Cardiovascular Disease, Hti dHtFilHypertension and...
70
Cardiovascular Disease, Cardiovascular Disease, H t i dH t F il H t i dH t F il Hypertension and Heart Failure Hypertension and Heart Failure Markey Pathway September 27, 2012 Victor G. Dávila-Román, M.D. Professor of Medicine Anesthesiology and Radiology Professor of Medicine, Anesthesiology and Radiology Director, Cardiovascular Imaging and Clinical Research Core Laboratory W ashington University in St Louis University in St Louis University in St. Louis University in St. Louis SCHOOL OF MEDICINE SCHOOL OF MEDICINE http://circl.wustl.edu http://circl.wustl.edu
Transcript of Cardiovascular Disease, Hti dHtFilHypertension and...

Cardiovascular Disease, Cardiovascular Disease, H t i d H t F ilH t i d H t F ilHypertension and Heart FailureHypertension and Heart Failure
Markey PathwaySeptember 27, 2012
Victor G. Dávila-Román, M.D.Professor of Medicine Anesthesiology and RadiologyProfessor of Medicine, Anesthesiology and Radiology
Director, Cardiovascular Imaging and Clinical Research Core Laboratory
WashingtonUniversity in St LouisUniversity in St LouisUniversity in St. LouisUniversity in St. LouisSCHOOL OF MEDICINESCHOOL OF MEDICINEhttp://circl.wustl.eduhttp://circl.wustl.edu
Markey Pathway: Cardiovascular Markey Pathway: Cardiovascular Di H t i d H t F ilDi H t i d H t F ilDisease, Hypertension and Heart FailureDisease, Hypertension and Heart Failure
1. Tue, Sep 25 John A. Curci, MD, FACSAbdominal Aortic AneurysmsAbdominal Aortic Aneurysms
2. Thu, Sep 27 Victor G. Dávila-Román, MDOverview of CVD, HTN and Heart Failure
3. Tue, Oct 2 Murali Chakinala, MD and Maribeth Duncan, ANP-BCPulmonary HypertensionPulmonary Hypertension*Note: Presentation will be 12:30-2:00pm
4. Thu, Oct 4 Lisa de las Fuentes, MDCardiac Imaging Laboratory
5. Tue, Oct 9 Gregory M. Lanza, MD, PhD5. Tue, Oct 9 Gregory M. Lanza, MD, PhD Nanomedicine opportunities in Cardiovascular Medicine
6. Thu, Oct 11 Linda Peterson, MDObesity and the Heart
7. Tue, Oct 16 Jeffrey E. Saffitz, MD, PhD, Visiting Professor7. Tue, Oct 16 Jeffrey E. Saffitz, MD, PhD, Visiting ProfessorMallinckrodt Professor of Pathology, Harvard Medical School Chief, Dept. of Pathology, Beth Israel Deaconess Medical CenterCardiac Pathology – Laboratory with pathologic specimens*Note: Lunch will be served at 12:15pm. Class will begin at 1:15pmNote: Lunch will be served at 12:15pm. Class will begin at 1:15pm
8. Thu, Oct 18 Edward Geltman, MDCongestive Heart Failure

CVD, Hypertension & Heart FailureOutline:I Cardiovascular DiseaseI. Cardiovascular Disease
Epidemiology
II. CHD Acute Coronary Syndromes
III. Hypertension / LVH
IV H t f ilIV. Heart failure

Cardiovascular DiseaseCardiovascular DiseaseEpidemiology - Deaths
AHA: www.americanheart.org

CVD deaths vs. Cancer Deaths, by age
United States: 2008. Source: NCHS.

Cardiovascular DiseaseCardiovascular DiseaseEpidemiology - Prevalence
2003 StatisticsCVD: 71.3 MHTN 65 M
2006 StatisticsCVD: 81.1 MHTN 75 4 M
2008 StatisticsCVD: 82.6 MHTN 76 MHTN: 65 M
CHD: 13.2 MMI: 7 2 M
HTN: 75.4 MCHD: 17.6 MMI: 5 5 M
HTN: 76 MCHD: 16.3 MMI: 7 9 MMI: 7.2 M
CHF: 5.0 MStroke: 5 5 M
MI: 5.5 MCHF: 5.8 MStroke: 6 4 M
MI: 7.9 MCHF: 5.7 MStroke: 7 0 MStroke: 5.5 M Stroke: 6.4 M Stroke: 7.0 MObesity: 75MOb&Ow:~149M
AHA: www.americanheart.org

Cardiovascular DiseaseCardiovascular DiseaseE id i l P l b dEpidemiology – Prevalence, by age and sex
United States: 2008 Source: NCHS and NHLBI.

CVD & other major causes of death: both sexes
United States: 2008. Source: NCHS and NHLBI.

CVD and stroke costs(estimated direct and indirect costs in $B)(estimated direct and indirect costs, in $B)
AHA2011: www.americanheart.org

Projected CVD Costs (in $B)
AHA2011: www.americanheart.org

IHD risk factors: 9 modifiable RFs account for 90% of 1st MI worldwideaccount for 90% of 1 MI worldwide
Yusuf S, Lancet 2004;364:937–52*INTERHEART case-control study (15,542 cases-14,820 controls) in 52 countries

Framingham Heart Study
1948: Start of Framingham Heart Study 1960: Cigarette smoking → increases risk of heart disease
Most Significant Milestones
1960: Cigarette smoking → increases risk of heart disease 1961: High Cholesterol & HBP → increases risk of heart disease 1967: Physical activity → reduces risk of heart disease 1967: Obesity → increases risk of heart disease 1967: Obesity → increases risk of heart disease 1970: HBP → increases risk of stroke 1976: Menopause → increases the risk of heart disease 1978: Psychosocial factors → affect heart disease y 1988: High HDL cholesterol → reduces risk of death 1990: Homocysteine (amino acid) → possible risk factor for heart disease 1994: LVH → increase the risk of stroke 1995: First Framingham report on diastolic heart failure 1996: Progression from hypertension to heart failure described 1997: Enlarged LV increases risk for HF in asymptomatic individuals
www.nhlbi.nih.gov/about/framingham/index.html

Framingham CHD prediction in men by risk factors
Wilson PWF, Circulation 1998:97:1837-1847www.nhlbi.nih.gov/about/framingham/index.html

Long Term Risk for CVD based on FHS
AHA2011: www.americanheart.org

Top 10 AHA Heart Disease and Stroke 2012 Statistics
1. 1998-2008, CVD death rates ↓ 30.6%. CVD still #1 cause of death in USA. 2. 2007-2008, CVD costs by >$11 billion. 3. HTN: ~76 M adults. 4 Ch l l 98 8M (TC≥200 /dL) 33 M (TC≥240 /dL)4. Cholesterol: ~98.8M (TC≥200 mg/dL); ~33.5M (TC≥240 mg/dL). 5. Diabetes: ~18.3M; ~7.1M undiagnosed diabetes; ~81.5M prediabetes. 6. Physical Activity: ~20.7% adults meet federal recommendations;
9 12 graders 37 0% meet recommendations9-12 graders: ~37.0% meet recommendations. 7. Healthy Diet: <1% U.S. adults meet the definition for Ideal Healthy Diet;
essentially no children meet the goal. 8 Smoking: >19% of 9-12 graders; ~21 2% men & 17 5% women8. Smoking: >19% of 9 12 graders; 21.2% men & 17.5% women. 9. BMI: ~68% overweight/obese (72% men, 62% women);
~32% children ages 2-19 overweight/obese (32% boys, 31% girls). 10. Compared to previous trends for adults: 0 Co pa ed to p e ous t e ds o adu ts
Improvements in CVD and stroke mortality, Improvements in prevalence of high cholesterol and physical activity; No changes in prevalence of HTN, smokingg p gWorsening of prevalence of diabetes and overweight.
Roger VL, Circ 2012, published online Dec 15, 2011,10.1161/CIR.0b013e31823ac046
CVD, Hypertension & Heart FailureOutline:I Cardiovascular DiseaseI. Cardiovascular Disease
Epidemiology – QUESTIONS?
II. CHD Acute Coronary Syndromes
III. Hypertension / LVH
IV H t f ilIV. Heart failure
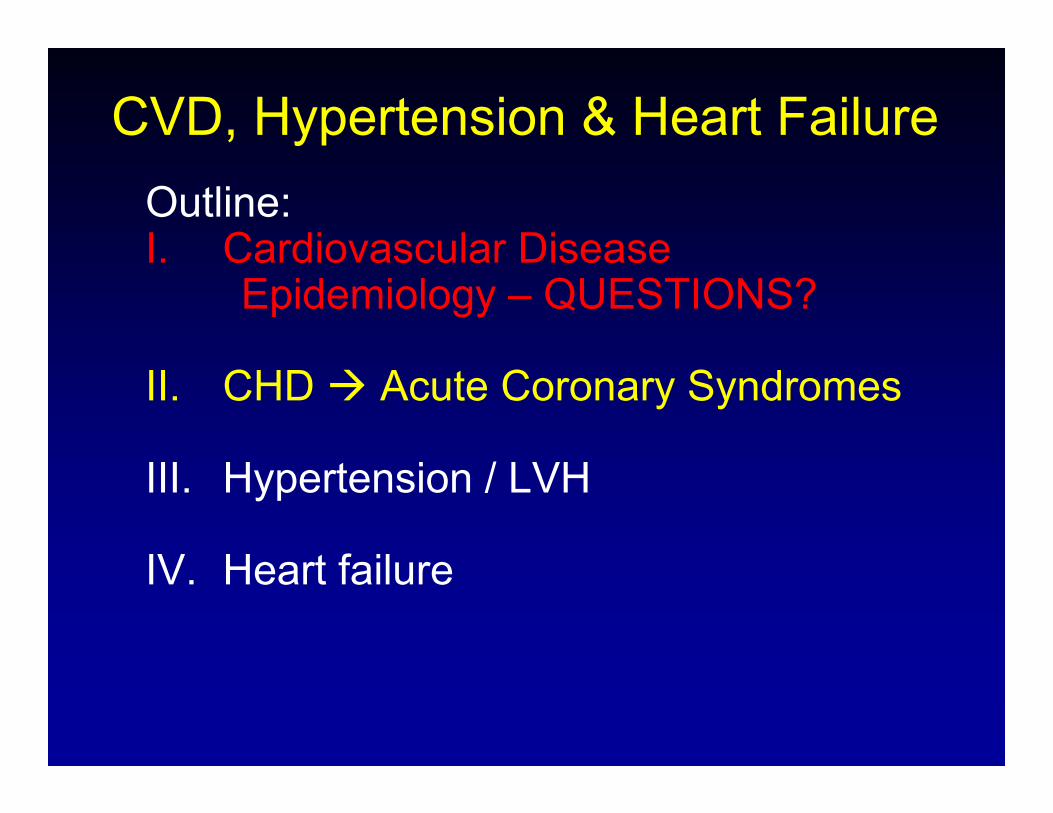
Cross-section view of arterial wallCross section view of arterial wall

Coronary EndotheliumCoronary EndotheliumNormal FunctionsNormal FunctionsNormal FunctionsNormal Functions
M d l i Modulates vasomotion In response to acetylcholine → release NO → SMC
dilationdilation Anti-thrombotic
A ti l t l t Anti-platelet Retards lipid accumulation Anti-leukocyte Anti-proliferative for SMC

Development of AtherosclerosisDevelopment of Atherosclerosis
Response-to-injury hypothesisd h li l d d i d f i endothelial denudation vs. dysfunction
Injury: physical forces (turbulent flow)toxins (tobacco)Oxidized LDLOxygen radicalsHTNDM

Development of AtherosclerosisDevelopment of AtherosclerosisEndothelial dysfunction in Atherosclerosis
Ross R. NEJM 1999
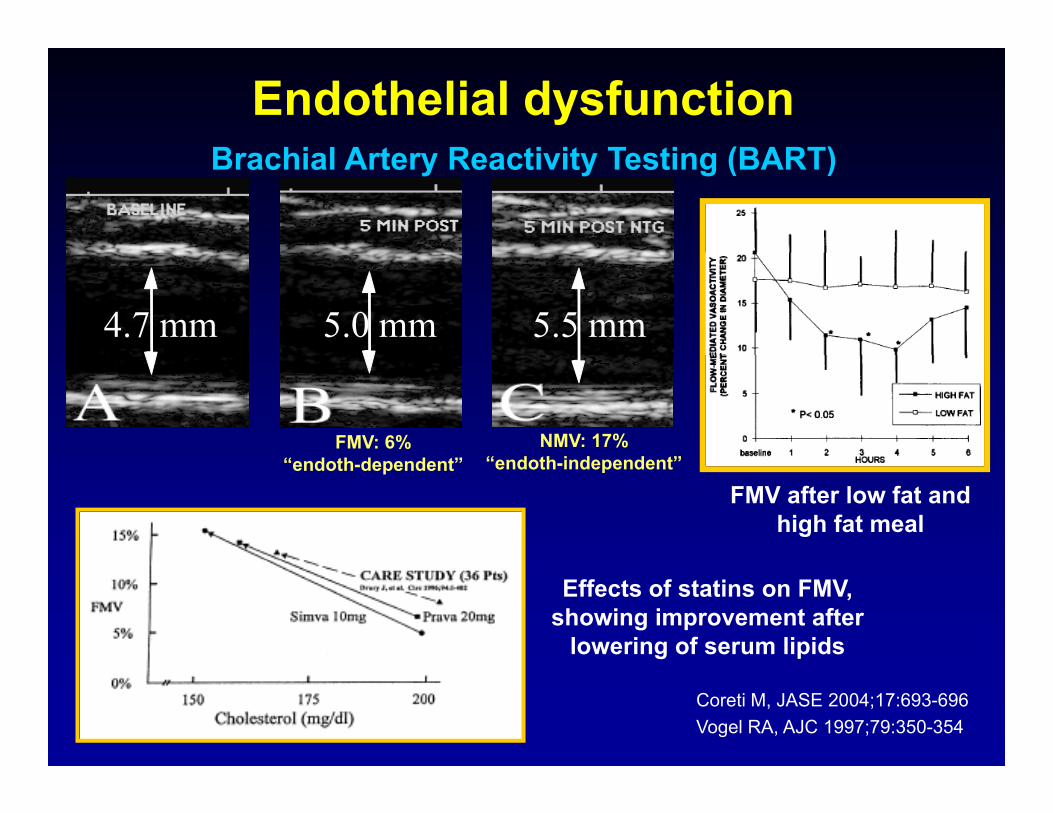
B hi l A t R ti it T ti (BART)Endothelial dysfunction
Brachial Artery Reactivity Testing (BART)
4.7 mm 5.0 mm 5.5 mm
FMV: 6% “ d th d d t”
NMV: 17%“ d th i d d t”“endoth-dependent” “endoth-independent”
FMV after low fat and high fat meal
Effects of statins on FMV, showing improvement after
lowering of serum lipids
Coreti M, JASE 2004;17:693-696Vogel RA, AJC 1997;79:350-354

F tt St k F ti i Ath l iDevelopment of AtherosclerosisDevelopment of Atherosclerosis
Fatty Streak Formation in Atherosclerosis
Ross R. NEJM 1999

F ti f Ad d C li t d L i f Ath l iDevelopment of AtherosclerosisDevelopment of Atherosclerosis
Formation of Advanced, Complicated Lesion of Atherosclerosis
Ross R. NEJM 1999
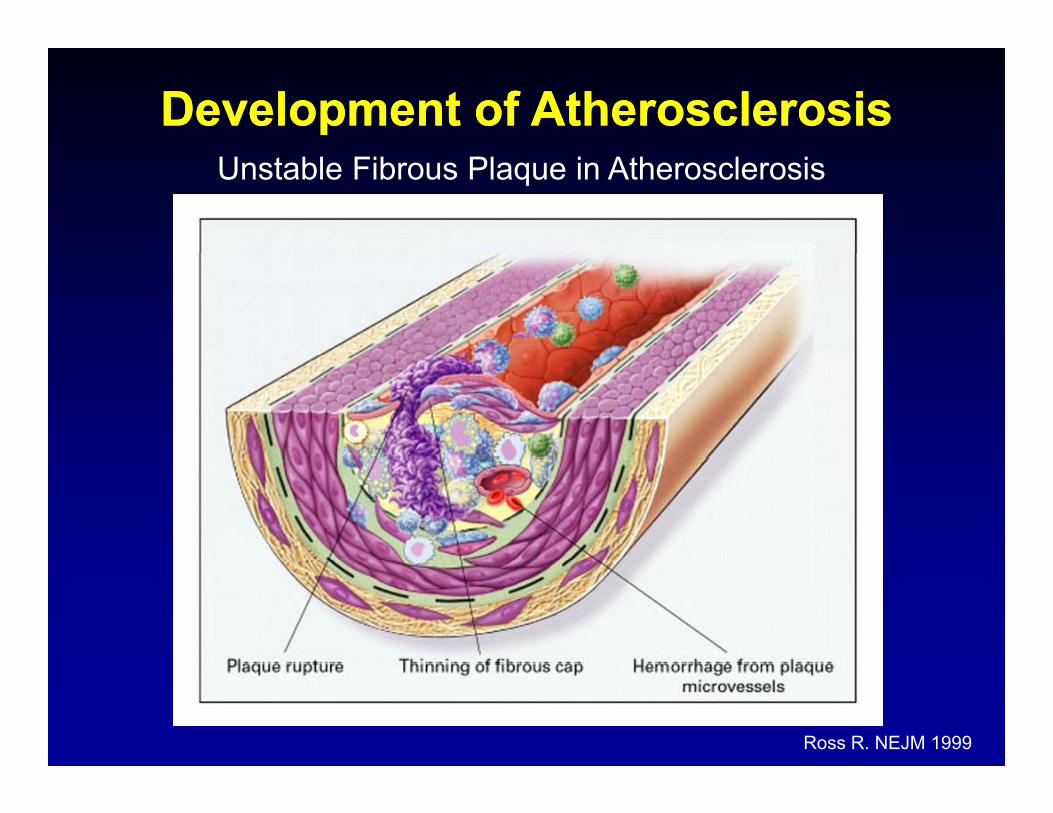
Development of AtherosclerosisDevelopment of AtherosclerosisUnstable Fibrous Plaque in Atherosclerosis
Ross R. NEJM 1999

Coronary heart disease Heart attack
Plaque rupture
y
NormalFattystreak
Fibrousplaque
Atheroscleroticplaque
Plaque rupture &
thrombosis
Increasing age
Heart attack
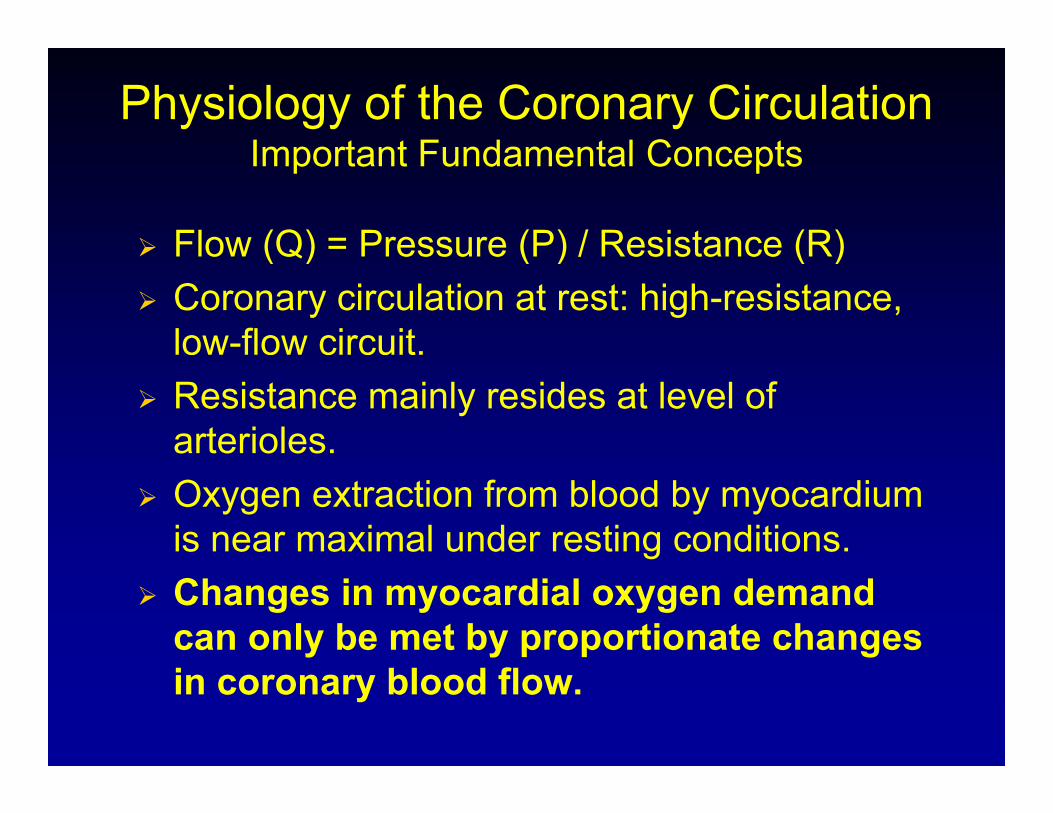
Physiology of the Coronary CirculationImportant Fundamental ConceptsImportant Fundamental Concepts
Flow (Q) = Pressure (P) / Resistance (R) Flow (Q) Pressure (P) / Resistance (R) Coronary circulation at rest: high-resistance,
low-flow circuit. Resistance mainly resides at level of
arterioles. Oxygen extraction from blood by myocardium
is near maximal under resting conditions. Changes in myocardial oxygen demand
can only be met by proportionate changes in coronary blood flow.

Physiology of the Coronary CirculationImportant Fundamental ConceptsImportant Fundamental Concepts
Coronary flow is maintained at a constant, steady state level over a wide range of aorticsteady-state level over a wide range of aortic pressures (coronary “autoregulation”)
Basal coronary resistance in normal vessels can be reduced (and coronary flow increased) 2 to 5-fold by arteriolar vasodilators such as adenosinefold by arteriolar vasodilators, such as adenosine or papaverine, indicating significant reserve that can be recruited under stress.
Coronary flow reserve = ratio of coronary flow at maximal vasodilation (peak hyperemic flow) tomaximal vasodilation (peak hyperemic flow) to flow under resting conditions.

Coronary Flow Catheter
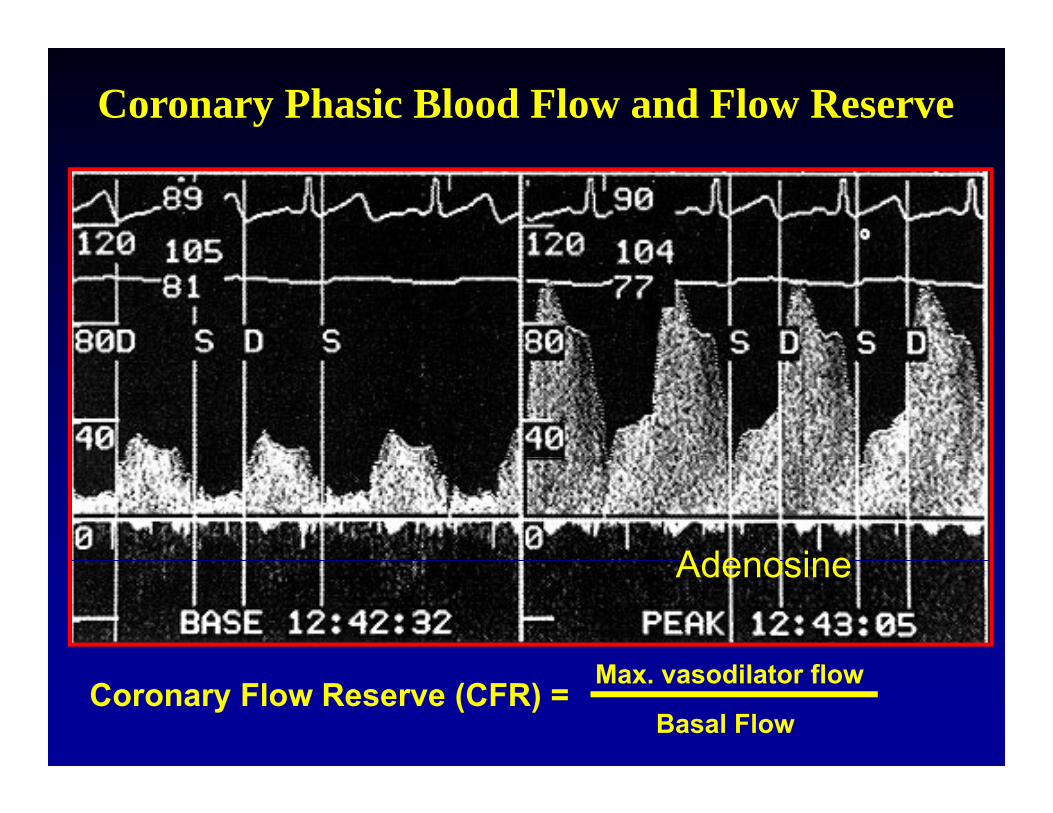
Coronary Phasic Blood Flow and Flow Reserve
AdenosineAdenosine
Coronary Flow Reserve (CFR) = Max. vasodilator flow
Basal Flow

The Concept of Coronary Flow Reserve

Stress Testing for Evaluation of CAD
Myocardial Oxygen Supply/Demand Mismatch

Thalli m Stress TestThalli m Stress TestNoninvasive Evaluation of CAD
Thallium Stress TestThallium Stress Test

Noninvasive Evaluation of CADMultidetectorMultidetector CT (MDCT): CT (MDCT): Coronary Coronary Calcium Calcium
ASC ASC ASCAO
RVOT RVOT RVOTRA
ASCAO
ASCAO AO
LA
No Moderate MarkedCalcification Calcification Calcification

Noninvasive Evaluation of CADMultidetectorMultidetector CT (MDCT): CT Angiography CT (MDCT): CT Angiography
LAD: diffuse mixed calcified and non-calcified plaques (30-40% stenoses)

CHD (or CAD)CHD (or CAD)
AsymptomaticAsymptomaticy py p Stable AnginaStable Angina Acute Coronary Syndromes (ACS)Acute Coronary Syndromes (ACS)
U bl A i (UA)U bl A i (UA) Unstable Angina (UA)Unstable Angina (UA) Myocardial Infarction (MI)Myocardial Infarction (MI)
NonNon ST Segment ElevationST Segment ElevationNonNon--ST Segment Elevation ST Segment Elevation Myocardial Infarction (NSTEMI)Myocardial Infarction (NSTEMI)ST Segment Elevation Myocardial ST Segment Elevation Myocardial I f i (STEMI)I f i (STEMI)Infarction (STEMI)Infarction (STEMI)
The TIMI Study Groupwww.timi.org
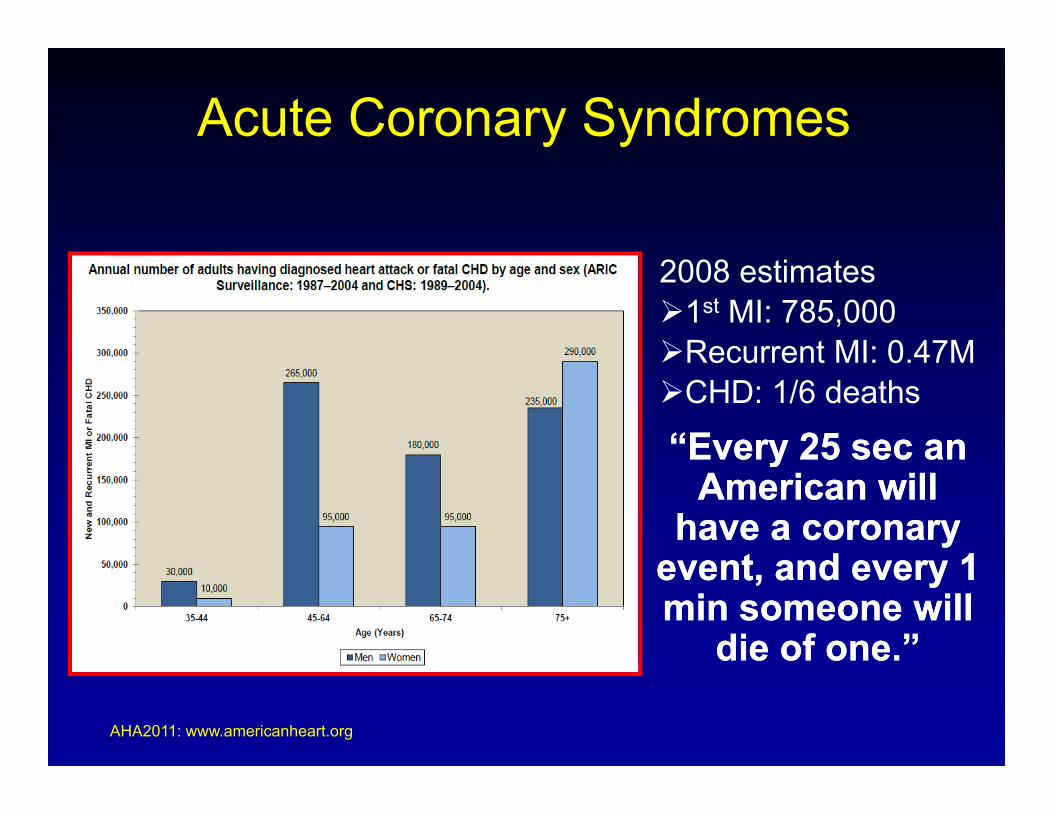
Acute Coronary Syndromes
2008 estimates1st MI: 785,000Recurrent MI: 0 47M
“Every 25 sec an“Every 25 sec an
Recurrent MI: 0.47MCHD: 1/6 deaths
Every 25 sec an Every 25 sec an American will American will
have a coronary have a coronary e ent and e er 1e ent and e er 1event, and every 1 event, and every 1 min someone will min someone will
die of one.”die of one.”
AHA2011: www.americanheart.org

ACS: Role of PlateletsACS: Role of Platelets
Adhesion Aggregation
Fib iFib i
Activated Gpllb/lllaActivated Gpllb/llla
1 3
FibrinogenFibrinogen
PlateletsPlatelets
CollagenCollagenG l /ll bi dG l /ll bi d
von Willebrandvon WillebrandFactor/Gplb bindFactor/Gplb bind
Activation
LipidLipidcorecore
Gpla/lla bindGpla/lla bind
Platelet Plug2 4ct at o
ThrombinThrombin
ADPADP
5 HT5 HT
ate et ug
5 HT5 HT
TXATXA22
Kumar A et al. Exp Opin Invest Drugs. 1997;6:1257–1267.

Acute Coronary Syndromes

Acute Coronary Syndromes

ECG changes in ACSECG changes in ACS
ST elevation MIST elevation MI(STEMI)(STEMI)
NonNon ST elevation MIST elevation MINonNon--ST elevation MIST elevation MI(NSTEMI)(NSTEMI)
Lilly L, Pathophysiology of Heart Disease, p. 159Lilly L, Pathophysiology of Heart Disease, p. 159

Time Course of Serum Cardiac Markers
Lilly L, Pathophysiology of Heart DiseaseLilly L, Pathophysiology of Heart Disease

ACS: Treatment GoalsACS: Treatment GoalsACS: Treatment GoalsACS: Treatment Goals
1. Restore blood flow1. Restore blood flow2. Inhibit thrombus progression2. Inhibit thrombus progressionp gp g3. Relieve pain3. Relieve pain4 R d di l d d4 R d di l d d4. Reduce myocardial oxygen demand4. Reduce myocardial oxygen demand5. Reduce inflammation5. Reduce inflammation

CVD, Hypertension & Heart FailureOutline:I Cardiovascular DiseaseI. Cardiovascular Disease
Epidemiology
II. CHD Acute Coronary SyndromesQUESTIONS?
III. Hypertension / LVH
IV. Heart failure

HTN: Prevalence US Adults, ~75MHTN: Prevalence US Adults, ~75M
AHA2011: www.americanheart.org
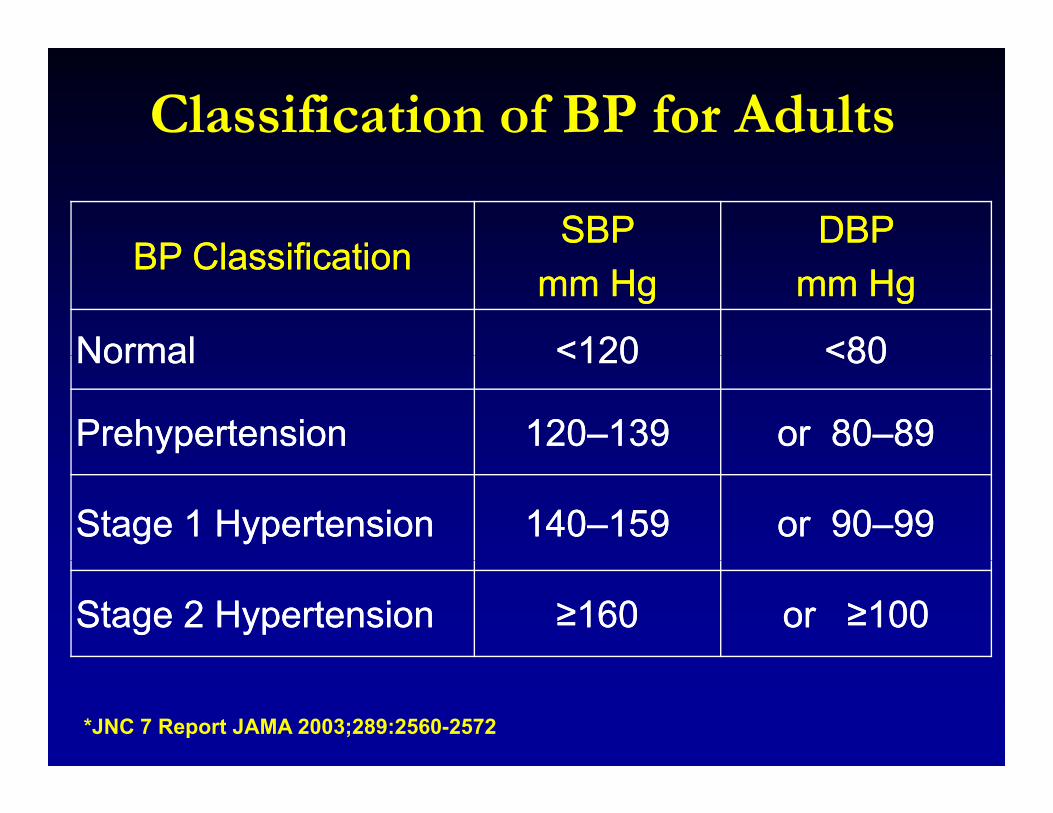
Classification of BP for Adults
BP ClassificationBP ClassificationSBP SBP DBP DBP
BP ClassificationBP Classificationmm Hgmm Hg mm Hgmm Hg
NormalNormal <120<120 <80<80NormalNormal <120<120 <80<80
PrehypertensionPrehypertension 120120––139139 or 80or 80––8989
Stage 1 HypertensionStage 1 Hypertension 140140––159159 or 90or 90––9999
Stage 2 HypertensionStage 2 Hypertension ≥≥160160 or or ≥≥100100
*JNC 7 Report JAMA 2003;289:2560-2572

Cardiac Cardiac HemodynamicsHemodynamics
Syst Diastole4 h4 phases

All Cause MortalityAll Cause MortalityAll Cause MortalityAll Cause Mortality
5Percent Mortality
3 54
4.52x Risk
2.5x Risk
2.53
3.5
NormalBorderline
11.5
2 Definite HTN
00.5
45-54 55-64 65-74 45-54 55-64 65-74
Framingham
Men Women

Cardiac MortalityCardiac MortalityCardiac MortalityCardiac Mortality
3Percent Mortality
2.5 3x Risk5x Risk
1.5
2
NormalBorderline
0 5
1 Definite HTN
0
0.5
45-54 55-64 65-74 45-54 55-64 65-74
Framingham
Men Women

Patient with HTN for 10 yrsPatient with HTN for 10 yrsPatient with HTN for 10 yrsPatient with HTN for 10 yrs
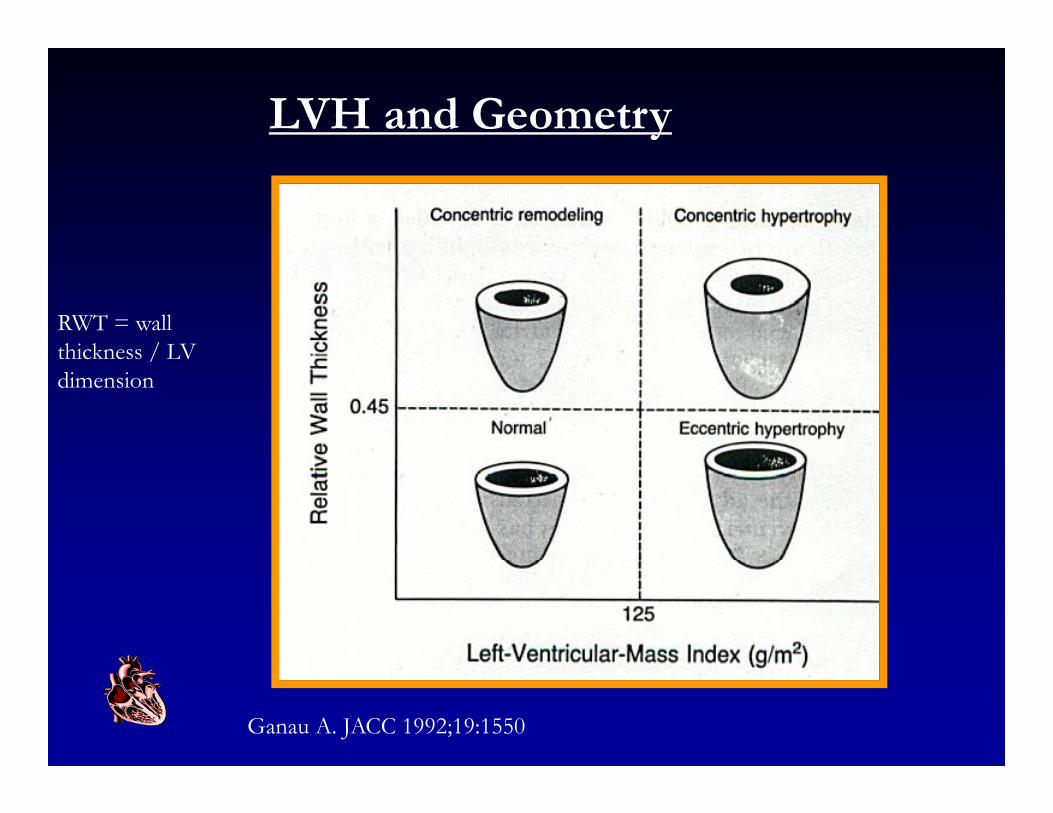
LVH and Geometry
RWT = wall thickness / LVthickness / LV dimension
Ganau A. JACC 1992;19:1550

Left ventricular hypertrophye e cu a ype op y
Asc Ao
LV
LA

Cardiac HemodynamicsAfterload Wall Stress*= P . r / 2h
– Pressure (systemic)
di (LV)– radius (LV)
– wall thickness (h) ( )
*Major Determinant of Myocardial Oxygen Demand*Major Determinant of Myocardial Oxygen Demand
Types of HypertrophyTypes of HypertrophyTypes of HypertrophyTypes of Hypertrophy
PhysiologicPhysiologicexercise inducedexercise induced
PathologicPathologichypertensionhypertension
valvular lesions, coarctationvalvular lesions, coarctation
post myocardial infarctionpost myocardial infarction
idiopathicidiopathic

ExerciseExerciseExerciseExercise
Concentric hypertrophyConcentric hypertrophy
• Eccentric hypertrophyyp p y

Physiological Growth of Heart(Reversible, Good Prognosis in Analysis of
40 Elite Athletes by Echo After Deconditioning)y g)

Poor Prognosis with Pathologic LVHPoor Prognosis with Pathologic LVHLIFE Study: Double blind RCT of 9193 men & women (mean ageLIFE Study: Double-blind, RCT of 9193 men & women (mean age
67y/o) with HTN and LVH by ECG
Severe LVH
Severe LVH
Conclusion: Antihypertensive therapy targeted at LVH regression (or prevention)Conclusion: Antihypertensive therapy targeted at LVH regression (or prevention) may become an additional goal of therapy beyond that of lowering BP, to further
decrease the risk of CV morbidity and mortality.

Clinical Progression of Clinical Progression of Hypertensive Heart DiseaseHypertensive Heart DiseaseHypertensive Heart DiseaseHypertensive Heart Disease
Hypertension CHFLVH
LVDD5M Americans81M Americans
25-50% HTN
LVH & LVDD: M & M compared with HTN alone
25 50% HTN
> 50% increase in CV events 4 - 6 times increased mortality
Fields LE, Hypertension 2004;44:1-7.Koren MJ, Ann Int Med 1991;114:345-352.

Two Major Forms of Cardiac Two Major Forms of Cardiac HypertrophyHypertrophyHypertrophyHypertrophy
Athletic Training Pressure Overload
Enhanced Contractility Diastolic Dysfunction, CHFEnhanced Contractility Diastolic Dysfunction, CHF
Adaptive electrical coupling Poor electrical coupling
Adequate Vascularization Oxygen-poorNo Fibrosis, Fibrosis, embryonicNo Fibrosis,No embryonic geneinduction
Fibrosis, embryonicgene induction (ANP, BNP, MHC)induction )

CVD, Hypertension & Heart FailureOutline:I Cardiovascular DiseaseI. Cardiovascular Disease
Epidemiology
II. CHD Acute Coronary Syndromes
III. Hypertension / LVH - QUESTIONS?
IV. Heart failure

Heart Failure vs. CM
CHF: Clinical DefinitionCHF: Clinical Definition Inability of the heart to pump enough blood to meet
the metabolic demands of the body
C di hCardiomyopathy Disorder of the heart muscle (myocardium) that Disorder of the heart muscle (myocardium) that
may or may not be associated with CHF
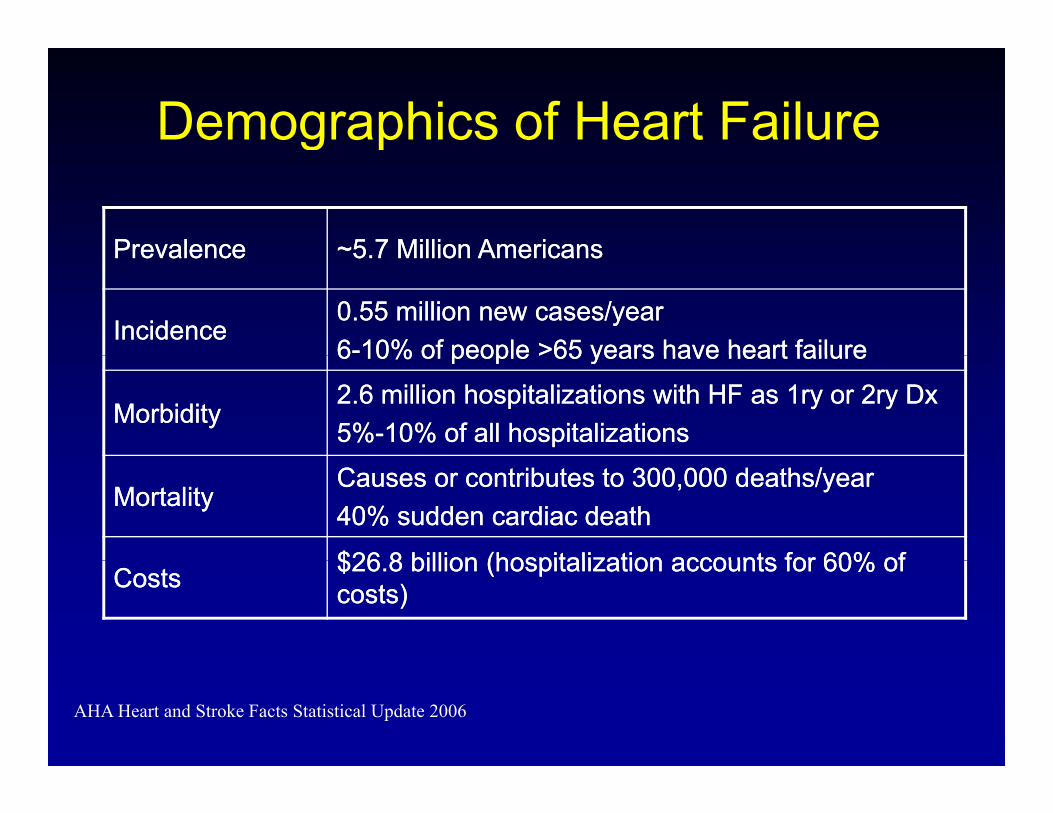
Demographics of Heart Failureg
PrevalencePrevalence ~5 7 Million Americans~5 7 Million AmericansPrevalencePrevalence 5.7 Million Americans5.7 Million Americans
IncidenceIncidence0.55 million new cases/year0.55 million new cases/year66--10% of people >65 years have heart failure10% of people >65 years have heart failure66 10% of people >65 years have heart failure10% of people >65 years have heart failure
MorbidityMorbidity2.6 million hospitalizations with HF as 1ry or 2ry 2.6 million hospitalizations with HF as 1ry or 2ry DxDx5%5%--10% of all hospitalizations10% of all hospitalizations
MortalityMortalityCauses or contributes to 300,000 deaths/yearCauses or contributes to 300,000 deaths/year40% sudden cardiac death40% sudden cardiac death
$26 8 billion (hospitalization accounts for 60% of$26 8 billion (hospitalization accounts for 60% ofCostsCosts $26.8 billion (hospitalization accounts for 60% of $26.8 billion (hospitalization accounts for 60% of costs)costs)
AHA Heart and Stroke Facts Statistical Update 2006

Classification of Heart Failure
5 million HF5 million HF
Systolic HF Diastolic HFy~60% ~40%
Impaired Myocardial ContractilityDecreased SV → Decreased blood flow to Body
Impaired LV fillingPulmonary congestion
flow to Body

Systolic vs. Diastolic Heart FailurePrognosis: long-term mortality in HF hospitalized cohort
SHF 5 li 60 70%SHF, 5-yr mortality: 60-70%
DHF, 5-yr mortality: 50-60%
Hogg K, JACC2004;43:317-327

RV and LV: two pump systems working in parallel
RA
TV
LA
Body capillaries
Lung capillaries
TV MV
RV
LVLV
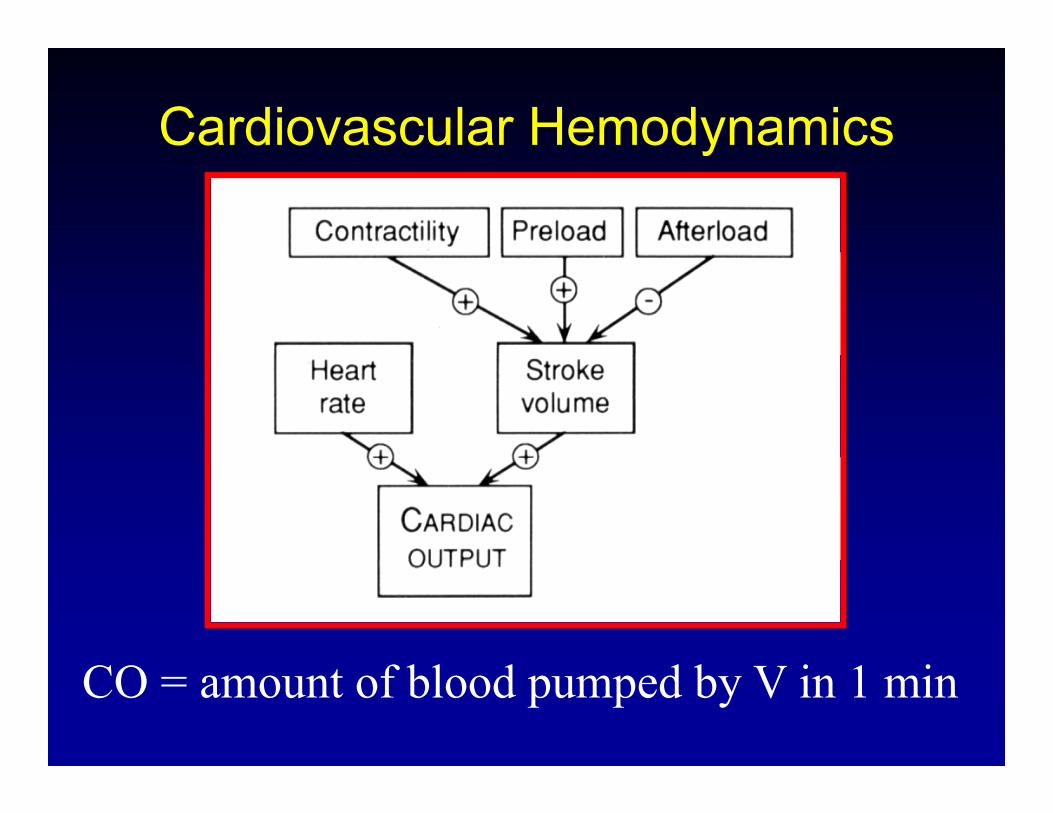
Cardiovascular Hemodynamicsy
CO = amount of blood pumped by V in 1 min
Cardiovascular HemodynamicsPreload
Cardiovascular Hemodynamics
Initial Stretch on Heart prior to Contraction
= End Diastolic Volume (EDV)
= End Diastolic Pressure (EDP)( )
The greater the stretch, EDV, the greater the force
of contraction
Frank-Starling - within physiologic limitsg p y g

Cardiovascular Hemodynamics
Afterload
Ca d o ascu a e ody a cs
Resistance against which the Heart Contracts Resistance against which the Heart Contracts
= Systemic Blood Pressure (SBP) or wall stress
Determines extent to which fibers can shorten
The lower the Afterload the greater the CO The lower the Afterload the greater the CO
(e.g. vasodilator drugs)

Cardiovascular Hemodynamics
Contractility
y
Contractility
Intrinsic Contractile force Intrinsic Contractile force Increased by: inotropic agents
d liadrenalinedobutamine
Reduced by: myocardial Injurybeta blockersbeta blockers

Post MI Left Ventricular Remodeling
Acute MI LVH LVE/LVD
LVHLVE

Geometric Patterns of LVH/CM/HFSmaller LV cavity, marked thickening of wall
Larger LV cavity, eccentric hypertrophy