
Emergency Management of Drug Overdose Russell Sharpswain, DO, FACEP, FAAEM December 3, 2015.
Upload
stella-sheltonCategory
view
215download
0
Carson R. Harris, MD, FAAEM, FACEPRegions Hospital Clinical Toxicology ServiceEmergency Medicine Department
Objectives Discuss the toxicological effects of salicylate overdose
Identify key management issues Discuss the limitations of the Done nomogram and how to avoid pitfalls of management
History and Demographics Hippocrates – 5th century B.C.▪ Powder from the willow bark
1800s sodium salicylate for arthritis▪ Abdominal pain
Felix Hoffmann▪ Acetylsalicylic acid (ASA)
Introduced 100 years ago▪ Antipyretic, analgesic, anti-inflammatory
History and Demographics Decline in use, but…▪ Prophylactic for migraine, colon ca▪ Antiplatelet agent▪ Decline in incidence of Reye’s
Childproof caps – 1970s legislature
OTC meds▪ Combined with antihistamines, caffeine, barbs, and opioids
Salicylate formulations Oil of wintergreen: 98% methyl salicylate▪ 1400 mg/mL
Bismuth subsalicylate Aggrenox
Therapeutic doses Pediatric 10-20 mg/kg Adults 650-1000 mg q 4-6 hrs▪ Produce a serum level of 5-10 mg/dL
Potential Toxic Acute dose > 150 mg/kg
Serious toxicity: 300-500 mg/kgChronic toxicity: >100 mg/kg/day
Peak levels Therapeutic – 1-2 hours Therapeutic EC – 4-6 hours OD – 10-60 hours▪ Reason for delay ? Concretions, contraction of the pylorus or combination of drugs that delay gastric emptying (opioids and anticholinergics)
Liquids absorbed in 1 hr
Distribution is facilitated by pH
Elimination dependent on dose First order kinetic to zero order ▪ From 4 hours to 15-29 hours
A 24-year-old male presented to the ED with nausea, vomiting, tinnitus, and tachypnea after ingesting 100 aspirin tablets. His 4-hour salicylate level was 78 mg/dL; Chem-8 revealed Na 143, Cl 105, K 4.2, HCO3 17; the ABGs showed pH 7.38, pO2 107, and pCO2 27 on room air. He was initially treated with reasonable volume and admitted to the ward.
Orders for sodium bicarbonate were given to alkalinize the urine, but this was ineffective in raising urine pH. Approximately 6 hours later the attending was notified that the patient had become confused.
He was transferred to the ICU where he was sedated and intubated.
Approximately 20 minutes after intubation, the patient rapidly deteriorated and died.
ASA is hydrolyzed to salicylic acid Responsible for therapeutic and toxic effects
Direct stimulation of respiratory center Medulla
Uncouples oxidative phosphorylation Increase in O2 consumption and CO2 production▪ Increase respiration▪ Respiratory alkalosis
Renal excretion of bicarb, Na and K Metabolic acidosis
Inhibition of mitochondrial respiration Increase pyruvate and lactic acid▪ Metabolic acidosis
Disruption of Krebs cycle metabolism and glycolysis Hyperglycemia, ketonemia
Dehydration Hyperpnea Diaphoresis Vomiting Fever (increased muscle metabolism)
Vasoconstriction of auditory microvasculature
Enhance insulin secretion => hypoglycemia
Decrease peripheral glucose utilization => hyperglycemia
Increase permeability of pulmonary vasculature
Increase the production of leukotrienes
Stimulate medullary chemoreceptor trigger zone
Hematologic effects
ASPIRIN Mnemonic Altered mental status (lethargy – coma) Sweating/diaphoresis Pulmonary edema Increased vital signs (HTN, inc RR, inc T, tachycardia)
Ringing in the ears Irritable Nausea and vomiting
Early Nausea, vomiting, diaphoresis, tinnitus, deafness▪ Level 25-30 mg/dL
HyperventilationLater
Hypotension, NCPE, oliguria, acidemia, cerebral edema, delirium, seizure, coma
Classic acid-base disturbance AGMA Respiratory alkalosis with metabolic acidosis
Acidemia Increases tissue distribution ▪ Brain, heart, lung
Severe hypokalemia
NCPE Older patients Smokers Levels >100 mg/dL Acidemia CNS involvement (hallucinations, sz)
Chronic toxicity
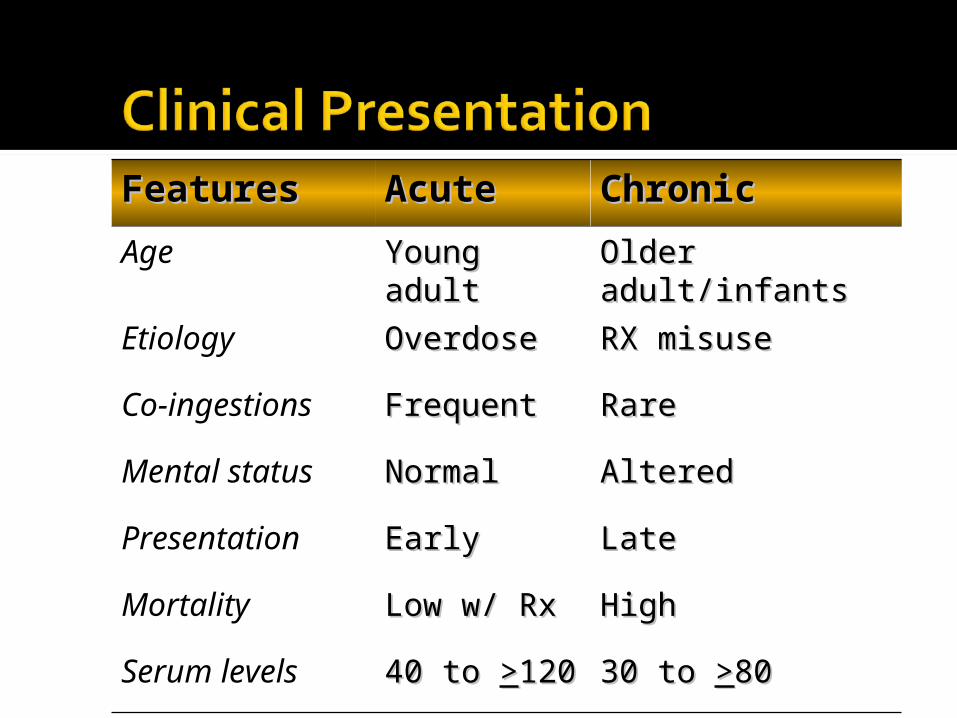
FeaturesFeatures AcuteAcute ChronicChronicAge Young Young
adultadultOlder Older adult/infantsadult/infants
Etiology OverdoseOverdose RX misuseRX misuse
Co-ingestions
FrequentFrequent RareRare
Mental status
NormalNormal AlteredAltered
Presentation EarlyEarly LateLate
Mortality Low w/ RxLow w/ Rx HighHigh
Serum levels 40 to 40 to >>120120 30 to 30 to >>8080
Salicylate level Peak 4-6 hr EC and SR preparations late rise Every 2-4 hours until clearly decreasing▪ Then q 4-6 until <30 mg/dL
Always confirm units!▪ Mg/dL vs. mg/L
Done Nomogram (Pediatrics 1960)
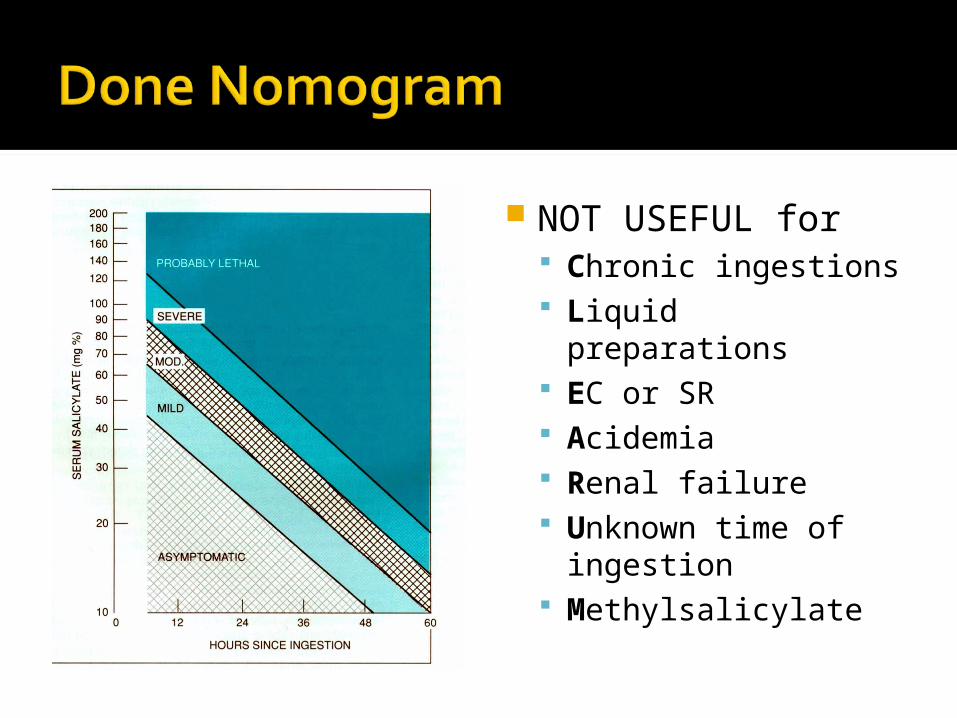
NOT USEFUL for Chronic ingestions
Liquid preparations
EC or SR Acidemia Renal failure Unknown time of ingestion
Methylsalicylate
Severity of ingestion Serum levels Acid-base status Acuteness of ingestion Mental status
Bedside Tests Trinder’s reagent – 10% ferric chloride
Ames phenistix
Chemistry Panel Q 4-6 h
LFTsCoagulation studiesABGsAPAPConsider: CT, Serum osm, ketones, LP, CO, serum Fe, blood cultures
Gastric lavage / WBI Activated charcoal - MDAC Hydration and electrolyte replacement
Correct hypokalemia aggressively Urine alkalinization
Increase salicylate excretion 1-2 mEq/kg NaHCO3 bolus IV Then 150 mL in 850 ml D5W run 1.5-2 times maintenance
Caution in elderly and chronic Monitor UO
Dialysis Serum levels > 100 in acute Levels > 60 in chronic Pulmonary edema Renal failure CHF Poor response to standard Rx AMS and acidemia
Enteric Coated aspirin Can cause delayed symptom onset
Don't wait for clinical deterioration. Alert you nephrology team early and call the poison center even earlier.
Serial salicylate levels are imperative.
One teaspoon of methyl salicylate contains 7,000 mg of salicylate which is equivalent to approximately 21 regular strength aspirin tablets!
The presence of fever is a poor prognostic sign in adults!
Cerebrospinal fluid salicylate levels correlate with symptoms better than blood levels
The Done nomogram, has limited usefulness
Be aware of the proper unit of measure (mg/dL not mg/L or µg/L or mmol/L)!
Start potassium supplementation early (in the absence of renal insufficiency) because hypokalemia makes urinary alkalization impossible!
Multiple-dose activated charcoal and alkalinization are currently the most popular methods of treatment.
Be aggressive. Dialyze early if signs of toxicity are evident.
ASA and elderly Impaired renal function▪ Decreased elimination
Impaired hepatic function The risk of salicylate nephrotoxicity is increased with age,
Upper gastrointestinal bleed is associated with increased mortality in older age groups.
Mortality and Epidemiology From 15% to 1.7% in 1977 Second leading cause of death from overdose in US (Analgesics first).
Approximately 500,000 overdoses annually
Female, age 20-29, single, employed, no history of drug abuse
Approximately 70% die pre-hospital
Indications Depression Chronic pain syndromes OCD Panic and Phobic disorders Migraine prophylaxis Peripheral neuropathies
Acute Toxic Doses Fatal ingestions range 10-210 mg/kg
2-4 mg/kg is therapeutic, 20 mg/kg is potentially fatal
Variable response
Absorption Rapidly and completely absorbed Massive OD delays absorption Enterohepatic re-circulation secretes 30%
Distribution Wide range in Vd (15-40 L/kg)▪ Genetic variation▪ Lipophilic▪ Elderly has higher Vd
Distribution (cont’d) Tissue levels usually 10 times plasma levels
Protein binding usually exceeds 90% with some variations▪ pH dependent
Elimination Genetic component Metabolism influenced by other drugs
Therapeutic effects Not completely understood Blocks serotonin and NE uptake Anticholinergic effects
Cardiac Effects Sinus tachycardia, dysrhythmias▪ Na channel blockade – quinidine effect
Hypotension▪ Alpha adrenergic blockade and NE depletion
Conduction delays / blocks
CNS Anticholinergic▪ Excitation, confusion, hallucination, ataxia
Seizures Coma
Respiratory Pulmonary edema ARDS Aspiration pneumonia
Gastrointestinal Delayed gastric emptying Decreased motility Prolonged transit time
Case #1 25 year-old man ingested 60 tablets of Elavil 50 mg each. He presented to the ED about 45 minutes post ingestion agitated and confused. Possibly hallucinating. BP 145/94, P 112, R22, T99.6. He became more agitated and combative and was intubated, lavaged and given AC.
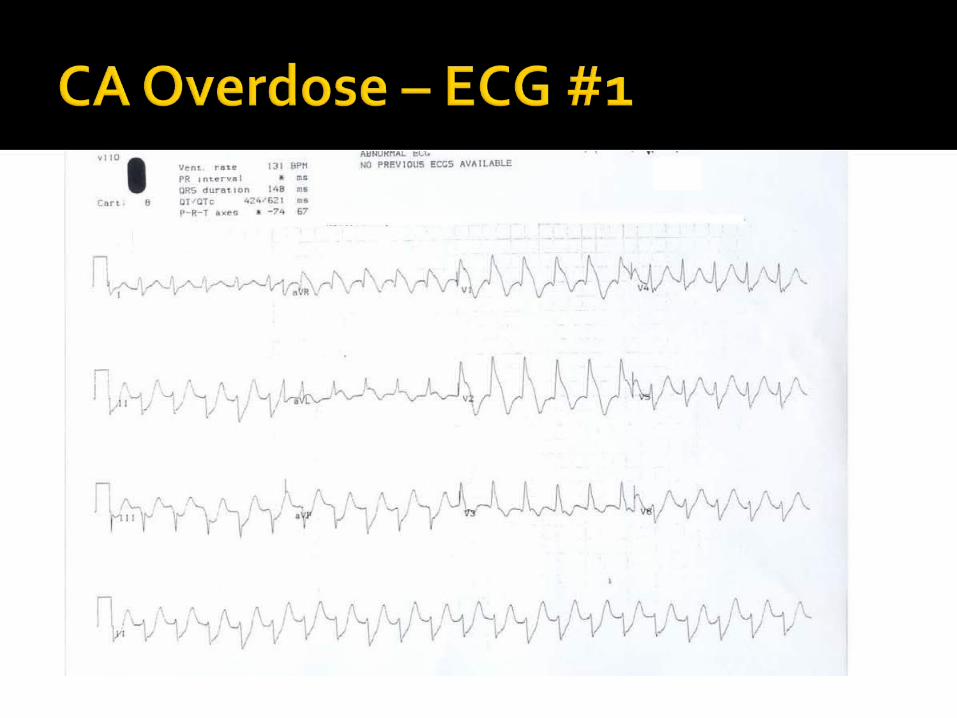
EKG revealed QRS 108 with rate 114 What are the critical ECG changes?
Prolongation of the QRS complex: ▪ Blockage of fast sodium channels slows phase 0 depolarization of the action potential.
▪ Ventricular depolarization is delayed, leading to a prolonged QRS interval. Patients with QRS intervals >100 ms are at risk for seizures and patient with QRS intervals >160 ms are at risk for arrhythmias.
▪ QRS interval is evaluated best using the limb leads.
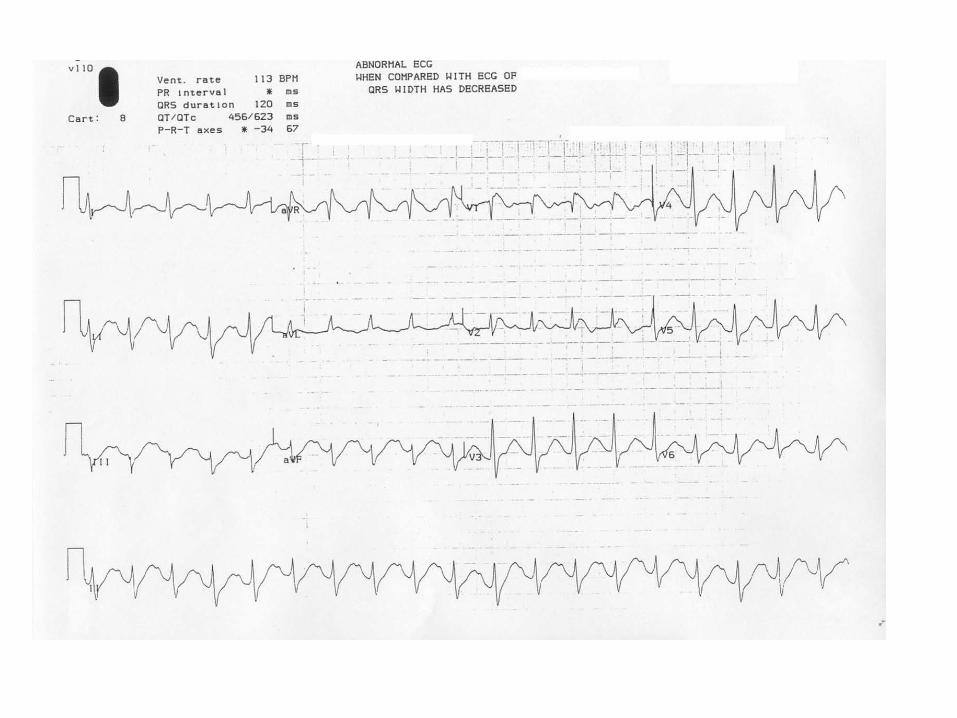
R wave in aVR >3 mm: ▪ greater selectivity and toxicity to the distal conduction system of the right side of the heart.
▪ effect can be observed as an exaggerated height of the R wave aVR.
▪ may be more predictive of seizure and arrhythmia than prolongation of the QRS complex.
R/S ratio >0.7 in aVR QT interval prolongation Arrhythmias How do you treat this?
ABCs Activated Charcoal: 30-50 gm
Sodium Bicarbonate Dose Endpoint
What is the mechanism?
Alkalinization appears to uncouple TCA from myocardial sodium channels.
Alkalinization may increase protein binding
Increases the extracellular sodium concentration improves the gradient across the channel.
The initial bolus of 1-2 mEq/kg A constant infusion of sodium bicarbonate commonly accepted clinical practice without any controlled studies validating the optimum administration
100 to 150 mEq of sodium bicarbonate to each liter of 5% dextrose, ▪ the resulting solution is hypotonic or nearly isotonic.
What if NaHCO3 doesn’t work? may require treatment with lidocaine and/or magnesium sulfate.
Class Ia and Ic agents contraindicated
Beta blockers and CCB▪ Worsen or potentiate hypotension
Hypotension, Persistent Direct acting alpha agonists, such as norepinephrine and phenylephrine
Dopamine may not be as effective ▪ Require release of endogenous catecholamines that may be depleted during TCA toxicity.
Dopamine or dobutamine alone may result in unopposed beta-adrenergic activity due to TCA induced alpha blockade and, therefore, may worsen hypotension.
Vasopressin (ADH)
What about Seizures from TCA Usually brief (<1 min) self-limiting acidosis increase cardiovascular toxicity.
Benzodiazepines Phenytoin is no longer recommended
limited efficacy and possible prodysrhythmic.
Phenobarbital may be used as a long-acting anticonvulsant.
Agitation from TCA Anticholinergic effects Benzodiazepines are also the treatment of choice
Physostigmine is contraindicated in TCA overdoses▪ May cause bradycardia and asystole in the setting of TCA cardiotoxicity.
Flumazenil is contraindicated even in the presence of a benzodiazepine co-ingestion. ▪ Several case reports - seizures
Emergency department discharge criteria At least 6 hour observation period No significant sign of toxicity during observation period, including normal follow-up ECG prior to discharge
Accidental ingestion Appropriate follow-up measures in place Adequately supervised home environment


















