Case report of metastatic colon adenocarcinoma with ... · Garvie S (218) Case report of metastatic...
2
Case Report Clinical and Medical Reports Clin Med Rep, 2018 doi: 10.15761/CMR.1000126 Volume 1(5): 1-2 ISSN: 2516-5283 Case report of metastatic colon adenocarcinoma with laryngeal deposits Stella Garvie 1 *, Polycarp Gana 1 and Jamal Uraiby 2 1 Kettering General Hospital Foundation Trust; Ear, Nose & Throat Department; Kettering; NN16 8UZ, UK 2 Kettering General Hospital Foundation Trust; Department of Cellular Pathology; Kettering; NN16 8UZ, UK Abstract e larynx is known to be a very rare site for metastases of tumours of various regions due to its terminal position in the lymphatic circulation system. e last case of a massive transglottic deposit of the larynx with associated classical symptoms was described in 1997. Our case describes a unique clinical history of a laryngeal metastasis of colon adenocarcinoma without typical physical presentation but mimicking Paget’s disease. Due to its scarce appearance in clinical practice and medical literature, laryngeal metastasis of cancer can be an immense diagnostic challenge. e aforementioned case is a great contribution to the understanding and management of such patients. *Correspondence to: Stella Garvie, MBBS, Kettering General Hospital Foundation Trust; Ear, Nose & roat Department; Kettering; NN16 8UZ; UK, Tel: +44 7930078513; E-mail: [email protected] Key words: Adenocarcinoma, cricoid, laryngeal, laryngoscopy, metastases, sclerosis Received: June 15, 2018; Accepted: June 25, 2018; Published: June 27, 2018 Introduction Metastases to the larynx are generally rare in clinical practice [1- 3]. e explanation of that is based on the terminal location of this organ in the lymphatic-vascular circulation. Among the laryngeal metastases that are described in literature, the most common sources of malignancy are melanomas and renal carcinomas, leaving Gastrointestinal tract, lung and breast cancer rather sporadic primary sources. In this background metastases of colon carcinoma to the larynx seem almost overly subtle [4]. is makes any clinical case of laryngeal secondary deposits from a primary colon tumour a very valuable clinical and educational finding. In this article we report a case of laryngeal metastases of colorectal adenocarcinoma with atypical presentation that posed a diagnostic dilemma. Clinical case A 71-year old patient with known history of colorectal carcinoma with lung metastases was admitted to the hospital because of respiratory distress. By then he had already received 29 cycles of chemotherapy and was due to undergo the 30 th one. Prior to admission he experienced a long-term shortness of breath with wheeze and productive cough which seemed not to improve aſter antibiotic therapy. He subsequently developed respiratory failure from an upper airway obstruction, intubation was attempted with multiple failures, so an urgent tracheostomy was conducted under local anaesthetic. Flexible naso - endoscopy showed significant narrowing of the subglottic airway, otherwise, examination of ear, nose and throat was unremarkable. CT and MRI scans of the neck were performed which showed an infra-glottic stenosis but no mass in the upper aero digestive tract or cervical lymphadenopathy. However, there was evidence of cricoid cartilage thickening, but the radiologist did not associate this finding with any possibility of malignant change (Figures 1 and 2). e laryngeal airway although narrowed, was still adequate with no mucosal breaches but only thickening of the laryngeal structures and congested post-cricoid and subglottic areas. e case was discussed at the Head and Neck Multi-Disciplinary Team meeting and the official MDT comment and diagnosis was “extensive sclerosis of cricoid” consistent with Paget’s disease. Direct laryngoscopy was performed, and biopsy of the subglottic area was taken on insistence of the oncologist for histology. Unfortunately, the patient was deceased before the histopathology report. Histopathological report Most of the sample consisted of fragments of respiratory type mucosa showing non-specific chronic inflammation. However, one fragment showed surface ulceration and contained occasional disrupted glands lined by dysplastic epithelium with associated Figure 1. CT scan of the neck of the patient with respiratory distress
Transcript of Case report of metastatic colon adenocarcinoma with ... · Garvie S (218) Case report of metastatic...

Case Report
Clinical and Medical Reports
Clin Med Rep, 2018 doi: 10.15761/CMR.1000126 Volume 1(5): 1-2
ISSN: 2516-5283
Case report of metastatic colon adenocarcinoma with laryngeal depositsStella Garvie1*, Polycarp Gana1 and Jamal Uraiby2
1Kettering General Hospital Foundation Trust; Ear, Nose & Throat Department; Kettering; NN16 8UZ, UK2Kettering General Hospital Foundation Trust; Department of Cellular Pathology; Kettering; NN16 8UZ, UK
AbstractThe larynx is known to be a very rare site for metastases of tumours of various regions due to its terminal position in the lymphatic circulation system. The last case of a massive transglottic deposit of the larynx with associated classical symptoms was described in 1997. Our case describes a unique clinical history of a laryngeal metastasis of colon adenocarcinoma without typical physical presentation but mimicking Paget’s disease.
Due to its scarce appearance in clinical practice and medical literature, laryngeal metastasis of cancer can be an immense diagnostic challenge. The aforementioned case is a great contribution to the understanding and management of such patients.
*Correspondence to: Stella Garvie, MBBS, Kettering General Hospital Foundation Trust; Ear, Nose & Throat Department; Kettering; NN16 8UZ; UK, Tel: +44 7930078513; E-mail: [email protected]
Key words: Adenocarcinoma, cricoid, laryngeal, laryngoscopy, metastases, sclerosis
Received: June 15, 2018; Accepted: June 25, 2018; Published: June 27, 2018
IntroductionMetastases to the larynx are generally rare in clinical practice [1-
3]. The explanation of that is based on the terminal location of this organ in the lymphatic-vascular circulation. Among the laryngeal metastases that are described in literature, the most common sources of malignancy are melanomas and renal carcinomas, leaving Gastrointestinal tract, lung and breast cancer rather sporadic primary sources. In this background metastases of colon carcinoma to the larynx seem almost overly subtle [4]. This makes any clinical case of laryngeal secondary deposits from a primary colon tumour a very valuable clinical and educational finding. In this article we report a case of laryngeal metastases of colorectal adenocarcinoma with atypical presentation that posed a diagnostic dilemma.
Clinical caseA 71-year old patient with known history of colorectal carcinoma
with lung metastases was admitted to the hospital because of respiratory distress. By then he had already received 29 cycles of chemotherapy and was due to undergo the 30th one. Prior to admission he experienced a long-term shortness of breath with wheeze and productive cough which seemed not to improve after antibiotic therapy. He subsequently developed respiratory failure from an upper airway obstruction, intubation was attempted with multiple failures, so an urgent tracheostomy was conducted under local anaesthetic.
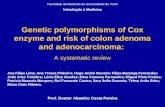
Flexible naso - endoscopy showed significant narrowing of the subglottic airway, otherwise, examination of ear, nose and throat was unremarkable. CT and MRI scans of the neck were performed which showed an infra-glottic stenosis but no mass in the upper aero digestive tract or cervical lymphadenopathy. However, there was evidence of cricoid cartilage thickening, but the radiologist did not associate this finding with any possibility of malignant change (Figures 1 and 2). The laryngeal airway although narrowed, was still adequate with no mucosal breaches but only thickening of the laryngeal structures and congested post-cricoid and subglottic areas.
The case was discussed at the Head and Neck Multi-Disciplinary Team meeting and the official MDT comment and diagnosis was “extensive sclerosis of cricoid” consistent with Paget’s disease. Direct laryngoscopy was performed, and biopsy of the subglottic area was taken on insistence of the oncologist for histology. Unfortunately, the patient was deceased before the histopathology report.
Histopathological reportMost of the sample consisted of fragments of respiratory type
mucosa showing non-specific chronic inflammation. However, one fragment showed surface ulceration and contained occasional disrupted glands lined by dysplastic epithelium with associated
Figure 1. CT scan of the neck of the patient with respiratory distress

Garvie S (2018) Case report of metastatic colon adenocarcinoma with laryngeal deposits
Volume 1(5): 2-2Clin Med Rep, 2018 doi: 10.15761/CMR.1000126
necrosis. Small fragments of squamous epithelium were also present. Immunohistochemistry confirmed dysplastic glandular epithelium that was CDX2 positive, CK positive, CEA positive, CK negative, P63 negative and TTF-1 negative. This immuno-stain profile was in keeping with colorectal epithelial origin and consistent with metastatic colorectal carcinoma.
DiscussionMajority of the tumours that metastasise to the larynx are
either melanomas (29%) or carcinomas, especially renal (25%), gastrointestinal (14%), lung (9%), breast (8%), and prostate (5%) but the overall incidence of secondary neoplasms of the larynx is rare accounting for 0.09 to 0.4% [5]. Adenocarcinoma deposits in laryngeal area are barely known [3]. Its frequency increases with age (median 58 years, range 24–83 years) and it tends to occur more commonly in males by a ratio of 2:1 [1,2].
The signs and symptoms are similar to those produced by primary laryngeal tumours, but the severity of presentation is dependent on the location of the tumour deposit. In our case the lesion was mostly within the cricoid cartilage with sclerotic expansion of the cartilage and consequent narrowing of the subglottis which triggered respiratory distress. The prognosis is generally poor as the condition is often associated with terminal widespread disseminated disease.
Our case describes a rare case of laryngeal metastasis of colon adenocarcinoma. A similar case was last described in 1997 by Puxeddu
and others who reported a case of colon adenocarcinoma with massive transglottic tumour metastasis obstructing the airway [5]. However, the uniqueness of our case is the vagueness of both endoscopic examination and radiological findings that are inconsistent with malignancy. A lack of classical changes of the larynx typical of malignant conditions was problematic in this case in arriving at a diagnosis but the possibility of metastasis as well as primary non-squamous neoplasms which are typically submucosal should be comtemplated. It can be only assumed how many underdiagnosed patients with laryngeal cartilages thickening on radiological report could have been diagnosed with secondary laryngeal neoplasms and possibly treated with a different approach. Thus, it is vitally important to be aware of rare locations for metastasis within the larynx and insisting on multiple site tissue biopsies for a diagnosis.
Conclusion• Laryngeal metastases are rare in general due to the anatomy of
lymphocirculatory system of larynx and are especially uncommon for cancer originating from colon.
• The presented case describes a unique clinical picture with a laryngeal metastasis mimicking extensive cricoid sclerosis. Such presentation has never been described before.
• Metastasis to the larynx and some nonsquamous primary neoplasms are typically subepithelial.
• Late recognition of atypical presentation of laryngeal metastases can negatively affect patient’s prognosis.
AcknowledgementsNone
Conflict of interestsNone
References1. Batsakis J, Luna M, Byers R (1985) Metastases to the larynx. Head & Neck Surgery
7: 458-460.
2. Foote R (1995) Neoplasms of the Larynx. Head & Neck 17: 367-368.
3. Weir N (2010) THE LARYNX. The journal of Laryngology & Otology 125: 109.
4. Ferlito A, Caruso G, Recher G (1988) Secondary Laryngeal Tumors: Report of Seven Cases with Review of the Literature. Archives of Otolaryngology - Head and Neck Surgery 114: 635-639.
5. Puxeddu R, Pelagatti CL, Ambu R (1997) Colon adenocarcinoma metastatic to the larynx. Eur Arch Otorhinolaryngol 254: 353-355.
Figure 2. Specimen with metastatic colorectal carcinoma. Staining P63, CK20, H&E and CDX2
Copyright: ©2018 Garvie S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.