Carotid Magnetic Resonance Imaging Depicted Intraplaque ... · Carotid Magnetic Resonance Imaging...
209
Carotid Magnetic Resonance Imaging Depicted Intraplaque Hemorrhage and a High-Risk Cardiovascular and Cerebrovascular Phenotype By Navneet Singh A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Institute of Medical Science University of Toronto © Copyright by Navneet Singh 2018
Transcript of Carotid Magnetic Resonance Imaging Depicted Intraplaque ... · Carotid Magnetic Resonance Imaging...

Carotid Magnetic Resonance Imaging Depicted Intraplaque
Hemorrhage and a High-Risk Cardiovascular and
Cerebrovascular Phenotype
By
Navneet Singh
A thesis submitted in conformity with the requirements
for the degree of Doctor of Philosophy
Institute of Medical Science
University of Toronto
© Copyright by Navneet Singh 2018

ii
Carotid Magnetic Resonance Imaging Depicted Intraplaque
Hemorrhage and a High-Risk Cardiovascular and
Cerebrovascular Phenotype Navneet Singh
Doctor of Philosophy
Institute of Medical Science
University of Toronto
2018
Abstract Intraplaque hemorrhage is an independent marker of cardiovascular outcomes including stroke
and myocardial infarction. Magnetic resonance imaging allows for the direct visualization of
intraplaque hemorrhage in the vessel wall of the carotid arteries. This thesis reports data from an
institutional magnetic resonance depicted intraplaque hemorrhage experience and clinical trials.
The work herein addresses areas particularly sparse on the relationship of intraplaque
hemorrhage with cardiovascular risk factors and its potential role in stroke, specifically reporting
on i) age-specific sex differences in low-grade stenosis, ii) the role in ipsilateral embolic stroke
of undetermined source, and iii) the relationship with a high-risk cardiovascular phenotype. The
results in this thesis support our hypotheses that i) males have greater age-specific odds of
magnetic resonance imaging depicted carotid intraplaque hemorrhage compared to females, and
that with increasing age, the odds of carotid intraplaque hemorrhage in females becomes closer
to that of males, ii) patients with embolic stroke of undetermined source have carotid intraplaque
hemorrhage ipsilateral to the affected brain, and iii) patients with carotid intraplaque hemorrhage
are of a high-cardiovascular risk. The culmination of projects supports the notion that intraplaque
hemorrhage is related to a high-risk cardiovascular phenotype and a need for the quantification

iii
of intraplaque hemorrhage is realized to further understand the significance of volume of
intraplaque hemorrhage, longitudinal changes in intraplaque hemorrhage over time, and
relationship of intraplaque hemorrhage with clinical outcomes. The final project in this thesis
therefore reports the development of a quantitative imaging analysis protocol, as well as its
reliability and agreement with an established standard. The protocol is intended for use on
carotid trial imaging data presently being acquired as part of the Canadian Atherosclerosis
Imaging Network Project 1.

iv
Dedication
In loving memory of my grandfather, Lt. Joginder Singh Baweja (May 26, 1929-June 12, 2016),
for taking an interest in the progress of my training upon each meeting, serving as a personal
and professional sounding board, and always encouraging me to go one step further.

v
Acknowledgments
First and foremost, I thank my supervisor, Dr. Alan R. Moody, for his supervision, mentorship,
and for piquing my interest in trials of vessel wall magnetic resonance imaging. His work to
potentially translate carotid intraplaque hemorrhage magnetic resonance imaging into clinical
practice to improve patient outcomes persuaded me to work alongside him for the past decade,
first as a medical student starting in 2006 and then via the Clinician Investigator Program’s joint
PhD and residency training pathway. I sincerely appreciate the opportunity to participate in his
competitively funded clinical imaging trials, including the Canadian Atherosclerosis Imaging
Network Project 1. Many lessons were learned including the day-to-day management of a
laboratory, obtaining grants, setting up protocols, reviewing images, administration such as
reporting incidental imaging findings and collaborating with and mentoring junior group
members, and the importance of granular and meticulous data collection to ensure that scientific
observations do not go unseen.
Many others have also helped me navigate my studies. My Program Advisory Committee
members, including Drs. Subodh Verma, Richard I. Aviv, and Laurent Milot, provided guidance
along the way. Drs. Eric Bartlett and Linda Probyn, my current and past residency program
directors, supported joint PhD and residency training. My sustained interest in academic
medicine is inspired by past and present mentors, and I am grateful to Drs. Gianluca Iacobellis,
David J. Gladstone, Sandra E. Black, Andrea Doria, Heather M. Arthur, Bhagu R. Bhavnani,
Arya M. Sharma, Del Harnish, Erika Kustra, Anna E. Zavodni, Sean P. Symons, and Allan J.
Fox.
To present and past research friends at the Sunnybrook Research Institute and the
Vascular Biology Imaging Research Group, thank you for your company and fellowship. My
infinitely patient and loving family has provided a vast array of the requisite supports to succeed
in completing my training—my parents, Tejinderpal Singh and Manninder Singh, and my
siblings, Raviraj Singh, Amandeep Singh, and Harleen Rosie Singh.
No words can convey my love and appreciation to Harleen K. Khanijoun my intelligent,
supportive, and insightful partner. I look forward to the next chapter along with our son Ajay and
daughter Apar, who have both unwittingly brought perspective and unfettered joy.

vi
Finally, I am grateful to the University of Toronto Diagnostic Radiology Residency
Program, Royal College of Physicians and Surgeons of Canada’s Clinician Investigator Program,
the Institute of Medical Science Doctor of Philosophy Program, and Cardiovascular Sciences
Collaborative Program. Training in these programs has helped me gain skills to advance me
toward a career as an independent physician-scientist. The programs have allowed for a
multitude of endeavors, a small fraction of which are reflected in this thesis.
Funding acknowledgments for some of the work included in this body of work are 2012-
2016 Canadian Institute of Health Research (CIHR) Fellowship in Priority Announcement:
Patient-Oriented Research (FRN 120988), 2015 RSNA R&E Research Resident Grant
(#RR1561), 2012 RSNA R&E Research Resident Grant (#RR1237), and 2012 Physician
Services Incorporated Grant.

vii
Contributions
Navneet Singh was responsible for the preparation of the thesis, including conception, ethics
approval, grant funding including CIHR FRN 120988, RSNA #1561, RSNA #1237, and PSI
Foundation 2012, data collection, analysis, and writing. The work contained in this thesis was
made possible by:
Alan R. Moody, supervisor, for supervision, assistance with all aspects of the thesis,
including study conception, direction, peer-review, access to patient data and images, and
laboratory resources;
Richard Aviv, Subodh Verma, Laurent Milot, PAC members, for thesis direction and
peer review;
Pascal Tyrrell, for database assistance and statistical peer-review of Chapter 2;
Kush Kapur, Alex Kiss, for statistical assistance with Chapters 2 and 4, respectively;
Bowen Zhang, Isabella Kaminski, and Genevieve-Rochon Terry, for assistance with data
collection related to Chapters 2 and 4;
David J. Gladstone, for access to clinical trial data and peer review of Chapter 3, and also
those who contributed to patient recruitment or data collection at Sunnybrook Health Sciences
Centre, Toronto (V. Basile, K. Boyle, J. Hopyan, R. Swartz, H. Vaid, G. Valencia, J. Ween, R.
Aviv, S. Symons, A. Fox, P. Howard, R. Yeung), trial design and operations (J. Hall, P. Dorian,
M. Spring, M. Mamdani, K. Thorpe, and members of the EMBRACE steering committee, and
staff at the Applied Health Research Centre, Li Ka Shing Knowledge Institute of St. Michael’s
Hospital, Toronto).
Tishan Maraj, for serving as a second image-rater for Chapter 5; and
Vivek Thayalasuthan, Lena Koh, and Natalie Rashkovan for research assistance
including ethics approval.

viii
Table of Contents
Dedication ...................................................................................................................................... iv
Acknowledgments............................................................................................................................v
Contributions................................................................................................................................. vii
Table of Contents ......................................................................................................................... viii
Tables ........................................................................................................................................... xiii
Figures.......................................................................................................................................... xiv
Abbreviations .............................................................................................................................. xvii
Peer-Reviewed Publications ........................................................................................................ xxi
Chapter 1—Carotid Atherosclerosis Imaging from Lumen to the Vessel Wall .........................1
1.1 Overview ..............................................................................................................................2
1.2 Cardiovascular Disease Burden ...........................................................................................4
1.2.1 Worldwide................................................................................................................4
1.2.2 North America .........................................................................................................5
1.3 Atherosclerosis .....................................................................................................................7
1.3.1 Pathological Stages of the Disease ..........................................................................7
1.3.2 Classification..........................................................................................................10
1.3.3 Progression .............................................................................................................13
1.3.4 End-Organ Outcomes.............................................................................................17
1.4 Carotid Artery Atherosclerosis ..........................................................................................24
1.4.1 Anatomy .................................................................................................................24
1.4.2 Anatomical Site Predilection .................................................................................28
1.4.3 Ischemic Stroke ......................................................................................................30
1.4.4 Systemic Disease ...................................................................................................34
1.5 Carotid Artery Stenosis ......................................................................................................34
1.6 Carotid Intima-Media Thickness .......................................................................................43
1.7 Advanced Carotid Plaque Imaging: Modalities, Biomarkers, and Cardiovascular
Disease ...............................................................................................................................45
1.7.1 Ultrasound ..............................................................................................................48

ix
1.7.2 Computed Tomography .........................................................................................50
1.7.3 Positron Emission Tomography .............................................................................54
1.7.4 Magnetic Resonance Imaging ................................................................................56
1.8 Carotid Magnetic Resonance-depicted Intraplaque Hemorrhage Imaging ........................63
1.8.1 Carotid Artery Disease Evaluation Paradigm Shift and Knowledge Gaps ............65
1.9 Aims and Hypotheses ........................................................................................................69
1.9.1 Age-Specific Sex Differences in MRI Depicted Carotid Intraplaque
Hemorrhage ............................................................................................................69
1.9.2 Carotid Magnetic Resonance Depicted Intraplaque Hemorrhage in Embolic
Stroke of Undetermined Source .............................................................................70
1.9.3 Identifying a High-risk Cardiovascular Phenotype by Carotid MRI-depicted
Intraplaque Hemorrhage ........................................................................................70
1.9.4 A Combined 3D Black-blood and Time-of-flight Magnetic Resonance
Imaging Approach for the Volumetric Quantification of Carotid Artery Vessel
Wall and Intraplaque Hemorrhage .........................................................................70
Chapter 2—Age-Specific Sex Differences in Magnetic Resonance Imaging Depicted
Carotid Intraplaque Hemorrhage...............................................................................................71
2.1 Overview ............................................................................................................................72
2.2 Introduction ........................................................................................................................72
2.3 Materials and Methods .......................................................................................................74
2.3.1 Participants and Study Groups ...............................................................................74
2.3.2 Carotid MRI Protocols ...........................................................................................74
2.3.3 Carotid IPH Imaging Analysis and Reliability ......................................................76
2.3.4 Clinical Records Review ........................................................................................78
2.3.5 Source Data Collection, Organization, and Storage ..............................................78
2.3.6 Data Cleaning, Handling of Missing Data, and Validation ...................................83
2.3.7 Statistical Analysis .................................................................................................86
2.4 Results ................................................................................................................................86
2.5 Discussion ..........................................................................................................................91
2.5.1 Findings..................................................................................................................91
2.5.2 Novelty ...................................................................................................................91

x
2.5.3 Other Studies ..........................................................................................................92
2.5.4 Strengths ................................................................................................................93
2.5.5 Limitations .............................................................................................................93
2.5.6 Future Studies ........................................................................................................94
2.6 Conclusions ........................................................................................................................95
Chapter 3—Carotid Magnetic Resonance Imaging Depicted Intraplaque Hemorrhage in
Embolic Stroke of Undetermined Source .................................................................................96
3.1 Overview ............................................................................................................................97
3.2 Introduction ........................................................................................................................97
3.3 Materials and Methods .......................................................................................................98
3.4 Results ..............................................................................................................................100
3.5 Discussion ........................................................................................................................102
Chapter 4—Identifying a High-Risk Cardiovascular Phenotype by Carotid Magnetic
Resonance Imaging Depicted Intraplaque Hemorrhage .........................................................104
4.1 Overview ..........................................................................................................................105
4.2 Introduction ......................................................................................................................105
4.3 Methods............................................................................................................................106
4.3.1 Participants ...........................................................................................................106
4.3.2 MRI Protocol .......................................................................................................108
4.3.3 Evaluation of Intraplaque Hemorrhage ................................................................108
4.3.4 Data Collection and Definition of Outcomes .......................................................109
4.3.5 Statistical and Data Analysis ...............................................................................110
4.4 Results ..............................................................................................................................110
4.5 Discussion ........................................................................................................................113
Chapter 5—A Combined 3D Black-Blood and Time-of-flight Magnetic Resonance
Imaging Approach for the Volumetric Quantification of Carotid Artery Vessel Wall and
Intraplaque Hemorrhage..........................................................................................................116
5.1 Overview ..........................................................................................................................117
5.2 Introduction ......................................................................................................................117
5.3 Methods............................................................................................................................118
5.3.1 Study Population ..................................................................................................119

xi
5.3.2 MRI Protocol .......................................................................................................119
5.3.3 MRI Post-processing ............................................................................................121
5.3.4 Vessel Wall Segmentation ...................................................................................122
5.3.5 Intraplaque Hemorrhage Segmentation ...............................................................123
5.3.6 MRI Review .........................................................................................................124
5.3.7 Statistical Analysis ...............................................................................................124
5.4 Results ..............................................................................................................................124
5.4.1 Intra- and Inter-Rater Reliability .........................................................................126
5.4.2 Scan-Rescan Reliability .......................................................................................127
5.4.3 3D vs. 2D carotid artery MRI ..............................................................................127
5.5 Discussion ........................................................................................................................129
5.6 Conclusions ......................................................................................................................131
Chapter 6—General Discussion ..............................................................................................133
6.1 Summary ..........................................................................................................................134
6.2 Novelty and Strengths ......................................................................................................135
6.3 Limitations .......................................................................................................................136
6.4 Relationship to Other Work .............................................................................................137
6.5 Conclusions ......................................................................................................................141
Chapter 7—Future Directions .................................................................................................142
7.1 Opportunity for Study ......................................................................................................143
7.2 Proposal Motivation .........................................................................................................143
7.3 Carotid Intraplaque Hemorrhage and Neurovascular Imaging Outcomes .......................145
7.4 Carotid IPH, Lacunes, and Brain Atrophy .......................................................................146
7.5 Carotid IPH and Clinical Cerebrovascular Outcomes .....................................................146
7.6 Carotid IPH and Cognitive Impairment ...........................................................................147
7.6.1 Novelty of the Proposed Study ............................................................................147
7.6.2 Clinical Implications ............................................................................................148
7.6.3 Preliminary Studies ..............................................................................................148
7.7 Research Design and Methods .........................................................................................149
7.7.1 Overview and Study Design ................................................................................149
7.7.2 Population ............................................................................................................149

xii
7.7.3 Image Acquisitions ..............................................................................................149
7.7.4 Image Analysis: Quantification of IPH and Neuroimaging Features of SVD .....150
7.7.5 Statistical Analysis ...............................................................................................151
7.7.6 Strengths and Limitations ....................................................................................152
7.8 Future of Cardiovascular Imaging ...................................................................................152
Chapter 8—References ...........................................................................................................154

xiii
Tables
Table 1.1: Lesion Nomenclature and Histological Features Along with Cross-
Sectional Sketch for the Stary Classification of Atherosclerosis.
Table 1.2: Morphological Features Related to Plaque Instability.
Table 1.3: Ultrasound Velocity Cut-off points to Classify Grade of Carotid Stenosis.
Table 1.4: Sensitivity and Specificity of Time-of-Flight and Contrast Enhanced
Magnetic Resonance Angiography for Evaluation of Stenosis against Gold
Standard Digital Subtraction Angiography.
Table 1.5: Plaque Component Signal Characteristics on Carotid Magnetic Resonance
Imaging.
Table 2.1: Summary of Data Variables Collected.
Table 2.2: Database Cleaning Steps.
Table 2.3: Demographic Characteristics of Study Participants.
Table 2.4: Age-specific Differences in Carotid Intraplaque Hemorrhage between
Men and Women.
Table 3.1: Characteristics of Study Participants.
Table 4.1: Demographic Characteristics of Participants by the Presence of Magnetic
Resonance Depicted Intraplaque Hemorrhage.
Table 4.2: Cardiovascular Events by the Presence of Magnetic Resonance Depicted
Intraplaque Hemorrhage.
Table 4.3: Odds Ratios of a Composite Cardiovascular Event.
Table 5.1: Carotid Magnetic Resonance Imaging Acquisition Parameters.
Table 5.2: Demographic Characteristics of Study Participants.
Table 5.3: Reliability of 3-Dimensional and 2-Dimensional Carotid 3-Tesla Magnetic
Resonance Imaging for the Volumetric Quantification of Vessel Wall and
Intraplaque Hemorrhage.
Table 5.4: Agreement of 3-Dimensional and 2-Dimensional Carotid Artery Magnetic
Resonance Imaging for the Volumetric Quantification of Vessel Wall.

xiv
Figures
Figure 1.1: Schematic of Carotid Intraplaque Hemorrhage.
Figure 1.2: Distribution of Noncommunicable Disease Mortality Worldwide.
Figure 1.3: Distribution of Worldwide Cardiovascular Disease Mortality by Sex and
Etiology.
Figure 1.4: Projected Direct and Indirect Costs of Cardiovascular Diseases, 2010 to
2013.
Figure 1.5: Atherosclerosis from Healthy Vessel to Thrombosis.
Figure 1.6: Pathology of Atherosclerosis Progression from Intimal Thickening to
Advanced Thin Cap Fibroatheroma.
Figure 1.7: Pathophysiology and Molecular Consequences of Intraplaque
Hemorrhage.
Figure 1.8: Pathology of Fibroatheromatous Plaque.
Figure 1.9: Relationships among Cerebral Blood Flow, Cerebral Reactivity, Vessel
Diameter, and Cerebral Perfusion Pressure.
Figure 1.10: Natural History of Atherosclerosis and Positive Remodeling of the Vessel
in Early Stages of Disease.
Figure 1.11: Progression of Atherosclerosis, Stenosis and Vessel Wall Plaque
Components.
Figure 1.12: Carotid Origin and the Aortic Arch.
Figure 1.13: Common Carotid Origin Variants.
Figure 1.14: True Bovine Arch.
Figure 1.15: External Carotid Artery Collateral Arterial Anastomoses.
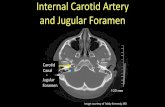
Figure 1.16: Internal Carotid Artery Segments.
Figure 1.17: Classification and Estimates of the Frequency of Stroke Etiology.
Figure 1.18: Sources of Thromboembolism.
Figure 1.19: Measuring Stenosis Using the North American Symptomatic Carotid
Endarterectomy Trial Method.
Figure 1.20: Near Occlusion in Carotid Artery Disease.

xv
Figure 1.21: Internal Carotid Artery Stenosis Diagnosed with Invasive Digital
Subtraction Angiography.
Figure 1.22: Carotid Artery Peak Systolic Velocity on Ultrasound and its
Corresponding Angiographic Stenosis.
Figure 1.23: Computed Tomography Angiography of Carotid Artery Disease
Demonstrating Ulceration and Stenosis.
Figure 1.24: Time-of-flight Angiography Demonstrating Stenosis at the Origin of the
Internal Carotid Artery.
Figure 1.25: Common Carotid Intima-media Thickness as Measured in the Multi-ethnic
Study of Atherosclerosis Trial.
Figure 1.26: Advanced Carotid Plaque Imaging for the Comprehensive Evaluation of
Atherosclerosis.
Figure 1.27: Quantification of Carotid Plaque Morphology and Components.
Figure 1.28: Total Plaque Area Regression using 2-Dimensional Ultrasound.
Figure 1.29: In-Vivo Computed Tomography Angiography Image of the Common
Carotid Artery and Matching Ex-Vivo Microcomputed Tomography and
Histologic Sections.
Figure 1.30: Positive Rim Sign and Carotid Intraplaque Hemorrhage.
Figure 1.31: Simultaneous Presence of Carotid Intraplaque Hemorrhage and Ulcer.
Figure 1.32: High-risk Carotid Plaque Characterized with Positron Emission
Tomography Magnetic Resonance Imaging.
Figure 1.33: Progression of White-matter Disease.
Figure 1.34: Development of Carotid Artery Ulceration.
Figure 1.35: Magnetic Resonance Imaging of Carotid Vessel Wall and Intraplaque
Hemorrhage.
Figure 1.36: Intraplaque Hemorrhage Underlying Patient with New Carotid Ulcer and
White-Matter Lesion.
Figure 1.37: Magnetic Resonance Imaging Surface Coils.
Figure 1.38: Three-Dimensional Carotid Magnetic Resonance Imaging of Intraplaque
Hemorrhage.
Figure 1.39: Thesis Overview.

xvi
Figure 2.1: Magnetic Resonance Imaging Depicted Carotid Intraplaque Hemorrhage
Indicated by Signal Hyperintensity in the Vessel Wall.
Figure 2.2: Axial Images of Low-grade Carotid Stenosis and Intraplaque Hemorrhage.
Figure 2.3: Data Collection Overview.
Figure 2.4: Study Flow Chart of Participants.
Figure 2.5: Age-specific Sex Differences in the Presence of Carotid Intraplaque
Hemorrhage.
Figure 3.1: Embolic stroke of Undetermined Source Patient Study Flow Chart.
Figure 3.2: Magnetic Resonance Imaging Depicted Carotid Intraplaque Hemorrhage
Ipsilateral to Acute Cortical Infarct Indicated by Restricted Diffusion.
Figure 4.1: Multiplanar Images of Carotid Intraplaque Hemorrhage within the Wall of
the Left Carotid Artery.
Figure 4.2: Multiplanar Images Showing Intraplaque Hemorrhage in the Left Carotid
Artery.
Figure 5.1: Summary of Reliability and Agreement of 3-Dimensional Intraplaque
Hemorrhage Imaging Study Participants.
Figure 5.2: 3-Dimensional T1-weighted Gradient Echo Black Blood Imaging Depicts
Intraplaque Hemorrhage.
Figure 5.3: Post-processing of Patients with 3-Dimensional and 2-Dimensional
Imaging.
Figure 5.4: Segmentation of Intraplaque Hemorrhage and the Vessel Wall.
Figure 5.5: Bland and Altman Plots of the Intra-rater and Inter-rater for the
Volumetric Quantification of Vessel Wall and Intraplaque Hemorrhage
with 3-Dimensional Carotid Artery Magnetic Resonance Imaging using a
Combined 3-Dimensional T1-weighted Gradient Echo Black Blood and 3-
Dimensional Time-of-flight Magnetic Resonance Angiography Approach.
Figure 5.6: Bland and Altman Plots of 3-Dimensional and 2-Dimensional Carotid
Artery Magnetic Resonance Imaging Depicting the Agreement for the
Volumetric Quantification of Vessel Wall.

xvii
Abbreviations
2D 2-Dimensional
3D 3-Dimensional
ACAS Asymptomatic Carotid Atherosclerosis Study
ACC American College of Cardiology
ACE Angiotensin Converting Enzyme
ACST Asymptomatic Carotid Surgery Trial
AHA American Heart Association
ARB Angiotensin Receptor Blocker
ARIC The Atherosclerosis Risk in Communities
ASCOD Atherosclerosis, Small-vessel Disease, Cardiac Pathology, Other Causes,
Dissection
B-A Bland-and-Altman
BB Black-blood
CAD Coronary Artery Disease
CAIN Canadian Atherosclerosis Imaging Network
CCA Common Carotid Artery
CD163 Cluster of Differentiation 163
CD68+ Cluster of Differentiation 68
CE Contrast Enhanced
CEA Carotid Endarterectomy
CI Confidence Interval
cIMT Carotid Intima-media Thickness
CRP C-reactive Protein
CT Computed Tomography
CTA Computed Tomography Angiography
CV Cardiovascular
DSA Digital Subtraction Angiography
ECA External Carotid Artery
ECG Electrocardiogram

xviii
ECST European Carotid Surgery Trial
EMBRACE Event Monitor Belt for Recording Atrial Fibrillation after a Cerebral
Ischemic Event
ESUS Embolic Stroke of Undetermined Source
FLAIR Fluid-attenuated Inversion Recovery
FOV Field of View
GRE Gradient Echo
HIF-1 Hypoxic Inducible Factor 1
HIPPA Health Insurance Portability and Accountability Act of 1996
HRCP High-risk Carotid Plaque
HU Hounsfield Unit
ICA Internal Carotid Artery
ICC Intra-class Correlation Coefficient
IMT Intima-media Thickness
IPH Intraplaque Hemorrhage
LR/NC Lipid Rich-necrotic Core
MACE Major Adverse Cardiovascular Events
MDCT Multidetector Computed Tomography
MDCTA Multidetector Computed Tomography Angiography
MESA Multi-Ethnic Study of Atherosclerosis
MI Myocardial Infarction
MIP Maximum Intensity Projection
MMP Matrix Metalloproteinase
MPR Multiplanar Reformats
MPRAGE Magnetization Prepared Rapid Acquisition with Gradient-Echo
MRA Magnetic Resonance Angiography
MRI Magnetic Resonance Imaging
MR-IPH Magnetic Resonance Depicted Intraplaque Hemorrhage
MSDE Motion Sensitized Driven Equilibrium
NASCET North American Symptomatic Carotid Endarterectomy Trial

xix
NAVIGATE New Approach riVaroxoban Inhibition of Factor Xa in a Global Trial
versus Aspirin to Prevent Embolism
OR Odds Ratio
OW Outer Wall
PD Proton Density
PET Positron Emission Tomography
PVD Peripheral Vascular Disease
RBC Red Blood Cell
RCT Randomized Controlled Trial
RESPECT Randomized Evaluation of Recurrent Stroke Comparing Patent Foramen
Ovale Closure to Established Current Standard of Care Treatment
ROI Region of Interest
SD Standard Deviation
SE Standard Error
SNR Signal-to-noise Ratio
SPIR Spectral Pre-saturation with Inversion Recovery
SVD Small Vessel Disease
T1w T1-weighted
TCD Transcranial Doppler
TEE Trans-esophageal Echocardiography
TIA Transient Ischemic Attack
TIMP Tissue Inhibitors of Metalloproteinases
TLR-4 Toll-like Receptor 4
TOAST Trial of ORG 10172 in Acute Stroke Treatment
TOF Time-of-flight
TPA Total Plaque Area
TPV Total Plaque Volume
TTE Transthoracic Echocardiography
VACAS Veterans Affairs Cooperative Atherosclerosis Study
VEGF Vascular Endothelial Growth Factor
VW Vessel Wall

xx
VWD Vessel Wall Disease
WMD White Matter Disease
WMHI White Matter Hyperintensity

xxi
Peer-Reviewed Publications
1. Singh N, Moody AR, Panzov V, Gladstone DJ. Carotid Intraplaque Hemorrhage in
Patients with Embolic Stroke of Undetermined Source. J Stroke Cerebrovasc Dis. 2018
Jul; 27(7): 1956-1959.
2. Singh N, Moody AR, Zhang B, Kaminski I, Kapur K, Chiu SE, Tyrrell PN. Age-Specific
Sex Differences in MRI Depicted Carotid Intraplaque Hemorrhage. Stroke. 2017; 48(8):
2129-2135.
3. Singh N, Moody AR, Roifman I, Bluemke D, Zavodni AE. Advanced MRI for Carotid
Plaque Imaging. Int J Cardiovasc Imaging. 2016 Jan; 32(1): 83-9.
4. Singh N, Moody AR, Rochon-Terry, Kiss A, Zavodni AE. Identifying Individuals with a
High-Risk Cardiovascular Phenotype Using MR Detected-Intraplaque Hemorrhage in
Patients Evaluated for Neurovascular Disease. Int J Cardiovasc Imaging. 2013; 29: 1477-
1483.
5. Singh N, Moody AR, Zavodni AE. Carotid Atherosclerosis and Risk of Stroke. Current
Cardiovascular Imaging Reports. 2013; 6(1): 25-33.
6. Moody AR, Singh N. Incorporating Carotid Plaque Imaging into Routine Clinical Carotid
MRA. Neuroimaging Clin N Am. 2016 Feb; 26(1): 29-44.
7. Fox AJ, Singh N. Clinical Trials for Carotid Stenosis Revascularization and Relation to
Methods of Stenosis Quantification. Neurovascular Imaging. 2015 Oct 21; (1): 1-7.
8. Ramirez J, Singh N, Adamo S, Goubran M, Thayalasuthan V, Zhang B, Tardif JC, Black
SE, Moody AR. Carotid Atherosclerosis and Cerebral Small Vessel Disease: Preliminary
Results from the Canadian Atherosclerosis Imaging Network Project 1. Atherosclerosis
Supplements. 2018; (32): 156.

xxii
International Meetings 9. Singh N, Moody AR, Zhang B, Koh L. The Effect of Sex and Age on Intraplaque
Hemorrhage Prevalence in Low-grade Carotid Stenosis. American Society of
Neuroradiology, Chicago, IL, USA. 2015. O-451.
10. Singh N, Moody AR, Maraj T, Marvasti TB, Afshin M. Quantification of Carotid
Intraplaque Hemorrhage and Vessel Wall by 3T Carotid 3D MRI. American Society of
Neuroradiology, Chicago, IL, USA. 2015. O-453.
11. Singh N, Moody AR, Rochon-Terry, Kiss A, Zavodni AE. Identifying Individuals with a
High-risk Cardiovascular Phenotype Using MR Detected-intraplaque Hemorrhage in
Patients Evaluated for Neurovascular Disease. North American Society of Cardiovascular
Imaging, San Diego, CA, USA. 2012.

1
Chapter 1—Carotid Atherosclerosis Imaging from Lumen to
the Vessel Wall
This chapter includes sections or content that were either adapted or reproduced with
permission from the following peer-reviewed literature.
• Singh N, Moody AR, Roifman I, Bluemke D, Zavodni AE. Advanced MRI for
Carotid Plaque Imaging. Int J Cardiovasc Imaging. 2016 Jan; 32(1): 83-9.
• Singh N, Moody AR, Zavodni AE. Carotid Atherosclerosis and Risk of Stroke.
Current Cardiovascular Imaging Reports. 2013; 6(1): 25-33.
• Moody AR, Singh N. Incorporating Carotid Plaque Imaging into Routine Clinical
Carotid MRA. Neuroimaging Clin N Am. 2016 Feb; 26(1):29-44.
• Fox AJ, Singh N. Clinical Trials for Carotid Stenosis Revascularization and Relation
to Methods of Stenosis Quantification. Neurovascular Imaging. 2015 Oct (1): 1-7.

2
1.1 Overview
Intraplaque hemorrhage (see Figure 1.1) is an independent marker of cardiovascular outcomes
including stroke and myocardial infarction. Magnetic resonance imaging allows for the direct
visualization of intraplaque hemorrhage in the vessel wall of the carotid arteries. This thesis
reports data from an institutional magnetic resonance depicted intraplaque hemorrhage
experience and a clinical trial. The work herein addresses areas particularly sparse regarding the
relationship of intraplaque hemorrhage with cardiovascular risk factors and its potential role in
stroke, specifically reporting on i) age-specific sex differences in low-grade stenosis, ii) the role
in ipsilateral embolic stroke of undetermined source, and iii) the relationship with a high-risk
cardiovascular phenotype. This section reviews the literature on the burden, pathophysiology,
and imaging of carotid atherosclerosis and culminates in the specific aims and projects presented
in the remainder of the thesis.

3
Figure 1.1: Schematic of Carotid Intraplaque Hemorrhage. The carotid arteries
serve as a conduit from the heart to the brain. The presence of a carotid
intraplaque hemorrhage is depicted here at the origin of the internal carotid
artery. The biomarker provides an opportunity to identify patients who are
vulnerable to major adverse cardiovascular events, including stroke and
myocardial infarction. Risk factors and consequences of carotid intraplaque
hemorrhage are investigated in this body of work using a ten-year institutional
experience of intraplaque hemorrhage magnetic resonance imaging. © Navneet
Singh, 2016. All rights reserved.

4
1.2 Cardiovascular Disease Burden
1.2.1 Worldwide
Cardiovascular diseases are a leading cause of mortality and morbidity worldwide (WHO, 2011).
Of 57 million total deaths worldwide per annum, 36 million are due to noncommunicable
diseases. Of these noncommunicable disease deaths, 17.3 million occur as a result of
cardiovascular disease. The distribution of noncommunicable disease mortality worldwide
reveals that death from cardiovascular disease exceeds mortality from respiratory illness, cancer,
and other noncommunicable diseases (see Figure 1.2). Cardiovascular diseases are the most
frequent cause of death worldwide, except in Africa. Noncommunicable diseases may also be
outnumbered by communicable diseases in the future.
Figure 1.2: Distribution of Noncommunicable Disease Mortality Worldwide.
Cardiovascular disease mortality includes myocardial infarction and stroke.
Figure reproduced from the 2011 Global Atlas on Cardiovascular Disease
Prevention and Control. The World Health Organization permits reproduction for
academic theses.
A closer look at the etiology of worldwide cardiovascular disease mortality reveals that
13.5 of the 17.3 million deaths, or 80%, are directly attributable to atherosclerosis.
Atherosclerosis-related myocardial infarction and stroke account for 7.3 and 6.2 million deaths,
respectively. The remaining 20% of cardiovascular disease mortality results from congenital

5
heart disease, rheumatic heart disease, cardiomyopathies, and cardiac arrhythmias. Both sexes
are significantly impacted by atherosclerosis-related cerebrovascular disease and ischemic heart
disease (see Figure 1.3).
Figure 1.3: Distribution of Worldwide Cardiovascular Disease Mortality by Sex
and Etiology. Figure reproduced from the 2011 Global Atlas on Cardiovascular
Disease Prevention and Control. The World Health Organization permits
reproduction for academic theses.
Compared with males, females have a marginally higher mortality from cerebrovascular
disease (37 vs. 34%) and a lower mortality from ischemic heart disease (38 vs. 46%) worldwide.
The precise reasons for the differences in sex-related mortality from cerebrovascular and
ischemic heart disease are topics of ongoing study.
1.2.2 North America
Estimates of mortality due to cardiovascular disease burden in North America from the
American Heart Association echo the worldwide burden of stroke and myocardial infarction.
Mortality estimates suggest that one death from cardiovascular disease occurs every 38.9
seconds in North America. In 2009, the annual age-standardized death rate attributable to all
cardiovascular diseases in the United States was 237.1 per 100,000 (Go et al., 2013). Given the
United States' population of 307 million in 2009, this rate would translate into 727,913 deaths
annually, or nearly 1,994 deaths daily as a result of cardiovascular disease (Bureau, 2009).

6
Extrapolation of this mortality rate to Canada’s population of 35.7 million in 2015 indicates that
84,762 deaths occur per annum, or 232 Canadians die each day as a consequence of
cardiovascular disease (Statistics-Canada, 2015).
Atherosclerosis-related myocardial infarction accounts for 20.3% of all deaths in the
United States (Marczak, O’Rourke, Shepard, for the Institute for Health, & Evaluation, 2016)
and is the leading cause of death in both men and women. Myocardial infarction, stroke, and
other cardiovascular causes of mortality are estimated to be 116.1, 38.9, and 81.0 per 100,000
persons in the United States per annum, respectively (Go et al., 2013). Although myocardial
infarction is responsible for more mortality than stroke, the American Heart Association
estimates that 7,000,000 Americans over the age of 20 have had a stroke (Roger et al., 2012).
Annually, 795,000 Americans experience a new or recurrent stroke (Roger et al., 2012).
Improvements in mortality from stroke over the past few decades are attributed, in part, to the
presence of regional stroke centers (Barnett & Buchan, 2000). Further improvements are likely
to evolve given that recent trials have demonstrated the benefit of intra-arterial therapy
(Berkhemer et al., 2015) for acute stroke. Currently, however, stroke is responsible for
approximately 1 out of every 18 deaths in the United States (Roger et al., 2012).
Stroke accounts for 1.7% of all health expenditures in the United States and is expected
to increase by 129% to nearly 240 billion by 2030 compared with 2010 (Ovbiagele et al., 2013).
By 2030, the total direct costs are estimated to increase to $184.13 billion from $71.55 billion.
Indirect costs such as loss of productivity are expected to rise to $56.54 billion, representing an
increase of nearly $23 billion.
Cardiovascular disease accounts for 17% of all health care expenditures in the United
States and is expected to increase by 61% to $1.094 trillion dollars by 2030 compared with 2010
(P. A. Heidenreich et al., 2011). By 2030, the total direct costs are estimated to increase to $818
billion from $273 billion (see Figure 1.4). Indirect costs such as loss of productivity are expected
to rise to $276 billion, representing an increase of nearly $100 billion (see Figure 1.4).

7
Figure 1.4: Projected Direct and Indirect Costs of Cardiovascular Diseases, 2010
to 2013. Figure reproduced from (P. A. Heidenreich et al., 2011) with permission
(License 3800421468832).
Forecasts from various organizations on the burden and cost of myocardial infarction and
stroke, including the World Health Organization, the American Heart Association, and the
American Stroke Association, suggest a significant and persistent burden of cardiovascular
disease. Additional cardiovascular disease prevention strategies seem to be needed to address the
burden of atherosclerosis.
1.3 Atherosclerosis
1.3.1 Pathological Stages of the Disease
Atherosclerosis is the underlying pathological state responsible for the majority of the
cardiovascular disease burden worldwide. The Greek origin of the word atherosclerosis
describes the pathological changes of a diseased vessel wall. The words athero and sclerosis
transliterate to gruel and hardening, respectively. Gruel, or various cellular debris, accumulates
in the vessel wall during more complicated stages of the disease associated with artery hardening
or stiffening compared with a healthy artery (Selwaness, van den Bouwhuijsen, Mattace-Raso, et
al., 2014).
The healthy vessel contains three layers. The first layer abutting the lumen is the tunica
intima and is comprised of a monolayer of endothelial cells that contact the blood. The intimal

8
layer contains smooth muscle cells in humans and is lined by a basement membrane. Second, the
medial layer is comprised of an extracellular matrix containing smooth muscle cells. Layers of
elastin separate the smooth muscle cells to ensure the elastic potential of the arteries required for
vasoactivity. Finally, the adventitial layer is comprised of mast cells, nerve endings, and
microvessels.
Figure 1.5 summarizes the stages of atherosclerosis from a healthy vessel to (a) intimal
thickening with macrophage accumulation, (b) attempted reparative stabilization with smooth
muscle cells and neovascularization, (c) and the ultimate consequences of atherosclerosis,
including luminal narrowing, plaque fibrous cap rupture, and/or intraluminal thrombosis (d).
Figure 1.5: Atherosclerosis from Healthy Vessel to Thrombosis. Healthy vessel
(a), intimal thickening with macrophage accumulation (b), attempted reparative
stabilization with smooth muscle cells and neovascularization (c), luminal
narrowing, plaque fibrous cap rupture and/or intraluminal thrombosis (d) ©
Navneet Singh, 2016. All rights reserved.

9
The formation of atherosclerotic plaque, a local manifestation of the systemic disease in
atherosclerosis (Tomey, Narula, & Kovacic, 2014), is initiated by several factors that disturb
endothelial function. These factors include aging, hyperglycemia, hypercholesterolemia,
hypertension, male gender, and smoking (Michel, Virmani, Arbustini, & Pasterkamp, 2011).
Endothelial dysfunction results in a loss of normal anti-inflammatory, anti-thrombotic, and
vasoactive functions (Cahill & Redmond, 2013). Endothelial dysfunction occurs due to the
inadequate bioavailability of nitrous oxide, a molecule that is important for the local regulation
of vascular tone. Nitric oxide is produced by the enzyme nitric oxide synthase in endothelial
cells. Factors such as female sex may be protective against atherosclerosis due to the ability of
estrogen to upregulate nitric oxide synthase expression and the production of nitric oxide.
Normal cholesterol handling at the interface between the vessel wall and the lumen is disturbed
such that there is a net ingress of cholesterol into the intima and increased cholesterol deposition.
Over time, the cholesterol coalesces into lipid pools. This intraplaque environment results in
lipid oxidation and the production of oxygen free radicals.
In response to early atherosclerotic changes in the vessel wall, circulating monocytes are
attracted within the plaque through endothelial activation and the expression of surface receptors.
Factors including dyslipidemia and hypertension may increase monocyte adhesion to the
endothelium. Figure 1.6 depicts, along with corresponding changes in macrophages, the
evolution of atherosclerosis from pathological intimal thickening to the development of a thin
cap fibroatheroma. Cluster of Differentiation 68 (CD68+), a glycoprotein that binds to low-
density lipoprotein, is expressed on the surface of monocytes and macrophages. The expression
of CD68+ appears dark brown after immunohistochemical processing. During pathologic intimal
thickening (see Figure 1.6a, panel 1), lipid pools may accumulate in the deeper part of the intima
(see Figure 1.6a, panel 2). Macrophages are present near the surface of the intima. As the lipid
pool increases in size into an early-stage necrotic core (see Figure 1.6b, panel 2), macrophages
infiltrate the core in an attempt to clear it. Macrophages are shown infiltrating the early necrotic
core (see Figure 1.6b, panel 2).
Phagocytosis of plaque lipids by macrophages results in foam cell formation commonly
leading to macrophage apoptosis rather than the removal lipids from the vessel wall. Thus, the

10
fibroatheroma with a late necrotic core has a lytic appearance and a larger size (see Figure 1.6c,
panel 1). A reparative response to disease within the plaque results in stimulation of smooth
muscle cell proliferation and development of intima-medial thickening in an attempt to stabilize
the inflammatory process. A thin fibrous cap characterizes the progression of the disease to the
more advanced fibroatheroma (see Figure 1.6d). The thin fibrous cap is prone to rupture and
results in intraluminal thrombosis.
Figure 1.6: Pathology of Atherosclerosis Progression from Intimal Thickening
to Advanced Thin Cap Fibroatheroma. (A) Pathologic intimal thickening, (B)
fibroatheroma with an early necrotic core, (C) fibroatheroma with a late necrotic
core, and (D) Thin-cap fibroatheroma. The coronary pathology is shown.
Reproduced with permission from (Fleg et al., 2012) (License 3800431075269).
1.3.2 Classification
Atherosclerotic lesions are commonly classified using definitions based on histology from Stary
et al. (see Table 1.1) (Stary et al., 1995). Observations of pathology in the coronary arteries
inform the classification system. In particular, Type VI plaques are considered complicated
plaques that are vulnerable to rupture and/or thromboembolism. Hemorrhage in the vessel wall

11
plaque resulting from leaky neoadventitia originating in the vasa vasorum is another feature of a
Type VI plaque. Several studies use this classification system to describe advanced stages of
atherosclerosis in the carotid arteries.

12
Table 1.1: Lesion Nomenclature and Histological Features along with a Cross-sectional Sketch of the
Stary Classification of Atherosclerosis. Adapted from (Stary et al., 1995) with permission from Wolters
Kluwer Health, Inc. (License 3793710463590).
Lesion Nomenclature Histological Features Cross-sectional Appearance Type I –Initial Isolated macrophage foam
cells
--
Type II—Fatty Streak Intracellular lipid accumulation
Type III—Intermediate Intracellular and
extracellular lipid pools
Type IV—Atheroma Extracellular lipid core
Type V—Fibroatheroma Lipid core(s) and fibrotic
layer(s), or mainly calcific, or primarily fibrotic
Type VI—Complicated Surface defect,
hematoma-hemorrhage, thrombus

13
1.3.3 Progression
The progression of disease may be accelerated as a result of a hypoxic intraplaque environment
leading to the development of leaky young vasa vasorum, which enhances the development of
the necrotic core. Specifically, an indirect effect of plaque surface thickening is the loss of the
usual oxygen diffusion from the lumen into the vessel wall once the thickening exceeds 200
microns. In response to this phenomenon and secondary to the release of factors such as HIF-1
(hypoxic inducible factor-1) and the presence of intraplaque macrophages, VEGF (vascular
endothelial growth factor) is released. These processes stimulate new vessel growth within the
plaque, predominantly originating from the vasa vasorum within the adventitia. The new vessel
growth, however, results in leaky, friable vessels that are vulnerable to red cell deposition and
frank hemorrhage within the vessel wall (Virmani, Kolodgie, Burke, et al., 2005). The trigger for
plaque hemorrhage is not clearly understood, but plaque morphology, hemodynamics, or changes
in systemic blood pressure, particularly changes in pulse pressure (Selwaness et al., 2013), may
result in repeated microhemorrhages within the plaque. Low diastolic pressure has also been
hypothesized in exploratory work to be associated with the presence of intraplaque hemorrhage
(Sun et al., 2016). Low diastolic pressure may reflect an acute change in hydrostatic pressure
resulting in a pressure gradient from the high-pressure vasa vasorum environment to the low-
pressure intraplaque environment.
The influx of red blood cells within the plaque leads to some deleterious effects. First, if
the volume of blood deposited in the atherosclerotic plaque is large, it can result in a significant
change in the vessel wall volume and potentially encroach on the lumen. The deposition of red
blood cells is considered one of the causes of rapid changes in stenosis; a rapid reduction can
also occur with blood resorption. More common are repeated small hemorrhages that do not
cause a significant change in plaque volume. These hemorrhages result in the repeated delivery
of red cells deep within the vessel wall lesion. There are two significant and related effects of
repeated red blood cell delivery. Red blood cell membranes have one of the highest cholesterol
contents of any cell in the human body, which is further increased during states of
hypercholesterolemia. Consequently, each red blood cell delivered into the plaque adds to the

14
lipid core. Following red blood cell lysis, the other major component that is directly introduced
into the plaque is hemoglobin.
Hemoglobin is bound to haptoglobin so that it may be taken up by macrophages via the
Cluster of Differentiation 163 (CD 163) receptor (see Figure 1.7). Hemoglobin is broken down
into heme and globin. Globin is further broken down into amino acids that are repurposed. Heme
is highly inflammatory, and through the Fenton reaction, drives the repetitive production of
oxygen free radicals, which contribute to the hostile plaque environment. Heme itself is broken
down by heme-oxygenase, resulting in iron and biliverdin. Biliverdin is converted into bilirubin
and transported by albumin to the liver, where it is conjugated and excreted into the intestines as
bile. Some of the bilirubin derivatives are absorbed into the blood from the intestines and are
excreted in the urine. Free iron in macrophages is bound to the protein ferritin and transported
via transferrin to the liver or the spleen for storage or to the bone marrow for the generation of
new red blood cells. Excess iron in macrophages is problematic for several reasons. First, it may
result in increased reactive oxygen species generation through the Fenton reaction. Second, the
inability to remove free iron may be associated with the failure to efflux cholesterol from
macrophages via ABCA1 (ATP-binding cassette transporter-1). Third, the inability to excrete
iron may activate the TLR-4 (Toll-like Receptor 4) signaling pathway. The processes involved in
lowering intracellular iron are also associated with increased expression of HIF-1 and VEGF,
which may contribute to angiogenesis.

15
Figure 1.7: Pathophysiology and Molecular Consequences of Intraplaque
Hemorrhage. Figure reproduced with permission from (Finn & Narula, 2012)
(License 3831440086383).
One of the key studies describing the contribution of red blood cells to the atherogenic
stimulus was reported in 2003. Kolodgie et al. suggested that erythrocyte membranes are a potent
and specific atherogenic stimulus. Glycophorin A is a glycoprotein located on the red blood cell
(RBC) membrane that is rich in sialic acid, allowing RBCs hydrophilicity and circulation without
adhering to the vessel wall. A small amount of glycophorin A and iron has been detected in
earlier stages of atherosclerosis. In contrast, large amounts of glycophorin A and iron were found
in later stages of atherosclerosis. Figure 1.8 demonstrates some of the findings associated with
fibroatheroma with late stage necrosis (see Figure 1.8, a-e) and a thin fibrous cap (see Figure 1.8,
f-j). The fibroatheroma with late stage necrosis is stained darkly for macrophages (see Figure
1.8b), glycophorin A (see Figure 1.8c), iron (see Figure 1.8d), and new vessels with perivascular
von Willebrand factor (vWF), indicating the presence of leaky vessels (see Figure 1.8e). The
presumably later stage fibrous cap atheroma has a thinner fibrous cap (see Figure 1.8f), positive
staining for macrophages (see Figure 1.8g), glycophorin (see Figure 1.8h), and iron (see Figure

16
1.8i), and darker staining associated with new vessels that are positive for vWF expression,
indicating the presence of leaky vessels.
Figure 1.8: Pathology of Fibroatheromatous Plaque. Intraplaque Hemorrhage in
Fibroatheroma with a Core in the Late Stage of Necrosis (panels a-e) and Thin-
Cap Fibroatheroma (panels f-j). Low power views of the necrotic core used
Movat’s Pentachrome at x20 magnification (panels a and f), macrophage
immunostaining for CD68+ with x200 magnification (panels b and g),
glycophorin A staining at x200 magnification (panels c and h), iron deposits
shown in blue stained with Mallory’s at x200 magnification (panels d and i), and
vasa vasorum and von Willebrand factor staining at x500 magnification (panels e
and j). Reproduced with permission from (Kolodgie et al., 2003), ©
Massachusetts Medical Society.
The combination of cholesterol and heme delivered with every red cell therefore provides
an inflammatory combination that drives the atherosclerotic process. Perpetual
monocyte/macrophage migration into the plaque results in increased expression of inflammatory
cytokines, enhanced angiogenesis, lipid oxidation, and cell death, resulting in enlargement of the
necrotic core of the plaque, neovascularization, and subsequent hemorrhage. This vicious cycle
likely accounts for the acceleration in atherosclerotic disease from a slow, predictable
progression to more rapid, unpredictable plaque progression and disruption. The presence of
plaque hemorrhage therefore denotes a more advanced atherosclerotic state consistent with the
increased plaque vulnerability and plaque progression. The role of intraplaque hemorrhage (IPH)

17
in clinically relevant carotid artery disease progression is one feature of atherosclerosis that is
addressed in this thesis.
1.3.4 End-Organ Outcomes
The progression of atherosclerosis into a later disease state may result in luminal narrowing or
plaque rupture. The carotid artery is used to highlight the principles of end-organ outcomes
related to atherosclerosis in this section. Brott et al. summarize at least five mechanisms that are
thought to be implicated in end-organ outcomes (Brott et al., 2011). First, artery-to-artery
embolism may occur as a result of the formation of a thrombus on the luminal surface of the
atherosclerotic plaque in the carotid artery. Subsequent downstream occlusion of a smaller artery
due to this thrombus may occur. Second, thromboembolism of cholesterol crystals or other
debris may occur. Third, plaque rupture may result in an acute thrombus, causing local
occlusion. Fourth, the presence of carotid atherosclerosis may lead to arterial wall ulceration at
the luminal surface of a plaque, resulting in dissection or sub-intimal hematoma. Finally, reduced
perfusion may occur due to higher grades of stenosis resulting from progressive plaque growth.
Typically, this mechanism requires compromised intracranial collateral circulation.
Regardless of the exact underlying mechanism, both luminal narrowing and plaque
rupture with subsequent thromboembolism are implicated in end-organ outcomes of
atherosclerosis such as infarction. The latter mechanism is more likely to be involved in end-
organ outcomes because high degrees of carotid stenosis, on the order of 60% to 75%, are
required to result in significant decreases in cerebral blood flow in-vivo. At first glance, this may
appear counterintuitive; considering the carotid artery in isolation in an ideal setting, it would
appear that luminal narrowing has the most profound effect on blood flow. The effect of luminal
narrowing on blood flow in an artery is dependent on the resistance (R) of liquid in a tube
(Klabunde, 2012). Resistance is affected by the tube length (L), viscosity (n), and tube radius (r),
among which the radius appears to exert the greatest impact:
𝑅𝑅 ∝𝑛𝑛 ∙ 𝐿𝐿𝑟𝑟4
Flow (Q) is affected by perfusion pressure (∆𝑃𝑃) and resistance (R):

18
𝑄𝑄 ∝∆𝑃𝑃𝑅𝑅
A combination of these equations for flow and resistance provides Poiseuille's equation,
which summarizes the relationship of flow with perfusion pressure, radius, length, and viscosity:
𝑄𝑄 = 𝜋𝜋∆𝑃𝑃 ∙ 𝑟𝑟4
8𝑛𝑛 ∙ 𝐿𝐿
As observed for resistance, the effect of radius on flow is exponential. The reduction in
the radius of an artery or arterial stenosis should have the largest quantitative impact on flow
among factors such as tube length, blood viscosity, and perfusion pressure.
However, several other factors must be considered in-vivo because the vessels are not
straight, blood is not a Newtonian fluid, blood may not flow in a laminar fashion, and most
importantly, the large carotid artery only accounts for a small portion of the resistance in the
neurovascular system. Carotid stenosis is much less likely to affect flow until approximately
60% to 75% stenosis is reached because of the aforementioned features and because the large
carotid artery accounts for a small part of the overall resistance in the neurovascular system.
To better understand the impact of the carotid artery as one factor that contributes to
neurovascular resistance, consider the following example. Given that the mean carotid artery
radius is in the range of 2.5 mm (Krejza et al., 2006), a 50% stenosis of the artery would indicate
a reduction in the radius of approximately 1.25 mm. Assuming that all other variables are kept
constant and assuming a straight tube, applying Poiseuille's equation shows an anticipated flow
rate reduction from 15.3 to .96 (or 16-fold):
𝑄𝑄𝑛𝑛𝑛𝑛 𝑠𝑠𝑠𝑠𝑠𝑠𝑛𝑛𝑛𝑛𝑠𝑠𝑠𝑠𝑠𝑠 = 𝜋𝜋∆𝑃𝑃 ∙ 𝑟𝑟4
8𝑛𝑛 ∙ 𝐿𝐿=
3.14 ∙ 1 ∙ 2.54
8 ∙ 1 ∙ 1= 15.3
𝑄𝑄50% 𝑠𝑠𝑠𝑠𝑠𝑠𝑛𝑛𝑛𝑛𝑠𝑠𝑠𝑠𝑠𝑠 = 𝜋𝜋∆𝑃𝑃 ∙ 𝑟𝑟4
8𝑛𝑛 ∙ 𝐿𝐿=
3.14 ∙ 1 ∙ 1.254
8 ∙ 1 ∙ 1= 0.96
Therefore, assuming a total neurovascular system resistance of 100, a stenosis of 50%
should increase the resistance to 1600. However, to maintain cerebral blood flow, there is a
progressive recruitment of cerebral collaterals as a result of cerebral autoregulation that results in
the dilation of resistance vessels (Fisch & Brown, 2016). The carotid artery resistance only
accounts for 1% of the total resistance of the neurovascular system (Klabunde, 2012), and
therefore only an increase in resistance of 16% occurs. The flow from the carotid accounts for

19
only a small amount of the resistance of the entire neurovascular system. The neurovascular
system is comprised of other vessels, either connected in parallel such as the contralateral carotid
or vertebrobasilar arteries or connected in series such as the smaller arteries and arterioles that
account for much of the resistance. An early report in a series of 17 patients with stenosis
undergoing carotid endarterectomy reported the mean internal carotid flow and regional cerebral
blood flow using a 133 Xenon injection technique (Boysen, Ladegaard-Pedersen, Valentin, &
Engell, 1970). Upon completion of the endarterectomy, the mean flow in the internal carotid
artery increased from 133 to 212 ml/min. However, the cerebral blood flow remained unchanged
from the preoperative values. Thus, even in patients with stenosis requiring endarterectomy,
cerebral autoregulatory mechanisms appear to be able to preserve cerebral blood flow. The
autoregulation curve of Lassen (see Figure 1.9) demonstrates the intrinsic ability of the brain to
maintain a stable blood flow despite fluctuations in perfusion pressure (Budohoski et al., 2013).
Figure 1.9: Relationships among Cerebral Blood Flow, Cerebral Reactivity,
Vessel Diameter, and Cerebral Perfusion Pressure. Autoregulation is essentially
the ability of the vessel to adapt to changes in cerebral perfusion pressure to
maintain blood flow. Reproduced with permission from (Budohoski et al., 2013)
(Nature Publishing Group, License 3800990878837).
This Lassen curve was generated using a thermal diffusion regional cerebral blood flow
monitoring system and demonstrates the relationships among cerebral blood flow, cerebral

20
perfusion pressure, cerebral vessel reactivity, and vessel diameter (Budohoski et al., 2013). In the
normal range of autoregulation, as cerebral perfusion pressure increases, the vascular diameter
decreases and cerebrovascular reactivity increases, allowing for the maintenance of cerebral
blood flow. Outside the normal range, cerebral blood flow is increased when above the upper
limit of normal autoregulation, and is decreased when below the limit of normal autoregulation.
Normal ranges are defined as cerebral perfusion pressure of 62 to 88 mmHg, cerebral blood flow
of approximately 27 ml/min/100 g, and cerebrovascular reactivity of 2 to 3 mmHg/ml/min/100
g).
Cerebral ischemia occurs as a result of a reduction in cerebral blood flow. The cerebral
blood flow continuum encompasses ischemia (<20 ml/100 g/min), oligemia (20 to 40 ml/100
g/min), normal (40 to 60 ml/100 g/min), and hyperperfusion (>60 ml/100 g/min). Within the
ischemic continuum, the infarction threshold is <8 ml/100 g/min. Critical and penumbra
thresholds are 12 and 20 ml/100 g/min, respectively.
Cerebral ischemia resulting from hemodynamic compromise therefore requires a
significant reduction in the carotid artery lumen and impaired autoregulation (Schoof et al.,
2007; White & Markus, 1997) or poor intracerebral vessel collateralization. Another
hemodynamic issue arises as a result of the natural history of carotid atherosclerosis progression
and the positive remodeling that takes place in the early phases of atherosclerosis. The
substantial burden of carotid artery atherosclerosis may exist before any significant reduction in
the lumen. Observations from Glagov, commonly referred to as the Glagov phenomenon,
suggest that stenosis alone does not accurately reflect atherosclerotic burden (S. Glagov et al.,
1987). Morphological changes in atherosclerosis begin with an outward expansion of the vessel.
Glagov demonstrated this in early pathological specimens of the left main coronary arteries (see
Figure 1.10).

21
Figure 1.10: Natural History of Atherosclerosis and Positive Remodeling of the
Vessel in Early Stages of Disease. The lumen initially enlarges up to 40%
stenosis, at which point plaque accumulation occurs at a higher rate, resulting in
luminal narrowing. Reproduced with permission from (Glagov, Weisenberg,
Zarins, Stankunavicius, & Kolettis, 1987), © Massachusetts Medical Society.
More recently, positive remodeling in the carotid arteries was preliminarily reported in
201 individuals with a low-moderate Framingham-risk score using CT angiography (CTA) and
magnetic resonance imaging (MRI). Intra-individual patient correlation between remodeling in
early atherosclerosis was found in left and right carotid arteries. Coronary arteries, however, did
not appear to correlate well with carotid artery remodeling (r=0.20, p<0.0001). These findings
suggest that there are differences in remodeling between the coronaries and the carotids.
However, both undergo similar remodeling in early stages of disease (Selwaness & Bluemke,
2015). The finding that carotid remodeling is not correlated with coronary remodeling also may
explain why carotid stenosis has limited utility for the identification of patients at risk of
ischemic coronary events.
Several issues surround the use of carotid stenosis for the identification of patients at risk
of cerebral ischemia. In patients with impaired cerebrovascular regulation, carotid artery stenosis
may not necessarily result in ischemia until higher grades of stenosis occur, and it may not
represent an atherosclerotic burden in the vessel wall (see Figure 1.11). These issues are among
those hypothesized to explain the reason that the degree of stenosis is unable to accurately
identify individuals at risk of ischemic cerebrovascular events. For example, among symptomatic
patients with severe stenosis, the number needed to treat to prevent one stroke two years after

22
carotid endarterectomy is eight patients (Gorelick, 1999). For symptomatic moderate and low-
grade carotid stenosis, the numbers needed to treat are as high as 20 and 67 patients,
respectively. Asymptomatic patients with greater than 50% to 60% stenosis require as many as
48 to 83 patients to prevent one stroke. Better indicators than luminal stenosis for the
identification of patients at risk of stroke are clearly necessary.
Figure 1.11: Progression of Atherosclerosis, Stenosis, and Vessel Wall Plaque
Components. This figure shows the progression of atherosclerosis and
demonstrates positive remodeling in early stages of atherosclerosis.
Encroachment of the lumen does not occur until later stages of the disease.
Evaluating the lumen may therefore underestimate the amount of true plaque
burden. Plaque components may not be assessed with traditional imaging
methods focusing on the lumen. Evaluation of the vessel wall may provide
improved quantification and characterization of atherosclerosis disease burden.
© Navneet Singh, 2016. All rights reserved.
Given that stenosis may not accurately reflect the underlying atherosclerosis burden and
the corresponding stroke risk, plaque components and vessel wall burden have become targets of
study. Thromboembolism related to advanced or complicated plaque characteristics, such as IPH,
is emerging as a leading mechanism of atherosclerosis related end-organ outcomes. Downstream
blockages from thromboembolism of smaller resistance arteries may impair blood flow and
result in ischemia. While some studies have suggested that plaque components directly affect
flow, it is unclear if plaque components can overcome the cerebrovascular hemodynamic
equilibrium to the point of ischemia. For example, IPH is implicated in the rapid expansion of

23
plaques potentially resulting in critical stenosis (Beach et al., 1993). More recently, the presence
of IPH has been implicated in affecting cerebral blood flow reduction, in addition to and
independent of stenosis (Hashimoto, Hama, Yamane, & Kurisu, 2013). However, based on
opportunities for cerebral collateralization, autoregulation, and the requirement for very high
grades of stenosis to reach a critical point, the instability of plaque components is a leading
reason for end-organ outcomes related to atherosclerotic plaque components.
Plaque components may also play a role in inducing vulnerability and rupture. Rupture of
the fibrous cap or ulceration of the plaque may result in the contact of intravascular blood with a
plaque. Platelets and coagulation proteins in the blood contacting various components of the
plaque, including tissue factors and collagen, can promote thrombosis (Brott et al., 2011).
Several morphological characteristics, such as the presence of IPH, a thin fibrous cap, and
ulceration, are also associated with plaque rupture (Hermus, Lefrandt, Tio, Breek, & Zeebregts,
2010) (see Table 1.2). These plaque components may also be associated with processes that
contribute to vulnerability, including inflammation, lipid accumulation, apoptosis, proteolysis,
thrombosis, and angiogenesis (Hermus et al., 2010). Plaque components themselves are not
necessarily indicated in expansive remodeling, and therefore, strategies for the direct
visualization of these components may be useful (Saam et al., 2016).
Table 1.2: Morphological Features Related to Plaque Instability. Reproduced from (Hermus et al.,
2010) with permission from Elsevier (License 3801400842160).
Unstable plaques Stable plaques
Atheromatous Fibrous
Thin fibrous cap Thick fibrous cap
Large lipid core Small lipid core
Less collagen Collagen-rich
Noncalcified Calcified
Ulceration No ulceration
Intraplaque hemorrhage No intraplaque hemorrhage
Infiltration of inflammatory cells (macrophages) No infiltration of inflammatory cells
Proteolysis and remodeling No remodeling

24
Vulnerable plaques may be transient, and the identification of patients who are unable to
undergo repair of higher-risk plaques—that is, high-risk patients, may be more important.
Managing patients at risk of cardiovascular outcomes is a greater priority than managing
individual plaques (Libby & Pasterkamp, 2015). The identification of a vulnerable plaque,
however, may prompt a search for the presence of a systemic disease or a high-risk
cardiovascular phenotype and allow for identification of patients at risk of cardiovascular events.
The characterization of plaque components may permit the identification of a cardiovascular
phenotype. Characterization may also provide greater insights into patients who are prone to
systemic atherosclerosis and associated complications.
1.4 Carotid Artery Atherosclerosis
Evaluation of the carotid arteries, the conduits between the heart and brain, provides an
opportunity to identify “vulnerable plaques” that are at risk of rupture and progression and
"vulnerable patients" who are at risk of stroke and myocardial infarction. This section reviews
the anatomy of the carotid artery and discusses anatomical site predilection to atherosclerosis.
The role of carotid atherosclerosis in ischemic stroke and the relationship of atherosclerosis with
systemic or polyvascular disease such as ischemic heart disease are discussed. The functions of
both contemporary and advanced carotid artery imaging in cardiovascular disease prevention are
emphasized in subsequent sections.
1.4.1 Anatomy
Carotid arteries at the aortic arch are subject to considerable variation. In 70% of cases, the right
and left carotid artery originate from the brachiocephalic (innominate) artery and aortic arch,
respectively (Layton, Kallmes, Cloft, Lindell, & Cox, 2006) (see Figure 1.12).

25
Figure 1.12: Carotid Origin and the Aortic Arch. The most common aortic arch
branching pattern in humans has separate origins for the innominate, left
common carotid, and left subclavian arteries. Reproduced with permission from
(Layton et al., 2006) (License: 3850340297028).
Other common variants of the arch exist, including arch origination of i) the left common
carotid artery from the innominate artery found in 13% of patients (see Figure 1.13), and ii) the
left common carotid artery from an innominate artery found in 9% of patients (see Figure 1.13).
These two variations are two to three times more likely to be found in African Americans than in
Caucasian individuals.
Figure 1.13: Common Carotid Origin Variants. Common Origin of the
Innominate Artery and Left Common Carotid Artery. Origin of the Left
Common Carotid Artery from the Innominate Artery. Reproduced with
permission from (Layton et al., 2006) (License: 3850340297028).

26
These common variants are sometimes erroneously referred to as bovine arches. A true
bovine arch, however, is characterized by a single brachiocephalic trunk from the aortic arch that
splits into bicarotid and bisubclavian arteries and is not common (see Figure 1.14). The bovine
arch is one of more than 20 arch variants.
Figure 1.14: True Bovine Arch. Reproduced with permission from (Layton et
al., 2006) (License: 3850340297028).
As the carotid arteries course through the neck, they bifurcate into the internal and
external branches at the thyroid cartilage. The right and left carotid bifurcations are usually
within 5 cm of each other (Brott et al., 2011). The internal carotid is dilated at the origin, and
beyond this bulb, the internal carotid artery walls become parallel. The internal carotid artery
does not have any extracranial branch vessels, unlike the external carotid artery. The external
carotid artery branches to supply the face. The extracranial external carotid artery also provides
collateral flow to the internal carotid artery via several pathways (Liebeskind, 2003; Shuaib,
Butcher, Mohammad, Saqqur, & Liebeskind) (see Figure 1.15).

27
Figure 1.15: External Carotid Artery Collateral Arterial Anastomoses. From the
facial (a), maxillary (b), and middle meningeal (c) arteries to the ophthalmic
artery and dural arteriolar anastomoses from the middle meningeal artery (d) and
occipital artery through the mastoid foramen (e) and parietal foramen (f). From
(Liebeskind, 2003) (License 3802050711023).
The internal carotid artery is comprised of seven segments, C1 to C7, per traditional
nomenclature (see Figure 1.16). The cervical segment (C1) courses through the neck from the
carotid bifurcation and does not contain any branches. The petrous segment (C2) is fixed to the
bone as it enters the skull base and is commonly cited as the reason that dissections do not extend
intracranially. The lacerum (C3) is the segment traversing the skull base foramen lacerum. The
cavernous (C4) segment is the portion of the carotid that courses through the cavernous sinus.
The C4 segment gives rise to the meningohypophyseal trunk, which supplies the pituitary,
tentorium, and dura of the clivus. The C4 segment also gives rise to the inferolateral trunk to
supply the third, fourth, and sixth nerve as well as the trigeminal ganglion. The C5, or clinoid
segment, is delineated by two rings that mark the proximal and distal portions of the clinoid
segment. The distal ring may prevent intracranial subarachnoid hemorrhage with rupture of a
clinoid segment aneurysm. The supraclinoid region (proximal C6, referred to as ophthalmic, and
distal C7, referred to as communicating) gives rise to several important branches. These branches
include the ophthalmic artery, which supplies the optic nerve, the posterior communicating artery

28
that anastomoses with the posterior circulation (if it supplies the entire posterior circulation via
an enlarged posterior communicating artery, it is referred to as a fetal posterior cerebral artery),
and the anterior choroidal artery that supplies the optic chiasm, hippocampus, and posterior limb
of the internal capsule.
Figure 1.16: Internal Carotid Artery Segments. Key landmarks defining each of
the segments from C1 through C7 are shown. C1 = Cervical segment, C2 =
Petrous segment, C3 = Lacerum segment, C4 = Cavernous segment, C5 =
Clinoid segment, C6 = Ophthalmic segment, C7 = Communicating segment. ©
Navneet Singh, 2016. All rights reserved.
1.4.2 Anatomical Site Predilection
Atherosclerosis has a predilection for the extracranial carotid bifurcation and other branch points
despite the exposure of the entire arterial tree to cardiovascular risk factors (Morbiducci et al.,
2016). Atherosclerosis progresses at higher rates in the internal carotid artery than the common
carotid artery, and disease in the internal carotid artery appears to more accurately correlate with

29
a patient’s clinical vascular risk factors (Mackinnon et al., 2004). The internal carotid artery is
located at a junction point, supplying the low-pressure cerebral circulation; the external carotid
branch provides blood to the high-resistance facial muscles. Hemodynamic disturbances, such as
low shear stress and a high oscillatory shear index, localized to these branch points and, in
particular, the bulb region of the internal carotid and common carotid regions (Markl et al.,
2010), are thought to be associated with atherosclerotic plaque progression and composition.
These particular regions have a predilection for atherosclerosis because they are subject to low or
oscillatory endothelial shear stress or are located near branch points (Bentzon, Otsuka, Virmani,
& Falk, 2014). Low shear stress is associated with disturbed flow, whereas high shear stress is
associated with normal laminar flow (Morbiducci et al., 2016). Reports have suggested that low
shear stress is involved in intimal thickening in hypertensive patients (Jiang, Kohara, & Hiwada,
1999). The role of shear stress in the pathogenesis of atherosclerosis may be related to
endothelial dysfunction due to decreased nitrous oxide production from endothelial nitrous oxide
synthase (Cahill & Redmond, 2013), which is discussed further here (Cunningham & Gotlieb,
2004; Morbiducci et al., 2016). Low shear stress surrogates, such as geometry (Morbiducci et al.,
2016), have also been implicated in the development of atherosclerosis (Phan et al., 2012). The
internal carotid artery angle of origin has been shown to be associated with atherosclerosis
(Sitzer et al., 2003). Ischemic stroke is more often diagnosed in the left compared with the right
hemisphere, and the underlying etiology of this discrepancy is unclear. Recently, differences in
plaque components have been described, with a greater prevalence of unstable plaque features in
the left versus the right carotid in the Rotterdam cohort (Selwaness, van den Bouwhuijsen, van
Onkelen, et al., 2014). The underlying reason for this predilection may be due to differences in
shear stress between the left and right carotid arteries due to the arterial anatomy. Blood flow to
the right carotid artery is more direct, presumably resulting in higher shear stress. In contrast, by
the time blood reaches the left internal carotid artery, it has travelled a longer path and has
curved along the aortic arch. Presumably, any presence of atherosclerosis along the way could
induce lower shear stress. While the increased diagnosis of stroke in the left hemisphere may be
related to the underdiagnosis of right hemisphere stroke in clinical practice (Paul A. Heidenreich
et al., 2011), the possibility of differences in plaque components and hemodynamic differences

30
remains to be studied. From a clinical perspective, regardless of differences in carotid artery
disease and the underlying etiology, both carotids are always included in imaging assessments.
1.4.3 Ischemic Stroke
Strokes are broadly classified as ischemic or hemorrhagic, reflecting the underlying etiology.
Nearly 85% of strokes are ischemic, and 15% are hemorrhagic. Carotid atherosclerosis causes
20% to 30% of ischemic strokes (see Figure 1.17).
Figure 1.17: Classification and Estimates of the Frequency of Stroke Etiology.
Reproduced from (Albers, Easton, Sacco, & Teal, 1998) with permission
(License: 3850340870541).
The etiology of stroke includes extracranial vasculature atherosclerosis that affects the aortic
arch or the vertebrobasilar arteries, intracranial penetrating artery atherosclerosis or disease,
cardioembolism related to atrial fibrillation, or cardiogenic emboli or valve disease (see Figure
1.18).

31
Figure 1.18: Sources of Thromboembolism. Reproduced from (Albers et al.,
1998) with permission (License: 3850340870541).
The relationship of the carotid with ischemic stroke was first documented in ancient
Greece. "Carotid," from the Greek word “karos,” means “to stupefy.” Compression of the carotid
arteries was known to induce stupefaction, as evidenced by art found in the architecture of the
Parthenon (Munster, Thapar, & Davies, 2016). The art on the column of the Parthenon shows a
centaur compressing the neck of a Lapith during the mythological battle of Centauromachy. In
400 B.C., Hippocrates was among the first people to propose that “unaccustomed attacks of
numbness and anesthesia” may predict apoplexy (Robicsek, Roush, Cook, & Reames, 2004).
Reports between 1600 and the 1900s presented several advances concerning the link
between the carotids and stroke. Wepfer observed a disrupted blood supply at the carotid in four
autopsy cases with apoplexy (1658) (Munster et al., 2016). Van Swieten proposed the theory that
cerebral embolism causes strokes (1754), although he treated no cases of this condition (Munster
et al., 2016). Carswell found that the brain softened with carotid occlusion or carotid division

32
occlusion (Carswell, 1838). Kussmaul, a student of Virchow, reported that carotid artery
thrombosis was associated with ipsilateral blindness (Kussmaul, 1872).
The most definitive link between carotid stenosis and ischemic stroke was reported in the
mid-1900s. Moniz presented the first carotid arteriogram in 1927 (Doby, 1992). Using carotid
arteriograms in 1951 and 1954, Miller Fisher presented the first definitive observations
concerning carotid stenosis and stroke (Fisher, 1951, 1954). In his 1951 paper, Fisher postulates
that bypass and anastomosis of an occluded carotid would be feasible. Soon after, on August 7,
1953, DeBakey performed the first successful carotid endarterectomy, resulting in a 19-year-long
event-free rate, at which point the patient died from coronary occlusion (DeBakey, 1975). In
1980, Charles Kerber performed the first angioplasty (Kerber, Cromwell, & Loehden, 1980). The
reader is referred to a more comprehensive review of the history of carotid stroke (Munster et al.,
2016) summarized above.
In the 1990s, trials investigated whether carotid endarterectomy based on the stenosis
grade improved clinical outcomes. Well known trials include the North American Symptomatic
Carotid Endarterectomy Trial (NASCET) (N. A. S. C. E. T. Collaborators, 1991), the European
Carotid Surgery Trial (ECST) (E. C. S. T. C. Group, 1998), the Asymptomatic Carotid
Atherosclerosis Study (ACAS) (E.C.A.C.A.S., 1995), and the Asymptomatic Carotid Surgery
Trial (ACST) (M. A. C. S. T. A. C. Group, 2004). Clinical trials have demonstrated the benefit of
carotid endarterectomy in moderate and severe grade carotid artery disease among symptomatic
patients. Collectively, the recommendations from these trials include surgical intervention for
moderate and severe symptomatic carotid stenosis and severe asymptomatic carotid stenosis in
patients with less than 3% perioperative risk.
Among asymptomatic patients, however, the management of carotid artery disease
remains highly controversial (Naylor, 2015). Optimal medical therapy is considered the standard
of care, and carotid endarterectomy is typically only considered in these asymptomatic patients if
they have greater than three to five years of life expectancy, less than 3% risk of perioperative
death, and are younger than 70 years of age (Hussain, 2015). Based on the ACST, which
included all patients with asymptomatic moderate carotid artery stenosis, a 43% relative risk
reduction in the five-year risk of disabling stroke from 6.1% to 3.5% was observed for patients

33
on optimal medical therapy versus those on optimal medical therapy who had undergone carotid
endarterectomy, respectively. Stroke rates in patients with moderate carotid artery disease remain
high, and whether surgical intervention is warranted is unclear (Naylor, 2015). Although current
care is based on the clinical evaluation of risk factors such as age, perioperative mortality, and
life expectancy (Hussain, 2015), many of these patients will develop stroke. Stroke rates are as
high as 16% at 10 years (Halliday, 2010). More precise tools such as vessel wall imaging for
risk-stratification of carotid artery disease are required.
Improved techniques may also reveal complicated carotid atherosclerosis as a source of
thromboembolism in cryptogenic stroke. Cryptogenic stroke is a major diagnostic dilemma, with
as many as a quarter of stroke patients and half of transient ischemic attack (TIA) patients
presenting with no underlying reason for stroke or TIA. Stroke and TIA patients, despite <50%
ipsilateral carotid stenosis according to Trial of ORG 10172 in Acute Stroke Treatment
(TOAST) (Adams et al., 1993) and less than 70-99% carotid stenosis according to ASCOD
(atherosclerosis, small-vessel disease, cardiac pathology, other causes, dissection) (Amarenco et
al., 2013), may be classified as cryptogenic, more recently termed embolic stroke of
undetermined source (ESUS). Paroxysmal atrial fibrillation and complicated carotid
atherosclerosis are thought to be likely underlying reasons for ESUS. As many as 16.1%
(Gladstone et al., 2014) to 30% (Rizos et al., 2012) of patients with cryptogenic stroke or TIA
have atrial fibrillation. These patients are often overlooked with routine monitoring techniques
due to paroxysmal atrial fibrillation. In the EMBRACE trial (Gladstone et al., 2014), a
prospective randomized control trial of a cohort of adults ≥55 years of age with cryptogenic
stroke, patients assigned to a diagnostic strategy of prolonged 30-day event-triggered
electrocardiography (ECG) monitoring (intervention) compared with conventional 24-hour ECG
monitoring (control) had an improved diagnosis of atrial fibrillation lasting 30 seconds or longer
within 90 days (16% vs. 3.2%).
Similarly, nonroutine evaluation of the carotid arteries using advanced imaging has
suggested that even in patients with less than 50% stenosis, the carotids may be a source of
thromboembolism in ESUS stroke. For example, carotid plaque MRI showed that complicated
plaque components are often present in patients with ESUS and low-grade stenosis (Cheung et

34
al., 2011; Freilinger et al., 2012; Gupta et al., 2016; Gupta, Gialdini, et al., 2015). Carotid
atherosclerosis is associated with ischemic stroke, and advanced imaging strategies may be
particularly useful for the evaluation of cerebrovascular disease in patients with asymptomatic
and ESUS.
1.4.4 Systemic Disease
Because atherosclerosis is a systemic disease, carotid atherosclerosis may indicate the presence
of disease in other vessels, including the coronaries, ileofemoral arteries, and abdominal aorta
(Gallino et al., 2014). Patients such as those with peripheral vascular disease are often
comprehensively examined for the presence of disease in other vascular beds such as the carotids
(Qureshi et al., 2007). The systemic nature of atherosclerosis presents the possibility of
identifying coronary atherosclerosis with noncoronary disease characterization (Gallino et al.,
2014). The identification of polyvascular disease may be significant because polyvascular or
multifocal disease patients are at higher risk of adverse clinical outcomes, including
cardiovascular death, nonfatal myocardial infarction (MI), nonfatal stroke, and hospitalization,
and a greater number of outcomes are associated with a greater number of locations of
symptomatic disease (Sirimarco et al., 2013; Steg et al., 2007). Steg et al. have reported that
these cardiovascular outcomes affect 5.31% of patients with only risk factors. In contrast, in
patients with one, two, and three symptomatic arterial locations, cardiovascular outcomes may
occur in 12.58%, 21.14%, and 26.27% of patients, respectively (P<0.001 for trend) (Steg et al.,
2007). Whether carotid plaque characterization can improve risk stratification or provide insights
into high-risk patients remains to be tested and is one area that is investigated further in this
thesis.
1.5 Carotid Artery Stenosis
Landmark carotid artery trials such as NASCET and ECST recognized stenosis as a major risk
factor for stroke. Clinical practice necessitates the evaluation of stenosis because major trials
studied surgical and medical interventions for patients with stenosis. The NASCET and ECST
trials describe two methods that are commonly used to quantify carotid stenosis. NASCET
effectively quantifies stenosis based on the luminal reduction compared with the internal carotid

35
artery (ICA) distal outflow (Allan J. Fox & Singh, 2015). The method described by the ESCT
trial measures the luminal reduction of stenosis and compares this value to the unseen ICA bulb
width visible on standard angiography (the stenotic atheroma covers the ICA bulb). This ECST
percentage of stenosis is derived from a denominator of up to twice the diameter of the distal
ICA, with the ICA bulb being the largest part of the artery.
Figure 1.19: Measuring Stenosis Using the NASCET Method. The degree of
stenosis = 1 - N/D. Reproduced from (A J Fox, 1993) with permission (Received
Mar 10, 2016).
The NASCET method for measuring carotid stenosis on angiography is employed most
commonly in current practice settings. The degree of carotid stenosis, defined as percent carotid
stenosis, is calculated using the formula 1 - N/D (see Figure 1.19). N indicates the numerator,
which is measured at the narrowest portion of the stenosis. D indicates the denominator and is
measured well beyond the tapering of the carotid bulb where the wall of the internal carotid
artery becomes parallel.
Several pitfalls are possible when measuring NASCET stenosis in clinical practice and
research. The use of the NASCET method for percent stenosis without complying with specific
details of how measurements are obtained is known to occur (A. J. Fox et al., 2009). A stenosis
that is characterized as moderate according to NASCET criteria may be identified as severe if it
is not properly measured (Allan J. Fox & Singh, 2015).

36
The lack of assessment for near occlusion is another concern when measuring stenosis.
The nearly complete collapse of the ICA lumen beyond a very severe stenosis (see Figure 1.20)
is referred to as a near occlusion in the NASCET trial.
Figure 1.20: Near Occlusion in Carotid Artery Disease. There is a collapsed
lumen beyond very severe stenosis with flow reduction associated with a
presumed physiological loss in the diameter of the distal ICA. Reproduced figure
published by Wolters Kluwer Health, Inc., from (N.A.S.C.E.T. Collaborators,
1991) (License 3833990759397).
Less well identified is a minor physiological loss of diameter in the ICA beyond severe
stenosis that can be considered “normal-looking” but otherwise exhibits partial collapse (Bartlett,
Walters, Symons, & Fox, 2006; A. J. Fox et al., 2005). Both categories are referred to as “near
occlusion” in the NASCET (N.A.S.C.E.T. Collaborators, 1991) representing complete and
partial collapse. These near occlusions cannot be correctly measured and calculated for percent
stenosis because the distal ICA diameter is too small and deformed. Researchers in the NASCET
trial did not obtain measurements for near occlusion because the yielded percent can be
substantially lower than that in severe stenosis. Using a partially collapsed denominator for a
percent calculation would artificially reduce the percent stenosis, with some cases of severe

37
stenosis calculated as 60% or less. NASCET findings suggest that before the measurement of
any stenosis, the carotid should first be evaluated for the presence of a subtle near occlusion.
The value obtained from the measurement of the distal ICA diameter, well beyond the
bulb where the walls are parallel, was used as the denominator in the calculation of percent
stenosis in the NASCET trial. This strategy was used because the shape of the ICA bulb
transitions from wide to narrow. Measuring the ICA at positions where it is larger than the distal
ICA (where the walls are parallel) falsely increases the calculated percent stenosis (A. J. Fox et
al., 2009).
Stenosis can be measured using various modalities, including ultrasound, MRI, CTA, and
invasive digital subtraction angiography (DSA). Ultrasound is the most commonly performed
technique for screening carotid stenosis, whereas CTA is more useful in the acute stroke setting.
Follow-up imaging of patients with known stenosis commonly consists of magnetic resonance
angiography. Magnetic resonance angiography is less operator dependent, does not expose the
patient to radiation, can be conducted without contrast injection, is noninvasive, and allows for
luminal evaluation from the aortic arch to the intracranial vasculature.
DSA is considered the gold standard for accurate measurement of stenosis but may be
reserved for patients undergoing intervention (see Figure 1.21).

38
Figure 1.21: Internal Carotid Artery Stenosis Diagnosed with Invasive Digital
Subtraction Angiography. Invasive digital subtraction angiography is considered
the gold standard for measuring carotid artery stenosis. Reproduced from (Hyde
et al., 2004) with permission (License 3802180168941).
Rates of neurological complication associated with catheter cerebral angiography have been
reported to be approximately 2.6%, with a 0.14% rate of permanent stroke (Kaufmann et al.,
2007). Features such as ulcers, calcifications, and dissections can be visualized. False positives
may result from washed-out contrast. Artifacts from anything dense in the region of the carotid
may hinder the evaluation of stenosis. Catheter-based angiographic studies remain the most
accurate means of assessing the degree of carotid stenosis and exhibit relatively low
complication rates, with an extensive study showing deaths and permanent stroke in 12 and 27 of
19,826 patients, respectively (Kaufmann et al., 2007).
Doppler ultrasound is widely used for the classification of the stenosis grade. Compared
with arteriography, Doppler ultrasound is excellent for the classification of the stenosis grade
(Grant et al., 2000); however, it exhibits subpar performance for determining the exact degree of
stenosis and limited utility for the evaluation of near occlusion. Peak systolic velocity or peak
systolic velocity ratio in the common carotid artery relative to the internal carotid artery is

39
usually converted to estimate carotid stenosis. The wide standard deviations of velocity for any
given stenosis grade (see Figure 1.22) demonstrate the limited use of Doppler ultrasound for
determining the absolute stenosis value using velocity.
Figure 1.22: Carotid Artery Peak Systolic Velocity on Ultrasound and its
Corresponding Angiographic Stenosis. Ultrasound velocity in cm/sec for each
decile of angiography-confirmed stenosis diameter in the internal carotid artery.
Reproduced from (Grant et al., 2000) with permission (License: 02.10.2016).
Standardization is required for vascular laboratories to determine corresponding cutoff points for
velocity parameters used with true stenosis (see Table 1.3 for an example).
Ultrasound is operator dependent, and the measurement of stenosis requires knowledge of
carotid anatomy to recognize kinking, contralateral disease, and the presence of plaque
components such as calcifications. Ipsilateral flow ratios of the common carotid artery to the
internal carotid artery may not be valid if a contralateral occlusion is present. The presence of
dense calcifications may lead to inaccuracy, and the evaluation of tandem lesions may be difficult
due to the limited field of view.

40
Table 1.3: Ultrasound Velocity Cut-off Points to Classify Grade of Carotid
Stenosis. Reproduced from (Grant et al., 2000) with permission (License:
02.10.2016).
CTA is a vital part of the evaluation of an acute stroke patient. The need for a rapid
assessment of stroke patients is driven, in part, by the need to assess the proximal anterior
circulation for thrombi that are treatable with intra-arterial therapy (Berkhemer et al., 2015).
CTA of the carotid artery is limited due to radiation exposure and the use of iodinated contrast
agents. The carotids are included as part of the CTA acquisition, allowing for the evaluation of
carotid stenosis.
CTA permits visualization of the carotid arteries from the aortic arch to the intracranial
collaterals. Multidetector computed tomography (MDCT) permits the acquisition of 1- to 2-mm
slices with a single breath hold. Current multisection computed tomography (CT) scanners
enable the acquisition of up to 16 sections for each gantry rotation. Each rotation may require as
little as 0.4 seconds. Axial collimation for cervical-cerebral CTA is performed using a
collimation of 0.75 mm with a reconstruction of 1.5 mm for each axial image.
Carotid stenosis measurement is more reliable with CTA compared with DSA
(Silvennoinen, Ikonen, Soinne, Railo, & Valanne, 2007). Intracranial disease is also reliably
assessed with CTA (Nguyen-Huynh et al., 2008). Axial images, multiplanar reformatted images,
and 3-Dimensional or 3D volume maximum intensity projection (MIP) and volume-model
images contribute to the sensitivity and accuracy of multisection CTA. The ability to review
images in various planes and reformats mitigates potential issues posed by superimposing

41
structures such as veins. Features including ulceration and calcification are easily evaluated at
the time of stenosis measurements (see Figure 1.23).
Figure 1.23: Computed Tomography Angiography of Carotid Artery Disease
Demonstrating Ulceration and Stenosis. Ulceration (dashed arrow), stenosis
(solid arrow) and the external carotid artery (arrowhead) are seen. Reproduced
with permission from (Bartlett et al., 2006) (License 501105841).
CTA images are acquired rapidly, with no issues related to pacemakers or implants. The
3D reformats are available to delineate the anatomy and simultaneously evaluate the proximal
carotid, arch, and intracranial vasculature. Some limitations to the measurement of stenosis
include the presence of calcifications or high-density artifacts, artifacts related to motion, or poor
cardiac function. Intravenous contrast requires the rapid injection of approximately 150 ml of
300 to 320 mg/ml of nonionic contrast agent. A density of at least 150 Hounsfield Units (HU) is
typically required, with imaging initiated immediately before the contrast density peaks in the
carotid artery (Nadalo, 2015).
Magnetic resonance angiography (MRA) is commonly used to evaluate carotid stenosis
(see Figure 1.24). The MRA field of view (FOV) allows visualization of the carotid artery from
the aortic arch to the circle of Willis. Post-processing of MRI images, such as the creation of

42
multiplanar reformats (MPRs), MIPs, and 3D reconstructions, may facilitate the diagnosis of
stenosis (Runck, Steiner, Bautz, & Lell, 2008).
Figure 1.24: Time-of-flight Angiography Demonstrating Stenosis at the Origin
of the Internal Carotid Artery. Figure reproduced with permission from (Alan R.
Moody & Singh, 2015) (License: 3857810000492).
Both time-of-flight (TOF)-MRA and contrast enhanced (CE)-MRA possess comparable
sensitivity and specificity for detecting severe stenosis and total occlusions. TOF-MRA is
slightly less sensitive for the evaluation of carotid stenosis compared with CE-MRA. A summary
of data from a meta-analysis performed by Debrey et al. is shown in Table 1.4.

43
Table 1.4: Sensitivity and Specificity of Time-of-Flight and Contrast Enhanced Magnetic
Resonance Angiography for Evaluation of Stenosis against Gold Standard Digital
Subtraction Angiography. Rounded figures from (Debrey et al., 2008).
Degree of Stenosis TOF-MRA CE-MRA
Sensitivity Specificity Sensitivity Specificity
100 95 99 99 99
70 - 99 91 88 95 92
50-70 38 92 66 94
More recent studies specifically investigating 3T have also found that 3D TOF-MRA and
CE-MRA at 3T are reliable tools for detecting high-grade proximal ICA stenoses (70-99%)
(Weber et al., 2015). This study has suggested that TOF-MRA may misclassify pseudo-
occlusions as complete occlusions. Comparison of 2-dimensional (2D) TOF-MRA to CE MRA
has also revealed that the addition of gadolinium does not offer an advantage for distinguishing
surgical or high-grade stenosis (Babiarz et al., 2009). Some authors have suggested that TOF-
generated reformats are more likely to agree with stenosis grading compared with CE-MRA
(Runck et al., 2008). TOF-MRA is also highly concordant with CTA, to a greater extent than
CE-MRA (Lell et al., 2007). Others, however, have proposed that CE-MRA provides better
image quality, improves diagnostic confidence, and has better inter-observer agreement (Mitra et
al., 2006). Overall, CE-MRA is mostly used as a primary MRI modality, especially for 3T field
strength magnets, to prevent the overestimation of stenosis by TOF-MRA (Platzek, Sieron,
Wiggermann, & Laniado, 2014), in the absence of contraindications for gadolinium or for more
accurate characterization of lower grades of stenosis.
1.6 Carotid Intima-Media Thickness
The Atherosclerosis Risk in Communities (Chambless et al., 1997) and Rotterdam (van der Meer
et al., 2004) studies have demonstrated the relationship of carotid intima-media thickness (cIMT)
with cardiovascular outcomes, including myocardial infarction, stroke, and mortality. They
suggest that cIMT may be useful for the reclassification of patients from intermediate risk to
higher cardiovascular risk. Proposed clinical applications include the use of cIMT among
intermediate-risk or hypertensive patients for primary prevention of cardiovascular events

44
(Simova, 2015; Stein et al., 2008). There is some debate on the true benefit of routine screening
of patients with cIMT to assess the risk of initial coronary events. Despite some of the
prospective data suggesting the use of cIMT for reclassification of cardiovascular risk, the
American College of Cardiology (ACC)/American Heart Association (AHA) guidelines do not
endorse the use of cIMT for the detection of a first event (Goff et al., 2014). The information
provided by cIMT in terms of Framingham Risk Scores is limited. Data from 14 population-
based cohorts, including data for 45,828 individuals, indicated that cIMT provides small but
likely not clinically significant value to the Framingham Risk score (Den Ruijter, Peters,
Anderson, & et al., 2012). Serial imaging for changes in cIMT are also not recommended
(Touboul et al., 2012) because it does not predict cardiovascular outcomes (Lorenz et al., 2012).
Concerns regarding cIMT measurement quality have contributed to the ACC/AHA
recommending against routine screening for cIMT (Goff et al., 2014).
B-mode or 2D ultrasound allows evaluation of the intima-media thickness of the vessel
wall. Ultrasound imaging of the intima-media thickness is perceived as simple, readily available,
and unlikely to produce incidental findings. Image acquisition and measurement, however, are
operator-dependent. Clear reporting of the type of IMT value (e.g., mean or max), wall used
(e.g., near or far), carotid segment (e.g., CCA), software (e.g., automated or manual and type)
and angle of the operator at the time of measurement (e.g., single or multiple) may be required to
interpret images or to allow comparisons between serial measures. The standardization of carotid
intima-media thickness protocols and interpretations in research and clinical medicine has been
proposed (Stein et al., 2008). Standardized imaging of carotid intima-media thickness
necessitates the following protocols from larger studies such as the Atherosclerosis Risk in
Communities (ARIC) or Multi-Ethnic Study of Atherosclerosis (MESA) (see Figure 1.25) to be
able to apply the cIMT findings of these studies to cardiovascular outcomes.

45
Figure 1.25: Common Carotid Intima-media Thickness as Measured in the
MESA Trial. The progression of common carotid intima-media thickness was
found to predict stroke. The rectangular box delineates the area in which
measurements were obtained and is approximately 0.5 to 1 cm below the carotid
bulb (indicated by the vertical line). The arrow is pointing to focal thickness
before the carotid blood suggestive of early plaque formation and was excluded
from the measurements. Figure reproduced with permission from (Polak,
Pencina, O'Leary, & D'Agostino, 2011) (License 3839510217834).
According to epidemiological studies, the interpretation of normal cIMT values can be
adjusted for data specific to age, gender, and race/ethnicity. Increasing age is associated with
thickening of the intima-media. Typically, ultrasound screening in these studies defined a normal
cIMT thickness of less than 0.9 mm at the far wall of the distal common carotid artery.
Advanced carotid plaque imaging may provide further cardiovascular and cerebrovascular risk
stratification information.
1.7 Advanced Carotid Plaque Imaging: Modalities, Biomarkers, and
Cardiovascular Disease
Advanced carotid plaque imaging allows for improved visualization of the vessel wall compared
with carotid stenosis and intima-media thickness imaging (see Figure 1.26). Plaque burden,
composition, and activity can be evaluated rather than lumen or wall thickness alone. The

46
information gleaned from imaging characteristics on burden, composition, and activity in the
carotids may improve cardiovascular risk stratification and disease prevention.
Figure 1.26: Advanced Carotid Plaque Imaging for the Comprehensive
Evaluation of Atherosclerosis. Magnetic resonance imaging allows depiction of
several atherosclerotic components, including the lipid core (asterisk). The signal
hypointensity (asterisk) indicates the lipid core of an eccentric atherosclerotic
plaque with luminal preservation on fat saturation T1-weighted imaging pre- (a),
and post-contrast (b). Multicontrast images usually also include T2 fat saturation
(c), time-of-flight (d), and magnetization prepared rapid acquisition with
gradient-echo (e). Figure from (Singh, Moody, Roifman, Bluemke, & Zavodni,
2015) without any changes and in accordance with the Creative Commons
License (see http://creativecommons.org/licenses/by/4.0/legalcode).
Advanced imaging provides a dearth of biomarkers, “characteristic[s] that [are]
objectively measured and evaluated as indicator[s] of normal biological processes, pathogenic
processes, or pharmacologic responses to a therapeutic intervention” (Atkinson, 2001). For
example, measurements such as wall thickness or lipid core volume are indicators of the
processes taking place in an atherosclerotic vessel wall (see Figure 1.27).

47
Figure 1.27: Quantification of Carotid Plaque Morphology and Components. A
T1-weighted contrast-enhanced fat saturation image through the common carotid
depicting the vessel morphology including the lumen area (dot-dash line), total
vessel area (dashed line), and mean wall thickness (a value obtained by
averaging the number of cords, represented by the solid lines). The wall area is
calculated by subtracting the lumen area from the total vessel area. The lipid-rich
necrotic core component is also outlined (dotted line). Figure from (N. Singh et
al., 2015) without any changes and in accordance with the Creative Commons
License (http://creativecommons.org/licenses/by/4.0/legalcode).
For biomarkers to be useful for cardiovascular risk stratification, they must add
incremental information to traditional cardiovascular risk factors. The biomarker results should
also impact clinical management in a meaningful way (T. J. Wang, 2011). Biomarkers should be
associated with outcomes, should improve discrimination and calibration, and accurately
reclassify a large proportion of patients.
Compared with more traditional serum biomarkers, imaging biomarkers allow direct
visualization of an individual’s vessel wall disease. The potential utility of serum biomarkers that
reflect inflammation and proteolysis of a vulnerable plaque has been suggested. These include

48
hs-CRP, IL-6, MMP-9, MMP-2, TIMP-1 and TIMP-2. Serum biomarkers may be nonspecific for
the evaluation of a local plaque and may reflect processes in the noncarotid circulation.
Similarly, imaging may provide more information than cardiovascular risk factor scores for
incident cardiovascular events (Vlachopoulos et al., 2015; Zavodni et al., 2014; Pen et al., 2013).
Measures from various modalities, including ultrasound, CT, FDG-PET, (Fludeoxyglucose-
positron emission tomography) and MRI, are available for the evaluation of carotid arteries.
1.7.1 Ultrasound
The 2D total plaque area (TPA) and 3D total plaque volume (TPV) are two of the more
contemporary measures proposed (compared with the intima-media thickness) for the evaluation
of cardiovascular risk. The evaluation of larger regions of the vessel wall, particularly for the
assessment of volumes, is thought to provide more accurate insight into a patient’s carotid
disease burden. A more comprehensive evaluation compared with the intima-media thickness is
reflected in the definition of the total plaque area, the longitudinally measured sum of the cross-
sectional areas of the plaques of both carotids in the common carotid artery (CCA), internal
carotid artery (ICA), and external carotid artery (ECA) (Spence et al., 2002). Figure 1.28 shows
an example of plaque regression measured by the total plaque area in a patient over three months
(Spence & Hackam, 2010). Such changes would likely be overlooked when measuring intima-
media thickness (IMT).

49
Figure 1.28: Total Plaque Area Regression Using 2-Dimensional Ultrasound.
This plaque had also become denser with regression of the soft plaque, and
increased calcification was observed in just over three months. Reproduced from
(Spence & Hackam, 2010) with permission from Wolters Kluwer Health, Inc.
(License 3840900998176).
Indeed, TPA has been suggested to be superior to IMT for the prediction of myocardial
infarction events (AUC 0.64 versus 0.61) in a meta-analysis of data from 11 population-based
studies (Inaba, Chen, & Bergmann, 2012). Over 10 years, the rates of MI were lower among
subjects with a negative result on TPA (4%) vs. cIMT (4.7%). TPV, however, has been
demonstrated to be superior for evaluation of the progression and regression of disease compared
with TPA and IMT. In a study of 349 patients, TPV progression over a one-year time frame
predicted stroke, death, or TIA (Wannarong et al., 2013). TPA predicted these outcomes weakly,
whereas IMT was found to have no relationship with cardiovascular outcomes. The limitations of
2D ultrasound include potential imaging variability and arbitrary angle imaging of a thin plane,
resulting in an incorrect diagnosis (Fenster, Downey, & Cardinal, 2001). While 3D ultrasound
attempts to address some of these issues, immediate optimal rendering may not be available or
may require complex intervention by the user.
While ultrasound is widely available and commonly used, its dependency on operator
technique, as well as the limited spatial and contrast resolutions available, make it less preferable
for evaluation of carotid plaque biomarkers. For example, carotid stenosis in surgical lesions
(Johnson, Wilkinson, Wattam, Venables, & Griffiths, 2000) and plaque components (Y.

50
Watanabe et al., 2008) have been shown to be less accurately characterized relative to magnetic
resonance angiography. Compared with histology, color Doppler is less sensitive, specific, and
accurate than MRI for the diagnosis of at-risk soft plaques (sensitivity, 75 vs. 96%; specificity,
63 vs. 93%; accuracy, 69% vs. 94%, respectively) (Y. Watanabe et al., 2008). MRI depicted soft
plaques are defined as containing substantial lipid and/or IPH components, and ultrasound soft
plaques are defined as mostly echolucent.
1.7.2 Computed Tomography
The composition of carotid atherosclerotic plaques can be determined using CT. For
example, in a multidetector CTA study of eight TIA patients undergoing carotid endarterectomy
(CEA), it was found that plaque components could be accurately detected (Wintermark et al.,
2008). CTA interpretation of plaque components requires automated classification algorithm
software that relies predominantly on tissue density (see Figure 1.29).

51
Figure 1.29: In-Vivo Computed Tomography Angiography Image of the
Common Carotid Artery and Matching Ex-Vivo Microcomputed Tomography
and Histologic Sections. Automated classification computer algorithm-derived
overlay showing the lipid-rich necrotic core (yellow), calcification (blue), blood
products (red), and remaining connective tissue (green). Computed tomography
angiography overlay demonstrating a plaque with a large lipid core, small
calcifications, and an ulceration, making it a VIa lesion according to the
American Heart Association classification, in agreement with the histologic
examination, the gold standard for noncalcified carotid wall components, similar
to ex-vivo microcomputed tomography, the reference for carotid wall calcium
(specimens were decalcified before histologic sectioning). Reproduced with
permission from (Wintermark et al., 2008) (License: 3854911432902).
Features on CTA may also indicate high-risk plaque components such as IPH. In a
retrospective study, Eisenmenger et al. suggested that the presence of the calcified rim sign (see
Figure 1.30) is strongly indicative of a soft plaque containing an IPH (Eisenmenger et al., 2016).

52
Similarly, U-King-Im et al. and colleagues suggested that ulceration (see Figure 1.31) is
predictive of the presence of IPH. The combined and incremental value of various features such
as the rim sign, ulceration, and density require further study to determine their utility for
predicting stroke or other cardiovascular events rather than IPH. Well-designed prospective
studies would certainly be of interest; however, the use of CT over other modalities such as MRI
remains questionable from a cost, value, and radiation safety perspective.
Figure 1.30: Positive Rim Sign and Carotid Intraplaque Hemorrhage. In the
upper panel, the carotid computed tomography angiography demonstrates
positive rim signs (arrows) in both carotid plaques. In the lower panel,
magnetization prepared rapid acquisition with gradient-echo with bilateral
carotid intraplaque hemorrhage (arrows) in the same patient. Intraplaque
hemorrhage was defined by magnetization prepared rapid acquisition with
gradient-echo-positive plaque using a signal threshold of two-fold signal
intensity over the adjacent sternocleidomastoid muscle. Reproduced with
permission from (Eisenmenger et al., 2016) (License: 3865990342864).

53
CT exhibits improved spatial resolution compared with ultrasound; however, it exposes
the patient to ionizing radiation and iodinated contrast. MRI, although not yet widely available,
has greater diagnostic value than CT. Symptomatic carotid plaques are better characterized on
MRI compared with multidetector computed tomography angiography (MDCTA), although
MDCTA offers higher specificity at the cost of lower sensitivity (Grimm et al., 2014). In a study
of 22 stroke unit patients with symptomatic unilateral carotid disease, Type VI AHA (American
Heart Association) plaques identified with MRI (using T1, T2, and TOF) were found to better
predict symptomatic disease (sensitivity, specificity, positive predictive value, and negative
predictive value = 80%) relative to ulceration on MDCTA (sensitivity, specificity, positive
predictive value, and negative predictive value = 40, 95, 89, and 61%, respectively) (Grimm et
al., 2014). The performance of 3T MRI for carotid imaging is likely underestimated in this
particular study, which did not employ 3D imaging sequences (discussed below) or sequences
designed to detect Type VI AHA plaque features such as IPH (A. R. Moody et al., 2003; Ota,
Yarnykh, et al., 2010).

54
Figure 1.31: Simultaneous Presence of Carotid Intraplaque Hemorrhage and
Ulcer. (A) Magnetic resonance imaging depicting intraplaque hemorrhage (white
arrow) as a strong signal within the wall of the left carotid bulb of a recently
symptomatic patient. Sagittal (B), axial source image (C), and coronal computed
tomography angiography reformats of the left carotid artery in the same patient
revealing a large atherosclerotic plaque, causing only 50% stenosis but with a
small ulcer (black arrow) within the plaque. Figure reproduced with permission
from (U-King-Im et al., 2010) (License 3865970608471).
1.7.3 Positron Emission Tomography
Positron Emission Tomography (PET) is a nuclear medicine functional imaging technique that
detects regional positron emission (gamma rays) from radiotracers, typically the glucose

55
analogue fludeoxyglucose (18-F). Uptake of 18-F increases proportionally with the metabolic
activity that occurs during, e.g., inflammation or tumor growth. Carotid PET imaging has been
shown to reveal plaque inflammation that may be associated with plaque instability and high-risk
features of carotid plaques (see Figure 1.32) (Hyafil et al., 2016). However, any suggested
incremental value of PET-MRI over MRI or PET-CT over MRI remains to be determined.
Figure 1.32: High-risk Carotid Plaque Characterized with Positron Emission
Tomography Magnetic Resonance Imaging. Representative example of a high-
risk carotid atherosclerotic plaque formed of lipid rich-necrotic core and
intraplaque hemorrhage imaged with combined 18 F-FDG positron emission
tomography and magnetic resonance imaging. Corresponding axial views of a

56
nonstenotic carotid atherosclerotic plaque acquired simultaneously using a
combined imaging system including magnetic resonance imaging with
successive high-resolution black-blood T2W (a), black-blood T1W before (b)
and 5 min after injection of gadolinium chelates (c) and time-of-flight sequences
(d) and positron emission tomography images (e) acquired 150 min after
injection of 18 F-FDG, allowing perfect matching of both acquisitions (f; fusion
image formed of time-of-flight and 18 F-FDG positron emission tomography
images). Note the presence of a nonstenotic atherosclerotic plaque ipsilateral to
the vascular territory of the stroke (a–d; white arrowheads) formed of a
hypointense area on T1W, and T2W and time-of-flight sequences and a
hyperintense area on T1W, T2W and time-of-flight sequences consistent with
the presence of lipid rich-necrotic core associated with intraplaque hemorrhage
type II. High accumulation of 18 F-FDG was detected with positron emission
tomography in the corresponding area (e–f; white arrowheads), supporting the
presence of elevated inflammatory activity in the atherosclerotic plaque.
Reproduced with permission from (Hyafil et al., 2016) (License:
3866010395175).
1.7.4 Magnetic Resonance Imaging
Carotid MRI offers several advantages for evaluation of carotid disease biomarkers over other
modalities. The modality permits accurate characterization and quantification of carotid
biomarkers, does not require administration of iodine or ionizing radiation, and is not operator-
dependent. Despite perceived limitations regarding availability, carotid MRI has been suggested
to be cost-effective among select subgroups (Gupta, Mushlin, Kamel, Navi, & Pandya, 2015;
Saam et al., 2013), clinically useful for identifying patients at risk of stroke (Gupta et al., 2013),
and appropriate for identifying patients with a high-risk cardiovascular phenotype or risk of
cardiovascular events (Noguchi, Yamada, Higashi, Goto, & Naito, 2011; Singh, Moody,
Rochon-Terry, Kiss, & Zavodni, 2013; Sun et al., 2015; Zavodni et al., 2014). Carotid pulse
sequences allow image acquisition within minutes (N. Balu et al., 2011).
Another advantage of carotid MRI is that it may already be included or appended to
neurovascular imaging examinations to provide simultaneous information on cerebrovascular
ischemic injury. For example, a 75-year-old male referred for peripheral vascular disease and

57
known carotid artery disease underwent neurovascular MRI in 2010 and 2012. A new white
matter lesion was found in 2012 (see Figure 1.33), suggesting interim carotid plaque instability.
Figure 1.33: Progression of White-Matter Disease. In these images, fluid-
attenuated inversion recovery magnetic resonance imaging depicts a new white
matter lesion (arrowhead) on the left in 2012 compared to 2010. Development of
new white-matter lesion in a patient with ipsilateral carotid plaque containing
ulcer and intraplaque hemorrhage. © Navneet Singh and Alan Moody, 2016. All
rights reserved.
Time-of-flight magnetic resonance angiography shows the development of a new ulcer in
the internal carotid artery, implicating the carotid artery as the source of the thromboembolism
(see Figure 1.34).

58
Figure 1.34: Development of Carotid Artery Ulceration. Time-of-flight 3-
dimensional magnetic resonance angiography demonstrates the development of a
new ulcer (arrowhead) in a patient with progression of ipsilateral white-matter
disease and underlying carotid intraplaque hemorrhage. Sagittal oblique
reformats (a, d) and corresponding axial images at the level of the blue lines (b-c,
e-f) are shown. © Navneet Singh and Alan Moody, 2016. All rights reserved.
The competitive edge of MRI lies in its ability to accurately characterize vessel wall
plaque biomarkers, including components, plaque burden, and luminal stenosis. MRI can
measure the wall thickness and include the adventitia, which is excluded on ultrasound (Zhang,
Guallar, Qiao, & Wasserman, 2014). This adventitia may be especially important given that vasa
vasorum initially proliferates in this region and is implicated in plaque progression related to IPH
(Virmani, Kolodgie, & Burke, 2005). Initial carotid MRI investigations have validated 2D
carotid imaging techniques against histology for plaque characterization using a combination of
bright and dark blood acquisitions. Multicontrast imaging techniques employ multiple T1 and T2
weighting, as well as an option for the addition of gadolinium, allowing for assessment of
disease burden, components, and activity. For example, standard carotid MRI acquisitions would
include T1, T2, PD, T1 post-contrast, and time-of-flight angiography. Plaque components may
be determined based on their signal characteristics in multicontrast magnetic resonance imaging.
The high lipid (i.e., cholesterol and cholesterol ester) content of the necrotic core results in rapid

59
T2 decay and manifests as a hypointense signal on T2 images. Post-contrast imaging allows
visualization of the fibrous cap and lipid core (Cai et al., 2005; Kwee et al., 2009). The lipid-rich
necrotic core is visualized due to poor vascularity in post-contrast T1-weighted studies. IPH is
identified by its T1 signal intensity and occurs as a result of the shortening of T1 caused by blood
methemoglobin (see Figure 1.35).
Figure 1.35: Magnetic Resonance Imaging of Carotid Vessel Wall and
Intraplaque Hemorrhage. (A) Vessel wall imaging showing bilateral vessel wall
thickening (arrows). (B) Time-of-flight (TOF) magnetic resonance angiography
shows no significant luminal narrowing. (C) One year later, an intense strong
signal is seen in the right common carotid vessel wall thickening, consistent with
the occurrence of IPH in the interim period (arrows). (D) Time-of-flight
magnetic resonance angiography one year later is unchanged. Figure reproduced
from (Alan R. Moody & Singh, 2015) with permission (License:
3857810000492).
The temporal resolution of IPH imaging is on the order of minutes, and therefore,
sequences for the evaluation of this plaque component can be appended to neurovascular
imaging exams. In the previous example of the patient with the simultaneous presence of a

60
carotid ulcer and a new white matter lesion on follow-up imaging, the ulcer occurs at the site of
prior IPH (see Figure 1.36) depicted on a black blood carotid MRI sequence.
Figure 1.36: Intraplaque Hemorrhage Underlying Patient with New Carotid
Ulcer and White-Matter Lesion. Magnetic resonance-intraplaque hemorrhage
(MR-IPH) 3-dimensional imaging (matrix, 272 x 224; field of view, 270 x 190
mm; slice thickness, 0.5 mm; 16-channel neurovascular coil) revealing
intraplaque hemorrhage (arrowhead) at the site of subsequent internal carotid
artery ulceration in 2012. A large amount of intraplaque hemorrhage underlies
the ulceration site in 2010 (a, c), with residual intraplaque hemorrhage remaining
in 2012 (outlined by the yellow-dashed line) (e, f). Sagittal oblique reformats (a,
d) and corresponding axial images at the level of the blue lines (b-c, e-f) are
shown. © Navneet Singh and Alan Moody, 2016. All rights reserved.
Various histological correlation studies have demonstrated the ability of MRI to
accurately and directly visualize the lipid-rich necrotic core, fibrous cap, and IPH (Bitar et al.,
2008b; Cai et al., 2005; Cappendijk et al., 2008; A. R. Moody et al., 2003; Yuan et al., 2001).
Table 1.5 summarizes the features of plaque components on carotid MRI based on various
histology-imaging correlation studies.

61
Table 1.5: Plaque Component Signal Characteristics on Carotid Magnetic Resonance Imaging. Table from (N. Singh et al., 2015) without any changes and in accordance with the Creative Commons License (http://creativecommons.org/licenses/by/4.0/legalcode).
Typical 2D multicontrast MRI permits the acquisition of images encompassing 3 to 4 cm
of the carotid artery (Yuan et al., 2001). The protocols are centered at the carotid bifurcation
(Yuan et al., 2001), a region with a predilection for atherosclerosis, and result in 2-mm-thick
slices in the through-plane direction. Thus, 3 or 4 cm of coverage would result in 16 to 20 slices.
However, earlier studies appeared to only match four to six locations across multiple acquisitions
to the histological findings (Yuan et al., 2001). Most of these sequences also employed a 256 x
256 matrix with a 13-cm field of view. This would result in a voxel size of 0.5 (in plane x) by 0.5
(in plane y) by 2 mm (through plane z). To reduce voxel sizes and minimize partial volume
artifacts, these protocols also employed a zero-filled Fourier transform, resulting in voxels of
0.254 by 0.254 by 2.0 mm (Yuan et al., 2001). To obtain black blood images for T1, T2, and
proton density (PD) weightings, flow was suppressed via double inversion recovery. The 2D
protocols also used fast spin echo. Furthermore, these protocols employed a custom-designed
phased-array surface coil, 1.5T scanners, and cardiac gating. Early prospective trials established
multicontrast MRI protocols (T. Saam et al., 2005; Yuan et al., 2001) and demonstrated the value
of these protocols for the prediction of ischemic neurovascular events (Takaya et al., 2006).
Multicontrast MRI has various limitations, including a long acquisition time, small
volumes of coverage, and variable image quality. Multicontrast imaging requires registration of
multispectral acquisitions because the acquisitions are obtained separately for each contrast (e.g.,
T1, T2) at different times throughout the imaging protocols. Patient motion may lead to
misregistration. The field of view is also limited to a few centimeters. Carotid MRI is, however,
advancing from 2D to 3D imaging techniques. The use of 3D imaging will allow acquisitions
from the Circle of Willis to the aortic arch, rather than bifurcation alone (A. R. Moody et al.,
2003). As a result, long segments of the vessel wall can be evaluated more completely.

62
Furthermore, such 3D sequences can be acquired in four to five minutes, which may be
particularly important for evaluating disease along the carotid artery, and in particular, some
areas such as the aortic arch may be of interest in the work-up of stroke patients or for
intervention planning. The aortic arch is often screened for disease prior to aortic clamping in the
coronary artery bypass graft.
Hardware such as a surface coil may introduce signal heterogeneity (see Figure 1.37) (N.
Singh et al., 2015). The use of neurovascular phased-array coils may be one solution to
ameliorate this issue.
Figure 1.37: Magnetic Resonance Imaging Surface Coils. Dedicated Surface
Coils Provide an Improved Signal-to-noise Ratio for Superficial Structures (A).
When these coils are applied to a cylindrical water phantom measuring 6 cm in
diameter, the drop-off in signal intensity on the T1-weighted images provides a
visual demonstration of the penetration depth of the coil (B). Figure from (N.
Singh et al., 2015) without any changes and in accordance with the Creative
Commons License (http://creativecommons.org/licenses/by/4.0/legalcode).
Despite the promising nature of 3D carotid MRI for evaluation of carotid atherosclerosis,
there are some challenges that would benefit from investigation. Flow suppression in 2D MRI
usually employs flow suppression techniques such as double inversion recovery of motion
sensitization. However, given that 3D volumes are on the order of 30 cm rather than 3 to 4 cm,
flow suppression may be challenging. Motion-sensitized dephasing, for example, by motion-
sensitized driven equilibrium (MSDE) preparation (J. Wang et al., 2007) requires that an image
be acquired immediately after application and before recovery of the longitudinal magnetization
vector (N. Balu et al., 2011). The length of the scan time using this strategy is four to five

63
minutes compared with 40 minutes, and may reduce motion-related artifact. Furthermore,
promising sequences in 3D carotid MRI are emerging that may allow the simultaneous
assessment of stenosis and the vessel wall in a single acquisition capable of imaging both bright
blood and dark blood (J. Wang et al., 2013).
In addition to a shift from 2D to 3D imaging for evaluation of carotid plaque, there have
also been improvements in the MRI field strength. Initial imaging was performed at 1.5 Tesla or
1.5T; however, 3T allows for greater signal-to-noise ratio (SNR). For example, when considering
3D magnetization-prepared rapid acquisition with gradient-echo (MPRAGE), image quality was
very slightly improved but mostly retained at 3T compared with 1.5T (S. McNally et al., 2014)
(mean 3.87 vs. 4.34 on a 5-point scale, P<0.0001). The reliability on 3T and 1.5T was similar
and approximately 0.8 for inter-rater reliability and 0.9 for intra-rater reliability. The greater field
strength may pose an issue for quantification of plaque components, such as calcium or IPH,
which are more susceptible. Using an automated quantification algorithm, Kerwin demonstrated
no significant differences in signal between 3T and 1.5T for plaque components, including IPH
(Kerwin et al., 2008). The next section addresses advanced carotid MRI for cardiovascular
disease prevention applications.
1.8 Carotid Magnetic Resonance-depicted Intraplaque Hemorrhage
Imaging
Carotid MRI has the potential to provide information regarding various plaque components and
morphological biomarkers. Among the various vessel wall plaque component biomarkers
available through carotid MRI, IPH can be easily imaged, routinely investigated in the clinical
setting, and provides useful clinical information. The presence of carotid IPH provides insight
into cardiovascular risk and aids in identification of culprit carotid lesions in stroke patients.
Carotid IPH has a hazard ratio of five to six for stroke, which outweighs any of the risk factors
for stroke (Bonati & Nederkoorn, 2015). There is increasing interest in evaluation of this
biomarker, given that the pathophysiology of IPH may enhance the progression of
atherosclerosis, exhibit relationships with other cardiovascular outcomes such as myocardial
infarction, and can be easily detected. The clinical feasibility and usefulness for identifying a

64
high-risk cardiovascular phenotype has prompted extensive MRI studies to evaluate IPH using
2D methods such as multicontrast imaging. Imaging of IPH using 3D modalities (see Figure
1.38) may be useful for routine clinical practice.
Figure 1.38: Three-Dimensional Carotid Magnetic Resonance Imaging of
Intraplaque Hemorrhage. © Navneet Singh and Alan Moody, 2016. All rights
reserved.
The sequences required to apply this technique are readily available on all scanner
platforms, images are rapidly acquired, IPH detection is accurate, and interpretation is simple,
presently consisting of dichotomization of the results into the presence or absence of IPH.
Furthermore, MRI is currently the only readily available imaging technique for the detection of
plaque hemorrhage, and it is already used for investigations of carotid artery disease, thus
making the addition of this one sequence to the standard carotid artery imaging protocol simple

65
and causing little time-cost impact. Our institution has employed this 3D carotid IPH imaging
approach (see Figure 1.38) as part of routine neurovascular imaging over the past decade. The
experience provides an opportunity to better understand both the determinants and consequences
of this biomarker. The thesis uses this IPH experience to address IPH and its age-specific sex
differences in low-grade stenosis, role in ipsilateral embolic stroke of undetermined source, and
the relationship with a high-risk cardiovascular phenotype. This work raises questions about the
significance of quantification of IPH and its relationship with clinical outcomes. The final project
in this thesis therefore demonstrates the reliability of a quantitative imaging analysis protocol
that may be used future trials.
1.8.1 Carotid Artery Disease Evaluation Paradigm Shift and Knowledge Gaps
500,000 new stroke events occur each year in the United States (J. Broderick et al., 1998).
Greater than 80% of strokes are ischemic, of which 15 to 20% result from carotid artery
atherosclerosis. Carotid artery atherosclerosis management has been directed by evidence from
NASCET and ECST; landmark carotid trials though dating from nearly 30 years ago
(N.A.S.C.E.T. Collaborators, 1991; E. C. S. T. Group, 1998). In these trials, carotid
atherosclerosis was estimated by measuring luminal stenosis as a surrogate. Patients found to
have high-grade carotid artery stenosis presumably due to significant atherosclerotic disease were
demonstrated to benefit from carotid endarterectomy. However, the number needed to undergo
surgery to prevent a single stroke required as many as 8 to 83 patients, depending on the degree
of stenosis and presence of symptoms (Gorelick, 1999). Patients with lower grades of stenosis
however may have significant carotid plaque with the lumen maintained until later stages of
disease in the progression of atherosclerosis. This phenomenon described by Glagov (Glagov et
al., 1987), may represent a missed opportunity for stroke intervention. Direct visualization of
carotid atherosclerosis disease burden and plaque components allows for identification of a high-
risk group of patients at risk of end-organ events and opportunity to intervene. Magnetic
resonance imaging may allow for the identification of plaque components at increased risk of
causing clinical end-organ outcomes.

66
1.8.1.1 MR-IPH and Outcomes
Systematic reviews and meta-analyses have demonstrated that MRI identified plaque
components such as intraplaque hemorrhage, fibrous cap thickness, and lipid core are associated
with cerebrovascular events (Hosseini, Kandiyil, Macsweeney, Altaf, & Auer, 2013). Patients
with IPH rather than other plaque components have higher odds of future cerebrovascular events
(Hellings et al., 2010; Hosseini et al., 2013). Metanalyses including those by Saam and
colleagues (Saam et al., 2013) and Gupta and colleagues (Gupta et al., 2013) have demonstrated
a 5.7- and 4.6-fold higher risk of cerebrovascular events in patients with IPH. IPH also appears to
perform better when compared to existing risk scores suggesting that direct visualization of
plaque components may provide an opportunity for personalized risk stratification. Altaf and
colleagues found that carotid IPH was associated with future cerebrovascular events whereas the
ECST risk scores were not (Altaf et al., 2014). Prospective multicenter trials accumulating
hundreds of patients with serial carotid MRI such as the Canadian Atherosclerosis Imaging
Network Project 1 are anticipated to confirm these observations in the Canadian context (Tardif
et al., 2013).
1.8.1.2 Gaps Overview
Understanding the relationship with risk factors, clinical outcomes, and natural history of IPH
may be facilitated by an IPH imaging database. The paucity of carotid MRI in routine clinical
practice is one hindrance to collecting a sizeable database of IPH imaging for research purposes.
Accumulating a database of patients with carotid MRI including patients of low-grade stenosis is
one particularly promising opportunity for studying intraplaque hemorrhage. A database of IPH
imaging including low-grade stenosis patients would supplement studies seeking to understand
the natural history and determinants of IPH (Kandiyil, Altaf, Hosseini, MacSweeney, & Auer,
2012), such as effect of age and sex, though limited to higher grades of stenosis. The database
would also allow for study of stroke etiology in patients with embolic stroke of undetermined
source (that by definition are deemed to have <50% stenosis). Knowledge gaps on carotid IPH
and cardiovascular events could also be studied if the database were to be populated with data on
cardiovascular history, imaging and clinical outcomes, and demographic information such as age,

67
sex and ethnicity. Others have demonstrated relationships of carotid intima-media thickness and
cardiovascular events in large population studies (Polak et al., 2011), though few studies address
the potential prognostic value of plaque components such as IPH.
In addition to testing hypotheses surrounding presence of IPH for the identification and
risk stratification of a high-risk cardiovascular and cerebrovascular phenotype, whether IPH
volume, location, age, surface features, co-plaque components, and geometry may improve
reclassification and patient outcomes come into question. IPH depicting pulse sequences, image
analysis tools and segmentation algorithms that are accurate, reliable and easy to use may assist
in evaluating IPH more robustly. Furthermore, the use of the IPH imaging information gleaned
either independently or in combination with patient’s status of circulating inflammatory markers,
genetics, comorbidities, sex and ethnicity, requires further study for identification of high-risk
patient groups and impact of these factors on IPH and outcomes. For example, genetics of a
patient such as haptoglobin genotype may assist in the targeted imaging detection of IPH
(Marvasti et al., 2018). Ultimately one goal is to target these high cardiovascular and
cerebrovascular risk groups for prevention and intervention. Reliable quantification of IPH may
be useful in evaluating response to therapy, testing for new therapeutic targets, and effectiveness
of preventative efforts. In particular, methodologies with good inter-, intra-, and scan-rescan
reliability of 3D carotid artery 3T MRI to volumetrically quantify IPH are among the next steps
towards furthering the clinical translation of IPH imaging.
1.8.1.3 Potential IPH Imaging Impact
Carotid IPH may allow for detection of patients at risk of stroke that would benefit from CEA.
Several trials have demonstrated the benefit of CEA in moderate and severe grade carotid artery
disease among symptomatic patients, though even this subgroup may benefit from further risk
stratification. Among asymptomatic patients, the management of carotid artery disease remains
highly controversial (Naylor, 2015) and is one specific group in whom further risk stratification
based on presence of IPH may be useful. OMT is considered the standard of care and CEA is
typically only considered in these asymptomatic patients only if they have greater than 3 to 5
years of life expectancy, less than 3% perioperative death, and are younger than 70 years of age

68
(Anas Hussain, Verma, Gupta, & Al-Omran, 2015). In asymptomatic moderate carotid artery
disease, stroke rates are as high as 16% at 10 years (Halliday et al., 2010) and better tools for
risk-stratification are required. Employing IPH imaging in specific groups such as asymptomatic
moderate carotid artery disease patient group may potentially translate into saved lives through
more precise identification of patients at high risk of stroke. A direct trial comparing
incorporation of IPH into the management of carotid artery disease algorithm is clearly needed.
To this end, various efforts, beyond the scope of this thesis incorporating such questions are
currently underway including the ECST-2 (European Carotid Surgery Trial-2) and ACTRIS
(Endarterectomy Combined with Optimal Medical Therapy (OMT) vs OMT Alone in Patients
with Asymptomatic Severe Atherosclerotic Carotid Artery Stenosis at Higher-than-average Risk
of Ipsilateral Stroke).

69
1.9 Aims and Hypotheses
We hypothesized that the presence of carotid MRI depicted IPH is associated with
cardiovascular risk factors and consequences that indicate a high-risk cardiovascular and
cerebrovascular phenotype (see Figure 1.39).
Figure 1.39: Thesis Overview.
1.9.1 Age-Specific Sex Differences in MRI Depicted Carotid Intraplaque
Hemorrhage
The aim of this project is to investigate age-specific sex differences in carotid MR-IPH between
males and females. We hypothesize carotid MR-IPH is more prevalent in the carotid arteries of
males compared to females, and age-specific sex differences in carotid MR-IPH converge
between males and females with increasing age.

70
1.9.2 Carotid Magnetic Resonance Depicted Intraplaque Hemorrhage in
Embolic Stroke of Undetermined Source
The aim of this project is to investigate whether carotid MR-IPH is present in embolic stroke of
undetermined source patients. We hypothesize that carotid IPH depicted by MRI is associated
with ipsilateral stroke or TIA among embolic stroke of undetermined source patients.
1.9.3 Identifying a High-risk Cardiovascular Phenotype by Carotid MRI-
depicted Intraplaque Hemorrhage
The aim of this project is to determine the ability of MR-IPH to identify past cardiovascular
events defined as MI, coronary intervention, and peripheral vascular disease (PVD) in patients
investigated with MRI for neurovascular disease. We hypothesize patients investigated for
neurovascular disease who are found to have MR-IPH have an increased number of prior
cardiovascular events indicative of a high risk cardiovascular phenotype.
1.9.4 A Combined 3D Black-blood and Time-of-flight Magnetic Resonance
Imaging Approach for the Volumetric Quantification of Carotid Artery
Vessel Wall and Intraplaque Hemorrhage
The aim of this project is to investigate the inter-, intra-, and scan-rescan reliability of 3D carotid
artery 3T MRI, using a 3D T1w gradient echo black blood (GRE BB) and TOF acquisition,
to volumetrically quantify vessel wall and IPH and assess agreement with 2D T1
MRI for measuring vessel wall volume. We hypothesize that volumetric quantification of vessel
wall (VW) and IPH is highly reliable on 3D carotid artery 3T MRI and that quantification of VW
has excellent agreement with the 2D carotid artery MRI.

71
Chapter 2—Age-Specific Sex Differences in Magnetic
Resonance Imaging Depicted Carotid Intraplaque
Hemorrhage
This chapter contains sections or content either adapted or reproduced with permission
from the following peer-reviewed literature:
• Singh N, Moody AR, Zhang B, Koh L. The Effect of Sex and Age on Intraplaque
Hemorrhage Prevalence in Low-grade Carotid Stenosis. American Society of
Neuroradiology, Chicago, IL, USA. 2015. O-451.
• Singh N, Moody AR, Zhang B, Kaminski I, Kapur K, Chiu SE, Tyrrell PN. Age-
specific Sex Differences in MRI Depicted Carotid Intraplaque Hemorrhage. Stroke.
2017. 48(8): 2129-2135.

72
2.1 Overview Background and Purpose: Stroke rates are higher in males compared to females in the fourth
through seventh decades of life, and higher rates may result from differences in carotid
intraplaque hemorrhage (IPH), an unstable atherosclerotic plaque component. We report age-
specific sex differences in the presence of MRI depicted carotid IPH. Methods: Patients
(n=1115) underwent MRI for carotid IPH between 2005 and 2014. Low-grade carotid stenosis
patients (n=906) without prior endarterectomy were eligible for this cross-sectional study.
Results: Of the 906 patients included (mean age ± SD in years, 66.98 +/- 15.15), 63 (6.95%) had
carotid IPH. In males and females, carotid IPH was present in 11.43% (48/420) and 3.09%
(15/486), respectively (p<0.0001). Multivariable logistic regression analysis confirmed greater
odds of carotid IPH in males for all ages: 45 to 54 (OR=45.45, 95% CI 3.43 to 500), 55 to 64
years (OR=21.74, 95% CI 3.21 to 142.86), 65 to 74 years (OR=10.42, 95% CI 2.91 to 37.04),
and ≥75 years (OR=5.00, 95% CI 2.31 to 10.75). Male sex modified the effect of age on the
presence of carotid IPH (β= 0.074, SE=0.036, p=0.0411). Conclusions: Males have greater age-
specific odds of MRI depicted carotid IPH compared to females. With increasing age post-
menopause, the odds of carotid IPH in females becomes closer to that of males. Delayed onset of
carotid IPH in females, an unstable plaque component, may partly explain differential stroke
rates between sexes and further studies are warranted.
2.2 Introduction
Stroke incidence is lower in females compared to males between the ages of 45 to 74 years
(Kissela et al., 2004; Reeves et al., 2008). The difference in stroke incidence, however, is
eliminated after 75 years of age (Kissela et al., 2004; Reeves et al., 2008). The protection from
stroke conferred upon females between the ages of 45 to 74 years may be related to the
protective effects of pre-menopausal sex hormones that delay the onset of atherosclerosis
(Jousilahti, Vartiainen, Tuomilehto, & Puska, 1999; Yahagi, Davis, Arbustini, & Virmani, 2015).
Women have been reported to have less plaque burden and more stenosis compared to men
(Iemolo, Martiniuk, Steinman, & Spence, 2004), suggesting that sex hormones play a role in

73
arterial remodeling. Data on the age-specific sex differences in carotid plaque components and
their natural course is sparse.
Pathology and imaging studies have reported carotid atherosclerosis composition
differences between the sexes (Ota, Reeves, et al., 2010; Ota et al., 2013). One specific plaque
component, intraplaque hemorrhage (IPH), is a biomarker of plaque instabilty associated with
the progression of atherosclerosis (Takaya et al., 2005), a high-risk cardiovascular phenotype
(Noguchi et al., 2011; Singh et al., 2013), and future cerebrovascular outcomes including stroke
(Gupta et al., 2013; Saam et al., 2013; Singh et al., 2009; Singh, Zavodni, & Moody, 2012).
Several recent studies point to IPH as a potential source of thromboembolism among patients
with embolic stroke of undetermined source, which by definition have non-stenotic carotid artery
disease (<50%) (Freilinger et al., 2012; Gupta et al., 2016). Studies are needed understand the
determinants of IPH in low-grade (<50%) carotid stenosis and data on the age-specific sex
differences in carotid plaque components and their natural course is sparse in these patients.
Further, prior studies have demonstrated that male sex and age are associated with the presence
of IPH (Ota, Reeves, et al., 2010; Ota et al., 2013; van den Bouwhuijsen et al., 2012). However,
whether sex modifies the effect of age remains to be investigated.
MRI can identify carotid IPH (Bitar et al., 2008; A. R. Moody et al., 2003; N. Singh et
al., 2015; Yuan & Parker, 2016). Validated carotid IPH pulse sequences such as 3D T1-weighted
gradient echo (GRE) (A. R. Moody, Allder, Lennox, Gladman, & Fentem, 1999; A. R. Moody et
al., 2003; A. R. Moody & Singh, 2016) may be implemented into routine clinical protocols (A.
R. Moody & Singh, 2016). 3D T1-weighted GRE is routinely combined with magnetic resonance
angiography (MRA) at our institution providing an opportunity to study the IPH biomarker in a
large clinical population.
The objective of this study was to report age-specific sex differences in MRI depicted
carotid IPH in an institutional sample comprising ten years of data. Given that age-specific
stroke rates are lower in females between age 45 to 74 compared to males, carotid artery disease
is a major cause of stroke, and females may have greater proportions of stable plaque
components, we hypothesized that age-specific sex differences in carotid IPH exist to help
explain previously reported differences in stroke rates. Specifically, we hypothesized that males

74
have greater age-specific odds of MRI depicted carotid IPH compared to females and that with
increasing age, the odds of carotid IPH in females becomes closer to that of males. We report
age-specific sex differences in the presence of MRI depicted carotid IPH in patients with less
than 50% stenosis.
2.3 Materials and Methods
Institutional ethics board approval was received for this retrospective study and the requirement
for informed consent was waived.
2.3.1 Participants and Study Groups
Patients (n=1115) referred for neurovascular MRI undergoing 3D T1-weighted GRE black-blood
imaging for the presence of carotid IPH between 2005 and 2014 were considered for study
inclusion. Study exclusion criteria included i) carotid artery disease ≥50% stenosis to exclude
patients with higher plaque volumes given that plaque volume and stenosis are positively
correlated(Rozie et al., 2009), and ii) patients with prior carotid endarterectomy since plaque
components may have been altered as a result of iatrogenic causes.
Age groups were defined a priori as < 45 years, 45 to 54 years, 55 to 64 years, 65 to 74
years, and ≥75 years paralleling studies of age-specific sex differences in stroke such as The
Greater Cincinnati/Northern Kentucky Stroke Study (Broderick et al., 1998; Kissela et al., 2004).
Patients undergoing neurovascular MRI including 3D T1 weighted GRE imaging at our
institution in this study included suspected neurovascular disease patients (usually symptomatic)
referred by physicians, including stroke neurologists for neurovascular evaluation.
2.3.2 Carotid MRI Protocols
3D T1-weighted GRE imaging allows for the identification of carotid IPH (Bitar et al., 2008; A.
R. Moody et al., 2003). This acquisition exploits the T1-shortening effects of methemoglobin
resulting in high signal intensity that indicates the presence of carotid IPH (See Figure 2.1 and
Figure 2.2) (Leung & Moody, 2010).
3D T1-weighted GRE imaging was performed on a Philips Medical System Scanner with
a 16 channel neurovascular coil employing a T1-weighted fat-saturated (using a selected water
excitation RF pulse) fast field echo sequence, with imaging acquired in the coronal plane

75
(repetition time (TR), 11 msec; echo time (TE), 4 msec; field of view (FOV), 270x190 mm2;
matrix, 512x256 mm2; slices, 100; through-plane thickness, 0.5mm; voxel size 0.5 mm x 0.7 mm
x 0.5 mm interpolated. Imaging was also performed on a GE 1.5 Tesla MR (Twinspeed) with an
eight-channel neurovascular phased-array coil (USA Instruments, Aurora, Ohio) using a T1-
weighted fat saturated (Special [spectral inversion at lipids]; GE Healthcare) GRE sequence (TR,
6.7 msec; TE, 1.7 msec; flip angle, 15°; field of view, 300 mm2; matrix size, 320 × 320; through-
plane thickness, 2 mm; pixel size, 0.94mm × 0.94mm × 1 mm). 3D T1-weighted GRE imaging is
robust, vendor agnostic, and similar IPH characteristics have been demonstrated at both 3T and
1.5T field strengths (S. McNally et al., 2014).
Figure 2.1: MRI Depicted Carotid Intraplaque Hemorrhage Indicated by Signal
Hyperintensity in the Vessel Wall. Singh et al. Stroke. 2017. 48(8): 2129-2135.

76
2.3.3 Carotid IPH Imaging Analysis and Reliability
Carotid IPH is defined as plaque signal intensity that exceeds the intensity of the adjacent
sternocleidomastoid by 50% (Altaf et al., 2014; Hosseini, Kandiyil, Macsweeney, Altaf, & Auer,
2013; Mendes, Parker, Kim, & Treiman, 2013; Murphy et al., 2003; Singh et al., 2013). Since
patients at our institution underwent imaging with neurovascular rather than surface coils, issues
of coil sensitivity related to magnetic field inhomogeneity were not as relevant as in surface coil
dependent imaging. Experienced neuroradiologists (range of experience, 15 to 40 years) and a
cardiothoracic radiologist with subspecialty and academic expertise in vascular biology imaging
(A.R.M., experience, 27 years), routinely report the presence of IPH on the clinically acquired
3D T1-weighted GRE imaging acquisition. Increased signal intensity was considered to be
carotid IPH if it was in the carotid artery wall. The dichotomous interpretation of carotid IPH has
well established reliability (Ota, Yarnykh, et al., 2010; S. McNally et al., 2014) and kappa
coefficients are 0.75 and 0.9 for inter- and intra-observer reliability (A. R. Moody et al., 2003).
Concordance of clinical reports and an independent rater (N.S.) (n=50) for carotid IPH was
found to have a kappa of 0.902 (95% CI, 0.769 to 1.000, SE 0.068).

77
Figure 2.2: Axial Images of Low-grade Carotid Stenosis and Intraplaque
Hemorrhage. Panel A depicts intraplaque hemorrhage in the 6 o’clock to 12
o’clock positions. Panel B demonstrates corresponding angiographic imaging
depicting low-grade stenosis. Singh et al. Stroke. 2017. 48(8): 2129-2135.

78
2.3.4 Clinical Records Review
Data collection included abstraction of data from neurovascular MRI reports and patients’ charts
using available physician consultation letters. Patients’ electronic and paper charts were
reviewed for cardiovascular risk factors, medication history, and atherosclerotic end-organ
events including history of transient ischemic stroke, stroke, and myocardial infarction.
Traditional cardiovascular risk factors were included since they are independently associated
with cardiovascular outcomes and therefore confound the evaluation of the effect of age and sex
on the presence of carotid IPH.
2.3.5 Source Data Collection, Organization, and Storage
Between 2003 and 2014, charts of a total of 2,102 patients (n=4204 carotid arteries) undergoing
neuro-vascular MRI including carotid imaging with 3D T1 weighted GRE acquisition at our
academic tertiary care center underwent review. Patients undergoing neurovascular MRI
including 3D T1 weighted GRE imaging at our institution were categorized into two subgroups
based on referral source: i) patients with established peripheral vascular disease, typically
referred by vascular surgeons for screening (usually asymptomatic) of the patients’ carotid
arteries as suggested by vascular guidelines (Qureshi et al., 2007), and ii) suspected
neurovascular disease patients (usually symptomatic), referred by physicians including stroke
neurologists for neurovascular evaluation. The imaging database provides unique data on IPH
imaging since the 3D T1 weighted GRE was included as part of routine clinical care at our
academic tertiary care center. The opportunity to ascertain IPH imaging was undertaken in part
due to the relative paucity of information available on carotid IPH, an emerging carotid
biomarker, compared to other biomarkers such as carotid intima-media thickness. For example,
GoogleScholar and PubMed return 116,000 and 9,318 results, respectively, for “carotid intima-
media thickness,” compared to only 7,120 and 371 for “carotid intraplaque hemorrhage” (search
date, July 2016). The sequence necessary for acquisition of this plaque component is not
typically considered a routine clinical sequence since the current standard of carotid imaging for
clinical decision-making is based on the lumen, or carotid stenosis. Therefore, the goal of data
collection for this database was to identify patients with and without the presence of MRI

79
depicted carotid IPH, as well as ascertain available information regarding demographic data,
cardiovascular risk factors, cardiovascular imaging test results, and clinical cardiovascular
outcomes. Such a database would allow for study of carotid IPH associated risk factors and
consequences. Data collection was structured to abstract data from various aspects of the
patients' charts, including neurovascular MRI reports, cardiovascular imaging reports such
including Doppler reports, and clinical medical history from the patients’ charts using available
physicians' consultation letters. Figure 2.3 overviews the components of data collection used in
this 10-year institutional experience of magnetic resonance depicted IPH imaging.
Figure 2.3: Data Collection Overview.
Each patient’s clinical records were searched for information on cardiovascular risk
factors, medical history, medication history, carotid imaging, and atherosclerotic end-organ
events. Charts were abstracted for presence of vascular risk factors, including hypertension,
diabetes, hypocholesterolemia, atrial fibrillation, smoking status, and family history of coronary
artery disease. These traditional cardiovascular risk factors were included since they are well
known to be independently associated with future clinical cardiovascular outcomes and are
Database
Neurovascular Imaging
MRI Report
MRI Consultation Request Form
Radiology Contrast Procedure Form
Cardiovascular Imaging
Echocardiography
Vascular Doppler Report
Chart Information
Medical History
Medication History
Atherosclerotic/ End-Organ Events

80
therefore included in cardiovascular risk-factor studies. Multimorbidity or the concomitant
presence of multiple risk factors is also associated with multiplicative mortality risk (The
Emerging Risk Factors Collaboration, 2015). Relevant vascular medical histories, including past
coronary artery disease, myocardial infarction, coronary interventions (angioplasty, stenting, or
coronary artery bypass graft), stroke, transient ischemic attack, amaurosis fugax, carotid
endarterectomy, carotid dissection, carotid aneurysm, intracerebral hemorrhage, aortic aneurysm,
patent foramen ovale, and fibromuscular dysplasia, were collected. This past medical history is
routinely recorded data in charts indicating a patient’s coronary or cerebrovascular status (e.g.,
prior stroke and myocardial infarction). Features such as patent foramen ovale, atrial fibrillation,
and proximal vessel wall dissections attempted to capture noncarotid artery atherosclerosis
causes of stroke. Intracerebral hemorrhage was collected to allow for differentiation of ischemic
versus nonischemic stroke. Information on causes of stroke as well as well as stroke type
provides a potential avenue to explore the brain and carotid IPH link.
Medication history using a created drug reference allowed for documentation of
medication use. Patients’ medication use for the following categories was recorded:
hypertension (angiotensin converting enzyme inhibitors, angiotensin II receptor blockers,
calcium-channel blockers, beta-blockers, and diuretics), diabetes (insulin, metformin, biguanides,
glitazones, and sulfonylureas), and nitroglycerin. These medications were selected to
comprehensively collect cardiovascular medications. Some of these medications have also been
implicated in the pathophysiology of IPH, although the data have been mostly cross-sectional
and therefore have only suggested associations rather than establishing cause and effect. As more
insights are gained into the pathophysiology of IPH, these medications become important to
consider while evaluating the relationship of carotid IPH and other cardiovascular risk factors
and outcomes. While attempts were made to obtain information that was as granular as possible
at the time of chart review, ultimately, data had to be collapsed as is discussed in the "Data
Cleaning, Validation and Handling of Missing Data" section due to the limitations of this dataset.
Carotid MRI data points from neurovascular imaging reports included stenosis grade or
stenosis grade category and presence of IPH. Stenosis grade and IPH status are routinely
reported for neurovascular MRI at our institution by subspecialty academic radiologists with

81
knowledge and interest in carotid artery imaging. In patients with multiple neurovascular MRI
examinations, the results of three consecutive MRI reports were recorded. Any available
ultrasound and computed tomography angiography (CTA) reports were also abstracted for
stenosis grade category. The presence of carotid ulceration was recorded based on CTA reports,
given that prior studies suggest ulceration to be a high-risk feature associated with the presence
of MR-IPH (U-King-Im et al., 2010). The data variables collected allowed for determination of
stenosis grade progression for patients who had serial imaging, change in IPH status, and time-
to-event or time-to-follow-up information. Time-to-follow-up data were calculated as the
number of days between two serial imaging scans. Table 2.1 summarizes the data variables
collected.
Data were entered directly into spreadsheets. In some cases, electronic case report forms
and paper forms were converted to Excel format and were used to prepare the data for cleaning
and validation steps. Data storage was also achieved using spreadsheets. Patients identified were
kept separately to comply with Research Ethics Board approval, ensure privacy of the patients
included in the database, and follow good research practice guidelines (Breault, 2013). Unique
identifiers were kept for each record in the database. Each record in the database was stored in a
row. Standardized reorganization of data was carried out. Text was coded numerically where
possible with “0” indicating "No" or "Absent" and “1” indicating "Yes" or "Present." Similarly,
ordinal categorical variables were ordered numerically, with larger numbers indicating a higher
rank order. Standardized reorganization for data to numerical form, when possible (e.g.,
conversion of clinical stenosis grade from 0 to 3 representing <50%, 50 to 70%, 70 to 99%, and
100% stenosis), facilitated data analysis. Database collection was achieved with the assistance of
supervised chart abstracters. Training included didactic teaching on the order of several hours per
abstracter and case-by-case review of queries throughout the data abstraction. Queries were
typically resolved on the day made or as close to the day made as possible, and chart abstraction
was periodically reviewed to ensure accuracy of data collection. Patients were randomly selected
for review of their entered data throughout the data collection process.

82
Table 2.1: Summary of Data Variables Collected. Demographic Diabetes, Any
ID Insulin Date of Birth Metformin Sex Biguanide
Vascular Risk Factors Glitazone Hypertension Sulfourea Diabetes Mellitus Cardiovascular Outcomes Dyslipidemia First Clinical Event Subsequent to First MRI Atrial Fibrillation Date of First Clinical Event Subsequent to First MRI Smoker, Any Second Clinical Event Subsequent to First MRI Smoker, Present Date of Second Clinical Event Subsequent to First MRI Family History of Coronary Artery Disease Third Clinical Event Subsequent to First MRI
Relevant Medical History Date of Third Clinical Event Subsequent to First MRI Cardiovascular Fourth Clinical Event Subsequent to First MRI
Myocardial Infarction Date of Fourth Clinical Event Subsequent to First MRI Coronary Artery Disease Death Coronary Artery Bypass Graft Date of Death Coronary Angioplasty or Stenting Imaging
Cerebrovascular First MRI Stroke Date of First MRI Transient Ischemic Attack Presence of Right Carotid IPH Amarosis Fugax Presence of Left Carotid IPH Carotid Endarterectomy Degree of Right Carotid Stenosis Carotid Dissection Degree of Left Carotid Stenosis Carotid Aneurysm Second MRI Intracerebral Hemorrhage Date of Second MRI
Other Vascular Presence of Right Carotid IPH Abdominal Aortic Aneurysm Presence of Left Carotid IPH Patent Foramen Ovale Degree of Right Carotid Stenosis Fibromuscular Dysplasia Degree of Left Carotid Stenosis
Medications CTA Hypertension Date of First CTA
Angiotensin Converting Enzyme Inhibitor Degree of Right Carotid Stenosis Calcium Channel Blocker Degree of Left Carotid Stenosis Beta-blocker Presence of Ulcer Diuretic Doppler Ultrasound Angiotensin II Receptor Blockers Date of Doppler Ultrasound
Statin Degree of Right Carotid Stenosis Antiplatelet Degree of Left Carotid Stenosis Anticoagulant Nitroglycerin

83
2.3.6 Data Cleaning, Handling of Missing Data, and Validation
The collected database underwent cleaning and validation steps to ensure that the data used were
internally consistent or reliable and produced accurate results. The approach to data cleaning
included: i) identifying invalid data, ii) investigating reasons for any invalid data, iii) reviewing
charts to address any invalid data, iv) spot checking random patient charts to ensure accuracy of
data, and v) testing validity, both intra-rater, inter-rater, and clinical report concordance for
carotid IPH status and clinical stenosis grade, the key imaging parameters of interest in this body
of work. Both manual and semi-automated steps were used to address each data cleaning and
validation step.
In the first step, manual inspection of the data was carried out to identify any obvious
issues and ensure the face validity of the database. Irregular or nonsense entries were corrected
or removed. This step included addressing visible issues for each case such as removing text
from a date field or converting text into numbers. Responses for each variable were numerically
standardized, including conversion of text stating a stenosis range to a categorical response.
Dates were formatted to ensure uniformity using an eight-character standardized classification
system. It was ensured that serial imaging was entered in chronological order with the earliest
scans being recorded as the first imaging tests and the latest scan being recorded as the last
imaging tests. No cases or variables had to be dropped from the database based on the face
validity step. During evaluating face validity, it was apparent that several variables had low
response rates, and therefore a strategy employing the exclusion of these variables was used.
Code was written using SAS® (version 9.4) to provide for additional data validation and
cleaning steps of the dataset. Data variables were relabeled to ensure clarity during data cleaning
and analysis steps. Automated checks included searches for outliers (range check), format
(character check), and proper documentation of response categories (category checks).
Specifically, validation for continuous variables included searches for outliers through range
searches and determining the frequency of missing data. Variables with less than 10 data points
were dropped from the database given that meaningful analysis would likely not be possible.
Furthermore, if only less than 10 responses were recorded, it was assumed that the data on the
variable were not regularly abstracted from charts, and these variables were deleted from the

84
database entirely. Otherwise, incomplete data points variables with greater than 10 responses
were identified as missing data points and coded in the database as “.” Ten responses were
selected as an arbitrary cut-off point representing a threshold of 0.5% of the potential available
dataset. The threshold was set at this level to ensure that potential subset analyses on rarer
conditions would be possible. For example, the threshold also allowed us to capture data of
patients with rare conditions such as fibromuscular dysplasia of the neurovasculature, which may
affect as few as 0.3 to 3% of patients (Varennes et al., 2015). While the data were retained in the
database, this did not necessarily translate into inclusion in the data analyses of individual
projects. The data variables would need to be considered on a project by project basis. The
decision to retain information is for potential review of more interesting cases, exploratory
analysis, and case-control type studies.
Records that could not be verified, such as those with missing subject identification
numbers without corresponding hospital file numbers in the link-list file, were discarded from
the database. Furthermore, duplicate entries were screened and reconciled. The detection of
duplicate entries was automated, and reconciliation was manual. In most instances, one of the
duplicate entries identified only had a subject identifier without any clinical data, so the
nonmeaningful record was removed, leaving the meaningful entry in the database. Reconciliation
of the records in which duplicate cases had meaningful clinical data was done via manual review
of the record and consolidation of information into one record. A limited number of cases with
discordant information prompted chart review of those cases. Case-by-case review for face
validity of data and random data checks were undertaken throughout the data collection and
cleaning processes. Table 2.2 provides the database cleaning steps.

85
Table 2.2: Database Cleaning Steps.
____________________________________________
Variables
• Relabeling of data variable names
• Visualization for obvious problems (face validity)
• Correction of date formats
• Conversion of text into numerical responses
• Standardization of numerical responses
• Validation of continuous variables
• Validation of categorical variables
• Handling of variables with insufficient data
• Setting of missing value codes
• Handling of missing data for retained variables
Records:
• Verification of records
• Reconciliation of duplicate data
• Case by case review (face validity)
• Random checks of record
______________________________________________
Various strategies may be used in the statistical handling of missing data in large
databases, including collapsing data. In our case, data were collapsed when necessary to
maximize its usability and minimize missing data at the cost of making it more difficult to
answer more granular questions. To maximize usable data on carotid stenosis, degree of carotid
stenosis was collapsed into four groups, <50%, 50 to 70%, 70 to 99%, and 100% or total
occlusion. Data on medications were also collapsed. For example, charts were reviewed for
specific medications such as type of antihypertensive (beta-blockers, calcium-channel blockers,
angiotensin converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs)). Since
the specific type of antihypertensive was not always available, considering presence or absence
of antihypertensive medication in analyses allowed for retention of more records in the database.
Of the 2,102 patients with 3D T1 GRE imaging between 2005 and 2014, 1,115 comprised
the source database. Patients were removed from the database if they did not have a

86
neurovascular MRI report (n=21), observations were not linkable to the master list and therefore
no corresponding hospital file number was available to verify any data (defined as a
nonverifiable record) (n=93), or their carotids may have been investigated because of known
peripheral vascular disease rather than for suspected neurovascular disease (n=661). The reason
for excluding patients with peripheral vascular disease was to ascertain a more homogenous
group of low-grade stenosis patients with as low as possible a burden of atherosclerosis to allow
for improving internal validity.
2.3.7 Statistical Analysis
Continuous variables with a normal distribution were expressed as a mean and accompanied by a
standard deviation. Comparisons of age between males and females were made using an
unpaired two-sided t-test. Pooled rather than Satterthwaite p-values were reported since equal
variances could be assumed. Categorical variables were reported as counts and percentages, and
were compared between the sexes using a two-sided Chi-squared test. Comparisons of binary
matched data for differences in carotid IPH in the right versus left carotid arteries were made
using a two-sided McNemar’s test.
Logistic regression was used to evaluate the relationship of sex and carotid IPH.
Multivariable logistic regression covariates included hypertension, dyslipidemia, diabetes
mellitus type two, and smoking history. To evaluate age-specific sex differences in carotid IPH,
we included an age-by-sex covariate interaction term in reference and adjusted models.
Statistical analysis was performed using SAS Version 9.4 (SAS Institute, Cary, NC, USA). A p-
value of less than 0.05 indicated a statistically significant difference.
2.4 Results Nine hundred and six patients (mean age ± SD in years, 66.98 +/- 15.15) were eligible for study
(See Figure 2.4).

87
Figure 2.4: Study Flow Chart of Participants. Singh et al.
Stroke. 2017. 48(8): 2129-2135.
Carotid IPH was found in 63 (6.95%) of included patients. Demographic, clinical characteristics
and carotid IPH presence are summarized in Table 2.3. Males had greater proportions of
hypertension, dyslipidemia, type 2 diabetes, and smoking history.

88
Table 2.3: Demographic Characteristics of Study Participants
In males and females, carotid IPH was present in 11.43% (48/420) and 3.09% (15/486),
respectively (p<0.0001). Figure 2.5 depicts the proportion of patients with carotid IPH stratified
by sex and age. No patients had carotid IPH under the age of 45. Between ages 45 to 54 years,
only two males had carotid IPH. Females less than the age of 65 were not found to have carotid
IPH. Table 2.4 includes the proportions of males and females with carotid IPH by age group.
All Patients
(n=906)
Men
(n=420)
Women
(n=486) p-value
Age, mean +/- SD 66.98 +/- 15.15 66.28+/-13.75 65.52+/-16.27 0.4548
MR-IPH, any 63 (6.95) 48 (11.43) 15 (3.09) <0.0001
MR-IPH, Right n (%) 31 (3.42) 23 (5.48) 8 (1.65) 0.0017
MR-IPH, Left, n (%) 43 (4.75) 34 (8.10) 9 (1.85) <0.0001
MR-IPH, Bilateral, n (%) 11 (1.21) 9 (2.14) 2 (0.41) 0.0287
Cardiovascular Risk Factors
Hypertension, n (%) 561 (61.92) 276 (65.71) 285 (58.64) 0.0334
Dyslipidemia, n (%) 497 (54.86) 252 (60.00) 245 (50.41) 0.0040
Diabetes Mellitus 2, n (%) 200 (22.08) 118 (28.10) 82 (16.87) <0.0001
Atrial Fibrillation, n (%) 120 (13.25) 62 (14.76) 58 (11.93) 0.2383
Smoking History (any), n (%) 280 (30.91) 165 (39.29) 115 (23.66) <0.0001
Family History CAD, n (%) 242 (26.71) 108 (25.71) 134 (27.57) 0.5475
Medication History
Antihypertensive, n (%) 452 (49.89) 223 (53.10) 229 (47.12) 0.0832
Statin, n (%) 384 (42.38) 203 (48.33) 181 (37.24) 0.0009
Antiplatelet, n (%) 169 (18.65) 81 (16.67) 88 (20.95) 0.1046
Anticoagulant, n (%) 501 (55.30) 237 (56.43) 264 (54.32) 0.5468
Antidiabetic Agent, n (%) 148 (16.34) 86 (20.48) 62 (12.76) 0.0021

89
Figure 2.5: Age-specific Sex Differences in the Presence of Carotid Intraplaque
Hemorrhage. Singh et al. Stroke. 2017. 48(8): 2129-2135.
Based on logistic regression, compared to women, men were found to have greater odds
of carotid IPH at ages 45 to 54 (OR=52.63, 95% CI 4.27 to 1000), 55 to 64 (OR=25.00, 95% CI
3.88 to 166.67), 65 to 74 (OR=11.90, 95% CI 3.39 to 41.67) and ≥ 75 years (OR=5.56, 95% CI
2.61 to 11.76).
Multivariable logistic regression confirmed that males have greater odds of carotid IPH
than females at ages 45 to 54 (OR=45.45, 95% CI 3.43 to 500), 55 to 64 (OR=21.74, 95% CI
3.21 to 142.86), 65 to 74 (OR=10.42, 95% CI 2.91 to 37.04) and ≥ 75 years (OR=5.00, 95% CI
2.31 to 10.75).
The odds of carotid IPH was greater with age in both males and females, and the effect of
carotid IPH on age was modified by sex in both univariable (β=0.075, SE=0.0352, p=0.0312)
and multivariable (β= 0.0737, SE=0.0361, p=0.0411) logistic regression. The odds of IPH among
females approached that of males with age as shown in the unadjusted and adjusted odds of age-
specific sex differences in carotid IPH reported in Table 2.4.

90
Bilateral carotid IPH was found in nine of 420 (2.14%) males, and two of 486 (0.41%)
females and significantly differed between the sexes (p=0.0287). Males in the older age
categories had higher proportions of bilateral IPH (see Table 2.4).
Of the 52 patients with only unilateral carotid IPH, 32 (61.54%) and 20 (38.46%) patients
had an affected left and right side, respectively (p<0.0001). In these patients with unilateral
disease, the left side was affected in 53.85% (7/13) of females (p=0.0006) and 64.10% (25/39)
males (p<0.0001).
Table 2.4: Age-Specific Differences in Carotid Intraplaque Hemorrhage between Men and Women.
Carotid IPH Presence, % Reference
Model*
Adjusted
Model†
Any Unilateral Only Bilateral Only
Age in
years
Men Women Men Women Men Women OR (95% CI) OR (95% CI)
<45 0.00
(0/30)
0.00
(0/60)
0.00
(0/30)
0.00
(0/60)
0.00
(0/30)
0.00
(0/60)
-- --
45 to 54 3.33
(2/60)
0.00
(0/63)
1.67
(1/60)
0.00
(0/63)
1.67
(1/60)
0.00
(0/63)
52.63 (4.27
to 1000)
45.45 (3.42 to
500)
55 to 64 11.34
(11/97)
0.00
(0/95)
9.28
(9/97)
0.00
(0/95)
2.06
(2/97)
0.00
(0/95)
25.00 (3.88
to 166.67)
21.74 (3.21 to
142.86)
65 to 74 11.11
(12/108)
2.04
(2/98)
9.26
(10/108)
2.04
(2/98)
1.85
(2/108)
0.00
(0/98)
11.90 (3.39
to 41.67)
10.42 (2.91 to
37.04)
≥75 18.40
(23/125)
7.65
(13/170)
15.20
(19/125)
6.47
(11/170)
3.20
(4/125)
1.18
(2/170)
5.56 (2.61 to
11.76)
5.00 (2.31 to
10.75)
* The reference model shows the odds of carotid intraplaque hemorrhage in males versus females, and was
adjusted for sex and a sex-by-age interaction term. † The adjusted model shows the odds of carotid intraplaque hemorrhage in males versus females and was adjusted
by hypertension, dyslipidemia, smoking history, diabetes, sex, and sex-by-age interaction term.

91
2.5 Discussion
2.5.1 Findings The data in this single institution study revealed that in patients with low-grade carotid artery
stenosis, carotid IPH occurs after the age of 45 years, is present in less than 1% of patients before
the age of 55 years, and by the age of 75 years, affects as many as 12% of all patients. Females
were not affected by carotid IPH before the age of 65 years. Moreover, males have greater odds
of carotid IPH compared to females, and with increasing age post-menopause, the odds of carotid
IPH in females also increases and becomes closer to that of males. In other words, sex modifies
the effect of age on carotid IPH. To our knowledge, no other studies have investigated or
demonstrated the convergence of risk of carotid IPH between the sexes with increasing age. The
infrequency of carotid IPH, an unstable plaque component associated with future stroke, in
women before the age of 75 may in part explain the reason that women are relatively protected
from stroke compared to men before the seventh decade of life. Our findings additionally suggest
a delayed onset of carotid IPH in females.
2.5.2 Novelty This study comprising nearly ten years of data, as a result of institutional incorporation of 3D
T1-weighted carotid MRI into routine neurovascular imaging, provided an opportunity to test our
hypothesis that carotid IPH exhibits age-specific sex differences. Thus, an opportunity was
afforded to evaluate the age-specific sex differences in a large group of patients without
significant carotid artery stenosis or higher pre-test probabilities of vessel wall disease. The use
of a large homogenous group of low vessel wall volume disease patients reduces confounding
factors in evaluating the relationship of age and sex that might be associated with higher-grade
disease such as lifestyle differences. Since only a few minutes additional scan time is necessary
to evaluate for IPH within existing neurovascular MRI protocols, it was possible to capture a
relatively large dataset of patients with low-grade carotid stenosis with information on their IPH
status.

92
2.5.3 Other Studies Observational and population studies including MRI of plaque components have found that age
and sex are determinants of carotid IPH (Ota et al., 2013; Kandiyil et al, 2012; Cheung et al.,
2011). Overall, our data found carotid IPH in 11% and 3% of males and females, respectively.
Ota and colleagues found a prevalence of 24% and 6% (Ota et al., 2013). The higher prevalence
of carotid IPH in the latter study may be attributed to Ota using an overall higher-risk group,
low-grade carotid stenosis arteries of patients with contralateral moderate-to-high grade carotid
stenosis. Similarly, Kandiyil investigated patients with moderate and severe carotid stenosis; in
their sample and meta-analysis they found that women with symptomatic carotid stenosis were
less likely to have IPH than men (Kandiyil, Altaf, Hosseini, MacSweeney, & Auer, 2012). In our
study, the carotid IPH status in patients with bilateral low-grade stenosis was captured by
incorporating carotid IPH imaging into routine clinical neurovascular MRI. This is in contrast to
other studies and trials that select patients for vessel wall imaging as a result of their carotid
stenosis (Ota et al., 2013) or intima-media thickness.
In our study, men had 4.1 (95% CI, 2.2 to 7.4) greater odds of carotid IPH compared to
women, which is similar to some reports (Ota et al., 2013). While our confidence intervals
overlap, our point estimate is higher compared to a population-based study reporting that plaques
from males had a 2.2 (95% CI, 1.7 to 2.9) greater odds of IPH compared to females (van den
Bouwhuijsen et al., 2012). One reason for the difference in our study may be that, among the
patients referred for neurovascular MRI and selected for <50% stenosis, rather than known
carotid artery disease, a greater proportion of females may have been referred for MRI for
neurovascular symptoms ultimately unrelated to carotid artery disease.
Men and women also had a slightly greater and statistically significant prevalence of
carotid IPH within the left carotid artery. Ischemic stroke is more often diagnosed in the left
hemisphere (Hedna et al., 2013), and the underlying etiology of this discrepancy is unclear. This
predilection may in theory be due to differences in shear stress resulting from anatomical
differences between the left and right carotid arteries and plaque components. While the
increased diagnosis of stroke in the left hemisphere may be related to the underdiagnoses of right
hemisphere stroke in clinical practice (Paul A. Heidenreich et al., 2011; Portegies et al., 2015),

93
the possibility of differences in plaque components and hemodynamic differences remains to be
rigorously studied. Recently, differences in plaque components have been described and our
findings of sidedness are in line with these (Selwaness, van den Bouwhuijsen, van Onkelen, et
al., 2014). Together, the findings of sidedness and lack of symmetry in carotid IPH between the
carotid arteries suggest that both local and systemic factors play a role in the development of
carotid IPH.
2.5.4 Strengths The strengths of the present study included the power to ascertain age-specific differences in
carotid IPH with MRI using data acquired in the routine clinical setting that allowed us to
capture a large dataset of patients with bilateral low-grade carotid stenosis. The benefit of
extracting our study sample from a clinical setting allows both potential application of any
results to the clinical population of the sample studied (i.e., external validity), as well as the
ability to apply strict inclusion and exclusion criteria to ensure sufficient homogeneity allowing
for greater internal validity. In addition to being rapid, the 3D T1-weighted GRE acquisition used
is scanner agnostic and multi-vendor for the diagnosis of carotid IPH. The acquisition can also be
incorporated into routine clinical protocols (A. R. Moody & Singh, 2016) as demonstrated in the
group within this study. We chose to use this particular pulse sequence since it does not require
surface coils and has been validated using neurovascular coils that are routinely available in the
clinical setting (A. R. Moody et al., 2003). The IPH biomarker is also detectable with other
validated MRI acquisitions.
2.5.5 Limitations This study had several limitations. First, the study was cross-sectional and retrospective rather
than longitudinal and prospective. Serial imaging studies are required to further understand the
natural history of carotid atherosclerosis and provide deeper insights into the natural course of
IPH. Such trials are underway, and their results are anticipated (Tardif et al., 2013). Serial
imaging studies involving advanced imaging are costly, and this study exploited an opportunity
to collect a large set of data in the course of routine clinical practice. While understanding the
incidence of disease would require cohort studies, cross-sectional studies cost-effectively provide

94
information on prevalence of disease. Second, information on age at menopause and menarche,
parity, and use of hormone replacement therapy, were not consistently available from charts. In
developed countries, the average age of natural menopause of 51 years is used as a reference in
cardiovascular studies (Appiah et al., 2016), and we interpreted our data with this knowledge.
Third, while we were able to restrict our analysis to patients with less than 50% stenosis to
exclude patients with higher plaque volumes given the correlation of stenosis with plaque
volume (Rozie et al., 2009), our analyses were not adjusted for degree of stenosis. Finally, we
did not evaluate plaque components such as lipid core, fibrous cap or calcium, and any age-
specific sex differences they may exhibit. Carotid IPH is emerging as a critically important
plaque component in prediction of end-organ events. Time constraints limit routine inclusion of
multi-contrast acquisitions necessary to identify other plaque components in routine clinical
practice, though more recent technological advancements in pulse sequence design may address
this issue in the future.
2.5.6 Future Studies Differences in sex-steroids may explain the observations in this study including the lower odds
of carotid IPH in women per decade of life, the delayed onset of IPH in women, and convergent
risk between men and women with increasing age. Estrogen is known to play a role in the age-
specific sex differences in cardiovascular disease and the 10 to 15 year delayed onset of coronary
disease in women (Jousilahti et al., 1999; Yahagi et al., 2015). Histopathology studies of the
coronaries have demonstrated that post-menopausal women are at an increased risk of plaque
rupture (Burke, Farb, Malcom, & Virmani, 2001). Carotid endarterectomy specimen studies have
shown that plaques obtained from women are less inflammatory with lower macrophage and
interleukin-8 content, and with greater smooth muscle and collagen (Hellings et al., 2007).
Plaque stabilization may be achieved via anti-inflammatory effects of estrogen modulated by its
antioxidant and anti-apoptosis effects (Nofer, 2012). Furthermore, estrogen may confer
protection against atherosclerosis via several mechanisms including the promotion of endothelial
mediated dilation and blood flow, and cerebrovascular reactivity. Nitric oxide synthase and nitric
oxide generation are increased by estrogen and may explain in part the protective role of
estrogen in atherosclerosis (Nofer, 2012). While the effects of estrogen on IPH require further

95
investigation, estrogen’s ability to attenuate the inflammatory processes that have been
implicated in IPH suggest that sex-steroid differences may account for some differences in
carotid IPH presence.
The potential of menopause hormone therapy providing cardiovascular benefits remains
unproven (Bhavnani & Strickler, 2005) although recent investigations demonstrate that timing of
hormone therapy administration is critical to appreciate cardiovascular protection benefits. Post-
menopausal administration of estradiol within six years of menopause onset may reduce
progression of carotid intima-media thickness (Hodis et al., 2016), a marker of atherosclerosis
that is strongly associated with cardiovascular outcomes. The relationship of post-menopause
hormone therapy with plaque components using well-designed trials appears to be an avenue for
future investigation.
Our results suggest that future cohort studies may be warranted to understand the role of
carotid IPH and age-specific stroke rates, as well as further investigate the possibility of delayed
incidence of carotid IPH in women. Prospective longitudinal studies to evaluate carotid IPH
incidence rates in men and women would also clarify the natural history of carotid IPH, and
affirm the role of estrogen in sex differences.
2.6 Conclusions
Males have greater age-specific odds of MRI depicted carotid IPH compared to females, and
with increasing age, the odds of carotid IPH in females becomes closer to that of males.
Differences in the presence of carotid IPH, an unstable plaque component, may partly explain
differential stroke rates between the sexes, and further studies are warranted.

96
Chapter 3—Carotid Magnetic Resonance Imaging Depicted
Intraplaque Hemorrhage in Embolic Stroke of
Undetermined Source
This chapter contains sections or content either adapted or reproduced with permission
from the following peer-reviewed literature.
• Singh N, Moody AR, Panzov V, Gladstone DJ. Carotid Intraplaque Hemorrhage in
Patients with Embolic Stroke of Undetermined Source. J Stroke Cerebrovasc Dis.
2018 Jul; 27(7): 1956-1959.

97
3.1 Overview
Background and Purpose: Many embolic strokes are of undetermined source (ESUS). Carotid
artery intraplaque hemorrhage (IPH), an unstable component of atherosclerosis, may be an
under-recognized etiology in ESUS patients. We investigated the prevalence of carotid IPH
detected non-invasively by magnetic resonance imaging (MRI). Methods: This pilot study
analyzed data from a prospective cohort of patients with a recent ESUS who underwent MRI for
carotid IPH assessment. All patients had carotid artery stenosis <50%. The primary outcome was
the presence of carotid IPH ipsilateral to the cerebral ischemic event. Results: The cohort
comprised 35 consecutive patients with a recent carotid-territory ESUS who underwent carotid
MRI (mean age 74.3 ± 9.6 years). We found ipsilateral and contralateral IPH in 7/35 (20.0%) and
3/35 (8.6%) of patients, respectively (p= 0.005). Conclusions: In this sample of ESUS patients,
one in five had carotid IPH ipsilateral to their acute infarct, as detected by vessel wall MRI.
Further studies are warranted to investigate carotid IPH as an etiology of ESUS.
3.2 Introduction
Embolic stroke of undetermined source (ESUS), a non-lacunar brain infarct without a significant
proximal artery stenosis or high-risk cardioembolic source, accounts for up to 25% of ischemic
strokes (R. G. Hart, Catanese, Perera, Ntaios, & Connolly, 2017; Robert G. Hart et al., 2014).
Large artery atherosclerotic stenosis (≥ 50%) is responsible for ≈25% of ischemic strokes
(Robert G. Hart et al., 2014). Stenosis ≥ 50% has been the traditional criterion for stroke
etiological classification (Adams et al., 1993). However, stenosis alone may underestimate the
role of atherosclerosis due to outward luminal remodeling in early atherosclerosis (Saam et al.,
2016) and provides little information on vulnerable plaque composition.
MRI of the carotid vessel wall allows characterization of plaque components. Intraplaque
hemorrhage (IPH) is a plaque component of particular interest since it is associated with
instability and has been linked with both incident and recurrent stroke (Hosseini et al., 2013;
Saam et al., 2013; Singh et al., 2009). IPH has been reported in lower grades of stenosis (Cheung
et al., 2011; Freilinger et al., 2012; Gupta et al., 2016; Gupta, Gialdini, et al., 2015) and may

98
represent an unrecognized source of thromboembolism in patients with ESUS. We, therefore,
sought to study the presence of IPH among ESUS patients.
3.3 Materials and Methods
In this single-site retrospective study, we analyzed prospectively-collected clinical and imaging
data in a sample of ESUS patients (n=60) who were enrolled in a clinical trial of cardiac rhythm
monitoring conducted between February 1, 2009 and February 1, 2013 (Gladstone et al., 2014).
Institutional ethics board approval was received, and informed consent was obtained.
We restricted the present analysis to a sample of patients presenting with a recent carotid-
territory index cerebral ischemic event who underwent baseline MRI for the detection of carotid
IPH. Carotid MRI for IPH detection was routinely acquired at our institution as part of our
clinical stroke MRI protocol. All participants underwent standard diagnostic workup by a stroke
neurologist with brain imaging (computed tomography (CT) and/or MRI brain), vascular
imaging (magnetic resonance angiography (MRA), computed tomography angiography (CTA),
and/or ultrasound), echocardiography (TTE and/or TEE), baseline 12 lead ECG and at least 24
hours of Holter ECG monitoring that did not reveal significant vessel stenosis, atrial fibrillation,
or other most responsible etiological diagnosis. Exclusion criteria were patients with i)
Oxfordshire classification of "posterior circulation syndrome" or "lacunar syndrome," ii) bilateral
or multi-territory acute ischemia on neuroimaging, iii) any carotid stenosis ≥ 50% by ultrasound,
MRI, or CTA, and iv) atrial fibrillation. The study participant flow chart is overviewed in Figure
3.1.

99
Figure 3.1: Embolic stroke of Undetermined Source Patient Study Flow Chart.
Clinical data were collected prospectively by a trained study coordinator. Carotid IPH
imaging was acquired using a 3D T1-weighted gradient echo (GRE) black-blood pulse sequence
on a 3T Philips Medical System Scanner in conjunction with a 16-channel neurovascular coil.
Neuroradiologists routinely interpret carotid IPH (see Figure 3.2) at our institution. Reliability
and technical pulse sequence parameters have been previously reported (A. R. Moody et al.,
2003; Singh et al., 2013).
The primary outcome was the presence of carotid IPH ipsilateral to the side of
cerebrovascular infarct. Descriptive statistics are reported. Fisher’s Exact test was used to assess
differences in the presence of IPH ipsilateral to events. The analysis was performed using SAS
Version 9.4 (SAS Institute, Cary, NC, USA).

100
Figure 3.2: MRI Depicted Carotid Intraplaque Hemorrhage Ipsilateral to Acute
Cortical Infarct Indicated by Restricted Diffusion.
3.4 Results
Among the ESUS cohort patients analyzed (n=35, mean age ± SD in years, 74.3 ± 9.6), no
significant differences were found in characteristics between patients with and without carotid
IPH (Table 3.1). No significant differences were found in the degree of carotid stenosis between
patients with and without IPH (14.3% vs. 10.7%, p=1.000), and of the four patients with carotid
stenosis in this cohort, one was found in ipsilateral carotid IPH patients.
Among the 35 ESUS patients, seven patients had carotid IPH (20.0%). Of the seven
patients with carotid IPH, three had bilateral vessel wall disease. IPH was more common in the
ipsilateral carotid artery (7/35 patients; 20.0%) than in the contralateral carotid artery (3/35
patients; 8.6%); (p=0.005). Among those with an acute infarct demonstrated by restricted

101
diffusion on DWI-MRI, ipsilateral and contralateral IPH was found in 4/16 patients (25.0%) vs.
3/16 patients (18.8%); (p=0.007). Table 3.1: Characteristics of Study Participants.
Total
(n=35)
Carotid Intraplaque
Hemorrhage (n=7)
No Carotid
Intraplaque
Hemorrhage (n=28)
Age, mean ± SD years 74.3 ± 9.6 73.1 ± 6.4 74.6 ± 10.4
Female, number (%) 19 (54.3) 3 (42.9) 16 (57.1)
Race, number (%)
White 26 (74.3) 4 (57.1) 22 (78.6)
Other 9 (25.6) 3 (42.9) 6 (21.4)
Modified Rankin Scale Score (>2) 1 (2.9) 0 (0.0) 1 (3.6)
Vascular Risk Factors or Comorbidities, number
(%)
Diabetes 10 (28.6) 2 (28.6) 8 (28.6)
Hypertension 26 (74.3) 7 (100.0) 19 (67.9)
Hyperlipidemia 28 (80.0) 6 (85.7) 22 (78.6)
Prior Ischemic Stroke 4 (11.4) 0 (0.0) 4 (14.3)
Myocardial Infarction 7 (20.0) 1 (14.3) 6 (21.4)
Coronary Angioplasty or Stenting 5 (14.3) 1 (14.3) 4 (14.3)
Coronary Bypass Surgery 4 (11.4) 1 (14.3) 3 (10.7)
Cardiac Valvular Surgery 1 (2.9) 0 (0.0) 1 (3.6)
Carotid Endarterectomy 1 (2.9) 0 (0.0) 1 (3.6)
Carotid Stenting 0 (0.0) 0 (0.0) 0 (0.0)
Peripheral Vascular Disease 3 (8.6) 0 (0.0) 3 (10.7)
Patent Foramen Ovale 0 (0.0) 0 (0.0) 0 (0.0)
Congestive Heart Failure 0 (0.0) 0 (0.0) 0 (0.0)
Current Smoker 2 (5.7) 1 (14.3) 1 (3.6)
Remote Smoker 18 (51.4) 2 (28.6) 16 (57.1)
Carotid Stenosis, number (%)
0% 31 (88.6) 6 (85.7) 25 (89.3)
1-49% 4 (11.4) 1 (14.3) 3 (10.7)

102
3.5 Discussion
Among ESUS patients, we found that one in five had carotid IPH identified by vessel wall MRI
ipsilateral to the side of the index stroke event. This observation raises the possibility that
embolism from unstable non-stenotic or mildly-stenotic atherosclerotic plaque may be the culprit
stroke etiology in some patients.
Our study adds to sparse data on IPH as a potential stroke etiology in ESUS (Freilinger et
al., 2012; Gupta et al., 2016; Gupta, Gialdini, et al., 2015). Our findings are consistent with
Gupta et al. and Freilinger et al. who found IPH ipsilateral to stroke in 22% (6/27) and 28%
(9/32) patients using axial 3D TOF-MRA and multi-contrast MRI, respectively. We used 3D T1
GRE fat-suppressed imaging, a highly sensitive and validated imaging method, which when first
described (A. R. Moody et al., 1999) also identified 5/20 patients with acute stroke who had IPH
but no significant stenosis ipsilateral to the side of cerebrovascular infarction. The 3D T1 GRE
fat-suppressed imaging acquisition is quick, with a scan time of 6 minutes, and does not require
contrast administration. Combined with MRA, this provides a sensitive means of assessing
possible causes of stroke arising from the carotid artery including small juxtaluminal IPH which
may otherwise be obscured by high signal within the lumen on TOF-MRA. The use of a standard
neurovascular coil, rather than dedicated carotid coils, make this technique easily translatable
into clinical practice (A. R. Moody et al., 2003; A. R. Moody & Singh, 2016).
We consider our results hypothesis-generating, requiring confirmation in larger
prospective studies. Strokes were defined as cryptogenic as part of a prospective trial by a stroke
neurologist; however, it is conceivable that not all stroke etiologies may have been detected since
not all patients underwent transesophageal echocardiography or prolonged ECG monitoring.
Furthermore, the finding of IPH may be incidental and asymptomatic, rather than etiologically
linked to the index stroke event. Further research should define its prognostic significance. An a
priori decision to use Fisher’s Exact test given the anticipated small sample size. Emboli from
one carotid are unlikely to enter the contralateral circulation allowing an assumption of
independence. In any case, secondary analysis using McNemar’s test, assuming dependence, was
also found to be significant for the presence of IPH ipsilateral to ESUS (p<0.05).

103
In conclusion, among patients with a recent ESUS, we observed one in five had carotid IPH
ipsilateral to the index acute stroke event. Further studies are warranted to investigate carotid
IPH as a potential etiology of ESUS.

104
Chapter 4—Identifying a High-Risk Cardiovascular
Phenotype by Carotid Magnetic Resonance Imaging
Depicted Intraplaque Hemorrhage
This chapter contains sections or content either adapted or reproduced with permission
from the following peer-reviewed literature.
• Singh N, Moody AR, Rochon-Terry, Kiss A, Zavodni AE. Identifying Individuals
with a High Risk Cardiovascular Phenotype Using MR-detected Intraplaque
Hemorrhage in Patients Evaluated for Neurovascular Disease. Int J Cardiovasc
Imaging. 2013; 29: 1477-1483.

105
4.1 Overview
Background and Purpose: Intraplaque hemorrhage (IPH), a component of late-stage
complicated plaque, identified within carotid endarterectomy surgical specimens, has been
recently demonstrated to predict cardiovascular (CV) events. Magnetic resonance imaging (MRI)
is able to depict carotid IPH. We investigated the ability of carotid MR-depicted IPH (MR-IPH)
to identify high-risk CV patients. Materials and Methods: From January 2008 to April 2011,
216 patients (mean age, 67.5 years; range, 31-100) referred for neurovascular MRI at an
academic tertiary care center underwent 3T carotid MRI with adjunct 3D high-spatial-resolution
coronal imaging to detect magnetic resonance (MR)-IPH. Five experienced neuroradiologists
made a binary decision about the presence or absence of MR-IPH. Patients’ charts were
reviewed blindly for demographic and CV outcomes data. Results: Of the patients with and
without MR-IPH, 62.5% (15/24) and 19.8% (38/192) had a composite CV event (defined as a
past myocardial infarction (MI), coronary intervention (i.e., angioplasty, stenting or bypass graft)
and/or peripheral vascular disease), respectively. The odds ratio (OR) of a composite CV event
in the MR-IPH group was 6.75 (bivariable analysis, 95% CI, 2.75-16.6, p< 0.0001) and 3.25
(multivariable regression analysis, 1.14-9.37, p=0.028). MR-IPH had the highest OR of a prior
CV event compared to other variables including age, sex, hypertension and stenosis. The OR of
individual CV events was also significant: MI (3.35, 95% CI 2.11-14.2, p<0.01), coronary
stenting (26.4, 95% CI 8.80-79.4, p<0.01), coronary angioplasty (21, 95% CI 4.84-91.1, p<0.01),
and PVD (3.35, 95% CI 1.09-10.3, P<0.05). Conclusions: MR-IPH is independently associated
with prior CV events in patients who are evaluated for neurovascular disease. Carotid MR-IPH,
employed easily in routine clinical practice, is emerging as an indicator of systemic vascular
disease and may potentially be a useful surrogate marker of CV risk, including in those already
undergoing neurovascular imaging.
4.2 Introduction
Intraplaque hemorrhage (IPH), a component of atherosclerotic plaque, is an emerging marker of
plaque instability (Freilinger et al., 2012; Lindsay et al., 2012b; A. Moody, 2012). Carotid IPH in
endarterectomy surgical specimens has been recently shown to predict an individual’s risk of

106
future cardiovascular (CV) events, defined as a composite endpoint of vascular events and
interventions (5) (Hellings et al., 2010). Similarly, in stable coronary artery disease (CAD)
patients, MR-depicted IPH (MR-IPH) is associated with future CV events (6) (Noguchi,
Yamada, Higashi, Goto, & Naito, 2011). Patients with neurovascular disease are at an increased
risk of CV events, in some reports, even more than patients with established CAD (Steg et al.,
2007). These findings support the evolving understanding that atherosclerosis is a systemic
disease that commonly affects multiple vascular beds.
Patients suspected of neurovascular disease routinely undergo MRI evaluation, and MR-
IPH has been suggested as a marker of future neurovascular ischemic events (Freilinger et al.,
2012; Lindsay et al., 2012b; Singh et al., 2009) (Gupta et al., 2013; Saam et al., 2013). We
therefore hypothesized that patients investigated for neurovascular disease found to have MR-
IPH would have an increased number of prior CV events indicative of a high risk CV phenotype.
Thus, this study aimed to determine the ability of MR-IPH to identify past CV events, defined as
myocardial infarction (MI), coronary intervention (i.e., angioplasty, stenting, or bypass graft),
and/or peripheral vascular disease (PVD), in patients investigated for neurovascular disease.
4.3 Methods
The institutional research ethics review board approved this chart review and waived the
requirement for informed consent because the MR images and data were obtained as part of
routine clinical care.
4.3.1 Participants
Patients referred from four stroke neurologists at our institution for MRI evaluation of
neurovascular disease from January 1, 2008 to April 30, 2011 were eligible for this cross-
sectional study (n=842). Patients being assessed for suspected neurovascular disease routinely
undergo an MR sequence to detect carotid IPH (see Figure 4.1) at our institution.

107
Figure 4.1: Multiplanar Images of Carotid Intraplaque Hemorrhage within the
Wall of the Left Carotid Artery. Multiplanar images (A, coronal; B, axial; c,
sagittal) of carotid intraplaque hemorrhage (arrowheads) within the wall of the
left carotid artery. Intraplaque hemorrhage is detected using a 3D-T1-weighted
fat-suppressed fast field echo sequence by exploiting the T1 shortening effects of
methemoglobin. The technique has been histologically validated. Reproduced
with permission from Singh et al., 2012 (License 4071520167464).
A sample of 216 patients was selected from the total eligible participants (n= 842). The
first 216 charts attained from the Health Records Department at our institution were included.
The study sample size (n=216) was based on the method previously described by Eng (Eng,
2003) and used a statistical power of 0.9 (corresponding to Zpwr = 1.282), conventional
significance criterion of p<0.05 (corresponding to Zcrit = 1.960), and pilot data that suggested
the minimum expected absolute difference in proportion of events in the MR-IPH group to be
20%. None of the 216 subjects was excluded from the study.
A B C

108
4.3.2 MRI Protocol
MRI to detect carotid vessel wall IPH has been validated with similar signal features
demonstrated on 1.5 Tesla and 3.0 Tesla field strengths (Kerwin et al., 2008; Underhill et al.,
2008). Patients were scanned using a 3.0-Tesla Philips Medical Systems Scanner with a 16
elements neurovascular coil (Philips Achieva, SENSE-NV-16). Three-D high-spatial-resolution
to detect MR-IPH was performed using a T1 weighted inversion recovery 3D Fast Field Echo
sequence in the coronal plane (echo time, 4 msec; repetition time, 11 msec; matrix 512x256; flip
angle 15°; field of view, 27x19 cm; number of excitations, 4; slice thickness, 0.5mm). The
imaging time was 8 minutes and 54 seconds. No contrast media was used.
4.3.3 Evaluation of Intraplaque Hemorrhage
MR-IPH was defined as plaque signal intensity that exceeded the intensity of the adjacent
skeletal muscle by 50% (see Figure 4.2) per the previously validated protocol (Bitar et al., 2008;
A. R. Moody et al., 2003). Five experienced neuroradiologists who routinely report MR-IPH
studies at our institution made a binary decision on the presence or absence of IPH. Increased
signal intensity was only considered to be carotid IPH if it was in the carotid artery wall; hyper-
intensities elsewhere were not considered.

109
Figure 4.2: Multiplanar Images Showing Intraplaque Hemorrhage in the Left
Carotid Artery. Multiplanar images (A, coronal; B, axial; C, sagittal) showing
intraplaque hemorrhage (arrowheads) in the left carotid artery. Intraplaque
hemorrhage is considered when high signal intensity is seen in the carotid artery
wall and is greater than 150% compared to the adjacent skeletal muscle.
Reproduced with permission from Singh et al., 2012 (License 4071520167464).
4.3.4 Data Collection and Definition of Outcomes
Patients’ electronic and paper charts were reviewed. The initial stroke neurologists’ consultation
letters were used to collect study subjects’ baseline data and past medical history of vascular
events. MR angiography was used to determine degree of carotid stenosis. A per patient design
was used—patients with one or both arteries with a stenosis greater than 30% were considered to
have a stenosis greater than 30% for the purpose of data analysis. A 30% cut-off was selected to
overestimate the value of stenosis in determining CV events (i.e., provide a conservative measure
of the role of MR-IPH in determining CV events when stenosis is controlled for). MR-IPH status

110
was similarly defined as the presence of MR-IPH in one or both arteries. A composite CV event
was defined as prior MI, and/or CV intervention (stenting, angioplasty, coronary artery bypass
graft), and/or PVD.
4.3.5 Statistical and Data Analysis
Statistical analysis was performed by a biostatistician using SAS Version 9.2 (SAS Institute,
Cary, NC, USA). A p-value of less than 0.05 was considered to indicate a significant difference.
Descriptive statistics were calculated for all variables of interest. Continuous variables were
summarized using means and standard deviations, whereas categorical variables were
summarized using counts and percentages.
Categorical baseline variables were compared using chi-square and Fisher’s exact tests
between patients with and without MR-IPH. Continuous variables were compared using two
sample two-sided t-tests between the groups. Multivariable logistic regression analysis, adjusted
for risk factors significantly different between the MR-IPH groups, was performed to evaluate
whether MR-IPH was an independent risk factor for CV events. Prior to analysis, predictor
variables were assessed for the presence of multicollinearity. A tolerance statistic less than 0.4
was considered to indicate the presence of multicollinearity, and in such cases, only one member
of a correlated set was retained for the multivariable model. Predictor estimates were reported as
odds ratios (OR) and their associated 95% confidence intervals (CI).
4.4 Results
All 216 patients (mean age, 67.5 years ± 14.60 [standard deviation]; range, 31-100) referred for
MRI evaluation of neurovascular disease were included for analysis. Of the 216 patients, 11.1%
(24/216) had MR-IPH in either one or both carotid arteries.
Patients with MR-IPH were 8.1 years older than patients without MR-IPH (mean age,
66.6±14.8 years; range, 53-100 vs. 74.7±11.1; range, 31-91). Compared to patients without MR-
IPH, patients with MR-IPH had a significantly greater proportion of males, history of
hypertension, and smokers (see Table 4.1). MR-IPH patients also had a significantly higher
proportion of current users of statins and antiplatelets. Otherwise, no significant differences were
noted between the groups in demographic variables.

111
Table 4.1: Demographic Characteristics of Participants by the Presence of Magnetic Resonance Depicted
Intraplaque Hemorrhage.
Patients with MR-IPH
(n=24)
Patients without MR-
IPH
(n=192)
P-value
Age, y (mean+/- sd) 74.7±11.1 66.6±14.8 <0.05
Female Sex, number (%) 4 (16.7) 109 (56.8) <0.01
Carotid Stenosis > 30%, number
(%)
18 (75) 40(20.8) <0.01
Patient History, number (%)
Hypertension 21 (87.5) 119 (62.0) <0.05
Diabetes Mellitus 6 (25) 35 (18.2) 0.41
Dyslipidemia 17(70.8) 110 (57.3) 0.20
Atrial Fibrillation 3(12.5) 20 (10.4) 0.73
Smoking 16(66.7) 70(36.5) <0.01
Alcohol 2(8.3) 19(9.9) 0.99
Cardiovascular Family History 5(20.8) 53(27.6) 0.48
Medication, number (%)
Hypertension 17(70.8) 111(57.8) 0.22
Diabetes Mellitus 7(29.2) 27(14.1) 0.07
Statin 19(79.2) 110(57.3) <0.05
Anticoagulant 17 (70.8) 123 (64.1) 0.51
Antiplatelet 11(45.8) 43(22.4) <0.05
MR-IPH indicates magnetic resonance imaging depicted intraplaque hemorrhage. P values for normally
distributed continuous variables are from two sample two-sided t tests (age). P values for categorical
variables are from the X2 test (female sex, carotid stenosis >30%, hypertension, dyslipidemia, smoking,
cardiovascular family history, hypertension medication, diabetes mellitus medication, statin medication,
anticoagulant medication, antiplatelet medication) or Fisher’s Exact Test (diabetes mellitus, atrial fibrillation,
alcohol).
Of the patients with and without MR-IPH, 62.5% (15/24) and 19.8% (38/192) had a
composite CV event, respectively (see Table 4.2). The odds ratio of a composite CV event in the
MR-IPH group was 6.75 (95% CI, 2.75-16.6, p< 0.0001). The odds ratio of each of PVD, MI,
coronary stenting, and coronary angioplasty was also greater in the MR-IPH group.

112
Table 4.2: Cardiovascular Events by the Presence of Magnetic Resonance Depicted Intraplaque Hemorrhage.
Patients
with MR-
IPH
n=24 (%)
Patients
without
MR-IPH
n=192 (%)
P-value Odds
Ratio
Confidence
Interval
Composite Cardiovascular
Outcome
15(62.5) 38(19.8) <0.01 6.75 2.75—16.6
Peripheral Vascular Disease 5(20.8) 14(7.29) <0.05 3.35 1.09—10.3
Myocardial Infarction 9(37.5) 19(9.90) <0.01 5.46 2.11—14.2
Coronary Stenting 12(50.0) 7(3.65) <0.01 26.4 8.80—79.4
Coronary Angioplasty 6(25.0) 3(1.56) <0.01 21.0 4.84—91.1
Coronary Artery Bypass Graft 2(8.33) 13(6.77) 0.68 1.25 0.27—5.92
MR-IPH indicates magnetic resonance imaging depicted intraplaque hemorrhage. All p-values are for categorical
variables from the X2 test.
Bivariable and multivariable regression analysis models utilized demographic variables
that were significantly different in the group with and without MR-IPH and included age, sex,
stenosis greater than 30%, hypertension, and smoking (see Table 4.1). The bivariable analysis of
these variables (i.e., known risk factors) demonstrated that each of the variables was
independently associated with the composite cardiovascular outcome (see Table 4.3). The
multivariable regression analysis demonstrated that MR-IPH, male sex, and hypertension were
most associated with the composite CV event (see Table 3.3). The odds ratio of a composite CV
event in the MR-IPH group using a multivariable regression analysis was 3.26 (1.14-9.37,
p=0.028), making it the most significant risk factor.

113
Table 4.3: Odds Ratios of a Composite Cardiovascular Event.
Bivariable, Odds
Ratio (95% CI)
P-value Multivariable,
Odds Ratio (95%
CI)
P-value
MR-IPH 6.75(2.75—16.6) <0.01 3.26(1.14—9.37) <0.05
Age 1.04 (1.01—1.06) <0.01 -- 0.19
Male Sex 3.03 (1.56, 5.88) <0.01 2.44 (1.19, 5.00) <0.05
Carotid Stenosis >30% 2.50(1.29—4.84) <0.01 -- 0.46
Hypertension 3.41(1.56—7.46) <0.01 2.41(1.02—5.74) <0.05
Smoking 1.35(0.72—2.52) 0.35 -- 0.84
MR-IPH indicates magnetic resonance imaging depicted intraplaque hemorrhage. The adjusted odds ratios
of MR-IPH after adjustment for characteristics that significantly differed between the groups at baseline
are shown. The bivariable odds ratio depicts the independent effect of the variable on composite
cardiovascular outcome; the multivariable odds ratio controls for all variables (MR-IPH, age, sex, stenosis,
hypertension, and smoking) in the model.
4.5 Discussion
This study demonstrates the ability of carotid MR-IPH to identify patients with a high risk CV
phenotype. Patients with MR-IPH have greater odds of having a history of MI, coronary
intervention, and/or PVD (i.e., patients considered to be high CV risk). The study suggests that
carotid intraplaque hemorrhage, a feature of late-stage complicated plaque, may be a surrogate
marker for systemic vascular disease, both CV disease and PVD.
Two imaging studies have shown a similar association in coronary artery disease patients
(Noguchi et al., 2011; X. Zhao, Underhill, & Zhao, 2011), but no studies have investigated this
relationship in patients selected because of their neurovascular disease. Such patients are an ideal
population for MR-IPH screening because the cohort is known to be at risk of CV events (Steg et
al., 2007) and their carotid arteries are routinely investigated in clinical practice with MRI. The
addition of a single sequence to a comprehensive neurovascular examination, adding only 8
minutes and 54 seconds to the scan time to assess for carotid MR-IPH, is both time and cost
efficient. Carotid MR-IPH is also practical to implement into routine clinical practice in the
evaluation of neurovascular patients; our study demonstrates the routine clinical use of MR-IPH
over a four-year period.

114
In this study of suspected neurovascular patients, MR-IPH was associated with prior CV
events, independent of degree of carotid stenosis and other established risk factors including age,
male sex, hypertension, and smoking, using a multivariable regression model. The findings
highlight that MR-IPH may be a better marker of plaque instability because it is associated with
prior CV events even when controlled for known predictors of CV outcomes. Also, the ability to
associate MR-IPH in a carotid artery with cardiac events suggests a common underlying
pathophysiology of systemic atherosclerosis.
Several recent studies have also demonstrated the emerging relationship between carotid
MR-IPH and plaque instability. In addition to the association of MR-IPH with CV outcomes,
carotid MR-IPH has been associated with various neurovascular outcomes. The presence of
carotid IPH has been demonstrated in varying degrees of stenosis (Cheung et al., 2011), and the
presence of complicated atheroma has been recently reported in a symptomatic population with
low-grade stenosis (Yoshida et al., 2012). Low-grade carotid stenosis patients with MR-IPH may
therefore potentially benefit from being considered of a high risk CV phenotype, despite the lack
of significant carotid disease defined by stenosis.
A significant advantage of this study is that the data were obtained in a routine clinical
setting in a population that could benefit from being identified with a high risk CV phenotype.
Using a routinely screened population also resulted in a sufficient study sample size to allow for
multivariable regression model analysis controlling for established CV risk factors. The MR-IPH
technique provides the relevant information by exploiting the generation of endogenous contrast,
thus not requiring the added cost and risks of injected exogenous contrast agents. The use of a 3-
D technique makes acquisition simple, and post-processing can provide vascular cross-sectional
images regardless of the tortuosity of the vessel under examination. Although the development of
MR-IPH techniques to visualize the coronary arteries is in progress, imaging the carotid artery
vascular bed is advantageous since it is a relatively spared cardiorespiratory artifact. Carotid
MR-IPH has good inter-observer and intra-observer reliability, as well as good inter-scan
reliability.
This study has limitations. The prior events for each individual relied on retrospective
chart review. Events were clinically defined using additional diagnostic data such as ECG and

115
blood work. A convenience sample was used. Of the total eligible patients, the first 216 returned
by the Health Records Department at our institution were reviewed. Ideally, a prospective
population outcome study of subsequent patients referred for investigation in this cohort would
allow for a more vigorous assessment of the ability of MR-IPH to identify individuals with a
high risk CV phenotype.
This study has shown the ability to retrospectively phenotype patients being investigated
for possible neurovascular disease using MRI. While the clinical information provided is already
known from the patients’ clinical histories, the study provides proof of the principle that IPH can
act as a systemic vascular phenotypic marker. If confirmed prospectively, the presence of IPH
detected while imaging the carotid vessels, could therefore be used to identify which patients are
at an increased risk of having occult, but significant, CV disease. Detection of MR-IPH would
then provide an opportunity to detect and potentially treat such disease before it becomes
symptomatic, avoiding subsequent morbidity and mortality and their associated societal costs.
The results also raise the possibility of expanding the use of carotid MR-IPH outside of
the realm of investigating neurovascular disease to identify high CV risk groups. The possibility
may therefore exist of screening known high-risk populations by the simple application of one
MRI sequence. To make this cost effective, this would likely need to be combined with simple
and cheap pre-testing, perhaps using blood tests that would allow the identification of smaller
groups of high risk individuals in already known vulnerable populations (e.g., diabetic patients).
MR-IPH may stratify prior CV risk in patients being assessed by MR for neurovascular
disease. The systemic nature of atherosclerosis, the clinical and research need to identify the
vulnerable patient at risk of CV events, and increasing realization of the importance of plaque
characteristics compared to stenosis all make in-vivo carotid MR-IPH a clinically promising
marker for individual CV risk phenotyping.

116
Chapter 5—A Combined 3D Black-Blood and Time-of-
flight Magnetic Resonance Imaging Approach for the
Volumetric Quantification of Carotid Artery Vessel Wall
and Intraplaque Hemorrhage
This chapter contains sections or content either adapted or reproduced with permission
from the following peer-reviewed literature.
• Singh N, Moody AR, Maraj T, Marvasti TB, Afshin M. Quantification of Carotid
Intraplaque Hemorrhage and Vessel Wall by 3T Carotid 3D MRI. American Society
of Neuroradiology, Chicago, IL, USA. 2015. O-453.

117
5.1 Overview
Background and Purpose: Addition of a 3D T1w gradient echo (GRE) black-blood acquisition
to routine 3D time-of-flight (TOF) provides an opportunity to evaluate both vessel wall and
intraplaque hemorrhage volume, an emerging predictive marker of stroke. We investigate inter-,
intra-, and scan-rescan reliability of this 3D carotid artery magnetic resonance imaging (MRI)
approach and assess agreement with 2D T1 MRI. Materials and Methods: Consecutive patients
(n=22) were recruited from a carotid artery clinical trial including 3D T1w GRE black-blood, 3D
TOF, and 2D MRI. Coregistered 3D and 2D axial images were created to assess vessel wall
volume agreement. Inter- and intra-rater reliability of vessel wall and intraplaque hemorrhage
volumes for 3D axial images and vessel wall volume for 2D axial images were additionally
evaluated. Scan-rescan reliability of vessel wall and intraplaque hemorrhage volumes was
evaluated in patients with repeat 3D MRI. Analysis included intra-class correlation coefficients
and Bland and Altman plots. Results: Three-D carotid artery MRI had excellent reliability for
the volumetric quantification of vessel wall (ICCintra=.859, ICCinter=.881, ICCscan-rescan=.928), and
intraplaque hemorrhage (ICCintra=.998, ICCinter=.996, ICCscan-rescan=.949). No significant
difference was found in vessel wall volume on 3D compared to 2D carotid artery MRI (mean
bias, 66 ± 367 mm3, p=0.13), and both methods had excellent absolute agreement (ICC3D-
2D=0.874, 95% CI 0.709 to 0.948, p<0.01). Conclusions: Addition of a 3D T1w GRE black-
blood acquisition to routine 3D TOF is a highly reliable approach for the volumetric
quantification of vessel wall and intraplaque hemorrhage. This approach had excellent agreement
with 2D T1 MRI for quantification of vessel wall volume.
5.2 Introduction
Carotid artery vessel wall (VW) volume is a surrogate marker for atherosclerosis burden used for
cardiovascular risk stratification and allows for evaluation of changes in disease status. Carotid
intraplaque hemorrhage (IPH), a complicated plaque component, is an emerging marker of
stroke (Singh et al., 2009; Singh et al., 2012; Takaya et al., 2006), myocardial infarction
(Hellings et al., 2010; Noguchi et al., 2011; Singh et al., 2013), and progression of
atherosclerosis (Sun et al., 2012; Takaya et al., 2005). Carotid artery VW volume and IPH are

118
emerging quantitative biomarkers under investigation in multicenter carotid atherosclerosis
trials.
Evaluation of carotid VW and IPH typically requires both 2D and 3D MRI acquisitions (T.
Saam et al., 2005; Touze et al., 2007) because 2D carotid artery MRI acquisitions are used to
evaluate VW (Touze et al., 2007; Yuan, Beach, Smith, & Hatsukami, 1998) and 3D gradient
echo sequences are used to evaluate lumen and IPH (Ota, Yarnykh, et al., 2010; J. Wang et al.,
2013). Quantitative evaluation of VW and IPH using only 3D MRI would allow for better image
registration due to improved spatial alignment and positioning of serial acquisitions. Three-D
carotid artery MRI also results in higher spatial resolution and isotropic voxels and may improve
accuracy of quantitative evaluation.
Three-D T1-weighted (T1w) gradient echo (GRE) black-blood (BB) sequences have been
validated for the detection of carotid IPH (Niranjan Balu, Chu, Hatsukami, Yuan, & Yarnykh,
2008; N. Balu et al., 2011; Bitar et al., 2008; Fan et al., 2014; McNally et al., 2012; A. R. Moody
et al., 2003; Ota, Yarnykh, et al., 2010; J. Wang et al., 2013; Zhu, Ferguson, & DeMarco, 2008).
The sequences also allow for visualization of the outer vessel wall. Three-D TOF, routinely
included in clinical neurovascular protocols, delineates the lumen. Together the sequences
therefore provide an opportunity to volumetrically quantify both VW and IPH using only 3D
carotid artery MRI. However, the use of a combined approach is yet to be investigated for the
volumetric quantification of VW and IPH.
We hypothesized that volumetric quantification of VW and IPH is highly reliable on 3D
carotid artery 3T MRI, and quantification of VW has excellent agreement with 2D carotid artery
MRI. Our purpose was to investigate the inter-, intra-, and scan-rescan reliability of 3D carotid
artery 3T MRI, using a 3D T1w GRE BB and TOF acquisition to volumetrically quantify vessel
wall and IPH and assess agreement with 2D T1 MRI for measuring vessel wall volume.
5.3 Methods
Institutional review board approval and written informed consent were obtained for this
prospective HIPAA-compliant study.

119
5.3.1 Study Population
Consecutive participants were recruited from the carotid imaging core site of an ongoing
multicenter carotid 3T MRI trial (Tardif et al., 2013) of patients with nonsurgical carotid disease.
Participants were eligible for this reproducibility study if both 3D (T1w GRE BB and TOF) and
2D carotid imaging was performed at baseline or repeat 3D imaging was performed within the
four months prior to the baseline 3D trial imaging (see Figure 5.1). Patients with 3D and 2D
imaging available at baseline are referred to as group 1. Patients with 3D imaging at the two
time-points are referred to as group 2.
Figure 5.1: Summary of Reliability and Agreement of 3D IPH Imaging Study
Participants.
5.3.2 MRI Protocol
All scans were completed on a 3T MR scanner (Philips Achieva). A dedicated 16-channel
neurovascular coil (16-NV-SENSE) was used to improve spatial resolution. Carotid MRI
acquisition parameters are summarized in Table 5.1. The 3D BB imaging sequence was
performed using a noncardiac gated T1 fat-suppressed (using a selected water excitation RF
pulse) fast field echo sequence, with imaging acquired in the coronal plane (see Figure 5.2)
(repetition time (TR), 11 msec; echo time (TE), 4 msec; field of view (FOV), 270x190 mm2;
matrix, 512x256 mm2; slices, 100; through-plane thickness, 0.5; voxel size 0.5 mm x 0.7 mm x
0.5 mm).

120
Figure 5.2: 3D T1w Gradient Echo Black Blood (GRE BB) Imaging Depicts
Intraplaque Hemorrhage. Intraplaque hemorrhage (arrowheads) is indicated by
high signal intensity in the vessel wall, as shown on the coronal (a) and the
corresponding magnified sagittal-oblique reformat (b). The 3D T1w GRE BB
sequence used allows for coverage of the entire neck and for vessel wall
visualization. The 3D time-of-flight (c) delineates the lumen. © Navneet Singh
and Alan Moody, 2016. All rights reserved.
Shimming was prescribed for a 10 cm region centered over the neck to ensure B0-field
homogeneity around the carotid arteries. The field of view of 3D T1w GRE BB acquisition
provided coverage from the top of the aortic arch to the Circle of Willis. Three-D TOF imaging
was acquired in the axial plane (TR, 26 msec; TE, 3.5 msec; field of view, 190x190 mm2; matrix,
360x232 mm2; slices, 160 slices; through-plane thickness, 0.7 mm; voxel size 0.5 mm x 0.8 mm
x 0.7 mm). Scan times for 3D T1w GRE BB and 3D TOF were 8:54 and 5:59 minutes,
respectively. Two-D imaging was performed acquiring 16 two-mm thick slices centered at the
index carotid bifurcation, resulting in a total of 3.2 cm coverage in the z-axis. Two-D T1
acquisitions were cardiac gated and used a double inversion recovery turbo spin echo fat
suppressed (using spectral presaturation with inversion recovery (SPIR)) technique, with

121
imaging acquired in the axial plane (TR, 833 msec; TE, 833 msec; field of view, 130x130 mm2;
matrix, 256x220 mm2, through-plane thickness, 2mm; pixel size, 0.5 mm x 0.6 mm ). The scan
time for 2D T1 was 5:20 minutes. Table 5.1: Carotid Magnetic Resonance Imaging Acquisition Parameters.
3D T1w GRE BB 3D TOF 2D T1
Plane of Acquisition Coronal Axial Axial
Cardiac Gating Nongated Nongated Gated
Slice thickness, mm 0.5 0.7 2
Number of slices 100 160 16
Matrix (mm2) 512 x 256 360 x 232 256 x 220
Field of view (mm2) 270 x 190 190 x 190 130 x 130
TE (ms) 4 3.5 8.6
TR (ms) 11 26 833
TI (ms) 800 None 600
Flip Angle (°) 15 18 90
TSE Factor - - 10
Scan time (mins) 8:54 5:59 5:20
5.3.3 MRI Post-processing
Reslicing, registration, and segmentation were carried out using VesselMASS (Version 2014,
Medis Medical Imaging SystemsBV, Leiden, the Netherlands) (van 't Klooster, de Koning, et al.,
2012; van 't Klooster, Patterson, et al., 2013; van 't Klooster, Staring, et al., 2013). Post-
processing of each carotid resulted in the creation of 16 two-mm thick slices per acquisition from
the original 3D data. For group 1 patients, using VesselMASS, 3D T1w GRE BB, and 3D TOF
data was registered and resliced to 2-mm thick axial images, corresponding to the 2D T1
acquisition. Figure 5.3 demonstrates the axial T1w GRE BB images created that correspond to
the 2D T1 reference.

122
Figure 5.3: Post-processing of Patients with 3D and 2D Imaging. Corresponding
2D T1 (a) and 3D T1w gradient echo black blood (GRE BB) (b) axial images of
the left carotid artery in a patient with an eccentric atherosclerotic plaque are
shown. Three-D T1w GRE BB imaging highlights presence of intraplaque
hemorrhage. The 3D T1w GRE BB sequence improves differentiation of
intraplaque hemorrhage from other plaque components within the vessel wall.
Three-D T1w GRE BB Imaging is also more sensitive for detection of
intraplaque hemorrhage, allowing for identification of small amounts
(arrowheads). © Navneet Singh and Alan Moody, 2016. All rights reserved.
For group 2 patients, using VesselMASS, 3D T1w GRE BB, and 3D TOF data was
resliced into 16 2-mm thick axial images centered around the carotid bifurcation (since
corresponding 2D T1 reference images were not acquired for these patients) (see Figure 5.1).
5.3.4 Vessel Wall Segmentation
For the 3D MRI acquisitions, the lumen was contoured using an automated MRA segmentation
function after indicating the center of the lumen on the first and last slice on the axial TOF
images. The outer wall of the vessel was contoured on the axial T1w GRE BB images using an
automatic VW segmentation function. For 2D T1 images, the lumen and outer wall were both

123
automatically contoured using the VW segmentation function after indicating the center of the
lumen on the first and last slice. Manual review of contours and registration was made, and
adjustments were made as required to ensure accurate segmentation.
5.3.5 Intraplaque Hemorrhage Segmentation
On the axial T1w GRE BB images, the primary slice distal to the flow divider was identified. A
region of interest (ROI) was identified on the sternocleidomastoid (ROI area, 20 ± 5 mm2) at the
same level as the carotid artery in the direction of frequency encodes (anterior-posterior) to
determine signal intensity. A signal intensity of 1.5 times the ROI was used as a threshold to
identify IPH in the VW. Classifying presence of IPH by detecting signal intensity greater than
1.5 times the intensity of the sternocleidomastoid is accepted to determine the presence of IPH
(Cheung et al., 2011; Hosseini et al., 2013; A. R. Moody et al., 2003; Murphy et al., 2003; Singh
et al., 2009; Singh et al., 2013). A ROI was drawn around the outer VW boundary, and a signal
above the threshold was included within the boundary (see Figure 5.4).
Figure 5.4: Segmentation of Intraplaque Hemorrhage and the Vessel Wall.
Corresponding 2 mm axial images of 2D T1 (a), 3D T1w gradient echo black
blood imaging (b) and 3D time-of-flight (c) with the results of semi-automated
contouring of the carotid vessel wall shown (lumen, red; outer wall, green). The

124
shaded blue region (b) within the vessel wall highlights the intraplaque
hemorrhage greater than 1.5 times the signal intensity of the adjacent
sternocleidomastoid (white). © Navneet Singh and Alan Moody, 2016. All rights
reserved.
5.3.6 MRI Review
Evaluation of 16 axial two-mm images per carotid artery was made by two independent readers
(N.S., T.M.). Carotid VW and IPH volume were measured for each image. Total carotid volumes
of VW and IPH were determined by VesselMASS by summation of the 16 axial slices per
carotid. Images were segmented at least two weeks a part. One rater resegmented all the images
after a further two weeks (N.S.). Each set of 16 comparisons was reviewed in a randomized
order. Raters were blinded to patient information and the results of prior reads.
5.3.7 Statistical Analysis
Descriptive statistics were reported with mean ± SD or median for continuous variables and as
percentages for categorical variables. An independent samples t-test was used to compare
normally distributed means, and the F-test was used to confirm equal variances.
Intra-rater reliability (N.S. 1 vs. N.S. 2), inter-rater reliability (N.S. 1 vs. T.M.), scan-
rescan reliability (N.S. 1 vs. N.S. 1), and agreement (N.S. 3D vs. N.S. 2D) were assessed with
single measure intra-class correlation coefficients (ICCs). Absolute type agreement was reported
for all measures except for outer wall and lumen measurements comparing 3D and 2D methods.
Interpretation of ICC was defined as poor reproducibility (ICC < 0.4), fair to good
reproducibility (0.4 ≤ ICC < 0.75), and excellent reproducibility (≥ 0.75) (Rosner, 2010). Bland
and Altman (B-A) plots were also used to depict measurement reliability of 3D carotid artery
MRI, as well as agreement between 3D and 2D carotid artery MRI. Statistical analysis was
performed using SPSS (SPSS Version 13.0, Chicago, IL, USA) and MedCalc (MedCalc Version
13.0, Ostend, Belgium).
5.4 Results
Demographic characteristics of the included study (n=16) participants (age, 74 ±10.8 years) are
summarized in Table 5.2. Six of the 22 study patients were excluded due to motion artifact (n =

125
4) and improperly acquired 2D imaging (n = 2). Additionally, a single carotid artery from each of
two patients in group 2 was excluded due to noninterpretable quality and a carotid
endarterectomy between scan and re-scan, resulting in 10 carotids (from six patients) available
for comparison in group 2. The majority of patients studied were asymptomatic (93%, 15/16),
male (75%, 12/16), hypertensive (93%, 15/16), dyslipidemic (62.5%, 10/16), and smokers
(66.7%, 11/16). VW volumes of carotid arteries ranged from 746 to 2444 mm3. Mild, moderate,
and severe carotid stenosis in the index carotid artery was present in 18.7%, 75%, and 6.3% of
patients, respectively. Table 5.2: Demographic Characteristics of Study Participants.
Characteristic All (n=16)
Age, y (mean± SD) 74 ± 10.8
Symptomatic, number (%) 1 (6.2)
Degree of Stenosis, number (%)
<50
50 to 79
80-99
3 (18.7)
12 (75)
1 (6.3)
Male Sex, number (%) 12 (75)
Patient History, number (%)
Hypertension 15 (93.7)
Diabetes Mellitus 4 (25)
Dyslipidemia 10 (62.5)
Smoking 11 (66.7)
Family History, Cardiovascular Disease 6 (37.5)
Medication History, number (%)
Hypertension 15 (93.7)
Diabetes Mellitus 3 (18.7)
Statin 12 (75)
Anticoagulant 1 (6.2)
Antiplatelet 3 (18.7)

126
5.4.1 Intra- and Inter-Rater Reliability
Intra- and inter-rater ICCs for the volumetric quantification of the VW and IPH on 3D carotid
artery MRI ranged from .859 to .998 (p<0.01) and are summarized in Table 5.3. Similar ICCs
ranging from .947 to .997 (p<0.01) resulted from evaluation of volumes on 2D carotid artery
MRI.
Figure 5.5 shows B-A plots of intra-rater and inter-rater reliability of the volumetric
quantification of VW and IPH from 3D carotid artery MRI. A mean bias of -7.4 mm3 for volume
of IPH was found among intra-rater measurement (95% CI, -13.2 to -1.60, p= 0.02). Otherwise,
no statistically significant bias was observed for intra- and inter-rater measurements. No
statistically significant Pearson correlations were observed between differences and means.
Figure 5.5: Bland and Altman Plots of the Intra-rater (a) and Inter-rater (b) for
the Volumetric Quantification of Vessel Wall and Intraplaque Hemorrhage with
3D Carotid Artery Magnetic Resonance Imaging Using a Combined 3D T1w
Gradient Echo Black Blood and 3D Time-of-flight Approach.

127
5.4.2 Scan-Rescan Reliability
Scan-rescan reliability (average scan-rescan, 58.2 days, range 7 to 100 days) ICCs for volumes
of lumen, outer wall, VW and IPH on 3D carotid artery MRI ranged from .928 to .994 and are
summarized in Table 5.3. No significant bias was observed for scan-rescan measurements.
Table 5.3: Reliability of 3-Dimensional and 2-Dimensional Carotid 3-Tesla Magnetic Resonance
Imaging for the Volumetric Quantification of Vessel Wall and Intraplaque Hemorrhage.
5.4.3 3D vs. 2D carotid artery MRI
Excellent absolute vessel wall volume agreement was found between 3D and 2D carotid artery
MRI (ICC=0.859, 95% CI, 0. 683 to 0.941). ICCs for the agreement of 3D and 2D carotid artery
MRI for the volumetric quantification of VW are summarized in Table 5.4.
ICC (95% CI)
Intra-Rater Inter-Rater Scan-Repeat Scan
3D Carotid Artery MRI
Lumen .988 (.971 to .996) .957 (.897 to .983) .994 (.978 to .998)
Outer Wall .959 (.899 to .984) .965 (.914 to .986) .972 (.932 to .989)
Vessel Wall .859 (.683 to .941) .881 (.720 to .951) .928 (.827 to .971)
Intraplaque Hemorrhage .998 (.992 to .999) .996 (.989 to .998) .949 (.877 to .979)
2D Carotid Artery MRI
Lumen .991 (.976 to .996) .989 (.973 to .996) --
Outer Wall .997 (.991 to .999) .981 (.952 to .992) --
Vessel Wall .994 (.984 to .998) .947 (.873 to .978) --

128
Table 5.4: Agreement of 3-Dimensional and 2-Dimesional Carotid Artery Magnetic Resonance Imaging for the Volumetric Quantification of Vessel Wall.
aConsistency type agreement bAbsolute type agreement
Figure 5.6 shows B-A plots of 3D versus 2D carotid artery MRI depicting the agreement
of the two acquisitions for the volumetric quantification of VW. A statistically significant mean
bias was observed in 3D versus 2D acquisitions for the volumes of lumen (181±127, p<0.01) and
outer wall (247±164 mm3, p<0.01). The mean bias of vessel wall volume was not found to be
statistically significant between the two methods (66±367 mm3, p=0.13).
3D carotid
artery MRI,
mean ± SD
2D carotid artery
MRI, mean ± SD
Bias, mean
+/SD
P-
value
ICC (95% CI),
3D vs. 2D
carotid artery
MRI
Volume
Lumen, mm3 1234 ± 333 1053 ± 273 181 ± 127 <0.01 .913 (.795 to .965)a
Outer Wall, mm3 2804 ± 576 2557 ± 569 247 ± 164 <0.01 .956 (.899 to .984)a
Vessel Wall, mm3 1569 ± 377 1503 ± 392 66 ± 187 0.13 .882 (.725 to .951)b

129
Figure 5.6: Bland and Altman Plots of 3D and 2D Carotid Artery MRI
Depicting the Agreement for the Volumetric Quantification of Vessel Wall.
5.5 Discussion
Addition of a 3D T1w GRE BB acquisition to routine 3D TOF was found to be highly reliable
for volumetric quantification of VW and IPH, and also demonstrated excellent agreement with
2D T1 MRI for measuring VW volume. The approach allowed for the provision of only 3D
carotid artery MRI to quantify VW, with 3D T1w GRE BB acquisition for outer VW delineation
and 3D TOF for lumen delineation. Use of a 3D T1w GRE BB acquisition allowed for the
simultaneous benefit of reliably identifying and quantifying IPH, an emerging marker of stroke.
Excellent intra-rater, inter-rater, and scan-rescan reliability of 3D carotid artery MRI
volumetric quantification of VW were found. The reliability of VW, lumen, and outer wall
measurements in our study all had ICCs of greater than 0.85 and were similar to multicontrast

130
studies assessing inter- and intra-rater reliability on 1.5T (T. Saam et al., 2005; Touze et al.,
2007) and scan-rescan reliability at 3T (Li et al., 2010).
Volumetric quantification of the VW on 3D carotid artery MRI had excellent absolute
agreement with 2D carotid artery MRI. However, comparison of absolute differences of OW and
lumen revealed that 3D carotid artery MRI consistently overestimated compared to 2D MRI.
Since both OW and lumen were overestimated, the VW volume, which is calculated by
subtracting volumes of lumen from OW, resulted in no VW volume difference and excellent
absolute agreement. The overestimation of both VW and lumen may be due two separate
reasons. First, the absence of cardiac gating on 3D carotid artery MRI resulting from averaging
the systolic and diastolic cardiac phases, compared to 2D acquisition which is gated to end
diastole. An increase in vessel diameter on 3D carotid artery MRI of 1 to 2 pixels (0.5 to 1 mm)
in the absence of cardiac gating has been previously reported (Sarkar, Moody, & Leung, 2009).
Since the gating affects both lumen and OW proportionally, comparisons of VW on 3D carotid
MRI and 2D carotid MRI can be made for VW. The second reason may be due to the difference
in voxel size in the x-y dimensions. The 3D TOF, 3D T1w GRE BB, and 2D T1 sequences have
x-y dimensions of 0.5x0.8, 0.5x0.7 and 0.5x0.6, respectively. We, however, advocate making
comparisons on the same modality whenever possible or mathematically adjusting for any
differences between two methods using calibration with phantoms.
The excellent reliability of IPH measurements in our study is likely due to assessment of
IPH relying only on a single gradient echo sequence and using semi-automated methods for
image processing and analysis. Intra- and inter- observer reliability of IPH measurements have
been reported with ICCs of 0.60 to 0.74 with multicontrast evaluation at 1.5T (T. Saam et al.,
2005; Touze et al., 2007). Use of multicontrast methods requires review of multiple image
weightings (e.g., T1, TOF, T2 and PD) for determination of IPH and thus requires increased
acquisitions and post-processing time. Carotid IPH at 3T is also detected with more sensitivity
on 3D rapid gradient echo sequences, compared to T1-weighted fast-spin echo and 3D TOF
sequences (Ota, Yarnykh, et al., 2010).
The strengths of our study included recruitment of patients with a wide distribution of

131
VW volumes ranging from 746 to 2444 mm3, thus demonstrating the reproducibility of 3D
carotid artery MRI in patients with variable amounts of disease. The use of 3D T1w GRE BB
sequence in the 3D carotid artery MRI method was also advantageous for several reasons. The
simultaneous assessment of VW and IPH on 3D carotid artery MRI was made possible by the
addition of a single sequence to 3D TOF that is routinely included in clinical protocols assessing
carotid disease. Through-plane resolution on the order of 0.5 mm in contrast to 2 mm with 2D
carotid artery MRI can be achieved and may allow for visualization of smaller quantities of IPH
or improved quantification. Three-D T1w GRE BB is also compatible with multiple platforms, is
easy to interpret, and allows for a large field of view. Use of 3D T1w GRE BB and 3D TOF
allows for assessing carotid disease from the aortic arch to the circle of Willis. In contrast, 2D
carotid artery MRI acquisitions are usually limited, due to time of acquisition, to a couple of
centimeters around the bifurcation. Finally, 3D carotid artery MRI allows for creation of
multiplanar 3D reconstructions and improved 3D to 3D registration of studies acquired at
different time points, thereby improving longitudinal study.
Given that the trial patients had nonsurgical carotid disease, the reference standard of
2D carotid artery MRI, rather than histology, was used to evaluate agreement of 3D carotid
artery MRI measurements. However, 2D carotid artery MRI imaging is generally regarded as the
present MRI imaging gold standard. Three-D and 2D carotid artery MRI had excellent
agreement, suggesting that both are useful for measuring changes in VW volume. Unlike
multicontrast 2D imaging (Yuan et al., 2001), 3D T1w BB imaging did not allow for reliable
characterization of the lipid core. Others have, however, suggested that a combination of three
3D carotid artery MRI sequences (time-of-flight (TOF), MP-RAGE, and MERGE) have
sufficient contrast to allow for identification of necrotic core, calcium, and loose matrix (Liu et
al., 2012). The consideration of plaque components other than IPH was beyond the scope of this
study and may warrant further investigation.
5.6 Conclusions
3D carotid artery MRI at 3T, using 3D T1w GRE BB and TOF acquisitions, allows for highly
reliable volumetric quantification of VW and IPH. Current clinical imaging trials on 3D carotid
artery 3T MRI of IPH may reliably quantify VW and IPH, which may allow for detection of

132
disease progression. Trials including volumetric quantification of VW and IPH may also allow
for improved cerebrovascular risk stratification and insight into the role of carotid IPH in
cerebrovascular outcomes. Further studies may also help demonstrate the potential clinical
benefits resulting from improvements in quantitative evaluation, image registration, or speed of
segmentation.

133
Chapter 6—General Discussion
This chapter contains sections or content either adapted or reproduced with permission
from the following peer-reviewed literature.
• Moody AR, Singh N. Incorporating Carotid Plaque Imaging into Routine Clinical
Carotid MRA. Neuroimaging Clin N Am. 2016 Feb; 26(1): 29-44.

134
6.1 Summary This thesis investigated magnetic resonance imaging depicted intraplaque hemorrhage (MR-IPH)
and its risk factors, presence in patients with embolic stroke of undetermined significance, and
relationship with a cardiovascular phenotype. MR-IPH imaging from both a clinical trial and
institutional experience was used throughout the thesis. Data herein support the hypotheses that
carotid MR-IPH is associated with a high-risk cardiovascular phenotype as indicated by its
association with cardiovascular and cerebrovascular risk factors and outcomes.
In this first study (Singh et al., 2017), data from our 10-year institutional experience
demonstrated that males have greater age-specific odds of magnetic resonance imaging (MRI)
depicted carotid IPH compared to females, and that with increasing age, the odds of carotid IPH
in females becomes closer to that of males. Among 906 patients with low-grade carotid stenosis,
males were found to have greater odds of carotid IPH than females at ages 45 to 54 (odds ratio
(OR)=45.45, 95% confidence interval (CI) 3.43 to 500), 55 to 64 (OR=21.74, 95% CI 3.21 to
142.86), 65 to 74 (OR=10.42, 95% CI 2.91 to 37.04), and ≥ 75 years (OR=5.00, 95% CI 2.31 to
10.75), with odds of IPH converging between the sexes with age. In other words, male sex
modified the effect of age on the presence of carotid IPH (β= 0.074, SE=0.036, p=0.0411).
In the second study (Singh, Moody, Panzov, & Gladstone, 2018), an embolic stroke of
undetermined source sample of patients was used from a clinical trial investigating atrial
fibrillation as an etiology. Embolic stroke of undetermined source patients have carotid IPH
ipsilateral to the affected brain in a sample of anterior stroke patients without evidence of atrial
fibrillation investigated in the clinical trial setting. Ipsilateral and contralateral IPH was found in
7/35 (20.0%) and 3/35 (8.6%) of patients, respectively (p= 0.005).
The third study (Singh et al., 2013) found that the odds of a composite cardiovascular
(CV) event in the MR-IPH patients was 6.75 (Bivariable analysis, 95% CI, 2.75 to 16.6, p<
0.0001) and 3.25 (Multivariable regression analysis, 1.14 to 9.37, p=0.028). MR-IPH had the
highest OR of a prior CV event compared to other variables, including age, sex, hypertension,
and stenosis. The OR of individual CV events was also significant: MI (3.35, 95% CI 2.11 to
14.2, p<0.01), coronary stenting (26.4, 95% CI 8.80 to 79.4, p<0.01), coronary angioplasty (21,
95% CI 4.84 to 91.1, p<0.01), and PVD (3.35, 95% CI 1.09 to 10.3, P<0.05).
These studies support the hypothesis that IPH is associated with a high-risk
cardiovascular phenotype, including cardiovascular risk factors such as age and sex and both

135
cerebrovascular and cardiovascular events. The studies raised the question of the significance of
IPH volume adjusted for plaque burden for further investigation of in the potential causal
relationship between IPH and a cardiovascular and cerebrovascular phenotype. Thus, the fourth
study (Singh et al., 2015) developed an approach to quantification and investigated inter-, intra-,
and scan-rescan reliability of this 3D carotid artery MRI approach and assessed agreement with
2D T1 MRI. The addition of a 3D T1w gradient echo black blood (GRE BB) acquisition to
routine 3D TOF was found to be highly reliable for quantification of VW volume and IPH and
also demonstrated excellent agreement with 2D T1 MRI for measuring VW volume. The
quantitative imaging analysis protocol is intended for use in carotid imaging trials, including the
proposed studies in Chapter 7 that seek to further explore the relationship between carotid MR-
IPH and cerebrovascular imaging outcomes.
6.2 Novelty and Strengths
Given that several emerging studies suggest the importance of IPH in plaque progression, future
stroke, and myocardial infarction, we exploited the opportunity to provide further insights into
IPH pathophysiology, determinants, and outcomes using a large institutional experience and data
from a clinical trial. The work in this thesis provides insight into the pathophysiology of IPH,
specifically the effect of age and sex on IPH in low-grade stenosis. To our knowledge, no other
studies have demonstrated the convergence of risk of carotid IPH between the sexes with
increasing age. The work also demonstrates the feasibility of application of IPH imaging in
patients undergoing neurovascular imaging to identify patients of a high-risk cardiovascular
phenotype. Furthermore, in the case of patients with embolic stroke of undetermined source, IPH
imaging is suggested to enhance the diagnosis by identifying culprit lesions as part of the
comprehensive search for possible underlying stroke etiology. Reliable quantification of IPH was
also demonstrated, and in the context of others’ suggestions that IPH has incremental prognostic
value compared to traditional factors alone for risk prediction and net reclassification of
cardiovascular outcomes, the ability to quantify IPH is essential in understanding its role in
clinical outcomes and establishing clinical cut-offs to ensure optimal thresholds in the trial
setting.
Incorporating imaging of IPH into routine clinical practice is feasible. First, the MR pulse
sequence required to apply the IPH imaging technique is readily available on all scanner
platforms; they are rapidly acquired; IPH detection is accurate and interpretation is simple,

136
presently comprising dichotomization into presence or absence of IPH. Furthermore, MR
imaging at present is the only readily available imaging technique for the detection of plaque
hemorrhage, and MR imaging is an already-used technique for investigating carotid artery
disease. Thus, the addition of a single sequence to the standard carotid artery imaging protocol is
simple with little time-cost impact. Additionally, routinely used neurovascular coils are used; no
specialty surface coils are required (Brinjikji et al., 2018). The imaging covers a large field of
view from the arch to circle of Willis. Finally, no contrast administration is necessary, and
therefore, there is no added risk of nephrogenic systemic fibrosis. Patients with chronic kidney
disease are well documented to be at high risk of stroke (Ueda et al., 2011), and silent brain
infarction is present in 37.5% of patients with grade three kidney disease (i.e., 30 to 44.9
ml/min/1.73m2 clearance) (Chou et al., 2011). Therefore, the absence of contrast administration
may be particularly useful when considering that high stroke risk populations such as those with
chronic kidney disease may benefit from risk stratification with carotid artery MRI (Rubin,
Rosas, Chirinos, & Townsend, 2011).
6.3 Limitations
Where possible, clinical trial data was used in this thesis. However, limitations include the use of
retrospective data collection that made it challenging to always access complete records and
obtain granular level data. Resource constraints limited the number of steps that could be taken
to obtain more granular data such as accessing administrative databases, interviews by telephone
or in person, or tapping other networks or administrative databases. While linking with
administrative datasets via Institute of Clinical Evaluative Sciences or with registries available
through networks such as the Canadian Stroke Network were a few options, infrastructure
constraints limited the ability to pursue these avenues over the duration of this thesis.
Nonetheless, the generalizability of this work that reflected data collected in routine
clinical practice is one distinct advantage (Patsopoulos, 2011). The biomarker of interest was
imaged in the routine clinical setting and therefore informs on its use in practice. Additionally,
retrospective databases are relatively time-efficient and inexpensive, allowing for large study
populations (Motheral et al., 2003). To prospectively collect information on 2,000 patients in an
MRI trial would have been cost-prohibitive, and assuming a cost of $1,500/patient, would
require approximately $3M to construct the database used in this thesis. Therefore, this thesis
allows assembly of a large database of patients in an efficient way.

137
6.4 Relationship to Other Work
6.4.1.1 Clinical Application
Addition of IPH imaging to routine carotid artery MRI assessment has the potential to impact
patient management in a number of clinical settings including whether the patient is:
asymptomatic but at high risk of vascular disease; symptomatic and being assessed for risk of
future event; or in the work up prior to carotid artery intervention. Newer application may
include identifying high risk disease requiring modified, intensive, or costly therapy;
identification of patients requiring increased monitoring; entry criteria for therapeutic trials; and
phenotyping of high risk patients who may require more comprehensive vascular investigation
and potentially therapy modification.
6.4.1.2 Primary Prevention
In the absence of organized vascular screening programs, asymptomatic carotid arteries are most
commonly imaged because of high risk atherosclerotic vascular disease in another vascular bed
such as the coronary or peripheral vascular circulation (Brott et al., 2011). Alternatively,
asymptomatic vessels will commonly be imaged in conjunction with a symptomatic contralateral
carotid artery. Despite the silent nature of these carotid vessels, study of asymptomatic cohorts
has repeatedly demonstrated an increased risk of future clinical events irrespective of the degree
of stenosis in those patients with MR demonstrated IPH rather than those without (Altaf,
MacSweeney, Gladman, & Auer, 2007; Singh et al., 2009). The very low rate of events in the
IPH negative groups is probably an even more compelling reason to investigate patients using
MR-IPH imaging. The absence of IPH appears to confer a level of low risk that might be useful
in managing patients, even those with significant carotid artery stenosis, potentially eliminating
the need for invasive interventions (Gupta & Marshall, 2015; Treiman, McNally, Kim, & Parker,
2015). Carotid vessels with no stenosis are also found to contain IPH, suggesting that advanced
vessel wall disease indicated by IPH can occur even when vessel wall thickening is minimal.
Large cohort trials currently underway may provide information on the relevance of finding this
high risk biomarker in otherwise normal people, potentially confirming whether this can act as
an early marker of future events even in the absence of other, more established risk markers.

138
Asymptomatic patients found to have IPH may be candidates for more intensive
management despite the lack of recognized risk factors such as luminal stenosis. Patients
screened for carotid disease because of vascular disease elsewhere are known to have
asymptomatic nonstenotic carotid disease identified with IPH MRI (Cheung et al., 2011).
Because IPH is a stimulus for plaque progression (Takaya et al., 2005) and potentially carotid
stenosis progression (Singh & Moody, 2015), these patients could be identified for more follow
up to better detect the occurrence of significant stenosis (which may then be eligible for surgical
intervention). Prior to the need for surgical intervention, the risk benefit of more intensive
medical therapy can be weighed because these patients are at higher risk of disease progression.
The concept of identifying the high risk patient by identifying high risk lesions could be
further expanded. From the prospective study of clinical outcomes of patients with histologically
proven IPH in their carotid endarterectomy specimens (Hellings et al., 2010) and the
retrospective review of comorbid cardiovascular conditions in patients with and without carotid
IPH (Singh et al., 2013), it appears that the status of the carotid artery, and in particular the
presence or absence of IPH, provides a useful biomarker of the patient’s vascular phenotype. IPH
in the carotid bed therefore seems to be associated with symptomatic vascular disease
peripherally and in the coronary circulation, and it is also able to predict risk of future
cardiovascular events. While it could be argued that medical therapy for one vascular bed (i.e.,
carotid) will have an equally beneficial effect in all vascular beds without the need for further
investigation, a case could be made for the investigation and exclusion of significant, silent
lesions, for instance, in the proximal coronary arteries, once carotid IPH has been detected.
Knowing that IPH represents a marker of increased risk of atherosclerotic progression
and clinical outcomes, the technique could be used to improve the selection of patients for proof
of principle trials of new interventions. Using MRI detected IPH as a predictive classifier to
select those patients at greater risk of events, smaller recruitment numbers will be required,
allowing a more efficient demonstration of effect.
6.4.1.3 Secondary Prevention
Patients with symptoms referable to the carotid artery circulation should always undergo carotid
artery investigation. First, defining the cause of a cerebral event impacts future therapy or
intervention and impacts accurate diagnosis of carotid artery disease because the source of

139
thrombo-emboli excludes other sources such as the heart. However, the current diagnostic
criteria for diagnosing significant carotid artery disease relies on the identification of a 50%
stenosis or more (Adams et al., 1993). Less than this, and the carotid artery is considered
asymptomatic. In reality, degrees of stenosis less than 50% can cause cerebral thrombo-emboli,
although the incidence of events decreases with the level of stenosis. It should be remembered,
however, that the cumulative number of cerebral events in the nonstenotic group is significant.
MR-IPH has been shown to be present even in low-grade (<50%) carotid artery stenosis and
associated with symptoms. While prospective outcome trials of this biomarker in this
"nonstenotic" group are yet to be performed, identification of IPH with MRI in these patients
may be useful in identifying symptom-causing carotid artery disease. However, because there is
not a direct cause and effect relationship between IPH and cerebral symptoms, further study of
the significance of IPH detection in these patients with cerebrovascular symptoms is required.
Commonly, patients are investigated for the causes of stroke, and none, using current
criteria, are found—the diagnosis remaining embolic stroke of undetermined source. While a
direct causal relationship between IPH and stroke cannot be made, one of the first descriptions of
MRI detected IPH (A. R. Moody et al., 1999) was in acute stroke patients, which noted that 5/11
patients with MRI high signal indicative of IPH had carotid stenosis less than 50%. Using MRI
to detect IPH may identify culprit lesions associated with stroke which otherwise would be
classified as cryptogenic. More recently, similar results were shown in DWI proven stroke
patients without significant (>50%) stenosis who demonstrated IPH ipsilateral to the index
cerebral infarct in 6/27 patients (22.2%), but none on the contralateral side (Gupta, Gialdini, et
al., 2015). As in many areas of carotid artery investigation, imaging for IPH has the potential to
add to the knowledge already provided by the current imaging techniques.
Due to the increasing interest in IPH, there are now sufficient studies that allow meta-
analysis of multiple trials concerning the relationship of IPH and cerebrovascular symptoms.
Studies by Hosseini et al. (OR 12.2) (Hosseini et al., 2013), Saam et al. (HR 5.69) (Saam et al.,
2013), and Gupta et al. (HR 4.59) (Gupta et al., 2013) all showed the positive association of
symptoms with IPH.
Treiman et al. (Treiman et al., 2015) projected the probability of stroke occurrence,
assuming an annual rate of symptomatic stroke of 2.2% and 4.0% of silent cerebral infarction in
the setting of a 5.2 hazard ratio for stroke in the presence of IPH. Projections to four years

140
showed the probability of symptomatic stroke with IPH was 18% and of
symptomatic/asymptomatic stroke combined was 43%. This compares with projections of 3%
and 8%, respectively, for IPH negative patients.
6.4.1.4 Progression of Vessel Wall Disease
From the pathobiology of IPH, it can be seen that the pro-inflammatory nature of free
hemoglobin within the plaque will be a stimulus for plaque growth through a mixture of
attempted repair and healing, lipid accumulation, and repeated plaque hemorrhage. Plaque
growth initially may be through positive remodeling with no encroachment upon the lumen, but
eventually, this will be expressed as an increasing degree of luminal stenosis. The positive
remodeling phase measurement of stenosis is therefore a poor means of detecting vessel wall
disease. Detection of vessel wall disease when there is no lumen stenosis, by the addition of
vessel wall imaging, is therefore particularly important.
IPH has been shown in a number of studies to predict progression of vessel wall disease.
More recently, this has been shown to be translated into progression of clinical stenosis as well
(Singh & Moody, 2015). The importance of IPH therefore seems amplified because not only may
it result in plaque destabilization, potential plaque rupture, and end organ ischemia, but it can
also produce a more gradual and persistent effect by driving plaque progression. The latter
eventually reaches a stage in which clinical events become manifest. The persistent presence of
IPH can therefore be thought of as acting as a slow, continual stimulus for plaque growth, likely
leading to further bleeding within the plaque and then punctuated with more sporadic and
unpredictable plaque rupture. The latter is likely dependent on local features of the plaque,
including geometry, hemodynamics, plaque composition, circulating factors, and vascular
function. The presence of IPH during the nonstenotic phase may therefore provide a useful
marker of those lesions more prone to increases in plaque volume and thus eventual increased
risk of future events. This provides a theoretical opportunity to target patients for more intensive
follow-up and medical therapy in an attempt to halt or potentially reverse the vessel wall disease.
These trials however have not yet been undertaken using the presence of IPH as the entry criteria
for treatment.

141
6.4.1.5 Pre-intervention Imaging
The relationship of IPH, as demonstrated by MRI, to periprocedural outcomes for carotid
interventions has been studied. Overall, as might be expected, the presence of IPH confers an
increased risk for the patient undergoing carotid intervention. This is not surprising because the
presence of plaque hemorrhage indicates a more advanced and complex morphology, such that
any manipulation of the carotid artery may result in thrombo-embolic disease. Even prior to
surgery, there is evidence that the resting rate of high intensity signals (HITS) on transcranial
Doppler is increased from carotid arteries containing IPH (Altaf et al., 2011). During
endarterectomy surgery, manipulation of carotid arteries containing IPH also results in more
perioperative HITS (Altaf, Beech, et al., 2007).
Carotid stenting might appear an attractive alternative to avoid the IPH risks associated
with carotid endarterectomy. However, the presence of IPH also increases the risks associated
with carotid artery stenting, resulting in more periprocedural cerebro-ischemic events compared
with endarterectomy (Yoshimura et al., 2011). Because the presence of IPH appears to confer
increased risk during carotid interventions, preprocedural imaging may be useful in
interventional planning and may provide insight into potential risks on a lesion-by-lesion basis.
6.5 Conclusions
Carotid IPH is an emerging biomarker of a high-risk cardiovascular phenotype, including
association with cardiovascular risk factors and determinants, and cerebrovascular and
cardiovascular events. The shift from evaluation of the carotid artery lumen to vessel wall
visualization for IPH may improve cardiovascular and cerebrovascular risk stratification.
Understanding determinants of IPH such as its modulation by sex provides insights into potential
avenues for therapeutic targeting. If observations on IPH and its relationship with various
vascular outcomes are confirmed in prospective and quantitative trials, IPH imaging is certainly
clinically feasible and cost effective, providing an opportunity to alter current patient
management strategies for improved patient health outcomes.

142
Chapter 7—Future Directions
This chapter contains sections or content either adapted or reproduced from an awarded
peer-reviewed grant competition and the following peer-reviewed literature.
• Singh N, Moody AR. RSNA R&E Foundation. # RR1561 Research Resident Grant.
Prospective Multicenter Imaging Clinical Trial: Quantitative Evaluation of 3D Carotid
MR-Depicted Intraplaque Hemorrhage and Its Relationship with Cerebral Small Vessel
Disease, Stroke and Cognitive Impairment.
• Ramirez J, Singh N, Adamo S, Goubran M, Thayalasuthan V, Zhang B, Tardif JC, Black
SE, Moody AR. Carotid Atherosclerosis and Cerebral Small Vessel Disease: Preliminary
Results from the Canadian Atherosclerosis Imaging Network Project 1. Atherosclerosis
Supplements. 2018 (32): 156.

143
7.1 Opportunity for Study
Several experimental opportunities exist for future investigation, including extension of 3D
magnetic resonance imaging (MRI) vessel wall imaging into other vascular beds (Hoshi et al.,
2015; J. Wang et al., 2016), improvement of current methods, evaluation of new or hybrid
imaging methods in contrast to existing methods (Vesey, Dweck, & Fayad, 2016), and
automated image processing to facilitate image processing (DeMarco & Huston, 2014). The
potential for global vascular burden and comprehensive MRI vascular imaging remains to be
investigated, although whole body imaging requires automated image processing methods,
addressing ethical and practical issues regarding incidental findings, and evaluation of cost-
effectiveness. One serial imaging trial in particular specifically addresses 3D intraplaque
hemorrhage (IPH) imaging discussed in this thesis, the Canadian Atherosclerosis Imaging
Network Project 1 (Tardif et al., 2013), and provides an opportunity to better understand the role
of carotid IPH's natural history and imaging outcomes. A baseline study for this project on the
Canadian Atherosclerosis Imaging Network Project 1 is proposed here to evaluate the
relationship between carotid IPH and neuroimaging outcomes.
7.2 Proposal Motivation
Stroke, cerebral small vessel disease (SVD), and cognitive impairment account for major
mortality and morbidity in the developed world (Lloyd-Jones et al., 2009; Mott, Pahigiannis, &
Koroshetz, 2014; Pantoni, 2010). Early identification of patients at risk for these neurovascular
diseases remains a challenge. Carotid artery imaging may provide a window into the
cardiovascular and neurovascular health of patients, creating an opportunity for early
intervention (Carcaillon et al., 2014). Current clinical guidelines use carotid stenosis to calculate
vascular risk such as stroke (Brott et al., 2011). Carotid studies demonstrate the limited use of
luminal stenosis as a biomarker of vascular events (A. R. Moody, Bitar, Leung, & Maggisano,
2006). For example, in the European Carotid Surgery Trial (ECST), 43.8% of the 3,018
participants with symptomatic disease had only low-grade (<30%) stenosis (N.A.S.C.E.T.
Collaborators, 1991; Gorelick, 1999; Rothwell, Gutnikov, & Warlow, 2003). The five-year rate
of any ipsilateral stroke in the North American Symptomatic Carotid Endarterectomy Trial
(NASCET) trial was 22.2% in the low-grade (<50%) stenosis group. Furthermore, eight to 83
endarterectomies indicated based on the criteria of luminal stenosis and symptoms are needed to

144
prevent one stroke. The search for in-vivo imaging of plaque characteristics to improve risk
stratification of patients at risk of atherosclerotic vascular events (i.e., identification of the
vulnerable vascular patient) is of great interest (Finn, Nakano, Narula, Kolodgie, & Virmani,
2010; Naghavi et al., 2003; Singh et al., 2013).
Carotid IPH, a component of complicated atherosclerosis, is an emerging marker of a
high risk neurovascular phenotype (Gupta et al., 2013; Singh et al., 2012). Studies, including
ours, suggest carotid IPH may be associated with plaque instability (Altaf, MacSweeney, et al.,
2007; Cheung et al., 2011; Gao, Chen, Bao, Jiao, & Ling, 2007), plaque progression (Sun et al.,
2012; Takaya et al., 2005), stroke (Beach et al., 1993; Gupta et al., 2013; Selwaness, van den
Bouwhuijsen, van Onkelen, et al., 2014; Singh et al., 2009), white-matter hyperintensities
(WMHIs) (Altaf et al., 2006), and a cardiovascular phenotype (Hellings et al., 2010; Singh et al.,
2013). MRI can reliably, rapidly, and noninvasively detect IPH in routine clinical practice (Bitar
et al., 2008; A. Moody, 2012; A. R. Moody et al., 1999; A. R. Moody et al., 2006; A. R. Moody
et al., 2003; Murphy et al., 2003). Systematic and quantitative evaluation of carotid IPH and
outcomes may facilitate translation of IPH imaging into clinical use to benefit patients (T. Saam
et al., 2005; Sun et al., 2014; Underhill, Hatsukami, Fayad, Fuster, & Yuan, 2010). Trials are
thus underway to prospectively evaluate the relationship of carotid IPH and vascular outcomes
(Tardif et al., 2013; Turc, Oppenheim, Naggara, Eker, Calvet, Lacour, Crozier, Guegan-
Massardier, Henon, Neau, Toussaint, Mas, Meder, & Touze, 2012; Wasserman, Astor, Sharrett,
Swingen, & Catellier, 2010; X. Q. Zhao et al., 2014).
Using one such national clinical trial of serial 3D carotid and brain MR imaging at 3T of
~450 participants (Tardif et al., 2013), the Canadian Atherosclerosis Imaging Network (CAIN),
we propose to investigate the baseline relationship of quantitative carotid IPH and quantitative
neuroimaging features of SVD (Wardlaw et al., 2013), including WMHIs, lacunes, and brain
atrophy. Quantification of both carotid IPH and SVD would utilize our established protocols.
Secondarily, we aim to assess the relationship of i) carotid IPH and clinical cerebrovascular
outcomes and ii) carotid IPH and cognitive impairment.

145
7.3 Carotid Intraplaque Hemorrhage and Neurovascular Imaging
Outcomes
WMHIs are neuroimaging features of SVD that are of particular interest due to their ability to
predict stroke, dementia, and death (Debette & Markus, 2010; Fujikawa, Yamawaki, &
Touhouda, 1993; Vermeer et al., 2003). Population studies such as the Rotterdam study have
associated WMHIs with measures of atherosclerosis (Bots et al., 1993). The exact etiology of
WMHIs remains unclear. The leading school of thought is that they are secondary to the
occlusion of the small arteries supplying the brain.
Carotid artery disease is a well-known source of thromboembolism to the brain and has
been implicated in 20% to 30% of strokes. Studies have, however, failed to establish a
convincing link between carotid artery disease measured by stenosis and WMHIs (Schulz,
Gruter, Briley, & Rothwell, 2013; Streifler et al., 1995). Failure to identify potentially targetable
contributors of WMHIs is a missed opportunity to curb irreversible cerebrovascular outcomes,
including dementia and stroke. The failure to link WMHIs and carotid stenosis is likely due to
current studies being underpowered for the detection of WMHIs (Kwee et al., 2011), use of
insensitive measures to assess WMHIs (e.g., visual scales rather than reliable quantification
techniques) (Schulz et al., 2013), and failure to consider atherosclerotic plaque components in
the vessel wall (Finn & Narula, 2012; Underhill et al., 2010). Furthermore, distinction of WMHI
type, periventricular versus deep, may also be important (Kandiah, Goh, Mak, Marmin, & Ng,
2014).
Plaque instability, increasingly associated with the presence of carotid IPH, may increase
the risk of thromboembolism resulting in downstream small vessel brain infarcts. Carotid IPH
has been retrospectively associated with increased WMHI volume in a cross-sectional study
(Altaf, Morgan, et al., 2008). Two other underpowered exploratory studies are also suggestive of
an association (Altaf et al., 2006; Patterson et al., 2009). The only prospective observational
study that attempted to assess WMHI related to IPH had a follow-up period of one year in 50
patients (Kwee et al., 2011), which is likely underpowered. Systematic prospective study of
quantitative IPH and quantitative WMHIs is lacking. Demonstration of the ability of carotid IPH
to contribute to WMHIs potentially elucidates a novel etiology for WMHIs (i.e., unstable carotid
plaque with IPH).

146
7.4 Carotid IPH, Lacunes, and Brain Atrophy
Lacunes, presumed to be of mostly vascular origin due to small subcortical infarcts of
perforating arteriole region, are another neuroimaging feature of SVD that is of interest
(Wardlaw et al., 2013). Frequently seen in asymptomatic patients on imaging, lacunes are
associated with subsequent risk of stroke, gait impairment, cognitive impairment, and dementia
(Benjamin et al., 2014; Santos et al., 2009; Wardlaw et al., 2013). The relationship between
carotid atherosclerosis and lacunes has been suggested (Brisset et al., 2013; Fanning, Wong, &
Fraser, 2014; Hong et al., 2011). Studies have yet to address whether carotid IPH may play a role
in the development of lacunes (Fanning et al., 2014). Given the presumed etiology of lacunes
being occlusion of perforating arterioles (e.g., subcortical infarcts), unstable carotid plaques are
hypothesized to play a role. CAIN patients have proton density (PD) and T1-weighted
neurovascular MR acquisitions, allowing for quantification of lacune volume (Wardlaw et al.,
2013).
Cerebral atrophy may be an important measure of the effect of vascular disease burden
and possibly a reason for changes in cognition due to vascular lesions. Atrophy has also been
associated with carotid atherosclerosis, although the specific role of carotid IPH remains to be
evaluated (Jochemsen et al., 2014; Muller et al., 2011). Vascular related atrophy may be
preventable, and whether identification of patients at risk of atrophy using their carotid IPH
status may be useful is of interest. CAIN includes neuroimaging, including T1-weighted
acquisitions with good grey-white differentiation at an isotropic resolution <1 mm allowing for
quantitative volumetric assessment of atrophy (Wardlaw et al., 2013).
Other neuroimaging features of SVD, including cerebral microbleeds and perivascular
spaces, are of interest. Their quantitative protocols are under development.
7.5 Carotid IPH and Clinical Cerebrovascular Outcomes
IPH has been shown to be a marker of future neurovascular ischemic events (Altaf,
MacSweeney, et al., 2007; Gao et al., 2007; Gupta et al., 2013; Lindsay et al., 2012; McNally et
al., 2012; Pasterkamp & van der Steen, 2012; Singh et al., 2009; Takaya et al., 2006; Turc,
Oppenheim, Naggara, Eker, Calvet, Lacour, Crozier, Guegan-Massardier, Henon, Neau,
Toussaint, Mas, Meder, Touze, et al., 2012). We previously reported an association between IPH
and neurovascular outcomes in a peripheral vascular disease patient population with

147
asymptomatic carotid disease (Singh et al., 2009). Our findings were in line with those (hazard
ratio, 5.2; p=.005) reported by Takaya et al. for the relationship between IPH and future
ipsilateral cerebrovascular events (Takaya et al., 2006). The relationship is also consistent with
the findings of Altaf et al., who concluded that the presence of carotid MR-IPH predicts the
recurrence of ipsilateral cerebrovascular events in symptomatic patients with high-grade stenosis
(Altaf, MacSweeney, et al., 2007) and moderate stenosis (Altaf, Daniels, et al., 2008). Although
the relationship between carotid IPH and stroke has been reported in various groups (Singh et al.,
2012), results from CAIN may further contribute to the body of evidence for the role of IPH
imaging in clinical practice.
7.6 Carotid IPH and Cognitive Impairment
Carotid stenosis has been associated with decreased scores on the Montreal Cognitive
Assessment (MoCA) and Mini-Mental Status Exam (MMSE) (Buratti et al., 2014; Guo et al.,
2014; Kirkpatrick, Vincent, Guthery, & Prodan, 2014; J. Watanabe et al., 2014). Improved
scores have been reported subsequent to endarterectomy, suggesting that carotids may be
associated with altered cognition (J. Watanabe et al., 2014). Whether the presence of carotid IPH
is associated with decreased scores remains to be studied. Curbing cognitive impairment by
targeting high risk vascular patients phenotyped via their carotids remains to be evaluated.
7.6.1 Novelty of the Proposed Study
Using a national clinical trial of serial 3D carotid and brain MR imaging at 3T of ~450
participants (Tardif et al., 2013), we propose to investigate the relationship of quantitative carotid
IPH and quantitative neuroimaging features of SVD. Prior studies that have evaluated the
relationship of carotid IPH and SVD have only considered WMHIs. The WMHI studies are
limited because they are generally conducted using low resolution imaging, retrospective
designs, small sample sizes, varying imaging techniques that are less clinically useful (i.e., have
longer scan times), or are restricted to small groups of specific patient types. The single
prospective IPH and WMHI study is underpowered. Potential carotid IPH outcomes, including
lacunes, cerebral atrophy, and cognitive impairment measures, remain to be studied. In our study,
quantification of both carotid IPH and SVD will utilize our established protocols. We also
propose to study the relationship between carotid IPH and SVD features prospectively, with a
high power (β ≥ 0.9), and using reliable quantitative methods, including a histologically

148
validated 3D MRI technique to quantify IPH (Bitar et al., 2008). The use of the 3D MRI
technique improves the accuracy of quantification due to its ability to image isotropic voxels.
The technique is easily implementable from a technical perspective (e.g., use of MRI protocols,
ease of radiologist interpretation), and we have published prior studies from data collected in
routine clinical practice (Cheung et al., 2011; Singh et al., 2009; Singh et al., 2013).
7.6.2 Clinical Implications
Improved risk stratification of carotid atherosclerosis patients may provide an opportunity for
early intervention, decreased mortality, and societal cost-benefits (Finn et al., 2010; Finn &
Narula, 2012; Fleg et al., 2012; Hatsukami & Yuan, 2010; Naghavi et al., 2003; Virmani,
Kolodgie, Burke, et al., 2005). Understanding the role of carotid IPH as an etiology of WMHIs
and other SVD correlates may be one avenue to target patients. Questions remain about whether
patients with carotid IPH may benefit from clinical surveillance or altered clinical management,
including the treatment of their unstable atheroma. Large scale trials are emerging, and CAIN
provides an opportunity to contribute to the growing literature on carotid IPH by uniquely
reporting neuroimaging outcomes in a prospective setting with a large number of patients for an
MRI trial. While further trials may be required, the proposed study aims to facilitate the
translation of IPH imaging into clinical practice.
7.6.3 Preliminary Studies
Several studies conducted in our carotid imaging laboratory form the basis for the current
proposed study (Bitar et al., 2008; Cheung et al., 2011; A. Moody, 2012; A. R. Moody et al.,
1999; A. R. Moody et al., 2006; A. R. Moody et al., 2003; Murphy et al., 2003; J. Ramirez et al.,
2018; Sarkar et al., 2009; Singh et al., 2009; Singh et al., 2013; Singh et al., 2012; Tardif et al.,
2013). With regard to the quantitative evaluation of the 3D carotid 3T MRI, we reported that 3D
carotid artery 3TMRI is highly reliable for the volumetric quantitative evaluation of IPH
(ICCintra=.998, ICCinter=.996, ICCscan-rescan=.949) (N. Singh et al., 2015). Reproducibility of
quantification of neuroimaging features of SVD, specifically WMHIs, lacunes, and brain
atrophy, have also been established by our collaborating group (Dade et al., 2004; McNeely et
al., 2015; J. Ramirez et al., 2015; J. Ramirez et al., 2011; J. Ramirez, McNeely, Scott, Stuss, &
Black, 2014; J. Ramirez, Scott, & Black, 2013; J. Ramirez, Scott, et al., 2014). While cerebral

149
microbleeds and perivascular spaces are also neuroimaging features of interest indicating SVD,
their protocols are in development and are excluded from this proposal.
7.7 Research Design and Methods
7.7.1 Overview and Study Design
The proposed study uses baseline data from a multicenter study of participants undergoing serial
imaging over two years as part of CAIN (Tardif et al., 2013). Patients undergo imaging and
clinical visits at baseline, one year, and two years. Baseline clinical evaluation includes clinical
assessment, including a comprehensive history and physical exam, a battery of neurocognitive
tests, detailed cardiovascular and cerebrovascular history, medication history, and basic blood
work. Baseline imaging evaluation includes MRI of the carotids and brain, including MRI pulse
sequences that allow for the assessment and quantification of IPH, and neuroimaging features of
SVD, including WMHIs.
7.7.2 Population
Patients are recruited from eight academic tertiary care centers across Canada between March
2010 and March 2015. Study patients are those with nonsurgical carotid disease indicated by
stenosis in at least one carotid between 30% to 95%. The primary analysis group will be those
with no carotid intervention prior to or during the course of the study. Patients with >70%
stenosis in either carotid artery or carotid intervention during the follow up will be treated as a
separate group in the analyses for the proposed study. Patients with >70% stenosis are indicated
for carotid endarterectomy based on NASCET ( N.A.S.C.E.T. Collaborators, 1991) and ESCT
(Rothwell et al., 2003) are more likely to undergo carotid intervention and are therefore
considered a separate group to minimize selection biases. Exclusion criteria include i)
contraindication for MRI including a GFR<30ml/min that may increase risk of contrast-related
nephrogenic cystic fibrosis (Daftari Besheli, Aran, Shaqdan, Kay, & Abujudeh, 2014) or ii)
patients with non-MRI compatible implants or hardware (Shellock & Spinazzi, 2008).
7.7.3 Image Acquisitions
Three-D carotid MRI acquisitions include 3D MR-IPH and 3D TOF imaging. Three-D MR-IPH
is performed using a noncardiac gated T1-weighted fat-suppressed (using a selected water
excitation RF pulse) fast field echo sequence, with imaging acquired in the coronal plane

150
(repetition time (TR), 11 msec; echo time (TE), 4 msec; field of view (FOV), 270x190 mm2;
matrix, 512x256 mm2; slices, 100; through-plane thickness, 0.5; and voxel size 0.5 mm x 0.7 mm
x 0.5 mm). Shimming is prescribed for a 10 cm region centered over the neck to ensure B0-field
homogeneity around the carotid arteries. The field of view of 3D MRIPH provides coverage
from the top of the aortic arch to the Circle of Willis. Three-D TOF imaging was acquired in the
axial plane (TR, 26 msec; TE, 3.5 msec; field of view, 190x190 mm2; matrix, 360x232 mm2;
slices, 160 slices; through-plane thickness, 0.7 mm; and voxel size 0.5 mm x 0.8 mm x 0.7 mm).
Scan times for 3D MRIPH and 3D TOF are 8:54 and 5:59 minutes, respectively. Neuroimaging
acquisitions conform with the National Institute of Neurological Disorders and Stroke vascular
cognitive impairment guidelines, and include 3D T1, proton density, FLAIR, T2, and DWI to
allow quantitative tissue compartment classification for volumes of SVD.
7.7.4 Image Analysis: Quantification of IPH and Neuroimaging Features of
SVD
IPH is quantified using semi-automated segmentation methods using imaging processing
software (VesselMass software, Leiden) (van 't Klooster, de Koning, et al., 2012; van 't Klooster,
Naggara, et al., 2012; van 't Klooster, Patterson, et al., 2013; van 't Klooster, Staring, et al., 2013;
van 't Klooster et al., 2014). The intra-class correlation coefficients (ICC) for intra-rater
reliability, inter-rater reliability, and scan-rescan reliability has been demonstrated to be excellent
for the quantification of IPH volume (N. Singh et al., 2015). The details of the re-slicing,
registration, and segmentation are also found in our recent work. For IPH quantification, on the
axial MRIPH images, the primary slice distal to the flow divider is identified. A region of
interest (ROI) was identified on the sternocleidomastoid (ROI area, 20 ± 5 mm2) at the same
level as the carotid artery in the direction of frequency encodes (anterior-posterior) to determine
signal intensity. A signal intensity of 1.5 times the ROI is used as a threshold to identify IPH in
the vessel wall. Classifying presence of IPH by detecting signal intensity greater than 1.5x
intensity of the sternocleidomastoid is accepted to determine the presence of IPH (Altaf, Morgan,
et al., 2008; Hosseini et al., 2013; Singh et al., 2009; Singh et al., 2013). A ROI is drawn around
the outer VW boundary, and a signal above the threshold is included within the boundary. The
reviewer is blinded to clinical status and the volume of WMHI disease.
WMHI will be quantified by a second and independent neuroimaging processing
laboratory with an established protocol for WMHI analysis. The imaging laboratory uses

151
experienced and trained imaging analysts, as well as semi-automated registration, segmentation,
and quantification techniques using Lesion-explorer software (McNeely et al., 2015; J. Ramirez
et al., 2015; J. Ramirez et al., 2011; J. Ramirez, McNeely, et al., 2014; J. Ramirez et al., 2013; J.
Ramirez, Scott, et al., 2014). Lesion explorer exploits proton density MRI, as opposed to fluid-
attenuated inversion recovery (FLAIR) MRI, to prevent underestimation of WMHIs. Regional
quantification of disease provides information, including by hemisphere. Therefore, WMHI
volume ipsilateral to each carotid artery can be used as an outcome. Secondary analyses may
consider the type of WMHI (e.g., deep or periventricular) because others have suggested separate
etiological mechanisms (Kandiah et al., 2014). The protocol has been used in other studies and
has demonstrated reproducibility. The neuroimaging laboratory and analysts are blinded to
carotid artery disease status and clinical patient status.
7.7.5 Statistical Analysis
Statistical analysis will be performed by the author of this thesis and by an independent
biostatistician using statistical software (e.g., SAS Version 9.2, SAS Institute, Cary, NC, USA).
A p-value of less than 0.05 will indicate a significant difference. Descriptive statistics will be
calculated for all variables of interest. Continuous variables with normal distributions will be
reported with mean and standard deviations. Nonnormal distributions will have median and
inter-quartile range reported. Categorical variables will be reported as proportions. Normality
will be assessed by the Shapiro-Wilk test. Patients with and without carotid IPH will be
compared on categorical baseline variables using chi-square and continuous baseline variables
using two sample two-sided t-tests (or Wilcoxin Rank Sum test in the event of nonnormal
outcomes). Multivariable regression analyses, adjusted for risk factors significantly different
between the IPH groups, will be performed to evaluate whether IPH is an independent risk factor
or predictor of outcomes of interest (e.g., SVD, cerebrovascular outcomes, cognitive
impairment).
With regard to the primary aim, we propose to model carotid IPH volume’s relationship
with ipsilateral WMHI volume with a linear regression model: E(Y)=B0 + B1I(L=1) + B2(X). In
the model, WMHI volume is indicated by Y, IPH volume is indicated by X, and L indicates
carotid side. The model will be adjusted for confounders, including age, sex, hypertension,
carotid stenosis, and presence of symptoms at baseline. Collinearity will be tested using variance
inflation factor analysis, and collinear covariates will be excluded from the model. The model

152
will be tested using standard methods, including tests for parallelism and appropriateness of the
assumption of linearity by comparison with analysis of response profiles.
7.7.6 Strengths and Limitations
Methodological strengths of this proposal include the prospective multicenter trial design, high
power to investigate the relationship between IPH and SVD (and secondary outcomes), and use
of semi-automated quantification methods that have been demonstrated to be reliable.
Methodological limitations include loss of a small number of patients due to inability to
complete baseline MRI or analyze their acquisitions with a failure rate of <5 to 7%.
7.8 Future of Cardiovascular Imaging
Noninvasive cardiovascular imaging technology and applications are rapidly emerging. The last
two decades have “witnessed an explosive expansion in the armamentarium of
noninvasive…imaging technologies capable of providing detailed information about the
structure and function of the heart and vasculature” (Di Carli, Geva, & Davidoff, 2016).
Noninvasive cardiovascular imaging provides an avenue to phenotype patients in the clinical and
research settings for identifying patients with vessel wall atherosclerosis, quantifying its burden,
and examining involvement of various end organs. From a biomedical research perspective,
insights might be gained into the pathophysiology of disease. As discussed, various authors have
studied IPH using MRI and have provided insights, including risk factors for IPH, potentially
allowing for targeted and personalized intervention. Understanding the role of IPH in end-organ
outcomes provides impetus to pursue development of therapies targeting IPH.
Advancing technologies result in the sequelae of clinical utilization and increasing costs
to the health-care system. This necessitates responsible use of advanced cardiovascular imaging
techniques. The future of cardiovascular imaging then involves not only development of imaging
technologies and using them to gain insights into the pathophysiology of disease processes, but
also ensuring that they are truly patient-oriented and effective in the clinical setting. What then
makes noninvasive cardiovascular imaging patient-oriented and effective? In the early 1990s,
Fryback and Thornbury described the hierarchal levels of evidence of diagnostic tests: i)
technical quality—is the test reliable, valid, and accessible?; ii) diagnostic accuracy—is it better
than an alternative or has a better cost-benefit ratio?; iii) impact—does it impact clinical
decision-making, and how does it compare to other tests with regard to impact on clinical

153
decision-making?; iv) therapeutic impact—does it improve selection of patients who may benefit
from a given therapy?; and v) patient and societal outcomes—does the test improve outcomes
cost-effectively? In addition to discussing the role of carotid MRI for studying pathophysiology
of disease, this thesis discussed many of these patient-oriented aspects of carotid MRI and MR-
IPH imaging effectiveness, and the balance of evidence seems to point to carotid MR-IPH being
a patient-oriented and cost-effective test.
Finally, the responsible use and logistics of noninvasive cardiovascular technologies will
surely require interdisciplinary collaboration while attempting to maximally improve patient
outcomes. Medical imaging specialists in particular may play a role in identifying the best tests
to answer clinical questions, ensure validity of techniques being used, develop quantitative
protocols, and extract information on the pathophysiology of disease processes. Imaging
specialists are also well positioned to maximize research efficiencies and make the most of
imaging through the development of quantitative translational research programs that might
serve a dual clinical and research purpose.

154
Chapter 8—References

155
Adams, H. P., Jr., Bendixen, B. H., Kappelle, L. J., Biller, J., Love, B. B., Gordon, D. L., &
Marsh, E. E., 3rd. (1993). Classification of subtype of acute ischemic stroke. Definitions
for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke
Treatment. Stroke, 24(1), 35-41.
Albers, G. W., Easton, J. D., Sacco, R. L., & Teal, P. (1998). Antithrombotic and thrombolytic
therapy for ischemic stroke. Chest, 114(5 Suppl), 683s-698s.
Altaf, N., Beech, A., Goode, S. D., Gladman, J. R., Moody, A. R., Auer, D. P., & MacSweeney,
S. T. (2007). Carotid intraplaque hemorrhage detected by magnetic resonance imaging
predicts embolization during carotid endarterectomy. J Vasc Surg, 46(1), 31-36.
Altaf, N., Daniels, L., Morgan, P. S., Auer, D., MacSweeney, S. T., Moody, A. R., & Gladman,
J. R. (2008). Detection of intraplaque hemorrhage by magnetic resonance imaging in
symptomatic patients with mild to moderate carotid stenosis predicts recurrent
neurological events. J Vasc Surg, 47(2), 337-342.
Altaf, N., Daniels, L., Morgan, P. S., Lowe, J., Gladman, J., MacSweeney, S. T., . . . Auer, D. P.
(2006). Cerebral white matter hyperintense lesions are associated with unstable carotid
plaques. Eur J Vasc Endovasc Surg, 31(1), 8-13.
Altaf, N., Goode, S. D., Beech, A., Gladman, J. R., Morgan, P. S., MacSweeney, S. T., & Auer,
D. P. (2011). Plaque hemorrhage is a marker of thromboembolic activity in patients with
symptomatic carotid disease. Radiology, 258(2), 538-545.
Altaf, N., Kandiyil, N., Hosseini, A., Mehta, R., MacSweeney, S., & Auer, D. (2014). Risk
factors associated with cerebrovascular recurrence in symptomatic carotid disease: a
comparative study of carotid plaque morphology, microemboli assessment and the
European carotid surgery trial risk model. J Am Heart Assoc, 3(3), e000173.
Altaf, N., MacSweeney, S. T., Gladman, J., & Auer, D. P. (2007). Carotid intraplaque
hemorrhage predicts recurrent symptoms in patients with high-grade carotid stenosis.
Stroke, 38(5), 1633-1635.

156
Altaf, N., Morgan, P. S., Moody, A., MacSweeney, S. T., Gladman, J. R., & Auer, D. P. (2008).
Brain white matter hyperintensities are associated with carotid intraplaque hemorrhage.
Radiology, 248(1), 202-209.
Amarenco, P., Bogousslavsky, J., Caplan, L. R., Donnan, G. A., Wolf, M. E., & Hennerici, M.
G. (2013). The ASCOD phenotyping of ischemic stroke (Updated ASCO Phenotyping).
Cerebrovasc Dis, 36(1), 1-5.
Appiah, D., Schreiner, P. J., Demerath, E. W., Loehr, L. R., Chang, P. P., & Folsom, A. R.
(2016). Association of Age at Menopause With Incident Heart Failure: A Prospective
Cohort Study and Meta‐Analysis. Journal of the American Heart Association:
Cardiovascular and Cerebrovascular Disease, 5(8), e003769.
Babiarz, L. S., Romero, J. M., Murphy, E. K., Brobeck, B., Schaefer, P. W., Gonzalez, R. G., &
Lev, M. H. (2009). Contrast-enhanced MR angiography is not more accurate than
unenhanced 2D time-of-flight MR angiography for determining > or = 70% internal
carotid artery stenosis. AJNR Am J Neuroradiol, 30(4), 761-768.
Balu, N., Chu, B., Hatsukami, T. S., Yuan, C., & Yarnykh, V. L. (2008). Comparison between
2D and 3D high-resolution black-blood techniques for carotid artery wall imaging in
clinically significant atherosclerosis. Journal of Magnetic Resonance Imaging, 27(4),
918-924.
Balu, N., Yarnykh, V. L., Chu, B., Wang, J., Hatsukami, T., & Yuan, C. (2011). Carotid plaque
assessment using fast 3D isotropic resolution black-blood MRI. Magn Reson Med, 65(3),
627-637.
Barnett, H. M., & Buchan, A. M. (2000). The imperative to develop dedicated stroke centers.
JAMA, 283(23), 3125-3126.
Bartlett, E. S., Walters, T. D., Symons, S. P., & Fox, A. J. (2006). Diagnosing carotid stenosis
near-occlusion by using CT angiography. AJNR Am J Neuroradiol, 27(3), 632-637.

157
Beach, K. W., Hatsukami, T., Detmer, P. R., Primozich, J. F., Ferguson, M. S., Gordon, D., . . .
Strandness, D. E., Jr. (1993). Carotid artery intraplaque hemorrhage and stenotic velocity.
Stroke, 24(2), 314-319.
Benjamin, P., Lawrence, A. J., Lambert, C., Patel, B., Chung, A. W., MacKinnon, A. D., . . .
Markus, H. S. (2014). Strategic lacunes and their relationship to cognitive impairment in
cerebral small vessel disease. Neuroimage Clin, 4, 828-837.
Bentzon, J. F., Otsuka, F., Virmani, R., & Falk, E. (2014). Mechanisms of Plaque Formation and
Rupture. Circ Res, 114(12), 1852-1866.
Berkhemer, O. A., Fransen, P. S., Beumer, D., van den Berg, L. A., Lingsma, H. F., Yoo, A. J., .
. . Dippel, D. W. (2015). A randomized trial of intraarterial treatment for acute ischemic
stroke. N Engl J Med, 372(1), 11-20.
Bhavnani, B. R., & Strickler, R. C. (2005). Menopausal hormone therapy. J Obstet Gynaecol
Can, 27(2), 137-162.
Bitar, R., Moody, A. R., Leung, G., Symons, S., Crisp, S., Butany, J., . . . Maggisano, R. (2008).
In vivo 3D high-spatial-resolution MR imaging of intraplaque hemorrhage. Radiology,
249(1), 259-267.
Bonati, L. H., & Nederkoorn, P. J. (2015). Clinical Perspective of Carotid Plaque Imaging.
Neuroimaging Clin N Am, 26(1), 175-82.
Bots, M. L., van Swieten, J. C., Breteler, M. M., de Jong, P. T., van Gijn, J., Hofman, A., &
Grobbee, D. E. (1993). Cerebral white matter lesions and atherosclerosis in the
Rotterdam Study. Lancet, 341(8855), 1232-1237.
Boysen, G., Ladegaard-Pedersen, H. J., Valentin, N., & Engell, H. C. (1970). Cerebral blood
flow and internal carotid artery flow during carotid surgery. Stroke, 1(4), 253-260.
Breault, J. L. (2013). Bioethics in practice - a quarterly column about medical ethics: ethics of
chart review research. Ochsner J, 13(4), 481-482.

158
Brinjikji, W., DeMarco, J. K., Shih, R., Lanzino, G., Rabinstein, A. A., Hilditch, C. A., . . .
Huston, J., 3rd. (2018). Diagnostic accuracy of a clinical carotid plaque MR protocol
using a neurovascular coil compared to a surface coil protocol. J Magn Reson Imaging,
Feb 25, ahead of print.
Brisset, M., Boutouyrie, P., Pico, F., Zhu, Y., Zureik, M., Schilling, S., . . . Debette, S. (2013).
Large-vessel correlates of cerebral small-vessel disease. Neurology, 80(7), 662-669.
Broderick, J., Brott, T., Kothari, R., Miller, R., Khoury, J., Pancioli, A., . . . Shukla, R. (1998).
The Greater Cincinnati/Northern Kentucky Stroke Study: preliminary first-ever and total
incidence rates of stroke among blacks. Stroke, 29(2), 415-421.
Brott, T. G., Halperin, J. L., Abbara, S., Bacharach, J. M., Barr, J. D., Bush, R. L., . . . Taylor, A.
J. (2011). 2011
ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS
guideline on the management of patients with extracranial carotid and vertebral artery
disease: executive summary. A report of the American College of Cardiology
Foundation/American Heart Association Task Force on Practice Guidelines, and the
American Stroke Association, American Association of Neuroscience Nurses, American
Association of Neurological Surgeons, American College of Radiology, American
Society of Neuroradiology, Congress of Neurological Surgeons, Society of
Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and
Interventions, Society of Interventional Radiology, Society of NeuroInterventional
Surgery, Society for Vascular Medicine, and Society for Vascular Surgery. Circulation,
124(4), 489-532.
Budohoski, K. P., Czosnyka, M., Kirkpatrick, P. J., Smielewski, P., Steiner, L. A., & Pickard, J.
D. (2013). Clinical relevance of cerebral autoregulation following subarachnoid
haemorrhage. Nat Rev Neurol, 9(3), 152-163.
Buratti, L., Balucani, C., Viticchi, G., Falsetti, L., Altamura, C., Avitabile, E., . . . Silvestrini, M.
(2014). Cognitive deterioration in bilateral asymptomatic severe carotid stenosis. Stroke,
45(7), 2072-2077.

159
Bureau, U. S. C. (2009). Population Estimates Vintage 2009: National Tables: U.S. Department
of Commerce.
Burke, A. P., Farb, A., Malcom, G., & Virmani, R. (2001). Effect of menopause on plaque
morphologic characteristics in coronary atherosclerosis. Am Heart J, 141(2 Suppl), S58-
62.
Cahill, P. A., & Redmond, E. M. (2013). Vascular endothelium - Gatekeeper of vessel health.
Atherosclerosis, 248, 97-109.
Cai, J., Hatsukami, T. S., Ferguson, M. S., Kerwin, W. S., Saam, T., Chu, B., . . . Yuan, C.
(2005). In vivo quantitative measurement of intact fibrous cap and lipid-rich necrotic core
size in atherosclerotic carotid plaque: comparison of high-resolution, contrast-enhanced
magnetic resonance imaging and histology. Circulation, 112(22), 3437-3444.
Cappendijk, V. C., Kessels, A. G., Heeneman, S., Cleutjens, K. B., Schurink, G. W., Welten, R.
J., . . . Kooi, M. E. (2008). Comparison of lipid-rich necrotic core size in symptomatic
and asymptomatic carotid atherosclerotic plaque: Initial results. J Magn Reson Imaging,
27(6), 1356-1361.
Carcaillon, L., Plichart, M., Zureik, M., Rouaud, O., Majed, B., Ritchie, K., . . . Empana, J.
(2014). Carotid plaque as a predictor of dementia in older adults: The Three-City Study.
Alzheimers Dement, 11(3), 239-248.
Carswell, R. (1838). Pathological anatomy: illustrations of the elementary forms of disease:
Longman, Orme, Brown, Green and Longman.
Chambless, L. E., Heiss, G., Folsom, A. R., Rosamond, W., Szklo, M., Sharrett, A. R., & Clegg,
L. X. (1997). Association of coronary heart disease incidence with carotid arterial wall
thickness and major risk factors: the Atherosclerosis Risk in Communities (ARIC) Study,
1987-1993. Am J Epidemiol, 146(6), 483-494.
Cheung, H. M., Moody, A. R., Singh, N., Bitar, R., Zhan, J., & Leung, G. (2011). Late stage
complicated atheroma in low-grade stenotic carotid disease: MR imaging depiction--
prevalence and risk factors. Radiology, 260(3), 841-847.

160
Chou, C. C., Lien, L. M., Chen, W. H., Wu, M. S., Lin, S. M., Chiu, H. C., . . . Bai, C. H. (2011).
Adults with late stage 3 chronic kidney disease are at high risk for prevalent silent brain
infarction: a population-based study. Stroke, 42, 2120-2125.
Collaborators, N. A. S. C. E. T. (1991). North American Symptomatic Carotid Endarterectomy
Trial. Methods, patient characteristics, and progress. Stroke, 22(6), 711-720.
Collaborators, N. A. S. C. E. T. (1991). Beneficial effect of carotid endarterectomy in
symptomatic patients with high-grade carotid stenosis. The New England journal of
medicine, 325(7), 445.
Cunningham, K. S., & Gotlieb, A. I. (2004). The role of shear stress in the pathogenesis of
atherosclerosis. Lab Invest, 85(1), 9-23.
Dade, L. A., Gao, F. Q., Kovacevic, N., Roy, P., Rockel, C., O'Toole, C. M., . . . Black, S. E.
(2004). Semiautomatic brain region extraction: a method of parcellating brain regions
from structural magnetic resonance images. Neuroimage, 22(4), 1492-1502.
Daftari Besheli, L., Aran, S., Shaqdan, K., Kay, J., & Abujudeh, H. (2014). Current status of
nephrogenic systemic fibrosis. Clin Radiol, 69(7), 661-668.
DeBakey, M. E. (1975). Successful carotid endarterectomy for cerebrovascular insufficiency.
Nineteen-year follow-up. JAMA, 233(10), 1083-1085.
Debette, S., & Markus, H. S. (2010). The clinical importance of white matter hyperintensities on
brain magnetic resonance imaging: systematic review and meta-analysis. BMJ, 341,
c3666.
Debrey, S. M., Yu, H., Lynch, J. K., Lövblad, K.-O., Wright, V. L., Janket, S.-J. D., & Baird, A.
E. (2008). Diagnostic Accuracy of Magnetic Resonance Angiography for Internal Carotid
Artery Disease: A Systematic Review and Meta-Analysis. Stroke, 39(8), 2237-2248.
DeMarco, J. K., & Huston, J., 3rd. (2014). Imaging of high-risk carotid artery plaques: current
status and future directions. Neurosurg Focus, 36(1), E1.

161
Den Ruijter, H. M., Peters, S. E., Anderson, T. J., & et al. (2012). Common carotid intima-media
thickness measurements in cardiovascular risk prediction: A meta-analysis. JAMA,
308(8), 796-803.
Di Carli, M. F., Geva, T., & Davidoff, R. (2016). The Future of Cardiovascular Imaging.
Circulation, 133(25), 2640-2661.
Doby, T. (1992). Cerebral angiography and Egas Moniz. AJR Am J Roentgenol, 159(2), 364.
E.C.A.C.A.S. -- Executive Committee for the Asymptomatic Carotid Atherosclerosis Study.
(1995). Endarterectomy for asymptomatic carotid artery stenosis. JAMA, 273(18), 1421-
1428.
Eisenmenger, L. B., Aldred, B. W., Kim, S. E., Stoddard, G. J., de Havenon, A., Treiman, G. S., .
. . McNally, J. S. (2016). Prediction of Carotid Intraplaque Hemorrhage Using
Adventitial Calcification and Plaque Thickness on CTA. AJNR Am J Neuroradiol, 37(8),
1496-503.
The Emerging Risk Factors Collaboration, C., Di Angelantonio, E., Kaptoge, S., Wormser, D.,
Willeit, P., Butterworth, A. S., . . . Danesh, J. (2015). Association of Cardiometabolic
Multimorbidity With Mortality. JAMA, 314(1), 52-60.
Eng, J. (2003). Sample size estimation: how many individuals should be studied? Radiology,
227(2), 309-313.
Fan, Z., Yu, W., Xie, Y., Dong, L., Yang, L., Wang, Z., . . . Li, D. (2014). Multi-contrast
atherosclerosis characterization (MATCH) of carotid plaque with a single 5-min scan:
technical development and clinical feasibility. J Cardiovasc Magn Reson, 16, 53.
Fanning, J. P., Wong, A. A., & Fraser, J. F. (2014). The epidemiology of silent brain infarction: a
systematic review of population-based cohorts. BMC Med, 12, 119.
Fenster, A., Downey, D. B., & Cardinal, H. N. (2001). Three-dimensional ultrasound imaging.
Phys Med Biol, 46(5), R67-99.

162
Finn, A. V., Nakano, M., Narula, J., Kolodgie, F. D., & Virmani, R. (2010). Concept of
vulnerable/unstable plaque. Arterioscler Thromb Vasc Biol, 30(7), 1282-1292.
Finn, A. V., & Narula, J. (2012). Intraplaque hemorrhage: most dangerous is the wound that
bleedeth inwardly. JACC Cardiovasc Imaging, 5(8), 856-858.
Fisch, L., & Brown, M. M. (2016). Management of carotid near-occlusion and acute carotid
occlusion. J Cardiovasc Surg (Torino), 57(2), 145-151.
Fisher, M. (1951). Occlusion of the internal carotid artery. AMA Archives of Neurology &
Psychiatry, 65(3), 346-377.
Fisher, M. (1954). Occlusion of the carotid arteries: further experiences. AMA Archives of
Neurology & Psychiatry, 72(2), 187-204.
Fleg, J. L., Stone, G. W., Fayad, Z. A., Granada, J. F., Hatsukami, T. S., Kolodgie, F. D., . . .
Narula, J. (2012). Detection of high-risk atherosclerotic plaque: report of the NHLBI
Working Group on current status and future directions. JACC Cardiovasc Imaging, 5(9),
941-955.
Fox, A. J. (1993). How to measure carotid stenosis. Radiology, 186(2), 316-318.
Fox, A. J., Eliasziw, M., Rothwell, P. M., Schmidt, M. H., Warlow, C. P., & Barnett, H. J.
(2005). Identification, prognosis, and management of patients with carotid artery near
occlusion. AJNR Am J Neuroradiol, 26(8), 2086-2094.
Fox, A. J., & Singh, N. (2015). Clinical trials for carotid stenosis revascularization and relation
to methods of stenosis quantification. Neurovascular Imaging, 1(1).
Fox, A. J., Symons, S. P., Aviv, R. I., Howard, P., Yeung, R., Bartlett, E. S., . . . Passariello, R.
(2009). Falsely claiming use of NASCET percentage stenosis method. Radiology, 253(2),
574-575; author reply 575.

163
Freilinger, T. M., Schindler, A., Schmidt, C., Grimm, J., Cyran, C., Schwarz, F., . . . Saam, T.
(2012). Prevalence of nonstenosing, complicated atherosclerotic plaques in cryptogenic
stroke. JACC Cardiovasc Imaging, 5(4), 397-405.
Fujikawa, T., Yamawaki, S., & Touhouda, Y. (1993). Incidence of silent cerebral infarction in
patients with major depression. Stroke, 24(11), 1631-1634.
Gallino, A., Aboyans, V., Diehm, C., Cosentino, F., Stricker, H., Falk, E., . . . Baumgartner, I.
(2014). Non-coronary atherosclerosis. Eur Heart J, 35(17), 1112-1119.
Gao, P., Chen, Z. Q., Bao, Y. H., Jiao, L. Q., & Ling, F. (2007). Correlation between carotid
intraplaque hemorrhage and clinical symptoms: systematic review of observational
studies. Stroke, 38(8), 2382-2390.
Gladstone, D. J., Spring, M., Dorian, P., Panzov, V., Thorpe, K. E., Hall, J., . . . Mamdani, M.
(2014). Atrial fibrillation in patients with cryptogenic stroke. N Engl J Med, 370(26),
2467-2477.
Glagov, S., Weisenberg, E., Zarins, C. K., Stankunavicius, R., & Kolettis, G. J. (1987).
Compensatory enlargement of human atherosclerotic coronary arteries. New England
Journal of Medicine, 316(22), 1371-1375.
Go, A. S., Mozaffarian, D., Roger, V. L., Benjamin, E. J., Berry, J. D., Borden, W. B., . . . Stroke
Statistics, S. (2013). Heart disease and stroke statistics--2013 update: a report from the
American Heart Association. Circulation, 127(1), e6-e245.
Goff, D. C., Lloyd-Jones, D. M., Bennett, G., Coady, S., D’Agostino, R. B., Gibbons, R., . . .
Wilson, P. W. F. (2014). 2013 ACC/AHA Guideline on the Assessment of
Cardiovascular Risk. J Am Coll Cardiol, 63(25), 2935-2959.
Gorelick, P. B. (1999). Carotid Endarterectomy Where Do We Draw the Line? Stroke, 30(9),
1745-1750.

164
Grant, E. G., Duerinckx, A. J., Saden, S. M. E., Melany, M. L., Hathout, G. M., Zimmerman, P.
T., . . . Baker, J. D. (2000). Ability to Use Duplex US to Quantify Internal Carotid
Arterial Stenoses: Fact or Fiction? Radiology, 214(1), 247-252.
Grimm, J. M., Schindler, A., Schwarz, F., Cyran, C. C., Bayer-Karpinska, A., Freilinger, T., . . .
Saam, T. (2014). Computed tomography angiography vs 3 T black-blood cardiovascular
magnetic resonance for identification of symptomatic carotid plaques. J Cardiovasc Magn
Reson, 16, 84.
Group, E. C. S. T. C. (1998). Randomised trial of endarterectomy for recently symptomatic
carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST).
Lancet, 351(9113), 1379-1387.
Group, M. A. C. S. T. A. C. (2004). Prevention of disabling and fatal strokes by successful
carotid endarterectomy in patients without recent neurological symptoms: randomised
controlled trial. The Lancet, 363(9420), 1491-1502.
Guo, J., Wang, S., Li, R., Chen, N., Zhou, M., Chen, H., . . . He, L. (2014). Cognitive
impairment and whole brain diffusion in patients with carotid artery disease and
ipsilateral transient ischemic attack. Neurol Res, 36(1), 41-46.
Gupta, A., Baradaran, H., Schweitzer, A. D., Kamel, H., Pandya, A., Delgado, D., . . . Sanelli, P.
C. (2013). Carotid plaque MRI and stroke risk: a systematic review and meta-analysis.
Stroke, 44(11), 3071-3077.
Gupta, A., Gialdini, G., Giambrone, A. E., Lerario, M. P., Baradaran, H., Navi, B. B., . . . Kamel,
H. (2016). Association Between Nonstenosing Carotid Artery Plaque on MR
Angiography and Acute Ischemic Stroke. JACC Cardiovasc Imaging, 9(10), 1228-1229.
Gupta, A., Gialdini, G., Lerario, M. P., Baradaran, H., Giambrone, A., Navi, B. B., . . . Kamel,
H. (2015). Magnetic Resonance Angiography Detection of Abnormal Carotid Artery
Plaque in Patients With Cryptogenic Stroke. J Am Heart Assoc, 4(6), e002012.
Gupta, A., & Marshall, R. S. (2015). Moving beyond luminal stenosis: imaging strategies for
stroke prevention in asymptomatic carotid stenosis. Cerebrovasc Dis, 39(5-6), 253-261.

165
Gupta, A., Mushlin, A. I., Kamel, H., Navi, B. B., & Pandya, A. (2015). Cost-Effectiveness of
Carotid Plaque MR Imaging as a Stroke Risk Stratification Tool in Asymptomatic
Carotid Artery Stenosis. Radiology, 277(3), 763-772.
Hart, R. G., Catanese, L., Perera, K. S., Ntaios, G., & Connolly, S. J. (2017). Embolic Stroke of
Undetermined Source: A Systematic Review and Clinical Update. Stroke, 48(4), 867-
872.
Hart, R. G., Diener, H.-C., Coutts, S. B., Easton, J. D., Granger, C. B., O'Donnell, M. J., . . .
Connolly, S. J. (2014). Embolic strokes of undetermined source: the case for a new
clinical construct. The Lancet Neurology, 13(4), 429-438.
Hashimoto, N., Hama, S., Yamane, K., & Kurisu, K. (2013). Carotid arterial intraplaque
hemorrhage and calcification influences cerebral hemodynamics. Neurosurg Rev, 36(3),
421-427.
Hatsukami, T. S., & Yuan, C. (2010). MRI in the early identification and classification of high-
risk atherosclerotic carotid plaques. Imaging Med, 2(1), 63-75.
Hedna, V. S., Bodhit, A. N., Ansari, S., Falchook, A. D., Stead, L., Heilman, K. M., & Waters,
M. F. (2013). Hemispheric Differences in Ischemic Stroke: Is Left-Hemisphere Stroke
More Common? Journal of Clinical Neurology (Seoul, Korea), 9(2), 97-102.
Heidenreich, P. A., Trogdon, J. G., Khavjou, O. A., Butler, J., Dracup, K., Ezekowitz, M. D., . . .
Woo, Y. J. (2011). Forecasting the future of cardiovascular disease in the United States: a
policy statement from the American Heart Association. Circulation, 123(8), 933-944.
Heidenreich, P. A., Trogdon, J. G., Khavjou, O. A., Butler, J., Dracup, K., Ezekowitz, M. D., . . .
Woo, Y. J. (2011). Forecasting the Future of Cardiovascular Disease in the United States:
A Policy Statement From the American Heart Association. Circulation, 123(8), 933-944.
Hellings, W. E., Pasterkamp, G., Verhoeven, B. A., De Kleijn, D. P., De Vries, J. P., Seldenrijk,
K. A., . . . Moll, F. L. (2007). Gender-associated differences in plaque phenotype of
patients undergoing carotid endarterectomy. J Vasc Surg, 45(2), 289-296; discussion 296-
287.

166
Hellings, W. E., Peeters, W., Moll, F. L., Piers, S. R., van Setten, J., Van der Spek, P. J., . . .
Pasterkamp, G. (2010). Composition of carotid atherosclerotic plaque is associated with
cardiovascular outcome: a prognostic study. Circulation, 121(17), 1941-1950.
Hermus, L., Lefrandt, J. D., Tio, R. A., Breek, J. C., & Zeebregts, C. J. (2010). Carotid plaque
formation and serum biomarkers. Atherosclerosis, 213(1), 21-29.
Hodis, H. N., Mack, W. J., Henderson, V. W., Shoupe, D., Budoff, M. J., Hwang-Levine, J., . . .
Azen, S. P. (2016). Vascular Effects of Early versus Late Postmenopausal Treatment with
Estradiol. N Engl J Med, 374(13), 1221-1231.
Hong, N. R., Seo, H. S., Lee, Y. H., Kim, J. H., Seol, H. Y., Lee, N. J., & Suh, S. I. (2011). The
correlation between carotid siphon calcification and lacunar infarction. Neuroradiology,
53(9), 643-649.
Hoshi, T., Sato, A., Akiyama, D., Hiraya, D., Sakai, S., Shindo, M., . . . Aonuma, K. (2015).
Coronary high-intensity plaque on T1-weighted magnetic resonance imaging and its
association with myocardial injury after percutaneous coronary intervention. Eur Heart J,
36(29), 1913-1922.
Hosseini, A. A., Kandiyil, N., Macsweeney, S. T., Altaf, N., & Auer, D. P. (2013). Carotid
plaque hemorrhage on magnetic resonance imaging strongly predicts recurrent ischemia
and stroke. Ann Neurol, 73(6), 774-784.
Hyafil, F., Schindler, A., Sepp, D., Obenhuber, T., Bayer-Karpinska, A., Boeckh-Behrens, T., . .
. Poppert, H. (2016). High-risk plaque features can be detected in non-stenotic carotid
plaques of patients with ischaemic stroke classified as cryptogenic using combined (18)F-
FDG PET/MR imaging. Eur J Nucl Med Mol Imaging, 43(2), 270-279.
Hyde, D. E., Fox, A. J., Gulka, I., Kalapos, P., Lee, D. H., Pelz, D. M., & Holdsworth, D. W.
(2004). Internal Carotid Artery Stenosis Measurement: Comparison of 3D Computed
Rotational Angiography and Conventional Digital Subtraction Angiography. Stroke,
35(12), 2776-2781.

167
Iemolo, F., Martiniuk, A., Steinman, D. A., & Spence, J. D. (2004). Sex differences in carotid
plaque and stenosis. Stroke, 35(2), 477-481.
Inaba, Y., Chen, J. A., & Bergmann, S. R. (2012). Carotid plaque, compared with carotid intima-
media thickness, more accurately predicts coronary artery disease events: a meta-
analysis. Atherosclerosis, 220(1), 128-133.
Jiang, Y., Kohara, K., & Hiwada, K. (1999). Low wall shear stress contributes to atherosclerosis
of the carotid artery in hypertensive patients. Hypertens Res, 22(3), 203-207.
Jochemsen, H. M., Muller, M., Bots, M. L., Scheltens, P., Vincken, K. L., Mali, W. P., . . .
Geerlings, M. I. (2014). Arterial stiffness and progression of structural brain changes:
The SMART-MR study. Neurology, 84(5), 448-55.
Johnson, M. B., Wilkinson, I. D., Wattam, J., Venables, G. S., & Griffiths, P. D. (2000).
Comparison of Doppler ultrasound, magnetic resonance angiographic techniques and
catheter angiography in evaluation of carotid stenosis. Clin Radiol, 55(12), 912-920.
Jousilahti, P., Vartiainen, E., Tuomilehto, J., & Puska, P. (1999). Sex, age, cardiovascular risk
factors, and coronary heart disease: a prospective follow-up study of 14 786 middle-aged
men and women in Finland. Circulation, 99(9), 1165-1172.
Kandiah, N., Goh, O., Mak, E., Marmin, M., & Ng, A. (2014). Carotid stenosis: a risk factor for
cerebral white-matter disease. J Stroke Cerebrovasc Dis, 23(1), 136-139.
Kandiyil, N., Altaf, N., Hosseini, A. A., MacSweeney, S. T., & Auer, D. P. (2012). Lower
prevalence of carotid plaque hemorrhage in women, and its mediator effect on sex
differences in recurrent cerebrovascular events. PLoS One, 7(10), e47319.
Kaufmann, T. J., Huston, J., 3rd, Mandrekar, J. N., Schleck, C. D., Thielen, K. R., & Kallmes, D.
F. (2007). Complications of diagnostic cerebral angiography: evaluation of 19,826
consecutive patients. Radiology, 243(3), 812-819.

168
Kerber, C. W., Cromwell, L. D., & Loehden, O. L. (1980). Catheter dilatation of proximal
carotid stenosis during distal bifurcation endarterectomy. American Journal of
Neuroradiology, 1(4), 348-349.
Kerwin, W. S., Liu, F., Yarnykh, V., Underhill, H., Oikawa, M., Yu, W., . . . Yuan, C. (2008).
Signal Features of the Atherosclerotic Plaque at 3.0T versus 1.5T: Impact on Automatic
Classification. J Magn Reson Imaging, 28(4), 987-995.
Kirkpatrick, A. C., Vincent, A. S., Guthery, L., & Prodan, C. I. (2014). Cognitive impairment is
associated with medication nonadherence in asymptomatic carotid stenosis. Am J Med,
127(12), 1243-1246.
Kissela, B., Schneider, A., Kleindorfer, D., Khoury, J., Miller, R., Alwell, K., . . . Broderick, J.
(2004). Stroke in a biracial population: the excess burden of stroke among blacks. Stroke,
35(2), 426-431.
Klabunde, R. E. (2012). Cardiovascular physiology concepts. Philadelphia, PA: Lippincott
Williams & Wilkins/Wolters Kluwer.
Kolodgie, F. D., Gold, H. K., Burke, A. P., Fowler, D. R., Kruth, H. S., Weber, D. K., . . .
Virmani, R. (2003). Intraplaque Hemorrhage and Progression of Coronary Atheroma.
New England Journal of Medicine, 349(24), 2316-2325.
Krejza, J., Arkuszewski, M., Kasner, S. E., Weigele, J., Ustymowicz, A., Hurst, R. W., . . .
Messe, S. R. (2006). Carotid Artery Diameter in Men and Women and the Relation to
Body and Neck Size. Stroke, 37(4), 1103-1105.
Kussmaul, A. (1872). Zwei Falle von spontaner allmahlicher Verschliessung grosser
Halsarterienstamme. Deutsches klin, 24, 461.
Kwee, R. M., Hofman, P. A., Gronenschild, E. H., van Oostenbrugge, R. J., Mess, W. H., ter
Berg, J. W., . . . Kooi, M. E. (2011). Association between carotid plaque characteristics
and cerebral white matter lesions: one-year follow-up study by MRI. PLoS One, 6(2),
e17070.

169
Kwee, R. M., van Engelshoven, J. M., Mess, W. H., ter Berg, J. W., Schreuder, F. H., Franke, C.
L., . . . Kooi, M. E. (2009). Reproducibility of fibrous cap status assessment of carotid
artery plaques by contrast-enhanced MRI. Stroke, 40(9), 3017-3021.
Layton, K. F., Kallmes, D. F., Cloft, H. J., Lindell, E. P., & Cox, V. S. (2006). Bovine Aortic
Arch Variant in Humans: Clarification of a Common Misnomer. American Journal of
Neuroradiology, 27(7), 1541-1542.
Lell, M., Fellner, C., Baum, U., Hothorn, T., Steiner, R., Lang, W., . . . Fellner, F. A. (2007).
Evaluation of carotid artery stenosis with multisection CT and MR imaging: influence of
imaging modality and postprocessing. AJNR Am J Neuroradiol, 28(1), 104-110.
Leung, G., & Moody, A. R. (2010). MR imaging depicts oxidative stress induced by
methemoglobin. Radiology, 257(2), 470-476.
Li, F., Yarnykh, V. L., Hatsukami, T. S., Chu, B., Balu, N., Wang, J., . . . Yuan, C. (2010). Scan-
rescan reproducibility of carotid atherosclerotic plaque morphology and tissue
composition measurements using multicontrast MRI at 3T. J Magn Reson Imaging,
31(1), 168-176.
Libby, P., & Pasterkamp, G. (2015). Requiem for the ‘vulnerable plaque’. Eur Heart J, 36(43),
2984-2987.
Liebeskind, D. S. (2003). Collateral Circulation. Stroke, 34(9), 2279-2284.
Lindsay, A. C., Biasiolli, L., Lee, J. M., Kylintireas, I., MacIntosh, B. J., Watt, H., . . .
Choudhury, R. P. (2012). Plaque features associated with increased cerebral infarction
after minor stroke and TIA: a prospective, case-control, 3-T carotid artery MR imaging
study. JACC Cardiovasc Imaging, 5(4), 388-396.
Liu, W., Balu, N., Sun, J., Zhao, X., Chen, H., Yuan, C., . . . Kerwin, W. S. (2012). Segmentation
of carotid plaque using multicontrast 3D gradient echo MRI. J Magn Reson Imaging,
35(4), 812-819.

170
Lloyd-Jones, D., Adams, R., Carnethon, M., De Simone, G., Ferguson, T. B., Flegal, K., . . .
Hong, Y. (2009). Heart disease and stroke statistics--2009 update: a report from the
American Heart Association Statistics Committee and Stroke Statistics Subcommittee.
Circulation, 119(3), e21-181.
Lorenz, M. W., Polak, J. F., Kavousi, M., Mathiesen, E. B., Volzke, H., Tuomainen, T. P., . . .
Thompson, S. G. (2012). Carotid intima-media thickness progression to predict
cardiovascular events in the general population (the PROG-IMT collaborative project): a
meta-analysis of individual participant data. Lancet, 379(9831), 2053-2062.
Mackinnon, A. D., Jerrard-Dunne, P., Sitzer, M., Buehler, A., von Kegler, S., & Markus, H. S.
(2004). Rates and Determinants of Site-Specific Progression of Carotid Artery Intima-
Media Thickness: The Carotid Atherosclerosis Progression Study. Stroke, 35(9), 2150-
2154.
Marczak, L., O’Rourke, K., Shepard, D. (2016). When and why people die in the United States,
1990-2013. JAMA, 315(3), 241-241.
Markl, M., Wegent, F., Zech, T., Bauer, S., Strecker, C., Schumacher, M., . . . Harloff, A. (2010).
In Vivo Wall Shear Stress Distribution in the Carotid Artery: Effect of Bifurcation
Geometry, Internal Carotid Artery Stenosis, and Recanalization Therapy. Circulation:
Cardiovascular Imaging, 3(6), 647-655.
Marvasti, T. B., Moody, A. R., Singh, N., Maraj, T., Tyrrell, P., & Afshin, M. (2018).
Haptoglobin 2-2 genotype is associated with presence and progression of MRI depicted
atherosclerotic intraplaque hemorrhage. IJC Heart & Vasculature, 18, 96-100.
McNally, J. S., Kim, S. E., Yoon, H. C., Findeiss, L. K., Roberts, J. A., Nightingale, D. R., . . .
Treiman, G. S. (2012). Carotid magnetization-prepared rapid acquisition with gradient-
echo signal is associated with acute territorial cerebral ischemic events detected by
diffusion-weighted MRI. Circ Cardiovasc Imaging, 5(3), 376-382.

171
McNally, S. J., Yoon, H. C., Kim, S. E., Narra, K. K., McLaughlin, M. S., Parker, D. L., &
Treiman, G. S. (2014). Carotid MRI Detection of Intraplaque Hemorrhage at 3T and
1.5T. J Neuroimaging, 25(3),390-6
McNeely, A. A., Ramirez, J., Nestor, S. M., Zhao, J., Gao, F., Kiss, A., . . . Black, S. E. (2015).
Cholinergic subcortical hyperintensities in Alzheimer's disease patients from the
sunnybrook dementia study: relationships with cognitive dysfunction and hippocampal
atrophy. J Alzheimers Dis, 43(3), 785-796.
Mendes, J., Parker, D. L., Kim, S. E., & Treiman, G. S. (2013). Reduced blood flow artifact in
intraplaque hemorrhage imaging using CineMPRAGE. Magn Reson Med, 69(5), 1276-
1284.
Michel, J. B., Virmani, R., Arbustini, E., & Pasterkamp, G. (2011). Intraplaque haemorrhages as
the trigger of plaque vulnerability. Eur Heart J, 32(16), 1977-1985, 1985a, 1985b, 1985c.
Mitra, D., Connolly, D., Jenkins, S., English, P., Birchall, D., Mandel, C., . . . Gholkar, A.
(2006). Comparison of image quality, diagnostic confidence and interobserver variability
in contrast enhanced MR angiography and 2D time of flight angiography in evaluation of
carotid stenosis. Br J Radiol, 79(939), 201-207.
Moody, A. (2012). Stroke: cause and effect--seek and ye shall find. JACC Cardiovasc Imaging,
5(4), 406-408.
Moody, A. R., Allder, S., Lennox, G., Gladman, J., & Fentem, P. (1999). Direct magnetic
resonance imaging of carotid artery thrombus in acute stroke. The Lancet, 353(9147),
122-123.
Moody, A. R., Bitar, R., Leung, G., & Maggisano, R. (2006). Looking beyond the lumen does
make all the difference. Stroke, 37(7), 1648; author reply 1649.
Moody, A. R., Murphy, R. E., Morgan, P. S., Martel, A. L., Delay, G. S., Allder, S., . . . Hunt, B.
J. (2003). Characterization of complicated carotid plaque with magnetic resonance direct
thrombus imaging in patients with cerebral ischemia. Circulation, 107, 3047-3052.

172
Moody, A. R., & Singh, N. (2016). Incorporating Carotid Plaque Imaging into Routine Clinical
Carotid Magnetic Resonance Angiography. Neuroimaging Clin N Am, 26(1), 29-44.
Morbiducci, U., Kok, A. M., Kwak, B. R., Stone, P. H., Steinman, D. A., & Wentzel, J. J.
(2016). Atherosclerosis at arterial bifurcations: evidence for the role of haemodynamics
and geometry. Thromb Haemost, 115(4), 484-492.
Motheral, B., Brooks, J., Clark, M. A., Crown, W. H., Davey, P., Hutchins, D., . . . Stang, P.
(2003). A Checklist for Retrospective Database Studies—Report of the ISPOR Task
Force on Retrospective Databases. Value in Health, 6(2), 90-97.
Mott, M., Pahigiannis, K., & Koroshetz, W. (2014). Small Blood Vessels: Big Health Problems:
National Institute of Neurological Disorders and Stroke Update. Stroke, 45(12), e257-
e258.
Muller, M., van der Graaf, Y., Algra, A., Hendrikse, J., Mali, W. P., & Geerlings, M. I. (2011).
Carotid atherosclerosis and progression of brain atrophy: the SMART-MR study. Ann
Neurol, 70(2), 237-244.
Munster, A. B., Thapar, A., & Davies, A. H. (2016). History of Carotid Stroke. Stroke, 47(4),
e66-69.
Murphy, R. E., Moody, A. R., Morgan, P. S., Martel, A. L., Delay, G. S., Allder, S., . . . Hunt, B.
J. (2003). Prevalence of complicated carotid atheroma as detected by magnetic resonance
direct thrombus imaging in patients with suspected carotid artery stenosis and previous
acute cerebral ischemia. Circulation, 107(24), 3053-3058.
Nadalo, L. A. (2015, Sept 22, 2015). Carotid Artery Stenosis Imaging. Medscape Drugs &
Diseases. Available from https://emedicine.medscape.com/article/417524.
Naghavi, M., Libby, P., Falk, E., Casscells, S. W., Litovsky, S., Rumberger, J., . . . Willerson, J.
T. (2003). From vulnerable plaque to vulnerable patient: a call for new definitions and
risk assessment strategies: Part I. Circulation, 108(14), 1664-1672.

173
Nguyen-Huynh, M. N., Wintermark, M., English, J., Lam, J., Vittinghoff, E., Smith, W. S., &
Johnston, S. C. (2008). How accurate is CT angiography in evaluating intracranial
atherosclerotic disease? Stroke, 39(4), 1184-1188.
Nofer, J. R. (2012). Estrogens and atherosclerosis: insights from animal models and cell systems.
J Mol Endocrinol, 48(2), R13-29.
Noguchi, T., Yamada, N., Higashi, M., Goto, Y., & Naito, H. (2011). High-intensity signals in
carotid plaques on T1-weighted magnetic resonance imaging predict coronary events in
patients with coronary artery disease. J Am Coll Cardiol, 58(4), 416-422.
Ota, H., Reeves, M. J., Zhu, D. C., Majid, A., Collar, A., Yuan, C., & DeMarco, J. K. (2010).
Sex differences in patients with asymptomatic carotid atherosclerotic plaque: in vivo 3.0-
T magnetic resonance study. Stroke, 41(8), 1630-1635.
Ota, H., Reeves, M. J., Zhu, D. C., Majid, A., Collar, A., Yuan, C., & DeMarco, J. K. (2013).
Sex Differences of High-Risk Carotid Atherosclerotic Plaque with Less Than 50%
Stenosis in Asymptomatic Patients: An In Vivo 3T MRI Study. American Journal of
Neuroradiology, 34(5), 1049-1055.
Ota, H., Yarnykh, V. L., Ferguson, M. S., Underhill, H. R., Demarco, J. K., Zhu, D. C., . . .
Yuan, C. (2010). Carotid intraplaque hemorrhage imaging at 3.0-T MR imaging:
comparison of the diagnostic performance of three T1-weighted sequences. Radiology,
254(2), 551-563.
Ovbiagele, B., Goldstein, L. B., Higashida, R. T., Howard, V. J., Johnston, S. C., Khavjou, O.
A., . . . Trogdon, J. G. (2013). Forecasting the future of stroke in the United States: a
policy statement from the American Heart Association and American Stroke Association.
Stroke, 44(8), 2361-2375.
Pantoni, L. (2010). Cerebral small vessel disease: from pathogenesis and clinical characteristics
to therapeutic challenges. Lancet Neurol, 9(7), 689-701.
Pasterkamp, G., & van der Steen, A. F. (2012). Intraplaque hemorrhage: an imaging marker for
atherosclerotic plaque destabilization? Arterioscler Thromb Vasc Biol, 32(2), 167-168.

174
Patsopoulos, N. A. (2011). A pragmatic view on pragmatic trials. Dialogues in Clinical
Neuroscience, 13(2), 217-224.
Patterson, A. J., JM, U. K.-I., Tang, T. Y., Scoffings, D. J., Howarth, S. P., Graves, M. J., &
Gillard, J. H. (2009). Association between white matter ischaemia and carotid plaque
morphology as defined by high-resolution in vivo MRI. Eur J Vasc Endovasc Surg,
38(2), 149-154.
Pen, A., Yam, Y., Chen, L., Dennie, C., McPherson, R., & Chow, B. J. (2013). Discordance
between Framingham Risk Score and atherosclerotic plaque burden. Eur Heart J, 34(14),
1075-1082.
Phan, T. G., Beare, R. J., Jolley, D., Das, G., Ren, M., Wong, K., . . . Srikanth, V. (2012).
Carotid artery anatomy and geometry as risk factors for carotid atherosclerotic disease.
Stroke, 43(6), 1596-1601.
Platzek, I., Sieron, D., Wiggermann, P., & Laniado, M. (2014). Carotid Artery Stenosis:
Comparison of 3D Time-of-Flight MR Angiography and Contrast-Enhanced MR
Angiography at 3T. Radiology Research and Practice, 2014, 508715.
Polak, J. F., Pencina, M. J., O'Leary, D. H., & D'Agostino, R. B. (2011). Common Carotid
Artery Intima-Media Thickness Progression as a Predictor of Stroke in Multi-Ethnic
Study of Atherosclerosis. Stroke, 42(11), 3017-3021.
Portegies, M. L. P., Selwaness, M., Hofman, A., Koudstaal, P. J., Vernooij, M. W., & Ikram, M.
A. (2015). Left-Sided Strokes Are More Often Recognized Than Right-Sided Strokes.
The Rotterdam Study, 46(1), 252-254.
Qureshi, A. I., Alexandrov, A. V., Tegeler, C. H., Hobson, R. W., 2nd, Dennis Baker, J., &
Hopkins, L. N. (2007). Guidelines for screening of extracranial carotid artery disease: a
statement for healthcare professionals from the multidisciplinary practice guidelines
committee of the American Society of Neuroimaging; cosponsored by the Society of
Vascular and Interventional Neurology. J Neuroimaging, 17(1), 19-47.

175
Ramirez, J., Berezuk, C., McNeely, A. A., Scott, C. J., Gao, F., & Black, S. E. (2015). Visible
Virchow-Robin spaces on magnetic resonance imaging of Alzheimer's disease patients
and normal elderly from the Sunnybrook Dementia Study. J Alzheimers Dis, 43(2), 415-
424.
Ramirez, J., Gibson, E., Quddus, A., Lobaugh, N. J., Feinstein, A., Levine, B., . . . Black, S. E.
(2011). Lesion Explorer: a comprehensive segmentation and parcellation package to
obtain regional volumetrics for subcortical hyperintensities and intracranial tissue.
Neuroimage, 54(2), 963-973.
Ramirez, J., McNeely, A. A., Scott, C. J., Stuss, D. T., & Black, S. E. (2014). Subcortical
hyperintensity volumetrics in Alzheimer's disease and normal elderly in the Sunnybrook
Dementia Study: correlations with atrophy, executive function, mental processing speed,
and verbal memory. Alzheimers Res Ther, 6(4), 49.
Ramirez, J., Scott, C. J., & Black, S. E. (2013). A short-term scan-rescan reliability test
measuring brain tissue and subcortical hyperintensity volumetrics obtained using the
lesion explorer structural MRI processing pipeline. Brain Topogr, 26(1), 35-38.
Ramirez, J., Scott, C. J., McNeely, A. A., Berezuk, C., Gao, F., Szilagyi, G. M., & Black, S. E.
(2014). Lesion Explorer: a video-guided, standardized protocol for accurate and reliable
MRI-derived volumetrics in Alzheimer's disease and normal elderly. J Vis Exp(86).
Ramirez, J., Singh, N., Adamo, S., Goubran, M., Thayalasuthan, V., Zhang, B., . . . Moody, A.
R. (2018). Carotid Atherosclerosis and Cerebral Small Vessel Disease: Preliminary
Results from the Canadian Atherosclerosis Imaging Network Project 1. Atherosclerosis
Supplements, 32, 156.
Reeves, M. J., Bushnell, C. D., Howard, G., Gargano, J. W., Duncan, P. W., Lynch, G., . . .
Lisabeth, L. (2008). Sex differences in stroke: epidemiology, clinical presentation,
medical care, and outcomes. Lancet Neurol, 7(10), 915-926.

176
Rizos, T., Guntner, J., Jenetzky, E., Marquardt, L., Reichardt, C., Becker, R., . . . Veltkamp, R.
(2012). Continuous stroke unit electrocardiographic monitoring versus 24-hour Holter
electrocardiography for detection of paroxysmal atrial fibrillation after stroke. Stroke,
43(10), 2689-2694.
Robicsek, F., Roush, T., Cook, J., & Reames, M. (2004). From Hippocrates to Palmaz-Schatz,
the history of carotid surgery. European journal of vascular and endovascular surgery,
27(4), 389-397.
Roger, V. L., Go, A. S., Lloyd-Jones, D. M., Benjamin, E. J., Berry, J. D., Borden, W. B., . . .
Turner, M. B. (2012). Heart disease and stroke statistics--2012 update: a report from the
American Heart Association. Circulation, 125, e2-e220.
Rosner, B. (2010). Fundamentals of biostatistics: Cengage Learning.
Rothwell, P., Gutnikov, S., & Warlow, C. (2003). Reanalysis of the final results of the European
Carotid Surgery Trial. Stroke, 34(2), 514-523.
Rozie, S., de Weert, T. T., de Monyé, C., Homburg, P. J., Tanghe, H. L. J., Dippel, D. W. J., &
van der Lugt, A. (2009). Atherosclerotic plaque volume and composition in symptomatic
carotid arteries assessed with multidetector CT angiography; relationship with severity of
stenosis and cardiovascular risk factors. Eur Radiol, 19(9), 2294-2301.
Rubin, M. F., Rosas, S. E., Chirinos, J. A., & Townsend, R. R. (2011). Surrogate markers of
cardiovascular disease in CKD: what's under the hood? Am J Kidney Dis, 57, 488-497.
Runck, F., Steiner, R. P., Bautz, W. A., & Lell, M. M. (2008). MR imaging: influence of imaging
technique and postprocessing on measurement of internal carotid artery stenosis. AJNR
Am J Neuroradiol, 29(9), 1736-1742.
Saam, T., Ferguson, M. S., Yarnykh, V. L., Takaya, N., Xu, D., Polissar, N. L., . . . Yuan, C.
(2005). Quantitative evaluation of carotid plaque composition by in vivo MRI.
Arterioscler Thromb Vasc Biol, 25(1), 234-239.

177
Saam, T., Habs, M., Buchholz, M., Schindler, A., Bayer-Karpinska, A., Cyran, C. C., . . . Helck,
A. (2016). Expansive arterial remodeling of the carotid arteries and its effect on
atherosclerotic plaque composition and vulnerability: an in-vivo black-blood 3T CMR
study in symptomatic stroke patients. J Cardiovasc Magn Reson, 18(1), 11.
Saam, T., Hetterich, H., Hoffmann, V., Yuan, C., Dichgans, M., Poppert, H., . . . Bamberg, F.
(2013). Meta-analysis and systematic review of the predictive value of carotid plaque
hemorrhage on cerebrovascular events by magnetic resonance imaging. J Am Coll
Cardiol, 62(12), 1081-1091.
Saam, T., Kerwin, W., Chu, B., Cai, J., Kampschulte, A., Hatsukami, T., . . . Yuan, C. (2005).
Sample Size Calculation for Clinical Trials Using Magnetic Resonance Imaging for the
Quantitative Assessment of Carotid Atherosclerosis. Journal of Cardiovascular Magnetic
Resonance, 7(5), 799-808.
Santos, M., Gold, G., Kovari, E., Herrmann, F. R., Bozikas, V. P., Bouras, C., &
Giannakopoulos, P. (2009). Differential impact of lacunes and microvascular lesions on
poststroke depression. Stroke, 40(11), 3557-3562.
Sarkar, R., Moody, A., & Leung, G. (2009). Effect of cardiac gating in high-resolution MRI of
the carotid vessel wall. Proc. Intl. Soc. Mag. Reson. Med, 17, 1825.
Schoof, J., Lubahn, W., Baeumer, M., Kross, R., Wallesch, C. W., Kozian, A., . . . Goertler, M.
(2007). Impaired cerebral autoregulation distal to carotid stenosis/occlusion is associated
with increased risk of stroke at cardiac surgery with cardiopulmonary bypass. J Thorac
Cardiovasc Surg, 134(3), 690-696.
Schulz, U. G., Gruter, B. E., Briley, D., & Rothwell, P. M. (2013). Leukoaraiosis and increased
cerebral susceptibility to ischemia: lack of confounding by carotid disease. J Am Heart
Assoc, 2(4), e000261.
Selwaness, M., & Bluemke, D. (2015). Early Atherosclerotic Disease Detected by MRI and CT
in the Carotid and Coronary Arteries in Low- moderate Risk Individuals (SSA17-08).
Paper presented at the RSNA, Chicago, IL.

178
Selwaness, M., van den Bouwhuijsen, Q., Mattace-Raso, F. U., Verwoert, G. C., Hofman, A.,
Franco, O. H., . . . Wentzel, J. J. (2014). Arterial stiffness is associated with carotid
intraplaque hemorrhage in the general population: the Rotterdam study. Arterioscler
Thromb Vasc Biol, 34(4), 927-932.
Selwaness, M., van den Bouwhuijsen, Q., van Onkelen, R. S., Hofman, A., Franco, O. H., van
der Lugt, A., . . . Vernooij, M. (2014). Atherosclerotic plaque in the left carotid artery is
more vulnerable than in the right. Stroke, 45(11), 3226-3230.
Selwaness, M., van den Bouwhuijsen, Q. J., Verwoert, G. C., Dehghan, A., Mattace-Raso, F. U.,
Vernooij, M., . . . Witteman, J. C. (2013). Blood pressure parameters and carotid
intraplaque hemorrhage as measured by magnetic resonance imaging: The Rotterdam
Study. Hypertension, 61(1), 76-81.
Shellock, F. G., & Spinazzi, A. (2008). MRI safety update 2008: part 2, screening patients for
MRI. AJR Am J Roentgenol, 191(4), 1140-1149.
Shuaib, A., Butcher, K., Mohammad, A. A., Saqqur, M., & Liebeskind, D. S. Collateral blood
vessels in acute ischaemic stroke: a potential therapeutic target. The Lancet Neurology,
10(10), 909-921.
Silvennoinen, H. M., Ikonen, S., Soinne, L., Railo, M., & Valanne, L. (2007). CT angiographic
analysis of carotid artery stenosis: comparison of manual assessment, semiautomatic
vessel analysis, and digital subtraction angiography. AJNR Am J Neuroradiol, 28(1), 97-
103.
Simova, I. (2015). Intima-media thickness: Appropriate evaluation and proper measurement,
described. E-journal of Cardiology Practice, 13(21).
Singh, N., Moody, A. (2015). Persistent Intraplaque Hemorrhage is Associated with the
Progression of Preexisting Low and Moderate Grade Carotid Stenosis: Results of a 10-
Year 3D Carotid MRI Clinical Experience. Paper presented at the ASNR 53rd Annual
Meeting, Chicago, IL.

179
Singh, N., Moody, A., Maraj, T., Marvasti, T. B., Tyrrell, P., Afshin, M., & Zavodni, A. (2015).
Quantitative Evaluation of Vessel Wall Volume and Intraplaque Hemorrhage by 3D
Carotid MRI. Paper presented at the ASNR 53rd Annual Meeting, Chicago, IL.
Singh, N., Moody, A. R., Gladstone, D. J., Leung, G., Ravikumar, R., Zhan, J., & Maggisano, R.
(2009). Moderate carotid artery stenosis: MR imaging-depicted intraplaque hemorrhage
predicts risk of cerebrovascular ischemic events in asymptomatic men. Radiology,
252(2), 502-508.
Singh, N., Moody, A. R., Panzov, V., & Gladstone, D. J. (2018). Carotid Intraplaque
Hemorrhage in Patients with Embolic Stroke of Undetermined Source. Journal of Stroke
and Cerebrovascular Diseases, 27(7), 1956-1959.
Singh, N., Moody, A. R., Rochon-Terry, G., Kiss, A., & Zavodni, A. (2013). Identifying a high
risk cardiovascular phenotype by carotid MRI-depicted intraplaque hemorrhage. Int J
Cardiovasc Imaging, 29(7), 1477-1483.
Singh, N., Moody, A. R., Roifman, I., Bluemke, D. A., & Zavodni, A. E. (2015). Advanced MRI
for carotid plaque imaging. Int J Cardiovasc Imaging, 32, 83–89.
Singh, N., Moody, A. R., Zhang, B., Kaminski, I., Kapur, K., Chiu, S., & Tyrrell, P. N. (2017).
Age-Specific Sex Differences in Magnetic Resonance Imaging-Depicted Carotid
Intraplaque Hemorrhage. Stroke, 48(8), 2129-2135.
Singh, N., Zavodni, A. E., & Moody, A. R. (2012). Magnetic Resonance Imaging of Carotid
Atherosclerosis and the Risk of Stroke. Current Cardiovascular Imaging Reports, 6(1),
25-33.
Sirimarco, G., Amarenco, P., Labreuche, J., Touboul, P. J., Alberts, M., Goto, S., . . .
Investigators, R. R. (2013). Carotid atherosclerosis and risk of subsequent coronary event
in outpatients with atherothrombosis. Stroke, 44(2), 373-379.
Sitzer, M., Puac, D., Buehler, A., Steckel, D. A., von Kegler, S., Markus, H. S., & Steinmetz, H.
(2003). Internal Carotid Artery Angle of Origin: A Novel Risk Factor for Early Carotid
Atherosclerosis. Stroke, 34(4), 950-955.

180
Murphy, S, Xu J, Kochanek MA. (2013). Deaths: Final data for 2010. National vital statistics
reports (Vol. 61). Available at
https://www.cdc.gov/nchs/data/nvsr/nvsr61/nvsr61_04.pdf.
Spence, J. D., Eliasziw, M., DiCicco, M., Hackam, D. G., Galil, R., & Lohmann, T. (2002).
Carotid plaque area: a tool for targeting and evaluating vascular preventive therapy.
Stroke, 33(12), 2916-2922.
Spence, J. D., & Hackam, D. G. (2010). Treating arteries instead of risk factors: a paradigm
change in management of atherosclerosis. Stroke, 41(6), 1193-1199.
Stary, H. C., Chandler, A. B., Dinsmore, R. E., Fuster, V., Glagov, S., Insull, W., . . . Wissler, R.
W. (1995). A Definition of Advanced Types of Atherosclerotic Lesions and a
Histological Classification of Atherosclerosis: A Report From the Committee on
Vascular Lesions of the Council on Arteriosclerosis, American Heart Association.
Circulation, 92(5), 1355-1374.
Statistics-Canada. (2015). Canada's population estimates, first quarter 2015. Statistics Canada.
Available at https://www150.statcan.gc.ca/n1/en/daily-quotidien/150617/dq150617c-
eng.pdf?st=yOMK0DNl.
Steg, P. G., Bhatt, D. L., Wilson, P. W., D'Agostino, R., Sr., Ohman, E. M., Rother, J., . . . Goto,
S. (2007). One-year cardiovascular event rates in outpatients with atherothrombosis.
JAMA, 297(11), 1197-1206.
Stein, J. H., Korcarz, C. E., Hurst, R. T., Lonn, E., Kendall, C. B., Mohler, E. R., . . . American
Society of Echocardiography Carotid Intima-Media Thickness Task, F. (2008). Use of
carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular
disease risk: a consensus statement from the American Society of Echocardiography
Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular
Medicine. J Am Soc Echocardiogr, 21(2), 93-111.

181
Streifler, J. Y., Eliasziw, M., Benavente, O. R., Hachinski, V. C., Fox, A. J., & Barnett, H. J.
(1995). Lack of relationship between leukoaraiosis and carotid artery disease. The North
American Symptomatic Carotid Endarterectomy Trial. Arch Neurol, 52(1), 21-24.
Sun, J., Canton, G., Balu, N., Hippe, D. S., Xu, D., Liu, J., . . . Yuan, C. (2016). Blood Pressure
Is a Major Modifiable Risk Factor Implicated in Pathogenesis of Intraplaque
Hemorrhage: An In Vivo Magnetic Resonance Imaging Study. Arterioscler Thromb Vasc
Biol, 36(4), 743-749.
Sun, J., Hippe, D. S., Underhill, H. R., Chu, B., Saam, T., Takaya, N., . . . Hatsukami, T. S.
(2015). Incremental value of carotid intraplaque hemorrhage for discriminating prior
coronary events. Neurovascular Imaging, 1(1), 1-7.
Sun, J., Underhill, H. R., Hippe, D. S., Xue, Y., Yuan, C., & Hatsukami, T. S. (2012). Sustained
acceleration in carotid atherosclerotic plaque progression with intraplaque hemorrhage: a
long-term time course study. JACC Cardiovasc Imaging, 5(8), 798-804.
Sun, J., Zhao, X. Q., Balu, N., Hippe, D. S., Hatsukami, T. S., Isquith, D. A., . . . Yuan, C.
(2014). Carotid magnetic resonance imaging for monitoring atherosclerotic plaque
progression: a multicenter reproducibility study. Int J Cardiovasc Imaging, 31(1), 95-103
Takaya, N., Yuan, C., Chu, B., Saam, T., Polissar, N. L., Jarvik, G. P., . . . Hatsukami, T. S.
(2005). Presence of intraplaque hemorrhage stimulates progression of carotid
atherosclerotic plaques: a high-resolution magnetic resonance imaging study. Circulation,
111(21), 2768-2775.
Takaya, N., Yuan, C., Chu, B., Saam, T., Underhill, H., Cai, J., . . . Hatsukami, T. S. (2006).
Association between carotid plaque characteristics and subsequent ischemic
cerebrovascular events: a prospective assessment with MRI--initial results. Stroke, 37(3),
818-823.
Tardif, J. C., Spence, J. D., Heinonen, T. M., Moody, A., Pressacco, J., Frayne, R., . . .
Beanlands, R. (2013). Atherosclerosis imaging and the Canadian Atherosclerosis Imaging
Network. Can J Cardiol, 29(3), 297-303.

182
Tomey, M. I., Narula, J., & Kovacic, J. C. (2014). Advances in the understanding of plaque
composition and treatment options: year in review. J Am Coll Cardiol, 63(16), 1604-
1616.
Touboul, P. J., Hennerici, M. G., Meairs, S., Adams, H., Amarenco, P., Bornstein, N., . . . Woo,
K. S. (2012). Mannheim Carotid Intima-Media Thickness and Plaque Consensus (2004–
2006–2011): An Update on Behalf of the Advisory Board of the 3rd and 4th Watching
the Risk Symposium 13th and 15th European Stroke Conferences, Mannheim, Germany,
2004, and Brussels, Belgium, 2006. Cerebrovascular diseases (Basel, Switzerland), 34(4),
290-296.
Touze, E., Toussaint, J. F., Coste, J., Schmitt, E., Bonneville, F., Vandermarcq, P., . . . group, H.
I.-R. m. r. I. i. a. S. o. t. C. a. s. (2007). Reproducibility of high-resolution MRI for the
identification and the quantification of carotid atherosclerotic plaque components:
consequences for prognosis studies and therapeutic trials. Stroke, 38(6), 1812-1819.
Treiman, G. S., McNally, J. S., Kim, S. E., & Parker, D. L. (2015). Correlation of Carotid
Intraplaque Hemorrhage and Stroke Using 1.5 T and 3 T MRI. Magn Reson Insights,
8(Suppl 1), 1-8.
Turc, G., Oppenheim, C., Naggara, O., Eker, O. F., Calvet, D., Lacour, J. C., . . . Touze, E.
(2012). Relationships between recent intraplaque hemorrhage and stroke risk factors in
patients with carotid stenosis: the HIRISC study. Arterioscler Thromb Vasc Biol, 32(2),
492-499.
U-King-Im, J. M., Fox, A. J., Aviv, R. I., Howard, P., Yeung, R., Moody, A. R., & Symons, S. P.
(2010). Characterization of carotid plaque hemorrhage: a CT angiography and MR
intraplaque hemorrhage study. Stroke, 41(8), 1623-1629.
Ueda, K., Watanabe, Y., Katsumata, T., Kaneko, T., Otori, T., Utsumi, K., . . . Katayama, Y.
(2011). Carotid intima-media thickness and cerebral white matter lesions are more
advanced in acute ischemic stroke patients with renal dysfunction. Clin Nephrol, 76, 290-
295.

183
Underhill, H. R., Hatsukami, T. S., Fayad, Z. A., Fuster, V., & Yuan, C. (2010). MRI of carotid
atherosclerosis: clinical implications and future directions. Nat Rev Cardiol, 7(3), 165-
173.
Underhill, H. R., Yarnykh, V. L., Hatsukami, T. S., Wang, J., Balu, N., Hayes, C. E., . . . Yuan,
C. (2008). Carotid plaque morphology and composition: initial comparison between 1.5-
and 3.0-T magnetic field strengths. Radiology, 248(2), 550-560.
van 't Klooster, R., de Koning, P. J., Dehnavi, R. A., Tamsma, J. T., de Roos, A., Reiber, J. H., &
van der Geest, R. J. (2012). Automatic lumen and outer wall segmentation of the carotid
artery using deformable three-dimensional models in MR angiography and vessel wall
images. J Magn Reson Imaging, 35(1), 156-165.
van 't Klooster, R., Naggara, O., Marsico, R., Reiber, J. H., Meder, J. F., van der Geest, R. J., . . .
Oppenheim, C. (2012). Automated versus manual in vivo segmentation of carotid plaque
MRI. AJNR Am J Neuroradiol, 33(8), 1621-1627.
van 't Klooster, R., Patterson, A. J., Young, V. E., Gillard, J. H., Reiber, J. H., & van der Geest,
R. J. (2013). An objective method to optimize the MR sequence set for plaque
classification in carotid vessel wall images using automated image segmentation. PLoS
One, 8(10), e78492.
van 't Klooster, R., Staring, M., Klein, S., Kwee, R. M., Kooi, M. E., Reiber, J. H., . . . van der
Geest, R. J. (2013). Automated registration of multispectral MR vessel wall images of the
carotid artery. Med Phys, 40(12), 121904.
van 't Klooster, R., Truijman, M. T., van Dijk, A. C., Schreuder, F. H., Kooi, M. E., van der
Lugt, A., & van der Geest, R. J. (2014). Visualization of local changes in vessel wall
morphology and plaque progression in serial carotid artery magnetic resonance imaging.
Stroke, 45(8), e160-163.

184
van den Bouwhuijsen, Q. J., Vernooij, M. W., Hofman, A., Krestin, G. P., van der Lugt, A., &
Witteman, J. C. (2012). Determinants of magnetic resonance imaging detected carotid
plaque components: the Rotterdam Study. Eur Heart J, 33(2), 221-229.
van der Meer, I. M., Bots, M. L., Hofman, A., del Sol, A. I., van der Kuip, D. A., & Witteman, J.
C. (2004). Predictive value of noninvasive measures of atherosclerosis for incident
myocardial infarction: the Rotterdam Study. Circulation, 109(9), 1089-1094.
Varennes, L., Tahon, F., Kastler, A., Grand, S., Thony, F., Baguet, J. P., . . . Krainik, A. (2015).
Fibromuscular dysplasia: what the radiologist should know: a pictorial review. Insights
Imaging, 6(3), 295-307.
Vermeer, S. E., Prins, N. D., den Heijer, T., Hofman, A., Koudstaal, P. J., & Breteler, M. M.
(2003). Silent brain infarcts and the risk of dementia and cognitive decline. N Engl J
Med, 348(13), 1215-1222.
Vesey, A. T., Dweck, M. R., & Fayad, Z. A. (2016). Utility of Combining PET and MR Imaging
of Carotid Plaque. Neuroimaging Clin N Am, 26(1), 55-68.
Virmani, R., Kolodgie, F. D., Burke, A. P., Finn, A. V., Gold, H. K., Tulenko, T. N., . . . Narula,
J. (2005). Atherosclerotic plaque progression and vulnerability to rupture: angiogenesis
as a source of intraplaque hemorrhage. Arterioscler Thromb Vasc Biol, 25(10), 2054-
2061.
Vlachopoulos, C., Xaplanteris, P., Aboyans, V., Brodmann, M., Cifkova, R., Cosentino, F., . . .
Townsend, R. R. (2015). The role of vascular biomarkers for primary and secondary
prevention. A position paper from the European Society of Cardiology Working Group
on peripheral circulation: Endorsed by the Association for Research into Arterial
Structure and Physiology (ARTERY) Society. Atherosclerosis, 241(2), 507-532.
Wang, J., Bornert, P., Zhao, H., Hippe, D. S., Zhao, X., Balu, N., . . . Kerwin, W. S. (2013).
Simultaneous noncontrast angiography and intraplaque hemorrhage (SNAP) imaging for
carotid atherosclerotic disease evaluation. Magn Reson Med, 69(2), 337-345.

185
Wang, J., Guan, M., Yamada, K., Hippe, D. S., Kerwin, W. S., Yuan, C., . . . Zhao, X. (2016). In
Vivo Validation of Simultaneous Non-Contrast Angiography and intraPlaque
Hemorrhage (SNAP) Magnetic Resonance Angiography: An Intracranial Artery Study.
PLoS One, 11(2), e0149130.
Wang, J., Yarnykh, V. L., Hatsukami, T., Chu, B., Balu, N., & Yuan, C. (2007). Improved
suppression of plaque-mimicking artifacts in black-blood carotid atherosclerosis imaging
using a multislice motion-sensitized driven-equilibrium (MSDE) turbo spin-echo (TSE)
sequence. Magn Reson Med, 58(5), 973-981.
Wang, T. J. (2011). Assessing the Role of Circulating, Genetic, and Imaging Biomarkers in
Cardiovascular Risk Prediction. Circulation, 123(5), 551-565.
Wannarong, T., Parraga, G., Buchanan, D., Fenster, A., House, A. A., Hackam, D. G., & Spence,
J. D. (2013). Progression of carotid plaque volume predicts cardiovascular events. Stroke,
44(7), 1859-1865.
Wardlaw, J. M., Smith, E. E., Biessels, G. J., Cordonnier, C., Fazekas, F., Frayne, R., . . .
Dichgans, M. (2013). Neuroimaging standards for research into small vessel disease and
its contribution to ageing and neurodegeneration. The Lancet Neurology, 12(8), 822-838.
Wasserman, B. A., Astor, B. C., Sharrett, A. R., Swingen, C., & Catellier, D. (2010). MRI
measurements of carotid plaque in the atherosclerosis risk in communities (ARIC) study:
methods, reliability and descriptive statistics. J Magn Reson Imaging, 31(2), 406-415.
Watanabe, J., Ogata, T., Hamada, O., Nonaka, M., Abe, H., Higashi, T., . . . Inoue, T. (2014).
Improvement of cognitive function after carotid endarterectomy--a new strategy for the
evaluation of cognitive function. J Stroke Cerebrovasc Dis, 23(6), 1332-1336.
Watanabe, Y., Nagayama, M., Suga, T., Yoshida, K., Yamagata, S., Okumura, A., . . . Dodo, Y.
(2008). Characterization of atherosclerotic plaque of carotid arteries with
histopathological correlation: vascular wall MR imaging vs. color Doppler
ultrasonography (US). J Magn Reson Imaging, 28(2), 478-485.

186
Weber, J., Veith, P., Jung, B., Ihorst, G., Moske-Eick, O., Meckel, S., . . . Taschner, C. A.
(2015). MR Angiography at 3 Tesla to Assess Proximal Internal Carotid Artery Stenoses:
Contrast-Enhanced or 3D Time-of-Flight MR Angiography? Clin Neuroradiol, 25(1), 41-
48.
White, R. P., & Markus, H. S. (1997). Impaired Dynamic Cerebral Autoregulation in Carotid
Artery Stenosis. Stroke, 28(7), 1340-1344.
WHO. (2011). Global Atlas on cardiovascular disease prevention and control: World Health
Organization. Available at
http://www.who.int/cardiovascular_diseases/publications/atlas_cvd/en/.
Wintermark, M., Jawadi, S. S., Rapp, J. H., Tihan, T., Tong, E., Glidden, D. V., . . . Saloner, D.
(2008). High-Resolution CT Imaging of Carotid Artery Atherosclerotic Plaques.
American Journal of Neuroradiology, 29(5), 875-882.
Yahagi, K., Davis, H. R., Arbustini, E., & Virmani, R. (2015). Sex differences in coronary artery
disease: pathological observations. Atherosclerosis, 239(1), 260-267.
Yoshida, K., Sadamasa, N., Narumi, O., Chin, M., Yamagata, S., & Miyamoto, S. (2012).
Symptomatic low-grade carotid stenosis with intraplaque hemorrhage and expansive
arterial remodeling is associated with a high relapse rate refractory to medical treatment.
Neurosurgery, 70(5), 1143-1150; discussion 1150-1141.
Yoshimura, S., Yamada, K., Kawasaki, M., Asano, T., Kanematsu, M., Takamatsu, M., . . .
Iwama, T. (2011). High-intensity signal on time-of-flight magnetic resonance
angiography indicates carotid plaques at high risk for cerebral embolism during stenting.
Stroke, 42(11), 3132-3137.
Yuan, C., Beach, K. W., Smith, L. H., & Hatsukami, T. S. (1998). Measurement of
Atherosclerotic Carotid Plaque Size In Vivo Using High Resolution Magnetic Resonance
Imaging. Circulation, 98(24), 2666-2671.
Yuan, C., Mitsumori, L. M., Ferguson, M. S., Polissar, N. L., Echelard, D., Ortiz, G., . . .
Hatsukami, T. S. (2001). In Vivo Accuracy of Multispectral Magnetic Resonance

187
Imaging for Identifying Lipid-Rich Necrotic Cores and Intraplaque Hemorrhage in
Advanced Human Carotid Plaques. Circulation, 104(17), 2051-2056.
Yuan, C., & Parker, D. L. (2016). Three-Dimensional Carotid Plaque MR Imaging.
Neuroimaging Clin N Am, 26(1), 1-12.
Zavodni, A. E., Wasserman, B. A., McClelland, R. L., Gomes, A. S., Folsom, A. R., Polak, J. F.,
. . . Bluemke, D. A. (2014). Carotid artery plaque morphology and composition in
relation to incident cardiovascular events: the Multi-Ethnic Study of Atherosclerosis
(MESA). Radiology, 271(2), 381-389.
Zhang, Y., Guallar, E., Qiao, Y., & Wasserman, B. A. (2014). Is carotid intima-media thickness
as predictive as other noninvasive techniques for the detection of coronary artery disease?
Arterioscler Thromb Vasc Biol, 34(7), 1341-1345.
Zhao, X., Underhill, H. R., & Zhao, Q. (2011). Discriminating Carotid Atherosclerotic Lesion
Severity by Luminal Stenosis and Plaque Burden: A Comparison Utilizing High-
Resolution Magnetic Resonance Imaging at 3.0 Tesla. Stroke, 42(2), 347-353.
Zhao, X. Q., Hatsukami, T. S., Hippe, D. S., Sun, J., Balu, N., Isquith, D. A., . . . Yuan, C.
(2014). Clinical Factors Associated With High-Risk Carotid Plaque Features as Assessed
by Magnetic Resonance Imaging in Patients With Established Vascular Disease (from the
AIM-HIGH Study). Am J Cardiol, 114(9), 1412-1419.
Zhu, D. C., Ferguson, M. S., & DeMarco, J. K. (2008). An optimized 3D inversion recovery
prepared fast spoiled gradient recalled sequence for carotid plaque hemorrhage imaging
at 3.0 T. Magn Reson Imaging, 26(10), 1360-1366.