Case Study 1: MERS-CoV - Society for Healthcare...
44
© SHEA 2017 SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM Case Study 1: MERS-CoV Trish M. Perl, MD, MSc Chief, Infectious Diseases Jay P. Sanford Professor of Medicine UT Southwestern Medical Center
Transcript of Case Study 1: MERS-CoV - Society for Healthcare...

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Case Study 1: MERS-CoV
Trish M. Perl, MD, MSc
Chief, Infectious Diseases
Jay P. Sanford Professor of Medicine
UT Southwestern Medical Center

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Financial Disclosures
Trish M. Perl, MD, MSc
Research support: VA and CDC (mask study), Medimmune
(not vaccine related)
Advisory Boards: Pfizer, Inc., Merck & Co, Inc., DebMed
Worked for Ministry of Health and National Guard Hospital on
MERS-CoV mitigation and control

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Learning Objectives
Upon completion, participants should be able to:
Recognize when to be concerned about potential emerging infections
Understand universal actions that can and should be taken to care for
patients, staff, and public

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Outline
Part I: Background on emerging respiratory infections
Part II: Case study: MERS-CoV
Part III: Reflections and recommendations

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Part I: Background on Emerging Respiratory Infections

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
When Should You Be Concerned About an Emerging Infection? An unusual case or cluster of cases
A previously undetected or unknown infectious agent
A known agent that has:
Spread to new geographic locations or new populations
Re-emerged following a declining incidence of disease
A genetic adaptation changing illness severity
Examples: SARS, MERS-CoV, measles, Zika, human adenovirus 14p1,
influenza (variants H3N2, H7N9)

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Geographic Distribution of Recent Outbreaks*
*As of 2/28/2017. Publichealthwatch.
www.publichealthwatch.wordpress.com; Smith KF, et al. J R Soc Interface. 2014;11:20140950.
HCV
Cryptosporidiosis
Cyclosporiasis
E coli 0157:H7
Vancomycin-resistant
S aureus
Human
monkeypox
Anthrax
bioterrorism
Whitewater
arroyo virus
Hantavirus
pulmonary
syndrome
Dengue
Yellow fever Cholera
Human monkeypox
Diphtheria
Drug-resistant malaria
Multidrug-resistant tuberculosis
Typhoid
fever
Rift Valley
fever
Plague
HIV
Enterovirus 71
Hendra virus
Nipah virus
SARS
H5N1
influenza
Lassa fever
Marburg
haemorrhagic fever
vCJD
West Nile virus
Lyme disease
Ebola
haemorrhagic fever
Vancomycin-resistant
S aureus
E coli 0157:H7

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Transmission of Respiratory Viruses
Remains a source of controversy
Observational studies in healthcare settings indicate that contact
(direct and indirect) and droplet transmission are the primary means
of spread
Relative contributions of each type of transmission is unknown
Anecdotal experience with airborne transmission can be helpful in
understanding the factors that contribute to transmission
Drinka PJ, et al. J Am Geriatr Soc. 2004;52:847-8; Brankston G, et al. Lancet Infect Dis. 2007;7:257-65;
Cunney RJ, et al. Infect Control Hosp Epidemiol. 2000;21:449-54; Morens DM, et al. Infect Control Hosp Epidemiol. 1995;16:275-80.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Which Interventions Are Best at Preventing Respiratory Infections?
Jefferson T, et al. Cochrane Database Syst Rev. 2011;7:CD006207.
Outcome or Subgroup Title
No. of
Studies
No. of
Participants Statistical Method Effect Size
Thorough disinfection
of living quarters
1 990 OR (M-H, Fixed, 95% CI) 0.30 [0.23, 0.39]
Frequent handwashing 6 2,077 OR (M-H, Fixed, 95% CI) 0.45 [0.36, 0.57]
Wearing mask 5 1,991 OR (M-H, Fixed, 95% CI) 0.32 [0.25, 0.40]
Wearing N95 mask 2 340 OR (M-H, Fixed, 95% CI) 0.09 [0.03, 0.30]
Wearing gloves 4 712 OR (M-H, Fixed, 95% CI) 0.43 [0.29, 0.65]
Wearing gowns 4 712 OR (M-H, Fixed, 95% CI) 0.23 [0.14, 0.37]
All interventions 2 369 OR (M-H, Fixed, 95% CI) 0.09 [0.02, 0.35]
Comparison 1. Case Control Studies

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Effectiveness of Precautions: Lessons From SARS
Case-control study in 5 Hong Kong hospitals with 241 noninfected
and 13 infected staff
Retrospective cohort study in 2 Toronto critical care units with
35 noninfected and 8 infected nurses
Seto WH, et al. Lancet. 2003;36:1519-20; Loeb M, et al. Emerg Infect Dis. 2004;10:251-5.
RR (95% CI)
Precaution Hong Kong Toronto
Handwashing 0.2 (0.07-1) N/A
Gloves 0.5 (0.14-1.6) 0.45 (0.14-1.46)
Gown Undef (P = .066) 0.36 (0.10-1.24)
Mask 0.08 (0.02-0.33) 0.23 (0.07-0.78)

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Source Control: Efficacy of Surgical and N95 Masks to Filter Influenza in Positive Patients
Johnson DF, et al. Clin Infect Dis. 2009;49:275-7.
Cycle Number
Patient or Variable Influenza
Type Nasal Swab
No Mask, Before Control (Step 1)
N95 Mask (Step 2)
Surgical Mask
(Step 3)
No Mask, After
Control (Step 4)
Duration of Illness, Days Per
Week
Patient
1 A 31 38 Negative Negative 39 3
2 A 26 40 Negative Negative Negative 1
3 A 22 Negative Negative Negative 40 3
4 A 26 34 Negative Negative 35 1
5 A 23 32 Negative Negative 33 2
6 A 25 27 Negative Negative 25 1
7 B 22 38 Negative Negative 27 2
8 A 29 34 Negative Negative Negative 3
9 B 27 Negative Negative Negative 39 3
Mean cycle time for patients with detected influenza A … 26a 34.17a 0 0 34.4a 2b
Estimated viral load for detected influenza A, copies/mL … 5 milliona 50,000a 0 0 50,000a …
Note: Cycle number indicates real-time RT-PCR cycle number. The cycle number value is inversely proportional to the titer of virus present. aMean value calculated from patients with detectable influenza A. bMean duration.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Nosocomial ARI Outbreaks
Nosocomial outbreaks documented in a variety of healthcare settings, including general medical wards, LTCFs, and pediatrics and oncology units
In 2009, among 1,520 hospitalized patients with pH1N1, 30 acquired influenza nosocomially
57% received antivirals, 53% received escalated care, and 27% died
Nosocomial outbreaks can also result in up to 50% attack rates in staff, staff furloughs, and increased costs for the institution
Enstone JE, et al. Emerg Infect Dis. 2011;17:592-8; Stott DJ, et al. Occup Med (Lond). 2002;52:249-53.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Healthcare-Associated Respiratory Infections: Pediatrics
Of 96 patients, 9% died and 3% of deaths were attributed to FRI
15% (2/13) of children with influenza had been vaccinated, and 80% (4/5) of children with RSV had received
anti-RSV monoclonal antibody Vayalumkal JV, et al. Infect Control Hosp Epidemiol. 2009;30:652-8.
Redraw
Surveillance
Site No. of Cases
Surveillance
Period, Days
No. of
Patient-Days
Infections per
1,000 Patient-Days No. of Admissions
Infections per
1,000 Admissions
A 7 81 7,699 0.91 1,306 5.36
B 35 111 32,413 1.08 4,338 8.07
C 13 111 11,691 1.11 2,301 5.65
D 3 90 4,906 0.61 747 4.02
E 20 119 13,311 1.50 911 24.66
F 11 113 11,461 0.96 1,938 5.68
G 5 119 11,013 0.45 1,750 2.86
H 2 119 6,802 0.29 491 4.07
Total 96 … 99,296 0.97 13,682 7.02
Incidence of Healthcare-Acquired FRI in Patients Younger Than 18 Years Old, Canadian Nosocomial Infection Surveillance Program
Surveillance, 2005

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Healthcare-Associated Respiratory Infections: Pediatrics (cont.)
Vayalumkal JV, et al. Infect Control Hosp Epidemiol. 2009;30:652-8.
Pathogen
No. (%) of
Isolates
RSV 38 (38)
Influenza A 9 (9)
Influenza B 8 (8)
Parainfluenza 11 (11)
Adenovirus 6 (6)
Staphylococcus aureus 7 (7)
Haemophilus influenza 4 (4)
Moraxella catarrhalis 4 (4)
Streptococcus pneumoniae 3 (3)
Pseudomonas aeruginosa 2 (2)
Enterobacter cloacae 2 (2)
Other bacteria 6 (6)
= 72%

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Speciesa Total No. of Outbreaksb
Outbreaks Including Some Kind of Closure Closure Rate P Value
S aureus 223 23 10.3% NS
Hepatitis virus 150 6 4.0% .002
Pseudomonas spp 130 10 7.7% NS
Klebsiella spp 115 10 8.7% NS
Acinetobacter spp 105 24 22.9% .02
Serratia spp 94 14 14.9% NS
Enterococci 67 8 11.9% NS
Enterobacter spp 66 10 15.2% NS
Streptococci 63 18 28.6% .001
Salmonella spp 56 4 7.1% NS
Legionella spp 48 2 4.2% NS
Norovirus 34 15 44.1% < .001
Clostridium spp 34 4 11.8% NS
Aspergillus spp 25 5 20.0% NS
Influenza/parainfluenza virus 26 10 28.5% < .001
Citrobacter spp 12 3 25.0% NS
Adenovirus 11 3 27.3% NS
Shigella spp 11 4 36.4% .04
Rotavirus 27 7 25.9% .05
SARS coronavirus 12 4 33.3% NS
Total 1,561 194 12.4% —
Unit Closure Rates for Various Pathogens
Hansen S, et al. J Hosp Infect. 2007;65:348-53.
Closure Rates in Outbreaks Stratified by the Causative Pathogen (Outbreak Database, N = 1,561)
aOnly pathogens that had been reported in at least 10 outbreaks are included. bMultiple answers possible.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Part II: MERS-CoV Outbreaks

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
MERS-CoV: Saudi Arabia, 2012
60-year-old Saudi man admitted to
hospital on June 13, 2012
7-day history of fever, productive
cough, and shortness of breath
No history of cardiopulmonary or
renal disease, no long-term
medications, nonsmoker
Treatment
Oseltamivir, levofloxacin, piperacillin-
tazobactam, and micafungin
Physical Examination
Findings
BP 140/80 mm Hg
HR 117 beats/min
Temp 38.3° C
RR 20 breaths/min
Zaki AM, et al. N Engl J Med. 2012;367:1814-20.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Immediate Steps
Data to collect and/or consider
Exposures Other ill persons
Animals
Season
Travel
How do I protect HCP, visitors, and other patients?
Isolation/cohorting
PPE
Source control

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Re-Evaluate
Data to collect and/or consider Exposures
Other ill persons
Animals
Season Travel
Do I need additional measures in place to protect HCP, visitors, and other patients? Isolation/cohorting PPE Source control

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
What Now?
We have:
Atypical and severe
respiratory illness with
routine diagnostic testing not
revealing expected pathogens
Unusual finding on viral
cultures
No expected “exposures”
We should:
Send specimen for additional
testing
Ensure appropriate isolation
and PPE
Conduct a literature search
Call public health authorities
regarding other potential cases
Call colleagues regarding other
potential cases

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
ProMED-mail: Saturday, September 15, 2012
A new human coronavirus was isolated from...sputum of a male patient aged
60 years old presenting with pneumonia associated with acute renal failure.
Testing with a pancoronavirus RT-PCR yielded a band at a molecular weight
appropriate for a coronavirus. The virus RNA was also tested in Dr. Ron
Fouchier's laboratory in the Netherlands and was confirmed to be a new
member of the beta group of coronaviruses, closely related to bat
coronaviruses.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
What Do We Know About Coronavirus?
Single-stranded RNA
Common cause of respiratory
virus infections
Mild infections: alpha 229E and
NL63, beta OC43
Severe infections: SARS-CoV,
MERS-CoV
Natural hosts include bats, civet
cats, dogs, and rodents
CDC. www.cdc.gov;
Graham RL, et al. Nat Rev Microbiol. 2013;11:836-48.
Membrane protein
Nucleocapsid protein
Spike protein
RNA
Envelope protein

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Sequencing MERS-CoV
Originally named HCoV-EMC
Belongs to lineage C of the
genus β-coronavirus (with
bat coronaviruses HKU4
and HKU5)
SARS-CoV is lineage B
6 human coronaviruses
indicated in red
Milne-Price S, et al. Pathog Dis. 2014;71:121-36.
δ
β
α
γ
A
B
D
C
94
80
100
100
96
88 88
100
100
100
96
83
100
100
100
100
96
BtC
oV
-HK
U7
96

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Bermingham A, et al. Euro Surveill. 2012;17:20290; Pebody RG, et al. Euro Surveill. 2012;17:20292.
MERS-CoV: England, 2012
On September 14, 2012, a patient with unexplained severe respiratory illness was transferred to intensive care in London after traveling from Qatar
Negative for specific and well-known coronaviruses
Positive for general coronavirus family
Sequence showed genus β-coronavirus with closest relationships to bat coronaviruses HKU4 and HKU5
99.5% sequence similarity to novel human coronavirus recovered from a Saudi Arabian man who died in June 2012
13 close contacts (all HCWs) with mild self-limiting respiratory illnesses

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
WHO Global Alert: Sunday, September 23, 2012
WHO. www.who.int.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
MERS-CoV: Saudi Arabia (Al-Hasa), 2013
7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 1 2 3 4 5 6 7 8 9 10 11 12 13 14
0
4
2
3
4
April 2013 May 2013
No
. o
f N
ew
Ca
se
s
Acquired in Dialysis Unit, Hospital A
Acquired in Hospital B, C, or D
Acquired in ICU, Hospital A
Acquired in Ward 1, Hospital A
Acquired in Ward 2, Hospital A
Community-Acquired
Assiri A, et al. N Engl J Med. 2013;369:407-16.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Evaluating the Situation Further
What key facts do you need to determine?
Who?
What?
Where?
When?
What is the likely transmission? Or source?
What is the incubation period? Serial interval?
What is a case?
Line list
Epidemic curve
Exposure history

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
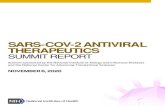
Who, What, When, Where: Al-Hasa, 2013
Important epidemiologic
findings from the Al-Hasa
outbreak
Interhospital transmission
Transmission in ICU and
crowded settings
Key individuals who spread
to many other individuals
Assiri A, et al. N Engl J Med. 2013;369:407-16.
Family Member
HCW
Patient
Confirmed Case
Probable Cause
Community
Ward 1, Hospital A
Ward 2, Hospital B
Dialysis, Hospital A
ICU, Hospital A
Ward, Hospital B
Dialysis, Hospital C
ICU, Hospital D
Ward, Hospital D
Transmission Map of Outbreak of MERS-CoV Infection
All confirmed cases and the two probable cases linked to transmission
events are shown. Putative transmissions are indicated as well as the
date of onset of illness and settings.
April
8 13
6 29 22 15
May

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Transmission Dynamics
Incubation period
The time from exposure to developing symptoms
Serial interval
The time between successive cases
Ex: the time between when the first case develops symptoms and the onset in a
secondary case

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Outbreak Transmission Dynamics: Al-Hasa, 2013
Estimated incubation period: 5.2 days (95% CI, 2.2-12.4) (SARS 4.0 days [95% CI, 1.8-10.6])
Estimated serial interval: 7.6 days (95% CI, 3.0-19.4) (SARS median 8.4 days) Assiri A, et al. N Engl J Med. 2013;369:407-16.
0 15 10 5
0.0
0.2
0.4
0.6
0.8
1.0
Days After Infection
Pro
po
rti
on
Wit
h S
ym
pto
ms
Incubation Period
0 5 10 15 20 25 30
0.0
0.2
0.4
0.6
0.8
1.0
Days After Symptom Onset in Patient
Transmitting Infection
Pro
po
rti
on
Wit
h S
ym
pto
ms
Serial Interval

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Basic Reproduction Number (R0): How Infectious Is MERS-CoV?
R0 is the number of secondary infections caused by a primary case
in an entirely susceptible population
Al-Hasa MERS-CoV R0 estimated to be in the range of 0.6-0.69
Prepandemic SARS-CoV was 0.8
Relatively small cluster sizes indicate transmission can be controlled
once the clusters are detected and interventions put in place
In the absence of controls, Rindex of clusters was in the range of 0.8-1.3
Chains of transmission were not sustained with infection control
measures
Breban R, et al. Lancet. 2013;382:694-9; Cauchemez S, et al. Lancet Infect Dis. 2014;14:50-6.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
MAR APR MAY JUN JUL AUG SEP OCT NOV DEC JAN FEB MAR APR MAY JUN JUL AUG SEP OCT NOV DEC
2012 2013
Jordan: Two deceased
patients are
retrospectively
diagnosed with MERS-
CoV (Hjawi et al 2013)
September 20, 2013: Dr. Ali
Mohamed Zaki reports the
isolation of a novel
coronavirus in a ProMED-mail
post
A family cluster in the UK
provides definitive evidence of
human-to-human transmission
(Health Protection Agency
2013)
A hospital outbreak of MERS-
CoV in Saudi Arabia forms the
largest cluster to date (Assiri
et al 2013)
October 13-18, 2013:
Almost 2 million pilgrims
gather in Saudi Arabia for
the 2013 Haij
MERS-CoV detected in
three camels in Qatar; the
animals are linked to human
cases (ProMED-mail)
MERS-COV–specific RT-
PCR assays are developed
and used for the diagnosis of
the second MERS-CoV
patient (Bermingham et al
2012; Corman et al 2012)
Erasmus Medical Center
characterizes the full genome
of MERS-CoV (van
Boheemen et al 2012)
DPP4 is established as the
cellular receptor for MERS-
CoV (Raj et al 2013)
MERS-CoV infection in
rhesus macaques fulfills
Koch’s postulates (Munster
et al 2013)
Crystal structure for MERS-
CoV bound to its receptor is
determined (Lu et al 2013;
Wang et al 2013)
MERS-CoV neutralizing
antibodies are found in Omani
camels (Reuskein et al 2013)
Treatment with
interferon alfa-2b and
ribavirin improves
outcome in MERS-
CoV–infected rhesus
macaques (Fatzarano
et al 2013)
An RNA fragment identical to MERS-CoV
is recovered from an Egyptian tomb bat
in Saudi Arabia (Mernish et al 2013)
A phylogenetic analysis of 21
MERS-CoV genomes suggests
multiple zoonotic introductions
(Cotton et al 2013)
Timeline of MERS-CoV Outbreaks (2012-2013)
Milne-Price S, et al. Pathog Dis. 2014;71:121-36.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
MERS-CoV: South Korea, 2015
A 68-year-old South Korean man developed fever and myalgia
on May 11, 2015, after returning from a business trip to the
Middle East
He was diagnosed with MERS-CoV on May 20, 2015, after
contacting approximately 600 people during his visits to health
centers
26 cases were confirmed from these initial contacts; transmission
via nosocomial infection followed after that
Korea Centers for Disease Control and Prevention. Osong Public Health Res Perspect. 2015;6:269-78.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
MERS-CoV: South Korea, 2015
Approximately one-half of the MERS-CoV cases (92/186) in South
Korea were associated with a 1,950-bed, tertiary care university
hospital
82 cases originated from one unprotected exposure
Crowded emergency department
Experimental evidence later supported the possible contribution
of MERS-CoV contamination of air and surrounding materials in
the outbreak
Park GE, et al. Ann Intern Med. 2016;165:87-93; Cho SY, et al. Lancet. 2016;388:994-1001;
Kim SH, et al. Clin Infect Dis. 2016;63:363-9.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Environmental Contamination: South Korea, 2015
Rooms of 4 patients in 2 hospitals examined for environmental
contamination of MERS-CoV
Gathered air samples and swabbed high-touch and ventilation
surfaces for viral culture and PCR
4/7 air samples tested positive
15/68 surfaces contaminated with MERS-CoV live virus
Room, anteroom, medical equipment (bed sheets and rails, IV fluid
hangers, tables, outlets)
Many surfaces PCR-positive up to 27 days after symptom onset
Kim SH, et al. Clin Infect Dis. 2016;63:363-9.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Comparison of Case and Environment: South Korea, 2015
Patient Data Environmental Data
Hospital No. Case Status
Time of Sampling for
PCR (Days After
Symptom Onset) MERS-CoV PCR Results
Environmental
Sampling
RT-PCR
From
Samples
RT-PCR
From Viral
Culture
A 1 Pneumonia on mechanical ventilation
and ECMO 22 (+) at the time of sampling Air sampling 2/2 1/2
Fomites swab 4/6 2/6
Fixed-structure swab 7/13 2/13
2 Pneumonia on mechanical ventilation 16 (+) at the time of sampling Air sampling 2/2 2/2
Fomites swab 4/4 3/4
Fixed-structure swab 12/12 5/12
Elevator Fixed-structure swab 1/5 0/5
B 3 Pneumonia and bedridden 19 (-) at the time of sampling Air sampling 3/3 1/3
Fomites swab 5/6 2/6
Fixed-structure swab 8/17 0/17
Elevator Fixed-structure swab 1/5 1/5
Kim SH, et al. Clin Infect Dis. 2016;63:363-9.
Patient Case Status and Environmental Test Results in 2 MERS-Designated Hospitals, Republic of Korea

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Part III: Reflections and Recommendations

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Why Did These Outbreaks Occur?
Surveillance and case finding are limited
Unable to identify cases in a timely fashion (diagnostic and logistics)
PCR testing can take 4 or 5 days
Serology is unreliable
Variable approaches to screening
Poor recognition of syndromes and risk factors
Spectrum of disease not identified early
Risk factors for transmission in healthcare not fully understood

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Why Did These Outbreaks Occur? (cont.)
System issues
Intrahospital transfers
Visitation and family care policies
Poor internal and external communication
Lack of transparency about outbreak facts to public health community
Isolation precautions and use of barrier precautions not followed or understood
Inadequate quantities of isolation materials
Confusion about recommendations for barrier precautions to be used (CDC vs WHO)

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Guidelines for MERS-CoV: Before the First Case Preparation
Surveillance
Education
Laboratory readiness
Communication
Planning
Case treatment
PIDAC. www.picnet.ca.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Guidelines for MERS-CoV: Management
Accommodation
Additional precautions
Diagnosis
Communication
Education/training
Follow-up for identification of transmission
PIDAC. www.picnet.ca.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
The Science: SARS vs MERS* SARS MERS
Cumulative number of case(s) 8,098 1,905
Number of deaths 774 677
Case fatality ratio (%) 9.6% 35%
Number of countries 29 27
Total publications 2,854 475
Case reports 135 21
Clinical trials 33 1
Comparative studies 145 9
Evaluation studies 48 0
Meta-analysis 1 0
Perl TM, et al. Ann Intern Med. 2015;163:313-4; WHO. www.who.int; Arabi YM, et al. Ann Intern Med. 2014;160:389-97.
*As of 2/28/2017.

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Summary
MERS-CoV provides a recent example of an emerging pathogen that was amplified in healthcare where transmission resulted from a failure of recognition, issues with collaboration and communication, and suboptimal laboratory identification
Risk factors are not well studied (mostly observational), and case-control studies are essential
Current prevention strategies (including standard recommendations):
Early recognition and diagnosis, hand hygiene, isolation, appropriate use of and adherence to PPE, cohorting, reporting, cleaning and disinfection
Research is essential to answer key questions about transmission and risk factors for transmission

© SHEA 2017
SHEA/CDC OUTBREAK RESPONSE TRAINING PROGRAM
Additional Resources
MERS Provider and Facility Preparedness Checklists. Centers for Disease
Control and Prevention.
www.cdc.gov/coronavirus/mers/preparedness/index.html
Preparedness Resources (MERS). Centers for Disease Control and
Prevention. www.cdc.gov/coronavirus/mers/preparedness/resources-
preparedness.html
MERS: Information for Healthcare Professionals. Centers for Disease Control
and Prevention. www.cdc.gov/coronavirus/mers/hcp.html
Interim Infection Prevention and Control Recommendations for Hospitalized
Patients with MERS-CoV. Centers for Disease Control and Prevention.
www.cdc.gov/coronavirus/mers/infection-prevention-control.html