
Care Delivery with Electronic Prior Authorization 5-7-14 NCPDP Conference Presentation
61
Care Delivery with Electronic Prior Authorization Melissa Brown Dr. Anita Murcko Allison Orenstein May 7, 2014
-
Upload
rick-camp -
Category
Healthcare
-
view
156 -
download
0
Transcript of Care Delivery with Electronic Prior Authorization 5-7-14 NCPDP Conference Presentation

Care Delivery with Electronic Prior Authorization
Melissa Brown Dr. Anita Murcko Allison Orenstein May 7, 2014
Presentation Description
Prior authorization is an important process for ensuring appropriate pharmaceutical care and cost control. This largely manual process today is an administrative burden, highly reliant on forms, faxes and phone calls.
Implementation of the new standard for electronic prior authorization promises improved efficiency, cost and quality of care delivery.
About NCPDP
Founded in 1977, NCPDP is a not-for-profit, ANSI-accredited, Standards Development Organization with over 1,600 members representing virtually every sector of the pharmacy services industry.
NCPDP members have created standards such as the Telecommunication Standard and Batch Standard, the SCRIPT Standard for e-Prescribing, the Manufacturers Rebate Standard and more to improve communication within the pharmacy industry.
Our data products include dataQ®, a robust database of information on more than 76,000 pharmacies, and HCIdea®, a database of continually updated information on more than 2.3 million prescribers. NCPDP's RxReconn® is a legislative tracking product for real-time monitoring of pharmacy-related state and national legislative and regulatory activity. www.ncpdp.org

About Surescripts
Formed in 2001, Surescripts has evolved into the nation’s most comprehensive clinical network. Surescripts connects pharmacies, payers, pharmacy benefit managers, physicians, hospitals, integrated delivery networks, health information exchanges and health technology firms to enable the efficient and secure exchange of health information. More than 500,000 prescribers, 600 EHR applications and 94% of community pharmacists are active on the Surescripts network. Guided by the principles of neutrality, transparency, physician and patient choice, open standards, collaboration and privacy, Surescripts provides information for routine, recurring and emergency care. Together with our network participants, Surescripts is committed to saving lives, improving efficiency and reducing the cost of health care for all. For more information, go to www.surescripts.com and follow us at twitter.com/surescripts.
Today’s Speaker
Anita Murcko, MD, FACP – President and CEO of Cambiare, LLC
Dr. Anita Murcko is president and CEO of Cambiare, LLC and a clinical associate professor with more than 20 years of practice experience as an internal medicine physician. She has been formative in Arizona’s health information exchange (HIE), e-prescribing and electronic health records (EHR) initiatives. She is a recent recipient of the American College of Physicians (ACP) Laureate Award, The Arizona Capital Times as a Leader of the Year in Public Policy for Healthcare and selected by the Arizona Business Magazine as a Health Care Leader of the Year in Public Policy for Healthcare finalist.
Most recently, Dr. Murcko provided clinical leadership for the Arizona Medical Information Exchange (AMIE) and the Purchasing & Assistance Collaborative for Electronic Health Records (PACeHR) as its Medical Director for Clinical Informatics & Provider Adoption.
Dr. Murcko received her MD from the University of Pittsburgh School of Medicine and completed her internal medicine residency at Indiana University.

Today’s Speaker
Melissa Brown – Director of Benefits Messaging, Surescripts
Melissa Brown is a Product Director at Surescripts where she is responsible for Electronic Prior Authorization and other product offerings that leverage NCPDP Standards.
Melissa is an active member of NCPDP and has more than 19 years of experience with the development, launch and implementation of health care information technology products and services. Melissa has a Bachelor of Science Degree from the University of Wisconsin.
Today’s Speaker
Allison Orenstein - Director of Physician Connectivity and Marketing, CVS Caremark
Allison Orenstein is the director of Physician Connectivity and Marketing for CVS Caremark, where she is responsible for developing and implementing the strategy for connecting with the growing network of physicians utilizing electronic health records.
Allison works to identify new opportunities to better control healthcare costs and improve healthcare outcomes by leveraging the e-prescribing and electronic health records channel, coordinating efforts with the PBM, pharmacy and MinuteClinic divisions. Allison has been with CVS Caremark for 12 years. She earned an MBA from Santa Clara University and her BS from Northwestern University.
Learning Objectives
1. Define the impact of common prior authorization processes today
2. Describe the different types of ePA
3. Communicate how the NCPDP ePA standard will work with provider EHRs
4. Discuss the existence of state regulations around ePA
5. Explain the role of pharmacists in implementing the NCPDP ePA standard

Pre-Test Questions
• Describe challenges represented by medication prior authorization today
• List the various types of ePA services
• Explain the requirements for effective ePA implementation
Anita Murcko, MD, FACP
Forms, Fax, Phones and Portals The impact of prior authorization (PA) today

PA Forms and Formats Differ by Plan and Drug Class
manual completion and submission is burdensome
“It’s a nuisance-time-consuming, and often not in the patient’s best interest”
–George G. Ellis, Jr., MD Internal
medicine physician & Medical Economics editorial advisor
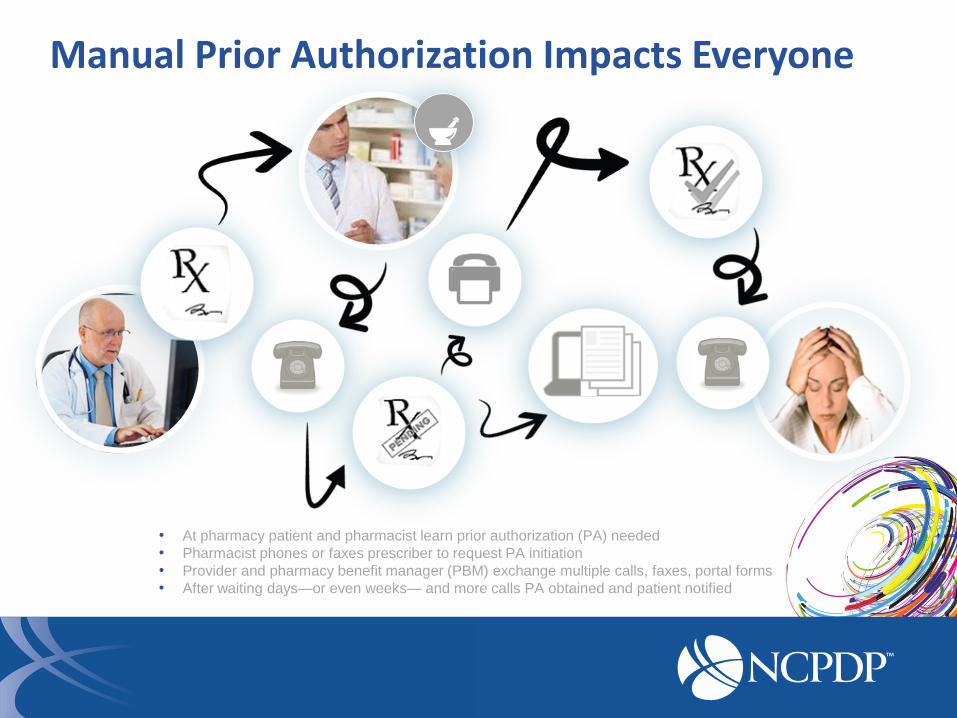
Manual Prior Authorization Impacts Everyone
• At pharmacy patient and pharmacist learn prior authorization (PA) needed
• Pharmacist phones or faxes prescriber to request PA initiation
• Provider and pharmacy benefit manager (PBM) exchange multiple calls, faxes, portal forms
• After waiting days—or even weeks— and more calls PA obtained and patient notified
Prior Authorization: Measurable Burden
“On average, physicians spent more time dealing with [drug PAs] than any other interaction”
May 2009
“What Does It Cost Physician Practices To Interact With Health Insurance Plans?”

4 Billion+
Prior Authorization Impact on Prescribers
$ Thousands Per physician each year1
3 - 8 hours Per physician each week1
1.Health Affairs, Volume 28 No4 w533. July/August 2009: “What Does it Cost Physician
Practices to Interact with Health Plans?” Lawrence P. Casalino, et al.
“Interactions with health
plans cost practices
$23 to $31 billion yearly”

Prior Authorization Impact on PBMs
1. Managed Healthcare Executive, 2009, Manage Medical Advances with Automated Prior Authorization, D. Moeller
2. American Journal of Managed Care, A Physician-Friendly Alternative to Prior Authorization for Prescription Drugs, Published Online, Dec. 2009
3. National Council for Prescription Drug Programs (NCPDP) ePA Task Group, December 2011
4. HealthCare Payer News, Streamlining Pre-authorizations to Prevent Physician Abrasion, Feb. 2013
90% OF PA REQUESTS
REQUIRE
PHONE OR FAX¹
91% OF PHYSICIANS ARE
“FRUSTRATED
WITH PAs”³
PHYSICIAN ABRASION
DAMAGED
REPUTATION4
PATIENT COMPLAINTS
$20 -25
PER SUBMISSION
TO PBM2
OPERATIONAL INEFFICIENCY
Prior Authorization Impact on Pharmacy
1 Krieger, Leah (2011, Spring). Prescription for Prior Authorizations: A Better Way. Retrieved March 2014, from
http://www.policymattersjournal.org/krieger.html.
• $11,440 cost per
pharmacist per year1
• 4 hours median time
spent on PAs per week1
“My doctor increased the dose from 2mg to 4mg. I went to pick up
my new script only to find out my insurance requires a Prior Auth. So I can’t pick up my script until this is settled and I am out of meds.” - Patient, Online Forum
Quote from http://www.crazymeds.us/CrazyTalk/index.php/topic/16320-abilify-pre-authorization-cant-get-script/
Manual PA Impacts Patient Wait Times for Medicine

4 Billion+
Streamlining Prior Authorization is a Top Priority for Providers
1 NCPDP ePA Task Group, 2011 2 Surescripts Survey (n = 2,391) http://www.ncpdp.org/pdf/NCPDPePATaskGroup_WhereHaveWeBeen_%20Final121511.pdf 3 Surescripts Survey (n=123)
91% Frustrated with
prior authorization2
#1 Most desired
e-prescribing
capability is ePA1
28% Would switch EHR
vendor for ePA3
Melissa Brown
The New Standard for Electronic Prior Authorization Improved workflow efficiency solution

NCPDP SCRIPT Standards for E-Prescribing
• Formulary, benefit, eligibility capabilities o exchange between prescribers and payers for pharmacy benefits
• Prescription routing and medication history capabilities o exchange between prescribers, pharmacies, intermediaries, payers
• Electronic prior authorization capabilities o exchange between prescribers and payers for pharmacy benefits
NCPDP Standard for Electronic Prior Authorization (ePA) Transactions • Officially approved as part of the NCPDP SCRIPT Standard in July 2013
Increasing workflow efficiency
Reducing administrative burden
Physician EHR PBM

NCPDP National ePA Standard was Successfully Pilot Tested
Pilot supported by industry leading
companies
• Allscripts
• CVS Caremark
• Navinet/CoverMyMeds
• Surescripts
New Standard Enables Options for ePrior Authorization Workflow
• Prospective workflow initiated at prescriber level before sending e-prescription to pharmacy o Physician identifies drugs requiring a PA before prescription is sent
• Retrospective workflow initiated at pharmacy after prescriptions is sent and rejected by PBM

ELIGIBILITY REQUEST / RESPONSE
PA INITIATION REQUEST / RESPONSE
Prospective ePA Implementation Approves PA Before RX is Sent
EHR
PBM PHYSICIAN notified if selected drug
needs prior authorization
Pre-approved
e-prescription
Benefit & formulary data referenced

Prospective EPA Integration Within the eRx Workflow - New Best Practice
• Leverages eligibility & formulary data to notify providers of medication PA requirements before e-prescribing
• Instead of forms, specific PA questions are sent to the EHR, based on patient, plan, and medication
• Pre-population of required patient information adds efficiency and accuracy to administrative tasks
• Real-time communications with PBM to complete prior authorization review before sending e-prescription
• Preapproved e-prescriptions routed to pharmacy and won’t be subject to PA block
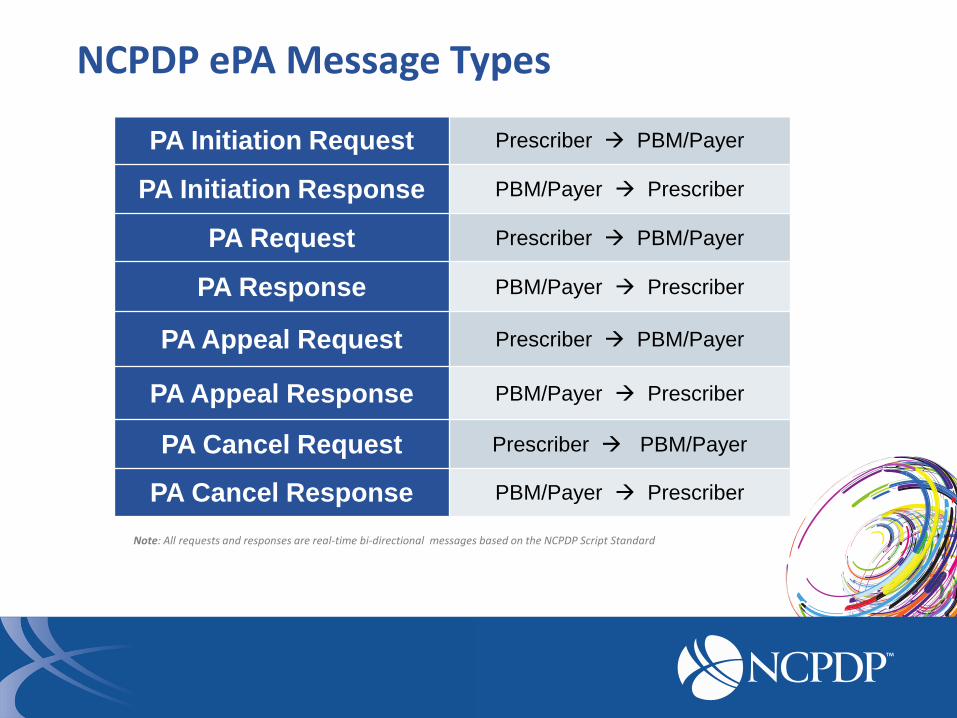
NCPDP ePA Message Types
Note: All requests and responses are real-time bi-directional messages based on the NCPDP Script Standard
PA Initiation Request Prescriber PBM/Payer
PA Initiation Response PBM/Payer Prescriber
PA Request Prescriber PBM/Payer
PA Response PBM/Payer Prescriber
PA Appeal Request Prescriber PBM/Payer
PA Appeal Response PBM/Payer Prescriber
PA Cancel Request Prescriber PBM/Payer
PA Cancel Response PBM/Payer Prescriber
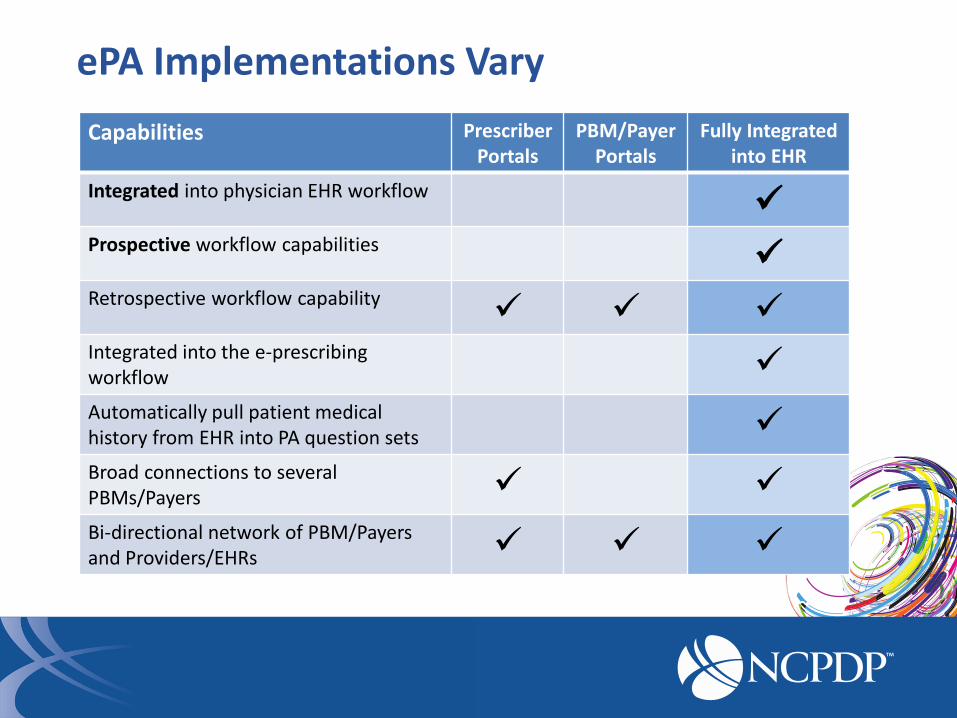
ePA Implementations Vary
Capabilities Prescriber Portals
PBM/Payer Portals
Fully Integrated into EHR
Integrated into physician EHR workflow
Prospective workflow capabilities
Retrospective workflow capability
Integrated into the e-prescribing workflow
Automatically pull patient medical history from EHR into PA question sets
Broad connections to several PBMs/Payers
Bi-directional network of PBM/Payers and Providers/EHRs
Allison Orenstein
Implementing the New Standard for Electronic Prior Authorization Lessons from ePA Pilot
“ePA speeds processing of prior authorizations and ensures that health plan members have quick access to care that is medically appropriate and cost effective.”
—Troyen A. Brennan, M.D., M.P.H., Chief Medical Officer, CVS Caremark

Large scale ePA pilot conducted through collaboration of industry leaders
• Launched in 2012 through CVS Caremark, Surescripts and two physician end-points: Allscripts ePrescribe and NaviNet/CoverMyMeds
• Several thousand prescribers sending transactions • Provided physicians with access to ePA for all clients for
whom CVS Caremark manages prior authorization process – Commercial Health Plans and Employers, Medicare, Medicaid, and
Specialty Medication – “Pilot” version continues to be supported through vendors, however,
evaluation period focused on proving success of transaction set in order to support NCPDP standards process

Payors interested in ePA and require flexibility enabled by NCPDP standard
• Early industry pilot work in mid- to late 2000s left payors dissatisfied – efforts tried to standardize questions
• Payors – particularly health plans – were still interested in driving an ePA product ahead to support provider networks
• The pilot transactions – on which the NCPDP standard was based – standardized the workflow and data format, while: – Allowing payors to retain customization of criteria – Allowing electronic health record vendors to retain unique
user interface and bring ePA into workflow

Pilot results showed great improvement over current options
• ePA can support an end-to-end communications for coverage determination
• ePA can effectuate an automated determination and approval – All potential denials were sent to a work queue for review
• ePA can also be used to streamline communications within necessitating implementation of automated determinations
• Most criteria returned in less than 60 seconds – typically in less than 30 seconds
• End-to-end process can be done in less than 5 minutes (including time for provider to answer questions)
• Client audit of traditional vs ePA approval/denial rate shows no difference in approval rate

Successfully implementing ePA: Payor View • Evaluate your current workflow
• Evaluate how your criteria is written • Skip logic • Free text
• You can use a complete criteria with no skip logic – the communications process is still more efficient for a provider
• Consider eventual development of criteria including LOINC codes so EHRs can further automate
• The goal of a fully-automated approvals in near real-time is the goal – however, making your criteria available electronically is still a win that allows the industry to support provider adoption
Successfully implementing ePA: EHR View
• Today’s ePA means a provider learns one process – that of their EHR – to request and respond to PAs for any payor
• Create the user experience that best fits within the workflow of that EHR
– Evaluate current workflow
– Signal that a prior authorization is required: Highlight formulary and benefit
– Consider creating a work queue that allows a provider to initiate ePA within a patient visit but complete it at a later time
– Consider how the system will communicate to a provider in the “in-between” times when responses not immediate
– Consider the prescription – do you hold for an approval or send to the pharmacy
Pharmacy View of ePA
• Prior Authorization presents a challenge to today’s pharmacist – Patient waiting to fill medication – often with no warning that
authorization required
– Creates back-and-forth between physician and pharmacist
• ePA has the ability to help alert physicians and patients before the prescription is sent to the pharmacy
– Benefits if authorizations can be completed prior to sending prescription to pharmacy
• Need more experience to understand how ePA will work in practice and affect pharmacy workflow

Pilot prescribers reported a positive experience
85% found ePA supportive of the process and that requesting criteria was easy, while 80% found it easy to submit the PA criteria
CVS Caremark Survey 2014; N = 100
Prescriber reactions from survey interviews
“It's much easier and
faster than before. I
really like it.”
“I think it is easier and
faster. once I got used
to doing it I got an
answer back real
quick.”
“It's very useful. We
love. It's a lot easier.
Saves a lot of time.”
“I first found it hard but
now it is easier than
what we usually do.”
Improving E-Prescribing Workflow with Electronic Prior Authorization Using NCPDP Script Standard for ePA
EMR Example
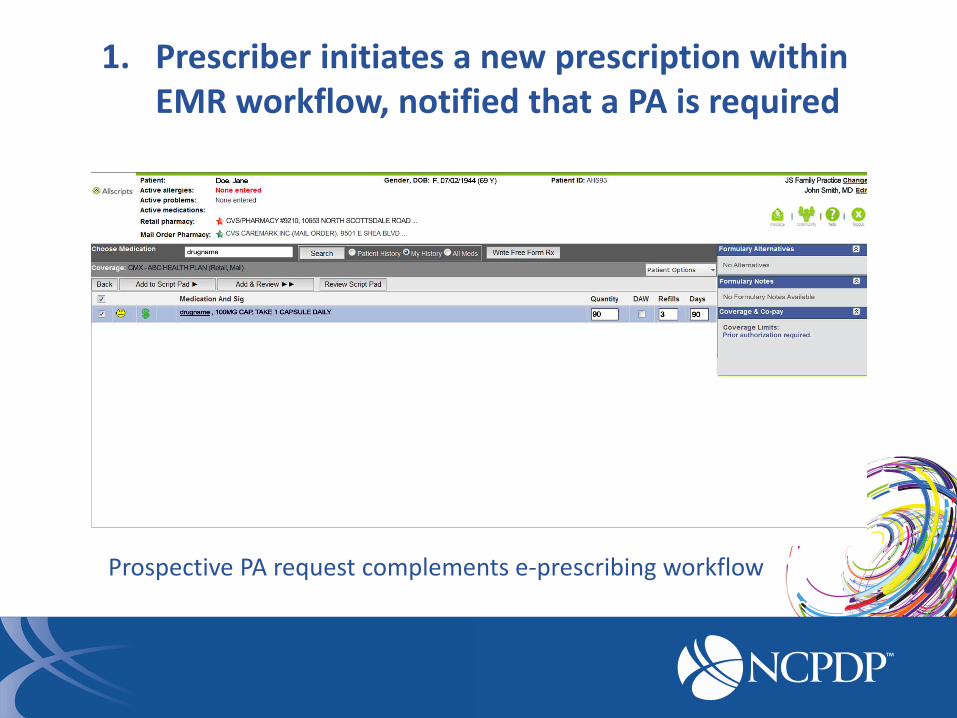
1. Prescriber initiates a new prescription within EMR workflow, notified that a PA is required
Prospective PA request complements e-prescribing workflow
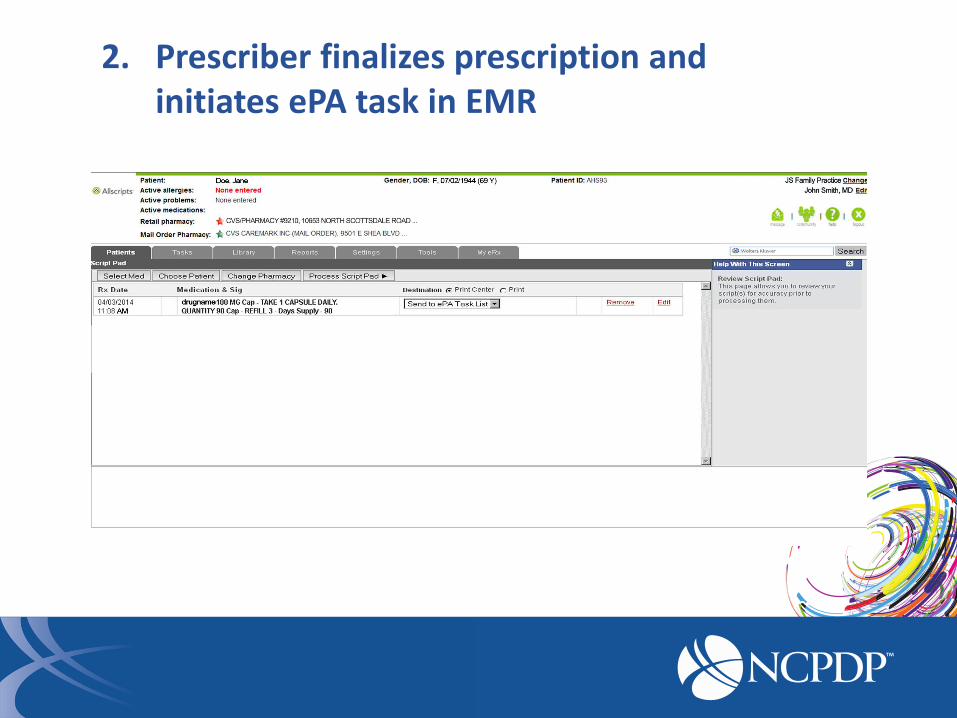
2. Prescriber finalizes prescription and initiates ePA task in EMR
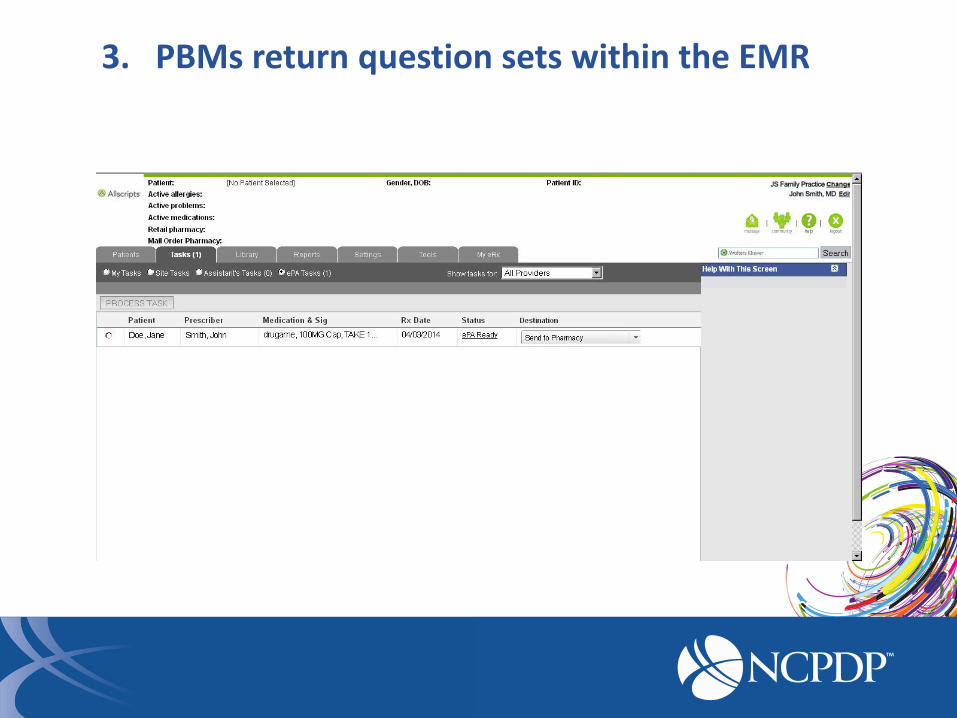
3. PBMs return question sets within the EMR
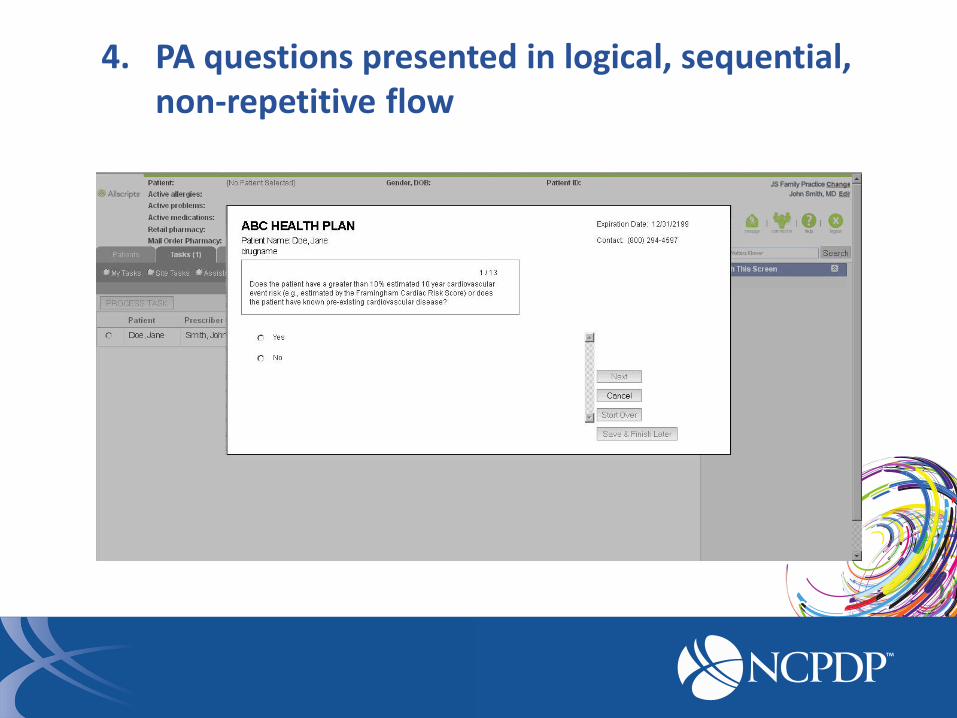
4. PA questions presented in logical, sequential, non-repetitive flow
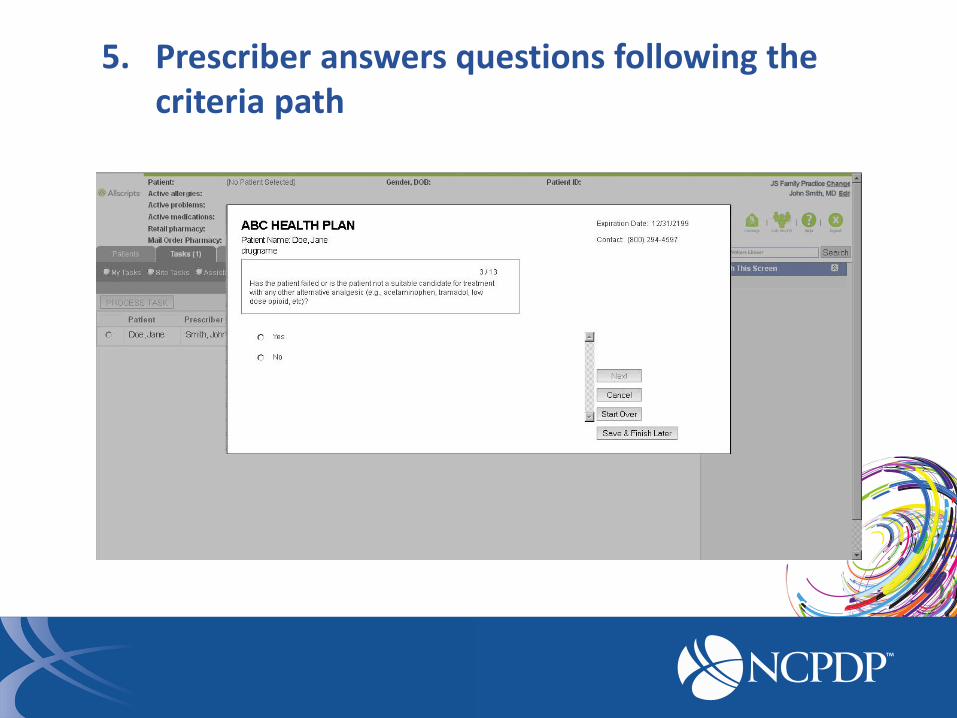
5. Prescriber answers questions following the criteria path

6. Additional questions easily reviewed and completed

7. Additional questions easily reviewed and completed
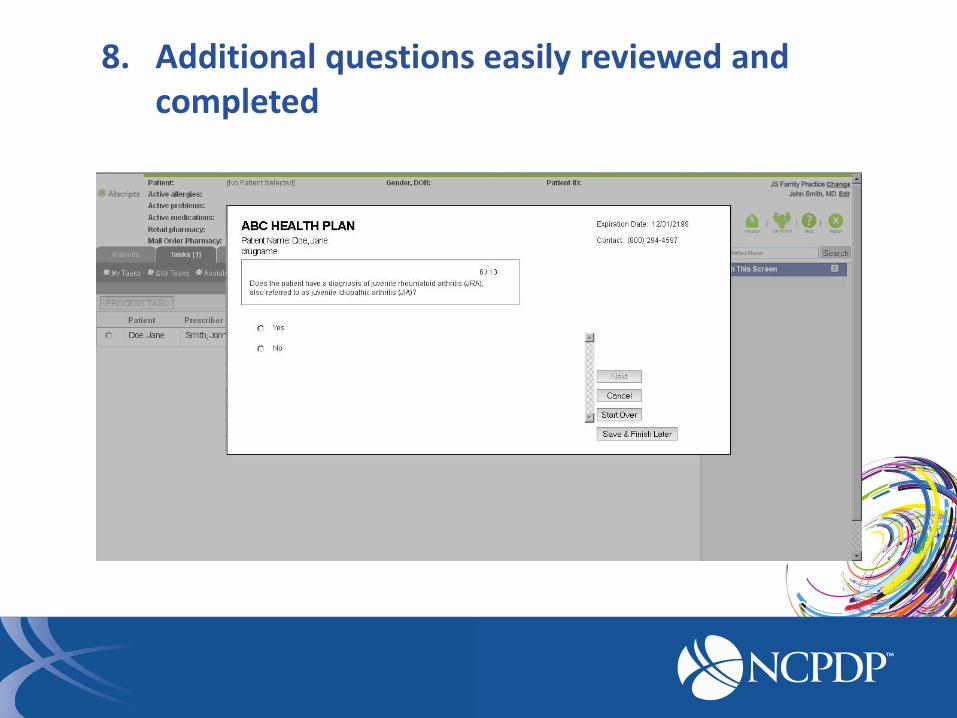
8. Additional questions easily reviewed and completed

9. Additional questions easily reviewed and completed
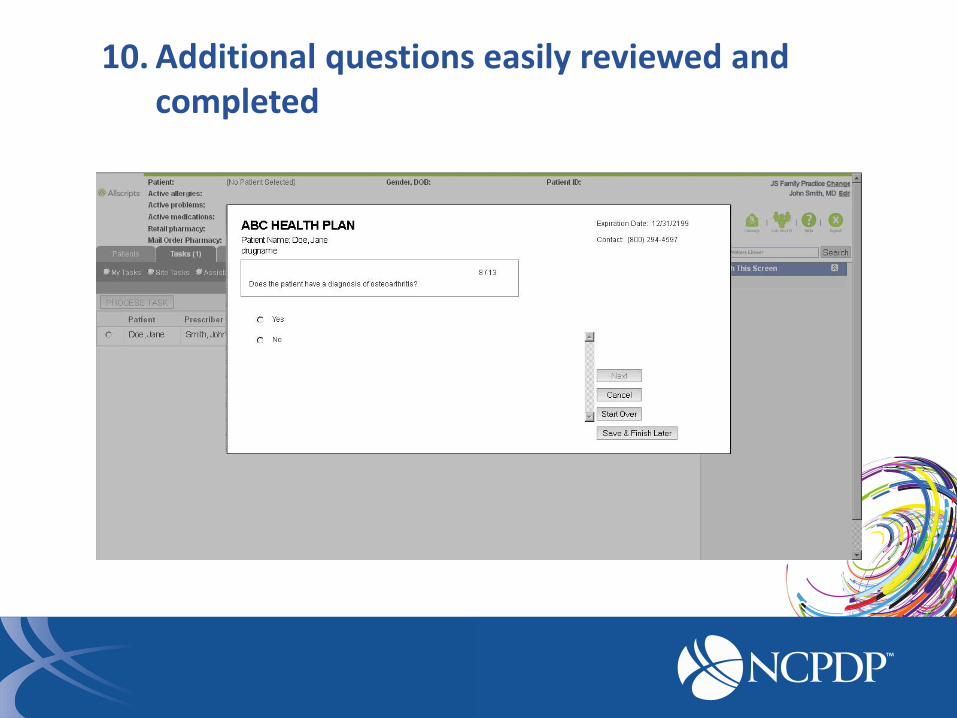
10. Additional questions easily reviewed and completed
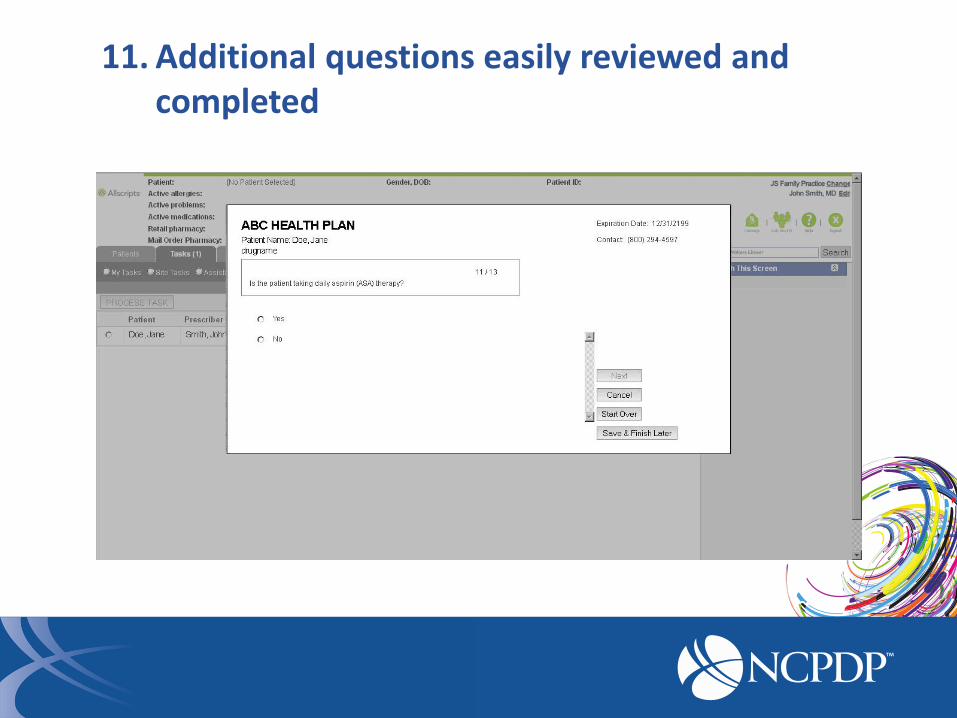
11. Additional questions easily reviewed and completed

12. Additional questions easily reviewed and completed

13. Prescriber can review answers and attach supporting documents
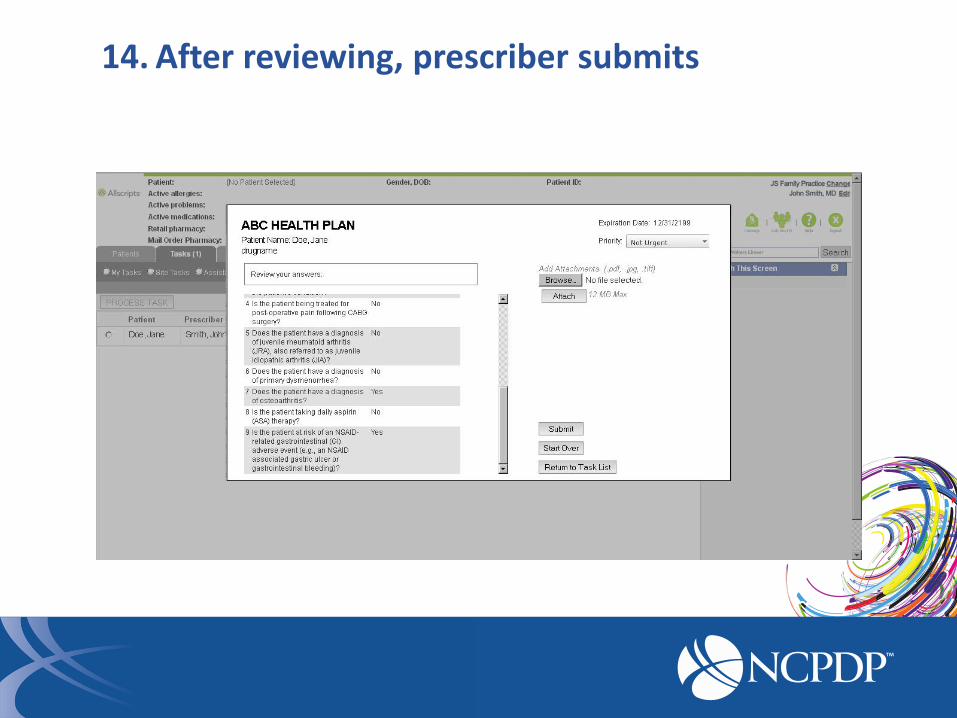
14. After reviewing, prescriber submits
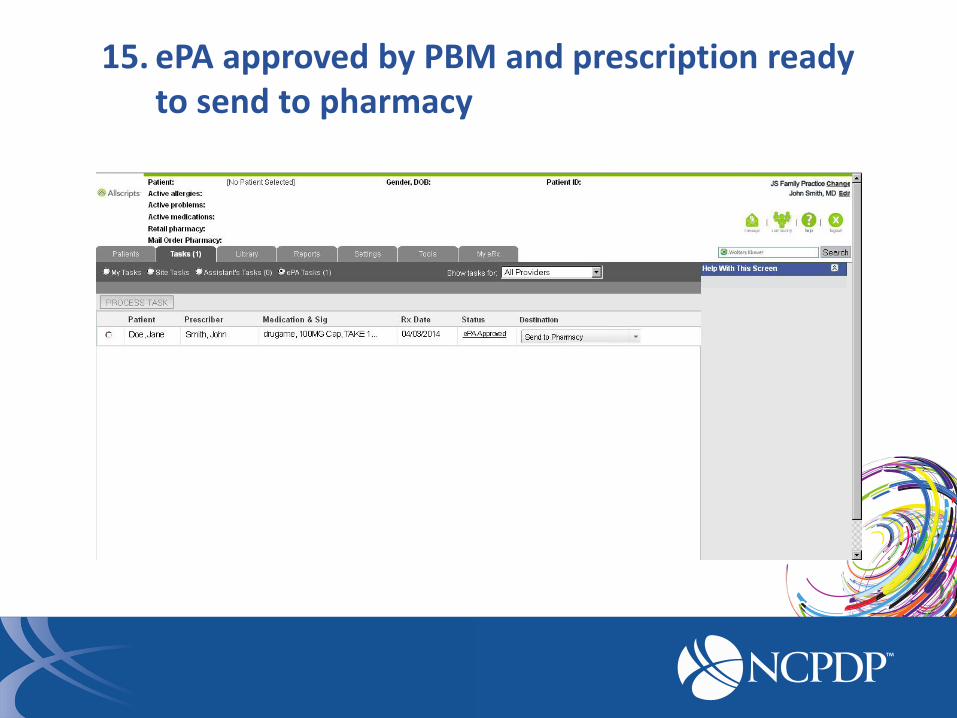
15. ePA approved by PBM and prescription ready to send to pharmacy

NCPDP SCRIPT STANDARD for ePA TODAY

States Requiring ePA for Medications
KY
MN
CO
GA
ND
NM
TX
VT
• Eight states have mandates for some type of ePA
• Other states require uniform PA forms
• Numerous states drafted study laws, planning ePA mandates upon completion
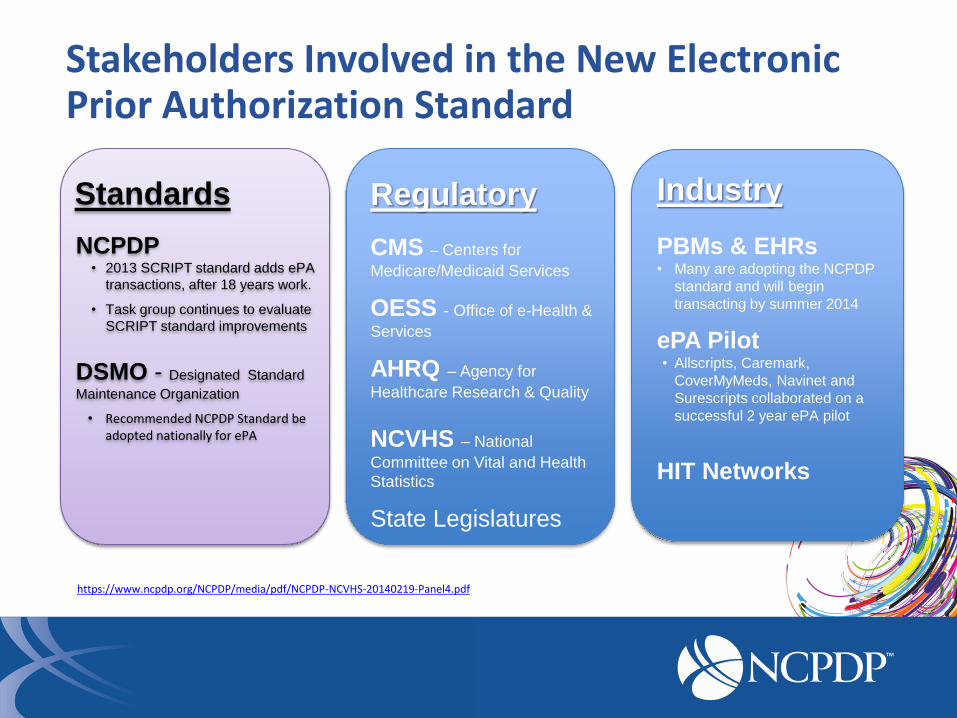
Stakeholders Involved in the New Electronic Prior Authorization Standard
Regulatory
CMS – Centers for
Medicare/Medicaid Services
OESS - Office of e-Health &
Services
AHRQ – Agency for
Healthcare Research & Quality
NCVHS – National
Committee on Vital and Health
Statistics
State Legislatures
PBMs & EHRs • Many are adopting the NCPDP
standard and will begin
transacting by summer 2014
ePA Pilot • Allscripts, Caremark,
CoverMyMeds, Navinet and
Surescripts collaborated on a
successful 2 year ePA pilot
HIT Networks
Industry Standards
NCPDP • 2013 SCRIPT standard adds ePA
transactions, after 18 years work.
• Task group continues to evaluate
SCRIPT standard improvements
DSMO - Designated Standard
Maintenance Organization
• Recommended NCPDP Standard be adopted nationally for ePA
https://www.ncpdp.org/NCPDP/media/pdf/NCPDP-NCVHS-20140219-Panel4.pdf
What You Can Do To Accelerate EPA Adoption
• Spread awareness about new SCRIPT standard for electronic prior authorization and its value
• Learn more about ePA
o www.NCPCP.org
o www.CompletEPA.com
o www2.caremark.com/epa/epa-faq.pdf
• Prioritize the ePA SCRIPT standard with your EHR, health plan, PBM or pharmacy information network
• Educate your legislators about this ePA standard and improved care opportunities
Integrated SCRIPT Standard for Electronic Prior Authorization
EHR
Another step towards better care, better health and lower costs
Test Questions
1. What is the estimated nationwide annual cost of prior authorization management for medical practices?
Answer: $23 to $31 billion
2. When was the NCPCP SCRIPT standard for ePA approved?
Answer: July 2013
3. The SCRIPT standard for ePA is a transaction between prescriber and PBM/Payer?
Answer: Yes
Test Questions
4. Is prospective alert and processing of a prior authorization possible before an e-prescription is sent to the pharmacy?
Answer: Yes
5. Do all ePA services have the same capabilities?
Answer: No. The levels of integration, automation and completeness vary


















