Case Management Monthly - Revenue Cycle Advisor · HCP R. C C C copyright.com . HCPRO.COM Case...
12
FEBRUARY 2017 Volume 14 Issue No. 2 Case Management Monthly Filling out the MOON: Steps to help ensure accuracy Accredited Case Manager certi- fication The requirements for ACM™ certification are changing. Ask the expert Our expert answers your latest ques- tions about the MOON. Inpatient or outpatient Use this CMS document to help explain inpatient and outpatient status to patients. From the Director’s Desk The dynamic nature of discharge planning. Complex Case A case manager assists in developing a discharge plan for a family member, but not everything goes as hoped. P5 P6 P8 P8 P10 Learning objective: At the completion of this educational activity, the learner will be able to: • Discuss challenges and strategies to fill out the Medicare Outpatient Observation Notice (MOON) form required under the Notice of Observation Treatment and Im- plication for Care Eligibility (NOTICE) Act The March 6 MOON implementation deadline is quickly approaching, which means organizations must act now to ensure that their staff mem- bers are ready accurately and completely to fill out and deliver the form. There were some changes from the proposed version of the form CMS first released to the final version it ultimately approved December 7, 2016. “The proposed version was more of a notification that the patient was in outpatient observation status. It included space for a hospital to add INSIDE THIS ISSUE Copyright: spxChrome. Image Source: istock.com
Transcript of Case Management Monthly - Revenue Cycle Advisor · HCP R. C C C copyright.com . HCPRO.COM Case...

FEBRUARY 2017Volume 14 Issue No. 2
Case Management Monthly
Filling out the MOON: Steps to help ensure accuracy Accredited Case Manager certi-
fication
The requirements for ACM™ certification are changing.
Ask the expert
Our expert answers your latest ques-tions about the MOON.
Inpatient or outpatient
Use this CMS document to help explain inpatient and outpatient status to patients.
From the Director’s Desk
The dynamic nature of discharge planning.
Complex Case
A case manager assists in developing a discharge plan for a family member, but not everything goes as hoped.
P5
P6
P8
P8
P10
Learning objective:At the completion of this educational activity, the learner will be able to:
• Discuss challenges and strategies to fill out the Medicare Outpatient Observation
Notice (MOON) form required under the Notice of Observation Treatment and Im-
plication for Care Eligibility (NOTICE) Act
The March 6 MOON implementation deadline is quickly approaching, which means organizations must act now to ensure that their staff mem-bers are ready accurately and completely to fill out and deliver the form.
There were some changes from the proposed version of the form CMS first released to the final version it ultimately approved December 7, 2016.
“The proposed version was more of a notification that the patient was in outpatient observation status. It included space for a hospital to add
INSIDE THIS ISSUE
Copyright: spxChrome. Image Source: istock.com

HCPRO.COM © 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
2 |Case Management Monthly February 2017
Case Management Monthly (ISSN: 1547-4739 [print]; 1937-7495 [online]) is published monthly by HCPro, a division of BLR®. Subscription rate: $379/year. • Case Management Monthly, 100 Winners Circle, Suite 300, Brentwood, TN 37027. • Copyright © 2016 HCPro, a division of BLR. All rights reserved. Printed in the USA. Except where specifically encouraged, no part of this publication may be reproduced, in any form or by any means, without prior written consent of HCPro or the Copyright Clearance Center at 978-750-8400. Please notify us immediately if you have received an unauthorized copy. • For editorial comments or questions, call 781-639-1872 or fax 781-639-7857. For renewal or subscription information, call customer service at 800-650-6787, fax 800-785-9212, or email [email protected]. • Visit our website at www.hcpro.com. • Occasionally, we make our subscriber list available to selected companies/vendors. If you do not wish to be included on this mailing list, please write to the marketing department at the address above. • Opinions expressed are not necessarily those of CMM. Mention of products and services does not constitute endorsement. Advice given is general, and readers should consult professional counsel for specific legal, ethical, or clinical questions. CMM is not affiliated in any way with The Joint Commission, which owns the JCAHO and Joint Commission trademarks.
CMM STAFF MEMBERS EDITORIAL ADVISORY BOARD
Jackie Birmingham, RN, BSN, MS, CMACVice President Emeritus, Clinical Leadership Curaspan Health Group, Inc. Newton, Massachusetts
Stefani Daniels, RN, MSNA, CMAC, ACM President and Managing PartnerPhoenix Medical Management, Inc. Pompano Beach, Florida
Wendy DeVreugd, RN, BSN, PHN, FNP, CCDS, MBADirector of Case Management, Clinical Social Work, and Clinical Documentation Improvement ProgramsUC Health (UCI Medical Center) Orange, California
Deborah K. Hale, CCS, CCDSPresidentAdministrative Consultant Service, LLC Shawnee, Oklahoma
Shawna Grossman Kates, MSW, MBA, LSW, CMAC Director, Case Management and Bed ManagementRWJBarnabas HealthToms River, New Jersey
Robert Marder, MDPractice Director of Quality and Patient SafetyThe Greeley Company Danvers, Massachusetts
Peter C. Moran, RN, C, BSN, MS, CCMNurse Case ManagerMassachusetts General Hospital Boston, Massachusetts
Loretta Olsen, MSN, RN, ACMDirector of Case ManagementMercy Medical Center North Iowa Mason City, Iowa
June Stark, RN, BSN, MEdDirector of Care CoordinationSt. Elizabeth’s Medical Center Boston, Massachusetts
Karen Zander, RN, MS, CMAC, FAANPresident and CEO The Center for Case Management, Inc. Wellesley, Massachusetts
This document contains privileged, copyrighted information. If you have not purchased it or are not otherwise entitled to it by agreement with HCPro, a division of BLR, any use, disclosure, forwarding, copying, or other communication of the contents is prohibited without permission.
Background on the NOTICE Act
Under the NOTICE Act, the MOON requirement was set to go into effect August 6, 2016, but was delayed with the August 2, 2016, release of the 2017 inpatient prospective payment system (IPPS) final rule. The delay afforded CMS additional time to revise the MOON form and respond to comments on the form.
The NOTICE Act, which was signed by President Barack Obama, requires hospitals to provide a verbal and written notice (using the MOON form) of outpa-tient status to any patient who has been in observation for more than 24 hours. The hospital must provide notice to the patient within 36 hours of the start of the service, or at the time of discharge or inpatient admis-sion. The goal of the legislation is to ensure patients are aware of their observation status and what it might mean for them financially—in particular, how it might affect their postacute care options. Patients often (wrongly) assume that if they’re in a hospital bed, they are an inpatient. They also rarely understand the implications of outpatient billing status. One of the biggest issues that can crop up when a patient’s care orders place him or her on observation status is that the patient will not be eligible for Medicare coverage
whatever details it wanted,” says Janet L. Blondo, LCSW-C, MSW, CMAC, ACM, CCM, C-ASWCM, ACSW, manager of case management at Washington Adventist Hospital in Takoma Park, Maryland.
The proposed form also highlighted what the patient may need to pay out of pocket for his or her care and clearly stated that the patient would not qualify for skilled nursing facility (SNF) benefits unless admitted as an inpatient.
“The final version forces the hospital to inform the patient why he or she is not an inpatient but takes a more positive tone in stating what Medicare Part B will cover instead of focusing on what the patient is not getting while not qualifying as an admitted inpatient,” says Blondo. “The changes will require organizations to take more time to complete the form and explain it to patients.”
Accurately completing the form will likely bring numerous challenges, including clearly documenting the reason why the patient doesn’t qualify as an inpatient, appropriately timing the delivery of the notice, and determining who will deliver it to the patient, she says.
Senior EditorJaclyn [email protected]
Contributing EditorKelly Bilodeau
Follow Us! Follow and chat with us about all things healthcare com-
pliance, management, and reimbursement. @HCPro_Inc

HCPRO.COM© 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Case Management Monthly | 3February 2017
for a postacute stay in a skilled nursing facility (SNF) and therefore may need to pay more out of pocket for a SNF stay. Medicare currently only covers SNF extended care rehabilitation services for patients who have three consecutive medically necessary inpatient days in a hospital within 30-days preceding a SNF stay. One day in observation and two days as inpatient, for example, does not meet that requirement because it only includes two inpatient days.
These uncovered SNF stays can be costly, with an average out-of-pocket fee of more than $10,000 per beneficiary, according to the Office of Inspector General.
To comply with the NOTICE Act, hospitals will need to designate someone—potentially the case manager—to provide the MOON. In fact, the form specifies that if an individual has a Medicare Advantage plan, Medicaid or another health plan there may be different rules for payment for SNF care and the beneficiary should check with Medicaid or their insurance com-pany to learn the details.
Filling out the MOON
Complying with requirements for the MOON may not be as straightforward as it sounds.
“Hospitals are discussing the best way to fill out the form,” says Blondo. “Completing the top part of the form, which explains why the patient is receiving outpatient observation services and is not an inpatient, is more complex. Some hospitals would rather put a generic answer on all the forms, such as, ‘because your doctor has determined you do not meet the criteria to be an inpatient.’”
Beyond deciding who presents the form to the patient, organizations will also need to decide what to write on the form.
Stefani Daniels, RN, MSNA, CMAC, ACM, manag-ing partner at Phoenix Medical Management, Inc., in Pompano Beach, Florida, says the general consensus among physician advisors she has spoken with is that the free text field on page one of the form should not
be left as free text, she says. But this approach may be challenging.
Marianne Ramey, a senior partner at Phoenix Medical Management, wrote the following in a blog post on MOON: “Since a physician is the only authorized individual to make a status determination, we recom-mend that the physician complete that section. To make it as convenient as possible, print the form using a check box format to list the reasons.”
The text section begins with the phrase, “You’re a hospital outpatient receiving observation services. You are not an inpatient because …”
“The first check box might state something like ‘according to Medicare rules, we are using this time to complete an evaluation of your current condition to
Continuing education information
Nursing Contact Hours (ANCC)HCPro is accredited as a provider of continuing nursingeducation by the American Nurses Credentialing Center’sCommission on Accreditation.
2.5 contact hours for nurses are available each quarter(March, June, September, December).
Commission for Case Manager Certification (CCMC)This program is approved by the Commission for Case Manager Certification for 6 continuing education units per quarter.
To obtain your contact hours, you must:
• Read each issue of Case Management Monthly within the quarter
• Successfully complete and submit the quarterly quiz (offered in the March, June, September, and Decem-ber issues; passing score is 80%)
• Complete and submit the evaluation Each quarter’s continuing education hours expire after one year.
Disclosure statement:The planners, authors, and contributors for this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity.

HCPRO.COM © 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
4 |Case Management Monthly February 2017
determine if you need to be admitted or discharged,’” Ramey wrote. “The second box might state, ‘we do not anticipate that the care you need right now will exceed two midnights in the hospital and according to Medi-care rules that does not qualify for a hospital admis-sion.’ The third box should be ‘other’ to give physicians the opportunity to write their own reasons.” The intent of this wording is to enforce the fact that the decision is not being indiscriminately made by the physician, but is instead describing the physician’s responsibility to follow Medicare rules, says Daniels.
Blondo says that she has also heard that some hospitals are working on common language for the MOON. Hospitals might opt to include statements such as “your doctor believes that based on your medical condition you will likely leave in a day or so” or “based on your medical needs, an inpatient stay is not required.”
Some hospitals are creating observation videos in the most common languages of their patients for viewing in the ED waiting rooms, registration area, and patient rooms or on tablets to further explain what it means to be in observation, says Blondo.
Delivering the MOON
CMS does not dictate who gives the notice to the patient, which gives organizations some leeway in their choice. But making the right choice is not easy.
“In some hospitals patient access/registration is giving the notice once it is determined the patient will stay,” says Blondo. “But patient access/registration is not clinical so they may need help or coaching to know what to put on the forms if the physician does not explain clearly.”
While some organizations choose patient access/registration, others may give this responsibility to case management or nursing staff members.
“In one hospital where my colleague works, patient access gives the initial form and case management gives it only if condition code 44 occurs,” says Blondo. “In our hospital, nursing gives it to the patients on the
observation unit and case management gives it to patients on the other units.”
Ramey wrote that the staff member chosen “must be able to explain the contents of the MOON and be prepared to answer any potential questions from the patient.” If the form is included in the packet of registration documents, then the registrar must be able to describe the form—as they currently do with all the other required hospital and Medicare documents. However, it would be wise to orient all care team members about the MOON so no matter who the patient or family member approaches, they could provide an overview of the content, according to Ramey.
Some organizations have decided that this person is the case manager. “Recently a hospital requested additional case management staff—and had been denied—but with this new requirement have re-visited the request since they believe case managers should be the ones giving the observation forms to patients as it requires someone with clinical knowledge,” says Blondo.
In addition to challenges associated with determining who will deliver the form, hospitals may also face challenges with tracking down patients when it is time to give them the MOON. If a patient placed in the ED is on another hospital floor for testing at the time when staff would deliver the MOON, the patient may be overlooked and never receive the form. Hospitals need to put processes in place to ensure patients are not missed when it is time for them to receive the form.
“Management should allow time to sup-port staff during this new process and plan
for regular auditing to make sure staff is implementing the forms cor rectly.”
Janet L. Blondo, LCSW-C, MSW, CMAC, ACM, CCM, C-ASWCM, ACSW
HCPRO.COM© 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Case Management Monthly | 5February 2017
State law on observation notices
Another challenge exists in states that already have their own laws requiring an observation notice. In these states, hospitals must be sure to train staff on delivering the correct forms. “In states like Maryland with an existing law to give observation notice to all patients, not just those with Medicare, training is crucial to make sure patients get the right notice,” says Blondo.
In her blog post, Ramey recommended that hospitals involve the chief compliance officer in decisions about complying with the NOTICE Act and any state laws that may come into play in this area.
Hospitals need to take careful consideration when any differences are found between the state and federal requirements.
“Additional Information statement or a separate attachment can be included with the MOON to align the MOON with state law requirements, if possible,” Ramey wrote. “However, where state law and the NOTICE Act do not align, hospitals and [critical
access hospitals] may be required to provide duplicate
notices at different times.”
Focus on training staff
Training is critical to ensuring staff properly complete the MOON form.
“Management should allow time to support staff during this new process and plan for regular auditing to make sure staff is implementing the forms cor-rectly,” says Blondo. “States that have never given observation notices before should expect patients will have lots of questions and may demand to be admitted as inpatients.” Advise staff to remain calm and have patience when addressing patient concerns about the MOON as this is a new process for both staff and patients in many instances.
Whatever process and training your organization implements, it must be true to the intent of the MOON form itself in that it should provide the patient with clear and easy to understand information about his or her patient status. H
Learning objective: At the completion of this educational activity, the learner will be
able to:
• Discuss the new requirement to sit for the Accredited Case
Manager (ACM™) certification.
Looking to get an ACM™ certification? In December, the American Case Management Association (ACMA) and National Board for Case Management (NBCM) announced a change to the exam eligibility requirements that may be of interest to those looking to earn ACM certification.
The NBCM now allows applicants with at least one year of full-time supervised work experience to sit for
the ACM-RN (Registered Nurse) and ACM-SW (Social Work) exams. Prior to this change, candidates had to have at least two years of case management experience before they could take either exam.
“The change was made in response to the evolution of case management as a profession,” says Christine Hinrichs, communications and social media strategist for the ACMA. “The National Board for Case Man-agement, which oversees the Accredited Case Manager exam, felt that some nurses and social workers would have the necessary expertise and knowledge to sit for the exam after only a year of full-time case manage-ment experience.”
The changing nature of case management programs may help bolster skills in a shorter time frame. “Many
NBCM changes requirements for the ACM™ certification

HCPRO.COM © 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
6 |Case Management Monthly February 2017
Learning objective:At the completion of this educational activity, the learner will be
able to:
• Discuss some common questions related to the Notice of
Observation Treatment and Implication for Care Eligibility
(NOTICE) Act requirements and Medicare Outpatient Obser-
vation Notice (MOON)
As hospitals get ready to start notifying patients about their status under the requirements of the NOTICE Act using the MOON form, many still have questions about the process and the form itself.
The NOTICE Act requires hospitals to provide a verbal and written notice (using the MOON form) of outpatient status to any patient who has been in observation for more than 24 hours. The hospital must provide notice to the patient within 36 hours of the start of the service, or at the time of discharge or
inpatient admission. “The notice must be provided no later than 36 hours after observation services are initiated or, if sooner, upon release,” according to CMS.
CMS has also stated that “MOON will inform more than one million beneficiaries annually of the reason(s) they are an outpatient receiving observation services and the implications of such status with regard to Medicare cost sharing and coverage for post-hospital-ization skilled nursing facility (SNF) services.”
The following are some common questions about the notification, which were answered by Ronald Hirsch, MD, FACP, CHCQM, vice president of the Regula-tions and Education Group at R1 Physician Advisory Services in Chicago.
Q Are hospitals required to deliver the MOON in its standard format or can they
modify the language on the form?
Ask the ExpertQA&
healthcare delivery employers provide particularly
strong case management orientation and training
programs accompanied with supervision,” said NBCM
Board Chairman Chris Carpenter in a statement.
“These programs are capable of preparing nurses and
social workers for the exam after only a year of full-
time case management experience.”
Jackie Birmingham, RN, BSN, MS, CMAC, a case
management expert, agrees. “With the speed with
which case managers need to be proficient in their jobs,
by 12 months they should have a grasp of the require-
ments for doing the job,” she says. “And, the idea that
the individual can use the certification guide as a tool
to identify learning needs, having a shorter time frame
should encourage nurses and social workers to get up
to speed more quickly.”
Certification may help case managers stand out from their peers. According to the 2015 National Case Management Survey, the only national source of 95% confidence-level hospital case management research, 66% of hospitals report that the ACM™ credential is influential in hiring decisions,” according to informa-tion provided by ACMA.
In order to receive ACM certification, candidates must take an exam that includes a multiple-choice section and a “discipline-specific simulation component,” according to the ACM. A full list of requirements needed to sit for the exam is available on the ACMA website.
ACMA believes that nurses and social workers with 36 months of health system experience should have their Accredited Case Manager credential, ACM™, to practice Health Delivery System Case Management.H
Questions from the MOON and back

HCPRO.COM© 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Case Management Monthly | 7February 2017
A The wording of the MOON cannot be altered in any way. Hospitals may, however, add details in
the “additional information” section and must also write the reason for observation in the appropriate spot on the form. Aside from these changes, you can only modify the MOON slightly to allow placement of a label or other identifier.
Q Do you have any recommendations as to who is best suited to fill out the MOON
form? Why?
A We are expecting additional guidance from CMS on this. As it stands now, I feel a registra-
tion clerk can present the form provided case managers and financial counselors are available if the patient has questions about the form.
The reason the patient is not inpatient is typically due to the fact that the patient does not meet the require-ments spelled out in the 2-midnight rule to be admit-ted as inpatient. It is not likely that CMS would expect the physician to have to indicate a clinical reason, such as “your asthma attack is only mild and should get better in a day,” in instances when a patient does not meet admission criteria.
The related story on p. 1 provides information about who hospitals might select to deliver the MOON.
Q What are the consequences if hospitals don’t issue the MOON in the required
time period or fail to deliver it entirely?
A The MOON has the same standing as the Im-portant Message from Medicare (IMM). It is a
federal document that must be completed and deliv-ered as required. Compliance will be assessed by sur-veyors such as a state agency on behalf of CMS and the national accrediting agencies. The consequences of failing to deliver the MOON in a timely manner or at all would be similar to those imposed when organiza-tions fail to deliver the IMM, with deficiencies and the need for correction plans.
Q What is the organization’s responsibility with regard to the MOON if a patient
starts treatment as an outpatient but then is moved to inpatient status? Does the hospital still need to issue the MOON?
A If the patient received 24 or more hours of ob-servation and had not yet received the MOON
at the time he or she was moved to inpatient status, the hospital must still deliver the MOON with notation of the date and time of presentation.
Q What verbal notification is needed in ad-dition to providing a completed MOON
form?
A CMS states that an oral explanation of the MOON must accompany the written form. Ide-
ally, officials say, it should be provided at the same time as the written notification.
We are expecting additional guidance from CMS but for now a simple explanation that the patient is in observation, that the notice explains it in detail, and that someone is available to answer questions should suffice.
Upon delivery of the notice, the patient or a person acting on his or her behalf must sign the MOON to acknowledge receipt. “In cases where such individual or person refuses to sign the MOON the staff member of the hospital or CAH providing the notice must sign the notice to certify that notification was presented,” states CMS.
Hirsch advises hospitals to attach a copy of the Medi-care brochure “Are you an Inpatient or Outpatient” (see pp. 7–8 for an excerpt) or an internally designed form to each MOON.
EDITOR’S NOTE:
Do you have a question for our experts on MOON or another case
management–related topic? Please email it to Kelly Bilodeau at
[email protected], and we’ll submit it to our panel of experts. H
Ask the ExpertQA&

HCPRO.COM © 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
8 |Case Management Monthly February 2017
Help patients understand inpatient and outpatient statusCMS’ document “Are You a Hospital Inpatient or Outpatient?” to help patients understand their status.
The following is an excerpt from this document. Hospitals may choose to provide this document to patients when delivering the
MOON form to help patients understand the financial implications of their status. what their status might mean for their finances.
Are You a Hospital Inpatient or Outpatient?If You Have Medicare – Ask!
Revised May 2014
Did you know that even if you stay in a hospital overnight, you might still be considered an “outpatient?” Your hospital status (whether the hospital considers you an “inpatient” or “outpatient”) affects how much you pay for hospital services (like X-rays, drugs, and lab tests) and may also affect whether Medicare will cover care you get in a skilled nursing facility (SNF) following your hospital stay. • You’re an inpatient starting when you’re formally admitted to a hospital with
a doctor’s order. The day before you’re discharged is your last inpatient day.
• You’re an outpatient if you’re getting emergency department services, observation services, outpatient surgery, lab tests, X-rays, or any other hospital services, and the doctor hasn’t written an order to admit you to a hospital as an inpatient. In these cases, you’re an outpatient even if you spend the night at the hospital.
Note: Observation services are hospital outpatient services given to help the doctor decide if the patient needs to be admitted as an inpatient or can be discharged. Observation services may be given in the emergency department or another area of the hospital. The decision for inpatient hospital admission is a complex medical decision based on your doctor’s judgment and your need for medically necessary hospital care. An inpatient admission is generally appropriate when you’re expected to need 2 or more midnights of medically necessary hospital care, but your doctor must order such admission and the hospital must formally admit you in order for you to become an inpatient.Read on to understand the differences in Original Medicare coverage for hospital inpatients and outpatients, and how these rules apply to some common situations. If you have a Medicare Advantage Plan (like an HMO or PPO), your costs and coverage may be different. Check with your plan.
Source: The Centers for Medicare and Medicaid Services.

HCPRO.COM© 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Case Management Monthly | 9February 2017
Help patients understand inpatient and outpatient status (cont.)
2
What do I pay as an inpatient?• Medicare Part A (Hospital Insurance) covers inpatient hospital services.
Generally, this means you pay a one-time deductible for all of your hospital services for the first 60 days you’re in a hospital.
• Medicare Part B (Medical Insurance) covers most of your doctor services when you’re an inpatient. You pay 20% of the Medicare-approved amount for doctor services after paying the Part B deductible.
What do I pay as an outpatient?• Part B covers outpatient hospital services. Generally, this means you pay a
copayment for each individual outpatient hospital service. This amount may vary by service. Note: The copayment for a single outpatient hospital service can’t be more than the inpatient hospital deductible. However, your total copayment for all outpatient services may be more than the inpatient hospital deductible.
• Part B also covers most of your doctor services when you’re a hospital outpatient. You pay 20% of the Medicare-approved amount after you pay the Part B deductible.
• Generally, prescription and over-the-counter drugs you get in an outpatient setting (like an emergency department), sometimes called “self-administered drugs,” aren’t covered by Part B. Also, for safety reasons, many hospitals have policies that don’t allow patients to bring prescription or other drugs from home. If you have Medicare prescription drug coverage (Part D), these drugs may be covered under certain circumstances. You’ll likely need to pay out-of-pocket for these drugs and submit a claim to your drug plan for a refund. Call your drug plan for more information.
For more detailed information on how Medicare covers hospital services, including premiums, deductibles, and copayments, visit Medicare.gov/publications to view the “Medicare & You” handbook. You can also call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048.
Source: The Centers for Medicare and Medicaid Services.

HCPRO.COM © 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
10 |Case Management Monthly February 2017
EDITOR’S NOTE:
The following is an excerpt from HCPro’s Discharge Planning Guide: Tools for Compliance, Fourth Edition, written by Jackie Birmingham, RN, BSN, MS, CMAC. The book discusses issues related to discharge planning from case management’s role as well as various legislative and regulatory initiatives that make getting discharge planning right more important than ever.
Discharge planning, which is integral to providing continuity of care, is a dynamic process in which the goals are to:
• Assess patient needs
• Identify the resources necessary to meet those needs
• Establish and implement plans to meet those needs
• Transition the patient to the most appropri-ate level of care
The steps make this process dynamic—they sometimes occur in order, they sometimes overlap, and they sometimes move back and forth.
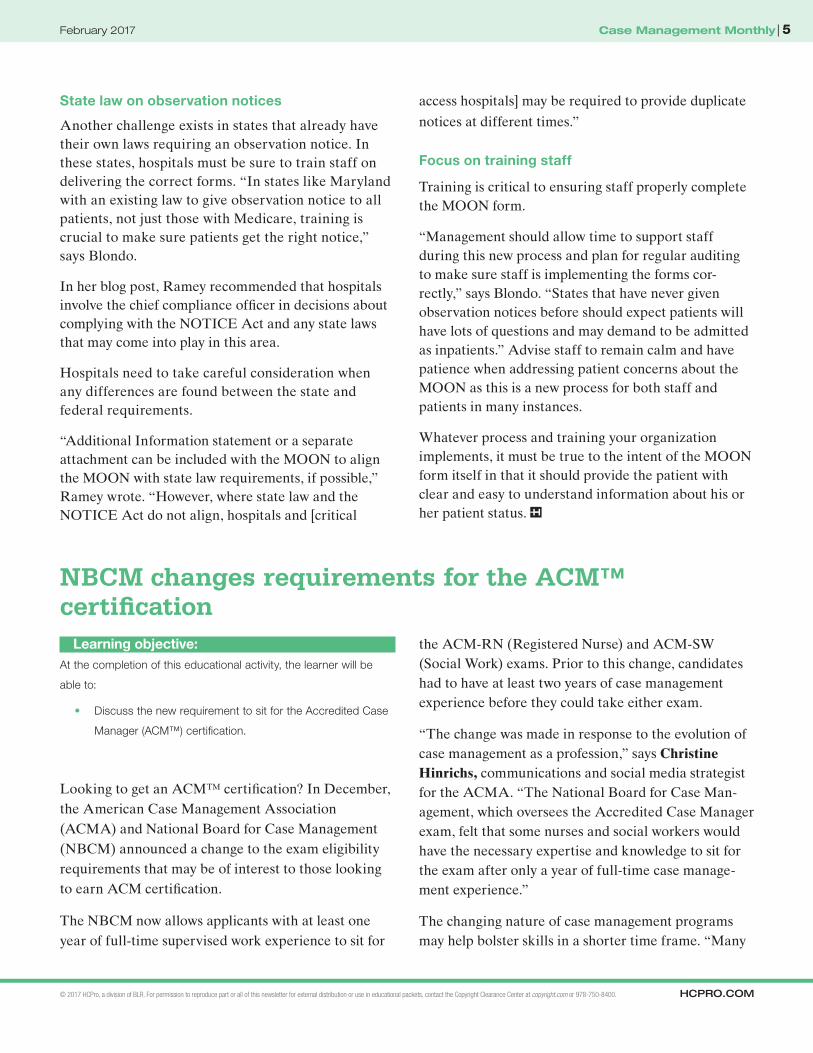
The patient-centered process of discharge planning consists of six dynamic steps (see the figure below for more information):
1. Initial assessment: identifying the discharge needs of all patients and those in need of specialized discharge planning
2. Evaluation of the patient’s continuity-of-care needs, sometimes called transition needs assessment
3. Assessment of post-discharge resources: those resources available to the individual patient
4. Problem identification/goal setting
5. Planning
6. Implementation (discharge, transfer, or referral)
Monitoring is part of the dynamic nature of discharge planning. It should occur throughout the discharge planning process to ensure that the plan accounts for the patient’s progress or lack thereof. H
From the Director’s Desk
The dynamic nature of discharge planningThe Dynamic Nature of Discharge Planning
Legend: Start/Stop
Internal process
Decision
External process
1. Initial assessment
Discharge the patient
2. Evaluate thepatient
4. Set goals &preferences withteam-patient
5. Make a planRevise the plan?
3. Assessresources
6. Implementthe plan
The six steps of discharge planning
Source: Reprinted from Discharge Planning Guide: Tools for Compliance, Fourth Edition, by Jackie Birmingham, RN, BSN, MS, CMAC.

HCPRO.COM© 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
Case Management Monthly | 11February 2017
Complex Case
Ever since Pat became a nurse case manager three years ago, both family and friends have reached out to her for healthcare advice. She really doesn’t mind and almost expects it, especially since healthcare can be complex and challenging.
By sharing her knowledge as a case manager, Pat can often help people navigate healthcare complexities.
While Pat is great at helping patients at her hospi-tal, she will often go to extremes to help friends and family. For example, Pat’s 92-year-old father-in-law, Ray, was hospitalized with heart failure (HF) while Pat was vacationing in Quebec, Can-ada. Ray is brought to Hospital X, which is in Pat’s community but is not where she is employed. However, Pat knows several of the case managers at Hospital X and reaches out to them.
Ray has not been hospitalized for his HF in two years. He has been successfully living at home with minimal medical intervention and a good quality of life.
Pat is worried about Ray but is vacationing too far away to visit Hospital X. The best she can do is to speak with Ray and other family members to piece the case together so she can try to help plan his hospital stay and discharge. After assessing Ray over the phone, Pat decides that it was a pretty straight forward case. She believes this acute exacerbation of her Ray’s HF is brought on by normal aging.
The cardiologist orders a Lasix IV drip with cardiac monitoring, at which point it appears he will discharge Ray with three new medications. However, the cardiologist wants further diagnostic testing to confirm his medical course, so the length of stay is targeted at four days.
But over the course of the stay, Ray becomes slightly physically deconditioned and his need for home physical therapy and possible occupational therapy becomes evident. It is then determined that home care intervention is needed to evaluate Ray’s response to the new medications and rein-force the education the hospital provides Ray about his medication. Pat realizes that her father-in-law has many immediate needs, but her primary concern is that he returns to the same level of health he was at prior to admission.
Pat believes Ray should be referred to a HF telemonitoring program that incorporates the national HF best practice standards. Since Ray will be discharged home on three new medications, it is particularly important that he see a cardiologist and/or primary care provider within three to five days of discharge, which is a best practice standard. Pat recommends homecare cardiac telemonitoring for daily assessment of Ray’s weights while on his new diuretic regime and to prevent future admis-sions. Daily blood pressure checks are also part of the plan.
Lastly, Pat requests that the cardiologist order a sliding Lasix administration scale to be provided by the home care nurse to intervene at the begin-ning of any episode of weight gain, ultimately avoiding any future hospitalizations.
Pat cares about Ray and knows repeat hospitaliza-tions would put him at great risk for unforeseen complications and could affect his quality of life.
Pat begins regular discussions with Ray’s case managers, who state that they agree with the discharge plan. However, to Pat’s surprise and disbelief, not one of her requests is met post-dis-charge. Ray has home care in place to help with his
A case manager coordinates care for a loved one

HCPRO.COM © 2017 HCPro, a division of BLR. For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at copyright.com or 978-750-8400.
12 |Case Management Monthly February 2017
Complex Case
new medications and physical and occupational therapy, but there is no telemonitoring component or element of a HF transitions in care component. In addition, Ray’s visit with his cardiologist is scheduled for three weeks post-discharge. Pat considers this lack of follow-through from personal and clinical case manager perspective and realizes that Ray’s case is a clear example of why there are such high readmission rates for patients with HF conditions.
Pat steps in to reinforce her discharge plan, believ-ing that Ray would surely be readmitted to the hospital if her plan were not followed. Pat confirms
that Ray is still in agreement with the original discharge plan.
Pat becomes Ray’s healthcare proxy, which allows her to contact the cardiologist and home care staff to implement her transition plan. Pat is satisfied that she has taken the right steps to ensure Ray’s maxi-mal recovery and health.
Pat isn’t sure why the case management team failed to incorporate her wishes into Ray’s transition plan, but this case taught her that HF standards that were once new innovations are now a critical component of routine HF care for all patients. H
![Creating a Conducive Policy Environment for Micro, Small ... · Rosewood Drive, Danvers, MA 01923 [Fax: (+1) (978) 750 4470; e-mail: info@copyright.com] or in other countries with](https://static.fdocuments.in/doc/165x107/5f6fd5275a9fad3d4e5b86db/creating-a-conducive-policy-environment-for-micro-small-rosewood-drive-danvers.jpg)



![Beyond the Employment/Unemployment Dichotomy: Measuring ...oit.org/wcmsp5/groups/public/---dgreports/... · Rosewood Drive, Danvers, MA 01923 [Fax: (+1) (978) 750 4470; email: info@copyright.com]](https://static.fdocuments.in/doc/165x107/603df7cbb38daf330076fc97/beyond-the-employmentunemployment-dichotomy-measuring-oitorgwcmsp5groupspublic-dgreports.jpg)





![Copyright © International Labour Organization 2003...Rosewood Drive, Danvers, MA 01923 [Fax: (+1) (978) 750 4470; email: info@copyright.com] or in other countries with associated](https://static.fdocuments.in/doc/165x107/5ebef2ab37101b6f1b7dbaa1/copyright-international-labour-organization-rosewood-drive-danvers-ma-01923.jpg)





![SEED WORKING PAPER No. 52...Rosewood Drive, Danvers, MA 01923 [Fax: (+1) (978) 750 4470; e-mail: info@copyright.com] or in other countries with associated Reproduction Rights Organizations,](https://static.fdocuments.in/doc/165x107/5fd86f5be456a51fbe0e8b0d/seed-working-paper-no-52-rosewood-drive-danvers-ma-01923-fax-1-978.jpg)