
Mitochondria Death/Survival Signaling Pathways in Cardiotoxicity

Cardiotoxicity in Drug Development: Cardiac Function Monitoring
Nuclear Core Lab Imaging
Diwakar Jain MD, FRCP, FACC, FASNCProfessor of Medicine and Director of Nuclear
Cardiovascular Imaging LaboratoryDrexel University College of Medicine
Philadelphia

Oncology and Cardiology Cardiologists and oncologists often share the same pt
population Another shared concern: cardiotoxicity associated with
cancer chemotherapy Several forms of cancer therapy can affect
cardiovascular system Two groups of agents are well known for cardiotoxicity:
Anthracyclines HER2 receptor monoclonal antibody (Trastuzmab,
Herceptin) and other TK inhibitors

Anthracyclines Anthracycline glycoside antibiotics are potent broad spectrum
anticancer agents. Doxorubicin (DOX), or adriamycin is the most widely used agent in this category
Cardiotoxicity, characterized by progressive LV dysfunction & CHF which in extreme cases can be fatal is a well recognized clinical entity limiting the use of all anthracyclines
Dose related with significant inter-individual variability
Life-time cumulative dose the best predictor for CHF:
3% at 300mg/m2, 7% at 450mg/m2, 20% at 600mg/m2
Risk factors: age, pre-existing heart disease, thoracic irradiation, combined use of other agents: high dose cyclophosphemide, taxanes, herceptin

Anthracyclines Mechanism of cardiotoxicity:
Sarcoplasmic Ca++ overload Binding to topoisomerases
Oxidative damage: Redox cycling Approaches to reduce cardiotoxicity:
newer DOX analogues slow iv infusion over 24-72 hrs iron chelators (Zinecard) and antioxidants liposome-incorporated DOX
Close LVEF monitoring and prompt discontinuation at the appearance of a predetermined fall in LVEF

Cum Dox dose and lowest LVEF
10
20
30
40
50
60
70
80
Low
est
LVEF
0 100 200 300 400 500 600 700 800 900Adria final dosage
CHFNo CHF
n=265

At-Risk v Non-Risk Pts
Variables
nAge (yrs) FemalesPrior CV Dis (Hypertension, MI)Dox Total Dose (mg/m2)Overt CHFHosp admission for CHFCardiac DeathCancer Related DeathsFollow up from last DOX DoseNumber of ERNAsBaseline LVEF (%)Lowest EF During Follow up(%)
At-Risk41 (15% )53±1428 (68% )12 (29% )304±1245 (12% )2 ( 5% )1 (2.5%)24 (59% )691±4453.9±1.558±842±8
Non-Risk224 (85% )54±16173 (78% )
39 (17% )284±110
2 ( 1% )1 (0.4%)066 (30% )
676±4243.2±1.364±857±7
P0.6
0.20.060.3<0.00010.010.020.00030.80.002<0.0001<0.0001
No difference in D Mellitus, Prior DOX Therapy Cytoxan Therapy, Dexrazoxane Therapy & Mediastinal Irradiation

0
50
100
150
200
250
300
ERNA#1ERNA#2ERNA#3ERNA#4ERNA#5ERNA#6ERNA#7ERNA#8ERNA#9ERNA#10
RiskNon-Risk
Sequential ERNA and pts at risk
Mitani I et al. JNC 2000

Overt CHF preceded by subclinical LV dys, which is rapidly progressive with continuation of therapy, but can be arrested by prompt discontinuation of offending agent
Need for close LV function monitoring during therapy using a technique which can reliably detect subclinical LV dysfunction
Serial LVEF monitoring with ERNA continues to be the only cost effective approach for the prevention of cardiac morbidity and mortality from DOX chemotherapy
LV Function Monitoring

Guidelines for LVEF Monitoring during Dox Therapy
Bsl EF
Bslat 250-300mg/m2
At 450 mg/m2 *Prior to each subsequent dose
BslPrior to each subsequent dose
Avoid doxorubicin
At Risk for CHF
Nl≥50%
ERNAs
* At 400 mg/m2 with Known heart disease, hypertension, radiation exposure, ab ECG, cyclophosphamide therapy
30- <50%
<30%
≥10% EF Fallto <50%
≥10% EF fall or EF <30%
Schwartz R et al. Ann of Int Med 1985

Prevention of DOX Cardiotoxicity
Free radical injury mediated mechanism thought to contribute towards DOX cardiotoxicity
Iron forms a complex with drug resulting in generation of free radicals
Contribution of body iron stores towards DOX cardiotoxicity is not clear
Higher body iron stores are strongly suspected to potentiate DOX cardiotoxicity

5
Inj
wks 0 4
Sacrifice
Multi DOX Dose (2.5 mg ip twice/wk x 4 wks, cum 20 mg/Kg)
Inj
wks 0 3
Sacrifice
2
Single 6mg iv DOX Dose
DOX cardiotoxicity in Iron Loaded rats
Imaging
Mortality,wt. change &histology
Imaging
Mortality,wt. change &histology
Panjrath G et al JACC 2007

Body wt. Changes
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Multi DoseSingle Dose
-0.2
-0.15
-0.1
-0.05
0
0.05
0.1
0.15
0.2
% b
ody
wt.
chan
ge
1 2 3
saline iron DOX DOX + iron
wks
% b
ody
wt.
chan
ge5
saline iron DOX DOX + iron
wks

EM
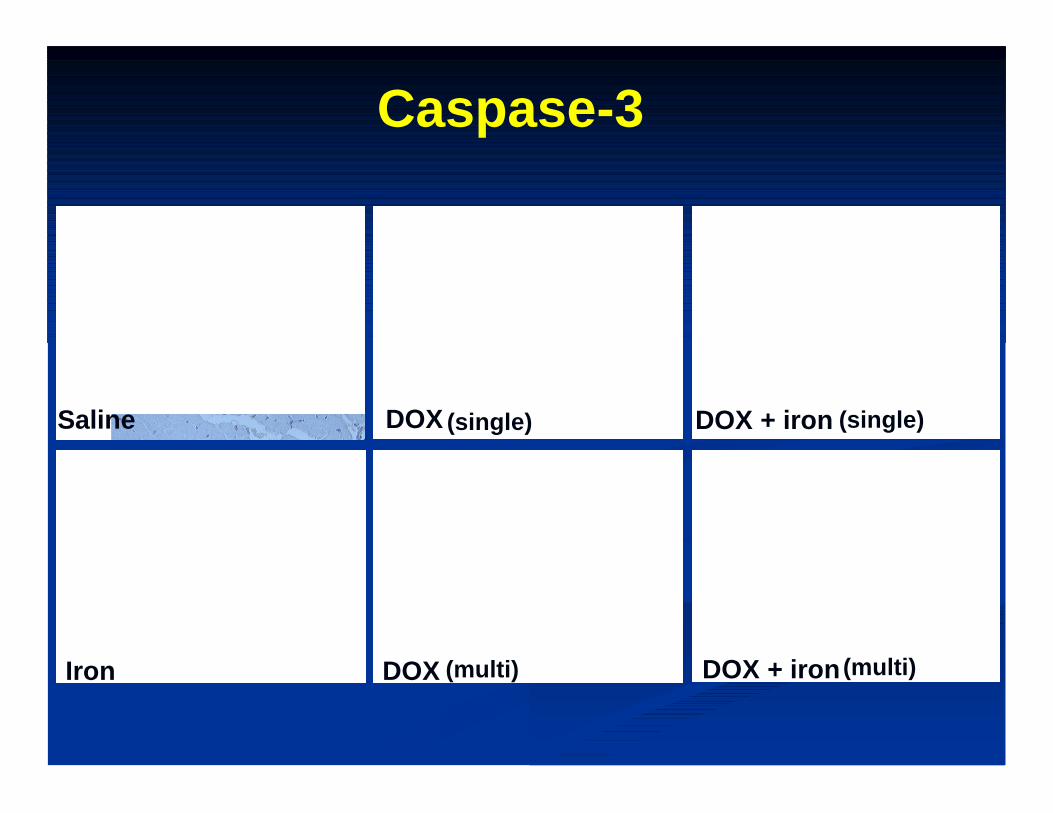
Caspase-3
Saline DOX
DOXIron
DOX + iron
DOX + iron
Saline (single)
(multi)
(single)
(multi)

Body Iron and Dox Cardiotoxicity
Body iron stores and iron bioavailability may be important determinants of DOX cardiotoxicity
HFE+/+ 1 in 250 but HFE+/- 7%, HD+/- 20%
Blood transfusions, iron supplementations common in cancer pts
More appropriate and logical use of iron chelators for preventing DOX cardiotoxicity

Trastuzumab• Humanized monoclonal antibody• Binds selectively to human epidermal growth factor-2
(HER2 also known as ErbB2) • Amplification of HER2 gene in ≈20% of breast Ca• HER2 encodes a membrane transporter belonging to
the family of tyrosine kinases• Used to treat HER2 over-expressing metastatic breast
Ca as a monotherapy or with anthracyclines• efficacious in increasing median survival times• Given as weekly iv injections starting during the
course of chemotherapy or soon after the completion of initial chemotherapy for 9-12 months

Mechanism of Trastuzumab Induced Cardiac Dysfunction
• Not fully known• Important difference with anthracycline cardiotoxicity• HER receptors form a group of receptors present on the
myocardium, involved in cell survival under stress challenge
• Blockage of cell survival receptors predispose myocytes to apoptosis particularly when challenged by other cardiotoxic agents
• This property may be shared with other TK receptor blocking agents
• Recently Gleevec another TK inhibitor has been found to have cardiotoxicity

Panjrath G et al NMC 2006

Cardiotoxicity of TK inhihitors Over-expression of PDGFR in several cancers, which
promotes cell growth Several chemotherapeutic agents imatinib (Gleevec),
Sunitnib (Sutent), Sorafinib (Nexavar) target tumor PDGFR receptors, which slows tumor growth
PDGFR expression and activation in the myocardium is also associated with angiogenesis
PDGFR expression increases in response to pressure overload
Cardiac PDGFR KO mice developed heart failure on pressure overload with aortic banding
Khakoo A et al. JCI 2010

Conclusion Cardiotoxicity continues to be a major issue with
the use of anthracyclines: Body iron content is an important determinant of DOX cardiotoxicity
Newer anticancer drugs such as trastuzumumab also have significant cardiotoxicity
Need for closer observation of newer monoclonal antibodies and TK inhibitors for potential cardiotoxicity
Need for further research to better understand the mechanisms and prevention of cardiotoxicity

Conclusions Meanwhile close LV function monitoring with
serial ERNA using the recommended guidelines can be used to effectively reduce the incidence of overt CHF
Currently no large central data bases exist regarding LV function, cancer chemotherapy and cardiotoxicity
There is a critical need for the creation of such data bases to gain better insight into therapy induced cardiotoxicity and to keep up with the changing trends in this field



















