Case Studies AMA5, 2011 WA F M - acdmed.org · AMA Guides 5th Ed. Case Studies Syllabus Mohammed I...
153
AMA Guides 5th Ed. Case Studies Syllabus Mohammed I Ranavaya MD, MS, FRCP, FFOM 1 © 2011 Format only ACDM Inc. American Board of Independent Medical Examiners And American College of Dis/Ability Medicine PRESENTS AMA Guides 5th Ed. Training Program Format © 2007 Mohammed I. Ranavaya, M.D., M.S. Introduction This Teaching program was created by Prof. Ranavaya MD,JD, MS, FRCP, for American College of Dis/Ability Medicine to teach physicians and others how to use the Guides to the Evaluation of Permanent Impairment, 5th ed. published by the American Medical Association. It is essential to have the AMA Guides to the Evaluation of Permanent Impairment 5 th ed for the best learning experience from this program
Transcript of Case Studies AMA5, 2011 WA F M - acdmed.org · AMA Guides 5th Ed. Case Studies Syllabus Mohammed I...
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
1© 2011 Format only ACDM Inc.
American Board of Independent Medical ExaminersAnd
American College of Dis/Ability MedicinePRESENTS
AMA Guides 5th Ed. Training Program
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Introduction
This Teaching program was created
by Prof. Ranavaya MD,JD, MS, FRCP, forAmerican College of Dis/Ability Medicineto teach physicians and others how touse the Guides to the Evaluation ofPermanent Impairment, 5th ed. publishedby the American Medical Association.
It is essential to have theAMA Guides to theEvaluation of PermanentImpairment 5th ed for thebest learning experiencefrom this program

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
2© 2011 Format only ACDM Inc.
Mohammed I. Ranavaya, MD, JD, MS, FRCPI, FFOM, CIME
Professor, Marshall Univ. School of Medicine
WEST VIRGINIA
Appalachian Institute of Occupational and Environmental Medicine100 Constitutional Avenue, Chapmanville, WV 25508. USA
PHONE: (304)733-0095 EMAIL: [email protected]
AMA Guides 5TH Edition
Advanced Case Studies
CASE STUDIESThe AMA Guides to the Evaluation of
Permanent Impairment, 5th Edition
SpineCASE STUDY #1
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
3© 2011 Format only ACDM Inc.
Cervical Spine
Ms Brown is a 35 Y/O Flight attendant.
Previously in excellent health with nomedical history of illness, operations, orinjuries of any significance.
Aerobic exercise enthusiast, involved inregular swimming, aerobics, and walking.
Case of pain in the Neck
She was driving home from work 12 months ago
and was stopped at a stop sign.
She was wearing her seat belt and recalls
hearing the screech of brakes and then a crash in
the rear of her car.
The impact threw her body backward and then
forward, but no direct trauma to her body
Cervical Spine
Case of pain in the Neck
No further impact of vehicles.
She recalls soreness in her neck almost
immediately after she had the accident but
was preoccupied with the business of getting
the other driver’s details, speaking to the
police, and then getting her car towed to a
body shop.
Cervical SpineCase of pain in the Neck

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
4© 2011 Format only ACDM Inc.
By the time she got home her neck was very
painful and stiff, and her right arm was aching.
She did not have loss of sensation in the
arm or dysthesia (OWS).
She went to ER that evening and had
C-spine X-rays, which showed some early
degenerative disease but no acute injury
ER Doc gave her a soft cervical collar, NSAID,
physical therapy and follow up with PCP.
Cervical SpineCase of pain in the Neck
After continued soreness and a stiff neck forweeks, her family doctor decided to obtainflexion and extension cervical x-rays.
X-rays reported as normal, apart from someflattening of normal lordosis, i.e. muscle spasm.
She continued her NSAID medications andphysical therapy, but felt that neither of thesewere helpful in relieving her symptoms, howeverher right arm pain had resolved.
Cervical Spine
Case of pain in the Neck
She discontinued treatment after 3 months.
4 months after the accident, she went to
Orthopedist, still complaining of pain &stiffness in the neck,
Orthopod ordered an MRI of the neck,which was reportedly normal.
Cervical SpineCase of pain in the Neck

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
5© 2011 Format only ACDM Inc.
Orthopedist diagnosed resolving Cervical strain/sprain “a whiplash injury to the neck”.
Recommended that she continue walking andswimming, but avoid aerobics.
Orthopedist saw nothing further to test or treat
He said “she would probably be better within next6 to 12 months.”
Cervical SpineCase of pain in the Neck
On IME for Impairment rating a year later:– She says that over the last 9 months there has
been a lot of improvement.
– Occasionally she feels stiffness in the neckbut only when she is tired or after a hardday’s work. she finds that stiffness getsbetter with rest.
– She has no symptoms that suggest cervicalnerve root irritation or cervical radiculopathy.
Cervical SpineCase of pain in the Neck
Cervical Spine
Case of pain in the Neck
Examination– Cervical range of motion found normal
– No evidence of spasm or muscle guarding.
Rest of the physical exam is normal withoutany clinical evidence of neurologicalabnormality in the upper limbs (power,sensation, and reflexes all normal).
There is no muscular atrophy in the arms.

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
6© 2011 Format only ACDM Inc.
Cervical Spine
Impairment Rating
This is an example of an uncomplicatedneck injury that had been symptomatic,but has clearly improved with minorintermittent residual symptoms and noother clinical (objective) abnormalitysuggestive of a more serious injury orresidual impairment.
Cervical Spine
Impairment Rating
Acceleration/deceleration injuries to thecervical spine are relatively common events
Next Step: Determine the Appropriatemethod for Assessment under AMA5– “The DRE method is the principal methodology
used to evaluate an individual who has had adistinct injury” (AMA 5, pg. 379)
Cervical Spine
Impairment Rating
The diagnosis-related estimates methodmust be used to assess impairment inthis case, since the impairment is due toan injury, and none of the five clinicalsituations are present that would requirethe use of range-of-motion method.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
7© 2011 Format only ACDM Inc.
Cervical Spine
Impairment Rating
To use the DRE method:
– obtain an individual’s history
– examine the individual
– review the results of appropriate diagnosticstudies
– place the individual in the appropriate category
Cervical SpineImpairment Rating
All findings must be carefullyassessed and documented, such as:
– The nature of the injury
– The clinical progress of the case
– The presence or absence of significantradiographic findings
– The presence or absence of clinicalabnormalities
Cervical Spine
Impairment Rating
The presence or absence of clinical
abnormalities are:
– cervical spinal mobility
– spasm and guarding
– peripheral nervous system findings
– central nervous system findings
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
8© 2011 Format only ACDM Inc.
Cervical Spine
Impairment Rating
These clinical findings provide thecriteria (including categorydifferentiators) that allow the evaluatingdoctor to be accurate and consistent inthe impairment assessment under theDRE model.
15.6 DRE: Cervical Spine
15.6
392-394
Cervical Spine
Impairment Rating
Almost all individuals will fall into oneof the first three DRE categories
The physician can assign an individualto DRE category I, II, or III.
An individual in category I has onlysubjective findings
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
9© 2011 Format only ACDM Inc.
392
5 Categories based
on Symptoms, signs,
Tests Fractures and/
or dislocations
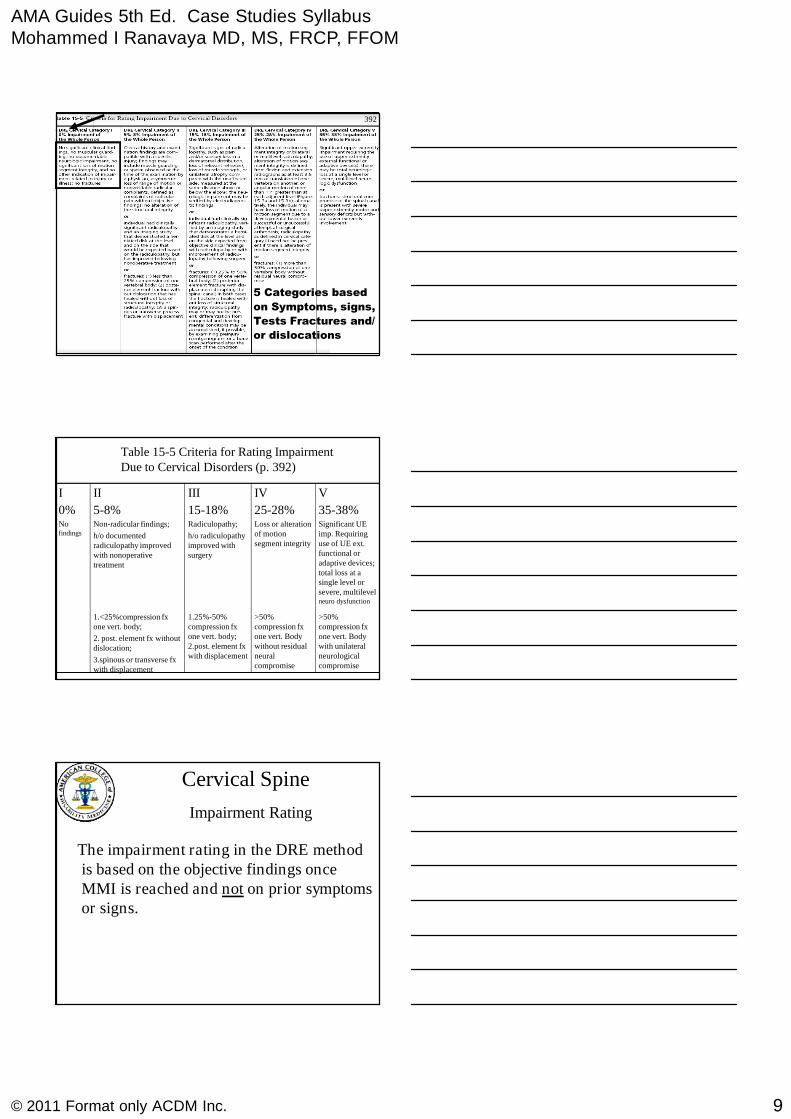
Table 15-5 Criteria for Rating ImpairmentDue to Cervical Disorders (p. 392)
>50%compression fxone vert. Bodywith unilateralneurologicalcompromise
>50%compression fxone vert. Bodywithout residualneuralcompromise
1.25%-50%compression fxone vert. body;2.post. element fxwith displacement
1.<25%compression fxone vert. body;
2. post. element fx withoutdislocation;
3.spinous or transverse fxwith displacement
Significant UEimp. Requiringuse of UE ext.functional oradaptive devices;total loss at asingle level orsevere, multilevelneuro dysfunction
Loss or alterationof motionsegment integrity
Radiculopathy;
h/o radiculopathyimproved withsurgery
Non-radicular findings;
h/o documentedradiculopathy improvedwith nonoperativetreatment
Nofindings
35-38%25-28%15-18%5-8%0%
VIVIIIIII
Cervical Spine
Impairment Rating
The impairment rating in the DRE methodis based on the objective findings onceMMI is reached and not on prior symptomsor signs.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
10© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Cervical Spine
Impairment Rating
Ms Brown had no significant clinicalfindings when she was at MMI; therefore,she meets the definition of a DRE cervicalcategory I in Table 15-5 (AMA Guides 5th ed, p 392)
Impairment:
0% impairment of the whole person
SpineCASE STUDY #2
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Back Injury Case StudyDocumented radiculopathy - resolved
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
11© 2011 Format only ACDM Inc.
Cervical Spine
Impairment Rating
A 40 year old construction worker hurthis back pulling on a drill bit that wasstuck in the ground.
He experienced severe back and rightsided leg and foot pain.
Diminished sensation in S1 distribution
No motor weakness found in foot/leg
Cervical Spine
Impairment Rating
Right ankle reflex somewhat diminished
Imaging studies revealed L5-S1 leveldisk herniation.
Right S1 radiculopathy was diagnosed.
He declined surgery and respondedwell to conservative care
Cervical Spine
Impairment Rating
He was back to light work in six weeks,and back to his usual work in 4 months.
One year later on IME, he had no legpain, occasional back pain mainly afterwork and some stiffness in back.
He was working regularly full duty

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
12© 2011 Format only ACDM Inc.
Cervical Spine
Impairment Rating
His back exam revealed no tenderness
on palpation
Lumbar range of motion normal
Neurological examination normal.
No motor weakness or sensory lossfound in foot/leg
He can walk on heels and toes well
15.2 Determining the AppropriateMethod for Assessment
Diagnosis-Related Estimate (DRE) VSRange-of-Motion (ROM) Method
15.2
379-381
Diagnosis-Related Estimate (DRE)VS
Range-of-Motion (ROM) Method
“The DRE method is the principalmethodology used to evaluate anindividual who has had a distinct injury”
WorkCover WA Guides 3rd Ed excludesRange of motion method in spine cases.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
13© 2011 Format only ACDM Inc.
392
5 Categories based
on Symptoms, signs,
Tests Fractures and/
or dislocations
DRE Category II5 % - 8 % Whole Person
History and examination findings compatiblewith a specific injury.
“Clinical findings” (Box 15-1) when at MMI
No radiculopathy OR
Had (past tense) radiculopathy, imaging studyrevealed HNP “at the level and on the side thatwould be expected based on … radiculopathy,but no longer has the radiculopathy followingconservative treatment.”
15.4
385
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
• According to the 5th edition, at MMI hiscondition best fits into Lumbar DRE II,since radiculopathy has resolved.His impairment is 5% - 8% of the wholeperson. Since he is asymptomatic and hisphysical examination is normal, I wouldrate him at lower end-- 5% WPI.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
14© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Why is his condition not in DRE III?
Because….. At MMI
DRE category III requires…...
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
DRE Category III10 – 13 % Impairment
Significant Radiculopathy– “Significant Pain and/or” (Findings) …
Dermatomal sensory loss (undefined)
– Loss of relevant reflex(es)
– Loss of strength or Atrophy.
– May be verified by Electrodiagnositic Studies
OR: “Individuals who had surgery forradiculopathy but are now asymptomatic.”
15.4
386
SpineCASE STUDY # 3

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
15© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Recurrent radiculopathy
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Time Marches on……..
Five years later, the same individualin the preceding example, fell at workand re-injured his back. He hadsevere back and right leg pain, and a
diminished right ankle reflex.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
When he failed to respond toconservative measures, a laminectomywas performed. He did not do wellafter surgery, and continued withsevere back pain and some moderate
residual leg pain.

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
16© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
One year after surgery, he had notreturned to work. He had gained 35pounds, and took 3-4 Vicodin and 6-8Tylenol a day to control his pain.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
He reported some ADL difficulties.Driving long distance caused foot togo to sleep. Inability to mow thelawn. Mild sleep disturbance
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
His wife had gone to work, andhe did some light housework andtook care of his children.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
17© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Examination revealed motions asfollows:Hip flexion: 50 °Lumbar flexion 20 °Lumbar extension 10 °Right lateral bending 15 °Left lateral bending 15 °
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
There was still a diminished rightankle reflex. Strength of ankleflexion was normal, and sensibility inhis foot was normal. X-rays wereunremarkable.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
MRI showed findings compatiblewith scarring, but no disc protrusioncausing compression.

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
18© 2011 Format only ACDM Inc.
Impairment Rating Low Back Injurywith Recurrent Radiculopathy
DRE vs. ROM
Which Method to use?WorkCover WA Guides 3rd Ed
excludes Range of motion method
in spine cases. So Use DRE method
392
5 Categories based
on Symptoms, signs,
Tests Fractures and/
or dislocations
DRE Category III ???10 – 13 % Impairment
AT MMISignificant Radiculopathy
– “Significant Pain and/or” (Findings) …Dermatomal sensory loss (undefined)
– Loss of relevant reflex(es)
– Loss of strength or Atrophy.
– May be verified by Electrodiagnositic Studies
OR: “Individuals who had surgery forradiculopathy but are now asymptomatic.”
15.4
386
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
19© 2011 Format only ACDM Inc.
Using the DRE Method……..
He is now in Lumbar category III.10% - 13% impairment of the wholeperson. Because of the severity ofsymptoms, I would rate him at thehigher value. 13% impairment of thewhole person
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
We can apportion between the twoinjuries, the first work related, and thesecond work related, the differenceaccording to the 5th edition is:13% - 5% = 8% whole person impairment
Apportionment??
SpineCASE STUDY # 4

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
20© 2011 Format only ACDM Inc.
A 49-year-old dock worker experiencedsudden low back pain and bilateral lowerextremity “numbness” after lifting a heavycrate at work.
Several episodes of Bladder incontinence
No prior history of similar episodes.
Low Back Injury withCauda Equina
Low Back Injury withCauda Equina
Initial examination revealed:
– muscle guarding
– Dsymetria
– diminished strength of bilateral quadriceps
– full strength of his bilateral gastrocnemius ,
extensor hallucis longus, anterior tibialis
Low Back Injury withCauda Equina
Examination con’t:
– diminished sensation of his perineum andbilateral proximal anterior calf
– absent patellar tendon reflexes bilaterally
– normal Achilles tendon reflexes
– normal anal sphincter tone

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
21© 2011 Format only ACDM Inc.
Low Back Injury withCauda Equina
Examination con’t:
– Lumbar spine MRI revealed a large posterocentralherniated nucleus pulposus at L3-4 with a free diskfragment, resulting in multilevel nerve root compression
– Lumbar plain films with flexion and extension viewsrevealed no loss of motion segment integrity
Low Back Injury withCauda Equina
Surgical treatment included decompressivelaminectomy at L3-4 with excision of theherniated disk material and free fragment.
One year after surgery, he reported mild residuallow back pain and difficulty with ADL mainlywalking limited to level surfaces. Can not climbstairs due to leg weakness.
He denied difficulty with bowel or bladdercontrol.
Low Back Injury withCauda Equina
On examination 1 year after surgery:
– He reported diminished sensation in his anterio-lateral thigh/knee area bilaterally
– patellar deep tendon reflexes were absent
– muscular strength of his quadriceps femoris wasdiminished (4/5 - manual testing) but the remainderof his neurological examination was normal
– straight-leg raising was negative bilaterally
– Lumbar ROM were measured and found normal
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
22© 2011 Format only ACDM Inc.
Low Back Injury withCauda Equina
Impairment Rating --What Method to Use?
DRE VS ROM ?
Determining the Appropriate Method
for Assessment: “The DRE method
is the principal methodology used to
evaluate an individual who has had a
distinct injury”
Low Back Injury withCauda Equina
Impairment Rating --What Method to Use?
DRE VS ROM ?
Claimant’s injury was cauda equinasyndrome with initial bladdercompromise.
The residual bilateral leg weakness iscorticospinal tract involvement
Low Back Injury withCauda Equina
Impairment Rating --What Method to Use?
DRE VS ROM ?The DRE method combined with a
rating for corticospinal tract damage isused to assess impairment in this case,because instruction on pg.380, #3 state
“use the DRE method forcorticospinal tract involvement”.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
23© 2011 Format only ACDM Inc.
Low Back Injury withCauda Equina
According to the GUIDES lumbar nerveroot injuries that result in cauda equinasyndrome are rated as Corticospinal Tractinvolvement as in cervical and thoracicinjuries that damage the corticospinal tractof the spinal cord.
Low Back Injury withCauda Equina
Impairment Rating Corticospinal Tract injury
The recommended system is thatfrom the nervous system chapter,which has been reprinted in thespine chapter as Table 15-6, 396-7
Low Back Injury withCauda Equina
Rating Corticospinal Tract Impairmentresulting from Station & Gait Disorders
Table 15-6, 396, Sec C
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
24© 2011 Format only ACDM Inc.
Low Back Injury withCauda Equina
Impairment Rating Corticospinal Tract injury
According to Table 15-6, RatingCorticospinal Tract Impairment, Sectionc, Criteria for Rating Impairments Dueto Station and Gait Disorders, this casemeets the definition of class 2.
Low Back Injury withCauda Equina
Impairment Rating Corticospinal Tract injury
This corresponds with a 10% to 19%impairment of whole person.
A higher value of 19% was selected due tosignificant effect on ADL.
This must be combined with applicableDRE impairments
Low Back Injury withCauda Equina
Impairment Rating using DRE Method
DRE Method Classification:
– Lumbar (low back) injury in rated accordingto the Table 15-3, Criteria for RatingImpairment Due to Lumbar Disorders.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
25© 2011 Format only ACDM Inc.
392
5 Categories based
on Symptoms, signs,
Tests Fractures and/
or dislocations
Low Back Injury withCauda Equina
Impairment Rating using DRE Method
Claimant had surgery for radiculopathy;therefore, he meets the second definitionof DRE lumbar category III in Table 15-3.
This corresponds with a rating of 10% to13% impairment of the whole person.
Low Back Injury withCauda Equina
Impairment Rating using DRE Method
The Guides’ states, “if residual symptoms orobjective findings impact the ability toperform ADL, despite treatment, the higherpercentage in each range should be assigned”
Therefore the claimant was assigned13% impairment of whole person
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
26© 2011 Format only ACDM Inc.
Low Back Injury withCauda Equina
Impairment Rating Corticospinal Tract injury
Final Impairment Calculation:
19% impairment from table 15-6combined with 13% impairment fromtable 15-5 (Cervical DRE table) comesto a total 30% of whole person
SpineCASE STUDY # 5
A 27 year old man fell from a building underconstruction, sustaining a fracture dislocationat the thoraco lumbar junction, with >50%T12 compression with immediate & completeparaplegia at this level. He had surgicaldecompression at T12 and fusion from T10 to
L2, but recovered no neurologic function.
Thoracic spine fracturewith paraplegia

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
27© 2011 Format only ACDM Inc.
One year later IME for rating:
He has no neurologic function below L2
He is wheel chair bound
Has intermittent bladder dribbling, novoluntary control and requires intermittentself catheterization.
Thoracic spine fracturewith paraplegia
One year later IME for rating:
His bowel function has reflex regulationbut no voluntary control-- requires enemas
He has no sexual functioning .
He has a deep ulcer 5 cm. in diameter overhis left ischial tuberosity.
Thoracic spine fracturewith paraplegia
15.5 DRE: Thoracic Spine
15.4
388-391
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
28© 2011 Format only ACDM Inc.
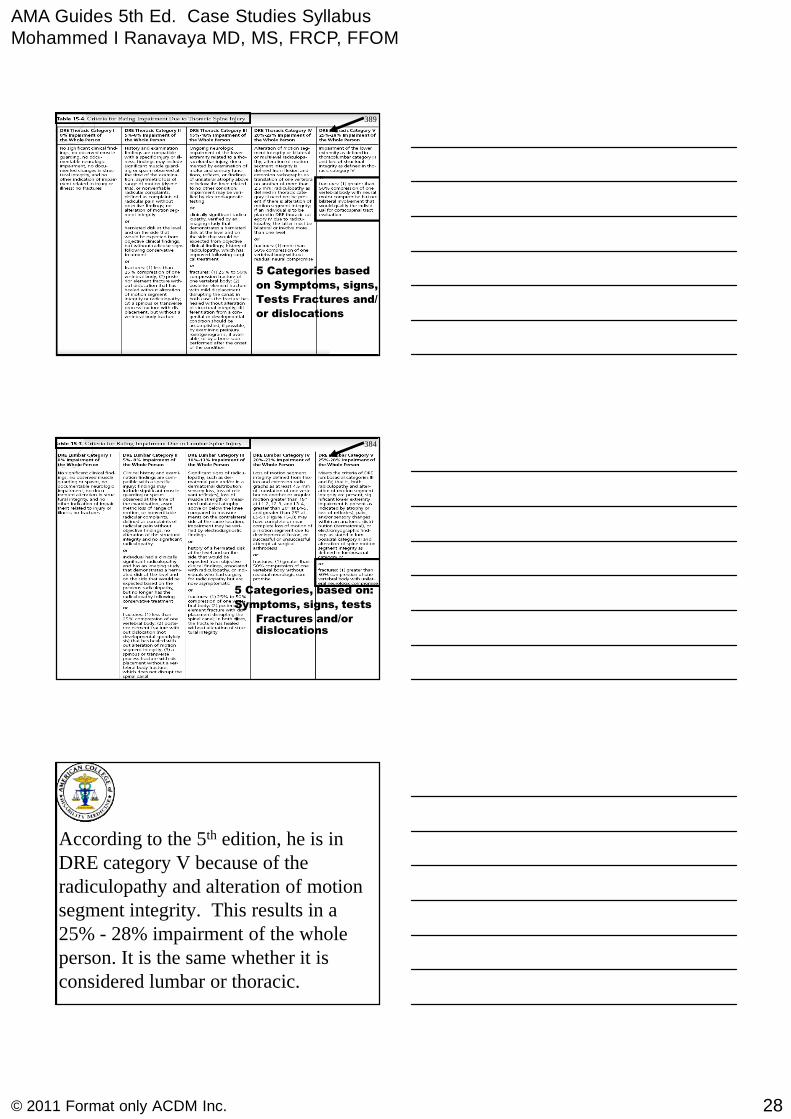
389
5 Categories based
on Symptoms, signs,
Tests Fractures and/
or dislocations
384
5 Categories, based on:
Symptoms, signs, tests
• Fractures and/ordislocations
According to the 5th edition, he is inDRE category V because of theradiculopathy and alteration of motionsegment integrity. This results in a25% - 28% impairment of the wholeperson. It is the same whether it isconsidered lumbar or thoracic.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
29© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
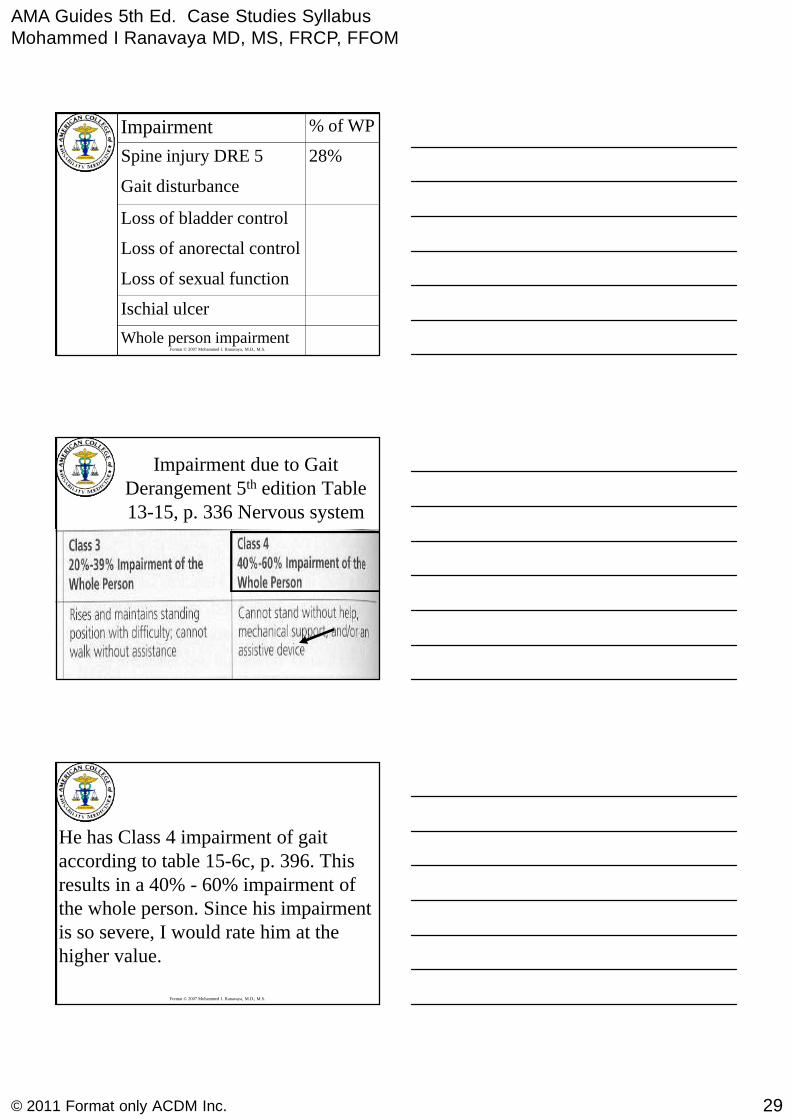
Ischial ulcer
Loss of anorectal control
Loss of sexual function
Whole person impairment
Loss of bladder control
Gait disturbance
28%Spine injury DRE 5
% of WPImpairment
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Impairment due to GaitDerangement 5th edition Table13-15, p. 336 Nervous system
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
He has Class 4 impairment of gaitaccording to table 15-6c, p. 396. Thisresults in a 40% - 60% impairment ofthe whole person. Since his impairmentis so severe, I would rate him at thehigher value.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
30© 2011 Format only ACDM Inc.
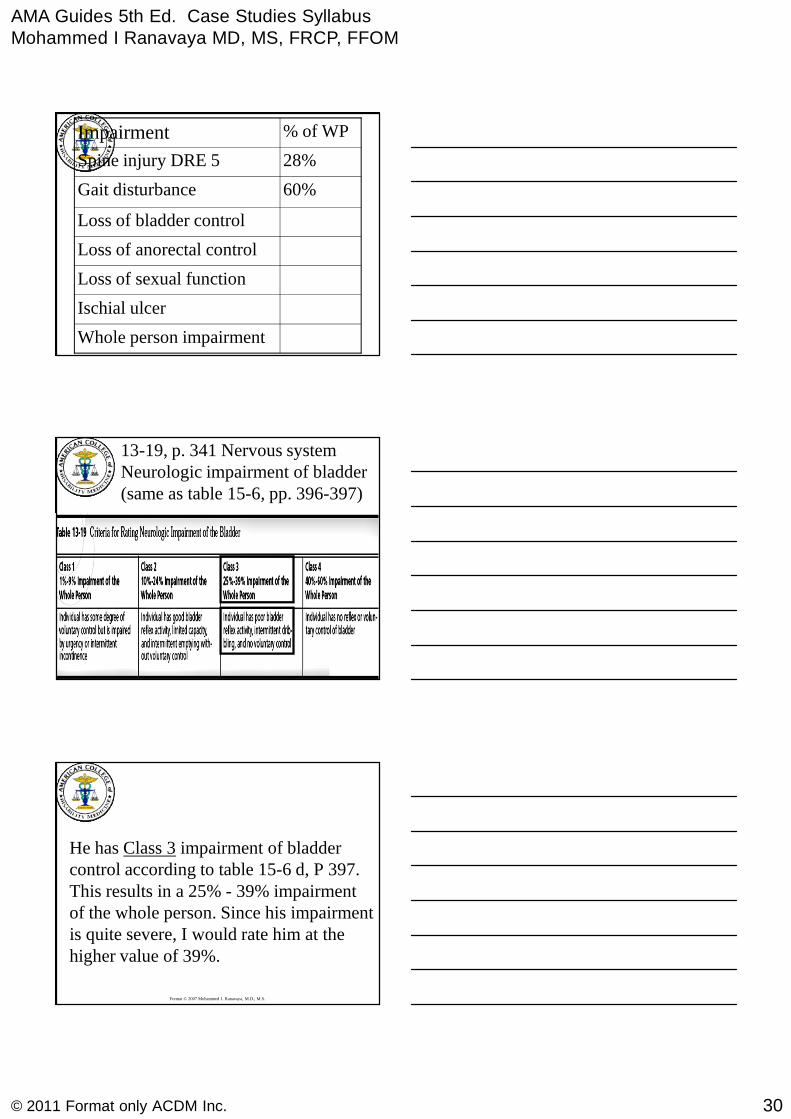
Ischial ulcer
Loss of anorectal control
Loss of sexual function
Whole person impairment
Loss of bladder control
60%Gait disturbance
28%Spine injury DRE 5
% of WPImpairment
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
13-19, p. 341 Nervous systemNeurologic impairment of bladder(same as table 15-6, pp. 396-397)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
He has Class 3 impairment of bladdercontrol according to table 15-6 d, P 397.This results in a 25% - 39% impairmentof the whole person. Since his impairmentis quite severe, I would rate him at thehigher value of 39%.

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
31© 2011 Format only ACDM Inc.
Ischial ulcer
Loss of anorectal control
Loss of sexual function
Whole person impairment
39%Loss of bladder control
60%Gait disturbance
28%Spine injury DRE 5
% of WPImpairment
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
13-20, p. 342 Nervous systemNeurologic impairment of Bowel(same as table 15-6, pp. 396-397)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
He has Class 2 impairment ofanorectal control according to table15-6e, p. 397. This results in a 29% -39% impairment of the whole person.Since his impairment is quite severe, Iwould rate him at the higher value.

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
32© 2011 Format only ACDM Inc.
Ischial ulcer
39%Loss of anorectal control
Loss of sexual function
Whole person impairment
39%Loss of bladder control
60%Gait disturbance
28%Spine injury DRE 5
% of WPImpairment
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
13-21, p. 342 Nervous systemNeurologic Sexual Dysfunction(same as table 15-6, pp. 396-397)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
He has Class 3 impairment of sexualfunction according to table 15-6f, p. 397.
This results in a 20% impairment of thewhole person.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
33© 2011 Format only ACDM Inc.
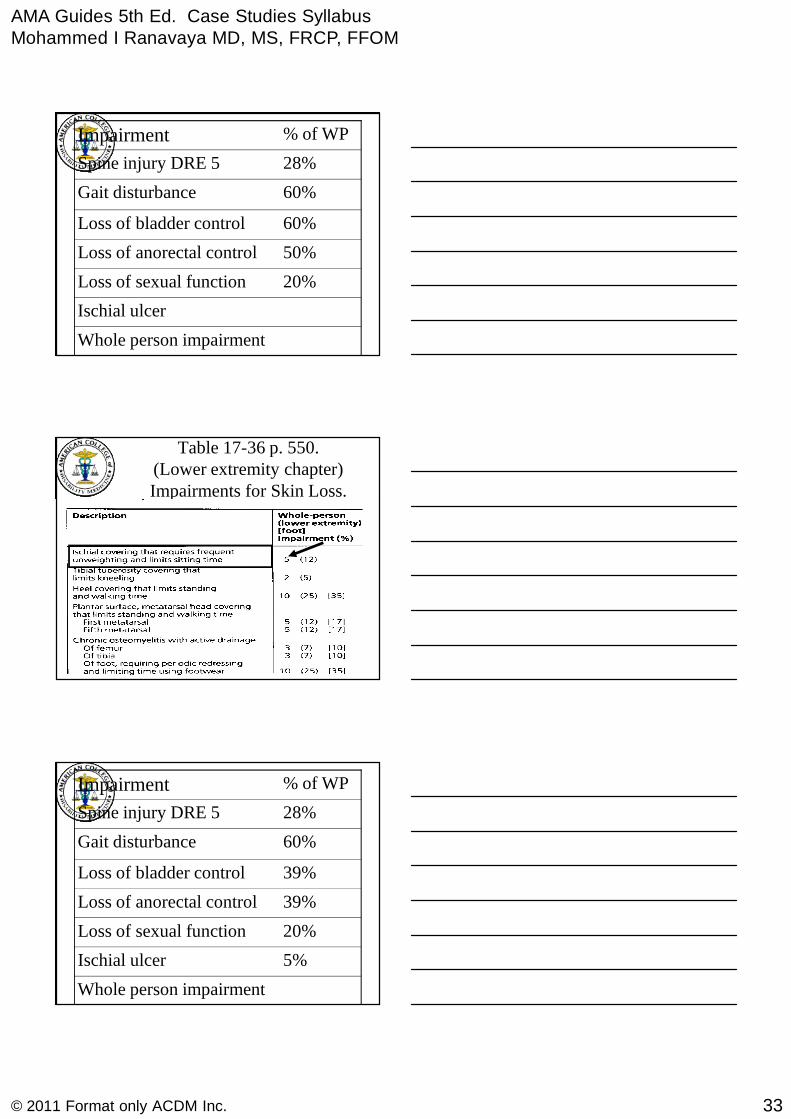
Ischial ulcer
50%Loss of anorectal control
20%Loss of sexual function
Whole person impairment
60%Loss of bladder control
60%Gait disturbance
28%Spine injury DRE 5
% of WPImpairment
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-36 p. 550.(Lower extremity chapter)Impairments for Skin Loss.
5%Ischial ulcer
39%Loss of anorectal control
20%Loss of sexual function
Whole person impairment
39%Loss of bladder control
60%Gait disturbance
28%Spine injury DRE 5
% of WPImpairment
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
34© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
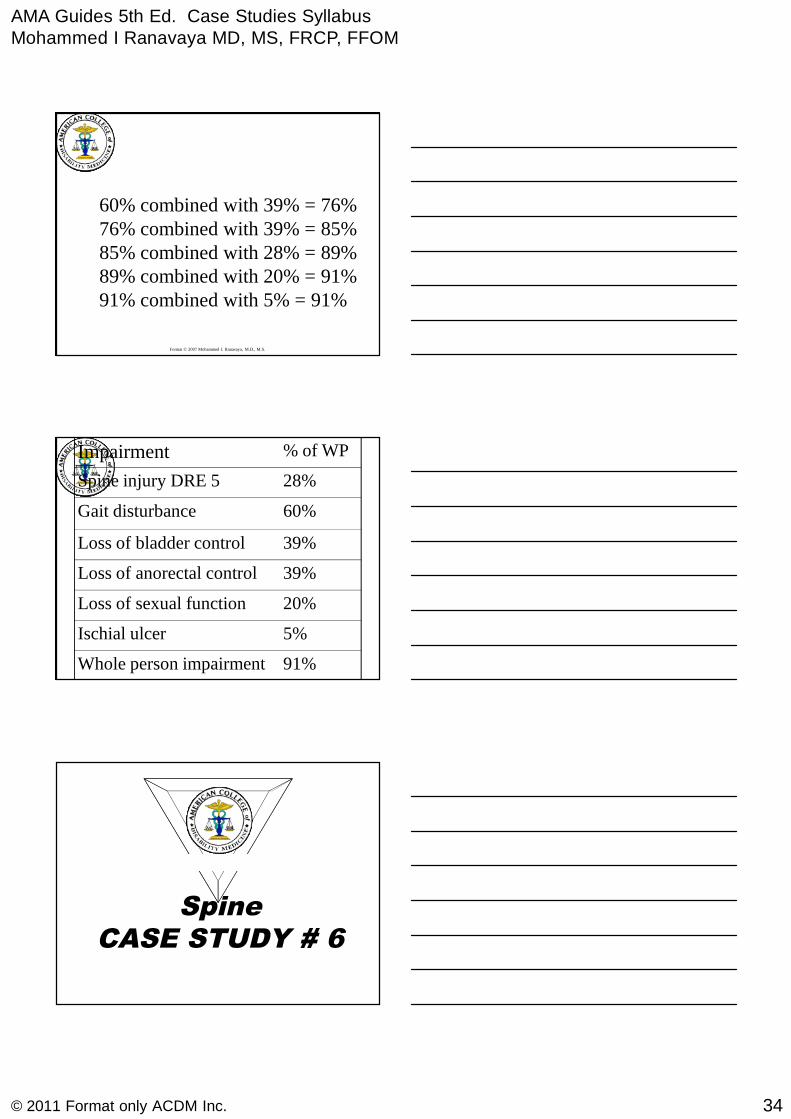
60% combined with 39% = 76%76% combined with 39% = 85%85% combined with 28% = 89%89% combined with 20% = 91%91% combined with 5% = 91%
5%Ischial ulcer
39%Loss of anorectal control
20%Loss of sexual function
91%Whole person impairment
39%Loss of bladder control
60%Gait disturbance
28%Spine injury DRE 5
% of WPImpairment
SpineCASE STUDY # 6
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
35© 2011 Format only ACDM Inc.
Low Back Injury withVertebral Fracture
35-year-old woman who worked as alibrarian in the public library fell froma ladder while putting away books
She sustained a mild burst fracture ofL1 with a 55% loss of height withoutneurologic deficits
Low Back Injury withVertebral Fracture
History con’t:
–Treated with bracing
–Fracture healed
–6 months after the injury, was able to domost ADL
Low Back Injury withVertebral Fracture
Current Complaints:
–Has back pain after heavy activity orwith weather changes
–No neurologic complaints
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
36© 2011 Format only ACDM Inc.
Low Back Injury withVertebral Fracture
Physical Exam:
– Mild tenderness to palpation at thefracture site
– Neurologic examination : negative
– SLR : negative
– Range of motion is mildly decreased
Low Back Injury withVertebral Fracture
Clinical Studies:
– Radiograph : fracture healed with 60% loss ofheight
Diagnosis:
– Burst fracture L1 > 50%
What is the Impairment Rating?
Low Back Injury withVertebral Fracture
Impairment Rating
Analysis:
–Is she at MMI?
–What Method to Use?
–DRE Vs ROM
She is at MMI—Use DRE

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
37© 2011 Format only ACDM Inc.
384
5 Categories, based on:
Symptoms, signs, tests
• Fractures and/ordislocations
Low Back Injury withVertebral Fracture
Impairment Rating
Analysis:
–Individual qualifies for lumbar DREcategory IV based on the fracture.
–Neurologic deficit, if present, wouldwarrant category V or Section 15.7.
20% whole person impairment
SpineCASE STUDY # 7
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
38© 2011 Format only ACDM Inc.
Low Back Injury withDegenerative Disc Disease
28-year-old elementary school teacher fell onconcrete surface, while carrying a box full ofactivities for her class into the school.
Onset of back and left leg pain
Transported to ER via EMS
Low Back Injury withDegenerative Disc Disease
Examination in the ER:
muscle spasm of the back
SLR on the left side at 60°
Positive crossed SLR at 70°
An absent left Achilles tendon reflex
MRI : severely degenerated L5-S1disk with aherniation on the left side
Low Back Injury withDegenerative Disc Disease
History con’t:
– Treated conservatively by Neurosurgeon withmedication, physical therapy but did not improve
– Surgical diskectomy and arthrodesis of L5-S1Three months after injury
– After 9 months of rehabilitation, leg and backsymptoms were diminished but persistent
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
39© 2011 Format only ACDM Inc.
Low Back Injury withDegenerative Disc Disease
On IME a year after injury:
Current Symptoms:
– Back pain off and on—No lower limb pain
– Prolonged standing or walking, or performing herprior work, recreational and some householdactivities caused back pain
– Persistent numbness along the lateral side of thefoot one year after onset of symptoms
Low Back Injury withDegenerative Disc Disease
On IME a year after injury:
Physical Exam:
– mildly restricted range of motion
– Loss of Achilles reflex
– Numbness in the S1 nerve root distribution
– No motor loss in the lower limb
– Normal gait
Low Back Injury withDegenerative Disc Disease
Imaging Studies:
–Postoperative MRI with gadolinium :fibrosis, but no residual or recurrentherniation
–Fusion appears solid
–Electrodiagnostic study consistentwith current left S1 radiculopathy
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
40© 2011 Format only ACDM Inc.
Low Back Injury withDegenerative Disc Disease
Diagnosis:–Left posterolateral L5-S1 disk herniation
with S1 radiculopathy
–Unresolved radiculopathy status postdiskectomy with L5-S1 fusion
What is the Impairment Rating?
Low Back Injury withDegenerative Disc Disease
Impairment Rating
Analysis:– Symptoms, physical findings, and imaging
studies are all consistent with a symptomaticherniated disk and a persistent radiculopathy.
– Excision of the offending disk and a single-level fusion did not relieve all symptoms,which is supported by signs of a persistentradiculopathy.
384
5 Categories, based on:
Symptoms, signs, tests
• Fractures and/ordislocations
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
41© 2011 Format only ACDM Inc.
Low Back Injury withDegenerative Disc Disease
Impairment Rating
Analysis con’t:
– Individual with persistent radiculopathy as wellas single-level alteration of motion segmentintegrity qualifies for lumbar DRE category V(25%-28% impairment of the whole person)
– Her Final whole person impairment is 28%because She has persistent ADL problems
SpineCASE STUDY # 8
Mid Back (Thoracic injury)
40-year-old electrician, worked for thepower company, fell from a power pole 30feet high and sustained a 55% compressionfracture of T12
– Conservative treatment for 8 months
– Able to perform most ADL, and walk withoutbraces or crutches, but is limited to levelsurfaces
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
42© 2011 Format only ACDM Inc.
Mid Back (Thoracic injury)
Current Symptoms:
–Back pain with heavy physicalactivity
–Left extremity weakness, difficultywalking uphill
–Numbness in the left leg
Mid Back (Thoracic injury)
Physical Exam:
–Spotty numbness in the left leg
–Grade 4/5 left leg weakness
–2 cm atrophy of left thigh and leg
–Left leg reflexes are hypoactive
Mid Back (Thoracic injury)
Clinical Studies:
–Compression fracture of T8 -55%
Diagnosis:
–Compression fracture T8 with residual leftlower extremity neurologic involvement
What is the Impairment Rating?
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
43© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Mid Back (Thoracic injury)Impairment Rating
Analysis:
–This individual qualifies for DREthoracic category V because of hisongoing unilateral neurologic deficits &structural inclusion of a compressionfracture with >50% loss of height.
389
5 Categories based
on Symptoms, signs,
Tests Fractures and/
or dislocations
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Mid Back (Thoracic injury)Impairment Rating
Analysis:
– DRE thoracic category V is 25% -28%whole person impairment.
–Based on the effect on ADL, he wouldbe rated at 28% impairment of thewhole person
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
44© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Mid Back (Thoracic injury)Impairment Rating
Impairment Rating Corticospinal Tract injury
The recommended system is thatfrom the nervous system chapter,which has been reprinted in thespine chapter as Table 15-6, 396-7
Mid Back (Thoracic injury)Impairment Rating
What if he had bilateral leg weakness andlimited to walking surface only?
Then in addition to the Thoracic DRE V, hewould also be rated for Corticospinal Tractinjury Section c, Table 15-6, p 396-Criteria forRating Impairments Due to Station & Gait
This would be combined with the DRE. Iwould assign him lower limit for DRE as theStation & Gait number would account for ADL
Low Back Injury withCauda Equina
Rating Corticospinal Tract Impairmentresulting from Station & Gait Disorders
Table 15-6, 396, Sec C
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
45© 2011 Format only ACDM Inc.
Low Back Injury withCauda Equina
Impairment Rating Corticospinal Tract injury
According to Table 15-6, RatingCorticospinal Tract Impairment, Sectionc, Criteria for Rating Impairments Dueto Station and Gait Disorders, this casemeets the definition of class 2.
Mid Back (Thoracic injury)Impairment Rating
This corresponds with a 10% to 19%impairment of whole person.
A higher value of 19% was selected.
This must be combined with 25%impairment of the whole person fromThoracic DRE V making it a 39%whole person impairment.
SpineCASE STUDY # 9
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
46© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Thoracic spine Injury withVertebral Fracture
28-year dozer operator fell and struck hishead and neck while at work.
Had severe and persistent pain in the neck,radiating to lateral right upper limbextending into the thumb
MRI showed a herniated disk at C5-6 onthe right
Thoracic spine Injury withVertebral Fracture
History con’t:
–Failed nonoperative treatment
–Underwent a diskectomy of C5-6 level &Fusion of C5 to C6--Single level
–Underwent Physical therapy for 6 weeks
Thoracic spine Injury withVertebral Fracture
History at IME a year later:
– Has continued neck and right upperextremity pain
–Unable to perform most ADL
–Uses assistive devices for right sidegripping and turning objects

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
47© 2011 Format only ACDM Inc.
Thoracic spine Injury withVertebral Fracture
A year later, his current symptoms are:
– Severe neck and right upper extremity pain
– Aggravated by movements of the neck anduse of the right upper extremity
– Persistent numbness in the radial forearm,hand, and digits particularly of thumb
– requires the use of adaptive devices
Thoracic spine Injury withVertebral Fracture
Physical Exam:
– Mild loss of cervical motion
– Neurologic examination reveals decreasedsensation in the right thumb, index finger andthe Dosolateral aspect of the forearm
– weakness of bicep ans wrist extensors on right
– Diminished brachioradialis reflex on right
Thoracic spine Injury withVertebral Fracture
Clinical Studies:–Radiographs : healed fusion C5-C6

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
48© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Thoracic spine Injury withVertebral Fracture
Diagnosis:
– Herniated C5-6 disk treated withdiskectomy and single level fusion withresidual right C6 radiculopathy
What is the Impairment rating?
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Thoracic spine Injury withVertebral Fracture
Impairment Rating
Analysis:–Meets criteria for DRE cervical
category V because of objectivefindings supportive of significantupper extremity impairmentrequiring the use of adaptive devices
392
5 Categories based
on Symptoms, signs,
Tests Fractures and/
or dislocations

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
49© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Thoracic spine Injury withVertebral Fracture
Impairment Rating
Conclusion:
– DRE cervical category V
–38% impairment of the whole person
Discussion
AMA Guides to the Evaluation ofPermanent Impairment - Fifth Edition
Chapter16_The Upper Extremities
Mohammed I Ranavaya MD, MS, FRCPI
16
433-521
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
50© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper ExtremitiesCase studies
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper ExtremitiesCase Study 1
Shoulder and Elbow Injury
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
A 48 year old file clerk fell down the stairsA 48 year old file clerk fell down the stairsat work sustaining a fracture of her rightat work sustaining a fracture of her rightdistal humerus. Open reduction of thedistal humerus. Open reduction of thefracture was necessary. Six months afterfracture was necessary. Six months afterinjury, healing of the fracture wasinjury, healing of the fracture wascomplete and serial measurements showedcomplete and serial measurements showedno further improvement in range ofno further improvement in range ofmotion.motion.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
51© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
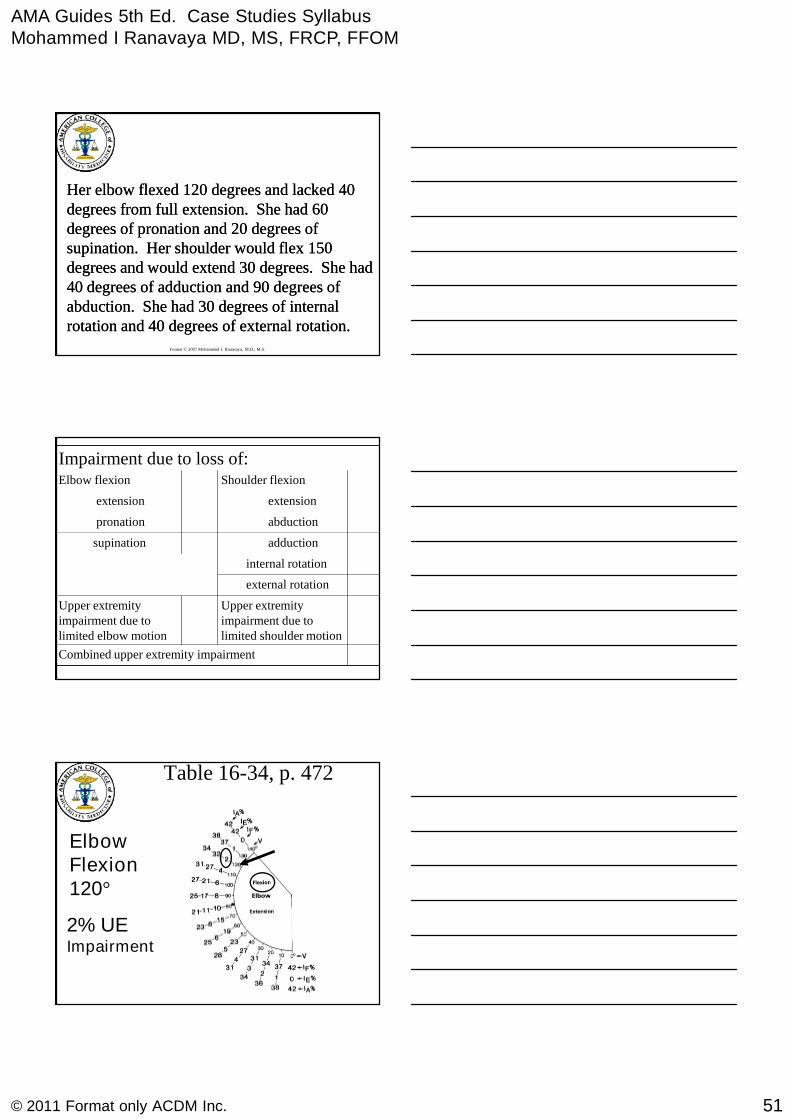
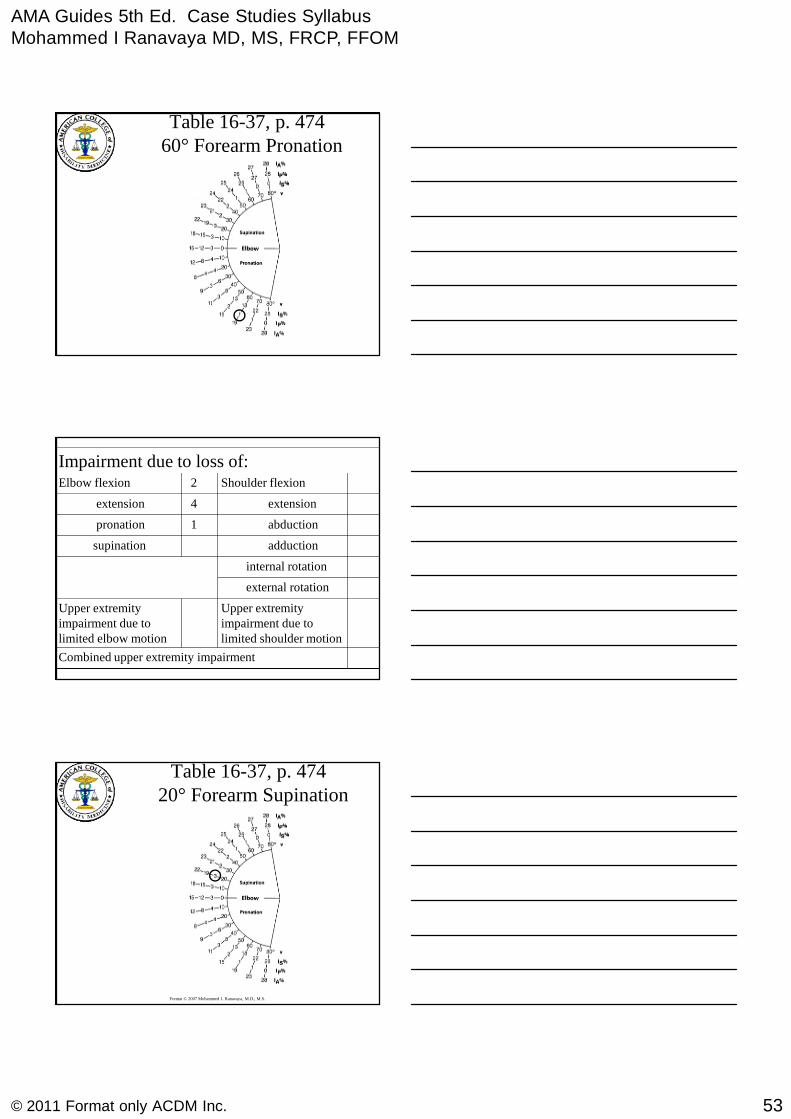
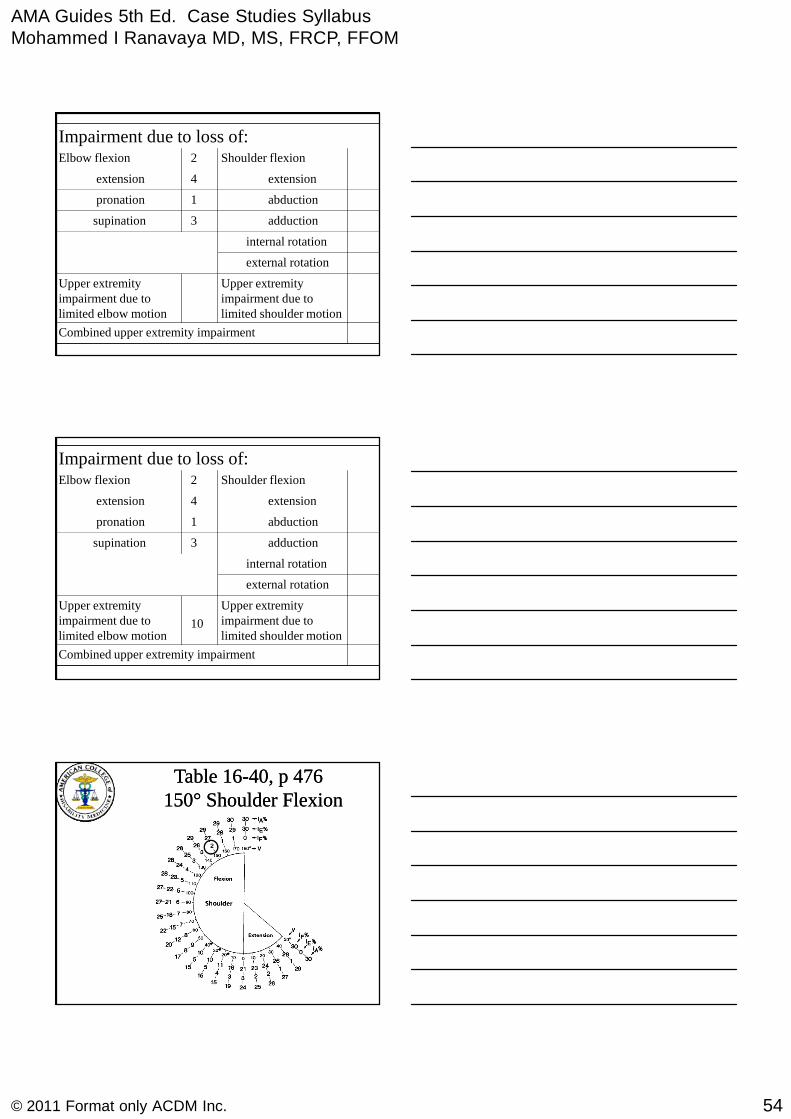
Her elbow flexed 120 degrees and lacked 40Her elbow flexed 120 degrees and lacked 40degrees from full extension. She had 60degrees from full extension. She had 60degrees of pronation and 20 degrees ofdegrees of pronation and 20 degrees ofsupination. Her shoulder would flex 150supination. Her shoulder would flex 150degrees and would extend 30 degrees. She haddegrees and would extend 30 degrees. She had40 degrees of adduction and 90 degrees of40 degrees of adduction and 90 degrees ofabduction. She had 30 degrees of internalabduction. She had 30 degrees of internalrotation and 40 degrees of external rotation.rotation and 40 degrees of external rotation.
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
Upper extremityimpairment due tolimited elbow motion
external rotation
internal rotation
adductionsupination
abductionpronation
extensionextension
Shoulder flexionElbow flexion
Table 16-34, p. 472
ElbowFlexion120°
2% UEImpairment
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
52© 2011 Format only ACDM Inc.
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
Upper extremityimpairment due tolimited elbow motion
external rotation
internal rotation
adductionsupination
abductionpronation
extensionextension
Shoulder flexion2Elbow flexion
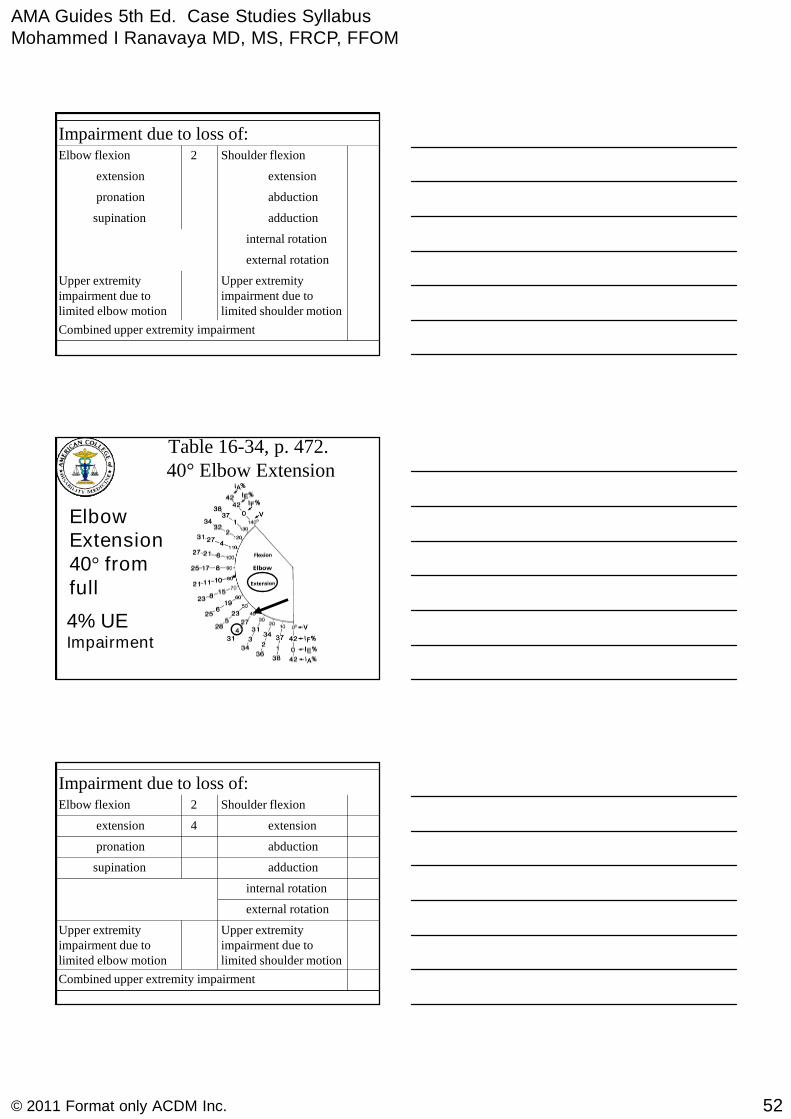
Table 16-34, p. 472.40° Elbow Extension
ElbowExtension40° fromfull
4% UEImpairment
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
Upper extremityimpairment due tolimited elbow motion
external rotation
internal rotation
adductionsupination
abductionpronation
extension4extension
Shoulder flexion2Elbow flexion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
53© 2011 Format only ACDM Inc.
Table 16-37, p. 47460° Forearm Pronation
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
Upper extremityimpairment due tolimited elbow motion
external rotation
internal rotation
adductionsupination
abduction1pronation
extension4extension
Shoulder flexion2Elbow flexion
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 16-37, p. 47420° Forearm Supination
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
54© 2011 Format only ACDM Inc.
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
Upper extremityimpairment due tolimited elbow motion
external rotation
internal rotation
adduction3supination
abduction1pronation
extension4extension
Shoulder flexion2Elbow flexion
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
10
Upper extremityimpairment due tolimited elbow motion
external rotation
internal rotation
adduction3supination
abduction1pronation
extension4extension
Shoulder flexion2Elbow flexion
Table 16Table 16--40, p 47640, p 476150150°° Shoulder FlexionShoulder Flexion

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
55© 2011 Format only ACDM Inc.
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
10
Upper extremityimpairment due tolimited elbow motion
external rotation
internal rotation
adduction3supination
abduction1pronation
extension4extension
2Shoulder flexion2Elbow flexion
Table 16Table 16--40, p 47640, p 4763030°° Shoulder ExtensionShoulder Extension
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
10
Upper extremityimpairment due tolimited elbow motion
external rotation
internal rotation
adduction3supination
abduction1pronation
1extension4extension
2Shoulder flexion2Elbow flexion

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
56© 2011 Format only ACDM Inc.
Table 16-43, p. 47790° Shoulder Abduction
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
10
Upper extremityimpairment due tolimited elbow motion
external rotation
internal rotation
adduction3supination
4abduction1pronation
1extension4extension
2Shoulder flexion2Elbow flexion
Table 16-43, p. 477
40° Shoulder Adduction

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
57© 2011 Format only ACDM Inc.
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
10
Upper extremityimpairment due tolimited elbow motion
external rotation
internal rotation
0adduction3supination
4abduction1pronation
1extension4extension
2Shoulder flexion2Elbow flexion
Table 16-46, p. 47930° Internal Rotation
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
10
Upper extremityimpairment due tolimited elbow motion
external rotation
4internal rotation
0adduction3supination
4abduction1pronation
1extension4extension
2Shoulder flexion2Elbow flexion

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
58© 2011 Format only ACDM Inc.
Table 16-46, p. 47940° External Rotation
Impairment due to loss of:
Combined upper extremity impairment
Upper extremityimpairment due tolimited shoulder motion
10
Upper extremityimpairment due tolimited elbow motion
1external rotation
4internal rotation
0adduction3supination
4abduction1pronation
1extension4extension
2Shoulder flexion2Elbow flexion
Impairment due to loss of:
Combined upper extremity impairment
12
Upper extremityimpairment due tolimited shoulder motion
10
Upper extremityimpairment due tolimited elbow motion
1external rotation
4internal rotation
0adduction3supination
4abduction1pronation
1extension4extension
2Shoulder flexion2Elbow flexion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
59© 2011 Format only ACDM Inc.
Impairment due to loss of:
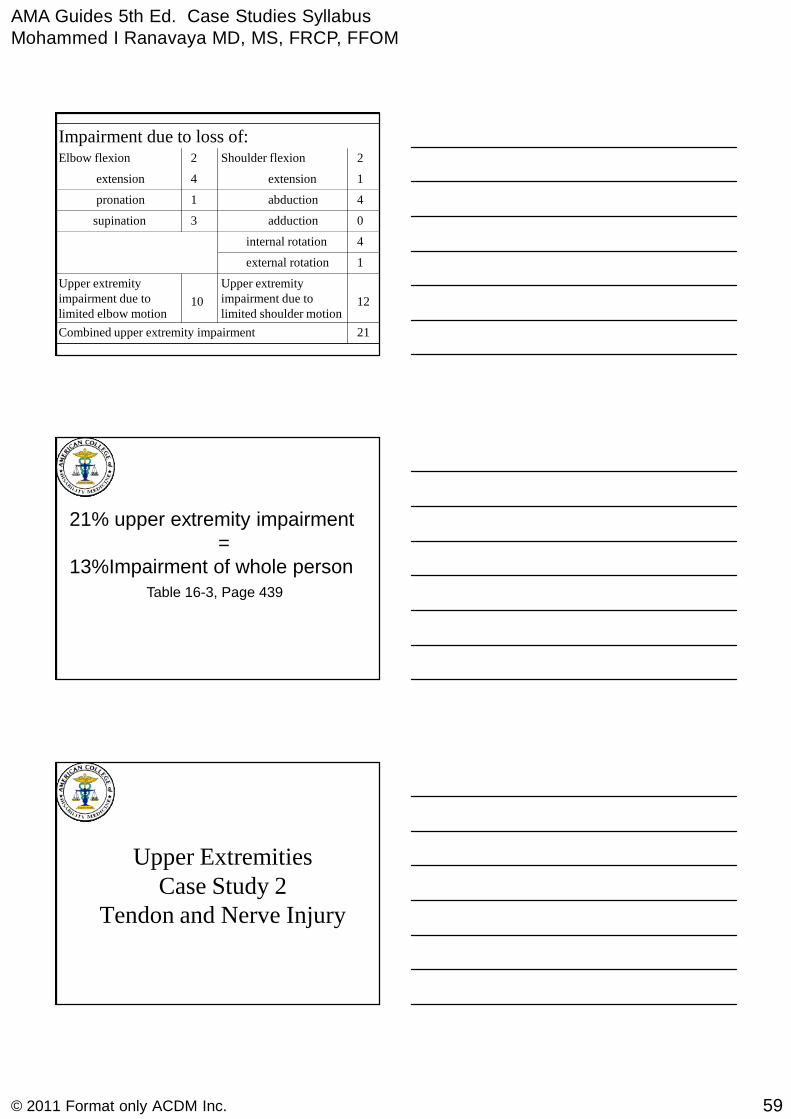
21Combined upper extremity impairment
12
Upper extremityimpairment due tolimited shoulder motion
10
Upper extremityimpairment due tolimited elbow motion
1external rotation
4internal rotation
0adduction3supination
4abduction1pronation
1extension4extension
2Shoulder flexion2Elbow flexion
21% upper extremity impairment=
13%Impairment of whole personTable 16-3, Page 439
Upper ExtremitiesCase Study 2
Tendon and Nerve Injury
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
60© 2011 Format only ACDM Inc.
A 27 year old right handed meatA 27 year old right handed meatpacking worker sustained apacking worker sustained alaceration of his right index fingerlaceration of his right index fingerwith tendon and nerve damage.with tendon and nerve damage.Surgical repairs were done, and heSurgical repairs were done, and heunderwent appropriateunderwent appropriaterehabilitation.rehabilitation.
At MMI, physical examination is as follows:At MMI, physical examination is as follows:
Transverse scar on the palmar side of theTransverse scar on the palmar side of the
finger at the level of the PIP joint.finger at the level of the PIP joint.
Radial side of the finger distal to the scar,Radial side of the finger distal to the scar,
the twothe two--point discrimination is 8 mm.point discrimination is 8 mm.
Ulnar side of the finger distal to the scar, theUlnar side of the finger distal to the scar, the
twotwo-- point discrimination is 18 mm.point discrimination is 18 mm.
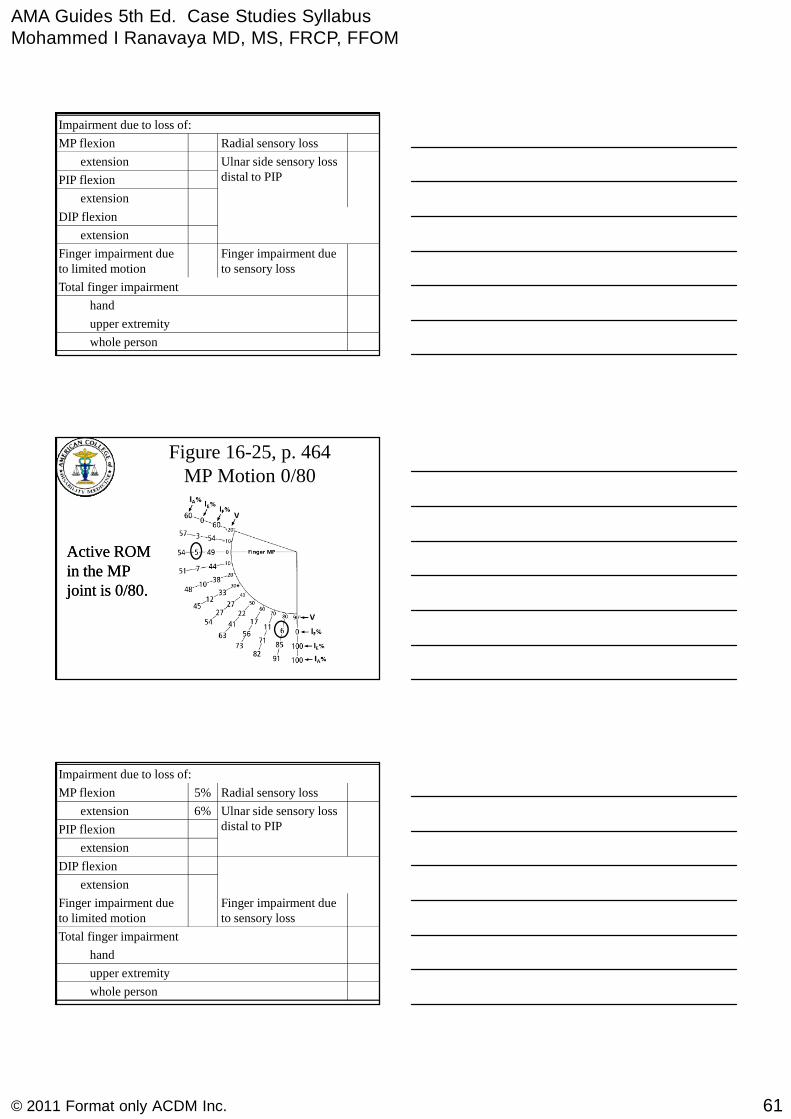
Active ROM in the MP joint is 0 degreeActive ROM in the MP joint is 0 degreeextension to 80 degree flexion.extension to 80 degree flexion.
PIP flexion 100 deg, extensionPIP flexion 100 deg, extension toto ++1010 deg.deg.
DIP limited to flexion 10 to 20 degrees.DIP limited to flexion 10 to 20 degrees.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
61© 2011 Format only ACDM Inc.
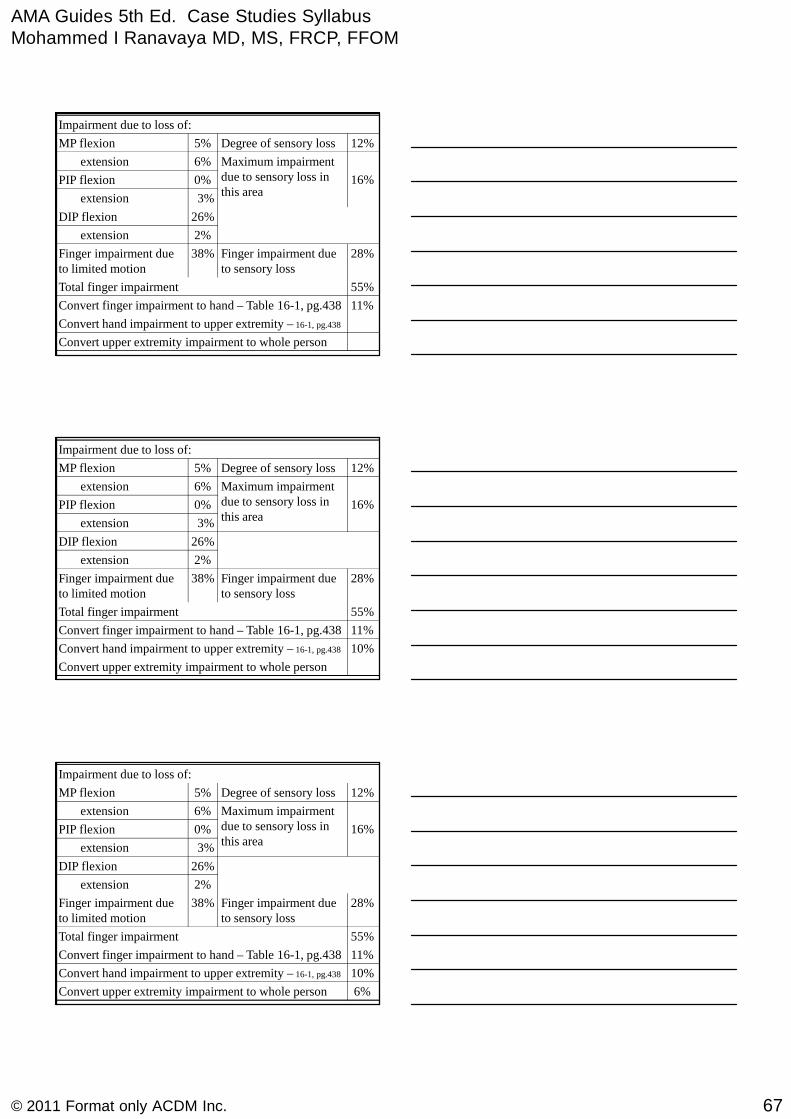
Impairment due to loss of:
whole person
upper extremity
hand
Total finger impairment
Finger impairment dueto sensory loss
Finger impairment dueto limited motion
extension
DIP flexion
extension
PIP flexion
Ulnar side sensory lossdistal to PIP
extension
Radial sensory lossMP flexion
Figure 16-25, p. 464MP Motion 0/80
Active ROMActive ROMin the MPin the MPjoint is 0/80.joint is 0/80.
Impairment due to loss of:
whole person
upper extremity
hand
Total finger impairment
Finger impairment dueto sensory loss
Finger impairment dueto limited motion
extension
DIP flexion
extension
PIP flexion
Ulnar side sensory lossdistal to PIP
6%extension
Radial sensory loss5%MP flexion

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
62© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Figure 16-23, p. 463PIP Motion 10/100
PIP Flexion 100°
PIP Extension +10°
3% UEImpairment
Impairment due to loss of:
whole person
upper extremity
hand
Total finger impairment
Finger impairment dueto sensory loss
Finger impairment dueto limited motion
extension
DIP flexion
3%extension
0%PIP flexion
Ulnar side sensory lossdistal to PIP
6%extension
Radial sensory loss5%MP flexion
Figure 16-21, p. 461.DIP Motion 10/20
DIP motion,DIP motion,10/20.10/20.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
63© 2011 Format only ACDM Inc.
Impairment due to loss of:
whole person
upper extremity
hand
Total finger impairment
Finger impairment dueto sensory loss
Finger impairment dueto limited motion
2%extension
26%DIP flexion
3%extension
0%PIP flexion
Ulnar side sensory lossdistal to PIP
6%extension
Radial sensory loss5%MP flexion
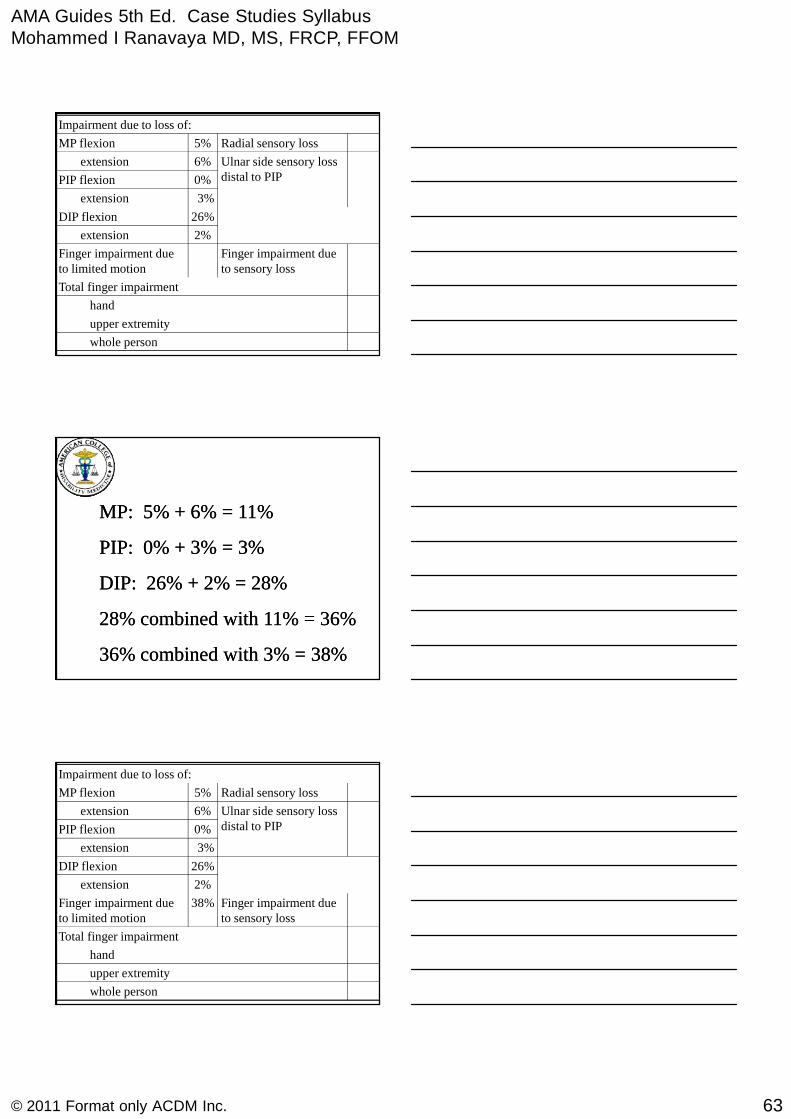
MP: 5% + 6% = 11%MP: 5% + 6% = 11%
PIP: 0% + 3% = 3%PIP: 0% + 3% = 3%
DIP: 26% + 2% = 28%DIP: 26% + 2% = 28%
28% combined with 11% = 36%28% combined with 11% = 36%
36% combined with 3% = 38%36% combined with 3% = 38%
Impairment due to loss of:
whole person
upper extremity
hand
Total finger impairment
Finger impairment dueto sensory loss
38%Finger impairment dueto limited motion
2%extension
26%DIP flexion
3%extension
0%PIP flexion
Ulnar side sensory lossdistal to PIP
6%extension
Radial sensory loss5%MP flexion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
64© 2011 Format only ACDM Inc.
Impairment due to loss of:
whole person
upper extremity
hand
Total finger impairment
Finger impairment dueto sensory loss
38%Finger impairment dueto limited motion
2%extension
26%DIP flexion
3%extension
0%PIP flexion
Ulnar side sensory lossdistal to PIP
6%extension
Radial sensory loss5%MP flexion
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
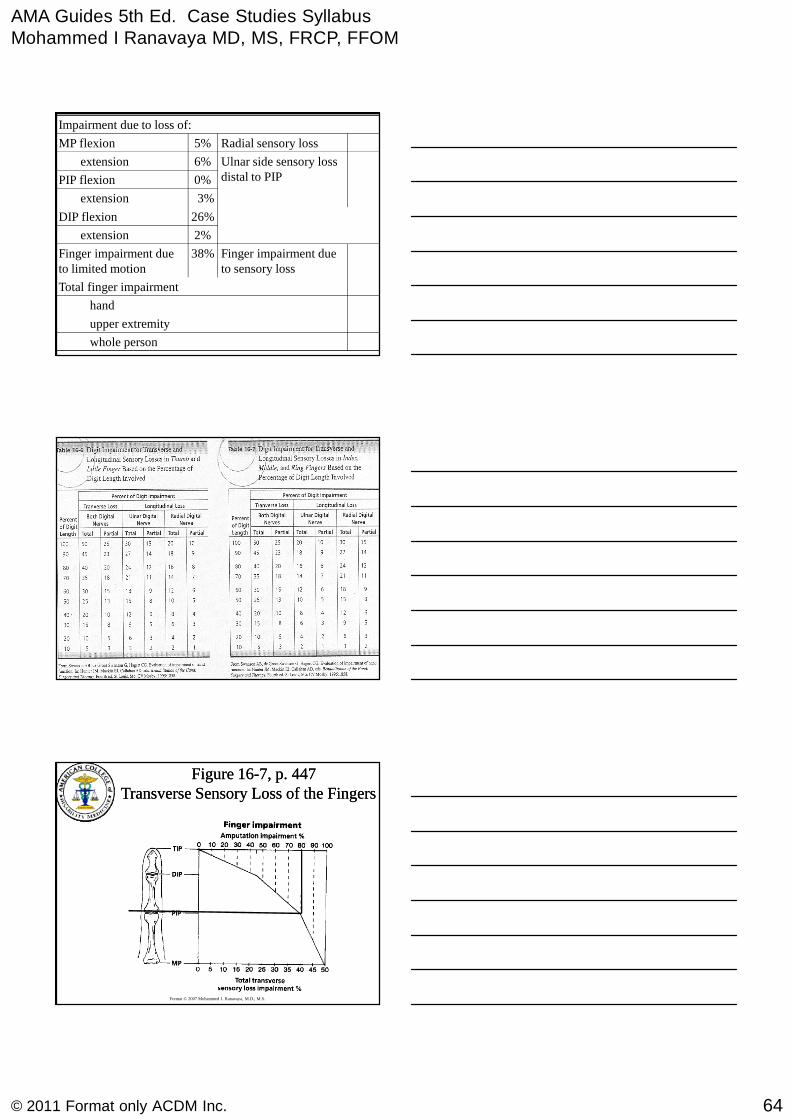
Figure 16Figure 16--7, p. 4477, p. 447Transverse Sensory Loss of the FingersTransverse Sensory Loss of the Fingers
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
65© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
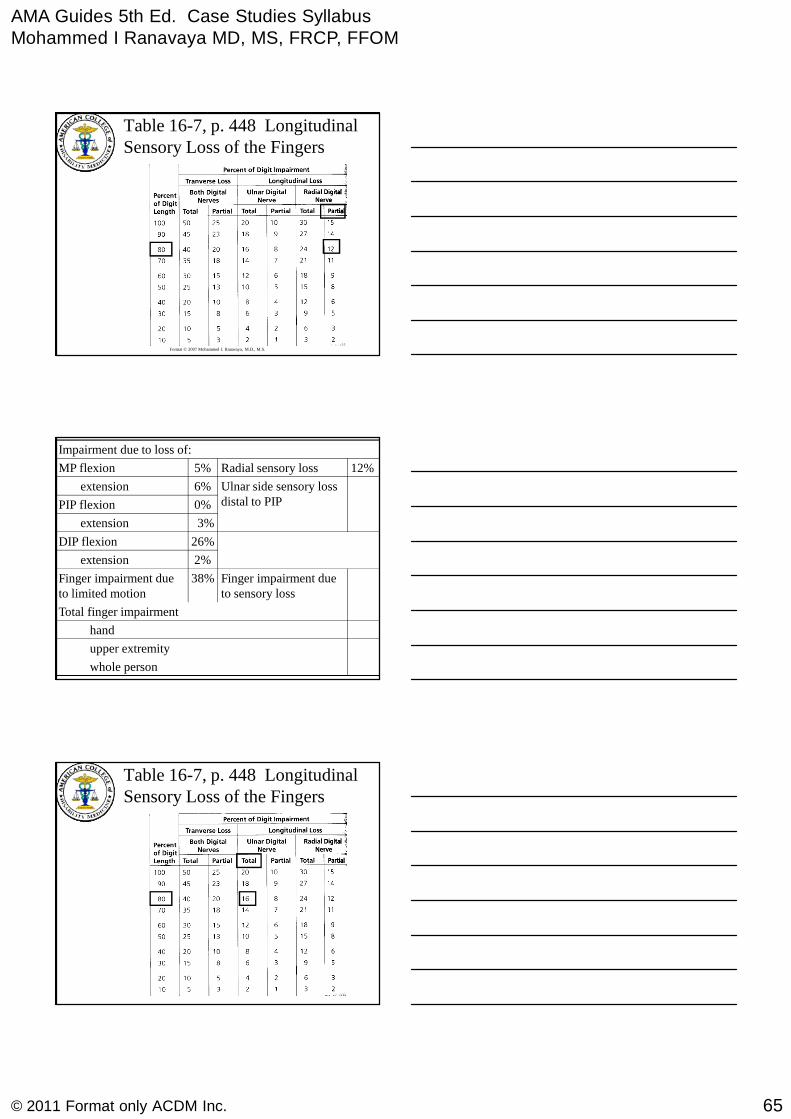
Table 16-7, p. 448 LongitudinalSensory Loss of the Fingers
Impairment due to loss of:
whole person
upper extremity
hand
Total finger impairment
Finger impairment dueto sensory loss
38%Finger impairment dueto limited motion
2%extension
26%DIP flexion
3%extension
0%PIP flexion
Ulnar side sensory lossdistal to PIP
6%extension
12%Radial sensory loss5%MP flexion
Table 16-7, p. 448 LongitudinalSensory Loss of the Fingers

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
66© 2011 Format only ACDM Inc.
Impairment due to loss of:
whole person
upper extremity
hand
Total finger impairment
Finger impairment dueto sensory loss
38%Finger impairment dueto limited motion
2%extension
26%DIP flexion
3%extension
0%PIP flexion 16%
Maximum impairmentdue to sensory loss inthis area
6%extension
12%Degree of sensory loss5%MP flexion
Impairment due to loss of:
whole person
upper extremity
hand
Total finger impairment
28%Finger impairment dueto sensory loss
38%Finger impairment dueto limited motion
2%extension
26%DIP flexion
3%extension
0%PIP flexion 16%
Maximum impairmentdue to sensory loss inthis area
6%extension
12%Degree of sensory loss5%MP flexion
Impairment due to loss of:
whole person
upper extremity
hand
55%Total finger impairment– Combine 38% with 28%
28%Finger impairment dueto sensory loss
38%Finger impairment dueto limited motion
2%extension
26%DIP flexion
3%extension
0%PIP flexion 16%
Maximum impairmentdue to sensory loss inthis area
6%extension
12%Degree of sensory loss5%MP flexion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
67© 2011 Format only ACDM Inc.
Impairment due to loss of:
Convert upper extremity impairment to whole person
Convert hand impairment to upper extremity – 16-1, pg.438
11%Convert finger impairment to hand – Table 16-1, pg.438
55%Total finger impairment
28%Finger impairment dueto sensory loss
38%Finger impairment dueto limited motion
2%extension
26%DIP flexion
3%extension
0%PIP flexion 16%
Maximum impairmentdue to sensory loss inthis area
6%extension
12%Degree of sensory loss5%MP flexion
Impairment due to loss of:
Convert upper extremity impairment to whole person
10%Convert hand impairment to upper extremity – 16-1, pg.438
11%Convert finger impairment to hand – Table 16-1, pg.438
55%Total finger impairment
28%Finger impairment dueto sensory loss
38%Finger impairment dueto limited motion
2%extension
26%DIP flexion
3%extension
0%PIP flexion 16%
Maximum impairmentdue to sensory loss inthis area
6%extension
12%Degree of sensory loss5%MP flexion
Impairment due to loss of:
6%Convert upper extremity impairment to whole person
10%Convert hand impairment to upper extremity – 16-1, pg.438
11%Convert finger impairment to hand – Table 16-1, pg.438
55%Total finger impairment
28%Finger impairment dueto sensory loss
38%Finger impairment dueto limited motion
2%extension
26%DIP flexion
3%extension
0%PIP flexion 16%
Maximum impairmentdue to sensory loss inthis area
6%extension
12%Degree of sensory loss5%MP flexion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
68© 2011 Format only ACDM Inc.
Upper ExtremitiesCase Study 3
Shoulder Dislocation
A 54 year old construction worker injured his leftshoulder in a fall at work. Anterior dislocationwas confirmed by x-ray in the emergency room,and the shoulder was reduced by closedmanipulation. He was started on a rehabilitationprogram right away, and returned to light work intwo weeks and his usual work in a month.
Six months later, he dislocatedhis shoulder again in a ball game.Another player, who is aparamedic, put it back in place,and he did not see a doctor.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
69© 2011 Format only ACDM Inc.
A year after his initial injury, he felt hisshoulder “came loose” while he wasreaching up to get some materials off ashelf at work. He was quite apprehensiveand went to ER. He was found to have thehumeral head sublux over the glenoid rimwhich reduced spontaneously when axialload was withdrawn (class II)
His orthopedist said that the recurrentshoulder instability was the result ofinadequate immobilization, and put himin a shoulder immobilizer for six weeks.Six months later he was evaluated.
Clinical shoulder instability test positiveMRI showed anterior glenoid labrum tear He refused surgery
At the time of his evaluation, sixmonths later, he had motions asfollows:Flexion 140°Extension 30°Adduction 30°Abduction 90°External rotation 50°Internal rotation 60°
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
70© 2011 Format only ACDM Inc.
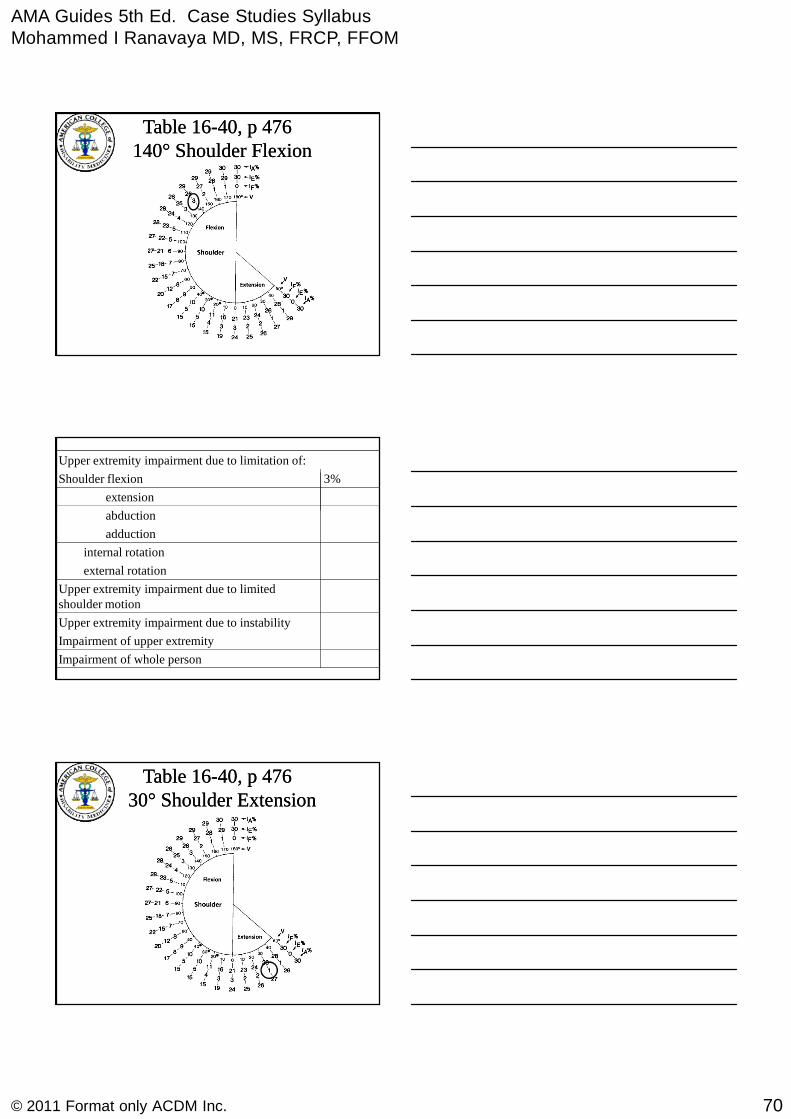
Table 16Table 16--40, p 47640, p 476140140°° Shoulder FlexionShoulder Flexion
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to instability
Upper extremity impairment due to limitedshoulder motion
external rotation
internal rotation
adduction
abduction
extension
3%Shoulder flexion
Table 16Table 16--40, p 47640, p 4763030°° Shoulder ExtensionShoulder Extension

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
71© 2011 Format only ACDM Inc.
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to instability
Upper extremity impairment due to limitedshoulder motion
external rotation
internal rotation
adduction
abduction
1%extension
3%Shoulder flexion
Table 16-43, p. 47790° Shoulder Abduction
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to instability
Upper extremity impairment due to limitedshoulder motion
external rotation
internal rotation
adduction
4%abduction
1%extension
3%Shoulder flexion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
72© 2011 Format only ACDM Inc.
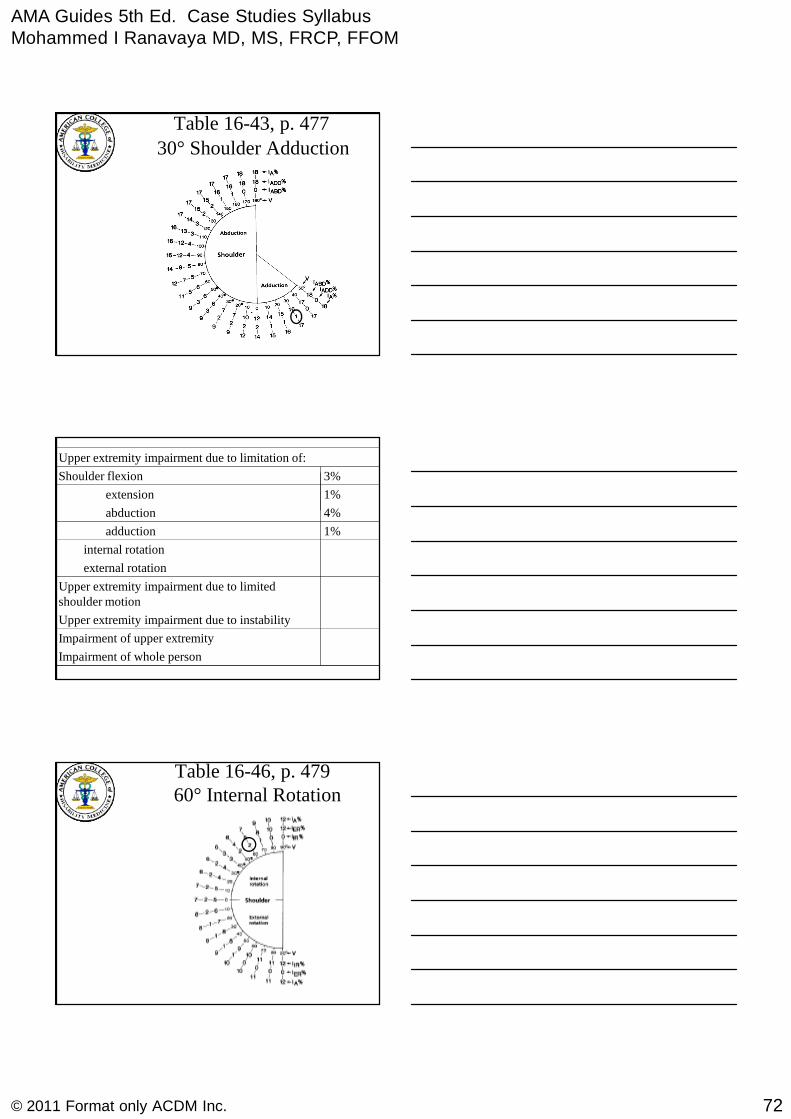
Table 16-43, p. 477
30° Shoulder Adduction
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to instability
Upper extremity impairment due to limitedshoulder motion
external rotation
internal rotation
1%adduction
4%abduction
1%extension
3%Shoulder flexion
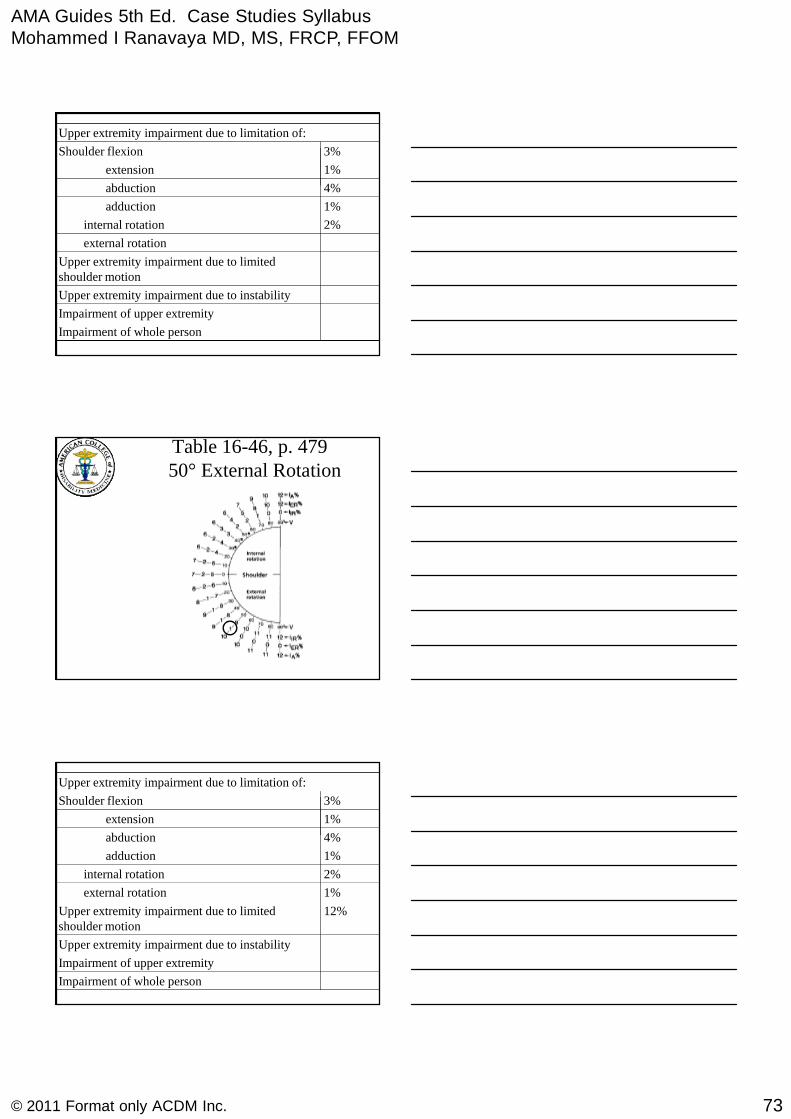
Table 16-46, p. 47960° Internal Rotation
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
73© 2011 Format only ACDM Inc.
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to instability
Upper extremity impairment due to limitedshoulder motion
external rotation
2%internal rotation
1%adduction
4%abduction
1%extension
3%Shoulder flexion
Table 16-46, p. 47950° External Rotation
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to instability
12%Upper extremity impairment due to limitedshoulder motion
1%external rotation
2%internal rotation
1%adduction
4%abduction
1%extension
3%Shoulder flexion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
74© 2011 Format only ACDM Inc.
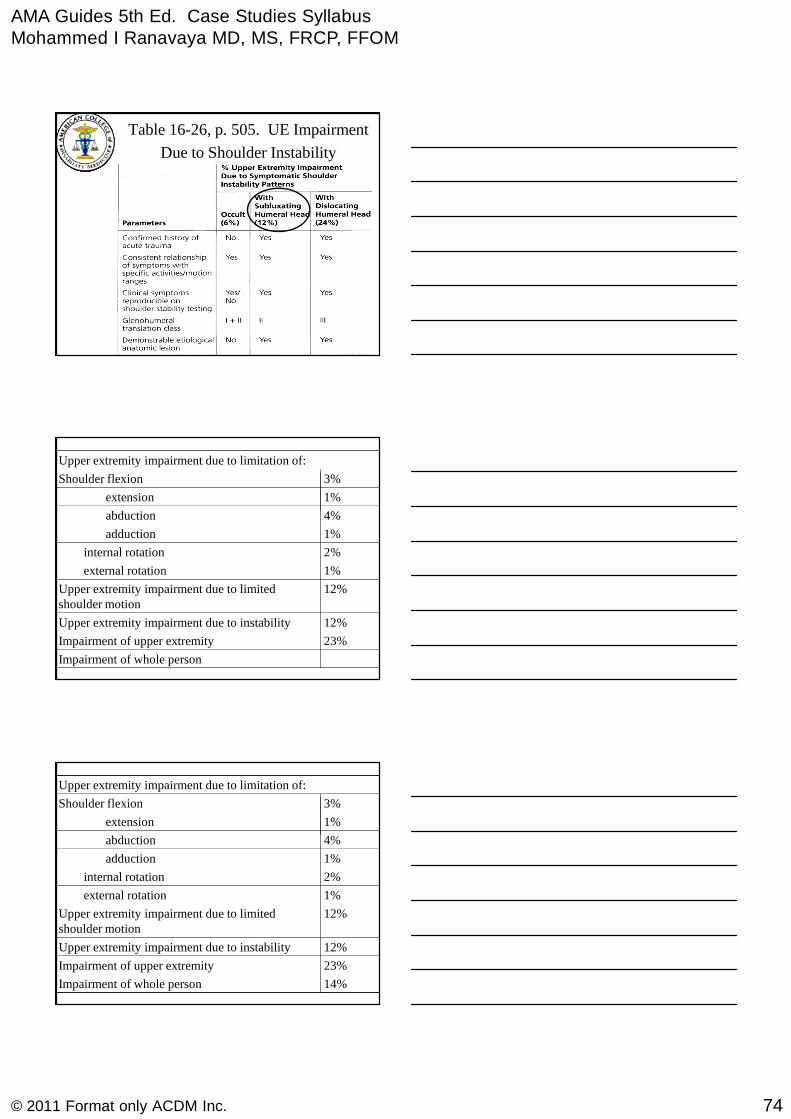
Table 16-26, p. 505. UE Impairment
Due to Shoulder Instability
23%Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
12%Upper extremity impairment due to instability
12%Upper extremity impairment due to limitedshoulder motion
1%external rotation
2%internal rotation
1%adduction
4%abduction
1%extension
3%Shoulder flexion
23%Impairment of upper extremity
Upper extremity impairment due to limitation of:
14%Impairment of whole person
12%Upper extremity impairment due to instability
12%Upper extremity impairment due to limitedshoulder motion
1%external rotation
2%internal rotation
1%adduction
4%abduction
1%extension
3%Shoulder flexion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
75© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper ExtremitiesCase Study 4Nerve Injury
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
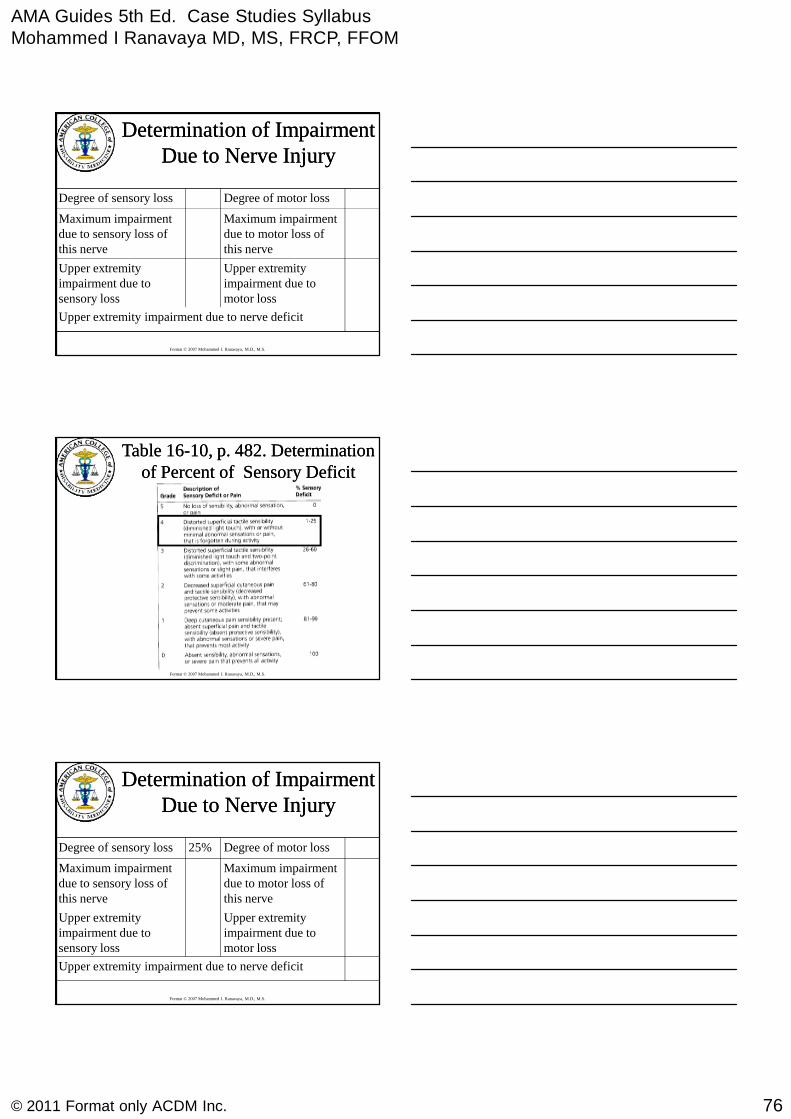
A right handed operating room nursesustained a penetrating wound of his leftupper arm, when a rushed Co workeraccidentally stabbed him with the scalpel
damaging his musculo-cutaneous nerve.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
One year later, he has full activeelbow flexion against gravity withsome resistance. He can detectpinprick on the radial side of hisforearm most of the time, but itdoesn't "feel right" in this area. Hehas no pain.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
76© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper extremity impairment due to nerve deficit
Upper extremityimpairment due tomotor loss
Upper extremityimpairment due tosensory loss
Maximum impairmentdue to motor loss ofthis nerve
Maximum impairmentdue to sensory loss ofthis nerve
Degree of motor lossDegree of sensory loss
Determination of ImpairmentDetermination of ImpairmentDue to Nerve InjuryDue to Nerve Injury
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 16Table 16--10, p. 482. Determination10, p. 482. Determinationof Percent of Sensory Deficitof Percent of Sensory Deficit
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper extremity impairment due to nerve deficit
Upper extremityimpairment due tomotor loss
Upper extremityimpairment due tosensory loss
Maximum impairmentdue to motor loss ofthis nerve
Maximum impairmentdue to sensory loss ofthis nerve
Degree of motor loss25%Degree of sensory loss
Determination of ImpairmentDetermination of ImpairmentDue to Nerve InjuryDue to Nerve Injury
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
77© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
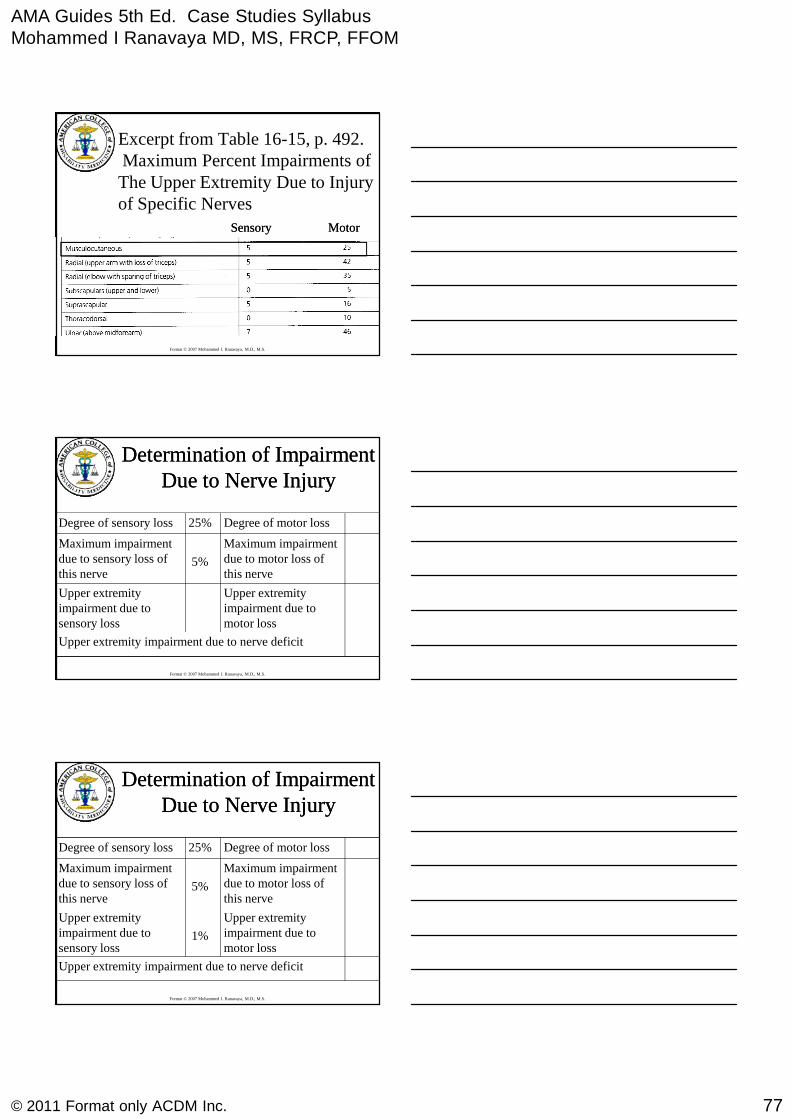
Excerpt from Table 16-15, p. 492.Maximum Percent Impairments ofThe Upper Extremity Due to Injuryof Specific Nerves
Sensory MotorSensory Motor
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper extremity impairment due to nerve deficit
Upper extremityimpairment due tomotor loss
Upper extremityimpairment due tosensory loss
Maximum impairmentdue to motor loss ofthis nerve
5%
Maximum impairmentdue to sensory loss ofthis nerve
Degree of motor loss25%Degree of sensory loss
Determination of ImpairmentDetermination of ImpairmentDue to Nerve InjuryDue to Nerve Injury
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper extremity impairment due to nerve deficit
Upper extremityimpairment due tomotor loss
1%
Upper extremityimpairment due tosensory loss
Maximum impairmentdue to motor loss ofthis nerve
5%
Maximum impairmentdue to sensory loss ofthis nerve
Degree of motor loss25%Degree of sensory loss
Determination of ImpairmentDetermination of ImpairmentDue to Nerve InjuryDue to Nerve Injury

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
78© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 16Table 16--11, p. 484.11, p. 484.Determination of Percent of Motor DeficitDetermination of Percent of Motor Deficit
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper extremity impairment due to nerve deficit
Upper extremityimpairment due tomotor loss
1%
Upper extremityimpairment due tosensory loss
Maximum impairmentdue to motor loss ofthis nerve
5%
Maximum impairmentdue to sensory loss ofthis nerve
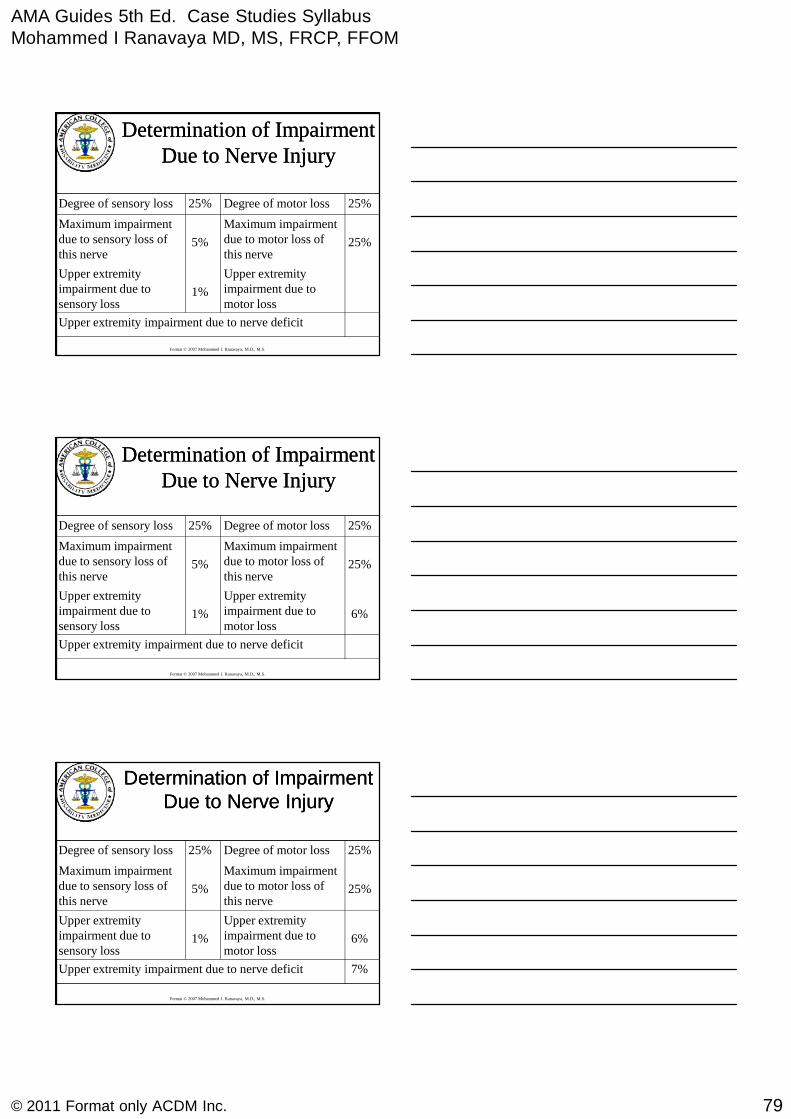
25%Degree of motor loss25%Degree of sensory loss
Determination of ImpairmentDetermination of ImpairmentDue to Nerve InjuryDue to Nerve Injury
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Excerpt from Table 16-15, p. 492.Maximum Percent Impairments ofthe Upper Extremity Due to Injuryof Specific Nerves
Sensory MotorSensory Motor
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
79© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper extremity impairment due to nerve deficit
Upper extremityimpairment due tomotor loss
1%
Upper extremityimpairment due tosensory loss
25%
Maximum impairmentdue to motor loss ofthis nerve
5%
Maximum impairmentdue to sensory loss ofthis nerve
25%Degree of motor loss25%Degree of sensory loss
Determination of ImpairmentDetermination of ImpairmentDue to Nerve InjuryDue to Nerve Injury
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper extremity impairment due to nerve deficit
6%
Upper extremityimpairment due tomotor loss
1%
Upper extremityimpairment due tosensory loss
25%
Maximum impairmentdue to motor loss ofthis nerve
5%
Maximum impairmentdue to sensory loss ofthis nerve
25%Degree of motor loss25%Degree of sensory loss
Determination of ImpairmentDetermination of ImpairmentDue to Nerve InjuryDue to Nerve Injury
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
7%Upper extremity impairment due to nerve deficit
6%
Upper extremityimpairment due tomotor loss
1%
Upper extremityimpairment due tosensory loss
25%
Maximum impairmentdue to motor loss ofthis nerve
5%
Maximum impairmentdue to sensory loss ofthis nerve
25%Degree of motor loss25%Degree of sensory loss
Determination of ImpairmentDetermination of ImpairmentDue to Nerve InjuryDue to Nerve Injury

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
80© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
7% upper extremity impairment=
4%Impairment of whole personTable 16-3, Page 439
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper ExtremitiesCase study 5
Amputations and otherinjuries
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
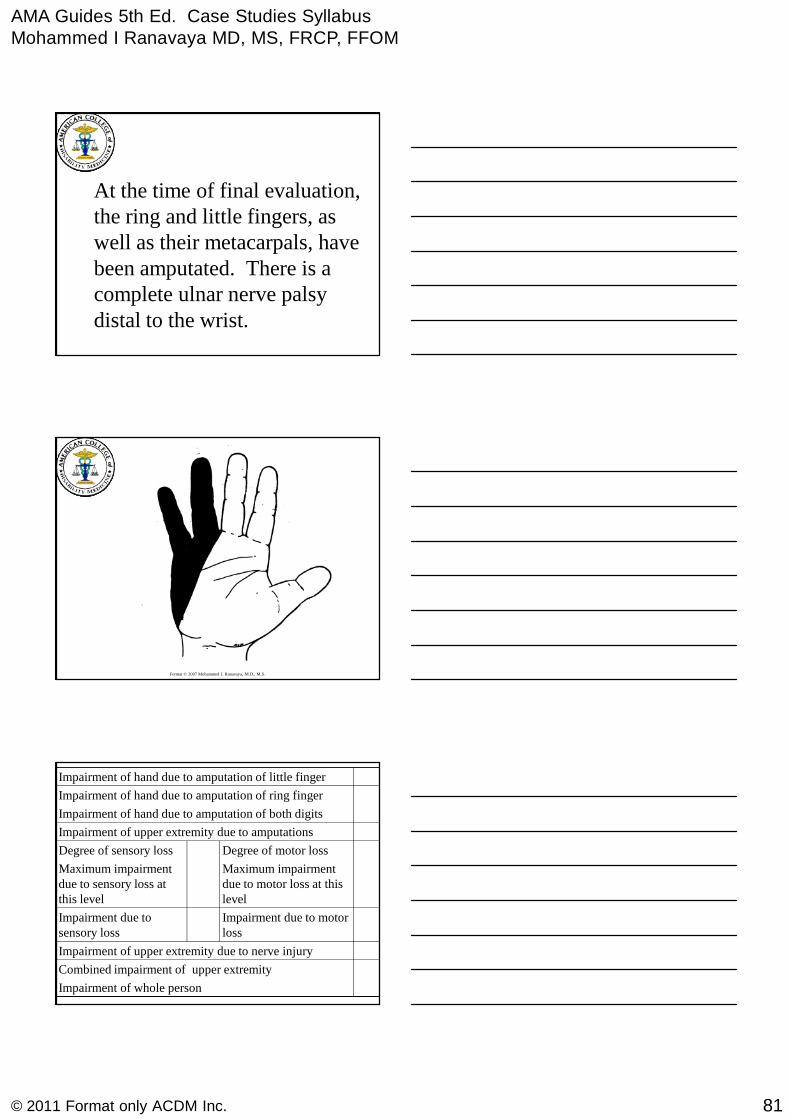
A 54 year old right handed carpentersustained a partial amputation of hisleft hand with a power saw. The sawcut began between the middle and ringfingers and came proximally andmedially to exit at the base of his
hypothenar eminence near the wrist.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
81© 2011 Format only ACDM Inc.
At the time of final evaluation,the ring and little fingers, aswell as their metacarpals, havebeen amputated. There is acomplete ulnar nerve palsydistal to the wrist.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Impairment of upper extremity due to amputations
Impairment of whole person
Combined impairment of upper extremity
Impairment of upper extremity due to nerve injury
Impairment due to motorloss
Impairment due tosensory loss
Maximum impairmentdue to motor loss at thislevel
Maximum impairmentdue to sensory loss atthis level
Degree of motor lossDegree of sensory loss
Impairment of hand due to amputation of both digits
Impairment of hand due to amputation of ring finger
Impairment of hand due to amputation of little finger
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
82© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
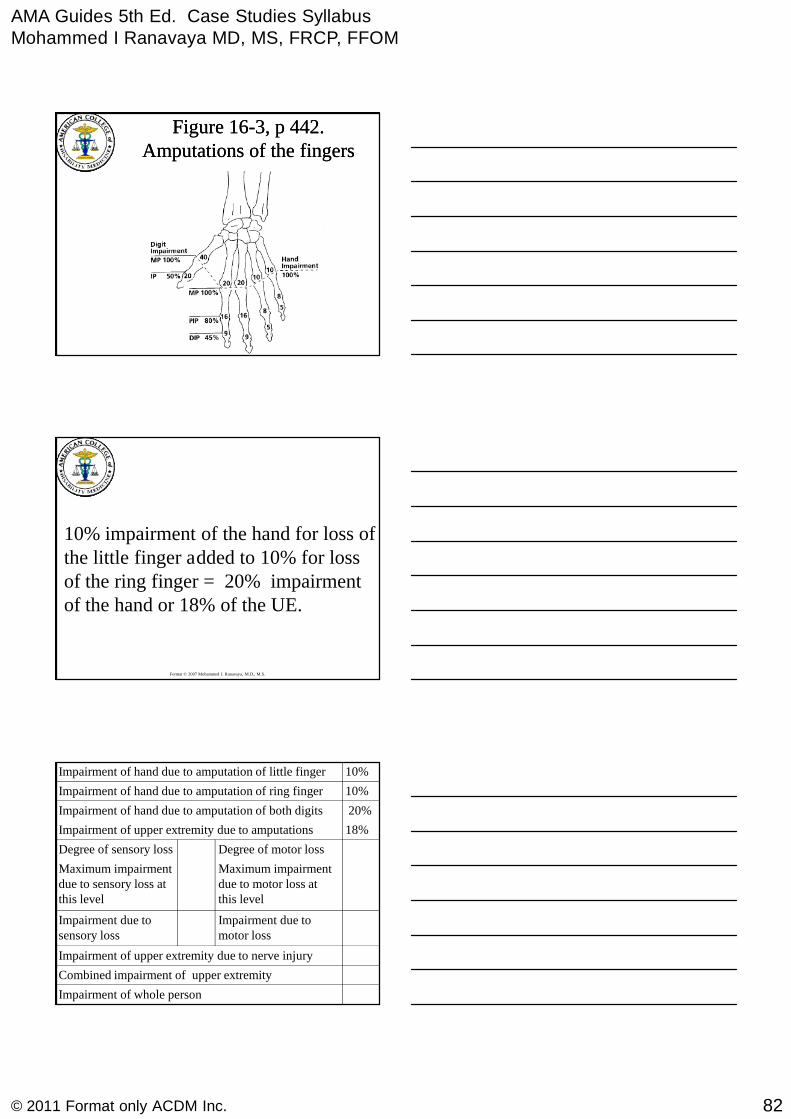
Figure 16Figure 16--3, p 442.3, p 442.Amputations of the fingersAmputations of the fingers
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
10% impairment of the hand for loss ofthe little finger added to 10% for lossof the ring finger = 20% impairmentof the hand or 18% of the UE.
18%Impairment of upper extremity due to amputations
Impairment of whole person
Combined impairment of upper extremity
Impairment of upper extremity due to nerve injury
Impairment due tomotor loss
Impairment due tosensory loss
Maximum impairmentdue to motor loss atthis level
Maximum impairmentdue to sensory loss atthis level
Degree of motor lossDegree of sensory loss
20%Impairment of hand due to amputation of both digits
10%Impairment of hand due to amputation of ring finger
10%Impairment of hand due to amputation of little finger
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
83© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
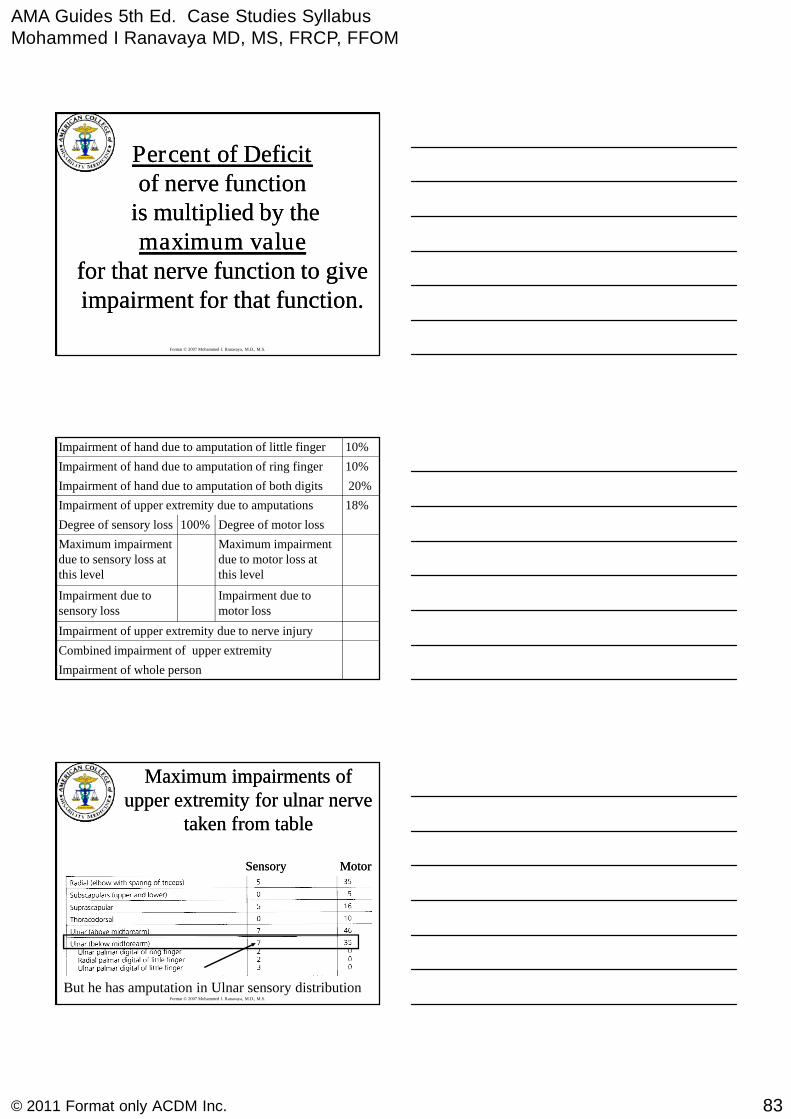
Percent of DeficitPercent of Deficitof nerve functionof nerve function
is multiplied by theis multiplied by themaximum valuemaximum value
for that nerve function to givefor that nerve function to giveimpairment for that function.impairment for that function.
18%Impairment of upper extremity due to amputations
Impairment of whole person
Combined impairment of upper extremity
Impairment of upper extremity due to nerve injury
Impairment due tomotor loss
Impairment due tosensory loss
Maximum impairmentdue to motor loss atthis level
Maximum impairmentdue to sensory loss atthis level
Degree of motor loss100%Degree of sensory loss
20%Impairment of hand due to amputation of both digits
10%Impairment of hand due to amputation of ring finger
10%Impairment of hand due to amputation of little finger
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Maximum impairments ofMaximum impairments ofupper extremity for ulnar nerveupper extremity for ulnar nerve
taken from tabletaken from table
Sensory MotorSensory Motor
But he has amputation in Ulnar sensory distribution

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
84© 2011 Format only ACDM Inc.
18%Impairment of upper extremity due to amputations
Impairment of whole person
Combined impairment of upper extremity
Impairment of upper extremity due to nerve injury
Impairment due tomotor loss
0%Impairment due tosensory loss
Maximum impairmentdue to motor loss atthis level
0%
Maximum impairmentdue to sensory loss atthis level
Degree of motor loss100%Degree of sensory loss
20%Impairment of hand due to amputation of both digits
10%Impairment of hand due to amputation of ring finger
10%Impairment of hand due to amputation of little finger
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 16Table 16--11, p. 48411, p. 484Determination of PercentDetermination of Percent
of Motor Deficitof Motor Deficit
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Maximum impairments ofMaximum impairments ofupper extremity for ulnarupper extremity for ulnar
nerve taken from table 16nerve taken from table 16--1515
Sensory MotorSensory Motor
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
85© 2011 Format only ACDM Inc.
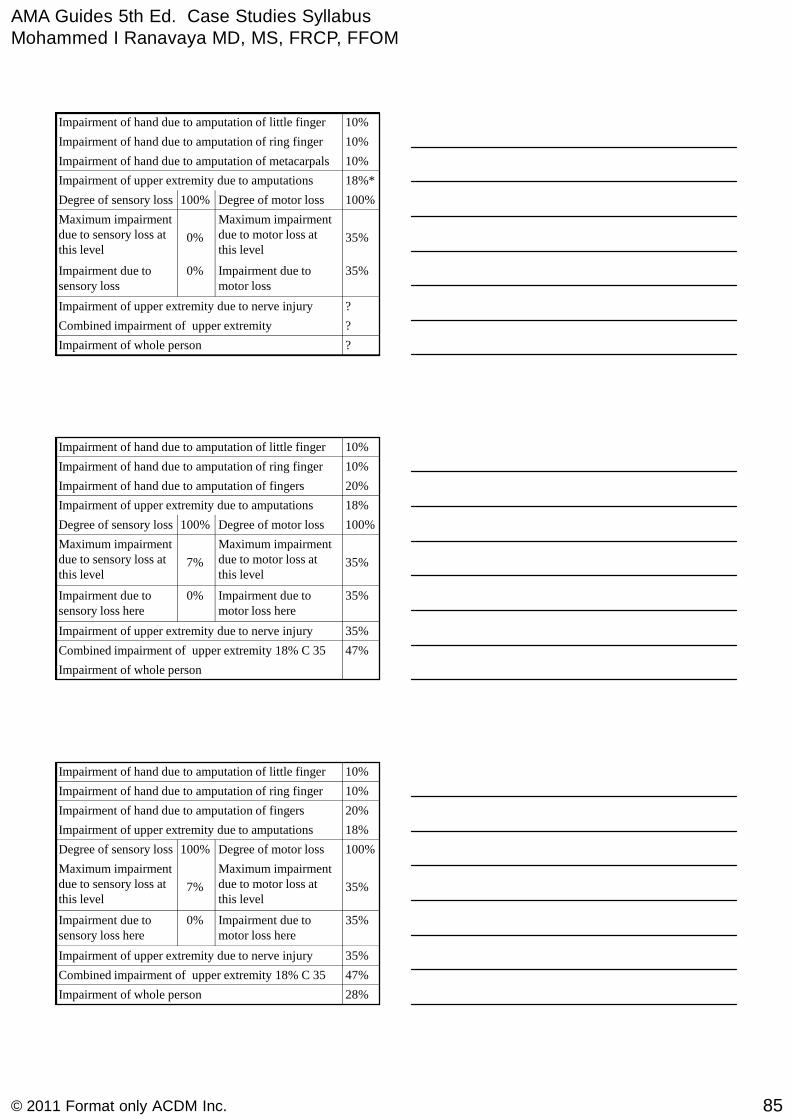
18%*Impairment of upper extremity due to amputations
?Impairment of whole person
?Combined impairment of upper extremity
?Impairment of upper extremity due to nerve injury
35%Impairment due tomotor loss
0%Impairment due tosensory loss
35%
Maximum impairmentdue to motor loss atthis level
0%
Maximum impairmentdue to sensory loss atthis level
100%Degree of motor loss100%Degree of sensory loss
10%Impairment of hand due to amputation of metacarpals
10%Impairment of hand due to amputation of ring finger
10%Impairment of hand due to amputation of little finger
18%Impairment of upper extremity due to amputations
Impairment of whole person
47%Combined impairment of upper extremity 18% C 35
35%Impairment of upper extremity due to nerve injury
35%Impairment due tomotor loss here
0%Impairment due tosensory loss here
35%
Maximum impairmentdue to motor loss atthis level
7%
Maximum impairmentdue to sensory loss atthis level
100%Degree of motor loss100%Degree of sensory loss
20%Impairment of hand due to amputation of fingers
10%Impairment of hand due to amputation of ring finger
10%Impairment of hand due to amputation of little finger
18%Impairment of upper extremity due to amputations
28%Impairment of whole person
47%Combined impairment of upper extremity 18% C 35
35%Impairment of upper extremity due to nerve injury
35%Impairment due tomotor loss here
0%Impairment due tosensory loss here
35%
Maximum impairmentdue to motor loss atthis level
7%
Maximum impairmentdue to sensory loss atthis level
100%Degree of motor loss100%Degree of sensory loss
20%Impairment of hand due to amputation of fingers
10%Impairment of hand due to amputation of ring finger
10%Impairment of hand due to amputation of little finger
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
86© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper ExtremitiesCase Study 6
Carpal Tunnel Syndrome
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
A 48 year old worker in a meat packing plantcomplained of paresthesias in her right thumb,index, and ring fingers of six months duration.She was treated with oral medications andwrist splints, and was given temporary lightwork, but continued to have significantsymptoms which bothered her during the day,
and often awakened her at night.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Surgery was suggested, but since thesurgeon told her that she probablywould be unable to return to heroriginal job without symptoms aftersurgery, she decided not to havesurgery, and changed her Job.
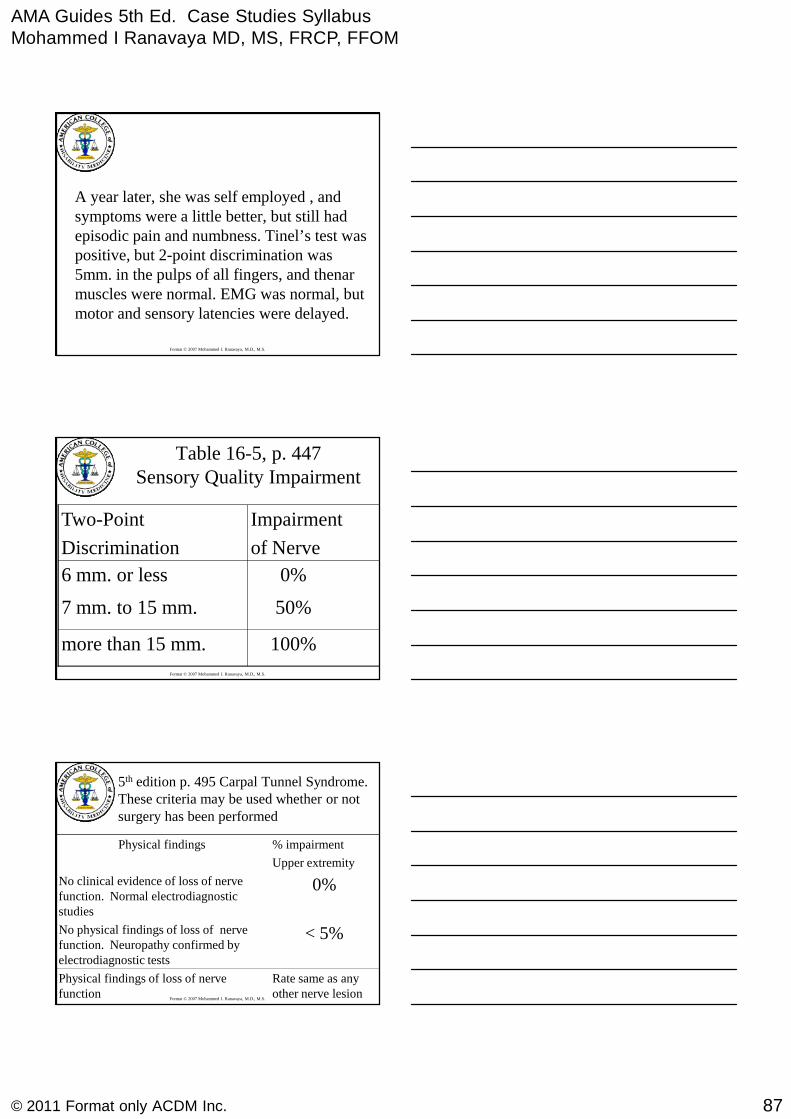
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
87© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
A year later, she was self employed , andsymptoms were a little better, but still hadepisodic pain and numbness. Tinel’s test waspositive, but 2-point discrimination was5mm. in the pulps of all fingers, and thenarmuscles were normal. EMG was normal, butmotor and sensory latencies were delayed.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 16-5, p. 447Sensory Quality Impairment
100%more than 15 mm.
50%7 mm. to 15 mm.
0%6 mm. or less
Impairment
of Nerve
Two-Point
Discrimination
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
5th edition p. 495 Carpal Tunnel Syndrome.These criteria may be used whether or notsurgery has been performed
< 5%No physical findings of loss of nervefunction. Neuropathy confirmed byelectrodiagnostic tests
Rate same as anyother nerve lesion
Physical findings of loss of nervefunction
0%No clinical evidence of loss of nervefunction. Normal electrodiagnosticstudies
% impairment
Upper extremity
Physical findings
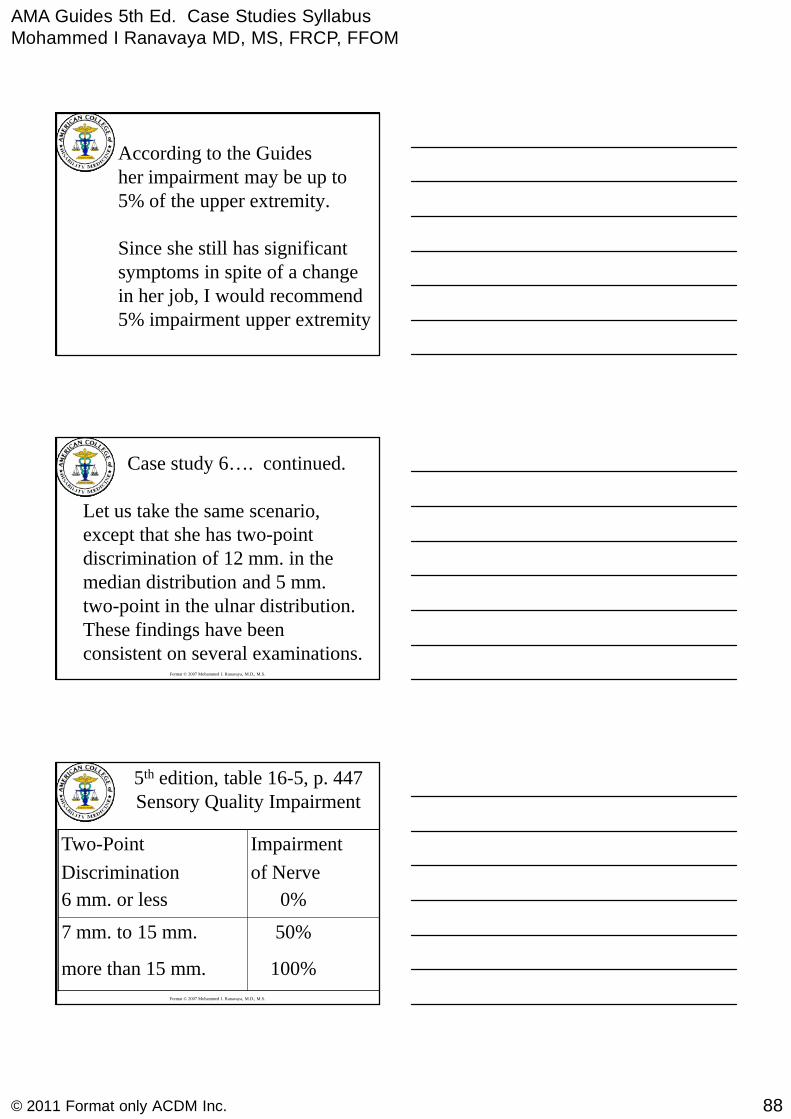
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
88© 2011 Format only ACDM Inc.
According to the Guidesher impairment may be up to5% of the upper extremity.
Since she still has significantsymptoms in spite of a changein her job, I would recommend5% impairment upper extremity
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Case study 6…. continued.
Let us take the same scenario,except that she has two-pointdiscrimination of 12 mm. in themedian distribution and 5 mm.two-point in the ulnar distribution.These findings have beenconsistent on several examinations.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
5th edition, table 16-5, p. 447Sensory Quality Impairment
100%more than 15 mm.
50%7 mm. to 15 mm.
0%6 mm. or less
Impairment
of Nerve
Two-Point
Discrimination

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
89© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Percent of DeficitPercent of Deficitof nerve functionof nerve function
is multiplied by theis multiplied by themaximum valuemaximum value
for that nerve function to givefor that nerve function to giveimpairment for that function.impairment for that function.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
5th edition, table 16-15, p. 492
Maximum percent impairments of theupper extremity from loss of sensoryor motor function
sensorysensory motormotor
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
39% of the UE is the maximumimpairment of sensory functionof the median nerve at the wrist.She has 50% impairment of thisfunction.39% X 50% = 20% of the UE12% of the Whole Person.
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
90© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper ExtremitiesCase Study 7Carpal Injury
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
A 48 year old electriciansustained a dislocated lunate ofhis left wrist in a fall from aladder. After closed reduction,the lunate underwent asepticnecrosis, necessitating aproximal row carpectomy.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
At MMI six months later, he hasflexion of 15°, extension of 30°,radial deviation of 10°, and ulnardeviation of 15°. There ispersistent moderate wrist swelling.
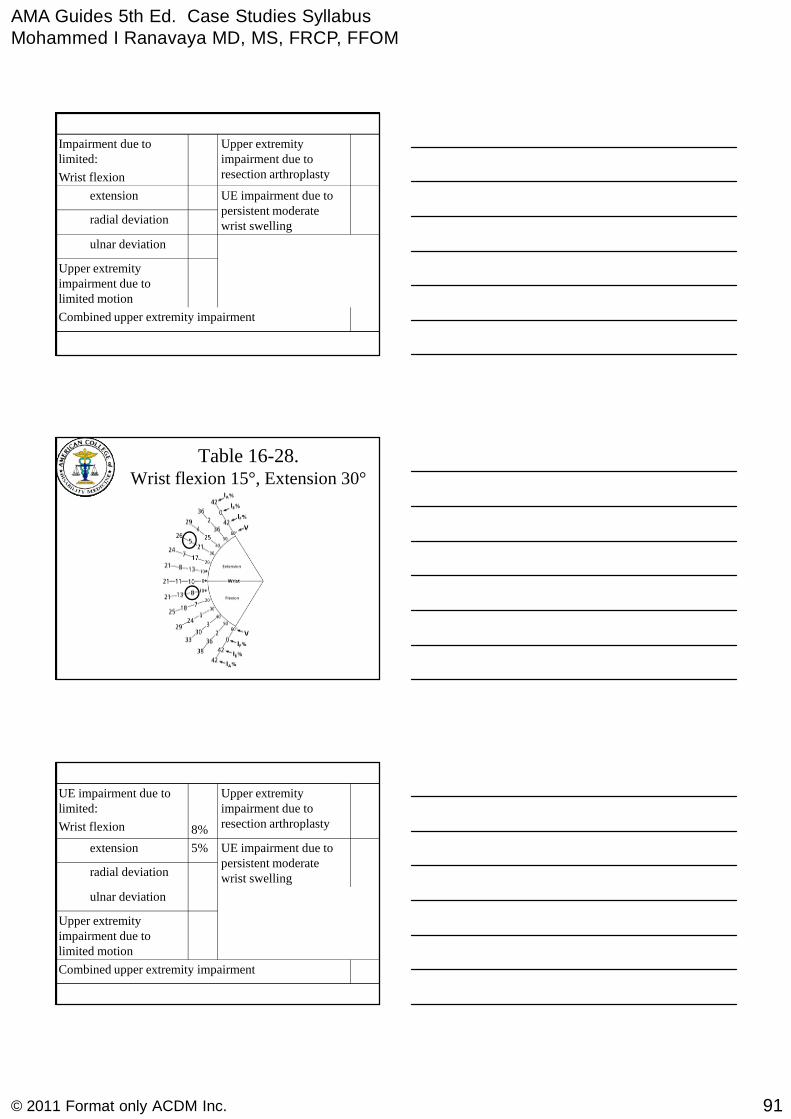
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
91© 2011 Format only ACDM Inc.
Combined upper extremity impairment
Upper extremityimpairment due tolimited motion
ulnar deviation
radial deviation
UE impairment due topersistent moderatewrist swelling
extension
Upper extremityimpairment due toresection arthroplasty
Impairment due tolimited:
Wrist flexion
Table 16-28.Wrist flexion 15°, Extension 30°
Combined upper extremity impairment
Upper extremityimpairment due tolimited motion
ulnar deviation
radial deviation
UE impairment due topersistent moderatewrist swelling
5%extension
Upper extremityimpairment due toresection arthroplasty8%
UE impairment due tolimited:
Wrist flexion
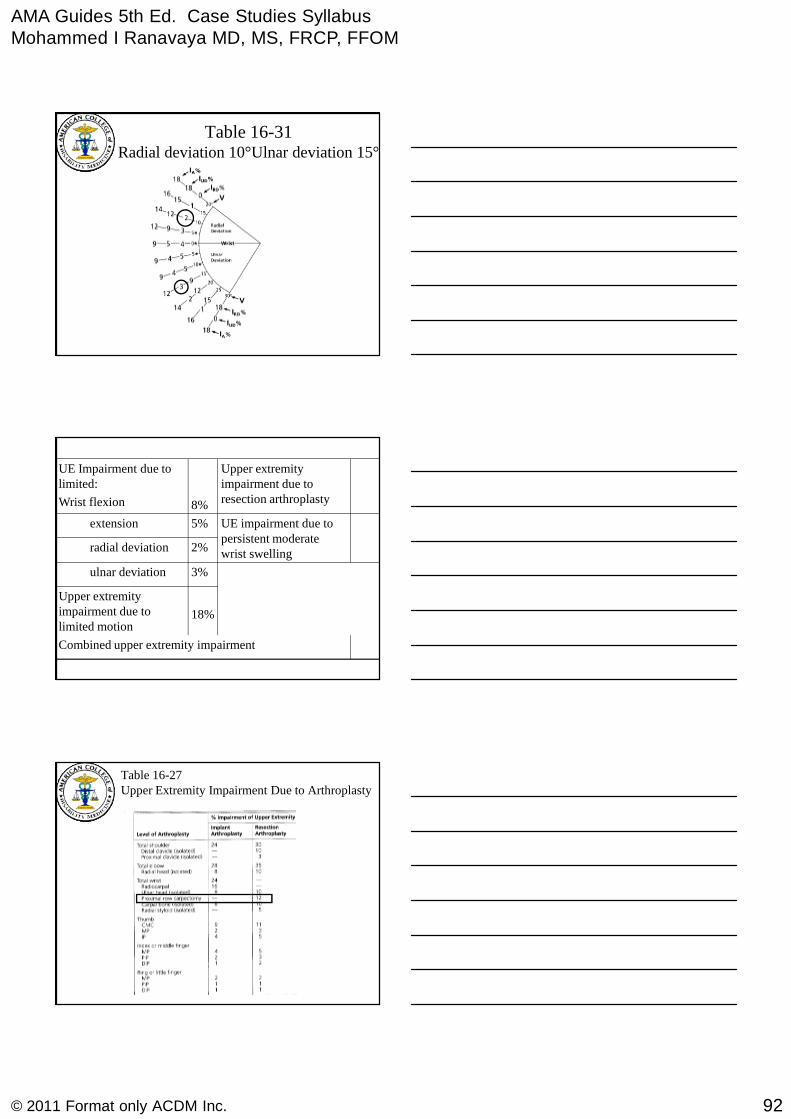
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
92© 2011 Format only ACDM Inc.
Table 16-31Radial deviation 10°Ulnar deviation 15°
Combined upper extremity impairment
18%
Upper extremityimpairment due tolimited motion
3%ulnar deviation
2%radial deviation
UE impairment due topersistent moderatewrist swelling
5%extension
Upper extremityimpairment due toresection arthroplasty8%
UE Impairment due tolimited:
Wrist flexion
Table 16-27Upper Extremity Impairment Due to Arthroplasty

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
93© 2011 Format only ACDM Inc.
Combined upper extremity impairment
18%
Upper extremityimpairment due tolimited motion
3%ulnar deviation
2%radial deviation
UE impairment due topersistent moderatewrist swelling
5%extension
12%
Upper extremityimpairment due toresection arthroplasty8%
UE Impairment due tolimited:
Wrist flexion
Table 16-19Impairment Due to Joint Swelling
Table 16-18 (499)Table 18 (58)
Impairment Values for Digits,Hand, Upper Extremity, and theWhole Person for Disorders of
Specific Joints or Units
Never used alone, always usedwith a multiplier

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
94© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
According to table 16-7, p. 498, 5th
edition, the radio-carpal joint is40% of the upper extremity.
20% of the radio-carpal joint is 8%of the upper extremity.
Combined upper extremity impairment
18%
Upper extremityimpairment due tolimited motion
3%ulnar deviation
2%radial deviation 8%
Upper extremityimpairment due toswelling
5%extension
12%
Upper extremityimpairment due toresection arthroplasty8%
UE Impairment due tolimited:
Wrist flexion
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Rules to Avoid Duplication
Joint swelling can not be rated separately
and combined with decreased jointmotion or other findings. (Pg. 500)
Take home lesson – Check carefully
Avoid Double Dipping

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
95© 2011 Format only ACDM Inc.
Combined upper extremity impairment
18%
Upper extremityimpairment due tolimited motion
3%ulnar deviation
2%radial deviation 8%
Upper extremityimpairment due toswelling
5%extension
12%
Upper extremityimpairment due toresection arthroplasty8%
UE Impairment due tolimited:
Wrist flexion
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
18% impairment of the upperextremity due to limited motionis combined with 12%impairment of the UE due toresection arthroplasty.The result is 28% of the upperextremity.
28%Combined upper extremity impairment
OR 17% Whole Person impairment
18%
Upper extremityimpairment due tolimited motion
3%ulnar deviation
2%radial deviation 8%
Upper extremityimpairment due toswelling
5%extension
12%
Upper extremityimpairment due toresection arthroplasty8%
UE Impairment due tolimited:
Wrist flexion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
96© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper ExtremitiesCase Study 8
Rotator Cuff Injury
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
A 47 year old carpenter sustained amajor rotator cuff tear of his rightshoulder while at work. He hadsurgical repair and appropriaterehabilitation.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Six months later, he was back atwork as a carpenter, although heneeded help on some parts of hisjob that he used to do by himself.He had some aching pain afterwork, and occasionally had painat night.
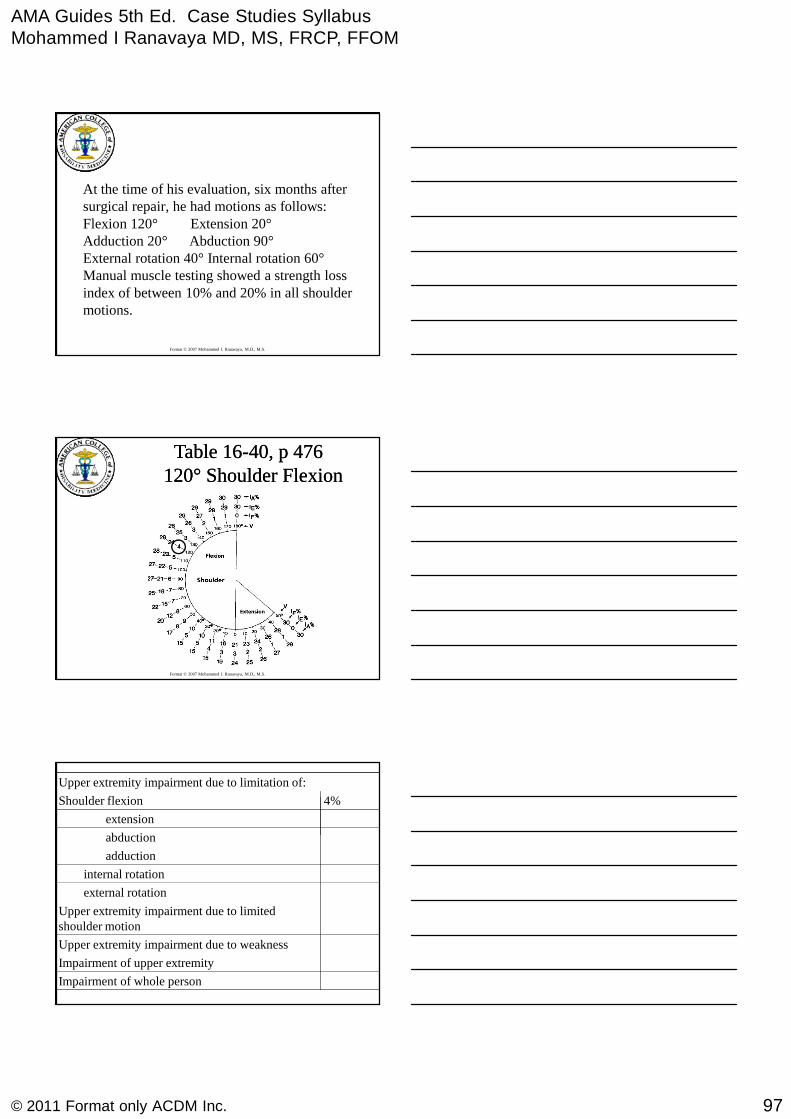
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
97© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
At the time of his evaluation, six months aftersurgical repair, he had motions as follows:Flexion 120° Extension 20°Adduction 20° Abduction 90°External rotation 40° Internal rotation 60°Manual muscle testing showed a strength lossindex of between 10% and 20% in all shouldermotions.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 16Table 16--40, p 47640, p 476120120°° Shoulder FlexionShoulder Flexion
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to weakness
Upper extremity impairment due to limitedshoulder motion
external rotation
internal rotation
adduction
abduction
extension
4%Shoulder flexion

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
98© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 16Table 16--40, p 47640, p 4762020°° Shoulder ExtensionShoulder Extension
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to weakness
Upper extremity impairment due to limitedshoulder motion
external rotation
internal rotation
adduction
abduction
2%extension
4%Shoulder flexion
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 16-43, p. 47790° Shoulder Abduction
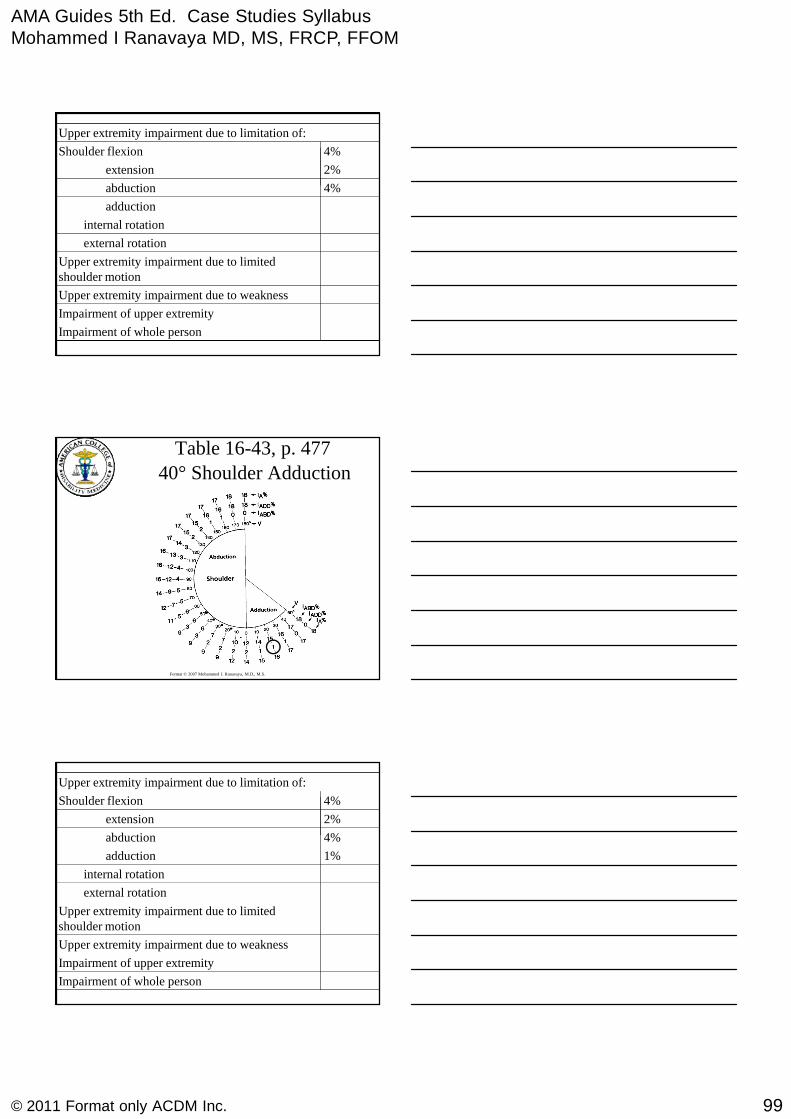
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
99© 2011 Format only ACDM Inc.
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to weakness
Upper extremity impairment due to limitedshoulder motion
external rotation
internal rotation
adduction
4%abduction
2%extension
4%Shoulder flexion
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 16-43, p. 477
40° Shoulder Adduction
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to weakness
Upper extremity impairment due to limitedshoulder motion
external rotation
internal rotation
1%adduction
4%abduction
2%extension
4%Shoulder flexion
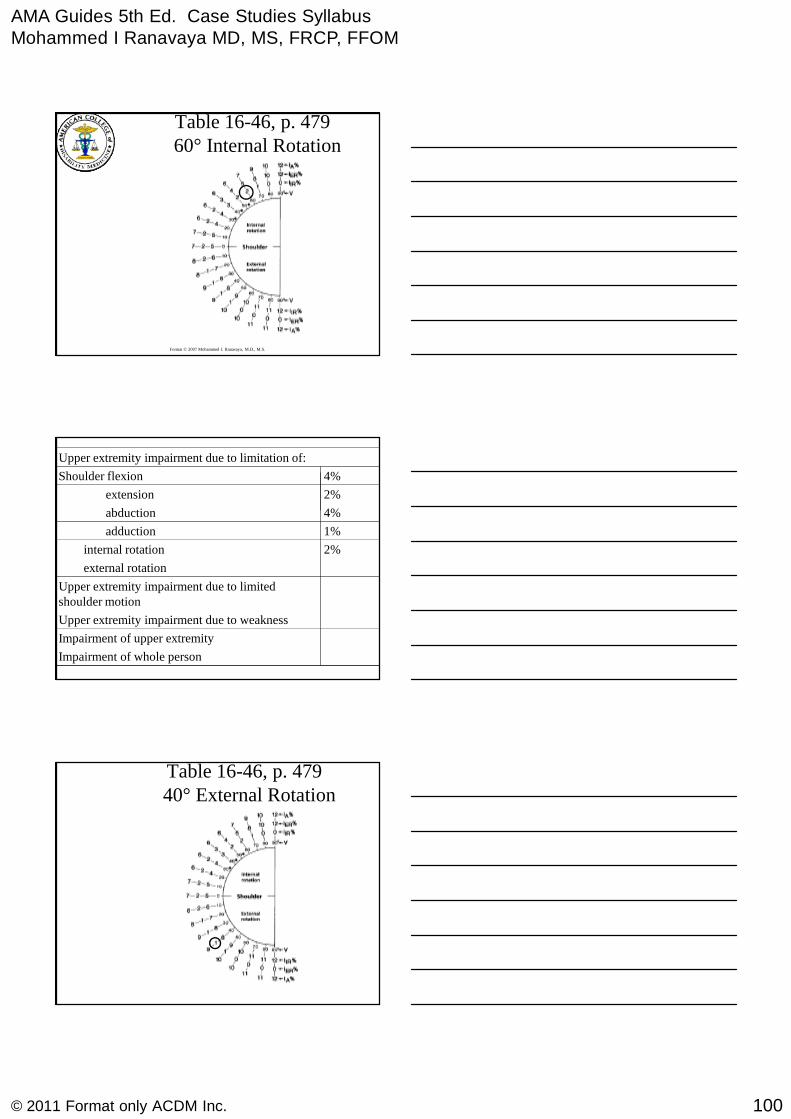
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
100© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 16-46, p. 47960° Internal Rotation
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to weakness
Upper extremity impairment due to limitedshoulder motion
external rotation
2%internal rotation
1%adduction
4%abduction
2%extension
4%Shoulder flexion
Table 16-46, p. 47940° External Rotation
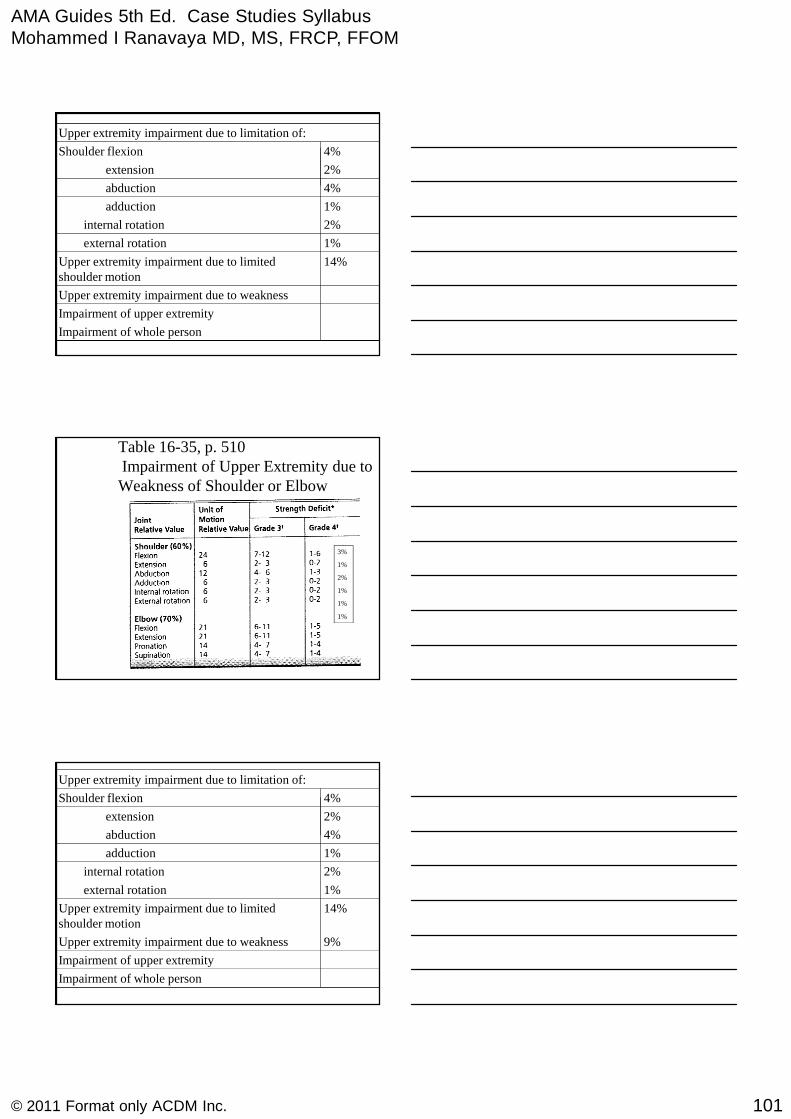
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
101© 2011 Format only ACDM Inc.
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
Upper extremity impairment due to weakness
14%Upper extremity impairment due to limitedshoulder motion
1%external rotation
2%internal rotation
1%adduction
4%abduction
2%extension
4%Shoulder flexion
Table 16-35, p. 510Impairment of Upper Extremity due toWeakness of Shoulder or Elbow
3%
1%
2%
1%
1%
1%
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
9%Upper extremity impairment due to weakness
14%Upper extremity impairment due to limitedshoulder motion
1%external rotation
2%internal rotation
1%adduction
4%abduction
2%extension
4%Shoulder flexion
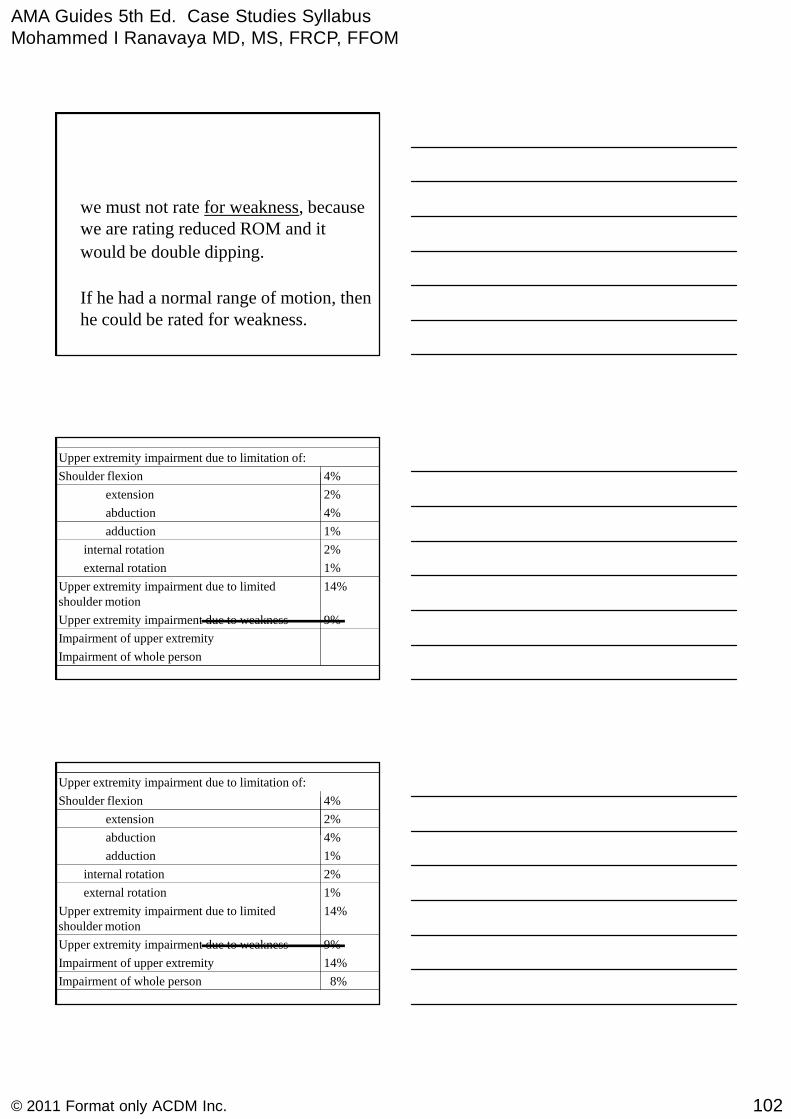
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
102© 2011 Format only ACDM Inc.
we must not rate for weakness, becausewe are rating reduced ROM and it
would be double dipping.
If he had a normal range of motion, thenhe could be rated for weakness.
Impairment of upper extremity
Upper extremity impairment due to limitation of:
Impairment of whole person
9%Upper extremity impairment due to weakness
14%Upper extremity impairment due to limitedshoulder motion
1%external rotation
2%internal rotation
1%adduction
4%abduction
2%extension
4%Shoulder flexion
14%Impairment of upper extremity
Upper extremity impairment due to limitation of:
8%Impairment of whole person
9%Upper extremity impairment due to weakness
14%Upper extremity impairment due to limitedshoulder motion
1%external rotation
2%internal rotation
1%adduction
4%abduction
2%extension
4%Shoulder flexion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
103© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper ExtremitiesCase Study 9
Apportionment ofRotator Cuff Injury
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Case 9: Rotator Cuff Tear
54 year old auto mechanic
Transmission repair, car on an overheadrack, strained right shoulder lifting thetransmission onto place (overhead heavylift)
No prior problems with right shoulder
Immediate shoulder pain
X-ray = normal, MRI = cuff tear
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Case 9: Rotator Cuff Tear
Rx = open repair -
Op Note: compliant with Post-Op physical therapy
Evaluated 1 year later, @ MMI
Mild pain with overhead activity
Back at full duty
Exam: No atrophy, Normal neurologic and vascularexams. No tenderness. No weakness, but pain onresisted abduction. Neer and Hawkins impingementsigns Negative
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
104© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Shoulder ROM
Motion Right () Left ()Flexion 140 170Extension 50 70
Abduction 120 160
Adduction 40 50
Internal Rotation 50 60
External Rotation 70 80
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
And theImpairmentRating Is ?
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Key Principles:
Upper Extremity Section rates mainly byphysical exam findings, not usually byDiagnosis
No Table for “Rotator cuff rupture orrepair”
Usually rate by ROM (Active ROM) Loss

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
105© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
ROM: Key Principles
Upper Extremity Figures for ROM Impairment donot adjust for age
Many “normal” people do not have “normal”ROM by Guides criteria, especially in the shoulder
Principle: always measure the motion in the contralateral “normal” joint
Injury Impairment = ROM impairment of theinjured minus the uninjured joint
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Right:
Flexion = 140°
Extension = 50°
Left:
Flexion = 170°
Extension = 70°
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Right:
Flexion = 140°
Extension = 50°
Left:
Flexion = 170°
Extension = 70°
Right Impairment:
Flexion = 3 %
Extension = 0 %
Left Impairment:
Flexion = 1 %
Extension = 0 %
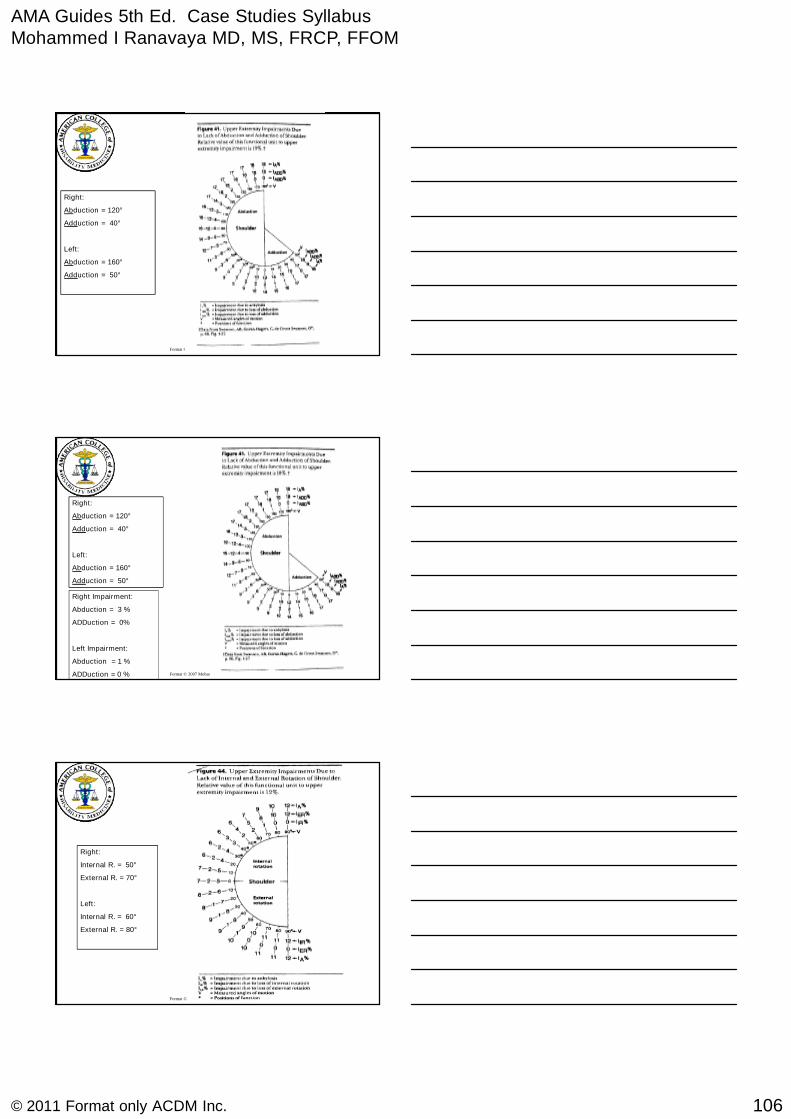
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
106© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Right:
Abduction = 120°
Adduction = 40°
Left:
Abduction = 160°
Adduction = 50°
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Right:
Abduction = 120°
Adduction = 40°
Left:
Abduction = 160°
Adduction = 50°
Right Impairment:
Abduction = 3 %
ADDuction = 0%
Left Impairment:
Abduction = 1 %
ADDuction = 0 %
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Right:
Internal R. = 50°
External R. = 70°
Left:
Internal R. = 60°
External R. = 80°
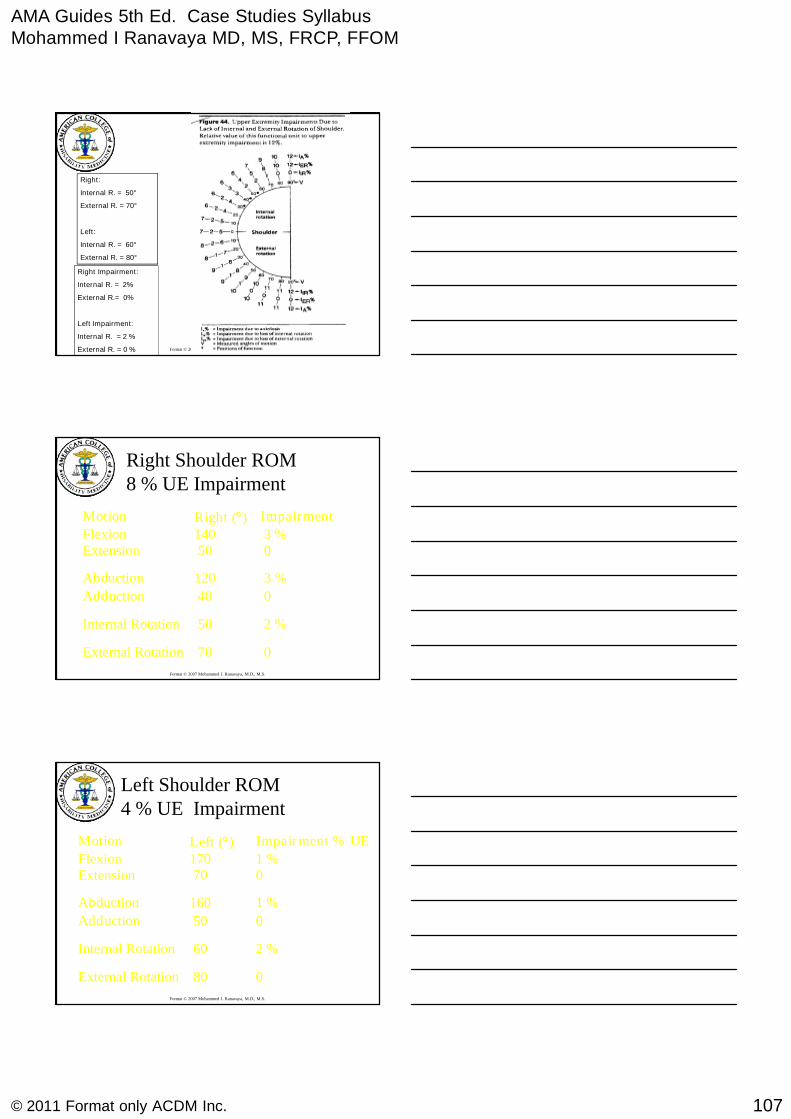
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
107© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Right:
Internal R. = 50°
External R. = 70°
Left:
Internal R. = 60°
External R. = 80°
Right Impairment:
Internal R. = 2%
External R.= 0%
Left Impairment:
Internal R. = 2 %
External R. = 0 %
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Right Shoulder ROM8 % UE Impairment
Motion Right () Impairment
Flexion 140 3 %Extension 50 0
Abduction 120 3 %
Adduction 40 0
Internal Rotation 50 2 %
External Rotation 70 0
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Left Shoulder ROM4 % UE Impairment
Motion Left () Impairment % UE
Flexion 170 1 %Extension 70 0
Abduction 160 1 %
Adduction 50 0
Internal Rotation 60 2 %
External Rotation 80 0
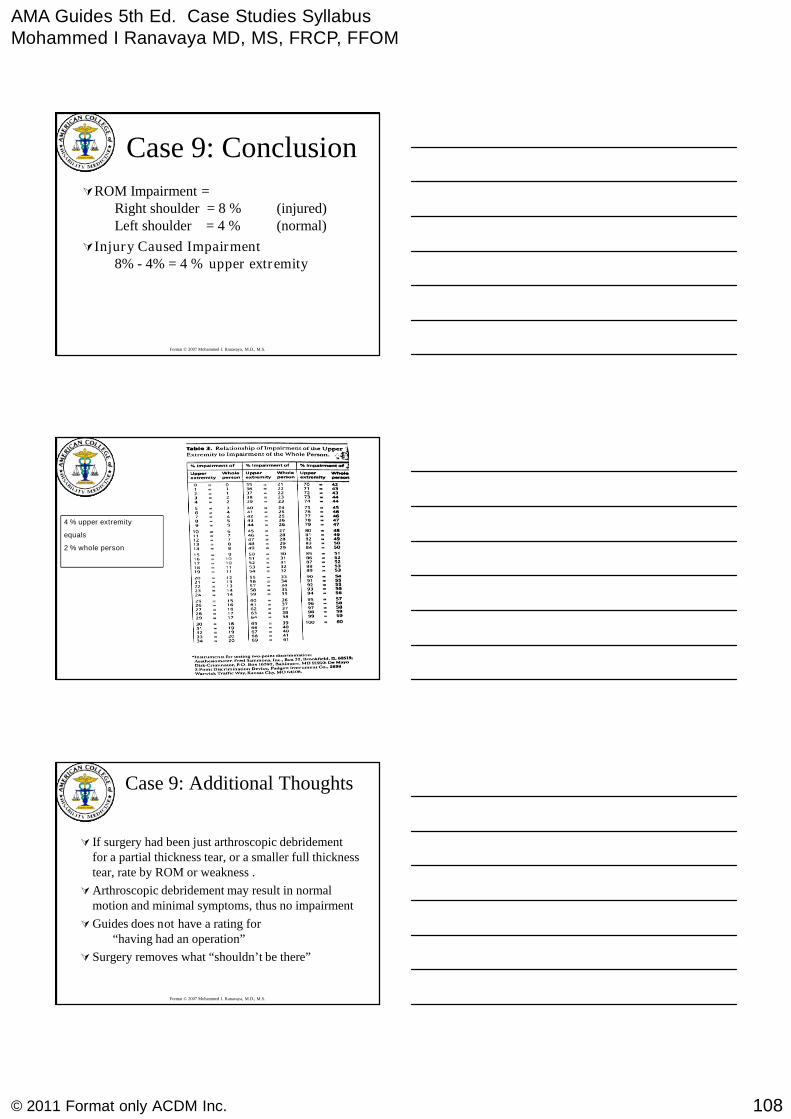
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
108© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Case 9: Conclusion
ROM Impairment =Right shoulder = 8 % (injured)Left shoulder = 4 % (normal)
Injury Caused Impairment8% - 4% = 4 % upper extremity
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
4 % upper extremity
equals
2 % whole person
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Case 9: Additional Thoughts
If surgery had been just arthroscopic debridementfor a partial thickness tear, or a smaller full thicknesstear, rate by ROM or weakness .
Arthroscopic debridement may result in normalmotion and minimal symptoms, thus no impairment
Guides does not have a rating for“having had an operation”
Surgery removes what “shouldn’t be there”

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
109© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Yet Another ThoughtResection Arthroplasty
If, at the time of rotator cuff repair, orimpingement debridement, a resection ofthe distal clavicle was performed (not justremoval of osteophyte, but removal of thedistal 1 cm including the articular surface),use Table 16-27, pg. 506 “Arthroplasty” torate the resection, and then combine withthe rating for loss of motion
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Upper ExtremitiesCase Study 10Crushed Thumb
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Case 10: Crushed Thumb
22 year old newly hired factory worker
Right dominant thumb caught in and crushed by amachine at work
Fractures
Immediate surgery (Debridement), and stagedreconstructions
Never infected
Back at work 3 months after injury
@ MMI 1 year after injury
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
110© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Case 10: Crushed ThumbExamination
IP Joint: Ankylosed @ 40°
MCP Joint: ROM = 0 - 60 °
CMC Joint: ADDuction = 6 cmRadial Abduction = 0 - 30°Opposition = 4 cm
Sensation, circulation and skin coverage:All normal
Fractures: All healed without infection or mal union
And the Impairment Is ?Thumb
Hand
Upper Extremity
Whole Person
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
ROM IP joint for the thumbFigure 16-12 (456)
ROM deficits:
IP joint ankylosed
at 40 degrees, which
equates to 10% of
the thumb –
Figure 16-12 (456)
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
111© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Metacarpophalangeal (MP) Joint:Flexion - Extension
Figure Positions16-13 (456)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Metacarpophalangeal (MP)Joint: Flexion – ExtensionFigure 16-15 (457)
MP joint ROM = 0 - 60 °
equates to 0% of the thumb
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Adduction
Measure and record thesmallest possible distancein centimeters from theflexor crease of the thumbIP joint to the distalpalmar crease over theMP joint of the littlefinger (Normal =0-1 cm.)
Note: % impairmentrelates to adduction losswhich is 20% thumb

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
112© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Adduction
Table 16-8b (459)
ImpairmentValues
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Radial Abduction
Measure and recordthe largest possibleangle in degreesformed by the firstand secondmetacarpals
30
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Radial Abduction
Table 16-8a (459)
ImpairmentValues
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
113© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Opposition
Measure and record thelargest possible distancein centimeters from theflexor crease of thethumb IP joint to thedistal palmar creasedirectly over the thirdMP joint
Figure 16-19 (460) LinearMeasurements
Note: Impairment refersto opposition loss whichis equal to 45% thumb
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Opposition
Table 16-9 (460)
ThumbImpairmentsDue to Lack
of Oppositionand to
Ankylosis
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Case 10: Crushed ThumbImpairment Summary
Add all the impairment because of the Thumb
IP Joint Ankylosis 10 %
MCP Joint ROM 0
CMC ADDuction 8 %Radial Abduction 3 %Opposition 9 %
Total thumb impairment 30 %
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
114© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
30 % Thumb Impairment =
12 % Hand Impairment
Page 438
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
12 % Hand Impairment =
11 % Upper Extremity
Page 439
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
11 % Upper ExtremityImpairment
Equivalent to:
7 % Whole Person Impairment
Page 439
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
115© 2011 Format only ACDM Inc.
AMA Guides to the Evaluationof Permanent Impairment
Fifth EditionCHAP 17
Lower Extremities
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Lower Extremities Impairment Rating
Case Study 1
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
A construction workersustains a partial medialand lateral meniscustear. She has a partialmedial and lateralmeniscectomy, andundergoes appropriaterehabilitation. Youexamine her one yearlater and find:
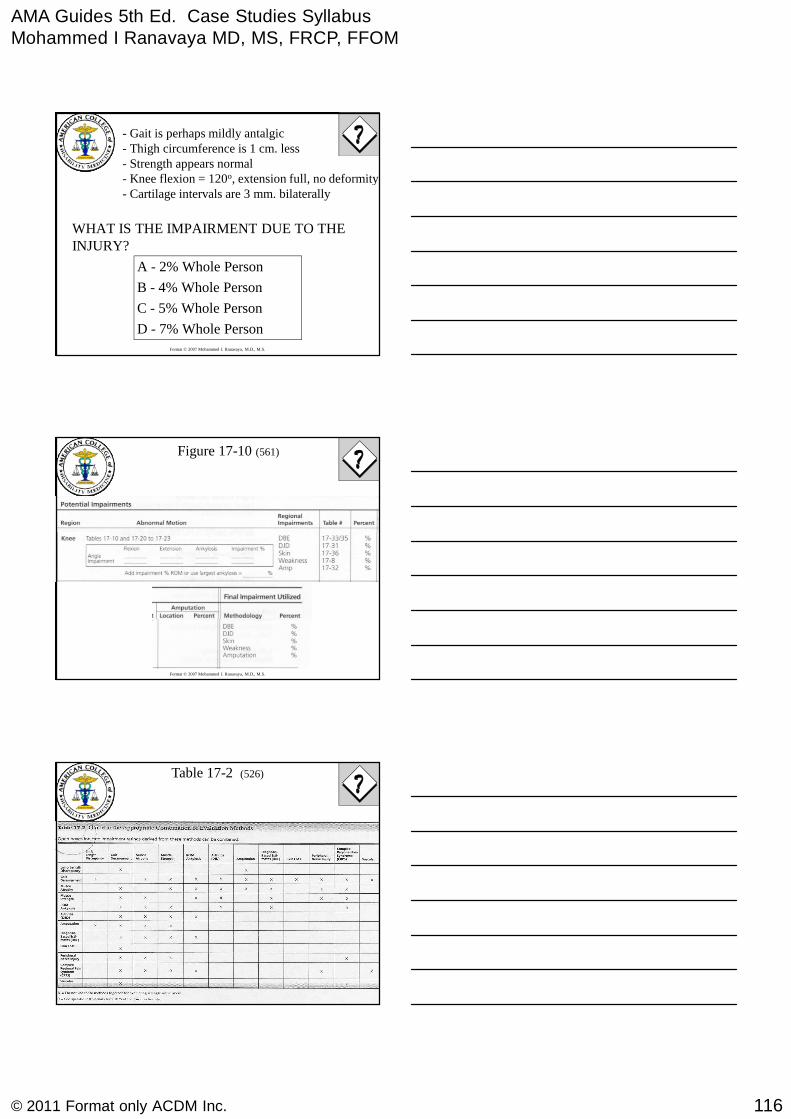
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
116© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
- Gait is perhaps mildly antalgic- Thigh circumference is 1 cm. less- Strength appears normal- Knee flexion = 120o, extension full, no deformity- Cartilage intervals are 3 mm. bilaterally
WHAT IS THE IMPAIRMENT DUE TO THEINJURY?
A - 2% Whole Person
B - 4% Whole Person
C - 5% Whole Person
D - 7% Whole Person
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Figure 17-10 (561)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-2 (526)

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
117© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-5 (529)
Not preferred methodology, morespecific methods available,therefore do not use.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-6 (530) Impairmentsfrom leg muscle atrophy
1 cm. difference, therefore 1%whole person
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-7 (531) Criteria for Grades ofMuscle Function of the Lower Extremity
No strength deficit, therefore noimpairment.
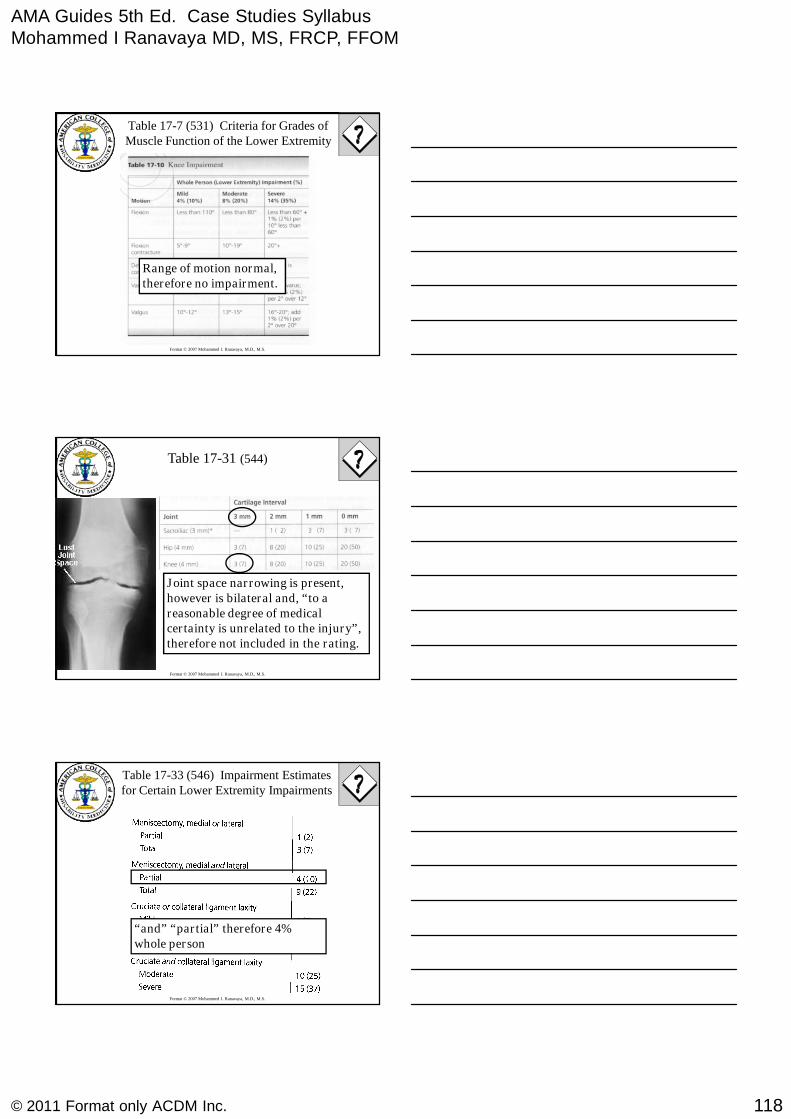
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
118© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-7 (531) Criteria for Grades ofMuscle Function of the Lower Extremity
Range of motion normal,therefore no impairment.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-31 (544)
Joint space narrowing is present,however is bilateral and, “to areasonable degree of medicalcertainty is unrelated to the injury”,therefore not included in the rating.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-33 (546) Impairment Estimatesfor Certain Lower Extremity Impairments
“and” “partial” therefore 4%whole person

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
119© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-2 (526)
Neither gait nor arthritisappropriate.
DBE = 4%, muscle atrophy =1%, however cannot combine.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Figure 17-10 (561)
120 0
43
4
1
B - 4% Whole Person
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Lower Extremities Impairment Rating
Case Study 2
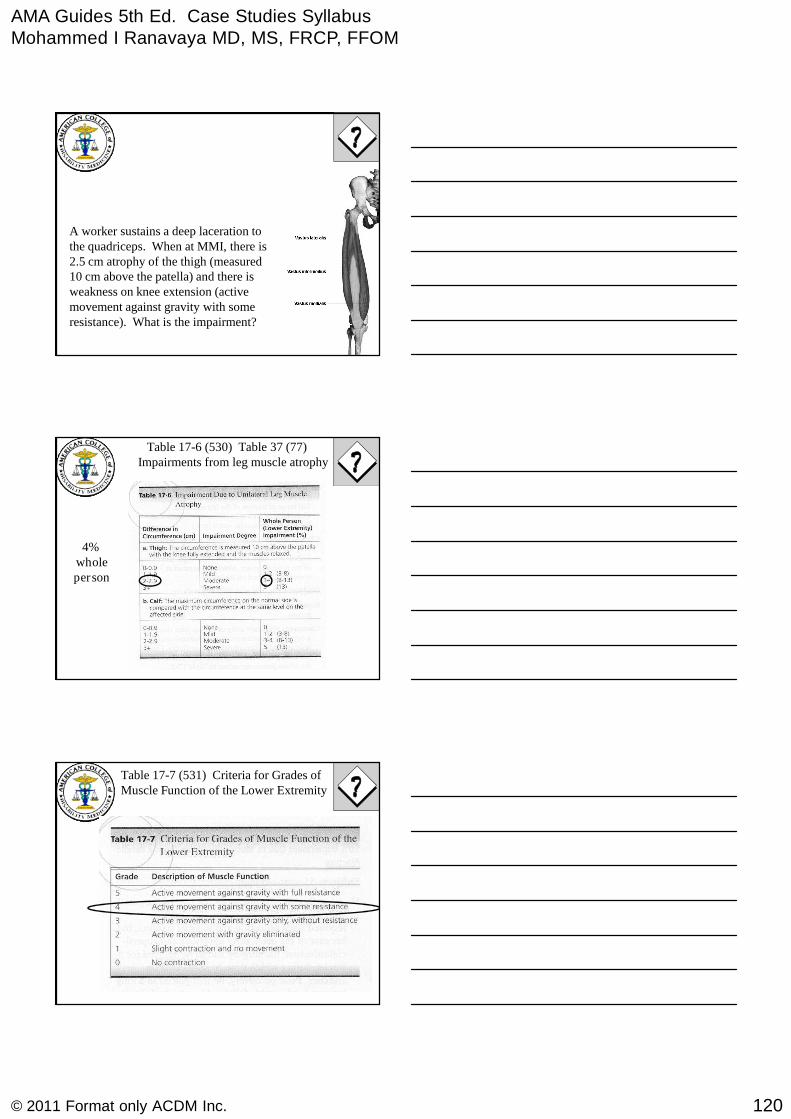
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
120© 2011 Format only ACDM Inc.
A worker sustains a deep laceration tothe quadriceps. When at MMI, there is2.5 cm atrophy of the thigh (measured10 cm above the patella) and there isweakness on knee extension (activemovement against gravity with someresistance). What is the impairment?
Table 17-6 (530) Table 37 (77)Impairments from leg muscle atrophy
4%wholeperson
Table 17-7 (531) Criteria for Grades ofMuscle Function of the Lower Extremity
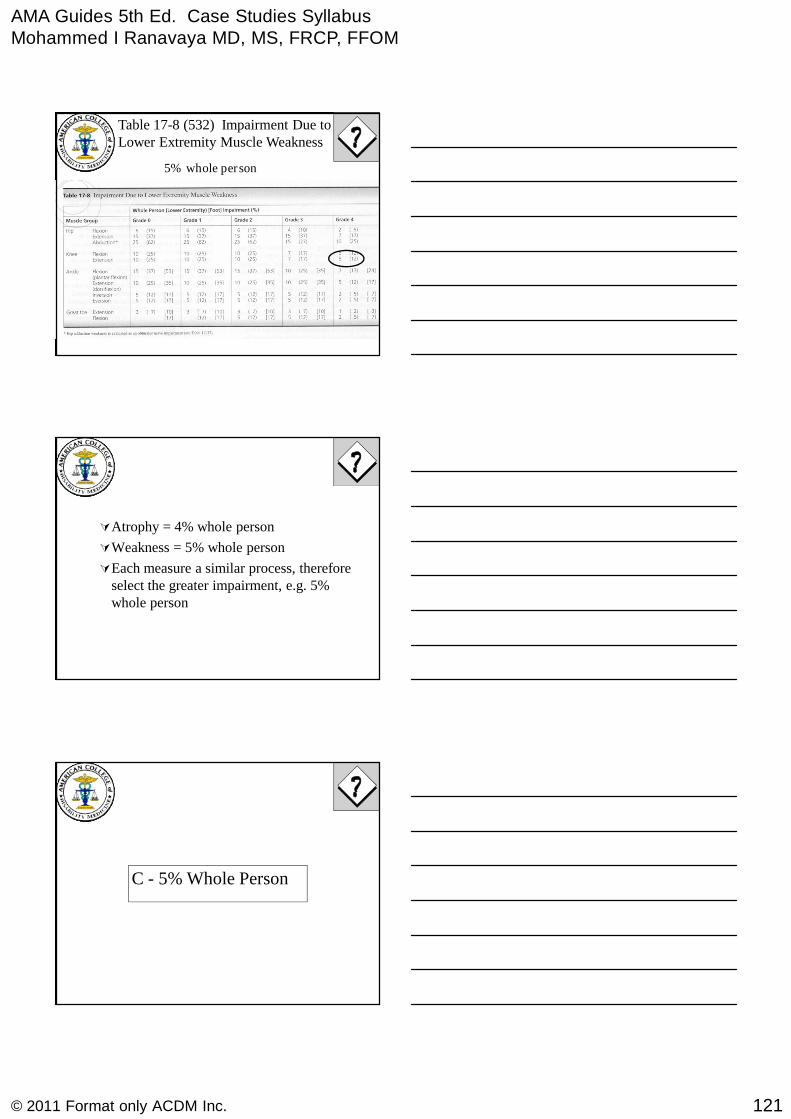
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
121© 2011 Format only ACDM Inc.
Table 17-8 (532) Impairment Due toLower Extremity Muscle Weakness
5% whole person
Atrophy = 4% whole person
Weakness = 5% whole person
Each measure a similar process, thereforeselect the greater impairment, e.g. 5%whole person
C - 5% Whole Person

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
122© 2011 Format only ACDM Inc.
The AMA Guides to theEvaluation of PermanentImpairment, 5th Edition
CASE STUDY 3
Lower Extremity
Below-Knee Amputation Case Study:– A 30-year-old mechanic who was working on a car
when the jack failed. His left leg was crushed underthe car.
– He underwent a left below-knee amputation (BKA).
Below-Knee Amputation
Lower Extremity
Below-Knee Amputation Case Study:– He underwent rehabilitation for 4 weeks.
– 12 weeks after the BKA a permanent below-kneeprosthesis was fitted.
Below-Knee Amputation

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
123© 2011 Format only ACDM Inc.
Lower Extremity
Examination of the left lower extremity reveals:
– a residual limb 5 inches below knee
– sensation, skin and circulation to be intact
– range of knee motion is restricted from 10 to 100°
– muscle power is normal (5/5) in knee flexion/Extension
– suture site is well healed without evidence of neuroma orphantom limb pain.
Below-Knee Amputation
Lower Extremity
Examination of the left lower extremity reveals:
– He is independent with donning/doffing theprosthesis as well as self-care skills
– evaluation of left hip and non affected right lowerextremity is normal
– He uses a straight cane routinely for gait stability
Below-Knee Amputation
Lower Extremity
Permanent impairment evaluation is based onSection 17.2i, Amputations; Table 17-32,Impairment Estimates for Amputations;Section 17.2f, Range of Motion; and Table17-10, Knee Impairment.
Below-Knee Amputation
Fifth Edition Rating

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
124© 2011 Format only ACDM Inc.
Lower Extremity
BKA with a residual limb more than 3 incheslong qualifies for a 28% whole personimpairment or 70% lower extremity rating.
10° knee flexion contracture as a moderateimpairment of 8% of the whole person or20% of the lower extremity.
Below-Knee Amputation
Fifth Edition Rating
Lower Extremity
Limited flexion to 100° is listed as a mildimpairment with a 4% whole person or 10%lower extremity impairment rating.
Range-of-motion restrictions in multipledirections do increase the impairment.
Below-Knee Amputation
Fifth Edition Rating
Lower Extremity
Add range-of-motion impairments for a singlejoint to determine the total joint range-of-motion impairments.
The impairment form loss of motion andflexion contracture is 30% of the lowerextremity or 12% of the whole person .
Below-Knee Amputation
Fifth Edition Rating
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
125© 2011 Format only ACDM Inc.
Lower Extremity
The Fifth contains a table to determine whenmultiple impairments can be combined andwhen they cannot (to avoid “double rating”the same condition).
Below-Knee Amputation
Fifth Edition Rating
Lower Extremity
Impairment Calculation:
The 70% of LE impairment fromBKA is combined with 30% of theLE impairment from knee loss ofmotion and flexion contracturecomes to 79% of LE impairment
32% impairment of whole person per
Below-Knee Amputation
Lower Extremity
No additional impairment rating was givenfor the routine use of a cane.
The routine use of a cane is listed as 20%whole person impairment - Lower LimbImpairment From Gait Derangement.
Below-Knee Amputation

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
126© 2011 Format only ACDM Inc.
Lower Extremity
Based on 3.2b (4th ed, p75) or Section17.2c (5thed, p529), Gait Derangement is a stand-aloneimpairment not combined with any otherimpairments method, and, whenever possible, theevaluator should use a more specific method.
In this case, the below-knee amputation withrestricted knee range of motion is the specificcondition determining the impairment.
Below-Knee Amputation
Lower Extremity
To combine these 2 ratings would beinappropriate and only inflate theimpairment rating unjustifiably.
Below-Knee Amputation
Discussion
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
127© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Lower ExtremitiesImpairment Rating
Femur fracture and sciaticnerve injuryCASE STUDY 4
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
A 27 year old electrician sustained acomminuted open subtrochantericfracture of his femur, with injury tohis sciatic nerve. He was treated withopen reduction and internal fixationof the fracture.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
One year later, he walked with a significantlimp, and wore a short leg brace. There was acomplete sciatic nerve palsy at the level ofthe upper thigh. Because of his anestheticfoot, he had an ulcer on his heel. There was 2cm. atrophy of his thigh, and 3cm. atrophy ofhis calf.

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
128© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
He had 2 cm. shortening of hisLE. Hip motions were asfollows: flexion 135°, extension0°, adduction 10°, abduction 20°,internal rotation 0°, externalrotation 50°.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-4 (528)
Limb length discrepancy
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment
5% LELeg length discrepancy (2 cm.)
Limited hip motion
Calf atrophy
Thigh atrophy
whole person
Total impairment of lower extremity
Nerve deficit (complete sciatic palsy)
Skin loss (ulcer on heel)
Gait derangement (use of SL brace)

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
129© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
WP Impairment %Clinical signs
30
Full time cane or crutch
and short leg brace
20
Full time cane or crutch
or long leg brace
15Full time short leg brace
15Part time cane or crutch
10Positive Trendelenberg
7Antalgic limp
From Table 17-5 (529)
Gait Derangement
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment
5% LELeg length discrepancy (2 cm.)
Limited hip motion
Calf atrophy
Thigh atrophy
whole person
Total impairment of lower extremity
Nerve deficit (complete sciatic palsy)
Skin loss (ulcer on heel)
15%Gait derangement (use of SL brace)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-6 (530)
Impairment From Leg Muscle Atrophy
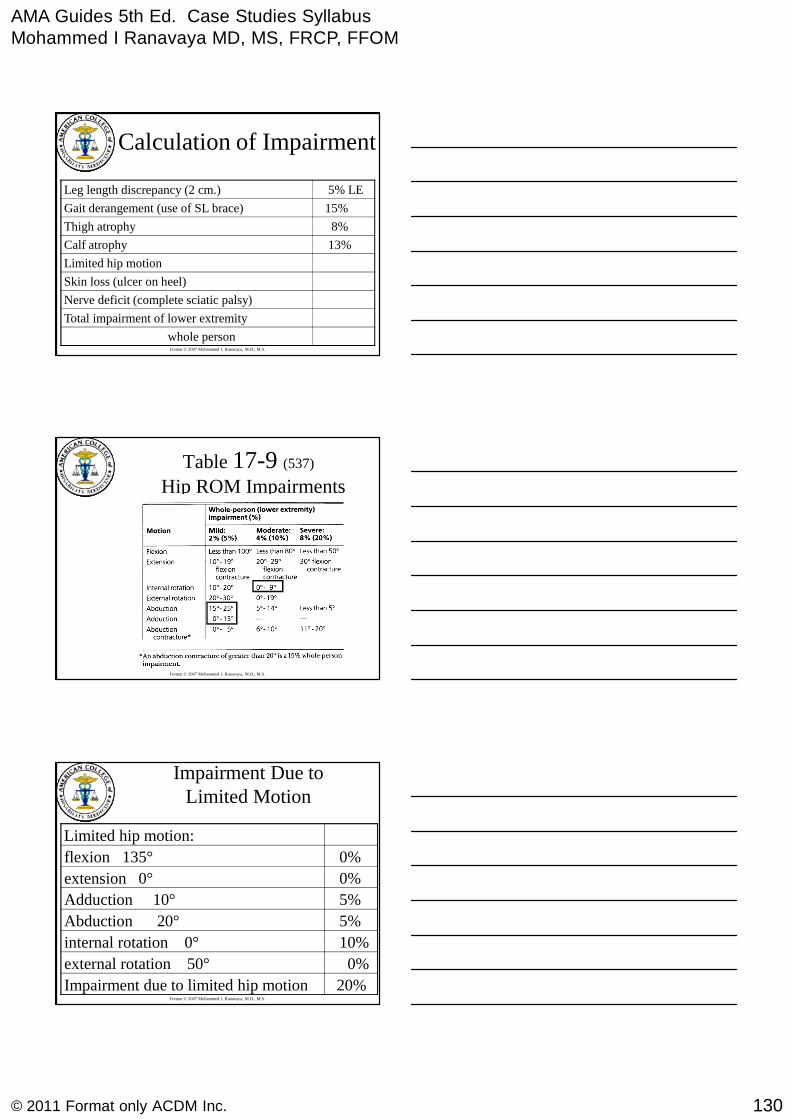
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
130© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment
5% LELeg length discrepancy (2 cm.)
Limited hip motion
13%Calf atrophy
8%Thigh atrophy
whole person
Total impairment of lower extremity
Nerve deficit (complete sciatic palsy)
Skin loss (ulcer on heel)
15%Gait derangement (use of SL brace)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-9 (537)
Hip ROM Impairments
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Impairment Due toLimited Motion
Limited hip motion:
20%Impairment due to limited hip motion
0%external rotation 50°
10%internal rotation 0°
5%Abduction 20°
5%Adduction 10°
0%extension 0°
0%flexion 135°
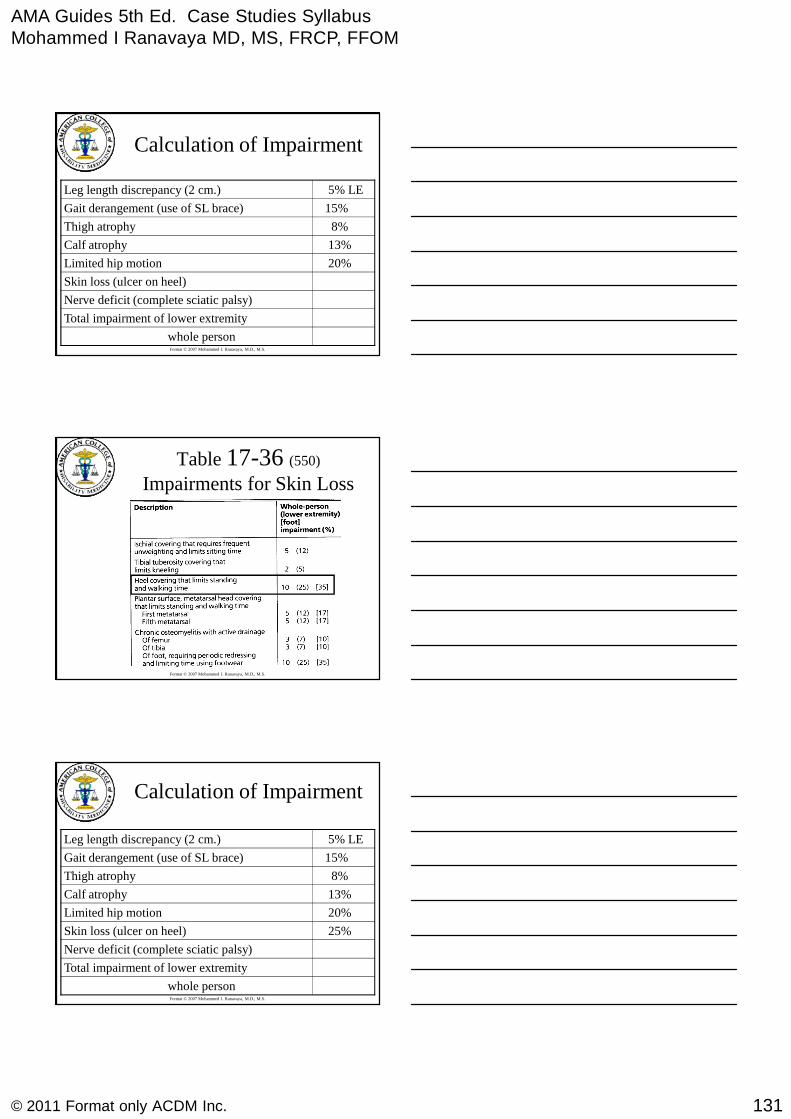
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
131© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment
5% LELeg length discrepancy (2 cm.)
20%Limited hip motion
13%Calf atrophy
8%Thigh atrophy
whole person
Total impairment of lower extremity
Nerve deficit (complete sciatic palsy)
Skin loss (ulcer on heel)
15%Gait derangement (use of SL brace)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-36 (550)
Impairments for Skin Loss
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment
5% LELeg length discrepancy (2 cm.)
20%Limited hip motion
13%Calf atrophy
8%Thigh atrophy
whole person
Total impairment of lower extremity
Nerve deficit (complete sciatic palsy)
25%Skin loss (ulcer on heel)
15%Gait derangement (use of SL brace)
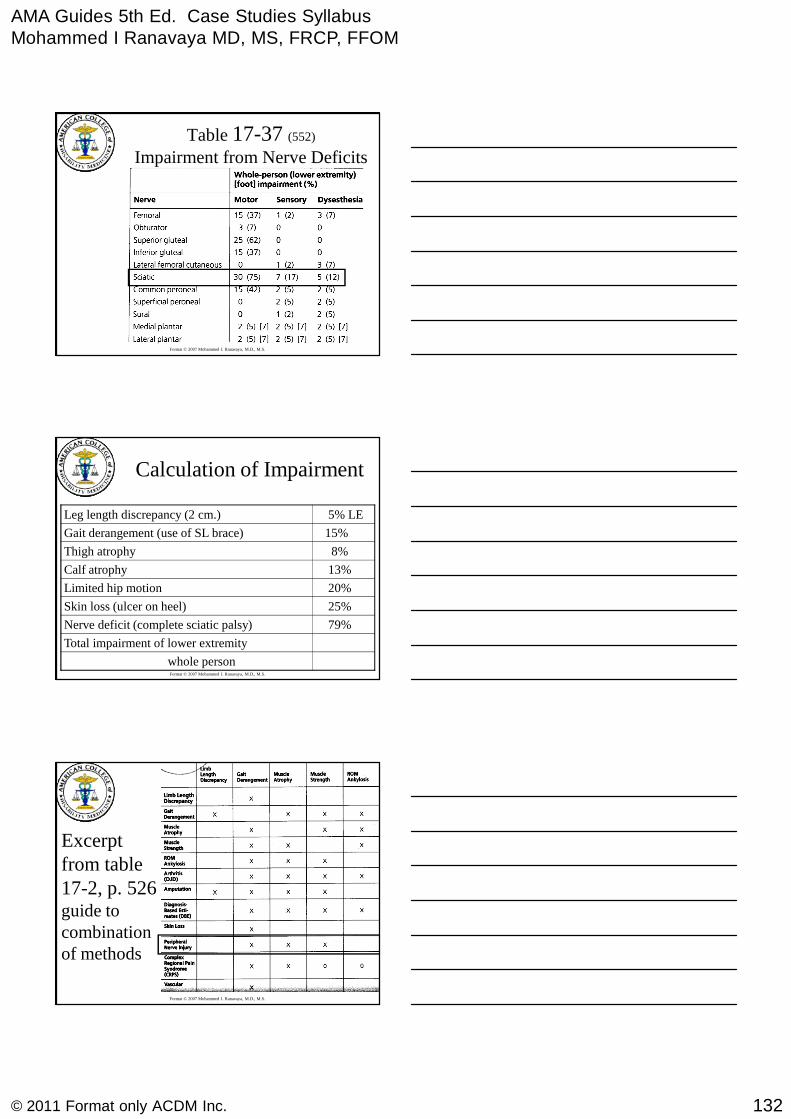
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
132© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Table 17-37 (552)
Impairment from Nerve Deficits
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment
5% LELeg length discrepancy (2 cm.)
20%Limited hip motion
13%Calf atrophy
8%Thigh atrophy
whole person
Total impairment of lower extremity
79%Nerve deficit (complete sciatic palsy)
25%Skin loss (ulcer on heel)
15%Gait derangement (use of SL brace)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Excerptfrom table17-2, p. 526guide tocombinationof methods

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
133© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment
5% LELeg length discrepancy (2 cm.)
20%Limited hip motion
13%Calf atrophy
8%Thigh atrophy
whole person
Total impairment of lower extremity
79%Nerve deficit (complete sciatic palsy)
25%Skin loss (ulcer on heel)
15%Gait derangement (use of SL brace)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
79% combined with 25%= 84%84% combined with 20% = 87%87% combined with 5% =88%
88% of LE =35% of WP
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment
5% LELeg length discrepancy (2 cm.)
20%Limited hip motion
13%Calf atrophy
8%Thigh atrophy
35%whole person
88%Total impairment of lower extremity
79%Nerve deficit (complete sciatic palsy)
25%Skin loss (ulcer on heel)
15%Gait derangement (use of SL brace)

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
134© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Lower Extremities Impairment Rating
Fracture dislocation hip with fusion.
Case Study 5
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
At age 28, a man sustained a fracture-dislocation of his hip in a fall at work. Hedeveloped a severe post traumatic arthritis ofhis hip. Since he was not a candidate for ahip replacement, a fusion was performed atage 33. While drinking with some friends, heconvinced them to help him cut the spica castoff, and he did not return for follow up for sixmonths.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
At MMI one year after surgery, X-raysshowed a solid hip fusion. Cartilage spacewas 0 mm. He had no pain, but had a severelimp, and used one crutch full time. Hipmotions were as follows:Flexion 45°Adduction 10°External rotation 15°

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
135© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment ofLower Extremity
Impairment due to loss of cartilage space
Total impairment of lower extremity
Impairment due to gait derangement
Impairment due to nonfunctional position inadduction
Impairment due to nonfunctional position inrotation
Impairment due to nonfunctional position inflexion
Impairment of LE due to ankylosis of the hip
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Ankylosis (total loss of motion) of the hip in themost functional position (25° - 40° flexion, < 5°internal rotation, adduction or abduction, < 10°external rotation) results in an impairment of 50%of the lower extremity or 20% of the whole person.If the joint is ankylosed in a less than optimumposition, additional impairments are combined andthe result is added to this percentage.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment ofLower Extremity
Impairment due to loss of cartilage space
Impairment due to gait derangement
Impairment due to nonfunctional position inadduction
Impairment due to nonfunctional position inrotation
Impairment due to nonfunctional position inflexion
50%Impairment of LE due to ankylosis of the hip
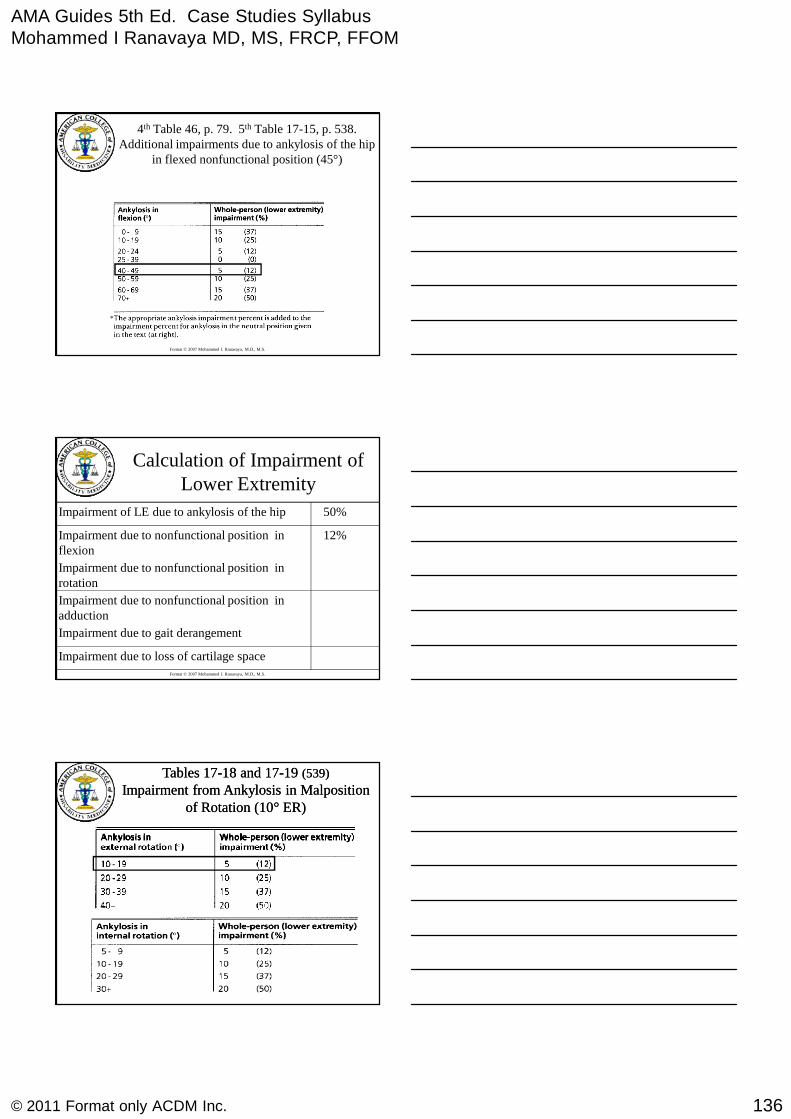
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
136© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
4th Table 46, p. 79. 5th Table 17-15, p. 538.Additional impairments due to ankylosis of the hip
in flexed nonfunctional position (45°)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment ofLower Extremity
Impairment due to loss of cartilage space
Impairment due to gait derangement
Impairment due to nonfunctional position inadduction
Impairment due to nonfunctional position inrotation
12%Impairment due to nonfunctional position inflexion
50%Impairment of LE due to ankylosis of the hip
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Tables 17Tables 17--18 and 1718 and 17--1919 (539)(539)
Impairment from Ankylosis in MalpositionImpairment from Ankylosis in Malpositionof Rotation (10of Rotation (10°° ER)ER)
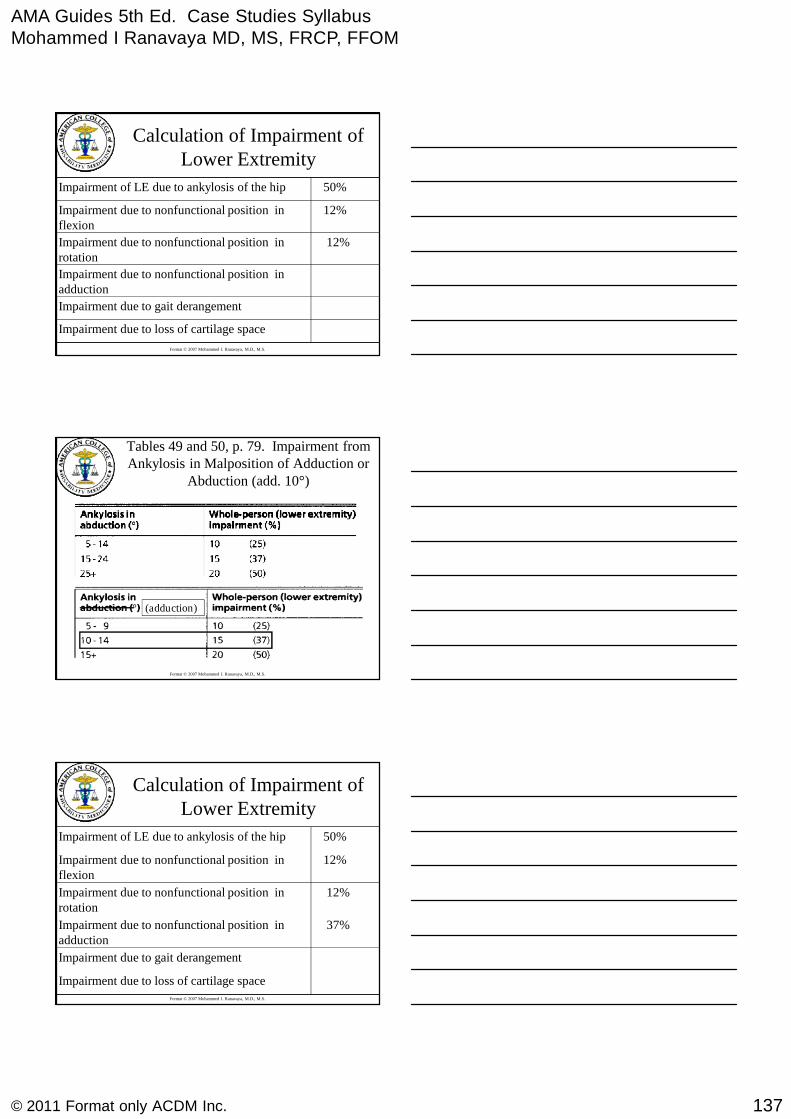
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
137© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment ofLower Extremity
Impairment due to loss of cartilage space
Impairment due to gait derangement
Impairment due to nonfunctional position inadduction
12%Impairment due to nonfunctional position inrotation
12%Impairment due to nonfunctional position inflexion
50%Impairment of LE due to ankylosis of the hip
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Tables 49 and 50, p. 79. Impairment fromAnkylosis in Malposition of Adduction or
Abduction (add. 10°)
(adduction)
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment ofLower Extremity
Impairment due to loss of cartilage space
Impairment due to gait derangement
37%Impairment due to nonfunctional position inadduction
12%Impairment due to nonfunctional position inrotation
12%Impairment due to nonfunctional position inflexion
50%Impairment of LE due to ankylosis of the hip
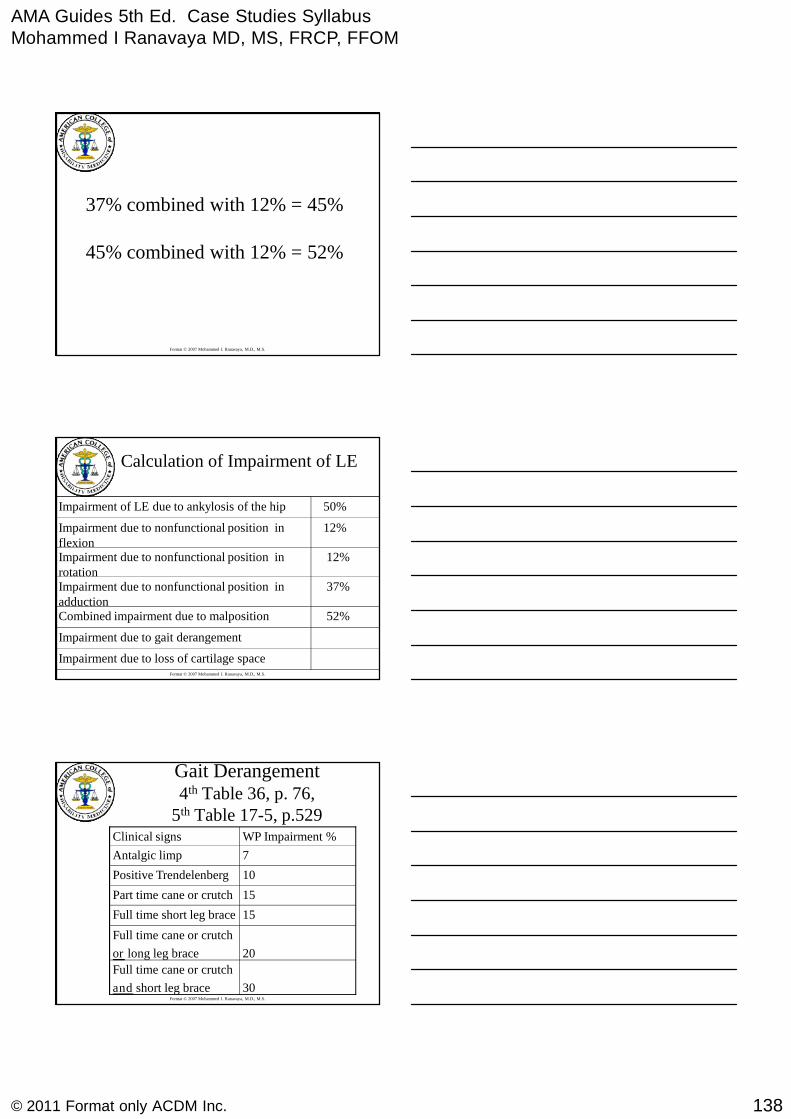
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
138© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
37% combined with 12% = 45%
45% combined with 12% = 52%
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment of LE
37%Impairment due to nonfunctional position inadduction
52%Combined impairment due to malposition
Impairment due to loss of cartilage space
Impairment due to gait derangement
12%Impairment due to nonfunctional position inrotation
12%Impairment due to nonfunctional position inflexion
50%Impairment of LE due to ankylosis of the hip
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
WP Impairment %Clinical signs
30
Full time cane or crutch
and short leg brace
20
Full time cane or crutch
or long leg brace
15Full time short leg brace
15Part time cane or crutch
10Positive Trendelenberg
7Antalgic limp
Gait Derangement4th Table 36, p. 76,
5th Table 17-5, p.529
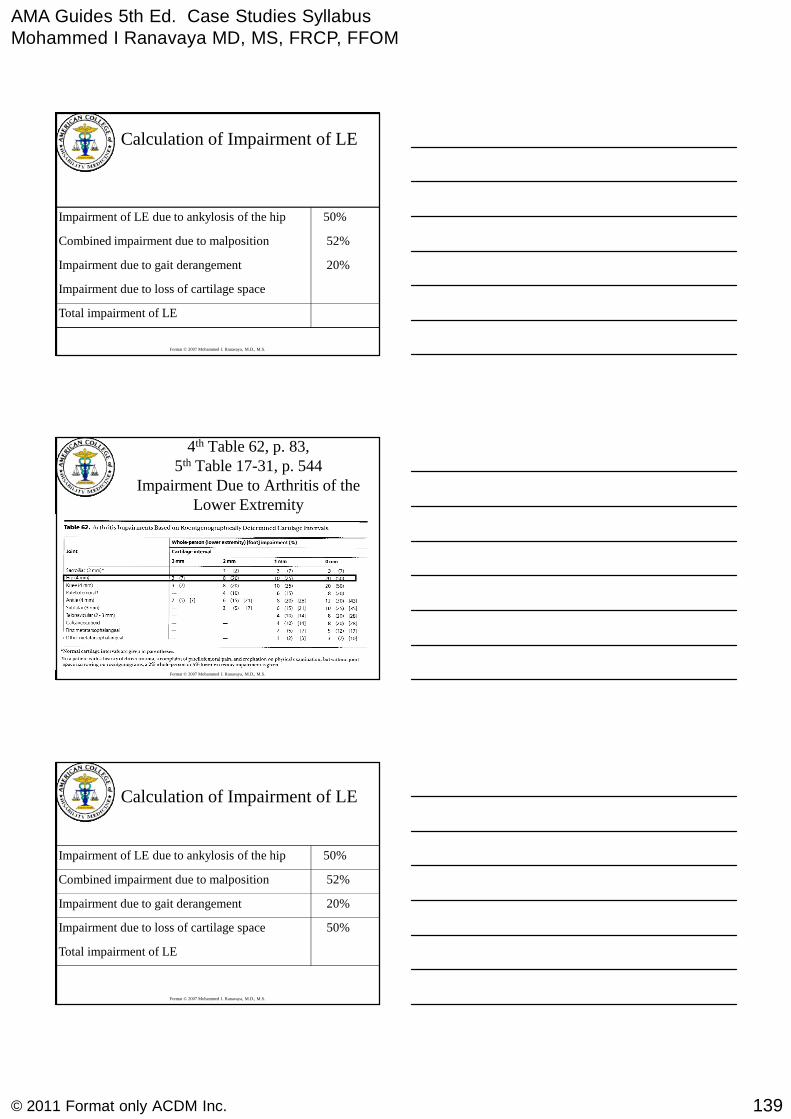
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
139© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment of LE
Impairment due to loss of cartilage space
52%Combined impairment due to malposition
Total impairment of LE
20%Impairment due to gait derangement
50%Impairment of LE due to ankylosis of the hip
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
4th Table 62, p. 83,5th Table 17-31, p. 544
Impairment Due to Arthritis of theLower Extremity
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment of LE
50%Impairment due to loss of cartilage space
52%Combined impairment due to malposition
Total impairment of LE
20%Impairment due to gait derangement
50%Impairment of LE due to ankylosis of the hip
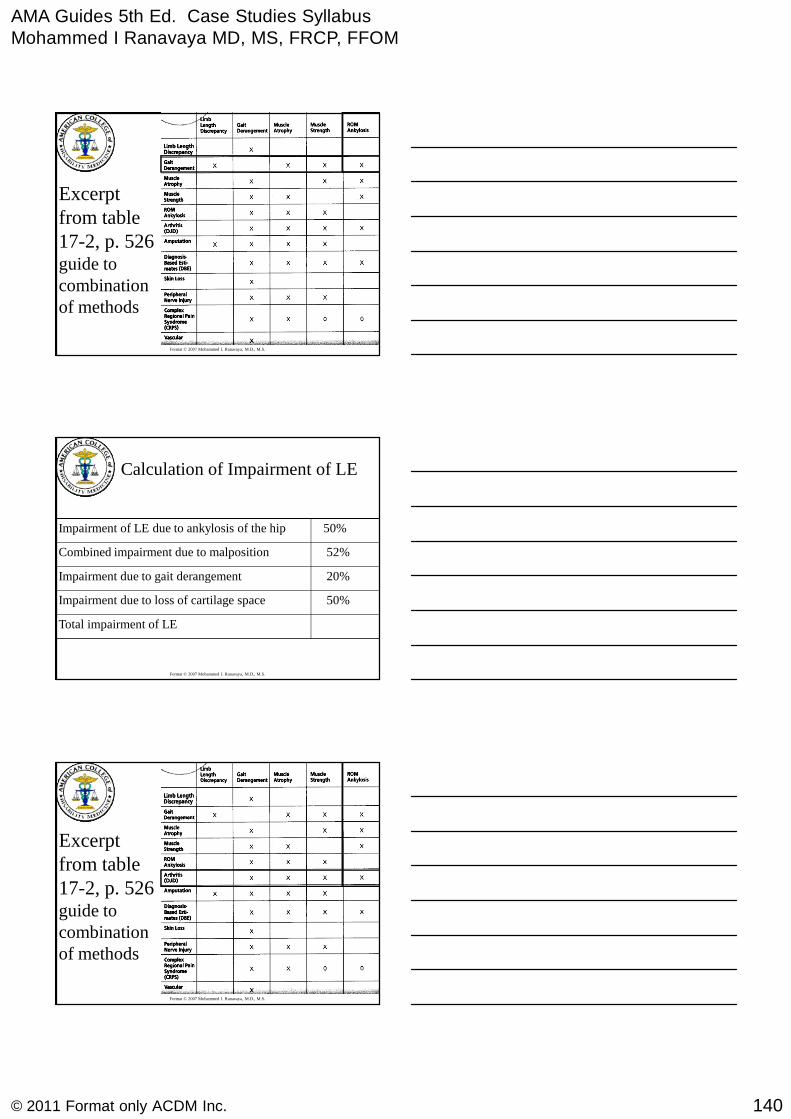
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
140© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Excerptfrom table17-2, p. 526guide tocombinationof methods
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment of LE
50%Impairment due to loss of cartilage space
52%Combined impairment due to malposition
Total impairment of LE
20%Impairment due to gait derangement
50%Impairment of LE due to ankylosis of the hip
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Excerptfrom table17-2, p. 526guide tocombinationof methods
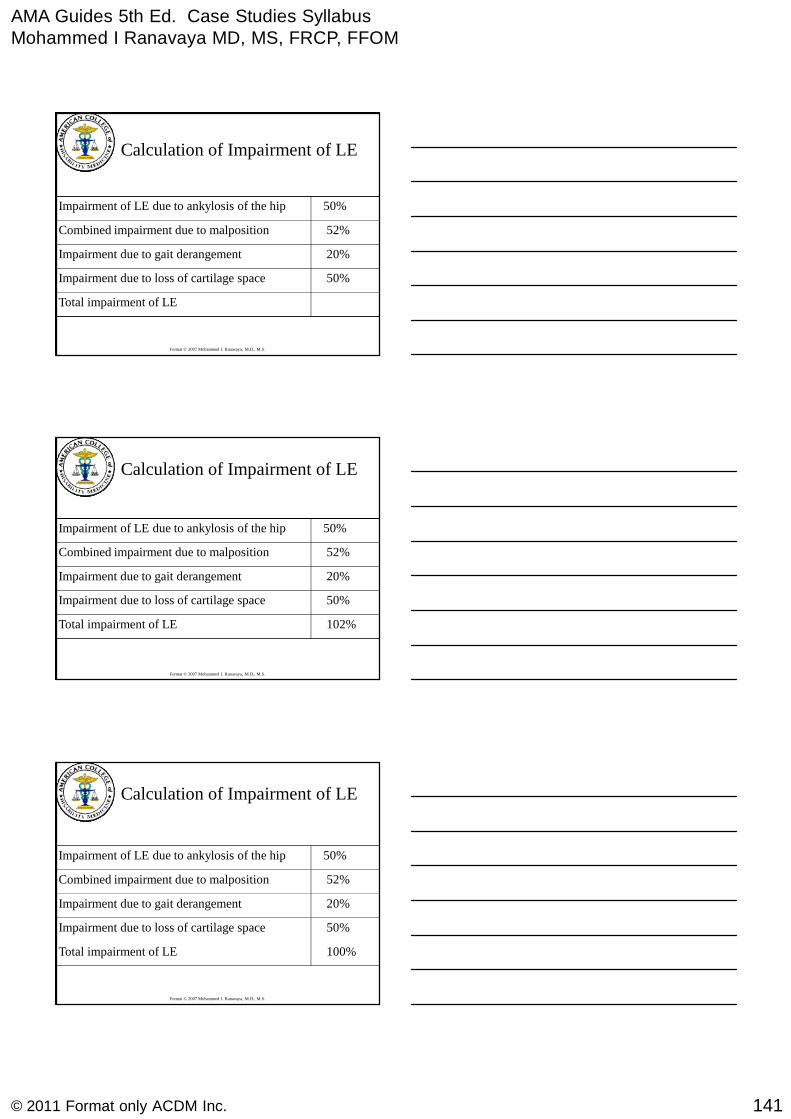
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
141© 2011 Format only ACDM Inc.
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment of LE
50%Impairment due to loss of cartilage space
52%Combined impairment due to malposition
Total impairment of LE
20%Impairment due to gait derangement
50%Impairment of LE due to ankylosis of the hip
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment of LE
50%Impairment due to loss of cartilage space
52%Combined impairment due to malposition
102%Total impairment of LE
20%Impairment due to gait derangement
50%Impairment of LE due to ankylosis of the hip
Format © 2007 Mohammed I. Ranavaya, M.D., M.S.
Calculation of Impairment of LE
50%Impairment due to loss of cartilage space
52%Combined impairment due to malposition
100%Total impairment of LE
20%Impairment due to gait derangement
50%Impairment of LE due to ankylosis of the hip
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
142© 2011 Format only ACDM Inc.
AMA Guides to the Evaluation of PermanentImpairment V
Chapter 13The Central and Peripheral Nervous System
Example 1
• 25 year old male involved in a head-on MVA with LOC.Now MMI
• Moderate difficulty finding his own room at home,difficulty following commands, often gets lost in familiarsurroundings, and lacks interest in home chores orcurrent events. Needs reminders to shower. Not activeout of the house, few friends. Often agitated, impulsive,and frustrated when given new tasks. Falls asleepfrequently when left alone, can’t drive for more than 1hour without excessive tiredness.
• On exam: MMST = 21/30, oriented to name not date orplace
• Normal cranial nerves, motor, sensory exam.
Individual functions associated with aninjury to the nervous system
NervousSystem
HigherCortical
Functions
CranialNerve
Functions
Station, Gaitand
MovementDisorders
ExtremitySpinalCord
Chronic
Pain
Peripheral
Nerve
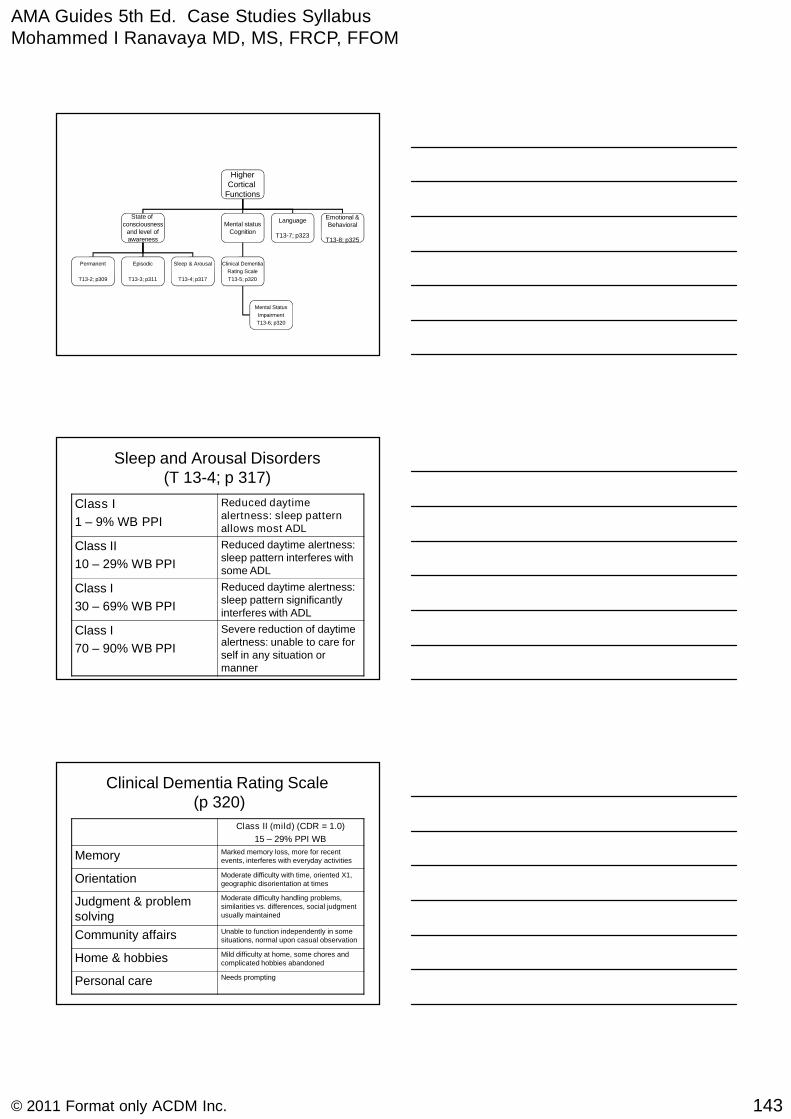
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
143© 2011 Format only ACDM Inc.
HigherCortical
Functions
State ofconsciousness
and level ofawareness
Mental statusCognition
Language
T13-7; p323
Emotional &Behavioral
T13-8; p325
Permanent
T13-2; p309
Episodic
T13-3; p311
Sleep & Arousal
T13-4; p317
Clinical Dementia
Rating Scale
T13-5; p320
Mental Status
Impairment
T13-6; p320
Sleep and Arousal Disorders(T 13-4; p 317)
Class I
1 – 9% WB PPI
Reduced daytimealertness: sleep patternallows most ADL
Class II
10 – 29% WB PPI
Reduced daytime alertness:sleep pattern interferes withsome ADL
Class I
30 – 69% WB PPI
Reduced daytime alertness:sleep pattern significantlyinterferes with ADL
Class I
70 – 90% WB PPI
Severe reduction of daytimealertness: unable to care forself in any situation ormanner
Clinical Dementia Rating Scale(p 320)
Class II (mild) (CDR = 1.0)
15 – 29% PPI WB
Memory Marked memory loss, more for recentevents, interferes with everyday activities
Orientation Moderate difficulty with time, oriented X1,geographic disorientation at times
Judgment & problemsolving
Moderate difficulty handling problems,similarities vs. differences, social judgmentusually maintained
Community affairs Unable to function independently in somesituations, normal upon casual observation
Home & hobbies Mild difficulty at home, some chores andcomplicated hobbies abandoned
Personal care Needs prompting

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
144© 2011 Format only ACDM Inc.
Impairment due to Emotional & BehavioralDisorders (T 13-8; p 325)
Class I
0 -14% PPI WB
Mild limitation of ADL, daily socialand interpersonal functioning
Class II
15 – 29% PPI WB
Moderate limitation of someADL and some social andinterpersonal functioning
Class III
30 – 69% PPI WB
Severe limitation in most ADLimpeding useful function in mostdaily social and interpersonalfunctioning
Class IV
70 – 90% PPI WB
Severe limitation of all ADL,requires total dependence onothers
Calculation
Higher Cortical Functions →
1. State of Consciousness & Level of Awareness• Sleep and Arousal
• Class I impairment = 1 – 9% PPI
2. Mental Status & Cognition– Class II Impairment; 15 – 29% PPI
3. Emotional & Behavior– Class II = 15 – 29% PPI
• Choose the highest impairment due to“higher cortical dysfunction” and combinewith other nervous system impairments(no others)
• 20% PPI WB (15 – 29)
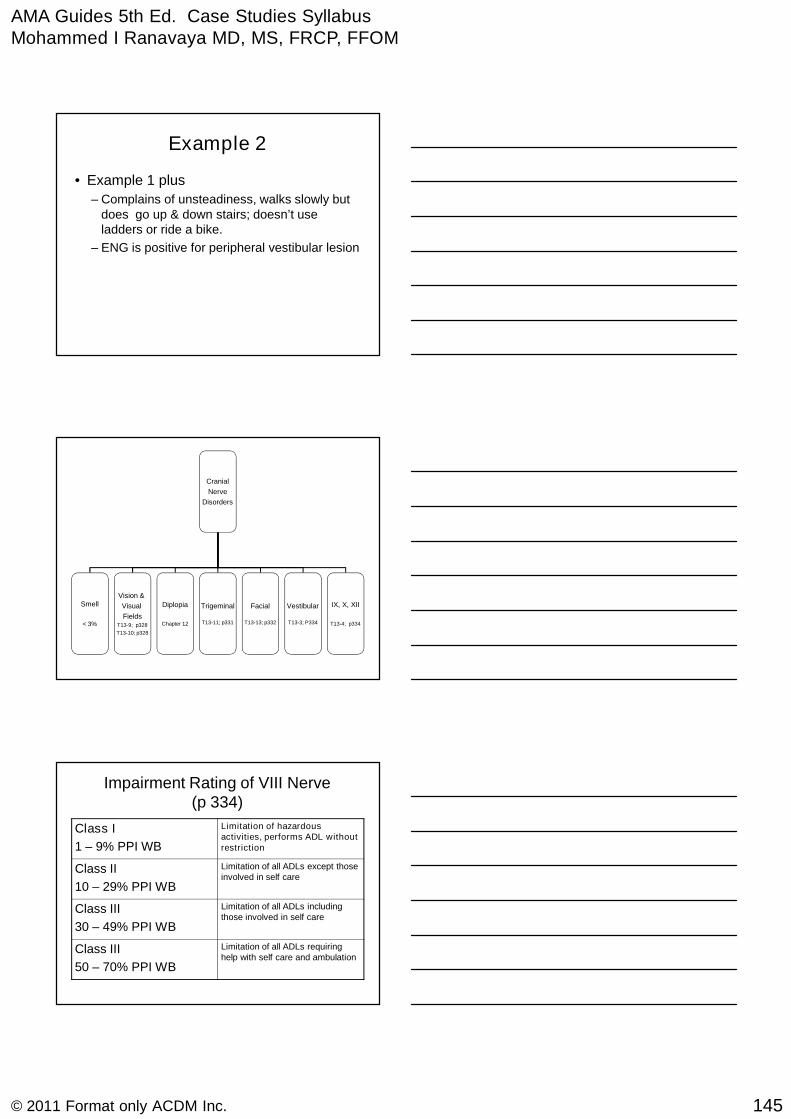
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
145© 2011 Format only ACDM Inc.
Example 2
• Example 1 plus
– Complains of unsteadiness, walks slowly butdoes go up & down stairs; doesn’t useladders or ride a bike.
– ENG is positive for peripheral vestibular lesion
Cranial
Nerve
Disorders
Smell
< 3%
Vision &
Visual
FieldsT13-9; p328
T13-10; p328
Diplopia
Chapter 12
Trigeminal
T13-11; p331
Facial
T13-13; p332
Vestibular
T13-3; P334
IX, X, XII
T13-4; p334
Impairment Rating of VIII Nerve(p 334)
Class I
1 – 9% PPI WB
Limitation of hazardousactivities, performs ADL withoutrestriction
Class II
10 – 29% PPI WB
Limitation of all ADLs except thoseinvolved in self care
Class III
30 – 49% PPI WB
Limitation of all ADLs includingthose involved in self care
Class III
50 – 70% PPI WB
Limitation of all ADLs requiringhelp with self care and ambulation
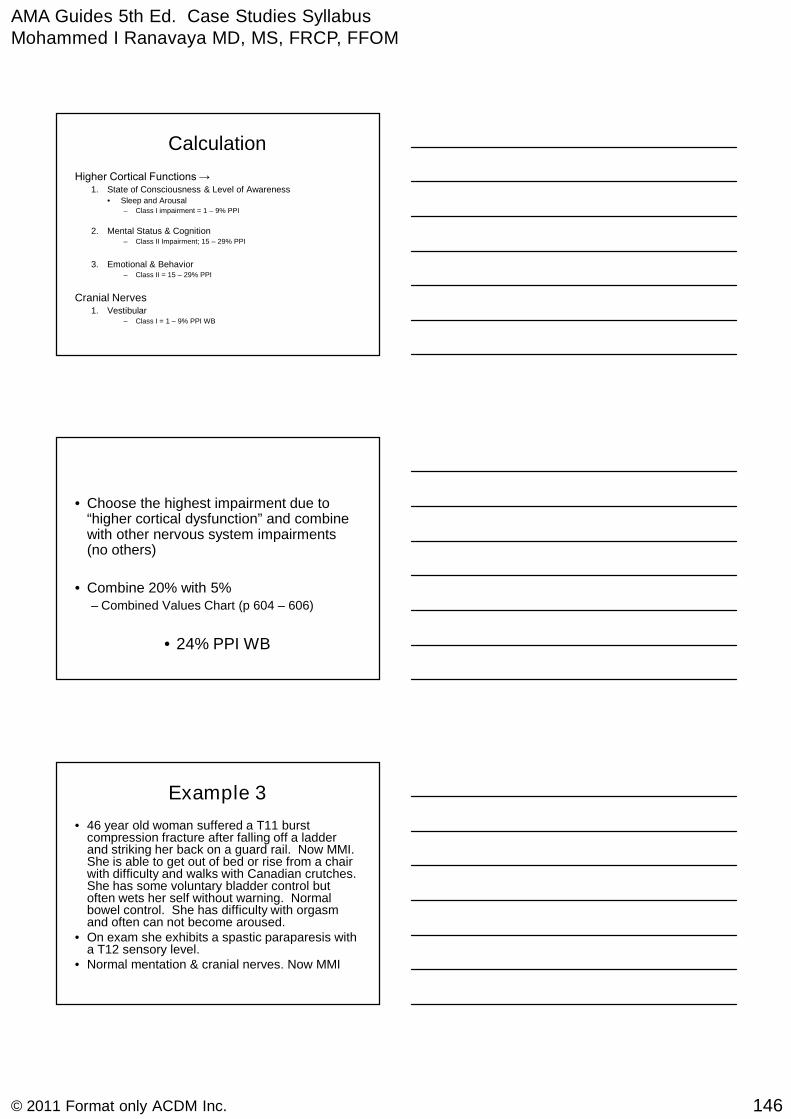
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
146© 2011 Format only ACDM Inc.
Calculation
Higher Cortical Functions →1. State of Consciousness & Level of Awareness
• Sleep and Arousal– Class I impairment = 1 – 9% PPI
2. Mental Status & Cognition– Class II Impairment; 15 – 29% PPI
3. Emotional & Behavior– Class II = 15 – 29% PPI
Cranial Nerves1. Vestibular
– Class I = 1 – 9% PPI WB
• Choose the highest impairment due to“higher cortical dysfunction” and combinewith other nervous system impairments(no others)
• Combine 20% with 5%– Combined Values Chart (p 604 – 606)
• 24% PPI WB
Example 3
• 46 year old woman suffered a T11 burstcompression fracture after falling off a ladderand striking her back on a guard rail. Now MMI.She is able to get out of bed or rise from a chairwith difficulty and walks with Canadian crutches.She has some voluntary bladder control butoften wets her self without warning. Normalbowel control. She has difficulty with orgasmand often can not become aroused.
• On exam she exhibits a spastic paraparesis witha T12 sensory level.
• Normal mentation & cranial nerves. Now MMI
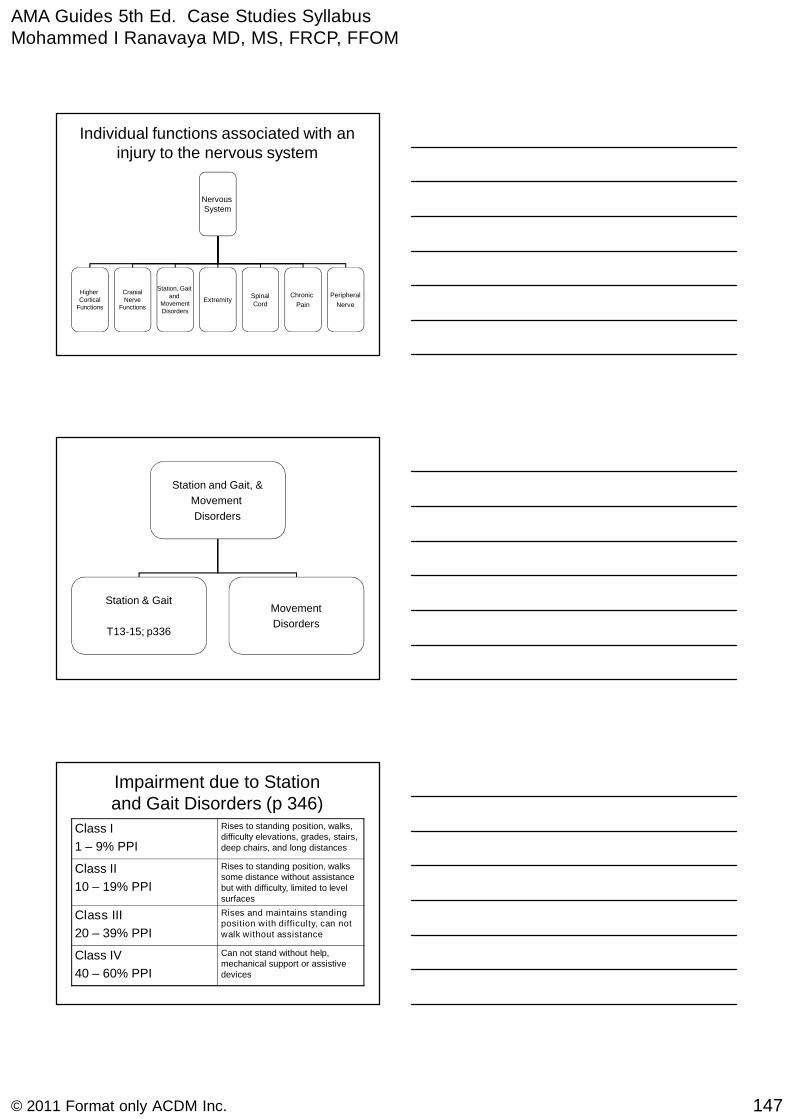
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
147© 2011 Format only ACDM Inc.
Individual functions associated with aninjury to the nervous system
NervousSystem
HigherCortical
Functions
CranialNerve
Functions
Station, Gaitand
MovementDisorders
ExtremitySpinalCord
Chronic
Pain
Peripheral
Nerve
Station and Gait, &
Movement
Disorders
Station & Gait
T13-15; p336
Movement
Disorders
Impairment due to Stationand Gait Disorders (p 346)
Class I
1 – 9% PPI
Rises to standing position, walks,difficulty elevations, grades, stairs,deep chairs, and long distances
Class II
10 – 19% PPI
Rises to standing position, walkssome distance without assistancebut with difficulty, limited to levelsurfaces
Class III
20 – 39% PPI
Rises and maintains standingposition with difficulty, can notwalk without assistance
Class IV
40 – 60% PPI
Can not stand without help,mechanical support or assistivedevices

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
148© 2011 Format only ACDM Inc.
Spinal Cord
Respiration
T13-18; p341
Bladder
T13-19; p341
Anorectal
T13-20; p342
Sexual
T13-21; p342
Neurologic Bladder Impairment(p341)
Class I
1 – 9% PPI
Some degree of voluntary controlwith urgency and frequency
Class II
10 – 24% PPI
Good bladder reflex activity,limited capacity withintermittent emptying withoutvoluntary control
Class III
25 – 39% PPI
Poor bladder reflex control,intermittent dribbling, no voluntarycontrol
Class IV
40 – 60% PPI
No reflex or voluntary bladdercontrol
Neurologic Sexual Impairment(p 342)
Class I
1 – 9% PPI
Sexual functioning is possible withdifficulty with difficulty in erectionor ejaculation in men or lack ofawareness, excitement orlubrication in women
Class II
10 – 19% PPI
Reflex sexual activity withoutawareness
Class III
20% PPI
No sexual functioning
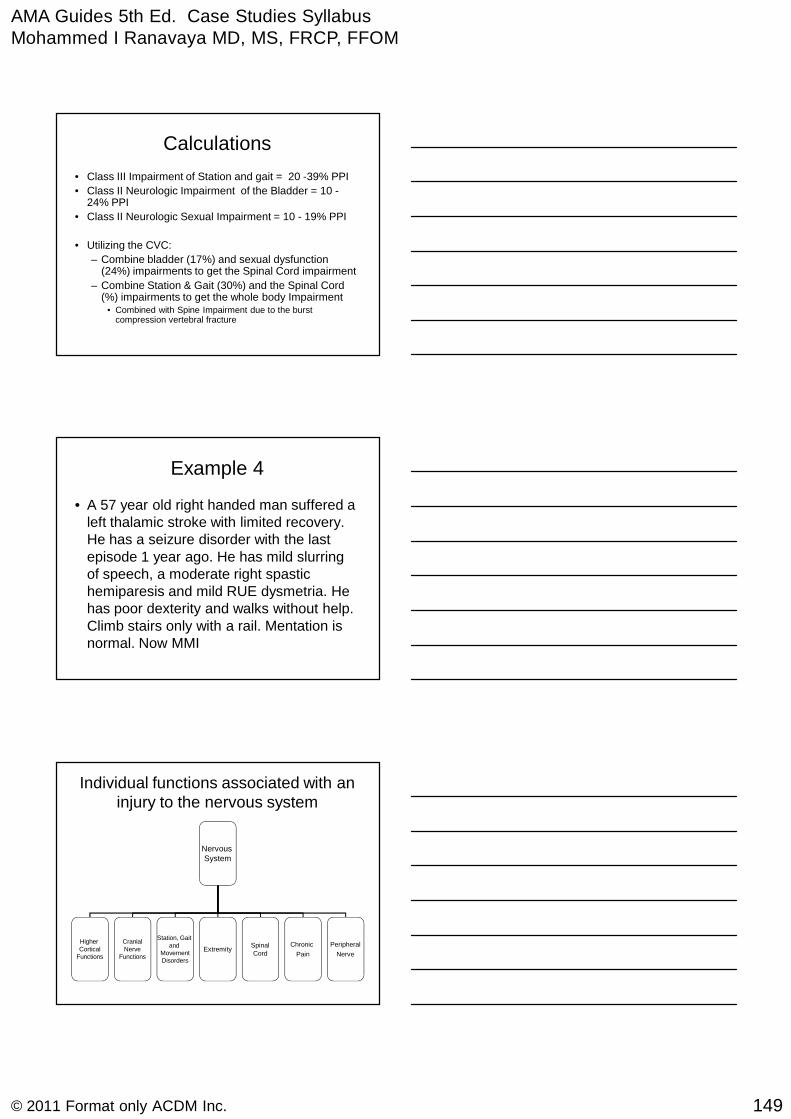
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
149© 2011 Format only ACDM Inc.
Calculations
• Class III Impairment of Station and gait = 20 -39% PPI
• Class II Neurologic Impairment of the Bladder = 10 -24% PPI
• Class II Neurologic Sexual Impairment = 10 - 19% PPI
• Utilizing the CVC:
– Combine bladder (17%) and sexual dysfunction(24%) impairments to get the Spinal Cord impairment
– Combine Station & Gait (30%) and the Spinal Cord(%) impairments to get the whole body Impairment
• Combined with Spine Impairment due to the burstcompression vertebral fracture
Example 4
• A 57 year old right handed man suffered aleft thalamic stroke with limited recovery.He has a seizure disorder with the lastepisode 1 year ago. He has mild slurringof speech, a moderate right spastichemiparesis and mild RUE dysmetria. Hehas poor dexterity and walks without help.Climb stairs only with a rail. Mentation isnormal. Now MMI
Individual functions associated with aninjury to the nervous system
NervousSystem
HigherCortical
Functions
CranialNerve
Functions
Station, Gaitand
MovementDisorders
ExtremitySpinalCord
Chronic
Pain
Peripheral
Nerve

AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
150© 2011 Format only ACDM Inc.
HigherCortical
Functions
State ofconsciousness
and level ofawareness
Mental statusCognition
Language
T13-7; p323
Emotional &Behavioral
T13-8; p325
Permanent
T13-2; p309
Episodic
T13-3; p311
Sleep & Arousal
T13-4; p317
Clinical Dementia
Rating Scale
T13-5; p320
Mental Status
Impairment
T13-6; p320
Impairment due to Episodic Loss ofConsciousness or Awareness
(p 312)
Class I
0 – 14% PPI
Paroxysmal disorderwith predictablecharacteristics butunpredictableoccurrence that doesnot limit usualactivities but is a riskto the individual orlimits daily activities.
Impairment due to Language orDysphasia (p 323)
Class I
0 – 9% PPI
Minimal disturbance ofcomprehension and productionof language symbols of dailyliving.
Class II
10 – 24% PPI
Moderate limitation incomprehension and production oflanguage symbols of daily living.
Class III
25 – 39% PPI
Able to comprehend nonverbalcommunication, expressivespeech in unintelligible for ADL
Class IV
40 – 60% PPI
Completely unable tocommunicate or comprehendlanguage symbols
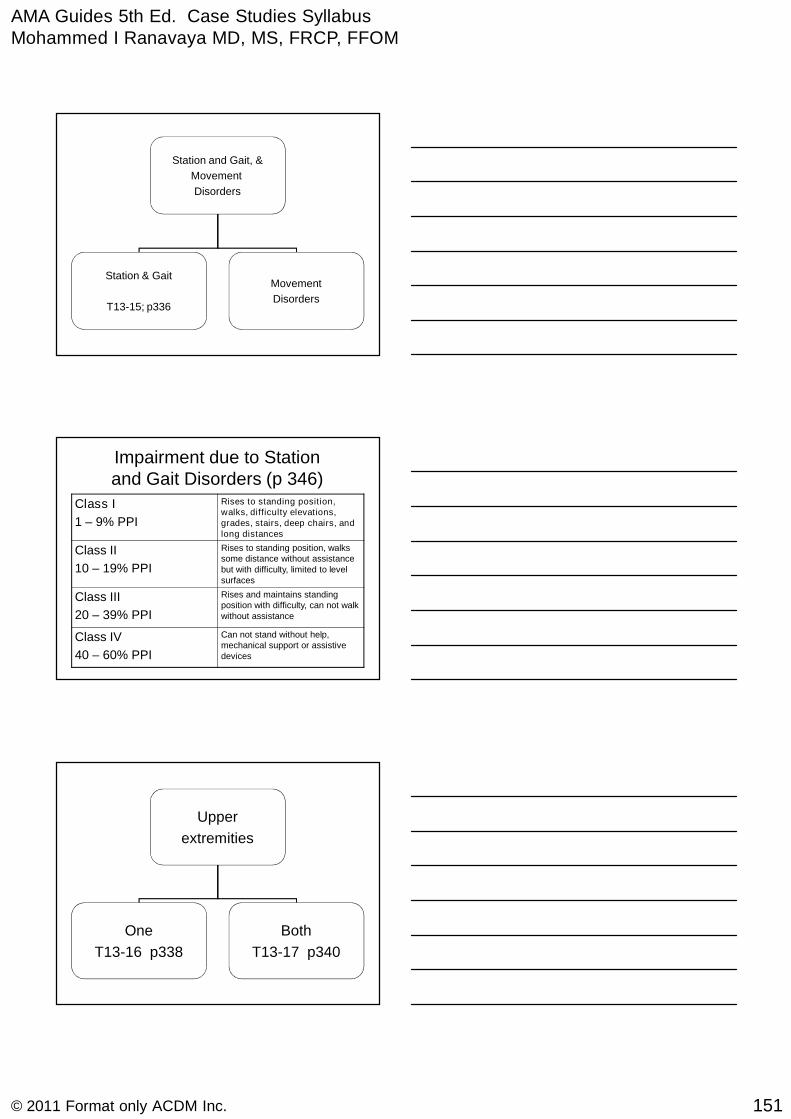
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
151© 2011 Format only ACDM Inc.
Station and Gait, &
Movement
Disorders
Station & Gait
T13-15; p336
Movement
Disorders
Impairment due to Stationand Gait Disorders (p 346)
Class I
1 – 9% PPI
Rises to standing position,walks, difficulty elevations,grades, stairs, deep chairs, andlong distances
Class II
10 – 19% PPI
Rises to standing position, walkssome distance without assistancebut with difficulty, limited to levelsurfaces
Class III
20 – 39% PPI
Rises and maintains standingposition with difficulty, can not walkwithout assistance
Class IV
40 – 60% PPI
Can not stand without help,mechanical support or assistivedevices
Upper
extremities
One
T13-16 p338
Both
T13-17 p340
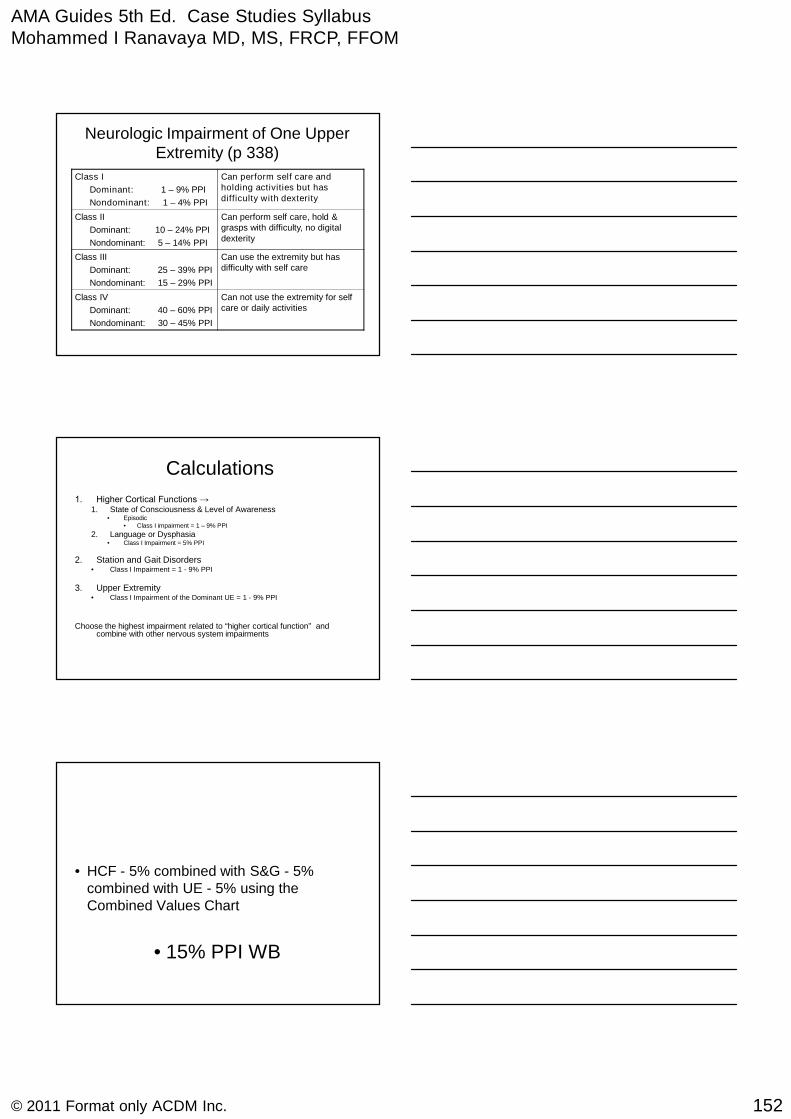
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
152© 2011 Format only ACDM Inc.
Neurologic Impairment of One UpperExtremity (p 338)
Class I
Dominant: 1 – 9% PPI
Nondominant: 1 – 4% PPI
Can perform self care andholding activities but hasdifficulty with dexterity
Class II
Dominant: 10 – 24% PPI
Nondominant: 5 – 14% PPI
Can perform self care, hold &grasps with difficulty, no digitaldexterity
Class III
Dominant: 25 – 39% PPI
Nondominant: 15 – 29% PPI
Can use the extremity but hasdifficulty with self care
Class IV
Dominant: 40 – 60% PPI
Nondominant: 30 – 45% PPI
Can not use the extremity for selfcare or daily activities
Calculations
1. Higher Cortical Functions →1. State of Consciousness & Level of Awareness
• Episodic• Class I impairment = 1 – 9% PPI
2. Language or Dysphasia• Class I Impairment = 5% PPI
2. Station and Gait Disorders• Class I Impairment = 1 - 9% PPI
3. Upper Extremity• Class I Impairment of the Dominant UE = 1 - 9% PPI
Choose the highest impairment related to “higher cortical function” andcombine with other nervous system impairments
• HCF - 5% combined with S&G - 5%combined with UE - 5% using theCombined Values Chart
• 15% PPI WB
AMA Guides 5th Ed. Case Studies SyllabusMohammed I Ranavaya MD, MS, FRCP, FFOM
153© 2011 Format only ACDM Inc.
Summary: 1
Higher
Cortical
FunctionsCranial
Nerves
Station
Gait
Movement
ExtremitySpinal
Cord
Chronic
Pain
Peripheral
Nerve &
Muscle
Nervous
System
Summary 2
• Choose the highest impairment of the“higher cortical functions”
• Combine all other nervous systemimpairments
• Keep the crib sheets ± Guides in the examroom