
Case Report Intra-Articular Calsified Synovial...
3
Case Report Intra-Articular Calsified Synovial Sarcoma Of Knee – A Case Report Of An Imitating Pathology Pankaj Kumar Mishra¹, Vishal Yadav¹, Deepak Singh Maravi¹, Sanjeev Gaur¹ Introduction: Although the association of calcification/ossification with the synovial sarcoma is an uncommon finding, Here we are presenting a rare case of the intra-articular synovial sarcoma of the knee with calcification as a perusal of rare entity, showing that the intra-articular calcification may also be the presentation of the synovial sarcoma. Case Report: It is a case presentation of 35 years old female, who presented to us with a knee lump at the postero-lateral aspect of her left knee. MRI finding speculated the differential diagnosis of synovial sarcoma, soft tissue sarcoma and peripheral nerve sheath tumor. The fine needle aspiration cytology of the swelling sent for the clinical correlation, and it showed the benign cytology. Excision of the tumor done with the, safety margin. After the 12 months of the postoperative follow-up, the patient again visited to the hospital with the same complaint. Resurgery done for the tumor and it got excised with the safety margin as we could achieve again. Now the histology of the tumor was characteristically of monophasic pattern of synovial cell sarcoma. Conclusion: Here we are acknowledging this case as an experience of the calcified intra-articular synovial sarcoma and want to add the note that, the calcified lesion within the joint may be mistaken as a benign pathology by the orthopedist if he/she is unwary to the imitating presentation of the synovial sarcoma. Keywords: Intra-Articular Synovial Sarcoma, Knee, Calcification. International Journal of Surgical Cases 2015 Oct-Dec: 1(2):Page 11-13 Abstract 1 Department Of Orthopaedics, G.M.C And Hamidia Hospital Bhopal. M.P. India.. Address of Correspondence Pankaj Kumar Mishra Assistant Professor (Department Of Orthopaedics) G.M.C And Hamidia Hospital Bhopal. M.P. India. E-mail- [email protected] Copyright © 2015 by International Journal of Surgical Cases International Journal of Surgical Cases | eISSN 2321-3817 | Available on www.surgicalcasesjournal.com/ | This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. 11 Author’s Photo Gallery Dr. Pankaj K Mishra Dr. Vishal Yadav Dr. Deepak S M aravi Dr. Sanjeev Gaur Introduction Synovial sarcoma (also known as malignant synovioma) depicts up to the 8 % of the all the soft tissue sarcomas. The pinnacle of incidence is between the adolescents and young age groups, before the 30th birth day. Among the population, male and female ration of distribution is 1.2:1 [1]. Although the association of calcification/ossification with the synovial sarcoma is an uncommon finding, and there are very few cases mentioned in the literature [2, 3]. Here we are presenting a rare case of the intra-articular synovial sarcoma of the knee with calcification as a perusal of rare entity, showing that the intra-articular calcification may also be the presentation of the synovial sarcoma. Case Report It is a case presentation of 35 years old female, who presented to us (in 2007) with a knee lump at the postero-lateral aspect of her left knee. She noticed it 5 months back and since then the swelling had been growing slowly and in the last 2 months, it was more noticeable. The patient complained to us, for this disfiguring swelling and the mild vague pain. On clinical examination the swelling seemed benign in nature (Fig 1). X-ray of the knee sought and the clinico-radiological differential diagnosis of, synovial chondromatosis, paraosteal osteosarcoma and fractured intra-articular osteochondroma conceded [Fig 2]. The magnetic resonance imaging (MRI) of knee showed the multi-loculated mass in popliteal fossa. It had iso to hypointesce Access this article online Website: www.surgicalcasesjournal.com DOI:
Transcript of Case Report Intra-Articular Calsified Synovial...

Case Report
Intra-Articular Calsified Synovial Sarcoma Of Knee – A Case Report Of An Imitating Pathology
Pankaj Kumar Mishra¹, Vishal Yadav¹, Deepak Singh Maravi¹, Sanjeev Gaur¹
Introduction: Although the association of calcification/ossification with the synovial sarcoma is an uncommon finding,
Here we are presenting a rare case of the intra-articular synovial sarcoma of the knee with calcification as a perusal of rare entity, showing that the intra-articular calcification may also be the presentation of the synovial sarcoma.Case Report: It is a case presentation of 35 years old female, who presented to us with a knee lump at the postero-lateral
aspect of her left knee. MRI finding speculated the differential diagnosis of synovial sarcoma, soft tissue sarcoma and peripheral nerve sheath tumor. The fine needle aspiration cytology of the swelling sent for the clinical correlation, and it showed the benign cytology. Excision of the tumor done with the, safety margin. After the 12 months of the postoperative follow-up, the patient again visited to the hospital with the same complaint. Resurgery done for the tumor and it got excised with the safety margin as we could achieve again. Now the histology of the tumor was characteristically of monophasic pattern of synovial cell sarcoma.Conclusion: Here we are acknowledging this case as an experience of the calcified intra-articular synovial sarcoma and
want to add the note that, the calcified lesion within the joint may be mistaken as a benign pathology by the orthopedist if he/she is unwary to the imitating presentation of the synovial sarcoma.Keywords: Intra-Articular Synovial Sarcoma, Knee, Calcification.
International Journal of Surgical Cases 2015 Oct-Dec: 1(2):Page 11-13
Abstract
1Department Of Orthopaedics, G.M.C And Hamidia Hospital Bhopal. M.P. India..
Address of Correspondence
Pankaj Kumar Mishra
Assistant Professor (Department Of Orthopaedics)
G.M.C And Hamidia Hospital Bhopal. M.P. India.
E-mail- [email protected]
Copyright © 2015 by International Journal of Surgical CasesInternational Journal of Surgical Cases | eISSN 2321-3817 | Available on www.surgicalcasesjournal.com/ |
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
11
Author’s Photo Gallery
Dr. Pankaj K Mishra Dr. Vishal Yadav Dr. Deepak SMaravi Dr. Sanjeev Gaur
IntroductionSynovial sarcoma (also known as malignant synovioma) depicts up to the 8 % of the all the soft tissue sarcomas. The pinnacle of incidence is between the adolescents and young age groups, before the 30th birth day. Among the population, male and female ration of distribution is 1.2:1 [1]. Although the association of calcification/ossification with the synovial sarcoma is an uncommon finding, and there are very few cases mentioned in the literature [2, 3].Here we are presenting a rare case of the
intra-articular synovial sarcoma of the knee with calcification as a perusal of rare entity, showing that the intra-articular calcification may also be the presentation of the synovial sarcoma.
Case ReportIt is a case presentation of 35 years old female, who presented to us (in 2007) with a knee lump at the postero-lateral aspect of her left knee. She noticed it 5 months back and since then the swelling had been growing slowly and in the last 2 months, it
was more noticeable. The patient complained to us, for this disfiguring swelling and the mild vague pain. On clinical examination the swelling seemed benign in nature (Fig 1). X-ray of the knee sought and the clinico-radiological differential diagnosis of, synovial chondromatosis, paraosteal osteosarcoma and fractured intra-articular osteochondroma conceded [Fig 2]. The magnetic resonance imaging (MRI) of knee showed the multi-loculated mass in popliteal fossa. It had iso to hypointesce
Access this article online
Website:www.surgicalcasesjournal.com
DOI:
signal in T1 and predominantly hyper-intense signal on T2 sequence with few amorphous calcification. The lesion was extended to the intracapsular lateral tibio-femoral joint (dimension 4.5 X 4.3 X 14.5 centimeter) with the involvement of lateral patellar retinaculum [Fig 3]. Superiorly it tapered to the semimembranosus and inferiorly infiltrated to the gastronemius. And neither there was any cortical erosion or any new bone formation. MRI finding speculated the differential diagnosis of synovial sarcoma, soft tissue sarcoma and peripheral nerve sheath tumor. The fine needle aspiration cytology of the swelling sent for the clinical correlation, and it showed the benign cytology. Finally the patient posted for operative procedure and excision of the tumor with safety margin done as much we could do it, and the excised material sent at the two centers for histological confirmation. One of the center confirmed that it was the fibrofatty tissue with cystic space filled with calcified debris, without any evidence of malignancy and at the second center the histological study revealed that it was the cartilaginous bodies in the synovial membrane (synovial chondromatosis). Post-operative period was uneventful except the injury of common peroneal nerve, that did not recover till the date of last follow up. After the 12 months of the postoperative follow-up, the patient again visited to the hospital with the same complains. Now the clinical scenario of the swelling was different from the previous presentation. The swelling was now tender, warm, with variable consistency and venous dilations over the overlying skin along with restricted range of movements [Fig 4].Follow up MRI showed the recurrence of
the tumor nevertheless it appeared significantly reduced in size (4.5 X 5.3 centimeter) and displacing the neurovascular structures medially. Chest X-ray and sonology of abdomen did not reveal any metastatic lesion. In 2008 the resurgery done for tumor and it got excised with the safety margin as we could achieve again. Now the histology of the tumor was characteristically of monophasic pattern of synovial cell sarcoma, containing the malignant spindle cells. Immunohistochemistry of the synovial sarcoma showed the positivity for viamentin. After the recuperation, the patients sent for radiotherapy where she received the 50 Gray of radiations.After the 5 years of the follow up the, patient is asymptomatic and free from the local recurrence and metastasis. While, the aggressive pathology of the synovial sarcoma needs a more number of the cases of longer follow-up, but even this case report also suggests the propulsive prognosis of the calcified synovial sarcoma of the knee joint.
DiscussionIn 1936 the Knox named it as a synovial sarcoma, on the belief that since the tumor has the tendency to arise near to joint and tumor cell originated from the synovial tissue. But now days the name synovial sarcoma is misnomer sometimes, because in majority cases the synovial sarcoma originates where the synovial tissue is not present (extra-articular location) and the actual cells of the tumor is not necessarily a synovial cell. In that case, the term used is neoplasm of uncertain histogenesis [4, 5]. Usually the synovial tumor are circumscribed and situated adjacent to the joints (≤ 5 cm), but unusually in the 5%
cases they are within the joints or bursa and interdigitates to the surrounding muscles, tendons or vessels [6, 7].Exact pathology of synovial sarcoma is not well understood. But the literature has shown that genetic aberration plays a role for the occurrence of synovial sarcoma. Usually in the clinical practice the synovial sarcoma is diagnosed by histopathology but it is the molecular genetics that confirms the pathology by the presence of t(X;18) gene as a result of reciprocal translocation [8]. This Reciprocal translocation occurs between the SS18 gene (of chromosome 18) and among one of the SSX genes ( SSX1, SSX2 and SSX4 of chromosome X). This reciprocal translocation is usually found in more than 90% of the synovial sarcoma [9]. Utmost important components of diagnostic tools for synovial sarcoma are immunohistochemistry and cytogenetic analysis. Immunohistochemistry make the diagnosis by expressing the epithelial markers (cytokeratin or epithelial membrane antigen) in epitheloid and viamentin in the spindle form. Cytogenetics use the reverse-transcriptase polymerase chain reaction or fluorescent in situ hybridization probes, that locates the t(X;18) gene [10, 11].Histopathology of synovial sarcoma is being classified as biphasic, monophasic and poorly differentiated type and between them the biphasic form is a most common (2/3rd of synovial sarcomas) presentation [12]. In biphasic form the dual cell line is found, it is composed of elongated basophilic spindle cells and columnar epithelial cells. On the contrary the monophasic form has either spindle cell or very uncommonly the epithelial cell. If the monophasic form is comprised of only
www.surgicalcasesjournal.com Mishra P K et al
12
International Journal of Surgical Cases Volume 1 Issue 2 Oct-Dec 2015 Page 11-13 | | | |
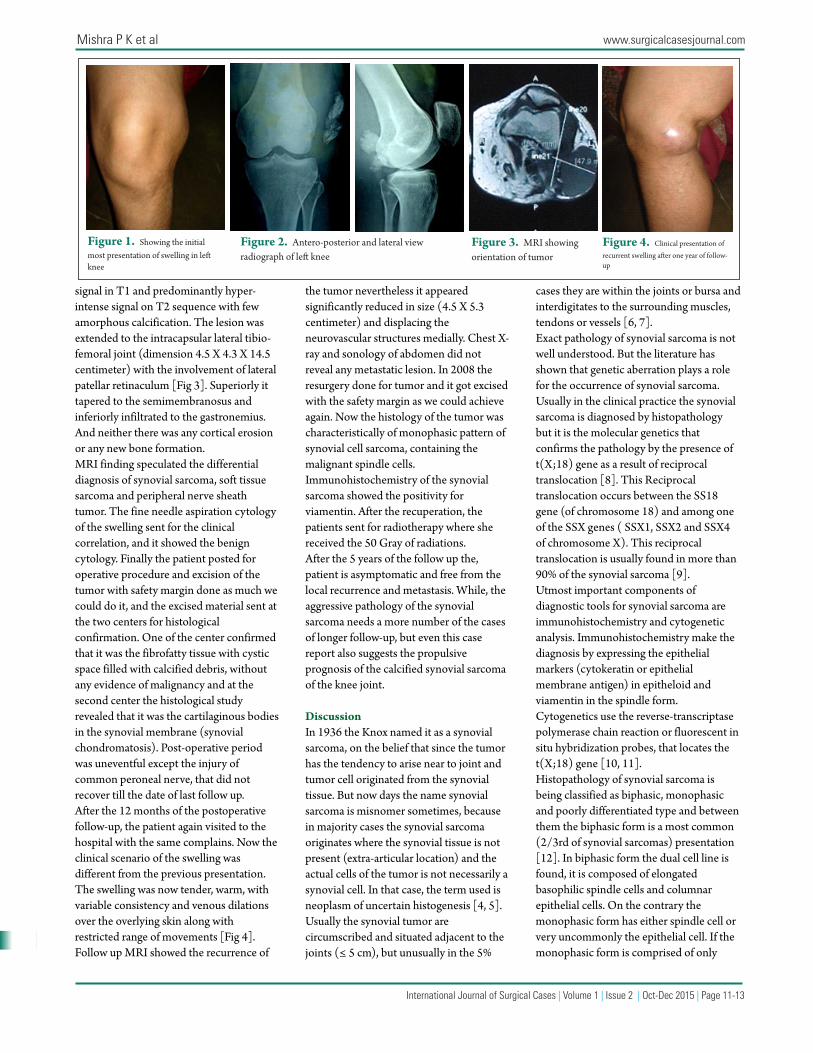
Figure 1. Showing the initial most presentation of swelling in le� knee
Figure 2. Antero-posterior and lateral view radiograph of le� knee
Figure 3. MRI showing orientation of tumor
Figure 4. Clinical presentation of recurrent swelling a�er one year of follow-up

International Journal of Surgical Cases Volume 1 Issue 2 Oct-Dec 2015 Page 11-13 | | | |
13
www.surgicalcasesjournal.com Mishra P K et al
spindle cells, in that condition the malignant peripheral nerve sheath tumour and fibrosarcoma may be the misdiagnosis.Study of G. T. Pack et al (done over 60 patients in 1950) found that, alone surgery for synovial sarcoma has recurrence rate of 63% [13]. And the further study of Lewis et al (2000) found that radiation therapy greatly reduces the local recurrence (up to the10%) [14]. It is assumed that, at the time of clinical presentation of the sarcoma, there is the germane chance of the harbourage of subclinical micrometastasis. So since the few decades the chemotherapy (neoadjuvant/adjuvant) has been used to ameliorate the consequences of sarcomas. F. C. Eilber et al in his study concluded that chemotherapy is strongly correlated to improved disease specific survival [15]. But the toxicity of the chemotherapy and smaller impact on the disease survival, the use of the chemotherapy in primary synovial sarcoma has been controversial [16, 17]. Although the primary amputation
have also been used as a treatment modality [18] but due to the virtue-of its thin incidence, the natural history of the synovial sarcoma is not well known due to the littleness of datum.Since there is no any optimal guideline for the treatment of synovial sarcoma, meanwhile the surgical resection with clear margins and the adjuvant chemotherapy and/or radiotherapy is available treatment modality for the synovial sarcoma. Thus the enhanced surgical techniques as well as irradiation/chemotherapy have better control over local recurrence, but the occurrence of distant metastasis is still a bet for us, so the prognosis of the synovial sarcoma is still forlorn.
ConclusionEarly diagnosis of synovial sarcoma is a diagnostic dare due to its multifarious array of competing differential diagnosis and its rarebit incidence. Splenetic nature of the pathology, the high rate of metastasis and
low five-year survival rates needs a formulation of gold standard of the treatment regime and the longer follow-up. Here we are acknowledging this case as an experience of the calcified intra-articular synovial sarcoma and want to add the note that, the calcified lesion within the joint may be mistaken as a benign pathology by the orthopedist if he/she is unwary to the imitating presentation of the synovial sarcoma.
Clinical MessageIntra-articular (calcified) synovial sarcoma of knee is a rarer presentation. Calcified soft tissue mass is an important but non-distinctive diagnostic hint. So the dissertation of diagnosis, mere on the foundation of radiological study is very difficult. Despite of double occurrence and absent metastasis, the five year survival rate of present case denotes the better prognosis.
References1. Ferrari and Collini (2012). "Synovial Sarcoma". ESUN 9 (5).2. Hisaoka M, Matsuyama A, Shimajiri S, Akiba J, Kusano H, Hiraoka K, Shoda T, Hashimoto H. Ossifying synovial sarcoma. Pathol Res Pract. 2009;205(3):195-8.3. Winnepenninckx V, De Vos R, Debiec-Rychter M, Samson I, Brys P, Hagemeijer A, Sciot R. Calcifying/ossifying synovial sarcoma shows t(X;18) with SSX2 involvement and mitochondrial calci�cations. Histopathology. 2001 Feb;38(2):141-5.4. S. C. Jung, J. A. Choi, J. H. Chung, J. H. Oh, J. W. Lee, and H. S. Kang, “Synovial sarcoma of primary bone origin: a rare case in a rare site with atypical features,” Skeletal Radiology, vol. 36, no. 1, pp. 67–71, 2007.5. M. Haldar, R. L. Randall, and M. R. Capecchi, “Synovial sarcoma: from genetics to genetic-based animal modeling,” Clinical Orthopaedics and Related Research, vol. 466, no. 9, pp. 2156–2167, 2008. 6. P Mohite, A Bhatnagar, S Mehta, H Patel. Synovial sarcoma of the knee joint compressing the popliteal artery: A case report. �e Internet Journal of Surgery. 2006 Volume 12 Number 1.7. M. Vliet, M. Kliffen, G. P. Krestin, and C. F. Dijke, “So� tissue sarcomas at a glance: clinical, histological, and MR imaging features of malignant extremity so� tissue tumors,” European Radiology, vol. 19, no. 6, pp. 1499–1511, 2009. 8- Coindre JM, Pelmus M, Hostein I, Lussan C, Bui BN, Guillou L (2003). "Should molecular testing be required for diagnosing ynovial sarcoma? A prospective study of 204 cases". Cancer 98 (12): 2700–7. 9- R. Jeganathan, R. Davis, L. Wilson, J. McGuigan, and P. Sidhu, “Primary mediastinal synovial sarcoma,”Ulster Medical Journal, vol. 76, no. 2, pp. 109–111, 2007.
10- Brooks JS. Immunohistochemistry in the differential diagnosis of so� tissue tumors. Monogr Pathol 1996; 38:65-128.11- Sandberg AA, Bridge JA. Updates on the cytogenetics and molecular genetics of bone and so� tissue tumors. Synovial sarcoma. Cancer Genet Cytogenet 2002; 133: 1-23.12- Fletcher CDM, McKee : So� tissue tumours. In Oxford Textbook of Pathology. Volume 2b. Edited by McGee J O'D, Isaacson PG, Wright NA. Oxford University Press; 1992::2131-2132.13- G. T. Pack and I. M. Ariel, “Synovial sarcoma (malignant synovioma). A report of 60 cases,” Surgery, vol. 28, no. 6, pp. 1047–1084, 1950.14- J. J. Lewis, C. R. Antonescu, D. H. Y. Leung et al., “Synovial sarcoma: a multivariate analysis of prognostic factors in 112 patients with primary localized tumors of the extremity,” Journal of Clinical Oncology, vol. 18, no. 10, pp. 2087–2094, 2000.15- F. C. Eilber, M. F. Brennan, F. R. Eilber et al., “Chemotherapy is associated with improved survival in adult patients with primary extremity synovial sarcoma,” Annals of Surgery, vol. 246, no. 1, pp. 105–113, 2007.16. Sarcoma Meta-analysis Collaboration. Adjuvant chemotherapy for localized resectable so�-tissue sarcoma of adults: meta-analysis of individual data. Lancet. 1997;350:1647–1654. 17. Verweij J, Seynaeve C. �e reason for con�ning the use of adjuvant chemotherapy in so� tissue sarcoma to the investigational se�ing. Semin Radiat Oncol. 1999;9:352–359. 18- Gresswell SD, Corsini AA, Balsamo LH, Miles EF. Intra-articular synovial sarcoma treated with a transfemoral amputation: a case report and review of the literature. Mil Med. 2013 Aug;178(8):e956-62.
Conflict of Interest: Nil Source of Support: None
How to Cite this Article
Mishra P K, Yadav V, Maravi D S, Gaur S. INTRA-ARTICULAR CALSIFIED SYNOVIAL
SARCOMA OF KNEE – A case report of an imitating pathology. International Journal
of Surgical Cases 2015 Oct-Dec;1(2): 11-13.










![A single intra-articular injection of 2.0% non-chemically ... · i.e., much longer than intra-articular corticosteroid injections [14–27]. Intra-articular HA even seems to offer](https://static.fdocuments.in/doc/165x107/5e6e7a63d7b9dc553774f316/a-single-intra-articular-injection-of-20-non-chemically-ie-much-longer.jpg)







