CARDIOVASCULAR RESPONSE TO EXERCISE · creased cardiac output. The increased venous return is aided...
17
277:S244-S259, 1999. Advan in Physiol Edu M. Harold Laughlin CARDIOVASCULAR RESPONSE TO EXERCISE You might find this additional info useful... 2 other HighWire hosted articles This article has been cited by [PDF] [Full Text] [Abstract] , December 1, 2006; 291 (6): H2735-H2742. Am J Physiol Heart Circ Physiol Satoshi Koba, Zhaohui Gao, Jihong Xing, Lawrence I. Sinoway and Jianhua Li Sympathetic responses to exercise in myocardial infarction rats: a role of central command [PDF] [Full Text] [Abstract] , October 1, 2007; 293 (4): H2335-H2343. Am J Physiol Heart Circ Physiol Satoshi Koba, Jihong Xing, Lawrence I. Sinoway and Jianhua Li Differential sympathetic outflow elicited by active muscle in rats including high resolution figures, can be found at: Updated information and services http://advan.physiology.org/content/277/6/S244.citation can be found at: Advances in Physiology Education about Additional material and information http://www.the-aps.org/publications/advan This infomation is current as of July 19, 2011. Physiological Society. ISSN: 1043-4046, ESSN: 1522-1229. Visit our website at http://www.the-aps.org/. the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyright © 1999 by the American and in the broader context of general biology education. It is published four times a year in March, June, September and December by is dedicated to the improvement of teaching and learning physiology, both in specialized courses Advances in Physiology Education on July 19, 2011 advan.physiology.org Downloaded from
Transcript of CARDIOVASCULAR RESPONSE TO EXERCISE · creased cardiac output. The increased venous return is aided...

277:S244-S259, 1999.Advan in Physiol EduM. Harold LaughlinCARDIOVASCULAR RESPONSE TO EXERCISE
You might find this additional info useful...
2 other HighWire hosted articlesThis article has been cited by
[PDF] [Full Text] [Abstract]
, December 1, 2006; 291 (6): H2735-H2742.Am J Physiol Heart Circ PhysiolSatoshi Koba, Zhaohui Gao, Jihong Xing, Lawrence I. Sinoway and Jianhua LiSympathetic responses to exercise in myocardial infarction rats: a role of central command
[PDF] [Full Text] [Abstract], October 1, 2007; 293 (4): H2335-H2343.Am J Physiol Heart Circ Physiol
Satoshi Koba, Jihong Xing, Lawrence I. Sinoway and Jianhua LiDifferential sympathetic outflow elicited by active muscle in rats
including high resolution figures, can be found at:Updated information and services http://advan.physiology.org/content/277/6/S244.citation
can be found at:Advances in Physiology Educationabout Additional material and information http://www.the-aps.org/publications/advan
This infomation is current as of July 19, 2011.
Physiological Society. ISSN: 1043-4046, ESSN: 1522-1229. Visit our website at http://www.the-aps.org/.the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyright © 1999 by the Americanand in the broader context of general biology education. It is published four times a year in March, June, September and December by
is dedicated to the improvement of teaching and learning physiology, both in specialized coursesAdvances in Physiology Education
on July 19, 2011advan.physiology.org
Dow
nloaded from

CARDIOVASCULAR RESPONSE TO EXERCISE
M. Harold Laughlin
Department of Veterinary Biomedical Sciences, Department of Physiology, and DaltonCardiovascular Research Center, University of Missouri, Columbia, Missouri 65211
This article is intended for instructors who teach cardiovascular physiology. In our
physiology course exercise physiology is used as a tool to review and integrate
cardiovascular and respiratory physiology. It is assumed that the students already
have mastered the fundamentals of cardiovascular and respiratory physiology. Because
this paper is part of a cardiovascular refresher course, I have deleted much of the
respiratory physiology. The objectives of this presentation are for the student to 1)
understand the relationship between maximal oxygen consumption and endurance
during sustained exercise and be able to define ‘‘maximal oxygen consumption’’; 2)
understand the determinants of maximal oxygen consumption; 3) understand the effects
of dynamic exercise on the cardiovascular system and mechanisms for these effects; 4)
understand the relationships between exercise intensity and major cardiorespiratory
parameters, including heart rate, cardiac output, blood flow distribution, left ventricular
stroke volume, arterial pressures, total peripheral resistance, and arterial and venous
blood oxygen content; 5) be able to compare and contrast the cardiovascular effects of
dynamic and isometric exercise in man and the mechanisms responsible for the major
differences; and 6) be able to apply knowledge of the cardiovascular effects of exercise to
understanding causes of cardiovascular symptoms in disease and in diagnosis of disease
states. This material contains many areas that stimulate discussion with students and
allow exploration of concepts that are challenging for the student. This give and take
between teachers and student is difficult to summarize in an article of this sort.
Therefore, subjects that in my experience often stimulate questions and discussion with
the students are indicated in the text.
AM. J. PHYSIOL. 277 (ADV. PHYSIOL. EDUC. 22): S244–S259, 1999.
Dynamic exercise produces the most striking burdenon the cardiorespiratory systems of any of the variousstresses encountered in normal life. The study ofexercise physiology provides an excellent method toimprove understanding of how the circulatory andrespiratory systems respond and interact. Exercisestress is also used clinically to evaluate and quantify theseverity of cardiovascular and/or respiratory disease.
Most of the cardiorespiratory effects of exercise arerelated to supplying adequate oxygen and nutrients tothe working muscles. This task becomes more difficult
when the exercise is performed in a hot environment.In this lecture we will only consider exercise in athermal-neutral environment. There are many formsof physical activity that can be considered as exercise.These can be grouped into two general types ofexercise: dynamic exercise (walking, running, cy-cling, and swimming) and isometric exercise. We willconsider the cardiovascular effects of these two gen-eral types of exercise separately. In dynamic exercisethere is a linear relationship between oxygen consump-tion and exercise intensity up to the maximal amountof oxygen a subject can consume.
A P S R E F R E S H E R C O U R S E R E P O R T
1043 - 4046 / 99 – $5.00 – COPYRIGHT r 1999 THE AMERICAN PHYSIOLOGICAL SOCIETY
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S244
on July 19, 2011advan.physiology.org
Dow
nloaded from

DETERMINANTS OF MAXIMAL OXYGENCONSUMPTION IN DYNAMIC EXERCISE
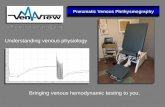
Figure 1A illustrates the time course of changes inoxygen consumption from initiation of exercise. Atthe onset of dynamic exercise, oxygen consumptionbegins to increase, continues to increase over the firstminute of sustained exercise, and then plateaus as theoxygen uptake and transport are increased sufficientlyso that oxygen consumption becomes matched todemand of the tissues. At the end of the exercise boutthere is a gradual decrease in oxygen consumptionduring recovery. The excess postexercise oxygenconsumption, above resting baseline oxygen consump-tion, observed during recovery has been referred to as‘‘oxygen debt.’’ In Fig. 1B, left, the time course ofchanges in oxygen consumption from initiation ofexercise is illustrated for six different workloads. InFig. 1B, right, the relationship between steady-stateoxygen uptake and exercise intensity obtainedfrom these data is shown. Note that as exerciseintensity increases, oxygen consumption (measuredat the plateau) increases until maximal oxygen con-sumption is reached. Maximal oxygen consumption isreflected as the point at which there is no furtherincrease in oxygen uptake despite further increases inworkload. When workload exceeds intensity thatproduces the subject’s maximum oxygen consump-tion, the increased workload is possible becauseenergy is provided by nonaerobic processes, whichresults in a rapid buildup of lactic acid and a pro-longed increase in oxygen consumption during recov-ery (Fig. 1C).
Figure 2 presents data for oxygen consumption plot-ted as a function of exercise workload for normalsubjects and for subjects who were sedentary, condi-tioned, or highly trained athletes. Note that the levelof physical conditioning influences the magnitude ofmaximal oxygen consumption; sedentary humans havethe lowest maximal oxygen uptake, and enduranceathletes have the greatest (Fig. 2). What are the factorsin the cardiovascular system that contribute to thedifferences in maximal oxygen consumption seen invarious human subjects?
Determinants of maximal oxygen consumption.There are several important determinants of maximaloxygen consumption that can limit exercise perfor-
mance in health and disease. In this lecture we willfocus on cardiovascular determinants of maximaloxygen consumption. The oxygen Fick equation isone useful way to summarize these determinants:V̇O2 5 CO(CaO2
2 CvO2), where V̇O2 is oxygen con-
sumption (l/min), CO is cardiac output (l/min), CaO2is
arterial blood oxygen content, and CvO2is mixed
venous blood oxygen content. Let us consider theeffects of exercise on each of these determinants ofoxygen consumption.
The relationship between cardiac output and exerciseintensity is similar to that shown for oxygen consump-tion as illustrated in Fig. 2, reflecting the dominantrole of cardiac output as a determinant of maximaloxygen consumption. Cardiac output is determinedby heart rate and stroke volume. As is true for oxygenconsumption and cardiac output, there is a linearrelationship between heart rate and exercise intensityup to maximal heart rates. [At this point I encouragethe students to plot cardiac output and heart rate asfunctions of exercise intensity on Fig. 2. It is importantthat they appreciate the tight coupling between theseparameters and exercise intensity.]
The other major determinant of cardiac output, strokevolume, is determined by the difference betweenend-diastolic and end-systolic volumes. [It is oftennecessary to review the determinants of end-diastolicand end-systolic volumes at this point in the lecture:heart rate, contractility, preload, afterload, ejectiontime, etc. You can tell from the reaction of thestudents if they understand the determinants of ven-tricular stroke volume.] The major causes of increasedstroke volume during exercise in humans are in-creased myocardial contractility and increased venousreturn to the heart. Contractility increases with increas-ing heart rate. This allows greater ejection of blood atthe end of systole and shortens systole, allowing moretime for diastolic filling of the ventricles.
The relationships between exercise intensity and 1)stroke volume, 2) end-systolic volume, and 3) end-diastolic volume are different when exercise is per-formed in the supine posture versus exercise in theupright posture, as illustrated in Fig. 3. These differ-ences are largely the result of the effects of the force ofgravity on venous return. During dynamic exercise,venous return is increased in proportion with in-
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S245
on July 19, 2011advan.physiology.org
Dow
nloaded from

creased cardiac output. The increased venous returnis aided by a redistribution of blood flow and venousvolumes from viscera to active skeletal muscle and bythe effects of the muscle pump and the respiratorypump on venous return.
Another major determinant of oxygen consumption isthe difference between the arterial and venous oxy-gen contents (CaO2
2 CvO2) (i.e., the amount of
oxygen from each ml of blood transported to andconsumed by the tissue). Arterial oxygen content is
FIG 1.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S246
on July 19, 2011advan.physiology.org
Dow
nloaded from

determined by arterial oxygen carrying capacity (hema-tocrit) and by the ability of the respiratory system toload oxygen in the pulmonary capillaries. As illus-trated in Fig. 4, arterial oxygen carrying capacity andcontent increase slightly with increasing exerciseintensity in humans. Arterial oxygen carrying capacityis increased because of increased arterial hematocritresulting from splenic constriction. The increase inhematocrit produced by this mechanism is muchgreater in other, more athletic animals such as horsesand dogs, in which hematocrit can reach 60% (restinghematocrits are similar to those for humans) duringintense exercise. [I believe it is beneficial to presentdata for arterial oxygen content of the horse duringexercise and review the importance of hematocrit andhemoglobin content in determination of oxygen carry-ing capacity of blood. It is also beneficial to ask thestudents to consider what effect anemia will have onexercise capacity.]
The huge increase in (CaO22 CvO2
) observed duringintense exercise is primarily the result of decreasedmixed venous oxygen content. Mixed venous oxygen
content decreases with increasing exercise intensity(Fig. 4). The decrease in mixed venous oxygen con-tent during exercise is primarily the result of redistribu-tion of cardiac output from tissues that extract smallamounts of oxygen, such as the liver and kidney, totissues that extract large amounts of oxygen, such ascardiac and active skeletal muscle. The data in Fig. 5illustrate this effect. At rest, 20–30% of cardiac outputis distributed to cardiac and skeletal muscle. Theoxygen content of blood in the coronary veins andveins draining active skeletal muscle is very low (2–4vol%). During maximal exercise, ,95% of total cardiacoutput is going to the heart and active skeletal muscle(Fig. 5), and as a result, 95% of venous return comesfrom muscle tissue where venous oxygen content isvery low. Thus, with increasing exercise intensity, therelative amount of venous blood returning to the heartfrom active striated muscle increases so that mixedvenous oxygen content decreases as shown in Fig. 4.With this review of the determinants of maximaloxygen consumption as background, let us considerthe cardiovascular effects of dynamic exercise in moredetail.
FIG. 2.The relationship between exercise intensity and oxy-gen uptake is similar in human subjects with differentlevels of physical conditioning, but their maximaloxygen uptakes are quite different. Values for oxygenconsumption are expressed in l/min (left) andml.min21.kg21 (right). [Reprinted from Rowell (7)with permission.]FIG. 1.
Oxygen consumption (O2 uptake) as a function of timeduring and after steady-state, dynamic exercise. A: Withinitiation of steady-state exercise (time 0), oxygen uptakeincreases over the first 1–2 minutes and levels off at asteady-state value. During the 1st minute of exercise, oxygenuptake does not match oxygen demand, resulting in anoxygen deficit (crosshatched area, upper left). During theplateau, oxygen demand of the exercise is matched tooxygen supply. During recovery, there is a gradual decreasein the oxygen uptake down to resting levels. The excessoxygen consumed during recovery (crosshatched area, lowerright), above resting values, has been called the oxygen debt.B: increases in exercise intensity modify the time course ofchanges in oxygen uptake and the steady-state amount ofoxygen uptake (left). Oxygen uptake at 5 minutes of exerciseis plotted as a function of exercise intensity in watts (right).Note that when exercise intensity was increased from 250 to300 W, oxygen uptake did not increase. The increasedworkload was fueled by anaerobic processes (C). C: Whenexercise intensity produces an oxygen demand that exceedsthe subject’s maximal oxygen consumption (in this case,when exercise intensity was 300 W), anaerobic processesprovide the needed energy. The portion of the exerciseoxygen requirement that cannot be supplied by aerobicmetabolism is illustrated above the maximal oxygen con-sumption (V̇O2max; shaded area). Note that recovery oxygenconsumption is elevated above resting for a longer period oftime. [Modified from Astrand and Rodahl (1) with permis-sion.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S247
on July 19, 2011advan.physiology.org
Dow
nloaded from

FIG. 3.Ventricular volumes at rest and as a function of exercise intensity insupine and upright postures. Note that end-diastolic volume in-creases during exercise. Also, in the upright posture, end-systolicvolume decreases with increasing exercise intensity. R, rest; exerciseintensities were mild (1), moderate (2), and peak (Pk). Values aremeans 6 SE. [Reprinted from Rowell (7) with permission.]
FIG. 4.Arterial and venous oxygen contents and arterial oxygen carrying capacityplotted as a function of exercise intensity, reflected in measurements ofoxygen uptake. Mean values for 5 male (left) and 5 female (right) subjects arepresented. [Reprinted from Astrand and Rodahl (1) with permission.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S248
on July 19, 2011advan.physiology.org
Dow
nloaded from

CARDIOVASCULAR EFFECTS OF DYNAMICEXERCISE
As described above, heart rate, cardiac output andoxygen consumption all increase linearly with exer-cise intensity up to maximal levels. Dynamic exercisealso alters other key cardiovascular parameters. Dy-namic exercise has modest effects on arterial bloodpressures. As illustrated in Fig. 6, mean and systolicblood pressures increase with increasing exerciseintensity. When dynamic exercise is performed withthe arms, the magnitude of increases in arterial pres-sure are ,10% greater than those seen with the legexercise shown in Fig. 6.
In contrast to most other conditions under whicharterial blood pressure is increased, the increase inblood pressure observed during dynamic exercise isnot the result of increased total peripheral resistance.Indeed, during dynamic exercise at maximal levels,total peripheral resistance is less than one-half its
value at rest. [At this point I encourage the students toplot total peripheral resistance as a function of oxygenconsumption on Fig. 2. It is common for them toassociate vasoconstriction in the viscera with in-creases in arterial pressure and be confused.] Thedecrease in total peripheral resistance is the result ofdecreased vascular resistance in skeletal muscle vascu-lar beds, leading to increased blood flow. The increasein blood flow to cardiac and skeletal muscle producedby exercise is called exercise hyperemia. Providingadequate cardiac output to support exercise hyper-emia is the primary driving force for most of thecardiovascular effects of dynamic exercise. There arefive important features of skeletal muscle exercisehyperemia.
Important features of exercise hyperemia. Thefirst major determinant is the magnitude of the re-sponse. As illustrated in Fig. 5, there is simply a hugeamount of blood flowing through skeletal muscleduring high-intensity exercise. Note that cardiac out-put increases nearly sixfold and that all of this in-creased cardiac output is going to skeletal muscle.
FIG. 5.Cardiac output and distribution of cardiac output toskeletal muscle (muscle), heart, visceral tissues, andother tissues of miniature swine as a function ofexercise intensity, reflected in measurements of oxy-gen consumption. Note that with increasing intensityof exercise the portion of cardiac output distributed toskeletal muscle increases, whereas the amount ofcardiac output distributed to viscera decreases. [Re-printed from Laughlin et al. (4).]
FIG. 6.Systolic, mean, and diastolic arterial pressures ofhuman subjects graphed as a function of exerciseintensity (bicycle exercise), reflected in measure-ments of oxygen consumption. V̇O2max, maximal oxy-gen consumption. Note that with increasing intensityof exercise, systolic and mean arterial pressures in-crease. Values are means 6 SE for systolic and diastolicpressures. [Reprinted from MacDougall (5) with per-mission of Futura.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S249
on July 19, 2011advan.physiology.org
Dow
nloaded from

Indeed, blood flow is also redistributed away fromvisceral tissues to active skeletal muscle (1, 6, 7).Similar changes in muscle blood flow, cardiac output,and its distribution occur in most mammals (4). Bloodflow is not uniformly distributed within the skeletalmuscles during locomotory exercise; rather, the pat-tern of blood flow, as a function of exercise intensity,is not the same for different muscle tissue. Blood flowdecreases in white skeletal muscle whereas it in-creases in red muscle of animals during exercise atlow intensity. In contrast, during sprinting, blood flowincreases even in the white skeletal muscle. However,during sprinting, the magnitude of the increase inblood flow is much greater in red muscle than inwhite. It seems likely that similar patterns of bloodflow distribution within and among muscles are pres-ent in humans during locomotory exercise.
How do these dramatic changes in muscle blood flowoccur during exercise? To answer that question, we needto consider the primary forces that cause the movementof fluid through tubes. The force that causes fluid to movethrough a tube, pipe, or blood vessel is a pressuregradient. In the vascular system the pressure gradient ismost often in the form of the difference between arterialpressure and venous pressure. The second major determi-nant of blood flow is vascular resistance to flow throughthe vascular tree (tubes). The primary cause of increasedblood flow to the active muscle is a decrease in vascularresistance. Vascular resistance is determined primarily bythe caliber (radius) of resistance arteries and arterioles,which is controlled by the contraction of vascular smoothmuscle in the walls of these arteries. Thus the third featureof exercise hyperemia is that it occurs because of dramaticincreases in vascular conductance (decreased vascular
FIG. 7.Recordings of blood pressure, limb blood flow, and conductance as a function of time for a dog at rest and duringdynamic exercise. Note that limb blood flow and conductance increased at the initiation of exercise at 6 miles/h.Note the rapid increase in blood flow that occurs at the initiation of exercise. As shown, prazosin (0.1 mg; arrow)was administered (intra-arterially unilaterally to the experimental limb) at 2 minutes of exercise to blocka1-adrenergic receptors, providing evidence of a1-adrenergic vasoconstriction during exercise. [Reprinted fromBuckwalter et al. (2) with permission.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S250
on July 19, 2011advan.physiology.org
Dow
nloaded from

resistance) mediated by relaxation of vascular smoothmuscle in the resistance arteries and arterioles feeding theactive skeletal muscle.
The fourth important feature of exercise hyperemia isthe fact that blood flow to active striated muscleincreases in a linear fashion with increasing oxygenconsumption. Although the relationship is not as tightat very low oxygen consumption levels, in the skeletalmuscles of conscious animals performing exercise itappears that blood flow is linearly related to oxygenconsumption. This relationship is part of a host ofevidence that metabolic rate of muscle plays a key rolein control of muscle blood flow during exercise (4).
The fifth and final feature of exercise hyperemia inconscious subjects is the rapid onset of the increasesin blood flow associated with the initiation of exer-cise. For example, Buckwalter et al. (2) measuredblood flow and conductance in the iliac arteries ofdogs during the transition from rest to exercise. Figure7 presents data which illustrate the rapid increase inblood flow that occurs at the time the dogs begin to
exercise. Blood flow increases with the first step andreaches a plateau within 3–5 seconds (Fig. 7).
Mechanisms for exercise hyperemia. It is gener-ally believed that exercise hyperemia is a local phenom-enon. Perhaps the strongest evidence in support ofthis notion is the fact that isolated, perfused skeletalmuscle preparations exhibit exercise hyperemia. In anintact subject, central control systems are superim-posed on the local vascular control processes dis-cussed below. Thus exercise hyperemia appears to beprimarily a local event that is modulated by centralcardiovascular control processes.
Blood flow to skeletal muscle is determined by theinteractions among perfusion pressure, extravascularmechanical effects of muscle contraction, and the caliberof resistance vessels. Thus, during high intensities ofexercise, the increase in mean arterial pressure contrib-utes to the increase in skeletal muscle blood flow.
During contraction of both cardiac and skeletal muscle,extravascular mechanical effects of contraction in-
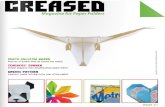
FIG. 8.Illustration of muscle pump effect on venous return and muscle blood flowto active muscle tissue. A: hemodynamic conditions for a skeletal muscle oflower limb of a subject in upright posture, at rest. DP, change in pressure.B: effects of muscle contraction on vasculature. Muscle contraction forcesblood out of venous segments, increasing venous driving pressure towardthe heart, and blocks arterial inflow. C: conditions believed to existimmediately after muscle contraction. Note that pressures in small veinsfall to zero and that, because of venous valves, refilling must occur from thearterial system through the capillary bed. The net effect of the muscle pump isto increase driving pressure for blood flow through muscle and to enhancevenous return to the heart. [Reprinted from Rowell (6) with permission.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S251
on July 19, 2011advan.physiology.org
Dow
nloaded from

crease resistance to blood flow so that blood flowceases during contraction. However, with the rhyth-mic contractions of skeletal muscle associated withdynamic exercise, the ‘‘muscle pump effect’’ appearsto increase blood flow during dynamic exercise (3, 4,6, 7). As illustrated in Fig. 8, the interactions ofcompression of the small veins produced by musclecontraction and the venous valves facilitate venousreturn of blood to the heart and perfusion of themuscle tissue (3, 6).
Another important cause of increased blood flow inskeletal muscle is the fact that vascular conductance istightly coupled to metabolic rate so that conductanceincreases with increased muscle activity. The caliberof resistance arteries is regulated by local controlfactors, including metabolic, myogenic, and endothe-lial components (4). Metabolic control appears to playa central role in exercise hyperemia in both cardiacand skeletal muscle tissue as evidenced by the tight
relationship between blood flow and metabolism.Relaxation of vascular smooth muscle in arteries andarterioles produced by increased metabolism in-creases blood flow and recruits more perfused capillar-ies in the muscle tissue.
The mechanisms responsible for arteriolar vascularsmooth muscle relaxation in arterioles appear to besimilar in cardiac and skeletal muscle during exercise,but the relative importance of these mechanisms isdifferent in cardiac and skeletal muscle and amongtypes of skeletal muscle (4). The metabolites respon-sible for metabolic vascular control have not beenclearly established. Recent research indicates thatendothelium-mediated vascular control also plays animportant role in exercise hyperemia of cardiac andskeletal muscle through flow-induced dilation and/orpropagated vasodilation (4). At this time it appearsthat exercise hyperemia in skeletal muscle is mediatedby a combination of metabolic vasodilation, endothe-
FIG. 9.Illustration of effects of increasing exercise intensity on sympathetic controlof blood flow and vascular conductance in humans, reflected in measure-ments of heart rate. Note that at rest, when heart rate is low, the heart is undervagal (parasympathetic) control. Sympathetic nervous system activity in-creases as vagal control is withdrawn. Sympathetic nervous activity increaseswith increasing exercise intensity as reflected in decreases in splanchnic(SBF) and renal blood flow (RBF) to vascular beds, increased plasma norepi-nephrine concentrations ([NE]), increased plasma renin activity (PRA), andincreased muscle sympathetic nerve activity (MSNA). Blood lactate concentra-tion (HLa) does not increase until exercise intensity is 50–60% of maximal(heart rates of 130–140 beats/min). [Reprinted from Laughlin et al. (4) asadapted from Rowell (6, 7).]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S252
on July 19, 2011advan.physiology.org
Dow
nloaded from

lial vasodilator mechanisms, and the muscle pumpmechanism. As illustrated in Fig. 9, there is alsoevidence that sympathetic nervous activity to skeletalmuscle increases with increasing exercise intensity.The effects of the increased sympathetic stimulationappear to be blunted by the aforementioned vasodila-tor signals leading to the integrated response. Theenormous decrease in vascular resistance in skeletalmuscle vascular beds during dynamic exercise causestotal systemic vascular resistance to decrease. Mean
arterial pressure is increased despite the decrease inresistance because cardiac output is increased morethan vascular resistance is decreased.
As shown in Fig. 5, at the same time that vascularresistance in skeletal muscle vascular beds and thecoronary circulation is decreasing, vascular resistanceis increasing in visceral tissues, causing blood flow tothese tissues to decrease. The increase in vascularresistance in the visceral tissues (renal and splanchnic
FIG. 10.Hemodynamic effects of isometric contraction of forearm muscle(isometric handgrip) at 10, 20, and 50% maximal voluntary contraction(MVC) for 1 subject. Peripheral resistance units (PRU) are expressed asdyn.s21.cm25 3 103. Note that with increasing intensity of exercise,systolic and mean arterial pressures increase and the magnitude ofincrease is greater than that observed in subjects during dynamicexercise (see Fig. 6). Values are means 6 SE for systolic and diastolicpressures. [Reprinted from Rowell (7) with permission.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S253
on July 19, 2011advan.physiology.org
Dow
nloaded from

tissues) is the result of a progressive increase insympathetic stimulation to these vascular beds. Asillustrated in Fig. 9, as exercise intensity increases,producing heart rates .100 beats/min, sympatheticconstriction of resistance arteries in renal and splanch-nic vascular beds increases as evidenced by increasingplasma norepinephrine levels. Also, plasma reninactivity increases with increasing exercise intensity,contributing to the increased vascular resistance anddecreased blood flow to the viscera. Figure 9 alsoillustrates the fact that muscle sympathetic nerveactivity (MSNA) increases with increasing exercise inten-sity. However, in the active skeletal muscle, increasedmetabolism and other mechanisms discussed above resultin a net decrease in vascular resistance and increase inblood flow to skeletal muscle (Fig. 5).
CARDIOVASCULAR EFFECTS OF ISOMETRICEXERCISE
The effects of sustained isometric muscle contractionare much different than those seen in dynamic exer-cise. The effects of isometric arm exercise on the
cardiovascular system can be appreciated from thedata presented in Fig. 10. Note that mean arterialpressure, cardiac output, and heart rate all increasewith increases in isometric contractile force. Theincrease in blood pressure produced by isometricvoluntary muscle contraction is far greater than themetabolic cost of the exercise. Indeed, in general, theheart rate and blood pressure increases produced byisometric exercise exceed those of dynamic exercisewhen duration, intensity, and active muscle mass aresimilar. For example, note in Fig. 11 that systolicpressures are in excess of 220 mmHg and meanpressures in excess of 180 mmHg during maximalisometric contraction of the arm. Figure 12 illustratesthe fact that the magnitude of increase in arterialpressures is proportional to the size of the musclemass activated and the duration of sustained contrac-tion. Another important difference between dynamicexercise and isometric muscle contraction is thatcardiovascular adjustments to isometric contractiondo not reach a steady state. As shown in Figs. 10 and12, even after several minutes of exercise, bloodpressures and heart rates are continuing to increase.
Blood flow to muscles contracting isometrically in-creases if the contractions develop ,30% maximal
FIG. 11.Systolic, mean, and diastolic arterial pressures ofhuman subjects graphed as a function of exerciseintensity (isometric handgrip) expressed as %MVC.Note that with increasing intensity of exercise, systolicand mean arterial pressures increase and that themagnitude of increase is greater than that observed insubjects during dynamic exercise (see Fig. 6). Values aremeans 6 SE for systolic and diastolic pressures. [Re-printed from MacDougall (5) with permission of Futura.]
FIG. 12.Mean arterial pressures of human subjects graphed asa function of duration of contraction (isometric exer-cise). Note that pressure is highest during dead liftexercise and lowest during handgrip exercise and thatpressure increases with time of contraction for all 3types of exercise. Values are means 6 SE for systolicand diastolic pressures. [Reprinted from MacDougall(5) with permission of Futura.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S254
on July 19, 2011advan.physiology.org
Dow
nloaded from

voluntary contraction (MVC). When contraction devel-ops .40–60% MVC, blood flow is decreased or ceasesduring contraction and increases with muscle relax-ation. The large increases in blood pressure seenduring intense isometric contractions appear to bepartially the result of the muscle chemoreflex. Theseeffects of isometric arm exercise have importantconsequences in cardiovascular disease such as coro-nary heart disease. For example, shoveling snow is acommon cause of angina and heart attack in patientswith coronary heart disease. This appears to be theresult of the excessive increases in heart rate andblood pressure produced by isometric arm exercise.
CHRONIC INACTIVITY AND TRAINING ALTERCARDIOVASCULAR RESPONSE TO EXERCISE
When normal humans become restricted to bed restor prolonged exposure to weightlessness, their exer-cise tolerance is dramatically decreased. This is associ-
ated with a decrease in maximal oxygen consump-tion. This is illustrated in Fig. 13 from the classic studyby Saltin et al. (8). Note that after 21 days of bed rest,all 5 subjects had decreased maximal oxygen uptake.Equally important, when the subjects began exercisetraining, their maximal oxygen consumption began torecover within days and by 50 days was even greaterthan values before bed rest. Figure 14 summarizes datacollected from these subjects and allows analysis ofthe determinants of maximal oxygen uptake respon-sible for changes related to bed rest and exercisetraining. First, note that the subjects exhibited linearrelationships between cardiac output and oxygenuptake that were similar except that the maximalcardiac output was least after 21 days bed rest andgreatest after training. (CaO2
2 CvO2) was similar in
controls and after bed rest but was increased slightlyafter exercise training. Stroke volume was signifi-cantly decreased at rest and at all intensities of
FIG. 13.Effects of 21 days of bed rest and subsequent exercise training on maximal oxygenuptake measured during treadmill exercise in 5 human subjects. Circulatory studiessummarized in Figs. 14 and 15 were performed at times indicated by arrows.Symbols represent subjects’ initials. [Reprinted from Astrand and Rodahl (1) usingdata of Saltin et al. (8) with permission.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S255
on July 19, 2011advan.physiology.org
Dow
nloaded from

exercise in the bed rest subjects. Resting strokevolume was similar in control conditions and aftertraining. However, with exercise, stroke volume in-creased more after exercise training. Finally, restingheart rate was decreased after training and was slightlyhigher than control after bed rest. Heart rate increasedwith increases in exercise intensity under all threeconditions, and the maximal heart rate was similar.However, the heart rate tended to be less at eachgiven level of oxygen uptake after exercise training.
Figure 15 summarizes what these data indicate werethe changes that produced decreases in maximaloxygen consumption when these subjects underwent21 days of bed rest. Maximal cardiac output wasdecreased because of decreased stroke volume. Thedecreased stoke volume appears to be primarily causedby decreased venous return. With exercise training,these subjects exhibited increased stroke volumecompared with controls and an increased (CaO2
2CvO2
) at maximal exercise. This appears to result from
FIG. 14.Cardiac output, arteriovenous oxygen content difference, stroke volume,and heart rate as functions of exercise intensity, reflected as oxygen uptakefor the subjects illustrated in Fig. 13. c, control values before intervention; b,after a 20-day period of bed rest; t, after 50 days of exercise training.[Reprinted from Astrand and Rodahl (1) using data of Saltin et al. (8) withpermission.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S256
on July 19, 2011advan.physiology.org
Dow
nloaded from

the increased muscle blood flow available in thesubjects after training. The increased stroke volumeappears to result from increased venous return duringexercise and improved cardiac performance. Theseresults reflect how these hemodynamic parametersinfluence maximal oxygen consumption and themechanisms involved in changes in oxygen transport
capacity produced by chronic changes in a person’slevel of physical activity.
Examination of cardiorespiratory responses to exer-cise can also be used in diagnosis of cardiorespiratorydisease. In general, if a patient has limited exercisetolerance, he or she has disease or pathology at somepoint in the pathway for oxygen leading to decreasedmaximal oxygen uptake. If the problem is respiratory,
FIG. 15.Illustration of mechanisms for changes in maximaloxygen uptake produced by altered physical activity.Data are for 3 subjects after 20 days of bed rest wheremaximal oxygen uptake was 1.74 l/min. In thesesubjects before bed rest, oxygen uptake was greaterthan bed rest values because of increased maximalstroke volume (SV) and cardiac output. Increases inmaximal oxygen uptake (Q̇) produced by exercisetraining were results of further increases in strokevolume and cardiac output and increases in arteriove-nous oxygen content difference. [Reprinted from As-trand and Rodahl (1) using data of Saltin et al. (8) withpermission.]
FIG. 16.Illustration of cardiovascular responses to dynamic exerciseof increasing intensity, reflected in measurements of oxygenuptake. Results are presented for normal subjects (NA),highly trained athletes (ATH), and subjects with mitral steno-sis (MS). Vertical dashed lines represent maximal oxygenuptake for each group. Note that the splanchnic and renalblood flows begin to decrease and plasma [NE] (NE conc.)begin to increase when heart rates are equal to D100beats/min, as shown in Fig. 9. These data illustrate that, in all3 groups of subjects, sympathetic vasoconstriction in vis-ceral vascular beds increases in proportion to relative exer-cise intensity. [Adapted from Rowell (6) with permission.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S257
on July 19, 2011advan.physiology.org
Dow
nloaded from

then hemodynamic parameters will be normal and thepatient will have systemic hypoxia (CaO2
will bedecreased). If the patient has cardiovascular disease,then CaO2
will usually be normal but blood flowdelivery to skeletal muscle will be limited because oflimited cardiac output and/or peripheral vasculardisease. For example, let us compare and contrastresults from normal subjects, trained athletes, andpatients with decreased cardiac function caused bymitral stenosis. Mitral stenosis serves here only as anexample. Any condition that limits cardiac functionand cardiac output will have similar effects.
EFFECTS OF MITRAL STENOSIS ONCARDIOVASCULAR EFFECTS OF EXERCISE
Mitral stenosis will limit the flow of blood into the leftventricle and, as a result, limit cardiac output. Figure16 summarizes the expected effects of mitral stenosison the cardiovascular response to exercise and allowscomparison with responses in normal adults andathletes. Note that the major problem is limitedmaximal cardiac output (Fig. 16, top). This limitationis caused by low stroke volume, because maximalheart rate is similar across the three subjects. Maximal(CaO2
2 CvO2) is also similar across subjects. The mitral
stenosis subjects compensate for the low stroke vol-ume at rest by having increased heart rate and (CaO2
2CvO2
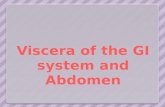
). The results presented in Fig. 17 illustrate theregional distribution of cardiac output in these sub-jects. Note that at rest, blood flows are similar in themitral stenosis, normal, and trained (athletes) sub-jects. When the subjects exercise at their maximallevel, blood flow to all tissues except muscle aresimilar across the subjects but muscle blood flow isvery limited in the mitral stenosis subjects. The majordifference is that the mitral stenosis subjects havemuch less cardiac output left to distribute to skeletalmuscle.
An important feature of the relationship betweenexercise intensity and sympathetic stimulation to theviscera is revealed in the results presented in Fig. 16,bottom, where visceral blood flows are decreasedmaximally and sympathetic stimulation is near maxi-mal in the mitral stenosis subjects at an oxygenconsumption of only 1.5 l/min. At this same level ofoxygen consumption there is only a modest decreasein blood flow in normal subjects and no change fromresting in the athletes. However, if the x-axis is
changed to percent maximal oxygen consumption,then the three curves superimpose. [At this point Iencourage the students to regraph these data bychanging the x-axis to %maximal oxygen consump-
FIG. 17.Cardiac output and distribution of cardiac output totissues at rest and during exercise at intensities produc-ing maximal oxygen uptake (maximal exercise). Re-sults are presented similarly to data in Fig. 16. At rest,cardiac output and blood flow distributions are similarin all 3 groups. Also, blood flows to nonmuscularregions are similar in all 3 groups during maximalexercise. However, blood flow to active skeletal muscleand total cardiac output is much different among the 3groups. GI, gastrointestinal. [Adapted from Rowell (7)with permission.]
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S258
on July 19, 2011advan.physiology.org
Dow
nloaded from

tion. As a result, the data for all 3 groups of subjectsbecome superimposable.]. Thus these results indicatethat the sympathetic nervous system response islinked to ‘‘relative’’ exercise intensity. Because themitral stenosis subject is exercising at a maximaloxygen consumption of 1.5 l/min, sympathetic con-strictor tone is maximal to the renal and splanchnicvascular beds.
In summary, the cardiovascular effects of dynamicexercise are driven by the demands of active skeletalmuscle for oxygen. During dynamic exercise, cardiacoutput increases five- to sixfold. The dramatic in-creases in cardiac output result from increased pumpfunction of the heart and increased venous return tothe heart. All of this increased blood flow is distrib-uted to skeletal muscle. In addition, sympatheticvasoconstrictor tone is increased in visceral vascularbeds diverting blood flow to active skeletal muscle.Sustained isometric muscle contractions produce exag-gerated increases in heart rate and arterial pressures.Anything that decreases the ability of the cardiovascu-lar system to deliver oxygenated blood to activemuscle will limit exercise performance. Such changescan be produced in normal subjects. For example,during heat stress, skin blood flow increases to controlcore body temperature. As much as 7.0 l/min ofcardiac output can be distributed to skin in severeheat stress. As a result, exercise capacity is limited inhot, humid environments because less cardiac outputcan be delivered to active muscle. Also, exercise stresscan be used in diagnosis of cardiorespiratory diseasebecause of the tight relationship between exercise
intensity, heart rate, cardiac output, and cardiovascu-lar function.
This work was supported in part by National Heart, Lung, and BloodInstitute Grants HL-52490 and HL-36088.
Address for reprint requests and other correspondence: M. H.Laughlin, Dept. of Veterinary Biomedical Sciences, E102, VeterinaryMedicine Bldg., Univ. of Missouri, Columbia, MO 65211 (E-mail:[email protected]).
References
1. Astrand, P., and K. Rodahl. Textbook of Work Physiology.New York: McGraw-Hill, chapt. 6, 9, and 12, 1970, p. 117–183,279–318, and 375–430.
2. Buckwalter, J. B., P. J. Mueller, and P. S. Clifford. Sympa-thetic vasoconstriction in active skeletal muscles during dynamicexercise. J. Appl. Physiol. 83: 1575–1580, 1997.
3. Laughlin, M. H. Skeletal muscle blood flow capacity: the role ofthe muscle pump in exercise hyperemia. Am. J. Physiol. 253(Heart Circ. Physiol. 22): H993–H1004, 1987.
4. Laughlin, M. H., R. J. Korthuis, D. J. Duncker, and R. J.Bache. Control of blood flow to cardiac and skeletal muscleduring exercise. Handbook of Physiology. Exercise: Regulationand Integration of Multiple Systems. Bethesda, MD: Am. Physiol.Soc., 1996, sect. 12, chapt. 16, p. 705–769.
5. MacDougall, J. D. Blood pressure responses to resistive, static,and dynamic exercise. In: Cardiovascular Response to Exercise.Mount Kisco, NY: Am. Heart. Assoc., 1994, chapt. 9, p. 155–173.
6. Rowell, L. B. Human Circulation. New York: Oxford Univ.Press, 1986, chapt. 7–9, p. 137–256.
7. Rowell, L. B. Human Cardiovascular Control. New York:Oxford Univ. Press, 1993, chapt. 5–8, p. 162–325.
8. Saltin, B., B. Blomqvist, J. H. Mitchell, R. L. Johnson, Jr., K.Wildenthal, and C. B. Chapman. Response to submaximal andmaximal exercise after bed rest and training. Circulation 38,Suppl. 7: 1–78, 1968.
A P S R E F R E S H E R C O U R S E R E P O R T
VOLUME 22 : NUMBER 1 – ADVANCES IN PHYSIOLOGY EDUCATION – DECEMBER 1999
S259
on July 19, 2011advan.physiology.org
Dow
nloaded from