Carina Cure’ Nelson PA-C Surgical Hospitalist
41
Carina Cure’ Nelson PA-C Surgical Hospitalist Plastic Surgery Emergencies
Transcript of Carina Cure’ Nelson PA-C Surgical Hospitalist

Carina Cure’ Nelson PA-CSurgical Hospitalist
Plastic Surgery Emergencies

Page 1
xxx00.#####.ppt 3/10/20 10:24:10 AMPage 1
Objectives •Evaluation and treatment of facial lacerations in the pediatric population
•Classification and treatment of burns not greater than 10% BSA
•Repair and appropriate treatment for animal bites
•Evaluation and recommendations for facial fractures

Facial Lacerations

Page 3
xxx00.#####.ppt 3/10/20 10:24:11 AMPage 3
History•Mechanism of injury
•How long ago did the injury occur?-Less than 24 hours for facial wounds is ideal
•Last tetanus booster-Any grossly contaminated deep wound should receive tetanus prophylaxis if > 5 years since booster

Page 4
xxx00.#####.ppt 3/10/20 10:24:11 AMPage 4
Assessment •Note size, location, and shape
•Evaluate for foreign bodies
•Palpate for depressions, focal tenderness, edema, and crepitus
•Assess cranial nerve function

Page 5
xxx00.#####.ppt 3/10/20 10:24:12 AMPage 5
Examination of Cranial Nerves •Assess cranial nerves II-XII for any facial trauma
•Sensory innervation of the face is provided primarily by the trigeminal nerve (CN V)
•Motor innervation to the muscles of facial expression is supplied by the facial nerve (CN VII)

Page 6
xxx00.#####.ppt 3/10/20 10:24:13 AMPage 6
Sensory Innervation of the Face •Trigeminal Nerve (CN V)
-Ophthalmic branch (V1) – sensory
•Exits via the supraorbital foramen
- Maxillary branch (V2) – sensory
•Exits via the infraorbital foramen
- Mandibular branch (V3) – sensory & motor
•Exits via the mental foramen

Page 7
xxx00.#####.ppt 3/10/20 10:24:13 AMPage 7
Sensory Innervation of the Face •Assessment of CN V
-Sensory – Light touch is assessed along the 3 main branches bilaterally
•Ask patient if the sensation of touch is felt the same on both sides of the face
-Motor – Ask patient to bite down and open, feeling for deviation at the temporal-mandibular joint

Page 8
xxx00.#####.ppt 3/10/20 10:24:14 AMPage 8
Motor Innervation of the Face •The facial nerve (CN VII) is responsible for supplying the majority of motor innervation to the face
•Facial nerve deficits will present as hemifacialweakness
•To assess the facial nerve ask patient to:-Close eyes tightly then open
-Puff out cheeks
-Raise eyebrows
-Smile and frown

Page 9
xxx00.#####.ppt 3/10/20 10:24:15 AMPage 9
Treatment
•Hemostasis
•Pain Control
-Local and topical anesthesia
•Irrigation
-Pressurized saline wound wash for smaller wounds
-1 L normal saline for larger areas
•Repair

Page 10
xxx00.#####.ppt 3/10/20 10:24:15 AMPage 10
Local and Topical Anesthesia •Pain control is key in the pediatric population
•Application of LET (lidocaine-epinephrine-tetracaine)
- Apply gel directly to wound for 20-30 minutes prior to repair. Analgesia is achieved when skin blanches.
•Injection of lidocaine with epinephrine (if needed)
-Epinephrine aides in hemostasis and prolongs duration of anesthesia

Page 11
xxx00.#####.ppt 3/10/20 10:24:20 AMPage 11
Application of LET

Page 12
xxx00.#####.ppt 3/10/20 10:24:20 AMPage 12
Suture Selection•Absorbable sutures are preferred in the pediatric population
Suture Type Absorption Profile Common UsesFast gut 7 days (least tensile
strength)Preferred for facial lacerations
Plain gut 10-14 days Nail bed lacerations, facial lacerations
Chromic gut 21 days Mucosa, extremity lacerations
Monocryl 3 months Deep dermal
Vicryl 2-3 months Deep dermal, muscle

Page 13
xxx00.#####.ppt 3/10/20 10:24:21 AMPage 13
Repair of Facial Lacerations •Simple interrupted for the majority of lacerations
•If gaping, use Monocryl for deep dermal sutures to reduce wound tension. When in doubt, place a deep dermal suture.
•Apply steri strips with Mastisol liquid adhesive to cover wound and keep dry.

Page 14
xxx00.#####.ppt 3/10/20 10:24:21 AMPage 14
Post-operative Care of Lacerations•Keep wounds covered and dry for the first 48 hours
•Wounds are most susceptible to infection within the first 48 hours
•If scabs form over the sutures, use clean Q-tip and soap to remove after daily cleansing
•Bacitracin for 3-5 days to help create moist wound environment
•Sunscreen to help improve cosmetic outcome of scar

Animal Bites

Page 16
xxx00.#####.ppt 3/10/20 10:24:22 AMPage 16
Assessment •Determine if rabies and tetanus prophylaxis is appropriate
•Local anesthesia
•Evaluate for any foreign bodies (retained teeth etc.)
•Assess for crepitus

Page 17
xxx00.#####.ppt 3/10/20 10:24:22 AMPage 17
Treatment•Copious irrigation with normal saline and debridement with 4x4 gauze
•Loosely close wounds and apply bacitracin. Avoid steristrips.
•Do NOT close puncture wounds as they have a high rate of infection
•Administer antibiotics-First line: Augmentin BID x 10 days - IV Unasyn for severely infected wounds-PCN Allergy: Clindamycin + Bactrim

Burns

Page 19
xxx00.#####.ppt 3/10/20 10:24:23 AMPage 19
Burns •Scope of Care for Burns at TCH:
-<10% BSA without inhalation injury excluding face, feet, genitals, perineum, hands or crossing major joints
•Basic Wound Care:-Liberal application of bacitracin, Xeroform or other non-stick dressing, and cover with gauze dressing
-Keep dressing in place for first 48 hours prior to first dressing change
-Change dressing daily until follow-up
-Follow-up with plastic surgery clinic in 1 week

Page 20
xxx00.#####.ppt 3/10/20 10:24:24 AMPage 20
Rule of Nines
Patient’s palm is 1% BSA

Page 21
xxx00.#####.ppt 3/10/20 10:24:25 AMPage 21
Classification of Burns First Degree
- Involves epidermis only
-Sunburn like
-Non-blanching erythema
-Very painful, heals in 1 week
Superficial Partial-Thickness- Involves epidermis and upper dermis
-Blistering common
-Painful
-Minimal scarring, heals in 2 weeks

Page 22
xxx00.#####.ppt 3/10/20 10:24:26 AMPage 22
Classification of Burns Deep Partial-Thickness
- Extends deeper into the dermis
- Mottled pink and white
- Heals in 2 to 4 weeks
- Scarring more likely
Full-Thickness- Extends completely through the dermis
- Wound appears white and dry
- Wounds are painless
- Referral to burn center likely

Facial Fractures

Page 24
xxx00.#####.ppt 3/10/20 10:24:27 AMPage 24
Evaluation•Maxillofacial CT scan is preferred
to evaluate for fractures
•Assess cranial nerves
-Facial nerve
-Trigeminal Nerve
•Assess for crepitus and bony
step-offs
•Any extension into the sinuses
requires antibiotics

Page 25
xxx00.#####.ppt 3/10/20 10:24:28 AMPage 25
Orbital Fractures•Consult ophthalmology if suspected injury to globe
-Patient will need detailed ophthalmologic exam
•Most commonly involve orbital floor or medial wall
•Assess CN III, IV, and VI
•Assess sensory and motor innervation of the face
•Assess for entrapment
Page 26
xxx00.#####.ppt 3/10/20 10:24:28 AMPage 26
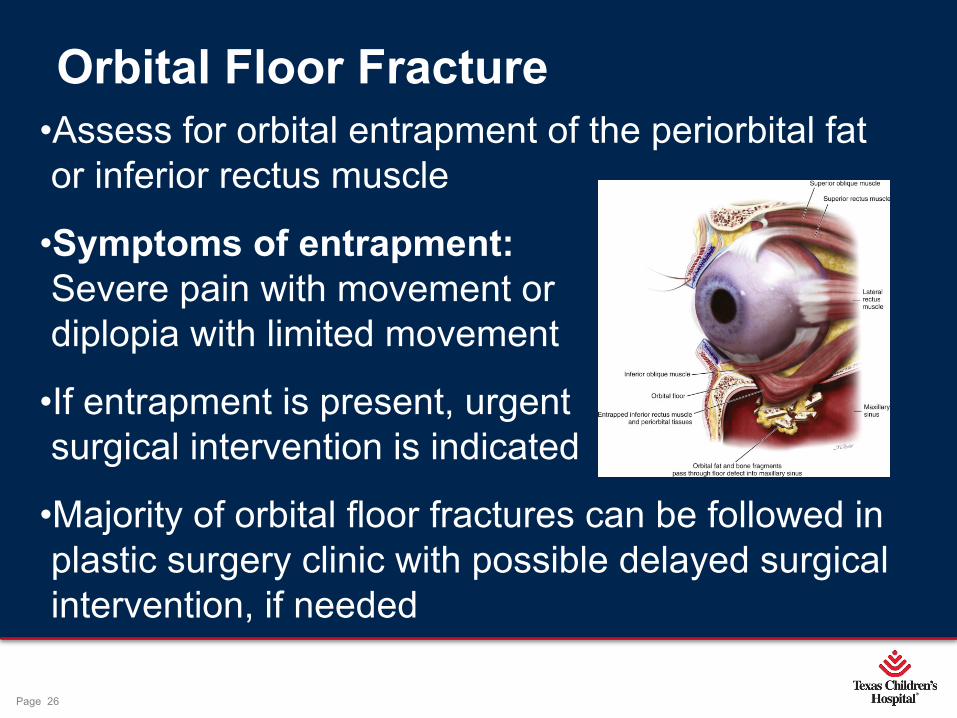
•Assess for orbital entrapment of the periorbital fat
or inferior rectus muscle
•Symptoms of entrapment: Severe pain with movement or
diplopia with limited movement
•If entrapment is present, urgent
surgical intervention is indicated
•Majority of orbital floor fractures can be followed in
plastic surgery clinic with possible delayed surgical
intervention, if needed
Orbital Floor Fracture

Page 27
xxx00.#####.ppt 3/10/20 10:24:29 AMPage 27
Sinus Precautions •Elevate head of bed
•Avoid forcefully blowing nose
•Avoid traveling on airplanes
•Sneeze with your mouth open
•Avoid using straws

Page 28
xxx00.#####.ppt 3/10/20 10:24:29 AMPage 28
Nasal Fractures•Control epistaxis
-Hold pressure for 15 minutes
-Administer Afrin if bleeding continue
•Evaluate for septal hematomas-Bleeding between the septum and mucosa
-Clinical diagnosis
-Requires immediate drainage and compression dressing
- If not addressed, can lead to necrosis of the septum

Page 29
xxx00.#####.ppt 3/10/20 10:24:30 AMPage 29
Mandibular Fractures•Evaluate for malocclusion and loose teeth
-Have patient open and bite down
•Non-operative management
-Soft chew diet for 6 weeks
-Peridex mouthwash for intraoral lacerations
•Maxillomandibular Fixation (MMF) -Reserved for comminuted, open, or displaced fractures

Hand Injuries
Page 31
xxx00.#####.ppt 3/10/20 10:24:31 AMPage 31
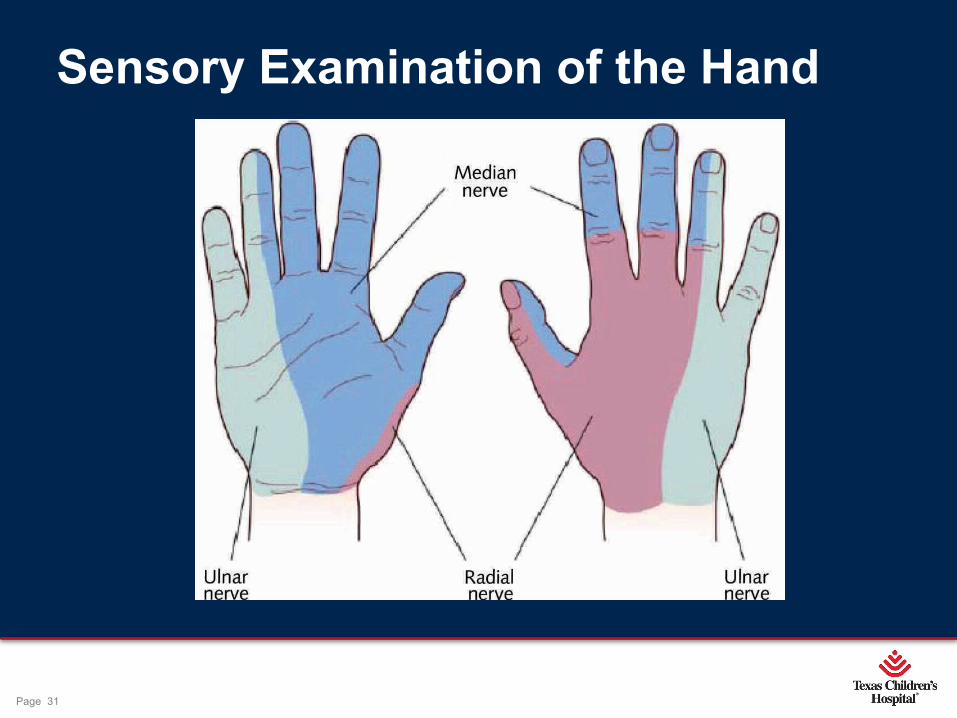
Sensory Examination of the Hand

Page 32
xxx00.#####.ppt 3/10/20 10:24:33 AMPage 32
Motor Innervation of the Hand•Median Nerve
-AIN (anterior interosseous nerve)-“Okay” sign
•Radial Nerve-PIN (posterior interosseous nerve)-Thumbs up!
•Ulnar Nerve-Able to cross fingers-Resisted abduction-Adducting fingers against a piece of paper

Page 33
xxx00.#####.ppt 3/10/20 10:24:33 AMPage 33
Tendon Assessment
Any concern for tendinous injury should be referred to hand surgery

Page 34
xxx00.#####.ppt 3/10/20 10:24:34 AMPage 34
Assessment Continued
•Ask about hand dominance
•Capillary refill -Less than 3 seconds is normal
•Palpate radial artery

Page 35
xxx00.#####.ppt 3/10/20 10:24:35 AMPage 35
Fingertip Injuries•Crush injury commonly seen in children
•Can occur with nail avulsion and tuft fracture
•Repair-Digital block performed
-Copious irrigation
-Nail is removed
-Nail bed is repaired
-Nail is replaced to ensure growth of new nail

Page 36
xxx00.#####.ppt 3/10/20 10:24:35 AMPage 36
Post-operative Care of Fingertip Injuries
•Keep wounds covered and dry for the first 48 hours
•Xeroform or petroleum gauze to prevent dressing from sticking to wound
•Splint tuft fractures
•Antibiotics prescribed for open fractures
•Follow-up in hand clinic in 1 week

Page 37
xxx00.#####.ppt 3/10/20 10:24:36 AMPage 37
Digit Amputation•Timing is critical
•Warm ischemia <12 hours
•Cold ischemia <24 hours (preferred)-Wrap severed digit in saline soaked gauze-Place in plastic bag then on ice-Container should be labeled and not leave patient’s side
•Hand surgeon to attempt replantation of severed digit in pediatric population

Page 38
xxx00.#####.ppt 3/10/20 10:24:36 AMPage 38
Compartment Syndrome•Any crush injury of the extremity should be evaluated for compartment syndrome
•Symptoms:-Pain out of proportion to injury-Pain with passive extension-Tense compartments -Late signs:
•Decreased sensation•Cool extremity•Absent pulse
•Diagnosis-Stryker needle pressure >30mmg -Positive clinical signs
•Treatment is urgent Fasciotomy

Thank you

Page 40
xxx00.#####.ppt 3/10/20 10:24:37 AMPage 40
References •Attum B. Physical Exam of the Hand. Orthobullets. https://www.orthobullets.com/hand/6008/physical-exam-of-the-hand.
•Bullocks JM, Hsu PW, Izaddoost SA, Hollier LH. Plastic Surgery Emergencies: Principles and Techniques. NY, NY: Thieme; 2017
•Jancin B. LET Gel Eases the Pain of Pediatric Wound Suturing. Pediatric News. 2012;46(2):22. doi:10.1016/s0031-398x(12)70047-4.
•UpToDate. https://www.uptodate.com/contents/assessment-and-management-of-facial-lacerations.