
Cardiovascular Emergencies
167
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved. Cardiovascular Emergencies
-
Upload
ruth-aponte -
Category
Documents
-
view
30 -
download
2
description
DIABETES Y CETOACIDOSIS DIABETICA
Transcript of Cardiovascular Emergencies
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiovascular Emergencies

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Objectives
Define the following terms: afterload, preload, cardiac output, and stroke volume.
List assessment findings consistent with circulatory compromise.
Define shock (hypoperfusion).
Discuss the common causes of shock in infants and children.
Describe the clinical classifications of shock.
Describe the assessment findings that indicate shock in infants and children.
Differentiate between compensated and decompensated shock.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Objectives
Describe the initial management of hypovolemic, cardiogenic, distributive (septic, anaphylactic, neurogenic), and obstructive shock in infants and children.
Describe assessment findings that indicate cardiopulmonary failure or arrest in children.
Discuss the primary etiologies of cardiopulmonary arrest in infants and children.
Identify the major classifications of pediatric cardiac dysrhythmias.
Identify four essential questions to ask in the initial emergency management of a pediatric patient with a dysrhythmia.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Objectives
Recognize the following dysrhythmias: bradycardia,
sinus tachycardia, supraventricular tachycardia,
ventricular tachycardia, ventricular fibrillation, and
asystole.
Differentiate sinus tachycardia from supraventricular
tachycardia and supraventricular tachycardia from
ventricular tachycardia.
Recognize a ―sick‖ (unstable) and ―not sick‖ (stable)
infant or child with a cardiac dysrhythmia.
Discuss the dysrhythmias associated with pediatric
cardiopulmonary failure or arrest.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Objectives
Discuss the management of cardiac dysrhythmias in
infants and children.
Discuss the pharmacology of medications used
during shock, symptomatic bradycardia, stable and
unstable tachycardia, and cardiopulmonary arrest.
Given a patient situation, formulate a management
plan (including assessment, airway management,
CPR, pharmacological, and electrical interventions
where applicable) for a patient in shock, or presenting
with symptomatic bradycardia, stable or unstable
tachycardia, or cardiopulmonary arrest.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Review of the
Cardiovascular System

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
The Heart – A Two-sided Pump

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Pulmonary and Systemic
Circulation

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Coronary Arteries
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Blood Vessels
Arteries are conductance vessels
Arterioles are resistance vessels
Capillaries are exchange vessels
Veins are capacitance vessels

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Arteries

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
PALS Pearl
Infants and children are capable of
more effective vasoconstriction
than adults are.
As a result, a previously healthy
infant or child is able to maintain a
normal blood pressure and organ
perfusion for a longer time in the
presence of shock.
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
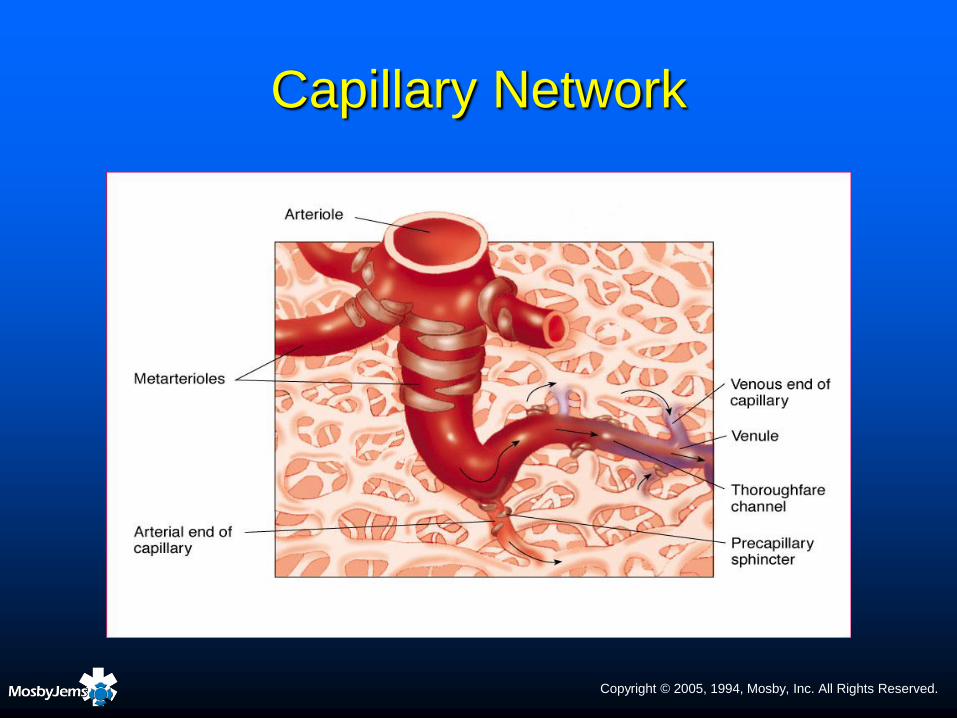
Capillary Network

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiac Cycle
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Perfusion
Perfusion
Circulation of blood through an organ or a part of
the body
Delivers oxygen and other nutrients to the cells of
all organ systems and removes waste products
Hypoperfusion (shock)
Inadequate circulation of blood through an organ
or a part of the body

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Heart Rate
Autonomic nervous system
Sympathetic division
• Mobilizes the body
• Allows body to function under
stress
• ―Fight or flight‖ response
Parasympathetic division
• Responsible for conservation
and restoration of body
resources
• ―Feed and breed‖ response

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiac Output
Cardiac output = stroke volume x heart rate
Normal cardiac output
Neonates: 200 mL/kg/min
Infants and children: 150 mL/kg/min
Adolescents: 100 mL/kg/min

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiac Output
Changes in heart rate OR stroke volume can
affect cardiac output
↑ stroke volume or heart rate → ↑ cardiac output
↓ stroke volume or heart rate → ↓ cardiac output
Tachycardia is the initial compensatory
response to the demand for increased
cardiac output

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
PALS Pearl
Because of the immaturity of sympathetic innervation to the ventricles, infants and children have a relatively fixed stroke volume.
They are dependent on an adequate heart rate to maintain adequate cardiac output.
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Blood Pressure
Systolic pressure
Diastolic pressure
Pulse pressure
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
PALS Pearl
An early sign of impending
shock is a slight increase in
diastolic pressure without a
change in the systolic pressure
(i.e., narrowed pulse pressure).

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Vascular Resistance

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Stroke Volume
Stroke volume is determined by:
The degree of ventricular filling during diastole
(preload)
The resistance against which the ventricle must
pump (afterload)
The contractile state of the myocardium
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiovascular Assessment

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiovascular Assessment
Compare strength/quality of central and peripheral pulses
Evaluate cardiac rhythm – normal, fast, slow, or absent
Look for visible hemorrhage; control bleeding if present
Evaluate skin color, temperature, moisture
Assess skin turgor
Evaluate capillary refill
Blood pressure
Pulse pressure
Urine output

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Normal Heart Rates by Age
Age Beats/Minute*
Infant (1 to 12 months) 100 to 160
Toddler (1 to 3 years) 90 to 150
Preschooler (4 to 5 years) 80 to 140
School-age (6 to 12 years) 70 to 120
Adolescent (13 to 18 years) 60 to 100
*Pulse rates for a sleeping child may be 10% lower than the low rate
listed in age group.
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
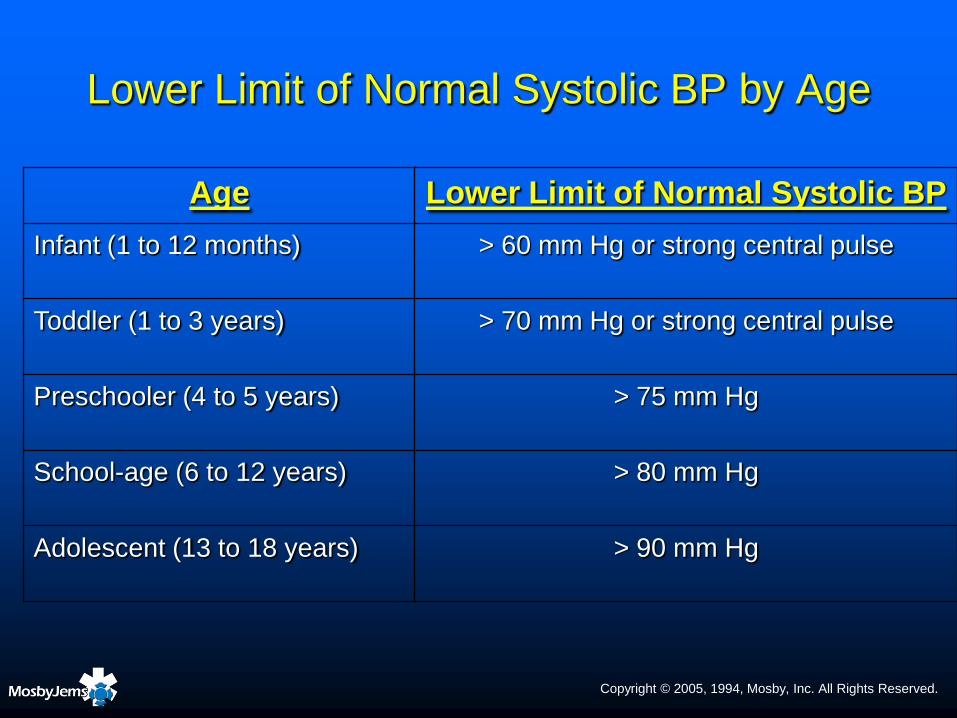
Lower Limit of Normal Systolic BP by Age
Age Lower Limit of Normal Systolic BP
Infant (1 to 12 months) > 60 mm Hg or strong central pulse
Toddler (1 to 3 years) > 70 mm Hg or strong central pulse
Preschooler (4 to 5 years) > 75 mm Hg
School-age (6 to 12 years) > 80 mm Hg
Adolescent (13 to 18 years) > 90 mm Hg

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Shock

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Stages of Shock
Early (compensated) shock
Also called reversible shock
Late (decompensated) shock
Also called progressive shock
Irreversible shock
Also called terminal shock
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Early Shock
Shock with a "normal" blood pressure
Presence of compensated shock can be
identified by:
Evaluation of heart rate
Presence and volume (strength) of peripheral pulses
Adequacy of end-organ perfusion
• Brain – assess mental status
• Skin – assess capillary refill, skin temperature
• Kidneys – assess urine output

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
PALS Pearl
The initial signs of shock may be subtle in an infant or child.
The effectiveness of compensatory mechanisms is largely dependent on the child’s previous cardiac and pulmonary health.
In the pediatric patient, the progression from compensated to decompensated shock occurs suddenly and rapidly.
When decompensation occurs, cardiopulmonary arrest may be imminent.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Late (Decompensated) Shock
―Classic‖ signs and symptoms of shock are
evident
Difficult to treat, but still reversible if
appropriate aggressive treatment is initiated

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Shock
The presence of hypotension differentiates
compensated shock from decompensated
shock.
Hypotension is a late sign of cardiovascular
compromise in an infant or child.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Irreversible Shock
Compensatory mechanisms fail
Cardiac dysrhythmias may develop as ventricular irritability increases
Cell membranes break down and release harmful enzymes
Irreversible damage to vital organs occurs because of sustained altered perfusion and metabolism, resulting in organ failure and death

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
PALS Pearl
Although the amount and type of
information gathered will vary depending
on the child’s presentation, a history
should be obtained as soon as possible
from the parent or caregiver.
The information obtained may help identify
the type of shock present, ascertain the
child’s previous health, and the onset and
duration of symptoms.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Classification of Shock
by Etiology
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Hypovolemic Shock
Hypovolemia – most common cause of shock
in children
Inadequate volume
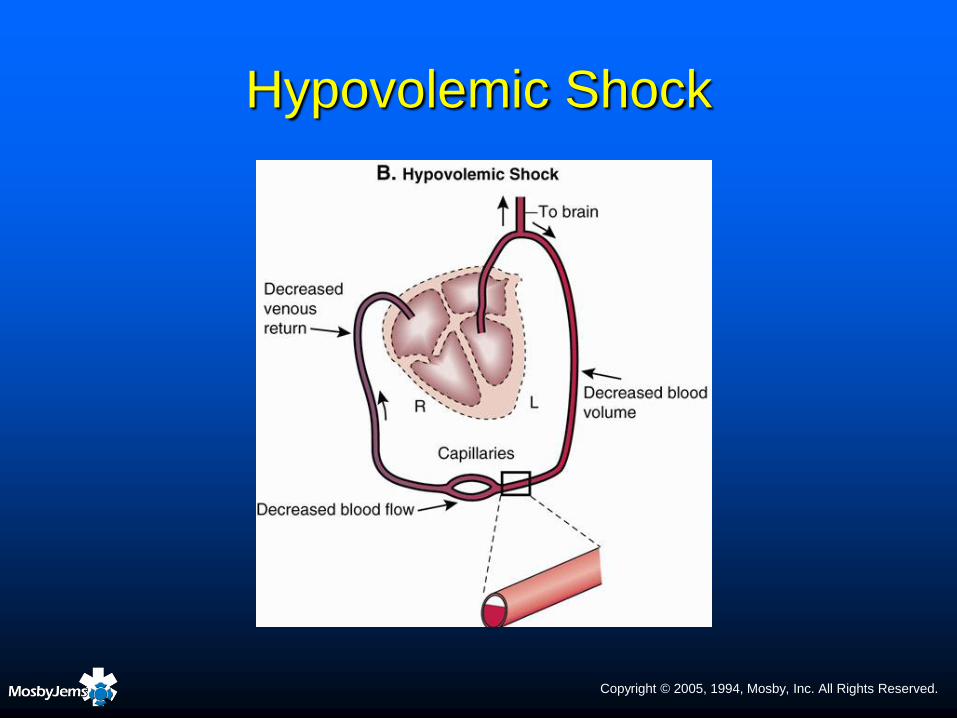
↓ intravascular volume → ↓ venous return
(preload) → ↓ ventricular filling → ↓ stroke volume
→ ↓ cardiac output → inadequate tissue perfusion
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Hypovolemic Shock

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Average Circulating Blood Volume by Age
Age Normal Blood Volume (Average)
Preterm infant 90 to 105 mL/kg
Term newborn 85 mL/kg
Infant
> 1 month to 11 months
75 mL/kg
Beyond 1 year 67 to 75 mL/kg
Adult 55 to 75 mL/kg
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Hypovolemic Shock –
Assessment Findings
Compensated shock
Normal blood pressure
Narrowed pulse pressure
Increased heart rate
Peripheral
vasoconstriction
• Skin mottling
• Delayed capillary refill
• Cool extremities
Normal or minimally
impaired mental status
Decreased urine output
Decompensated shock
Hypotension
Significant tachycardia
Markedly delayed capillary
refill
Pale, mottled, mild
peripheral cyanosis
Altered mental status –
irritability, lethargy
Minimal urine output
Weak central pulses

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
PALS Pearl
Venous access may be difficult to obtain in an infant or child in shock.
When shock is present, the most readily available vascular access site is
preferred.
Peripheral or central venous access is sufficient for fluid resuscitation in
most patients.
If immediate vascular access is needed and reliable venous access
cannot be rapidly achieved, establish IO access. If decompensated
shock is present, immediate IO access is appropriate.
If CPR is in progress, attempt vascular access by the route most readily
available that will not require interruption of CPR.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Hypovolemic Shock –
Interventions
Type and cross emergently if the child has severe
trauma and life-threatening blood loss
Administer a bolus of 20 mL/kg of isotonic
crystalloid solution (NS or LR) over 5 to 20
minutes
Assess response (i.e., mental status, capillary
refill, heart rate, respiratory effort, BP)
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Hypovolemic Shock – Interventions
Check glucose; give dextrose if indicated
Maintain normal body temperature
Obtain a history as soon as possible
Insert a urinary catheter
Obtain appropriate laboratory studies
Consider vasopressors if poor perfusion persists

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiogenic Shock
Inadequate pump

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiogenic Shock –
Assessment Findings
Compensated shock Anxiety
Pale skin, cool extremities
Diaphoresis
Normal or delayed capillary refill
Weak, thready peripheral pulses
Mild tachycardia
Jugular venous distention (indicating right ventricular failure)
Narrowed pulse pressure (rise in diastolic pressure with normal systolic blood pressure)
Mild basilar crackles
Normal or mild decrease in urine output
Orthopnea
Decompensated shock Lethargy
Pale, mottled, or cyanotic skin
Diaphoresis
Markedly delayed capillary refill
Weak, thready central pulses; peripheral pulses may be absent
Hypotension
Tachypnea with decreased tidal volume
Increasing pulmonary congestion and crackles
Oliguria

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiogenic Shock – Interventions
Perform an initial assessment
If a pulse is absent or ineffective, begin CPR
Consider giving a small IV/IO fluid bolus of isotonic
crystalloid solution (5 to 10 mL/kg of LR or NS)
Repeat the primary survey after each fluid bolus
An inotrope may be necessary to improve myocardial
contractility and increase cardiac output
Vasodilators may be used to reduce preload and afterload
Treat dysrhythmias if present and contributing to shock
Obtain a chest x-ray

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
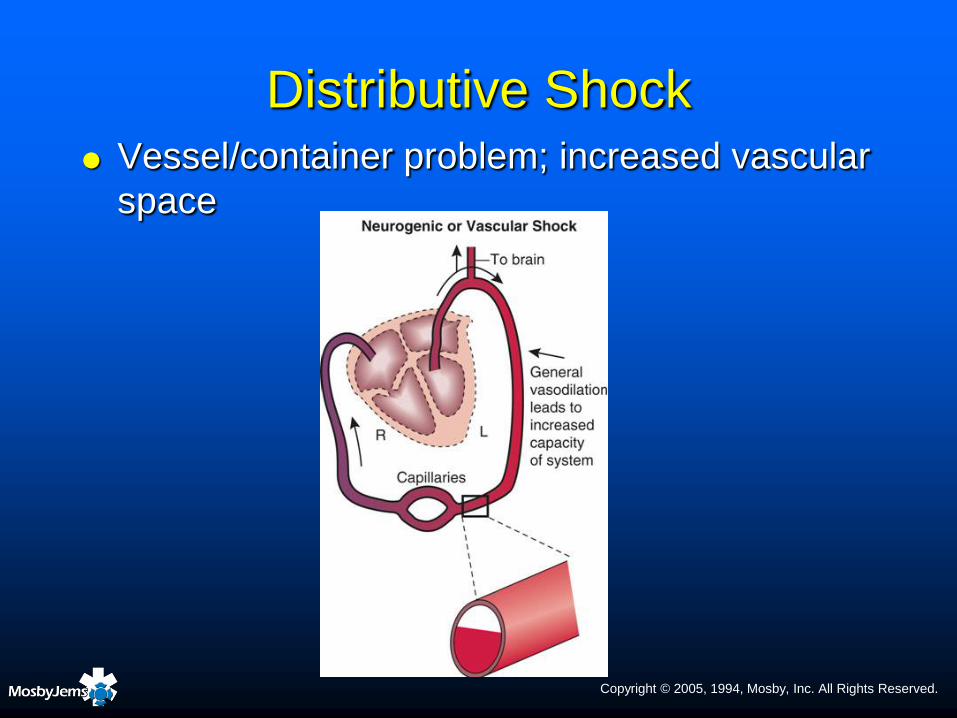
Distributive Shock
May be caused by:
Severe infection (septic shock)
Severe allergic reaction (anaphylactic shock)
Spinal cord injury (neurogenic shock)
Certain overdoses (e.g., sedatives, narcotics)
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Distributive Shock Vessel/container problem; increased vascular
space
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Septic Shock –
Assessment Findings
Early phase (increased
cardiac output)
Warm, dry, flushed skin
Blood pressure may be
normal or possible widened
pulse pressure
Bounding peripheral pulses
Brisk capillary refill
Tachycardia
Tachypnea
Late (decompensated)
phase
Mottled, cool extremities
Diminished or absent
peripheral pulses
Altered mental status
Tachycardia
Delayed capillary refill
Decreased urine output

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
PALS Pearl
Late septic shock is usually indistinguishable
from other types of shock.
If you observe a change in mental status in a
febrile child (inconsolable, inability to
recognize parents, unarousable), immediately
consider the possibility of septic shock.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Septic Shock – Interventions
Perform an initial assessment
If a pulse is absent or ineffective, begin CPR
Obtain vascular access Give 20 mL/kg isotonic crystalloid solution (NS or LR) or colloid IV
boluses up to and over 60 mL/kg
Check glucose; treat if serum glucose is < 60 mg/dL
Correct hypocalcemia

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Anaphylaxis – Assessment Findings
Stridor, wheezing, coughing, hoarseness, intercostal and suprasternal retractions
Tachycardia, hypotension, dysrhythmias
Vomiting, diarrhea
Anxiety, restlessness
Angioedema
Urticaria (hives)
Abdominal pain, cramping
Pruritus (itching)

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Anaphylaxis – Interventions
Perform an initial assessment
If a pulse is absent or ineffective, begin CPR
Remove/discontinue the causative agent
Give epinephrine IM or SC
Obtain vascular access
Administer 20 mL/kg NS or LR over 5 to 20 minutes
Consider inhaled bronchodilator therapy (e.g., albuterol)
Administer other medications to help stop the inflammatory reaction
Consider diphenhydramine
Consider methylprednisolone
Give epinephrine IV infusion for signs of decompensated shock

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Diphenhydramine
Diphenhydramine (Benadryl) is an
antihistamine/H1 receptor antagonist
Stimulation of H1 receptors causes bronchoconstriction
Stimulation of H2 receptors causes peripheral
vasodilation and secretion of gastric acids
Diphenhydramine blocks cellular histamine
response, but does not prevent histamine release
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Neurogenic Shock
Caused by a severe injury to the head or
spinal cord that results in a loss of
sympathetic vascular tone below the level of
the spinal cord injury
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Neurogenic Shock
Loss of peripheral vascular tone results in
widespread vasodilation below the level of
the injury → ↓ venous return → ↓ stroke
volume → ↓ cardiac output → ↓ tissue
perfusion
Total blood volume remains the same, but vessel
capacity is increased (relative hypovolemia)

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Neurogenic Shock –
Assessment Findings
Skin is warm and dry
Sweating does not occur below level of the injury
Heart rate within normal limits or bradycardic
Hypotension
Wide pulse pressure
Respiratory rate/effort and breathing pattern may
be affected depending on the location of the injury
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Neurogenic Shock – Interventions
Perform an initial assessment
Spinal immobilization
Use spinal precautions if airway assistance is necessary
Obtain vascular access Administer 20 mL/kg of NS or LR over 5 to 20 min
Assess response

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Obstructive Shock
Develops from cardiac tamponade, tension
pneumothorax, or a massive pulmonary
embolism
Common pathophysiology in these conditions
is obstruction to blood flow from the heart

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Tension Pneumothorax –
Assessment Findings
Early
Dyspnea
Anxiety
Tachypnea
Tachycardia
Hyperresonance of chest
wall on affected side
Diminished or absent breath
sounds on affected side
Late
Decreased level of
responsiveness
Tracheal deviation toward
the unaffected side
Hypotension
Distension of neck veins
(may not be present if
hypovolemic or in cases of
severe hypotension)
Cyanosis
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiac Tamponade –
Assessment Findings
Beck’s triad
Increased jugular venous pressure
Hypotension
Muffled heart sounds
Dyspnea
Anxiety, restlessness
Cold extremities
Pale, mottled, or cyanotic skin
Tachycardia
Weak or absent peripheral pulses
Narrowed pulse pressure
Pulsus paradoxus

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Obstructive Shock – Interventions
Perform an initial assessment
If a pulse is absent or ineffective, begin CPR
Obtain vascular access
Administer 20 mL/kg of NS or LR over 5 to 20 minutes
Check glucose
Maintain normal body temperature
Obtain a history as soon as possible
Perform needle decompression of the affected side for tension pneumothorax
Cardiac tamponade
Volume expansion to maintain an adequate circulating blood volume
Pericardiocentesis is definitive treatment
Obtain appropriate laboratory studies
Insert a urinary catheter if necessary
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiopulmonary Failure

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Signs of
Cardiopulmonary Failure
Bradypnea with irregular, ineffective respirations
Decreasing work of breathing
Delayed capillary refill time (longer than 5 seconds)
Bradycardia
Weak central pulses and absent peripheral pulses
Cool extremities
Mottled or cyanotic skin
Diminished level of responsiveness
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiopulmonary Arrest
In children, usually the result of respiratory
failure or shock → cardiopulmonary failure →
profound hypoxemia and acidosis →
cardiopulmonary arrest
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Rhythm Disturbances

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiac Dysrhythmias
Disorders of heart rate and rhythm are
uncommon in infants and children
When they do occur, they are most often a
result of hypoxia secondary to respiratory
arrest and asphyxia

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiac Dysrhythmias –
Four Categories
Dysrhythmias are divided into four broad
categories based on heart rate:
Normal for age
Slower than normal for age (bradycardia)
Faster than normal for age (tachycardia)
Absent/pulseless (cardiac arrest)

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiac Conduction System

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Electrode Placement for
ECG Monitoring

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
ECG Paper

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Waveforms

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Artifact
Loose electrode
Muscle tremor

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Analyzing a Rhythm Strip
Assess the rate Determine if the rate is normal for age, too fast, too slow, or
absent
Assess width of the QRS complex
Assess rhythm/regularity
Evaluate the rhythm’s clinical significance Stable (not sick)
• Asymptomatic (i.e., normal BP, mental status, and respiratory status)
Unstable (sick)
• Decreased responsiveness, hypotension, or respiratory failure
• Chest pain due to ischemia may be present in older child and adolescent
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
PALS Pearl
The initial emergency management of pediatric dysrhythmias requires a response to four important questions:
Is a pulse (and other signs of circulation) present?
Is the rate within normal limits for age, too fast, too slow, or absent?
Is the QRS wide (ventricular in origin) or narrow (supraventricular in origin)?
Is the patient sick (unstable) or not sick (stable)?

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Rhythm Recognition

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Sinus Rhythm
Rate Within normal limits for age
Rhythm Regular
P waves Uniform in appearance, positive (upright) in lead II, one
precedes each QRS complex
PR interval Within normal limits for age; constant from beat to beat
QRS duration 0.08 second or less
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
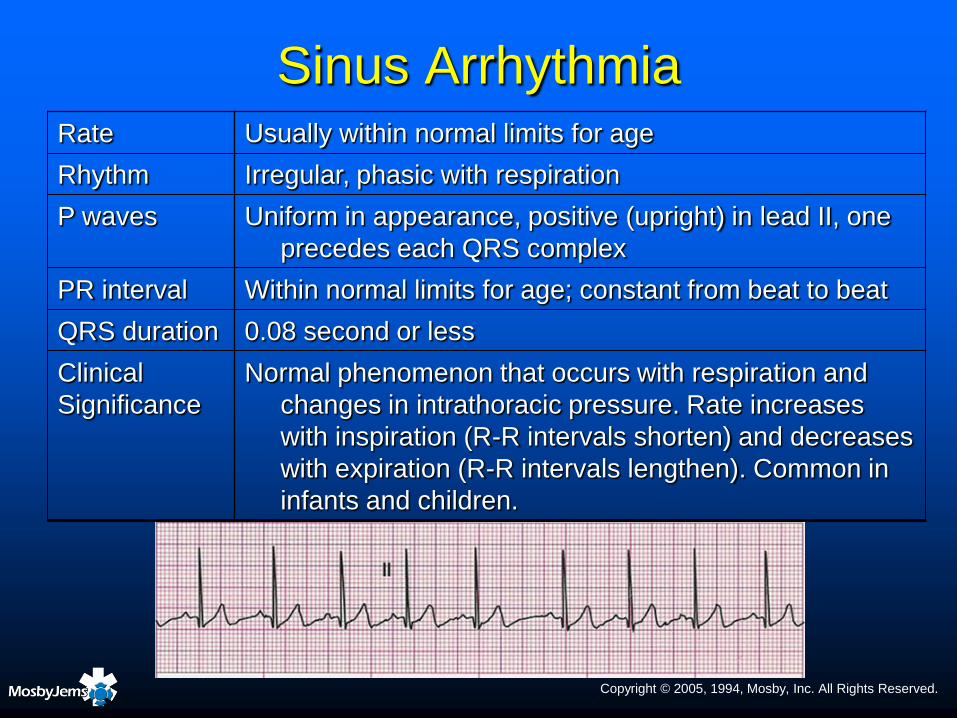
Sinus ArrhythmiaRate Usually within normal limits for age
Rhythm Irregular, phasic with respiration
P waves Uniform in appearance, positive (upright) in lead II, one
precedes each QRS complex
PR interval Within normal limits for age; constant from beat to beat
QRS duration 0.08 second or less
Clinical
Significance
Normal phenomenon that occurs with respiration and
changes in intrathoracic pressure. Rate increases
with inspiration (R-R intervals shorten) and decreases
with expiration (R-R intervals lengthen). Common in
infants and children.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Tachydysrhythmias:
Too Fast Rhythms

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Sinus Tachycardia
Rate Faster than the upper limit of normal for age; rate usually
< 220 beats/min in infants and < 180 beats/min in
children
Rhythm Regular
P waves Uniform in appearance, positive (upright) in lead II, one
precedes each QRS complex
PR interval Within normal limits for age; constant from beat to beat
QRS duration 0.08 second or less
Cause Anxiety, fear, fever, crying, hypovolemia, hypoxemia,
pain, congestive heart failure, respiratory distress,
toxins/poisonings/drugs, myocardial disease
Clinical
Significance
Compensatory response to the body’s need for
increased cardiac output or O2 delivery. Increased
myocardial workload is usually well tolerated by the
infant or child with a healthy heart.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Sinus Tachycardia

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Supraventricular Tachycardia
Most common tachydysrhythmia that necessitates
treatment in the pediatric patient
Most frequent age of presentation is in first 3 months of life
Secondary peaks occurring at 8 to 10 years of age and
again during adolescence
No heart disease is found in about one-half of patients
WPW syndrome is present in 10% to 20% of cases
SVT is not a normal compensatory response to
physiologic stress

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Supraventricular Tachycardia Rate 240 40 beats/min; may be as high as 300 beats/min in infants
Rhythm Regular
P waves Often indiscernible due to rapid rate; may be lost in the T wave
of the preceding beat. If P waves are visible, they differ in
appearance from P waves that originate in the SA node and
there is a 1 to 1 relationship to the QRS.
PR interval Usually not measurable because P waves are not visible
QRS duration 0.08 second or less unless an intraventricular conduction delay
exists
Cause Most often due to a reentrant mechanism that involves AV
junction or an accessory pathway
Clinical
Significance
Onset and termination of the rhythm are often abrupt
(paroxysmal); tachydysrhythmias may result in decreased
cardiac output (↑ heart rate → ↓ ventricular filling time → ↓
stroke volume → ↓ cardiac output)
Treatment Vagal maneuvers, antidysrhythmics, or synchronized
cardioversion depending on stability of patient

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Supraventricular Tachycardia
SVT in a child complaining of chest pain
Same child after one IV dose of adenosine
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Stable Supraventricular
Tachycardia
Secure the airway and administer 100% oxygen
Establish vascular access
Initiate continuous ECG monitoring
Consider vagal maneuvers
If the rhythm persists, give adenosine IV

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Adenosine
Slows the rate of the SA node
Slows conduction time through the AV node
Can interrupt reentry pathways that involve the
AV node
Can restore sinus rhythm in SVT
Half-life < 10 seconds
Onset of action of 10 to 40 seconds
Duration of action: 1 to 2 minutes

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Adenosine
Administer the drug medication IV or IO as rapidly as fast as possible (i.e., over a period of seconds) and immediately follow with a saline flush of at least 5 mL
May cause facial flushing because the drug is a mild cutaneous vasodilator
May cause coughing, dyspnea, and bronchospasm because it is a mild bronchoconstrictor

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Unstable Supraventricular
Tachycardia
Unstable
Increased work of breathing with altered mental
status
Hypotension
Congestive heart failure with diminished peripheral
perfusion)
If unstable, immediate treatment is warranted

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Unstable Supraventricular
Tachycardia
Secure the airway and begin bag-valve-mask ventilation with 100% oxygen
Initiate continuous ECG monitoring
If vascular access is already available, adenosine may be administered before electrical cardioversion Do not delay cardioversion if establishment of vascular
access (IV or IO) will take more than 20 to 30 seconds to accomplish

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Unstable Supraventricular
Tachycardia
If vascular access is immediately available, give adenosine
If the child is responsive, consider sedation and analgesia before performing cardioversion
If vascular access has not been established, or if the child fails to respond to adenosine, perform synchronized cardioversion Begin with 0.5 to 1 J/kg
If cardioversion does not terminate the dysrhythmia, increase the energy level to 2 J/kg
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
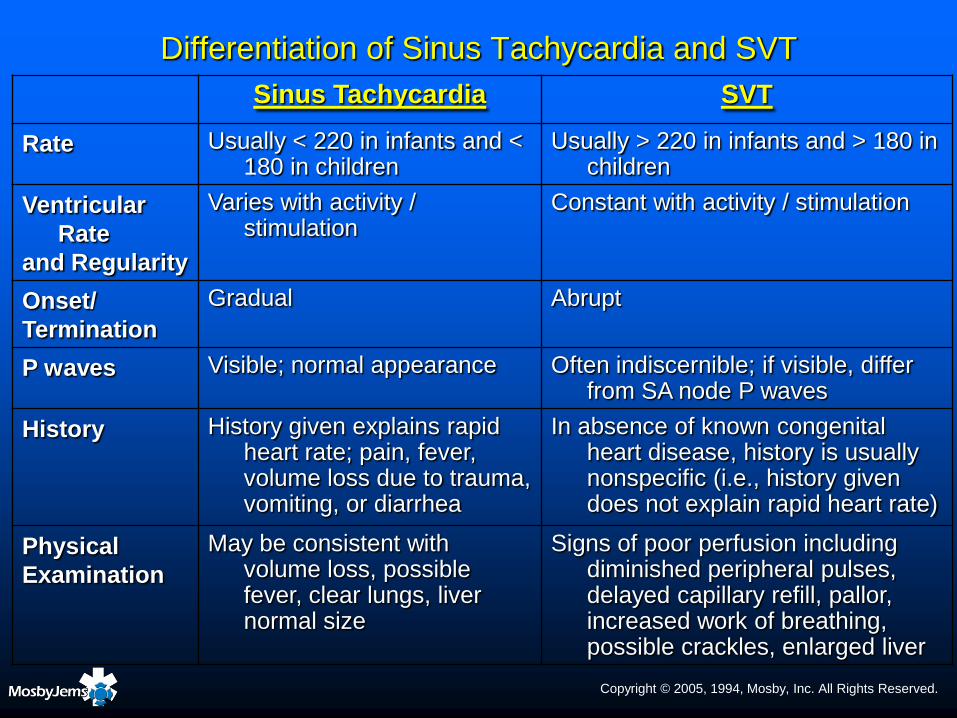
Differentiation of Sinus Tachycardia and SVT
Sinus Tachycardia SVT
Rate Usually < 220 in infants and < 180 in children
Usually > 220 in infants and > 180 in children
Ventricular
Rate
and Regularity
Varies with activity / stimulation
Constant with activity / stimulation
Onset/
Termination
Gradual Abrupt
P waves Visible; normal appearance Often indiscernible; if visible, differ from SA node P waves
History History given explains rapid heart rate; pain, fever, volume loss due to trauma, vomiting, or diarrhea
In absence of known congenital heart disease, history is usually nonspecific (i.e., history given does not explain rapid heart rate)
Physical
Examination
May be consistent with volume loss, possible fever, clear lungs, liver normal size
Signs of poor perfusion including diminished peripheral pulses, delayed capillary refill, pallor, increased work of breathing, possible crackles, enlarged liver

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Ventricular Tachycardia

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Monomorphic Ventricular Tachycardia
Rate 120 to 250 beats/minute
Rhythm Essentially regular
P waves Usually not seen; if present, they have no set relationship to the
QRS complexes appearing between them at a rate different
from that of the VT
PR interval None
QRS
Duration
Greater than 0.08 second; may be difficult to differentiate
between the QRS and T wave
Cause May be caused by acute hypoxemia, acidosis, electrolyte
imbalance, reactions to medications, toxins/poisons/drugs,
myocarditis
Clinical
Significance
Slower rates may be well tolerated. Rapid rates often result in
decreased ventricular filling time and decreased cardiac
output; may degenerate into ventricular fibrillation
Treatment If no pulse, defibrillation. Pulse present—antidysrhythmics or
synchronized cardioversion depending on stability of patient

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Monomorphic
Ventricular Tachycardia

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Polymorphic
Ventricular Tachycardia
Rapid ventricular dysrhythmia with beat-to-beat
changes in the shape and amplitude of the QRS
complexes
Polymorphic VT associated with a long QT
interval is called torsades de pointes (TdP)
Polymorphic VT associated with a normal QT
interval is simply called polymorphic VT
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
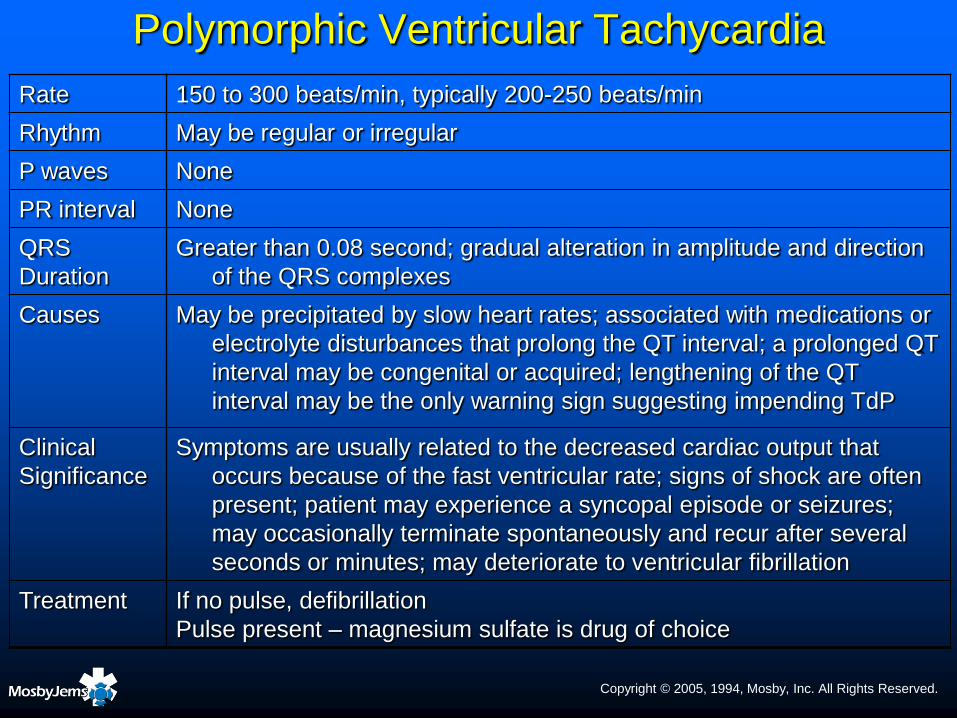
Polymorphic Ventricular Tachycardia
Rate 150 to 300 beats/min, typically 200-250 beats/min
Rhythm May be regular or irregular
P waves None
PR interval None
QRS
Duration
Greater than 0.08 second; gradual alteration in amplitude and direction
of the QRS complexes
Causes May be precipitated by slow heart rates; associated with medications or
electrolyte disturbances that prolong the QT interval; a prolonged QT
interval may be congenital or acquired; lengthening of the QT
interval may be the only warning sign suggesting impending TdP
Clinical
Significance
Symptoms are usually related to the decreased cardiac output that
occurs because of the fast ventricular rate; signs of shock are often
present; patient may experience a syncopal episode or seizures;
may occasionally terminate spontaneously and recur after several
seconds or minutes; may deteriorate to ventricular fibrillation
Treatment If no pulse, defibrillation
Pulse present – magnesium sulfate is drug of choice

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Ventricular Tachycardia
Monomorphic VT
Polymorphic VT

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Stable Ventricular Tachycardia
Secure the airway and administer 100% oxygen
Establish vascular access
Consult a pediatric cardiologist
Obtain a 12-lead ECG
Obtain a focused history, including family history for ventricular dysrhythmias or sudden death
Consider drug or metabolic causes of the VT, especially in a child without a known predisposing cause for the dysrhythmia

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Stable Ventricular Tachycardia
If the rhythm is polymorphic VT, administer magnesium sulfate 25 mg/kg slowly IV/IO bolus over 10 to 20 min
If the rhythm is monomorphic VT, give one of the following: Amiodarone 5 mg/kg IV/IO over 20 to 60 min
Procainamide 15 mg/kg IV/IO over 30 to 60 min
Lidocaine 1 mg/kg IV/IO over 2 to 4 min
If one of these medications successfully converts VT to a sinus rhythm, a continuous IV infusion of that medication is usually administered
If VT does not convert to a sinus rhythm, perform synchronized cardioversion Begin with 0.5 to 1 J/kg
If cardioversion does not terminate the dysrhythmia, increase the energy level to 2 J/kg

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Amiodarone
Directly depresses the automaticity of the SA and AV nodes
Slows conduction through the AV node and in the accessory
pathway of patients with WPW syndrome
Inhibits alpha- and beta-adrenergic receptors
Has both vagolytic and calcium-channel blocking properties
Used for a wide range of atrial and ventricular dysrhythmias
Prolongs the PR, QRS, and QT intervals
Side effects include hypotension, bradycardia, and AV block

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Procainamide
Used for both atrial and ventricular dysrhythmias
Suppresses automaticity in the atria and ventricles
Depresses conduction velocity within the conduction system
Observe ECG closely for increasing PR and QT intervals, widening of the QRS complex, heart block, and/or onset of Torsades de Pointes
If the QRS widens to >50% of its original width or hypotension occurs, stop the infusion
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Lidocaine
Depresses spontaneous ventricular depolarization
Does not affect SA or AV node depolarization
Used in the treatment of ventricular dysrhythmias
(e.g., VT, VF)
Lidocaine toxicity may be seen in patients with
persistently poor cardiac output and hepatic failure

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Bradydysrhythmias:
Too Slow Rhythms
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Bradycardias
Bradycardia – Heart rate slower than lower limit of normal for patient’s age
In children, most bradycardias occur secondary to hypoxia and acidosis
Primary bradycardia Usually caused by structural heart disease
Secondary bradycardia Due to a non-cardiac cause
• Increased vagal tone
• Hypothermia
• Hyperkalemia
• Medications (e.g., calcium channel blockers, digoxin)

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Bradycardia – Interventions
If an infant or child is symptomatic because of a
bradycardia:
Initial interventions focus on airway and ventilation
Begin CPR
If heart rate is < 60 beats/min despite adequate
oxygenation and ventilation and accompanied by:
• Abnormal skin color
• Decreased level of responsiveness
• Capillary refill >2 seconds
• Hypotension

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
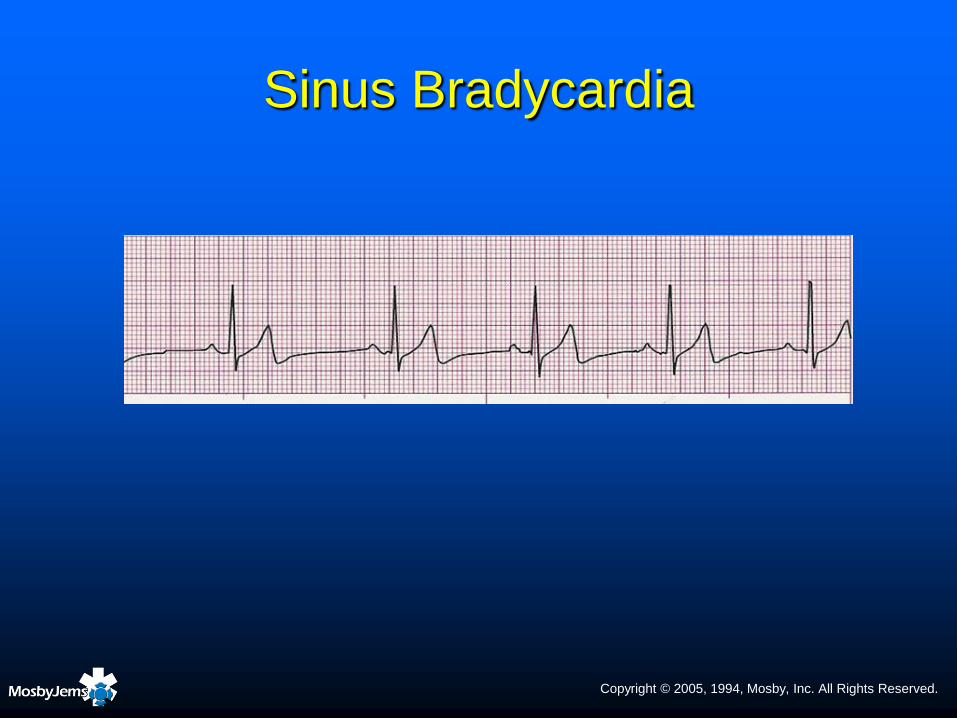
Sinus BradycardiaRate Slower than lower range of normal for age
Rhythm Essentially regular
P waves Uniform in appearance, positive (upright) in lead II, one
precedes each QRS complex
PR interval Within normal limits for age; constant from beat to beat
QRS 0.08 second or less
Cause Hypoxemia, acidosis, increased vagal tone
Clinical
Significance
May be normal in conditioned adolescent athletes and in
some children during sleep. In other patients, decreased
cardiac output may occur because of slow rate, despite
normal stroke volume.
Treatment Search for treatable cause. Ensure good oxygenation and
ventilation. Begin CPR if heart rate < 60 beats/min in an
infant or child with poor systemic perfusion despite
oxygenation and ventilation. Establish vascular access.
Epinephrine, atropine, possible pacing.
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Sinus Bradycardia

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Atrioventricular (AV) Blocks
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Epinephrine
Direct-acting endogenous catecholamine
Moderate beta-2 (bronchodilation) properties
Potent alpha (vasoconstriction) properties
Potent beta-1 (↑heart rate, ↑ force of contraction)
properties

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Epinephrine
Although beta-1 effects ↑ myocardial oxygen
consumption, it is generally well tolerated in
pediatric patient
In cardiac arrest, epinephrine produces beneficial
effects primarily because of its alpha-adrenergic
stimulating effects:
↑ peripheral vascular resistance (vasoconstriction) → ↑
diastolic pressure → ↑ myocardial and cerebral blood
flow during CPR

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Atropine
Enhances AV conduction
Increases heart rate by accelerating SA node
discharge rate and blocking vagus nerve
Has little or no effect on force of contraction
Do not give atropine slowly or in smaller than
recommended doses (0.1 mg)
Paradoxical slowing of heart rate can occur; may last
two minutes
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Atropine
Epinephrine is drug of choice if bradycardia is due
to hypoxia and oxygenation and ventilation do not
correct the bradycardia
Give atropine before epinephrine if bradycardia is
due to increased vagal tone or if AV block is
present
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Drug Pearl – Dopamine
Endogenous catecholamine with dose-related
actions
Low doses (0.5 to 5 mcg/kg/min)
• Acts on dopaminergic receptors located mainly in mesenteric,
renal, and coronary vessels, causing vasodilation
Moderate doses (5 to 10 mcg/kg/min)
• Stimulates beta-1 adrenergic receptors, increasing myocardial
contractility and stroke volume, thereby increasing cardiac output
High doses (10 to 20 mcg/kg/min)
• Acts on vascular alpha-adrenergic receptors, producing systemic
vasoconstriction

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Absent/Pulseless Rhythms
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Absent/Pulseless Rhythms
Absent/pulseless rhythms include: Pulseless VT
• ECG displays a wide QRS complex at a rate faster than 120 beats/minute
VF• Irregular chaotic deflections that vary in shape and amplitude are
observed on the ECG, but there is no coordinated ventricular contraction
Asystole• No cardiac electrical activity is present
Pulseless electrical activity (PEA)• Electrical activity is visible on ECG but central pulses are absent
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Ventricular Fibrillation
Rate Cannot be determined because there are no discernible
waves or complexes to measure
Rhythm Rapid and chaotic with no pattern or regularity
P waves Not discernible
PR interval Not discernible
QRS Not discernible
Causes Severe hypoxia and/or poor perfusion, electrolyte imbalance,
hypothermia, toxins/poisons/drugs (e.g., digitalis, tricyclic
antidepressants)
Significance Terminal rhythm
Treatment Confirm patient is apneic and pulseless (check leads). Begin
ventilation, oxygenation, and chest compressions until a
defibrillator is available.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Ventricular Fibrillation
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
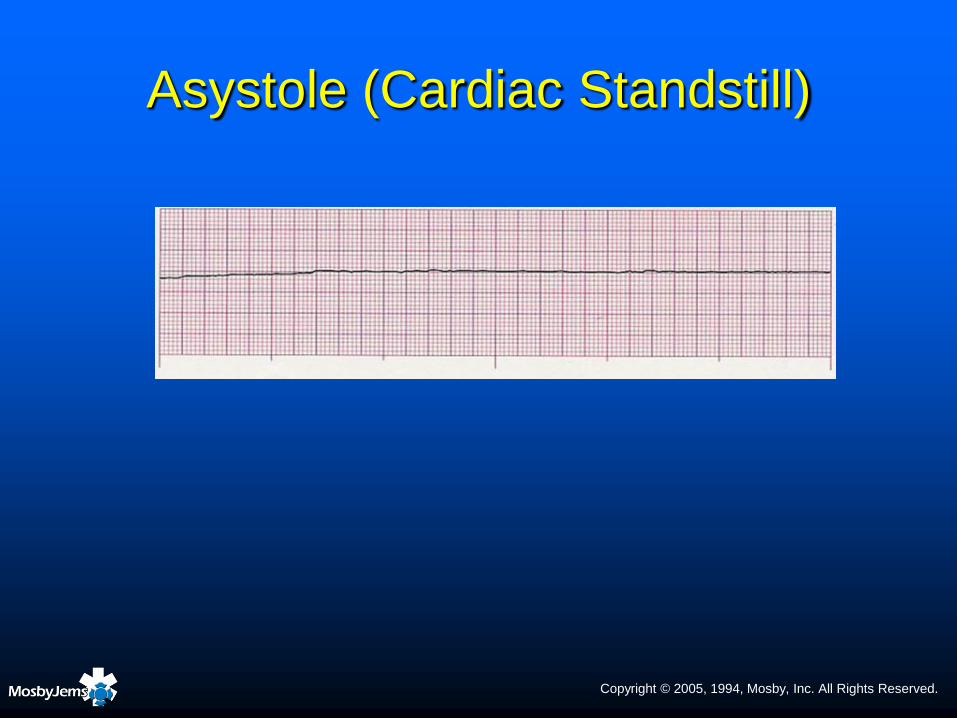
Asystole (Cardiac Standstill)
Rate Ventricular usually not discernible but atrial activity may be
observed (―P-wave‖ asystole)
Rhythm Ventricular not discernible, atrial may be discernible
P waves Usually not discernible
PR interval Not measurable
QRS Absent
Causes Hypoxia, hypokalemia, hyperkalemia, hypothermia, acidosis,
toxins/poisons, respiratory failure, traumatic cardiac arrest
(among other causes). Ventricular asystole may occur
temporarily following termination of a tachydysrhythmia
following medication administration, defibrillation, or
synchronized cardioversion.
Clinical
Significance
Absence of cardiac output; terminal rhythm. Patient is
unresponsive, apneic, and pulseless.
Treatment See Pulseless Arrest algorithm
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Asystole (Cardiac Standstill)

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Pulseless Electrical Activity
Pulseless electrical activity (PEA) is a clinical
situation, not a specific dysrhythmia
PEA exists when organized electrical activity
(other than VT) is observed on the cardiac
monitor, but the patient is pulseless

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Pulseless Electrical Activity
PEA has a poor prognosis unless the underlying cause can be rapidly identified and appropriately managed
Causes of PEA – 4 H’s and 4 T’s
Hypovolemia
Hypoxemia
Hypothermia
Hyperkalemia
Tamponade, cardiac
Tension pneumothorax
Thrombosis: lungs (massive pulmonary embolism)
Tablets/toxins: drug overdose
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope
Syncope (fainting)
Brief loss of consciousness caused by transient cerebral
hypoxia
Loss of consciousness typically occurs within a few
seconds of symptom onset
Complete recovery shortly after patient assumes a
supine position
Causes no residual neurological problems
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope
Non–life-threatening causes
Increased vagal tone
Psychogenic reactions
Prolonged standing, fatigue, dehydration

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope
Potentially life-threatening causes
Dysrhythmias including SVT, bradycardia, prolonged
QT syndrome
Cardiac abnormalities that decrease blood flow to the
heart, lungs, brain and body
Myocardial ischemia
Certain drug intoxications
Hypoglycemia, anemia, hypoxia, head trauma

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Types of Syncope
Circulatory causes
Vasovagal syncope
Orthostatic hypotension
Cardiac syncope
Extremely fast or slow heart rates
Prolonged QT syndrome
Metabolic causes
Respiratory causes
Psychogenic causes

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope –
Epidemiology and Demographics
Uncommon before age 10 to 12 years but is quite prevalent in adolescent girls
Minor injuries are common (25%)
Serious injuries occur in 1% to 2%
If recurrent, may have a major effect on lifestyle and/or quality of life
Family history positive for similar episodes in 90% of patients

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope – History
Frequently preceded by lightheadedness, nausea,
―gray-out,‖ sweating, and pallor (presyncope)
May occur while sitting, standing, walking, and
occasionally during exercise
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope –
Common Prodromal Symptoms
Lightheadedness 89%
Visual disturbances 71%
Sensation of warmth 39%
Nausea 35%
Diaphoresis 33%
Altered hearing 25%
Sharp frontal headache 15%
Mild tachycardia 13%

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope – Physical Examination
Brief tonic-clonic activity observed in 6%
Urinary incontinence in 2%
Consider orthostatic vital signs if volume loss
is suspected
Do not perform if tachycardia or severe
hypotension exist
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
PALS Pearl
An infant described as having been dusky or pallid during syncope, with apnea, hypotonia, and a lifeless look may have experienced an apparent life-threatening event (ALTE).
These patients require physician evaluation.

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope – Physical Examination
Physical findings that suggest a life-threatening cause of
syncope:
Evidence of serious injury, particularly head trauma
Continuing altered mental status, particularly unresponsiveness
Sternal scar indicating cardiac surgery
Significant persistent abnormalities in vital signs
Prominent heart murmur

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope –
Therapeutic Interventions
Treatment is directed toward underlying cause
If assessment reveals a potentially life-threatening
cause of syncope:
Secure the airway, provide high-concentration oxygen
Initiate pulse oximetry and cardiac monitoring
Establish vascular access if possible
Check blood glucose levels and treat for hypoglycemia
as indicated

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Syncope –
Therapeutic Interventions
If the child appears stable and there are no
findings to indicate a potentially life-threatening
cause of syncope:
Allow the child to maintain a position of comfort
Keep the child warm
Provide reassurance

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Chest Pain

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Chest Pain in Children
Most common causes of pediatric chest pain:
A pathologic condition of the chest wall
• Trauma or muscle strain
Costochondritis
Respiratory disease

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Chest Pain in Children
Chest pain
Can occur in a child of any age
Rarely has a life-threatening cause
Relatively infrequent chief complaint in the
young child
• Increases in frequency as the child ages
No cause for chest pain can be found
in 12% to 45% of patients
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Chest Pain in Children
Costochondritis
Esophageal reflux
Chest trauma
Severe cough, asthma, or pneumonia

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Chest Pain in Children
Acute myocardial infarction
Rare in children
When it does occur:
• Acute inflammatory condition of the coronary arteries
• Anomalous origin of the left coronary artery
• Or history of glue sniffing or cocaine use

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Chest Pain in Children
Cardiac dysrhythmias
Marfan syndrome
Pericarditis
Myocarditis Marfan Syndrome
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Chest Pain in Children –
Interventions
Perform an initial assessment
If a cardiac cause for chest pain is suspected:
Administer high-concentration oxygen
Attach pulse oximeter and cardiac monitor
Establish IV access if possible
Consult a pediatric cardiologist
Reassess frequently

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Congenital Heart Disease
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Acyanotic Heart Defects
Classified according to their hemodynamic
effects:
Increased pulmonary blood flow
• Atrial septal defect (ASD)
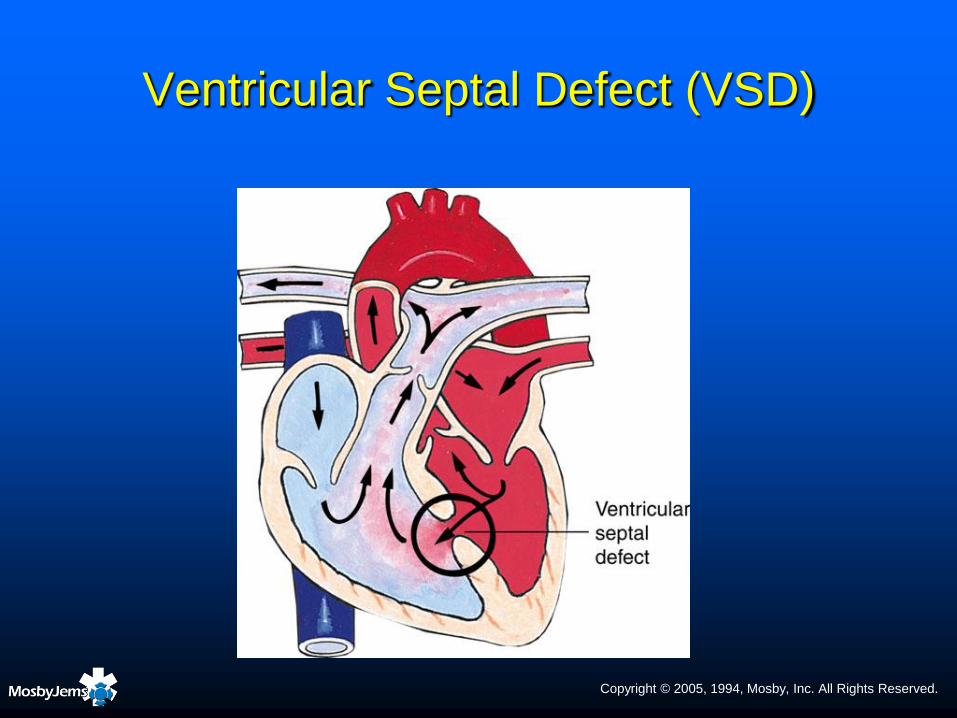
• Ventricular septal defect (VSD)
• Patent ductus arteriosus (PDA)
Obstruction to blood flow from the ventricles
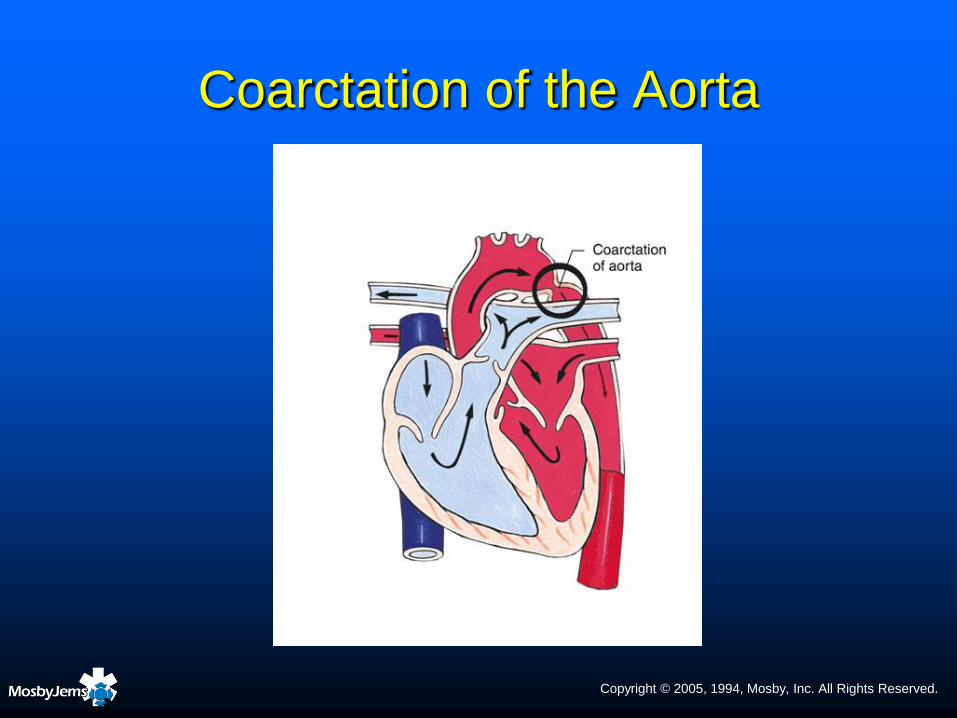
• Coarctation of the aorta (COA)
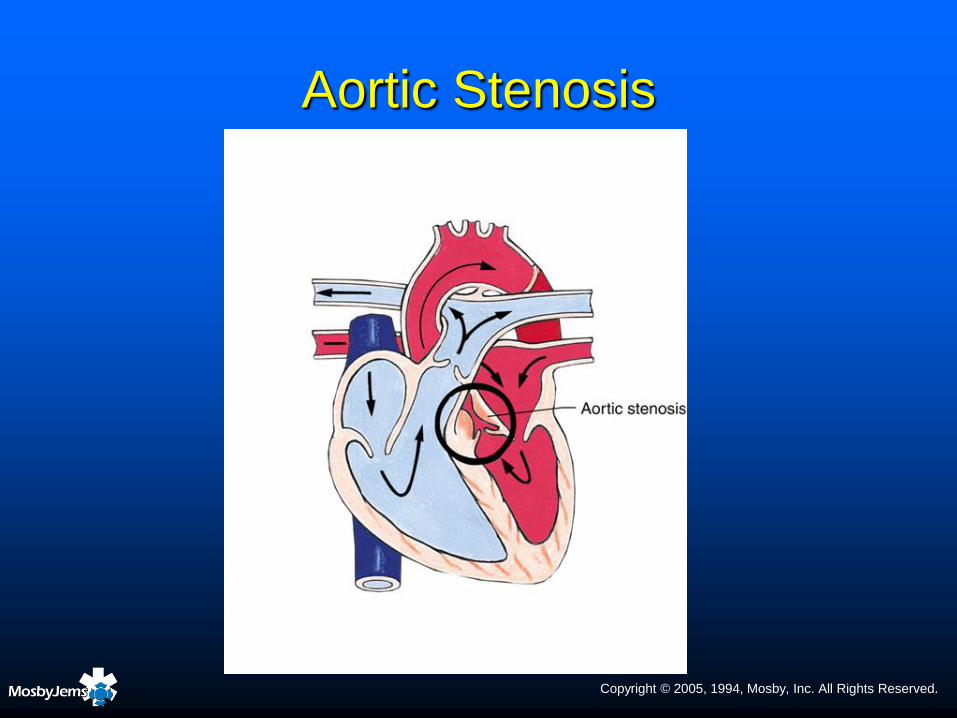
• Aortic stenosis (AS)
• Pulmonary stenosis (PS)

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Atrial Septal Defect (ASD)
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Ventricular Septal Defect (VSD)

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Patent Ductus Arteriosus
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Coarctation of the Aorta
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Aortic Stenosis

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Pulmonary Stenosis

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cyanotic Heart Defects
May be classified according to their
hemodynamic effects:
Decreased pulmonary blood flow
• Tetralogy of Fallot (TOF)
• Tricuspid atresia
Mixed blood flow
• Transposition of great vessels (TGV)
• Total anomalous pulmonary venous return or communication
• Truncus arteriosus
• Hypoplastic heart syndrome
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Tetralogy of Fallot
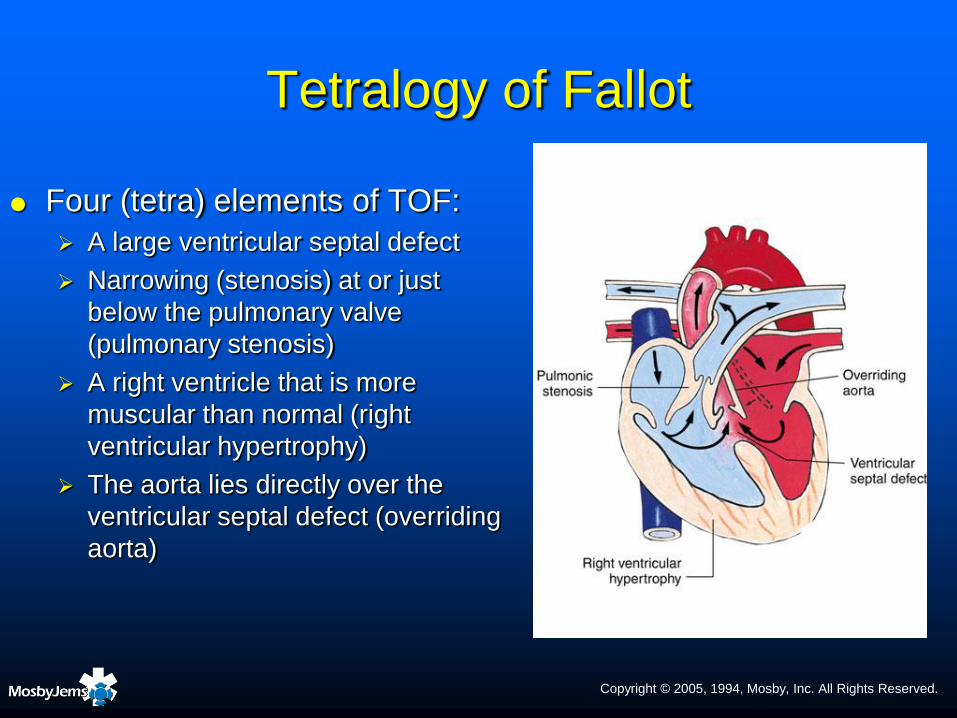
Four (tetra) elements of TOF:
A large ventricular septal defect
Narrowing (stenosis) at or just
below the pulmonary valve
(pulmonary stenosis)
A right ventricle that is more
muscular than normal (right
ventricular hypertrophy)
The aorta lies directly over the
ventricular septal defect (overriding
aorta)
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
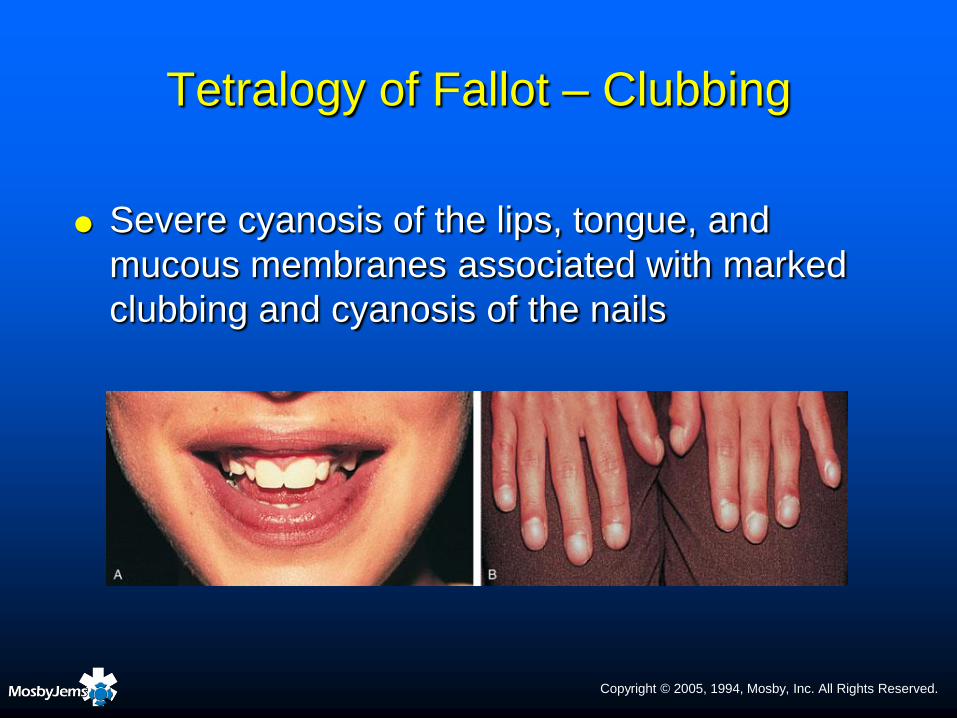
Tetralogy of Fallot – Clubbing
Severe cyanosis of the lips, tongue, and
mucous membranes associated with marked
clubbing and cyanosis of the nails

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Tetralogy of Fallot – ―Tet‖ Spell

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Tetralogy of Fallot – ―Tet‖ Spell

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Transposition of the
Great Vessels

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Congestive Heart Failure

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Congestive Heart Failure – Etiology
Excessive workload Volume-overload
• Ventricular septal defect
• Patent ductus arteriosus
• Single ventricle
Pressure overload
• Coarctation of the aorta
• Valvular stenosis
Normal workload on damaged myocardium Asphyxia
Myocarditis
Cariomyopathy
Secondary heart failure
Supraventricular tachycardia
Complete heart block associated with structural disease

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
CHF – History
Poor feeding of recent onset due to fatigue and shortness of breath
Tachypnea that worsens during feeding
Diaphoresis on the forehead and/or back of the neck during sleep and feeding
Poor weight gain
Increased fatigue, long naps, easy fatigability
Shortness of breath with activity
Peripheral edema appearing first around the face and eyes, later in the hands and feet
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
CHF – Physical Examination
Cyanosis that worsens with crying
Tachypnea, often > 50 breaths/min
Tachycardia – resting heart rate > 150 beats/min in infants, > 100 beats/min in child
Crackles Infrequent in infants and young children
Presence suggests severe edema
Wheezes Often confused with bronchospasm; poor response to bronchodilators
Increased work of breathing, retractions
Diaphoresis
Peripheral pulses may be diminished
Third heart sound
Hepatomegaly
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
CHF – Interventions
Semi-Fowler’s position
Administer oxygen
Minimize stress and energy output
Monitor intake and output, electrolytes, hematocrit
Daily weight measurement
Administer a rapid-acting diuretic
Administer digoxin if directed by pediatric cardiologist
Rapid-acting inotropic medication if severe distress and
cardiac output compromised

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiomyopathy

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Cardiomyopathy
Disease of the heart muscle itself
Primary types
Dilated
Hypertrophic
Restrictive

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Kawasaki Disease
Inflammation of the walls of small and medium-sized arteries throughout the body
Leading cause of acquired heart disease in children
Possible causes: Bacteria, viruses, and environmental chemicals or
pollutants
None has proven to be the cause of the disease

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Kawasaki Disease
Usually occurs in children 6 months to 5 years of age
Occurs year round but is more common in the winter and
spring
In North America, the highest incidence rates are in
children of Asian ethnicity
Especially those of Japanese or Korean background
Associated with coronary artery aneurysms in
approximately 25% of cases

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Kawasaki Disease
Fever (usually > 103ºF) for 5 or more days and
presence of at least 4 of following 5 principal
features:
Skin rash
Swollen, dry, cracked lips or a red tongue with small,
raised bumps (papillae)
Red (―bloodshot‖) eyes
Swollen lymph nodes in the neck
Swelling and redness of the hands and feet
Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.
Kawasaki Disease – Interventions
Cardiac monitoring
IV immune globulin (IG)
Aspirin
IV methylprednisolone
Warfarin (Coumadin)

Copyright © 2005, 1994, Mosby, Inc. All Rights Reserved.


















