Case Report Platipnea-Ortodeoxia and PFO · 2018. 3. 21. · J Cardiol Clin Res 6(1): 1129 (2018)...
3
Central Journal of Cardiology & Clinical Research Cite this article: Fasullo S, Maringhini G (2018) Platipnea-Ortodeoxia and PFO Syndrome: Intuition or Praise of the Practice? J Cardiol Clin Res 6(1): 1129. *Corresponding author Sergio Fasullo (MD), Chief of Coronary Coronary Unit “O.Barberi”, Department Cardiology “ Paolo Borsellino”, Corso Calatafimi 1002, 90100 Palermo Italy, Tel: 3387965572; Email: Submitted: 17 February 2018 Accepted: 14 March 2018 Published: 16 March 2018 Copyright © 2018 Fasullo et al. OPEN ACCESS Keywords • Platypnea • Orthodeoxia • O2 orthostatic desaturation • Patent foramen ovale Case Report Platipnea-Ortodeoxia and PFO Syndrome: Intuition or Praise of the Practice? Sergio Fasullo* and Giorgio Maringhini Department of Cardiology, “Paolo Borsellino”, “G.F.Ingrassia” Hospital Palermo, Italy Abstract We present the case of a patient with platypnea-orthodeoxia syndrome (POS) and we discuss its clinical features and its physiopathology. The manifestations of the syndrome are dyspnea and oxygen desaturation that occur in an upright position and that improve in the supine position.In February 2018 a 26-year-old girl presented herself at our department of cardiology, reporting on palpitations and fainting. She also complained about unusual fatigue. Why not think about minor syndromes associated with PFO? After a series of examinations, the diagnostic conclusion of a patent oval foramen (PFO) associated with an interatrial aneurysm was reached. It is believed that the syndrome remains very underdiagnosed, although cases in the literature have been described from the original description of Burtchell and Wood in 1949. INTRODUCTION The most important clue for the diagnosis of POS is the emergence of hypoxia with postural alterations. Several previous cases have shown that the increase in shunt flow through PFO or atrial septal defect (ASD) with changes of posture from supine to straight induces hypoxia. POS is caused by the coexistence of anatomical and functional abnormalities. Anatomical abnormalities include ASD, PFO, or atrial septal aneurysm. Because of the lower sensitivity of TTE for small shunts, the prevalence of PFO observed for TTE of contrast in the general population was lower than that observed by TEE or transcranial ultrasound; this indicates that only the TTE can fail to diagnose ASD or PFO. The POS caused by the PFO can be clearly demonstrated by the contrast technique. CASE PRESENTATION A 26-year-old woman presented herself to our cardiology department, reporting on palpitations and fainting. His clinical history was normal - in particular, there was no history of cardiovascular disease; he also claimed to regularly engage in sports. The patient was admitted to the hospital for diagnostic tests. His vital signs upon arrival were as follows: blood pressure, 90/60 mmHg; heart rate 59 beats / minute; respiratory rate, 18 breaths / minute; and axillary temperature, 36.9 ° C. From a neurological point of view, she was attentive, time-oriented [1,2]. Blood tests revealed microcitosis (hemoglobin = 13.8 g / dL, mean corpuscular volume = 63 fL, mean corpuscular hemoglobin = 20.8 pg), a common condition. No alterations in the coagulation / coagulation profile were found. No electrocardiographic changes were detected. A transthoracic echocardiogram (TTE) revealed an interatrial aneurysm but the flow derived through the PFO on the Doppler color image was apparently not observed (Figure 1). Given the suspicion of a foramen ovale, the patient was subjected to transcranial ultrasound (Figure 2). The right middle cerebral artery is visualized, which after the injection into a peripheral vein of physiological solution and Valsalva maneuver, shows the passage of microbubbles in a significant number indicative of PFO. The diagnosis is often delayed, so the clinical suspicion is important. Considering these results, we concluded that the cause of hypoxia was POS with right-to-left interatrial shunting across the PFO. POS can be treated by closing the interatrial shunt
Transcript of Case Report Platipnea-Ortodeoxia and PFO · 2018. 3. 21. · J Cardiol Clin Res 6(1): 1129 (2018)...

CentralBringing Excellence in Open Access
Journal of Cardiology & Clinical Research
Cite this article: Fasullo S, Maringhini G (2018) Platipnea-Ortodeoxia and PFO Syndrome: Intuition or Praise of the Practice? J Cardiol Clin Res 6(1): 1129.
*Corresponding author
Sergio Fasullo (MD), Chief of Coronary Coronary Unit “O.Barberi”, Department Cardiology “ Paolo Borsellino”, Corso Calatafimi 1002, 90100 Palermo Italy, Tel: 3387965572; Email:
Submitted: 17 February 2018
Accepted: 14 March 2018
Published: 16 March 2018
Copyright© 2018 Fasullo et al.
OPEN ACCESS
Keywords• Platypnea• Orthodeoxia• O2 orthostatic desaturation• Patent foramen ovale
Case Report
Platipnea-Ortodeoxia and PFO Syndrome: Intuition or Praise of the Practice?Sergio Fasullo* and Giorgio MaringhiniDepartment of Cardiology, “Paolo Borsellino”, “G.F.Ingrassia” Hospital Palermo, Italy
Abstract
We present the case of a patient with platypnea-orthodeoxia syndrome (POS) and we discuss its clinical features and its physiopathology. The manifestations of the syndrome are dyspnea and oxygen desaturation that occur in an upright position and that improve in the supine position.In February 2018 a 26-year-old girl presented herself at our department of cardiology, reporting on palpitations and fainting. She also complained about unusual fatigue. Why not think about minor syndromes associated with PFO? After a series of examinations, the diagnostic conclusion of a patent oval foramen (PFO) associated with an interatrial aneurysm was reached.
It is believed that the syndrome remains very underdiagnosed, although cases in the literature have been described from the original description of Burtchell and Wood in 1949.
INTRODUCTIONThe most important clue for the diagnosis of POS is the
emergence of hypoxia with postural alterations. Several previous cases have shown that the increase in shunt flow through PFO or atrial septal defect (ASD) with changes of posture from supine to straight induces hypoxia.
POS is caused by the coexistence of anatomical and functional abnormalities. Anatomical abnormalities include ASD, PFO, or atrial septal aneurysm.
Because of the lower sensitivity of TTE for small shunts, the prevalence of PFO observed for TTE of contrast in the general population was lower than that observed by TEE or transcranial ultrasound; this indicates that only the TTE can fail to diagnose ASD or PFO. The POS caused by the PFO can be clearly demonstrated by the contrast technique.
CASE PRESENTATIONA 26-year-old woman presented herself to our cardiology
department, reporting on palpitations and fainting. His clinical history was normal - in particular, there was no history of cardiovascular disease; he also claimed to regularly engage in sports. The patient was admitted to the hospital for diagnostic tests.
His vital signs upon arrival were as follows: blood pressure, 90/60 mmHg; heart rate 59 beats / minute; respiratory rate, 18 breaths / minute; and axillary temperature, 36.9 ° C. From a neurological point of view, she was attentive, time-oriented [1,2].
Blood tests revealed microcitosis (hemoglobin = 13.8 g / dL, mean corpuscular volume = 63 fL, mean corpuscular hemoglobin = 20.8 pg), a common condition. No alterations in the coagulation / coagulation profile were found. No electrocardiographic changes were detected.
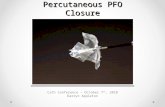
A transthoracic echocardiogram (TTE) revealed an interatrial aneurysm but the flow derived through the PFO on the Doppler color image was apparently not observed (Figure 1).
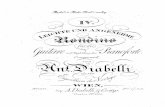
Given the suspicion of a foramen ovale, the patient was subjected to transcranial ultrasound (Figure 2). The right middle cerebral artery is visualized, which after the injection into a peripheral vein of physiological solution and Valsalva maneuver, shows the passage of microbubbles in a significant number indicative of PFO.
The diagnosis is often delayed, so the clinical suspicion is important.
Considering these results, we concluded that the cause of hypoxia was POS with right-to-left interatrial shunting across the PFO. POS can be treated by closing the interatrial shunt

CentralBringing Excellence in Open Access
Fasullo et al. (2018)Email:
2/3J Cardiol Clin Res 6(1): 1129 (2018)
by thoracotomy or percutaneous cardiac catheterization. The closure of the PFO has not been performed due to failure to obtain informed consent. For these reasons she was discharged after receiving a medical opinion on her posture. The patient was discharged with aspirin [3,4].
DISCUSSIONThis case showed a PFO associated with an aneurysmatic
interatrial septum.The PFO is a common finding in the general population and may be completely asymptomatic. Nonetheless; PFO has been associated with an increased risk of cryptogenic ischemic stroke and even more in cases of association with atrial septal aneurysm.
The mean percentage of cryptogenic strokes among ischemic strokes is 31%, of which one-third may be associated with patent foramen ovale. The foramen ovale is required for blood flow through the fetal atrial septum. In 75% of cases, its closure is complete by 2 years of age, but it may persist in 25% of patients.
There after careful clinical and instrumental evaluation a platypnea-orthodeoxia syndrome has been diagnosed.
Platypnea-orthodeoxia syndrome (POS) is an uncommon disorder characterized by dyspnea (=platypnea) and desaturation
(=orthodeoxia) in upright position and improvement of symptoms and blood oxygenation in supine position. Clinical presentation is heterogeneous and often confuses the clinician.
It is characterized by a significant reduction of the arterial oxygen saturation in the transition from the supine position to the orthostatic position. It would be ‘precipitated’ by a reduction of the systemic arterial pressure in an upright position thus increasing the right-left shunt.In these conditions, in fact, the increase of the right-left pressure gradient resulting in an upright position leads to an increase in the deoxygenated venous blood flow between the right and left chambers and therefore the finding of a greater oximetry desaturation in orthostatism.
Once Platipnea-Ortodeoxia syndrome is diagnosed in agreement with other authors, both an anatomical and functional cause must be sought.
Additional tests will demonstrate the existence of a patent foramen ovale. This diagnosis was suitable with the patient’s syndrome and was eligible for percutaneous closure procedure allowing immediate resolution of symptoms and confirming the diagnosis.
The anatomical defect consists almost exclusively in the patency of the oval foramen or in a misrecognized interatrial defect
Figure 1 A transthoracic echocardiogram (TTE) revealed an interatrial aneurysm but the flow shunted through the PFO on the Doppler color image was apparently not observed.
Figure 2 The right middle cerebral artery is visualized, which after injection into a peripheral vein of physiological solution and Valsalva maneuver, shows the passage of microbubbles in a significant number indicative of PFO.

CentralBringing Excellence in Open Access
Fasullo et al. (2018)Email:
3/3J Cardiol Clin Res 6(1): 1129 (2018)
Fasullo S, Maringhini G (2018) Platipnea-Ortodeoxia and PFO Syndrome: Intuition or Praise of the Practice? J Cardiol Clin Res 6(1): 1129.
Cite this article
while the functional defect may be due or those that determine a preferential blood flow through interatrial communication (ex: aneurysm of the inter-atrial septum) or those causing a transient increase in pressure in the right atrium with an increase in the left right atrial gradient (ex: chronic obstructive pulmonary disease).
In the case that we described at the end we have diagnosed a misunderstood wide patency of the foramen ovale or a true interatrial aneurysm .
In fact, the aneurysm of the interatrial septum can in itself facilitate the movement of the hinge valve of the oval fossa, being able to become more horizontally in an orthostatic position, thus favoring the deoxygenated blood flow coming from the inferior vena cava.
It is recalled that the patency of the oval foramen is not a rare condition; in fact it has a prevalence of 20-35% in autopsy studies and 9.2% in patients who undergo a transesophageal echocardiography.
The correction of the patency of the oval foramen is curative for the syndrome platipnea-orthodoxy, but there are still conflicting data [5,6].
Although the syndrome still remains undiagnosed, it will be increasingly recognized for the use of the echocardiographic method not only transthoracic but above all transesophagous and transcranial echo. Furthermore, there is an increasing awareness of the existence of the syndrome and of the healing correction if diagnosed in time.
CONCLUSIONSPlatypnea-orthodeoxia syndrome is rare and difficult
to diagnose. The present case suggests that hypoxia due to postural changes should be considered a differential diagnosis of platypnea-orthodeoxia syndrome.
The abnormal shunt in a vertical position can be the result of different basic conditions, which require an accurate workup and a tailor-made treatment.
Why not think of minor syndromes associated with PFO? After a series of tests, the diagnostic conclusion of a patented oval foramen (PFO) associated with an interatrial aneurysm was achieved.
Medical therapy with asprin (and postural advice), a valid alternative not decisive in the management of young patients.
The percutaneous correction of patency of the oval foramen is curative for the platipnea-orthodoxy syndrome.
REFERENCES1. Campbell EJM, Howell JBL. The sensation of breathlessness. Br Med
Bull. 1963; 19: 36-40.
2. Cheng TO. Platypnea-orthodeoxia and blockpnea as two unrecognized or underdiagnosed causes of medically unexplained dyspnea. Chin Med J. 2004; 117: 1116.
3. Tsuzuki I, Iigaya K, Matsubara T, Takagi S, Inohara T, Ohgino Y, et al. Platypnea-orthodeoxia syndrome in the right lateral decubitus position: a case report. J Med Case Rep. 2017; 11: 109.
4. Chen GP, Goldberg SL, Gill EA Jr. Patent foramen ovale and the platypnea-orthodeoxia syndrome. Cardiol Clin. 2005; 23: 85–89.
5. Rao PS, Palacios IF, Bach RG, Bitar SR, Sideris EB. Platypnea-orthodeoxia: management by transcatheter buttoned device implantation. Catheter Cardio Catheter Cardiovasc Inter. 2001; 54: 77–82.
6. Fisher DC, Fisher EA, Budd JH, Rosen SE, Goldman M. The incidence of patent foramen ovale in 1,000 consecutive patients. A contrast transesophageal echocardiography study. Chest 1995; 107: 1504– 1509.