
Case 29 -2007.pdf
8
case records of the massachusetts general hospital T h e new england journal o f medicine n engl j med 357;12 www.nejm.org september 20, 2007 1239 Founded by Richard C. Cabot Nancy Lee Harris, m.d., Editor Eric S. Rosenberg, m.d., Associate Editor Jo-Anne O. Shepard, m.d., Associate Editor Alice M. Cort, m.d., Associate Editor Sally H. Ebeling, Assistant Editor Christine C. Peters, Assistant Editor From the Division of Infectious Disease (E.T.R.) and the Departments of Radiology (S.L.A.) and Pathology (R.L.K.), Massa- chusetts General Hospital; and the De- partments of Medicine (E.T.R.), Radiology (S.L.A.), and Pathology (R.L.K.), Harvard Medical School. N Engl J Med 2007;357:1239-46. Copyright © 2007 Massachusetts Medical Society. Presentation of Case Dr. Allison L. McDonough (Internal Medicine): A 51-year-old man with a history of gastric cancer was admitted to t he hospital because of a new pulmonary lesion. The patient had been in good health until approximately 5 year s before admis- sion, when he had a decreased appetite and epigastric discomfort; evaluation at another facility revealed a hiatal hernia, gastroesophageal reflux, and a duodenal ulcer. Testing for Helicoba cter pylori was positive. Omeprazole and metoclopramide were administered, and t he hiatal hernia was surgically repaired. Pain, persistent gastroesophageal ref lux, and weight loss developed app roximately 2.5 years before admission. A primary care physician at this hospital prescribed combination therapy (lansoprazole, amoxicillin, and clarithromycin) for 2 weeks to treat the H. pylori infection; th is therapy was repeated 3 months later because of noncompliance, but the symptoms persisted. At that ti me, the hematocrit was 38.8%, and the remainder of the complete blood count was normal. The phosphorus level was 1.3 mg per deci- liter (0.4 mmol per liter; reference range, 2.6 to 4.5 mg per deciliter [0.8 to 1.5 mmol per liter]), the lipase level was 77 U per liter (reference range, 13 to 60), and the amylase level was 164 U per l iter (reference range, 3 to 100) . Electrolyte levels and the results of renal- and liver-function tests were normal. Ultrasonography of the abdome n was normal. Abdominal pain recurred intermittently, and 2 years before admission, upper gastrointestin al endoscopy revealed distal esophagitis; a nonblee ding linear ulcer- ation, 10 mm in the greatest dimension, in the gastric antrum; marked edema in the prepyloric antrum; a nonbl eeding, cratered ulcer, 12 mm in diameter, in t he pyloric channel; and partial gastr ic-ou tlet obstruction. Pathological examination of biopsy specimens from the pylorus revealed poorly differentiated adenocarci- noma with signet-ring cells. Thiazine staining of biopsy specimens was negative for H. pylori. Computed tomography (CT) of the abdomen showed thickening of the wall of the antrum, withou t evidence of local invasion or intraabd ominal metastases. A subtotal gastrectomy was performed. Pathological examination revealed a poorly differentiated signet-ring–cell adeno- carcinoma of the pylorus, 4.0 cm in the g reatest dimension, leading to a diagnosis of stage II cancer (T2,N1,MX), with 2 of 12 lymph nodes positive for tumor and Case 29-2007: A 51-Year-Old Man with Gastric Cancer and Lung Nodules Edward T. Ryan, M.D., Suzanne L. Aquino, M.D., and Richard L. Kradin, M.D. reserved. Downloade d from www.nejm.org on October 1, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights
-
Upload
ana-di-jaya -
Category
Documents
-
view
220 -
download
0
Transcript of Case 29 -2007.pdf

7/27/2019 Case 29 -2007.pdf
http://slidepdf.com/reader/full/case-29-2007pdf 1/8
case records of the massachusetts general hospital
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 357;12 www.nejm.org september 20, 2007 1239
Founded by Richard C. CabotNancy Lee Harris, m.d., Editor Eric S. Rosenberg, m.d., Associate Editor Jo-Anne O. Shepard, m.d., Associate Editor Alice M. Cort, m.d., Associate Editor Sally H. Ebeling, Assistant Editor Christine C. Peters, Assistant Editor
From the Division of Infectious Disease(E.T.R.) and the Departments of Radiology(S.L.A.) and Pathology (R.L.K.), Massa-chusetts General Hospital; and the De-partments of Medicine (E.T.R.), Radiology(S.L.A.), and Pathology (R.L.K .), HarvardMedical School.
N Engl J Med 2007;357:1239-46.Copyright © 2007 Massachusetts Medical Society.
Presentation of Case
Dr. Allison L. McDonough (Internal Medicine): A 51-year-old man with a history of gastric cancer was admitted to the hospital because of a new pulmonary lesion.
The patient had been in good health until approximately 5 years before admis-sion, when he had a decreased appetite and epigastric discomfort; evaluation at another facility revealed a hiatal hernia, gastroesophageal reflux, and a duodenalulcer. Testing for Helicobacter pylori was positive. Omeprazole and metoclopramide were administered, and the hiatal hernia was surgically repaired. Pain, persistent gastroesophageal reflux, and weight loss developed approximately 2.5 years beforeadmission. A primary care physician at this hospital prescribed combination therapy (lansoprazole, amoxicillin, and clarithromycin) for 2 weeks to treat the H. pylori
infection; this therapy was repeated 3 months later because of noncompliance, but the symptoms persisted. At that time, the hematocrit was 38.8%, and the remainderof the complete blood count was normal. The phosphorus level was 1.3 mg per deci-liter (0.4 mmol per liter; reference range, 2.6 to 4.5 mg per deciliter [0.8 to 1.5 mmolper liter]), the lipase level was 77 U per liter (reference range, 13 to 60), and theamylase level was 164 U per liter (reference range, 3 to 100). Electrolyte levels andthe results of renal- and liver-function tests were normal. Ultrasonography of theabdomen was normal.
Abdominal pain recurred intermittently, and 2 years before admission, uppergastrointestinal endoscopy revealed distal esophagitis; a nonbleeding linear ulcer-ation, 10 mm in the greatest dimension, in the gastric antrum; marked edema inthe prepyloric antrum; a nonbleeding, cratered ulcer, 12 mm in diameter, in the
pyloric channel; and partial gastric-outlet obstruction. Pathological examinationof biopsy specimens from the pylorus revealed poorly differentiated adenocarci-noma with signet-ring cells. Thiazine staining of biopsy specimens was negative forH. pylori. Computed tomography (CT) of the abdomen showed thickening of the wall of the antrum, without evidence of local invasion or intraabdominal metastases.A subtotal gastrectomy was performed.
Pathological examination revealed a poorly differentiated signet-ring–cell adeno-carcinoma of the pylorus, 4.0 cm in the greatest dimension, leading to a diagnosisof stage II cancer (T2,N1,MX), with 2 of 12 lymph nodes positive for tumor and
Case 29-2007: A 51-Year-Old Man withGastric Cancer and Lung Nodules
Edward T. Ryan, M.D., Suzanne L. Aquino, M.D., and Richard L. Kradin, M.D.
reserved.Downloaded from www.nejm.org on October 1, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights

7/27/2019 Case 29 -2007.pdf
http://slidepdf.com/reader/full/case-29-2007pdf 2/8
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 357;12 www.nejm.org september 20, 20071240
perineural invasion, with no vascular or lym-phatic invasion. The tumor had invaded the sub-serosa but did not involve the serosal surface. Theproximal, distal, and radial margins were freeof tumor. Reactive gastropathy with mildchronic inflammation and intestinal metaplasia was present. Thiazine staining for H. pylori was
negative. The hematocrit was 37.7%, the white-cell count was 12,000 per cubic millimeter, with12% eosinophils (normal range, 0 to 8%), andthe remainder of the complete blood count wasnormal. The phosphorus level was 2.2 mg perdeciliter (0.7 mmol per liter), and the calciumlevel was 8.8 mg per deciliter (2.2 mmol per li-ter). The results of renal- and liver-function tests were normal. The patient was referred for an on-cology evaluation but did not keep the appoint-ments.
Eleven months before admission, the patient
came to the emergency department of this hos-pital because of a 3-month history of back andchest pain, as well as bilateral sharp, pleuritic,subscapular pain that had occurred occasionally.He had had early satiety since his abdominal sur-gery. A chest radiograph showed a nodule, 4 mmin diameter, with the density of metal that wasoverlying the fifth posterior rib; the nodule wasthought to represent a foreign body outside thechest cavity. The radiograph was otherwise nor-mal. The hematocrit was 40.2%. The remainderof the complete blood count and measurementsof electrolytes and renal function were normal.
One month later, the patient was seen by pul-monary and gastroenterology specialists. He re-ported that his weight had increased after hispartial gastrectomy but that he had lost weight in recent months. The subscapular pain had re-solved spontaneously, and he had no respiratory symptoms, fever, or chills. Physical examinationshowed that he was a thin, anxious man withmild temporal wasting. The weight was 58.1 kg,and the oxygen saturation was 97% while the
patient was breathing ambient air. The abdominalscar was well healed, and there was moderateclubbing of the fingers; the remainder of theexamination was normal. CT of the chest revealedmultiple, small centrilobular nodules and smallcysts, each less than 3 mm in diameter. Thepatient was advised to have a follow-up CT scan3 months later.
A follow-up CT scan obtained 5.5 months later(4.5 months before admission) revealed persistent centrilobular ground-glass nodules and scattered,
small parenchymal cysts in the lungs, with noevidence of metastatic disease in the abdomenor pelvis. The patient had pain in the abdominal wall at the site of the surgical scar, early satiety,nausea, fatigue, and weight loss. He appearedthin and chronically ill, with a weight of 56.7 kg.There was clubbing of all digits, and a small,
tender, firm nodule consistent with a keloid waspalpated in the surgical scar. The hematocrit was40.1%, and the white-cell count 7700 per cubicmillimeter, with 9% eosinophils. The remainderof the complete blood count was normal. Mea-surements of serum electrolytes and liver-func-tion tests were normal. The urea nitrogen level was 21 mg per deciliter (7.5 mmol per liter), thecreatinine level 1.0 mg per deciliter (88.4 μmolper liter), and the lipase level 163 U per liter.Upper gastrointestinal endoscopy revealed mildreactive gastropathy and a nodule, 1 cm in diam-
eter, in the gastric body; biopsy specimens of thenodule and of gastric and small-intestine mu-cosa at the anastomosis site showed both acuteand chronic inflammation.
Two weeks before admission, a CT scan of theabdomen and pelvis was unchanged, but CT of the chest showed a new nodule, 4.5 mm in diam-eter, in the lower lobe of the left lung, with a rimof ground-glass opacification. The small ground-glass nodules and cysts were unchanged as com-pared with those on the previous scans. He wasadmitted to this hospital.
The patient did not have cough, hemoptysis,bone pain, or headaches, and his weight had beenstable for the previous 4 months. His medicationsincluded metoclopramide, omeprazole, and cyclo-benzaprine; he had no allergies. He had beenborn in Brazil and had immigrated to the UnitedStates more than 20 years earlier. He visitedBrazil approximately annually, and 7 years earlier,he had lived in Japan for 1 year. He was married toa woman of Japanese–Brazilian ancestry and hadlived with his wife and children until 4 months
before admission, when his family returned toBrazil after he left his job in a factory because of poor health. He ate cooked, but not raw, shell-fish. His father had died at 39 years of age fromgastric cancer, and his mother had died at 65 years of age from bronchitis. His children andsiblings were healthy. He had smoked cigarettesfor 25 years but had stopped 3 months beforeadmission.
The vital signs were normal, and the physicalexamination was unchanged. An electrocardio-
reserved.Downloaded from www.nejm.org on October 1, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights

7/27/2019 Case 29 -2007.pdf
http://slidepdf.com/reader/full/case-29-2007pdf 3/8
case records of the massachusetts general hospital
n engl j med 357;12 www.nejm.org september 20, 2007 1241
gram was normal, and pulmonary-function testsshowed a low diffusion capacity of the lung forcarbon monoxide, after correction for alveolar volume. The complete blood count, serum electro-lyte levels, liver function, and renal function werenormal.
A diagnostic procedure was performed.
First Differential Diagnosis
Dr. Edward T. Ryan: I was involved in the care of this patient and am aware of the diagnosis. I be-lieve that this 51-year-old man originally fromBrazil, with gastric cancer and a new pulmonary nodule, has sequelae of two common infectiousdiseases.
Is this patient’s gastric cancer a sequela of aninfection? The World Heath Organization current-ly estimates that approximately one fifth of all
cancer cases worldwide are due to chronic infec-tions, including cases of liver cancer associated with hepatitis B, cervical cancer associated withthe human papillomavirus, lymphoma associated with the human immunodeficiency virus and Ka-posi’s sarcoma, bladder cancer associated withschistosomiasis, cholangiocarcinoma associated with liver-fluke infection, and gastric cancer as-sociated with H. pylori infection.1 Gastric adeno-carcinoma has historically been the most commonnonskin cancer and the most common cause of cancer-related deaths in humans, and a numberof prospective and retrospective studies have clear-ly linked H. pylori colonization of the stomach toboth distal gastric adenocarcinoma and gastricB-cell lymphoma.2‑5
H. pylori Infection and Gastric Cancer
Five years before admission, the patient had re-ceived a diagnosis of H. pylori infection, based onsymptoms of gastroesophageal ref lux and pepticulcer disease and evidence of H. pylori on exami-nation of gastric tissue. H. pylori is a motile gram-
negative bacillus that infects more than half thehuman population. Infection usually occurs inchildhood and is associated with crowding, poorsanitation, and residence in resource-poor areasof the world, suggesting oral–oral or fecal–oraltransmission. This patient was raised in Brazil, where both H. pylori infection and gastric cancerare relatively common. Persons with H. pylori in-fection have a risk of gastric cancer that is threeto six times that of persons without such infec-tion, as well as an attributable risk of 50 to 80%
for gastric adenocarcinoma.2,4 The risk of gastricadenocarcinoma varies even among geographicareas in which H. pylori infection is highly preva-lent, suggesting that additional factors lead toH. pylori–associated gastric cancer. For instance,certain polymorphisms in genes coding for pro-inflammatory cytokines have been associated
with gastric cancer, suggesting that differencesin host inf lammatory responses to H. pylori infec-tion may affect the development of gastric carci-noma.6 This patient has a family history of gas-tric cancer and infection with H. pylori; both arerisk factors for distal gastric adenocarcinoma.Persons of Japanese–Brazilian ancestry have ahigh risk of gastric cancer, which remains relative-ly high even after emigration; however, althoughthe patient has lived in Japan, he is not of Japa-nese descent.7‑9
Although the majority of H. pylori infections
are asymptomatic, this patient had multiple com-plications. H. pylori strains that are positive forCagA, a toxin injected by the bacteria into eukary-otic cells, are most likely to cause illness in hu-mans, including chronic gastritis, peptic ulcerdisease, and gastric adenocarcinoma, all of whichthis patient had.10‑12 Chronic gastritis caused by infection with H. pylori is associated with intesti-nal metaplasia and loss of production of gastricacid, and the strains of H. pylori that cause gastri-tis and gastric cancer have been associated witha protective effect against gastroesophageal refluxdisease, Barrett’s esophagus, and adenocarcino-ma of the distal esophagus.13,14 The incidenceof gastric cancer has decreased in resource-richareas in recent decades, predominantly becauseof a decrease in the incidence of adenocarcino-mas of the distal stomach, and concomitantly,there has been an increase in the incidence of adenocarcinomas of the proximal stomach anddistal esophagus, cancers associated with gastro-esophageal reflux disease.15 Therefore, paradoxi-cally, an adverse effect of H. pylori infection may
be replaced by an adverse effect of its eradication.Not surprisingly, our patient’s symptoms of gas-troesophageal reflux persisted after the H. pylori infection was treated.
At the time of the diagnosis of gastric adeno-carcinoma, no organisms were seen in the patho-logical specimens. This finding is not infrequent.In studies in Brazil, 15 to 45% of patients withgastric carcinoma had no evidence of active H. py-
lori infection on microscopical examination at thetime of treatment of their gastric cancer.16,17
reserved.Downloaded from www.nejm.org on October 1, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights
7/27/2019 Case 29 -2007.pdf
http://slidepdf.com/reader/full/case-29-2007pdf 4/8
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 357;12 www.nejm.org september 20, 20071242
Pulmonary Nodules
In summary, this patient’s gastric carcinoma is inall likelihood a complication of an infectious dis-ease ― namely, infection with H. pylori. One yearafter his gastrectomy, he presented with symp-toms of pleuritic chest pain and abnormalities onimaging studies of the chest. May we review the
imaging studies?Dr. Suzanne L. Aquino: The chest radiograph ob-
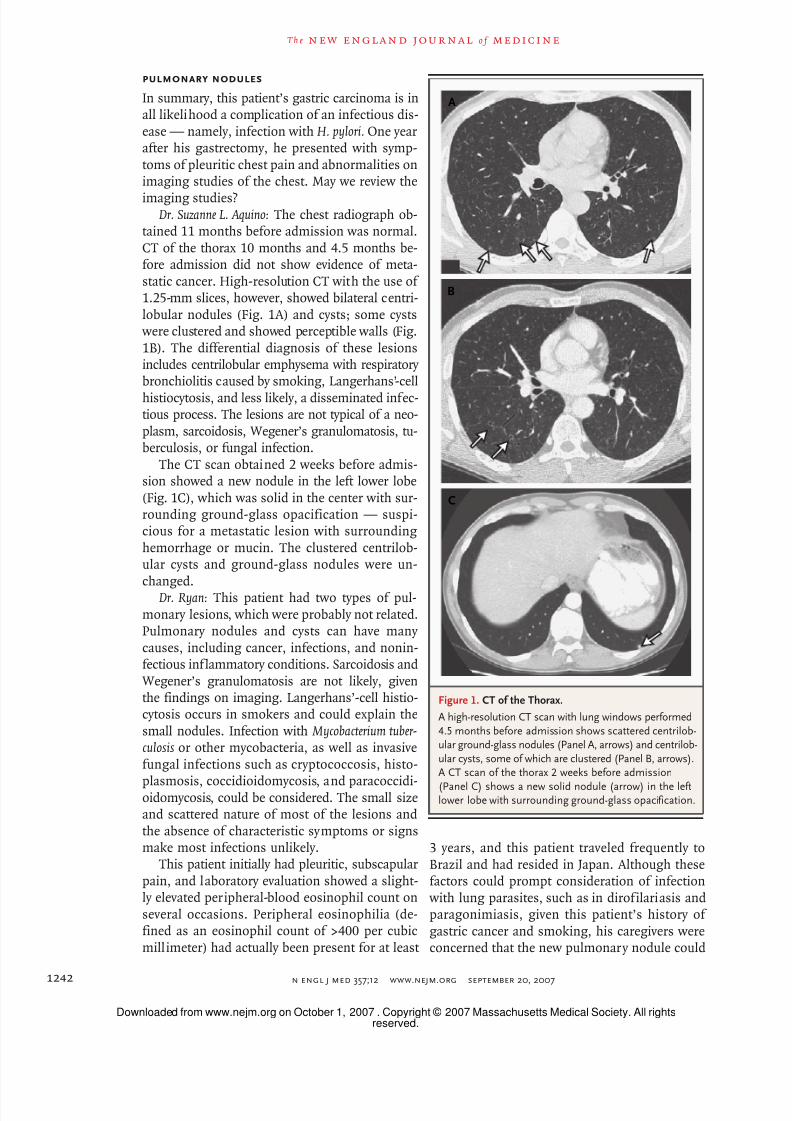
tained 11 months before admission was normal.CT of the thorax 10 months and 4.5 months be-fore admission did not show evidence of meta-static cancer. High-resolution CT with the use of 1.25-mm slices, however, showed bilateral centri-lobular nodules (Fig. 1A) and cysts; some cysts were clustered and showed perceptible walls (Fig.
1B). The differential diagnosis of these lesionsincludes centrilobular emphysema with respiratory bronchiolitis caused by smoking, Langerhans’-cell
histiocytosis, and less likely, a disseminated infec-tious process. The lesions are not typical of a neo-plasm, sarcoidosis, Wegener’s granulomatosis, tu-berculosis, or fungal infection.
The CT scan obtained 2 weeks before admis-sion showed a new nodule in the left lower lobe(Fig. 1C), which was solid in the center with sur-rounding ground-glass opacification — suspi-cious for a metastatic lesion with surroundinghemorrhage or mucin. The clustered centrilob-ular cysts and ground-glass nodules were un-changed.
Dr. Ryan: This patient had two types of pul-monary lesions, which were probably not related.Pulmonary nodules and cysts can have many causes, including cancer, infections, and nonin-fectious inflammatory conditions. Sarcoidosis andWegener’s granulomatosis are not likely, giventhe findings on imaging. Langerhans’-cell histio-cytosis occurs in smokers and could explain thesmall nodules. Infection with Mycobacterium tuber-
culosis or other mycobacteria, as well as invasivefungal infections such as cryptococcosis, histo-
plasmosis, coccidioidomycosis, and paracoccidi-oidomycosis, could be considered. The small sizeand scattered nature of most of the lesions andthe absence of characteristic symptoms or signsmake most infections unlikely.
This patient initially had pleuritic, subscapularpain, and laboratory evaluation showed a slight-ly elevated peripheral-blood eosinophil count onseveral occasions. Peripheral eosinophilia (de-fined as an eosinophil count of >400 per cubicmillimeter) had actually been present for at least
3 years, and this patient traveled frequently toBrazil and had resided in Japan. Although thesefactors could prompt consideration of infection with lung parasites, such as in dirofilariasis andparagonimiasis, given this patient’s history of gastric cancer and smoking, his caregivers wereconcerned that the new pulmonary nodule could
l
A
B
C
Figure 1. CT of the Thorax.
A high-resolution CT scan with lung windows performed
4.5 months before admission shows scattered centrilob-ular ground-glass nodules (Panel A, arrows) and centrilob-
ular cysts, some of which are clustered (Panel B, arrows).A CT scan of the thorax 2 weeks before admission
(Panel C) shows a new solid nodule (arrow) in the leftlower lobe with surrounding ground-glass opacification.
reserved.Downloaded from www.nejm.org on October 1, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights

7/27/2019 Case 29 -2007.pdf
http://slidepdf.com/reader/full/case-29-2007pdf 5/8
case records of the massachusetts general hospital
n engl j med 357;12 www.nejm.org september 20, 2007 1243
be a manifestation of a malignant tumor in thelung — either metastatic gastric cancer or a new primary lung cancer. Evaluation of tissue speci-mens was warranted, and the nodule was resectedby means of video-assisted thoracoscopic surgery.
Clinical Diagnoses
Adenocarcinoma of the stomach, associated withH. pylori infection.
Possible metastasis of the cancer to the lung.
First Pathological Discussion
Dr. Richard L. Kradin: Examination of the specimenfrom the wedge resection of the left lung (Fig. 2A)revealed two tracts of necrotizing granulomatousinflammation with eosinophilic debris at theircenters. There was centriacinar emphysema of the
surrounding lung and pigmented macrophages, which are typically found in the lungs of smokers.
Within the debris at the center of the granu-lomas, examination at a higher magnificationshowed a severely degenerated helminth withtegument composed of layers of smooth muscleand dead tegumental cells (Fig. 2B). The morpho-logic characteristics were consistent with thoseof a trematode or fluke, but given the degree of degeneration, it was impossible to accurately mea-sure the size. A second fluke was seen in an ad- jacent section. Ova with refractile cortexes (Fig. 2C) were surrounded by granulomatous inflammationand foreign-body giant cells.
Paragonimus is the most common fluke toinfect the lung. It is a plump, oval fluke that onaverage is approximately 10 mm long and 5 mm wide, with both oral and ventral suckers. Thebody wall is composed of a tegument that in-cludes two layers of smooth muscle and tegu-mental cells and is characteristically covered withspines, which were not seen in this case. Theeggs are ovoid, varying in size among species
from 80 to 120 μm in length, and birefringent, with a double-layered cortex. The ova in this case were highly refractile, but they did not show strong birefringence under polarized light.
Schistosomiasis can also involve the lung,typically through translocation of ova into thepulmonary arterial system, but aberrant migra-tion of adult schistosomes into the lung doesoccasionally occur. Adult schistosoma are typi-cally longer and thinner than adult paragonimus,and their ova are larger. The cortical surfaces of
the ova of Schistosoma mansoni or S. haematobium may exhibit prominent lateral or terminal spines,respectively, but these were not evident in the
l
A
B
C
Figure 2. Lung-Biopsy Specimen (Hematoxylin and Eosin
Stain).
A linear tract of necrotizing granulomatous inflammation
with eosinophilic debris is shown (Panel A). At a higher
magnification (Panel B), the degenerating tegument of a trematode, coated with dense eosinophilic material,
is visible (arrow). This appearance, called the Splendore–
Hoeppli phenomenon, is caused by the deposition of immunoglobulin and other plasma proteins at the hostinterface with the organism. There was also granulo-
matous inflammation with multinucleated giant cells.The refractile cortex of a degenerating ovum is visible
within a granuloma, with surrounding tissue eosino-philia (Panel C).
reserved.Downloaded from www.nejm.org on October 1, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights

7/27/2019 Case 29 -2007.pdf
http://slidepdf.com/reader/full/case-29-2007pdf 6/8
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 357;12 www.nejm.org september 20, 20071244
case under discussion. The degree of degenerationof both the parasites and ova in this case madeit impossible to establish a specific morphologicdiagnosis with certainty.
In summary, the large lung nodule is due toinfection with a trematode, which cannot be de-finitively identified but is most consistent with
paragonimus. The small centrilobular nodulesseen on CT most likely represent changes causedby smoking, with respiratory bronchiolitis, centri-acinar emphysema, and peribronchiolar scarring.
Second Differential Diagnosis
Dr. Ryan: I first saw this patient after examinationof the lung-biopsy specimen showed evidence of a worm. Helminths that infect humans includeroundworms (nematodes), flatworms (tapewormsor cestodes), and flukes (trematodes). Flukes that
infect humans include intravascular, hepatic, pul-monary, and intestinal flukes (Table 1). World- wide, the majority of the illness and death relatedto human infection with trematodes is due toschistosoma species; however, the vast majority of the approximately 20 million persons world- wide infected with lung flukes are infected with
paragonimus species, usually Paragonimus wes-termani.
Paragonimiasis
The majority of paragonimus infections in humansare reported in East and Southeast Asia, includ-ing Japan, where this patient had lived. Most peo-ple become infected after eating raw or under-cooked crabs or crayfish or the meat of infectedparatenic hosts such as pigs or boars. Althoughthis patient ate shellfish, he reported that he didnot eat uncooked shellfish.
Table 1. Common Trematode (Fluke) Infections in Humans.*
Species Animal Reservoir Route of Human
InfectionMeans of FlukeReproduction
UsualLocationof AdultFlukes inHumans
Means of Passage of Eggs fromHumans
Usual Manifestationsin Humans
Blood flukes
Schistosoma mansoni,S. haematobium,S. japonicum,S. mekongi,S. intercalatum
Usually humans(especially forS. mansoni); alsononhuman pri-mates, other
mammals
Exposure to freshwater, with directskin penetrationby cercariae
Male–femalepairing
Bloodvessels
Feces,urine
Colonic inflammatory pol-yps, hepatosplenomeg-aly, hepatic cirrhosis,hematuria, urinary ob-struction and scarring,
bladder cancer
Lung flukes
Paragonimus spp. Cats, dogs, othermammals
Ingestion of infectivefreshwater crus-taceans
Hermaphroditic Lungs Sputum,feces
Chronic cough, blood-tinged sputum, chestpain, or none
Liver flukes
Opisthorchis viverrini,O. felineus,Clonorchis sinensis
Cats, dogs, pigs,rats, fish-eatingmammals
Ingestion of infectivefreshwater fish
Hermaphroditic Biliary tract Feces Cholangitis, biliary obstruc-tion, cholangiocar-cinoma
Fasciola hepatica,F. gigantica
Sheep, goats, cattle,buffalo, camels,pigs, horses,other herbivores
Ingestion of infectivefreshwater plants
Hermaphroditic Biliary tract Feces Abdominal pain, cholangi-tis, biliary obstruction
Intestinal flukes
Fasciolopsis buski Pigs Ingestion of infectivefreshwater plants
Hermaphroditic Intestines Feces None or abdominal painor diarrhea
Heterophyes hetero-phyes, Metagoni-mus yokogawai
Mammals, birds Ingestion of infectivefreshwater fish
Hermaphroditic Intestines Feces None or abdominal painor diarrhea
Echinostoma spp. Mammals Ingestion of infectivefreshwater fish,snails, or mussels
Hermaphroditic Intestines Feces None or abdominal painor diarrhea
* The intermediate host in all cases is freshwater snails.
reserved.Downloaded from www.nejm.org on October 1, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights

7/27/2019 Case 29 -2007.pdf
http://slidepdf.com/reader/full/case-29-2007pdf 7/8
case records of the massachusetts general hospital
n engl j med 357;12 www.nejm.org september 20, 2007 1245
After the ingestion of paragonimus, metacer-cariae penetrate the intestinal wall, cross the dia-phragm, and migrate through the lungs, wherethey may cause pneumothorax, pleural effusions,and diffuse or nodular pulmonary infiltrates.16 Eventually, cystic structures from 1 to 5 cm indiameter form; these structures often contain
two or three worms, are filled with thick bloody fluid, and typically have bronchopulmonary fistu-las. During the acute phase of the disease, ab-dominal pain, pleurisy, cough, fever, eosinophilia,and urticaria may develop. Chronic pulmonary paragonimiasis is usually relatively asymptomat-ic, but patients may have cough, with brown orblood-tinged sputum.
A presumptive diagnosis of pulmonary para-gonimiasis is made on the basis of characteristicfindings on imaging, persistent cough, and epi-demiologic and geographic risk factors. This pa-
tient had resided in Japan and had a history of abdominal pain, pleurisy, and mild eosinophilia,but no cough; the radiologic findings are consis-tent with paragonimiasis, although the absenceof a central cavity in the lung nodule makes para-gonimiasis less likely. A specific diagnosis restson the identification of eggs in sputum, bron-chial washings, gastric aspirates, or stool speci-mens or on the pathological identification of worms in resected tissue, as in this case. Sero-logic assays17 and antigen-detection assays18 arealso available.
Although the diagnosis of paragonimiasis istempting in this case, a number of atypical fea-tures raise questions about this diagnosis. Whereand when could this patient have acquired thisinfection? Although paragonimiasis is endemic insome areas of Latin America, to my knowledge,human acquisition has not been convincingly doc-umented in Brazil. Although this patient couldhave acquired the infection in Japan, his last visit was 7 years earlier, and it is diff icult to link thenew pulmonary nodule with such a distant pos-
sible exposure to paragonimus. There have beenrare case reports of paragonimiasis in the UnitedStates,19 usually after ingestion of undercookedcrayfish.
Schistosomiasis
Could the degenerated trematodes in the lungrepresent another type of fluke? Schistosomiasisdue to S. mansoni is endemic in many areas of Brazil. Pairs of adult worms usually reside in the
mesenteric veins; a local inflammatory responseto the eggs permits passive transit of the eggsinto the intestinal lumen (where they are shed infeces) and also into the liver (where they may causeinf lammation, f ibrosis, and cirrhosis). Eggs may passively enter the pulmonary circulation, usually by means of portal shunting caused by hepatic
schistosomiasis, where they can lead to pulmo-nary inflammation, fibrosis, hypertension, andcor pulmonale. Rarely, pairs of adult schistosom-al worms may migrate aberrantly into the pulmo-nary vasculature, and they have been identified within pulmonary nodules.20
The pathological evaluation shows the pres-ence of lung flukes and eggs that could be due toparagonimiasis or schistosomiasis. The sequenceof events, epidemiologic factors, and exposurehistory are most consistent with pulmonary schis-tosomiasis caused by a worm pair that entered
the pulmonary circulation at about the time of the onset of the pleurisy. To distinguish betweenparagonimiasis and schistosomiasis, we recom-mended the analysis of stool specimens for ovaand parasites and conducted serum antibody test-ing. The treatment for both infections involves thesame drug, praziquantel; it has a favorable side-effect profile and is highly effective.21
Dr. Edward T. Ryan’s Diagnosis
Infection with a lung fluke.
Second Pathological Discussion
Dr. Kradin: A serum sample from the patient wassent to the Centers for Disease Control and Pre- vention. An immunoblot for the paragonimusantibody was negative (this assay has a 96% sen-sitivity in egg-proven cases of P. westermani infec-tion in Southeast Asians, with a 99% specificity).In contrast, S. mansoni antibodies were detected with both an enzyme-linked immunosorbent as-
say and an immunoblot assay, confirming thediagnosis of S. mansoni infection. No antibodiesagainst S. haematobium were detected. No stoolspecimen was submitted for analysis.
Dr. Ryan: Dr. McDonough, can you tell us about the treatment and follow-up of this patient?
Dr. McDonough: The patient was treated with a2-day course of praziquantel. Follow-up CT scansof the chest showed no change in the diffuseground-glass cystic lesions and no further large
reserved.Downloaded from www.nejm.org on October 1, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights

7/27/2019 Case 29 -2007.pdf
http://slidepdf.com/reader/full/case-29-2007pdf 8/8
n engl j med 357;12 www.nejm.org september 20, 20071246
case records of the massachusetts general hospital
nodules. Unfortunately, 8 months after the lungbiopsy, symptoms of pancreatic and biliary-duct obstruction developed; laparotomy showed exten-sive metastatic adenocarcinoma within the abdo-men. Treatment with chemotherapy was initiated,and 10 months later, the patient has relatively asymptomatic, stable metastatic disease. He in-
tends to return to Brazil to be with his family. A Physician: Both gastric cancer and infection
with schistosoma are prevalent in Asia. Is there any link between gastric cancer and schistosomiasis?
Dr. Ryan: There is no recognized association of schistosomiasis with gastric or intestinal cancer.This contrasts with S. haematobium infection, which
is associated with an increased risk of squamous-cell carcinoma of the bladder.
Anatomical Diagnoses
Schistosoma mansoni infection with pulmonary in- volvement.
Respiratory bronchiolitis, peribronchiolar scar-ring, and centrilobular emphysema.
Adenocarcinoma of the distal stomach, afterHelicobacter pylori infection.
Chronic gastritis with intestinal metaplasia.
No potential conflict of interest relevant to this article was re-ported.
References
Cancer fact sheet. Geneva: WorldHealth Organization, 2006. (Accessed
August 24, 2007, at http://www.who.int/mediacentre/factsheets/fs297/en/index.html.)
Nomura A, Stemmermann GN, ChyouPH, Kato I, Perez-Perez GI, Blaser MJ. Heli-
cobacter pylori infection and gastric carci-noma among Japanese Americans in Ha- waii. N Engl J Med 1991;325:1132-6.
Nomura A, Stemmermann GN, ChyouPH, Perez-Perez GI, Blaser MJ. Helicobacterpylori infection and the risk for duodenaland gastric ulceration. Ann Intern Med1994;120:977-81.
Parsonnet J, Friedman GD, Vander-steen DP, et al. Helicobacter pylori infectionand the risk of gastric carcinoma. N Engl
J Med 1991;325:1127-31.Parsonnet J, Hansen S, Rodriguez L,
et al. Helicobacter pylori infection and gas-tric lymphoma. N Engl J Med 1994;330:1267-71.
El-Omar EM, Rabkin CS, GammonMD, et al. Increased risk of noncardiagastric cancer associated with proinflam-matory cytokine gene polymorphisms.Gastroenterology 2003;124:1193-201.
Hamada GS, Kowalski LP, NishimotoIN, et al. Risk factors for stomach cancerin Brazil. II. A case-control study among Japanese Brazilians in São Paulo. Jpn JClin Oncol 2002;32:284-90.
Lourenço LG, Hamada GS. Gastric
1.
2.
3.
4.
5.
6.
7.
8.
cancer in Brazil. Gastric Cancer 2001;4:103-5.
Nishimoto IN, Hamada GS, KowalskiLP, et al. Risk factors for stomach cancerin Brazil. I. A case-control study amongnon-Japanese Brazilians in São Paulo. Jpn J Clin Oncol 2002;32:277-83.
Ashour AA, Magalhães PP, MendesEN, et al. Distribution of vacA genotypesin Helicobacter pylori strains isolated fromBrazilian adult patients with gastritis,duodenal ulcer or gastric carcinoma. FEMSImmunol Med Microbiol 2002;33:173-8.
Nomura AM, Lee J, StemmermannGN, Nomura RY, Perez-Perez GI, BlaserMJ. Helicobacter pylori CagA seropositiv-ity and gastric carcinoma risk in a JapaneseAmerican population. J Infect Dis 2002;
186:1138-44.Selbach M, Moese S, Hurwitz R,
Hauck CR, Meyer TF, Backert S. The Heli-cobacter pylori CagA protein induces cor-tactin dephosphorylation and actin rear-rangement by c-Src inactivation. EMBO J2003;22:515-28.
Chow WH, Blaser MJ, Blot WJ, et al.An inverse relation between cagA+ strainsof Helicobacter pylori infection and risk of esophageal and gastric cardia adeno-carcinoma. Cancer Res 1998;58:588-90.
Loffeld RJ, Werdmuller BF, Kuster JG,Perez-Perez GI, Blaser MJ, Kuipers EJ.Colonization with cagA-positive Helico-bacter pylori strains inversely associated
9.
10.
11.
12.
13.
14.
with ref lux esophagit is and Barret t’sesophagus. Digestion 2000;62:95-9.
Devesa SS, Blot WJ, Fraumeni JF Jr.Changing patterns in the incidence of esophageal and gastric carcinoma in theUnited States. Cancer 1998;83:2049-53.
Jeon K, Koh WJ, Kim H, et al. Clinicalfeatures of recently diagnosed pulmonary paragonimiasis in Korea. Chest 2005;128:1423-30.
Slemenda SB, Maddison SE, Jong EC,Moore DD. Diagnosis of paragonimiasisby immunoblot. Am J Trop Med Hyg 1988;39:469-71.
Zhang Z, Zhang Y, Shi Z, et al. Diag-nosis of active Paragonimus westermaniinfections with a monoclonal antibody-based antigen detect ion assay. Am J Trop
Med Hyg 1993;49:329-34.DeFrain M, Hooker R. North Ameri-
can paragonimiasis: case report of a se- vere clinical infect ion. Chest 2002;121:1368-72.
Lambertucci JR, Moreira RF, BarbosaAJ. Solitary pulmonary nodule caused by Schistosoma mansoni in a patient withmedullary thyroid carcinoma. Rev Soc BrasMed Trop 2005;38:536-7.
Johnson RJ, Jong EC, Dunning SB,Carberry WL, Minshew BH. Paragonimia-sis: diagnosis and the use of praziquan-tel in treatment. Rev Infect Dis 1985;7:200-6.Copyright © 2007 Massachusetts Medical Society.
15.
16.
17.
18.
19.
20.
21.
Lantern Slides Updated: Complete PowerPoint Slide Sets from the Clinicopathological Conferences
Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a teaching exercise or reference material is now eligible toreceive a complete set of PowerPoint slides, including digital images, with identifying legends, shown at the live Clinicopathological Conference (CPC)that is the basis of the Case Record. This slide set contains all of the images from the CPC, not only those published in the Journal. Radiographic, neuro-logic, and cardiac studies, gross specimens, and photomicrographs, as well as unpublished text slides, tables, and diagrams, are included. Every year 40sets are produced, averaging 50-60 slides per set. Each set is supplied on a compact disc and is mailed to coincide with the publication of the Case Record.
The cost of an annual subscription is $600, or individual sets may be purchased for $50 each. Application forms for the current subscription year, which began in January, may be obtained from the Lantern Slides Service, Department of Pathology, Massachusetts General Hospital, Boston, MA02114 (telephone 617-726-2974) or e-mail [email protected].
reserved.Downloaded from www.nejm.org on October 1, 2007 . Copyright © 2007 Massachusetts Medical Society. All rights


















