CARE Booklet B

of 16
-
Upload
anil-mishra -
Category
Documents
-
view
223 -
download
0
Transcript of CARE Booklet B
-
8/8/2019 CARE Booklet B
1/16
1
B. Newborn Care at the Community Level
N e w
b o r n
H e a
l t h
, M o
H F W
, G o
I
-
8/8/2019 CARE Booklet B
2/16
2
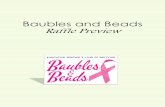
THE PROBLEM:TOO MANYNEWBORN INFANTSDIE IN INDIA
FIGURE 2Neonatal Mortality Rate in South Asian Countries (1995-2000)
N M R / 1 0 0 0 L i v e
B i r t h s
Source: State of the World s Newborns, Save the Children, 2001.
Sri Lanka Pakistan Nepal India Bangladesh
60
50
40
30
20
10
0
When an infant dies before completing
28 days of life, we call it neonatal or
newborn death. Each year, about 40
lakh babies die all over the world
before they are 28 days old. Of these,
about 10 lakhs are Indian (Figure 1).
Currently, of every 1000 live births in
India, about 40-60 do not survive
beyond 28 days after birth. This is what
we call the neonatal mortality rate
(NMR). In 2000, the average neonatal
mortality rate for India was 43/1000
live births. We can compare this with
some of our neighbours (Figure 2).
Within India, the NMR varies from a
high of over 60 per 1000 live births in
states like Orissa and Madhya Pradesh
to a low of around 11 per 1000 live
births in Kerala. The difference
between the states with the highest
and lowest NMRs is more than 5 times,
which indicates how much has yet to be
achieved. Clearly the example of Kerala
suggests that it is possible in India to
reduce NMR substantially.
In general, states, where deliveries
conducted by skilled health workers are
more frequent are also the states where
neonatal mortality is lower (Figure 3).
Why do newborn babies die?
They die of three main causes
asphyxia, prematurity and infections
Based on data from different studies in
a number of countries, WHO estimatesthat of all newborn deaths:
about 32% are caused by
infections, including tetanus
29% die of asphyxia (inability to
establish normal breathing at birth)
24% die due to complications
of being born prematurely
the remaining 15% from other
causes such as birth defects.
These figures are averages of figures
from many different settings, and
actual proportions for a given country
or state are likely to vary.
FIGURE 1Global Burden of Newborn Deaths
India
Rest of the world
Rest ofthe world
India10 lakhs
(25%)
30 lakhs (75%)
Roughly two-thirds of infantdeaths are neonatal deaths.Of these, almost two-thirdsoccur in the first week, andtwo-thirds of these on thefirst day after birth.
Source: State of the World s Newborns,Save the Children, 2001.
20
49 5043
48
-
8/8/2019 CARE Booklet B
3/16
3
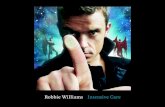
FIGURE 3NMR and Trained Healthworker Assisted Deliveries, Selected States, 1999
70
60
50
40
30
20
10
0
Source: Sample Registration Systems Statistical Report, 1999; NFHS 1998-99.
NMR Assisted Deliveries %
N M R / 1 0 0 0 L i v e B
i r t h s
D e
l i v e r i e s
A s s
i s t e
d b y
H e a
l t h P r o
f e s s
i o n
a l s %
100
90
80
70
60
50
40
30
20
10
0West
Bengal
Madhya
Pradesh
Andhra
Pradesh
Uttar
Pradesh
OrissaRajasthanKerala Bihar
FIGURE 4Causes of Neonatal Mortality
in a Rural Indian Study
Asphyxia20 %
Un-known10 %
Other3 %
Prematurity15 %
A study of newborn deaths in rural
Maharashtra (Figure 4) showed that
these causes were responsible for
about 88% of newborn deaths, of which
52% died due to infections.
Low birth weight (LBW) is an important
determinant of child mortality. The
lower the birth weight, the greater the
risk of death. In the Maharashtra study,
at least 90% of newborn deaths
occurred in neonates with a birth
weight less than 2.5 kg. (see Figure 4
and Table 1 on page 8) .
This has important implications on
programs aiming to reduce neonatal
mortality. Such programs must focus
primarily on reducing deaths from
these three specific causes: asphyxia,
prematurity and infections.
Newborn deaths occur due to lack
of care
Women in rural areas have poor access
to adequate nutrition and health care
before and during pregnancy. Children
born to such women are more likely to
be born with low birth weight and die
from common causes early in infancy.
Only about one-third of births in India
are attended by trained personnel,
even fewer in rural areas. This means,
most newborn babies do not get the
care they need at birth.
Most rural areas and many urban areas
do not have easy access to specialist
neonatal care hospitals. General
Low
Birthweight90 %
Sepsis52 %
Source: Bang AT et al, 1999.
hospitals, both in the public and private
sectors, are sometimes unable to
provide adequate care even for normal
newborn babies, and most do not have
the capability of taking care of
premature or sick newborns.
Often, family members are reluctant to
take newborn babies to available health
care facilities. Also families may not
recognize symptoms of illness early
enough for referral to be effective.
Unless adequate care is provided to
mothers before and during pregnancy,
to newborn infants at and after birth,
neonatal mortality will remain high.
What can be done to preventnewborn deaths?
Newborn deaths can be prevented by
addressing the major reasons for
newborn deaths:
A. Addressing issues related to lack of
adequate care
B. Addressing specific causes of
newborn death
Unhealthy Babies MakeUnhealthy Adults
While it is common sense that anunhealthy childhood can lead toan unhealthy adult life, a lot of
evidence is accumulating thatshows specific linkages betweenbabies with an unhealthy start inlife (such as those with low birthweight, asphyxia or sepsis), andlong term disability and disease.For instance, babies who areborn with low birth-weight aremore likely to develop diabetesand hypertension in later life.Such babies are also much lesslikely to reach their educationalor economic potential.
-
8/8/2019 CARE Booklet B
4/16
4
A. Addressing issues related tolack of adequate care
Ensuring the health and nutrition of
future and current mothers
Newborn health cannot be separatedfrom the health and health care of
women. Small girls grow into small
women, who develop into underweight
mothers who have undernourished
babies this is a vicious cycle of ill
health and high death rates. In turn,
the health and nutrition of mothers,
and the outcomes in terms of child
health are closely associated with the
status of women in society
opportunities for education, her roleand position in marriage and sexual
life, her contribution to decision
making at home, the degree of control
over family income, the willingness of
other family members to share routine
chores including child-care, access to
health care services are all related
to the place she is given in society, and
to how she demands her rights, and
exercises them. Ultimately, it is thecorrection of these distortions that will
help improve the care of women before
and during pregnancy.
Many of the conditions that cause
complications for the mother in
pregnancy, during delivery and after
delivery, also result in complications for
the baby. For instance maternal
reproductive tract infections may lead
to prematurity or still-birth, obstructedlabour can lead to asphyxia, and
hypertension in pregnancy (toxemia)
can lead to prematurity, still-birth and
asphyxia (as discussed later).
Addressing such specific maternal
problems will lead to better outcomes
for newborns. Specifically, certain
timely health interventions can make a
significant difference to the health of
the future mother, and thus to thechild (see Box below).
The Elements of Essential Newborn Care
A. Helping establish breathing at birth, with simple interventionsi. In case the baby has not cried, using simple physical stimuli for
inducing breathing/crying, like rubbing/flicking the palms and solesor rubbing the back of the baby
B. Ensuring adequate warmth from the moment of birthi. Immediately at birth, using a clean and dry cloth to wipe the baby,
and then using multiple layers of another cloth to wrap the babyfrom head to toe, keeping only the face exposed;
ii. Avoiding bathing for the first few days after birth;iii. Keeping the child adequately warm all the time particularly during
the first month
C. Ensuring adequate nutritioni. Breastfeeding the baby early and exclusivelyii. Detecting and managing common breastfeeding problems
D. Practicing clean handling to prevent infectionsi. Clean delivery by a trained attendant e.g. clean hands, clean
surface, clean blade, clean cord tie, and clean cord stumpii. Minimizing handling, and washing hands frequently before handling
the baby for the first few weeks
In addition, vaccines that are due at birth (BCG and OPV-0) are given asapplicable in the program. The care of babies with any special conditions(low birth-weight, asphyxia, sepsis, babies of HIV+ mothers, etc.) is dealtwith in separate sections.
Care of future mothersImprove the nutritional statusof girls. This should include theprevention or treatment ofanemia.Discourage early marriages andearly childbearing.Promote safer sexual practicesand birth spacing.
Care during pregnancyImprove the nutrition ofpregnant women, includingeating more food, and takingiron tablets to prevent ortreat anemia.Ensure tetanus immunizationScreen and treat infections(especially syphilis and malaria).Provide prophylaxis for malaria,if in a malaria endemic area.Ensure antenatal examinationsto detect maternal conditionssuch as anemia and toxemia, orcomplications related to thefetus or placenta. Ensureadequate action for anyproblems detected.Ensure birth preparedness:encourage planning for where todeliver, and to prepareadequately for home delivery,including for potentialemergencies. Encouragepreparedness for immediatecare of the newborn at birth.
Special attentionPromote voluntary counselingand testing for HIV (see sectionon HIV).Reduce the risk of mother-to-child transmission of HIV (seesection on HIV).
-
8/8/2019 CARE Booklet B
5/16
5
Essential Newborn Care
Essential newborn care is often defined
differently by different programs.
Here, it is used to denote basic care
that can be provided to every newborn
in any setting, in the periodimmediately after birth and for the
duration of the newborn period (the
first month of life). This includes all
the basic care that any healthy
newborn needs to ensure its health and
survival.
The commonest reason for failure to
provide basic care to newborn babies is
lack of awareness among care-givers,
including family members, about whatis best for the health and survival of
the newborn. Many, but not all,
traditional newborn care practices are
beneficial to the baby, and a program
that reaches out to communities must
take these into account. (For specific
elements of essential newborn care,
see Box on page 4).
Any program that aims to improve
newborn health and survival must
ensure that essential newborn care is
made available to all babies,
irrespective of where the baby is born.
B. Addressing specific causes of newborn death
Since asphyxia, low birth-weight/
prematurity and infections account for
around 90% of all deaths, interventions
that can deal effectively with these
causes should help reduce neonatal
deaths to a large extent.
Asphyxia and birth trauma
What is asphyxia?
Asphyxia is absent or depressed
breathing at birth. This is easily
recognized as a newborn baby who
does not cry at birth.
Birth trauma or injury, particularly to
the brain during birth, often results in
asphyxia. Hence, they are considered
together.
What causes asphyxia?Prolonged or obstructed labour.
Asphyxia is more likely to occur under
certain circumstances:
Multiple births, such as twins
The baby presenting abnormally
that is, emerging from the birth
canal in an abnormal position
First pregnancy of a woman
Short stature of the mother
Premature birth
How can asphyxia be prevented?
Some cases of asphyxia can be
prevented by careful monitoring of
labour, and timely intervention to
hasten delivery, such as by cesarean
section. This requires skilledattendance, at a hospital where
surgery is possible.
In rural homes, where most home
deliveries are attended by TBAs,
expecting close monitoring of labour
for asphyxia and quick action is
unrealistic.
Even in institutions, all asphyxia
cannot be prevented, and so personnelskilled in treatment of asphyxia must
be available at the moment of
childbirth.
How can asphyxia be treated?
When a newborn baby does not cry at
birth, it is an emergency situation.
Unless the baby can be helped to
breathe within a few minutes, the
baby s brain can be damaged by lack of
oxygen. The baby can even die.
Very few studies have investigated in detail the effectiveness of acomprehensive package of newborn care services delivered at the communitylevel. The few studies that have done so are all Indian.
A study conducted by an NGO called SEARCH in Gadchiroli district in ruralMaharashtra has shown that it is possible to train village health workers (villagewomen volunteers) to effectively reduce mortality from neonatal sepsis. Theworkers were intensively trained and supervised, and provided comprehensiveneonatal care in addition to antenatal care. The neonatal mortality rate in the
study dropped by about 62% and infant mortality by nearly half, over a periodof three years, most of the effect being due to a reduction in mortality due tosepsis. The incidence of sepsis and the mortality from sepsis were bothsubstantially reduced. The mortality from asphyxia and prematurity was alsoreduced, though less dramatically. Table 1 on page 8 shows the reduction inmortality pre and post intervention, i.e. following training of health workers indelivering neonatal care (Bang et al, 1999).
Newborn baby.
N e w b o r n
H e a l
t h ,
M o
H F W
, G o
I
-
8/8/2019 CARE Booklet B
6/16
6
When all facilities are available, such
babies can be resuscitated (see Box
below).
However, in the case of home deliveries
in rural areas:There are usually no facilities for
resuscitation.
Death or serious brain damage
occurs within minutes after birth.
The best time to refer is therefore
during or before labour if the
attendant can detect distress in a
baby still in the womb (see Box
alongside).
Since TBAs usually do not have
these skills, only the simplest ofcare can be given at home, as
described below.
Referral after a home delivery can
take time, and even if the baby
eventually survives, it may have
suffered considerable brain damage
by the time it is revived in a
hospital. Hence it is always
preferable to deliver in an
institution where facilities for
resuscitation are available.
Most deaths and disability from asphyxia
will be difficult to prevent, unless
deliveries take place in institutions able
to provide skills and equipment for
effective management of asphyxia.
However, the following steps can be
taken at all home deliveries, even if
attended by only a trained TBA:
As soon as a baby is born, it is
received in a sheet of clean, dry
cloth.
The baby is wiped dry with the
sheet of cloth. If the baby has not
cried by then, the stimulation
provided by rubbing the back and
limbs firmly with the cloth may beenough to make the baby cry.
A baby who still does not cry is
wrapped in another dry cloth to
maintain warmth, and the soles
and palms are rubbed firmly.
The baby is turned over on its side
or onto its face, which helps drain
out any liquid that is blocking its
airway in the throat or nose.
In addition, where such equipment and
training have been provided, the
attendant may take these steps:
Use a mucous sucker to suck out
any liquid from the throat of the
baby that is not crying or breathing.
Provide artificial respiration, either
tube and mask, or bag and mask,
depending on the equipment
available.
Detecting a baby in distress
When a baby is distressed inside the uterus, it becomes restless andpasses stool. The first stools, called meconium, are of a dark green color.This can be easily detected by the birth attendant when the water thatcomes out as the membranes burst is observed to be green. However,birth often occurs within minutes after passage of the water, and sothere may not be enough time to move the mother to the hospital.The distressed baby s movements may become excessively frequent orinfrequent, and the mother can often feel this. This is not alwaysreliable, but quickly reaching a hospital can help confirm suspicion.The heart rate of the baby in the womb shows characteristic patternswhen in distress. This can be reliably detected by closely monitoringthe labour. However, this is usually possible only by well-trained staffin a well-equipped hospital.Distress is not easy to detect in the case of home deliveries.
Resuscitating an asphyxiated newborn in institutions
Stimulating the baby by rubbing its back, soles or palms can get manybabies to start crying. This happens naturally when wiping a baby dryat birth.If this is not enough, the first step is to make sure that the airway(the passage for air to enter the lungs) is not blocked. A block is usuallydue to liquid and mucus, and this must be cleared by sucking it out.This requires simple equipment for suctioning, but suctioning is mosteffectively done while directly visualizing the airway with alaryngoscope.
If the baby still does not breathe, a small tube is inserted into thetrachea (windpipe) through the mouth and artificial respiration isinitiated. This requires special training and highly skilled care, which isavailable only in hospitals that specialize in neonatal care.In the absence of highly skilled personnel, artificial respiration can beprovided with a bag and mask or a tube and mask. However, this tooneeds considerable training, and is not as effective as using a tube inthe airway as described above.
What not to do:Do not hang the baby upside
down by its feet.
Do not slap the baby on its
back or chest.
Do not splash cold water on
the baby.
-
8/8/2019 CARE Booklet B
7/16
7
Low Birth Weight and Prematurity
What is low birth weight?
By convention, a baby who is less than
2.5 kg at birth is considered a low birth
weight (LBW) baby.
Most births in India occur in rural
homes, and most such babies are not
weighed at birth. Therefore, we do not
have reliable estimates of the
proportion of LBW babies. It is believed
that India (along with other South Asian
countries) has the highest proportion of
LBW babies in the world. The rates are
probably as high as 30-40%.
A baby may have low birth-weight dueto one or both of the following reasons:
Premature birth: Babies born too
early, before they have had a
chance to put on enough weight
Failure to put on adequate weight
while in the womb: Babies who
have not gained as much weight as
expected for their age. For
instance, a baby born at the end of
a pregnancy of normal duration
may weigh less than 2 kg at birth.
Such babies are said to have
A summary of what can and cannot be done for the preventionand treatment of asphyxia at the home level
What can work at the home level:Antenatal check-ups, particularly in the last three months, may detectconditions that predispose to asphyxiaEnsuring that the delivery is conducted by a trained attendantSimple stimulation of the baby to induce breathing/cryingUsing simple suction devices and equipment like a bag and maskProviding training and supervision of the birth attendants that isadequate.
What cannot work at the home level:Prevention of all or most cases of asphyxiaSophisticated resuscitation of the kind possible in institutional deliveries.Referral to institutions after birth, since it may not be effectiveenough to save lives or prevent disability.
suffered growth retardation while
in the womb (intra-uterine growth
retardation).
Some babies may be both, premature,as well as growth-retarded.
What is prematurity?
A normal pregnancy usually lasts about
40 weeks (i.e. 10 lunar or traditional
calendar months, or 9 modern calendar
months and 7 days). A pregnancy that
ends after 37 completed weeks but
before 42 completed weeks is
considered full-term . A baby born
before 37 weeks of pregnancy are
completed is considered premature or
preterm . A birth
after 42 completed
weeks is post-
term .
On an average,about 10% of all
pregnancies end in
premature births.
In general, the
more premature
the baby, the greater the risk of death
(see Table 1 on page 8).
Why is LBW dangerous?
LBW is a major contributing factor forneonatal death and birth weight is one
of the important predictors of neonatal
mortality (see Table 1 on page 8). This
is because both, premature babies and
growth-retarded babies are more likely
to die than normal babies.
Why premature babies are more likely
to die
As a baby grows inside the womb, each
organ continues to mature throughout
pregnancy. A baby who is born after 37
weeks is sufficiently mature to perform
certain critical functions that allow
them to survive on their own, with
normal care from the mother:
The ability to breath normally
The ability to suck at the breast
and swallow milk without choking
The ability to maintain a steady
body temperature even when the
outside temperature is low or high
The ability to fight infections
Babies born before completing 37
weeks of pregnancy are not sufficiently
mature to perform these functions
normally. The earlier the birth, the less
mature these body systems will be.
N e w
b o r n
H e a l
t h ,
M o H
F W ,
G o I
Low birth weight baby.
-
8/8/2019 CARE Booklet B
8/16
8
With adequate care from the family, it
is possible to maintain temperature
and to minimize infection. However,
the baby must still be able to breathe
normally, and suck and swallow milk,
in order to survive at home.
Almost all babies become sufficiently
mature to be able to perform these
critical functions independently by
about 34 weeks of pregnancy. Any baby
born after these functions mature has
a fair chance of survival even if it is
cared for at home.
Babies who are born before these
functions become mature need very
special care that is available only in
specialist neonatal care hospitals. Less
the maturity, the greater the intensity
of care needed.
Why growth retarded babies are more
likely to die
As discussed below, failure to gain
weight adequately in the womb is often
due to maternal ill-health. This affects
the baby s health as well, and such
babies are more susceptible to die from
causes such as asphyxia and sepsis, as
well as hypoglycemia and hypothermia
(which are discussed later).
What causes low birth weight?
Prematurity or a failure to gain weight
in the womb can be due to numerous
causes. The pre-pregnant nutritional
status of the mother (i.e. mother s
height and weight), as well as the
nutrition and weight gain of mothers
during pregnancy are crucial factors.
Demanding physical work, short
spacing between pregnancies and
adolescent pregnancies are all
associated with prematurity and LBW.
Smoking mothers tend to have lighter
babies.
Most of the weight gain of the baby in
the womb occurs in the last three
months of pregnancy. Maternal
conditions like toxemia (pre-
eclampsia), malaria, certain other
maternal infections and any condition
that affects the health of the placenta
adversely affects the growth of the
baby in these months.
This table illustrates that:1. The likelihood of death is more when the birth weight is less, or when the maturity is lower.2. After intervention, the greatest reductions in death rates were among newborn babies born with a low birth weight,
and with moderate prematurity (between 34 and 37 weeks). This is the group that programs are likely to affect the most.3. The proportion of premature babies, or babies with a weight less than 2 kg is likely to be around 10% (or less) of all births
this is the proportion of newborn who will need special care
TABLE 1Likelihood of death by birthweight and maturity, pre and post intervention, Gadchiroli district study, 1995-1998
Source: Adapted from Bang et al, Lancet, 1999
1995-96 (baseline) 1997-98 (after intervention)
Number of live % of births Number Number of live % of births Numbernewborns in this category dying % newborns in this category dying %
Birth Weight
< 2 kg 74 8 27 36 63 6 9 14
2-2.5 kg 246 32 9 4 258 28 4 2
>2.5 kg 417 54 1 < 1 574 62 5 1
Unknown 26 3 3 12 18 1 4 22
Gestation
37 weeks 673 88.2 14 2 801 82 11 1
Unknown 15 1.9 1 7 19 2 2 11
Total 763 100 40 5 913 100 22 2
-
8/8/2019 CARE Booklet B
9/16
9
A number of other conditions are
known to cause early labour:
Twins or multiple pregnancy
Incompetent cervix (mouth of
uterus not tight enough to hold
the growing baby)Obstetric complications such as
placenta praevia (low lying
placenta that blocks the cervix),
placental abruption (placenta
separating from the uterus before
baby is delivered)
Urinary or reproductive tract
infections in the mother.
How far can low birth-weight be
prevented? How far can labour bedelayed to prevent premature birth?
Some of these conditions, if detected
early, can be controlled to a certain
extent. However, premature labour is
difficult to prevent even in hospitals.
Even in developed countries,
prematurity is likely to remain the
leading cause of neonatal morbidity
and mortality for many years to come.
Protein and energy supplements in
pregnancy can reduce the incidence of
intrauterine growth retardation and
improve birthweight, with an average
increase of about 100 grams. Increases
in birth weight are particularly
observed in moderately and severely
malnourished mothers. A recent
community-based trial found that
supplements delivered to pregnant
women in Gambia through a primary
health care system resulted in
significant increase in mean
birthweight. This effect was particularly
marked in the hungry season, when the
rate of LBW was reduced by 33 percent.
However, particularly in the context of
home deliveries, even with the best of
antenatal care and counselling for
better nutrition, it is difficult to
reduce the proportion of LBW babies.
What can be done to help LBW babies
survive?
Low birth-weight babies born in well-
equipped and staffed institutions will
receive adequate care at the
institution. However, since a large
proportion of births in rural India still
take place in homes (or in ill-equipped
hospitals), far from institutions
capable of taking care of newborn
babies, it is important to focus on what
can be done under such circumstances.
For many such babies, it may be
difficult to have a reliable estimate of
either gestational age or birth weight,
and so even identification of low birth-
weight or prematurity may not be
easy. Based on wide-ranging
experience from community and
The relationship between maturity and birth weight
A premature baby is often LBW by definition (less than 2.5 kg), even ifit has put on weight adequately for the duration of its pregnancy. Forinstance, the average expected weight for a gestational age of 20 weeksis 300g, at 32 weeks it is 1700g and at 37 weeks it is around 2900g.Maturity of systems is linked closely to the duration of pregnancy,rather than to birth weight.Since failure to put on adequate weight in the womb is so common inIndia, it is common to find a fully mature baby weighing less than2.0 kg, and a grossly premature baby of the same weight.For any given level of maturity, a lower birth weight carries a higherrisk of death.
Weighing babies.
A n
k u r
C h i t k a r a /
C A R E I n d i a
-
8/8/2019 CARE Booklet B
10/16
10
hospital studies criteria for identifying
a baby likely to need special care are
suggested in the Box above. Depending
on feasibility in terms of complexity
that service providers can handle, other
indicators of maturity can be added.
Ideally, premature and LBW babies
would be cared for in hospitals specially
set up for such babies. However, such
special hospitals are found only in a few
large cities. Most babies born in rural
homes do not have access to these
special hospitals. In any case, it is
difficult to persuade rural families to
take sick newborn babies to these
hospitals across long distances and at
considerable cost. Until specialist
hospitals become more generally
accessible, we need a simple protocol
that can be followed by the family and
health workers to care for these LBW
babies at home. Based on the
experience of a handful of small
studies, the following steps are
suggested. They will need validationand adaptation to different settings.
A. Assessment of all newborn babies
to identify those who need special
care, and provision of simple care
at home.
a. A baby needing special care can be
identified using the criteria in the
box alongside.
b. In specialist neonatal care
hospitals, premature or weakbabies are nursed at constant
temperature and fed breast milk
or a suitable alternative by highly
skilled nurses. Strict discipline
among handlers minimizes risk of
transmitting infection to the baby.
If needed, respiration is supported
by various means. When cared for
at home, however, such equipment
and skilled nursing are not
available, but the same principles
can be followed to the extent
possible at home:
Providing adequate warmth,
preferably by placing the
baby in skin-to-skin contact
with the mother, popularly
called kangaroo mother care,
or by adequately wrapping up
in enough warm clothing.
Minimizing risk of infection
from handlers by minimizing
handling, and frequent hand-
washing. Clean birthing and
handling practices are
applicable to all newborn
babies. These practices are
particularly important in the
case of premature/LBW babies.
Frequent feeding of breast
milk, either directly from the
breast, or expressed with a
cup or spoon. Babies who
thrive well with this simplemanagement can be taken
care of at home. They will
continue to need special care
for a week or two until they
grow strong enough to feed
well and maintain their body
temperature well. They will,
however, need to be carefully
protected from infection until
many weeks later.
B. Assessment of all babies needing
special care to determine if they
cannot be cared for at home, and
referral to appropriate institutions.
Simple ways to tell which babies cannot
be taken care of at home include:
a. A baby who is unable to feed even
with a cup or spoon, because it
either chokes while feeding, or
does not have the strength even to
sip and swallow from the cup or
spoon. Such babies are probably
too premature to be fed orally, and
need much more intensive care
than is possible at home.
b. A baby who becomes sick with such
an infection cannot be cared for at
home.
Identifying the newborn inneed of extra care
(the weak newborn)
A baby with a birth weight of less than 2000 g, (if birth
weight is available). While acut-off of 2.5 kg would includeall LBW babies, babies of lessthan 2 kg are at a much higherrisk of disease and death.A baby born more than a monthbefore the expected date of delivery (if the expected dateof delivery can be determined).A baby is premature bydefinition if < 37 completedweeks. However, this is difficultto measure exactly under field
conditions.A baby who does not suckvigorously at the breast fromthe time of birth . In theabsence of birth-weight andestimate of maturity, thisindicator will detect thosebabies who definitely needspecial care.
Kangaroo mother care.
-
8/8/2019 CARE Booklet B
11/16
11
Potentially fatal infections,
or sepsis
Infections are responsible for more
than a third of deaths in the newborn
period. In the study of neonatal deaths
in Gadchiroli district of Maharashtra,52% of newborn deaths were due to
such infections.
What is sepsis?
The term sepsis is usually used to
indicate a bacterial infection.
When the immune system is not
sufficiently effective, an infection
tends to easily spread to other parts of
the body, usually through the bloodstream. This is called septicemia .
Since their immune systems are not
fully developed, newborn babies are
particularly vulnerable to septicemia
from even minor infections. The less
mature the baby, the greater the risk
of septicemia.
Tetanus is a specific, highly fatal
bacterial disease that is entirely
preventable using tetanus toxoid
vaccine during pregnancy, and by
ensuring clean delivery and cord care.
Tetanus does not cause septicemia.
What is the source of the bacteria in
potentially fatal infections?
The source of bacteria causing sepsis is
usually either the mother or a care-
giver. Table 2 on page 12 summarizes
the likely routes of infection.
How can infection be prevented?
Most infections can be prevented by
following these simple procedures:
Use of clean materials (cord-tie,
blade, cloth) at childbirth.
Close attention to adequate hand-
washing at birth (keeping nails
short and clean, use of soap and
water in enough quantity,
scrubbing adequately, and air-
drying hands).
Proper cord care until the cord
falls off (keeping cord stump clean
and dry after birth, applying
nothing and leaving it open), and
appropriate care of the umbilicus
until it is dry (applying nothing
and leaving it open).
Minimal handling after birth
(restricting the number of persons
who handle the baby) and
handling the baby only when
necessary.
Adequate hand-washing each
time before handling the baby
for several weeks after birth.
Avoidance of all feeds other than
breast milk (until the baby is
about six months old).
A summary of what can and cannot be done to prevent and treatLBW and prematurity at the home level
What can work at the home level:Adequate antenatal care, particularly in the last three months,including:o adequate diet and rest, may increase birth weighto regular check ups to detect potential causes of LBWo malaria chemoprophylaxis and treatment where indicatedReferral of premature labour for institutional deliveryRecognition of weak babies who can be cared for at home andadequate care of such weak babies, including ensuring warmth(kangaroo mother care), support for breastfeeding, cleanliness, earlyidentification and management of illnessRecognition of premature babies who are too premature to be caredfor at home and referral of such babies to appropriate institutions
What cannot work at the home level:Prevention of most premature birthsCare of premature babies who cannot safely swallow milk.
Five cleans.
-
8/8/2019 CARE Booklet B
12/16
12
If the baby is not born for more than 6
hours after the membranes have
ruptured, antibiotics may help reduce
the risk of infection. Such a mother
usually needs referral to an institution
for completing the delivery.
After birth, breastfeeding the baby
immediately reduces the risk of serious
infection, since breast milk, especially
the first milk or colostrum , is rich in
immune components that are
extremely useful in fighting infection.
Breast milk itself is free of disease-
causing bacteria.
Tetanus toxoid vaccine administered to
the mother before or during pregnancy
can effectively eliminate chances of
tetanus in the newborn baby.
With the simple measures outlined
above, a large proportion of infections
can be prevented. However, some
babies will still acquire infections, and
such babies can be treated if
recognized and referred early.
How do we recognize severe
infections in a newborn baby?
The symptoms of infection that are
common in older children, like fever,
pain and swelling, or typical symptoms
of specific infections like meningitis
(infection of the coverings of the
brain), are often absent in newborn
babies. This is mainly because the
immune system is not mature enough
to fight infections as adults do, and to
produce these symptoms.
Even where specific symptoms of
serious infections like pneumonia or
meningitis are seen, infection tends to
spread so rapidly that in a matter of a
few hours, the specific symptoms may
disappear or get replaced by general
symptoms of septicemia.
Based on the findings of the
Maharashtra study on neonatal deaths,
the authors have recommended a set of
criteria to be used for suspecting
neonatal sepsis and referral (See Box on
page 13).
Specific symptoms may be seen in some
cases:
Pneumonia will cause increased
respiratory rate, and in-drawing of
inter-costal spaces (spaces
between ribs) during rapid
breathing.
Meningitis may cause vomiting or
convulsions and a bulging
fontanelle (the soft spot at the
center of the head in newborn
babies).
Neonatal tetanus makes the
baby s body spasm on touch or on
crying, and the jaw to become
stiffand locked . Unlike the
convulsions of meningitis, the baby
Causes How Infection is Transmitted
A. Non intact membranes In the womb, the baby floats in water inside a sac made of thin membranes.Bacterial infection of the baby in the womb is rare in the presence of intactmembranes. When membranes rupture but birth is delayed (by more than 6
hours), the baby has a high chance of being infected.
B. Childbirth and delivery Infection acquired during childbirth can come from the mother s reproductivetract, the unclean hands of the person assisting the delivery, or an uncleanpiece of equipment.
C. Immediate postnatal period The baby can become infected at any time after birth until the baby becomesmore resistant to infection. Such infections can be transmitted by touch,feeds, or air; invariably the source of infection is either the mother or otherhandlers.
D. Unhygienic practices Cowdung or other unclean substances applied to the umbilical stump canlead to serious infections, including tetanus.
E. Inadequate facilities Babies born in hospitals with inadequate facilities or inadequately trained
staff for the conduct of clean deliveries, run the risk of potentially fatalinfections from other patients.
The bacteria affecting newborns in developing countries like India include Pneumococcus, E. coli, Staphylococcus and Clostridium tetani(organism causing tetanus). However in the developed world, group B Streptococcus is the major organism causing neonatal sepsis.
TABLE 2: Likely routes of infection
-
8/8/2019 CARE Booklet B
13/16
13
usually remains awake during a
spasm, and continues to cry.
Umbilical abscess can present as
a red, painful swelling of the
abdominal wall around the
umbilicus, and needs immediatetreatment. However, the more
common symptoms of discharge of
a pus like liquid from the
umbilical stump are usually not
serious, in the absence of swelling.
Gastrointestinal infections can
present with diarrhea and vomiting.
Diarrhea is often difficult to
distinguish from the normally high
frequency of stools that a normal
newborn passes, and normalregurgitation of milk can be easily
mistaken for vomiting. Hence,
these are not reliable signs of
serious disease.
Skin conditions appearing to be
pustules are common in the first
few days after birth. Most of these
are not infections, and even true
pustules do not often lead to
serious disease.
Eye infections usually present as
a small discharge from the corners
of the eyes, and are usually
benign. Serious eye infections
present as sudden red swellings of
the eyelids, with pus discharge,and need emergency treatment to
save the eyes.
However, none of these symptoms is
necessary for suspecting sepsis.
What is the treatment of potentially
fatal infections?
The only confirmative test for
septicemia is a positive blood culture.
Since it usually takes at least 48 hoursto get a blood culture result, and since
death can occur within a few hours
after onset of symptoms if untreated,
treatment is begun immediately on
suspicion of septicemia or other major
infection, without waiting for
laboratory test results.
Irrespective of the source or site of
infection, all serious infections are
usually treated as septicemia. Two
antibiotics administered parenterally
(as injections) in recommended doses
for at least one week is the minimum
treatment. In addition, depending on
the condition of the baby, othersupportive treatment may be needed.
Since this treatment needs well-trained
personnel, it is best administered in a
hospital having staff trained in treating
serious neonatal disease.
Tetanus is very difficult to treat, even
in the best of institutions, and most
babies will probably die before
reaching such institutions.
Where can neonatal sepsis be treated?
Only those hospitals that have trained
staff and equipment to handle serious
neonatal illnesses can reliably treat
sepsis. At present, most areas in rural
India do not have ready access to such
centers.
The Government of India and the
National Neonatology Forum are taking
steps to increase the availability of
centers where such treatment can be
provided.
Until reliable centers are established,
referral of suspected sepsis will
continue to be at the nearest and best
centers that the family can afford. It is
therefore important to use a set of
criteria for referral that does not
excessively over-diagnose septicemia.
Other causes of neonatal death
Birth defects
Since preventable deaths are not
common in developed countries, it is
birth defects that are the major cause
of neonatal deaths in these countries.
Criteria to be used for suspecting septicemiaat the community level
1. A baby who is feeding poorly, or has stopped breastfeeding, after earlierfeeding well (i.e. any baby whose vigor of feeding has deteriorated).
2. A baby who is drowsy/unconscious (or inactive or lethargic after beingnormally active earlier). This is a baby, who is difficult to awaken, or ababy whose limbs are limp or loose , or a baby who does not cry aswell as before.
3. A baby who is cold to touch.4. A baby who is breathing very fast. Newborn babies normally breathe
quite fast. Fast breathing without pause, or a breathing rate greaterthan 60 per minute is likely to be pneumonia.
5. A baby who has chest in-drawing while breathing. This is often expressedas seeing pits in the lower chest wall, and locals may have a specificexpression for describing this sign of pneumonia.
The presence of even one of these signs is sufficient reason for suspectingsepsis.
-
8/8/2019 CARE Booklet B
14/16
14
In the developing countries, however,
they cause less than 10% of newborn
deaths. There are numerous causes of
congenital or birth defects, a few of
which are preventable:
Neural tube defects that show upas soft, fluid-filled swellings on
the back over the spine often
associated with brain defects and
paralysis. These are partly
preventable by folic acid
supplementation for the mother in
the period around conception.
Iodine deficiency disorders,
including different degrees of
mental retardation. These are
preventable by regular maternalintake of iodized salt.
Congenital rubella syndrome,
which can cause severe eye, heart
and other organ defects if the
mother gets rubella (a mild viral
infection, also called German
measles) during early pregnancy.
This is preventable by rubella
immunization of the mother well
before pregnancy.
Hypothermia
Hypothermia is defined as a core body
temperature of less than 36o
C. Human
adults can maintain a steady body
temperature of around 37o
C,
irrespective of what the external
environmental temperature is. For
various reasons, newborn babies are
unable to do this effectively, and the
less mature a baby, the less it is able to
do so. Once body temperature drops,
the baby becomes more prone to
infections and other metabolic
disturbances. Unless quickly corrected,
death can occur. It is much easier to
prevent hypothermia, using simple
ways of keeping the baby warm, than to
treat it. It should be noted that it is
probably more common to find
hypothermia as a consequence of sepsis
or asphyxia, rather than as a cause.
Hypoglycemia
Hypoglycemia is defined as blood sugar
less than 70 mg/100 ml. Severe
hypoglycemia increases the risk of
death, even moderate hypoglycemia
Criteria to identifyinstitutions for referral of the
weak or sick newborn
1. Availability of trained
pediatrician/neonatologist
at the hospital
2. Availability of basic
equipment for neonatal care
such as a radiant warmer.
3. Availability of nursing staff
trained in neonatal care
4. Distance from village and
access to transportation
5. Cost of care
A summary of what can and cannot be done at home to preventor treat sepsis
What can work at the home levelTetanus toxoid vaccine to the mother before and during pregnancyAttendance by a trained birth attendant who follows procedures forclean delivery *Early and exclusive breastfeedingClean cord and umbilical careMinimal handl ingClean handling by a few care-givers, including frequent handwashingSuspicion of sepsis using easily understood danger signs, and referral tothe best available institution for treatment
What cannot work at the home levelUse of appropriate antibiotics for treatment of suspected sepsis, unlessintensive training of health workers is possibleTreatment of tetanus
* Clean hands, clean surface, clean blade, clean cord tie, and clean cord
stump, often referred to as the 5 cleans
may cause long term reduction in
intelligence. Hypoglycemia often
occurs as a result of other neonatal
conditions such as sepsis or asphyxia.
Hypoglycemia can be prevented in the
community setting by early, exclusive
and frequent breastfeeding.
Jaundice
In the neonatal period jaundice
(yellow colour of skin) is common.
In most cases, it is mild, appears
around the third day after birth, and
disappears before the end of the first
week. This is called physiological
jaundice, and is one consequence of
the many adjustments that a baby has
to make when shifting from life within
the womb, to an independent
existence outside. This does not need
any treatment. In a very few cases,
babies can have deep yellow
jaundice, that can be easily seen all
over the body. Such severe jaundice
is usually because of some infection
or disease, and needs urgent
treatment in a specialist hospital.
-
8/8/2019 CARE Booklet B
15/16
15
The National Population Policy of 2001 recognizes the link between high infant mortality and excessive population growth.
The Policy commits the nation to a reduction of the infant mortality rate to under 30 per 1000 live births by the year 2010.This necessitates a rapid reduction in neonatal deaths which form a major component of infant mortality.
The Policy also aims to achieve 80% deliveries in institutions and 100% deliveries by trained personnel by the year 2010.
Newborn care at district and sub-district levels is being operationalized by the Ministry of Health and Family Welfare withthe technical assistance of the National Neonatology Forum.
What interventions are likely to be feasible and effectivein reducing neonatal mortality at the community level?
A. Adequate antenatal care:1. Tetanus toxoid vaccine, one or two doses, depending on the previous
vaccination status2. Adequate diet and rest
3. Iron and folate supplements4. Regular check-ups and appropriate follow up (using home visits) on
detection of problems5. Planning for birth, including for emergencies at childbirth6. Recognition of danger signs in the mother and referral to an appropriate
institution
B. Appropriate delivery care:1. Delivery according to plan2. Attendance by a trained TBA or nurse3. Use of disposable delivery kit / 5 cleans
C. Essential care for all newborns:1. Ensuring breathing with simple interventions2. Ensuring adequate warmth3. Ensuring adequate nutrition4. Preventing infections
D. Special care for the premature/weak newborn:1. Recognition of a premature/weak baby who can be taken care of at home2. Extra warmth, more frequent feeds, feeding expressed breast milk with
a cup if need be, extra care to prevent infections3. Kangaroo mother care wherever acceptable
E. Recognition and referral of suspected septicemia1. Using easily recognizable danger signs for suspecting sepsis2. Immediate referral to an appropriate institution.
Newborn health is a high priority of the Government of India
Further Reading
1. Bang AT, et al. Effect of home-basedneonatal care and management of sepsison neonatal mortality: field trial in ruralIndia, Lancet 1999; 354:1955-1961.
2. National Family Health Survey (NFHS-2),India; 1998-1999.
3. Newborn Health Key to Child Survival.Present scenario, current strategies andfuture directions for Newborn Health inIndia, Child Health Division, Departmentof Family Welfare, Ministry of Healthand Family Welfare, Government of India; 2001.
4. Paul VK. Newborn care in India Apromising beginning, but a long way togo. Newborn Care in the South-East AsiaRegion Current Status and Priorities.Report of the Regional Expert GroupMeeting, Nov 16-17; 1998.
5. Pratinidhi A, Shah U, Shrotri A, Bodhani N.Risk-approach strategy in neonatal care.Bulletin of the World Health Organization1986; 64:291-297.
6. Saving Newborn Lives. State of theWorld s Newborns . Washington, DC, Savethe Children Federation-US; 2001:1-49.
7. Stoll BJ. The global impact of neonatalinfection. Clinical Perinatol 1997;24:1-21.
8. The Healthy Newborn: A ReferenceManual for Program Managers. The CARE/
CDC Collaborative Health Initiative; 2001.
-
8/8/2019 CARE Booklet B
16/16
16












![Homework Booklet [B]](https://static.fdocuments.in/doc/165x107/55cf926d550346f57b9672b7/homework-booklet-b.jpg)


