Case Study
37
Case Study Mr. D B: Cirrhosis and Ascites Erica Bennett
-
Upload
erica-bennett -
Category
Documents
-
view
19 -
download
1
Transcript of Case Study

Case StudyMr. D B: Cirrhosis and Ascites
Erica Bennett

I. Primary Disease Process: Cirrhosis
Cirrhosis of the liver is the final stage of chronic hepatic diseases, characterized by fibrosis
(permanent scarring) and loss of function of the hepatic tissue. As the satellite cells of the liver
respond to chronic injury and inflammation, they transform into fibroblasts and begin producing
collagen, which stiffens the organ and cuts off much of the hepatic circulation, leading to portal
hypertension.8
In the year 2010, cirrhosis was the eighth leading cause of death in the United States, leading
to 49,500 deaths nationwide.16 The main etiologies of cirrhosis are chronic viral hepatitis (HBV
and HBC), alcoholism, and nonalcoholic fatty liver disease. 8
Cirrhosis can be diagnosed most definitively by liver biopsy, but can also be detected by
MRI, CT scan, and ultrasonography, especially in patients who are symptomatic. Symptoms are
not always apparent in compensated cirrhosis, where the liver is damaged but still able to
perform its functions, or may be so nonspecific that it is hard to ascertain the cause. Some more
specific symptoms of later-stage compensated cirrhosis include muscle wasting, hardened liver,
spider angiomas, esophageal varices, and palmar erythema, or redness of the palm.6 Symptoms
of decompensated cirrhosis include ascites, edema, hematemesis (suggestive of variceal
bleeding), osteopenia and osteoporosis, diabetes, jaundice, vitamin and mineral deficiencies,
hepatocellular carcinoma (HCC), and hepatic encephalopathy. 1
Cirrhosis can be classified into one of four stages upon diagnosis by the presence of certain
complications. Stages one and two of cirrhosis are considered compensated, with stage one
characterized by presence of cirrhosis without esophageal varices or ascites, and stage two
characterized by presence of esophageal varies without further complication. Stages three and
four are considered decompensated cirrhosis; these are the stages in which cirrhosis is generally

diagnosed, as the symptoms become more distinctive. Stage three cirrhosis is characterized by
the presence of ascites, and stage four cirrhosis by the presence of gastrointestinal bleeding.8
Ascites is the most common complication of cirrhosis, caused by extreme vasodilation of the
arteries in the abdomen. Scarring of the liver leads to shutting off of some hepatic blood vessels,
resulting in portal hypertension and formation of collateral veins to compensate for the loss of
others. Blood that builds up in the decompensated liver begins to be shunted to the systemic
circulation and nitric oxide is produced by nearby cells to help dilate blood vessels in the area,
both mechanisms intended to help relieve portal hypertension. The vasodilation caused by nitric
oxide becomes extreme as cirrhosis worsens and portal hypertension increases, affecting not just
the portal vessels but also the neighboring splanchnic arteries. Arterial pressure in these vessels
falls dramatically, and mechanisms such as sodium and fluid retention are activated in an effort
to maintain blood pressure. Retained fluid is eventually pushed into the abdominal cavity, where
it can accumulate in massive volumes.4
Another complication related to portal hypertension is splenomegaly. The increased blood
pressure in the portal vein, to which blood from the spleen flows, causes increased blood
pressure in the spleen and enlargement of the spleen. This back-up of blood can lead to a
decrease in the number of red and white blood cells, as well as platelets, in the systemic
circulation. The bone marrow blood cell production mechanism may also be suppressed by
alcohol intake and hepatitis viruses, which may contribute to low peripheral blood cell count in
many patients with cirrhosis.6
Important laboratory values to watch in cirrhosis patients include the liver function tests,
such as bilirubin, prothrombin time, albumin, and ALT/AST; electrolytes and glucose; hepatitis
marker like BUN and glucose; blood counts and clotting factors; protein levels like albumin,

prealbumin, and transferrin (as disease indicators, not indicators of protein status); and vitamin
and mineral levels. The most validated test combination in the diagnosis and staging of cirrhosis
is a high ALT/AST ratio, low albumin, extended prothrombin time, and thrombocytopenia.8 The
AST/ALT ratio was studied in patients with and without cirrhosis by Nyblom et al, whose
experimentally determined normal range of 0.5-1.0 is used in this research paper.10 Electrolyte
labs such as sodium are important in order to diagnose hyponatremia. Glucose monitoring is
important to catch and treat hypoglycemia and hyperglycemia. Vitamin and mineral levels are
also vital to check to ensure that the patient’s micronutrients needs are being met.1 When
cirrhosis patients with ascites undergo paracentesis, a procedure in which a needle is inserted
into the abdominal cavity and used to draw out the trapped fluid, the collected fluid should be
analyzed in the lab for presence of infection and any other remarkable fluid abnormalities.4
Another important lab test in cirrhosis evaluation is hepatitis B and C testing, since both are
potential causes of cirrhosis. Serum creatinine and urine protein are other important lab values to
monitor, as abnormalities could point to hepatorenal syndrome. Regular screening for
hepatocellular carcinoma is also important for cirrhosis patients.8
Treating the cirrhosis patient based on the underlying etiology of their disease is important in
ensuring the best outcome. For example, treatment of hepatitis B and C when they are the cause,
and drinking cessation when alcoholism is the cause, greatly improve complications like ascites,
and can improve therapeutic outcomes.7 The long-term treatment for cirrhosis is generally liver
transplantation when patients reach decompensated cirrhosis. Patients with ascites tend to have
poor prognosis without transplant, so they are often given priority on liver transplant lists.4
Patients who are diagnosed with compensated cirrhosis can live up to 20 years without

experiencing symptoms; however, following diagnosis with decompensated cirrhosis, patients
generally live less than two years.8
Nutrition therapy for cirrhosis patients includes meeting basal energy and nutrient needs and
then providing the extra nutrients needed in the hypermetabolic state. Energy needs may be
increased, with estimated needs ranging from 25-40 kilocalories per kilogram dry body weight
per day,13 or basal energy expenditure, calculated using dry weight, plus twenty percent.1 Excess
calorie intake, however, should be avoided to prevent fat accumulation in the liver.5 Protein
needs may also be increased, estimated at 0.8-1.5 grams per kilogram dry body weight per day,
due to disease-induced protein loss and muscle protein breakdown. 1, 13 Patients with liver disease
were at one time encouraged to restrict protein, but it is now believed that it is more important to
prevent muscle catabolism than to rest the liver. Patients with hepatic encephalopathy should
take in normalized amounts of protein with each meal to meet protein needs.5 Branched chain
amino acids are encouraged, since they are processed by the muscles and theoretically do not
significantly add to the liver’s workload. They show promise in improving muscle mass, but
have not yet been proven to improve hepatic encephalopathy.11
Carbohydrate intake and blood glucose should be monitored, as there is potential for both
hypoglycemia and hyperglycemia in patients with cirrhosis due to decreased liver glycogen
stores, decreased gluconeogenesis, and insulin resistance.13 If insulin resistance worsens to the
point of a diabetes mellitus diagnosis, the patient should be managed with a diabetic dietary plan
and diabetic medications such as metformin. Fat intake should also be modified and limited to
less than 30 percent of total calories if the patient experiences steatorrhea due to bile acid
deficiency. Total fat intake should be decreased and intake of medium-chain triglycerides should
be considered to maximize absorption.13

Sodium intake should be restricted if fluid retention is evident, as in ascites, to 2000 mg per
day. However, according to Nusrat, restrictions under two grams per day “are not recommended
because they are less palatable and create the potential to reduce food intake and worsen the co-
existing malnutrition.” 9 Research in this patient population has found that mortality rate is
significantly higher in patients with low serum sodium concentrations. In the same study, low
serum sodium was also associated with presence of ascites, but not associated with other
common complications such as hepatic encephalopathy.15 Fluid intake goals should generally be
30-40 ml per kilogram per day, but for patients with serum sodium levels under 128 mEq per
liter, fluid intake should be restricted to 1200-1500 ml per day, and for patients with serum
sodium below 125 mEq per liter, restricted to 1000-1200 ml per day.1
Lactulose, a nonabsorbable (prebiotic) disaccharide which traps and prevents absorption of
ammonia in the colon, has been a widely accepted therapy for decades. However, it is being
reexamined, as some recent studies have shown no more improvement in patients on Lactulose
as opposed to a placebo.11 Other new therapies are emerging, however. Probiotic therapy shows
some potential in decreasing total ammonia in the portal circulation, reducing inflammation in
the liver, and decreasing toxin uptake in the gastrointestinal tract. Several studies have been done
to demonstrate its efficacy, one including fructo-oligosaccharides (prebiotics) along with the
probiotic Bifidobacterium and one with just probiotics. More studies need to be done, but
probiotics plus fructo-oligosaccharides are a potential future treatment recommendation for
cirrhosis patients in preventing and improving hepatic encephalopathy.5, 11
According to the Nutrition Care Manual, “The vast majority of patients with cirrhosis will be
at risk for nutritional compromise because of their liver disease and its symptoms.” 1 Nutrition
status is often moderate or severely compromised in patients with decompensated cirrhosis due

to hypermetabolism, decreased oral intake, decreased nutrient absorption and increased nutrient
losses, and decreased nutrient synthesis, secretion, and storage capacity.13 Weight loss, especially
loss of lean body mass even as fluid weight is accumulated, is common and often severe.
Malnutrition is a common sequela of cirrhosis, especially decompensated cirrhosis such as
cirrhosis with ascites. According to Johnson et al, “those with tense ascites generally have the
lowest protein energy intake and most compromised status.” 5 Liver disease can cause
malabsorption, dysmetabolism, and inadequate storage of vitamins and minerals. Liver disease
patients tend to have inadequate oral intake due to anorexia, abdominal distention and pain,
dysgeusia, nausea and vomiting, alcohol intake, encephalopathy, decreased gastric emptying, a
limited and less appetizing diet due to prescribed dietary restrictions, and increases in leptin
levels causing early satiety. Cirrhosis is also associated with low socioeconomic status and
alcoholism, both of which can lead to decreased dietary intake and decreased nutritional value of
intake,5 and, according to Singal et al, “the prevalence and severity of malnutrition are also high,
with increasing amounts of alcohol use, lower socioeconomic status, and lack if employment.” 13
It is therefore likely that many patients are already malnourished who become cirrhotic, and then
the cirrhosis further worsens their malnutrition, leading to worsened outcomes.
Deficiencies of the fat-soluble vitamins A, D, E, and K are very common, which can lead to
symptoms such as night blindness and scaly skin, osteopenic bone disease, neuropathy, and
increased bleeding, respectively. They are important to supplement in many liver disease
patients. Vitamin A deficiency also “promotes fibrosis and collagen deposition” in the liver,
worsening cirrhosis.13 Vitamin E is thought to play an interesting role in cirrhosis patients,
possibly reducing liver oxidative stress and thus discouraging inflammation. Deficiency may
lead to hemolytic anemia and increased red blood cell lysis.5 Iron deficiency can also lead to

anemia, but iron should not be supplemented unleash the patient is deficient, as excess can be
hepatotoxic. Zinc, another common deficiency, can lead to nutritional issues, such as anorexia,
ageusia, and altered protein metabolism.5 Alcoholic liver disease can cause deficiency of the
water-soluble vitamins as well, especially folate, niacin, pyridoxine, cyanocobalamin, thiamine,
and Vitamin C.13
II. General Patient Information
Mr. D. B. is a 51 year old Caucasian man who was living alone in a motel in St. Petersburg
prior to admission to the Bay Pines VA. He was born in Michigan, and is a high school graduate.
He served in the army from 1981-1984, and subsequently worked as a carpenter. 10 years ago,
he suffered a traumatic brain injury during a fight, after which he began to experience memory
problems and suffer from a mood disorder. He has been unemployed for eight years and receives
$997 monthly from Social Security Disability Insurance. Mr. B. has been married and divorced
three times, and has one 13 year old daughter; however, the girl’s aunt has custody, and he does
not get to see her often. In his motel, he has a mini-fridge and a microwave, which is his primary
cooking method. Mr. B. has been dependent on alcohol at least since 2007. He has been treated
for substance abuse several times, and has sobered up at the hospital only to go home and start
drinking again.
This patient was selected for an in depth case study because of his complex disease state
including both alcohol use and viral hepatitis in the etiology of his cirrhosis, and the vital
importance of nutrition therapy in giving him the best possible outcome. He was nutritionally
compromised upon admission due to his disease and its complications and, likely, his alcohol
intake, which may be greater than reported. Nutrition therapy was vital for him, to assist in

decreasing further fluid accumulation, to replete his body protein stores, and to prevent and
correct vitamin and mineral deficiencies.
III. Present Admission and Status
Mr. B. presented at the Bay Pines VA Emergency Room on August 17, 2014 with tense
ascites for the second time. He was diagnosed with cirrhosis in July 2014. His medical history
also includes GERD, a cholecystectomy, hepatitis C, alcohol dependence, tobacco use disorder
(smokes a pack a day), mood disorder, anxiety disorder, depression, and a subdural hematoma.
In July 2014, Mr. B. was also first diagnosed with ascites, and underwent his first paracentesis.
He was prescribed lactulose to manage his hyperammonemia, but has been noncompliant with
the medication because of fear of not making it to the bathroom in time. The bathroom in his
hotel is down the hall, making it difficult for him to get there quickly enough. The admitting
physician, Dr. Maysa Ahmad, prescribed a dose of furosemide and spironolactone that evening
(August 17) and recommended paracentesis.
Mr. B. was transferred to ward 5B once he was stabilized. According to his attending
physician, Dr. Ira Azneer, Mr. B. complained of nausea, vomiting, shortness of breath, and
abdominal pain persisting for the past four days. Along with the ascites, he also had 2++ edema
in his extremities. Mr. B.’s MRSA screening test came back positive, so he was placed in an
infection control setting. Dr. Azneer scheduled the paracentesis for August 18. The procedure
removed seven liters (approximately 15 pounds) of fluid. He was continued on the diuretic
regimen of spironolactone and furosemide to flush out excess fluid accumulation in the rest of
his body.

Dr. Azneer also prescribed Mr. B. a potassium chloride supplement, a magnesium sulfate
supplement, a thiamine supplement, and a multivitamin/mineral supplement. Ondansetron was
administered multiple times during his hospital stay for nausea and vomiting. Mr. B. was already
on lactulose, a laxative designed to help him clear ammonia from his system more effectively
and prevent hepatic encephalopathy, omeprazole, a proton-pump inhibitor for his GERD, and
trazodone and paroxetine, antidepressants. The medications and their nutrition-related effects are
shown in more detail in the table below.
Medication Type/Use Nutrition-Related EffectsSpironolactone Potassium-sparing diuretic –
treats fluid retention and edema
Hyperkalemia (avoid excessive potassium intake), possible hyponatremia. Can cause nausea, vomiting, and diarrhea.
Furosemide Loop diuretic – treats fluid retention and edema
Hyponatremia, hypokalemia, hypomagnesemia. Can also cause decreased serum chloride and calcium, and increased serum glucose. Need to increase the potassium and magnesium in the diet, and decrease caloric intake. Avoid natural licorice.
Lactulose Laxative – to treat hyperammonemia
High fiber diet with 1500-2000 mL liquid. Drug increases absorption of calcium and magnesium; supplementation with these is generally not recommended.
Omeprazole Proton pump inhibitor – anti-GERD
Decreases gastric acid secretion, increases gastric pH. Avoid alcohol. Can cause diarrhea. My decrease absorption of iron, vitamin B12, and calcium. Calcium citrate supplement recommended. Avoid gingko and St. John’s Wort.
Ondansetron Anti-emetic, anti-nauseant Can cause abdominal pain, constipation, and diarrhea.

Potassium Chloride Electrolyte, mineral supplement
Do not take with salt substitutes.
Magnesium Sulfate Mineral supplement, antacid, laxative.
May cause chalky taste and diarrhea. Do not take with high fiber, oxalate, or phytate food.
Thiamine B Complex Vitamin – prevent Wernicke/Korsakoff syndrome due to chronic alcohol abuse
Alcohol inhibits absorption.
Multivitamin/mineral Supplement – contains vitamin A, D, E, folic acid, niacin, pantothenic acid, riboflavin,Iron, calcium, magnesium, manganese,
Possible vitamin/mineral toxicities
After paracentesis, Mr. B.’s peritoneal fluid was assessed in the laboratory for bacteria and
white blood cells. Bacteria were not found, indicating that no infection of the peritoneal cavity
was present. White blood cells were found in normal amounts. The most important lab values in
monitoring cirrhosis and ascites are reported in the table below.6, 12
Normal values
August 17 August 19 August 20 August 21
Glucose 74-118 mg/dL 91 105 92 94Sodium 136-144
mEq/L133 (low) 136 136 137
Potassium 3.6-5.1 mEq/L 3.8 3.7 (low) 3.9 4.0Magnesium 1.8-2.4 mEq/L 1.7 (low) 1.8 1.8Calcium 8.9-10.3 8.2 (low) 7.7 (low) 7.8 (low) 7.8 (low)Prothrombin time
9.6-12.5 sec 17 (high) 19.6 (high) 18.6 (high) 18.9 (high)
BUN 8-20 mg/dL 6 (low) 7 (low) 4 (low) 7 (low)Albumin 3.5-4.8 g/dL 2 (low) 1.5 (low)Ammonia 9-33 umol/L 16Bilirubin 0.2-1.3 mg/dL 3.6 (high) 2.3 (high)AST/ALT ratio 0.5-1.1 2.84 (high) 2.63 (high)RBC 4.23-5.75
M/uL3.67 (low) 3.09 (low) 3.23 (low) 3.24 (low)
Hemoglobin 12.8-17 g/dL 12.7 (low) 10.6 (low) 11.2 (low) 11.1 (low)WBC 4.0-10.6 5.3 3.3 (low) 3.3 (low) 3.9 (low)Platelet 160-410 K/uL 98 (low) 57 (low) 65 (low) 72 (low)

During this hospital admission, Mr. B. had a consult with the Paracentesis Team on August
18, in which they compiled his labs and determined that he was eligible for the therapeutic and
diagnostic paracentesis procedure. He also had a consult with the Palliative Care Team to discuss
his quality of life and goals on August 18. Mr. B. expressed that he was not ready for hospice,
but wanted to be discharged to a skilled nursing facility where he could be rehabilitated to return
to living on his own. This request was granted upon discharge on August 21. He told the
Palliative Care consultant that he was going to stop drinking, but on August 20, when a consult
was sent for Outpatient Substance Abuse, he declined to complete their assessment and left with
a card with their contact information.
IV. Medical Nutrition Therapy
Though Mr. B. claims he has adequate access to healthy foods, financial troubles are evident,
as he lives in a motel and is unemployed. Mr. B.’s usual diet consists of ramen noodles and beef
stew from Dollar General, which he says he likes especially because it has carrots. He reports
that one can of soup and one package of noodles, mixed and cooked in the microwave, are
enough to feed him two to three days. He has a history of alcohol abuse; prior to his admission in
July, he typically drank a quarter of a gallon of vodka daily. After his hospitalization in July, he
reports that he decreased his alcohol consumption and now only drinks two to three four-packs
of beer a week, and claims that his drinking is mostly social while watching football with a
friend. He expressed intention to stop drinking, but consistently turned down counseling from the
substance abuse treatment program. He told the physician that he drinks to dull his abdominal
pain.

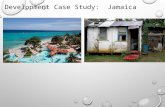
Mr. B. is 5’7” tall, and reports he usually weighs about 180 pounds, though he feels best
at 160 pounds. His ideal body weight is 148 pounds. Weight is not an accurate reflection of
nutritional status for patients with fluid alteration like Mr. B., but a chart is included below with
available recent weight history.
1/13/2014
1/21/2014
1/29/2014
2/6/2014
2/14/2014
2/22/2014
3/2/2014
3/10/2014
3/18/2014
3/26/2014
4/3/2014
4/11/2014
4/19/2014
4/27/2014
5/5/2014
5/13/2014
5/21/2014
5/29/2014
6/6/2014
6/14/2014
6/22/2014
6/30/2014
7/8/2014
7/16/2014
7/24/2014
8/1/2014
8/9/2014
8/17/2014
140
145
150
155
160
165
170
175
180
185
157.2
181.9
172175.4
Mr. B.'s WeightWeight
He was not weighed upon admission, but his estimated weight including accumulated fluid
was approximately 190 pounds. He was weighed on August 21, several days after paracentesis
and several days into his diuretic regimen, when he weighed 175.4 pounds. Assuming that this
was his dry body weight, Mr. B.’s BMI was roughly 27.5, which puts him into the overweight
category. However, considering this patient’s somewhat wasted physical appearance, including
evidence of moderate lipoatrophy in his triceps and evidence of severe temporal muscle wasting,
it is possible that this category could be misleading. His fluid status was greatly improved post
paracentesis, and Dr. Azneer’s notes indicate no edema at that time, but he likely had not reached
his dry body weight. The Veteran had another paracentesis procedure on September 2, 2014, and
following this procedure and further diuresis, the Veteran weighed 167 pounds. Unfortunately,

Mr. B. was not seen by a dietitian during this brief subsequent visit to ascertain if further lean
body mass loss had occurred along with further fluid loss.
Mr. B. had a good appetite after paracentesis on August 18, and reported consuming 75
percent of his dinner that evening and 75 percent of his breakfast the next morning. However, he
experienced nausea on the morning of August 19, and his appetite declined, eating only 50
percent of lunch and dinner that day and none of his breakfast the morning of August 20. He was
prescribed Ondansetron on August 20 to improve consumption. He has some trouble chewing
and reports he sometimes swallows large pieces of food because he is missing his top teeth but
finding it easier to eat without his top dentures. He has no trouble swallowing, and has no
problems with vomiting, constipation or diarrhea (aside from when he takes his Lactulose).
Using the VA Nutrition Status Classification guide, his poor appetite (score of three), his
increased metabolic stress (score of three), evidence of severe fluid alterations and moderately
altered body composition (score of four), Mr. B.’s overall rating is 10, putting him in the
moderately nutritionally compromised category.
Mr. B.’s nutrition diagnosis is:
Inadequate energy intake related to loss of appetite as evidenced by muscle and fat
wasting and diet recall.
In order to improve Mr. B.’s declining nutrition status, it is essential to increase his protein
and energy intake. Mr. B.’s hospital diet during his stay in August was the two gram sodium diet
due to his extreme fluid retention. His overall diet prescription includes calorie, protein, fluid,
sodium, alcohol, and vitamin/mineral recommendations. His nutrient needs are best estimated by
using his ideal body weight (148 pounds), since even diuresed and post-paracentesis, he does not
seem to have reached his dry body weight. His energy needs can be estimated by using the Harris

Benedict equation for basal energy expenditure times a stress factor of 1.2.1 This can be
calculated to 1790 kilocalories per day for Mr. B. The Nutrition Care Manual recommends
protein intake of 0.8 to 1.2 grams per kilogram ideal body weight, or 54 to 81 grams per day for
this patient.1 It is important for him to consume sufficient energy and protein, but not to
overconsume protein, as this will add excess stress to the liver.
It is also important for Mr. B., as a patient with repeated fluid retention and ascites, to restrict
his sodium intake to less than 2 grams a day. With his current diet, this may require major
changes from the canned and processed foods. A fluid restriction is currently not necessary for
hyponatremia according to the Nutrition Care Manual recommendations, as his sodium levels
have been consistently 133 milliequivalents per liter or above;1 however, the physician did order
a fluid restriction of 1200 milliliters per day along with the two gram sodium restriction as his
discharge diet.
Mr. B. also requires increased vitamin and mineral intake. Supplementation is recommended
by the Nutrition Care Manual with water-soluble forms of vitamins A, D, and E, folate, thiamine,
calcium, and zinc, all of which are included in the multivitamin/mineral supplement he was
prescribed. The physician prescribed magnesium and potassium supplements, though these
supplements are actually contraindicated by his medication regimen (potassium supplement with
a potassium-sparing diuretic, though he is simultaneously taking a potassium-losing loop
diuretic, and magnesium supplementation while taking Lactulose).12 It is important to monitor
these labs closely to ensure that he does not retain too much of the supplements and become
hypermagnesemic or hyperkalemic. His lab data indicates anemia, marked by low red blood cell
count, white blood cell count, hemoglobin, hematocrit, and platelet count. This looks like
aplastic anemia caused by his hepatitis C, or low peripheral blood cell count due to possible

splenomegaly, but tests should be done to ensure that it is not caused by a micronutrient
deficiency.6 It also appears that his serum calcium is consistently low, and his diet recall is
significantly calcium and vitamin D-deficient, which could warrant increased intake as well as a
higher dose calcium and vitamin D supplement (both are contained in modest amounts in the
prescribed multivitamin/mineral) to prevent osteopenic bone disease. A DEXA bone scan would
be a better way to check his bone mass and get a better idea of what his body stores are like.
Due to his anorexia and early satiety, eating four to six meals a day will assist with
optimizing energy intake. Daily physical activity may help in increasing hunger and preventing
loss of lean body mass.1 As a final important nutritional recommendation, it is essential for the
Veteran to stop drinking, as his alcohol intake is not only worsening his liver status and
promoting inadequate nutritional intake, but also causing increased vitamin and mineral losses.13
The Veteran’s reported pre-admission dietary intake of approximately half a package of
ramen noodles, half a can of beef stew, and one and a half beers (on average) per day does not
adhere to his calorie, protein, sodium, alcohol, or vitamin and mineral needs and restrictions.
Short-term nutritional goals for Mr. B. to move towards a better nutrition status during his
hospital stay include:
1) Improve intake by offering protein-rich supplements and foods between meals.
2) Consume more than 75 percent of meals and supplements provided.
In order to accomplish these goals during this admission, Boost Plus was provided as a
nourishment, providing 360 kilocalories and 14 grams of protein per serving. Making these
snacks available between meals may help the Veteran increase his intake by providing more
calories and protein throughout the day, allowing him to eat as much as he can whenever he gets
hungry.

On August 19, the Veteran was provided with education on nutrition in liver disease. This
education included limiting salt intake, increasing protein intake to meet needs, eating smaller,
more frequent meals to optimize intake, eliminating or significantly reducing alcohol
consumption, including why it will actually make his disease and his pain worse, and compliance
with medications such as Lactulose, including why he was on the medication and how it would
help him long-term. The Veteran was provided with a handout that reinforced these nutrition
messages. Mr. B. did not appear to be ready to change; though he reported to the dietetic intern
that he had significantly reduced his alcohol consumption following his previous paracentesis, it
is not clear if this really has occurred. He was receptive to education, but expected compliance
upon discharge was uncertain.
Long-term nutritional goals for the Veteran after discharge include:
1) Reduce sodium intake by replacing canned and packaged foods with low-sodium
versions.
2) Eliminate alcohol from the diet.
Since it was determined that Mr. B. would be discharged to Bay Pointe Nursing, a skilled
nursing facility, they were informed of his two gram sodium, 1200 milliliter fluid diet. Mr. B.’s
nurse at Bay Pointe indicated that the Veteran has been compliant with the sodium restriction
since his food is provided; however, he has not been compliant with the fluid restriction, as he
has continued to drink alcohol daily. He had a third paracentesis on September 2, and a fourth on
September 19. He is clearly worsening, and continues to need nutritional intervention. Follow-
ups should be done at least each time he is admitted for paracentesis, with continued education
on alcohol’s contribution to his liver failure. He has significant barriers to disease management
and compliance, including his mood and cognitive disorders, socioeconomic status, and

dependence on alcohol as a painkiller. However, at a skilled nursing facility and with help from
the substance abuse treatment program (if he will participate), these barriers can be overcome.
Mr. B. should continue to be monitored for further muscle and fat wasting, fluid status (both
edema and ascites), adequate protein and energy intake, consumption of alcohol, vitamin and
mineral status indicators, and liver function labs.
V. Summary
According to Dr. Azneer, the attending physician, Mr. B.’s prognosis is grave. Based on the
Model for End-Stage Liver Disease (MELD),7 Dr. Azneer estimated he has approximately three
months to live. Though he is currently in a skilled nursing facility and wishes to be rehabilitated
so he can go back to living on his own, the serious nature of his disease will more likely
necessitate his admission to hospice. Sadly, his health and nutrition status did not improve during
his hospital admission. His nurse at Bay Pointe reported no problems with his appetite and
consumption of 100 percent of his meals on September 17, which is a big change in a positive
direction. With optimal nutritional intake, sodium and fluid restriction, vitamin and mineral
supplementation, and alcohol cessation, Mr. B.’s nutritional status could conceivably improve,
which could improve his short-term survival.2 However, real improvement in his status is
unlikely due to his severe disease state and unwillingness to stop drinking. It is possible that if
his pain were better controlled in general, he would be more likely to stop drinking, but from his
past history with alcohol, complete cessation seems, sadly, unlikely. The only real treatment for
cirrhosis that has advanced to Mr. B.’s state is liver transplant, a treatment they are unlikely to do
on someone with his poor nutritional status, due to increased mortality risk.2

In retrospect, Mr. B.’s cognitive impairments and alcoholism were certainly bigger barriers
to change than it seemed at the time of education. While Mr. B. was agreeable and responsive to
learning about his nutrition care plan, and it seemed that he was making positive change in his
life already (such as decreasing the amount of alcohol he drank), his true self-efficacy and
readiness to change was likely very low. His underlying issues have taken a long time to develop
and could take a lot of time and multidisciplinary effort, as well as his buy-in, to repair. Nutrition
counseling is designed to create buy-in and bring patients from Mr. B.’s precontemplation stage
of change to readiness for action. Mr. B. might have benefited from implementation of the
Health Belief Model, which recommends health education on a personalized, applicable way.
The model is designed to focus on disease prevention, but can be expanded to prevent worsening
of disease. The dimensions of the Health Belief Model are perceived susceptibility to a disease,
perceived severity of the disease, perceived benefits of engaging in healthy behavior, and cues to
action, or stimuli that promote the healthy behavior.14 In Mr. B.’s case, this would have involved
spending more time with Mr. B. explaining the disease process, why his actions (especially
drinking alcohol, consuming too much sodium, and not eating enough) were exacerbating his
health problems and how following his nutrition prescription would help alleviate disease
symptoms and prevent his cirrhosis from worsening as quickly. It would also have involved
addressing the barriers of alcoholism, severe pain, early satiety, and food insecurity, and
acknowledging how they would affect his ability to comply with the nutrition prescription, as
well as creating plans for how to overcome the barriers. The barrier of alcoholism likely requires
professional guidance, such as from SATP, to overcome, but the barrier of food insecurity was at
least temporarily overcome when he was admitted to the skilled nursing facility. Establishing
clear, achievable goals for overcoming barriers will help in building Mr. B.’s self-efficacy and

thus making the change sustainable. Finally, his cues to action, such as abdominal pain cuing
him to take pain medication and stay away from alcohol, rather than drinking to numb the pain.
Application of this counseling method, as well as incorporating motivational interviewing,
building self-efficacy, and using the teachback method to ensure comprehension and to promote
information retention, are important in working with patients like Mr. B. with significant health
concerns and significant barriers to overcome. No patient is a lost cause, and with
multidisciplinary support and compassionate care, Mr. B.’s quality of life can still be
significantly improved.

VI. APPENDIX
a. Nutrition assessment (CPRS)
b. Estimated nutrient needs
c. Handouts provided to patient
d. References

D. References
1Academy of Nutrition and Dietetics (AND). Cirrhosis. Nutrition Care Manual.
http://www.nutritioncaremanual.org. Accessed 9/9/2014.
2Cabre E, Gassull M. Nutritional and metabolic issues in cirrhosis and liver transplantation. Curr
Opin Clin Nutr Metab Care. 2000;3:345-354.
3Fedeli U, Avossa F, Guzzinati S, Bovo E, Saugo M. Trends in mortality from chronic liver
disease. Annals of Epidemiology. 2014;24(7):522-526.
4Ginès P, Cárdenas A, Arroyo V, Rodès J. Management of cirrhosis and ascites. New Eng J
Med.2004;350(16):1646-1654.
5Johnson T, Overgard E, Cohen A, DiBaise J. Nutrition assessment and management in advanced
liver disease. Nutrition in Clinical Practice. 2013;28:15-29.
6Lu Y, Li X, Han X, Gong X, Chang S. Peripheral blood cell variations in cirrhotic portal
hypertension patients with hypersplenism. Asian Pacific Journal of Tropical Medicine.
2013;6(8):663-666.
7MayoClinic. The MELD model. http://www.mayoclinic.org. Accessed September 19, 2014.
8MICROMEDEX. Cirrhosis of liver. http://www.micromedexsolutions.com. Accessed
September 9, 2014.
9Nusrat S, Khan M, Fazili J, Madhoun M. Cirrhosis and its complication: evidence based
treatment. World J Gastroenterol. 2014;20(18):5442-5460.
10Nyblom H, Björnsson E, Simrén M, Aldenborg F, Almer S, Olsson R. The AST/ALT ratio as
an indicator of cirrhosis in patients with PBC. Liver International. 2006;26(7):840-845.
11Poh Z, Chang PEJ. A current review of the diagnostic and treatment strategies of hepatic
encephalopathy. International Journal of Hepatology. 2012. Doi:10.1155/2012/480309.

12Pronsky Z, Crowe S. Food medication interactions. 17th ed. Birchrunville, PA: Food-
Medication Interaction; 2012.
13Singal A, Charlton M. Nutrition in alcoholic liver disease. Clin Liver Dis. 2012;16:805-826.
14Solhi M, Zadeh D, Seraj B, Zadeh S. The application of the Health Belief Model in oral health
education. Iran J Public Health. 2010;39(4):114-119.
15Umemura T, Shibata S, Sekiguchi T, et al. Serum sodium concentration is associated with
increased risk of mortality in patients with compensated liver cirrhosis. Hepatology
Research. 2014. Doi: 10.1111/hepr.12412.
16US Burden of Disease Collaborators. The state of US health, 1990-2010: burden of disease,
injuries, and risk factors. JAMA. 2013;310:591-608.