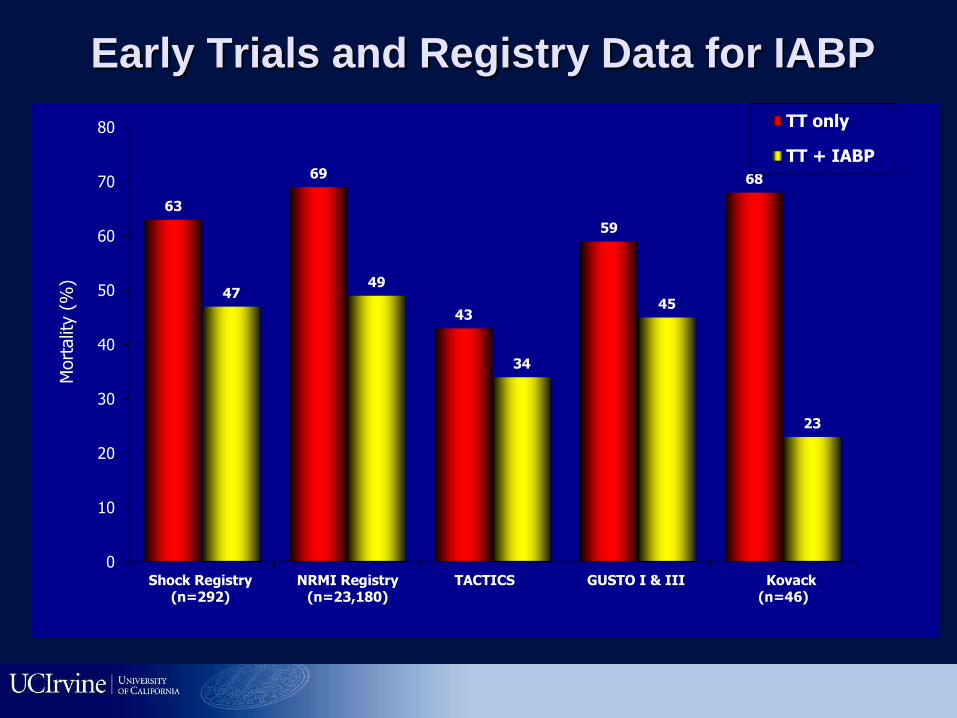
Early Trials and Registry Data for IABP
63
69
43
59
68
47 49
34
45
23
0
10
20
30
40
50
60
70
80
Shock Registry(n=292)
NRMI Registry(n=23,180)
TACTICS GUSTO I & III Kovack(n=46)
Mort
alit
y (
%)
TT only
TT + IABP

IABP in Cardiogenic Shock Primary PCI
67
49
42
46
0
10
20
30
40
50
60
70
80
Thrombolysis only Thrombolysis + IABP Primary PCI only Primary PCI + IABP
In-h
osp
ita
l M
ort
ali
ty (
%)
Retrospective analysis of 23,180 patients from NRMI database
7268 treated by IABP (trend towards improved mortality)

IABP-Shock II Trial: Results Primary Study Endpoint:
30-day Mortality (IABP in Cardiogenic Shock and Primary PCI)
Mo
rtality
(%
)
Time After Randomization (Days)
P=0.92 by log-rank test
Relative risk 0.96; 95% CI 0.79-1.17; P=0.69 by Chi2-Test
Thiele H et al. NEJM 2012;367:1287.
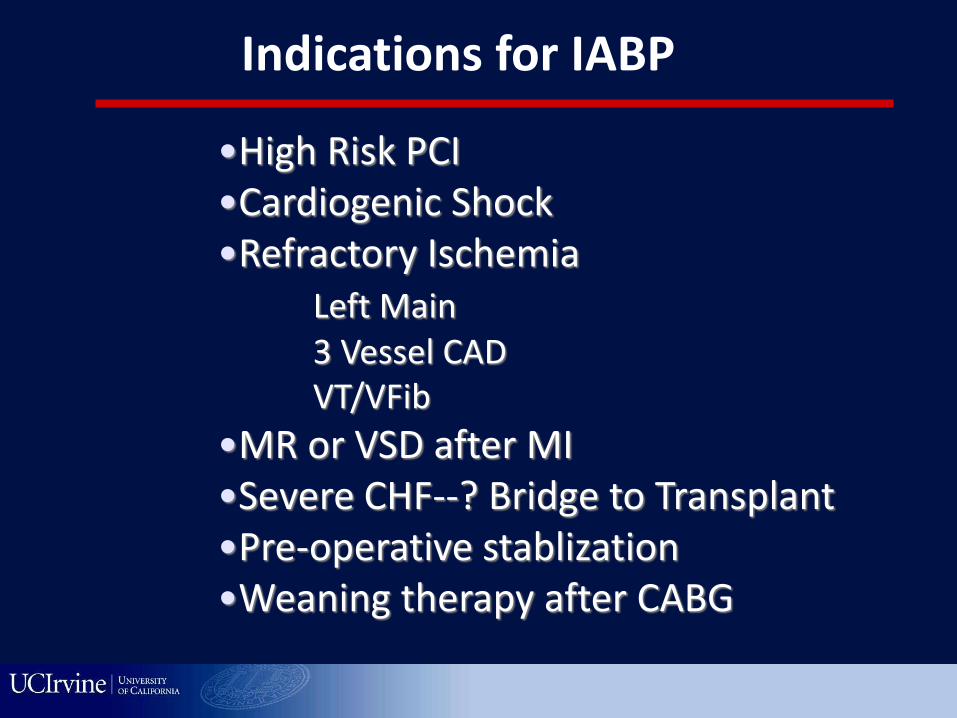
Indications for IABP
•High Risk PCI •Cardiogenic Shock •Refractory Ischemia Left Main 3 Vessel CAD VT/VFib
•MR or VSD after MI •Severe CHF--? Bridge to Transplant •Pre-operative stablization •Weaning therapy after CABG
Contraindication to IABP
• Peripheral vascular disease • Aortic regurgitation • Aortic Dissection • PDA
• HOCM • Heparin intolerance • Bleeding Diathesis • Sepsis
Complications of IABP
• Vascular Access bleeding/complications • Limb Ischemia • Infection • Thrombocytopenia • Migration and aortic arch trauma • Other non-vascular (CVA, embolization of
cholesterol, balloon rupture)
• Air embolism risk (reduced by using helium gas)
35
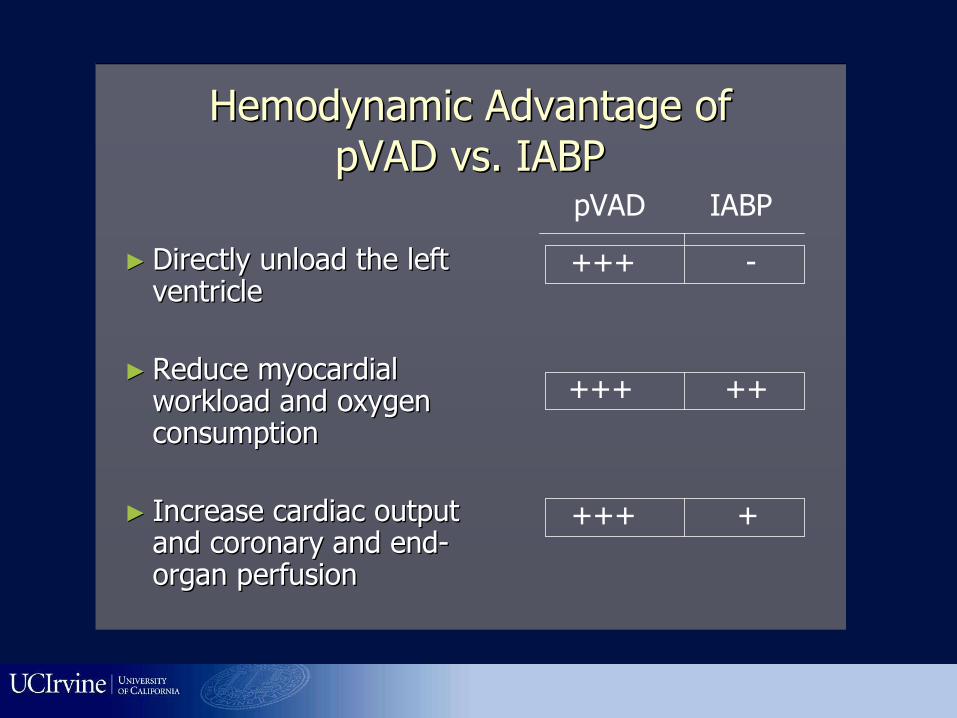
Hemodynamic Advantage of Hemodynamic Advantage of
pVADpVAD vs. IABPvs. IABP
►► Directly unload the left Directly unload the left ventricle ventricle
►► Reduce myocardial Reduce myocardial workload and oxygen workload and oxygen consumption consumption
►► Increase cardiac output Increase cardiac output and coronary and endand coronary and end--organ perfusion organ perfusion
pVAD IABP
+++ -
+++ ++
+++ +

CO
MAP
PCWP
Hemodynamic Effects
Tandem Heart
Left atrial-to-femoral
arterial LVAD
21F venous transeptal
cannula
17F arterial cannula
Maximum flow 4-5L/min
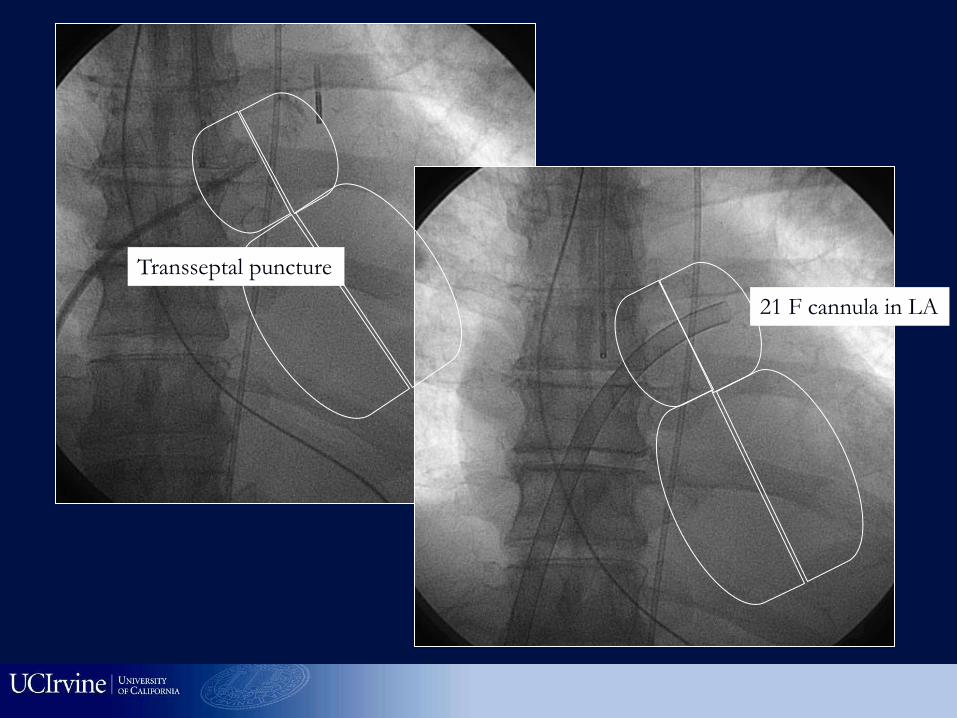
Transseptal puncture
21 F cannula in LA
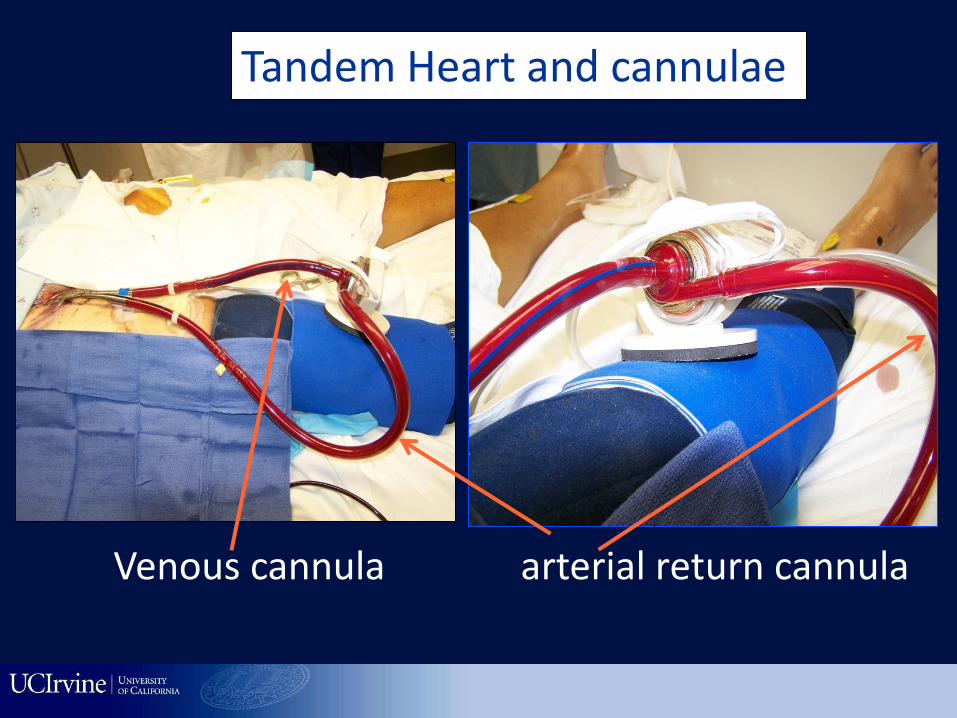
Tandem Heart and cannulae
Venous cannula arterial return cannula
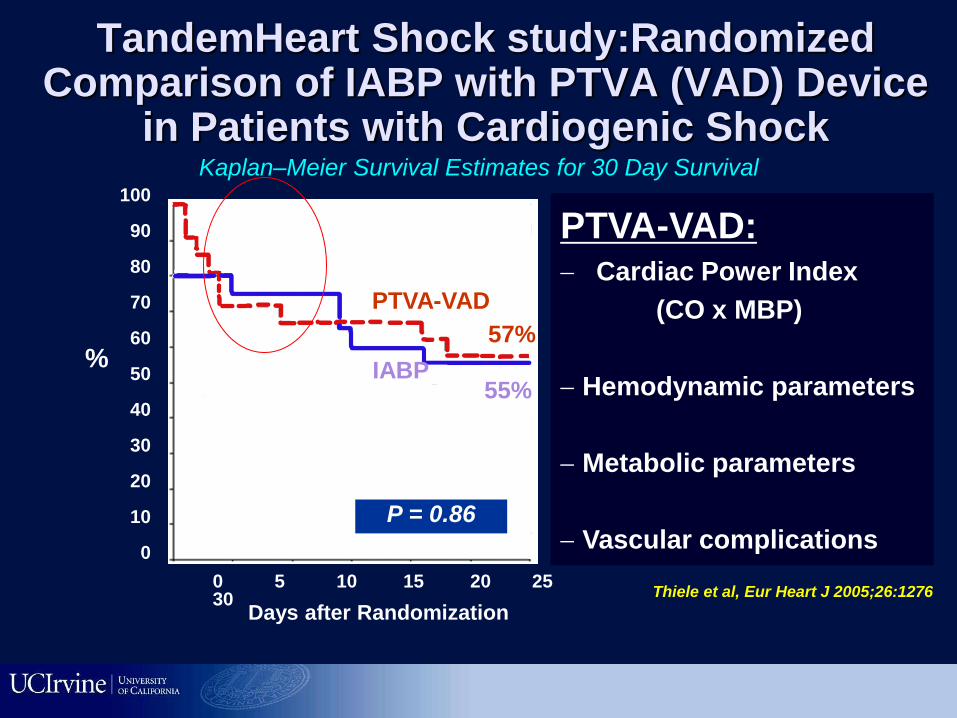
TandemHeart Shock study:Randomized Comparison of IABP with PTVA (VAD) Device
in Patients with Cardiogenic Shock
Thiele et al, Eur Heart J 2005;26:1276
Kaplan–Meier Survival Estimates for 30 Day Survival
0 5 10 15 20 25 30
100
90
80
70
60
50
40
30
20
10
0
%
Days after Randomization
P = 0.86
55%
57%
IABP
PTVA-VAD
PTVA-VAD:
Cardiac Power Index
(CO x MBP)
Hemodynamic parameters
Metabolic parameters
Vascular complications
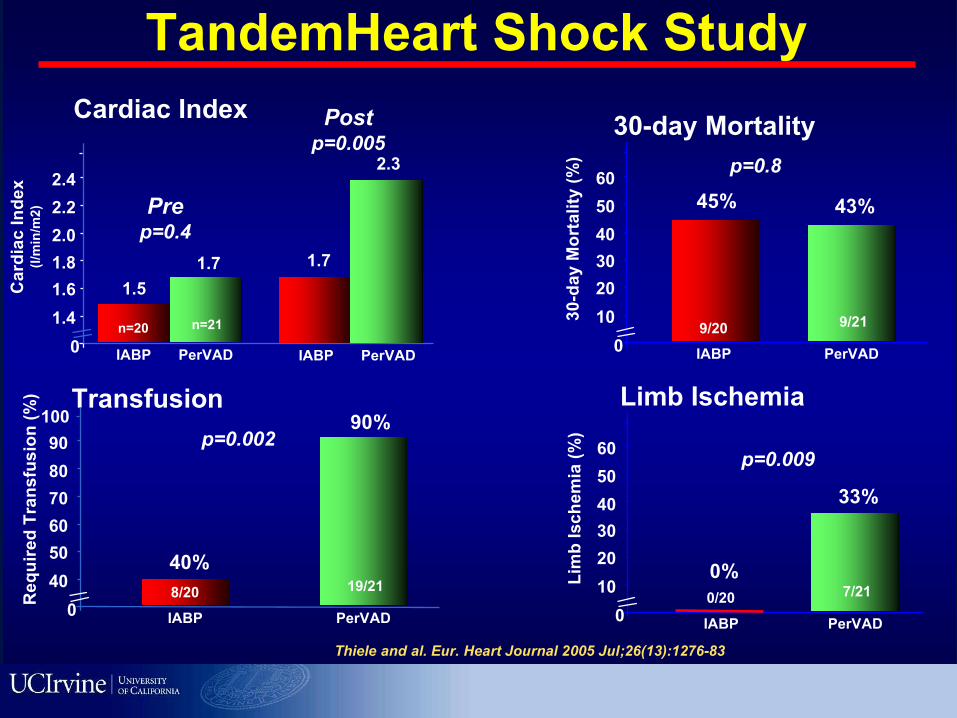
TandemHeart Shock Study
Cardiac Index
0
1.4
1.8
2.2
1.6
2.0
2.4
Card
iac
In
de
x(l
/min
/m2
)
IABP
1.5
1.7
PerVAD
1.7
2.3
Prep=0.4
n=20 n=21
Postp=0.005
IABP PerVAD
Thiele and al. Eur. Heart Journal 2005 Jul;26(13):1276-83
30-day Mortality
0
10
30
50
20
40
60
30
-day
Mo
rta
lity
(%
)
IABP
45%
PerVAD
43%
p=0.8
9/20 9/21
Limb Ischemia
0
10
30
50
20
40
60
Lim
b I
sc
he
mia
(%
)
IABP
0%
PerVAD
33%
p=0.009
0/20 7/21
Transfusion
IABP
40%
PerVAD
90%p=0.002
8/20 19/21
0
40
60
80
50
70
90
Re
qu
ire
d T
ran
sfu
sio
n (
%)
100

Impella
Axial flow pump
Much simpler to use
Increases cardiac
output & unloads LV
LP 2.5 – CO 2.5 L/min
CP 14 F percutaneous
approach; Maximum 4 L
flow
LP 5.0
21 F surgical
cutdown; Maximum
5L flow
Impella insertion
The Impella CP is built on the same foundation as the Impella 2.5, but
provides more than a 50% increase in pumped blood volume (approx. 4L/min)

Mimic Heart’s Natural Function
Inflow
(ventricle)
Outflow
(aortic root)
O2 Demand O2 Supply Cardiac Power
Output
EDV, EDP AOP Flow
Principles of Impella Design
Myocardial Protection Systemic Hemodynamic Support
Naidu S S Circulation 2011;123:533-543

• Impella 2.5
• High risk PCI patient
• Demonstrated net
CO increase with
simultaneous
ventricular unloading
7.4 L/min
Native
CO
Impella
(2.4)
6.0 L/min
Systemic Hemodynamic Support CO Increase … Valgimigli et al.,Cath Cardiov Interv (2005)
5.0
M.Valgimigli et al.,Catheterization & Cardiovascular Interventions 65:263–267 (2005)
Total
Cardiac Output
Pump
Off
6.0 L/min
9/21
Pump
On
7.4 L/min
Pump
OffPump
On
18 mmHg
11 mmHg
Pump
OffPump
On
94 mL
76 mL
IMPELLA Unloads Actively the Ventricle, Reduces
Work Loads and Increases Cardiac Output
LV LV
pump
End-Diastolic
LV PressureEnd-Diastolic
Stroke Volume

ISAR-SHOCK RANDOMIZED TRIAL: IMPELLA 2.5 Provides Better Hemodynamic
Support Than IABP in AMI Cardiogenic Shock*
Impella
Primary Endpoint:
Increase in Cardiac Index From Baseline
(measured after 30 min of support)
IABP
0.49
0.15
0.60
Card
iac I
nd
ex
Im
pro
vem
ent
(L/m
in/m
2)
p<0.01
0.45
0.30
0.75
00.11
*Seyfarth et al, J Am Coll Cardiol. 2008 Nov 4;52(19):1584-8
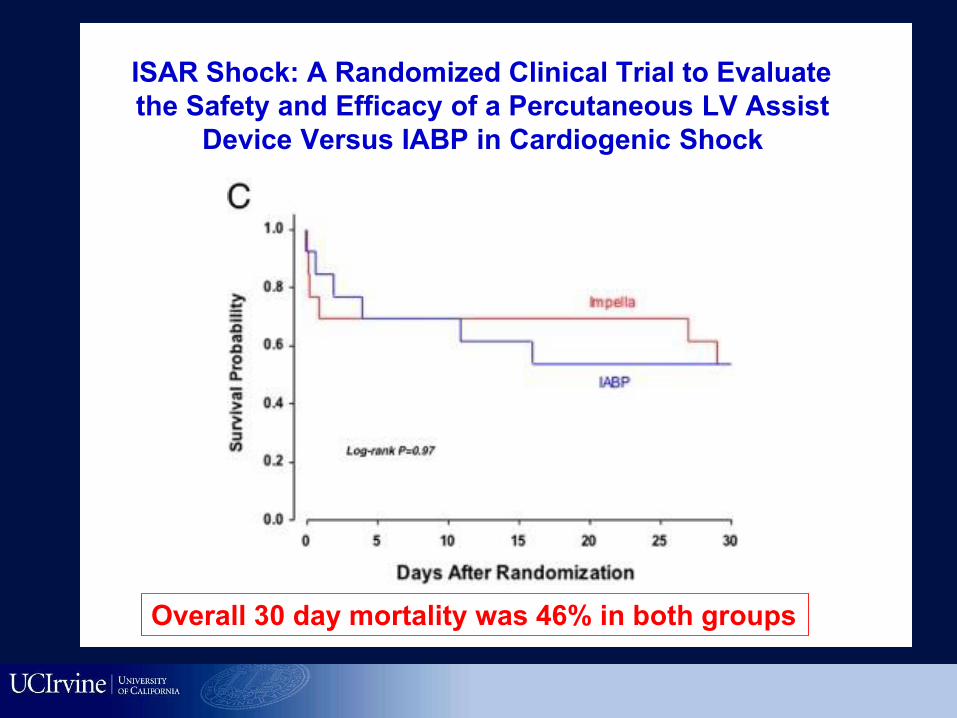
ISAR Shock: A Randomized Clinical Trial to Evaluate
the Safety and Efficacy of a Percutaneous LV Assist
Device Versus IABP in Cardiogenic Shock
Seyfarth M; JACC 52:1584
Overall 30 day mortality was 46% in both groups
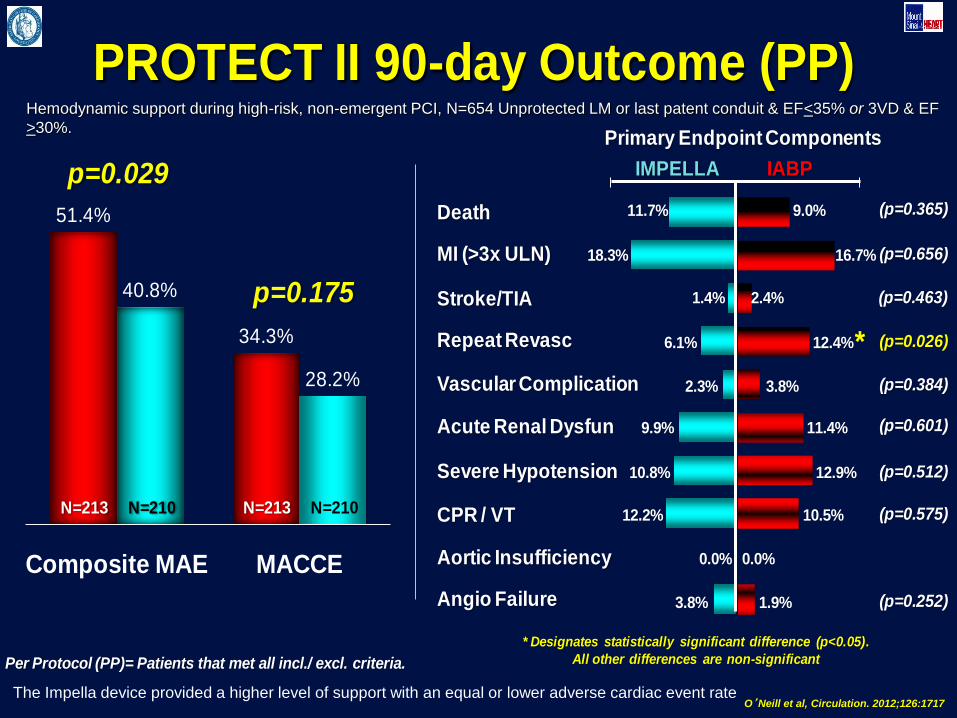
Primary Endpoint Components
Death
MI (>3x ULN)
Stroke/TIA
Repeat Revasc
Vascular Complication
Acute Renal Dysfun
Severe Hypotension
CPR / VT
Aortic Insufficiency
Angio Failure
11.7%
18.3%
1.4%
6.1%
2.3%
9.9%
10.8%
12.2%
0.0%
3.8%
9.0%
16.7%
2.4%
12.4%
3.8%
11.4%
12.9%
10.5%
0.0%
1.9%
IMPELLA IABP
PROTECT II 90-day Outcome (PP)
* Designates statistically significant difference (p<0.05).
All other differences are non-significant
51.4%
34.3%
40.8%
28.2%
Composite MAE MACCE
p=0.029
p=0.175
* (p=0.026)
N=210N=213 N=210N=213
Per Protocol (PP)= Patients that met all incl./ excl. criteria.
(p=0.365)
(p=0.656)
(p=0.463)
(p=0.384)
(p=0.601)
(p=0.512)
(p=0.575)
(p=0.252)
O’Neill et al, Circulation. 2012;126:1717
Hemodynamic support during high-risk, non-emergent PCI, N=654 Unprotected LM or last patent conduit & EF<35% or 3VD & EF
>30%.
The Impella device provided a higher level of support with an equal or lower adverse cardiac event rate

Impella demonstrates EF improvements
1. MACH II Trial – Academic Medical Center, Netherlands, Mechanical Assistance for Acute
Congestive Heart Failure, published in Journal of American College of Cardiology, March
11, 2008; 51: 1044-1046., 3-Year follow-up presented at TCT 2009
Baseline After*
29
37 37 37
30 28
LVEF Improvement w/Impella Support MACH II 1 Study-Impella support
post MI
Baseline 3 days 4 months 3 Years
2. USpella, N=25 subjects have LVEF measurements
* Longest available follow-up from PCI
All Combined No Shock Shock
28
40 37
42 41
45
51
47 Impella Arm
Control Arm
EF
(%
)
MACH II (N=20)
• Impella arm sicker at Baseline
• Impella arm increased EF by 23 points
• Control arm increased EF by 7
• Impella arm had better QOL/activity1
at 3 years
USpella2 Registry 9/2009
• Patients increased EF 7-9 points
• 68% failing on IAB in cardiogenic shock
• Age at 64 + 16
p= 0.01
Journal of American College of Cardiology, March 11, 2008
Ejection Fraction Ejection Fraction
EF
(%
)
Baseline Baseline After*
After*
33

Approach to cardiogenic shock Systolic BP > 70-85 mm Hg and good mentation:
consider IABP to help prevent shock. Consider IABP in:
Bridge to surgery Severe HF Cardiogenic shock (mild to severe)
BP < 70, or on inotropes and vasopressors: consider
Impella (2.5-5L CO) or Tandem heart (4-5L) Complete Cardiogenic arrest: Extracorporeal membrane
oxygenation and complete bypass

LV Support during High-Risk PCI: LVEF + Lesion Complexity
LVEF >35% LVEF 20-35% LVEF <20%
Simple PCI
Complex
PCI
No support
IABP SBP 75-80 mm Hg or mild Cardiogenic
shock Impella/Tandem
SBP 40-70 mm Hg, more
severe CS or multiple vasopressor/inotropic
agents
Simple or Complex: Inoperable cases
IABP
SBP 75-80 mm Hg or mild
Cardiogenic shock
Impella SBP 40-70 mm Hg, more severe CS or
multiple vasopressor/inotropic
agents
Simple PCI
Complex PCI: High Syntax score
>32 STS >5 Extensive revasc.
Questions
What are the complications of IABP?
A. vascular complications
B. CVA
C. embolization of cholesterol
D. balloon rupture
E. All of the above

Questions
The following statement is true/false
An IABP achieve its action through a counter
pulsation: Deflates during systole Inflates during Diastole
What is used to inflate and deflate the balloon?
helium used (reduced chance of air
embolism if the balloon were to rupture)




![· LV 01 - LV 02 - 14 - LV LV Of - LV - LV - LV - Skat Foru Out] Profil PM E-Mail Q Pik, Grand? 1272 x) Vorhand ist dran nach passe pa s se. Nach Skatauffiahme:](https://static.fdocuments.in/doc/165x107/5e0d1071f8f59d3156471103/lv-01-lv-02-14-lv-lv-of-lv-lv-lv-skat-foru-out-profil-pm-e-mail-q.jpg)













