Case Report Biclonal IgD and IgM Plasma Cell Myeloma: A...
6
Hindawi Publishing Corporation Case Reports in Hematology Volume 2013, Article ID 293150, 5 pages http://dx.doi.org/10.1155/2013/293150 Case Report Biclonal IgD and IgM Plasma Cell Myeloma: A Report of Two Cases and a Literature Review Zhongchuan W. Chen, 1 Ioanna Kotsikogianni, 2 Jay S. Raval, 3,4,5 Christine G. Roth, 3 and Marian A. Rollins-Raval 3,5 1 Department of Laboratory Medicine and Pathobiology, University of Toronto, Toronto, ON, Canada M5S 1A1 2 Pathology Laboratory, Patras General Hospital “O Agios Andreas,” 26500 Patras, Greece 3 Department of Pathology, University of Pittsburgh, Pittsburgh, PA 15261, USA 4 e Institute for Transfusion Medicine, Pittsburgh, PA 15213, USA 5 Department of Pathology and Laboratory Medicine, University of North Carolina, Chapel Hill, NC 27599-7525, USA Correspondence should be addressed to Marian A. Rollins-Raval; marian [email protected] Received 16 August 2013; Accepted 17 September 2013 Academic Editors: R. Herrmann, K. Konstantopoulos, A. Ohsaka, and T. Sonoki Copyright © 2013 Zhongchuan W. Chen et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Biclonal plasma cell myelomas producing two different isotypes of immunoglobulins are extremely rare entities; to date, the combination of IgD and IgM secretion by a biclonal plasma cell myeloma has not been reported. Bone marrow biopsy immuno- histochemical studies in two cases revealed neoplastic plasma cells coexpressing IgD and IgM, but serum protein electrophoresis identified only the IgM monoclonal paraprotein in both cases. Biclonal plasma cell myelomas, while currently not well characterized in terms of their clinical behavior, should be distinguished from B-cell lymphoma with plasmacytic differentiation, given the different therapeutic implications. Both cases reported herein demonstrated chemotherapy-resistant clinical courses. 1. Introduction Immunosecretory disorders are clonal proliferations of im- munoglobulin-producing plasma cells or lymphocytes that secrete a single isotype or polypeptide subunit of immu- noglobulin (Ig) usually detectable as a monoclonal protein peak (M-protein) on serum or urine protein electrophoresis studies. Most plasma cell myelomas (PCMs) result in a monoclonal gammopathy, with IgG M-protein produced in slightly more than 50% of cases and IgA in 20% of cases [1, 2]. Another 20% of cases produce only monoclonal light chains [1]. Fewer than 2% of cases produce monoclonal IgD, IgE, or IgM [3, 4]. Only rare PCMs result in biclonal gammopathy with the production of two different heavy chains and/or light chains. In a large review of 1027 PCM patients, only 2% had a biclonal gammopathy on protein electrophoresis studies [2]. However, the review did not specify which combinations of biclonal M-proteins were present. Other reports have described combinations of biclonal gammopathies, including IgD/IgG, IgG/IgM, IgA/IgG, and kappa/lambda light chain biclonal gammopathies [3, 5–9]. We report herein two cases of IgD/IgM biclonal PCM, a combination of heavy chain production that has not been previously described in the literature. 2. Case Presentations 2.1. Case 1. A 55-year-old male presented with anemia (he- moglobin 8.5 g/dL, reference range 14–17 g/dL). He had been on warfarin therapy following aortic valve replacement and mitral valve repair due to a recent episode of bacterial endo- carditis. His medical history was also significant for diabetes mellitus, sarcoidosis, hypothyroidism, and hypertension. A bone marrow biopsy was performed as part of the anemia evaluation. e aspirate smears were suboptimal in prepa- ration, but the bone marrow biopsy demonstrated normo- cellular marrow with a diffuse interstitial infiltrate of plasma cells comprising more than 30% of the marrow elements. e plasma cells were mildly atypical, with a rare Dutcher
Transcript of Case Report Biclonal IgD and IgM Plasma Cell Myeloma: A...

Hindawi Publishing CorporationCase Reports in HematologyVolume 2013 Article ID 293150 5 pageshttpdxdoiorg1011552013293150
Case ReportBiclonal IgD and IgM Plasma Cell MyelomaA Report of Two Cases and a Literature Review
Zhongchuan W Chen1 Ioanna Kotsikogianni2 Jay S Raval345
Christine G Roth3 and Marian A Rollins-Raval35
1 Department of Laboratory Medicine and Pathobiology University of Toronto Toronto ON Canada M5S 1A12 Pathology Laboratory Patras General Hospital ldquoO Agios Andreasrdquo 26500 Patras Greece3 Department of Pathology University of Pittsburgh Pittsburgh PA 15261 USA4The Institute for Transfusion Medicine Pittsburgh PA 15213 USA5Department of Pathology and Laboratory Medicine University of North Carolina Chapel Hill NC 27599-7525 USA
Correspondence should be addressed to Marian A Rollins-Raval marian ravalmeduncedu
Received 16 August 2013 Accepted 17 September 2013
Academic Editors R Herrmann K Konstantopoulos A Ohsaka and T Sonoki
Copyright copy 2013 Zhongchuan W Chen et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Biclonal plasma cell myelomas producing two different isotypes of immunoglobulins are extremely rare entities to date thecombination of IgD and IgM secretion by a biclonal plasma cell myeloma has not been reported Bone marrow biopsy immuno-histochemical studies in two cases revealed neoplastic plasma cells coexpressing IgD and IgM but serum protein electrophoresisidentified only the IgMmonoclonal paraprotein in both cases Biclonal plasma cellmyelomas while currently not well characterizedin terms of their clinical behavior should be distinguished from B-cell lymphoma with plasmacytic differentiation given thedifferent therapeutic implications Both cases reported herein demonstrated chemotherapy-resistant clinical courses
1 Introduction
Immunosecretory disorders are clonal proliferations of im-munoglobulin-producing plasma cells or lymphocytes thatsecrete a single isotype or polypeptide subunit of immu-noglobulin (Ig) usually detectable as a monoclonal proteinpeak (M-protein) on serum or urine protein electrophoresisstudies Most plasma cell myelomas (PCMs) result in amonoclonal gammopathy with IgG M-protein produced inslightly more than 50 of cases and IgA in 20 of cases [1 2]Another 20 of cases produce only monoclonal light chains[1] Fewer than 2 of cases produce monoclonal IgD IgE orIgM [3 4]
Only rare PCMs result in biclonal gammopathy withthe production of two different heavy chains andor lightchains In a large review of 1027 PCM patients only 2 had abiclonal gammopathy on protein electrophoresis studies [2]However the review did not specify which combinationsof biclonal M-proteins were present Other reports havedescribed combinations of biclonal gammopathies including
IgDIgG IgGIgM IgAIgG and kappalambda light chainbiclonal gammopathies [3 5ndash9] We report herein two casesof IgDIgM biclonal PCM a combination of heavy chainproduction that has not been previously described in theliterature
2 Case Presentations
21 Case 1 A 55-year-old male presented with anemia (he-moglobin 85 gdL reference range 14ndash17 gdL) He had beenon warfarin therapy following aortic valve replacement andmitral valve repair due to a recent episode of bacterial endo-carditis His medical history was also significant for diabetesmellitus sarcoidosis hypothyroidism and hypertension Abone marrow biopsy was performed as part of the anemiaevaluation The aspirate smears were suboptimal in prepa-ration but the bone marrow biopsy demonstrated normo-cellular marrow with a diffuse interstitial infiltrate of plasmacells comprising more than 30 of the marrow elementsThe plasma cells were mildly atypical with a rare Dutcher
2 Case Reports in Hematology
body identified Flow cytometry performed on the aspiratespecimen demonstrated that the CD138 positive plasma cellswere CD56 positive and exhibited surface and cytoplas-mic lambda light chain restriction Flow cytometric stud-ies did not identify an abnormal B-lymphoid populationImmunohistochemistry performed on paraffin embeddedsections of the bone marrow biopsy revealed the neoplas-tic cells to be CD138 positive CD20 negative IgM heavychain positive (Figure 1(a)) and lambda light chain restrictedInterestingly a subset of these cells expressed IgDheavy chain(Figure 1(b)) and cyclin D1 None of the cells expressed IgAor IgG Fluorescence in-situ hybridization (FISH) analysisfor CCND1IGH fusion indicating a t(1114) was negative in99 of the cells using Vysis DNA probes (Abbott MolecularInc Des Plaines IL USA) Following the bone marrowbiopsy serum protein electrophoresis demonstrated a mon-oclonal peak in the beta region (14 gdL) with immunofix-ation confirming an IgM-lambda monoclonal gammopa-thy Immunofixation for IgD was not assessed Biochemicalanalysis revealed a borderline low ionized calcium level(093mmolL reference range 10ndash14mmolL) and normalblood urea nitrogen and creatinine levels No lytic lesionswere observed by radiographic imaging At this point theneoplasm was best considered asymptomatic (smoldering)myeloma as the patient had more than 10 clonal plasmacells in the bone marrow but no organ or tissue impair-ment was attributed to the neoplasm Three months laterthe patient underwent a second surveillance bone marrowbiopsy This time the morphology of the neoplastic cells wasevaluable on the marrow aspirate smear and was ldquolymphop-lasmacytoidrdquo (Figure 1(c)) The neoplastic cells accountedfor 35 of the total cellularity based on the marrow aspi-rate smear differential Immunohistochemistry was not per-formed on the bone marrow biopsy but flow cytometricstudies confirmed the persistent CD138 positive and CD56positive lambda monoclonal plasma cell population that wasnegative for CD19 and CD20 Since his serum IgM levelwas elevated to 4660mgdL (reference range 40ndash230mgdL)with depression of IgA and IgG levels he was started ondexamethasone vincristine and doxorubicin however thistherapy did not decrease IgM levels and he was switchedto a thalidomidedexamethasone regimen The dexametha-sone was stopped eight months later due to uncontrollablehyperglycemia He was continued on the thalidomide andhis IgM levels decreased to 2270mgdL and appeared stableHowever within three months his IgM levels increased to3420mgdL and thalidomide was discontinued A third bonemarrow biopsy at this time demonstrated persistent diseasewith neoplastic plasma cells accounting for 23 of the totalcellularity based on the marrow aspirate differential Serumprotein electrophoresis continued to exhibit an IgM-lambdamonoclonal protein (017 gdL) as well as a second nonquan-tifiable free lambda light chain protein At this time nowtwo years after his initial diagnosis the patient underwenthigh dose melphalan autologous peripheral blood stem celltransplantation
A fourth bone marrow biopsy performed one yearlater demonstrated disease progression with 50 neoplasticplasma cells based on manual marrow aspirate differential
and 12 plasma cells in the peripheral blood At this timehe was started on lenalidomide but unfortunately the newtherapy was not tolerated A subsequent bonemarrow biopsythree months later demonstrated continued progression with82 plasma cells At this point there was also an evolution toplasma cell leukemia evidenced by 28 circulating plasmacells Within six months he underwent a second autologousperipheral blood stem cell transplantation complicated bypancytopenia requiring growth factor support and red bloodcell and platelet transfusions The transplantation was ulti-mately unsuccessful and his plasma cell leukemia despitereinitiation of lenalidomide and dexamethasone persistedHis clinical course was complicated by lower extremitycellulitis Klebsiella pneumoniae sepsis and uncontrollablehematuria and the patient died 4 years and 4 months afterhis initial diagnosis with persistent PCM
22 Case 2 A 71-year-old male presented with altered men-tal status and was initially diagnosed with streptococcalpneumonia sepsis and left lower extremity deep venousthrombosis Peripheral blood examination revealed ane-mia (hemoglobin 78 gdL reference range 129ndash169 gdL)with 9 plasma cells and significant rouleaux forma-tion Quantitative immunoglobulin determination showed amarked increase in IgM (7655mgdL reference range 40ndash274mgdL) Serum protein electrophoresis with immunofix-ation revealedmonoclonal IgM-kappaM-protein (534 gdL)Urine protein electrophoresis demonstrated the presence oftwo monoclonal spikes in the gamma region (1328mgdLand 10469mgdL) and immunofixation performed on theurine demonstrated a kappa light chain not associated withIgA IgG or IgM heavy chains CT scan of the abdomenand pelvis displayed neither lymphadenopathy nor hep-atosplenomegaly and a radiographic skeletal survey wasnegative for lytic lesions Due to the patientrsquos deterioratingclinical status which included worsening altered mentalstatus attributed to hyperviscosity (serumviscosity 88 cP ref-erence range 14ndash18 cP) from elevated IgM a course oftherapeutic plasma exchange (TPE) was initiated Ten 15volume TPE procedures with 5 albumin replacement wereperformed over a 20-day period to reduce IgM levels andimprove cognitive impairment Due to clinical suspicion forWaldenstrommacroglobulinemia a bonemarrow evaluationwas performed
The peripheral blood demonstrated rouleaux formationas well as circulating plasma cells some with cytoplas-mic immunoglobulin inclusions (Russell bodies) The mar-row aspirate smears contained numerous plasma cells withnumerous Dutcher bodies and Russell bodies as well as lym-phoplasmacytic morphology (Figure 2(a))The bonemarrowbiopsy demonstrated hypercellular marrow for the patientrsquosage that was extensively replaced by an infiltrate of predom-inantly mature-appearing plasma cells some of which werebinucleated and containing Dutcher bodies that accountedfor 95of the total cellularity on the core biopsy Flow cytom-etry confirmed the presence of a population CD138 positiveCD38 positive CD20 partially positive CD19 negative CD56negative and cytoplasmic kappa light chain restricted plasmacells with no abnormal B-lymphoid population identified
Case Reports in Hematology 3
(a) (b) (c)
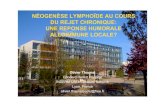
Figure 1 Case 1 (a) Biopsy from initial sample demonstrating that the majority of cells express IgM (b) A subset of cells express IgD (c)Aspirate smear of second pretreatment marrow evaluation Immunohistochemistry oil objective original magnification times500 ((a) and (b))Wright-Giemsa oil objective original magnification times1000 (c)
Immunohistochemistry performed on paraffin sections ofthe core biopsy demonstrated the neoplastic plasma cells tobe diffusely positive for IgM (Figure 2(b)) and a subset thatwas weakly positive for IgD (Figure 2(c)) Interestingly theareas with increased IgD positive cells were also CD20positive Cyclin D1 was positive on many of the plasmacells but highlighted fewer plasma cells as compared toIgM Conventional G-band karyotyping of the bone marrowrevealed a normal male karyotype 46 XY Using Vysis DNAprobes FISH analysis was positive for IGH break apart andCCND1IGH fusion gene rearrangements in approximately80 of cells examined indicating a t(1114) The presence ofan extra 31015840 signal for IGH corresponded to the finding of anextra fusion signal found in a proportion of cells examinedfor the CCND1IGH gene rearrangement (461) furthersupporting the presence of a t(1114) FISH analysis was alsopositive for the loss of D13S319 along with loss of the controlprobe at 13q34 suggesting either a large deletion of the longarm of chromosome 13 or alternatively monosomy 13 FISHanalysis was negative for loss of the TP53 tumor suppressorgene as well as for hyperdiploidy assessed by DNA probesspecific for chromosomes 5 7 and 9 At this point the patientwas felt to have a symptomatic plasma cell myeloma Imme-diately subsequent serum and urine protein electrophoresiswith immunofixation was negative for IgD heavy chains
TPE in conjunction with 6 cycles of cyclophosphamidebortezomib and dexamethasone chemotherapy resulted ina decrease in his IgM and serum viscosity to 1159mgdLand 29 cP respectively with concomitant improvement in hismental status Unfortunately the patient did not achieve adurable response with these treatments and by the seventhcycle of chemotherapy he had an exacerbation of his disease(IgM 5120mgdL and serum viscosity 73 cP) He received 3additional TPE procedures and was subsequently switched totreatment with lenalidomide but this was discontinued afteronly three days of therapy due to development of a skin rashBendamustine therapy was then initiated but once againno clinical response was observed Currently the patient isundergoing a trial of thalidomide
3 Discussion
The rarity of IgDIgM biclonal PCMmay be attributed to thefact that IgD and IgM paraproteins individually are amongthe rarest variants identified even in monoclonal plasma cellmyeloma representing 05 and 2 of cases respectively [2]Furthermore in previous studies biclonality was detectedusing serum or urine protein electrophoresis without directimmunohistochemical visualization of clonal populations[2 5ndash8] In the cases presented in this report routineimmunofixation electrophoresis studies only detected theIgM paraprotein As occurred in Case 1 many laboratoriesas a cost-saving measure due to the rarity of its secretion donot routinely perform immunofixation for IgD once anotherparaprotein is detected possibly leading to underdetection ofan IgD paraprotein If immunofixation for IgD is performedas in Case 2 the lack of detectable IgD secretion by serumprotein electrophoresis may be attributable to the decreasednumber of IgDpositive neoplastic cells when compared to theIgM positive cells or may represent a minimally secretory ornonsecretory clone [1]
These IgDIgM biclonal cases shared some characteristicmorphologic and immunophenotypic features which bothraised and resolved a differential diagnostic considerationBoth cases displayed lymphoplasmacytic morphology andprominent Dutcher and Russell bodies The lymphoplasma-cyticmorphology in these cases leads to a potential diagnosticdilemma The phenomenon of biclonal gammopathy is notrestricted to plasma cell neoplasms as other B-cell lymphomawith plasmacytic differentiation can produce paraproteinswhich on occasion can result in biclonal gammopathy [10]Lymphoplasmacytic lymphoma the prototypic lymphomawith plasmacytic differentiation has been reported to presentwith biclonal gammopathy including IgDwith IgM [11 12] Inthe light of the overlapping morphologic features and serummonoclonal paraproteins it may be difficult to separateIgDIgM plasma cell myeloma from a B-cell lymphomawith plasmacytic differentiation however this distinctionis extremely important given the differences in how these
4 Case Reports in Hematology
(a) (b) (c)
Figure 2 Case 2 (a) Bone marrow aspirate reveals large numbers of mature-appearing plasma cells with lymphoplasmacytoid morphologysome ofwhich containDutcher bodies and cytoplasmic immunoglobulin inclusions (b) Immunohistochemical studies on the trephine biopsydemonstrate that almost all cells express IgM some with Dutcher bodies (c) A subset of cells also express IgD but at a weaker intensity thanthose expressing IgM Wright-Giemsa original magnification times1000 (a) IgM original magnification times500 (b) IgD original magnificationtimes500 (c)
two entities are currently treated Fortunately in additionto an immunoprofile characteristic of plasma cell myeloma(diffuse positivity for CD138 negativity of CD19 and dimto negative expression for CD45) both cases demonstratedcyclin D1 expression which while characteristic of mantlecell lymphoma and hairy cell leukemia is not a feature ofB-cell lymphoma that commonly shows plasmacytic differ-entiation such as lymphoplasmacytic lymphoma [10] CyclinD1 expression is found in a subset of plasma cell myelomasespecially those with lymphoplasmacytic morphology [13]Although the finding of cyclin D1 expression in both casesis interesting it was only related to a t(1114) in Case 2 sug-gesting other mechanisms besides the rearrangement of theCCND1 gene for its overexpression This observation is inline with prior studies which show a high incidence oft(1114) reported in IgE IgM and non-secretory plasma cellmyelomas but not IgD myeloma [14]
In summary these two cases illustrate that PCM mayrarely exhibit biclonal expression of IgD and IgM heavychains a fact of which hematologists and hematopathologistsshould be aware As the expression of IgD and IgM is morecharacteristic of B-cell lymphoma particularly those thatmay be associated with Waldenstromrsquos macroglobulinemiasuch as lymphoplasmacytic lymphoma a diagnostic dilemmaexists Paraffin section immunohistochemistry is an essentialancillary study as serum protein electrophoresis may misscases with biclonality Clinically both of our cases werechemotherapy-resistant suggestive of more aggressive clin-ical courses however it is difficult to characterize the clinicalbehavior of IgDIgM PCM based on this small sample sizeWith the increased awareness of this entity additional datawill expectedly emerge and provide better characterizationof the clinicopathologic features and behavior of this raredisease
Conflict of Interests
The authors declare no conflict of interests
Authorsrsquo Contribution
ZhongchuanW Chen and Ioanna Kotsikogianni contributedequally in the preparation of this paper and are cofirstauthors
References
[1] International Agency for Research onCancer andWorldHealthOrganization WHO Classification of Tumours of Haematopoi-etic and Lymphoid Tissues International Agency for Researchon Cancer Lyon France 4th edition 2008
[2] R A Kyle M A Gertz T E Witzig et al ldquoReview of 1027patients with newly diagnosed multiple myelomardquoMayo ClinicProceedings vol 78 no 1 pp 21ndash33 2003
[3] N Juge-Morineau C Heirman M Bakkus et al ldquoImmuno-globulins D and M multiple myeloma variants are heavilymutatedrdquo Clinical Cancer Research vol 3 no 12 pp 2501ndash25061997
[4] D E Reece DHVesole S Shrestha et al ldquoOutcome of patientswith IgD and IgM multiple myeloma undergoing autologoushematopoietic stem cell transplantation a retrospective cibmtrstudyrdquo Clinical Lymphoma Myeloma and Leukemia vol 10 no6 pp 458ndash463 2010
[5] A R Huppmann M-L Liu and V E Nava ldquoConcurrent diag-noses of Hodgkin lymphoma and biclonal myeloma in the bonemarrowrdquo Annals of Diagnostic Pathology vol 14 no 4 pp 268ndash272 2010
[6] R A Kyle R A Robinson and J A Katzmann ldquoThe clinicalaspects of biclonal gammopathies review of 57 casesrdquo TheAmerican Journal of Medicine vol 71 no 6 pp 999ndash1008 1981
[7] N Y Kim S J Gong J Kim SM Youn and J-A Lee ldquoMultiplemyeloma with biclonal gammopathy accompanied by prostatecancerrdquoKorean Journal of LaboratoryMedicine vol 31 no 4 pp285ndash289 2011
[8] P Franck N Petitpain A P Guerci S Denisart C Jacob andJ L Gueant ldquoMyeloma with two monoclonal IgG and IgD inserum a case reportrdquo Acta Haematologica vol 92 no 3 pp144ndash147 1994
Case Reports in Hematology 5
[9] A M Tharp R D Woodruff and Z K Shihabi ldquoIgD-Kappamyeloma an unusual caserdquo Annals of Clinical and LaboratoryScience vol 33 no 1 pp 97ndash100 2003
[10] P Lin T J Molina J R Cook and S H Swerdlow ldquoLym-phoplasmacytic lymphoma and other non-marginal zone lym-phomaswith plasmacytic differentiationrdquoTheAmerican Journalof Clinical Pathology vol 136 no 2 pp 195ndash210 2011
[11] J Kriangkum B J Taylor S P Treon et al ldquoMolecular char-acterization of Waldenstromrsquos macroglobulinemia reveals fre-quent occurrence of two B-cell clones having distinct IgH VDJsequencesrdquo Clinical Cancer Research vol 13 no 7 pp 2005ndash2013 2007
[12] GDrsquoAngelo G Crovetti N Grizzetti andCGiardini ldquoBiclonalcomponent in lymphoplasmacyticlymphoplasmacytoid non-Hodgkin lymphomardquo Recenti Progressi in Medicina vol 85 no2 pp 104ndash107 1994
[13] R Fonseca E A Blood M M Oken et al ldquoMyeloma andthe t(1114)(q13q32) evidence for a biologically defined uniquesubset of patientsrdquo Blood vol 99 no 10 pp 3735ndash3741 2002
[14] H Avet-Loiseau R Garand L Lode J-L Harousseau and RBataille ldquoTranslocation t(1114)(q13q32) is the hallmark of IgMIgE and nonsecretory multiple myeloma variantsrdquo Blood vol101 no 4 pp 1570ndash1571 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Case Reports in Hematology
body identified Flow cytometry performed on the aspiratespecimen demonstrated that the CD138 positive plasma cellswere CD56 positive and exhibited surface and cytoplas-mic lambda light chain restriction Flow cytometric stud-ies did not identify an abnormal B-lymphoid populationImmunohistochemistry performed on paraffin embeddedsections of the bone marrow biopsy revealed the neoplas-tic cells to be CD138 positive CD20 negative IgM heavychain positive (Figure 1(a)) and lambda light chain restrictedInterestingly a subset of these cells expressed IgDheavy chain(Figure 1(b)) and cyclin D1 None of the cells expressed IgAor IgG Fluorescence in-situ hybridization (FISH) analysisfor CCND1IGH fusion indicating a t(1114) was negative in99 of the cells using Vysis DNA probes (Abbott MolecularInc Des Plaines IL USA) Following the bone marrowbiopsy serum protein electrophoresis demonstrated a mon-oclonal peak in the beta region (14 gdL) with immunofix-ation confirming an IgM-lambda monoclonal gammopa-thy Immunofixation for IgD was not assessed Biochemicalanalysis revealed a borderline low ionized calcium level(093mmolL reference range 10ndash14mmolL) and normalblood urea nitrogen and creatinine levels No lytic lesionswere observed by radiographic imaging At this point theneoplasm was best considered asymptomatic (smoldering)myeloma as the patient had more than 10 clonal plasmacells in the bone marrow but no organ or tissue impair-ment was attributed to the neoplasm Three months laterthe patient underwent a second surveillance bone marrowbiopsy This time the morphology of the neoplastic cells wasevaluable on the marrow aspirate smear and was ldquolymphop-lasmacytoidrdquo (Figure 1(c)) The neoplastic cells accountedfor 35 of the total cellularity based on the marrow aspi-rate smear differential Immunohistochemistry was not per-formed on the bone marrow biopsy but flow cytometricstudies confirmed the persistent CD138 positive and CD56positive lambda monoclonal plasma cell population that wasnegative for CD19 and CD20 Since his serum IgM levelwas elevated to 4660mgdL (reference range 40ndash230mgdL)with depression of IgA and IgG levels he was started ondexamethasone vincristine and doxorubicin however thistherapy did not decrease IgM levels and he was switchedto a thalidomidedexamethasone regimen The dexametha-sone was stopped eight months later due to uncontrollablehyperglycemia He was continued on the thalidomide andhis IgM levels decreased to 2270mgdL and appeared stableHowever within three months his IgM levels increased to3420mgdL and thalidomide was discontinued A third bonemarrow biopsy at this time demonstrated persistent diseasewith neoplastic plasma cells accounting for 23 of the totalcellularity based on the marrow aspirate differential Serumprotein electrophoresis continued to exhibit an IgM-lambdamonoclonal protein (017 gdL) as well as a second nonquan-tifiable free lambda light chain protein At this time nowtwo years after his initial diagnosis the patient underwenthigh dose melphalan autologous peripheral blood stem celltransplantation
A fourth bone marrow biopsy performed one yearlater demonstrated disease progression with 50 neoplasticplasma cells based on manual marrow aspirate differential
and 12 plasma cells in the peripheral blood At this timehe was started on lenalidomide but unfortunately the newtherapy was not tolerated A subsequent bonemarrow biopsythree months later demonstrated continued progression with82 plasma cells At this point there was also an evolution toplasma cell leukemia evidenced by 28 circulating plasmacells Within six months he underwent a second autologousperipheral blood stem cell transplantation complicated bypancytopenia requiring growth factor support and red bloodcell and platelet transfusions The transplantation was ulti-mately unsuccessful and his plasma cell leukemia despitereinitiation of lenalidomide and dexamethasone persistedHis clinical course was complicated by lower extremitycellulitis Klebsiella pneumoniae sepsis and uncontrollablehematuria and the patient died 4 years and 4 months afterhis initial diagnosis with persistent PCM
22 Case 2 A 71-year-old male presented with altered men-tal status and was initially diagnosed with streptococcalpneumonia sepsis and left lower extremity deep venousthrombosis Peripheral blood examination revealed ane-mia (hemoglobin 78 gdL reference range 129ndash169 gdL)with 9 plasma cells and significant rouleaux forma-tion Quantitative immunoglobulin determination showed amarked increase in IgM (7655mgdL reference range 40ndash274mgdL) Serum protein electrophoresis with immunofix-ation revealedmonoclonal IgM-kappaM-protein (534 gdL)Urine protein electrophoresis demonstrated the presence oftwo monoclonal spikes in the gamma region (1328mgdLand 10469mgdL) and immunofixation performed on theurine demonstrated a kappa light chain not associated withIgA IgG or IgM heavy chains CT scan of the abdomenand pelvis displayed neither lymphadenopathy nor hep-atosplenomegaly and a radiographic skeletal survey wasnegative for lytic lesions Due to the patientrsquos deterioratingclinical status which included worsening altered mentalstatus attributed to hyperviscosity (serumviscosity 88 cP ref-erence range 14ndash18 cP) from elevated IgM a course oftherapeutic plasma exchange (TPE) was initiated Ten 15volume TPE procedures with 5 albumin replacement wereperformed over a 20-day period to reduce IgM levels andimprove cognitive impairment Due to clinical suspicion forWaldenstrommacroglobulinemia a bonemarrow evaluationwas performed
The peripheral blood demonstrated rouleaux formationas well as circulating plasma cells some with cytoplas-mic immunoglobulin inclusions (Russell bodies) The mar-row aspirate smears contained numerous plasma cells withnumerous Dutcher bodies and Russell bodies as well as lym-phoplasmacytic morphology (Figure 2(a))The bonemarrowbiopsy demonstrated hypercellular marrow for the patientrsquosage that was extensively replaced by an infiltrate of predom-inantly mature-appearing plasma cells some of which werebinucleated and containing Dutcher bodies that accountedfor 95of the total cellularity on the core biopsy Flow cytom-etry confirmed the presence of a population CD138 positiveCD38 positive CD20 partially positive CD19 negative CD56negative and cytoplasmic kappa light chain restricted plasmacells with no abnormal B-lymphoid population identified
Case Reports in Hematology 3
(a) (b) (c)
Figure 1 Case 1 (a) Biopsy from initial sample demonstrating that the majority of cells express IgM (b) A subset of cells express IgD (c)Aspirate smear of second pretreatment marrow evaluation Immunohistochemistry oil objective original magnification times500 ((a) and (b))Wright-Giemsa oil objective original magnification times1000 (c)
Immunohistochemistry performed on paraffin sections ofthe core biopsy demonstrated the neoplastic plasma cells tobe diffusely positive for IgM (Figure 2(b)) and a subset thatwas weakly positive for IgD (Figure 2(c)) Interestingly theareas with increased IgD positive cells were also CD20positive Cyclin D1 was positive on many of the plasmacells but highlighted fewer plasma cells as compared toIgM Conventional G-band karyotyping of the bone marrowrevealed a normal male karyotype 46 XY Using Vysis DNAprobes FISH analysis was positive for IGH break apart andCCND1IGH fusion gene rearrangements in approximately80 of cells examined indicating a t(1114) The presence ofan extra 31015840 signal for IGH corresponded to the finding of anextra fusion signal found in a proportion of cells examinedfor the CCND1IGH gene rearrangement (461) furthersupporting the presence of a t(1114) FISH analysis was alsopositive for the loss of D13S319 along with loss of the controlprobe at 13q34 suggesting either a large deletion of the longarm of chromosome 13 or alternatively monosomy 13 FISHanalysis was negative for loss of the TP53 tumor suppressorgene as well as for hyperdiploidy assessed by DNA probesspecific for chromosomes 5 7 and 9 At this point the patientwas felt to have a symptomatic plasma cell myeloma Imme-diately subsequent serum and urine protein electrophoresiswith immunofixation was negative for IgD heavy chains
TPE in conjunction with 6 cycles of cyclophosphamidebortezomib and dexamethasone chemotherapy resulted ina decrease in his IgM and serum viscosity to 1159mgdLand 29 cP respectively with concomitant improvement in hismental status Unfortunately the patient did not achieve adurable response with these treatments and by the seventhcycle of chemotherapy he had an exacerbation of his disease(IgM 5120mgdL and serum viscosity 73 cP) He received 3additional TPE procedures and was subsequently switched totreatment with lenalidomide but this was discontinued afteronly three days of therapy due to development of a skin rashBendamustine therapy was then initiated but once againno clinical response was observed Currently the patient isundergoing a trial of thalidomide
3 Discussion
The rarity of IgDIgM biclonal PCMmay be attributed to thefact that IgD and IgM paraproteins individually are amongthe rarest variants identified even in monoclonal plasma cellmyeloma representing 05 and 2 of cases respectively [2]Furthermore in previous studies biclonality was detectedusing serum or urine protein electrophoresis without directimmunohistochemical visualization of clonal populations[2 5ndash8] In the cases presented in this report routineimmunofixation electrophoresis studies only detected theIgM paraprotein As occurred in Case 1 many laboratoriesas a cost-saving measure due to the rarity of its secretion donot routinely perform immunofixation for IgD once anotherparaprotein is detected possibly leading to underdetection ofan IgD paraprotein If immunofixation for IgD is performedas in Case 2 the lack of detectable IgD secretion by serumprotein electrophoresis may be attributable to the decreasednumber of IgDpositive neoplastic cells when compared to theIgM positive cells or may represent a minimally secretory ornonsecretory clone [1]
These IgDIgM biclonal cases shared some characteristicmorphologic and immunophenotypic features which bothraised and resolved a differential diagnostic considerationBoth cases displayed lymphoplasmacytic morphology andprominent Dutcher and Russell bodies The lymphoplasma-cyticmorphology in these cases leads to a potential diagnosticdilemma The phenomenon of biclonal gammopathy is notrestricted to plasma cell neoplasms as other B-cell lymphomawith plasmacytic differentiation can produce paraproteinswhich on occasion can result in biclonal gammopathy [10]Lymphoplasmacytic lymphoma the prototypic lymphomawith plasmacytic differentiation has been reported to presentwith biclonal gammopathy including IgDwith IgM [11 12] Inthe light of the overlapping morphologic features and serummonoclonal paraproteins it may be difficult to separateIgDIgM plasma cell myeloma from a B-cell lymphomawith plasmacytic differentiation however this distinctionis extremely important given the differences in how these
4 Case Reports in Hematology
(a) (b) (c)
Figure 2 Case 2 (a) Bone marrow aspirate reveals large numbers of mature-appearing plasma cells with lymphoplasmacytoid morphologysome ofwhich containDutcher bodies and cytoplasmic immunoglobulin inclusions (b) Immunohistochemical studies on the trephine biopsydemonstrate that almost all cells express IgM some with Dutcher bodies (c) A subset of cells also express IgD but at a weaker intensity thanthose expressing IgM Wright-Giemsa original magnification times1000 (a) IgM original magnification times500 (b) IgD original magnificationtimes500 (c)
two entities are currently treated Fortunately in additionto an immunoprofile characteristic of plasma cell myeloma(diffuse positivity for CD138 negativity of CD19 and dimto negative expression for CD45) both cases demonstratedcyclin D1 expression which while characteristic of mantlecell lymphoma and hairy cell leukemia is not a feature ofB-cell lymphoma that commonly shows plasmacytic differ-entiation such as lymphoplasmacytic lymphoma [10] CyclinD1 expression is found in a subset of plasma cell myelomasespecially those with lymphoplasmacytic morphology [13]Although the finding of cyclin D1 expression in both casesis interesting it was only related to a t(1114) in Case 2 sug-gesting other mechanisms besides the rearrangement of theCCND1 gene for its overexpression This observation is inline with prior studies which show a high incidence oft(1114) reported in IgE IgM and non-secretory plasma cellmyelomas but not IgD myeloma [14]
In summary these two cases illustrate that PCM mayrarely exhibit biclonal expression of IgD and IgM heavychains a fact of which hematologists and hematopathologistsshould be aware As the expression of IgD and IgM is morecharacteristic of B-cell lymphoma particularly those thatmay be associated with Waldenstromrsquos macroglobulinemiasuch as lymphoplasmacytic lymphoma a diagnostic dilemmaexists Paraffin section immunohistochemistry is an essentialancillary study as serum protein electrophoresis may misscases with biclonality Clinically both of our cases werechemotherapy-resistant suggestive of more aggressive clin-ical courses however it is difficult to characterize the clinicalbehavior of IgDIgM PCM based on this small sample sizeWith the increased awareness of this entity additional datawill expectedly emerge and provide better characterizationof the clinicopathologic features and behavior of this raredisease
Conflict of Interests
The authors declare no conflict of interests
Authorsrsquo Contribution
ZhongchuanW Chen and Ioanna Kotsikogianni contributedequally in the preparation of this paper and are cofirstauthors
References
[1] International Agency for Research onCancer andWorldHealthOrganization WHO Classification of Tumours of Haematopoi-etic and Lymphoid Tissues International Agency for Researchon Cancer Lyon France 4th edition 2008
[2] R A Kyle M A Gertz T E Witzig et al ldquoReview of 1027patients with newly diagnosed multiple myelomardquoMayo ClinicProceedings vol 78 no 1 pp 21ndash33 2003
[3] N Juge-Morineau C Heirman M Bakkus et al ldquoImmuno-globulins D and M multiple myeloma variants are heavilymutatedrdquo Clinical Cancer Research vol 3 no 12 pp 2501ndash25061997
[4] D E Reece DHVesole S Shrestha et al ldquoOutcome of patientswith IgD and IgM multiple myeloma undergoing autologoushematopoietic stem cell transplantation a retrospective cibmtrstudyrdquo Clinical Lymphoma Myeloma and Leukemia vol 10 no6 pp 458ndash463 2010
[5] A R Huppmann M-L Liu and V E Nava ldquoConcurrent diag-noses of Hodgkin lymphoma and biclonal myeloma in the bonemarrowrdquo Annals of Diagnostic Pathology vol 14 no 4 pp 268ndash272 2010
[6] R A Kyle R A Robinson and J A Katzmann ldquoThe clinicalaspects of biclonal gammopathies review of 57 casesrdquo TheAmerican Journal of Medicine vol 71 no 6 pp 999ndash1008 1981
[7] N Y Kim S J Gong J Kim SM Youn and J-A Lee ldquoMultiplemyeloma with biclonal gammopathy accompanied by prostatecancerrdquoKorean Journal of LaboratoryMedicine vol 31 no 4 pp285ndash289 2011
[8] P Franck N Petitpain A P Guerci S Denisart C Jacob andJ L Gueant ldquoMyeloma with two monoclonal IgG and IgD inserum a case reportrdquo Acta Haematologica vol 92 no 3 pp144ndash147 1994
Case Reports in Hematology 5
[9] A M Tharp R D Woodruff and Z K Shihabi ldquoIgD-Kappamyeloma an unusual caserdquo Annals of Clinical and LaboratoryScience vol 33 no 1 pp 97ndash100 2003
[10] P Lin T J Molina J R Cook and S H Swerdlow ldquoLym-phoplasmacytic lymphoma and other non-marginal zone lym-phomaswith plasmacytic differentiationrdquoTheAmerican Journalof Clinical Pathology vol 136 no 2 pp 195ndash210 2011
[11] J Kriangkum B J Taylor S P Treon et al ldquoMolecular char-acterization of Waldenstromrsquos macroglobulinemia reveals fre-quent occurrence of two B-cell clones having distinct IgH VDJsequencesrdquo Clinical Cancer Research vol 13 no 7 pp 2005ndash2013 2007
[12] GDrsquoAngelo G Crovetti N Grizzetti andCGiardini ldquoBiclonalcomponent in lymphoplasmacyticlymphoplasmacytoid non-Hodgkin lymphomardquo Recenti Progressi in Medicina vol 85 no2 pp 104ndash107 1994
[13] R Fonseca E A Blood M M Oken et al ldquoMyeloma andthe t(1114)(q13q32) evidence for a biologically defined uniquesubset of patientsrdquo Blood vol 99 no 10 pp 3735ndash3741 2002
[14] H Avet-Loiseau R Garand L Lode J-L Harousseau and RBataille ldquoTranslocation t(1114)(q13q32) is the hallmark of IgMIgE and nonsecretory multiple myeloma variantsrdquo Blood vol101 no 4 pp 1570ndash1571 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Hematology 3
(a) (b) (c)
Figure 1 Case 1 (a) Biopsy from initial sample demonstrating that the majority of cells express IgM (b) A subset of cells express IgD (c)Aspirate smear of second pretreatment marrow evaluation Immunohistochemistry oil objective original magnification times500 ((a) and (b))Wright-Giemsa oil objective original magnification times1000 (c)
Immunohistochemistry performed on paraffin sections ofthe core biopsy demonstrated the neoplastic plasma cells tobe diffusely positive for IgM (Figure 2(b)) and a subset thatwas weakly positive for IgD (Figure 2(c)) Interestingly theareas with increased IgD positive cells were also CD20positive Cyclin D1 was positive on many of the plasmacells but highlighted fewer plasma cells as compared toIgM Conventional G-band karyotyping of the bone marrowrevealed a normal male karyotype 46 XY Using Vysis DNAprobes FISH analysis was positive for IGH break apart andCCND1IGH fusion gene rearrangements in approximately80 of cells examined indicating a t(1114) The presence ofan extra 31015840 signal for IGH corresponded to the finding of anextra fusion signal found in a proportion of cells examinedfor the CCND1IGH gene rearrangement (461) furthersupporting the presence of a t(1114) FISH analysis was alsopositive for the loss of D13S319 along with loss of the controlprobe at 13q34 suggesting either a large deletion of the longarm of chromosome 13 or alternatively monosomy 13 FISHanalysis was negative for loss of the TP53 tumor suppressorgene as well as for hyperdiploidy assessed by DNA probesspecific for chromosomes 5 7 and 9 At this point the patientwas felt to have a symptomatic plasma cell myeloma Imme-diately subsequent serum and urine protein electrophoresiswith immunofixation was negative for IgD heavy chains
TPE in conjunction with 6 cycles of cyclophosphamidebortezomib and dexamethasone chemotherapy resulted ina decrease in his IgM and serum viscosity to 1159mgdLand 29 cP respectively with concomitant improvement in hismental status Unfortunately the patient did not achieve adurable response with these treatments and by the seventhcycle of chemotherapy he had an exacerbation of his disease(IgM 5120mgdL and serum viscosity 73 cP) He received 3additional TPE procedures and was subsequently switched totreatment with lenalidomide but this was discontinued afteronly three days of therapy due to development of a skin rashBendamustine therapy was then initiated but once againno clinical response was observed Currently the patient isundergoing a trial of thalidomide
3 Discussion
The rarity of IgDIgM biclonal PCMmay be attributed to thefact that IgD and IgM paraproteins individually are amongthe rarest variants identified even in monoclonal plasma cellmyeloma representing 05 and 2 of cases respectively [2]Furthermore in previous studies biclonality was detectedusing serum or urine protein electrophoresis without directimmunohistochemical visualization of clonal populations[2 5ndash8] In the cases presented in this report routineimmunofixation electrophoresis studies only detected theIgM paraprotein As occurred in Case 1 many laboratoriesas a cost-saving measure due to the rarity of its secretion donot routinely perform immunofixation for IgD once anotherparaprotein is detected possibly leading to underdetection ofan IgD paraprotein If immunofixation for IgD is performedas in Case 2 the lack of detectable IgD secretion by serumprotein electrophoresis may be attributable to the decreasednumber of IgDpositive neoplastic cells when compared to theIgM positive cells or may represent a minimally secretory ornonsecretory clone [1]
These IgDIgM biclonal cases shared some characteristicmorphologic and immunophenotypic features which bothraised and resolved a differential diagnostic considerationBoth cases displayed lymphoplasmacytic morphology andprominent Dutcher and Russell bodies The lymphoplasma-cyticmorphology in these cases leads to a potential diagnosticdilemma The phenomenon of biclonal gammopathy is notrestricted to plasma cell neoplasms as other B-cell lymphomawith plasmacytic differentiation can produce paraproteinswhich on occasion can result in biclonal gammopathy [10]Lymphoplasmacytic lymphoma the prototypic lymphomawith plasmacytic differentiation has been reported to presentwith biclonal gammopathy including IgDwith IgM [11 12] Inthe light of the overlapping morphologic features and serummonoclonal paraproteins it may be difficult to separateIgDIgM plasma cell myeloma from a B-cell lymphomawith plasmacytic differentiation however this distinctionis extremely important given the differences in how these
4 Case Reports in Hematology
(a) (b) (c)
Figure 2 Case 2 (a) Bone marrow aspirate reveals large numbers of mature-appearing plasma cells with lymphoplasmacytoid morphologysome ofwhich containDutcher bodies and cytoplasmic immunoglobulin inclusions (b) Immunohistochemical studies on the trephine biopsydemonstrate that almost all cells express IgM some with Dutcher bodies (c) A subset of cells also express IgD but at a weaker intensity thanthose expressing IgM Wright-Giemsa original magnification times1000 (a) IgM original magnification times500 (b) IgD original magnificationtimes500 (c)
two entities are currently treated Fortunately in additionto an immunoprofile characteristic of plasma cell myeloma(diffuse positivity for CD138 negativity of CD19 and dimto negative expression for CD45) both cases demonstratedcyclin D1 expression which while characteristic of mantlecell lymphoma and hairy cell leukemia is not a feature ofB-cell lymphoma that commonly shows plasmacytic differ-entiation such as lymphoplasmacytic lymphoma [10] CyclinD1 expression is found in a subset of plasma cell myelomasespecially those with lymphoplasmacytic morphology [13]Although the finding of cyclin D1 expression in both casesis interesting it was only related to a t(1114) in Case 2 sug-gesting other mechanisms besides the rearrangement of theCCND1 gene for its overexpression This observation is inline with prior studies which show a high incidence oft(1114) reported in IgE IgM and non-secretory plasma cellmyelomas but not IgD myeloma [14]
In summary these two cases illustrate that PCM mayrarely exhibit biclonal expression of IgD and IgM heavychains a fact of which hematologists and hematopathologistsshould be aware As the expression of IgD and IgM is morecharacteristic of B-cell lymphoma particularly those thatmay be associated with Waldenstromrsquos macroglobulinemiasuch as lymphoplasmacytic lymphoma a diagnostic dilemmaexists Paraffin section immunohistochemistry is an essentialancillary study as serum protein electrophoresis may misscases with biclonality Clinically both of our cases werechemotherapy-resistant suggestive of more aggressive clin-ical courses however it is difficult to characterize the clinicalbehavior of IgDIgM PCM based on this small sample sizeWith the increased awareness of this entity additional datawill expectedly emerge and provide better characterizationof the clinicopathologic features and behavior of this raredisease
Conflict of Interests
The authors declare no conflict of interests
Authorsrsquo Contribution
ZhongchuanW Chen and Ioanna Kotsikogianni contributedequally in the preparation of this paper and are cofirstauthors
References
[1] International Agency for Research onCancer andWorldHealthOrganization WHO Classification of Tumours of Haematopoi-etic and Lymphoid Tissues International Agency for Researchon Cancer Lyon France 4th edition 2008
[2] R A Kyle M A Gertz T E Witzig et al ldquoReview of 1027patients with newly diagnosed multiple myelomardquoMayo ClinicProceedings vol 78 no 1 pp 21ndash33 2003
[3] N Juge-Morineau C Heirman M Bakkus et al ldquoImmuno-globulins D and M multiple myeloma variants are heavilymutatedrdquo Clinical Cancer Research vol 3 no 12 pp 2501ndash25061997
[4] D E Reece DHVesole S Shrestha et al ldquoOutcome of patientswith IgD and IgM multiple myeloma undergoing autologoushematopoietic stem cell transplantation a retrospective cibmtrstudyrdquo Clinical Lymphoma Myeloma and Leukemia vol 10 no6 pp 458ndash463 2010
[5] A R Huppmann M-L Liu and V E Nava ldquoConcurrent diag-noses of Hodgkin lymphoma and biclonal myeloma in the bonemarrowrdquo Annals of Diagnostic Pathology vol 14 no 4 pp 268ndash272 2010
[6] R A Kyle R A Robinson and J A Katzmann ldquoThe clinicalaspects of biclonal gammopathies review of 57 casesrdquo TheAmerican Journal of Medicine vol 71 no 6 pp 999ndash1008 1981
[7] N Y Kim S J Gong J Kim SM Youn and J-A Lee ldquoMultiplemyeloma with biclonal gammopathy accompanied by prostatecancerrdquoKorean Journal of LaboratoryMedicine vol 31 no 4 pp285ndash289 2011
[8] P Franck N Petitpain A P Guerci S Denisart C Jacob andJ L Gueant ldquoMyeloma with two monoclonal IgG and IgD inserum a case reportrdquo Acta Haematologica vol 92 no 3 pp144ndash147 1994
Case Reports in Hematology 5
[9] A M Tharp R D Woodruff and Z K Shihabi ldquoIgD-Kappamyeloma an unusual caserdquo Annals of Clinical and LaboratoryScience vol 33 no 1 pp 97ndash100 2003
[10] P Lin T J Molina J R Cook and S H Swerdlow ldquoLym-phoplasmacytic lymphoma and other non-marginal zone lym-phomaswith plasmacytic differentiationrdquoTheAmerican Journalof Clinical Pathology vol 136 no 2 pp 195ndash210 2011
[11] J Kriangkum B J Taylor S P Treon et al ldquoMolecular char-acterization of Waldenstromrsquos macroglobulinemia reveals fre-quent occurrence of two B-cell clones having distinct IgH VDJsequencesrdquo Clinical Cancer Research vol 13 no 7 pp 2005ndash2013 2007
[12] GDrsquoAngelo G Crovetti N Grizzetti andCGiardini ldquoBiclonalcomponent in lymphoplasmacyticlymphoplasmacytoid non-Hodgkin lymphomardquo Recenti Progressi in Medicina vol 85 no2 pp 104ndash107 1994
[13] R Fonseca E A Blood M M Oken et al ldquoMyeloma andthe t(1114)(q13q32) evidence for a biologically defined uniquesubset of patientsrdquo Blood vol 99 no 10 pp 3735ndash3741 2002
[14] H Avet-Loiseau R Garand L Lode J-L Harousseau and RBataille ldquoTranslocation t(1114)(q13q32) is the hallmark of IgMIgE and nonsecretory multiple myeloma variantsrdquo Blood vol101 no 4 pp 1570ndash1571 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Case Reports in Hematology
(a) (b) (c)
Figure 2 Case 2 (a) Bone marrow aspirate reveals large numbers of mature-appearing plasma cells with lymphoplasmacytoid morphologysome ofwhich containDutcher bodies and cytoplasmic immunoglobulin inclusions (b) Immunohistochemical studies on the trephine biopsydemonstrate that almost all cells express IgM some with Dutcher bodies (c) A subset of cells also express IgD but at a weaker intensity thanthose expressing IgM Wright-Giemsa original magnification times1000 (a) IgM original magnification times500 (b) IgD original magnificationtimes500 (c)
two entities are currently treated Fortunately in additionto an immunoprofile characteristic of plasma cell myeloma(diffuse positivity for CD138 negativity of CD19 and dimto negative expression for CD45) both cases demonstratedcyclin D1 expression which while characteristic of mantlecell lymphoma and hairy cell leukemia is not a feature ofB-cell lymphoma that commonly shows plasmacytic differ-entiation such as lymphoplasmacytic lymphoma [10] CyclinD1 expression is found in a subset of plasma cell myelomasespecially those with lymphoplasmacytic morphology [13]Although the finding of cyclin D1 expression in both casesis interesting it was only related to a t(1114) in Case 2 sug-gesting other mechanisms besides the rearrangement of theCCND1 gene for its overexpression This observation is inline with prior studies which show a high incidence oft(1114) reported in IgE IgM and non-secretory plasma cellmyelomas but not IgD myeloma [14]
In summary these two cases illustrate that PCM mayrarely exhibit biclonal expression of IgD and IgM heavychains a fact of which hematologists and hematopathologistsshould be aware As the expression of IgD and IgM is morecharacteristic of B-cell lymphoma particularly those thatmay be associated with Waldenstromrsquos macroglobulinemiasuch as lymphoplasmacytic lymphoma a diagnostic dilemmaexists Paraffin section immunohistochemistry is an essentialancillary study as serum protein electrophoresis may misscases with biclonality Clinically both of our cases werechemotherapy-resistant suggestive of more aggressive clin-ical courses however it is difficult to characterize the clinicalbehavior of IgDIgM PCM based on this small sample sizeWith the increased awareness of this entity additional datawill expectedly emerge and provide better characterizationof the clinicopathologic features and behavior of this raredisease
Conflict of Interests
The authors declare no conflict of interests
Authorsrsquo Contribution
ZhongchuanW Chen and Ioanna Kotsikogianni contributedequally in the preparation of this paper and are cofirstauthors
References
[1] International Agency for Research onCancer andWorldHealthOrganization WHO Classification of Tumours of Haematopoi-etic and Lymphoid Tissues International Agency for Researchon Cancer Lyon France 4th edition 2008
[2] R A Kyle M A Gertz T E Witzig et al ldquoReview of 1027patients with newly diagnosed multiple myelomardquoMayo ClinicProceedings vol 78 no 1 pp 21ndash33 2003
[3] N Juge-Morineau C Heirman M Bakkus et al ldquoImmuno-globulins D and M multiple myeloma variants are heavilymutatedrdquo Clinical Cancer Research vol 3 no 12 pp 2501ndash25061997
[4] D E Reece DHVesole S Shrestha et al ldquoOutcome of patientswith IgD and IgM multiple myeloma undergoing autologoushematopoietic stem cell transplantation a retrospective cibmtrstudyrdquo Clinical Lymphoma Myeloma and Leukemia vol 10 no6 pp 458ndash463 2010
[5] A R Huppmann M-L Liu and V E Nava ldquoConcurrent diag-noses of Hodgkin lymphoma and biclonal myeloma in the bonemarrowrdquo Annals of Diagnostic Pathology vol 14 no 4 pp 268ndash272 2010
[6] R A Kyle R A Robinson and J A Katzmann ldquoThe clinicalaspects of biclonal gammopathies review of 57 casesrdquo TheAmerican Journal of Medicine vol 71 no 6 pp 999ndash1008 1981
[7] N Y Kim S J Gong J Kim SM Youn and J-A Lee ldquoMultiplemyeloma with biclonal gammopathy accompanied by prostatecancerrdquoKorean Journal of LaboratoryMedicine vol 31 no 4 pp285ndash289 2011
[8] P Franck N Petitpain A P Guerci S Denisart C Jacob andJ L Gueant ldquoMyeloma with two monoclonal IgG and IgD inserum a case reportrdquo Acta Haematologica vol 92 no 3 pp144ndash147 1994
Case Reports in Hematology 5
[9] A M Tharp R D Woodruff and Z K Shihabi ldquoIgD-Kappamyeloma an unusual caserdquo Annals of Clinical and LaboratoryScience vol 33 no 1 pp 97ndash100 2003
[10] P Lin T J Molina J R Cook and S H Swerdlow ldquoLym-phoplasmacytic lymphoma and other non-marginal zone lym-phomaswith plasmacytic differentiationrdquoTheAmerican Journalof Clinical Pathology vol 136 no 2 pp 195ndash210 2011
[11] J Kriangkum B J Taylor S P Treon et al ldquoMolecular char-acterization of Waldenstromrsquos macroglobulinemia reveals fre-quent occurrence of two B-cell clones having distinct IgH VDJsequencesrdquo Clinical Cancer Research vol 13 no 7 pp 2005ndash2013 2007
[12] GDrsquoAngelo G Crovetti N Grizzetti andCGiardini ldquoBiclonalcomponent in lymphoplasmacyticlymphoplasmacytoid non-Hodgkin lymphomardquo Recenti Progressi in Medicina vol 85 no2 pp 104ndash107 1994
[13] R Fonseca E A Blood M M Oken et al ldquoMyeloma andthe t(1114)(q13q32) evidence for a biologically defined uniquesubset of patientsrdquo Blood vol 99 no 10 pp 3735ndash3741 2002
[14] H Avet-Loiseau R Garand L Lode J-L Harousseau and RBataille ldquoTranslocation t(1114)(q13q32) is the hallmark of IgMIgE and nonsecretory multiple myeloma variantsrdquo Blood vol101 no 4 pp 1570ndash1571 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Hematology 5
[9] A M Tharp R D Woodruff and Z K Shihabi ldquoIgD-Kappamyeloma an unusual caserdquo Annals of Clinical and LaboratoryScience vol 33 no 1 pp 97ndash100 2003
[10] P Lin T J Molina J R Cook and S H Swerdlow ldquoLym-phoplasmacytic lymphoma and other non-marginal zone lym-phomaswith plasmacytic differentiationrdquoTheAmerican Journalof Clinical Pathology vol 136 no 2 pp 195ndash210 2011
[11] J Kriangkum B J Taylor S P Treon et al ldquoMolecular char-acterization of Waldenstromrsquos macroglobulinemia reveals fre-quent occurrence of two B-cell clones having distinct IgH VDJsequencesrdquo Clinical Cancer Research vol 13 no 7 pp 2005ndash2013 2007
[12] GDrsquoAngelo G Crovetti N Grizzetti andCGiardini ldquoBiclonalcomponent in lymphoplasmacyticlymphoplasmacytoid non-Hodgkin lymphomardquo Recenti Progressi in Medicina vol 85 no2 pp 104ndash107 1994
[13] R Fonseca E A Blood M M Oken et al ldquoMyeloma andthe t(1114)(q13q32) evidence for a biologically defined uniquesubset of patientsrdquo Blood vol 99 no 10 pp 3735ndash3741 2002
[14] H Avet-Loiseau R Garand L Lode J-L Harousseau and RBataille ldquoTranslocation t(1114)(q13q32) is the hallmark of IgMIgE and nonsecretory multiple myeloma variantsrdquo Blood vol101 no 4 pp 1570ndash1571 2003
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom