Case Report Idiopathic Hypertrophic Spinal Pachymeningitis ... · Idiopathic hypertrophic spinal...
7
1/7 https://kjnt.org ABSTRACT Idiopathic hypertrophic spinal pachymeningitis (IHSP) is a rare, diffuse inflammatory fibrosis of the dura mater that can lead to spinal cord compression. Though the optimal treatment is controversial, some reports recommend decompressive surgery and postoperative steroid therapy. However, we encountered a case of pachymeningitis that worsened aſter decompressive surgery. A 79-year-old woman presented with gait disturbance and bilateral lower extremity weakness that began 6 months prior. She had radiating pain on the C5 and T1 dermatomes and clumsiness in both hands. Magnetic resonance imaging (MRI) revealed diffuse thickening of the posterior longitudinal ligament of C6 to T4/5 and ligamentum flavum of C3/4 to T4/5, causing central canal stenosis and compressive myelopathy. She underwent posterior decompressive laminectomy from C4 to T1 total (T2 subtotal) and cervicothoracic screw fixation. During surgery, we found severe adhesion of the posterior longitudinal ligament and ligamentum flavum to the dura mater. Chronic inflammation with fibrosis and lymphoplasmacytic infiltration were present. Aſter surgery, the patient's motor weakness worsened. Despite steroid treatment, her symptom severity fluctuated. Follow-up MRI obtained 3 months postoperation revealed high signal intensity from C5 to T2, possibly indicating aggravated compressive myelopathy. Thus, in this case, decompressive surgery and steroid therapy were detrimental. Keywords: Pachymeningitis; Laminectomy; Compressive myelopathy; Cervical spinal cord INTRODUCTION Idiopathic hypertrophic spinal pachymeningitis (IHSP) is a rare, chronic, progressive diffuse inflammatory fibrosis of the dura mater that can lead to compression of the spine or brain. 15) The first report of IHSP was published by Charcot and Joffroy in 1869 3) with involvement of the spinal meninges, and intracranial idiopathic hypertrophic pachymeningitis was reported in 1918. 7) A diagnosis of IHSP is made via contrast-enhanced magnetic resonance imaging (MRI) and confirmed by pathological examination of the excised dura mater. Decompressive Korean J Neurotrauma. 2020 Oct;16(2):e17 https://doi.org/10.13004/kjnt.2020.16.e17 pISSN 2234-8999·eISSN 2288-2243 Case Report Received: Oct 24, 2019 Revised: Apr 30, 2020 Accepted: May 8, 2020 Address for correspondence: Il Choi Department of Neurosurgery, Hallym University Dongtan Sacred Heart Hospital, 7 Keunjaebong-gil, Hwaseong 18450, Korea. E-mail: [email protected] Copyright © 2020 Korean Neurotraumatology Society This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https:// creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ORCID iDs Jae yeon Park https://orcid.org/0000-0002-7052-8025 Il Choi https://orcid.org/0000-0003-0120-6564 Conflict of Interest The authors have no financial conflicts of interest. Jae yeon Park 1 , Il Choi 1 , Eun Kyung Khil 2 , Wu Jae Kim 1 , and Il Young Shin 1 1 Department of Neurological Surgery, Dongtan Sacred Heart Hospital, College of Medicine, Hallym University, Hwaseong, Korea. 2 Department of Radiology, Dongtan Sacred Heart Hospital, College of Medicine, Hallym University, Hwaseong, Korea. Idiopathic Hypertrophic Spinal Pachymeningitis with Spinal Cord Lesion: A Case Report Provisional Provisional
Transcript of Case Report Idiopathic Hypertrophic Spinal Pachymeningitis ... · Idiopathic hypertrophic spinal...

1/7https://kjnt.org
ABSTRACT
Idiopathic hypertrophic spinal pachymeningitis (IHSP) is a rare, diffuse inflammatory fibrosis of the dura mater that can lead to spinal cord compression. Though the optimal treatment is controversial, some reports recommend decompressive surgery and postoperative steroid therapy. However, we encountered a case of pachymeningitis that worsened after decompressive surgery. A 79-year-old woman presented with gait disturbance and bilateral lower extremity weakness that began 6 months prior. She had radiating pain on the C5 and T1 dermatomes and clumsiness in both hands. Magnetic resonance imaging (MRI) revealed diffuse thickening of the posterior longitudinal ligament of C6 to T4/5 and ligamentum flavum of C3/4 to T4/5, causing central canal stenosis and compressive myelopathy. She underwent posterior decompressive laminectomy from C4 to T1 total (T2 subtotal) and cervicothoracic screw fixation. During surgery, we found severe adhesion of the posterior longitudinal ligament and ligamentum flavum to the dura mater. Chronic inflammation with fibrosis and lymphoplasmacytic infiltration were present. After surgery, the patient's motor weakness worsened. Despite steroid treatment, her symptom severity fluctuated. Follow-up MRI obtained 3 months postoperation revealed high signal intensity from C5 to T2, possibly indicating aggravated compressive myelopathy. Thus, in this case, decompressive surgery and steroid therapy were detrimental.
Keywords: Pachymeningitis; Laminectomy; Compressive myelopathy; Cervical spinal cord
INTRODUCTION
Idiopathic hypertrophic spinal pachymeningitis (IHSP) is a rare, chronic, progressive diffuse inflammatory fibrosis of the dura mater that can lead to compression of the spine or brain.15) The first report of IHSP was published by Charcot and Joffroy in 18693) with involvement of the spinal meninges, and intracranial idiopathic hypertrophic pachymeningitis was reported in 1918.7)
A diagnosis of IHSP is made via contrast-enhanced magnetic resonance imaging (MRI) and confirmed by pathological examination of the excised dura mater. Decompressive
Korean J Neurotrauma. 2020 Oct;16(2):e17https://doi.org/10.13004/kjnt.2020.16.e17pISSN 2234-8999·eISSN 2288-2243
Case Report
Received: Oct 24, 2019Revised: Apr 30, 2020Accepted: May 8, 2020
Address for correspondence:Il ChoiDepartment of Neurosurgery, Hallym University Dongtan Sacred Heart Hospital, 7 Keunjaebong-gil, Hwaseong 18450, Korea.E-mail: [email protected]
Copyright © 2020 Korean Neurotraumatology SocietyThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ORCID iDs Jae yeon Park https://orcid.org/0000-0002-7052-8025Il Choi https://orcid.org/0000-0003-0120-6564
Conflict of InterestThe authors have no financial conflicts of interest.
Jae yeon Park 1, Il Choi 1, Eun Kyung Khil2, Wu Jae Kim1, and Il Young Shin1
1 Department of Neurological Surgery, Dongtan Sacred Heart Hospital, College of Medicine, Hallym University, Hwaseong, Korea.
2 Department of Radiology, Dongtan Sacred Heart Hospital, College of Medicine, Hallym University, Hwaseong, Korea.
Idiopathic Hypertrophic Spinal Pachymeningitis with Spinal Cord Lesion: A Case Report
Provisional
Provisional

laminectomy combined with immunosuppressive therapy using steroids has been found to be an effective treatment.9) However, we experienced a case of pachymeningitis with spinal cord lesion that worsened after sufficient decompressive surgery and steroid treatment. Herein, we present our case of IHSP with an unexpected outcome.
CASE REPORT
A 79-year-old female visited our hospital presenting with gait disturbance and bilateral lower extremity weakness. She also experienced radiating pain at both the C5 and T1 dermatomes and clumsiness in both hands. These symptoms began 6 months prior and worsened progressively. Her medical history included hypertension and dyslipidemia. In addition, she had been treated in the Endocrinology Department for several months because of steroid-induced diabetes mellitus and adrenal insufficiency.
The laboratory results on admission showed elevated erythrocyte sedimentation rate (45 mm/hr), C-reactive protein (20.4 mg/L), and rheumatoid factor (149.9 IU/mL) levels, which suggests inflammation. Laboratory results further confirmed that she did not have syphilis, fungal infection, neoplasm, or other systemic autoimmune disorders. On a neurological examination, her motor power in the lower extremities was grade IV/IV, upper extremity grasping power was grade IV/IV, and she had an ataxic gait. Her deep tendon reflex and ankle clonus were normal. Based on these findings, a diagnosis of progressive low cervical radiculomyelopathy was made and the patient's condition was investigated further.
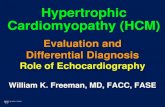
On MRI of the patient's cervical spine, we found diffuse low signal intensity at C3/4 to T4/5, causing central canal stenosis at C3/4 to T4/5 and compressive myelopathy at C6/7 to C7/T1 on the T2-weighted images (FIGURE 1 & 3A). Because of the patient's progressing paraplegia and compressive myelopathy on the preoperative cervical MRI, a treatment plan was established that included immediate decompressive surgery. The main compressive lesion was C6-7 and we considered about thoracic spine MRI sagittal image and the patient's old age (FIGURE 1), so she underwent posterior decompressive laminectomy at C4 to T1 total (T2 subtotal) and cervicothoracic screw fixation (C4 to T2 pedicle screw insertion, bilaterally) with allograft and autograft bone grafts. During surgery, we found severe adhesion of the posterior longitudinal ligament and ligamentum flavum to the dura mater. During the procedure to remove the thickened dura mater, there were multiple incidental dural tears. Consequently, the durotomy site was primarily repaired intra-operatively. The intraoperative neurophysiological monitoring (IONM) was placed and observed about the motor evoked potentials (MEPs). There was temporary MEPs decreasing when we did laminectomy, but recovered in final MEPs (FIGURE 2).
Chronic active inflammation with fibrosis and lymphoplasmacytic infiltration was found on the pathology report (FIGURE 4).
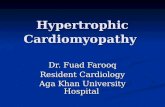
The postoperative cervical MRI obtained the day after surgery showed that the decompression was sufficient. However, a new, subtle change was observed in the spinal cord, specifically high signal intensity at the C3/4 (right), C4/5 (left), C5/6 (bilateral) level on the T2-weighted images (FIGURE 3B) After surgery, her motor weakness became more severe bilaterally. Her motor power in the lower extremities was grade II/III immediately after surgery, but it was reduced to grade I/II the next day. One week after surgery, her motor power
2/7https://kjnt.org https://doi.org/10.13004/kjnt.2020.16.e17
A Case of Idiopathic Hypertrophic Spinal Pachymeningitis
Provisional
Provisional

was grade II/III. The cervical MRI showed no significant changes to the new high signal intensity change at C3/4 to C5/6. Steroid treatment included dexamethasone administration
3/7https://kjnt.org https://doi.org/10.13004/kjnt.2020.16.e17
A Case of Idiopathic Hypertrophic Spinal Pachymeningitis
T1
T2
T3
T4
T5
T6
T7
T8
T9
T10
T11
T12
T2
T3
T4
T5
T6
T7
T8
T9
T10
T12
T1
C3
C4
C5
C6C7
T11
A
B
C
D E F
FIGURE 1. T2-weighted cervical magnetic resonance axial imaging scan obtained before surgery, C3/4 (A), C4/5 (B), C5/6 (C), C6/7 (D), T2-weighted thoracic magnetic resonance sagittal imaging scan obtained before surgery (E), and cervico-thoracic computed tomography (F).
FIGURE 2. Intraoperative neurophysiological monitoring (IONM) for motor evoked potentials (MEPs) of both lower leg, initial (A), exposure(B), screw instrumentation (C), laminectomy (D), and final (E).
Provisional
Provisional

beginning immediately after surgery (20 mg for 3 days, followed by half-dose tapering for 2 days). However, despite the steroid treatment, her symptom severity fluctuated.
One month after surgery, her lower motor power remained at grade I/II. Cervical MRI revealed a newly developed cerebrospinal fluid (CSF) collection (approximately 3.5×1.5×10 cm) along the dorsal aspect of central canal, at the operative site of C3/4 to the T1/2 level on
4/7https://kjnt.org https://doi.org/10.13004/kjnt.2020.16.e17
A Case of Idiopathic Hypertrophic Spinal Pachymeningitis
A B C D
T1
T2
C2
C3
C4
C5
C6
C7 T1
C2
C3
C4
C5
C6
C7T1
C2
C3C4
C5C6
C7
T1
C2
C3
C4C5
C6C7
FIGURE 3. T2-weighted cervical magnetic resonance imaging scan obtained before surgery (A), immediately after surgery (B), 1 month post-surgery (C), and 3 months post-surgery (D).
FIGURE 4. Photomicrographs of the surgical specimen showing chronic inflammation with fibrosis and lymphoplasmacytic infiltration (hematoxylin and eosin, ×40, ×200).
Provisional
Provisional

the T2-weighted images (FIGURE 3C). We suspected dural injury during surgery or a chronic inflammatory course of ISP, but because she experienced no other progressing symptoms, we decided to observe the CSF collection. The patient's next outpatient clinic follow-up occurred 2 months postoperation, and her lower power motor was grade III/IV. Follow-up MRI was performed 3 months postoperation. The CSF collection was almost completely resolved, but high signal intensity was observed at C5 to the T2 level on the T2-weighted images, which likely indicates aggravated compressive myelopathy (FIGURE 3D). At this visit, the patient's lower motor power had worsened to grade 0/I. During the 3 months after the surgery, she developed pulmonary and infective complications.
This research is about an individual case without the approval of an ethical research. We obtained informed consent from the patient.
DISCUSSION
IHSP is rare disease, and it represents an uncommon cause of spinal cord compression. It is caused by chronic inflammatory hypertrophy of the dura and arachnoid mater, typically involving multiple levels of the cervical and thoracic spine.15) The etiology of IHSP is unclear. Some reports postulate the involvement of a related disease, such as rheumatoid arthritis,6) Wegener's granulomatosis,11) sarcoidosis,8) infective disease (such as tuberculosis,18) fungal infection,17) or syphilis4)), metabolic disease,14) autoimmune disease,19) or transverse myelitis.16) As we could find no evidence of these potential causes in our patient, she was considered to have idiopathic HSP. Although she had a high level of rheumatoid factor (149.9 IU/mL), she had no clinically relevant symptoms of rheumatoid arthritis (for example, articular swelling, morning stiffness of the fingers, or arthralgia).
MRI can be a useful diagnostic method for IHSP, but it is easily misdiagnosed as another disease, such as an epidural abscess or spinal tumor, because of the similarity in the hypertrophic dura mater.
Some reports describe the IHSP lesion as hypointense with a hyperintense border on T2-weighted images. The hypointense signal occurs because of the dense fibrous tissue, while the hyperintense signal results from inflammatory infiltration or hypervascularity.9,12)
The gold standard treatment of IHSP is controversial, but some reports posit that removal of the IHSP lesion and sufficient decompressive laminectomy can be helpful for relieving symptoms and obtaining a pathologic diagnosis.2,5,10) In one case report, the author suggested methotrexate therapy for recurrent IHSP that was refractory to steroid administration, which produced a good outcome without complications.13) Many reports have suggested positive effects of postoperative immunosuppressive treatment, including methotrexate, cyclophosphamide, azathioprine, and radiotherapy.1,2,5) The treatment of our patient involved surgical excision of the lesion, decompressive laminectomy, and postoperative steroid therapy.
Many reports support the theory that if sufficient surgical decompression and postoperative immunosuppression therapy are performed properly in a patient with IHSP, the outcome may be favorable, aside from the possibility of remission or refractory response to steroids. Despite these successful cases, in our experience with this patient, decompressive surgery and steroid therapy was not effective. In addition, the compressive myelopathy observed before surgery was aggravated.
5/7https://kjnt.org https://doi.org/10.13004/kjnt.2020.16.e17
A Case of Idiopathic Hypertrophic Spinal Pachymeningitis
Provisional
Provisional

Our case of IHSP is the first to report worsening symptoms and increased signal change in the spinal cord despite sufficient decompression and postoperative immunosuppression therapy.
CONCLUSION
In our experience, sufficient decompression and postoperative immunosuppression therapy do not give favorable outcome in IHSP patient.
REFERENCES
1. Bosman T, Simonin C, Launay D, Caron S, Destée A, Defebvre L. Idiopathic hypertrophic cranial pachymeningitis treated by oral methotrexate: a case report and review of literature. Rheumatol Int 28:713-718, 2008 PUBMED | CROSSREF
2. Bucy PC, Freeman LW. Hypertrophic spinal pachymeningitis with special reference to appropriate surgical treatment. J Neurosurg 9:564-578, 1952 PUBMED | CROSSREF
3. Charcot JM, Joffory A. Deux cas d'atrophie musculaire progressive: avec lésions de la substance grise et des faisceaux antérolatéraux de la moelle épinière. Arch Physiol Norm Pathol 2: 354-369, 629-649, 744-760, 1869
4. Deshpande DH, Vidyasagar C. Hypertrophic pachymeningitis dorsalis. Surg Neurol 12:217-220, 1979PUBMED
5. Dumont AS, Clark AW, Sevick RJ, Myles ST. Idiopathic hypertrophic pachymeningitis: a report of two patients and review of the literature. Can J Neurol Sci 27:333-340, 2000 PUBMED | CROSSREF
6. Gutmann L, Hable K. Rheumatoid pachymeningitis. Neurology 13:901-905, 1963 PUBMED | CROSSREF
7. Hassin GB. Histogenesis of cerebral hypertrophic pachymeningitis. Am J Syphilis 2:715, 1918
8. Huang H, Haq N. Spinal leptomeningeal sarcoidosis. Neuroradiology 29:100, 1987 PUBMED | CROSSREF
9. Mamelak AN, Kelly WM, Davis RL, Rosenblum ML. Idiopathic hypertrophic cranial pachymeningitis. Report of three cases. J Neurosurg 79:270-276, 1993 PUBMED | CROSSREF
10. Naffziger HC, Stern WE. Chronic pachymeningitis; report of a case and review of the literature. Arch Neurol Psychiatry 62:383-411, 1949 PUBMED | CROSSREF
11. Nishino H, Rubino FA, Parisi JE. The spectrum of neurologic involvement in Wegener’s granulomatosis. Neurology 43:1334-1337, 1993 PUBMED | CROSSREF
12. Nishizaki T, Iwamoto F, Uesugi S, Akimura T, Yamashita K, Ito H. Idiopathic cranial pachymeningoencephalitis focally affecting the parietal dura mater and adjacent brain parenchyma: case report. Neurosurgery 40:840-843, 1997 PUBMED | CROSSREF
13. Park TJ, Seo WD, Kim SY, Cho JH, Kim DH, Kim KH. Effective response of methotrexate for recurrent idiopathic hypertrophic spinal pachymeningitis. Korean J Spine 13:200-203, 2016 PUBMED | CROSSREF
14. Paulson GW, Meagher JN, Burkhart J. Spinal pachymeningitis secondary to mucopolysaccharidosis. Case report. J Neurosurg 41:618-621, 1974 PUBMED | CROSSREF
15. Rosenfeld JV, Kaye AH, Davis S, Gonzales M. Pachymeningitis cervicalis hypertrophica. Case report. J Neurosurg 66:137-139, 1987 PUBMED | CROSSREF
16. Shu J, Gu C, Ren Y, Wei W. ANCA-associated hypertrophic spinal pachymeningitis presenting with longitudinally extensive transverse myelitis: a case report. Ann Indian Acad Neurol 23:131-132, 2020 PUBMED | CROSSREF
6/7https://kjnt.org https://doi.org/10.13004/kjnt.2020.16.e17
A Case of Idiopathic Hypertrophic Spinal Pachymeningitis
Provisional
Provisional

17. Van de Wyngaert FA, Sindic CJ, Rousseau JJ, Fernandes Xavier FG, Brucher JM, Laterre EC. Spinal arachnoiditis due to aspergillus meningitis in a previously healthy patient. J Neurol 233:41-43, 1986 PUBMED | CROSSREF
18. Wadia NH, Dastur DK. Spinal meningitides with radiculo-myelopathy. 1. Clinical and radiological features. J Neurol Sci 8:239-260, 1969 PUBMED | CROSSREF
19. Yakushiji Y, Kurohara K, Toda S, Abe M, Kuroda Y. A case of hypertrophic spinal pachymeningitis associated with MPO-ANCA. Rinsho Shinkeigaku 42:873-877, 2002PUBMED
7/7https://kjnt.org https://doi.org/10.13004/kjnt.2020.16.e17
A Case of Idiopathic Hypertrophic Spinal Pachymeningitis
Provisional
Provisional












![GENETIC BASIS OF HYPERTROPHIC CARDIOMYOPATHYThroughout the years, names such as idiopathic hypertrophic subaortic stenosis[5], muscular subaortic stenosis[6] and hypertrophic obstructive](https://static.fdocuments.in/doc/165x107/60571329c95e4748070a14f6/genetic-basis-of-hypertrophic-cardiomyopathy-throughout-the-years-names-such-as.jpg)