CASE REPORT - Bentham Science Publishers
5
Transcript of CASE REPORT - Bentham Science Publishers

0250-6882/20 Send Orders for Reprints to [email protected]
57
DOI: 10.2174/0250688202002022001, 2020, 1(2), 57-60
New Emirates Medical JournalContent list available at: https://newemiratesmedicaljournal.com
CASE REPORT
A Case of 2:1 Atrio-Ventricular Block- Unraveled by Exercise Testing
Sharada S. Kalavakolanu1,*, Madan M. Balakrishnan1 and Deepesh Venkataraman1
1Department of Cardiology, MGM Healthcare, Aminjikarai, Chennai, Tamilnadu, India
Abstract:
We present a case of a 75-year-old lady with effort intolerance and baseline ECG showing 2:1 atrioventricular block, in whom it was unclear as tothe requirement of permanent pacing, even after long term ECG monitoring. She underwent a treadmill test during which her QRS became wideand developed complete heart block within 2 minutes of the test. Thus, a simple exercise test confirmed the level of the block to be infra nodalwithout the need for the invasive study. In patients with exertional symptoms, even in elderly, and in those where ECG masquerades as a benignentity, exercise testing is useful to differentiate benign cases of atrioventricular block from the more serious cases that mandate pacemakerimplantation.
Keywords: Atrioventricular block, Complete heart block, Exercise test, Intra-Hisian block, Infra nodal, Coronary angiogram.
Article History Received: October 17, 2019 Revised: February 01, 2020 Accepted: February 10, 2020
1. INTRODUCTION
Intra-Hisian atrio-ventricular (AV) block associated with2:1 conduction is an uncommon phenomenon, but it isimportant for the development of complete AV block [1]. A2:1 Atrio-Ventricular (AV) block with narrow QRS complexes,presents a diagnostic challenge as to the level of block, whethera benign entity of Mobitz Type I (Wenckebach) or moresinister form of Mobitz Type 2 block necessitating permanentpacing. This confirmation usually requires invasive workup ofthe cardiac conduction system by an electrophysiologicalstudy. We discuss a case of an elderly lady with exertionalbreathlessness presenting with 2:1 AV block having narrowQRS conducted beats, in whom a simple exercise testunraveled site of the block to be within the His bundleconfirming the requirement for permanent pacing.
1.1. Patient Information
A 75-year old lady presented to the cardiology services ofour hospital with complaints of exertional dyspnea and fatigueof 6 months duration, progressively limiting her activities butwas comfortable at rest. She was a known hypertensive for thepast 10 years on dihydropyridine calcium-channel blocker -amlodipine, 5mg once daily with fair control of her bloodpressures.
* Address correspondence to this author at the Department of Cardiology MGMHealthcare, Nelson Manickam Road, Aminjikarai, Chennai, Tamilnadu, 600029,India; Tel: +91 44 45242444; E-mail: [email protected]
1.2. Diagnostic Assessment
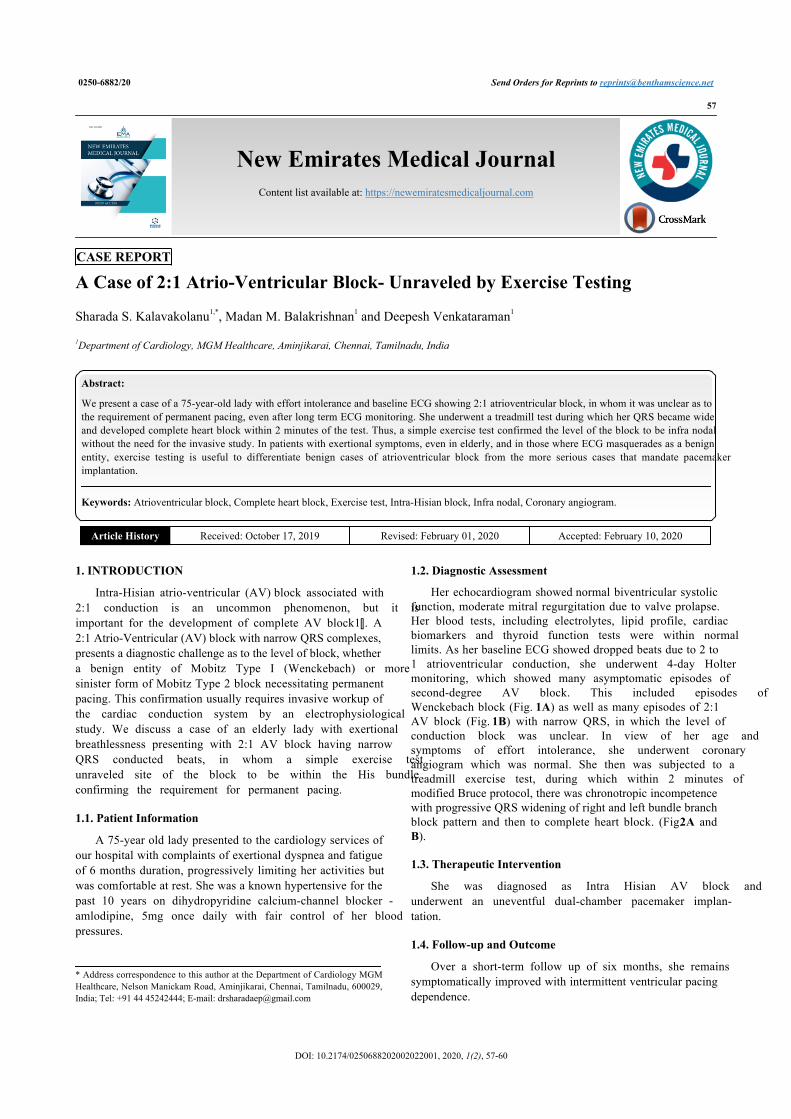
Her echocardiogram showed normal biventricular systolicfunction, moderate mitral regurgitation due to valve prolapse.Her blood tests, including electrolytes, lipid profile, cardiacbiomarkers and thyroid function tests were within normallimits. As her baseline ECG showed dropped beats due to 2 to1 atrioventricular conduction, she underwent 4-day Holtermonitoring, which showed many asymptomatic episodes ofsecond-degree AV block. This included episodes ofWenckebach block (Fig. 1A) as well as many episodes of 2:1AV block (Fig. 1B) with narrow QRS, in which the level ofconduction block was unclear. In view of her age andsymptoms of effort intolerance, she underwent coronaryangiogram which was normal. She then was subjected to atreadmill exercise test, during which within 2 minutes ofmodified Bruce protocol, there was chronotropic incompetencewith progressive QRS widening of right and left bundle branchblock pattern and then to complete heart block. (Fig. 2A andB).
1.3. Therapeutic Intervention
She was diagnosed as Intra Hisian AV block andunderwent an uneventful dual-chamber pacemaker implan-tation.
1.4. Follow-up and Outcome
Over a short-term follow up of six months, she remainssymptomatically improved with intermittent ventricular pacingdependence.
58 Kalavakolanu et al.
Fig. (1A). Holter showing second degree, mobitz type 1 atrio-ventricular block.
Fig. (1B). Holter showing 2:1 AV block.
Fig. (2A). Exercise testing 2min: Widened QRS with right bundle block and left bundle block pattern.
���� �� ����� !���"#
���� � ���� � ���� � ����
$% &%�&"%
'" &��&$$
$� &��&'$
$�
�(��)#
�%��)��
�%��&�&'
'#&#�#%#
�%��&��(
�%�"��������%��&��$�'*����� �+,-�$$�.�*� ��/��+�- #�
������
������
������
������
������
������
&%�(%0
&%�&"0
&%�&"0
&%�(�$
&%�(�$
�(��)#�%��)��
'#&#�#%#
�%�"������"%��%&��%�&*����� �+,-�'&�.�*� ��/��+�- #�
%��%&�0"%��%&�%1
���� �� ����� !2����/������ �+,-�&%*���������(��#
��� � ������
��
��
��
��
��
��
�����
�
��
���
���
���
��
�
��!"�� �#$��%��&' (���" �&%)* +��%,-��� ������������� ����������� � �������������
��
New Emirates Medical Journal, 2020, Volume 1, Number 2

A Case of 2:1 Atrio-Ventricular 59
Fig. (2B). Exercise testing -recovery stage: Complete heart block with narrow QRS escape rhythm.
2. DISCUSSION
Intra-Hisian 2:1 AV block is a relatively rare entity. Ourpatient on Holter had many episodes of Wenckebach block aswell as many episodes of 2:1 AV block, all with narrow QRSrhythm. AV block can occur at Supra-Hisian, Intra-Hisian andInfra-Hisian levels [3, 4]. Supra-Hisian block occurs due to AVnodal disease, usually presents with a narrow QRS escaperhythm of 40-60 Beats Per Minute (BPM), responsive toexercise and drugs, and is stable without abrupt deceleration inventricular rates [3, 4]. Infra-Hisian AV block presents withunreliable wide QRS escape rhythm at <40 BPM, isunresponsive to exercise or drugs, and causes Stokes-Adamsepisodes necessitating emergency pacing [3, 4]. AV block dueto disease within His bundle in early stages can present withQRS that is narrow in conducted beats but is unresponsive todrugs; when stressed with increasing atrial rates due to exerciseor catecholamines or atropine, His bundle and branchesconduct more slowly so that there is paradoxical slowing ofheart rates with widening of QRS complexes [2 - 4]. One casereport describes the occurrence of increasing right bundlebranch block occurring in an elderly 78-year old male onexercise testing [5]. When the PR interval in conducted beats is>160ms, the level of block is likely to be supra-Hisian [3, 4],but as seen in our patient, the PR interval not only was morethan 200ms but there was Wenckebach block despite having aninfra-nodal disease. Intra-Hisian block can present rarely asMobitz Type I with progressive PR prolongation [2], but morecommonly presents as abrupt drop in QRS complexes. WhileIntra-Hisian AV block masquerades as supra-Hisian (AVnodal) block because the QRS is narrow, it behavesfunctionally like Infra-Hisian block which manifests as anunstable rhythm with wide QRS, unresponsive to drugs and
exercise, leading to Stokes Adams episodes and even death,unless treated with ventricular pacing.
CONCLUSION
A 2:1 AV block with narrow QRS in conducted beat,offers a diagnostic challenge as to the level of block and needfor a permanent pacemaker. Our patient had progressive QRSwidening with subsequent complete heart block on low-levelexercise testing, and hence we postulate that she was anunusual case of Intra-Hisian second degree 2:1 AV blockpresenting both as Mobitz Type 1 and Type 2 conductionabnormalities. In such a situation, when a patient’s symptomsare effort-related, a low dose exercise test performed even in anelderly population helps in reaching correct diagnosis withoutinvasive electrophysiological testing.
ETHICS APPROVAL AND CONSENT TO PARTI-CIPATE
Not applicable.
HUMAN AND ANIMAL RIGHTS
Not applicable.
CONSENT FOR PUBLICATION
Informed consent of the patient had been obtained for thiscase report.
STANDARD FOR REPORTING
CARE guidelines have been followed in this case report.
�����
�
��
���
���
���
��
�
��!"�� �#$��%��&' (���" �&%)* +��%,-��� ������������� ����������� � �������������
��� � ������
��
��
��
��
��
��
��
New Emirates Medical Journal, 2020, Volume 1, Number 2

60 Kalavakolanu et al.
FUNDING
None.
CONFLICTS OF INTEREST
The authors declare no conflict of interest, financial orotherwise.
ACKNOWLEDGEMENTS
Declared none.
REFERENCES
Ishikawa T, Sumita S, Kikuchi M, Nakagawa T, Ogawa H, Hanada K,[1]
et al. Long-term follow-up in patients with intra-hisian atrioventricularblock. J Artif Organs 2000; 3: 149-53.[http://dx.doi.org/10.1007/BF02479982]Lee YS, Kim SY, Kim KS, Kim YN. Intra-His bundle block in[2]second-degree Mobitz I atrioventricular block with right bundle branchblock. Europace 2009; 11(9): 1251-2.[http://dx.doi.org/10.1093/europace/eup153] [PMID: 19542538]Josephson ME. Clinical Cardiac Electrophysiology: Techniques and[3]Interpretations. 3rd ed. Lippincott Williams & Wilkins 2001.Issa ZF, Miller JM, Zipes DP. Clinical arrhythmology and[4]electrophysiology: A companion to Braunwald’s heart disease. 1st ed.Philadelphia: Elsevier Saunders 2009.Singh S. The mischievous bundle: A case of varying degrees of right[5]bundle branch block on alternate beats during exercise stress testing.Ann Noninvasive Electrocardiol 2013; 18(3): 299-303.[http://dx.doi.org/10.1111/anec.12001] [PMID: 23714091]
© 2020 Kalavakolanu et al.
This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International Public License (CC-BY 4.0), a copy of which isavailable at: (https://creativecommons.org/licenses/by/4.0/legalcode). This license permits unrestricted use, distribution, and reproduction in any medium, providedthe original author and source are credited.
New Emirates Medical Journal, 2020, Volume 1, Number 2







![7-Deazapurine (Pyrrolo[2,3- d]pyrimidine) 2 ... Organic Chemistry, 2012, 16, 161-223 161 ©1875-5348/12 $58.00+.00 2012 Bentham Science Publishers 7-Deazapurine (Pyrrolo[2,3-d]pyrimidine)](https://static.fdocuments.in/doc/165x107/5abca4cf7f8b9a567c8e0793/7-deazapurine-pyrrolo23-dpyrimidine-2-organic-chemistry-2012-16-161-223.jpg)










