Catch of the Day · 2020. 7. 8. · Catch of the Day. Andrew Worster. Ken Milne. Katrina Hurley....
30
Catch of the Day Andrew Worster Ken Milne Katrina Hurley Gauri Ghate Tracy Meyer Justin Yan
Transcript of Catch of the Day · 2020. 7. 8. · Catch of the Day. Andrew Worster. Ken Milne. Katrina Hurley....
-
Catch of the Day Andrew WorsterKen MilneKatrina HurleyGauri GhateTracy MeyerJustin Yan
-
Andrew WorsterKen MilneKatrina HurleyGauri GhateTracy MeyerJustin Yan
Catch of the Day
PresenterPresentation NotesStart music
-
Faculty/Presenter Disclosure
Faculty: Andrew WorsterRelationships with financial sponsors:
• Grants/Research Support: Canadian Institutes for Health Research• Speakers Bureau/Honoraria: None• Consulting Fees: None• Patents: A Laboratory Score for Risk Stratification of Patients with
Possible Cardiac Injury• Other: BEEM’s Director & Editor-in-Chief
-
Faculty/Presenter Disclosure
Faculty: Ken MilneRelationships with financial sponsors:
• Grants/Research Support: None• Speakers Bureau/Honoraria: None• Consulting Fees: None• Patents: Ped-E-Board• Other: BEEM Author
-
Faculty/Presenter Disclosure
Faculty: Katrina HurleyRelationships with financial sponsors:
• Grants/Research Support: None• Speakers Bureau/Honoraria: None• Consulting Fees: None • Patents: None• Other: BEEM Author
-
Faculty/Presenter Disclosure
Faculty: Gauri GhateRelationships with financial sponsors:
• Grants/Research Support: None• Speakers Bureau/Honoraria: None• Consulting Fees: None • Patents: None• Other: BEEM Author
-
Faculty/Presenter Disclosure
Faculty: Tracy MeyerRelationships with financial sponsors:
• Grants/Research Support: WorksafeNB• Speakers Bureau/Honoraria: None• Consulting Fees: None • Patents: None• Other: None
-
Faculty/Presenter Disclosure
Faculty: Justin YanRelationships with financial sponsors:
• Grants/Research Support: Recipient of Lawson Health Research Institute Internal Research Fund, CAEP Junior Investigator Grant, Western Strategic Support for CIHR Success Grant
• Speakers Bureau/Honoraria: None• Consulting Fees: None • Patents: None• Other: BEEM Author
-
NNR = 1
Not for Profit
PresenterPresentation NotesWhat is BEEM?BEEM is a not-for-profit knowledge translation projectAW: We created a process the find the best evidence in emergency medicine: it incorporates input from emergency physicians like you from around the world and the hierarchy of levels of evidence. We’ve published 2 studies in Academic EM to show that our system is both reliable and valid in identifying the most clinically relevant studies and even predicting future citations. Today we’re going to talk about 9 studies that emergency physicians like you have told us are highly clinically relevant.
BEEM Journal Incentive Game: Visit Booth #206Business Cards for Natasha - One of our incentives is a business card game. There are 3 different cards but combined they form an image of the evidence pyramid. If an attendee can locate 2 other attendees with the other pieces, the 3 of them get a free Journal subscription.
-
Minor Stroke& TIA
Dual antiplatelet therapy with aspirin and clopidogrel for acute high risk transient ischaemic attack and minor ischaemic stroke: a clinical practice guideline.
Prasad K, et al. BMJ. 2018 Dec 18;363:k5130.
PresenterPresentation NotesThe 1st article is a clinical practice guideline. Why are clinical practice guidelines important? CPG can represent the highest level of evidence for clinical practice because they are systematic reviews of the literature analyzed by panels of expertsSo clinical practice guidelines are good and we should all follow them?No, not all CPGs are good and they are only meant to guide practice, not to dictate it.How can the developmental process be not good?The evidence is incomplete or weak or the experts are biased in their interpretations and recommendations.Why is this clinical practice guideline important?Following a minor stroke or high-risk transient ischemic attack (TIA), patients face an increased risk of recurrent ischemic event. The dual antiplatelet therapy (DAPT) of aspirin (ASA) and clopidogrel appears to synergistically inhibit platelet aggregation. Is this a good clinical practice guideline?It’s an excellent guideline with only a minor flaw in that EPs weren’t included as stakeholders.What are the recommendations?
-
Increased duration of dual therapy increases risk of bleeding but likely minimal
Clopidogrel 300 mg loading dose & 75 mg & ASA 50–325 mg PO daily for 10–21 days
PresenterPresentation NotesClopidogrel 300 mg loading dose and 75 mg & ASA 50 to 325 mg PO daily for 10 to 21 days. Increased duration of dual therapy increases risk of bleeding Short-term A+C is more effective and equally safe in comparison to aspirin alone in patients with acute IS or transient ischemic attack.What’s the catch?ABCD2 score has been reported as having very low discrimination. NIHSS better.
-
Maintenance Intravenous Fluids in Children. Feld LG, et al. Clinical Practice Guideline: Pediatrics. 2018 Dec;142(6).
Isotonic IVF with appropriate potassium chloride and dextrose for maintenance
PresenterPresentation NotesKatrina, you also have a CPG and this is on IV fluids for children: What factors should we consider when deciding what fluid to use in a child?
Tracy, what are some of the strengths and limitations of this article?
Katrina, how do the results of this study affect our management of patients in the ED?
-
Effect of Intranasal Ketamine vs Fentanyl on Pain Reduction for Extremity Injuries in Children: The PRIME Randomized Clinical Trial
Frey TM, et al. JAMA Pediatrics2019 Feb 1
PresenterPresentation NotesKatrina, while we're on the topics of small adults, how do we stop them crying during painful procedures?Why is this important?What are the limitations/threats to validity?How does it fit with previous findings about IN ketamine?
-
Ketamine IN provides similar analgesia than fentanyl but has more adverse effects
Effect of Intranasal Ketamine vs Fentanyl on Pain Reduction for Extremity Injuries in Children: The PRIME Randomized Clinical Trial
Frey TM, et al. JAMA Pediatrics2019 Feb 1
PresenterPresentation NotesHow does it impact clinical practice?Intranasal pain medications must be delivered using a mucosal atomizer device. Otherwise, the medication will drip into the posterior pharynx and mouth, and the absorption is quite poor from those surfaces.You must add 0.1ml of extra pain medication to your syringe in order to compensate for the atomizer tip’s dead space.IN ketamine shares the advantages of early and rapid pain management for children who lack vascular access but confers the added benefit of longer-lasting analgesia (60 minutes for IN ketamine vs 30 minutes for IN fentanyl).
-
Premedication With Midazolam or Haloperidol to Prevent Recovery Agitation in Adults Undergoing Procedural Sedation With Ketamine: A Randomized Double-Blind Clinical Trial
Akhlaghi N, et al. Annals of Emergency Medicine2019 May 7
PresenterPresentation NotesTracy, Justin you perform PSA on both big and little children.
Tracy, tell us about ketamine and how to prevent ketamine-associated agitation (KAA).
Justin, you’re a researcher, what study factors affect the generalizability and validity of applying the study results to your patient population?
-
Pre-medication with midazolamor haloperidol likely reduces KAA
Premedication With Midazolam or Haloperidol to Prevent Recovery Agitation in Adults Undergoing Procedural Sedation With Ketamine: A Randomized Double-Blind Clinical Trial
Akhlaghi N, et al. Annals of Emergency Medicine2019 May 7
PresenterPresentation NotesDo the results change your practice in the ED in any way?Pre-medication with midazolam or haloperidol likely reduces KAA but . . . it significantly increases post-sedation recovery times in adult ED patients and might not be any more effective than pre-sedation psychological preparation.
-
Will This Patient Be Difficult to Intubate?: The Rational Clinical Examination Systematic Review.Detsky ME, et al. JAMA. 2019 Feb; 321(5):493–503.
PresenterPresentation NotesJustin & Gauri, before we sedate someone, we need to assess their airway, is the malleate score the best way?
If not, which physical exam finding(s) best predict a difficult airway?
-
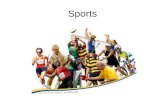
Class 1 Class 2 Class 3
Will This Patient Be Difficult to Intubate?: The Rational Clinical Examination Systematic Review. Detsky ME, et al. JAMA. 2019 Feb 5;321(5):493–503.
PresenterPresentation NotesCan you apply this study to ED practice?
-
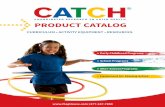
Index Test LR+ (95% CI) LR– (95% CI)Upper lip bite test Class 3 14 (8.9 to 22) 0.42 (0.27 to 0.65)Impaired mandibular protrusion 5.5 (2.1 to 15) 0.78 (0.54 to 1.1)Short hypomental distance 6.4 (4.1 to 10) 0.84 (0.73 to 0.96)Modified Mallampati score 4.1 (3.0 to 5.6) 0.52 (0.45 to 0.60)
PresenterPresentation NotesWhat is the take-home EBM teaching point from this study? (screening tests & likelihood ratios)A history of difficult intubation is the best predictor of a difficult intubation, while a Class 3 on the Upper Lip Bite test is the best physical exam predictor. This may prompt emergency providers to anticipate a difficult airway. However, because no single test or combination of tests can rule out a difficult airway, emergency airway providers should be prepared for a difficult intubation with advanced airway devices such as VL or a bougie despite the results of bedside airway examination tests.
-
Ultrasound Is Superior to Palpation in Identifying the Cricothyroid Membrane in Subjects with Poorly Defined Neck Landmarks: A Randomized Clinical Trial. Anesthesiology.
Siddiqui N, et al. 2018 Dec;129(6):1132–1139.
PresenterPresentation NotesWhat if we sedate but can't intubate or bag?Can you apply this study to ED practice? What is the take-home EBM teaching point from this study?
-
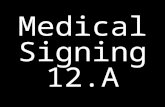
Ultrasound Is Superior to Palpation in Identifying the Cricothyroid Membrane in Subjects with Poorly Defined Neck Landmarks: A Randomized Clinical Trial. Siddiqui N, Yu E, Boulis S, et al. Anesthesiology. 2018 Dec;129(6):1132–1139.
Sig. Outcome Ultrasound Palpation NNT* (95% CI)SS Proportion of correctly localized cricothyroid membrane 92/114 9/109 1 (1 to 2)SS Absolute distance from the CT identified location (mm) 3.4 16.6 N/A
PresenterPresentation NotesIs US more accurate than palpation? And if so, are the findings in this study supported by others? How many scans are required for successful identification of the cricothyroid membrane?
-
Murata S, et al. Pediatrics. 2018 Nov;142(5)
Acetaminophen and Febrile Seizure Recurrences During the Same Fever Episode
PresenterPresentation NotesSince we're on the topic of scary events, Katrina & Tracy, tell us about seizures in children.
-
Murata S, et al. Pediatrics. 2018 Nov;142(5)
Acetaminophen and Febrile Seizure Recurrences During the Same Fever Episode
PresenterPresentation NotesFebrile seizures are a benign syndrome. They do not cause brain damage and the likelihood of developing epilepsy is very small. Febrile seizures occur in 2–5% of children aged 6 months to 5 years with a recurrence rate of approximately 30%. Peak incidence is between 12 and 18 months. The current standard of care for febrile seizures includes ruling out central nervous system infection (clinically or by lumbar puncture, if indicated). There are no routine diagnostic laboratory tests. Neuroimaging is rarely indicated. Treatment is entirely supportive.Risk factors for recurrent febrile seizures include early age at onset (< 12 months), history of febrile seizure in a first-degree relative, brief duration between the onset of fever and the initial seizure and low degree of fever while in the ED.Risk factors for the development of epilepsy following febrile seizures include abnormal child development before the first seizure, family history of afebrile seizures and complex first febrile seizure.
-
Shen J, et al.Cochrane Database Syst Rev2019 Jan 20
Interventions for Emergency Contraception
PresenterPresentation NotesSince children are so much trouble, how can we prevent them? Gauri, what role does the ED have in the provision of emergency contraception? What is the best method for EC in Canada?
Tracy, what were the results of this guideline and how do they compare to the current guidelines?
Gauri, can you comment on the quality of this Cochrane review?
-
Levonorgestrel 1.5 mg PO
Shen J, et al.Cochrane Database Syst Rev2019 Jan 20
PresenterPresentation NotesTracy, Any specific discharge instructions for patients seeking EC from the ED? A single, oral dose of LNG 1.5 mg is an affordable and accessible EC option in most countries with minimal adverse effects. In some countries, patients can access it directly at a pharmacy or health clinic without a physician’s prescription. However, the sooner it is taken after intercourse, the more effective it is. Patients should be advised that LNG does not cause a miscarriage or abortion so it will not work if the patient is already pregnant when she takes it.
-
Prognostic Accuracy of the HEART Score for Prediction of Major Adverse Cardiac Events in Patients Presenting With Chest Pain: A Systematic Review and Meta-analysis
Fernando SM, et al. Acad Emerg Med. 2019 Feb;26(2):140–151
PresenterPresentation NotesAndrew, let's wrap up and talk about the over-studied HEART score. What is the HEART score? �The HEART score is a health measurement scale to assess risk in patients presenting with symptoms of ACS and it assigns points based on the history, ECG, age, risk factors and troponin results. What’s the purpose of this systematic review? This systematic review summarizes the prognostic accuracy of the HEART score for prediction of MACE at 30 days and 6 weeks.
-
Prognostic Accuracy of the HEART Score for Prediction of Major Adverse Cardiac Events in Patients Presenting With Chest Pain: A Systematic Review and Meta-analysis
Fernando SM, et al. Acad Emerg Med. 2019 Feb;26(2):140–151
PresenterPresentation NotesFrom what we’ve heard systematic reviews can be complicated. Are there any issues with this one? Systematic reviews can provide us with the highest level of evidence to influence practice but they’re dependent on 3 factors: a thorough search strategy; the inclusion of high quality studies; and appropriate methods of analysis. More than half of included studies were at high risk of bias and the authors combined the results of RCTs with cohort studies which is a major source of heterogeneity and inflates the performance of the tests.Do you use or teach the HEART score? Personally, no. There is no evidence that the HEART score outperforms (or underperforms) clinical gestalt. It doesn’t outperform hs-troponin alone. However, the HEART score might be used to facilitate risk communication and shared decision-making with patients and other care providers.
If time, summarize all results.
-
Become a BEEM RaterNNR = 1
Not for Profit
PresenterPresentation NotesAW: On behalf of the BEEM Team, I’d like to thank you for coming today. BEEM is a not-for-profit KT project run by emergency physicians for emergency physicians. You can be part of BEEM and help us find the best evidence in emergency medicine by becoming a BEEM Rater. If you want to learn more about BEEM, visit our booth and or website.
-
PresenterPresentation NotesAndrew: Critically appraising studies is complicated in part because we only have the information that the authors and editors want us to have.
The devil is in the details: without those details we’re left making assumptions and estimations.
As Socrates said, “You don’t know what you don’t know”. No one knows everything about research and so the best CA is generated by having multiple experts critique each study.
He also said “It depends”. To avoid any perception of commercial promotion, I change that to “It all depends.” because the answers about research depend on many different factors.
-
Thank you!
Aloha BEEM 2020Hilton Hawaiian Village Waikiki Resort | April 8–10, 2020
Not for Profit
Booth #206
PresenterPresentation NotesSpecial CAEP Promotion:40% DiscountVisit Booth #206
Slide Number 1Slide Number 2Faculty/Presenter DisclosureFaculty/Presenter DisclosureFaculty/Presenter DisclosureFaculty/Presenter DisclosureFaculty/Presenter DisclosureFaculty/Presenter DisclosureSlide Number 9Slide Number 10Slide Number 11Slide Number 12Slide Number 13Slide Number 14Slide Number 15Slide Number 16Slide Number 17Slide Number 18Slide Number 19Slide Number 20Slide Number 21Slide Number 22Slide Number 23Slide Number 24Slide Number 25Slide Number 26Slide Number 27Slide Number 28Slide Number 29Slide Number 30